Embed Size (px)
Citation preview
international journal of athletic therapy & training january 2013 21
© 2013 Human Kinetics - IJATT 18(1), pp. 21-24
Recurrence of Jones Fracture After Intramedullary Screw Fixation
CASE REVIEW
David Brown, LAT, ATC • West Virginia University; Kyle Sanders, LAT, ATC • University of Indianapolis; Drew Farrar, LAT, ATC, CFO • Surgi-Care Inc., Bangor, ME; Joshua Newton; Adam J. Thompson, PhD, LAT, ATC; and Andrew T. Doyle, MA, LAT, ATC, CSCS • Indiana Wesleyan University
a nonunion rate of approximately 50%,1,3 which created concern about the potential for refracture upon return to play between 4 to 8 weeks postinjury.1,4,7 One possible complication of ISF is a screw break, which is believed to be less likely if the selected screw size ensures a snug fit within the surgically created bone canal.4,9
The “Jones Fracture” is one of the most common sport-related foot fractures. The fifth metatarsal is involved in 40–75% of all metatarsal fractures, which typically occur in one of five specific locations.7 By definition, a Jones fracture occurs in the boundary area
that separates the fifth metatarsal metaphy-sis from its diaphysis, approximately 1.5 cm distal to the styloid process.7 A fracture
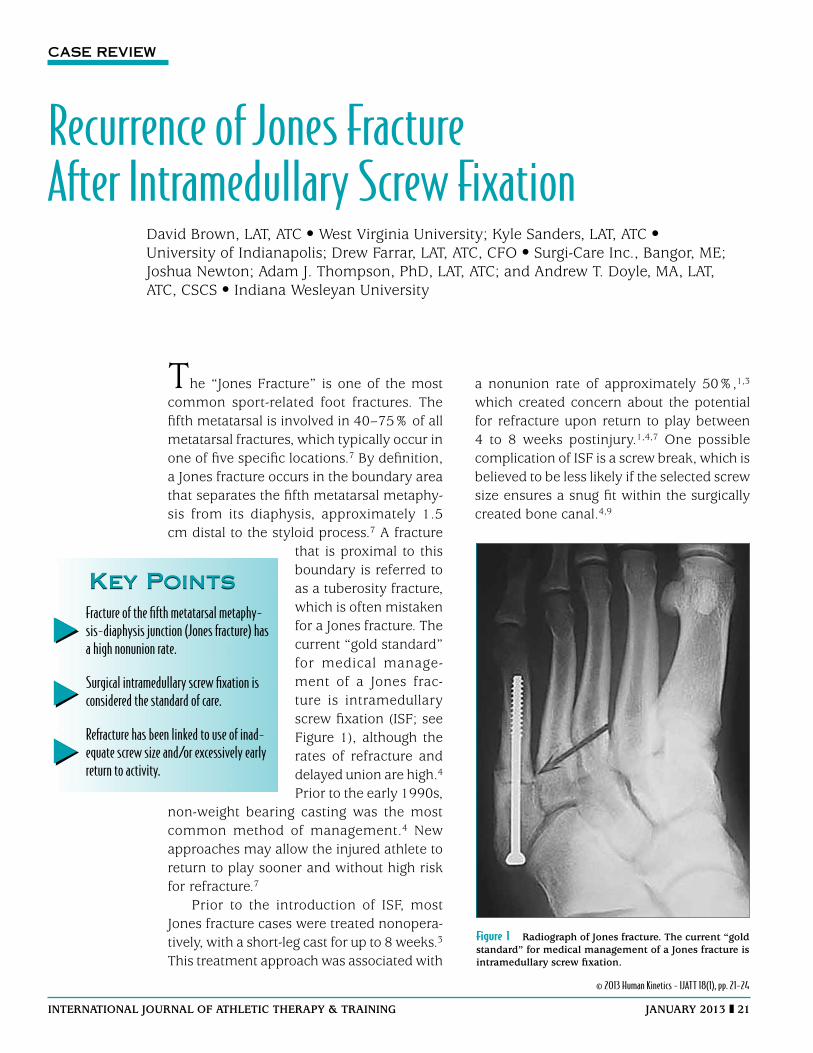
that is proximal to this boundary is referred to as a tuberosity fracture, which is often mistaken for a Jones fracture. The current “gold standard” for medical manage-ment of a Jones frac-ture is intramedullary screw fixation (ISF; see Figure 1), although the rates of refracture and delayed union are high.4
Prior to the early 1990s, non-weight bearing casting was the most common method of management.4 New approaches may allow the injured athlete to return to play sooner and without high risk for refracture.7
Prior to the introduction of ISF, most Jones fracture cases were treated nonopera-tively, with a short-leg cast for up to 8 weeks.3 This treatment approach was associated with
Fracture of the fifth metatarsal metaphy-sis-diaphysis junction (Jones fracture) has a high nonunion rate.
Surgical intramedullary screw fixation is considered the standard of care.
Refracture has been linked to use of inad-equate screw size and/or excessively early return to activity.
Key PointsKey Points
Figure 1 radiograph of jones fracture. the current “gold standard” for medical management of a jones fracture is intramedullary screw fixation.

22 january 2013 international journal of athletic therapy & training
Case ReportA male college basketball player sustained a Jones frac-ture near the end of the season of his freshman year. He was dribbling along the left baseline, and in the process of making a pass to a teammate in the deep baseline corner on the opposite side of the court, his right foot landed on top of the left foot of an opposing player. As his foot was forced into dorsiflexion, he heard a pop and felt pain. There was not any immediate swelling and he was capable of fully bearing his body weight on the injured foot. As his pain increased, cryotherapy was administered and he was instructed to use crutches for ambulation. A radiograph obtained immediately after the game demonstrated a Jones fracture. The injured was managed with a walking boot and crutches for the first two weeks postinjury, while a decision was being made about whether or not to perform surgery. Fol-lowing surgical intervention, the athlete was casted for two weeks and then transitioned to a walking boot and partial weight bearing on crutches for the next 4 weeks. After removal of the walking boot, 2 more weeks of partial weight bearing on crutches was imposed, before allowing return to full weight bearing. The athlete was then slowly reintroduced to sport-specific movement patterns and drills.
Two days before the athlete received full clearance to return to play, he fractured the fifth metatarsal in his left foot. The mechanism of injury involved stepping on a stray basketball, which forced his foot into extreme inversion. The athlete reported having experienced the same sensation as that associated with the first fracture and stated that he knew his foot had fractured immediately after the injury incident had occurred. He related that the injury was not as painful as the first incident and that he could walk relatively well with his body weight shifted to the inner side of his foot. A radiograph revealed a Jones fracture, and surgery was performed at 5 days postinjury. After surgery, the ath-lete was placed in a cast for 2 weeks, a walking boot for 4 weeks, and then partial weight bearing without the walking boot for 2 weeks before return to full weight bearing activities.
The athlete stated that his right foot felt normal when the second fracture occurred in the early summer and when he was cleared to return for his sophomore basketball season in the fall. At the beginning of the season, he reported feeling “not as explosive” from lack of participation in summer workouts. His coach allowed him to withdraw from some practice drills
because his feet bothered him. The athlete related that he noticed changes in his physical abilities and his mindset due to the bilateral foot injuries. Although he experienced aching discomfort from time to time throughout the season, which was greatest in the right foot, he became progressively more confident in his foot function.
The athlete’s third injury occurred during a mid-season game. After stepping forward with his right foot and pushing off his trailing left foot to make a pass, he reported the same symptoms in his right foot that he had previously experienced. Radiographs demon-strated that the athlete had sustained a fracture that extended the lateral side of the fifth metatarsal to the screw that had been placed through the first Jones fracture he had sustained.
Rehabilitation
Rehabilitation for the first injury primarily emphasized pool workouts during the partial weight bearing phase of fracture management, which involved walking and sprinting in the shallow end, swimming laps, jumping, defensive slides, AquaJogger® (Excel Sports Science, Inc., Springfield, OR) flotation exercise, and kickboard swimming. After full weight bearing was permitted, ankle strengthening exercises were performed against elastic band resistance and postural balancing exer-cises were performed on a BAPS® wobble board (Spec-trum Therapy Products, Inc., Jasper, MI). Rehabilitation for the second injury was similar to that for the first, except more of the exercises were in the pool at the athlete’s home.
Management of the third injury included use of the EXOGEN® Ultrasound Bone Healing System (Smith & Nephew, Inc., Andover, MA) for 20-minute treatments that were administered two times per day. Low-level bone stimulation has been reported to facilitate fracture healing.13-15 Pool workouts were performed three to four times per week. During the latter portion of the rehabilitation process, the athlete performed weight bearing squats and calf raises without additional resistance.
Discussion
Varus Foot Alignment
Raikin et al.1 reported that 90% of patients with a Jones fracture (16/20) had hind foot varus. Orthotics were
international journal of athletic therapy & training january 2013 23
deemed beneficial, because no refractures occurred in any of the cases. The authors suggested that failure to use a lateral wedge orthotic increases risk of refrac-ture.1 Measurement of “calcaneal pitch” and “Meary’s angles” according to the procedures used by Raikin et el.1 revealed that the patient had mild varus alignment and a high medial longitudinal arch.
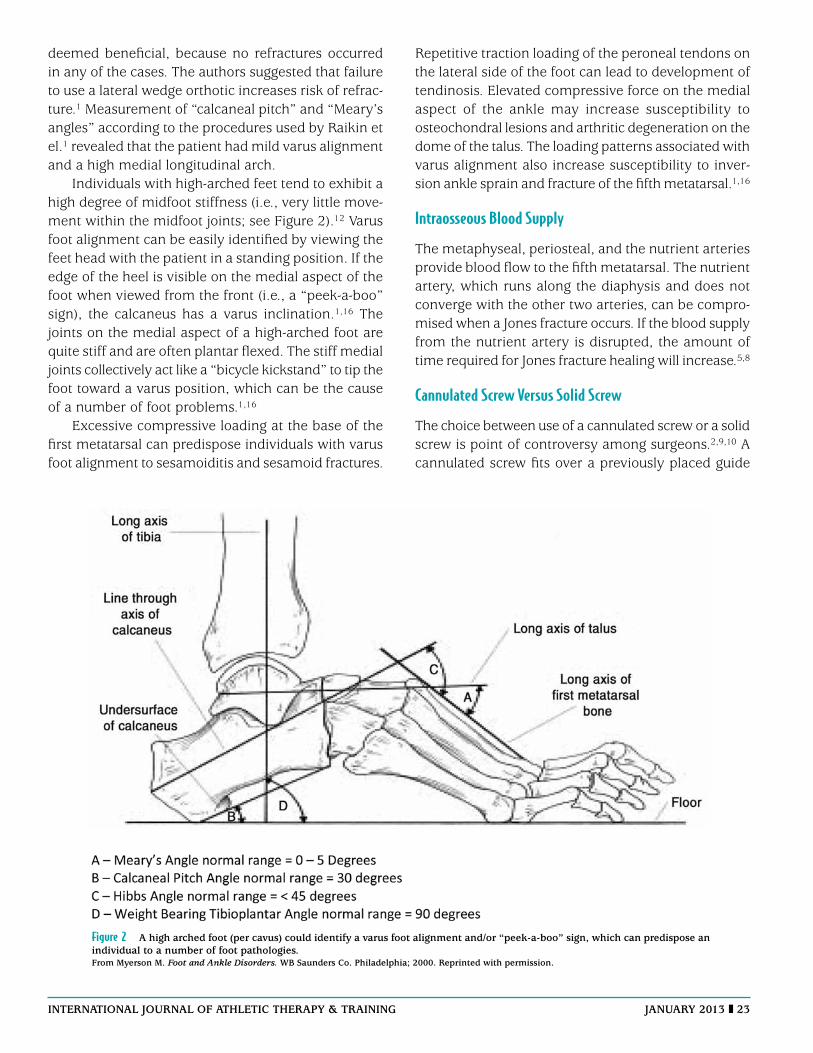
Individuals with high-arched feet tend to exhibit a high degree of midfoot stiffness (i.e., very little move-ment within the midfoot joints; see Figure 2).12 Varus foot alignment can be easily identified by viewing the feet head with the patient in a standing position. If the edge of the heel is visible on the medial aspect of the foot when viewed from the front (i.e., a “peek-a-boo” sign), the calcaneus has a varus inclination.1,16 The joints on the medial aspect of a high-arched foot are quite stiff and are often plantar flexed. The stiff medial joints collectively act like a “bicycle kickstand” to tip the foot toward a varus position, which can be the cause of a number of foot problems.1,16
Excessive compressive loading at the base of the first metatarsal can predispose individuals with varus foot alignment to sesamoiditis and sesamoid fractures.
Repetitive traction loading of the peroneal tendons on the lateral side of the foot can lead to development of tendinosis. Elevated compressive force on the medial aspect of the ankle may increase susceptibility to osteochondral lesions and arthritic degeneration on the dome of the talus. The loading patterns associated with varus alignment also increase susceptibility to inver-sion ankle sprain and fracture of the fifth metatarsal.1,16
Intraosseous Blood Supply
The metaphyseal, periosteal, and the nutrient arteries provide blood flow to the fifth metatarsal. The nutrient artery, which runs along the diaphysis and does not converge with the other two arteries, can be compro-mised when a Jones fracture occurs. If the blood supply from the nutrient artery is disrupted, the amount of time required for Jones fracture healing will increase.5,8
Cannulated Screw Versus Solid Screw
The choice between use of a cannulated screw or a solid screw is point of controversy among surgeons.2,9,10 A cannulated screw fits over a previously placed guide
Figure 2 a high arched foot (per cavus) could identify a varus foot alignment and/or “peek-a-boo” sign, which can predispose an individual to a number of foot pathologies.from Myerson M. Foot and Ankle Disorders. WB Saunders co. philadelphia; 2000. reprinted with permission.

24 january 2013 international journal of athletic therapy & training
pin, which has been shown to provide higher resistance to stress than a solid screw.10
Tension Band Wiring
The displaced ends of the fifth metatarsal fracture need be approximated as closely as possible by the surgical procedure. Tension band wiring involves drilling two holes into the fractured bone segments and spanning the fracture site with wire that is passed through the drilled holes in a figure-eight configuration. The wire ends are pulled together and tied with a knot on the outer surface of the skin to avoid irritation.6
SummaryIntramedullary screw fixation is widely accepted as the gold standard for management of a Jones fracture. Although other management options exist, ISF is the one most frequently utilized for athletes.
Further research is needed to identify the best approach to allow return to play without high risk for reinjury. Use of a bone stimulator may enhance the rate of bone healing.
Acknowledgments
We appreciate assistance provided by the physicians and staff of Central Indiana Orthopedics, PC for the preparation of this report. We also appreciate the patient’s willingness to provide information about his injury and his permission for its presentation.
References 1. Raikin S, Slenker N, Ratigan B. The Association of a varus hindfoot
and fracture of the fifth metatarsal metaphyseal-diaphyseal junction: the Jones fracture. Am J Sports Med. 2008;36:1367-1372.
2. Porter A, Duncan M, Meyer S. Fifth metatarsal Jones fracture fixation with a 4.5-mm cannulated stainless steel screw in the competitive and recreational athlete: a clinical and radiographic evaluation. Am J Sports Med. 2005;33:726-733.
3. Mologne T, Lundeen J, Clapper M, O’Brien T. Early screw fixation versus casting in the treatment of acute Jones fracture. Am J Sports Med. 2005;33:970-975.
4. Larson C, Almekinders L, Taft T, Garrett W. Intramedullary screw fixa-tion of Jones fractures: analysis of failure. Am J Sports Med. 2002;30:55-60.
5. Slomski A. IOM endorses vitamin D, calcium only for bone health, dispels deficiency claims. J AMA. 2011;305:453-456.
6. Sarimo J, Rantanen J, Orava S, Alanen J. Tension-band wiring for fractures of the fifth metatarsal located in the junction of the proximal metaphysis and diaphysis. Am J Sports Med. 2006;34:476-480.
7. Zwitser EW, Breederveld RS. Fractures of the fifth metatarsal; diagnosis and treatment. Int J Care Inj. 2010;41:555-562.
8. Smith JW, Arnoczky SP, Hersh A. The intraosseous blood supply of the fifth metatarsal: implications for promixal fracture healing. Foot Ankle. 1992;13:143-152.
9. Reese K, Litsky A, Kaeding C, Pedroza A, Shah N. Cannulated screw fixation of Jones fractures: a clinical and biomechanical study. Am J Sports Med. 2004;32:1736-1742.
10. Freshi SA, Vardaxis V, Dodson N. Analysis of compression forces between varying sizes of cannulated screws versus rail external fixa-tion for treatment of Jones type fifth metatarsal fracture. J Foot Ankle Surg. 2008;47:295-298.
11. Furia JP, Juliano PJ, Wade .M, Schaden W, Mittermayr R. Shock wave therapy compared with intramedullary screw fixation for nonunion of proximal fifth metatarsal metaphyseal-diaphyseal fractures. J Bone Joint Surg. 2010;92-A:846-854.
12. Myerson M. Foot and Ankle Disorders. WB Saunders Company: Phila-delphia; 2000.
13. Rosenburg G, Sferra J. Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg. 2000;8:332-338.
14. Wolff J. The classic: on the theory of fracture healing, Clin Orthop Rel Res. 2010 Apr;468(4):1052-1055.
15. Wolff J. The Law of Bone Remodeling. Berlin Heidelberg New York: Springer; 1986 (translation of the German 1892 edition).
16. Beals TC, Manoli A, II. The “peek-a-boo” heel sign in the evaluation of hindfoot varus. Foot. 1996;6:205-206.
David Brown is an athletic training graduate assistant in a master’s degree program at West Virginia University in Morgantown.
Kyle Sanders is a doctor of physical therapy student at the University of Indianapolis.
Drew Farrar is a clinical specialist for Surgi-Care, Inc. in Bangor, Maine.
Joshua Newton is pursuing graduate study in athletic training at Indiana Wesleyan University in Marion, IN.
Andrew T. Doyle is an assistant athletic trainer at Indiana Wesleyan University in Marion, IN.
Adam J. Thompson is the ATEP Director and Professor within the Division of Health and Human Performance at Indiana Wesleyan University in Marion, IN.
Trent Nessler, PT, DPT, MPT, Champion Sports Medicine/Physiotherapy Associates, is the report editor for this article.





























