Embed Size (px)
Citation preview

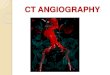
Catheter-directed gadolinium-enhanced MR angiography
Reed A. Omary, MD, MSa,*, Jordin Green, BSb, J. Paul Finn, MDb,Debiao Li, PhDb
aDepartment of Radiology, Northwestern University Medical School, 676 North Saint Clair, Suite 800, Chicago, IL 60611, USAbDepartment of Radiology, Northwestern University, Suite 700, 448 East Ontario Street, Chicago, IL 60611, USA
Magnetic resonance imaging (MRI) guidance for
endovascular procedures offers several important
advantages over conventional x-ray guidance. These
advantages include (1) lack of ionizing radiation
exposure, which benefits not only the patient, but
the operator and team who perform a lifetime of
procedures; (2) lack of iodinated contrast agents, with
their attendant risks of nephrotoxicity and allergic
reactions; (3) the ability to detect blood vessels and
three-dimensional (3D) anatomy at the same time, an
important feature for performing procedures such as
transjugular intrahepatic portosystemic shunt (TIPS)
placement; and (4) the ability to detect changes in end-
organ (eg, kidney, heart, or brain) function at the time
of an endovascular intervention, a capacity that is not
readily available with x-ray–guided techniques.
MRI-guided procedures are still early in their
development. Most studies have occurred in animals,
with little published about these procedures in humans.
In animal models, published applications of MRI-
guided endovascular interventions include inferior
vena cava filter placement [1,2], percutaneous trans-
luminal angioplasty (PTA) of the aorta [3–5] and renal
artery [6,7], stent placement within the iliac artery
[8,9] and aorta [9,10], coronary angiography [11,12],
TIPS [13], and carotid artery aneurysm embolization
[14]. In humans, MRI-guided hemodialysis, Brescia-
Cimino arteriovenous and loop graft fistulagraphy
[15], and iliac artery stent placement [16] also have
been performed.
Whether performed under x-ray or MRI guidance,
these endovascular procedures require multiple con-
trast-agent injections to define baseline vascular
anatomy, to confirm intraluminal position of endo-
vascular devices, and to document changes in vascular
anatomy following an intervention. Direct catheter-
based injections of gadolinium (Gd) chelates under
MRI guidance can be used in the same manner as
injections of iodinated contrast material under x-ray
guidance. The primary rationale for using catheter-
directed rather than conventional intravenous (IV)
injections under MRI is to conserve contrast agent.
Because multiple injections are required during an
MRI-guided endovascular intervention, the Food and
Drug Administration (FDA)-mandated daily dose
limit of Gd, 0.3 mmol/kg, is easily exceeded using
IV injections. Catheter -directed injections use smaller
volumes of dilute contrast agent. These smaller Gd
doses not only should help the operator remain below
the FDA dose limits, but also should reduce back-
ground tissue enhancement. A secondary benefit of
these catheter-based injections is that only the artery
of interest is enhanced. Other adjacent vascular beds
remain suppressed, which facilitates artery visualiza-
tion and disease detection.
This article reviews catheter-directed Gd-enhanced
MR angiography (MRA), with special focus on intra-
arterial (IA) injections. Catheter-directed IA Gd-
enhanced MRA has been used in animals in the aorta
[12,17–19], carotid arteries [12,14,18,20], renal arter-
ies [6,12,19,21], iliac arteries [18,19,21], and coronary
arteries [12,22]. The authors present background
theory; discuss IA injection protocols, MRA se-
quences, and methods to limit contrast agent dose;
0033-8389/02/$ – see front matter D 2002, Elsevier Science (USA). All rights reserved.
PII: S0033 -8389 (02 )00014 -3
R.A. Omary was supported in part by NIH K08
DK60020.
* Corresponding author.
E-mail address: [email protected]
(R.A. Omary).
Radiol Clin N Am 40 (2002) 953–963

and describe how to perform IA injections. Finally, the
authors discuss the accuracy, advantages, and limita-
tions of IA injections.
Theory of local Gd injections
Gd-enhanced MRA is based on the T1 shortening
effect of Gd in blood. T1 shortening increases MR
signal. Gd, however, also shortens blood T2*, which
results in MR signal loss with a gradient-echo
sequence. Consequently, there is an optimal Gd
concentration ([Gd]), where the T1 shortening signal
gain is balanced with the competing T2 signal loss,
and the blood signal is maximal. Fig. 1 compares T1
and T2* shortening effects during selective renal-
artery injections.
If dilute Gd is required, then what is the optimal
concentration? This question has been addressed
using (1) theoretic expressions [18,19], (2) static
[12,17] and dynamic [21] phantoms, and (3) in vivo
[12,18,19,21] experiments. Using complex theoretic
expressions, Frayne et al [18] derive 2% Gd as the
optimal concentration for MR vascular signal for
typical MRA acquisition parameters. Bos et al [19]
find that 3% to 6% is optimal. In initial static
phantom experiments, Omary et al [17] show that
optimal arterial [Gd] range between 1% and 6%,
depending on the selected imaging parameters. In
subsequent static phantom experiments, Serfaty et al
[12] find 6% [Gd] to be optimal. In vivo optimal
arterial Gd concentrations range from 1% to 5%
[18,21].
This spectrum of optimal values reinforces a key
point: satisfactory vascular depiction occurs over a
relatively broad range of arterial [Gd] [12,18,19].
There is little practical difference in vessel enhance-
ment or signal-to-noise ratio (SNR) between Gd sol-
utions ranging in concentrations between 1% and 6%.
Regarding nomenclature, dilute Gd solutions are
generally presented in one of three ways: (1) dilution
ratios (eg, 1:20, which is equivalent to 1 part Gd and
20 parts saline); (2) millimolar concentration (eg, 50
mM); and (3) percentage concentration (eg, 4% Gd).
While all these methods are equivalent, they have
varying degrees of scientific validity and practicality.
The dilution ratio and percentage concentration meth-
ods are clearly the most intuitive; one need not be
familiar with the standard molar concentration of Gd
(500 mM) to recognize how to produce these dilu-
tions. The mM method is scientifically most correct
because full-strength contrast agent within the dis-
pensing bottle is itself a solution of Gd chelate. The
mM method is limited in practice because it requires
a priori knowledge of this concentration and is not
readily intuitive to most radiologists.
Fig. 1. Coronal 2D MRA using selective Gd injection in swine right renal artery. (A) Injected [Gd] = 1.8%, injection rate = 1 mL/
second, arterial [Gd] = 1%, total injected Gd dose = 0.13 mL. (B) Injected [Gd] = 14%, injection rate = 2 mL/second, arterial
[Gd] = 10%, total injected Gd dose = 2.0 mL. The injection in (A) shows optimal signal-to-noise ratio, with T1 shortening effects
predominating over T2* effects. The injection in (B) shows signal loss due to T2* effects. (From Omary RA, Henseler KP, Unal
O, Smith RJ, Ryu RK, Resnick SA, et al. Validation of injection parameters for catheter-directed intraarterial gadolinium-
enhanced MR angiography. Acad Radiol 2002;9:172–85; with permission.)
R.A. Omary et al / Radiol Clin N Am 40 (2002) 953–963954

Intra-arterial injection protocol
Knowledge of the optimal arterial Gd concentra-
tion is only the first step in performing an IA
injection. It is paramount to recognize that the desired
arterial [Gd] differs in most instances from the
injected [Gd]. The difference between injected and
arterial Gd concentrations results from further dilu-
tion of injected Gd by inflowing blood. Arterial [Gd]
is based on three factors: injected [Gd], injection rate,
and arterial blood flow rate. Frayne et al [18] and Bos
et al [19] postulate relationships between these injec-
tion parameters by assuming that all injected Gd is
diluted by inflowing blood. Their injection relation-
ships are similar, except that Frayne et al [18] account
for the influence of injection rate on overall arterial
blood flow rates.
The IA injection protocol proposed by Frayne et al
[18] is:
½Gd�inj ¼ ð1þ Qartery
Qinj
Þ � ½Gd�artery
where [Gd]inj = injected [Gd] (%), Qartery = blood
flow rate in vessel of interest (mL/s), Qinj = injection
rate of Gd agent (mL/s), and [Gd]artery = desired
arterial concentration of Gd (%). By substituting
injection parameters into Equation 1, interventional
radiologists can devise injection protocols for IA
Gd-enhanced MRA.
This injection protocol has been validated in
dynamic flow phantoms and in swine [21]. Accord-
ing to the injection protocol, there is an inverse
relationship between injected [Gd] and injection rate.
To obtain a desired arterial [Gd], either (1) increase
the injection rate and reduce the injected [Gd] or (2)
increase the injected [Gd] and reduce the injection
rate. This trade-off occurs because both techniques
deliver the same local Gd mass flux [18] to the
blood vessel.
MRA sequences
The selection of MRA sequences should be
based on the intended purpose of an IA injection.
If a rapid vascular roadmap is desired and the blood
vessels are located within a defined thin-imaging slab,
then a standard two-dimensional (2D) time-resolved
sequence should be used. With tortuous vessels, it is
better to use a thicker 2D-imaging slab, arbitrarily
called ‘‘projection MRA.’’ The term ‘‘projection’’
refers to 2D imaging over a thick-imaging slab, gen-
erally 5 to 20 cm, similar to 2D x-ray fluoroscopy.
Projection MRA emphasizes a larger imaging slab at
the expense of vessel signal. If greater accuracy and the
ability to perform multiplanar volumetric reconstruc-
tions are desired, then three-dimensional (3D) se-
quences should be used. Potential problems with 3D
imaging are that the temporal resolution will be com-
promised and more contrast agent will be required. In
general, short repetition time (TR)/short echo time
(TE) T1-weighted sequences, similar to conventional
IV-Gd–enhanced MRA, can be used for 2D and 3D
MRA. Electrocardiographic (ECG) gating may be
used for some vascular distributions, such as the heart
(Fig. 2). Typical imaging parameters for each sequence
are shown in Table 1.
According to Equation 1, knowledge of the local
blood flow rate adjacent to the catheter is necessary to
use the injection protocol relationship. This blood
flow rate is empirically estimated based on experience
or estimates from the literature. To be more accurate,
however, a 2D cine-phase contrast sequence [18,21,
23,24] is used to measure the local blood flow rate.
There are several methods to suppress background
for IA-Gd–enhanced MRA. One involves subtraction
of source-imaging data obtained prior to the admin-
Fig. 2. Coronal 3D coronary MRA in canine using selective
left circumflex artery Gd injection. Electrocardiographic-
triggering was used. Injection parameters included injected
[Gd] = 6%, injection rate = 0.3 mL/second, injection vol-
ume = 10 mL, slice thickness = 16 mm (interpolated to
32 mm), and temporal resolution = 0.5 frames/second.
(Equation 1)
R.A. Omary et al / Radiol Clin N Am 40 (2002) 953–963 955

istration of contrast agent [25]. This method is limited
because it requires additional image processing.
Motion between data acquisitions also causes image
artifacts after subtraction. A gradient dephaser has
been used in the slice direction to suppress signals
from the thick, homogeneous background [26,27].
The effectiveness of this scheme, however, depends
on the anatomical structure of the imaging slice.
Recently, magnetization preparation has been used
to suppress background in contrast-enhanced MRA
[20,22,28,29]. This method may be a useful approach
for 2D projection MRA.
Limiting contrast-agent dose
Because MRI-guided endovascular interventions
require at least as many separate injections as x-ray
guided procedures, it is essential to limit contrast-
agent dose during each injection. Limiting injected-
Gd dose not only reduces the likelihood of exceeding
FDA Gd-dose limitations during an intervention, but
it also has the added imaging advantage of minimiz-
ing background tissue enhancement.
There are several techniques available to limit
contrast-agent dose. These can be categorized as
Table 1
Typical imaging parameters used for Gd-enhanced MRA
Technique Parameters
2D cine-phase contrast TR (repetition time)/TE (echo time)/flip = 10.1 ms/4.7 ms/45�;field of view (FOV) = 24 � 11 cm; acquisition matrix = 256 � 128;
reconstruction matrix = 256 � 256; slice thickness = 5 mm;
velocity-encoding value = 300 cm/s; duration = 18 s
Time-resolved 2D TR/TE/flip = 5.8 ms/1.4 ms/ 30�; FOV = 24 � 18 cm;
acquisition matrix = 256 � 160; reconstruction matrix = 256 � 256;
slice thickness = 20 mm; scan duration = 7 s
Single-phase 3D TR/TE/flip = 8.3 ms/ 1.6 ms/ 45�; FOV = 24 � 18 cm;
acquisition matrix = 512 � 192; reconstruction matrix = 512 � 512;
slice thickness = 2.6 mm with 16 partitions (acquired) and 1.3 mm
with 32 partitions (reconstructed); scan duration = 26 s
Fig. 3. Coronal 2D MRA using selective Gd injection in swine right-iliac artery. (A) Injected [Gd] = 10%, injection rate = 1 mL/
second, arterial [Gd] = 4%. (B) Injected [Gd] = 2.5%, injection rate = 1 mL/second, arterial [Gd] = 1%. There is no significant
difference in arterial depiction between images. The selective injection, however, depicted in (A) required a total of 0.70 mL of
undiluted Gd, while the injection depicted in (B) required only 0.18 mL. (From Omary RA, Henseler KP, Unal O, Smith RJ, Ryu
RK, Resnick SA, et al. Validation of injection parameters for catheter-directed intraarterial gadolinium-enhancedMR angiography.
Acad Radiol 2002;9:172–85; with permission.)
R.A. Omary et al / Radiol Clin N Am 40 (2002) 953–963956

injection parameters, imaging techniques, and cath-
eter location.
Injection parameters
These techniques use arterial [Gd] equal to 1%.
Whereas optimal SNR is obtained with arterial [Gd]
ranging from 1% to 6%, aiming for 1% reduces
contrast agent dose six-fold over 6%. This reduction
is a result of the direct relationship between arterial
[Gd] and injected dose (Equation 1). Fig. 3 depicts
selective iliac artery injections in a pig. Images show
how aiming for arterial [Gd] of 1% rather than 4%
reduces injected-Gd dose without appreciably affect-
ing vascular depiction.
Imaging techniques
1. Tailor injections toward imaging goal. Early
experience with IA injections [17] suggests that
injection duration should cover at least a
substantial portion of the image acquisition
period. Because image acquisition time is much
faster for 2D rather than 3D techniques, 2D IA-
MRA uses considerably less contrast agent than
3D IA-MRA. Roadmaps using 2D projection
methods thus save considerable contrast agent
over 3D IA-MRA. Reserve 3D methods for
occasions when high diagnostic accuracy or
multiplanar volumetric reconstructions are re-
quired. Fig. 4 shows how image quality differs
between 2D projection and 3D techniques for
catheter-directed MR aortography.
2. Reduce imaging times. This can be accom-
plished by: (1) shortening the TR, (2) using
partial Fourier acquisitions, or (3) reducing the
number of phase encoding steps.
3. Reduce injection duration. For 3D IA-MRA,
Hwang et al [30] show that injection duration
can be reduced to 50% of the image acquisition
Fig. 4. Catheter-based Gd injections in aorta of same pig. (A) 2D coronal projection MRA using injected [Gd] = 4%, injection
rate = 5 mL/second, injection duration = 1 second, total undiluted Gd dose = 0.2 mL, slice thickness = 50 mm, and temporal
resolution approximately 2 frames/second. (B) 3D coronal MRA (maximum intensity projection) using injected [Gd] = 4%,
injection rate = 5 mL/second, injection duration = 8 seconds, total undiluted Gd dose = 1.6 mL, slice thickness = 48 mm (after
interpolation), and temporal resolution = one image every 6 second. The 3D acquisition has better image quality than the 2D
projection acquisition but uses more contrast agent and requires a longer acquisition time.
R.A. Omary et al / Radiol Clin N Am 40 (2002) 953–963 957

time without significant loss of SNR in the
aorta and iliac arteries. For smaller vessels,
such as the renal arteries, injection duration can
be reduced to 75% of the image acquisition
time without significant loss of SNR. Hwang
et al [30] found no difference in SNR between
elliptical centric and conventional sequential
linear encoding schemes for IA-MRA. Fig. 5
depicts sample 3D IA-Gd–enhanced images
from a dynamic arterial flow phantom using
both encoding schemes at the different in-
jection durations.
Catheter location
Place catheters as selectively as possible. Major
reductions in contrast-agent dose occur when cathe-
ters are positioned within smaller vessels. This effect
on dose reduction can be seen from Equation 1:
smaller vessels have reduced blood flow rates com-
pared to larger vessels. Consequently, performing a
selective renal artery injection uses substantially less
contrast agent than an abdominal aortic injection.
For example, the selective 2D renal MRA shown in
Fig. 1a uses only 0.13 mL of undiluted Gd. In a 25-kg
pig, 115 separate similar injections can be per-
formed without exceeding the FDA Gd-dose limit of
0.3 mmol/kg/day.
How to perform an IA injection
Equation 1 describes the relationship between
three pertinent injection parameters: injection rate,
injected [Gd], and blood flow rate. Although Equa-
tion 1 can be used to establish an injection protocol
for IA-Gd–enhanced MRA, it still leaves many
injection parameter choices available to the operator.
The authors present the following method of
approaching an IA injection:
1. Place catheter selectively into vessel of interest.
2. Measure or estimate blood flow rate (Q) in
mL/second in the catheterized vessel. To meas-
Fig. 5. Coronal 3D MRA using aortic catheter-based injections in a dynamic aortorenal-iliac flow phantom. Two series of images
acquired with aortic blood flow rate of 29 mL/second and an injection rate of 4 mL/second, using elliptical (a–d) and sequential
(e–h) encoding. Both series are shown with decreasing injection coverage: 100% (a,e), 75% (b,f ), 50% (c,g), and 30% (d,h). No
statistical difference ( P > 0.05) in signal-to-noise ratio (SNR) is present between the two encoding schemes. When injection
coverage is dropped to 30%, there is a statistically significant drop in SNR for all vessel segments ( P < 0.05). (From Hwang KP,
Green JD, Li D, Simonetti OP, Resnick SA, Finn JP, et al. Minimizing contrast-agent dose during intraarterial gadolinium-
enhanced MR angiography: in vitro assessment. J Magn Reson Imaging 2002;15:55–61; with permission.)
R.A. Omary et al / Radiol Clin N Am 40 (2002) 953–963958

ure blood flow rates directly, use 2D cine-
phase contrast MRA [18,21,23,24]. Estimates
of blood flow rate can be obtained from the
literature or from operator experience. Esti-
mates are often sufficient, given the wide
variation in acceptable arterial [Gd]. This is not
unlike the case with x-ray digital subtraction
angiography (DSA). Significant vascular pa-
thology, however, might introduce more varia-
tion into estimates and potentially limit the
effectiveness of IA injections.
3. Select an injection rate. Injection rates might
range from 1 to 10 mL/second, given the
availability/preference of automated injectors
versus hand injections. A smaller injection rate
is beneficial because it uses smaller volumes of
dilute contrast agent. Smaller injection rates
might result in suboptimal mixing of contrast
Fig. 6. Pig following surgical induction of bilateral renal artery stenosis. (A) X-ray digital substration angiography shows 70%
right renal artery stenosis and 53% left renal artery stenosis; (B) IV-Gd–enhanced 3D MRA shows 68% right renal artery
stenosis and 65% left renal artery stenosis. (C) IA-Gd–enhanced 3D MRA shows 65% right renal artery stenosis and 75% left
renal artery stenosis. Both MR images are coronal-maximum intensity projections obtained with same 3D-fast spoiled gradient
echo acquisition. (From Omary RA, Henseler KP, Unal O, Maciolek LJ, Finn JP, Li D, et al. Comparison of intraarterial and
intravenous gadolinium-enhanced MR angiography with x-ray digital subtraction angiography for the detection of renal artery
stenosis in pigs. AJR Am J Roentgenol 2002;178:119–27; with permission.)
R.A. Omary et al / Radiol Clin N Am 40 (2002) 953–963 959

agent and blood. Faster injection rates should
improve mixing in large vessels. Use of
injection rate of 1 mL/second, however, will
simplify the math underlying Equation 1. This
injection rate works in most vessels, especially
if they are smaller.
4. Select desired arterial-Gd concentration
([Gd]artery). The authors suggest using
[Gd]artery = 1%, which should minimize
injected contrast dose and still provide ade-
quate images.
5. Determine injected-Gd concentration ([Gd]inj).
Assuming use of [Gd]artery = 1%, [Gd]inj = 1 +
(blood flow rate/injection rate)%. As an
example, for blood flow rate = 12 mL/second
and injection rate = 4 mL/second, substitution
yields [Gd]inj = 4%. Injecting at 1 ml/second,
requires [Gd]inj = 13%. To produce this injected
[Gd], dilute full-strength Gd (500 mM) with
normal saline.
6. Determine purpose of injection. Use 2DMRA to
verify catheter positioning, to confirm intra-
luminal catheter location, or to perform rapid
vascular roadmaps. These images can be pro-
jectional (5–20 cm slab) for tortuous vessels.
Use 3D MRA for its improved diagnostic ac-
curacy at the beginning and end of MRI-guided
endovascular procedures.
7. Determine injection duration. For fast time-
resolved 2D MRA, injection can coincide with
image acquisition and continue for the desired
number of arterial-phase imaging frames. For
3D MRA, injection should begin two seconds
prior to image acquisition, which will facilitate
adequate mixing of injected contrast agent with
inflowing blood. To minimize injected contrast
agent, injection duration can be reduced to the
first 50% of the image acquisition time in
medium or large vessels without loss of SNR.
For instance, injection duration should be
10 seconds for a 3D selective iliac artery
acquisition that lasts 16 seconds (2 second lead
time plus 8 seconds). In smaller vessels, such
as renal or coronary arteries, injection duration
should cover the first 75% of image acquisition
time. A similar 3D injection in a renal artery
might require injection duration of 14 seconds
(2 second lead time plus 12 seconds).
Fig. 7. Scatter plot shows swine renal artery stenosis measurements obtained for IV- and intraarterial (IA)-3D MRA using x-ray
digital substration angiography as reference standard. Stenoses were induced using reverse cable ties. IA MRA has slightly
greater scatter than IV MRA. (From Omary RA, Henseler KP, Unal O, Maciolek LJ, Finn JP, Li D, et al. Comparison of
intraarterial and intravenous gadolinium-enhanced MR angiography with x-ray digital subtraction angiography for the detection
of renal artery stenosis in pigs. AJR Am J Roentgenol 2002;178:119–27; with permission.)
R.A. Omary et al / Radiol Clin N Am 40 (2002) 953–963960

To simplify Equation 1, substitute [Gd]artery = 1%
and injection rate = 1 ml/second [21]. This substi-
tution leads to:
½Gd�inj ¼ ð1þ QÞ � 1%;
where [Gd]inj = injected [Gd] (%) and Q = blood
flow rate in vessel of interest (mL/second).
Using Equation 2, the injected [Gd] in percent
equals one plus the estimated blood flow rate in
mL/second.
Accuracy of IA injections
The accuracy of IA injections are theoretically at
least as effective as, if not better than, conventional
IV-Gd–enhanced MRA because both rely on T1
shortening by contrast agent to produce bright vas-
cular signal. There are limited data available to
confirm this accuracy. In a reverse-cable tie-swine
model of renal artery stenosis; however, Omary et al
[24] compare the accuracy of IV and IA MRA
methods using x-ray DSA as a reference standard.
In this study, the same 3D MRA sequence is used to
compare an IA injection protocol, using Equation 1,
with conventional IV double-dose (0.2 mmol/kg) Gd -
enhanced MRA. Fig. 6 shows sample images from
their experiments. Their results indicate that there is
no significant difference ( P >0.05) in accuracy
between IA- and IV-Gd–enhanced MRA. Both injec-
tion methods also have similar accuracy to x-ray DSA.
IA stenosis measurements have slightly greater varia-
tion than IV measurements (Fig. 7). The IA injections,
however, use approximately 38% less Gd dose than
IV injections.
Advantages to IA injections
During MRI-guided endovascular procedures, IA
injections offer several advantages over conventional
IV administration of contrast agent. The most impor-
tant advantage is reduced contrast-agent dosage. Sec-
ond, the local delivery of contrast agent is much more
efficient than IVadministration. Instead of waiting for
first-pass arterial passage of Gd, there is immediate
contrast-agent delivery into the vessel of interest,
analogous to x-ray DSA. IA injections thereby avoid
the need for a dose-timing test bolus [31] or other
complex schemes [25,32,33] to synchronize the arrival
of contrast agent with image acquisition. Third, per-
fusion assessment, although not yet proven, should be
superior with IA injections because the local delivery
provides a more compact immediate input bolus.
Fourth, IA injections are required for projection
imaging when there are other overlapping vascular
beds near the artery of interest, such as with the
coronary circulation (Fig. 8). Finally, IA injections
have reduced contrast-agent dispersion compared with
IV injections.
Limitations to IA injections
There are several important limitations to IA
injections of Gd. First, the FDA has not approved
catheter-directed injections for MRA. These injec-
tions represent an off-label use and unapproved route
of administration of contrast agent. Second, the
safety of IA-Gd injections is not proven. Because
the major use of IA injections will be during MRI-
guided endovascular interventions, there is little
Fig. 8. Coronal electrocardiographic-triggered 2D MRA in
canine using selective left circumflex artery Gd injection.
Injection parameters were: injected [Gd] = 6%, injection
rate = 1.5 mL/second, injection duration = 4 seconds, slice
thickness = 20 mm, and temporal resolution = 0.5 frames/
second. Direct contrast-agent injection into the left circumflex
artery prevents overlap with the left anterior descending
artery distribution during 2D projection imaging.
(Equation 2)
R.A. Omary et al / Radiol Clin N Am 40 (2002) 953–963 961

incremental risk for each injection. Gd as an alterna-
tive contrast agent for x-ray DSA has achieved
widespread use by interventional radiologists. Sev-
eral publications document its safety for DSA [34,35]
and endovascular interventions [36,37] performed
under x-ray guidance, particularly in patients with
underlying renal insufficiency. Third, there is limited
experience in humans. The expanded use of IA injec-
tions in humans is tied directly to increased use ofMRI
guidance for endovascular interventions. There may
be, however, a role for IA injections as a problem-
solving tool in selected diagnostic applications [38].
Finally, more research needs to be performed to
confirm its diagnostic accuracy for detecting stenoses
in multiple vascular distributions.
Summary
In the setting of MRI-guided endovascular inter-
ventions, catheter-directed Gd-enhanced MRA offers
many of the same capabilities as conventional x-ray
DSA. Local injections permit rapid depiction of
blood vessels and help guide interventions. The
primary benefit of IA injections is significant reduc-
tion of administered contrast-agent dose compared
with conventional IV injections. Another major bene-
fit is facilitated background suppression, including
that of adjacent vascular beds. As MRI guidance
methods improve, catheter-based Gd injections
should gain expanded use in clinical practice.
Acknowledgments
The authors thank Toye Spencer and David Botos
for assistancewithmanuscript preparation andRichard
Tang for expert help with the animal experiments.
References
[1] Bartels LW, Bos C, van der Weide R, Smits HFM,
Bakker CJG, Viergever MA. Placement of an inferior
vena cava filter in a pig guided by high resolution MR
fluoroscopy at 1.5T. J Magn Reson Imaging 2000;12:
599–605.
[2] Bucker A, Neurburg JM, Adam GB, Glowinski A,
Schaeffter T, Rasche V, et al. Real-time guidance for
inferior vena cava filter placement in an animal model.
J Vasc Interv Radiol 2001;12:753–6.
[3] Yang X, Bolster B, Kraitchman D, Atalar E. Intravas-
cular MR-monitored balloon angioplasty: an in vivo
feasibility study. J Vasc Interv Radiol 1998;9:953–9.
[4] Yang X, Atalar E. Intravascular MR imaging-guided
balloon angioplasty with an MR imaging guide wire:
feasibility study in rabbits. Radiology 2000;217:501–6.
[5] Godart F, Beregi JP, Nicol L, Occelli B, Vincentelli A,
Daanen V, et al. MR-guided balloon angioplasty of
stenosed aorta: in vivo evaluation using near-standard
instruments and a passive tracking technique. J Magn
Reson Imaging 2000;12:639–44.
[6] Omary RA, Frayne R, Unal O, et al. Magnetic reso-
nance-guided angioplasty of renal artery stenosis in a
pigmodel: a feasibility study. J Vasc Interv Radiol 2000;
11:373–81.
[7] Le Blanche AF, Rossert J, Wassef M, Levy B, Bigot
M, Boudghene F. MR-guided PTA in experimental bi-
lateral rabbit renal artery stenosis and MR angiography
follow-up versus histomorphometry. Cardiovasc Inter-
vent Radiol 2000;23:368–74.
[8] Buecker A, Neuerburg JM, Adam GB, Glowinski A,
Schaeffter T, Rasche V, et al. Real-time MR fluoros-
copy for MR-guided iliac artery stent placement. J
Magn Reson Imaging 2000;12:616–22.
[9] Dion YM, Ben El Kadi H, Boudoux C, Gourdon J,
Chakfe N, Traore A, et al. Endovascular procedures
under near-real-time magnetic resonance imaging guid-
ance: an experimental feasibility study. J Vasc Surg
2000;32:1006–14.
[10] Quick HH, Ladd ME, Nanz D, Mikolajczyk KP, De-
batin JF. Vascular stents as RF antennas for intravas-
cular MR guidance and imaging. Magn Reson Med
1999;42:738–45.
[11] Serfaty JM, Yang X, Aksit P, Quick HH, Solaiyappan
M, Atalar E. Toward MRI-guided coronary catheteri-
zation: visualization of guiding catheters, guidewires,
and anatomy in real time. J Magn Reson Imaging
2000;12:590–4.
[12] Serfaty JM, Atalar E, Declerck J, et al. Real-time pro-
jection MR angiography: feasibility study. Radiology
2000;217:290–5.
[13] Kee ST, Rhee JS, Butts K, Daniel B, Pauly J, Kerr A,
et al. MR-guided transjugular portosytemic shunt place-
ment in a swine model. J Vasc Interv Radiol 1999;
10:529–35.
[14] Strother CM, Unal O, Frayne R, Turk A, Omary RA,
Korosec FR, et al. Endovascular treatment of experi-
mental canine aneurysms: feasibility with MR imaging
guidance. Radiology 2000;215:516–9.
[15] Bos C, Smits HM, Zijlstra JJ, van der Mark WAMA,
Blankestijn PJ, Bakker CJG, et al. MRA of hemodialy-
sis access grafts and fistulae using selective contrast
injection and flow interruption. Magn Reson Med
2001;45:557–61.
[16] Manke C, Nitz WR, Djavidani B, Strotzer M, Lenhart
M, Volk M, et al. MR imaging-guided stent placement
in iliac arterial stenoses: a feasibility study. Radiology
2001;219:527–34.
[17] Omary RA, Frayne R, Unal O, Grist TM, Strother CM.
Intra-arterial gadolinium-enhanced 2D and 3D mag-
netic resonance angiography: a preliminary study. J
Vasc Interv Radiol 1999;10:1315–21.
R.A. Omary et al / Radiol Clin N Am 40 (2002) 953–963962

[18] Frayne R, Omary RA, Unal O, Strother CM. Determi-
nation of optimal injection parameters for intra-arterial
gadolinium-enhanced MR angiography. J Vasc Interv
Radiol 2000;11:1277–84.
[19] Bos C, Smits HFM, Bakker CJG, Viergever MA. Se-
lective contrast-enhanced MR angiography. Magn Re-
son Med 2000;44:575–82.
[20] Bos C, Bakker CJG, Viergever MA. Background sup-
pression using magnetization preparation for contrast-
enhanced MR projection angiography. Magn Reson
Med 2001;46:78–87.
[21] Omary RA, Henseler KP, Unal O, Smith RJ, Ryu RK,
Resnick SA, et al. Validation of injection parameters
for catheter-directed intraarterial gadolinium-enhanced
MR angiography. Acad Radiol 2002;9:172–85.
[22] Green JD, Omary RA, Vasireddy S, Tang R, Li Y, Finn
JP, et al. MR coronary angiography with intraarterial
gadolinium injection using an inversion recovery-
prepared sequence. Presented at the 29th Annual
Meeting and Scientific Session of the North American
Society for Cardiac Imaging. Chicago, October 2001.
[23] Schoenberg SO, Knopp MV, Bock M, et al. Renal
artery stenosis: grading of hemodynamic changes with
cine phase-contrast MR blood flow measurements. Ra-
diology 1997;203:45–53.
[24] Omary RA, Henseler KP, Unal O, Maciolek LJ, Finn JP,
Li D, et al. Comparison of intraarterial and intravenous
gadolinium-enhanced MR angiography with x-ray dig-
ital subtraction angiography for the detection of renal
artery stenosis in pigs. AJR Am J Roentgenol 2002;
178:119–27.
[25] Korosec FR, Frayne R, Grist TM, Mistretta CA. Time-
resolved contrast-enhanced 3D MR angiography.
Magn Reson Med 1996;36:345–51.
[26] Unal O, Korosec FR, Frayne R, Strother CM, Mistretta
CA. A rapid 2D time-resolved variable-rate k-space
sampling MR technique for passive catheter tracking
during endovascular procedures. Magn Reson Med
1998;40:356–62.
[27] Omary RA, Unal O, Koscielski DS, et al. Real-time
MR imaging-guided passive catheter tracking with use
of gadolinium-filled catheters. J Vasc Interv Radiol
2000;11:1079–85.
[28] Li D, Carr JC, Shea SM, Zheng J, Deshpande VS,
Wielopolski PA, et al. Coronary arteries: magnetiza-
tion-prepared contrast-enhanced three-dimensional vol-
ume-targeted breath-hold MR angiography. Radiology
2001;219:270–7.
[29] Omary RA, Green J, Tang R, Vasireddy S, Finn JP, Li
D. Catheter-directed Gd-enhanced renal MRA. Pres-
ented at the 13th International Workshop on MRA.
Madison (WI), September, 2001.
[30] Hwang KP, Green JD, Li D, Simonetti OP, Resnick SA,
Finn JP, et al. Minimizing contrast agent dose during
intraarterial gadolinium-enhanced MR angiography:
in vitro assessment. J Magn Reson Imaging 2002;15:
55–61.
[31] Earls JP, Rofsky NM, DeCorato DR, Krinsky GA,
Weinreb JC. Hepatic arterial-phase dynamic gadoli-
nium-enhanced MR imaging: optimization with a test
examination and a power injector. Radiology 1997;203:
268–73.
[32] Foo TKF, Saranathan M, Prince MR, Chenevert TL.
Automated detection of bolus arrival and initiation of
data acquisition in fast, three-dimensional, gadolinium-
enhanced MR angiography. Radiology 1997;203:275–
80.
[33] Wilman AH, Riederer SJ, King BF, Debbins JP, Ross-
man PJ, Ehman RL. Fluoroscopically triggered con-
trast-enhanced three-dimensional MR angiography
with elliptical centric view order: application to the
renal arteries. Radiology 1997;205:137–46.
[34] Kinno Y, Odagiri K, Andob K, Itoh Y, Tarao K. Ga-
dopentetate dimeglumine as an alternative contrast ma-
terial for use in angiography. AJR Am J Roentgenol
1993;160:1293–4.
[35] Matchett WJ, McFarland DR, Russell DK, Sailors DM,
Moursi MM. Azotemia: gadopentetate dimeglumine as
contrast agent at digital subtraction angiography. Radi-
ology 1996;201:569–71.
[36] Spinosa DJ, Matsumoto AH, Angle JF, Hagspiel KD.
Use of gadopentetate dimeglumine as a contrast agent
for percutaneous transluminal renal angioplasty and
stent placement. Kidney Int 1998;53:503–7.
[37] Spinosa DJ, Matsumoto AH, Angle JF, Hagspiel KD,
McGraw JK, Ayers C. Renal insufficiency: usefulness
of gadodiamide-enhanced renal angiography to supple-
ment CO2-enhanced renal angiography for diagnosis
and percutaneous treatment. Radiology 1999;210:
663–72.
[38] Taylor DJ, Brown G. Intra-arterial contrast enhanced
MR angiography (IA-CEMRA) In: Proceedings of the
International Society of Magnetic Resonance in Med-
icine. 8th edition. Berkeley (CA): International Society
of Magnetic Resonance in Medicine; 2000. p. 466
[abstract].
R.A. Omary et al / Radiol Clin N Am 40 (2002) 953–963 963