Embed Size (px)
Citation preview
CCERTIFIED
FFINANCIAL
CCOUNSELOR
Georgia Chapter
FFFIIISSSCCCAAALLLLLLYYY FFFIIITTT
Training and Reference Manual 2011-2012
CPAR / CFC 2011-2012 Committee
“FISCALLY FIT”
FACILITATOR Carmen Sessoms, FHFMA
Firstsource
BOARD MEMBER Gail Scarboro-Hritz, CHFP
Navigant Consulting - Healthcare Practice
CPAR/CFC CHAIRPERSON Ricky Wainscott
Gwinnett Hospital System
CPAR/CFC CO-CHAIR Linda Johnson
RelayHealth
CPAR/CFC COMMITTEE James Barwick
Gwinnett Hospital System
Bonnie Breland Phoebe Putney Memorial Hospital
Amon Buchanan Gwinnett Hospital System
Maria Cancela Chamberlin Edmonds
Cathy Dougherty, FHFMA
Gwinnett Hospital System
Janet Jester
The Medical Center of Central Georgia
Elizabeth Richards, FHFMA
Clinton A. Harkins, P.C. Attorney At Law
Brenda Stodghill, FHFMA
Tift Regional
Debbie Young
FirstSource
As this was the first year to
merge the CPAR and CFC
Committees, this dedicated
team of individuals have
exceeded all expectations to
provide you with the utmost
quality and level of expertise
in the pages of this manual.
A special thank you is
extended to Amon
Buchanan for her energy
and commitment as she so
graciously accepted the
technical challenge to
reformat the CPAR manual
and incorporate those items
identified as updates to the
content of both the
CPAR/CFC manuals.
ACKNOWLEDGEMENTS
The Georgia Chapter of HFMA & the CPAR/CFC Committee would like to extend its sincere
appreciation to the following individuals and organizations that volunteered in the production of
the 2011-2012 CPAR/CFC Training and Reference Manuals:
Chamberlin Edmonds
Linda Benefield
Firstsource
Mary Acosta
Gwinnett Hospital System
Carol Fowler
Susie Kelso
Jamie Lloyd
Carolyn Regen
Melissa Smith
RelayHealth
RoxAnne Anderson
Nicole Harris
Nicole Smith
Tift Regional
Sherry Robinson
Carole Walker
CERTIFIED FINANCIAL COUNSELOR
TABLE OF CONTENTS
INTRODUCTION Chapter 1 - ACCESSING A HOSPITAL Chapter 2 – COLLECTING FROM THE PATIENT OR GUARANTOR Chapter 3 – UNDERSTANDING COLLECTION LAW
The Fair Debt Collection Practices Act The Fair Credit Reporting Act
Chapter 4 – HOW TO COLLECT Chapter 5 – FINANCIAL ASSISTANCE PROGRAMS Chapter 6 – PAYMENT PLANS Chapter 7 – DISCOUNTS Chapter 8 – INSURANCE VERIFICATION & PRE-CERTIFICATION Chapter 9 – INSURANCE DENIALS AND APPEALS
Denial Types
Technical vs. Clinical Denials
Other Substantive Denials
Medical Necessity Denials
Hard vs. Soft Denials
Partial Denials The Appeals Process
Initial Steps
Know Your Contacts
Follow-Up
Exhaust All Available Options
CERTIFIED FINANCIAL COUNSELOR
TABLE OF CONTENTS, continued
Chapter 10 – MEDICAID, MEDICARE & WORKERS COMPENSATION Chapter 11 – ALTERNATIVE PAYER SOURCES
Third Party Liability
Cancer State Aid
Vocational Rehabilitation Program
Children’s Medical Services
Veterans Health Administration
Estates
Crime Victims Chapter 12 – LEGAL REMEDIES
Judgment Liens
Garnishments
Hospital Liens
Bankruptcy Chapter 13 – GEORGIA PROMPT PAY LAWS Chapter 14 – HEALTH SAVINGS ACCOUNTS (HSA’s) Chapter 15 - PROHIBITED PRACTICES (Senate Bill 476 Enacted) Sources

INTRODUCTION
The Certified Financial Counselor (CFC) program, organized by the Georgia Healthcare Financial Management Association in 2005, equips healthcare financial professionals with the tools and skills necessary to locate funding, secure payment and funding sources, and determine the best financial solution available for patients with a focus on the underinsured and uninsured. By providing training and access to financial solutions, Certified Financial Counselors promote the utilization of critical thinking skills, a friendly and helpful personality, social worker approach, and the treatment of all patients with dignity and respect.
Certification in Financial Counseling offers benefits such as increased self-esteem, educational advancement and improved job performance.
Congratulations on your commitment to becoming a Certified Financial Counselor.
Chapter 1 - ACCESSING A HOSPITAL
Pre-Registration Patients have their first interaction with hospitals for medical care in many ways:
Scheduling tests or procedures
The Emergency Room for an emergent condition
Their physician‘s office where hospital materials may be provided
Telephone contact from a hospital employee for pre-registration
Materials mailed to a patient for a future visit One of the most valuable access processes is the ―pre-registration program.‖ The objective of a pre-registration program should be to complete all possible processes prior to access (admission) or date of service, preferably by telephone. Mail will work, as well, if the patient is scheduled well in advance. There are a multitude of benefits to pre-registration, both for the patient and the hospital. For Example: 1) Going through the registration steps prior to admitting the patient familiarizes them with the entire access process, hospital regulations and procedures. 2) Pre-registration reduces processing time on the date of access by allowing patients to complete many requirements in advance. For the patient this means less waiting and faster throughput to care. 3) Pre-registration also educates the patient, giving them time to understand insurance/employer requirements and expected benefit levels. 4) Pre-registration allows time for complete and sound financial arrangements to be made, avoiding account issues after the fact. 5) Pre-registration facilitates the flow of information between the physician and the hospital. This timely data exchange can prevent unnecessary work duplication, improve the quality of patient information, and foster a more cooperative relationship between the hospital and the physician. 6) The pre-registration process allows the hospital to proactively plan for the patient visit. Scheduling of procedures and/or tests can also be incorporated at this time. 7) Pre-registration allows/sets the stage for pre-notification – the act of informing the patient of co-payment and deductible responsibility, of where to park, of where to go once in the hospital, of what other issues they may expect on the date of service.
Chapter 1 - ACCESSING A HOSPITAL, continued Pre-Registration, continued All hospitals should create some type of pre-registration form designed to capture all data necessary to assess the patient‘s ability to pay and meet the hospital‘s financial requirements. Financially securing accounts prior to rendering medical services is a proven best practice. For this reason, Financial Counselors should be involved in the pre-registration process as soon as possible. The following information should be the minimum data set of information obtained from the patient: Patient:
Name, address, telephone number and email address
Date of birth
Social security number
Next of kin and personal representative information
Employer information
Guarantor information (if not the patient)
Advance Directive information Guarantor (if different than the patient):
Name, address, telephone number and email address
Date of birth
Social security number
Employer information Insurance:
Name, address and telephone number of insurance company
Name of insured
Relationship of insured to patient (if different than patient)
Policy or contract number
Group number and group name
Retirement date (if applicable)
Claim mailing address
Pre-certification information
Accident type, date and place (if applicable)
Medicare Secondary Payer (MSP) questions (for all Medicare beneficiaries)
Chapter 1 - ACCESSING A HOSPITAL, continued Insurance, continued: Accessing a hospital through the Emergency Department presents many challenges for gathering accurate patient data and financially securing the account. Best practice has shown that a Financial Counseling function in Emergency Departments will produce increased point-of-service collections. Patient Access personnel may be made responsible for collecting money from patients during the discharge process (remember EMTALA prevents asking questions regarding ability to pay until the patients condition has been assessed). A better plan may be for a dedicated Financial Counselor who has more time to review a patient‘s history with the facility, to review online insurance eligibility, and review the charges being incurred to allow a realistic conversation with the patient/guarantor about payment options. The Financial Counselor may also provide a better customer service approach to collecting. Regardless of where the responsibility lies for collection of Emergency Department charges, it is recommended that a program for collection in Emergency settings be established. Once established, it is imperative that the Patient Access management work closely with nursing staff to assure that all (or most) patients are routed by the Financial Counselor or designated collector before leaving the Emergency Department. Finally, be certain to fairly apply any applicable prompt payment or other policy-approved discounts to your self-pay accounts. Pre-Notification
The benefits of pre-notification are only as good as the pre-registration process. The purpose of pre-notification is to alert scheduled patients to a variety of issues they need to be aware of prior to access. For example: 1) The patient‘s insurance may not cover the procedure they are scheduled to undergo. If the benefits are exhausted or the service is not covered, the patient must be made aware of the lack of coverage and that the responsibility for payment is theirs, so they can plan accordingly. 2) Where required, a pre-certification or pre-authorization from the person‘s insurance carrier must be obtained before the date of service. The patient must be made aware of the requirement and their potential liability if not completed. Patients may also be helpful in communicating with their insurance carrier and the ordering physician. 3) The out of pocket portion of the future hospital visit should be communicated to the patient. The patient should be instructed in a very polite tone to be prepared on the date of service/or pre-op date, to pay the out of pocket expenses. If the patient cannot pay all of what is owed, payment arrangements or financial assistance should be offered based on hospital policy. 4) Outstanding balances from prior visits should be resolved with the patient/guarantor. Chapter 1 - ACCESSING A HOSPITAL, continued
Pre-Notification, continued
5) Pre-notification should include instructions to the patient regarding when to arrive, where to go, directions, and personal items which should or should not be brought. If parking is problematic, it is a great time to advise on where to park, and if there is a charge for parking, the patient should be made aware at this time. As you can see, without a thorough pre-registration process, these important issues might not be spotted. It is critical that personnel in pre-registration/pre-notification work to resolve the problems prior to the date of service. Obviously any of the above-mentioned scenarios could negatively impact reimbursement. Using dedicated Financial Counselors in the pre-notification process has proven to be a best practice.
Chapter 2 - COLLECTING FROM THE PATIENT OR GUARANTOR
Point of Service Collections
The best time to collect healthcare self-pay portions from the patient is prior to the patient receiving service, except where EMTALA laws apply. The provider has a psychological advantage when collections are attempted prior to the patient‘s arrival at the medical facility or at point of service. The hospital (or other medical provider) should have methods in place to calculate patient portions of an estimated bill prior to the time of service. For example:
An out of pocket expense amount may be obtained by utilization of one of several automated programs designed to provide benefits verification within seconds – during the registration process
An out of pocket amount may be derived by verifying coverage limits and co-pay requirements telephonically. The telephone, though sometimes slow and tedious, is often the most reliable way to determine the patients out of pocket amount
An estimate of the out of pocket amount may be accomplished by taking an average out of pocket for a particular payer, type of service, etc. If this method is utilized, collect slightly lower than the average, which should help avoid over collecting which necessitates refunds
One may also just choose to come up with a reasonable deposit. The deposit should be more than simply a wild guess; it should be based on current verified data for the procedure.
Note: In each of the estimate, deposit, and even verified scenarios listed above, there should be disclaimers to state, ―This is only an estimate‖. When presenting the estimate to the patient, the Financial Counselor or other staff should offer detailed explanations. The best advice is to:
Reveal the range from which estimates were derived
Clarify that charges could be more or less than the estimated amount
Explain how charges are applied
Explain that final charges are based on actual services provided
Provide a written copy of the estimate, including a disclaimer statement
Be prepared to discuss payment options and means of payment (cash, check, charge
cards, debit cards, automated bank drafts)
Notify the patient regarding any applicable discounts which policy allows
Chapter 2 - COLLECTING FROM THE PATIENT OR GUARANTOR, continued
The Five Health Care Collection Control Points
1. Before Admissions / Registration and before service is provided, except when EMTALA laws apply
Obtain all critical information by telephone
Verify insurance and obtain any pre-authorizations
Estimate patients portion of bill and insurance coverage
State policy and financial counseling process
Have Financial Counselor interview patient, as needed
2. At Admission / Registration
Review information obtained with patient/guarantor
Obtain necessary signatures on legal documents
Triage consistent with EMTALA for Emergency Department admits
Obtain insurance and demographic info and estimate patient portion for all direct admits
Collect amounts due from patient/guarantor
Refer patients to a Financial Counselor for financial assessment, if needed
3. In-house
Monitor charges or any changes in benefit levels
For in-house admissions, hospital should set a dollar amount of charges and length of stay thresholds for Financial Counselor review (i.e., 7 days length of stay and/or $10,000 in charges)
Financial Counselors should work closely with in-house Case Managers/Utilization Management to ensure insurance coverage and funding for medical services
4. At Discharge
Collect patient‘s portion or make financial arrangements
Review insurance benefits as documented and explain the statement cycle that the patient/guarantor should expect
Refer patients to a Financial Counselor for financial assessment, if needed
5. Post Discharge – Collection follow-up
Follow-up overdue accounts from patient or insurance.
Follow-up by telephone, on payer web sites, by fax, or other payer specified access avenues
Take problematic accounts to periodic meetings your provider‘s Managed Care Department may have with payers
Don‘t just obtain a status – get a payment release date. Set tickler file for follow-up call on that date. If payment not yet released, demand payment from insurer
Chapter 3 – UNDERSTANDING COLLECTION LAW
The Fair Debt Collection Practices Act (FDCPA)
The Fair Debt Collection Practices Act (aka FDCPA) is a United States statute added in 1978 as Title VIII of the Consumer Credit Protection Act. Its purposes are to eliminate abusive practices in the collection of consumer debts, to promote fair debt collection and to provide consumers with an avenue for disputing and obtaining validation of debt information in order to ensure the information's accuracy. The Act creates guidelines under which debt collectors may conduct business, defines rights of consumers involved with debt collectors, and prescribes penalties and remedies for violations of the Act. It is sometimes used in conjunction with the Fair Credit Reporting Act, which will be discussed in more detail in this chapter.
The FDCPA broadly defines a debt collector as "any person who uses any instrumentality of interstate commerce or the mails in any business the principal purpose of which is the collection of any debts, or who regularly collects or attempts to collect, directly or indirectly, debts owed or due or asserted to be owed or due another." While the FDCPA generally only applies to third party debt collectors--not internal collectors for an "original creditor" e.g. the hospital -- some states, have similar state consumer protection laws which mirror the FDCPA, and regulate original creditors. In addition, courts have generally found debt buyers to be covered by the FDCPA even though they are collecting their own debts. The definitions and coverage have changed over time. The FDCPA itself contains numerous exceptions to the definition of a "debt collector," particularly after the October 13, 2006, passage of the Financial Services Regulatory Relief Act of 2006 (for an overview, see http://banking.senate.gov/public/_files/RegRel_summary.pdf). Attorneys, originally explicitly excepted from the definition of a debt collector, have been included (to the extent that they otherwise meet the definition) since 1986.
The FDCPA's definitions of ―consumers‖ and ―debt‖ specifically restrict the coverage of the act to personal, family or household transactions. These laws are for the protection of the debtor and debt collectors. Our society has become highly litigious. With information like the FDCPA so accessible, the person on the other end of the phone may very well be as equally knowledgeable of their rights under this act as the collector. How does this relate to Healthcare, you may ask? It is simple, each healthcare professional should be: Informed and thoroughly compliant with all aspects of this act, and; Have every applicable member of our organizations equally aware and in compliance
with the requirements. Although a full copy of the FDCPA is not included in this manual, a basic outline has been provided to guide collections in the most critical aspects of the Act as they relate to your job.
Chapter 3 – UNDERSTANDING COLLECTION LAW, continued The complete FDCPA is available on the FTC website @ www.ftc.gov/os/statutes/fdcpa/fdcpact.htm. This summary is not intended to provide all necessary information regarding the FDCPA. Here are the essentials: 1) Correspondence with the consumer:
Notify the consumer with a validation notice that the account is with a debt collection agency.
The consumer has 30 days from the date of their validation notice to dispute their debt in writing.
When the consumer disputes their debt in writing within the 30 days, the debt collector must either mail the consumer the requested validation information or cease collection efforts altogether or file suit.
2) Speaking with the consumer on the telephone:
Debt collector must identify themselves and notify the consumer that the communication is from a debt collector with the intent to collect a debt.
Calls must be placed between 8:00am and 9:00pm local time of the consumer.
If the consumer has made you aware that certain times or places are inconvenient, calls during such times or to such places must cease.
Calls to the consumer‘s place of employment are prohibited a) if you know or have reason to know that the employer forbids this type of communication and b) when the consumer has requested in writing that this contact is not acceptable.
Causing a telephone to ring or engaging a person in conversation repeatedly or continuously with the intent to annoy, abuse or harass is prohibited.
When a consumer requests in writing that all contact stop and that they refuse to pay the debt, you may not engage in telephone communications; however you can provide written notice that either a) collection efforts are being terminated or b) that you intend to file a lawsuit or pursue other remedies when permitted.
The debt collector may not contact the consumer after receipt of their dispute of a debt during their 30 days from the date of receipt of their validation notice of their debt.
3) Third-party involvement on the consumer‘s behalf:
If the consumer has acquired legal representation, as a collector, you are barred from legally speaking to anyone concerning the consumer‘s debt(s) other than the above-mentioned attorney.
If there is no attorney involved, you may contact people whom the debtor in question knows, but only to determine where the consumer lives and works. Take precaution that you not speak with this type of third party more than once, instead get the information you need while you are talking to them. You may at no time disclose – unless you are speaking with an attorney – that the consumer owes money
Chapter 3 – UNDERSTANDING COLLECTION LAW, continued
4) Certain types of behavior that are prohibited: Harassment:
Threats of violence against the person, their property, or their reputation
Publishing a list of consumers who refuse to pay their debts (except to a credit bureau)
Use of obscene or profane language
Repeatedly calling the consumer with the intent to unnerve or annoy False or Misleading Information:
Failing to identify yourself when calling the consumer
Falsely imply that you are an attorney or government representative
Falsely imply that the consumer has committed a crime
Falsely imply that you work for or represent a credit bureau
Failing to accurately communicate that actual dollar amount of the debt(s)
Claiming information being mailed is a legal document when it is not, or, that information being mailed is not a legal document when it is
Telling the consumer that he/she will be arrested for failure to pay the debt(s)
Threatening the consumer with seizure or garnishment
The use of any false representation or deceptive means to collect or attempt to collect any debt or obtain information concerning a consumer
Unfair Practices:
The collection of any amount (including any interest, fee, charge, or expense incidental to the principal obligation) unless such amount is expressly authorized by the agreement creating the debt
The acceptance by a debt collector from any person of a check or other payment instrument postdated by more than five days unless such person is notified in writing of the debt collector‘s intent to deposit such check or instrument not more than ten or less than three business days prior to such deposit
The solicitation by a debt collector of any postdated check or other postdated payment instrument for the purpose of threatening or instituting criminal prosecution
Depositing or threatening to deposit any postdated check or other postdated payment instrument prior to the date on such check or instrument.
Communicating with a consumer regarding a debt by post card. Violations of these ―practices‖ can be $1000.00 per offense.
The Fair Credit Reporting Act (FCRA) - The Fair Credit Reporting Act (FCRA) is United States federal law that regulates the collection, dissemination, and use of consumer credit information. As with the FDCPA, only a summary of the FCRA is included here. To read the Act in its entirety, it is available on www.ftc.gov/os/statutes/fcra.htm.
Chapter 3 – UNDERSTANDING COLLECTION LAW, continued
The Fair Credit Reporting Act (FCRA) is designed to promote accuracy, fairness, and privacy of information in the files of every "consumer-reporting agency" (CRA). Most CRAs are credit bureaus that gather and sell information about you to creditors, employers, and other businesses. This information includes:
where you work and live
if you pay your bills on time
whether you've been sued, arrested, or filed for bankruptcy
the types of debts you have, i.e. credit cards, homes, auto‘s etc.
The FCRA gives individuals specific rights in dealing with CRAs which requires them to provide consumers with a summary of these rights as listed below. The complete text of the FCRA, 15 U.S.C., 1681 et seq. at the Federal Trade Commission‘s web site (http://www.ftc.gov).
Individuals must be told if information in their file has been used against them. Anyone who uses information from a CRA to take action against an individual (such as denying an application for credit, insurance, or employment) must provide the name, address, and phone number of the CRA that provided the report.
Consumers are able to find out what is in their file. A CRA must provide all the information in one‘s file, and a list of everyone who has requested it recently. However, individuals are not entitled to a "risk score" or a "credit score" that is based on information in their file. There is no charge for the report if a person‘s application was denied because of information supplied by the CRA, although the request for the report must occur within 60 days of receiving the denial notice.
Individuals are also entitled to one free report a year if it is certified that (1) they are unemployed and plan to seek employment within 60 days, (2) they are on welfare, or (3) their report is inaccurate due to fraud. Otherwise, a CRA may charge you a fee of up to eight dollars. Currently, one free credit report per year (from each of the big three consumer reporting agencies - Equifax, Experian & Trans Union) has been made available courtesy of AnnualCreditReport.com.
Consumers can dispute inaccurate information with the CRA. If an individual tells a CRA that their file contains inaccurate information, the CRA must reinvestigate the items (usually within 30 days) unless the dispute is frivolous. The CRA must pass along to its source all relevant information the individual provides. The CRA also must supply written results of the investigation and a copy of the report, if it has changed. If an item is altered or deleted because it is disputed, the CRA cannot place it back in the file unless the source of the information verifies its accuracy and completeness, and the CRA provides a written notice that includes the name, address and phone number of the source.
Chapter 3 – UNDERSTANDING COLLECTION LAW, continued
Inaccurate information must be deleted. A CRA must remove inaccurate information from its files, usually within 30 days after disputing its accuracy. The largest credit bureaus must notify other national CRAs if items are altered or deleted. However, the CRA is not required to remove data from a file that is accurate unless it is outdated or cannot be verified.
It is possible to dispute inaccurate items with the source of the information. If mentioned (such as to a creditor who reports to a CRA) that an item is disputed, they may not then report the information to a CRA without including a notice of the dispute. In addition, once the source is notified of the error in writing, they may not continue to report it if it is in fact an error. Outdated information may not be reported. In most cases, a CRA may not report negative information that is more than seven years old; ten years for bankruptcies.
Access to an individual‘s file is limited. A CRA may provide information about a person only to those who have a need recognized by the FCRA (usually to consider an application you have submitted to a creditor, insurer, employer, landlord, or other business). One‘s consent is required for reports that are provided to employers or that contain medical information. A CRA may not report to an individual‘s employer, or prospective employer, about or without that person‘s written consent. A CRA may not divulge one‘s medical information without their permission.
It is possible to stop a CRA from including one‘s name on lists for unsolicited credit and insurance offers. Creditors and insurers may use file information as the basis for sending unsolicited offers of credit or insurance. Such offers must include a toll-free number to call if an individual wants their name and address excluded from future lists or offers. When notifying the CRA through the toll-free number, they must keep the requestor off the lists for two years. However, individuals may request and complete the CRA form provided for this purpose, thereby having their name and address removed indefinitely.
Individuals may seek damages from violators. Additionally, it is possible to sue a CRA or other party in state or federal court for violations of the FCRA. If such a suit is won, the defendant may have to pay damages and reimbursement of attorney fees. If the individual loses and the court specifically finds the suit to be in bad faith, the individual or their attorney may have to pay the defendant's fees.
Legal Implications of Credit Reporting:
Reporting medical debt to credit agencies is often a must in our industry, especially when a patient/guarantor continuously fails to make an agreed upon payment to satisfy their financial obligation. However, being informed about the process of credit reporting - especially its legal implications - will save everyone involved the potential difficulty of improperly reporting the debt.
First of all, most credit reporting agencies require membership before they will accept information from a creditor. Membership is generally fairly inexpensive, and usually entitles the member to receive credit reports that are not available to the general public. Typically, a nominal fee is charged for each credit report accessed.
Chapter 3 – UNDERSTANDING COLLECTION LAW, continued
Secondly, a creditor can only report truthful information to a CRA, such as a debtor who did not pay a bill on time. The focus should be appropriately placed on collecting the debt - that is the first priority. Reporting is a viable recourse when that debt is uncollectible.
For that very reason, it is a good idea to notify a debtor of the intent to report their debt to a credit-reporting agency. Here are several reasons:
1) It is a good public relations move on the part of the institution. There is not a single hospital in America that wants to be known as the one that ruined someone‘s credit over a $75.00 bill. Besides, repeat customers are good business for hospitals.
2) It gives the debtor one last opportunity to satisfy the debt, and perhaps that is the very opportunity they need. Being able to speak to the debtor, about the seriousness of the debt reinforcing the obligation to pay, is sometimes all it takes to get that commitment.
3) Although there will certainly be exceptions, many debtors may simply need to know that the possibility exists of being reported to a credit-reporting agency. Often this will be all the incentive needed to clear up the debt. Remember, that the goal is to collect the money, and as long as that is accomplished legally, ethically and honestly, it is a job well done.
Credit Report:
A credit report can be intimidating and confusing when one does not know what the abbreviations and alphanumeric codes indicate. This section on credit reports is a generalized explanation with a few keys provided on the most common credit reporting codes.
There are three different reporting agencies, Experian, Trans Union, and Equifax. All three agencies may have different information on a consumer because companies may or may not subscribe to all of them. Generally, a report is organized into five different sections: 1. identifying information 2. credit/account history (also known as trade lines) 3. collection agencies 4. public records 5. inquiries Depending on the reporting agency, other sections may be provided such as credit summary, special messages, and consumer statements.
Chapter 3 – UNDERSTANDING COLLECTION LAW, continued
All five sections are fairly easy to read and understand with the exception of one: the credit/account history section. The credit bureaus use industry standard codes to report the type of account, the manner of payment, and the account designator(s) which makes this section difficult. The sections are described below.
Credit/Account History: This section reveals information about account history and lines of credit. Also, it will provide insight into a consumer‘s buying and payment activities. The creditor name and account number will be displayed. Other items provided on the report include:
When the account was opened The type of account (installment, such as a mortgage or car loan, or revolving, such as
a department store credit card) Account Designator(s): whether the account is in the consumer‘s name alone or with
another person Total amount of the loan, high credit limit or highest balance on the card How much remains as balance due Fixed monthly payments or minimum monthly amount Status of the account (open, inactive, closed, paid, etc.) Manner of payment: how well the account has been paid
During the collection process, it is important for a financial counselor to be informed of available lines of credit. Therefore, being able to determine lines of credit on cards (subtract balance due from the credit limit) is key to successful collection negotiations.
Type of Account –
O - Open Account – provides the entire balance due each month R – Revolving or Option – amount due can change each month I – Installment – fixed amount due each month
Account Designator(s) – These codes may vary slightly depending on the reporting agency.
I Individual account. The subject of the report, and no one else, is responsible for payment on the account.
J Joint account. The subject and another person or persons are jointly
responsible for payment on the account. A Authorized Use. This is a shared account, but one person has responsibility for
payment, while the other person does not. U Undesignated. This code is an indication that the credit grantor does not have
enough information to give the account a more specific designator code.
Chapter 3 – UNDERSTANDING COLLECTION LAW, continued
T Terminated. The subject relationship to the account has ended, although other parties who once shared the account with the subject may continue to maintain the account. This code is used often after a divorce, when one party continues to maintain an account, while the other party is disassociated from it.
M Maker. The subject is responsible for payment of an installment loan, but a co-
maker is involved as assurance that the loan will be repaid. C Co-maker or Co-signor. The subject has co-signed for an installment loan, and
will be responsible for payment if the borrower should default – ―guarantor‖. B On behalf of another person. The subject has financial responsibility for an
account which is used exclusively by another person, as when a father opens a charge account for his daughter‘s use at college.
S Shared, but otherwise undesignated. This codes is an indication that the credit
grantor knows that the subject and at least one other person share the account, but not enough information is available to designate the account as either J (joint) or A (authorized use).
Manner of Payment – Manner of payment codes are standardized codes/numbers and are used to report a consumer‘s payment history.
The standard codes are: 0 – Approved, but account is too new to rate or not yet used 1 – Paid as agreed 2 – 30 or more days past due 3 – 60 or more days past due 4 – 90 or more days past due 5 – 120 or more days past due or is a collection account 7– Making regular payments under a wage earner plan or other repayment arrangement 8 – Repossession 9 – Charged off account (Bad Debt)
Some agencies report manner of payments in clear statements such paid as agreed. Where others may use payment codes ranging from 1 to 9; or a combination of ‗type of account‘ with the ‗manner of payment‘, such as an R1 or I1 on a report is an indication of a good payment history on a revolving or installment account.
Chapter 3 – UNDERSTANDING COLLECTION LAW, continued
As an example of variation, Trans Union uses the following codes in addition to the standard codes/numbers as their manner of payments: 8A – Voluntary repossession 8D – Legal repossession 8P – Paying or paid account with manner of payment 08 9B – Collection account 9P – Paying or paid account with manner of payment 09 or 9B UC – Unclassified UR – Unrated Often the ‗manner of payment‘ is used to determine if a consumer/patient will pay his/her hospital balance. The higher the ‗manner of payment‘ number, the less likely the consumer/patient will pay timely or at all which will add cost to collecting balances due over the long term. Manner of payments are used often to justify write-off adjustments to uncollectible or charity. Identifying information: This section is used to confirm the identity of the individual. It is not unusual for different variations of the consumer name to be displayed. This depends on how companies have reported the information to credit bureaus. Other information displayed may include current and previous addresses, date of birth, telephone numbers, driver‘s license numbers, employer information, and spouse‘s name. Collection Agencies: This section reports accounts that have been transferred to a collection agency. The section is easy to read as it provides the collection agency name, amount due, and the date the account was transferred to bad debt. Public Records: Information applied to a consumer‘s public record is provided by county, state, and federal courts. Items reported on a public record include tax liens, civil judgments, and bankruptcies. The items remain on a credit report will vary depending on the type of record. Civil judgments = seven years Unpaid tax liens = indefinite Paid tax liens = seven years from date paid Chapter 7, 11, or 12 bankruptcies = 10 years Chapter 13 bankruptcy filings = 10 years Chapter 13 bankruptcy dismissal or discharges = seven years Bankruptcies voluntarily dismissed = seven years
Chapter 3 – UNDERSTANDING COLLECTION LAW, continued
Inquiries: The inquiring section of a credit report provides a listing of all the companies that have requested and obtained a credit report. A ―hard‖ inquiry is defined as the consumer/patient completed a credit application, and the creditor requested his/her credit report.
A ―soft‖ inquiry is defined as a company requesting information for promotional/marketing opportunities. Not all information is released or provided for ‗soft‘ inquiries.
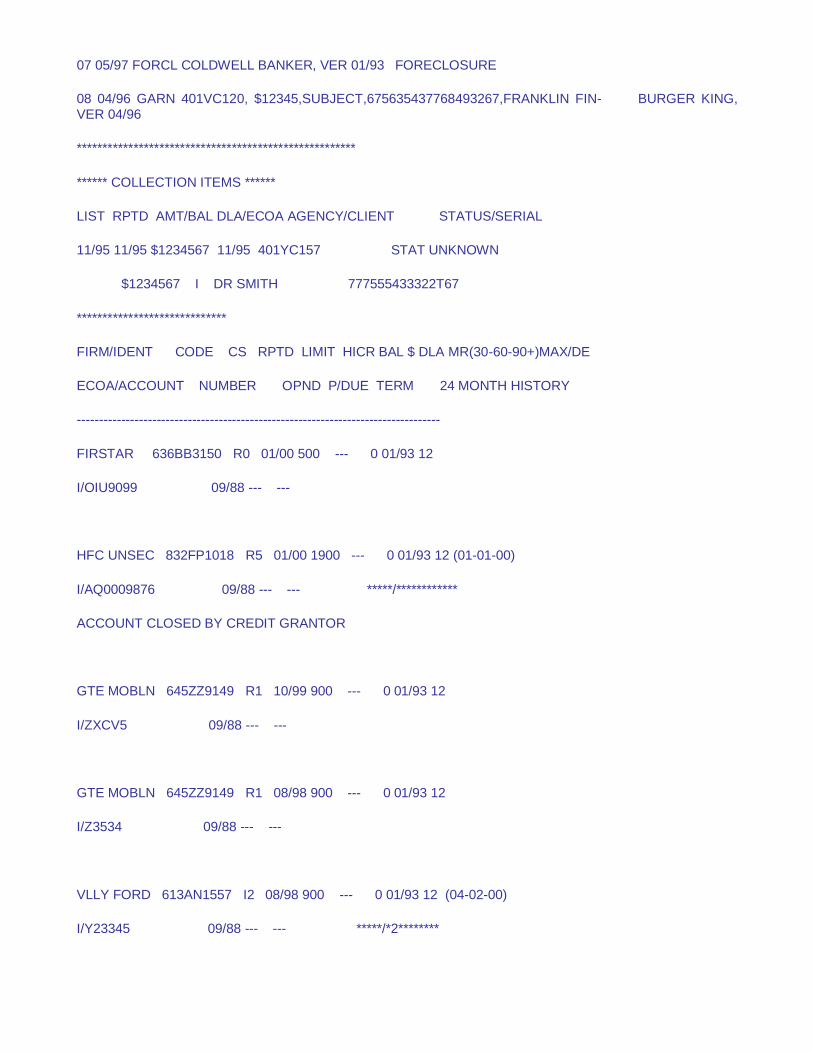
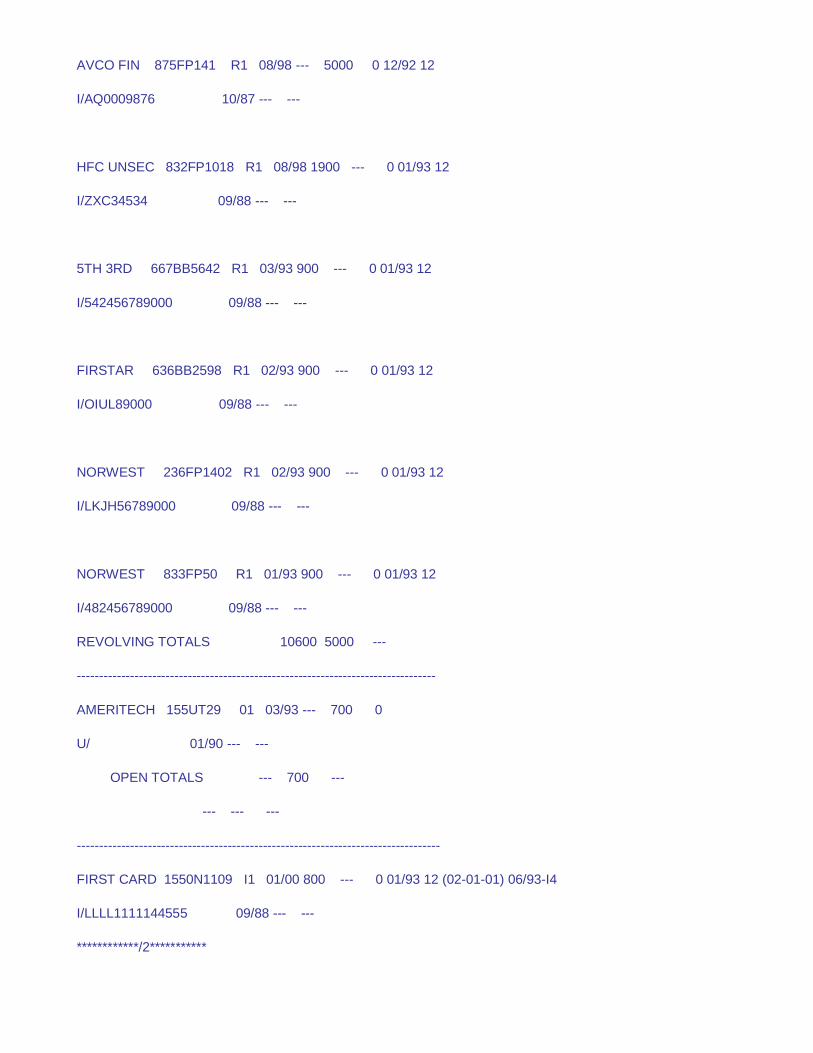
Following are examples of a Credit Report from Equifax and Experian.
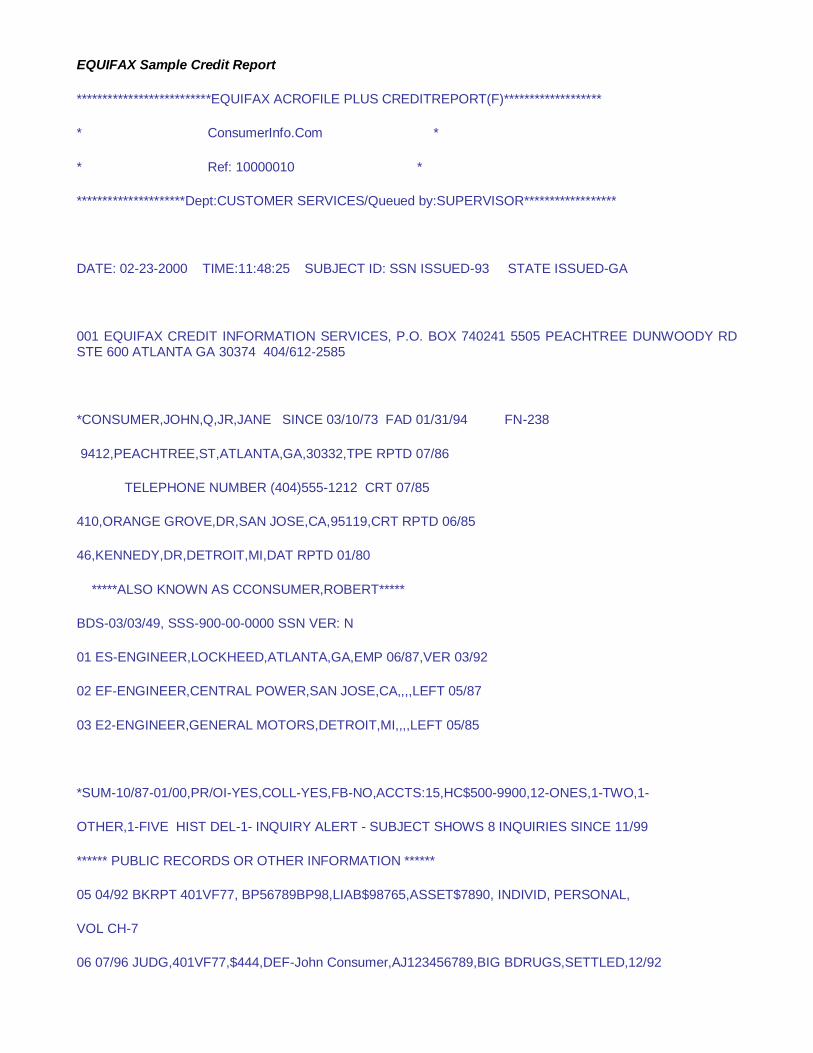
EQUIFAX Sample Credit Report
**************************EQUIFAX ACROFILE PLUS CREDITREPORT(F)*******************
* ConsumerInfo.Com *
* Ref: 10000010 *
*********************Dept:CUSTOMER SERVICES/Queued by:SUPERVISOR******************
DATE: 02-23-2000 TIME:11:48:25 SUBJECT ID: SSN ISSUED-93 STATE ISSUED-GA
001 EQUIFAX CREDIT INFORMATION SERVICES, P.O. BOX 740241 5505 PEACHTREE DUNWOODY RD STE 600 ATLANTA GA 30374 404/612-2585
*CONSUMER,JOHN,Q,JR,JANE SINCE 03/10/73 FAD 01/31/94 FN-238
9412,PEACHTREE,ST,ATLANTA,GA,30332,TPE RPTD 07/86
TELEPHONE NUMBER (404)555-1212 CRT 07/85
410,ORANGE GROVE,DR,SAN JOSE,CA,95119,CRT RPTD 06/85
46,KENNEDY,DR,DETROIT,MI,DAT RPTD 01/80
*****ALSO KNOWN AS CCONSUMER,ROBERT*****
BDS-03/03/49, SSS-900-00-0000 SSN VER: N
01 ES-ENGINEER,LOCKHEED,ATLANTA,GA,EMP 06/87,VER 03/92
02 EF-ENGINEER,CENTRAL POWER,SAN JOSE,CA,,,,LEFT 05/87
03 E2-ENGINEER,GENERAL MOTORS,DETROIT,MI,,,,LEFT 05/85
*SUM-10/87-01/00,PR/OI-YES,COLL-YES,FB-NO,ACCTS:15,HC$500-9900,12-ONES,1-TWO,1-
OTHER,1-FIVE HIST DEL-1- INQUIRY ALERT - SUBJECT SHOWS 8 INQUIRIES SINCE 11/99
****** PUBLIC RECORDS OR OTHER INFORMATION ******
05 04/92 BKRPT 401VF77, BP56789BP98,LIAB$98765,ASSET$7890, INDIVID, PERSONAL,
VOL CH-7
06 07/96 JUDG,401VF77,$444,DEF-John Consumer,AJ123456789,BIG BDRUGS,SETTLED,12/92
07 05/97 FORCL COLDWELL BANKER, VER 01/93 FORECLOSURE
08 04/96 GARN 401VC120, $12345,SUBJECT,675635437768493267,FRANKLIN FIN- BURGER KING, VER 04/96
******************************************************
****** COLLECTION ITEMS ******
LIST RPTD AMT/BAL DLA/ECOA AGENCY/CLIENT STATUS/SERIAL
11/95 11/95 $1234567 11/95 401YC157 STAT UNKNOWN
$1234567 I DR SMITH 777555433322T67
*****************************
FIRM/IDENT CODE CS RPTD LIMIT HICR BAL $ DLA MR(30-60-90+)MAX/DE
ECOA/ACCOUNT NUMBER OPND P/DUE TERM 24 MONTH HISTORY
----------------------------------------------------------------------------------
FIRSTAR 636BB3150 R0 01/00 500 --- 0 01/93 12
I/OIU9099 09/88 --- ---
HFC UNSEC 832FP1018 R5 01/00 1900 --- 0 01/93 12 (01-01-00)
I/AQ0009876 09/88 --- --- *****/************
ACCOUNT CLOSED BY CREDIT GRANTOR
GTE MOBLN 645ZZ9149 R1 10/99 900 --- 0 01/93 12
I/ZXCV5 09/88 --- ---
GTE MOBLN 645ZZ9149 R1 08/98 900 --- 0 01/93 12
I/Z3534 09/88 --- ---
VLLY FORD 613AN1557 I2 08/98 900 --- 0 01/93 12 (04-02-00)
I/Y23345 09/88 --- --- *****/*2********
AVCO FIN 875FP141 R1 08/98 --- 5000 0 12/92 12
I/AQ0009876 10/87 --- ---
HFC UNSEC 832FP1018 R1 08/98 1900 --- 0 01/93 12
I/ZXC34534 09/88 --- ---
5TH 3RD 667BB5642 R1 03/93 900 --- 0 01/93 12
I/542456789000 09/88 --- ---
FIRSTAR 636BB2598 R1 02/93 900 --- 0 01/93 12
I/OIUL89000 09/88 --- ---
NORWEST 236FP1402 R1 02/93 900 --- 0 01/93 12
I/LKJH56789000 09/88 --- ---
NORWEST 833FP50 R1 01/93 900 --- 0 01/93 12
I/482456789000 09/88 --- ---
REVOLVING TOTALS 10600 5000 ---
---------------------------------------------------------------------------------
AMERITECH 155UT29 01 03/93 --- 700 0
U/ 01/90 --- ---
OPEN TOTALS --- 700 ---
--- --- ---
----------------------------------------------------------------------------------
FIRST CARD 1550N1109 I1 01/00 800 --- 0 01/93 12 (02-01-01) 06/93-I4
I/LLLL1111144555 09/88 --- ---
************/2***********
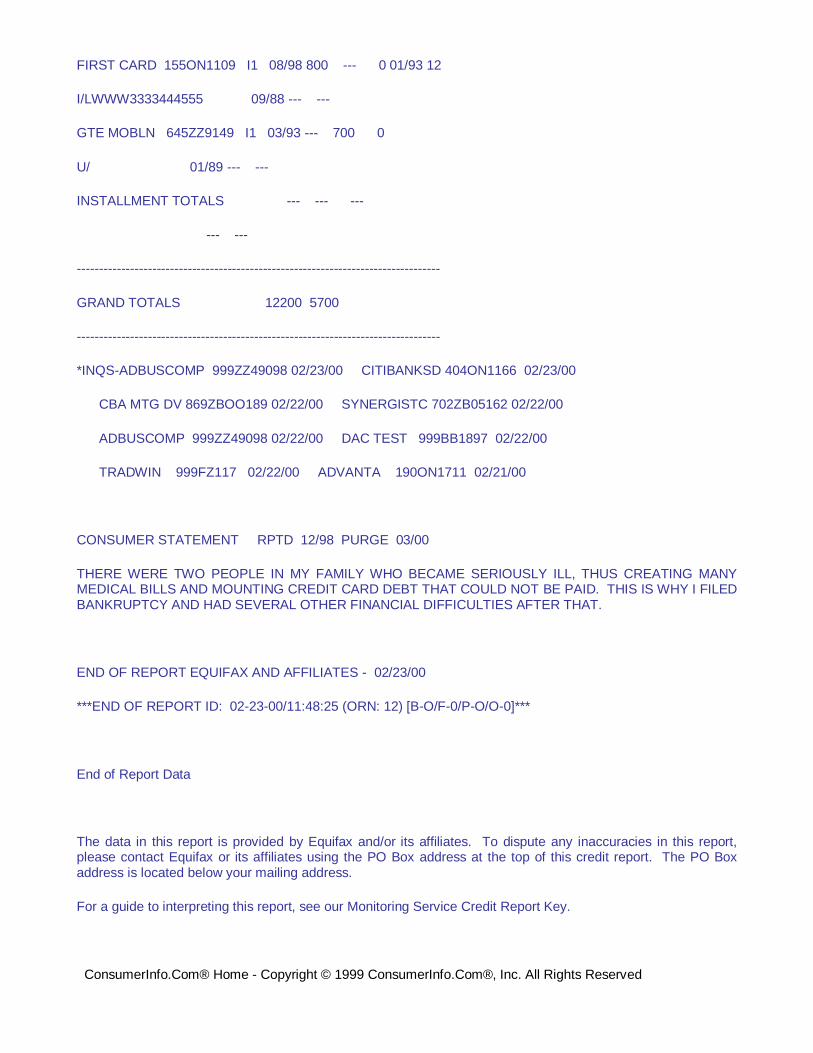
FIRST CARD 155ON1109 I1 08/98 800 --- 0 01/93 12
I/LWWW3333444555 09/88 --- ---
GTE MOBLN 645ZZ9149 I1 03/93 --- 700 0
U/ 01/89 --- ---
INSTALLMENT TOTALS --- --- ---
--- ---
----------------------------------------------------------------------------------
GRAND TOTALS 12200 5700
----------------------------------------------------------------------------------
*INQS-ADBUSCOMP 999ZZ49098 02/23/00 CITIBANKSD 404ON1166 02/23/00
CBA MTG DV 869ZBOO189 02/22/00 SYNERGISTC 702ZB05162 02/22/00
ADBUSCOMP 999ZZ49098 02/22/00 DAC TEST 999BB1897 02/22/00
TRADWIN 999FZ117 02/22/00 ADVANTA 190ON1711 02/21/00
CONSUMER STATEMENT RPTD 12/98 PURGE 03/00
THERE WERE TWO PEOPLE IN MY FAMILY WHO BECAME SERIOUSLY ILL, THUS CREATING MANY MEDICAL BILLS AND MOUNTING CREDIT CARD DEBT THAT COULD NOT BE PAID. THIS IS WHY I FILED BANKRUPTCY AND HAD SEVERAL OTHER FINANCIAL DIFFICULTIES AFTER THAT.
END OF REPORT EQUIFAX AND AFFILIATES - 02/23/00
***END OF REPORT ID: 02-23-00/11:48:25 (ORN: 12) [B-O/F-0/P-O/O-0]***
End of Report Data
The data in this report is provided by Equifax and/or its affiliates. To dispute any inaccuracies in this report, please contact Equifax or its affiliates using the PO Box address at the top of this credit report. The PO Box address is located below your mailing address.
For a guide to interpreting this report, see our Monitoring Service Credit Report Key.
ConsumerInfo.Com® Home - Copyright © 1999 ConsumerInfo.Com®, Inc. All Rights Reserved
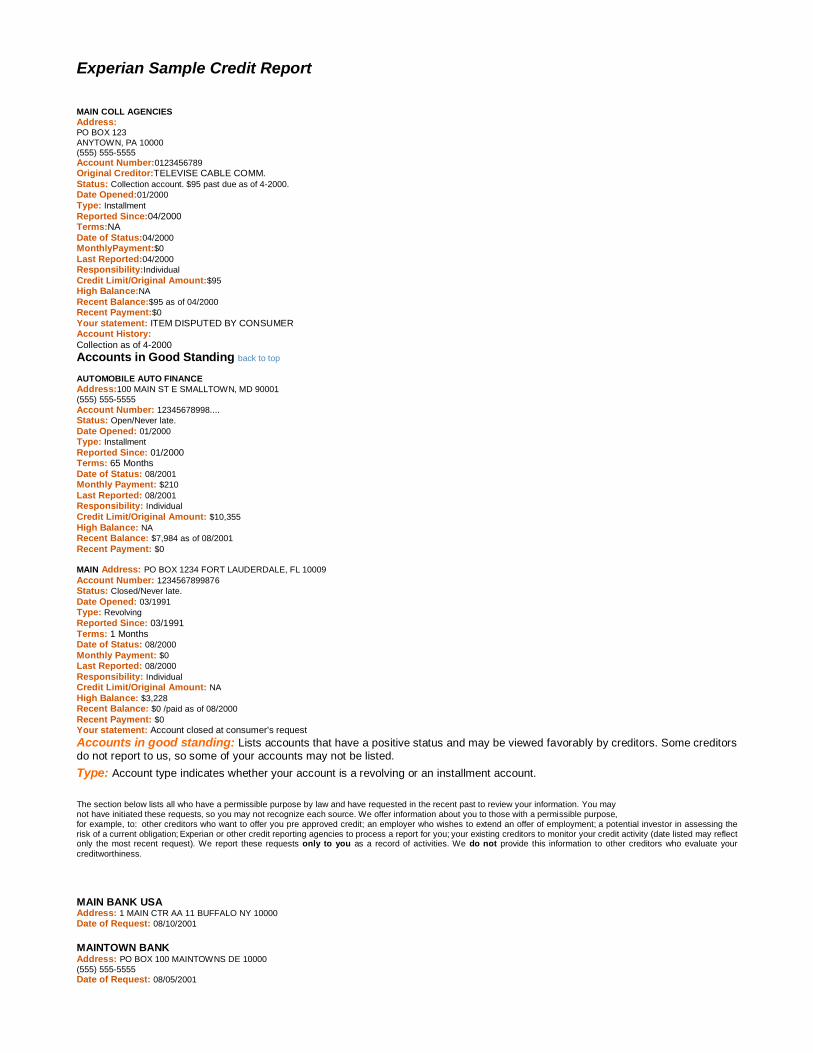
Experian Sample Credit Report
MAIN COLL AGENCIES
Address: PO BOX 123
ANYTOWN, PA 10000 (555) 555-5555
Account Number:0123456789
Original Creditor:TELEVISE CABLE COMM. Status: Collection account. $95 past due as of 4-2000.
Date Opened:01/2000
Type: Installment
Reported Since:04/2000 Terms:NA Date of Status:04/2000
MonthlyPayment:$0
Last Reported:04/2000
Responsibility:Individual
Credit Limit/Original Amount:$95
High Balance:NA
Recent Balance:$95 as of 04/2000
Recent Payment:$0
Your statement: ITEM DISPUTED BY CONSUMER Account History:
Collection as of 4-2000
Accounts in Good Standing back to top
AUTOMOBILE AUTO FINANCE
Address:100 MAIN ST E SMALLTOWN, MD 90001
(555) 555-5555
Account Number: 12345678998....
Status: Open/Never late.
Date Opened: 01/2000
Type: Installment
Reported Since: 01/2000 Terms: 65 Months Date of Status: 08/2001
Monthly Payment: $210
Last Reported: 08/2001
Responsibility: Individual
Credit Limit/Original Amount: $10,355
High Balance: NA
Recent Balance: $7,984 as of 08/2001
Recent Payment: $0
MAIN Address: PO BOX 1234 FORT LAUDERDALE, FL 10009
Account Number: 1234567899876
Status: Closed/Never late.
Date Opened: 03/1991
Type: Revolving
Reported Since: 03/1991 Terms: 1 Months Date of Status: 08/2000
Monthly Payment: $0
Last Reported: 08/2000
Responsibility: Individual
Credit Limit/Original Amount: NA
High Balance: $3,228
Recent Balance: $0 /paid as of 08/2000
Recent Payment: $0
Your statement: Account closed at consumer's request
Accounts in good standing: Lists accounts that have a positive status and may be viewed favorably by creditors. Some creditors do not report to us, so some of your accounts may not be listed.
Type: Account type indicates whether your account is a revolving or an installment account. 6 5 The section below lists all who have a permissible purpose by law and have requested in the recent past to review your information. You may not have initiated these requests, so you may not recognize each source. We offer information about you to those with a permissible purpose, for example, to: other creditors who want to offer you pre approved credit; an employer who wishes to extend an offer of employment; a potential investor in assessing the risk of a current obligation; Experian or other credit reporting agencies to process a report for you; your existing creditors to monitor your credit activity (date listed may reflect only the most recent request). We report these requests only to you as a record of activities. We do not provide this information to other creditors who evaluate your
creditworthiness.
MAIN BANK USA Address: 1 MAIN CTR AA 11 BUFFALO NY 10000
Date of Request: 08/10/2001
MAINTOWN BANK Address: PO BOX 100 MAINTOWNS DE 10000
(555) 555-5555
Date of Request: 08/05/2001
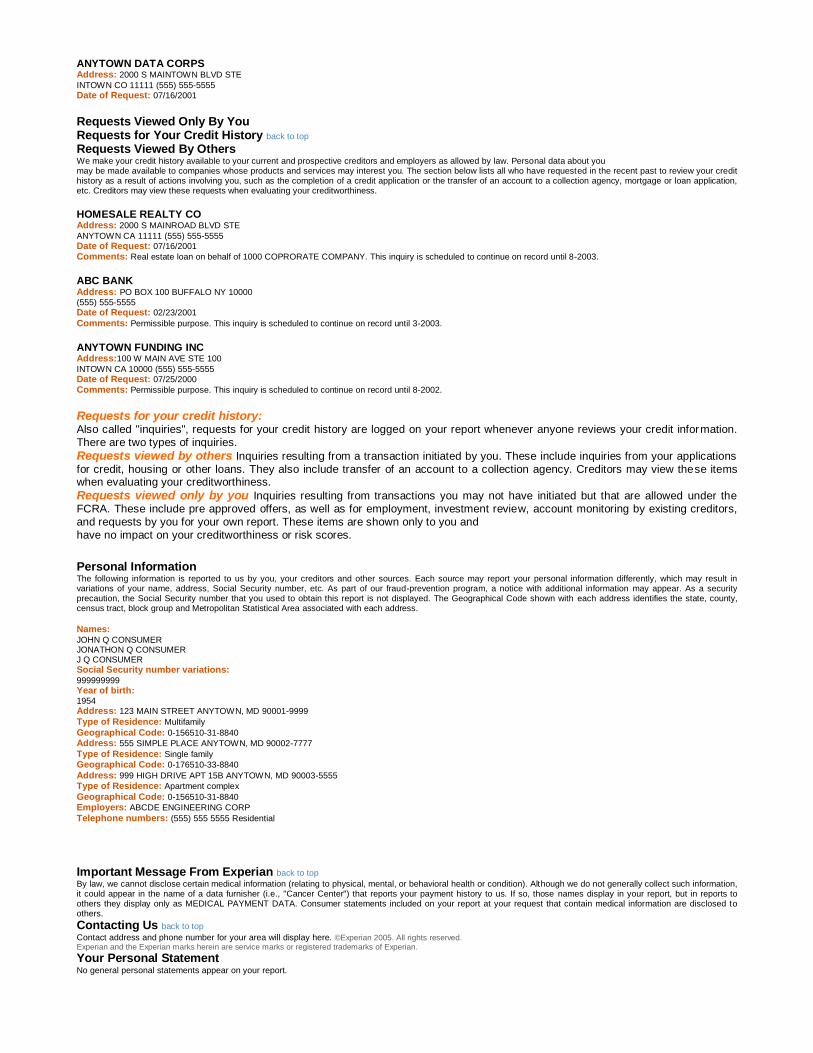
ANYTOWN DATA CORPS Address: 2000 S MAINTOWN BLVD STE
INTOWN CO 11111 (555) 555-5555
Date of Request: 07/16/2001
Requests Viewed Only By You Requests for Your Credit History back to top
Requests Viewed By Others We make your credit history available to your current and prospective creditors and employers as allowed by law. Personal data about you may be made available to companies whose products and services may interest you. The section below lists all who have requested in the recent past to review your credit history as a result of actions involving you, such as the completion of a credit application or the transfer of an account to a collection agency, mortgage or loan application, etc. Creditors may view these requests when evaluating your creditworthiness.
HOMESALE REALTY CO Address: 2000 S MAINROAD BLVD STE
ANYTOWN CA 11111 (555) 555-5555
Date of Request: 07/16/2001
Comments: Real estate loan on behalf of 1000 COPRORATE COMPANY. This inquiry is scheduled to continue on record until 8-2003.
ABC BANK Address: PO BOX 100 BUFFALO NY 10000
(555) 555-5555
Date of Request: 02/23/2001
Comments: Permissible purpose. This inquiry is scheduled to continue on record until 3-2003.
ANYTOWN FUNDING INC Address:100 W MAIN AVE STE 100
INTOWN CA 10000 (555) 555-5555
Date of Request: 07/25/2000
Comments: Permissible purpose. This inquiry is scheduled to continue on record until 8-2002.
Requests for your credit history: Also called "inquiries", requests for your credit history are logged on your report whenever anyone reviews your credit information. There are two types of inquiries.
Requests viewed by others Inquiries resulting from a transaction initiated by you. These include inquiries from your applications
for credit, housing or other loans. They also include transfer of an account to a collection agency. Creditors may view these items when evaluating your creditworthiness.
Requests viewed only by you Inquiries resulting from transactions you may not have initiated but that are allowed under the FCRA. These include pre approved offers, as well as for employment, investment review, account monitoring by existing creditors, and requests by you for your own report. These items are shown only to you and have no impact on your creditworthiness or risk scores.
7
Personal Information The following information is reported to us by you, your creditors and other sources. Each source may report your personal information differently, which may result in variations of your name, address, Social Security number, etc. As part of our fraud-prevention program, a notice with additional information may appear. As a security precaution, the Social Security number that you used to obtain this report is not displayed. The Geographical Code shown with each address identifies the state, county, census tract, block group and Metropolitan Statistical Area associated with each address.
Names: JOHN Q CONSUMER JONATHON Q CONSUMER J Q CONSUMER
Social Security number variations: 999999999
Year of birth: 1954
Address: 123 MAIN STREET ANYTOWN, MD 90001-9999
Type of Residence: Multifamily
Geographical Code: 0-156510-31-8840
Address: 555 SIMPLE PLACE ANYTOWN, MD 90002-7777
Type of Residence: Single family
Geographical Code: 0-176510-33-8840
Address: 999 HIGH DRIVE APT 15B ANYTOWN, MD 90003-5555
Type of Residence: Apartment complex
Geographical Code: 0-156510-31-8840
Employers: ABCDE ENGINEERING CORP
Telephone numbers: (555) 555 5555 Residential
Important Message From Experian back to top
By law, we cannot disclose certain medical information (relating to physical, mental, or behavioral health or condition). Although we do not generally collect such information, it could appear in the name of a data furnisher (i.e., "Cancer Center") that reports your payment history to us. If so, those names display in your report, but in reports to others they display only as MEDICAL PAYMENT DATA. Consumer statements included on your report at your request that contain medical information are disclosed to others.
Contacting Us back to top
Contact address and phone number for your area will display here. ©Experian 2005. All rights reserved. Experian and the Experian marks herein are service marks or registered trademarks of Experian.
Your Personal Statement No general personal statements appear on your report.
10 Personal information: Personal information associated with your history that has been reported to Experian by you, your
creditors and other sources. May include name and Social Security number variations, employers, telephone numbers, etc. Experian lists all variations so you know what is being reported to us as belonging to you.
Address information: Your current address and previous address(es)
Personal statement: Any personal statement that you added to your report appears here.
Note - statements remain as part of the report for 2 years and display to anyone who has permission to review your report.
8
Chapter 4 – HOW TO COLLECT
The Value of Role Playing
Although role-playing is used in many industries, very few people really enjoy role-playing. It makes one nervous, one may feel put on the spot, and often times find the entire process to be embarrassing. Let‘s take a look at role playing from a different perspective and see what benefits one can receive.
A simple definition of role playing is: Pretending to be someone you are not so as to be prepared to handle certain people and situations when they arise. Role-playing is common in a variety of industries. Police officers conduct role-playing exercises to learn how to handle any number of dangerous situations while removed from the actual threat of danger. If, as an officer, you have never experienced handcuffing someone until making your first arrest, you might find yourself wishing you could have practiced a few times in a controlled environment. Police role-playing is an example of the physical aspect of role-playing. However, there is a visual element to role-playing as well. Professional athletes make use of the visual element on a daily basis. Golfers visualize bringing the proper swing club back, the follow through, the ball falling where it is supposed to…and ultimately seeing the ball drop into the hole with one putt. Similarly, football players visualize catching a pass, or tackling the receiver. The accepted theory is, when the time comes and the pressure is on, the athlete will be able to rely on his or her mental preparedness to make the shot, score the touchdown, or whatever the case may be, simply because they were ready for the situation. The concept is ―been there – done that‖, so in the reality of the moment one finds oneself prepared.
Healthcare financial counselors, collectors, registrars, cashiers, and customer service personnel must prepare in the same way. There are practical benefits to role playing for anyone who spends time on the phone or in-person negotiating payments.
For the Collector
One could write a book simply based on the excuses heard from patients, where the patient attempts to explain why they did not follow through with promises to make a payment. Examples of excuses may be: (be careful not to judge too quickly)
―I am only 17, the head of my household because both of my parents were recently killed in an car accident‖
―I would have paid but I had a serious illness and had to pay all my money to the doctor‖
―My wallet was lost‖
―I am not responsible for this bill. I am divorced and my spouse is responsible‖
There often are excuses; however, the excuses are at times, correct and true. In fact, those excuses listed above are all true events the writer has heard. Many other excuses are far-fetched and easy to dismiss; others actually seem legitimate and might even pull at your heartstrings. Knowing how to respond to both false and real/legitimate excuses is critical to
Chapter 4 – HOW TO COLLECT, continued
For the Collector, continued
providing excellent customer service, as well as successfully collecting the debt. Role-playingcan significantly improve the way in which you interact with the person on the other end of the phone, as well as make you more comfortable with the entire process.
When collecting self-pay debt it is critical that, from the moment one picks up the phone, or interacts face-to-face with a debtor, one is prepared and in control. Most likely the patient is in a difficult financial situation, and one will need to know how to navigate through the obstacles he or she throws up as a reason to avoid paying this debt. Role-playing helps make navigation possible. There are several critical skills that one must have mastered before contacting the patient/guarantor, each of which consistently improves the hospital‘s chances of collecting the debt.
Critical Skills to Practice by Role Playing
1) Get comfortable introducing yourself and state from where you are calling. This may sound simple, but doing it properly can be the first thing you forget when the debtor picks up the phone. Scripting may be effective in knowing what to say. For instance – Something like:
- ―This is ___________ calling from XYZ Hospital, may I speak to Mr. Robert Jones?‖
It is important to get familiar with identifying the debtor by his or her first and last name, then simply by the appropriate title followed by their last name. In the example above, ―Mr. Jones‖ should be the way you address him during the remainder of the conversation.
2) Imagine what the patient has recently experienced health wise. Remember, the person you‘re speaking to has most likely recently been a hospital patient; if not, he/she is the guarantor for a patient, for example, a child. The possibility exists that this person might have gone through traumatic circumstances that led to their experience with the hospital. Unless one has been able to view medical records associated with the outstanding debt, one cannot be sure what event made it necessary for this person to seek treatment in your facility. It is quite possible that the person you will be speaking to has more on their mind at the moment than fulfilling their financial obligation to your institution. These facts do not make the debt any less real or important, but should serve as a reminder to the caller that rarely do patients fall into a consistent mold, and one should be prepared to address whatever issues arise.
3) Remember your primary responsibility. While circumstances may be difficult for the debtor you‘re speaking with, be mindful of your objective: collecting the money. Some people will talk to you for an hour if you let them. They will give you their entire life story twice, as well as the life stories of each of their family members. You should be on and off the phone in between three and five minutes, therefore you have to be in control of the conversation. Role-playing can make you more comfortable with saying things like, ―I understand this has been difficult Mr. Jones, but the issue we‘re dealing with today is your financial obligation to the hospital.‖ Stay on issue, and don‘t let up.
Chapter 4 – HOW TO COLLECT, continued
Critical Skills to Practice by Role Playing, continued
4) Control your emotions. As a collector, it is your job to be calmly assertive. The person on the other end of the phone or across the desk might break your heart with their sad stories or curse you for even having the nerve to talk about money at a time like this. Regardless, you must remain composed and unaffected by their response. While one certainly retains the right to end a phone conversation if the debtor becomes irrational, through it all one must handle his or herself with integrity. Role playing not only helps you get accustomed to one of the more difficult parts of collecting, it will also provide you with opportunities to work on overcoming even the most wild objections.
5) Don‘t take ―no‖ for an answer. As we mentioned earlier, debtors will come up with every possible excuse for not making a payment. It is your responsibility to know how to effectively overcome each of their objections, therefore, you must be in the habit of not taking ―no‖ for answer. Use role-playing to learn how to respond in a variety of scenarios, especially when a debtor is trying to stall on making a payment.
Negotiating Skills
To assume that every collection call you make, or every patient/guarantor you deal with, will be identical experiences would be a mistake. Although there are certainly common themes when dealing with debtors, there unfortunately isn‘t a guarantee, ―this works every time‖ plan that you can follow. You have to be prepared to negotiate, and in this case, there are three distinct steps in every negotiation:
1) Clarify the objections. Find out what the debtor wants and know what you want to accomplish. Negotiate with a strong sense of purpose. If your goal is payment in full, negotiate for it. Keep ―payment in full‖ on your mind during the conversation. Don‘t enter the discussion with a ―wishy-washy‖ attitude that says you‘ll take whatever you can get.
2) Gather information about the debtor. Some of the information may not have anything to do with the demands or needs of that person, but it will help you decide what strategy or method you will use. You cannot successfully negotiate with incomplete information, especially as it relates to sources of income and other assets. Review past hospital accounts to gather information about the payment personality of this person before talking with them.
3) Last resort - Reach an agreement or compromise. This is the stage every collector wants to get to, and sometimes too quickly. Stages one and two lay the groundwork for improving the chances of this final step being successful. Be patient as you begin negotiating with the debtor, even if they appear to be rushing you towards the agreement. You want to remain in control, and you will benefit greatly from gathering the necessary information before reaching your ultimate goal.
Chapter 4 – HOW TO COLLECT, continued
Negotiating Skills, continued
In an earlier section you read about the importance role-playing has on handling objections. Now it‘s time to learn how to actually handle them, specifically in the context of negotiation. When collecting, you hear many of the same excuses for not paying - from patients and insurance companies alike. Becoming an expert at handling these objections will lead to improved collection totals, as well as reduce some of the inherent stress of negotiating payments. The following six insights are the basic offenses that should be used when handling objections: Remember ―The best defense is a good offense‖.
1) Don’t argue. You might easily win an argument with a patient/guarantor, but would you get paid in full, probably not? Would you generate a complaint in the process, maybe? The goal is not to win an argument and make a patient feel angry, or helpless, but rather to collect payment in full, all the while maintaining and protecting patient relations.
2) Use intelligence - not emotion. Patients may become emotional when they are talking to you (and as we discussed above, that could mean tears or shouting). You need to express sympathy, but remain calm and logical. Avoid getting emotionally involved in the conversation.
3) Use a professional and businesslike manner. Treat manners seriously. State your facts with authority and assurance. Be friendly, but not too familiar. Stick to business-related matters without alienating patients.
4) Be courteous. Always consider the other person‘s feelings by being polite and practicing good manners. Treat the patient as you would want to be treated or as you would want your family member treated.
5) Be flexible. There is not a set-in-stone method for each collection encounter; therefore your collection approach should change if the situation warrants it. Remember, every patient will respond differently to your requests for payment. You will need to use a variety of motivators.
6) Be natural. Use simple, uncomplicated words and phrases. Avoid technical jargon and acronyms, which will confuse others. If people feel you are talking above them, they will have a difficult time trusting what you are telling them. Your delivery should be unhurried and deliberate.
Remember that good collectors are always in control of the conversation tone and their emotions when negotiating with a debtor or handling their objections. Quality collectors consistently provide patients and insurance companies with logical reasons why payment in full is necessary.
Chapter 4 – HOW TO COLLECT, continued
Collection Tactics
At its very core, quality collection is rooted in motivation. People might very well make a one-time payment just to ―get you off their back‖, or occasional payments in varying amounts simply as a means of keeping you off their back, and do so without any motivation whatsoever. However, to either obtain payment in full or to work a debtor into a consistent payment plan, you must motivate them.
Below are some of the motivators behind people paying their bills:
1) Having a good credit rating
2) Doing the right or fair thing
3) Not having to worry about the bill
4) Feeling good about paying their bills
5) Saving additional collection costs (interest, late charges, etc.)
6) Avoiding further collection action
Additionally, there are many more reasons why people pay their bills. For the most part, these reasons fall into one of three categories of motivators:
1) Pride Motivators
2) Honesty Motivators
3) Fear Motivators
If you understand that most people pay because of pride, honesty, or fear, these become your motivational building blocks - the ultimate tactics in collection. Your motivational phrases, designed to give patients a reason to pay, should be built around pride, honesty and fear.
Pride Motivators deal with the self-respect or reputation of the other person. People are usually proud that they can earn a good living for themselves or their family and pay their bills on time. A good credit rating and payment reputation are also things to be proud of. Examples of patient pride motivators include the following:
- ―It took many years to build such a good credit rating. You don‘t want to jeopardize it on this bill, do you?‖
- ―You‘ve always had an excellent payment reputation here at our hospital. Don‘t you want to clear this up today?‖
Chapter 4 – HOW TO COLLECT, continued
Collection Tactics, continued
Note: If your hospital does not utilize a credit-reporting agency (CRA), AKA credit bureau, you cannot utilize the argument regarding ―protecting ones credit rating.‖ If your hospital does utilize a CRA, do not threaten placement of the account with the agency unless that is your full intention. Such an accusation without the intent to follow through may be viewed as harassment and may subject the hospital to unwanted litigation and bad press. Read and understand the Fair Debt Collection Practices Act (FDCPA) to fully understand the implications of your hospital‘s policies if they support the type of collection tactics mentioned above. Examples of using pride motivators with insurance companies include:
- ―Your company has a great payment record with us. I‘m surprised to have this bill outstanding.‖
- ―Isn‘t your reputation as a good payer important to you?‖
Honesty motivators consider people‘s natural reaction to do what‘s right. Most people want to be known as someone who pays bills on time and is fair with others. Patients who received good care from your facility generally know it is only right to pay you in full. Honesty motivators are built around this sense of fair play. Examples of patient honesty motivators include the following:
- ―Do you believe it‘s fair to shortchange the hospital after we gave you our best care?‖
- ―Won‘t you feel better once this bill is off your conscience?‖
Examples of using honesty motivators with insurance companies include:
- ―The patient pays your premium on time. Isn‘t it fair to pay this bill on time too?‖
- ―We‘ve provided you with all the necessary information in a timely fashion. Don‘t you think it‘s only right to pay us now?‖
Fear motivators can be designed around anything that threatens the other person‘s well being. This could be the fear of loss of reputation, loss of future services at your facility, or loss of respect. Many patients fear further collection activity or loss of their good credit rating. Examples of patient fear motivators include the following:
- ―Legal action is expensive, but may be necessary if your promise is not kept. You don‘t want that, do you?‖
- ―Credit is a valuable asset. You don‘t want to risk it on an unpaid bill, do you?‖
Note: See note above in reference to FDCPA.
Chapter 4 – HOW TO COLLECT, continued
Collection Tactics, continued
Examples of using fear motivators with insurance companies include:
- ―If we don‘t get payment from you soon, I have no choice but to contact your subscriber for payment.‖
- ―The insurance commissioner requires payment of a clean claim in 30 days. If you can clear payment today, we won‘t notify them of your delinquency.‖
Sometimes collectors make the mistake of using only fear motivators in their collection strategy. This can lead to many complaints and possibly lost customers. Your collection approach should always start with pride and honesty motivators, because these are positive reasons for paying. Starting with these motivators sets a positive theme early in the call.
If pride and honesty motivators do not work, and one has to use fear motivators, patients will be in a better frame of mind if they‘ve already heard the positives. When one begins with fear motivators, one may create a defensive attitude, and the patient will resist even if you later present the positive pride and honesty motivations for paying.
But wait…what’s in it for me?
As a culture, we like to know what we‘re getting for our cooperation, simply put, ―what‘s in it for me (WIFM)?‖ We‘re all like this in certain ways and it is crucial that you remember this key element of people‘s psyche. Here is how it could work:
Patient objection: ―I‘ve always waited until my insurance pays. Why do you need me to pay my part now?‖
Collection approach without “what’s in it for me” concept: ―It is our policy to collect the patient liability at the time of service. We need you to pay now.‖
Collection approach with WIFM: ―You‘re right; you‘ve always had an excellent payment record with us. But many of our patients have asked us what their responsibility is up front, so they can take care of it right away, and not have to worry about it. We‘ve started this program as a courtesy to our patients.‖
Which approach will get a better response? Without WIFM, the collector uses words like ―our policy‖ and ―we need.‖ These types of words generally make people angry; basically, your patients don‘t care what you need.
Chapter 4 – HOW TO COLLECT, continued
But wait…what’s in it for me?, continued
WIFM is about giving patients what they need, which in this case is a reason to pay. People are motivated only when they have a reason to do something, and those reasons must be good for them - not you. It is critical as a collector to avoid reasons that sound like ―because I said so.‖ No one responds well to that, and even if the outcome is what you want, the end result could be far more detrimental. Phrases like that actually tend to de-motivate (a brief list is provided at the end of this chapter of de-motivational phrases). Here are some examples of specific motivational phrases you can use that give others solid reasons for others to pay:
Reason Motivational Phrase
Self-respect This account is already past due. I know you‘re an honest person and, since this is a legitimate debt, you will pay it in full today.
Freedom from worry Pay the whole balance now and you won‘t have to worry about it anymore.
Fair play We gave you our best service when you needed it. Paying off the balance is the only fair thing to do.
Doing the right thing This account is seriously delinquent. Don‘t you think it‘s time to do the right thing and pay what you owe?
Freedom to buy on credit A good payment reputation ensures that you‘ll have credit available when you need it.
Saving additional expense Paying in full now will keep you from possible expense later.
Security of family You owe it to your family to maintain good credit.
You may not feel comfortable using all of these motivational phrases. If you‘re not comfortable with them, you probably won‘t use them effectively when collecting. It‘s important that you at least try each of the phrases and practice using them effectively. However, if after practice, there is one or two you simply can‘t get comfortable with, don‘t use it. Find other motivational phrases that come more naturally to you.
Chapter 4 – HOW TO COLLECT, continued
But wait…what’s in it for me?, continued
De-motivational phrases:
1) You need to…
2) I need…
3) You must…
4) We require…
5) I want you to…
6) You have to…
7) I expect…
8) Our policy states
Motivational phrases: 1) Here are some options for you… 2) What can you do? 3) May I suggest…
4) You might want to try… 5) Did you know you can… 6) Will it help if…
Chapter 5 – FINANCIAL ASSISTANCE PROGRAMS
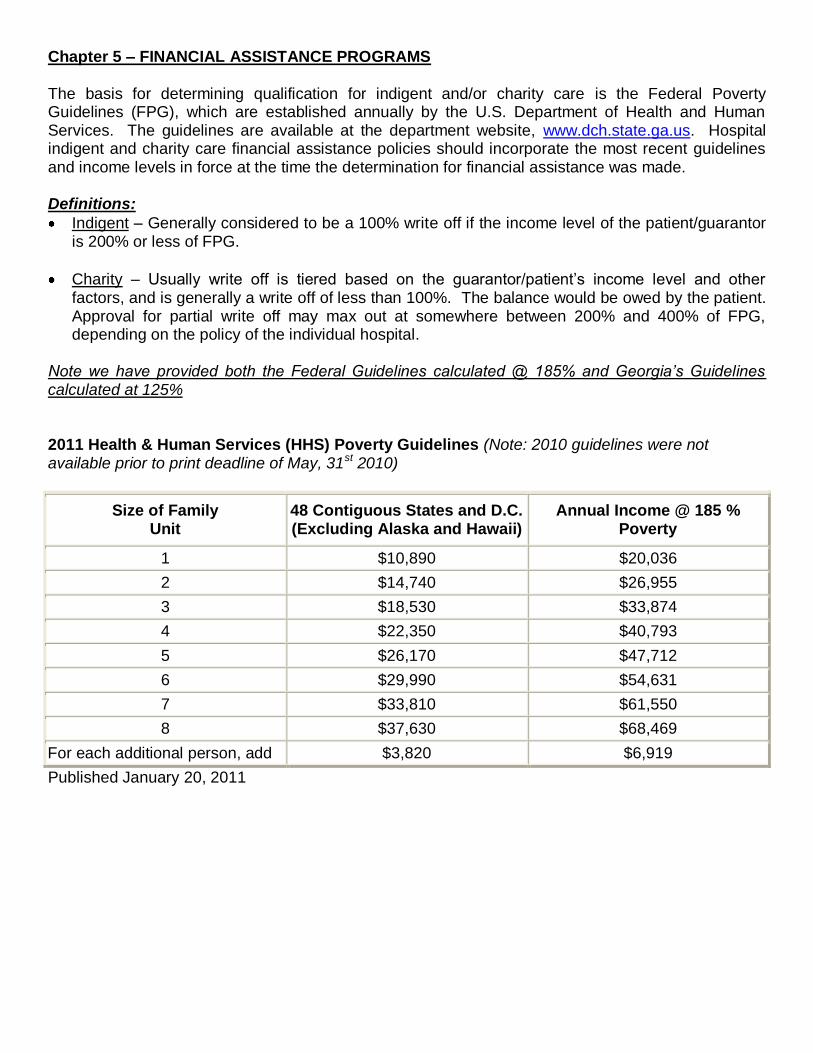
The basis for determining qualification for indigent and/or charity care is the Federal Poverty Guidelines (FPG), which are established annually by the U.S. Department of Health and Human Services. The guidelines are available at the department website, www.dch.state.ga.us. Hospital indigent and charity care financial assistance policies should incorporate the most recent guidelines and income levels in force at the time the determination for financial assistance was made. Definitions:
Indigent – Generally considered to be a 100% write off if the income level of the patient/guarantor is 200% or less of FPG.
Charity – Usually write off is tiered based on the guarantor/patient‘s income level and other factors, and is generally a write off of less than 100%. The balance would be owed by the patient. Approval for partial write off may max out at somewhere between 200% and 400% of FPG, depending on the policy of the individual hospital.
Note we have provided both the Federal Guidelines calculated @ 185% and Georgia’s Guidelines calculated at 125%
2011 Health & Human Services (HHS) Poverty Guidelines (Note: 2010 guidelines were not available prior to print deadline of May, 31st 2010)
Size of Family Unit
48 Contiguous States and D.C. (Excluding Alaska and Hawaii)
Annual Income @ 185 % Poverty
1 $10,890 $20,036
2 $14,740 $26,955
3 $18,530 $33,874
4 $22,350 $40,793
5 $26,170 $47,712
6 $29,990 $54,631
7 $33,810 $61,550
8 $37,630 $68,469
For each additional person, add $3,820 $6,919
Published January 20, 2011
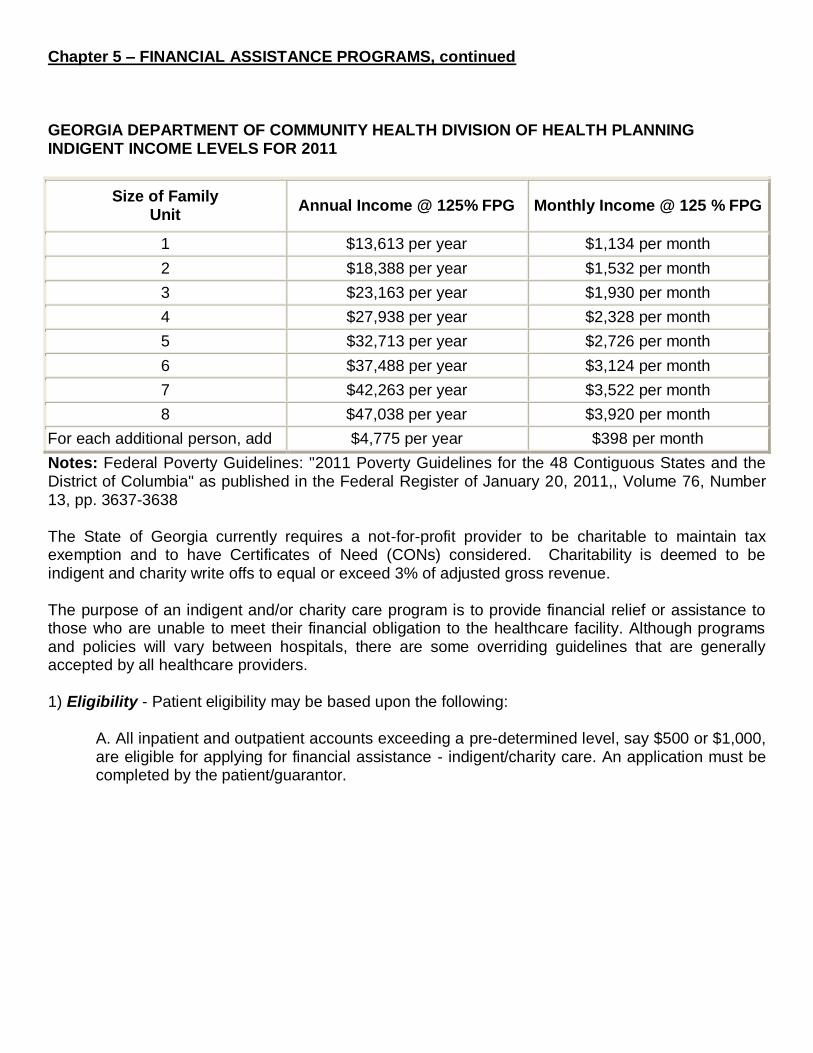
Chapter 5 – FINANCIAL ASSISTANCE PROGRAMS, continued
GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF HEALTH PLANNING INDIGENT INCOME LEVELS FOR 2011
Size of Family Unit
Annual Income @ 125% FPG Monthly Income @ 125 % FPG
1 $13,613 per year $1,134 per month
2 $18,388 per year $1,532 per month
3 $23,163 per year $1,930 per month
4 $27,938 per year $2,328 per month
5 $32,713 per year $2,726 per month
6 $37,488 per year $3,124 per month
7 $42,263 per year $3,522 per month
8 $47,038 per year $3,920 per month
For each additional person, add $4,775 per year $398 per month
Notes: Federal Poverty Guidelines: "2011 Poverty Guidelines for the 48 Contiguous States and the District of Columbia" as published in the Federal Register of January 20, 2011,, Volume 76, Number 13, pp. 3637-3638 The State of Georgia currently requires a not-for-profit provider to be charitable to maintain tax exemption and to have Certificates of Need (CONs) considered. Charitability is deemed to be indigent and charity write offs to equal or exceed 3% of adjusted gross revenue. The purpose of an indigent and/or charity care program is to provide financial relief or assistance to those who are unable to meet their financial obligation to the healthcare facility. Although programs and policies will vary between hospitals, there are some overriding guidelines that are generally accepted by all healthcare providers. 1) Eligibility - Patient eligibility may be based upon the following:
A. All inpatient and outpatient accounts exceeding a pre-determined level, say $500 or $1,000, are eligible for applying for financial assistance - indigent/charity care. An application must be completed by the patient/guarantor.
Chapter 5 – FINANCIAL ASSISTANCE PROGRAMS, continued
B. The application should include:
Income from all sources, listing, at a minimum, gross income for the most recent three-month period. Some providers may require additional documentation such as W2 for prior year.
Resources from savings and checking accounts, certificates of deposit, stocks, bonds, real estate, etc
Assets including homes, cars, boats, and any other vehicles, or assets
Monthly expenses
Number of dependents
A copy of the most recent federal income tax forms C. All third-party resources and non-hospital financial aid programs, including public assistance available through Medicaid, must be exhausted before financial assistance can be approved. D. Deductible and coinsurance amounts may be eligible for assistance if financial circumstances warrant. E. Some hospitals do not allow financial assistance applications after an account has been sent to legal counsel for collection.
2) Program Administration - The financial assistance (indigent/charity) program should be administered according to the following guidelines:
A. The application information, along with the federal income tax forms, should be reviewed and verified by a Financial Counselor or authorized person B. After reviewing income and expenses, the Financial Counselor or authorized person should determine if the patient/guarantor qualifies for financial assistance based on an Income and Assets Guideline Worksheet. A specific worksheet for use by Financial Counselors will ensure that all patients are assessed using the same criteria and represents a best practice
If the patient/guarantor qualifies for 100 percent write-off, he or she should be notified and the balance of the account should be written off per the facility‘s procedures
If the patient/guarantor qualifies for a reduction in liability, he or she should be notified and payment arrangements made for the non-write-off amount. Best practice dictates that the out of pocket payment should be received prior to the charity write-off on the account
C. Falsification of any information on the financial assistance application or refusal to cooperate should result in denial of financial assistance approval. For example, refusal to provide income documents or lack of cooperation to apply for Medicaid should disqualify a patient from receiving financial assistance. D. The healthcare facility‘s policy should reserve the right to change benefit determination if financial circumstances change.
Chapter 5 – FINANCIAL ASSISTANCE PROGRAMS, continued
3) Procedure - The financial assistance program should follow certain procedures:
A. Applicants for financial assistance should complete a financial information form. The healthcare facility should reserve the right to check the validity of the information at their discretion, including accessing credit bureau reports. B. A determination of eligibility should be made within a reasonable, pre-determined period, usually within seven to ten business days; and the patient should be informed in writing of that determination by a copy of the application or a formal approval letter sent within the stated period of time. C. Family size should be determined primarily by the information supplied on the federal income tax return. Income will include all income of the family unit. D. Best practice dictates that the patient/guarantor complete the financial assistance application prior to or at the time the service is given. Required documentation for validating the information may be delayed since most people do not routinely carry these documents with them. A time limit for receipt of the documents should be communicated to the patient. E. Each facility‘s policy should determine who has final approval of determination of eligibility, based on dollar amount of write-off, type of service, documents provided, etc. Some facilities allow the Financial Counselor full approval rights if all documentation is provided. Others require management approval. F. While the application for financial assistance consideration should be made by the time of service, payment from all other sources must be received and the patient must have been denied Medicaid, or otherwise be known not to qualify for Medicaid, before the financial assistance is approved and the indigent/charity allowance is applied to an account. G. Some organizations include all outstanding accounts when financial assistance has been approved. Others require that the patient/guarantor specify the accounts that he or she would like included for consideration. Whichever, the facility‘s policy should clearly indicate the specifics for the Financial Counselor. H. Each application should be considered effective for the calendar month in which it was made. Should a patient have services later in the month for which he or she wants consideration, best practice does not require an additional application, but the patient must notify a Financial Counselor that he or she desires the additional services be included in the original consideration. Some providers may allow an extension of eligibility beyond one month, to even three or six months depending on the hospital‘s approved policy. I. Medicare allows indigent and charity allowances for Medicare patients‘ deductibles and co-insurance amounts following the same policy as other patients. Clear documentation must be kept for Medicare auditing purposes. J. Lastly, documents should be retained for the required seven years.
Chapter 5 – FINANCIAL ASSISTANCE PROGRAMS, continued
Screening for Financial Assistance Needs
Uninsured Patient The Financial Counselor should be responsible for determining a self-pay inpatient or outpatient‘s eligibility for financial assistance or his or her ability to pay based on the hospital‘s indigent and charity care policy. In some cases, eligibility is readily apparent and a determination can be made before, on, or soon after the date of service. In other cases, it can take investigation to determine eligibility, particularly when the patient has limited ability or an unwillingness to provide necessary information. The Financial Counselor should execute the following steps in order to determine a patient‘s eligibility for financial assistance: 1) Receive a daily report or review an automated work list that lists the admissions, preadmissions, and outpatient surgeries registered or scheduled the previous day 2) Upon review of the daily report, initiate counseling - which should include pre-screening for financial assistance (indigent or charity care), or payment arrangements 3) If it is determined through the financial assistance pre-screening process that the patient is eligible for assistance, the specific procedures for that facility should be followed. Some best practices were listed earlier in this section 4) In the event that a patient does not qualify for financial assistance (uncompensated care), the same financial application should be used to determine a payment plan that is agreeable to the patient and the Financial Counselor 5) If there is insufficient information to fully evaluate all the criteria and the ability to pay cannot be reliably determined, the case should be reviewed by a designated management person in the organization Medicare Patients Medicare patients who have no supplemental insurance should be pre-screened for payment arrangements, or possible financial assistance. The same procedures outlined for self-pay patients should be used for Medicare patients. Because most Medicare patients have a static income level, many hospitals only require Medicare patients to complete financial assistance applications annually.
Chapter 5 – FINANCIAL ASSISTANCE PROGRAMS, continued Patients with Self Pay Balances After Insurance Through the insurance verification process, patients will be identified who have large patient co-pays or terminated benefits. The Insurance Verification Specialist normally will determine which accounts should be forwarded to the Financial Counselor for follow-up. Determining factors include, but are not limited to, service not covered, medical necessity denial, termination of benefits, size of co-pay/deductible (typically greater than $500 or $750), and preexisting condition. All inpatient accounts should be forwarded immediately to the Financial Counselor and the same procedures outlined for self-pay patients should be utilized. It is important that Financial Counselors document all conversations and decisions made during their process.
Communication of Financial Assistance Policies
It is critical that hospitals clearly communicate financial assistance policies to patients. The communication must be delivered in a way that the patient understands the program, how to access it, and who to go to for questions. Hospitals throughout Georgia and the U.S. communicate these policies in many ways. Some examples are:
Given upon request by patient
Included on billing statements
Provided by Financial Counselors
Included on information provided at point of registration
Posted on hospital‘s web site
Included on Financial Counselor‘s voice mail message
Posted on signage in the registration areas
Newspaper advertisements
A best practice would include all of these types of communications.
Chapter 6 - Payment Plans
Why Are Payment Plans Necessary? Payment plans would not be necessary if insurance payments and contractual allowances were sufficient to fully resolve all medical expenses, but they are not. There are a plethora of reasons why payment plans are necessary. The Financial Counselor should know the reasons which include, but are not limited to:
At the time of this printing there are reported to be nearly 46 million Americans who are uninsured
Millions more are underinsured, only having small private policies, cancer policies, or discount cards, which are either not assignable to the hospital, which cover only limited services or which are not accepted by all providers
Many insured persons are now selecting large/high deductible plans which reduce their month to month premium expenses, but significantly increase their out of pocket amount
Most others, those who do have some third party coverage, frequently owe some out of pocket amount for co-payments, co-insurance and/or deductibles
Some who are well insured may have a service performed which is not a covered insurance benefit. In other words, the service is not covered
Some claims may be ―covered by insurance‖, but may not be paid due to a technicality, in which case, depending on contract language, the patient may owe a portion of or the entire bill
Collection Steps Leading Up to Payment Plans Please refer to Chapter 11 which deals with sources of payment, primary insurance, secondary and even tertiary insurance, alternative payer sources, and collection at time of service. Considerable resources should be expended to collect all or most of the amount due for the claim via any source other than the patient. If there is no third party coverage, or if out-of-pocket amounts do exist after insurance is verified, the recommended steps which a Financial Counselor may consider are:
If self pay patients are pre-registered/pre-admitted, discuss payment options at that time and encourage the patient to bring payment with them.
Much effort should be given to collect the patient portion at the time of service. In some organizations it may not be practical to expect that 100% of all out-of-pocket amounts will be collected at the time of service, however, this is a best practice. Some organizations may not even allow or support collection at time of service.
If the patient portion cannot be collected in full at the time of service, collect as much as possible of the amount due and attempt to set up a Payment Plan for the balance.
Chapter 6 - Payment Plans, continued Payment Plan Policy Hospital size, profitability, administrative strategy, customer service initiatives, community politics, and other factors influence the options a hospital or other healthcare entity may employ in the setting up of Payment Plans. The CFC Study Guide is simply a guide, an iteration of common practices utilized in hospitals throughout Georgia. If you as a Financial Counselor participate in policy development, here are a few considerations before establishing a policy or modifying an existing Payment Plan Policy. If you do not actively participate in the process, you may still discuss your opinions with those who do, thus influencing the outcome.
Does your facility have a Payment Plan Policy? If not, it is suggested that one be developed.
If you have an existing Payment Plan Policy, how old is it? If the policy is in excess of two (2) years old, it is suggested that the policy be reviewed and updated.
Research community, State and Federal Government laws, regulations and proposed legislation prior to beginning the new policy or revisions of the existing policy.
The hospital‘s discount policy should be tied to the Payment Plan Policy. Prompt payment discounts, if sufficient enough, can create a desire on the patient‘s part to resolve the account on the date of service, thus eliminating the need to set up a payment plan.
Current community and government initiatives are under way to recommend, if not eventually legislate the discounts healthcare organizations offer their patient population. Carefully weigh your decision after researching the subject thoroughly.
Decisions Which Must be Made Prior to Policy Development
Will the organization charge interest or not?
If the organization does plan on charging interest, research or obtain consulting assistance (due diligence) regarding the organizations fiduciary (legal) responsibility to provide ―full disclosure‖ to anyone taking advantage of payment plans which impose an interest obligation.
If the organization does plan on charging interest, can your computer system handle the application of the additional fees?
The legacy system (primary computer and software) must also be able to manage the monitoring of expected payments, notification to the patient when a payment is missed, notification to the patient when they fall behind in their payment obligation by making only partial payments, a tickler file to trigger a collector to mail a letter, mail a notice, or make a phone call when payments are short or late, and be able to automatically close the account to bad debt once a claim defaults.
If the computer is not sophisticated enough to handle the issues just listed, one must perform all of the mentioned duties manually. If your organization must add resources to manage the payment plans, ―Is the juice worth the squeeze?‖ Is there enough benefit from the payments to offset the increased expenses?
What will the minimum payment be set at?
What will the maximum amount of time given be to pay the debt?
Chapter 6 - Payment Plans, continued
What repercussions to the patient will there be for partial, late, or missing payments?
If the computer cannot assist and manual management is not cost effective, then will the organization outsource the payment plan accounts?
Will the organization sell their private pay receivables?
Will the organization develop a credit card or loan program and request patients to go that route for Payment Plans?
Loan Programs/Medical Credit Cards Loan Programs have been utilized in healthcare for years; however, they have not been widely utilized and have not gained much ground in popularity until recently. There are several companies who are beginning to express an expanding interest in loan programs which extend payments for self pay patients with large accounts. There are other companies, such as venture capitalists, attorneys, etc, which traditionally have had no interest in entering the patient loan business, who are now offering various loan opportunities. Many of the current loan/credit card offerings require an assessment of the patient‘s ability to pay, which may include a review of the patients credit file. A review of the file is permissible due to the doctrine of ―permissible purpose‖. Not all money lenders require a ―needs assessment‖ as described. There are a number of companies who can assist with software which will automatically provide credit file information at the time of service. Other lenders may only require a patients ―good faith‖ upfront payment and proof of ability to pay the loan via some verifiable income stream, or some variation thereof. There is one thing in common with most companies willing to loan money for an existing account or extend credit for future visits to a healthcare facility. Most of these companies require ―full recourse‖, which means if the patient defaults, the hospital buys back the loan. Here are several very important questions and issues to consider before obligating your organization to participate in a Medical Credit Card or Patient Loan Program:
Whose responsibility is it to run the program – the vendor partner or the hospital?
If the vendor partner states that they are responsible have them specify what level of involvement is required of hospital staff.
If the hospital is large enough, will the vendor partner place staff at the hospital?
What fees are due to the vendor partner or the financing partner if different than the primary contracting agent? How are the fees remitted?
May the patient use the extension of credit or credit card for future visits or just the current services?
May the credit card be used for physicians and hospitals? How about the gift shop (not)?
What limits on the loan amount will be in place?
Does the company require full recourse upon default?
Define ―Late‖ payment and ―Default‖
What is the company‘s track record for other clients regarding percent of accounts requiring recourse?
Chapter 6 - Payment Plans, continued Loan Programs/Medical Credit Cards,continued
Check references
Who is responsible for contacting the patient if a payment is missed?
What is the interest rate paid to the lending agency?
Does the hospital wish to offer discounts sufficient to offset the interest?
What collection tactics are used by the lending agency?
How are partial payments handled?
Does the hospital buy back principal and interest?
Are there other fees, known or hidden, the hospital will be required to pay?
Factoring Factoring (selling accounts receivable, especially self pay) has been utilized in healthcare for years; however, like loan programs and credit cards, factoring has not been widely utilized and has not gained much ground, although the number of vendors offering such programs is significantly increasing. Factoring, or ―selling your paper‖ as attorneys like to refer to the practice, is literally selling ones accounts receivable to a third party. The accounts are written off at the hospital and the third party will then perform all collection activity. Companies offering to purchase a hospital‘s accounts receivable will obviously not offer full value. Depending on the age of the account, the financial class of the account, and the pre-determined estimation of the collectibility of the accounts, the purchasing agent will typically only offer pennies on the dollar for aged self pay, up to perhaps 50% or more for fully insured accounts. Questions and Issues to consider before agreeing to any Factoring partnership
Does the hospital wish to lose control of the accounts?
What effect will losing control have on customer service and public perception?
Will the organization be prepared to ―buy back‖ an account when the patient complains about mistreatment during the collection cycle?
What is the time value of money? Do I want 50% now or 60% in 60 days?
If my organization sells its A/R, can staff levels be adjusted down to match the reduced work load?
Contract Terms to Consider if Factoring is Being Considered Since your organization will lose control over the collection methods used in the collection of a ―sold‖ account, it is imperative to enter into an agreement with certain provisions, which will allow some degree of flexibility and control. Following are some contract terms which one might consider in a ―Factoring‖ agreement:
Insist on a 60-90 day termination clause, with or without cause
Pay special attention to the ―Indemnity‖ and ―Limitation of Liability‖ language to make sure your organization is very protected
Chapter 6 - Payment Plans, continued Contract Terms to Consider if Factoring is Being Considered, continued
A Business Associates Agreement is mandatory – preferably in your language, not theirs
HIPAA – HIPAA – HIPAA
No long term, self renewing contracts, unless there is a provision for written notification from the vendor to the provider, certified, response required, indicating that the term is ending in 90 days and renegotiations or termination must be consummated by a specific date
Do Due Diligence – think twice about the ramifications of taking the Factoring claims resolution avenue
Financial Counselors and Payment Plans are inseparable. Just remember that your primary goal is to assure the ultimate and earliest settlement/collection of the account. Payment plans should be the last resource for collection of the account, nevertheless, a very important component in the control of cash flow and Account Receivable.
Chapter 7 - DISCOUNTS Discounts for Uninsured Patients Many providers in Georgia and throughout the United States now have policies that offer discounts to uninsured patients. A few providers offer a flat discount off charges to all uninsured patients and others offer a ―prompt pay discount‖ incentive for paying at time of service or within timeframes after discharge. Examples of known discounting procedures in Georgia include:
5 to 40% flat percentage discount on any uninsured account
5 to 50% percentage discount for payment prior to or at time of service
5 to 50% percentage discount up to 30 days
5 to 20% percentage discount up after 30, 60, and 90 days. Usually the discount percentage reduces as the account ages
Prompt Pay Discounts have several benefits for hospitals. It has been clearly documented that providers will receive more patient payments at the time of service when discounts are offered. Not only will discounting increase collections, it should also reduce time spent on collection follow-up. In today‘s economy, consumers are looking for a good deal, and discounts may tone down negative perceptions regarding high medical costs. Discounting may motivate a patient who normally does not pay until the last minute. Some predict that discounts will eventually be mandated by State and Federal law. Public perceptions and government scrutiny demand that all providers review their discount policy and modify it for the private pay/uninsured population. HFMA supports this view. In addition, HFMA does not promote the discounting of co-payments and deductibles for the insured population. A document outlining some issues to consider when developing indigent and charity care guidelines and policies for offering discounts was developed by representatives of the hospital industry in Georgia in 2005. This document discusses overall principles, financial policies, and patient communication issues relative to indigent and charity care guidelines. Providers may wish to consider these points as they develop or revise their own guidelines. These guidelines include:
Overall Principles
Review their mission statements and decide how to best communicate their commitment to addressing their community‘s healthcare needs.
Engage the hospital board in developing and reviewing charity care and financial aid policies. The board can be particularly helpful in identifying community needs for financial assistance and can represent the hospital‘s policy and charitable support to appropriate community representatives.
Determine how frequently the indigent and charity care guidelines should be reviewed for possible updates.
Seek opportunities to work with government agencies, payers, businesses, consumer groups and others to address the underlying problems that lead to inadequate coverage for citizens.
Chapter 7 – DISCOUNTS, continued
Overall Principles, continued
Check with legal counsel to ensure that the hospital‘s indigent and charity care guidelines meet all federal and state requirements.
Financial Policies
Set targets for the amount of uncompensated care the hospital will attempt to provide after assessing the hospital‘s capability to provide such care.
Decide which staff should oversee implementation of the indigent and charity care guidelines.
Determine the most effective way to assist patients in obtaining insurance coverage from public and private sources including:
Medicaid
Peach Care
Medicare
Other programs for low-income patients
Develop their own policies regarding indigent and charity care and/or discounts that take into account an individual patient‘s ability to pay for the cost of his or her care. These guidelines may factor in:
Patient eligibility for other public or private coverage
Income eligibility threshold based on family size (percentage of Federal Poverty Guidelines, etc.)
Consideration of other resources available to a patient or responsible party
Patient or responsible party‘s employment status and earning capacity
Consider how to handle patients that are medically indigent or have had a catastrophic illness or injury
Other financial obligations of the patient or responsible party
Other sources of funds available to the hospital such as endowments or donations specified for charity care
Consider whether the indigent and charity care/financial aid policy applies only to patients from certain hospital service areas and, if so, defining those areas.
Consider the following when developing your hospital‘s plan:
Accepting all individuals for emergency medical screening and stabilization (within the hospital‘s scope of services and capabilities) regardless of the patient‘s ability to pay
Ensuring that emergency screening and stabilizing treatment is not delayed or denied pending determination of coverage or requirement for prepayment or deposit
Defining the type and scope of essential services eligible for financial aid, including hospital-employed physician fees.
Developing procedures for documenting whether financial counseling was offered and/or provided when appropriate
Informing patients about reapplying for financial assistance before, during or after care if their situation changes
Chapter 7 – DISCOUNTS, continued Financial Policies, continued
Defining acceptable documentation for income verification (e.g., personal statements of no income, letters of support, pay stubs, tax returns, rental papers, etc.)
Determining which personal assets and amount of assets that will be considered in determining eligibility for financial assistance
Incorporating flexible payment plans as appropriate
Training staff how to respond to inquiries about indigent/charity care and discounts
Requiring hospital personnel to treat all information collected as strictly confidential and to only release information consistent with applicable legal requirements
Implementing the policies impartially and consistently
Utilizing outside credit agencies
Providing credit rating checks
Providing credit counseling to patients
Clearly define discount policies:
Documenting that different discount scales may apply to different categories of services (e.g., ambulatory care, clinics, etc.)
Determine how discounts will based (i.e., relative to fixed standards such as Medicare, Medicaid or other rates, or as a percentage of charges)
Develop debt collection policies that reflect the hospital‘s mission statement and values for both hospital staff and external collections companies and which address the following:
Collection from an insurer or payment arrangements for the person who is responsible for the payment of the care rendered
Clear procedure for determining trigger points for sending a debt to collection and legal action
Collection policies that are consistent with the patient‘s ability to pay (e.g., recognizing that those at the very lowest level of Federal Poverty Level percentages are generally least able to cover their costs)
Appropriate monitoring mechanisms, especially for external debt collection organizations
Chapter 7 – DISCOUNTS, continued Patient Communication
Check that patient-oriented material is written in a clear and understandable manner and is presented in a manner that preserves the patient‘s dignity. Also make sure that it is accurate and written in languages appropriate for the major population groups served.
Determine policies regarding how the indigent and charity care guidelines and the process for applying for assistance will be made available to current and prospective patients at the time of service. Possibilities include:
Posting in key public areas
Information included with hospital bills
Counsel patients in advance of service, if appropriate, about their expected financial responsibilities and their duty to complete eligibility documentation
Inform patients that they will receive a hospital bill which includes full charges. They may pursue the hospital‘s financial aid assistance program when they provide the required financial information.
Include assurances to patients that all information collected to determine eligibility for financial assistance will be held in confidence, consistent with the requirements of applicable laws.
Discounts to Clear up Old Accounts Sometimes discounts are offered to patients or insurance companies to motivate them to clear up old accounts. Patients who have been making small monthly payments may pay in full if they can save a little money. Some hospitals allow collection agencies and other outsourced vendors to utilize special discount tactics to increase collections at times during the year. For example, a ―Valentines Day Special‖, ―End-of-the Year Special‖, or ―Christmas Offer‖ may be presented to all old accounts for immediate settlement. Others review long-term payment plan accounts and sometimes offer an early payout discount. Creativity works and is a win-win for the patient/guarantor and the hospital or other provider. Please stay within the parameters allowed by hospital policy and the law when offering discounts. Note: Non-Employment Retirement Income Security Act (ERISA) insurance plans are governed by Georgia‘s Prompt Pay Law, and have a legal obligation to pay timely. Failure to pay timely will lead to an interest penalty, and may lead to sanctions by the State if trends develop with specific payers stalling payment. In particular, payment discounts to Managed Care Companies, which are already receiving very heavy discounts, is discouraged. Hold the companies that are stalling to contract terms, and to State regulations and laws. In summary Before offering discounts, consider both the advantages and disadvantages. Check with other providers in your area to see if they offer discounts. Ask for specifics on cash flow improvement (dollars collected/written off), and check on how it affected patient relations, if at all. If you do implement a prompt-payment discount policy, be sure to track your own cash flow improvements versus discounts written off. There must be a positive, long-term effect on cash in order to justify continuation of the policy.
Chapter 8 – INSURANCE VERIFICATION & PRE-CERTIFICATION Insurance Verification It is critical that a patient‘s insurance be verified prior to services being performed. In fact, insurance verification should always be a part of pre-admission and registration procedures. As you might recall from previous reading or study in this area, pre-admission and registration is defined as the process of obtaining demographic, insurance, financial, and essential medical information from the patient prior to access. Verifying a patient‘s insurance should then be just as commonplace as finding out where the patient lives. The specific information that must be verified is as follows:
1) Name of hospitalization insurance/coverage (i.e. Medicare, Medicaid, Commercial, etc.) and ultimately if it is active 2) Name, address (where claims are filed) and telephone number of insurance carrier(s) 3) Policy or contract numbers and group numbers of plans 4) Requirements for pre-certification 5) Accident type, date and place (if applicable) 6) Medicare Secondary Payer questions (if applicable) 7) ABN for Medicare or Medical Necessity
The purpose of insurance verification (especially on the front end) is to avoid any surprises, both for the medical provider and the patient. It is a simple fact of the healthcare revenue cycle: Insurance eligibility drives payment. In the absence of proper eligibility determination, countless downstream problems are created which include delayed payment, rework, decreased patient satisfaction, increased errors, and potentially, nonpayment. If the patient has expired coverage, or limited coverage that will not cover the services being performed, the facility must be aware of this if at all possible. Payment arrangements will need to be made with the patient prior to treatment. Insurance verification is the foundation for each of three steps that follow: Pre-certification, Pre-registration, and Pre-notification. For efficiency purposes, providers are installing automated insurance verification systems. There are many third party vendors who offer these products. As an account is registered, the insurance verification request can be sent out to the payer and most times returned while the patient is still available. However, the return information is dependent on the payer‘s response time and varies by payer. Even if the verification information returns and the patient has moved through the registration process and into another area of the facility, the information is still valuable to ensure the first bill goes out to the right payer with accurate information. Affecting your collection efforts overall is also putting in place a collection of co-payment/deductible during this initial patient access experience. Many facilities have instituted this type of up front collection practice and it does a lot to educate the patient as well as set the precedent early on for future responsibility.
Chapter 8 – INSURANCE VERIFICATION & PRE-CERTIFICATION, continued
Insurance Verification, continued
When verification of insurance is done manually by phone, users typically experience long hold times. Furthermore, if verifying for multiple payers and accessing the many different payer websites, users will need to have many different user IDs/ passwords coupled with multiple entry formats to request the response. As an example it is different to place an order for a book at Amazon vs. Barnes and Nobles. When eligibility is not properly verified, those ripples become waves that are felt throughout the organization. Getting eligibility right has always been imperative for efficient and effective reimbursement. For those payers who do not accept electronic verification requests you may either access their websites if offered or make a phone call. In the state of GA, most electronic data/revenue cycle vendors have great connectivity to 80% or better of the patient population. This is also your first opportunity to identify self-pay patients and initiate the process to discover other coverage options through medical assistance programs or, if ineligible, to initiate financial counseling and take into consideration your facility‘s charity policy. It is valuable to screen for Medicaid at the time of scheduling and admission. You will come to find that some of those patients are unaware that they do indeed have this coverage. Pre-certification Determine and comply with all commercial and government health plan requirements, such as pre-certification, pre-authorization and/or documentation of physician referrals. Managed Care Plans Most hospitals are contracted with managed care insurance plans to provide medical care to their subscribers. Large payers such as Blue Cross, United Healthcare, Aetna, Humana, Coventry, and Cigna sell managed care plans to employers. Each managed care plan has its own unique requirements for services that must be pre-certified (prior to service). This non-standardization of requirements is problematic for providers of medical care. Staff in hospitals must have tools to assist them in complying with each plan‘s requirements. How does the Financial Counselor, Insurance Verification person, or Registration person keep up with these details? Hospitals throughout Georgia and the nation are moving toward more technological solutions. In most every instance, the Financial Counselor has to work closely with the ordering physician to determine the correct Current Procedural Terminology (CPT) code in order to ensure authorization and timely payment. Physicians and hospitals use the HCPCS system to report services provided to the patient. HCPCS (pronounced ―hicks-picks‖) is the acronym for the HCFA (Health Care Financing Administration) Common Procedural Coding System.
Chapter 8 – INSURANCE VERIFICATION & PRE-CERTIFICATION, continued HCPCS consists of three unique levels in the coding system.
Level I – CPT (Current Procedural Terminology)
The CPT consists of 5 digits with descriptive terms to accurately describe services provided to patients. The CPT was first published in 1966 and is maintained and updated annually by the American Medical Association (AMA). The new codes may be used after October 1st of each year with a deadline for usage of January 1st of the next year.
Services are grouped into six categories:
Evaluation and Management (E/M)
Anesthesiology
Surgery
Radiology
Pathology and Laboratory
Medicine Under each category, codes are further broken down into subsections specific to body part, service, or diagnosis.
Level II – National Codes – This level is often referred to as the HCPCS codes.
These codes begin with a single letter (A through V) followed by four numeric digits. These codes are grouped by the type of service or supply provided. HCPCS codes are required to report medical services and supplies provided to Medicare and Medicaid patients. Some private insurance carriers are also requiring their use. The codes are updated annually by HCFA.
Level III – Local Codes
These codes begin with a letter (W through Z) followed by four numeric digits. These codes are utilized to report services that are not yet a part of Level I or II. These codes are assigned by local carriers.
Modifiers
Modifiers are used to further describe, alter, or enhance the description of the services provided. There are also three levels of HCPCS modifiers – one for each level of codes.
o Level I – CPT modifiers are two numeric digits. They are maintained and updated annually
by the AMA. o Level II – HCPCS/National modifiers are two alphabetic digits (AA-VP). They are recognized
by carriers nationally and are updated annually by HCFA.
o Level III – Local modifiers assigned by state Medicare carriers. Physicians are notified of their release
and update via newsletters. The carriers may change, add, or delete as indicated.
Chapter 8 – INSURANCE VERIFICATION & PRE-CERTIFICATION, continued ICD-9-CM (International Classification of Disease, Ninth Edition, Clinical Modification)
ICD-9-CM coding system is utilized to report the diagnoses applicable to each service rendered. Medicare began requiring the usage of the ICD-9-CM codes after the passage of the Medicare Catastrophic Act of 1988. Commercial carriers soon followed. The original purpose of the ICD system was to provide morbidity statistics for the World Health Organization. Today, ICD-9 codes are used to report information to support the need for patient care or treatment. They are also still used to provide morbidity and mortality rates. The purpose of ICD coding is:
To establish medical necessity to facilitate reimbursement
To translate written terms or descriptions into numbers in order to provide a common universal language
To evaluate utilization patterns to study appropriateness of health care cost factors In a physician practice, the physician should be the chief source for both CPT and ICD-9-CM coding.
Linking CPT and ICD-9
It is critical to associate the correct ICD-9 code to the correct CPT code. This is called ―linking‖. If not done properly, the insurance carrier will deny payment with a ―not medically necessary‖ reason code. This could increase inappropriate contractual write-offs or create a delay in reimbursement as a result of the necessity to re-file the claim with the appropriate ICD-9 linked to the CPT code. This could also decrease patient satisfaction due to inappropriate balance billing to the patient. Only conditions affecting today‘s care should be included in the diagnoses for each specific visit. Chronic conditions are linked to specific visits when applicable to the care rendered at that service. In the absence of a definitive diagnosis, only signs and symptoms are coded. ―Rule out‖ and ―possible‖ are not diagnosis codes. Using ICD-9 codes to identify an illness or disease that has not been definitively diagnosed can result in the patient labeled with an incorrect diagnosis. Such occurrences can result in higher premiums for the patient or denied coverage for other types of insurance.
Chapter 8 – INSURANCE VERIFICATION & PRE-CERTIFICATION Pre-certification, continued Medicaid As a condition of reimbursement, the Department of Community Health requires the majority of inpatient hospital admissions and now many outpatient procedures to be pre-certified. As of September 1, 2005, many CPT Codes for outpatient imaging, such as CT, PET, MRI, and OB ultrasound, now require pre-certification, even in conjunction with Emergency Department visits and observation. Pre-certification pertains to the medical necessity and appropriateness of setting only; the patient must be eligible at the time the service is rendered. The purpose of the program is to ensure that medically necessary quality healthcare services are provided to eligible Medicaid recipients in the most cost effective setting. Pre-certification does not guarantee reimbursement. The medical records must substantiate the medical necessity including appropriateness of setting for the services provided and billed to the Division. All services, regardless of certification, are subject to review for medical necessity. Obviously, failure to obtain the required certification will result in denial of reimbursement. Unfortunately, many payers are not prepared to receive automated requests for pre-certification, as they do for insurance eligibility verification. This results in many hours of telephone calls to the payers and the use of the fax machine. Many vendors; however, do offer efficient means of connectivity (via the web) but it is universally lacking since that payer list tends to be limited. This is all subject to change due to the CORE initiative. CORE
Although individual and regional efforts are important, there is a need for a national approach that is standardized across plans. Over the past two years, nearly 100 healthcare industry stakeholders have collaborated to develop a set of enhanced, common operating rules for electronic eligibility and benefit verification. The Council for Affordable Quality Health Care‘s Committee on Operating Rules for Information Exchange (CORE) has brought together health plans, providers, vendors, the Centers for Medicare and Medicaid Services and other government agencies, associations (including HFMA), standard-setting organizations, and banking industry experts to make this vision a reality. Health plans participating in CORE (Aetna, Inc.; AultCare; Blue Cross Blue Shield of North Carolina; Emdeon; Health Net, Inc.; Health Plan of Michigan; Humana Inc.; Mayo Clinic; McKesson Provider Technologies; Montefiore Medical Center; Siemens; and WellPoint, Inc. and its 14 Blue-licensed subsidiaries) represent nearly 75 percent of the commercially insured U.S. population.
CORE‘s focus throughout this initiative has been to:
Streamline and enhance current HIPAA eligibility transactions Reduce the amount of time and resources providers spend verifying eligibility and benefits Enhance interoperability between providers and health plans
Chapter 8 – INSURANCE VERIFICATION & PRE-CERTIFICATION
CORE, continued
The first phase of rules developed by CORE was recently approved. With phase I rules, providers will be able to:
Determine which health plan covers a patient Identify patient benefit coverage Confirm coverage of certain service types
Establish the patient‘s co-payment amounts, coinsurance level, and base deductible level for the service types as defined in the member contract. In addition, the rules establish policies governing the exchange of that data, including:
System connectivity Standard inquiry acknowledgements Maximum response times Minimum hours a system must be available Standard 270/271 companion guide flow and format
Health plans, vendors, and providers across the country are preparing to adopt CORE‘s phase I rules through a national certification process to further the adoption of electronic eligibility. The vision of integrated, real-time eligibility inquiries and responses brings us one step closer to the reality of this resultant collaborative. Similar to the banking industry‘s use of electronic transactions, providers will be able to submit eligibility inquiries and receive a real-time response from any point of entry using any electronic system of their choice.
By March 31, 2007, these organizations will electronically exchange eligibility and benefits information; the CORE operating rules will allow providers to obtain information from any participating health plan within 20 seconds or less.
The CORE initiative will create operating rules to address additional eligibility components and business transactions in later phases that begin this year. CAQH plans to launch the CORE phase II operating rules in late 2007.
In conclusion
Benefits eligibility and verification has always mattered. But it matters even more now due to the changes in the consumer-directed plans to the pricing transparency. There are several steps that will help your organization make this vision a reality:
Gain internal management commitment to improve eligibility automation to enhance the organization‘s financial performance and patient satisfaction.
Approach potential business partners. Providers cannot achieve the vision alone; they depend on health plans and software vendors.

Ask your partners what they are doing to make seamless eligibility verification a reality. Make ongoing business relationships contingent upon partners supporting standard electronic commerce for eligibility and benefit verification.
Chapter 8 – INSURANCE VERIFICATION & PRE-CERTIFICATION, continued In conclusion, continued
Automate this process (if at all possible) in a pre-encounter and scheduling environment. It will enable your front-line staff to have the dialogue necessary to bill correctly.
Consider what payment predictability increases you gain with Eligibility automation and how it affects your charity measures too. It will arm your back office-PFS division with how to bill &/or write-off claims based on financial triage information.
The key is to obtain complete and accurate information while the patient is present during the pre-encounter phase. It may be worthwhile for your employer to set in motion assessment of achievement benchmarks and report on these. This assessment might include quality assurance reports that show the percentage of scheduled patients whose insurance has been verified by user and reward or train accordingly. Remember we must collect every penny that is owed to our facilities and not a penny less or a penny more!!
Chapter 9 – INSURANCE DENIALS & APPEALS We have all experienced it – it doesn‘t matter what we do. We can handle everything perfectly: verify benefits with specific attention to detail; pre-certify in accordance with all relevant rules and regulations (whether required by contract or otherwise) provide the utmost in quality, medically necessary care; continue to re-certify through the course of the admission or other ongoing service; bill a ―clean‖ claim in a timely manner; etc., BUT WE KNOW THAT THE FOLLOWING CAN STILL HAPPEN.
- Patient did not have benefits during dates of service after all so the insurer will not pay
the claim - Pre-certification for 5 days was found to be medically unnecessary per post-treatment
medical review - only 4 days were deemed ―necessary‖ and will therefore only be reimbursed for 4 days
- Facility is considered out-of-network by the payer so emergency treatment will not be covered
- Treatment was deemed ―non-emergent‖ though patient seen in emergency room - Health insurer denies claiming another party is liable Patient has not returned the Third
Party Liability (TPL) questionnaire to insurer and patient cannot be located. Questionnaire required in order for health insurer to process claim
And, even if it makes it through billing without issues:
- Provider of services receives no payment/no response whatsoever - Claim denied for no coverage, no pre-certification, not medically necessary, etc. long
after services complete - Payment is significantly delayed and while the claim is eventually paid, the insurer pays
no interest on the claim per state law - Payment is the wrong amount -- always under -- rarely over! - ―Contract discount‖ taken but you are an out-of-network provider - Patient‘s policy disallowed most services provided; only approximately 15% of total
billed charges deemed covered, facility is out-of-network, and EOB shows patient only being responsible for his $500 deductible with remaining balance shown in ―non-covered‖ column
- Proper payment is made - but 2 years later, you receive a refund demand due to retroactive termination of benefits as a result of a delay in notification by the patient‘s employer‘s regarding employment termination
- Payment is made via ―credit balance‖ payment from an alleged erroneous payment on another account, so no actual payment is made but account now shows as paid in full according to insurer (often times no EOB is even received on such transactions so necessary details are missing)
- Payer is an ERISA Plan that says it does not have to pay the claim nor does it have to comply with Georgia laws
BOTTOM LINE – Insurers will always find a way to NOT pay your claims, even when you do everything perfectly! This chapter provides you with the basics necessary to understand, prevent and counter the above situations.
Chapter 9 – INSURANCE DENIALS & APPEALS, continued
An important factor to always remember is that the process of claim submission and insurer denials is best considered to be ―a game‖. It is your role in the game to ensure that claims are payable; it is the insurers role to avoid payment when at all legitimately possible. Do not take the game lightly though; the rules are there for a reason. They may be bendable or avoidable, but they are not expendable. Both sides must ultimately abide by the rules (the law or the contract!). Use them to your advantage or lose them!
DENIAL TYPES In order to properly handle insurance denials, you must first determine the relevant nature of each denial. Denials generally fall within two main classifications, though problems arise when situations are forced ―inside the box‖ of a particular category. You must always think creatively, with an open mind, when reviewing account denials, though certain templates or standard protocols may be used to avoid re-inventing the wheel with each similar situation. The following information will provide you with generally applicable rules to assist you in handling insurance denials. It is up to you, however, to discover the processes and details necessary to determine the precise method to use for most effective and efficient handling.
Technical vs. Clinical Denials
“Technical” denials occur when there is alleged coding or informational errors on claims, which prevent them from being considered ―clean,‖ and, therefore, payable by an insurer.
A ―clean claim‖ is one in which all fields of a claim are properly completed with correct codes, all information is accurate, all procedures followed and submitted in a timely manner, all in accordance with any agreed upon contractual provisions (or following accepted industry standards when no contract exists).
An insurer may deny a claim for technical reasons when it has been deemed to have been improperly submitted without complete or accurate information. This causes the claim to remain unpaid until corrections are made. Examples of technical denials are as follows:
Claim untimely upon submission No out-of-network coverage Improper bill type Wrong or missing pre-certification number Wrong birthdate or member number Non-covered procedure or revenue code Need Primary carriers Explanation of Benefits-even though insurer was the primary
carrier Medical records needed to process claim CPT or ICD 9 codes inactive for dates of service Denied as duplicate but claim never processed
Chapter 9 – INSURANCE DENIALS & APPEALS, continued
“Clinical” denials may occur when certain medical criteria is not met in accordance with standards in
the industry or pursuant to insurance contracts and/or utilization review policies and procedures.
This may include various clinical denials such as:
No authorization/certification (either before or during service) Post-billing medical record review deemed care to not be medically necessary for
intensity of service or length of stay Pre-existing condition exclusions exist Experimental procedures were used/not approved Emergency medical care deemed non-emergent LCD errors
Other Substantive Denials There are other substantive denials that are not clearly within the above two categories, such as third-party liability matters, coordination of benefits, or retroactive termination of benefits, though most routine denials generally fit into either the ―technical‖ or ―clinical‖ realm. These other denials are most critical to watch for, since they do not logically or easily fit in either of the two main categories with established protocols for handling and can actually cross into either area based on other specifics of the accounts.
For instance, a third-party liability matter may be treated and handled as a technical denial when it
was denied for this reason simply because of a treatment code used on the claim. The patient‘s diagnosis may not actually involve injuries caused by another party, but the code used to describe the services provided has triggered a TPL (third party liability) review by the insurer and the patient could not be reached for further explanation.
A retroactive termination of benefits may actually fall into either the clinical or technical realm of
handling. Depending upon who in your facility handles pre-authorizations, that staff would be the most appropriate to handle the rescission of that pre-authorization (since that is what a retroactive termination of benefits results in). Once a pre-certification is provided by an insurer, it is contrary to Georgia law to rescind that authorization; therefore, it is best to deal with these denials using this method.
Claims that fall into such gray areas often result in denials that slip through the cracks
or fail to be properly addressed or managed by the most appropriate staff. Medical Necessity Denials-(LCD) Medical necessity denials occur at all stages – before, during and after provision of services. Obviously, if this sort of denial occurs prior to actually performing recommended services, a medical provider still has the choice whether or not to proceed with the services, unless, of course, the services are emergent. In that case, both the medical provider and the insurer are prohibited from denying medical services and prior authorization is not allowed to be mandated.
Chapter 9 – INSURANCE DENIALS & APPEALS, continued
When an insurer denies pre-authorization of non-emergent (scheduled) care for clinical reasons, prior to services actually being performed, it is up to the provider to prove the medical necessity of the requested services. If it is unable to attain that authorization, services provided will not be reimbursed by the insurer; however, if authorization is, in fact, granted, the health insurer is then prohibited from ever denying the submitted claim based on medical necessity, though it may still deny for other reasons (i.e. technical or other substantive denial). If a patient is treated (non-emergently) without prior authorization, the provider must request retro-authorization based on medical necessity. Assuming this is done in a timely manner, an insurer‘s utilization staff will review clinical information supplied by the provider, as well as the patient‘s medical chart, to determine whether or not services were medically necessary. Again, once authorization is granted, the insurer is prohibited from later denying the claim for clinical reasons. If retro-authorization is denied, the provider must appeal that decision and continue to try to prove medical necessity of care; otherwise, the services are not reimbursable by the insurer. Many insurers deny claims retrospectively (after services have already been provided) for clinical reasons. It is important to remember that pre-authorized services may not later be denied for medical necessity, as long as accurate clinical information was provided at the time of the requested and granted authorization. An insurer may not dictate the precise care a treating medical provider may or may not provide. The treating physician always has the final determination as to which services are medically necessary in any given situation. Insurers who attempt to override that decision are in violation of Georgia law, though particular insurance policies may not ―cover‖ specific services. It is critical to determine whether a claim is being clinically denied for ―non-covered‖ or ―not medically necessary‖ services, since there is a huge difference in methods used to deal with each of these type situations.
Hard vs. Soft Denials You might believe that a denial is a denial -- no money is being paid for services, so what is the difference? Well, it is important to recognize whether the denial issued is a ―hard‖ or ―soft‖ denial A hard denial means your claim is not going to be paid (without a fight!) and soft denials basically mean that the claim payment has been delayed pending additional information, documentation or require other changes necessary to process the claim. It is important that you have the appropriate staff handling the denials, A hard denial is one in which an ―appeal‖ will be required to rectify the technical, clinical or substantive denial, i.e. medical necessity, improper coding, untimely claims submission, etc. A soft denial requires additional work on the part of the medical provider in order to obtain payment, though the claim is not necessarily permanently unpayable by the insurer. For instance, you may have provided the wrong birthdate for the patient or may need to wait for the insured to answer and return a TPL questionnaire for further information. In any case, the medical provider should gather all necessary information/documentation or make any required changes to obtain claim payment, whether required of the patient or medical provider. Where information is necessary from the insured, a medical provider must still motivate and incentive the patient to complete and submit that documentation; otherwise, the claim will remain unpaid by the insurer.
Chapter 9 – INSURANCE DENIALS & APPEALS, continued Either way – a denial is a denial – left unattended! Soft denials are usually reasonably easy to rectify, so do not miss the opportunity to handle an easy one now and again.
Partial Denials Claims that are only partially payable are referred to as ―partial denials‖. When this occurs, there is something missing or additional information is necessary to prove or obtain payment on the remainder of the claim. Sometimes the balance of a claim is denied as a ―hard denial‖, i.e. authorization not obtained through a certain date and deemed by the insurer as not medically necessary beyond the authorized dates of service (which will require the appeals process). Sometimes, however, the balance of a claim is only a ―soft denial‖, i.e. requires treatment notes to show certain services included on the claim were, in fact, provided. It is important to note that an insurer must pay the allowable portion of a claim, even when a certain portion of it remains unpayable. And, the insurer must supply a detailed explanation and/or l ist of items or information necessary for the insurer to approve additional payments. The entire payment may NOT be held up while rectifying any unpayable portion. If this occurs, or if a detailed explanation of the denial is not provided, look to the Georgia Prompt Payment of Claims Act for remedies!
THE APPEALS PROCESS
Initial Steps Though all steps have been rigidly followed and all known rules adhered to so as to prevent denials, insurers may still find creative ways to deny payment on claims. Once you receive a denial, you must first determine the nature and extent of the denial:
Has it been partially or fully denied? Is the denial hard or soft? Does the denial relate to technical, clinical or other substantive issues? What precisely needs to be done to best handle the denial, to counter the contentions of
the insurer, to rectify the claim status? Has this particular situation been dealt with before? If so, were previous methods
successful? Is this a new situation requiring individual handling of a new methodology and procedure? Who is the best to handle the circumstances at-hand?
Once you know specifically what you are dealing with, what needs to be done, and who needs to do it, you then must obtain some other relevant information:
Are you in-network or out-of-network? Were benefits verified? Authorized? What types of services are covered? What type of policy does the patient have?
Chapter 9 – INSURANCE DENIALS & APPEALS, continued
What is the patient‘s financial responsibility? Was the proper dollar amount allocated to all
responsible parties (contractual write-off, patient, etc.)? Were all conditions and provisions of the contract (if relevant) met? Was your claim ―clean‖? Did your facility do what it was supposed to do? Did the patient? Did the insurer? Who is ―at-fault‖ – what ―caused‖ this denial? Were all relevant insurance laws followed by both parties?
If you can answer most or all of these questions, you are already halfway to resolving the denial. Gather all of your information and prepare your argument(s)! Keep Appeal Forms Handy Most carriers have a set appeal form that is used to handle denials. If you keep these forms close, it will be much easier to locate them and start appealing your claims.
Know Your Contracts The most critical piece of information when dealing with any denial is the one most often overlooked or forgotten! You must know your contracts (when applicable) to effectively handle insurers‘ denials. Many times, the solution is stated within the language of your contract. How do you know if the insurer‘s denial is allowable, legitimate and/or rectifiable? You must determine what is required on your part in order to determine if you, the medical provider has met those conditions, if the claim submitted was in accordance with applicable provisions, if the insurer has treated the claim appropriately by denying it, etc. and what actions may or can be taken to rectify the situation. You must be aware of the appeals process available to you. Do you have but one level of appeal available or are multiple levels afforded? Imagine driving a car with your eyes closed! Once you get in a wreck, try telling the police officer that you weren‘t aware of any traffic laws! Dealing with a claim denial without knowing the applicable contract is just as dangerous (especially to the bottom line!)
Follow-Up Equally important as the above determinations is the follow-up performed both before and after a corrected claim and/or appeal is submitted. It is critical to make contact with the insurer, patient or any other relevant party before spinning your wheels in attempts to correct claims or prepare appeals. You must first ensure that all necessary information has been attained. The explanation of benefits or letter, which denied the claim, in whole or in part, may actually contain erroneous or incomplete information. Many times, an insurer will deny a claim for only one reason and will stop reviewing once that error or omission is identified. Other problems may, in fact, exist but not have been fully addressed at that time. This is actually a well-known delay tactic used by many insurers to further legitimately lengthen the time for ultimate payment of your claim. If you make initial contact prior to acting, you may prevent further denials and additional delays.
Chapter 9 – INSURANCE DENIALS & APPEALS, continued
Once correct claims or appeals have been submitted, you must follow-up accordingly with the appropriate insurer representatives. Merely contacting customer service representatives on a monthly basis is woefully insufficient to ensure proper handling of your issues. Simply asking for a ―status‖ of the claim also falls short of optimal follow up. Blanketed acceptance, as the gospel, of what you are told is also unacceptable. You must do more than merely ask questions and acknowledge answers…..you must press for answers and resolutions.
Proper ―follow-up‖ is the gathering of factual information, prying for additional details, forcing of proper handling and documenting of all actions and information. Anything less than this is insufficient and will result in further delay of payment -- and may actually cause additional complications with your claims. As stated earlier in this section, this is a game – insurers count on you dropping the ball! This stage is the prime opportunity for that to happen. Don‘t lose out simply by failing to finish the game! Follow-up is as important as any other stage of the process. If you can forget about a claim, the insurance company surely will too!
Exhaust All Available Options As previously stated, you must know your contracts. Management should make sure all parties that have a need to know have access to contractual specifics. If the relevant information about the contract is not available to you, you must ask pertinent questions of the insurer to determine what exactly you may do to rectify certain situations. Granted, asking the insurer for this sets up quite a biased situation, since you cannot expect them to know or educate you on all of the terms of your contract. Insurers aren‘t likely to tell you what THEY are required to do and not do, but if it is all you have available, then it is better than nothing at all.
Once you have determined (to the best of your knowledge) the processes you must adhere to, proceed with preparation of your action plan. Again, this is a game – you MUST know the rules in order to properly formulate your game plan! First, determine whose rules you must follow. If no contract exists and you are an out-of-network provider, Georgia laws strictly dictate all handling by both parties. If you are in-network, your contract dictates accordingly.
Before proceeding, you must decide how many levels of review and what methods are available to you. For instance, if you are in-network with Blue Cross Blue Shield of Georgia and it is determined that only one appeal level is accepted, do you allow your new, inexperienced employee to attempt resolution? You only have one try to get it right, so, know that going in and make your appeal a well founded one. Once that first level of appeal is over, are there any other avenues of recourse? Is the situation at-hand worthy of going to all available lengths? This is a critical question to ask before beginning any process, no matter how many levels are available, but especially if only a very small window of opportunity to resolve exists. If you are willing and the account denial is worthy based on quality, quantity, dollar amount, principle or otherwise, you are best suited for action by being aware of that upfront, and more importantly, by informing the insurer of that upfront.

Chapter 9 – INSURANCE DENIALS & APPEALS, continued Regardless of the situation, it is always prudent to exhaust all available levels of appeal. You just never know what that next set of eyes will see, whether from your staff or the insurer‘s. Mistakes are made and opportunities missed simply by failing to run the course!
Chapter 10-MEDICAID, MEDICARE & WORKERS COMP Traditional Medicaid Medicaid is a state managed program funded jointly by individual state and federal government funds to provide health insurance for individuals and families with low incomes and resources, and meeting a specific set of eligibility criteria (e.g. pregnant, aged, blind, or disabled). Medicaid is the largest source of funding for medical and health-related services for people with limited income. Among the groups of people served by Medicaid are eligible low-income parents, children, seniors, and people with disabilities.
If an individual is not a Medicaid recipient on the date of service, but later is evaluated for eligibility and determined to have been eligible at the time service was rendered, a claim may be filed for payment. These claims must be received within six months of the month in which the determination of retroactive eligibility is made. After the individual has been approved for Medicaid, they will receive a Medicaid card and will continue to be eligible for benefits. Essentially, a provider has accounts that have been sitting in self-pay or bad debt, it is possible that some of those patients would qualify for retroactive Medicaid coverage, and if the proper filings are made in a timely manner, those claims can be easily resolved. Many providers utilize various methods to assist in screening uninsured patients for Medicaid eligibility. Regardless of the method, HFMA encourages hospitals to assess the uninsured patient population for Medicaid using one or more of the following avenues:
1. Contract with a vendor partner 2. Use automated or web based software 3. Interact with the local DFACS (Department of Family and Children Services) 4. Create an internal program with Financial Counselors
Medicaid is prohibited from making payment for sterilizations performed on any person under the age of 21, or who is not mentally competent, is institutionalized in a correctional facility, mental hospital, or other rehabilitation facility. A sterilization consent form (DMA 69) must be properly completed and signed for all sterilization procedures. The signed consent expires 180 days from the date of the recipient‘s signature. The physician must sign the consent form after the sterilization. The mandatory waiting time between signed consent and sterilization is 30 days. Find more information @ Web portal: http://www.mmis.georgia.gov
Chapter 10-MEDICAID, MEDICARE, & WORKERS COMP, continued
Medically Needy Spend-down
Medically Needy Spend Down is a Medicaid eligibility profile that has no set income limit. Individuals may qualify for Medically Needy Spend Down when they have medical bills large enough to exceed the amount by which their income exceeds the eligibility limit. Pregnant women and children whose family income exceeds the established income limit may be eligible under the Medically Needy program. The Medically Needy program allows a person to use incurred/unpaid medical bills to "spend down" the difference between their income and the income limit to become eligible. This program covers children under the age of 18, pregnant women and aged and/or disabled persons who otherwise would be not Medicaid eligible because their monthly income exceeds the AFDC eligibility payment standards.
Spend-down recipients are issued a DMA 964 for the first partial month of eligibility and a DMA 400 form. The DMA 400 form indicates the amount of liability the Medicaid recipient will owe the provider. The Medicaid payment will be reduced by the spend-down amount. Financial Counselors can attempt to collect the spend-down amount listed on the DMA 400 form.
Georgia Healthy Families – CMOs & PeachCare Georgia Healthy Families is a partnership which was formed between the Department of Community Health (DCH) and private health plans (also referred to as ―care management organizations‖ or ―CMOs‖) to provide health care services to certain portions of its Medicaid population and PeachCare members via a managed care delivery system. The Georgia Healthy Families initiative was fully implemented throughout the state in 2006. Eligibility requirements for this initiative are limited to children enrolled in PeachCare, pregnant women, women with breast or cervical cancer previously receiving Medicaid benefits and children who met eligibility/household income requirements. Members will continue to obtain eligibility information through local DFACS offices.
DCH awarded contracts to the following CMOs.
Amerigroup Community Care – 1-800-600-4441 – www.realsolutions.com
Peach State Health Plan – 1-800-704-1484 – www.pshpgeorgia.com
WellCare of Georgia – 1-866-231-1821 – www.wellcare.com
Eligible members receive an identification card from the selected CMO at time of enrollment. The card lists the member‘s selected Primary Care Physician (PCP) just as any other commercial insurance card. Financial Counselors should ensure that all Medicaid recipients are verified either electronically or via phone to determine the recipients CMO. Each CMO has specific prior authorization and pre-certification requirements. Financial Counselors can access the applicable provider manuals on the CMO websites.
Chapter 10-MEDICAID, MEDICARE, & WORKERS COMP, continued
Medicare The Medicare program was implemented by the federal government on July 1, 1966. It is administered by the Center for Medicare and Medicaid Services (CMS), an agency within the Department of Health and Human Services (HHS). The Social Security Administration (SSA) is responsible for enrolling people in the Medicare program. Patient eligibility requirements for Medicare:
Age 65 or older
Under age 65 with disabilities
End-stage renal disease (ESRD) patients with permanent kidney failure requiring dialysis or a kidney transplant
Medicare eligibility can be determined by researching the Common Working File (CWF) information in the Federal Intermediary Shared System. Medicare has three parts: Part A – Hospital Insurance Part B – Medical Insurance Part D – Prescription Drug Insurance The majority of people do not pay premiums for Medicare Part A coverage upon reaching their eligibility as a result of ―paying for it‖ over time via taxes during their working years. However, there are some exceptions to this rule, i.e., if an individual has either not paid enough in due to self-employment, retiring early, etc.
Part "A" provides coverage for the following:
Inpatient care, critical access hospitals and skilled nursing facilities
Hospice care
Some home health care
Blood and blood products
Ambulance services during inpatient admits
Part ―A‖ does not cover private duty nursing, television or telephone in a hospital room, or a private room, unless these items are deemed medically necessary. The majority of people do pay premiums for Medicare Part B coverage. Medicare Part ―B‖ is considered optional coverage even though it covers more of your medical services.
Part ―B‖ provides coverage for the following:
Doctors‘ services
Outpatient hospital care for medical & surgical services, including diagnostic tests
Ambulatory surgery center facility fees
Outpatient physical & occupational therapists, including speech & language therapy
Outpatient mental health care
DME – Durable Medical Equipment
Some home health care
Second surgical opinions
Chapter 10-MEDICAID, MEDICARE, & WORKERS COMP, continued
Part ―D‖ became effective January 1, 2006. It provides prescription drug coverage and is available to everyone with Medicare (Aged, Disabled and ESRD). This coverage provides limited benefits to Medicare recipients through private companies. Beneficiaries choose their own drug plan and pay monthly premiums.
Medicare Secondary Payer In 1966, Medicare was the primary payer for all beneficiaries except those who received benefits from:
The Federal Black Lung Program
Workers‘ Compensation
The Veterans Health Administration (known as the VA)
In 1980, Medicare laws changed and increased the number of coverage and benefit programs primary to Medicare. The additions to the Medicare Secondary Payer (MSP) regulations included:
Automobile, liability, and no-fault insurance that may provide benefits for an accident or injury
Group Health Plans
Large Group Health Plans
Group Health Plans for persons with ESRD
To assist providers in implementing these MSP rules, CMS began to require providers to use the Medicare Secondary Payer Questionnaire. The purpose of the MSP Questionnaire is to assist the provider in identifying payers primary to Medicare to ensure Medicare is billed appropriately.
The Federal Black Lung Program covers certain medical expenses for beneficiaries who have black lung disease, commonly known as coal workers‘ pneumoconiosis. When a patient with Black Lung Disease requests medical care, they should be asked if the diagnosis for the specific encounter is related to black lung disease. This is part of the MSP Questionnaire. VHA benefits pay for services rendered to persons who served in our nation‘s armed forces. Even though services are usually rendered to these beneficiaries at a VHA facility, patients may appear at other hospitals when the VHA is unable to provide a certain service. An MSP scenario occurs with third party liability cases. The Medicare patient must be asked if the illness or injury for the specific encounter is due to a work-related accident or condition and if the illness or injury is covered under liability insurance, such as automobile insurance, no-fault insurance, personal injury insurance, or a medical ―set aside‖ account from a legal settlement. Medicare is also secondary when the patient is covered by a group health plan; either his or her own working plan or a plan from a spouse.
Chapter 10-MEDICAID, MEDICARE, & WORKERS COMP, continued The completion of the MSP Questionnaire on each medical visit is required by Medicare and will ensure compliance with Medicare regulations. MSP Questionnaires must be available for Medicare auditing at any time.
Medicare Spell of Illness – Benefit Period
Medicare will cover a maximum of 150 covered days for inpatient hospital services during any spell of illness/benefit period. These benefits include:
Days 1- 60 60 Full Coverage Days
Days 61-90 30 Co-Insurance Days
Days 91-150 60 Lifetime Reserve Days
The Medicare deductible is renewable during each benefit period. Medicare covers all Medicare covered services except the inpatient deductible. Full days renew with each benefit period. For example, if a patient has a hospital admission in January and does not have a second admission until October, the deductible will be due for both admissions. However, if the patient had a second admission in February, the deductible would not be due on the February admission. During the co-insurance days, a Medicare patient will owe ¼ of the current inpatient deductible per day. The 30 co-insurance days are renewable with each new benefit period. Lifetime Reserve Days are not renewable. Once they are used, they are gone. The Medicare patient will owe ½ of the current inpatient deductible for each day of hospitalization for days 91 –150. Medicare requires the hospital to notify the patient when they reach their Lifetime Reserve Days. The patient can refuse to consent to the use of the LTR days; however; the patient would then be responsible for the hospital‘s full charges. Because of the higher expense to the patient who has an extended benefit period, it is critical that Financial Counselors understand this Medicare regulation and communicate on a timely basis with the Medicare beneficiary/patient. Medicare‘s Common Working File will indicate the days used in a benefit period. This should be reviewed for each Medicare admission. Other Medicare Information Medicare also has Medicare HMO or Medicare Replacement Plans available for its beneficiaries. Financial Counselors should gain knowledge about these programs to better serve their patients.
Workers’ Compensation Workers‘ compensation is a benefits program created by state law in 1920 that provides medical, rehabilitation, income, death and other benefits to employees and dependents for injuries, illness, and death sustained as a result of a compensable work-related claim covered by the law.
Chapter 10-MEDICAID, MEDICARE, & WORKERS COMP, continued
Employers with three or more employees, in the same line of business, are required by law to provide workers‘ compensation coverage. If an employee is injured while performing assigned job duties, during assigned work hours, he/she will be covered under the workers‘ compensation program. However, injuries sustained while engaging in unassigned or unauthorized duties, during lunch, while taking a break, etc. will not be the responsibility of employer‘s workers‘ compensation insurance. Also, any injuries that occur during an employee‘s normal commute to and from work shall not be covered. Furthermore, workers‘ compensation does not provide benefits for an injury or accident sustained as a result of an employee‘s willful misconduct, i.e., fighting, horse play, injuries related to alcohol or drug abuse.
Hospital inpatient stays are covered by a DRG payment methodology. Any DRGs outside of the fee schedule will be reimbursed at a percent of the total charges. If a diagnosis is submitted that has not been assigned a DRG, the workers‘ compensation carrier must pay per CPT codes, ICD-9 codes or the reasonable and customary rate. Outpatient surgery shall be reimbursed based on ICD-9 codes or at a percent of total charges plus the cost of implants if applicable. Workers‘ Compensation accounts should be loaded as self pay until they can be verified. If a workers‘ compensation claim is denied and the patient appeals to the State Board, the hospital cannot pursue the patient for payment while the appeal is pending. Appeals can last many years.
Chapter 11 – ALTERNATIVE PAYER SOURCES
Third-Party Liability Third-Party Liability (TPL) refers to insurance carried by parties other than the patient, which may be liable for paying the patient‘s medical expenses. For example, take the case of a patient who is admitted to your hospital due to injuries sustained in an automobile accident. They have full health insurance coverage through Blue Cross/Blue Shield, which is their primary form of coverage. Additionally, the person who caused the accident may have automobile insurance through State Farm. Some elements of the hospitalization may be covered, and if so, State Farm becomes a third-party responsible for bearing some of the liability for the healthcare costs which resulted from the accident. There are many scenarios in which a third-party can be located and determined to be partially liable for hospital expenses. Automobile Insurance Georgia‘s mandatory auto insurance law requires that drivers have at least the following minimum liability coverage:
Bodily injury (BI) - $25,000 per person, $50,000 per accident payable for bodily injury to
others
Property damage liability (PD) - $25,000 per occurrence, payable for damage to the property of others Medical payments coverage is insurance the patient can buy on their own auto policy to cover
medical expenses related to an accident, whether the accident is their fault or the fault of a third party. Med-pay is no longer a requirement, but is still available for those who wish to purchase this coverage. Georgia repealed its ―no fault‖ law in 1991; therefore auto insurance policies no longer mandate coverage to pay for medical expenses or wage loss for injured occupants of the insured vehicle.
It is vitally important to monitor hospital accounts where medical payment (Med Pay) benefits
exist. This responsibility usually falls to the Financial Counselors. Since Med Pay benefits are usually paid on a ―first come first serve‖ basis, the Financial Counselor should request an interim billing to the auto insurance carrier as soon as the hospital account reaches Med Pay limits. This will usually ―protect‖ the payment. However, it should be noted that the patient directs where their Med Pay benefits are directed.
Automobile insurance companies should be billed on a hard copy UB (universal billing). Most
insurance companies providing medical benefits will coordinate with existing med-pay coverage.
Coverage can be purchased in almost any amount above the minimum.
Uninsured / Underinsured motorist (UM)
Insurance is a category of coverage that protects the policyholder in the event a motorist causes an accident and does not have insurance, has inadequate amounts of liability insurance, or flees the scene of an accident. UM coverage also covers the gap between the liability insurance of the person
who causes the accident, and the amount of your UM coverage. UM coverage is automatically equal to the policyholder‘s auto liability coverage unless it is rejected in writing.
Chapter 11 – ALTERNATIVE PAYER SOURCES, continued
If you have multiple cars in your household covered under separate insurance policies, you may be able to ―stack‖ the UM coverage‘s of each of the separate policies. In stacking UM coverage‘s, priority is determined according to the relationship of the injured person to the person paying the premiums. A lien can be filed so that the hospital bill can be considered at the time a settlement is reached with the uninsured/underinsured insurance carrier.
Liability Insurance All patients should be questioned as to the nature of their illness and/or injury to determine whether an accident was involved. Most insurance companies will not reimburse a claim until all accident / incident information has been provided so that primary payer responsibility can be established. In the event a patient sustained an injury as the result of someone else‘s negligence, liability insurance information should be obtained. These situations include but are not limited to, a fall at a store, a dog bite from someone other than the patients‘ dog, an injury at someone‘s home, a car accident etc. Some liability insurance can be filed directly and some must be awarded through the court systems. In these situations, a hospital lien is beneficial. Liability insurance should be filed and is primary over health insurance.
Homeowners Insurance Homeowners insurance exists to provide medical benefits in the event a person other than the resident family is injured while visiting or working at your home. Tort Liability A ―tort‖ is not a crime but a civil wrong-doing, other than a breach of contract done to another person. An injured person may sue anyone who commits a tort against him and collect damages – money to help compensate him for the wrong. The person who is injured and sues for damages as a result of the wrongful conduct is the plaintiff in the lawsuit. The person who has acted wrongfully and becomes liable to the plaintiff is the tort feasor, or defendant.
The law of torts deals with the allocation of responsibility for loss or harm arising out of human activities. Virtually any type of activity – driving a car, engaging in business, speaking, writing, owning or using property – may be a source of harm and, therefore, of tort liability. Examples of tort include:
If one purchases a new gun and the first time it is fired the gun explodes, both the
manufacturer and the dealer may be made to pay damages
If a neighbor‘s dog enters your yard and bites your child, the owner of the dog may be made to
pay damages
Chapter 11 – ALTERNATIVE PAYER SOURCES, continued
COBRA The US Department of Labor, via the Consolidated Omnibus Budget Reconciliation Act (COBRA), gives workers and their families who lose their health benefits the right to choose to continue group health benefits provided by their group health plan for limited periods of time under certain circumstances such as:
Voluntary or involuntary job loss
Reduction in hours worked
Transition between jobs
Death
Divorce
Other life events.
Qualified individuals may be required to pay the entire premium for coverage up to 102 percent of the cost of the plan.‖ ―COBRA generally requires that group health plans sponsored by employers with 20 or more employees in the prior year, offer employees and their families the opportunity for a temporary extension of health coverage.‖ (US Department of Labor. Home Page) Employers must notify employees of the availability of COBRA benefits within a specified time frame following notification to the employer of any qualifying circumstance.
Business Office and Admission employees should always inquire as to the employment status on self-pay accounts to see if a patient could be retroactively eligible for COBRA benefits. The hospital may choose to encourage the patient to pay their COBRA premiums or may even pay the initial premium on the patient‘s behalf to ensure reimbursement for services. This has become an acceptable process to assist patients in securing insurance coverage for their unexpected medical care. Note: If a patients ―qualifying event‖ was involuntary termination of employment that occurred on or after September, 1 2008 through May 31st, 2010, the patient may be eligible for an additional election opportunity. For more information concerning the American Recovery and Reinvestment Act of 2009 (ARRA), contact a benefit advisor through the US Department of Labor at 866-444-3272.
Chapter 11 – ALTERNATIVE PAYER SOURCES, continued Cancer State Aid The Cancer State Aid Program for the Georgia Department of Human Resources exists to provide financial assistance in covering expenses for the treatment of cancer for eligible patients. It was established in 1937 by the Georgia legislature at the request of Georgia physicians to provide cancer treatment to uninsured and under-insured cancer patients. The treatment program is available to eligible Georgians who would benefit most from treatment.
For the Hospital: To be a participating Georgia hospital in the Cancer State Aid Program, hospitals must have a Cancer Program approved by the American College of Surgeons and the hospital must be accredited by the Joint Commission on Accreditation of Hospitals.
For the Patient: Eligibility for patients within the Cancer State Aid Program is based on Federal Income Poverty Guidelines (FPG), with qualifying individuals at or below 200% of Federal Poverty Level for the year the patient is applying.
Additionally, individuals:
Must have a cancer that will benefit from treatment
Must have either no or limited health insurance coverage. (will cover Medicare participants for medications; will not cover patients with full coverage Medicaid)
Must be a U.S. citizen or alien lawfully admitted to be a permanent resident
Must be a resident of Georgia
Must be accepted for treatment by a physician affiliated with a participating facility.
Patient must also receive treatment at a participating facility.
The completed application should be sent to: Cancer State Aid Program Georgia Department of Human Resources Division of Public Health 2 Peachtree Street 16th floor Atlanta, GA 30303 (404) 463-5111 Email: [email protected]
More Information: http://health.state.ga.us/programs/cancerstateaid/index.asp
Chapter 11 – ALTERNATIVE PAYER SOURCES, continued
Vocational Rehabilitation Program (VRS)
Vocational Rehabilitation (known as VRS or Voc Rehab) may authorize the provision of a physical or a mental restoration service for a qualified individual to correct or substantially improve a physical or a mental condition, which affects his/her work outcome. The medical provider must be willing to accept the Voc Rehab established fee(s) and not bill the patient for any remaining balance. The eligibility criteria for Voc Rehab services are:
Applicant meets the definition of an individual with a disability
The disabled individual requires VRS to prepare for, secure, retain or regain employment
Applicant is a Supplemental Security Income (SSI), Social Security Disability Income (SSDI), or Temporary Assistance to Needy Families (TANF) beneficiary
Applicant is a Resident of Georgia
Applicant meets financial need assessments
Chapter 11 – ALTERNATIVE PAYER SOURCES, continued
Disability Adjudication Services (DAS) is a specialized program of Rehabilitation Services and works with the Social Security Administration to make disability determinations for Georgia citizens who apply for entitlement programs administered by the Social Security Administration. The VRS website for more information: www.vocrehabga.org
Children’s Medical Services (CMS)
CMS is the state and federally funded Title V Maternal and Child Health Services program. The CMS program receives an annual appropriation from the Georgia Legislature and grant funds available to the program. Program eligibility includes medical and financial requirements. Families with greater than 150% through 236% of the Federal Poverty Guidelines will be required to cost participate in the care of their child. Children who are Medicaid/PeachCare enrolled, receive SSI, or are in foster care are eligible for CMS services.
The medical eligibility includes, but is not limited to: burns, cardiac conditions, chronic lung diseases, craniofacial anomalies, diabetes mellitus, gastrointestinal disorders, hearing disorders, spina bifida, neurological and neurosurgical conditions, orthopedic disorders, cerebral palsy, congenital or traumatic amputation of limbs, and vision disorders. The Georgia CMS program requires prior authorization for all services. CMS is the payer of last resort, and all other resources must be completely pursued and documented prior to approval for funding. CMS will not cover admissions that have been denied by Medicaid because of failure to meet timely filing limits or failure to obtain a pre-certification. Receipt of a ―Prior Authorization‖ form for medical services is the only mechanism to assure that the patient is active on the CMS program and will cover services. The family should have this document and present it at time of service. Notification of and approval for payment of emergency room visits must be requested at the time of the ER visit or no later than the next business day. Notification of an emergency hospital admission must be made at the time of admission, or no later than the next business day. Failure to meet these requirements will negatively impact reimbursement.
Veterans Health Administration (VHA)
The VHA is a component of the United States Department of Veterans Affairs that implements the medical assistance program of the VA through the administration and operation of numerous VA outpatient clinics, hospitals, medical centers and long-term healthcare facilities (i.e. nursing homes). Because of the growing burden of health care costs, the VA has had to become more conservative in the provision of benefits in recent years. Many expensive diagnostic tests and medicines are subject to pre-approval, and fairly tight formulary restrictions are in place to control costs.
Chapter 11 – ALTERNATIVE PAYER SOURCES, continued
The VA provides a Medical Benefits Package, a standard enhanced health benefits plan available to all enrolled veterans. This plan emphasizes preventive and primary care, and offers a full range of outpatient and inpatient services within the VA health care system. The VA maintains an annual enrollment system to manage the provision of quality hospital and outpatient medical care and treatment to all enrolled veterans. A priority system ensures that veterans with service-connected disabilities and those below the low-income threshold are able to be enrolled in VA‘s health care system. Note: Veterans are required to seek healthcare services from a VA doctor and facility. The exception would be if the local VA hospital could not provide the necessary services. In such a case, the Veteran would have to obtain approval and a referral from his physician to go to a non-VA facility.
Non-VA hospitals should verify that the referral is in hand prior to admitting a Veteran. Failure to obtain the referral will lead to non-payment and the patient may not be billed. Reimbursement to non-VA hospitals for services provided to a Veteran is similar to the Medicaid/Medicare reimbursement methodologies.
Eligibility requirements are as follows: 1) Previously active military service in the Army, Navy, Air Force, Marines, Coast Guard (or Merchant
Marines in WWII), and discharged under other than dishonorable conditions 2) Injury and illness does not have to be related to service in the military 3) Reservists and National Guard members who were called to duty by a Federal Executive Order 4) Applies to both men and women who served in any of the branches of the military
Estates In common law, an estate is the total of a person‘s property (including money), entitlements and obligations. The term is often used in the context of wills and probate. In bankruptcy law, an estate is defined as all assets or property of any kind belonging to the debtor which is available for distribution to creditors. The person with legal responsibility for the estate is called the trustee. Often times, when an individual dies with debt still in their name, the estate of that individual is liquidated to pay the outstanding debt. It is critical that hospitals be aware of the death of former patients, especially when that patient still has open accounts for which they are the guarantor. It is vital that the hospital contact the estate trustee (generally a family member of the deceased patient) and explain the unfinished business needing resolution. Many creditors fail to follow-up in this way, and in doing so never realize the potential of resolving an open account through the deceased‘s estate. Take full advantage of this last opportunity to settle the account.
Chapter 11 – ALTERNATIVE PAYER SOURCES, continued
The order of preference in payment of creditors in an estate is:
Year‘s support for family
Funeral expenses
Other necessary estate administration fees
Reasonable expenses of last illness
Taxes, unpaid or other debts
Judgments, secured interest, and other liens
All other claims
A person who dies without a valid will is considered ―intestate‖. Special laws apply to intestate situations in order to control the disposition of property.
Crime Victims
Victims of a crime often end up in hospitals with injuries sustained, whether from a hit-and-run car accident, a mugging, or something far more serious. The hope is always that, once the police get involved, the perpetrator of the crime will be found and punished for his or her act of violence, negligence or criminal activity. If a victim of a crime is unable to pay for medical treatment, assistance is often available through the Crime Victim Compensation Fund.
Crime Victim Compensation Fund Crime victim compensation is a government program to reimburse victims of violent crimes, such as assault and battery, homicide, vehicular homicide, sexual assault, child abuse, domestic violence, DUI crash victims, hit and run, and - in some states - burglary, as well as their families for many of their out-of-pocket expenses. Every state has a crime victim compensation program. Crime victim compensation programs will generally pay for the following: 1) Medical and dental expenses 2) Counseling costs 3) Funeral and burial expenses 4) Lost wages or support
The direct victim of a violent crime is generally eligible for compensation. Some states only compensate victims who were physically injured in the course of a crime, while others also compensate victims of a violent crime who were traumatized but not physically injured by the crime. Families of homicide victims can get compensation to pay the medical bills and funeral/burial expenses, and to pay for counseling and loss of support. Some states will compensate family members in certain other types of cases, for example, paying for counseling for family members in cases of sexual assault, child abuse, or domestic violence.
Chapter 11 – ALTERNATIVE PAYER SOURCES, continued
In Georgia the eligibility requirements include:
The crime must be reported to government authorities, for instance, the police, child protective services, the courts, etc., within 72 hours. The 72 hour requirement may be waived if ―good cause‖ is demonstrated
The claim must be filed within one year of the crime
Applications must be received within two years after the crime or cannot be considered under any circumstances
Victims of domestic violence may be eligible for loss of support reimbursement
A parent of a child victim may be eligible for lost wages, to compensate for medical time spent away from work with the injured child
A criminal history will be provided and analyzed on all victim 18 years and older
Those not eligible include:
Victims of property crime
Victims who consent to or provoke the crime
Victims who were participants in the criminal act
Victims who do not report the crime to law enforcement officials within 72 hours
Victims who have not exhausted coverage and/or funds from other sources such as health insurance, auto insurance, social security, annual sick pay leave, disability insurance, worker‘s compensation, unemployment or funds from other government agencies
Payment cannot exceed $25,000. The caps for various categories are:
Medical expenses $15,000
Counseling bills $ 3,000
Funeral expenses $ 3,000
Lost wages $10,000
Crime scene cleanup$ $1,500
Compensation can be paid even when no one is arrested or convicted for the crime. For additional information concerning the Georgia fund, or to point a victim or their family to this resource:
Crime Victim Compensation Program 104 Marietta Street NW Suite 440 Atlanta, GA 30349 (404) 657-2222
Chapter 12 – LEGAL REMEDIES
Judgment Liens ―Lien‖ is the all-encompassing term given to any act of charge or encumbrance against an item/piece of property that secures the payment of a debt or performance of some other obligation. Liens can be consensual as well as non-consensual. Consensual liens are imposed by a contract between the creditor and the debtor (on items like car loans, mortgages, etc.). Non-consensual liens typically arise due to legal proceedings, and give the creditor the right to impose a lien on an item/piece of property simply based on the relationship between the creditor and the debtor. Judgment liens result when self-pay patients or responsible parties do not honor their obligation, and a lawsuit is filed to enforce their obligations. This suit can be based on ‗contract‘ due to their contractual obligation created upon signing the hospital‘s admission form or upon ‗open account‘ occurring as treatment is received. After judicial consideration of the pleadings and arguments, the court makes a determination and issues a ‗judgment‘. This judgment creates the basis for the Judgment Lien, which attaches to the debtor‘s property and/or assets thereby preventing any liquidation of the property or assets without satisfying the Judgment Lien first. Lawsuit has to be decided in favor of hospital or patient agrees to a ―consent Judgment‖ then fifa (a writ ordering a levy on the belongings of a debtor to satisfy a dept) is issued.
The Department of Social Services may impose a lien on the property of a Medicaid recipient if he or she retains a home and resides in a nursing home with the intent to return to the home and is unable to do so. The Department will notify a recipient if it intends to impose a lien. The amount claimed as a lien will be equal to the amount of assistance that the Department of Social Services provides to a Medicaid recipient while residing in the institution. The lien will dissolve when the recipient is medically released from the nursing facility or institution and returns to his or her home.
The Department of Social Services will not impose a lien on the home of a Medicaid recipient if:
1) The recipient has a spouse lawfully residing in the home
2) The recipient has a child under 21
3) The recipient has a child that is blind, disabled as determined by Supplemental Security Income
4) The recipient's sibling has co-ownership in the home property and has lawfully resided there continuously for at least one year immediately before the recipient was admitted to the nursing facility or institution
Chapter 12 – LEGAL REMEDIES, continued
Garnishments
―Garnishments can be filed in the Civil Division of the State Court Clerk‘s Office, Magistrate Court or Superior Court. A garnishment is filed against a party as a means of collecting a judgment that has been entered. There are several types of Garnishments. The two most common types are a Regular Garnishment and a Continuing Garnishment. A regular Garnishment is used primarily for garnishing a bank account or other financial institution. A continuing Garnishment is used solely for garnishing wages. All Garnishments are filed, processed and served upon the Garnishee (entity holding funds) e.g. the employer. ―The forms for filing a garnishment are provided‖ by the Clerk‘s Office. ―The Plaintiff‖ (hospital or their attorney) ―may appear in person to file…or may request the forms by mail or internet by sending a request and a self-addressed stamped envelope to‖ the Clerk‘s Office in the county where the hospital is located. ―The plaintiff or the plaintiff‘s attorney, in the presence of a Deputy Clerk or another court or a Notary Public, must sign the affidavit. The filing fee is due at the time of f iling. Once the proceeding is filed with‖ the Clerk‘s Office, ―it is approved, assigned a case number, processed and sent to the Sheriff‘s Office for service.‖ ―The plaintiff‘s attorney/plaintiff will receive back from this office a copy of the summons marked ‗Defendant‘s Copy‘ unless he/she elected to have the defendant served by the Sheriff. This copy must be served upon the defendant as provided by the law‖ within 3 days of notifying the garnishee.
Summons of Continuing Garnishment by Clerk
―YOU ARE HEREBY COMMANDED to hold immediately all property, money, wages, except what is exempt, belonging to the defendant, or debts owed to the defendant named above at the time of service of this summons and between the time of service of this summons to and including the one hundred seventy-ninth day thereafter. Not later than 45 days after you are served with this summons, you are commanded to file your answer in writing with the clerk of this court and serve a cop upon the plaintiff or his attorney named above. This answer shall state what property, money, and wages, except what is exempt, belonging to the defendant or debts owed to the defendant, you hold or owe at the time of service of this summons and between the time of such service and the time of making your first answer…The last answer required by this summons shall be filed no later than the one hundred ninety-fifty day after you receive this summons. Money or other property admitted in an answer to be subject to continuing garnishment must be delivered to the court with your answers. Should you fail to file answers as required by this summons, a judgment will be rendered against you for the amount the plaintiff claims due by the defendant.‖ Summons of Regular Garnishment by Clerk: ―YOU ARE HEREBY COMMANDED to hold immediately all property, money, wages, except what is exempt, belonging to the Defendant, or debts owed to the defendant named above at the time of service of this summons and between the time of service of this summons and the time of making your answer. Not sooner than 30 days but not later than 45 days after you are serviced with this summons, you are commanded to file your answer in writing with the Clerk of this Court and serve a copy upon the plaintiff or his attorney named below. Money or other property subject to this Summons should be delivered to the Court with your answer. Should you fail to answer this summons; a judgment will be rendered against you for the amount the plaintiff claims due by the defendant.‖
Chapter 12 – LEGAL REMEDIES, continued
Answer of Garnishee
―When the garnishee answers a garnishment and pays funds into the court the Clerk must hold the funds for 20 days. After 20 days, the Clerk will pay the money to the Plaintiff‘s Attorney/Plaintiff if an affidavit of compliance as to service on the defendant and request to condemn funds has been filed. If the plaintiff has an attorney the money will be paid to the attorney unless the Clerk has something in writing from the attorney authorizing the Clerk to pay it directly to the plaintiff.‖ ―If at any time the plaintiff‘s attorney/plaintiff wishes to stop the garnishment a written dismissal must be filed with the Clerk and the Clerk will issue a release to the garnishee with a copy to the defendant.‖
Payment by Defendant
―The Clerk will accept only full payment of a garnishment from the defendant. This payment must be made in cash.‖
Note: All funds in a bank account (regular garnishment) are recoverable up to the amount of the judgment, subject to any exemptions. Wage garnishments limit recovery to 25% of take-home pay and are also subject to any exemptions.
(Cobb State Court Clerk, Diane B. Webb, Clerk, web site www.cobbstatecourtclerk.com/garnishm.htm)
HOSPITAL LIENS - (Changes effective July 1, 2006)
PLEASE NOTE THAT NEW CHANGES WERE MADE TO THE HOSPITAL LIEN STATUTES EFFECTIVE JULY 1, 2006
When does a Lien Apply? -- When a person who has been injured by another party, at no fault of their own, (auto accident, negligent condition on a property, gunshot wound, slip and fall in a store, etc.) presents to a medical facility for treatment of those injuries, the hospital may have a right to place a lien on the patient‘s recovery from the at-fault party.
What it Means to the Medical Provider? - In order to encourage the treatment of accident victims
who may have no health insurance as well as better ensure payment to the treating medical provider, the Georgia Legislature enacted statutes located in the Official Code of Georgia Annotated at 44-14-470 et seq. stating that the provider (which now not only includes hospitals and nursing homes, but physician practices and traumatic burn care medical practices with charges in excess of $50k) shall
be entitled to a lien for the reasonable charges for cost of treatment on any and all causes of action accruing to the patient or their legal representative arising out of the accident causing the injuries which necessitated the treatment. However, the patient remains ultimately responsible for the medical charges, if not recovered from the third party, or if the patient is deemed responsible for his own injuries. Note: If the patient has health insurance, and if the provider is obligated to accept payment only for the insurer as payment in full under specific contract provisions, the patient shall not bear any personal responsibility beyond co-pays, deductibles and non-covered services.
Chapter 12 – LEGAL REMEDIES, continued
Further note that if patients have Medicaid or Medicare and you initially opt to pursue those payer sources, you are prohibited from pursuing the patient or third party payer for payment of full charges. Refer to Medicaid and Medicare regulations form further details. Hospital Liens are not:
Liens against the injured party
Liens against the patients legal representative
Liens against property
Liens against other assets
Evidence of the persons failure to pay a debt
Securing the Lien – Medical Providers must do the following to secure the lien:
The letter of intent, or ―notice letter‖ must be sent both certified and regular mail and the
sender must retain the postal receipt acknowledgments. This letter must explain to the patient that the hospital intends to file a lien on any settlement received. It must also explain to the patient that the lien is not against them or their assets.
No sooner than 15 days after mailing the letter of intent defined above, file a lien with the Clerk of the Superior Court in the county where the patient resides, as well as, the county where the hospital is located.
Send a copy of the lien to the patient and to any other liable party, such as the person, firm or corporation liable for the injury, or the insurance company of the third party.
The lien must be filed within 75-days from the date of discharge for hospitals, nursing homes and traumatic burn care facilities. However, physician practices are allowed 90-days from the date of discharge to file their liens.
You MUST complete these steps within the timeframes allotted to secure a perfected lien.
No settlement or release of third party monies shall be effective against a lien properly perfected unless the Provider is a party to the release or settlement. The provider may enforce the lien by an action against the person, firm, or corporation liable for the damages or such person‘s insurer. The action must be originated within one year of the date of the settlement.
Chapter 12 – LEGAL REMEDIES, continued A Medical Lien must contain the following:
Name and address of patient as it appears on medical record
Name and address of provider
Name and address of the operator of the medical facility
Dates of admission and discharge of patient
Amount of the medical bill
Names and addresses of all known persons or corporations allegedly liable for the injuries to the patient
The lien must be notarized and signed by the person preparing the lien
Upon Receipt of Payment -- If the medical bill is paid, the lien must be marked as ―paid and
satisfied‖ and the satisfaction should be filed with the Clerk of Superior Court where the lien is filed. The hospital Financial Counselor or attorney should be in regular contact with the patient and his/her attorney to obtain a status of the claim. Some hospitals in Georgia contract with an attorney to handle the filing of these liens and the resulting negotiations; others handle internally.
Bankruptcy
The number of bankruptcies filed in the United States increases every year, and even with the new filing laws, which make it more difficult to file, the number of bankruptcies is expected to rise. Collectors across the country are seeing the effect of the increases in the number of bankruptcies. Healthcare collectors are now met with more and more patients filing bankruptcy on their medical bills. Not only are most providers left holding the bag on these patients‘ balances, but also much time is wasted performing unnecessary work on accounts that are, for practical purposes, virtually uncollectible. The Basics of Bankruptcy
There are three types of bankruptcy that Financial Counselors should understand. Those are Chapter 7, Chapter 13, and Chapter 11. Chapter 7 filings are the most common bankruptcy proceedings. This type of bankruptcy is also
known as ―straight‖ or ―liquidation bankruptcy.‖ Its goal is to relieve patients of their debts. Under Chapter 7, an individual debtor is permitted to keep certain secured or exempt assets, but other assets may be liquidated to pay for some of the debts. For the most part, Chapter 7 results in the cancellation of debts, so the patient can get a fresh start. Unfortunately, hospitals and other creditors are often left with an uncollectible account.
Chapter 12 – LEGAL REMEDIES, continued
Chapter 13 bankruptcy is also known as a ―wage earner‘s‖ or ―payment bankruptcy.‖ As these names
imply, it is designed to have debtors repay all, or at least some, of the money owed to their creditors. Basically, Chapter 13 is a repayment proposal for individuals with a regular income. It is set up to use three years to repay the patient‘s debts, but with court approval it can be extended for up to five years. Payments to creditors are handled through a court-appointed trustee, and it is common to have repayment plans set up to pay less than the full amount owed to creditors usually 1% of the debt. The hospital's chances of getting payment on a Chapter 13 are slim but better than chapter 7. If one does receive payment, it will potentially take years, and it‘s unlikely that one will receive the entire amount owed.
Chapter 11 is a reorganization proceeding where debtors are trying to keep their property and use it
in the reorganization, but creditors want the property back. Chapter 11 is reserved for corporate entities and is to assist the company in ―reorganization under the protection of a Federal Court.‖ Medical providers should only be concerned when a company they are doing business with files chapter 11, such as a collection agency or Medicaid enrollment specialty company. Since a medical provider is an unsecured creditor (meaning you have no property to take back), ones chances of receiving payment are remote.
NOTE: The most important thing to remember when working with bankruptcy is that one cannot continue collection efforts once notification is received of the bankruptcy filing. The entire purpose of bankruptcy is to provide relief to debtors from the people they owe. A creditor, in this case a hospital, can be fined and/or sanctioned by the U.S. Bankruptcy Court by attempting to collect from someone who has included your billing in their bankruptcy.
Secured and Unsecured Debt There are two types of debts involved in a bankruptcy: secured and unsecured. Secured debts are backed up by some type of property (house, car, boat, jewelry, etc.). When the debt or loan was incurred, the debtor signed a document giving the creditor some rights to the property. The signed documents guarantee the debtor will repay the full amount of the debt plus interest. The creditors‘ secured interest stays intact, even when the debtor files bankruptcy. A medical bill is an unsecured debt. Unsecured debts are usually for consumer goods and services, such as credit cards, utilities, and of course, healthcare bills. These debts are usually discharged in bankruptcy. This is why hospitals seldom get paid, even if a claim is filed.
What to Do When a Patient Files Bankruptcy?
1) Obtain and document all pertinent bankruptcy information: A. Chapter filed
B. Date bankruptcy filed (patients are responsible for bills incurred after the file date) C. Case number D. Attorney name and phone number
2) Pull all accounts where the patient is guarantor, and note that bankruptcy proceedings have started
Chapter 12 – LEGAL REMEDIES, continued
3) Immediately stop routine collection efforts on all applicable accounts including phone calls and statements
4) Contact the attorney and verify all bankruptcy information. Make sure your bill is listed the bankruptcy. Ask the attorney‘s opinion as to the probability of recovering the debt 5) If the balance warrants, and there is a possibility of recovery, you may file a proof of claim on the bankruptcy. (It is always better to err on the side of caution and file a proof of claim, when in doubt.) 6) After you file a proof of claim, or if you decide not to file because it‘s simply not worth it, write off the balance. There is no reason to keep the account open any longer. If you do recover some money from the bankruptcy, or if the case is dismissed, you could always reverse the write-off if necessary.
Filing a Proof of Claim
Results from national surveys of healthcare providers clearly show filing a proof of claim is often perceived to be a waste of time. Less that 40 percent of the collection offices surveyed go through the process of filing claims on bankruptcies or pay an attorney to do so. Of those offices that do file a claim, less than 6 percent ever remember recovering any payment from a bankruptcy proceeding.
One‘s chances of receiving payment from a bankrupt patient are negligible, so it might be in the best interest of the hospital to avoid filing a claim. If one does run across anything that seems suspicious about a case, always refer it to an attorney. Many providers have discontinued filing a proof of claim. Some have set procedures to file claims only on large-balance accounts or Chapter 13 cases, but not Chapter 7 cases. If one spends a substantial amount of time filing claims, you may want to take a look at how profitable your procedure is. Track the amount of money your facility actually collects from the claims, which are filed, and compare it to the time and money that is spent filing the claims. Keep in mind that the time spent filing a claim on these likely uncollectible accounts could be better spent on more profitable accounts. When bankruptcy is filed, there is an alternative to writing off the claims without any effort to collect. There are a few companies that specialize in recovery of bankruptcy dollars. Companies such as this may offer to purchase your bankruptcy cases, in hopes of recovering a few pennies on the dollar. Of course, the purchaser offers the hospital even fewer pennies on the dollar, but recall the old adage, ―A bird in the hand is worth two in the bush.‖ Hospital policy would dictate how a hospital handles these cases.
Chapter 12 – LEGAL REMEDIES, continued
When a Patient Threatens Bankruptcy
―If you push me for payment, I‘ll file bankruptcy!‖ Not only are actual bankruptcies increasing, but also so is the use of the threat that one will file. Patients hope the hospital will back off and give them more time to pay, or even forget about the debt. Just because a patient threatens bankruptcy, do not back down on your requests for payment. Usually it‘s just a bluff. Instead, remain calm and professional, and say something like: ―Mr. Jones, if and when you file bankruptcy, please inform us of the date filed and the case number, however, I really think that, between the two of us, we can come to an agreement, so you won‘t have to go through the trouble and expense of filing bankruptcy.‖ Negotiating is an effective way of letting patients know your hospital will not be put off by threats. Standing firm shows them you would rather work out a mutually acceptable payment arrangement and that the hospital can be both firm and cooperative.
Bankruptcy: Understanding New Changes to the Law Now that the new bankruptcy law is in effect, the landscape has changed for those who are considering bankruptcy. All debtors will have to get credit counseling before they can file a bankruptcy case (and additional counseling on budgeting and debt management before their debts can be wiped out). Some filers with higher incomes won't be allowed to use Chapter 7, but will instead have to repay at least some of their debt under Chapter 13. And, because the law imposes new requirements on lawyers, it will be more difficult to find an attorney for representation in a bankruptcy case.
Here are some of the most important changes
Counseling Requirements
Before an individual can file for bankruptcy under either Chapter 7 or Chapter 13, they must complete credit counseling with an agency approved by the United States Trustee's office. The purpose of this counseling is to give them an idea of whether they actually need to file for bankruptcy or whether an informal repayment plan would get them back on their economic feet. Counseling is required even if it's obvious that a repayment plan isn't feasible or the individual is facing debts that they find unfair and don't want to pay. Individuals are required only to participate, not to go along with any repayment plan the agency proposes. However, if the agency does come up with a repayment plan, they will have to submit it to the court, along with a certificate showing that they completed the counseling, before filing for bankruptcy. Once their bankruptcy case is over, they will have to attend another counseling session, this time to learn personal financial management. Only after submitted proof to the court that this requirement has been fulfilled can the individual get a bankruptcy discharge wiping out their debts.
Restricted Eligibility for Chapter 7
Under the old rules, most filers could choose the type of bankruptcy that seemed best for them (and most chose Chapter 7 over Chapter 13). The new law will prohibit some filers with higher incomes from using Chapter 7.
Chapter 12 – LEGAL REMEDIES, continued
How High is Your Income?
Under the new rules, the first step in figuring out whether one can file for Chapter 7 is to measure their "current monthly income" against the median income for a family of their size in their state. One‘s "current monthly income" is not their income at the time they file, however: It is their average income over the last six months before they file. For many people, particularly those who are filing for bankruptcy because they recently lost a job, their "current monthly income" according to these rules will be much more than they take in each month by the 0time they file for bankruptcy. Once the calculation of income is complete, the individual must compare it to the median income for their state (you can find median income tables, by state and family size, at the website of the United States Trustee, www.usdoj.gov/ust; click "Means Testing Information"). If your income is less than or equal to the median, you can file for Chapter 7. If it is more than the median, however, you must pass "the means test" (another requirement of the new law) in order to file for Chapter 7.
The Means Test
The purpose of the means test is to figure out whether you have enough disposable income, after subtracting certain allowed expenses and required debt payments, to make payments on a Chapter 13 plan. To find out whether you pass the means test, you start with your "current monthly income," calculated as described above. From that amount, you subtract both of the following:
Certain allowed expenses, in amounts set by the IRS. Generally, you cannot subtract what you actually spend for things like transportation, food, clothing, and so on; instead, you have to use the limits the IRS imposes, which may be lower than the cost of living in your area
Monthly payments you will have to make on secured and priority debts. Secured debts are those for which the creditor is entitled to seize property if you don't pay (such as a mortgage or car loan); priority debts are obligations that the law deems to be so important that they are entitled to jump to the head of the repayment line. Typical priority debts include child support, alimony, tax debts, and wages owed to employees
If your total monthly disposable income after subtracting these amounts is less than $100, you pass the means test, and will be allowed to file for Chapter 7. If your total remaining monthly disposable income is more than $166.66, you have flunked the means test, and will be prohibited from using Chapter 7. So what about those in the middle? They have to do some more math. If your remaining monthly disposable income is between $100 and $166.66, you must figure out whether what you have left over is enough to pay more than 25% of your unsecured, non-priority debts (such as credit card bills, student loans, medical bills, and so on) over a five-year period. If so, you flunk the means test, and Chapter 7 won't be available to you. If not, you pass the means test, and Chapter 7 remains an option.
Chapter 12 – LEGAL REMEDIES, continued
Lawyers May Be More Difficult to Find, and More Expensive
As you can see, the new law adds some complicated requirements to the field of bankruptcy. This is going to make it more expensive (and time consuming) for lawyers to represent clients in bankruptcy cases, which means attorney fees are going to go up. The new law also imposes some additional requirements on lawyers, chief among them that the lawyer must personally vouch for the accuracy of all of the information their clients provide them. This means attorneys will have to spend even more time on bankruptcy cases, and charge their clients accordingly. Some experts predict that this combination of new requirements may drive some bankruptcy lawyers out of the field altogether.
Some Chapter 13 Filers Will Have to Live on Less
Under the old rules, people who filed under Chapter 13 had to devote all of their disposable income (what they had left after paying their actual living expenses) to their repayment plan. The new law adds a wrinkle to this equation: Although Chapter 13 filers still have to hand over all of their disposable income, they have to calculate their disposable income using allowed expense amounts dictated by the IRS (not their actual expenses) if their income is higher than the median in their state (see "Restricted Eligibility for Chapter 7," above). These expenses are often lower than actual costs. Potentially worse for the filer is that these allowed expense amounts must be subtracted, not from the filer's actual earnings each month, but from the filer's average income during the six months before filing. This means that debtors may be required to pay a much larger amount of "disposable income" into their plan than they actually have to spare every month, which, in turn, means that many more Chapter 13 plans will fail.
Property Must Be Valued at Replacement Cost
Under the old law, Chapter 7 filers could value their property at what they could sell it for in a "fire sale" or auction. This meant that used furniture, hobby items, cars, heirlooms, and other property a debtor might want to keep were typically assumed to have little value and, therefore, that it often fell well within the "exempt property" categories offered by most states. (Exempt property is property that cannot be taken by creditors or the trustee -- you are entitled to keep it.) Under the new law, you must value your property at what it would cost to replace it from a retail vendor, taking into account the property's age and condition. This requirement is sure to jack up the value of property, which means more debtors stand to have their property taken and sold by the trustee.
Chapter 12 – LEGAL REMEDIES, continued
State Exemptions Aren't Available to Recent State Residents
Under the old bankruptcy law, the personal property debtors were allowed to keep in Chapter 7 bankruptcy was determined by the laws of the state where they lived (as long as they lived there for at least three months). Under the new law, you must live in a state for at least two years prior to filing in order to use that state's exemption laws. Otherwise, you must use the exemptions available in the state where you used to live. Similar rules apply to homestead exemptions, which determine how much equity in a home you can keep when filing for Chapter 7 bankruptcy. However, to use your new state's homestead exemption, you must live there for at least 40 months.
Chapter 13 - Georgia’s Prompt Pay Law
Interest in the issue of prompt payment of health care claims has been increasing during the last several years as hospitals and health systems have experienced slower payment and the financial pressures caused by lower payment levels under both public and private health plans. Effective July 1,1999, the Georgia General Assembly enacted one of the strongest prompt payment laws in the country. The prompt pay laws are designed to ensure that patients who are covered by a health insurance policy have their benefits paid to their provider of service in a timely manner. The Official Code of Georgia Annotated (OCGA) §33-24-59.5 (3)(b)(1) states that ―all benefits under a health benefit plan will be payable by the insurer which is obligated to finance or deliver health care services under that plan upon such insurers receipt of written proof of loss or claim for payment for health care goods or services provided. The insurer shall within 15 working days after such receipt mail to the insured or other person claiming payments under the plan payment for such benefits or a letter or notice which states the reasons the insurer may have for failing to pay the claim, either in whole or in part, and which also gives the person so notified a written itemization of any documents or other information needed to process the claim or any portions thereof which are not being paid.‖
The statute further states that ―where the insurer disputes a portion of the claim, any undisputed portion of the claim shall be paid by the insurer in accordance with this chapter.‖
If a health insurer fails to comply with the prompt payment provisions in the Georgia law, they are required to pay a penalty in the form of interest at the rate of 18% per annum on the proceeds or benefits due. The Georgia prompt payment law does not apply to self-funded ERISA (Employee Retirement Income Security Act of 1974) plans; however, for non-ERISA plans, the prompt payment law provides a powerful tool that health care providers can use when health plans are slow to pay claims. Enforcement of the prompt payment law is the responsibility of the Georgia Office of Insurance Commissioner. The Life and Health Division‘s Managed Care Section works to resolve complex claims problems between health care providers and managed care insurers, including health plan compliance with the prompt payment law. A copy of the form that providers should use when submitting a complaint with the Insurance Commissioner‘s office is attached. The form is also available on the Georgia Insurance Commissioner‘s web site at www.inscomm.state.ga.us.
Chapter 14 - Health Savings Accounts (HSA’s)
One may pick up a current communication from healthcare consultants, read any issue of a healthcare journal, such as HFM, or ―Google‖ Health Savings Account (HSA), and to some degree Medical Savings Account (MSA), and find an abundance of information and speculation regarding the hot topic of a High Deductible Health Plan (HDHP) with a Health Savings Account (HSA) or a Health Reimbursement Arrangement (HRA) providing traditional medical coverage and a tax free way to help you build savings for future medical expenses. The HDHP/HSA or HRA gives you greater flexibility and discretion over how you use your health care benefits. This chapter is designed to provide enough information to the Financial Counselor, to furnish a degree of knowledge sufficient to intelligently discuss the subject with patients/guarantors, and allow the Financial Counselor the edge in negotiating a payment for services from the savings account.
What is an HSA?
According to the March 2006 issue of HFM‘s feature story written by Debbie-Welle-Powell, ―An HSA is a new type of health insurance coverage, authorized by the Medicare Prescription Drug, Improvement, and Modernization Act for 2003, and introduced in early 2004. It combines a high deductible policy with a tax-exempt healthcare savings account. HSAs are like health reimbursement accounts in that they are linked to high deductible health plans and come under the umbrella of consumer-directed health plans. Both HSAs and HRAs give consumers more responsibility for managing their healthcare spending.‖ (March 2006, healthcare financial management, page 77)
HSAs are similar to individual retirement accounts (IRAs), but even better:
Pre-tax money is deposited each year into an HSA and can be easily withdrawn at any time with no penalty or taxes to pay for qualified medical expenses. Withdrawals can also be made for non-medical purposes, but will be taxed as normal income and are subject to a 10 percent penalty if done prior to age 65.
Any HSA funds not used each year remain in the account, and earn interest tax-free to supplement medical expenses at any time in the future.
Like an IRA, the account belongs to you, not your employer. But unlike an IRA, your employer CAN contribute to your HSA.
Chapter 14 - Health Savings Accounts (HSA’s), continued
What are qualified Medical Expenses? HSAs can be used to pay for many types of medical expenses, even some which are often excluded on health insurance plans. These include:
Health insurance plan deductibles, copayments, and coinsurance Prescription and over-the-counter drugs Dental services, including braces, bridges, and crowns Vision care, including glasses and Lasik eye surgery Psychiatric and certain psychological treatments Long-term care services Medically-related transportation and lodging
Typically HSAs cannot be used to pay health insurance premiums, although there are exceptions for:
Health insurance premiums if you are receiving federal or state unemployment benefits
Premiums for COBRA qualified health insurance Certain qualified long-term care insurance premiums Premiums for a health plan (other than a Medicare supplemental
policy) for an individual age 65 or older
Note: You must establish an HSA before incurring any expenses or the expenses will not qualify.
Consumerism, consumer driven healthcare is a new force in the industry and one which healthcare providers will need to be able to cope with. One of the major changes in consumer driven healthcare will be the proliferation of HSAs. HSAs will give power, choice, and decisions to the individual patient never before seen in the industry. One definite result will be a reduction of use of healthcare services, because HSA owners will be reluctant to spend their hard earned and saved dollars on doctors and hospitals, which potentially can be part of their retirement. ―Early reports from Definity Health, a Minneapolis based provider of consumer-directed health plans, showed and 11 percent decrease in healthcare utilization for consumers with HSAs‖. (March 2006 , healthcare financial management, page 77).
Chapter 14 - Health Savings Accounts (HSA’s), continued How Wide Spread Are HSAs? ―In 2005, about…1 million (Americans) had HSAs, according to a report sponsored by the Foundation for Agency Management Excellence. However, HSAs appear to be gaining in popularity because they are employee owned and fully portable. The FAME report notes that as many as 32 percent of employers may add HSAs to their employee benefits in 2006.‖ (March 2006, healthcare financial management, page 76) How Are HSAs Funded?
―Both employee and employer make deposits into an HSA to pay for qualifying medical expenses.‖ (March 2006, healthcare financial management, page 77)
What Does the Law Say Regarding Use of HSA Saved Funds?
―HSAs allow tax-free savings for healthcare expenses for participants under age 65 covered under high-deductible health plans. The contributions and the earnings on the account and the distributions are all income-tax free if certain requirements are met.
In addition to the benefits of tax-free savings for healthcare expenses, HSA participants potentially may use these accounts to save and invest tax-free for retirement.‖ (March 2006, healthcare financial management, page 77) For 2011:
Deductibles start at $1,200 for individuals & $2,400 for families
Maximum out-of-pocket annual expense must not exceed $5,950 for individuals & $11,900 for families
Some employers may cover preventive services
After deductibles are met, normal coverage takes over for the remainder of the year
You may have the choice of using in-network and out-of-network providers. Using in-network providers will save you money. With the exception of preventive care, you must meet the annual deductible before the plan pays benefits. Preventive care services are generally paid as first dollar coverage or after a small deductible or copayment. A maximum dollar amount may apply.
Please note that there are no mandates to date, which require HSA participants to fund their savings or require them to spend the savings on specific health expenses.
Chapter 14 - Health Savings Accounts (HSA’s), continued Patient using funds in your Health Savings Account
Typically, an HSA will provide a checkbook or debit card. When qualified medical expenses are paid the patient will use the debit card or check to make the payment.
You do not need to get approval from the HSA administrator when the patient uses funds from their account.
Patient does not need to submit receipts to the HSA administrator, although they should save them just as they keep receipts for other items that are deducted from their taxes.
NOTE: The patient must establish the HSA before they incur medical expenses otherwise the expenses will not qualify.
How Does the Hospital Access the Funds in an HSA?
Hope and pray the account is funded
Hope and pray that the account owner is willing to release the funds
If the account owner is not openly willing to release the funds – Beg
Seriously, one must use scripting, powers of persuasion, appeals to ones need to remain debt free, or whatever legal and ethical tactics one can employ to encourage the patient/guarantor to release the saved funds, if they exist at all. Some reports have stated recently that roughly only about one quarter of all 1 million HSAs are funded today.
What Alternatives Does the Hospital Have If the HSA is not Funded?
Revert to collection practices utilized for self pay patients.
Benefits of HSAs To the Patient
Patients gain control over the expenditures of first dollar spent for healthcare services
Patient‘s responsibility to make key decisions regarding healthcare increases. Because it is ―my money‖ one may become much more choosey about the place they seek services, the convenience, the cost, and the quality of the services. In fact, hospitals should expect usage/volume slowdowns as HSAs further proliferate
HSAs provide an incentive to save
To the Employer
Employers will save money on premiums
Employers may have happier, more satisfied worker‘s who feel they are saving money and gaining control of saving and spending
To the Healthcare Provider: (One may say “none” but think about it)
Providers will be forced to revisit their policies regarding insurance verification, collection at time of service, use of credit cards, and perhaps discounting
Chapter 14 - Health Savings Accounts (HSA’s), continued
Providers will have to increase technology and efficiency, which may include: o Use of electronic real time eligibility o Accurately edited claims which will allow early claims adjudication o Greater use of credit and debit cards o Creation of On-Line payment capabilities for guarantors o On-Line self registration o And finally – Do we dare be so bold – Force providers to pre-register, pre-verify,
pre-certify, pre-notify the patient – FOR ALL SCHEDULED SERVICES – Which may lead to closer relationships and greater collaboration with physicians than ever before seen in the industry
o Finally – Finally – Providers may need to get more vocal about requesting legislation which would require funding of HSAs and require all HSAs to be debited for verified healthcare expenses
Providers will have to improve the activity and efficiency in their Reimbursement Departments and begin looking for revenue and cash in other areas of the Revenue Cycle
Providers may have to develop better relationships with Payors and local employers in order to control contracts and policies regarding funding and release of funds
Other related subjects worth researching:
MSA (Medical Savings Account)
HRA (Health Reimbursement Arrangement)
HDHP (High Deductible Health Plan)
LEX HCFSA (Limited Expense Health Care Flexible Spending Account
FSA (Flex Spending Account) ( sometimes referred to as Flex Savings Account) aka HCFSA (Health Care Flexible Spending Account)
Chapter 15 - Prohibited Practices (Senate Bill 476 Enacted)
In 2002, the Georgia General Assembly passed Senate Bill 476—the Consumers‘ Health Insurance Protection Act. This legislation contains a number of provisions that are designed to improve managed care payments to hospitals. This Chapter will cover some of the most important provisions and prohibited practices that were signed into law on April 19, 2002. In accordance with O.C.G.A. §33-20A-62, no carrier may conduct a post-payment audit or impose a retroactive denial of payment on any claim relating to the provision of health care services that was submitted within 90 days of the last date of service or discharge covered by such claim unless:
Notice of the following is supplied in writing to the Provider: o Specific Claim in which the audit or review relates to o Specific Reason for the review or audit
Not more than 12 months can lapse between the claim ―date of service‖ or ―discharge covered‖ prior to receiving the notice
& The review/audit must be completed and refund requested and/or money paid prior to the expiration of 18 months from the last date of service
It is important to note that if the provider fails to bill a patient for services within 45 days of the date that it became aware that further payment was due as a result of a post-payment audit, retroactive denial, etc., the patient shall be relieved of any and all legal obligations to respond to a request for
additional payment. Further, when precertification has been obtained, the insurer shall be prohibited from requesting payment, contesting or reopening the claim or any portion thereof at any time following precertification except to the extent that the insurer is not liable under 33-20A-7.1 (Note that this statute (33-20A-7.1) provides the precertification requirements for insurers). Also, if a provider obtains precertification for any covered health care service, the managed care plan is required to pay for such precertified services, unless one of the following conditions is present:
The services are not obtained within the time limits set in the precertification
The enrollee is no longer covered under the plan at the time the services are provided
Benefits are exhausted
The enrollee or provider commits fraud
Chapter 15 - Prohibited Practices (Senate Bill 476 Enacted), continued Another significant provision of the Consumer‘s Health Insurance Protection Act concerns continuity of care rights. If a managed care plan terminates a physician‘s participation in a managed care plan network, an enrollee receiving active health care services for a chronic or terminal condition, or who is an inpatient, has the right to continue receiving health care services from the terminated physician for a period of up to 60 days after termination of the contract. Pregnant enrollees receiving pregnancy-related treatment at the time of termination have the right to continue to receive services from the terminated physician throughout the remainder of the pregnancy and for six-weeks of post delivery care. (These provisions don‘t apply if the physician contract is terminated due to the suspension or revocation of the physician‘s license, or for reasons related to the health, safety, or welfare of enrollees). The provisions discussed above became effective October 1, 2002.
GLOSSARY ABN The abbreviation for the term, Advance Beneficiary Notice. It is a notification that the patient may be expected to pay for tests that Medicare has determined are not medically necessary, based on the information provided by the ordering physician (ICD-9 diagnosis codes and CPT-4 codes). By signing the ABN, the patient understands they will be financially responsible for the test(s) in the event Medicare denies payment to the hospital. AFDC The ―Aid to Families with Dependent Children‖ program (AFDC) provides cash welfare to: (1) needy children who have been deprived of parental support, and (2) certain others in the household of such child. Allowable Charge The maximum charge for which a third party will reimburse a provider for a given service. APC Ambulatory Patient Classification – A system similar to DRGs to be used for outpatients. Bad Debt An account that is uncollectible from a patient, although the patient has or may have the ability to pay. This results in a credit loss for the hospital. These losses may be reflected as an allowance from revenue or as an expense of doing business. In hospitals bad debt accounts are normally outsourced to an external collection agency for enhanced collection activity. Beneficiary Individual who is either using or eligible to use insurance benefits under an insurance contract. An individual who receives benefits from or is covered by an insurance policy. Case Rate An established amount that compensates a hospital for all the care rendered and provided to a patient for a particular diagnosis or procedure. CMS Centers for Medicare and Medicaid Services – A Federal agency within the U.S. Department of Health and Human Services. CMS is responsible for programs such as Medicare, Medicaid, Sate Children‘s Health Insurance Program (SCHIP), HIPAA and CLIA. Formerly known as HCFA. COBRA Consolidated Omnibus Budget Reconciliation Act – Federal law that continues health care benefits for employees whose employment has been terminated. Co-Insurance A cost-sharing requirement under a health insurance policy that provides that the insured will assume a portion or percentage of the costs of covered services.
Contract A legal agreement between a payer and a subscribing group or individual that specifies rates, performance covenants, the relationship among the parties, schedule of benefits and other pertinent conditions. Coordination of Benefits Provision regulating payments to eliminate duplicate coverage when a claimant is covered by multiple group plans. Co-Payment A cost-sharing arrangement in which the HMO enrollee pays a specified flat amount for a specific service. It does not vary with the cost of the service, unlike co-insurance that is based on some percentage of the cost. CPT Current Procedural Terminology – A standardized mechanism of reporting services using numeric codes as established and updated annually by the AMA. Deductible The amount of money or value of certain services, a patient or family must pay before costs are covered by the health plan or insurance company, usually per year. DRG Diagnostic Related Group – A system for classifying hospital stays according to the diagnosis of the medical problem being treated, for the purpose of payment. EMTALA Emergency Medical Treatment and Labor Act – An act pertaining to emergency medical situations. EMTALA requires hospitals to provide emergency treatment to individuals, regardless of insurance status and ability to pay. ERISA Employee Retirement Income Security Act – A Federal act, passed in 1974, which regulates the majority of private pension and welfare group benefit plans in the U.S. Garnishment Filed against a party as a means of collecting a judgment that has been entered. ICD-9-CM International Classification of Diseases, Ninth Revision, and Clinical Modification – The universal coding method used to document the incidence of disease, injury, mortality and illness. A diagnosis and procedure classification system designed to facilitate collection of uniform and comparable health information. Lifetime Reserve Days Under Medicare, each beneficiary has a lifetime reserve of 60 additional days of inpatient hospital services after using 90 days of inpatient hospital services during a spell of illness.
Medicaid Government entitlement program for the poor, blind, aged, disabled or member of families with dependent children. Each state has its own standards for qualification. Medically Needy Persons who are categorically eligible for Medicaid and whose income less accumulated medical bills are below state income limits for the Medicaid program. Medicare A Federal program for the elderly and disabled, regardless of financial status. Medicare Secondary Payer A system that requires providers to identify payers that are primary to Medicare as part of the registration process. Medigap Plans Private health insurance plans that supplement Medicare benefits by covering some costs not paid for by Medicare. Out of Network Benefits With most HMOs, a patient cannot have any services reimbursed if provided by a hospital or doctor who is not in the network. With PPO plans, there may be a provision for reimbursement but usually with a higher co-pay or lower reimbursement. Out of Pocket Expense The maximum amount of money that a patient must pay before his/her insurance will consider benefits at 100%. Out of Pocket Limit A cap placed on out of pocket costs, after which benefits increase to provide full coverage for the rest of the year. Outlier A patient whose length of stay or treatment costs differs substantially from the stays or cost of most other patients in a diagnosis related group. Part A Medicare Refers to the inpatient portion of benefits under the Medicare Program, covering beneficiaries for inpatient hospital, home health, hospice, and limited skilled nursing facility services. Part B Medicare Refers to the outpatient portion of benefits under the Medicare Program, covering beneficiaries for physician services, medical supplies, and other outpatient treatment. Patient Liability The dollar amount that an insured is legally obligated to pay for services rendered by a provider.
Per Diem A pre-established price per day paid for medical services, usually for a type of service, i.e., ICU, surgical or medical. Pre-Certification The processing of obtaining certification or authorization from a health plan for hospital services. Pre-Existing Condition A medical condition developed prior to issuance of a health insurance policy that may result in the limitation of coverage or benefits. Self-Insured A type of insurance arrangement where employers pay for medical claims out of their own funds rather than contracting with an insurance company for coverage. SSI Supplemental Security income – A federal cash assistance program for low-income, aged, blind and disabled individuals established by Title XVI of the Social Security Act. Stop Loss A pre-determined dollar threshold at which a payer may no longer apply its reimbursement schedule. It will convert to a different methodology. Used to protect the hospital from excessive discounts on larger claims. Triage The act of categorizing patients according to acuity and by doing so, determining who needs services first. Uncompensated Care Service provided by hospitals and physicians for which no payment is received from the patient or from third party payers. Workers Compensation A state-mandated program providing insurance coverage for work-related injuries and disabilities.

SOURCES Health Care Billing & Collections: Forms, Checklists & Guidelines (Aspen Health & Administration Development Group The Georgia Chapter of HFMA CPAR Manual Cobb County Clerk‘s Office Web Site Georgia Department of Community Health website





























