Embed Size (px)
Citation preview

CASE REPORT
Discospondylitis and Orchitis Associated withHigh Brucella Titre in a Dog
G.I. ANDERSON AND A.G. BINNINGTON
Department of Clinical Studies, Ontario Veterinary College, University ofGuelph, Guelph, Ontario Ni G 2 WI
SummaryA case of discospondylitis and
orchitis associated with high Brucellatitre in a dog is presented. Clinicalsigns included intermittent pain, poorappetite and a decreased level of phys-ical activity. Radiographic evidence ofdiscospondylitis was found. Histopa-thological findings on the testes areincluded. Treatment regime and clini-cal progress are given. Diagnosis andtreatment of B. canis are described anda brief review of the treatment of dis-cospondylitis is presented.
ResumeDisen-spondylite et orchite associees aun taux eleve d'anticorps a 1'endroit deBrucella, chez un chien
Cet article presente un cas de disco-spondylite et d'orchite associees 'a untaux eleve d'anticorps a l'endroit deBrucella, chez un chien qui manifestaitles signes cliniques suivants: douleurintermittente, anorexie et reduction del'activite physique. Des radiographiesdemontrerent des lesions de disco-spondylite. L'article enumere leslesions testiculaires microscopiques; ildonne aussi le genre de traitementqu'on administra au chien et lesprogres cliniques qu'il enregistra; ildecrit egalement le diagnostic et letraitement de la brucellose canine; ilpresente enfin une breve revue dutraitement de la disco-spondylite.
IntroductionBrucella canis infection in bitches
causes abortion and infertility, whilstin males, infertility is due to abnormalsperm production with decreasedmotility. Male dogs may show signs of
orchitis, epididymitis and scrotal swel-ling (1,2,3). In systemic Brucella infec-tion lymphadenitis, splenitis, nephritisand osteomyelitis/discospondylitismay occur (3).
Information on the incidence of B.canis is scarce. A recent survey of 2 000dogs in southern Ontario, indicatesthat 0.3% of sera tested showed sero-logical evidence of B. canis infection(4), but only one animal had a tubeagglutination titre greater than 1:200.Results of a serological survey inQuebec using 341 dogs suggest that1.6% of dogs had a significant titrewith the mercaptoethanol tube agglut-ination test (5). Only two dogs showedtitres of greater than 1:200, which isconsidered indicative of active infec-tion (3,6,7,8). This unusual case isreported here to draw attention to theability of B. canis to cause discospon-dylitis in the dog in Canada.
Case HistoryA three year old Golden Retriever
cross intact male dog was presented atthe Ontario Veterinary College (OVC)with a history of episodes of pain forfour months. The owner reported thatthe dog did not exhibit signs of pain atrest but that the level of voluntaryexercise had reduced along with theappetite.
Four months prior to presentationthe dog had been treated for orchitiswith a seven day course of oral tetracy-clines. At that time the referring vete-rinarian had noticed one testis to beenlarged and painful on palpation.There was no evidence of scrotal der-matitis. In the four month periodbetween the onset of signs and presen-
tation at OVC the dog was seen by thereferring veterinarian for episodes ofstiffness and pain involving theshoulder or the cervical region. Radi-ographic examination of both regionshad revealed no lesions. Results ofhematological and blood chemistryexaminations performed on theseoccasions were within normal limits.
Clinical SignsOn physical examination the dog was
in good bodily condition although itwas reported to have lost weight in themonth prior to presentation. It was afe-brile (38.70C) with a dry haircoat andmild bilateral otitis externa. On deeppalpation of the anterior abdomen, itexhibited discomfort but failed to reactto any other manipulation or palpation.However, on being lifted from theexamination table, the dog exhibitedpain associated with the movement ofthe thoracolumbar (T-L) spine. Deepdigital palpation of this area elicitedpain and inconsistently reproduciblecrepitus. Neurological examinationrevealed no abnormalities.
Laboratory FindingsA complete blood count, biochemi-
cal profile, urinalysis and fecal exami-nation were performed. (TablesI,I ,1II,IV and V). Radiographicexamination was carried out underdroperidol-fentanyl' sedation.The results of hematology, bio-
chemical profile and urinalysis werenormal. The endoparasitic infectionAncylostoma caninum, Trichuris vul-pis, Toxocara canis was treated withan anthelmintic preparation.2
'Innovar-vet, Pitman-Moore Ltd., Scarborough, Ontario.2Pyr-A-Pam plus, Rogar/STB division of BTI Products Inc., London, Ontario.
Can Vet J 1983; 24: 249-252 249

TABLE IHEMATOLOGICAL VALUES ON INITIAL
PRESENTATION OF A DOG WITH ORCHITISAND DISCOSPONDYLITIS
Complete Blood Normal ValuesCount Test at OVC
WBC (109/L) 9.3 6.6 - 1.84RBC (10'2/L) 7.18 5.5 - 8.2Hb (g/L) 178 126 - 194Hct (L/ L) 0.47 0.37 - 0.55MCV (fL) 66 62 - 70MCH (pg) 24.6 22 - 25MCHC (g/L) 371 330 - 360
Radiological ResultsAbnormalities were not seen on
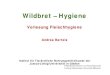
abdominal radiographs. On the thora-columbar radiographs there was nar-rowing of the intervertebral disc spaceat T12-Ti3 with sclerosis of adjacentarticular surfaces and spondylosis ven-trally on both vertebral bodies. Asmall lytic area was seen on the cranialarticular surface of T13. The lytic areawas presumed to be due to osteomyeli-tis and the spondylitis due to instabil-ity between the two vertebral bodies.
Serological ResultsWith the prior history of orchitis
and current radiographic evidence ofdiscospondylitis, blood was taken fora B. canis screening test [rapid slideagglutination test-serum aspartatetransminase (SAT)].3 The result waspositive. Further blood was submittedfor the tube agglutination test [mer-captoethanol tube agglutination test(ME-TAT)]. The ME-TAT yielded atitre of 1:400.
Treatment and ResultsThe dog was discharged from OVC
with a positive SAT but whilst stillawaiting the ME-TAT result. Hometreatment consisted of oral tetracy-cline hydrochloride4 at 60 mg/ kgdivided into three daily doses, untilconfirmation of the SAT by the mer-captoethanol tube agglutination testwas received. After one week of anti-biotic therapy there was clinicalimprovement. When the ME-TATtitre of 1:400 was received, the dogreturned for a six day course of dihy-drostreptomycin5 intramuscularly at20 mg/kg twice daily (9,10). Oral
TABLE IIDIFFERENTIAL WHITE BLOOD CELL COUNT ON
PRESENTATION OF A DoG WITH ORCHITISAND DISCOSPONDYLITIS
Normal Valuesat OVC
(109/L) (%) (109/L) (%)Basophils 0 0% 0.0- 0.2 0- 1%Eosinophils 0.56 6% 0.0- 1.9 0-14%ImmaturePMNs 0.47 5% 0.0- 1.0 0- 5%
Lymphocytes 1.86 30% 0.8- 5.6 10-40%MaturePMNs 4.5 49% 3.9-12.0 46-76%
Monocytes 0.93 10% 0.1- 1.8 1-14%
tetracycline hydrochloride was con-tinued during this second period ofhospitalization and the dog was cas-trated. Due to lack of libido, semensamples were not obtained from thedog before castration.
Radiographs taken on readmissionshowed further spondylitic bridgingventral to T12-T 13 and increased scle-rosis of the endplates. Oral tetracy-clines were continued for 25 days. Thedog continued to improve clinically athome and eight weeks posttreatmentremained free of pain and active.A telephone recheck five months
after cessation of treatment found thedog asymptomatic. Repeat serologyposttreatment, unfortunately, was notobtainable as the owner and dog hadmoved out of the district.
A:G RatioAlbumin (g/dL)Amylase (, / L)Calcium (mmol/ L)Cholesterol (mmol/ L)Conjugated bilirubin (,imol L)CPK (i/L)Creatinine (,uLmol / L)Free Bilirubin (,umol/ L)Glucose (mmol/ L)Phosphorus (mmol / L)SAP (U/ L)SAST (U/ L)SALT (U/ L)Total bilirubin (j,mol/ L)Total protein (g/ L)Urea (mmol/ L)
Histopathological FindingsThe testes removed at surgery were
grossly normal measuring approxi-mately 4 cm in diameter. Lesions inboth testes were similar, consisting ofdiffuse tubular degeneration andatrophy. There was very little evidenceof spermatogenesis. Interstitial edemaand postnecrotic foci were seenbetween the tubules. The epididymallesions were characterized by multifo-cal lymphocytic and mononuclear cellinfiltrations in the interstitium (I1).The epididymal epithelium was nor-mal. Intracellular B. canis organismswere not observed on Gram stainedpreparations of testicular tissue. A his-topathological diagnosis of chronicmultifocal interstitial orchitis and epi-didymitis was made.
DiscussionBrucella canis may cause inapparent
infection or discospondylitis andorchitis as in this dog. Diagnosis in thiscase was based on the history of orchi-tis, discospondylitis, testicular andepididymal lesions in conjunction withthe positive SAT and ME-TAT. Sus-picious animals can first be screenedusing the rapid slide agglutination testavailable in a commercial kit. TheSAT gives a percentage of false posi-tives but is efficient in identifying neg-ative, or noninfected, dogs (1). Serumsamples positive on SAT should be
Test
0.630
11362.884.710.0
7688.41.04.61.32
8837.0241.0
826.07
NormalRangeat OVC
0.6 1.2024 - 36
740 - 16702.57 2.973.23 7.890.0 - 3
30 - 25060 - 1100 - 0.33.8 - 5.90.81 - 1.87
40 - 3508 - 389 - 450 - 3
52 - 691.8 - 10.4
3Canine Brucellosis Diagnostic Test, Pitman-Moore, Inc., Washington Crossing, New Jersey.
4Tetracycline HCI, Sounds, Div Terram Pharmaceuticals Ltd., Toronto, Ontario.
5U Streptomycin injection, Pfizer Canada Inc., Montreal, Quebec.
250
TABLE IIISERUM CHEMISTRY RESULTS ON PRESENTATION OF A DOG WITH ORCHITIS AND DISCOSPONDYLITIS
FIGURE 1. Thoracolumbar spine. The disc space at TI2-13 is narrowed, the vertebral end plates aresclerotic and roughened and early ventral bridging between T12-T13 is seen. Small lytic area ispresent on cranial articular surface of T13.
checked using the mercaptoethanoltube agglutination test. Sera givingreactions in dilutions of 1:200 orgreater are considered positive, inaccordance with the guidelines estab-lished by the World Health Commis-sion on Brucellosis (3,6,12,13). Tomake a definitive diagnosis, culture ofB. canis from semen, testicular tissuesor blood, or visualization of intracellu-lar Brucella organisms in the testiculartissue sections would be necessary.Attempts at semen collection and cul-tures of tissues in this case were unsuc-cessful. However, these attempts weremade after initiation of antibiotictherapy. In chronic cases of brucello-sis, the bacteremia is intermittent soeven serial blood cultures may beunsuccessful (1,2).Although B. canis organisms were
not seen on histopathological sections,the lesions are compatible with thoseof B. canis epididymitis and orchitis.Again, antibiotic therapy prior to cas-tration, may have interfered with tes-ticular cultures and / or visualization ofthe organism on Gram-stainedsections.Although the dog had a ME-TAT of
1:400 indicative ofactive infection andosteomyelitis, orchitis and epididymi-tis all highly suggestive of B. canisinfection, a presumptive diagnosisonly can be made (1).
Brucella canis, being an intracellu-lar organism, can be difficult to elimi-nate, especially from prostatic andosseous tissue (2). The response tocombination antibiotic therapy is sim-ilar to previous reports (9,10). Toestablish whether the organism hadtruly been eliminated in this case,serial serology at bimonthly intervalswould be necessary (2). Unfortunately,as the owner and dog moved out of thedistrict, this was not possible. A tele-
phone report made five months post-treatment found the dog to be clini-cally normal and active; presumptiveevidence only that, at that stage, thedog was free of B. canis infection andback pain. In the healing of disco-spondylitis vertebral fusion or bridg-ing occurs resulting in the eliminationof instability and pain (12,14).Dogs in which there was minimal
neurological dysfunction, have beensuccessfully treated with antibioticsalone, although curettage and antibio-tics give more reliable results wherethere is a single lesion (14,15,16). Indogs with marked neurological dys-function, treatment has involved hemi-laminectomy, vertebral immobiliza-tion and prolonged antibiotic treat-ment. Success rates in dogs withneurological dysfunction were muchlower.Two cases of B. canis discospondyli-
tis have been treated successfully withlaminectomy, currettage and a 30 daycourse or oral tetracycline hydrochlo-ride (17). The ME-TAT titre fell from1:200 at surgery to 1:40, 28 weeks post-surgery in one case with good clinicalimprovement.
Prognosis with discospondylitisdepends on two factors: (a) the easewith which the infecting organism canbe eliminated from body tissues and(b) the degree of neurological dysfunc-tion present.
In this dog there were no neurologi-cal deficits despite the chronicity ofthe
TABLE IVURINALYSIS OF FREE FLOW SAMPLE ON PRESENTATION OF A DOG WITH
ORCHITIS AND DISCOSPONDYLITIS
UrinalysisAcetoneBloodBileGlucoseGross appearance
pHProteinSp gr
CytologyBacteriaBacteria in catheterized sampleCrystalsErythrocytesGlitter cellsNeutrophilsRenal epithelial cellsSquamous epithelial cellsTransitional cellsUrine culture
negativenegativenegativenegative
- slightly cloudydark yellow
6.0negative1.055
occasionalnil
- low numbers triple phosphate crystalsnil
- low numbers- 3-4 cells per high power field
niloccasionaloccasional
- no bacterial growth achieved
251

FIGURE 2. Radiograph taken ten days after initial examination. There is increased bridging ven-trally, decreased roughening and increased sclerosis of end plate areas of both T12 and T13.
signs. Brucella canis, however, can bevery difficult to eliminate from alltissues because of its intracellularnature. Despite the early clinicalimprovement with tetracyclines anddihydrostreptomycin, recurrence isstill possible. Serial negative bloodcultures, falling titres and radiogra-phic evidence of healing would benecessary before success could beclaimed. Whenever there is a history oforchitis and discospondylitis occur-ring in the dog, there should be a highindex of suspicion of B. canis involve-ment and Brucella serological testingis indicated.
References1. CARMICHAEL LE. Canine brucellosis - an
annotated review with selected cautionarycomments. Theriogenology 1976; 6:105-116.
2. FLORES-CASTRO R, CARMICHAEL LE. Caninebrucellosis: current status of methods ofdiagnosis and treatment. Gaines Vet: Sym-posium in Conjunction with Texas A&MUniversity Veterinary College, 1977; 27:17-24.
3. HUBBERT NL, BECH-NELSON 0, BARTA 0.Canine brucellosis: comparison of clinicalmanifestations with serological test results.J Am Vet Med Assoc 1980; 177: 168-171.
4. BOSU WTK, PRESCOTT JF. A serological sur-vey of dogs for Brucella canis in southwest-ern Ontario. Can Vet J 1980; 21: 198-200.
5. HIGGINS R, HOQUET F, BOURQUE R, GOSSELINY. A serological survey for Brucella canis inthe province of Quebec. Can Vet J 1979; 20:315-317.
6. FREDRICKSON LE, BARTON CE. A serologicsurvey for canine brucellosis in a metropoli-tan area. J Am Vet Med Assoc 1974; 165:987-989.
7. MUNFORD RS. Brucella canis infects man. JAm Med Assoc 1975; 231: 1267.
8. THIERMAN AB. Brucellosis in stray dogs inDetroit. J Am Vet Med Assoc 1980; 177:1216-1217.
9. JENNINGS PB, CRUMRINE MH, LEWIS GE.FARISS BL. The effect of a two-stage antibio-tic regime on dogs infected with Brucellacanis. J Am Vet Med Assoc 1974; 164:513-514.
10. LEWIS GE, CRUMRINE MH, JENNINGS PB,FARISS BL. Therapeutic value of tetracyclineand ampicillin in dogs infected with B.canis. J Am Vet Med Assoc 1973; 163:239-241.
11. RHOADES HE, MESFIN GM. Brucella canisinfection in a kennel. Vet Med Small AnimClin 1980; 75: 595-599.
12. HUROV L, TROY G, TURNWALD G. Discospon-dylitis in the dog -27 cases. J Am Vet MedAssoc 1978; 173: 275-280.
13. CANINE BRUCELLOSIS: Current status. J.A.Baker Institute Report. Ithaca: New YorkState College of Veterinary Medicine. Sep-tember 1976.
14. GAGE ED. Treatment of discospondylitis indogs. J Am Vet Med Assoc 1975; 166:1164-1169.
15. KORNEGAY JN. Canine discospondylitis.Compend Contin Educ Small Anim Pract1979; 1:930-933.
16. KORNEGAY JN. BARBER DL. Discospondylitisin dogs. J Am Vet Med Assoc 1980; 177:337-341.
17. HENDERSON RA, HOERLEIN BF, KRAMER TT,MEYER ME. Discospondylitis in three dogsinfected with Brucella canis. J Am Vet MedAssoc 1974; 165: 451-454.
DEMANDE DE FONDS DE RECHERCHENous invitons les demandes de fonds de recherche sur les maladies ani-
males au Canada. Les demandes doivent nous parvenir avant le 30 novembre.Pour plus de renseignements et pour obtenir des formules de demande,
s'adresser au:SecretaireLa fondation canadienne pour la recherche veterinaire339, rue BoothOttawa (Ontario) Kl R 7K1
252




![Epididymitis Due to Bilateral Ectopic Vas Deferens …orchitis episodes. Discussion Epididymitis is associated with anorectal malformation in 1.2-6.1% [2]. This uncommon urologic condition](https://img.pdfslide.net/doc/110x75/5f37581ebe40af7a227a9d32/epididymitis-due-to-bilateral-ectopic-vas-deferens-orchitis-episodes-discussion.jpg)