Embed Size (px)
Citation preview

Int J Clin Exp Pathol 2014;7(7):4519-4522www.ijcep.com /ISSN:1936-2625/IJCEP0000961
Case Report Successful treatment of recurrent Kimura’s disease with radiotherapy: a case report
Zongye Wang1, Jianzhong Zhang2, Ye Ren1, Zhuojie Dai1, Huizhen Ma1, Di Cui1, Xiaoming Su1, Shu-Jun Song2
1Department of Radiation Oncology, 306 Hospital of PLA, Beijing 100101, China; 2Department of Pathology and Experimental Medicine, 306 Hospital of PLA, Beijing 100101, China
Received May 31, 2014; Accepted June 24, 2014; Epub June 15, 2014; Published July 1, 2014
Abstract: Kimura’s disease is a rare, chronic inflammatory disorder affecting the skin and subcutaneous tissue, predominantly in the head and neck region. It is benign but may be recurrent and difficult to eradicate. A case of recurrent Kimura disease in a 53-year-old man was reported. Radiation therapy was performed for recurrence after surgical excision twice. The prescribed radiation dose was 36 Gy. With a follow-up time of 68 months, the patient was free of the disease.
Keywords: Kimura’s disease, recurrence, radiotherapy
Introduction
Kimura’s disease (KD) or eosinophilic lymphfol-liculoid granuloma is rare benign disorder and was first described by Kim and Zeto in China in 1937 [1] and characterized by Kimura et al in 1948 [2]. The disease most commonly occurs in young adult Asian men and has a favorable prognosis. The peak age of onset is the third decade. It is a chronic inflammation lesion and predominantly involves deep subcutaneous tis-sue and lymph nodes of head and neck region. Kimura’s disease is often associated with regional lymphadenopathy, solitary or multiple subcutaneous nodules, sometimes with sali-vary gland enlargement and elevated serum immunoglobulin E (IgE) levels and peripheral blood eosinophilia [3]. Histopathology of KD shows a marked follicular hyperplasia, eosino-philic infiltrates, and proliferation of post capil-lary venules [4]. Although KD is a benign condi-tion the lesions can be very difficult to manage. Recurrence rate is very high (above 60%) after local excision [5]. Previous cases of KD treated with surgery and cyclosporine have been pub-lished. We report a patient of recurrent neck KD successfully treated with radiotherapy.
Case report
A 53-year-old Chinese man with diabetes for two years and presented with recurrence of
multiple small firmed subcutaneous masses mainly on his right side neck. Two years ago, he was first found several firmed nodules on his right side neck with red and swollen skin. He was diagnosed of tuberculosis (TB) and treated with rimifon (Nydrazid or isoniazid) and rifampin (rifampicin) for one month by local hospital and stopped treatments since the side effects of medicine on liver. However, the size of masses became larger (growing) during the treatment. After 2 months, the masses had been removed by surgery in local hospital and were diagnosed as inflammation of lymph nodes. Ten months after the surgery and nodules were recurrent at right side neck and treated by using anti-TB drugs for two months, but the treatment was terminated owing to skin allergy. Then the patient was referred to a hospital in Beijing. The masses were excision second time by surgery 10 months after recurrence. Based on the his-tology he was diagnosed as KD. Four months later, he developed masses third time on the same location and was referred to this hospital. Excision biopsy was performed.
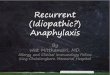
Histological examination (Figure 1) revealed a reactive lymph follicular hyperplasia with promi-nent germinal centers that were surrounded by fibrous tissue. This was accompanied by promi-nent proliferative blood vessels and postcapil-lary venule proliferation. Numerous eosinophils infiltrated the interfollicular areas and formed

Kimura’s disease with radiotherapy
4520 Int J Clin Exp Pathol 2014;7(7):4519-4522
scattered eosinophilic microabscesses in some areas. Based on these clinical and histological findings, He was made a diagnosis of recurrent KD.
Laboratory investigations revealed increased eosinophils (1.01 x 109 ⁄ L; normal 0.02-0.52 x 109 ⁄ L) and elevated serum IgE levels (537.2 IU⁄mL, normal 1.31-165.3 IU/ml). Results of other investigations including kidney and liver function were all within normal.
B ultrasound scan revealed that multiple small subcutaneous masses occupying the neck region. The largest one was 1.9 cm x 0.7 cm x 0.7 cm in size. CT scan showed that the largest mass was 1.7 cm x 1.1 cm x 1.1 cm (Figure 2A).
The patient was treated with X-ray radiation therapy. The prescribed radiation doses were
36 Gy, with 2 Gy per fraction, 5 fractions per week. After treatment the masses significantly reduced in size (Figure 2B). The patient’s condi-tion has remained free from recurrence throughout the 68-month follow-up period.
Discussion
So far, the etiology for KDis still unknown [6]. Kimura’s disease is a rare benign eosinophilic folliculoid granuloma. Clinical presentation is predominantly affecting deep subcutaneous tissue and lymph nodes of head and neck region [6, 7]. Its histological characteristics are the follicular hyperplasia, eosinophilic infiltrates and proliferation of postcapillary venules [8]. The clinical and histological features of this present case are consistent with the changes of KD. Although it was developed in a common
Figure 1. Photomicrographic features of Kimura’s disease (H&E). A. Markedly reactive follicular lymphoid hyperpla-sia with prominent germinal centers and diffuse inflammatory cell infiltrate separated with fibrous tissue. Original magnification, x 100. B. Hyperplastic lymphoid follicle with eosinophilic infiltrate within the skeletal muscle. Original magnification, x 100. C. The interfollicular infiltration was rich in proliferative blood vessels and eosinophilic infil-trate. Original magnification, x 400. D. Eosinophils forming eosinophilic microabscesses with higher magnification. Original magnification x 400.

Kimura’s disease with radiotherapy
4521 Int J Clin Exp Pathol 2014;7(7):4519-4522
location of KD, it was a rare disease and recur-rent twice. So far only hundreds of patients were reported. It does not become widely rec-ognized, and very easily to be misdiagnosed as other diseases. For current case it was misdi-agnosed as TB in a local hospital and treated with anti-TB drugs. In addition to TB, differential diagnosis should also be made from subcuta-neous soft tissue tumors, lymphoproliferative or granulomatous lesions, reactive lymphade-nopathy, hyperplasia and benign tumors of sub-cutaneous vascular proliferations.
Though KD is a benign disease, its unpredict-able response to the therapeutic interventions, poses a great challenge to the treating physi-cian and the patients. There is no consensus about the optimal treatment for Kimura’s dis-ease. The medical therapies for Kimura dis-ease including surgical resection, regional or systemic steroid therapy, radiotherapy, cytotox-ic and laser therapy have been utilized, but none has been proved to be the optimum modality [6, 9, 10]. Surgery with complete exci-sion is difficult since the infiltrative nature of the lesion and swelling of regional lymph nodes [11]. Recurrent lesions may develop several times after initial presentation and surgical removal. It has been suggested that drug ther-apy is the first choice in middle-aged or elderly
patients with KD [12]. Steroid therapy has been shown transiently effective, after weaning, the tumors often increase in size [4]. Recently, anti-IgE therapy has been introduced [13]. In the report there patients of KD were treated with anti-IgE (omalizumab) for four months. The size of diseased regions and the peripheral blood eosinophil were all decreased after anti-IgE therapy, but complete remission of the tumor was not observed. Radiotherapy has been used in cases of refractory disease [14], and shown to be effective for local control of KD [11, 15]. The present case provides evidence that recur-rent KD can be treated successfully with radia-tion therapy after surgical removal. This sug-gests that radiation therapy may be an effective noninvasive therapeutic alternative for recur-rent KD that provided local control and prevent recurrence (68 months at the time this paper was written) and without side-effects at the dose applied (36 Gy).
Disclosure of conflict of interest
None.
Address correspondence to: Dr. Shu-Jun Song, Department of Pathology and Experimental Medi- cine, 306 Hospital of PLA, Beijing 100101, P.R. China. Tel: +86-10-66356729-2344; Fax: +86-10-66356306; E-mail: [email protected]
Figure 2. Photographs of CT scan. A. CT scan shows one of the lesions (1.7 x 1.1 cm, arrowed) at submaxillary re-gion, before radiotherapy. B. CT scan shows the same lesion (1.0 x 0.5 cm, arrowed), after radiotherapy.

Kimura’s disease with radiotherapy
4522 Int J Clin Exp Pathol 2014;7(7):4519-4522
References
[1] Kim HT and Szeto C. Eosinophilic hyperplastic lymphogranuloma, comparison with Muku-licz’s disease. J Chin Med 1937; 23: 699-700.
[2] Kimura T, Yoshimura S and Ishikawa E. On the unusual granulation combined with hyperplas-tic changes of lymphatic tissue. Trans Soc Pathol Jpn 1948; 37: 179-180.
[3] Kuo TT, Shih LY and Chan HL. Kimura’s dis-ease: involvement of regional lymph nodes and distinction from angiolymphoid hyperpla-sia with eosinophilia. Am J Surg Pathol 1988; 12: 843-854.
[4] Chen H, Thompson LD, Aguilera NS and Ab-bondanzo SL. Kimura disease: a clinicopatho-logic study of 21 cases. Am J Surg Pathol 2004; 28: 505-513.
[5] Rajpoot DK, Pahl M and Clark J. Nephrotic syn-drome associated with Kimura disease. Pedi-atr Nephrol 2000; 14: 486-488.
[6] Abuel-Haija M and Hurford MT. Kimura dis-ease. Arch Pathol Lab Med 2007; 131: 650-1.
[7] Kar IB and Sethi AK. Kimura’s Disease: Report of a Case & Review of Literature. J Maxillofac Oral Surg 2013; 12: 109-112.
[8] Buder K, Ruppert S, Trautmann A, Bröcker EB, Goebeler M and Kerstan A. Angiolymphoid hy-perplasia with eosinophilia and Kimura’s dis-ease - a clinical and histopathological compar-ison. J Dtsch Dermatol Ges 2014; 12: 224-228.
[9] Meningaud JP, Pitak-Arnnop P, Fouret P and Bertrand JC. Kimura’s disease of the parotid region: report of 2 cases and review of the lit-erature. J Oral Maxillofac Surg 2007; 65: 134-140.
[10] Alcántara González J, Boixeda P, Truchuelo Díez MT, Pérez García B and Jaén Olasolo P. Angiolymphoid hyperplasia with eosinophilia treated with vascular laser. Lasers Med Sci 2011; 26: 285-290.
[11] Hareyama M, Oouchi A, Nagakura H, Asakura K, Saito A, Satoh M, Tamakawa M, Akiba H, Sakata K, Yoshida S, Koito K, Imai K, Kataura A and Morita K. Radiotherapy for Kimura’s dis-ease: the optimum dosage. Int J Radiat Oncol Biol Phys 1998; 40: 647-651.
[12] Monzen Y, Kiya K and Nishisaka T. Kimura’s Disease of the Orbit Successfully Treated with Radiotherapy Alone: A Case Report. Case Rep Ophthalmol 2014; 5: 87-91.
[13] Nonaka M, Sakitani E and Yoshihara T. Anti-IgE therapy to Kimura’s disease: A pilot study. Au-ris Nasus Larynx 2014; 41: 384-388.
[14] Castro C and Winkelmann RK. Angiolymphoid hyperplasia with eosinophilia in the skin. Can-cer 1974; 34: 1696-1705.
[15] Chang AR, Kim K, Kim HJ, Kim IH, Park CI and Jun YK. Outcomes of Kimura’s disease after radiotherapy or non-radiotherapeutic treat-ment modalities. Int J Radiat Oncol Biol Phys 2006; 65: 1233-1239.