Embed Size (px)
Citation preview

Case summary – ICase summary – I
51 year old male
CC: Chest tightness and blood tinged sputum for 12 months
No fever, cough, dyspnea or weight changes
Ex-Smoker
PH: AR and sinusitis history, but no history of chronic asthma
X-ray Pleural effusion, Left 9 months ago
Pleural fluid: eosinophilia (21%), and exudate findings with high ADA level (65 U/L)
Lab: ELISA for PW/CS : positive, peripheral eosinophilia: 800/mm3
Imp: Tuberculous pleurisy and pulmonary paragonimiasis
Management: Ant-tbc medications and praziquantal for 3days
Follow up 1 month of anti-TB medicationFollow up 1 month of anti-TB medication
Still not resolved problemsStill not resolved problems
1. Wheezing developed
2. Persistent left pleural effusion
3. Peripheral eosinophilia: 3300/mm³ ( from 808)
4. Persistent blood tinged sputum, but normal BFS
5. Normal nerve conduction velocity
Imp) Churg-Strauss syndrome
Start oral prednisolone 30 mg/d, but not-well-controlled

After 6 month of anti-TB medication After 6 month of anti-TB medication
Pleural effusion: improved
Normalized blood eosinophil count-stopped steroid
Two months before the admission, recurred eosi
nophilia with increased pleural effusion developed
Case summary – II, problems on Case summary – II, problems on admissionadmission
Recurred blood eosinophilia & pleural effusion
No fever, crackle sound on chest
Peripheral eosinophilia: 1660/mm3, serum total IgE: 500 IU/ml
PFT: moderate obstruction pattern without bronchodilating response
Chest X-ray: left pleural effusion, Chest C-T: mass like lesion
The key findings of this patient..The key findings of this patient..
1. Persistent peripheral eosinophilia
2. Pleural effusion with eosinophilic infiltration
3. Airway obstruction findings including wheezy episode, reversible with steroid treatment history of allergic rhinitis, sinusitis and asthma
4. Mass like lesion

Diagnosis suggestedDiagnosis suggested
1. Pulmonary paragonimiasis : Based on recurrent blood tinged sp
utum, pleural effusion with mass like lesion, persistent eosinophi
lia , but no history of crayfish or crab history, high ADA level in
pleural fluid, failure to praziquantel treatment
2. Churg-Strauss syndrome : Commonly found asthma patients wit
h eosinophilia
3. Malignancy : Mass like lesion with pleural effusion in 51-yr old
male patient
4. TB granuloma : effusion, mass like lesion, high ADA level

Eosinophilia related diseasesEosinophilia related diseases
1. 1. Allergic diseasesAllergic diseases: severity related: severity related -asthma, AR, atopic dermatitis-asthma, AR, atopic dermatitis- ABPA- ABPA- Churg-Strauss syndrome- Churg-Strauss syndrome
2. 2. Parasite infectionsParasite infections: toxocara, An: toxocara, Ansakiasis, Paragonimiasissakiasis, Paragonimiasis
3. 3. DrugDrug induced induced
4. 4. Malignancy : Malignancy : lympho-proliferatilympho-proliferative diseasesve diseases
Paragonimiasis (1) Paragonimiasis (1)
• Caused by the lung fluke, the trematode of the genus Paragonimus
• Clinical symptoms depend on the location and developmental stage of worms.
• Cough (62-100%), Hemoptysis (61-95%), Chest pain (38-94%)
• Pleuritic chest pain, Pneumotherax caused by penetration of larvae through diaphragm/pleura
• Pleural effusions
typically eosinophilic with low glucose, low pH, and high LDH.
(CSS is the only other disease that produces this constellation of pleural fluid findings)
Paragonimiasis (2)Paragonimiasis (2)
• Radiologic findings
pulmonary nodule
pneumotherax
interstitial infiltrates
cavity formations
ring cysts resembling bronchiectasis
• Pleural effusion (48-62%) – most common finding
Parenchymal consolidation
• Treatment
Praziquantel 25mg/kg tid for 2 days is effective in > 90% of cases
Diagnostic criteria of CSSDiagnostic criteria of CSS
American College of Rheumatology (1990)
1. Asthma
2. Eosinophilia>10%, 1500 >
3. Neuropathy, mononeuropathy, or polyneuropathy
4. Pulmonary infiltrates
5. Paranasal sinus abnormality
6. Extravascular eosinophil infiltration on biopsy finding
Diagnosis when four of the six criteria are present
From J Allergy Clin Immunol 2001;108:s1-19
Typical case of CSSTypical case of CSS
1. Long standing asthma and rhino-sinusitis ( > 5 yrs) - uncontrolled cases requiring daily medications
2. Lung parenchymal infiltration
3. Evidence of vasculitis involving nerve, skin, reticulo-endoth
elial systems
4. Remission of eosinophilia after stopping oral corticosteroid i
s very rare
5. Remission of asthma symptoms without any medications is
very rare

Typical case of CSSTypical case of CSS

Lung cancerLung cancer
1. Pleural effusion
eosinophilia (>10%) is unusual in malignant effusion,
but, 20% of eosinophilic effusions malignant
20% of noneosinophilic effusions malignant
2. Peripheral eosinophilia
Eosinophilia occurs in patients who have lung cancer,
more frequently associated with Hodgkin’s disease
3. No systemic symptoms suggesting malignancy, long standing sy
mptoms, normal BFS and sputum result, PET finding– tissue bio
psy was done…
Chest 1996;110:1271-4
TB granulomaTB granuloma
1. No evidence of TB infection in sputum, pleural effusion and BFS
2. No eosinophils in pleural effusion or blood
3. Recurred pleural effusion after 6 months anti-TB medication
s
4. High ADA in pleural effusion
5. Positive PPD skin test
6. Positive Qunatiferon-TB GOLD test
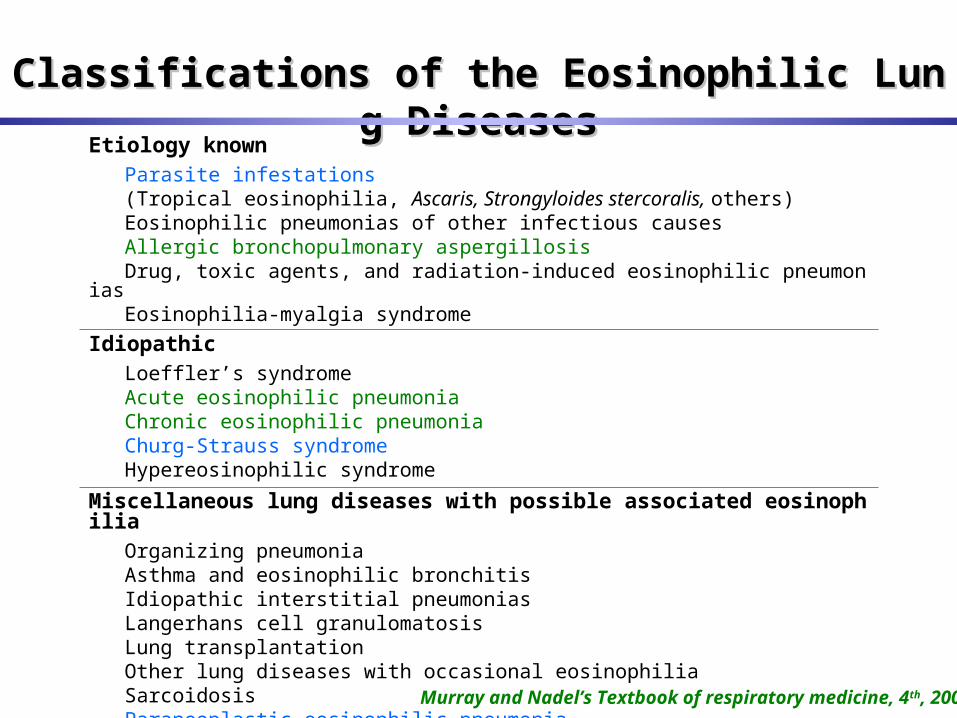
Etiology known Parasite infestations (Tropical eosinophilia, Ascaris, Strongyloides stercoralis, others) Eosinophilic pneumonias of other infectious causes Allergic bronchopulmonary aspergillosis Drug, toxic agents, and radiation-induced eosinophilic pneumonias Eosinophilia-myalgia syndrome
Idiopathic Loeffler’s syndrome Acute eosinophilic pneumonia Chronic eosinophilic pneumonia Churg-Strauss syndrome Hypereosinophilic syndrome
Miscellaneous lung diseases with possible associated eosinophilia Organizing pneumonia Asthma and eosinophilic bronchitis Idiopathic interstitial pneumonias Langerhans cell granulomatosis Lung transplantation Other lung diseases with occasional eosinophilia Sarcoidosis Paraneoplastic eosinophilic pneumonia
Murray and Nadel’s Textbook of respiratory medicine, 4 th, 2005
Classifications of the Eosinophilic Lung DiseasesClassifications of the Eosinophilic Lung Diseases
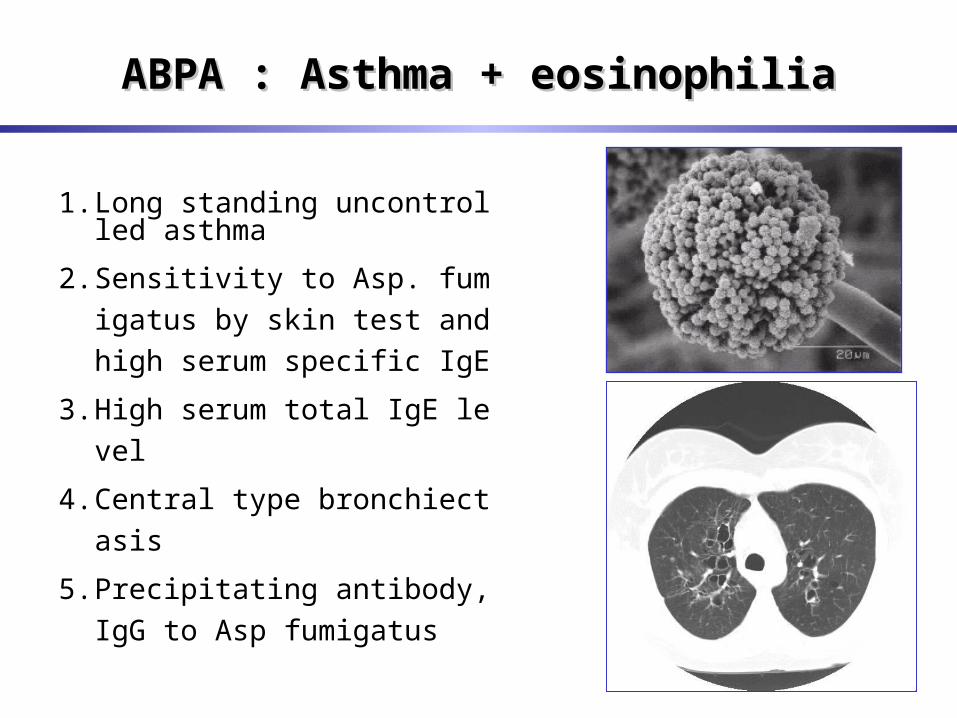
ABPA : Asthma + eosinophiliaABPA : Asthma + eosinophilia
1. Long standing uncontrolled asthma
2. Sensitivity to Asp. fumigatus b
y skin test and high serum spec
ific IgE
3. High serum total IgE level
4. Central type bronchiectasis
5. Precipitating antibody, IgG to
Asp fumigatus

Acute and chronic eosinophilic pneumoniaAcute and chronic eosinophilic pneumonia
Drug induced, idiopathic, drug history, typical radiologic findings, Drug induced, idiopathic, drug history, typical radiologic findings, evidence tissue eosinophilia in BAL and sputumevidence tissue eosinophilia in BAL and sputum
ImpressionImpression
1. Pulmonary paragonimiasis
Persistent blood tinged sputum, pleural effusion, persistent
eosinophilia , granuloma formation
2. Malignancy, less likely