Embed Size (px)
Citation preview
1
Casey Hansen, PT, DPT, TPS
• The listener will understand the pain neuromatrixand how it affects our perception of pain
• The listener will understand neuroplasticity’s role in the pain neuromatrix
• The listener will understand current treatments to help desensitize a sensitive nervous system
2
} Doctor of Physical Therapy from the University of North Dakota
} Therapeutic Pain Specialist Certification from the International Spine and Pain Institute
} Currently working in the outpatient setting with a focus on neck and back pain as well as chronic pain including complex regional pain syndrome, chronic fatigue, and fibromyalgia.
◦ Focus on pain neuroscience education◦ Using different techniques to calm down a
sensitive nervous system◦ Use this in conjunction with standard
therapy practices to begin to resume activities of daily living
3
} To understand where we are headed we need to know where we started
} René Descartes theorized that the body was more similar to a machine, and that pain was a disturbance that passed down along nerve fibers until the disturbance reached the brain. (Moayedi and Davis 2013)
} Specificity Theory-First to recognize specific sensory receptors and fibers, eventually lead to the idea of nociception.
} Intensity Theory of Pain-Looked at summation of input as a potential for pain
} Pattern Theory of Pain-Pain was determined by specific and particular patterns of neural firing. (Moayedi and Davis 2013)
4
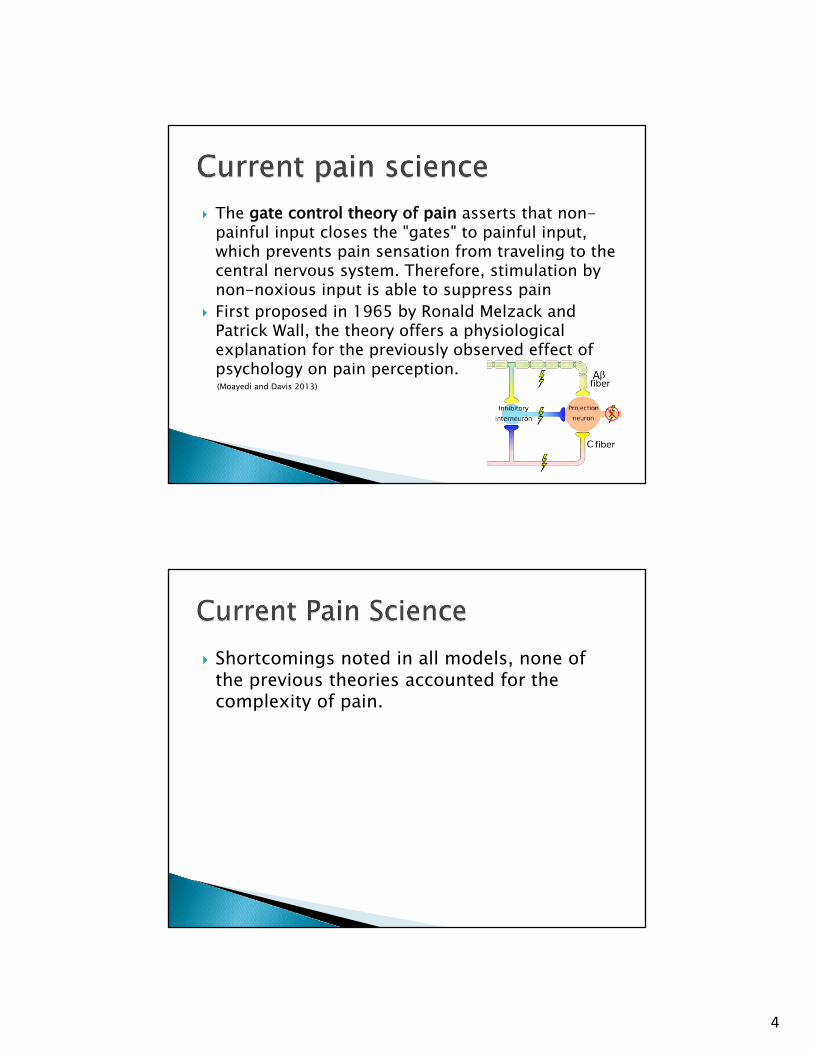
} The gate control theory of pain asserts that non-painful input closes the "gates" to painful input, which prevents pain sensation from traveling to the central nervous system. Therefore, stimulation by non-noxious input is able to suppress pain
} First proposed in 1965 by Ronald Melzack and Patrick Wall, the theory offers a physiological explanation for the previously observed effect of psychology on pain perception. (Moayedi and Davis 2013)
} Shortcomings noted in all models, none of the previous theories accounted for the complexity of pain.
5
} Neuromatrix Theory-Pain is an output of the central nervous system that occurs when the organism perceives a threat
} Pain is very complex and involves all the systems of the body from central nervous system to the endocrine system.
} Tissue injury does not necessarily mean pain} 25-50% of general population (Kjaer et al 2005) :
� –Hypointense disc signal � –Annular tears � –High intensity zones � –Disc protrusions � –Endplate changes � –Zygapophyseal joint degeneration � -Asymmetry � –Foraminal stenosis.
6
} After successful rotator cuff repairs and clinically sound examination (Spielmann, Forster et al. 1999) : ◦ •90% abnormal signaling ◦ •16% partial tears ◦ •20% complete tears ◦ •33% sub-acromial effusion ◦ •16% joint effusion ◦ •20% bone marrow edema
} Over age 70: 2 out of 3 have asymptomatic RC tear(Milgrom, Schaffler et al. 1995)
} The increased sensitivity to outside forces◦ Allodynia-Non painful stimulus that causes pain◦ Hyperalgesia-Increased pain experience
with stimulus} Changes in the pain experience◦ Mirrored pain◦ Spreading pain◦ Inflammatory responses◦ Increased activation in different systems in the body
7
} We have 45 miles of nerves in the human body
} Ion channels◦ Located along areas of decreased myelin along the
nerve◦ Many different types of channels that can sense
chemicals surrounding the nerve, mechanical input and electrical voltage◦ The more ion channels the more sensitive the nerve◦ We replace ion channels every 48 hours
8
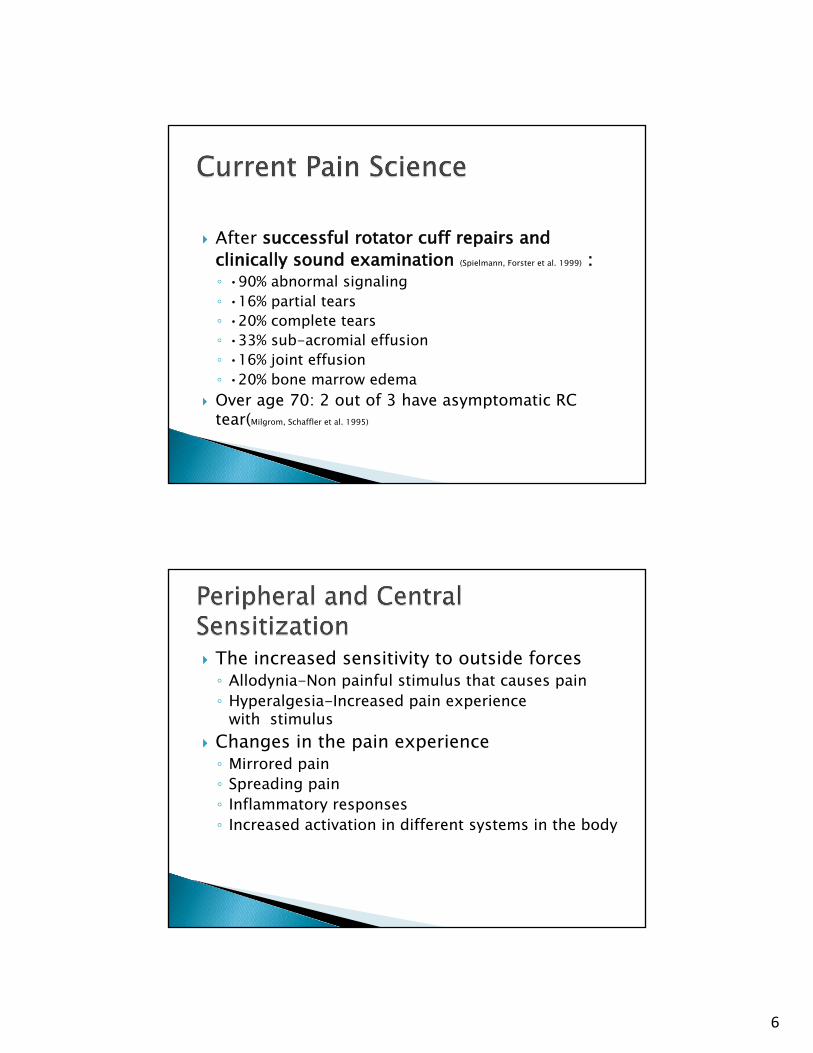
} Dorsal Horn and the interneuron
} Interneuron Inhibition causes input from levels above and below to now send signals to the brain as well and input from the other side of the body
} This bombardment of signals causes mirror pain as well as spreading pain, begins to cause allodynia as sensory input is no longer inhibited as well.
9
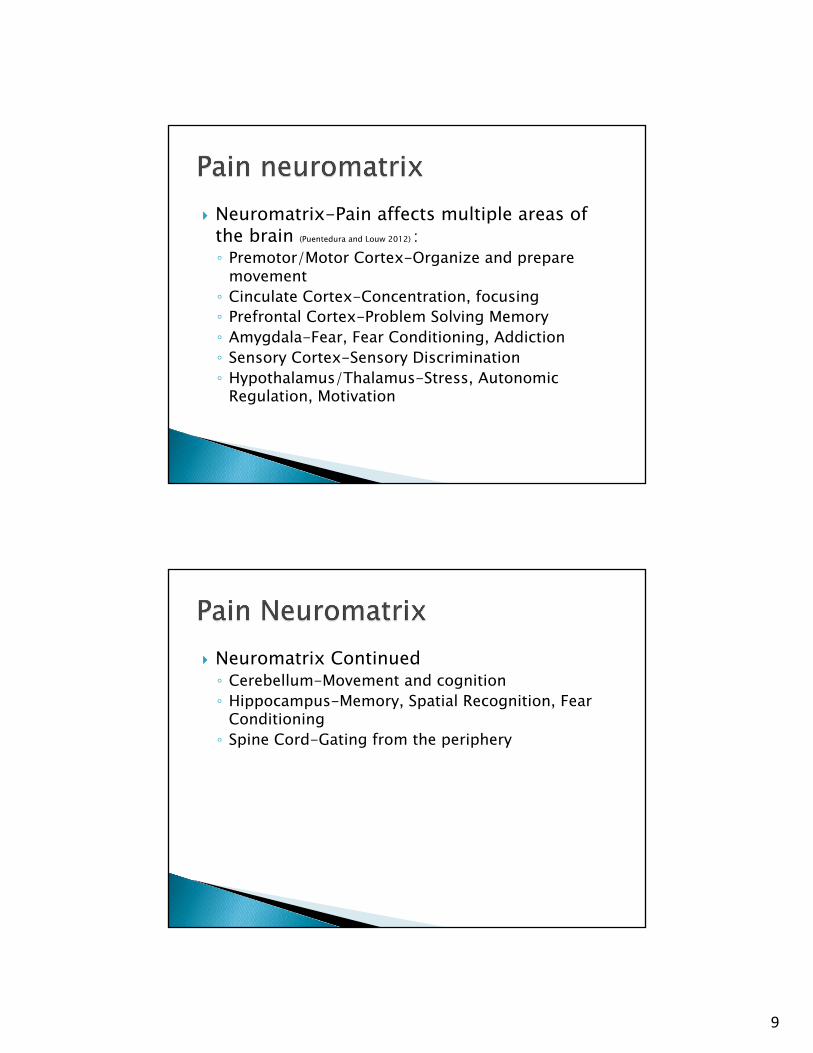
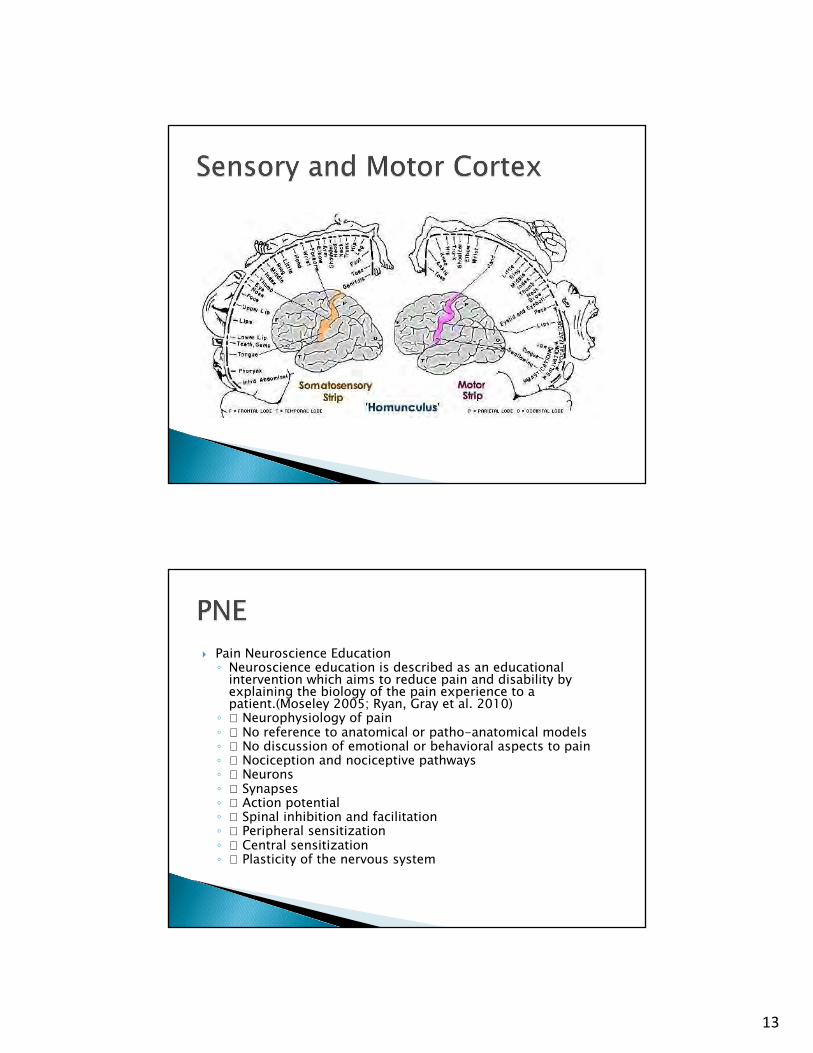
} Neuromatrix-Pain affects multiple areas of the brain (Puentedura and Louw 2012) :◦ Premotor/Motor Cortex-Organize and prepare
movement◦ Cinculate Cortex-Concentration, focusing◦ Prefrontal Cortex-Problem Solving Memory◦ Amygdala-Fear, Fear Conditioning, Addiction◦ Sensory Cortex-Sensory Discrimination◦ Hypothalamus/Thalamus-Stress, Autonomic
Regulation, Motivation
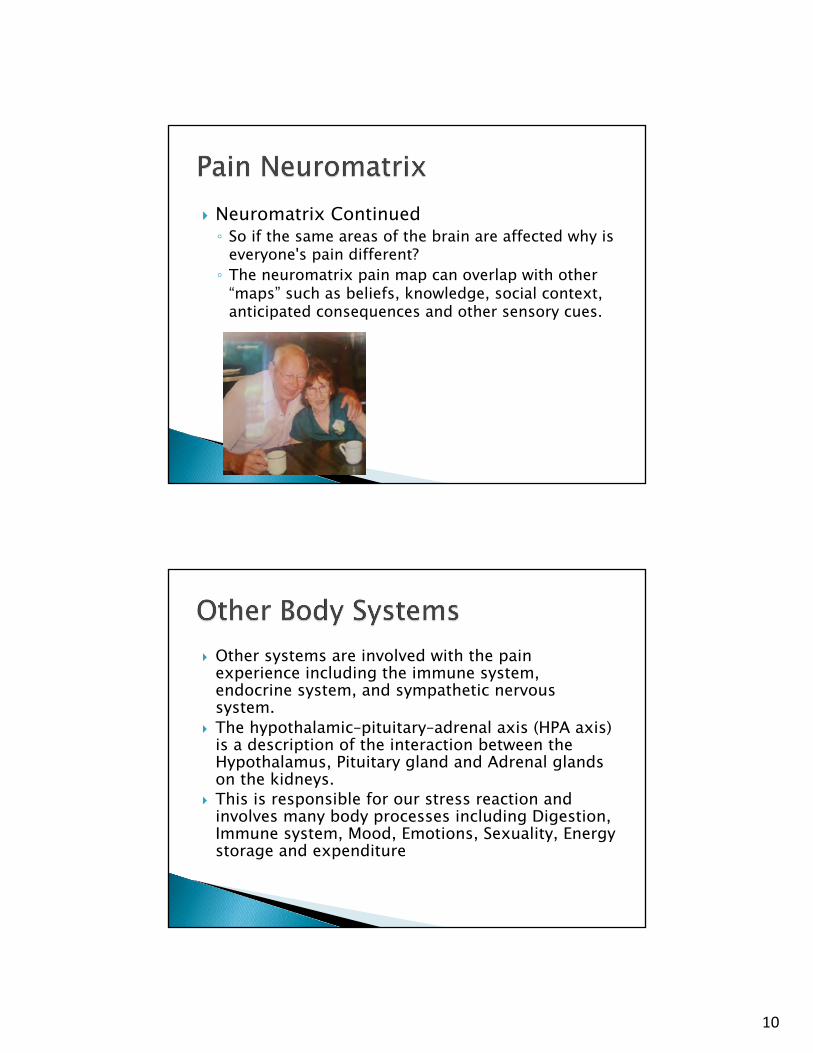
} Neuromatrix Continued◦ Cerebellum-Movement and cognition◦ Hippocampus-Memory, Spatial Recognition, Fear
Conditioning◦ Spine Cord-Gating from the periphery
10
} Neuromatrix Continued◦ So if the same areas of the brain are affected why is
everyone's pain different?◦ The neuromatrix pain map can overlap with other
“maps” such as beliefs, knowledge, social context, anticipated consequences and other sensory cues.
} Other systems are involved with the pain experience including the immune system, endocrine system, and sympathetic nervous system.
} The hypothalamic–pituitary–adrenal axis (HPA axis) is a description of the interaction between the Hypothalamus, Pituitary gland and Adrenal glands on the kidneys.
} This is responsible for our stress reaction and involves many body processes including Digestion, Immune system, Mood, Emotions, Sexuality, Energy storage and expenditure
11
} Increasing substance P release can cause the HPA axis to blunt corticotrophin-releasing hormone causing allodynia, hyperalgesia and dysautonomia(Rodriguez-Pinto, I., N. Agmon-Levin, et al. (2014)
} HPA axis causes the release of Cortisol as well. } During a pain experience we also release cytokines
which can be both pro-inflammatory and anti-inflammatory and in a health system these are well balanced.
} Neuroplasticity is the mechanism by which the brain encodes experience and learns new behaviors.
} This is also the mechanism by which the damaged brain relearns lost behavior
} Research strongly suggest that neurons as well as other brain cells have the ability to alter their structure and function in response to internal and external input
12
} 1)Use it or lose it} 2)Use it and improve it} 3)Specificity} 4)Repetition matters} 5)Intensity matters} 6)Time matters} 7)Salience matters} 8)Age matters} 9)Transference } 10)Interference} (Kleim and Jones, 2008)
} Pain Neuroscience Education} Laterality-left/right discrimination} Motor Imagery} Sensory Discrimination and Graphesthesia} Mirror therapy
13
} Pain Neuroscience Education◦ Neuroscience education is described as an educational
intervention which aims to reduce pain and disability by explaining the biology of the pain experience to a patient.(Moseley 2005; Ryan, Gray et al. 2010)◦ � Neurophysiology of pain ◦ � No reference to anatomical or patho-anatomical models ◦ � No discussion of emotional or behavioral aspects to pain ◦ � Nociception and nociceptive pathways◦ � Neurons ◦ � Synapses ◦ � Action potential ◦ � Spinal inhibition and facilitation ◦ � Peripheral sensitization ◦ � Central sensitization ◦ � Plasticity of the nervous system
14
} 1st off does it work?◦ In 2011 a systematic review of TNE was
conducted for musculoskeletal pain. (Louw, Diener et al. 2011)� This review includes 8 studies comprising 6
high-quality RCTs, 1 pseudo-RCT, and 1 comparative study involving 401 subjects.
� Narrative synthesis of results, based on effect size, established compelling evidence that TNE may be effective in reducing pain ratings, increasing function, addressing catastrophization, and improving movement in chronic MSK pain.
} Laterality◦ We use flash cards, phone apps, magazines to help patients
get more accurate and faster with the ability to discern left and right. ◦ If the area that is affected is to painful or emotional we can
use adjacent areas first.} Motor Imagery◦ We know now that the same neurons that fire during an
activity also fire when watching someone else do the act, this is the reason yawns seem to be contagious. ◦ Start with static positions and progress to dynamic
positions◦ Create flash card based on patient goals and progress as
tolerated
15
} Sensory discrimination◦ Moseley has shown that discrimination is more
effective that integration due to the brain being active vs passive (Mosely, Zalucki et al. 2007)◦ Treatment options include two point discrimination,
sharp/dull, feather, cotton wool. � Verbally teaching themselves keeps the brain more
active� Just like laterality we can start with a neighbor if
needed.
} Graphesthesia-begin with easy to discriminate shapes and progress to more similar shapes
} Stereognosis-Start with less options and progress to similar objects, focus on time, place into beans/rice, combining objects, etc.
16
} Usually towards the end, if the brain does not understand and becomes more confused pain will increase.
} Must prepare the patient as it can be very emotional
} Try to limit distortions, make sure the box is sturdy, sit evenly, remove jewelry and cover tattoos.
} Progress tasks with noninvolved extremity
} PNE is one part of the pain puzzle, traditional therapy still works and we know that there are many things that we can do to help calm down the nervous system
} PNE, Goal Setting, Aerobic Exercise and Sleep Hygiene are requirements for our patients.
} Other treatments include: Meditation, Diet, Journaling, General Stabilization, Manual Therapy, Social Interaction, Graded Motor Imagery, Welcoming/Safe/Healing Environment, Humor, Mindfulness, Diaphragmatic breathing, Appropriate Bracing, Modalities, Home Exercise Program, Coping Skills, Relaxation, Skillful Delivery of Medication
17
} This is why a multidisciplinary approach is so important, there are so many options to help our patients and when everyone is on the same page we can create a significant decrease in pain by calming down the sensitive nervous systems and begin to normal the pain experience.
} Thank you all for your time!

18
Apkarian AV, Hasmi JA, Baliki MN. (2010) "Pain and the brain: Specificity and plasticity of the brain in clinical chronic pain". Pain. 152 (2011) S43-S64.
Bray H, Moseley GL. (2011). “Disrupted working body schema of the trunk in people with back pain”. Br J Sports Med. 45:168-173.
Busch AJ, Barber KA, etal (2007). “Exercise for treating fibromyalgia syndrome”. The Cochrane database of systemic reviews. (4):CD003786
Butler, DS. (2000). The sensitive nervous system. Adelaide, Noigroup Publications.Bulter DS, Moseley GL. (2003). Explain Pain. Adelaide, Noigroup Publications.Catley MJ, O’Connell NE, Moseley GL. (2013). “How good is the neurophysiology of pain
questionnaire? A rasch analysis of psychometric properties”. Journal of Pain. 14(8):818-827.Coppieteres MW, Bulter DS (2008). “Do ‘sliders’ slide and do ‘tensioners’ tension? An analysis of
neurodynamic techniques and considerations regarding their applications”. Manual Therapy. 13(3):213-221.
Crombez G, Vlaeyen JWS, etal (1999). “Fear of pain is more disabling than pain itself. Evidence on the role of pain related fear in chronic back pain disability. Pain. 80:329-340.
Doidge, N. (2007). The brain that changes itself. New York. Penguin books.Dommisse GF. (1994) “The bood supply of the spinal cord and the consequences of failure”.
Grieves Modern Manual Therapy. J Boyling and N Palastanga. Edinburgh, Churchill Livingstone.
Gifford L. (2014). Aches and pains. Cornwall, Wordpress.Goldenberg DL. (2009). “Multidisciplinary care to treat fibromyalgia. The journal of clinical
psychiatry. 70 (5):e13International Association for the study of pain (1979). Pain. 6:250.International Narcotics Control Board Report 2008. United Nations Pubns. 2009. p. 20Kamper SJ, Apeldoorn AT, etal (2014). “Multidisciplinary biopsychosocial rehabilitation for
chronic low back pain”. The Cochrane database of systemic reviews. 9:CD000963Kiecolt-Glaser JK, etal. (2002). “Psychoimmunology: Pshycological influences on immune
function and health. Journal of consulting and clinical psychology. 70(3):537-547.Kliem JA, Jones TA. (2008). "Principles of Experience-Dependent Neural Plasticity:
Implications for Rehabilitation After Brain Damage. Journal of speech, language, and hearing research. 51: S225-S239.
Larun K, Brurberg KG, etal (2015). “Exercise therapy for chronic fatigue syndrome”. The Cochrane database of systemic reviews. 2: CD003200
Lewis JS, Kersten, etal (2007). “Body perception disturbance: A contribution to pain in complex regional pain syndrome”. Pain. 133(1-3):111-119.
Louw A. (2015). “Treating the brain in chronic pain”. In CFdiP, JC, Dommerholt J, eds. Manual therapy for musculoskeletal pain syndromes. Vol 1. London. Chruchill Livingston.
Louw A, Butler DS, etal (2012). “Preoperative education for lumbar radiculopathy: A survey of US spine surgeons”. International Journal of Spine Surgery. 6:130-139

19
Louw A, Butler DS, etal (2013). “Development of a preoperative neuroscience educational program for patients with lumbar radiculopathy”. American journal of physical medicine & rehabilitation/Association of academic physiatrists. 92(5):446-452.
Louw A, Diener I, etal. (2013). “Preoperative education addressing postoperative pain in total joint arthroplasty: Review of content and educational delivery methods”. Physiotherapy theory and practice. 29(3):175-194.
Louw A, Diener I etal (2014). “Preoperative pain neuroscience education for lumbar radiculopathy: A multicenter randomized controlled trial with 1-year follow up”. Spine. 39(18):1149-1457.
Louw A, Louw Q, Crous L. (2009). “Preoperative education for lumbar surgery for radiculopathy”. SA Journal of physiotherapy. 65(2):3-8.
Louw A, Puentedura E. (2013). Therapeutic Neuroscience Education. Teaching patients about pain. A guide for clinicians. Minneapolis, MN. OPTP
Magni G, Marchetti M, etal. (1993). “Chronic musculoskeletal pain and depressive symptoms in the national health and nutrition examination. 1. Epidemiologic follow up-study”. Pain. 53:163
Meeus M, Nijs J, etal. (2007). “Chronic musculoskeletal pain in patients with the chronic fatigue syndrome”. Europe Journal of Pain. 11(4):377-386.
Melzack, R. (2001). “Pain and the neuromatrix in the brain”. Journal of dental education. 65:1378-1382.
Moayedi M, Davis KD. (2013). “Theories of pain: from specificity to gate control”. Journal of neurophysiology. 109(1):5-12.
Moseley GL (2003). “Unraveling the barriers to reconceptualisation of the problem in chronic pain: the actual and perceived ability of patients and health professionals to understand the neurophysiology. J. Pain. 4(4):184-189.
Moseley GL (2003). “A pain neuromatrix approach to patients with chronic pain”. Manual therapy. 8(3):130-140.
Moseley GL. (2004). “Why do people with complex regional pain syndrome take longer to recognize their affected hand?” Neurology. 62(12):2182-2186.
Moseley GL. (2007). “Using visual illusion to reduce at-level neuropathic pain in paraplegia”. Pain. 130:294-298.
Moseley GL. (2008). “I can’t find it! Distorted body image and tactile dysfunction in patients with chronic back pain”. Pain. 140:239-243.
Moseley GL, Flor H. (2012). “Targeting cortical representations in the treatment of chronic pain: A review. Neurorehabilitation and neural repair. XX(X):1-7.
Moseley GL, Herbert RD, etal. (2014). “Intense pain soon after wrist fracture strongly predicts who will develop complex regional pain syndrome: Prospective cohort study”. The journal of pain: Official journal of the American pain society. 15(1):16-23.
Moseley GL, Zalucki NM, Wiech K. (2007)”Tactile Discrimination, but not tactile stimulation alone, reduces chronic limb pain. Pain. 137(3):600-8.

20
NIDA. (2015, November 24). Prescription and Over-the-Counter Medications. Retrieved from https://www.drugabuse.gov/publications/drugfacts/prescription-over-counter-medications on 2017, May 24
NIDA. (2017, May 12). Pain. Retrieved from https://www.drugabuse.gov/related-topics/pain on 2017, May 24
NIDA. (2017, April 24). Trends & Statistics. Retrieved from https://www.drugabuse.gov/related-topics/trends-statistics on 2017, May 24
Nijs J, Aelbrechts S, etal (2011). “Tired of being inactive: a system literature review of physical activity, physiological exercise capacity and muscle strength in patients with chronic fatigue syndrome”. Disability and rehabilitation. 33(17-18):1493-1500
Oliveira A, Gevirtz R, Hubbard D. (2006). “A psycho-educational video used in the emergency department provided effective treatment for whiplash injuries”. Spine. 31(15):1652-1657.
Puentedura EJ, Louw A. (2012). “A neuroscience approach to managing athletes with low back pain”. Physical therapy in sport: Official journal of the association of charted physiotherapists in sports medicine. 13(3):123-133.
Rodriguez-Pinto, I., N. Agmon-Levin, et al. (2014). "Fibromyalgia and cytokines." Immunology letters 161(2): 200-203.
Shacklock M (1995). “Neurodynamics”. Physiotherapy. 1(1):9-16.Shacklock M. (2005). Clinical Neurodynamics. Edinburgh, Elsevier.
Sterling MG, Jull, etal. (2003). “Sensory hypersensitivity occurs soon after whiplash injury and is associated with poor recovery”. Pain. 104(3):509-517.
Toyone T, Tanaka T, etal (2005). “Patients expectations and satisfaction in lumbar spine surgery”. Spine. 30(23):2689-2694.
Vowles KE, McEntee ML, Julnes PS, Frohe T, Ney JP, van der Goes DN. Rates of opioid misuse, abuse, and addiction in chronic pain: a systematic review and data synthesis. Pain. 2015;156(4):569-576.
Wainner RS, Fritz JM, etal (2003). “Reliability and diagnostic accuracy of the clinical examination and patient self report measures for cervical radiculopathy”. Spine. 28(1):52-62.





























