Embed Size (px)
Citation preview

Central Annals of Otolaryngology and Rhinology
Cite this article: Zucker I, O’Sullivan B, McConn Walsh R, O’Neill JP (2015) High Risk Cutaneous Squamous Cell Carcinomas of the Pinna with Dissemination to the Temporal Bone Contemporary Oncological Management. Ann Otolaryngol Rhinol 2(7): 1049.
*Corresponding authorJames Paul O’ Neil,Department of Otolaryngology:Head and Neck Surgery, The Royal College of Surgeons, RCSI Education & Research Centre, Beaumont Hospital, Beaumont, Dublin 9, Ireland, Tel: 01-8093738; Email
Submitted: 15 June 2015
Accepted: 13 July 2015
Published: 14 July 2015
Copyright© 2015 O’Neill et al.
OPEN ACCESS
Keywords•Temporal bone malignancies•External auditory canal•Lateral temporal bone resection•Facial reconstruction
Case Report
High Risk Cutaneous Squamous Cell Carcinomas of the Pinna with Dissemination to the Temporal Bone Contemporary Oncological ManagementIsaac Zucker1, Barry O’Sullivan2, Rory McConn Walsh1 and James Paul O’Neill1*1The Department of Otolaryngology: Head and Neck Surgery, The Royal College of Surgeons, Ireland2The Department of Plastic and Reconstructive Surgery, The Royal College of Surgeons, Ireland
Abstract
Background: Temporal Bone Malignancies (TBMs) are a rare but distinct set of neoplasms with a multifactorial etiology.
Case Presentation: We report a case of a present a case of 62 year old male with high risk squamous cell carcinoma of the pinna which despite primary surgery and adjuvant radiation disseminated into the temporal bone requiring combined salvage surgery.
Discussion: The Etiology, symptoms, staging system and surgical procedure of TBMs are discussed along with a detailed review of the three-team approach involving a neuro-otology surgeon, head and neck oncologic surgeon and plastic surgeon, are discussed in approaching surgery of TBMs.
Conclusion: In our center a multidisciplinary approach including a neuro-otology surgeon, head and neck oncologic surgeon and plastic surgeon are essential for surgical salvage resection and reconstruction of TBMs.
ABBREVIATIONSTBM: Temporal Bone Malignancies; EAC: External Auditory
Canal; SCC: Squamous Cell Carcinoma; FNAB: Fine Needle Aspiration Biopsy; PET: Positron Emission Tomography; TMJ: Temporomandibular Joint; LTBR: Lateral Temporal Bone Resection; STBR: Sub Temporal Bone Resection
INTRODUCTIONTemporal Bone Malignancies (TBMs) are a rare set of
neoplasms that account for 0.2% of all head and neck malignancies [1]. The suggested etiology is multifactorial including ionizing radiation of the external auditory canal (EAC) and pinna along with a hypothesized genetic susceptibility for people not exposed to radiation [2]. TBMs are not restricted just to the EAC; although primary malignant tumors of the temporal bone are rare, cutaneous cancers spreading to the temporal bone are a problem that deserves more attention as they are reportedly more aggressive than those arising in other areas of the skin [3].
CASE PRESENTATIONA 62-year old male was referred from another tertiary
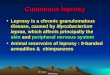
center with a history of squamous cell carcinoma (SCC) of the left pinna and EAC. Previous surgery was performed on a poorly differentiated baso-squamous cell carcinoma in which a subtotal pinnectomy and superficial parotidectomy were performed with reconstruction with a local rotation flap and a split skin graft. Pathology noted a close margin in their report. Following the surgery, adjuvant chemoradiation therapy was completed. The patient returned 6 months later with a fluctuant swelling over the superior pinna remnant for the previous 2 months. A Fine Needle Aspiration Biopsy (FNAB) and PET/CT scan was performed (SUV 7.4) which confirmed recurrence (Figure 1).
SURGERYThe patient was discussed at the Multi-disciplinary Oncology
meeting where it was agreed salvage surgery would be required incorporating radical parotidectomy, facial nerve sacrifice,

Central
O’Neill et al. (2015)Email:
Ann Otolaryngol Rhinol 2(7): 1049 (2015) 2/3
modified radical neck dissection and lateral temporal bone resection. Plastic surgery proposed an anterolateral thigh flap for reconstruction along with facial nerve reanimation. This included a brow lift, mid facial lift, lower lid tarsorraphy with 1.8-gram weight inserted. Surgery was performed with clear oncological margins and no morbidity in the post-operative recovery time period.
DISCUSSION TBMs are a rare set of tumors that only account for 0.2%
of all head and neck malignancies [1]. Most tumors arise from squamous cells (43%); however basal cells and melanoctyes are also common origins [1]. The epidemiology of the disease is multifactorial with ionization radiation of the EAC and the pinna, and a higher predisposition if previous radiotherapy of the head and neck has been performed. A genetic susceptibility has also been hypothesized [2]. The signs and symptoms of TBMs are usually non-specific and are often diagnosed quite late after the cancer occurs [3].The symptoms include aural discharge or bleeding (24-100%), otalgia (19-81%), hearing loss (2-75%) and facial nerve palsy (7-64%) [1-3].
Due to the rarity of this disease, there has been no recognized staging system. For TBMs of the squamous cell carcinoma originating in the EAC, the T staging system has been developed by the Pittsburgh University group (Table 1) [3]. There has been no serious attempt to classify and stage TBMs of other histologies and sites of origin other than the EAC.
In terms of therapeutic modality for TBMs, surgery is the preferred method. The surgical procedure, which we advocate in advanced or salvage cases, should be completed as a three-team approach including a Neuro-otology, Head and Neck and a Plastic surgeon. The three steps include first a soft tissue step, followed by a temporal bone resection and concluding with reconstruction, microvascular and facial reanimation if the facial nerve is sacrificed.
TBMs have a higher risk of local/ nodal extension of the tumor into the Fissures of Santorini, the Foramen of Huschke and the Petro-sqamous suture, with the incidence of extension between 10-62% [1,3]. As a result, a superficial parotidectomy with or without a deep lobe parotidectomy is mandatory for T-2, 3 and
4 tumors [4]. Because the cancer can develop within the bony structures, lymph node metastases can occur with rates between 10-23% [1,3] and as a result even in T1 tumors a selective supraomohyoid neck dissection (levels IIa/IIb/III) is performed in our centre (Figure 2a, 2b). This facilitates oncological clearance and assists further in definitive staging.
The second stage is the temporal bone resection where three different resections may be performed depending on the stage of the tumor. In early stage tumors (T1/2) a Lateral Temporal Bone Resection (LTBR) is performed (Figure 3). This would require en bloc removal of the entire osseous and cartilaginous portions of the EAC and tympanic membrane using the extending facial recess approach [5]. In more advanced tumors (T3/4), a Sub-Temporal Bone Resection (STBR) is the surgical method
Figure 1 A clinical photograph of the 62-year-old patient with fluctuant swelling to the pinna remnant, this is confirmed as recurrent squamous cell carcinoma.
Figure 2 Head and neck component. En bloc resection of the recurrent disease including a radical neck dissection of the left neck.
Figure 3 Soft tissue component of the resection now complete which include radical neck dissection, total parotidectomy and excision of the pinna remnant.
Table 1: T staging system.
Stage Description
T1 -A carcinoma that is limited to the EAC with no bone erosion or soft tissue involvement
T2 -A carcinoma that is limited to the EAC but with limited bone erosion and soft tissue involvement (<0.5 cm)
T3 -Full thickness erosion of the EAC along with limited soft tissue (<0.5 cm) and middle ear or mastoid involvement
T4
-Involves a tumor that has metastasized to adjacent structures including the Dura, petrous apex, temporomandibular Joint (TMJ), cochlea, carotid canal and jugular foramen compounded with extensive soft tissue involvement and facial nerve palsy.

Central
O’Neill et al. (2015)Email:
Ann Otolaryngol Rhinol 2(7): 1049 (2015) 3/3
Zucker I, O’Sullivan B, McConn Walsh R, O’Neill JP (2015) High Risk Cutaneous Squamous Cell Carcinomas of the Pinna with Dissemination to the Temporal Bone Contemporary Oncological Management. Ann Otolaryngol Rhinol 2(7): 1049.
Cite this article
which involves an en bloc resection of the medial surfaces of the mesotympanum and leaves the air cells in the petrous apex and portions of the bony labyrinth [5]. The final resection technique, Total Temporal Bone Resection, is no longer performed. The final step of the three-team approach is reconstruction in which the aims are to close the defect, cover the dura and facial reanimation. The reconstruction is done with a free flap taken from the anterolateral thigh for bulk, which is easy to harvest and has a good blood supply through large caliber vessels [3]. Facial reanimation often includes a brow lift, facial lift and lower lid tarsorraphy (Figure 4).
Following surgery, adjuvant radiotherapy is effective but should not be used as a primary treatment method [6]. XRT or Radiotherapy is used in advanced tumors (T2, 3, 4) that
Figure 4 The lateral temporal bone component. Clinical photograph of the operative site following soft tissue excision and subtotal temporal bone resection.
Figure 5 Plastic surgery micro vascular reconstruction and facial reanimation. Patient has undergone an ALT free flap reconstruction followed by a brow lift, mid facial lift, lower lid tarsorraphy with 1.8-gram weight inserted.
often include perineural invasion, positive margins and lymph node metastasis. However the use of radiotherapy in T1/2 is controversial [7] and should be performed on a case-by-case basis. If the tumor has metastasized beyond the dura and there is Internal Carotid Artery involvement, the treatment method is often palliative care.
New methods to treat TBMs are being developed, along with refinements in the staging system, all of which will hopefully assist in helping to cure this disease.
CONCLUSION‘High risk’ squamous cell carcinomas of the head and
neck must be recognized as a separate disease to standard cutaneous squamous cell carcinoma. Nearly 90% of patients who undergo temporal bone resection have primary cutaneous malignancies that have disseminated into the temporal bone. A multidisciplinary approach including a Neuro-otology surgeon, Head and Neck oncologic surgeon and Plastic surgeon offer the best curative opportunity for patients requiring salvage surgery for TBM. Survival rates for T1/2 cancers is 90-100% however T3/4 survival drops to 86 and 46% respectively.
REFERENCES1. Prasad SC, D’Orazio F, Medina M, Bacciu A, Sanna M. State of the art in
temporal bone malignancies. Curr Opin Otolaryngol Head Neck Surg. 2014; 22: 154-165.
2. Moffat DA, Wagstaff SA. Squamous cell carcinoma of the temporal bone. Curr Opin Otolaryngol Head Neck Surg. 2003; 11: 107-111.
3. Lionello M, Stritoni P, Facciolo MC, Staffieri A, Martini A, Mazzoni A, et al. Temporal bone carcinoma. Current diagnostic, therapeutic, and prognostic concepts. J Surg Oncol. 2014; 110: 383-392.
4. Morris LG, Mehra S, Shah JP, Bilsky MH, Selesnick SH, Kraus DH. Predictors of survival and recurrence after temporal bone resection for cancer. Head Neck. 2012; 34: 1231-1239.
5. Flint PW, Haughey BH, Lund VJ, Niparko JK, Richardson MA, Robbins KT, et al. Cummings otolaryngology. 6th ed. Philadelphia: Saunders. 2015.
6. Zhang T, Li W, Dai C, Chi F, Wang S, Wang Z. Evidence-based surgical management of T1 or T2 temporal bone malignancies. Laryngoscope. 2013; 123: 244-248.
7. Bacciu A, Clemente IA, Piccirillo E, Ferrari S, Sanna M. Guidelines for treating temporal bone carcinoma based on long-term outcomes. Otol Neurotol. 2013; 34: 898-907.