Embed Size (px)
Citation preview
Amal et al. Diagnostic Pathology 2013, 8:36http://www.diagnosticpathology.org/content/8/1/36
CASE REPORT Open Access
A rare primary tumor of the thyroid gland: reporta new case of leiomyosarcoma and literaturereviewBennani Amal*, Hinde El Fatemi, Ihsane Souaf, Kaouthar Moumna and Amarti Affaf
Abstract
Primary leiomyosarcomas of the thyroid gland are extremely rare. we report a case of a 72 year-old women with apainful growing mass of the left neck with skin fistula. The patient underwent a lobectomy. The tumor histologyshowed spindle-shaped cells arranged in interlacing fascicles that expressed desmine and Hcaldesmone, but werenegative for cytokeratins and thyroglobulin. Total body CT scan didnt show any other tumor. The patient died twomonths after surgery. Primary thyroid leiomyosarcoma may be mistaken for other tumors, such as anaplastic ormedullary carcinomas. Therefore, the diagnosis is difficult and requires numerous clinical, radiological, andpathological investigations.Virtual Slides: The virtual slide(s) for this article can be found here: http://www.diagnosticpathology.diagnomx.eu/vs/1917621950869224
Keywords: Primary leiomyosarcoma, Thyroid gland, Anaplastic carcinoma, Medullary carcinoma
IntroductionLeiomyosarcomas are commonly seen in the pelvis, thegastrointestinal tract and the retroperitoneum. They ac-count for 6% of the head and neck tumors. Sarcomas arethought to originate from the wall of blood vessels [1].Primary leiomyosarcomas of the thyroid gland areextremely rare. To the best of our knowledge, only 18cases have been reported around the world. Immunohis-tochemistry showing a smooth muscle-specific antigen ishelpful in establishing the diagnosis. Surgical excision isthe primary treatment of choice. Survival rate is low andapproximately half of the patients die within a shortperiod of time after the diagnosis. We report this newcase in the aim of shedding more light on the primaryleiomyosarcoma of the thyroid and the challenges inmaking the diagnosis and the differential diagnosis withanaplastic and medullary carcinomas.
Case reportWe present a case of a 72 year-old woman with a rapidlygrowing neck mass over a period of two months. Her
* Correspondence: [email protected] of pathology, Hassan II University Hospital, Fez 30000, Morocco
© 2013 Amal et al.; licensee BioMed Central LCommons Attribution License (http://creativecreproduction in any medium, provided the or
past medical history includes a multinodular goiter diag-nosed two years ago with no follow-up.At the physical exam we found a painful mass of the left
neck with fistulae to the skin. She is clinically euthyroidwith normal plasma level of thyroid stimulating hormones.A total body scan didn’t show any other mass.The patient underwent a surgical exploration. There
was a hard, irregular tumor of the whole left lobe of thethyroid gland, which was attached to the sterno-thyroidianmuscle and the left cervical pedicle. A left lobectomy wasrealized. As the tumor largely invaded the surrounding tis-sues, a curative operation seemed impossible.The resected lobe measured 8.5 cm in the largest dimen-
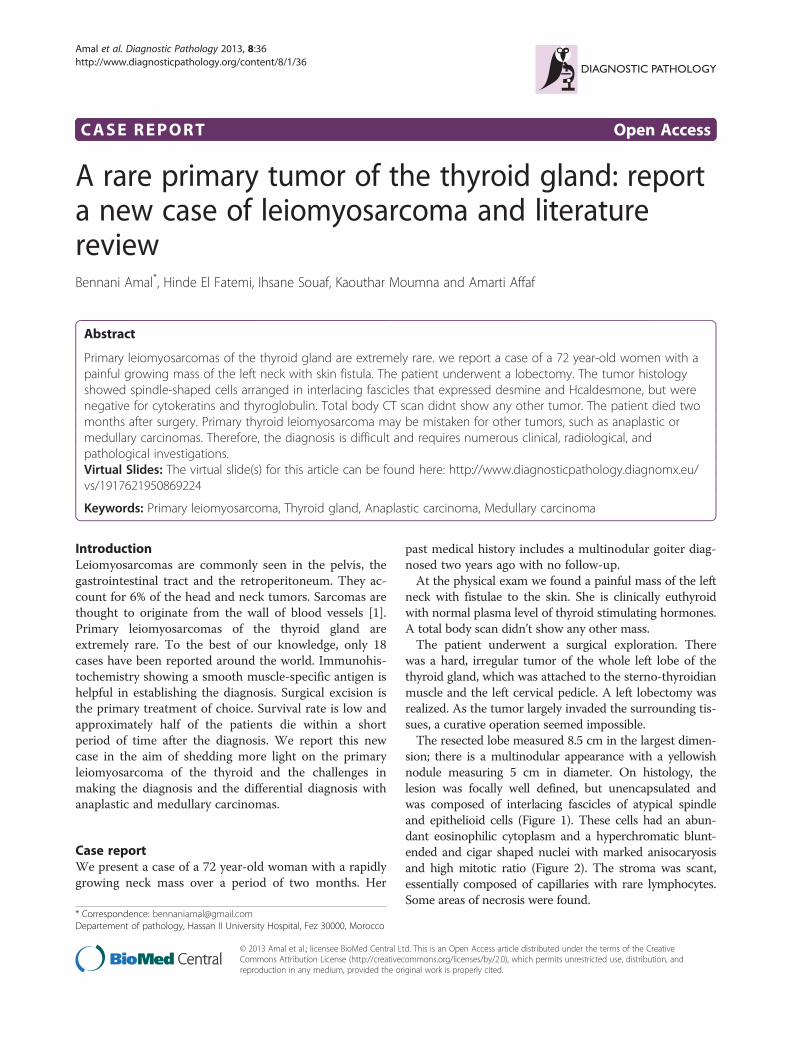
sion; there is a multinodular appearance with a yellowishnodule measuring 5 cm in diameter. On histology, thelesion was focally well defined, but unencapsulated andwas composed of interlacing fascicles of atypical spindleand epithelioid cells (Figure 1). These cells had an abun-dant eosinophilic cytoplasm and a hyperchromatic blunt-ended and cigar shaped nuclei with marked anisocaryosisand high mitotic ratio (Figure 2). The stroma was scant,essentially composed of capillaries with rare lymphocytes.Some areas of necrosis were found.
td. This is an Open Access article distributed under the terms of the Creativeommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andiginal work is properly cited.
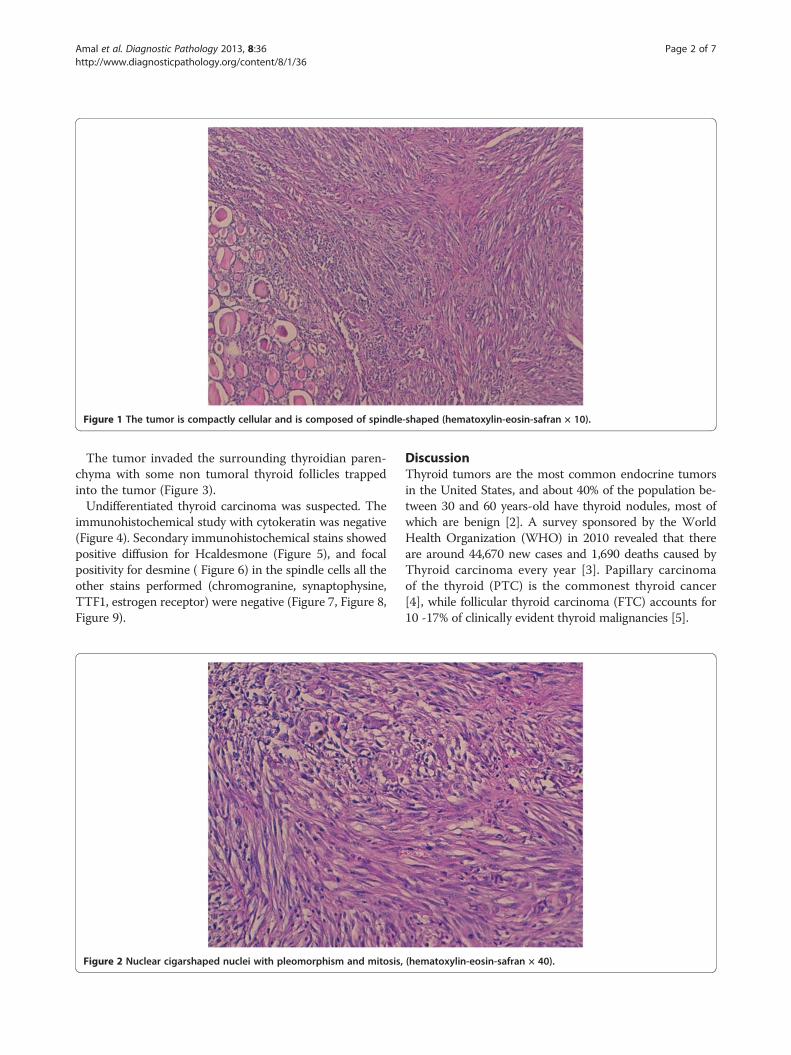
Figure 1 The tumor is compactly cellular and is composed of spindle-shaped (hematoxylin-eosin-safran × 10).
Amal et al. Diagnostic Pathology 2013, 8:36 Page 2 of 7http://www.diagnosticpathology.org/content/8/1/36
The tumor invaded the surrounding thyroidian paren-chyma with some non tumoral thyroid follicles trappedinto the tumor (Figure 3).Undifferentiated thyroid carcinoma was suspected. The
immunohistochemical study with cytokeratin was negative(Figure 4). Secondary immunohistochemical stains showedpositive diffusion for Hcaldesmone (Figure 5), and focalpositivity for desmine ( Figure 6) in the spindle cells all theother stains performed (chromogranine, synaptophysine,TTF1, estrogen receptor) were negative (Figure 7, Figure 8,Figure 9).
Figure 2 Nuclear cigarshaped nuclei with pleomorphism and mitosis,
DiscussionThyroid tumors are the most common endocrine tumorsin the United States, and about 40% of the population be-tween 30 and 60 years-old have thyroid nodules, most ofwhich are benign [2]. A survey sponsored by the WorldHealth Organization (WHO) in 2010 revealed that thereare around 44,670 new cases and 1,690 deaths caused byThyroid carcinoma every year [3]. Papillary carcinomaof the thyroid (PTC) is the commonest thyroid cancer[4], while follicular thyroid carcinoma (FTC) accounts for10 -17% of clinically evident thyroid malignancies [5].
(hematoxylin-eosin-safran × 40).

Figure 3 The tumor often invades the surrounding thyroidian parenchyma with some non tumoral thyroid follicles trapped into thetumor (×5).
Amal et al. Diagnostic Pathology 2013, 8:36 Page 3 of 7http://www.diagnosticpathology.org/content/8/1/36
Primary leiomyosarcoma of the thyroid gland is ex-ceedingly rare and accounts for 0.014% of 28 630 thyroidtumors in one series [6]. It occurred in older patientswith a mean age of 67 years with a predominance ofwomen, though one pediatric case of a 6-year-old boyhad been reported [7]. Patients often complained of anenlarging cervical mass with Obstructive symptoms.Most reports in the literature showed that the thyroid
function test is often normal. Thyroid scans can show a
Figure 4 Immunohistochemical study with cytokeratin which was neg
cold nodule or an enlarged gland with areas of increasedand decreased uptake of radioactive iodine. Ultrasoundsshow an ill-defined or well-defined hypoechogenic mass, asolid partially cystic nodule , or a calcified nodule. At com-puted tomography, the tumor presents as a low-densitymass with dense calcification and necrotic portions. Inaddition, computed tomography sometimes shows a directtumoral invasion of the adjacent structures. In the currentcase, the patient had clinically a locoregional extension.
ative.

Figure 5 The tumor cells are stained with anti–hcaldesmone.
Amal et al. Diagnostic Pathology 2013, 8:36 Page 4 of 7http://www.diagnosticpathology.org/content/8/1/36
At gross examination, the tumors either almost entirelyreplace one thyroid lobe or presents as an irregularlyoutlined or a well-demarcated intrathyroidian nodule.Cut surfaces show a pinkish, yellowish, white, fascicular
or homogenous, unencapsulated nodule with necrosis orcystic degeneration. Histologicaly, the tumor is composedof interlacing fascicles or bundles of eosinophilic spindlecells with normochromatic to hyperchromatic, blunt-ended, and cigar shaped nuclei, generally centrally locatedwithin the cell. Mitoses are occasional to frequent. Variablelevels of cellular and nuclear pleomorphism are present.Areas of hemorrhage, hyalinization, myxoid changes, and
Figure 6 The tumor cells are stained with anti–desmine.
necrosis may be found with occasional calcifications.Thetumor often invades the surrounding thyroidian paren-chyma. Vascular invasion can be seen. Tumor cells arestained with vimentin, (alpha-) smooth muscle actin, andmuscle-specific actin with a variable expression of desmin.Cytokeratin, thyroglobulin, calcitonin, protein S100, andchromogranin are never expressed.The diagnosis of primary leiomyosarcomas of the thy-
roid gland requires particular prudence, because they areoften ill-defined, and invade the thyroid capsule and theadjacent cervical structures. It seems important to excludea direct extension to the thyroid gland by a non thyroidian

Figure 7 There is no positivity for estrogen receptor.
Amal et al. Diagnostic Pathology 2013, 8:36 Page 5 of 7http://www.diagnosticpathology.org/content/8/1/36
cervical leiomyosarcoma. Indeed, approximately 1% of thehead and neck sarcomas are leiomyosarcomas, most com-monly located at the scalp, paranasal sinuses, and jaws [8].Surgical explorations as well as gross and microscopicpathologic examinations are indispensable for a correctidentification of tumor origin. In our case, it showed atumor of the thyroid that was attached to the muscleand cervical pedicle. Furthermore, it is important to ex-clude thyroid metastases of a distant leiomyosarcoma. Itis believed that approximately 1% of thyroid cancers are
Figure 8 There is no positivity for TTF1.
metastases to the thyroid gland. In autopsy series, thy-roid metastases have been found to occur in up to 24%of patients who died of cancer [9]. Thus, only clinicalexamination and appropriate imaging studies will helpin making the diagnosis. In our case, both physical examand total body scan didn’t show any other tumor. More-over, more features were in favor of primitive lesion: itis a solitary lesion (all the few cases of metastaticleiomyosarcoma reported in literature presented clinic-ally with multiple metastasis at lungs and bones), and it

Figure 9 There is no positivity for chromogranine or synaptophysine.
Amal et al. Diagnostic Pathology 2013, 8:36 Page 6 of 7http://www.diagnosticpathology.org/content/8/1/36
had bad outcome (patient died within two months aftersurgery).The main differential pathologic diagnoses includes un-
differentiated (anaplastic) thyroid carcinomas (UTCs), soli-tary fibrous tumors, spindle cell tumors with thymus-likedifferentiation, medullary carcinoma and other sarcomas.Undifferentiated (anaplastic) thyroid carcinomas may dis-play a very polymorphic microscopic features, includingspindle cells that can mimic the microscopic appearanceof fibrosarcoma, leiomyosarcoma, or malignant fibroushistiocytoma. Epithelial markers can be missing in approxi-mately 20% of cases [10] and even more often in spindlecell sarcomatoid UTCs. Vimentin is also expressed in morethan 50% of UTCs [11]. Desmin and muscle-specific actin,which are good markers of leiomyosarcomas, are neverexpressed in UTCs [11]. Solitary fibrous tumors are pre-dominantly composed of spindle cells, with various ar-rangement. It is usually positive for CD34, BCL2, CD99,and vimentin. Spindle cell tumors with thymus-like differ-entiation is in most case biphasic, composed of compactinterlacing, or reticulated highly cellular fascicles of spindlecells and tubulopapillary glands. In immunohistochemistry,both spindle cells and glandular cells are positive forcytokeratins, and rarely the spindle cells exhibit stainingwith some muscle markers. Medullary carcinoma canmimic any tumor structurally and functionally [12]. It canshow variable microscopic features, including spindle cells.In immunochemistry, tumor cells are positive for chromo-granine A, synaptophysine, ACE and calcitonine.The etiology of primary leiomyosarcomas of the thyroid
gland still remains unknown. No history of previous cer-vical radiation exposure in such cases had been reportedtill now. As it was observed that a blood vessel was the
point of origin of a leiomyosarcoma of the thyroid gland[13], the histogenesis of leiomyosarcoma may be from thesmooth muscle in the vascular walls.In our case, the diagnosis of leiomyosarcoma was
made on the pathological, and immunohistochemicalfeatures of the tumor, which were similar to those foundin the literature.Despite surgical excision, most patients die after 1 to
51 months or get a metastatic disease: (lungs, lymphnodes, liver, myocardium, kidney, pancreas, small bowel,colon, peritoneum, brain, and bones) [14]. Two caseshave been reported, in which the patients were still alivewith no evidence of disease, with a follow-up of 15 and25 months [15].
ConclusionIn summary, primary leiomyosarcoma of the thyroid isextremely rare. It is a challenging diagnosis to make dueto its differential diagnosis with anaplastic and medullarycarcinoma. But before making this diagnosis, it is im-portant to exclude a metastasis to the thyroid gland of adistant leiomyosarcoma or a thyroid extension of a nonthyroidian cervical leiomyosarcoma.
ConsentWritten informed consent was obtained from the pa-tient’s parents for publication of this case report and anyaccompanying images.
Competing interestsThe authors declare that they have no competing interests.

Amal et al. Diagnostic Pathology 2013, 8:36 Page 7 of 7http://www.diagnosticpathology.org/content/8/1/36
Authors’ contributionsAB wrote the manuscript and performed the literature review. HE revised themanuscript for important intellectual content, IS, KM and AA were majorcontributors to writing the manuscript. All authors read and approved thefinal manuscript.
AcknowledgmentsThe authors thank SOUFI LAMIAA and LAKHSASSI MOHAMED KARIM MD.who participated in the English translation of the manuscript.
Received: 11 December 2012 Accepted: 20 February 2013Published: 27 February 2013
References1. Tran LM, Mark R, Meier R, Calcaterra TC, Parker RG: Sarcomas of the head
and neck: prognostic factors and treatment strategies. Cancer 1992,70:169–177.
2. Saleh HA, Bo J, John B, Opada A: Utility of immunohistochemical markersin differentiating benign from malignant follicular-derived thyroidnodules. Diagn Pathol 2010, 5:9 (26 January 2010).
3. Qingbin S, Deguang W, Yi L, Changsi L, Changqing F, Xiangmin H, JianhuaL: Diagnostic significance of CK19, TG, Ki67 and galectin-3 expression forpapillary thyroid carcinoma in the northeastern region of China. DiagnPathol 2011, 6:126 (21 December 2011).
4. Dina El D, Ahmed N, Salem A: Application of CD56, P63 and CK19immunohistochemistry in the diagnosis of papillary carcinoma of thethyroid. Diagn Pathol 2008, 3:5 (6 February 2008).
5. Xiaoqi L, Bing Z, Yulin L, Silverman JF: Follicular thyroid carcinoma invadesvenous rather than lymphatic vessels. Diagn Pathol 2010, 5:8 (22 January 2010).
6. Thompson LD, Wenig BM, Adair CF, Shmookler BM, Heffess CS: Primarysmooth muscle tumors of the thyroid gland. Cancer 1997, 79:579–587.
7. Andrion A, Bellis D, Delsedime L, et al: Leiomyoma and neurilemoma:report of two unusual non-epithelial tumours of the thyroid gland.Virchows Archiv Pathol Anat 1988, 413:367–372.
8. Akcam T, Oysul K, Birkent H, et al: Leiomyosarcoma of the head and neck:report of two cases and review of the literature. Auris Nasus Larynx 2005,32:209–212.
9. Lin JD, Weng HF, Ho YS: Clinical and pathological characteristics ofsecondary thyroid cancer. Thyroid 1998, 8:149–153.
10. Ordonez NG, El-Naggar AK, Hickey RC, et al: Anaplastic thyroid carcinoma.Immunocytochemical study of 32 cases. Am J Clin Pathol 1991, 96:15–24.
11. Just PA, Guillevin R, Capron F, et al: An unusual clinical presentation of arare tumor of the thyroid gland: report on one case of leiomyosarcomaand review of literature. An of Diag Path 2008, 12:50–56.
12. Kamaljeet S, Sharma MC, Deepali J, Rajinder K: Melanotic medullarycarcinoma of thyroid – report of a rare case with brief review ofliterature. Diagn Pathol 2008, 3:2 (11 January 2008).
13. Thompson LD, Wenig BM, Adair CF: Primary smooth muscle tumors of thethyroid gland. Cancer 1997, 79:579–587.
14. Adachi M, Wellmann KF, Garcia R: Metastatic leiomyosarcoma in brain andheart. J Pathol 1969, 98:294–296.
15. Ozaki O, Sugino K, Mimura T, et al: Primary leiomyosarcoma of the thyroidgland. Surg Today 1997, 27:177–180.
doi:10.1186/1746-1596-8-36Cite this article as: Amal et al.: A rare primary tumor of the thyroidgland: report a new case of leiomyosarcoma and literature review.Diagnostic Pathology 2013 8:36.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit






![Metastatic Spermatic Cord Tumor From Colorectal Cancer...A spermatic cord tumor is unusual, and, in particular, a metastatic tumor of the spermatic cord is very rare [1, 2]. The primary](https://img.pdfslide.net/doc/110x75/60f81a86b8201957b46aac37/metastatic-spermatic-cord-tumor-from-colorectal-cancer-a-spermatic-cord-tumor.jpg)






















