Embed Size (px)
Citation preview

Int J Clin Exp Med 2017;10(5):8301-8308www.ijcem.com /ISSN:1940-5901/IJCEM0036203
Case ReportMetastasis of nasopharyngeal carcinoma: a case report and review
Yongtao Yang, Kongliang Li, Yufan Wang, Hongyu Yang
Department of Oral and Maxillofacial Surgery, Peking University Shenzhen Hospital, Shenzhen 518001, China
Received July 19, 2016; Accepted November 11, 2016; Epub May 15, 2017; Published May 30, 2017
Abstract: Nasopharyngeal carcinoma (NPC) is one of the most common epithelial malignancies in the head and neck region with a marked racial predilection in Southern Chinese, which metastasize to parotid gland, and it is extremely rare. In these populations, it is usually associated with Epstein-Barr virus (EBV). The existence of EBV in tumor cells, aberrant type of antibodies against EBV antigens in patient sera, and the same increased viral DNA in patient circulation as nasopharyngeal region highlights the role of EBV during NPC development. Here we report a rare case of parotid gland metastasis of nasopharyngeal carcinoma. A 37-year-old male, was admitted to Peking University Shenzhen Hospital for diagnosis of a pre-existent (half-year) painless mass in the left parotid region. A 3.5 cm mass was found in the left parotid. It was firm, fixed and medium hardness. On the basis of clinical medical his-tory, morphological, immunohistochemical and molecular biology findings, a diagnosis of stage II, Epstein Barr-virus positive, parotid gland metastasis of nasopharyngeal carcinoma and nasopharyngeal non-keratinizing carcinoma were made. The primary symptom of parotid gland mass with NPC is often misdiagnosed, which has been admitted to be a pivotal cause of therapy failure in patients.
Keywords: Parotid gland metastasis, nasopharyngeal carcinoma, Epstein-Barr virus, clinicopathological feature, therapy
Introduction
A variety of metastatic neoplasms can present as masses in the parotid gland. Approximately 25% of malignant parotid tumors are metasta-ses originating from head and neck tumors i.e. face, oral cavity, and oropharynx. Squamous cell carcinoma and malignant melanoma are one of the most common ones among malig-nant parotid tumors [1-3]. However, parotid gl- and tumors metastases originating from naso-pharyngeal carcinoma (NPC) are extremely ra- re, and according to a recent study reported by Francis CH Ho et al, low-risk node groups in- cluded the supraclavicular, levels IA/IB and VI nodes, and parotid nodes with involvement rates at 3%, 0%, 3%, 0%, and 1%, respectively [4]. NPC is a common malignant head and neck cancer, especially in Southern China, where the annual incidence is 15-25 cases per 100,000 [5]. It has a high preference for local lymph node metastasis, and over 80% of cases pre-sented with lymphadenopathy at diagnosis. Its
etiology includes genetic epigenetic, backgro- und and environmental factors [6]. EBV infec-tion belongs to environmental factors, which has attracted increasing attention, and a large number of emerging evidences have elucidated the close relationship between EBV and NPC [7, 8]. Illocal EBV infection in human suggests th- at most individuals carry EBV-infected cells, whereas a direct causal relationship between both events were difficult to establish by mere detection of the virus in individualwith tumor, but instead requires definite detection of viral nucleic acids or viral proteins in the tumor cells. The diagnosis of parotid metastasis in NPC is primarily based on magnetic resonance imag-ing (MRI) and/or transnasal endoscopic biopsy. Compared with biopsy, MRI is a noninvasive and tremendous useful in the evaluation of cer-vical and retropharyngeal lymphadenopathy, which is the commonly used method for dis-crimination between benign and malignant parotid masses [9-11]. Histologically, the naso-pharyngeal stroma is so full of lymphoid tissue

Metastasis of NPC
8302 Int J Clin Exp Med 2017;10(5):8301-8308
and lymphaticplexus that usually involves reac-tive lymphoid follicles, and many small lym-phoid cells infiltrate the epithelium commonly. Rad- iotherapy is the most efficacious therapeutic approach for NPC and the conventional dose of radiotherapy is between 60 and 70 Gy, while chemotherapy is also needed in advanced dis-ease [12]. Although the incidence of parotid gland metastasis of nasopharyngeal carcino-ma is quite low, it should always be considered in the differential diagnosis of a parotid mass.
In this study we focused on reviewing and inves-tigating English literatures with reference to this rare metastatic site over the past two decades, the diagnosis of parotid gland metas-tasis and, the advancing of the therapeutic methods inpatients with metastasis of NPC to the parotid gland.
Case report
In September 2015, a 37 years old male, which was born and lived in Guangdong Province, was
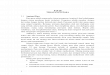
Figure 1. (A) Sagittal and (B) axial magnetic resonance images show a 2.9 cm × 4.0 cm × 3.5 cm well circumscribed mass located on the superficial lobe of the left parotid, located on the left parotid gland. Multiple swollen lymph nodes were identified in the area of bilateral carotid sheath and the bigger one measured about 1.5 cm × 0.6 cm in size. (C) Sagittal and (D) axial magnetic resonance images show a size about 9.4 mm × 5.6 mm of oval spot in the left top retropharyngeal wall.

Metastasis of NPC
8303 Int J Clin Exp Med 2017;10(5):8301-8308
admitted to Peking University Shenzhen Hos- pital for diagnosis of a pre-existent (half-year) painless mass of the left parotid region, with progressive-growing since he perceived. Initial diagnosis was the left parotid gland mass. During examination, a medium hardness tumor was visible, which was fixed to the underlying soft tissues in the left parotid gland and the size is about 2.9 cm × 4.0 cm × 3.5 cm with a defined boundary. Several tender and unfixed lymph nodes could be palpated in bilateral neck. There were no lesions found in skin of the cervical region in appearance and the oral cav-ity. No facial nerve palsy was presented. During his illness, there had been no symptoms of headache, abnormal deglutition, nasal occlu-sion or blood-stained nasal discharge. A normal thoracic image was presented by chest X-ray. Serum anti-EBV antibodies was positive (Titers: VCA-IgA was >1:10 and EA-IgA was >1:10), oth- er laboratory data were within the reference range. Magnetic resonance imaging (MRI) of head and neck region delineated a 2.9 cm × 4.0 cm × 3.5 cm well-circumscribed mass loca- ted on the superficial lobe of the left parotid (Figure 1), the mass exhibited isointensity or hypointense signal on T1-weighted images and hyperintensity on T2-weighted images, with a moderately enhanced effect; the top left retro-pharyngeal wall showed abnormal enhanced signal and 9.4 mm × 5.6 mm size of oval spot (Figure 1), suggesting further examination; mul-tiple abnormal enlargement of the lymph nodes were identified in the area of bilateral carotid sheath and the bigger one was measured about
1.5 cm × 0.6 cm in size. Nasopharyngoscopy examination revealed an ill-defined elevated lesion in the top left retropharyngeal wall which suspected as a neoplasm. The patient was oth-erwise well, with no other significant evidences in the medical history.
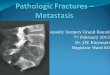
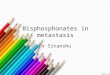
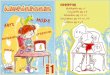
Then, a rhinopharyngeal biopsy of the neo-plasm was performed. The specimen was pale in color and the histopathological examination of a tissue sample revealed an abnormal tumor nests of undifferentiated epithelial cells closely mixed with lymphocytes. The tumor cells showed an indistinct cell borders, bare nuclei, vesicular nuclei, and situated centrally in the nucleolus (Figure 2). Immunohistochemically and in situ hybridization, the tumor cells were widely positive for pan cytokeratin (PCK), cyto-keratin 5/6 (CK5/6) and p63 (Figure 3), EBV-encoded RNA was widely positive in undifferen-tiated carcinoma (Figure 4), thus, with taking the results of MRI features, immunohistochem-ical and in situ hybridization of specimens, and basic information of patient, including ethnic, birthplace, EBV infection into consideration, the diagnosis of non-keratinizing undifferenti-ated carcinoma of the nasopharynx was estab-lished. Under general anesthesia, left paroti-dectomy with resection of several satellite lymph nodes and neck dissection and the left parotid duct resection were performed, and pathological examination revealed morphologi-cal features of the left parotid gland tumor identical to the specimen from rhinopharyngeal biopsy and the tumor cells were diffusely posi-
Figure 2. Histopathology of specimen of rhinopharyngeal biopsy (A) and the tumor of parotid gland (B) showing tumor cells with indistinct cell borders, bare nuclei and vesicular nuclei intermingled with lymphocytes and plasma cells (staining by hematoxylin and eosin; × 400).

Metastasis of NPC
8304 Int J Clin Exp Med 2017;10(5):8301-8308
tive for PCK, CK5/6 and p63 in immunohisto-chemical (Figure 3), resection of the left parotid duct was also positive for PCK and CK5/6 (Figure 5), however, there were no tumor cells observed in histopathology of satellite lymph nodes of left parotid gland. The safe margin status exhibited no malignancy, no extracapsu-lar extension, and no lymphovascular or peri-neural invasion. To conclud, a final diagnosis
of Epstein-Barr virus-associated parotid gland metastasis of nasopharyngeal carcinoma was determined. After one month of surgery, a dose of 50 Gy intensity-modulated radiotherapy (IMRT) was suggested and he accepted that treatment. Clinical and instrumental examina-tion every three months in the first year after therapy and every six months thereafter exclud-ed local and distant recurrences. The patient
Figure 3. Immunohistochemical staining of nasopharyngeal carcinoma, the left parotid gland tumor. Thetwo tissues were positive for PCK (A1, A2), CK5/6 (B1, B2) and p63 (C1, C2) (× 400).

Metastasis of NPC
8305 Int J Clin Exp Med 2017;10(5):8301-8308
was living a normal life with a good condition at the time of last follow up in October 2016.
Discussion
NPC is relatively uncommon in the western countries, however, incidence of NPC is high in southern China and Southeast Asia, especially in the Guangdong Province. NPC has a high ten-dency for regional lymph node metastasis, lymphadenopathy occurs in almost 84.9% of patients after diagnosis [4]. The pattern of nodal metastasis in NPC follows an orderly spread down the neck with rare node skipping; the retropharyngeal space is the most com-monly involved regions, and the sequence of incidence level is as follows: levels II, III, IV, V, IB and the supraclavicular nodes [4]. According to the latest International Consensus Guidelines
for nodal levels, the parotid lymph nodes were classified as level VIII; it has an extremely low risk metastasis from the nasopharynx. In Francis CH Ho et al [4] meta-analysis of clinical evidence study, the nodal stations may be divided into high, intermediate and low risk groups, and the low risk group of draining nodes in NPC include the supraclavicular as well as parotid lymph nodes, with an incidence of involvement at 8.8% and 0.9%, respectively. NPC can metastasize to the parotid gland lymph nodes (PLNs) via three approaches: (1) lateral retropharyngeal lymph nodes to the parotid gland tissue; (2) superior deep cervical lymph nodes; and (3) parotid gland tissue involvement. It can also infiltrate the parotid gland tissue directly by the primary lesion in the nasopharynx via peripharyngeal space. In term of our case, the major pathway of invading the
Figure 4. Nasopharyngeal carcinoma associated with Epstein-Barr virus. A and B. In situ hybridisation with EBER probes revealing extensive positivity in the tumor cells (× 100 and × 400, respectively).
Figure 5. Immunohistochemical staining of left parotid duct. The tissues were positive for PCK (A), CK5/6 (B) (× 400).

Metastasis of NPC
8306 Int J Clin Exp Med 2017;10(5):8301-8308
parotid gland tissue is via the peripharyngeal space considering the MRI which revealed the tumor with a sprawl pattern of growth in all directions, pushing the left parotid gland back-ward, and creeping into the left peripharyngeal space by surrounding ramus of mandible. How- ever, there is another possibility of invasion, the tumor cells of left retropharyngeal wall could be planted in the left parotid gland through parotid duct. The positive for PCK, CK5/6 and tumor cells infiltrating were obviously detected in the resection of left parotid duct.
The definite diagnosis of PLN metastasis in the present case study was mainly based on MRI and nasopharyngoscopy examination rather than fine-needle aspiration cytology (FNAC) or radiologic criteria [13] because of these rea-sons. First of all, NPC is mainly staged by MRI. FNAC is an invasive examination and easy to generate needle-path tumor implantation, sel-dom executed in patients with parotid lesions, unless pathologic verification of the primary tumor is unavailable. The second, radiologic cri-teria for PLN metastasis have not been admit-ted yet, and during process of surgery, the PLNs are not resected routinely, therefore, the radio-logic criteria, is unable to be applied to the PLNs, which based on clinicopathologic analy-sis of the neck lymph nodes in dissection speci-mens [13]. The third, Once a patient with (or without) EBV infection has a suspected neo-plasm that was detected in nasopharynx or
neck by MRI, a careful nasopharyngoscopy examination is essential and, if relevant, ran-dom nasopharyngeal biopsy must be per-formed. The principal differential diagnosis of our case is lymphoepithelial carcinoma (LEC), which is also a rare and unique malignant sali-vary gland tumor with morphological character-istics identical to that of metastatic nasopha-ryngeal carcinoma. Morphologically, parotid gland metastasis of nasopharyngeal carcinoma is difficult to distinguish from LEC of the parotid gland, which has extremely similar architectural and cytological features which is a lymphoid rich tumor composed of sheets and nests of large vesicular cells with prominent nucleoli and syncytial cytoplasm, the same ethnic predi-lection, and a strong association with EBV infections. Thus, a careful nasopharyngoscopy examination is necessary for detection of pri-mary tumor and definite diagnosis, then, if posi-tive results were presented, multiple nasopha-ryngeal biopsies must be executed.
To the best of our knowledge, a retrospective review of English literatures and abstracts ana-lyzing the distant metastasis status of patients with NPC was performed by searching electron-ic database PUBMED from 1995 to 2015. Patients who was previously treated or present with recurrence of disease were excluded from analysis, or had received MRI examination of the neck and nasopharynx. Altogether, 7958 cases with NPC of 14 included studies were
Table 1. Clinical characteristics of the 7958 patients with NPC of 14 included studies
Paper NO. NO. of patients
Case of Ab Parotid Cervical R Level I Level Ib Level II Level III Level IV Level V Level VI SCF
LN LN LN LN LN LN LN LN LN LN LN LN[14] 114 91 58 59 58[15] 44 39 39 13[16] 150 115 2 115 108 115 3 66[17] 101 89 3 73 2 85 24 2 20[18] 275 215 4 175 175 175 174 65 16 18 8[19] 94 82 82 82[20] 159 148 139 108 139[21] 202 193 162 190 172 22[22] 618 543 7 508 392 508 21 506 237 72 200[23] 924 786 6 679 24 590 226 56 87 31[24] 63 44 44 44[25] 3100 2679 53 2012 2341 1184 350 576 10[26] 303 265 265[27] 1811 1780 21Abbreviations: Ab, abnormal; LN, lymph nodes; R LN, Retropharyngal LN; SCF, supraclavicular fossa.

Metastasis of NPC
8307 Int J Clin Exp Med 2017;10(5):8301-8308
included in the study. A total of 7069 (88.83%) patients involved abnormal lymph nodes and, the detailed distribution were summarized in Table 1 [14-27]. 96 PLN metastases were detected in 7069 patients; the incidence of PLN metastasis was 1.21%, which is identical to the rates reported in former study [4]. Although such a low incidence it is, reports of long-term survival inpatients with PLN me- tastasis at presentation are rare. The earlier diagnosis and aggressive treatment for pa- tients with parotid gland metastasis of naso-pharyngeal carcinoma may better improve the outcomes and the PLN metastasis with NPC misdiagnoses should be avoided as possible. In clinical practice, a combination of radio/che-motherapy is currently the gold standard but the rates of failure arising from 7% up to 58%. Because EBV infection is closely linked to NPC development and the current NPC therapy is based on radiochemotherapy which is affec- ted by severe side effects and high rate of recurrences, many efforts were made to de- velop an effective treatment against EBV la- tent cycle, moreover, many studies on EBV directed therapy and their application on NPC have been made in last few years. Future researches on this topic are warranted. The optimal treatment for patients with NPC who involved in PLN metastasis is controversial. In the present case, we recommend the removal of partial parotidectomy and parotid tail nodes. However, there is still controversy on the selection of surgery to treat metastasis to parotid lymph nodes; while some surgeons prefer superficial parotidectomy, others prefer complete parotidectomy. Facial nerve preser-vation should be attempted unless the nerve is grossly involved with the tumor.
In conclusion, PLN metastasis from NCP is highly rare that often being neglected. According to a retrospective review of English literatures, the incidence of PLN metastasis was only 1.21% over the past two decades and, its treat-ment has not been standardized. Thus, in order to improve the clinical outcome and quality of life, therapeutic decision-making rely on the clinical disease extent, and surgery and/or che-mo-radiation therapy must be tailored to the individual patient. A careful nasopharyngosco-py examination is necessary for patients who were suspected PLN metastasis from NPC. The earlier the diagnosis and more aggressive of the treatment for patients with parotid gland
metastasis of nasopharyngeal carcinoma may better improve outcomes.
Acknowledgements
This study was supported by National Natural Science Foundation of China (no. 81572654), and the Basic Research Program of Shenzhen Innovation Council of China (no. JCYJ20140- 415162338806, JCYJ20150403091443286 and JCYJ20150403091443303).
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Hongyu Yang, De- partment of Oral and Maxillofacial Surgery, Peking University, Shenzhen Hospital, 1120 Lianhua Road, Futian District, Shenzhen 518001, Guangdong, China. E-mail: [email protected]
References
[1] Nuyens M, Schüpbach J, Stauffer E, Zbären P. Metastatic disease to the parotid gland. Oto-laryngol Head Neck Surg 2006; 135: 844-848.
[2] Sanders JG, Smith KG, Jameson MB, de Groot C, White J. Persistent neck disease after chemoradiation for head and neck squamous cell carcinoma. J Laryngol Otol 2012; 126: 1121-1126.
[3] Antonio JK, Santini S, Politi D, Sulfaro S, Spa-ziante R, Alberti A, Pin M, Barzan L. Sentinel lymph node biopsy in squamous cell carcino-ma of the head and neck: 10 years of experi-ence. Acta Otorhinolaryngol Ital 2012; 32: 18-25.
[4] Ho FC, Tham IW, Earnest A, Lee KM, Lu JJ. Pat-terns of regional lymph node metastasis of na-sopharyngeal carcinoma: a meta-analysis of clinical evidence. BMC Cancer 2012; 12: 98.
[5] Cancer incidence in five continents. Volume IX. IARC Sci Publ 2008; 1-837.
[6] Huang PH, Shyng YC, Sloan P, Ou KL, Hsia YJ, Devlin H. Nasopharyngeal carcinoma meta-static to the mandible. Open Dent J 2010; 4: 195-197.
[7] Delecluse HJ, Feederle R, O’Sullivan B, Taniere P. Epstein-Barr virus-associated tumours: an update for the attention of the working pathol-ogist. J Clin Pathol 2007; 60: 1358-1364.
[8] Hutajulu SH, Kurnianda J, Tan IB, Middeldorp JM. Therapeutic implications of Epstein-Barr virus infection for the treatment of nasopha-ryngeal carcinoma. Ther Clin Risk Manag 2014; 10: 721-736.

Metastasis of NPC
8308 Int J Clin Exp Med 2017;10(5):8301-8308
[9] Yerli H, Aydin E, Haberal N, Harman A, Kaskati T, Alibek S. Diagnosing common parotid tu-mours with magnetic resonance imaging in-cluding diffusion-weighted imaging vs fine-nee-dle aspiration cytology: a comparative study. Dentomaxillofac Radiol 2010; 39: 349-355.
[10] Inohara H, Akahani S, Yamamoto Y, Hattori K, Tomiyama Y, Tomita Y, Aozasa K, Kubo T. The role of fine-needle aspiration cytology and magnetic resonance imaging in the manage-ment of parotid mass lesions. Acta Otolaryngol 2008; 128: 1152-1158.
[11] King AD, Ahuja AT, Leung SF, Lam WW, Teo P, Chan YL, Metreweli C. Neck node metastases from nasopharyngeal carcinoma: MR imaging of patterns of disease. Head Neck 2000; 22: 275-281.
[12] Ma BB, Chan AT. Recent perspectives in the role of chemotherapy in the management of advanced nasopharyngeal carcinoma. Cancer 2005; 103: 22-31.
[13] Van den Brekel MW, Stel HV, Castelijns JA, Nauta JJ, van der Waal I, Valk J, Meyer CJ, Snow GB. Cervical lymph node metastasis: as-sessment of radiologic criteria. Radiology 1990; 177: 379-384.
[14] Chong VF, Fan YF, Khoo JB. Retropharyngeal lymphadenopathy in nasopharyngeal carcino-ma. Eur J Radiol 1995; 21: 100-105.
[15] Lam WW, Chan YL, Leung SF, Metreweli C. Ret-ropharyngeal lymphadenopathy in nasopha-ryngeal carcinoma. Head Neck 1997; 19: 176-181.
[16] King AD, Ahuja AT, Leung SF, Lam WW, Teo P, Chan YL, Metreweli C. Neck node metastases from nasopharyngeal carcinoma: MR imaging of patterns of disease. Head Neck 2000; 22: 275-281.
[17] Ng SH, Chang JC, Chan SC, Ko SF, Wang HM, Liao CT, Chang YC, Yen TC. Nodal metastases of nasopharyngeal carcinoma: patterns of dis-ease on MRI and FDG PET. Eur J Nucl Med Mol Imaging 2004; 31: 1073-1080.
[18] Liu LZ, Zhang GY, Xie CM, Liu XW, Cui CY, Li L. Magnetic resonance imaging of retropharyn-geal lymph node metastasis in nasopharyn-geal carcinoma: patterns of spread. Int J Radi-at Oncol Biol Phys 2006; 66: 721-730.
[19] Fuwa N, Ariji Y, Daimon T, Wakisaka M, Matsu-moto A, Kodaira T, Tachibana H, Nakamua T, Satou Y. Relationship between the growth pat-tern of nasopharyngeal cancer and the cervi-cal lymph nodes based on MRI findings: can the cervical radiation field be reduced in pa-tients with nasopharyngeal cancer? Br J Radiol 2006; 79: 725-729.
[20] Lu JC, Wei BQ, Chen WZ, Qian PD, Zhang YQ, Wei Q, Cha WW, Li F, Ni M. Staging of nasopha-ryngeal carcinoma investigated by magnetic resonance imaging. Radiother Oncol 2006; 79: 21-26.
[21] Ng WT, Lee AW, Kan WK, Chan J, Pang ESY, Yau TK, Lau KY. N-staging by magnetic resonance imaging for patients with nasopharyngeal car-cinoma: pattern of nodal involvement by radio-logical levels. Radiother Oncol 2007; 82: 70-75.
[22] Wang X, Li L, Hu C, Zhou Z, Ying H, Ding J, Feng Y. Patterns of level II node metastasis in naso-pharyngeal carcinoma. Radiother Oncol 2008; 89: 28-32.
[23] Tang L, Mao Y, Liu L, Liang S, Chen Y, Sun Y, Liao X, Lin A, Liu M, Li L, Ma J. The volume to be irradiated during selective neck irradiation in nasopharyngeal carcinoma. Cancer 2009; 115: 680-688.
[24] Kam MK, Teo PM, Chau RM, Cheung KY, Choi PH, Kwan WH, Leung SF, Zee B, Chan AT. Treat-ment of nasopharyngeal carcinoma with inten-sity-modulated radiotherapy: the Hong Kong experience. Int J Radiat Oncol Biol Phys 2004; 60: 1440-1450.
[25] Wang X, Hu C, Ying H, He X, Zhu G, Kong L, Ding J. Patterns of lymph node metastasis from na-sopharyngeal carcinoma based on the 2013 updated consensus guidelines for neck node levels. Radiother Oncol 2015; 115: 41-45.
[26] Zhang GY, Liu LZ, Wei WH, Deng YM, Li YZ, Liu XW. Radiologic criteria of retropharyngeal lymph node metastasis in nasopharyngeal car-cinoma treated with radiation therapy. Radiol-ogy 2010; 255: 605-612.
[27] Zhang Y, Li WF, Chen L, Mao YP, Guo R, Zhang F, Peng H, Liu LZ, Li L, Liu Q, Ma J. Prognostic value of parotid lymph node metastasis in pa-tients with nasopharyngeal carcinoma receiv-ing intensity-modulated radiotherapy. Sci Rep 2015; 5: 13919.