Embed Size (px)
Citation preview

Anatomy Shape
a biconvex lens and capable of changing shape colorless transparent avascular
size 4mm thick and 9mm in diameter
position behind the iris and the pupil In front of the vitreous suspended by suspensary ligament


Lens

Anatomy structure
capsule:an elastic transparent basement membrane admit water and electrolytes pass through the lens fibers are enveloped in it
epithelium : this single cell layer located anteriorly and
extending to the equator fibers:continuously produced by epthelium
the nucleus:old fibers ,harder at the centre the cortex: new fibers,softer, at the periphery
With age,the lens gradually becomes larger, harder and less elastic

Physiology composition
water -64% The water content of the lens decreases with age.
protein -35% the highest protein content in any body tissue soluble protein insoluble protein:With age, the percent of it increases
1%- A trace of minerals are present (Potassium, Ascorbic acid and Glutathione) The lens has complex metabolic process. It`s nourishment comes from aqueous humor.When there are changes of aqueous or capsule or metabolism,the transparent lens
becomes opaque.

Physiology
Function one of important refractive medias focus light rays upon the retina filter a part of ultraviolet rays ,it is beneficial
to the retina

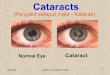
CataractCataract –transparent lens becomes
opaque

Cataract Epidemiology
Cataract is a common ocular disease and one of the main causes of blindness.It is estimated that 30 to 45 million people in the world are blind,with cataract accounting for as much as 45% of this blindness.
The prevalence of cataract varies widely with striking regional differences.It is more common in areas where people eyes expose to sunlight greatly.
The prevalence rises with age and is higher in females.
WHO defines blindness as best corrected visual acuity less than 20/400(0.05) or visual field restricted to 10°or less.

Classification Senile cataract-age related cataract Complicated cataract-due to ocular inflammation or degeneration affects lens metabolism Congenital cataract-a result of developmental
disturbance of lens during the process of development of fetus
Traumatic cataract-eye trauma cause lens opacities Metabolic cataract-metabolic disturbance Toxic cataract-many drugs and chemicals have been
shown to induce cataracts After-cataract-after cataract surgery,remained cortex
and epithelial cells exfoliated to form opacity

CAUSESCataracts have several causes and may be
age-related, present at birth, or formed as a result of trauma or exposure to a toxic substance, Cataracts are classified by the cause
Senile cataracts develop in elderly people Congenital cataracts occur in neonates
from inborn errors of metabolism or from maternal rubella infection during the first trimester
Traumatic cataracts develop after a foreign body injures the lens with sufficient force to allow aqueous or vitreous humor to enter the lens capsule

Complicated cataracts occur secondary to uveitis, glaucoma, retinitis pigmentosa, or retinal detachment
Toxic cataracts result from drug or chemical toxicity with prednisone, ergot alkaloids, naphthalene, and phenothiazines.
Genetic Considerations; Epidemiological studies indicate that cataracts have strong genetic components. Several loci have been identified for an autosomal dominant form of cataracts. Congenital cataracts occur with galactosemia and these can appear within just a few days of birth. The specific genetic contributions of the more common age-associated cataracts are still unclear. Ethnicity and race have no known effect on the risk of cataracts

Senile cataract Senile cataract is by far the most common type. It
often occurred over the age of 40. With aging,it`s incidence increases.we call it “age related cataract”
Etiology It is a lens disorder formed on the basis of
decreasing of lens metabolic function with aging of whole body
and plus many other factors. It has relation to Heredity Ultraviolet rays-plateau (expanse of level land high
above sea-level) long periods of strong sunlight Systematic disorders-diabetes Nourishment condition

Senile cataract
Clinical findings Symptom:progressively blurred vision is the
only symptom Types:according to the place of opacity
appear first Cortical cataract Nuclear cataract Posterior subcapsular cataract

Senile cataract-cortical cataract There are 4 stages in its developing
Incipient stage (beginning;in an early stage) The lens is only slightly opaque These spoke-like opacities
begin in the lens periphery Pupillary area isn`t affected No blurred vision takes place

Senile cataract-cortical cataract
Intumescent stage (immature stage) Lens opacity develop gradually,the fibers absorb
water,the lens edema,the cortex become swollen. The anterior chamber is shallow .
It is easy to induce
onset of glaucoma. Visual acuity
decrease.

Senile cataract –cortical cataract Mature stage
The lens is completely opaque, The color is greywhite. The depth of the anterior chamber restores to normal. Because the swollen decreases. The vision is obviously decreased to FC or HM

Senile cataract-cortical cataract Hypermature stage
The degenerated cortex has been decomposed to form milklike substance.
The lens nucleus
fall down. The capsule wrinkled
and shrunk.
Due to water
escaping from lens.

Senile cataract-nuclear cataract
The nucleus becomes harder(sclerotic) and increasingly pigmented with age.
At beginning, nucleus appears yellowish,its color becomes more and more dark with development
It generally produce more blurring of distance vision than near vision

Senile cataract-posterior subcapsular cataract
Golden yellow or white particles,mixed with small vacuoles in them occur at shallow layer of subcapsular cortex in posterior pole lens.
The opaque area situates in the area of visual axis,so blurred vision takes place in early stage

Congenital cataract○ It is a result of developmental disturbance of
lens during the process of development of fetus
○ EtiologyGenetic factor-autosomal dominant inheritanceDamage of fetal lens caused by systemic disorders
of mother or fetus-viral infections,nourishment and metabolic disturbance of mother

Congenital cataract
Commonly are as follows:polar cataract,nuclear cataract,lamellar
cataract,complete cataract,coronary cataract
axiality cataract

Complicated cataractIt is a lens opacity induced by ocular
inflammation or degeneration disorder
Uveitis,glaucoma,too low IOP,retinal pigmentary degeneration

Traumatic cataract
It may be caused by mechanical injury,physical forces(radiation,electrical current,heat and cold),and osmotic influences
Penetrating cataract

Metabolic cataract Diabetic cataract Hypocalcemic cataract

Toxic cataract and After cataract
Many drugs and chemicals have been shown to induce cataract-
After cataract surgery,remained cortex and epithelial cells exfoliated onto lens posterior capsule proliferate to form opacity

Management of cataract Medical management
No medical treatment has been proven conclusively to delay,prevent,or reverse the development of cataract
Indication for surgery The most common indication for cataract
surgery is the patient`s desire for improved visual function.
When visual acuity impairment interferes with the patient`s normal activities,the surgery of cataract well be performed.

Lens surgery Microsurgical techniques is employed for all
cataract surgery. There are 3 principal types of lens extraction
Intracapsular cataract extraction(ICCE) It involves complete removal of the lens within its
capsule.
through a larger (12mm length) superior limbal incision
The larger incision may increase the risk of wound-related problems.

Lens surgery Extracapsular cataract extraction(ECCE)
It involves removal of the lens nucleus and cortex through an opening in the anterior capsule, leaving the posterior capsule in place.
A superior limbal incision is made,it is shorter than ICCE
The anterior portion of the capsule is ruptured and removed
The nucleus is extracted The cortex is either irrigated or aspirated from
the eye leaving the posterior capsule behind.

ECCE and IOL

IOL

Lens surgery Phacoemulsification(Phaco)
It is a relatively new technique.In recent years, it has become popular.
It is a method of extracting the nucleus through a small incision(3mm).
The nucleus is extracted by ultrasonic vibration. This technique results in a lower incidence of
wound-related complications, faster healing, and more rapid visual rehabilitation than procedures requiring larger incisions.

Phaco

ICCE vs ECCE vs Phaco
TYPE ADVANTAGES DISADVANTAGES ICCE Removes all lens Larger incision
material, no posterior Cystoid macular edema capsular opacity Vitreous complications Endophthalmodonesis Increased incidence of RD
ECCE Smaller incision Posterior capsule opacity No vitreous complications Less endophthalmodonesis Less CME,RD Allows implants pcIOL
Phaco Smallest incision Demanding technique Less induced astigmatism Complications while learning Fastest technique

Visual rehabilitation Removal of the lens causes a marked
reduction of the refractive power of the eye,we call it aphakia
Aphakia may be corrected by three methods include spectacles(glasses),contact lens or intraocular lens(IOL) to increase its refractive power
IOL is the best among them and now is widely used in the world

NURSING MANAGEMENTPREOPERATIVE
· Because surgery is performed on an outpatients basis, instruct patient to make arrangements for transportation home, care that evening, and a follow-up visit to the surgeon the next day.
· Withhold any anticoagulants the patient is receiving, if medically appropriate. Aspirin should be withheld for 5 to 7 days, nonsteroidal anti-inflammatory drugs (NSAIDs) for 3 to 5 days, and warfarin (Coumadin) until the prothrombin time of 1.5 is almost reached.

INTRAOPERATIVE
Administer dilating drops every 10 minutes for four doses at least 1 hour before surgery. Antibiotic, corticosteroid, and NSAID drops may be administered prophylactically to prevent postoperative infection and inflammation.

POSOPERATIVE
· Instruct patient to wear a protective eye patch for 24 hours after surgery to prevent accidental rubbing or poking of the eye. After 24 hours, eyeglasses (sunglasses in bright light) should be worn during the day and a metal shield worn at night for 1 to 4 weeks.
· Provide postoperative discharge teaching concerning eye medications, cleansing and protection, activity level and restrictions, diet, pain control, positioning, office appointments, expected postoperative course, and symptoms to report immediately to the surgeon.

· Instruct patient to restrict bending and lifting heavy objects.
· Caution patient that vision may blur for several days to weeks.
· Inform patient that vision gradually improves as the eye heals; IOL implants improve vision faster than glasses or contact lenses.
· Reinforce that vision correction is usually needed for remaining visual acuity deficit.

Diagnoses that may occur in Nursing Care Plans For Cataract
Anxiety Deficient knowledge (diagnosis and
treatment) Disturbed sensory perception: Visual Risk for infection Risk for injury