Embed Size (px)
Citation preview

Caudal epidural
Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip.
Diab. DCA, Dip. Software statistics – Ph D physiology.
Mahatma gandhi medical college and research institute, puducherry, India

2
Introduction
• easiest and safest approach to the epidural space
• sole anaesthetic for some procedures, or it may be combined with general anaesthesia.
• peri and post operative analgesia in adults and children

3
History
• Cathelin 1901 • Hingson 1943 (labour pain )• Brazilian anaesthetists 1962 popularized for
paediatrics • Failures??
• 5 % failure if selection of cases is commonsense based

4
INDICATIONS
• Anaesthesia and analgesia below the umbilicus• Obstetric analgesia for the 2nd stage or
instrumental deliveries• Chronic pain problems such as leg pain after
prolapsed intervertebral disc, or post shingles pain below the umbilicus.
• Common in paediatrics – circumcision, hernia, orchiopexy, hypospadias

5
Newer adult indications
• vasospastic or vasocclusive disease, including frostbite and ergotamine toxicity
• Cancer pain management

6
Newer adult indications
• percutaneous epidural neuroplasty• the use of caudal analgesia following lumbar
spinal surgery
• caudal analgesia after emergency orthopedic
lower extremity surgery;

7
And extra
• Better post op period • Preemptive analgesia • Only technique for premature
infants

8
Contraindications
• Infection near the site of the needle insertion.• Coagulopathy or anti coagulation. • Pilonidal cyst • Congenital abnormalities of the lower spine or
meninges,• Hydrocephalus and intracranial tumors
decrease intracranial compliance

9
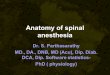
Anatomy

10
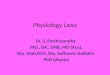
Triangle

11
• The sacral hiatus is a defect in the lower part of the posterior wall of the sacrum formed by the failure of the laminae of S5 and/or S4 to meet and fuse in the midline
• The sacral canal is a continuation of the lumbar spinal canal which terminates at the sacral hiatus.

12
The sacral canal contains
• The terminal part of the dural sac, ending between S1 and S3.
• The five sacral nerves and coccygeal nerves making up the cauda equina
• The filum terminale• Epidural fat, the character of which changes from a
loose texture in children to a more fibrous close-meshed texture in adults.

13
So the problem is puberty

14
Technique
• There are three main approaches:
• prone, • semi-prone, • lateral

15
Practical problems in anatomy
• Size, position of sacral hiatus :• Semi closed, closed or asymmetrical• AP diameter • 2 mm to 1.5 cm• Lateral width

16
Practical problems in anatomy
• Volume of sacral canal :• 12 ml to 65 ml • Sacral foramina • Posterior sacral foramina – sacro
spinalis muscles.• Anterior sacral foramina unobstructed • Curvature :• Less – more straight needle – females

17
Practical problems in anatomy
• Lordosis and lumbosacral angle
• Cephalad flow less in lordotics • Epidural fat • Loose wide meshed to tight
fibrous in adults • Predictable in children to
unpredictable spread in adults

18
Equipment
• A Crawford needle similar to Touhy needle
• Crawford needle's bevel is in alignment with
the shaft of the needle so that a catheter
exits the needle in a straight line.
• The Crawford needle is ideal for either
single-shot local anesthetic injection or for
placement of a caudal epidural catheter.
• Routine needles of 21 to 25 G

19
Adults –prone ok -internal rotation of ankle -not sedated

20
Semiprone & lateral
• Sedation is ok • Children - lateral is fine • Easy to find landmarks • Don’t overflex knees as in lumbar epidural

21
Palpate up from down coccyx feel hiatus
depression- distance

22
Technique
• Local anaesth.• Less than 0.5 ml • 45 * from the sacrum • Pierce sacro coc. Mem• Angle to 30 - 15 degrees • Two methods

23
Aspirate Midline lump??Whoosch test

24
Gauge needle
• 22 or 23 or 21 • 21 = feel good • Easy
• 23 or 24 good in infants

25
Flouroscopy

26
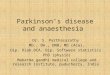
USG guided
• Ultrasound may be used as an effective screening tool for caudal epidural injections. Anatomic variations of the sacral hiatus can be clearly observed using ultrasound.

27
Dose ??
• Segment • Age • Weight • Local anaesthetics

28
Dose
• 0.25 mg / kg / segment of 0.25 % bupivacaine
• T 10 level , 10 kg
• 13 * 10 * 0.25 = 32.5 mg of bupivacaine • = 6.5 ml of 0.5 % bupi or 13 ml of 0.25 %

29
Armitage schedule
• Armitage recommends bupivacaine
• 0.5ml/kg for a lumbosacral block, • 1 ml/kg for a thoraco-lumbar block,• 1.25 ml/kg for a mid thoracic block• one part of 0.9% NaCl to three parts local
anaesthetic to produce a 0.19%

30
Verghese
• Sacral : 0.5 ml/kg
• Lumbar : 1 ml/kg
• Thoracolumbar : 1.25 ml/kg

31
Schrock
• Sacral : 0.7 ml/kg
• Lumbar : 1 ml/kg
• Thoracolumbar : 1.3 ml/kg

32
Dose with age
0.1 mL/ segment/year of age
1% lidocaine or 0.25% bupivacaine.
Dose : adults = 3 ml /segment

33
Other drugs
• 1 mL/kg of 0.2% ropivacaine,
• 1 ml/kg of 1% lignocaine
• Levobupi 0.25 % 1 mg /kg •

34
Tingling is OK
• Tingling or a feeling of fullness that extends from the sacrum to the soles of the feet is common during injection.
• The injection should never be more than 10 ml/30 seconds.

35
Additives
• Epinephrine : 1 in 2 lakh • Ketamine : 0.5 mg/kg• Clonidine at 1 to 2 mcg/kg • Tramadol 1 mg/kg • Neostigmine 2 mcg/kg • Morphine 30 mic/kg --
others??

36
The large capacity of the sacral canal
• significant volumes may be lost through the wide
anterior sacral foramina.
• the caudal dose requirements of local anaesthetics are
significantly larger to effect the same segmental
spread. Roughly twice
• Drugs injected in the caudal space take longer to
spread

37
Caudal catheters
• Intraop and postop analgesia and stress reduction in major cases
• 0.1 % bupi - 0.4 mL/kg per hr • Add opioids – if necessary - fentanyl sos

38
Complications
• Intravascular or intraosseous injection. This may lead to grand mal seizures and/or cardio-respiratory arrest.
• Test dose & aspiration• Perforation of the rectum – beware
of infection than needle prick

39
Complications- continued
• Sepsis – very rare • Urinary retention.• Subcutaneous injection• Inadequate block • Haematoma • Unpredictability • Hypotension ??

40
Some examples
• 2 kg infant for herniotomy
• 0.25 mg / kg / segment
• 13 * 2 * 0.25 = 6.5 mg = 2.6 ml of 0.25% bupi

41
Some examples what to follow ??
• 15 kg 4 years child - club foot • 0.25 mg / kg / segment • 0.25 * 15 * 10 = 37.5 mg • 15 ml of 0.25 % BUPI • OR 0.1 mL/ segment/year of age • 0.1 * 10 * 4 = 4 ml

42
Thank you for listening like this