Embed Size (px)
Citation preview

5/8/2017
1
Case Study: Intercollegiate Football Running Back with
Traumatic Knee Dislocation and Multiple Ligament Injury
Ron Courson, ATC, PT, NRAEMT, CSCS
Senior Associate Athletic Director – Sports Medicine
University of Georgia Athletic Association
Athens, GA
Objectives
• Review mechanism of injury and
on-field clinical findings with knee dislocation
• Discuss emergency care
considerations
• Review role of diagnostic testing
with knee dislocation
• Review surgical considerations with multiple-ligament injury
• Discuss coordination of pre- and
post-op rehabilitation and use of
novel techniques within rehabilitation
Traumatic Knee Dislocations
• Traumatic knee dislocations
leading to multiple ligament injury are relatively uncommon
but not rare injuries
• These injuries demand prompt
and appropriate attention
• Knee dislocations represent one of the few true orthopedic
emergencies due to potential
limb-threatening nature
• Post-operative management must be carefully coordinated
with early ROM to restore
functional motion without compromising knee stability
Mechanism of Injury
Initial Exam
• NV check (serial exams)
• Stabilize extremity
• Thorough exam
• Appropriate supporting studies
Work up• Xrays
• MRI
• CT scan

5/8/2017
2
Selective Arteriography (CTA)
Serial Physical Exam (6, 24, 48hrs)
Equal pulses
• ABI <0.9
• Expanding hematoma
• Hx dysvascular foot
• 90% positive predictive value
• 100% negative predictive value
– Stannard 2004
Surgical Plan
• Multiple surgeons
• Multiple injuries
• Multiple scenarios
• Multiple options
Plan
• Scope, I & D
• Open Lateral repair +/-reconstrxn
• Scope repair PCL, MMT’s
Case Study• Post-Operative Diagnosis:
– PCL tear
– Posterior lateral corner tear
– LCL tear
– Biceps femoris tear
– Medial mensicus tear both anterior and
posterior horns
• Procedure:
– Arthroscopically assisted PCL repair
– Medial meniscus repairs anterior and
posterior with debridement
– Open LCL, posterolateral corner and biceps femoris repairs with peronealnerve neurolysis and allograft figure-of-
eight posterolateral corner reconstruction
Lateral Approach 3 Working Windows

5/8/2017
3
Bony Preparation Fibular-Based PLC Recon
Arthroscopic
Portion
• Proximal PCL Repair
• Ant and Post horn MMR
Immediate Postop
• “Controlled Arthrofibrosis”
• Hinged knee brace locked in
full extension for 1st 2 wks
Rehab Program Considerations• Problem-solving approach
– physiologic healing constraints
– pain
– swelling
– ROM restrictions
– muscle atrophy
– decreased
balance/proprioception
– DVT/PE prophylaxis
– deconditioning/weight loss
Rehab Program Considerations
• Is rehabilitation program:
– evidence based ?
– communicated with all parties
?
– challenging/fun ?
• Does rehabilitation:
– avoid redundancy ?
– vary rehab activities ?
– utilize all available resources ?
• Is progression based upon:
– physiologic healing
constraints ?
– achieving rehab goals ?
– MD direction ?
5/8/2017
4
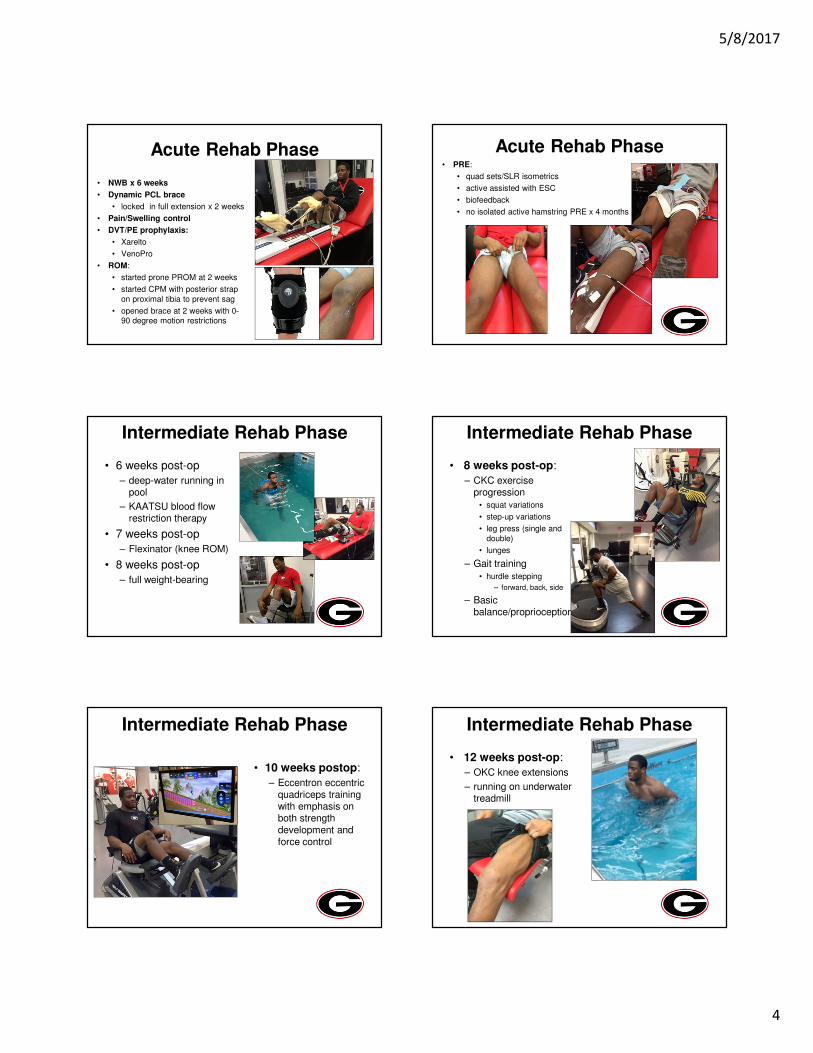
Acute Rehab Phase
• NWB x 6 weeks
• Dynamic PCL brace
• locked in full extension x 2 weeks
• Pain/Swelling control
• DVT/PE prophylaxis:
• Xarelto
• VenoPro
• ROM:
• started prone PROM at 2 weeks
• started CPM with posterior strap
on proximal tibia to prevent sag
• opened brace at 2 weeks with 0-90 degree motion restrictions
Acute Rehab Phase• PRE:
• quad sets/SLR isometrics
• active assisted with ESC
• biofeedback
• no isolated active hamstring PRE x 4 months
Intermediate Rehab Phase
• 6 weeks post-op
– deep-water running in pool
– KAATSU blood flow restriction therapy
• 7 weeks post-op
– Flexinator (knee ROM)
• 8 weeks post-op
– full weight-bearing
Intermediate Rehab Phase
• 8 weeks post-op:
– CKC exercise progression
• squat variations
• step-up variations
• leg press (single and
double)
• lunges
– Gait training
• hurdle stepping
– forward, back, side
– Basic balance/proprioception
Intermediate Rehab Phase
• 10 weeks postop:
– Eccentron eccentric quadriceps training with emphasis on both strength development and force control
Intermediate Rehab Phase
• 12 weeks post-op:
– OKC knee extensions
– running on underwater treadmill

5/8/2017
5
Intermediate Rehab Phase
14 weeks post-op:
• began walking stadium steps
• gradual progression in time and number
• body weight initially with progression over time to 20 lb. weight vest
Advanced Rehab Phase15 weeks post-op: advanced
balance/proprioception activities
Advanced Rehab Phase
� 16 weeks post-op:
� straight ahead running on land
� 18 weeks post-op:
� began jumping
� 20 weeks post-op:
� began change of direction drills
� L drill
� 5-10-5 drill
� Hoop drill
� LEFT test (Davies)
� Reaction drills
Functional Progression• Form running drills:
– Dynamic flexibility
– High knees
– Kick backs
– Skipping
– A, B, C skips
– Backpeddle
– Lateral slide
– Carrioca
– Ladder drills
• flat
• Raised
– Sled push/pull
Functional Progression
• Progression to non-contact football drills:
– QB/RB ball exchange
– pitches
– passes out of backfield
– simulated plays
Return to ActivityTae Kwon Do: 22 weeks post-op
� Performed under strict supervision 1 on 1
� Emphasis on kicking to promote terminal extension, quadriceps development, and confidence in planting on foot
� Ground based fighting to develop core and assist with knee flexion

5/8/2017
6
Return to ActivityTae Kwon Do:
– Performed under strict supervision 1 on 1
– Emphasis on kicking to promote terminal extension, quadriceps development, and confidence in planting on foot
– Ground based fighting to develop core and assist with knee flexion
Return to ActivityTae Kwon Do:
– Performed under strict supervision 1 on 1
– Emphasis on kicking to promote terminal extension, quadriceps development, and confidence in planting on foot
– Ground based fighting to develop core and assist with knee flexion
Return to ActivityTae Kwon Do:
– Performed under strict supervision 1 on 1
– Emphasis on kicking to promote terminal extension, quadriceps development, and confidence in planting on foot
– Ground based fighting to develop core and assist with knee flexion
Functional Progression
Sprint training:
– 24 weeks post-op
– Curved treadmill
– Keiser resistance runner
– Track practice under supervision of sprint coach
Functional Progression
• 26 weeks post-op:
– progressed to full S&C activities without restrictions
• 30 weeks post-op:
– summer football work-outs without restrictions
• 40 weeks post-op:
– pre-season FB camp without restrictions (29 practices)
Functional Progression• 40 weeks post-op: pre-season FB camp without
restrictions (29 practices)
• 42 weeks post-op: 1st scrimmage wearing brace limited snaps
• 43 weeks post-op: 2nd scrimmage lighter brace full snaps

5/8/2017
7
Return to Activity
• 45 weeks post-op:
– 1st game returning from injury vs. UNC
• 32 rushing attempts
• 222 yards
• 2 TDs
Return to Activity
• 2016 Season Statistics
– 224 rushes
– 1130 yards
– 8 TDs
– 5.0 avg. yds/rush
– long rush 55 yds.
– 5 receptions for 86 yds. and 1 TD
Follow-Up





























