Embed Size (px)
Citation preview
© CDISC 2015
CDISC Members Only Webinar-Questionnaire Supplements04 June 2015
1
© CDISC 2015
Agenda• Questionnaire Supplements
Gary Cunningham, The Griesser Group Steve Kopko, CDISC Karin LaPann, Theorem Clinical Research 60 minutes
• Attendee Q&A 30 minutes
• CDISC Education and Events Updates* John Ezzell, CDISC
*After Q&A session & time permitting
2
© CDISC 2015
Question & Answer• ‘Panelist’: QuestionOR• ‘Presentation’: Question
Examples:
Gary: Can operationally-derived values be statistically adjusted?ORCDISC: When can we start registering for the next US Interchange?
3
© CDISC 2015
Note on Webinar ContentAll content included in this presentation is for educational and informational purposes only. References to any specific commercial product, process, or service, or the use of any corporation name are for the information of our members, and do not constitute endorsement, recommendation, or favoring by CDISC or the CDISC community.
4
© CDISC 2015
Presented by Gary Cunningham, Steve Kopko, Karin LaPann
5
Development & Use of Questionnaire Supplements
CDISC Webinar June 4, 2015
© CDISC 2015
QS Sub-Team ActivitiesSDS QS Sub-Team was initiated in 2009 chaired by Gary Cunningham
Mission: Progress the maintenance and implementation of the QS domain standard
2011 Initiation of CDISC Therapeutic Area Standards - Questionnaires requested to be implemented as part of the TA standard requirements
The team was re-focusedGary Cunningham and Steve Kopko appointed as co-chairsMaintain the SDTMIG QS domain document for future versions of the
SDTMIGPrepared a QS Content Guidance DocumentQS Sub-Team Charter createdDirect the development/review/approval of individual Questionnaire
Supplements to the SDTMIGCreated a template approach to develop QS supplements
6
© CDISC 2015
QS Sub-Team ActivitiesCOP 017 CDISC SDTMIG Questionnaire Supplements released 2-Jul-2013
2Q13 COP 017 – Describes the development of QS Supplements by the CDISC community under the direction and guidance of the QS Sub-Team Annotated QS CRFQS Supplement Document Published this documentation for public access
QS Sub-Team volunteers began developing QS supplements
3Q14 - ADaM ADQS sub-team chaired by Nancy Brucken and Karin LaPann Add the ADaM dataset creation steps to the existing published QS Supplements Update to be provided later in this presentation
7
© CDISC 2015
QS Sub-Team Activities 2Q13 Multiple Sclerosis TA Standards Team identified the need for
standard performance and classification measures that differed from the Questionnaires domain definition Functional Tests (FT) domain – SDTMIG 3.3 Batch 1 Public Review Clinical Classifications (CC) domain - SDTMIG 3.3 Batch 2 Public Review Supplement development process is the same as for QS Supplements
Based on COP 017 – to be revised to include FT & CC and the ADaM dataset creation
FDA Clinical Outcome Assessment (COA) website was researched to determine how the CDISC QS/FT/CC domains aligned to their definitions of COAs QS Sub-Team thought QS/FT/CC measures were represented in COAs FDA comment on SDTM Batch 2 public review
Clinical Classifications measures are not always clinical outcome assessments COAs reference additional data types (biomarkers, assessments, AE’s, etc.)
beyond CDISC Questionnaires, Functional Tests and Clinical Classifications
8
© CDISC 2015
QS Sub-Team ActivitiesQS Sub-Team Issue How to combine QS/FT/CC domains into a
single concept?
9
© CDISC 2015
CDISC Definitions QS/FT/CC Domains
10
• Questionnaires (QS)
Questionnaires are named, stand-alone instruments designed to provide an assessment of a concept. They consist of a predetermined set of questions that are conceptually related and have specific answers. Questionnaires have a defined standard structure, format, and content; consist of conceptually related items that are typically scored; and have documented methods for administration and analysis. Most often, questionnaires have as their primary purpose the generation of a quantitative statistic to assess a qualitative concept. They may be documented in the public domain or are owned by a copyright holder.
© CDISC 2015
CDISC Definitions QS/FT/CC Domains
11
• Functional Test (FT) - Provisional
Functional tests are named, stand-alone task-based evaluations designed to provide an assessment on performing a task or activity (.ex mobility, dexterity, and/or cognitive ability). A functional test is not a subjective assessment of how the subject generally performs a task. Rather it is an objective measurement of the performance of the task by the subject in a specific instance. Functional tests have documented methods for administration and analysis and require a subject to perform specific activities that are evaluated and recorded. Most often, functional tests are direct quantitative measurements. They may be documented in the public domain or be owned by a copyright holder.
© CDISC 2015
CDISC Definitions QS/FT/CC Domains
12
• Clinical Classifications (CC) - Draft
The Clinical Classifications domain are named measures whose output is an ordinal or categorical score that serves as a surrogate for, or ranking of, disease status or other physiological or biological status. They are based on observable findings as opposed to rigidly structured patient interviews or patient self-reports. They are sometimes composite scores based on multiple findings that may be found in other SDTM domains such as labs, vital signs, or clinical events.
© CDISC 2015
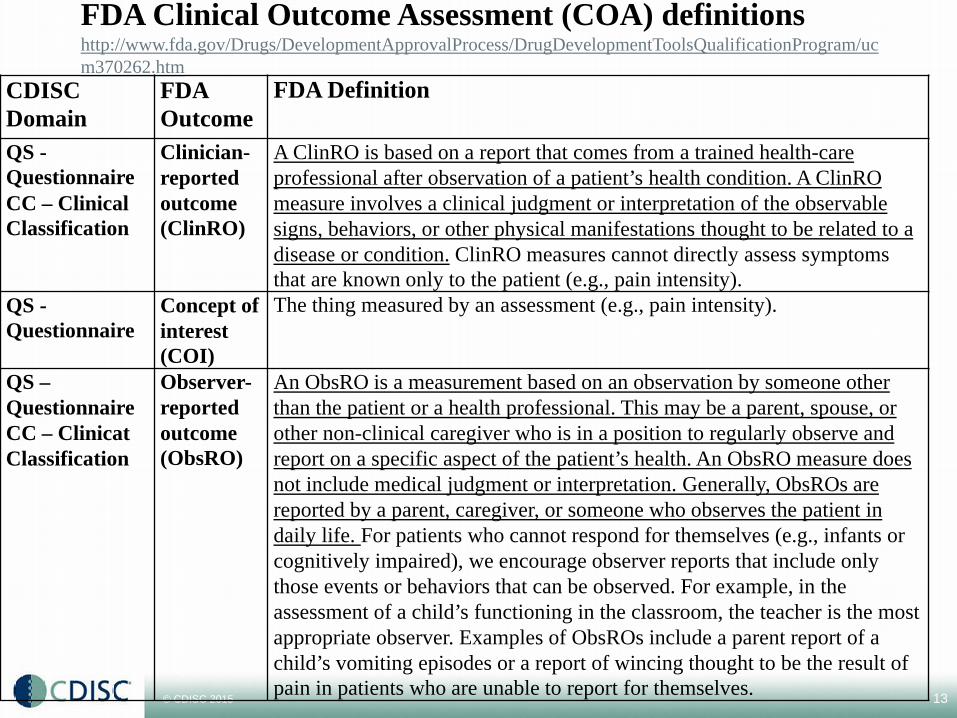
FDA Clinical Outcome Assessment (COA) definitionshttp://www.fda.gov/Drugs/DevelopmentApprovalProcess/DrugDevelopmentToolsQualificationProgram/ucm370262.htm
CDISC Domain
FDA Outcome
FDA Definition
QS -QuestionnaireCC – Clinical Classification
Clinician-reported outcome (ClinRO)
A ClinRO is based on a report that comes from a trained health-care professional after observation of a patient’s health condition. A ClinRO measure involves a clinical judgment or interpretation of the observable signs, behaviors, or other physical manifestations thought to be related to a disease or condition. ClinRO measures cannot directly assess symptoms that are known only to the patient (e.g., pain intensity).
QS -Questionnaire
Concept of interest (COI)
The thing measured by an assessment (e.g., pain intensity).
QS –QuestionnaireCC – Clinicat Classification
Observer-reported outcome (ObsRO)
An ObsRO is a measurement based on an observation by someone other than the patient or a health professional. This may be a parent, spouse, or other non-clinical caregiver who is in a position to regularly observe and report on a specific aspect of the patient’s health. An ObsRO measure does not include medical judgment or interpretation. Generally, ObsROs are reported by a parent, caregiver, or someone who observes the patient in daily life. For patients who cannot respond for themselves (e.g., infants or cognitively impaired), we encourage observer reports that include only those events or behaviors that can be observed. For example, in the assessment of a child’s functioning in the classroom, the teacher is the most appropriate observer. Examples of ObsROs include a parent report of a child’s vomiting episodes or a report of wincing thought to be the result of pain in patients who are unable to report for themselves. 13
© CDISC 2015
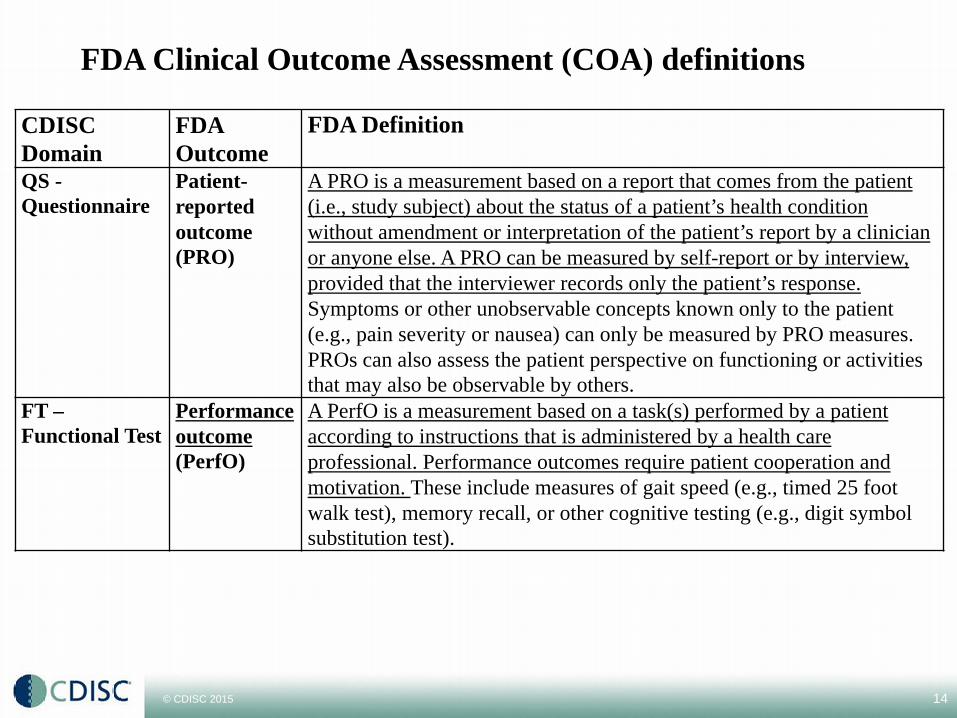
FDA Clinical Outcome Assessment (COA) definitions
CDISC Domain
FDA Outcome
FDA Definition
QS -Questionnaire
Patient-reported outcome (PRO)
A PRO is a measurement based on a report that comes from the patient (i.e., study subject) about the status of a patient’s health condition without amendment or interpretation of the patient’s report by a clinician or anyone else. A PRO can be measured by self-report or by interview, provided that the interviewer records only the patient’s response. Symptoms or other unobservable concepts known only to the patient (e.g., pain severity or nausea) can only be measured by PRO measures. PROs can also assess the patient perspective on functioning or activities that may also be observable by others.
FT –Functional Test
Performance outcome(PerfO)
A PerfO is a measurement based on a task(s) performed by a patient according to instructions that is administered by a health care professional. Performance outcomes require patient cooperation and motivation. These include measures of gait speed (e.g., timed 25 foot walk test), memory recall, or other cognitive testing (e.g., digit symbol substitution test).
14
© CDISC 2015
QS Sub-Team ActivitiesReviewed a single concept strategy moving forward with the SDS Team
SDS WIKI Poll obtained consensus as “Questionnaires, Ratings and Scales” (QRS) Rating: a classification or ranking of someone or something based on a comparative
assessment of their quality, standard, or performance. (Functional Tests (FT) would be a rating)
Scale: an object defined on a set of points (for example real numbers) and used for a wide variety of applications; a succession or progression of steps or degrees; graduated series; series of marks laid down at determinate distances, as along a line, for purposes of measurement or computation; a graduated line, as on a map, representing proportionate size. (Clinical Classifications (CC) would be a scale)
Currently the QS/FT/CC domain are represented for new Questionnaires, Ratings and Scales requirements
New QRS concept does not impact the SDTMIG QS/FT/CC supplements Development of supplements remains based on the steps in COP 017 Same template base approach
15
© CDISC 2015
QuestionnairesToday’s focus will be on Questionnaires
What you need to know about QS Supplements to the SDTMIG
Development process
Community use in creating SDTM datasets
Upcoming ADaM Addendum to QS Supplements
16
© CDISC 2015
QuestionnairesContent
Consists of conceptually related items that solicit responses that are usually scoredEach item contributes to the overall concept assessment. Together the
items represent a cohesive group, where all are essential for assessing the concept and none is intended to be used outside of the constructs of the questionnaire.
Has as its primary purpose the generation of a score to provide an assessment of a specific concept at a certain point in time or interval of timeA score from a questionnaire likely has no relevant meaning outside the
realm of the instrument itself and will require supportive documentation for interpretation and analysis.
Has a defined and documented structure, format, and content for items and any pre-defined responses.
Has documented methods for administration and scoring, and typically methods for analysis and interpretation of results.
•17
© CDISC 2015
QuestionnairesWhat is not a Questionnaire
Data from instruments that consist of items that are not scored, including items that are direct quantitative measurements, should not be submitted in the SDTM QS Domain. Sponsors should choose another appropriate Findings domain model.
patient diary that collects the number of tablets of study medication taken per day
polysomnography study that measures the number of apnea and hypopnea events per hour.
18
© CDISC 2015
QuestionnairesQuestionnaire Sub-Total and Total Scores
CDISC Fundamental DefinitionsOperationally-Derived: An operationally-derived value is one that is
computed at the point of data capture or by the data management systems during study conduct, prior to making data available for analysis. Operationally-derived values are not statistically adjusted in any way due to
missing or ill-conditioned values. Examples: a value computed by an EDC or data management system (e.g., AGE, BMI, a duration, a flag to indicate last non-missing value prior to first dose, a QS total or mean score for a series of questions) or values computed or merged in by a Lab Processing operational system (e.g., values in standard units, lab normal ranges, etc.).
These variables, which are outputs of the data management process and may often be included in SDTM tabulations, should be clearly and consistently derivable based on standard methods. However, while such variables are sometimes inputs to analysis (and may be included in ADAM datasets to enhance traceability), not all operationally-derived values will be suitable for analysis purposes since the derivations would not include methods for statistical adjustment or record selection.
19
© CDISC 2015
QuestionnairesQuestionnaire Sub-Total and Total Scores
CDISC Fundamental DefinitionsAnalysis-Derived: An analysis-derived value is one that is computed after
data capture and is associated with derivation logic that is specified by a statistician and/or statistical programmer. These data are derived for the sole purpose of directly analyzing study data as
per the Protocol/Statistical Analysis Plan (SAP) or for supporting said analyses, and are located in ADaM datasets but not in SDTM tabulations.
As needed, the derivation logic for analysis-derived values will specify how to handle missing or ill-conditioned data values and how to select individual records to use for the derivation.
Analysis-derived values may be represented as a wholly derived record within a dataset
20
© CDISC 2015
QuestionnairesQuestionnaire Sub-Total and Total Scores
CDISC Fundamental DefinitionsAnalysis-Derived:
Examples: a weight-adjusted QS mean score that accounts for the degree of missing responses to individual questions, an imputation of a lab value due to the reporting of the lab value as below or above quantifiable limits, analysis baseline flag/value (e.g., a baseline value that is derived from a subset of values that were collected during a defined period of time, such as the geometric mean of all values prior to first dose), change-from-baseline value, analysis set/population flags, and any other analysis flags.
If the operationally-derived and analysis-derived values differ, then the analysis-derived value is the one used in the analysis for which it was created. In general, the analysis-derived value is more accurate.
21
© CDISC 2015
QuestionnairesQuestionnaire Sub-Total and Total Scores
QSTESTCD/QSTEST terminology is created only if these items are displayed on the CRFConsidered as captured data on CRFAn investigator derived score written on a CRF will be considered a
captured score and not flagged.May be considered operational derived data by sponsor - It is the sponsor's
responsibility to set the --DRVFL flag based on their eCRF process to derive sub-totals and total scores.
When subtotal and total scores are derived by the sponsor, the derived flag (--DRVFL) is set to Y. However, when the subtotal and total scores are received from a central provider or vendor, the value would go into --ORRES and --DRVFL would be null [See Section 4: 4.1.1.8.1, Origin Metadata for Variables].
QSDRVFL will no longer be included in data examples ADaM datasets will define appropriate derivation algorithms for all
analysis derived data according to a Statistical Analysis Plan (SAP)
22
© CDISC 2015
CDISC COP 017CDISC SDTMIG Questionnaire Supplements • Located at CDISC HOME/ABOUT CDISC/Bylaws & Policies
http://www.cdisc.org/bylaws-and-policies
• Purpose This document describes the policies and processes related to the
implementation and maintenance for CDISC SDTMIG Questionnaire Supplements.
This process is coordinated with the CDISC SDTM QRS Sub-Team as a governing body for all QS supplements implemented as a CDISC QS standard.
The implementation involves drafting the controlled terminology and defining questionnaire-specific standardized values for qualifier, timing and result variables to populate the SDTM QS, FT or CC Domain, along with providing examples of use.
© CDISC 2015
COP 017 Sections• Definitions• References and Related Documents are listed under QRS
Implementation Documents on the new QRS web pagehttp://cdisc.org/qrs
QRS Standard Request Form QRS Public Domain Copyright Verification Document CDISC QRS Copyright Letter QRS Supplement Examples
• (Based on appropriate domains, such as QS, FT and CC) QRS Terminology Spreadsheet Example QRS Terminology Naming Rules QRS Supplement QC Checklist v1
© CDISC 2015
COP 017 Sections• Identifying Candidate Questionnaire• CDISC SDS QRS Sub-Team Review Process
QS Owner Permission Approval Process• QS Implementation Process
Obtain the QS CRF QS Terminology Annotate QS CRF with SDTM variables Create an SDTMIG QS Supplement Production Release of QS Supplement and Annotated CRF
© CDISC 2015
Process Flows• QRS Sub-Team Review Process
• Copyright Owner Permission Process
• Supplement Development Process
© CDISC 2015
CDISC QRS Supplements
27
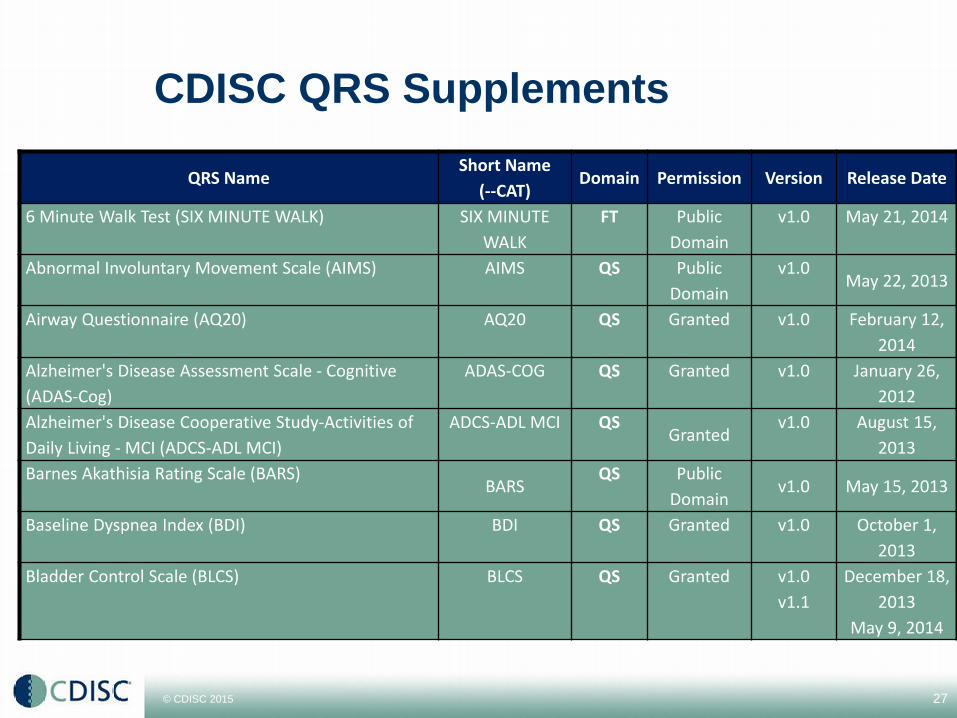
QRS NameShort Name
(--CAT)Domain Permission Version Release Date
6 Minute Walk Test (SIX MINUTE WALK) SIX MINUTE WALK
FT Public Domain
v1.0 May 21, 2014
Abnormal Involuntary Movement Scale (AIMS) AIMS QS Public Domain
v1.0May 22, 2013
Airway Questionnaire (AQ20) AQ20 QS Granted v1.0 February 12, 2014
Alzheimer's Disease Assessment Scale - Cognitive (ADAS-Cog)
ADAS-COG QS Granted v1.0 January 26, 2012
Alzheimer's Disease Cooperative Study-Activities of Daily Living - MCI (ADCS-ADL MCI)
ADCS-ADL MCI QSGranted
v1.0 August 15, 2013
Barnes Akathisia Rating Scale (BARS)BARS
QS Public Domain
v1.0 May 15, 2013
Baseline Dyspnea Index (BDI) BDI QS Granted v1.0 October 1, 2013
Bladder Control Scale (BLCS) BLCS QS Granted v1.0v1.1
December 18, 2013
May 9, 2014
© CDISC 2015
QRS Sub-Team ActivitiesCore Sub-Team members and sponsor volunteers are implementing
QS/FT/CC Supplements based on resource availability Priority for Core Sub-Team are Supplements required for TA User
Guides. “Extended” team of volunteers primarily works on backlog.(Business
Decisions, Boehringer-Ingelheim, new volunteers) – backlog supplements TA Projects identify supplement implementers to expedite the process
Examples: AD, PD, MS, TBI, Influenza, Schizophrenia, COPD, Hepatitis C, Dyslipidemia
Coordinate with the ADQS team on ADaM addendums to each published supplement Nancy Brucken & Karin LaPann co-leads ADQS Update
28
© CDISC 2015
ADQS ADaM Sub-TeamADQS team… who are we?
The sub-team is made of ADaM team members plus any SDS volunteers from other CDISC and SDS groups willing to put the in the time to create these documents
Additional members recruited from the PhUSE organization
Purpose is to develop the ADaM addendums to the Questionnaire, Ratings and Scales Supplements already defined for SDTM by the QRS team
29
© CDISC 2015
ADQS Sub-Team MethodologyStarting with questionnaires that the QRS team
has obtained copyright approval for, or are public domain
Only defining instruments that have been defined by the QRS team first
Only looking at instruments that require one or more added rows for a score calculation
Adding an ADaM section to the existing QS guides, rather than creating a separate document to provide a single place for end-to-end documentation.
The Geriatric Depression Scale Short Form (GDS-SF) was chosen as the first questionnaire to work on
30
© CDISC 2015
ADQS ADaM Section OutlineThe ADaM instructions follow the QS instructions starting with Part 2. Here is the general outline:1. General considerations2. Published Rules and References3. Published Scoring Software4. Sample Table Shells annotated with ADaM
variables5. Sample SAP text6. Analysis Data Set Metadata, mapping
instructions7. Transposed/Reversed Questions8. Example Analysis Data Set9. Key data checks
31
© CDISC 2015
ADQS Best PracticesInclude PARCAT1, mapped to QS.QSCATPARCAT2 is allowed if needed, and should
contain the subscale name.Create Controlled Terminology for ADaM for the
Scale Scores and Sub-scale score PARAMCD/ PARAM.
Bring QSTEST and QSTESTCD directly into PARAM and PARAMCD for original data rows for maximum traceability back to QS
Set ANLzzFL and ABLFL only on scale score rowsDon’t include the fragment QS FT or CC in the
ADaM dataset namesDocument the scoring rules in your define.xml
32
© CDISC 2015
ADQS Current StatusThe GDS-SF (Geriatric DS Short Form) is in final
draft and has been submitted to the ADaM Leadership Team (ALT) for review and approval.
Starting on next set of questionnaires. These were requested by the therapeutic area user groups (TAUGS): BARS BPRS-A CHART-SF (Interview and paper forms) GAD-7
Updating the QRS (formerly COA) documentation to add the ADaM process
33
© CDISC 2015
QRS Sub-Team Activities (continued)
Team developed and published over 90 QRS Supplements
Team continually updating a QRS “FAQ” document for best practices when developing QRS Supplements and annotated CRFs
CDISC Education Department is researching an online QS Supplement course
Continue to publish 6-10 QRS Supplements per quarter Make TA Standards required Standard Measure Supplements a priority Eliminate backlog with new volunteers
34
© CDISC 2015
Additional QRS Sub-Team Activities
Address various QRS issues: Use --METHOD for response option types? Create a Domain-specific METHOD
codelist? Where do publisher question codes belong? Finalize guidance on derived individual question and total “scores”. What metadata needs to be in the submission? How to represent metadata in the submission?
SDTMIG v3.3 updates
35
© CDISC 2015
QRS Sub-Team Membership
36
QS Sub-Team MembersRole Name CompanyCo-Leader QS Gary Cunningham The Griesser GroupCo-Leader QS Steve Kopko CDISCCo-Leader FT/CC Jon Neville Critical Path InstituteCo-Leader FT/CC Bess LeRoy Critical Path InstituteCoordinator Dana Booth CDISC
Member Amy Palmer CDISCMember Bernice Yost CDISCMember Bob Stafford Critical Path InstituteMember Cliff Reinhardt UCB BioSciences, Inc.Member Diane Corey Critical Path InstituteMember Donna Sattler IndependentMember Eanna Kiely ParexelMember Emily Hartley Critical Path InstituteMember Fred Wood AccentureMember Janet Reich AmgenMember Janet Siani ShireMember Yun Lu KAI - ResearchMember Kristin Kelly AccentureMember Kim Minkalis IndependentMember Madhavi Vemuri Johnson & JohnsonMember Nate Freimark The Griesser GroupMember Pat Wozniak Advanced ClinicalMember Richard Lewis AccentureMember Rohit Dhanjal GenzymeMember Sandy Lei Johnson & JohnsonMember Tom Guinter Independent
© CDISC 2015
Q&A
© CDISC 2015
CDISC Education Events Announcements
38

© CDISC 2015
Upcoming USA Public Course Events
42
Location Dates Courses Offered
Online RegistrationDeadline
Early RegistrationDiscounts
Host
Minneapolis, MN
23-26 June 2015
SDTM for Med. Devices, CDASH, CT
Expired
Durham, NC 27-31 July 2015
SDTM, ADaM 27 June 2015
Gaithersburg, MD
1-4 Sep 2015 SDTM, CDASH, ADaM
Expired
Seattle, WA 6-9 Oct 2015 SDTM, ADaM,ODM/Define-XML
USA InterchaneChicago, IL
9-13 Nov 2015
TBD
Registration deadline indicates online deadline. Offline registration deadlines for each event can be found here. Additional 2015 public training events can be found @ http://cdisc.org/public-courses.

© CDISC 2015
Upcoming Europe Public Course Events
43
Location Dates Courses Offered
OnlineRegistrationDeadline
Early RegistrationDiscounts
Host
Eschborn(Frankfurt), Germany
28-31 Jul 2015
SDTM, CDASH, ADaM
28 June 2015
Brussels, Belgium
7-10 Sep 2015
SDTM, CDASH, ADaM
7 August 2015
Registration deadline indicates online deadline. Offline registration deadlines for each event can be found here. Additional 2015 public training events can be found @ http://cdisc.org/public-courses.

© CDISC 2015
Upcoming Asia Public Course Events
44
Location Dates Courses Offered
Online RegistrationDeadline
Early RegistrationDiscounts
Host
Japan Interchange
22-26 Jun 2015
SDTM, CDASH, ODM, Dataset-XML, Define-XML, ADaM
8 June 2015
Guangzhou, China
8-11 Sep 2015
SDTM, CDASH, ADaM
8 August 2015
Guangdong Provincial Hospital of Chinese Medicine
Registration deadline indicates online deadline. Offline registration deadlines for each event can be found here. Additional 2015 public training events can be found @ http://cdisc.org/public-courses.
© CDISC 2015
Next Members Only Webinar• Agenda:
ADaM Validation Checks
• Date: 16 July 2015, 11:00-12:30 PM EST
• Speakers: Shelley Dunn, d-Wise Ed Lombardi, Agility Clinical
• Register here.Webinar details also at www.cdisc.org/webinars
45
© CDISC 2015
CDISC’s vision is to:Inform Patient Care & Safety Through Higher Quality Medical Research
46
Any more questions?
Thank you for attending this webinar.

© CDISC 2015
CDISC Members Drive Global Standards
Thank you for your support!
47





























