Embed Size (px)
Citation preview

CASE REPORT Open Access
A child with autoimmune polyendocrinopathycandidiasis and ectodermal dysplasia treatedwith immunosuppression: a case reportClodagh S O’Gorman1,2,9,10,11*, Rayzel Shulman1,2,9, Irene Lara-Corrales2,3,9, Elena Pope2,3,9, Margaret Marcon2,4,9,Hartmut Grasemann2,4,5,9, Rayfel Schneider2,6,9, Julia Upton2,7,9, Etienne B Sochett1,2,9, Dror Koltin1,2,9
and Eyal Cohen2,8,9
Abstract
Introduction: Common features of autoimmune polyendocrinopathy-candidiasis-ectodermal dysplasia includecandidiasis, hypoparathyroidism and hypoadrenalism. The initial manifestation of autoimmunepolyendocrinopathy-candidiasis-ectodermal dysplasia may be autoimmune hepatitis, keratoconjunctivitis,frequent fever with or without a rash, chronic diarrhea, or different combinations of these with or withoutoral candidiasis.
Case presentation: We discuss a profoundly affected 2.9-year-old Caucasian girl of Western Europeandescent with a dramatic response to immunosuppression (initially azathioprine and oral steroids, and thensubsequently mycophenolate mofetil monotherapy). At four years of follow-up, her response tomycophenolate mofetil is excellent.
Conclusion: The clinical features of autoimmune polyendocrinopathy-candidiasis-ectodermal dysplasia maycontinue for years before some of the more common components appear. In such cases, it may be life-saving todiagnose autoimmune polyendocrinopathy-candidiasis-ectodermal dysplasia and commence therapy withimmunosuppressive agents. The response of our patient to immunosuppression with mycophenolate mofetil hasbeen dramatic. It is possible that other patients with this condition might also benefit from immunosuppression.
Keywords: APECED (autoimmune polyendocrinopathy-candidiasis-ectodermal dysplasia), APS (autoimmunepolyendocrinopathy syndrome), Autoimmunity, Immunosuppression, Endocrinopathies
IntroductionThe autoimmune regulator (AIRE) gene, on chromo-some 21, expresses self-antigens in the thymus and med-iates negative selection of self-reactive T-cells [1].Autoimmune polyendocrinopathy-candidiasis-ectodermaldysplasia (APECED), or autoimmune polyendocrinopathysyndrome type I, occurs due to loss of function of AIRE,with resultant loss of thymic tolerance to self-antigens [1].Common features of APECED include candidiasis,
hypoparathyroidism and adrenal insufficiency [2]. Theinitial manifestation of APECED may be autoimmune
hepatitis, keratoconjunctivitis, frequent fever with orwithout a rash, chronic diarrhea, or different combina-tions of these with or without oral candidiasis. Thisclinical picture may continue for years before the ap-pearance of the more common components [2]. In suchcases, it may be life-saving to diagnose APECED andcommence therapy with immunosuppressive agents.The literature on therapeutic options for severe mani-festations of this rare condition is scarce. Some datasuggest that a younger age at presentation is associatedwith increased disease severity, although the authors donot specify how young [2]. We discuss a profoundlyaffected young patient with a dramatic response to im-munosuppression using mycophenolate mofetil (MMF).
* Correspondence: [email protected] of Endocrinology, The Hospital for Sick Children, Toronto, Canada2Department of Pediatrics, The Hospital for Sick Children, Toronto, CanadaFull list of author information is available at the end of the article
JOURNAL OF MEDICALCASE REPORTS
© 2013 O’Gorman et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of theCreative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use,distribution, and reproduction in any medium, provided the original work is properly cited.
O’Gorman et al. Journal of Medical Case Reports 2013, 7:44http://www.jmedicalcasereports.com/content/7/1/44
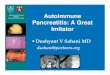
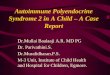
Case presentationA 2-year-old girl of non-consanguineous Caucasian par-ents of Western European descent, developed the follow-ing clinical features over 12 months: hypoparathyroidismwith hypocalcemia and borderline high serum phosphate(parathyroid hormone 20ng/L, normal 10 to 65; totalcalcium 1.98mmol/L, normal 2.2 to 2.6; phosphate2.1mmol/L, normal 1.6 to 2.1); mucocutaneous candid-iasis (Figure 1); keratoconjunctivitis; sialoadenitis; viti-ligo (Figure 2); urticaria-like rash (Figure 3); andalopecia. At age 2.9 years, she required intensive careadmission and ventilation for aspiration pneumoniaand significant respiratory compromise. During this ad-mission, severe hypoparathyroidism with significanthypocalcemia was managed with high doses of intra-venous and subsequently oral calcium and calcitriol.APECED was confirmed following identification of ahomozygous 13 base pair deletion on AIRE exon 8;both parents were heterozygous carriers.Previously, she had been investigated and treated for
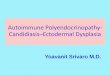
several episodes of aspiration pneumonia, frequent diar-rhea, intermittent urticaria-like eruptions (Figure 3) withlymphocytic vasculitis on biopsy and frequent fevers ofunknown origin. Between diarrheal illnesses, she had se-vere constipation, including a partial small bowel ob-struction at 1.3 years old.Laboratory evaluation revealed: normal thyroid func-
tion tests; positive anti-thyroid peroxidase antibodies;normal glucocorticoid function following adrenal stimu-lation; positive anti-adrenal and anti-21-hydroxylaseantibodies; normal electrolytes and mineralocorticoidfunction; intercurrent stress hyperglycemia; positiveanti-glutamic acid decarboxylase antibodies but negativeislet cell and anti-insulin antibodies. While ventilated,Candida albicans was cultured from her endotrachealtube; C. albicans and organic food material were isolatedfollowing closed lung biopsy.
Her diarrhea worsened, and became associated withdeterioration of her hypoparathyroidism and hypocalce-mia requiring prolonged parenteral calcium. Hypocalce-mia was marked after discontinuing parenteral calciumfor even a few hours. She then developed mineralocor-ticoid insufficiency, worsening sicca symptoms, and re-current life-threatening respiratory tract infections.After seven months of hospitalization, immunosup-
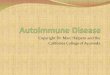
pression was commenced, first using high dose oralprednisone (two mg/kg), then azathioprine (1.5mg/kg).Calcium and diarrhea stabilized somewhat. However,repeated attempts to wean maintenance steroids faileddue to exacerbations of diarrhea and hypocalcemia.Therefore, immunosuppression was changed to MMFmonotherapy (900mg/m2). Prednisone was weaned suc-cessfully to physiological maintenance doses, and contin-ued at these doses.Her clinical response to immunosuppression was dra-
matic. Intravenous calcium was discontinued after oneweek; diarrhea began to resolve (Figure 4). Within one
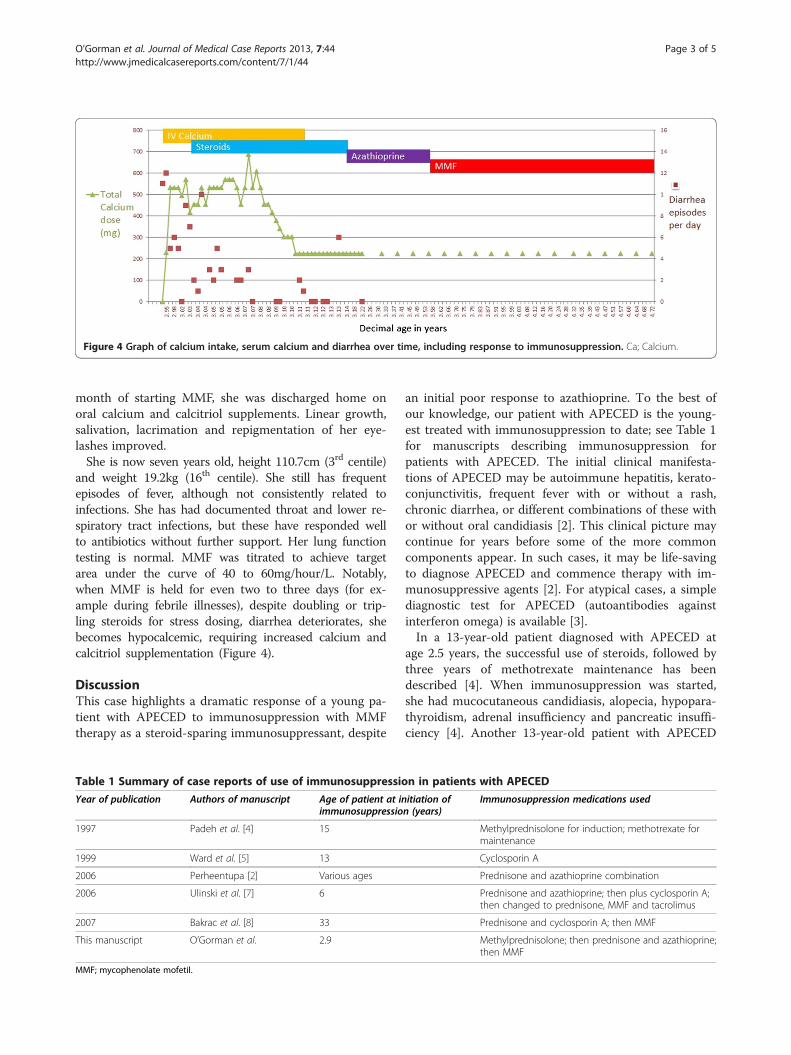
Figure 1 Mucocutaneous candidiasis (red arrow).
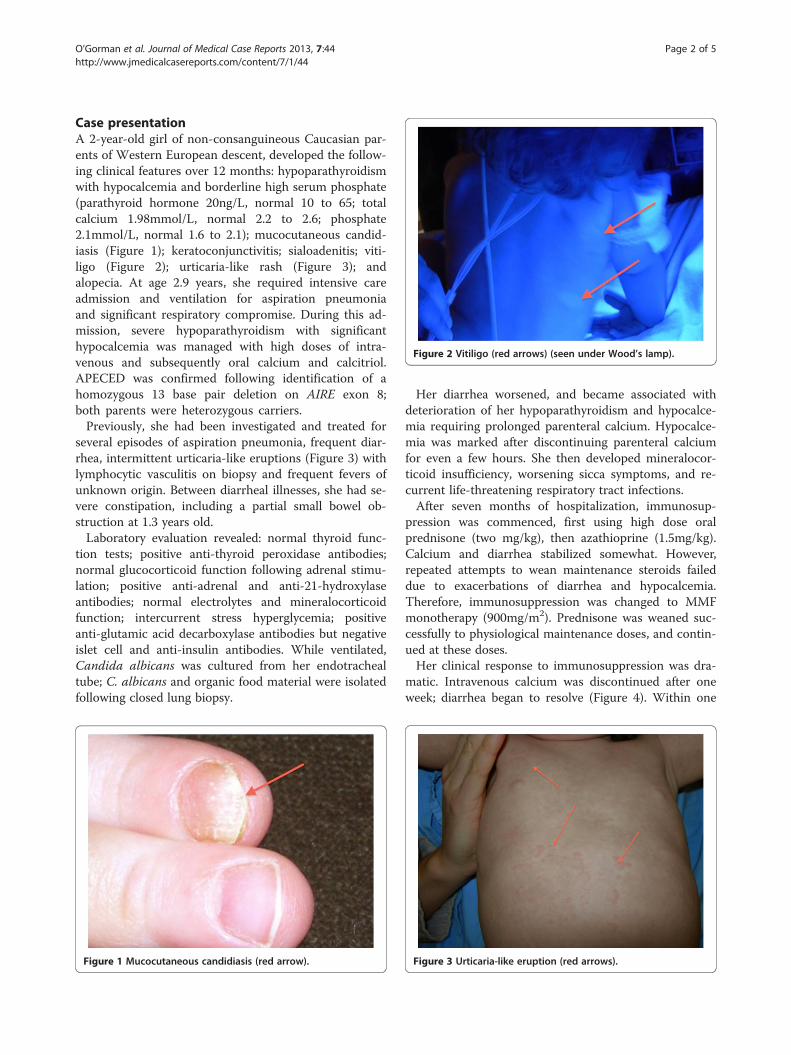
Figure 2 Vitiligo (red arrows) (seen under Wood’s lamp).
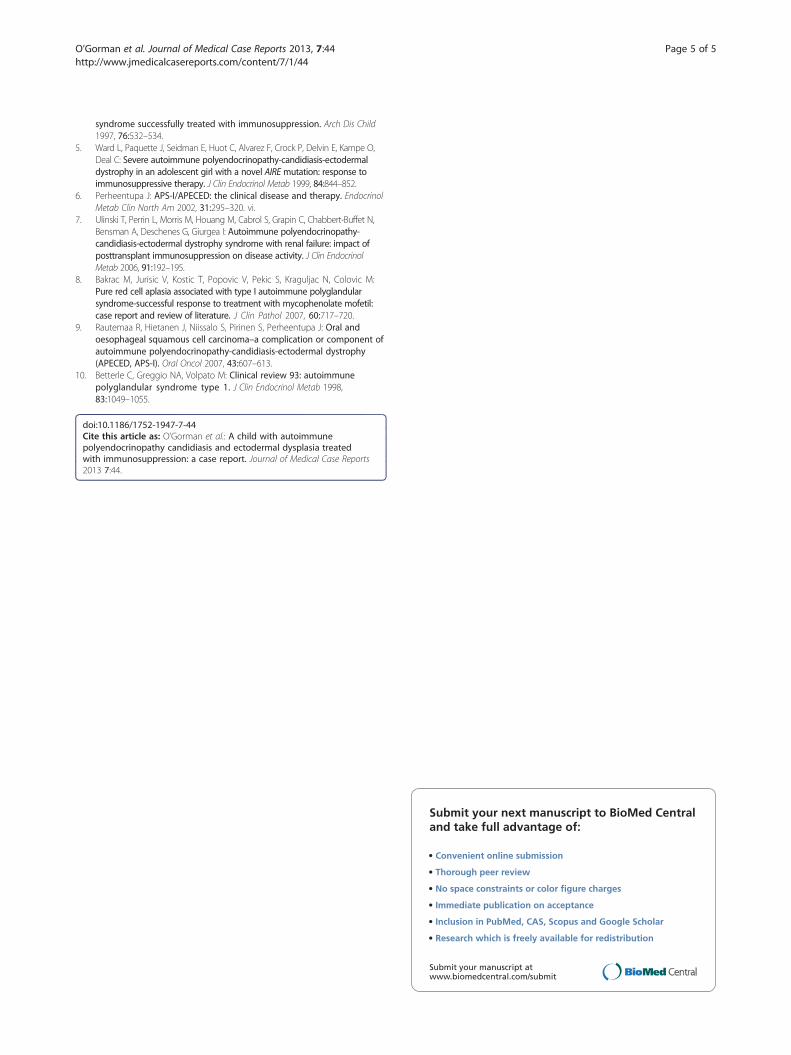
Figure 3 Urticaria-like eruption (red arrows).
O’Gorman et al. Journal of Medical Case Reports 2013, 7:44 Page 2 of 5http://www.jmedicalcasereports.com/content/7/1/44
month of starting MMF, she was discharged home onoral calcium and calcitriol supplements. Linear growth,salivation, lacrimation and repigmentation of her eye-lashes improved.She is now seven years old, height 110.7cm (3rd centile)
and weight 19.2kg (16th centile). She still has frequentepisodes of fever, although not consistently related toinfections. She has had documented throat and lower re-spiratory tract infections, but these have responded wellto antibiotics without further support. Her lung functiontesting is normal. MMF was titrated to achieve targetarea under the curve of 40 to 60mg/hour/L. Notably,when MMF is held for even two to three days (for ex-ample during febrile illnesses), despite doubling or trip-ling steroids for stress dosing, diarrhea deteriorates, shebecomes hypocalcemic, requiring increased calcium andcalcitriol supplementation (Figure 4).
DiscussionThis case highlights a dramatic response of a young pa-tient with APECED to immunosuppression with MMFtherapy as a steroid-sparing immunosuppressant, despite
an initial poor response to azathioprine. To the best ofour knowledge, our patient with APECED is the young-est treated with immunosuppression to date; see Table 1for manuscripts describing immunosuppression forpatients with APECED. The initial clinical manifesta-tions of APECED may be autoimmune hepatitis, kerato-conjunctivitis, frequent fever with or without a rash,chronic diarrhea, or different combinations of these withor without oral candidiasis [2]. This clinical picture maycontinue for years before some of the more commoncomponents appear. In such cases, it may be life-savingto diagnose APECED and commence therapy with im-munosuppressive agents [2]. For atypical cases, a simplediagnostic test for APECED (autoantibodies againstinterferon omega) is available [3].In a 13-year-old patient diagnosed with APECED at
age 2.5 years, the successful use of steroids, followed bythree years of methotrexate maintenance has beendescribed [4]. When immunosuppression was started,she had mucocutaneous candidiasis, alopecia, hypopara-thyroidism, adrenal insufficiency and pancreatic insuffi-ciency [4]. Another 13-year-old patient with APECED
Figure 4 Graph of calcium intake, serum calcium and diarrhea over time, including response to immunosuppression. Ca; Calcium.
Table 1 Summary of case reports of use of immunosuppression in patients with APECED
Year of publication Authors of manuscript Age of patient at initiation ofimmunosuppression (years)
Immunosuppression medications used
1997 Padeh et al. [4] 15 Methylprednisolone for induction; methotrexate formaintenance
1999 Ward et al. [5] 13 Cyclosporin A
2006 Perheentupa [2] Various ages Prednisone and azathioprine combination
2006 Ulinski et al. [7] 6 Prednisone and azathioprine; then plus cyclosporin A;then changed to prednisone, MMF and tacrolimus
2007 Bakrac et al. [8] 33 Prednisone and cyclosporin A; then MMF
This manuscript O’Gorman et al. 2.9 Methylprednisolone; then prednisone and azathioprine;then MMF
MMF; mycophenolate mofetil.
O’Gorman et al. Journal of Medical Case Reports 2013, 7:44 Page 3 of 5http://www.jmedicalcasereports.com/content/7/1/44

had improvements in diarrhea and growth following sixmonths of immunosuppression [5]. This patient’s diseaseis now controlled with MMF (Personal communication,Cheri Deal, 2009). In 2002, Perheentupa discussed pred-nisone and azathioprine for chronic hepatitis in a patientwith APECED and referred to glucocorticoids and eitherazathioprine or methotrexate in several patients withdiarrhea [6]. Immunosuppression with prednisone andazathioprine, and subsequently with cyclosporin A, wasreported following renal transplantation for chronicinterstitial nephritis in a patient with APECED. Im-munosuppression was unsuccessful with azathioprinebut successful with cyclosporin A [7]. A patient withAPECED with pure red cell aplasia responding well toMMF has also been described [8].Two cautions regarding the use of immunosuppres-
sion for patients with APECED are reported [6]:increased risk of candidiasis-related malignancies, suchas oral malignancies; and increased risk of the progres-sion from localized to systemic candidiasis. Six patientswith APECED with oral or esophageal squamous cellcarcinomas have been described; the youngest was 29years old and immunosuppressed for six years; theothers were not immunosuppressed [6]. It is unclear ifcandida-related malignancies in APECED are related toAPECED or to its treatments [9]. It is also important tonote that immunosuppression for a patient withAPECED is really a decision tailored to the specificdetails of an individual patient. In this case, significantconsideration and discussion among many healthprofessionals and the patient’s family occurred beforeimmunosuppression was started. Furthermore, anydecision to initiate immunosuppression should be ac-companied by a definite plan for monitoring the re-sponse to this new therapy.After four years of follow-up, we have not observed sig-
nificant side-effects of immunosuppression in our youngpatient. When she presents with febrile or infectious ill-nesses, MMF is temporarily discontinued but, within 2–3days, diarrhea increases and she develops hypocalcemia,requiring increased enteral calcium and calcitriol supple-mentation. For our patient, inflammatory markers, diar-rhea, required doses of calcium supplementation andweight gain are good markers of disease activity. Abnor-mal swallowing and silent aspirations are not recognizedfeatures of APECED and it is possible that our patient’srespiratory symptoms may represent new autoimmune-related APECED manifestations or another co-incidentdisease process. Chronic diarrhea is a recognized featureof APECED [6]. Our patient’s diarrhea may representautoimmune gastrointestinal disease, but this was not bi-opsy proven before immunosuppression. Obstipation is arecognized manifestation [10] and our patient has nothad bowel obstructions since MMF was commenced.
ConclusionsImmunosuppression is well tolerated and has resulted indramatic improvement in our young patient with severemanifestations of APECED. We suggest that early initi-ation of immunosuppression, with appropriate monitor-ing, is an acceptable therapy for patients severely affectedwith APECED and that failure of one immunosuppres-sive agent does not infer failure of others.
ConsentWritten informed consent was obtained from the par-ents of this patient (minor) for publication of this casereport and accompanying images. A copy of the writtenconsent is available for review by the Editor-in-Chief ofthe Journal of Medical Case Reports.
AbbreviationsAIRE: Autoimmune regulator; APECED: Autoimmune polyendocrinopathy-candidiasis-ectodermal dysplasia; MMF: Mycophenolate mofetil.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsCSOG conceived the case report, collected the data, interpreted the data,and was a major contributor in writing the manuscript including writing thefirst draft. RSh participated in collection and interpretation of data, andcontributed to writing the manuscript. ILC participated in collection andinterpretation of data and contributed to writing the manuscript. EP, MM,HG, RSch, JU, and EBS participated in data interpretation and contributed towriting the manuscript. DK participated in collection and interpretation ofdata, and was a major contributor in writing the manuscript. EC conceivedthe case report, participated in data interpretation, was a major contributorin writing the manuscript. All authors read and approved the finalmanuscript.
Author details1Divisions of Endocrinology, The Hospital for Sick Children, Toronto, Canada.2Department of Pediatrics, The Hospital for Sick Children, Toronto, Canada.3Divisions of Dermatology, The Hospital for Sick Children, Toronto, Canada.4Divisions of Gastroenterology, Hepatology and Nutrition, The Hospital forSick Children, Toronto, Canada. 5Divisions of Respiratory Medicine, TheHospital for Sick Children, Toronto, Canada. 6Divisions of Rheumatology, TheHospital for Sick Children, Toronto, Canada. 7Divisions of Immunology, TheHospital for Sick Children, Toronto, Canada. 8Divisions of Pediatric Medicine,The Hospital for Sick Children, Toronto, Canada. 9University of Toronto,Toronto, Canada. 10Current affiliation is Department of Paediatrics, GraduateEntry Medical School, University of Limerick, and University Hospital, Limerick,Ireland. 11Graduate Entry Medical School, University of Limerick, Limerick,Ireland.
Received: 1 October 2012 Accepted: 19 December 2012Published: 14 February 2013
References1. Cheng MH, Shum AK, Anderson MS: What’s new in the Aire? Trends
Immunol 2007, 28:321–327.2. Perheentupa J: Autoimmune polyendocrinopathy-candidiasis-ectodermal
dystrophy. J Clin Endocrinol Metab 2006, 91:2843–2850.3. Oftedal BE, Wolff AS, Bratland E, Kampe O, Perheentupa J, Myhre AG,
Meager A, Purushothaman R, Ten S, Husebye ES: Radioimmunoassay forautoantibodies against interferon omega; its use in the diagnosis ofautoimmune polyendocrine syndrome type I. Clin Immunol 2008,129:163–169.
4. Padeh S, Theodor R, Jonas A, Passwell JH: Severe malabsorption inautoimmune polyendocrinopathy-candidosis-ectodermal dystrophy
O’Gorman et al. Journal of Medical Case Reports 2013, 7:44 Page 4 of 5http://www.jmedicalcasereports.com/content/7/1/44
syndrome successfully treated with immunosuppression. Arch Dis Child1997, 76:532–534.
5. Ward L, Paquette J, Seidman E, Huot C, Alvarez F, Crock P, Delvin E, Kampe O,Deal C: Severe autoimmune polyendocrinopathy-candidiasis-ectodermaldystrophy in an adolescent girl with a novel AIREmutation: response toimmunosuppressive therapy. J Clin Endocrinol Metab 1999, 84:844–852.
6. Perheentupa J: APS-I/APECED: the clinical disease and therapy. EndocrinolMetab Clin North Am 2002, 31:295–320. vi.
7. Ulinski T, Perrin L, Morris M, Houang M, Cabrol S, Grapin C, Chabbert-Buffet N,Bensman A, Deschenes G, Giurgea I: Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy syndrome with renal failure: impact ofposttransplant immunosuppression on disease activity. J Clin EndocrinolMetab 2006, 91:192–195.
8. Bakrac M, Jurisic V, Kostic T, Popovic V, Pekic S, Kraguljac N, Colovic M:Pure red cell aplasia associated with type I autoimmune polyglandularsyndrome-successful response to treatment with mycophenolate mofetil:case report and review of literature. J Clin Pathol 2007, 60:717–720.
9. Rautemaa R, Hietanen J, Niissalo S, Pirinen S, Perheentupa J: Oral andoesophageal squamous cell carcinoma–a complication or component ofautoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy(APECED, APS-I). Oral Oncol 2007, 43:607–613.
10. Betterle C, Greggio NA, Volpato M: Clinical review 93: autoimmunepolyglandular syndrome type 1. J Clin Endocrinol Metab 1998,83:1049–1055.
doi:10.1186/1752-1947-7-44Cite this article as: O’Gorman et al.: A child with autoimmunepolyendocrinopathy candidiasis and ectodermal dysplasia treatedwith immunosuppression: a case report. Journal of Medical Case Reports2013 7:44.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit
O’Gorman et al. Journal of Medical Case Reports 2013, 7:44 Page 5 of 5http://www.jmedicalcasereports.com/content/7/1/44