Embed Size (px)
Citation preview

Annals ofthe Rheumatic Diseases, 1983, 42, 98-102
Case report
Pachydermoperiostosis: scintigraphic,thermographic, plethysmographic, andcapillaroscopic observationsADEL G. FAM, HYACINTH CHIN-SANG, AND COLIN A. RAMSAYFrom the Departments of Medicine and Radiology, University of Toronto, and Rheumatic Disease Unit,Sunnybrook Medical Centre, Toronto, Ontario, Canada
SUMMARY A unique case of pachydermoperiostosis, multiple epiphyseal dysplasia, and secondaryosteoarthritis is described. An additional interesting feature was the presence of acroosteolysis ofthe distal phalanges of fingers and toes. Scintigraphic, thermographic, plethysmographic, andcapillaroscopic studies suggested increased blood flow through clubbed fingers, raising the possibil-ity that this may play a role in the pathogenesis of pachydermoperiostosis.
Pachydermoperiostosis (primary or idiopathic hyper-trophic osteoarthropathy) is a rare, often familialdisease characterised by digital clubbing, cylindricalthickening of legs and forearms, sebaceous glandoveractivity, hyperhidrosis, and symmetri-cal irregular periosteal ossification predominantlyaffecting the distal ends of long bones.`-3Reported here is a unique case of pachydermo-
periostosis and multiple epiphyseal dysplasia. Scinti-graphic, thermographic, plethysmographic, andcapillaroscopic findings suggested increased bloodflow through clubbed digits. An additional, interest- ;.ing feature was the presence of acroosteolysis of thedistal phalanges of fingers and toes, a finding whichhas rarely been described in pachydermo-periostosis.`
Case report
A 56-year-old single Italian woman presented in1979 with a history of clubbed fingers and toesassociated with deformities of feet, knees, and elbowsdating back to childhood. Excessive greasiness ofskin, profuse perspiration of hands and feet, and -'marked thickening of the skin of the face, forearms,hands, and legs had been present for an indeter-minate period. She had noticed pain in the legs andlforearms since her late teens. Arthritis involving hips,knees, elbows, wrists, and ankles had been no*d for _ _Accepted for publication 8 December 1981.Correspondence to Dr Adel G. Fam, Rheumatic Disease Unit,Sunnybrook Medical Centre, 2075 Bayview Avenue, Toronto, Fig. 1 Symmetrical cylindrical enlargement oflegs, genuOntario, Canada M4N 3M5. valgus deformity, and clubbing of the toes.
98
on July 7, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.42.1.98 on 1 F
ebruary 1983. Dow
nloaded from

Pachydermoperiostosis 99
Fig. 2 Patient's right hand showing clubbing andthickening of the digits.
many years. Pain and stiffness in knees and hipsbecame progressively worse during the previous 2years, and she experienced great difficulty walking.There was no family history of the disease.
She was of average intelligence and 130 cm (4 ft3 in) tall. Pertinent findings included an oily skin,general hyperhidrosis, deep furrowing of the fore-head, symmetrical cylindrical enlargement of legsand forearms (Fig. 1), with irregular thickening oftibiae and fibulae, and unusually large hands and feet
Fig. 3 Right ankle showing diffuse, shaggy periostealthickening of distal end of the tibia (arrows) and fibula andslanting of the ankle joint mortise from the lateral to themedial side.
with gross bulbous clubbing (Fig. 2). She hadrestricted movement of hip, knee, ankle, talocal-caneal, shoulder, elbow, and wrist joints; flexiondeformity and crepitus of the elbows; valgus defor-mity of the knees without effusion; and planovalgus
Fig. 4 Radiographs ofhandshowing resorption of distalphalanges.
on July 7, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.42.1.98 on 1 F
ebruary 1983. Dow
nloaded from

100 Fam, Chin-Sang, Ramsay
Fig. 5 Anteroposteriorradiographs ofknees showingangular tibial condyles withirregular articular surfaces,degenerative arthritis, and osseousbodies in the left knee.
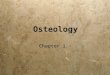
Fig. 6 Scintigraphs of the hands showing accumulation ofthe isotope in the finger tips.
deformity of the feet, with short metatarsals andstubby toes. Neurological examination was un-
remarkable.Her haemoglobin was 14 2 g/dl, leucocyte count
9200/mm3 (9.2 x 109/l), erythrocyte sedimentationrate 28 mm/h, and normal serum calcium, phos-phorus, alkaline phosphatase, uric acid, protein
electrophoresis, thyroid indices, creatinine, and urineanalysis. Tests for rheumatoid and antinuclear fac-tors were negative, the VDRL was nonreactive, andtotal haemolytic complement was normal. Radio-graphic examination showed generalised soft-tissueswelling with digital clubbing, irregular periostealproliferation with cortical thickening of distal parts ofthe tibiae, fibulae, radii, and ulnae (Fig. 3), andresorption of the distal phalanges of the fingers (Fig.4) and toes. Multiple epiphyseal abnormalities,including irregular tibial surfaces, deficient epiphysesof tibial tuberosities (Fig. 5), flattening of femoralheads, and irregularities of distal humeral epiphysesand tarsal and carpal bones, were also observed.Other findings included a characteristic downwardinclination of the distal tibial articular surface fromlateral to medial side (Fig. 3); short, broad metatar-sals, and secondary osteoarthritis of hip, knee, ankle,talocalcaneal, shoulder, elbow, and wrist joints.Radiographs of the chest, skull, and spine were nor-mal.
SPECIAL STUDIESA 99mTc methylene diphosphonate bone scintiscanrevealed pericortical linear concentration of theradionuclide along the distal tibial and fibular shafts,and increased uptake in the elbows and knees. Theblood pool images also showed accumulation of thenuclide in the finger tips (Fig. 6). Thermography ofthe hands showed hyperthermia of the distal ends of
on July 7, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.42.1.98 on 1 F
ebruary 1983. Dow
nloaded from

Pachydermoperiostosis 101
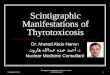
Fig. 7 Svnovial biopsy from theright knee showing mild svnoviallining cell hyperplasia andthickening ofsubsynovial bloodvessels. (Haematoxvlin and eosin,x 235).
several digits, most marked in the thumbs and leftindex finger. Photoelectric plethysmography(method of Challoner and Ramsay') revealedincreased blood flow to several of the clubbed fingersas compared with a control. Nail bed capillary micro-scopy revealed slight capillary enlargement andincreased tortuosity. A needle synovial biopsy of theright knee showed mild synovial lining cell hyper-plasia, increased vascularity, and marked thickening ofsmall subsynovial blood vessels with fibrosis (Fig. 7).
Discussion
Points of interest in this report pertain to clinicalfeatures and results of special investigations. Thepatient described fits all the classic features ofpachydermoperiostosis.1- Although patients withpachydermoperiostosis often complain of arthralgiaand bone pains, deforming arthritis is not a promi-nent feature.1-3 In this patient, however, severedegenerative arthritis, particularly of knees, wrists,elbows, and hips, dominated the clinical picture. Shewas of below average height, and further radio-graphic studies revealed typical findings of multipleepiphyseal dysplasia (MED),P-` with defectiveepiphyseal development, marked deformities ofarticular surfaces, secondary osteoarthritis, shortstubby metatarsals, and characteristic sloping of theankle mortise (slant sign).-10 Spondyloepiphysealdysplasia was excluded by the lack of spinalinvolvement.Another unusual finding in this case was the pres-
ence of acroosteolysis of the distal phalanges of fingersand toes. This rare feature of pachydermoperiostosis
is not widely recognised. The occurrence of acro-osteolysis in association with finger clubbing in thesepatients helps to differentiate pachydermoperiostosisfrom other conditions of which osteolysis is a fea-ture.'The association of pachydermoperiostosis and
MED has not to our knowledge been previouslyreported. A familial incidence has been observed inboth conditions. The 2 diseases are often transmittedas an autosomal dominant with variable express-ivity.1-5 8-11There is also evidence in some cases of MED for a
pattern of autosomal recessive inheritance.12 Theoccurrence of MED in association with pachydermo-periostosis in this case is probably coincidental andraises the possibility of multiple gene abnormalities.No suggestion of either condition was found in othermembers-of the family, suggesting that the geneticdefect arose de novo in this patient.
Synovial histopathological findings in our patientincluded mild synovial lining cell hyperplasia,increased vascularity, and marked thickening of sub-synovial blood vessels. Synovial membrane abnor-malities were described in 2 other patients withpachydermoperiostosis.-13 Similar pathologicalchanges were observed in both, and electron micro-scopy in one of them11 revealed multilayered base-ment membrane laminae around small subsynovialblood vessels. It is of interest that morphological andultrastructural studies of the synovial membrane insecondary hypertrophic osteoarthropathy have alsoshown prominent microvascular abnormalities.14The scintigraphic findings in this case are anal-
ogous to those described in secondary hypertrophic
on July 7, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.42.1.98 on 1 F
ebruary 1983. Dow
nloaded from

102 Fam, Chin-Sang, Ramsay
osteoarthropathy: symmetrical pericortical uptakeover long bones, increased concentration of theradionuclide by involved joints, and accumulation ofthe nuclide in the finger tips."-'6 In a recent studyfrom Yugoslavia7 similar scintigraphic abnormalitieswere observed in 10 of 13 patients with pachydermo-periostosis.
Little is known of the pathogenesis ofpachydermoperiostosis with the exception of thegenetic factor. Similarities in clinical manifestationsand anatomical findings in pachydermoperiostosisand secondary hypertrophic osteoarthropathy havesuggested a common pathogenetic mechanism.' Evi-dence of an increased rate of blood flow through theaffected parts has been demonstrated in patients withsecondary hypertrophic osteoarthropathy. 17-19Scintigraphic, thermographic, plethysmographic,and capillaroscopic studies in our patient stronglysuggested an increased blood flow in the clubbedfingers. Our findings are in agreement with theYugoslavian study.7 Hypervascularity of distal partsof fingers was observed in all 5 patients in whomarteriography was performed. Scintigraphy in 10 of13 patients of the same study showed accumulationof the radionuclide in the distal ends of digits, sug-gesting that the metabolic activity and/or blood flowto the clubbed digits is increased. These results arecontrary to 2 previous studies of peripheral bloodflow in pachydermoperiostosis. In one study of 2patients2 angiography revealed decreased blood flowthrough the forearms and hands, while water-sealplethysmography of the distal forearms showed anormal flow rate. In a second study20 of a case ofpachydermoperiostosis angiography showed ob-struction of blood flow through the forearms andhands, and nail bed capillaroscopy showed scanty,irregular capillary loops. It should be emphasised,however, that these 2 studies were performed at atime when the disease was thought to be inactive. Thedisease was probably still active in our patient, assuggested by the scintigraphic and thermographicfindings and the presence of persistent bone pain andtenderness. These observations are in agreementwith the view that peripheral blood flow is increasedduring the early active phase of pachydermo-periostosis and is reduced in the late inactivephase."220 The postulate is further supported by theresults of pathological studies showing highly vascu-lar periosteal new bone in early phases of the diseaseand compact, relatively avascular bone in late stages.'The question whether local vascular disturbances
relate to the pathogenesis of pachydermoperiostosisremains unresolved. The present study indicates thatsuch a relationship may exist and that the active
phase of the disease is associated with increasedblood flow through the clubbed digits. A systematicstudy of a larger population of patients withpachydermoperiostosis is needed.
The authors thank Dr Frances Leung for performing the nail bedcapillaroscopy and Mrs Janet Hays for preparation of the manu-script.
References
1 Vogl A, Goldfischer S. Pachydermoperiostosis: primary oridiopathic hypertrophic osteoarthropathy. Am J Med 1962; 33:166-87.Rimoin D L. Pachydermoperiostosis (idiopathic clubbing andperiostosis). Genetic and physiologic considerations. N Engl JMed 1965; 272: 924-31.Herbert D A, Fessel W J. Idiopathic hypertrophic osteoarth-ropathy (pachydermoperiostosis). WestJ Med 198 1; 134: 354-7.Guyer P B, Brunton F J, Wren M W G. Pachydernoperiostosiswith acro-osteolysis. A report of five cases. J Bone Joint Surg1978; 60B: 219-23.Hedayati H, Barmada R, Skosey J L. Acrolysis in pachyder-moperiostosis. Primary or idiopathic hypertrophic osteoarth-ropathy. Arch Intern Med 1980; 140: 1087-8.
6 Challoner A V J, Ramsay C A. A photoelectric plethysmographfor the measurement of cutaneous blood flow. Phys Med Biol1974; 19: 317-28.Jajic I, Pecina M, Krstulovic B, Kovacevic D, Pavicic F, SpaventiS. Primary hypertrophic osteoarthropathy (PHO) and changes inthe joints. Scand J Rheumatol 1980; 9: 89-96.Barrie H, Carter C, Sutcliffe J. Multiple epiphyseal dysplasia. BrMed J 1958; ii: 133-7.Leeds N E. Epiphyseal dysplasia multiplex. A J R 1960; 84:506-1 0.
10 Murphy M C, Shine I B, Stevens D B. Multiple epiphysealdysplasia. Report of a pedigree. J Bone Joint Surg 1973; 55A:814-20.Gibson T, Highton J. Multiple epiphyseal dysplasia: a familystudy. Rheumatol Rehabil 1979; 18: 239-42.
12 Gamboa I, lisker R. Multiple epiphyseal dysplasia tarda. A familywith autosomal recessive inheritance. Clin Genet 1974; 6: 15-9.13 Lauter S A, Vasey F B, Huttner I, Osterland C K. Pachyder-moperiostosis: studies on the synovium. J Rheumatol 1978; 5:
85-95.4 Schumacher Jr H R. Articular manifestations of hypertrophicpulmonary osteoarthropathy in bronchogenic carcinoma. A clini-
cal and pathologic study. Arthritis Rheum 1976; 19: 629-36.Rosenthall L, Kirsh J. Observations on radionuclide imaging inhypertrophic pulmonary osteoarthropathy. Radiology 1976; 120:359-62.
16 Altman R D, Tenenbaum J. Hypertrophic osteoarthropathy. In:Kelley W N, Harris E D, Ruddy J, Sledge C B, eds. Textbook ofRheumatology. 1st ed. New York: Saunders, 1981: 1647-57.
1 Vogl A, Blumenfeld S, Gutner L B. Diagnostic significance ofpulmonary hypertrophic osteoarthropathy. Am J Med 1955; 18:51-65.
18 Holing H E, Brodey R S, Boland H C. Pulmonary hypertrophicosteoarthropathy. Lancet 1961; ii: 1269-74.9 Rutherford R B, Rhodes B A, Wagner H N. The distribution ofextremity blood flow before and after vagotomy in a patient withhypertrophic pulmonary osteoarthropathy. Dis Chest 1969; 56:19-23.Kerber R E, Vogl A. Pachydermoperiostosis. Peripheral circulat-ory studies. Arch Intern Med 1973; 132: 245-8.
on July 7, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.42.1.98 on 1 F
ebruary 1983. Dow
nloaded from