Upload
huber-munoz
View
221
Download
0
Embed Size (px)
Citation preview
8/2/2019 Ce to Acidosis Diabetic A
1/23
DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001 131
Diabetic ketoacidosis (DKA) and hyper-osmolar hyperglycemic state (HHS)are two of the most serious acute
complications of diabetes. These hypergly-cemic emergencies continue to be impor-tant causes of morbidity and mortalityamong patients with diabetes in spite of
major advances in the understanding oftheir pathogenesis and more uniform agree-ment about their diagnosis and treatment.The annual incidence rate for DKA esti-mated from population-based studiesranges from 4.6 to 8 episodes per 1,000patients with diabetes (1,2), and in morerecent epidemiological studies in the U.S., itwas estimated that hospitalizations for DKAduring the past two decades are increasing(3). Currently, DKA appears in 49% of allhospital discharge summaries amongpatients with diabetes (4,5). The incidenceof HHS is difficult to determine because of
the lack of population-based studies and themultiple combined illnesses often found inthese patients. In general, it is estimated thatthe rate of hospital admissions due to HHSis lower than the rate due to DKA andaccounts for 1% of all primary diabeticadmissions (46).
Treatment of patients with DKA andHHS uses significant health care resources,which increases health care costs. In 1983,the cost of hospitalization for DKA in
Rhode Island for 1 year was estimated to be$225 million (2). It was recently reportedthat treatment of DKA episodes representsmore than one of every four health caredollars spent on direct medical care foradult patients with type 1 diabetes and forone of every two dollars in those patients
experiencing multiple episodes of ketoaci-dosis (7). Based on an annual average of100,000 hospitalizations for DKA in theU.S. (4) and estimated annual mean med-ical care charges of$13,000 per patientexperiencing a DKA episode (7), the annualhospital cost for patients with DKA mayexceed $1 billion per year.
Mortality rates, which are 5% in DKAand15% in HHS (46,812,13), increasesubstantially with aging and the presence ofconcomitant life-threatening illnesses. Simi-lar outcomes of treatment of DKA have beennoted in both community and teaching hos-
pitals (1416), and outcomes have not beenaltered by whether the managing physicianis a family physician, general internist, houseofficer with attending supervision, orendocrinologist, so long as standard writtentherapeutic guidelines are followed (17,18).
This technical review aims to presentupdated recommendations for manage-ment of patients with hyperglycemic crisesbased on the pathophysiological basis ofthese conditions.
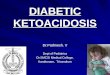
DEFINITION OF TERMS,CLASSIFICATION, ANDCRITERIA FOR DIAGNOSIS DKA consists of the biochemical triad ofhyperglycemia, ketonemia, and acidemia(Fig. 1). As indicated, each of these featuresby itself can be caused by other metabolicconditions (19). Although it has been diffi-cult to classify the degree and severity ofDKA, we propose a working classificationthat may be useful for management of sucha condition. Table 1 provides an empiricalclassification for DKA and HHS, with thecaveat that the severity of illness will be
influenced by the presence of concomitantintercurrent illnesses.The terms hyperglycemic hyperosmo-
lar nonketotic coma and hyperglycemichyperosmolar nonketotic state have beenreplaced with the term hyperglycemichyperosmolar state (HHS) (20) to reflectthe facts that 1) alterations of sensoria mayoften be present without coma and2) thehyperosmolar hyperglycemic state mayconsist of moderate to variable degrees ofclinical ketosis as determined by the nitro-prusside method. As indicated, the degreeof hyperglycemia in DKA is quite variable
and may not be a determinant of the sever-ity of DKA. Serum osmolality has beenshown to correlate significantly with men-tal status in DKA and HHS (5,6,2023) andis the most important determinant of men-tal status, as demonstrated by several stud-ies. Table 2 provides estimates of typicaldeficits of water and electrolytes in DKAand HHS (20,24,25).
PRECIPITATING EVENTS Although it has been repeatedly shown thatinfection is a common precipitating event inDKA and HHS in this country and abroad
(4,12), recent studies suggest that omissionof insulin or undertreatment with insulinmay be the most important precipitatingfactor in urban African-American popula-tions (5,26). Table 3 summarizes variousstudies (2,5,6,2730) describing precipitat-ing events for DKA. It is important to notethat up to 20% of patients may present inthe emergency room with either DKA orHHS without a previous diagnosis of dia-betes (Table 3). In the African-Americanpopulation, DKA has been increasingly
From the Division of Endocrinology (A.E.K., G.E.U., M.B.M.), University of Tennessee, and the Departmentof Nephrology (B.M.W.), Veterans Administration Hospital, Memphis, Tennessee; the Division of Endocrinol-
ogy (E.J.B.), University of Virginia, Charlottesville, Virginia; the College of Medicine (R.A.K.), University ofSouth Alabama, Mobile, Alabama; and the Department of Pediatrics (J.I.M.), University of South Florida,Tampa, Florida.
Address correspondence and reprint requests to Abbas E. Kitabchi, PhD, MD, University of Tennessee,Memphis, Division of Endocrinology, 951 Court Ave., Room 335M, Memphis, TN 38163. E-mail: [email protected].
This paper was peer-reviewed, modified, and approved by the Professional Practice Committee, Octo-ber 2000.
Abbreviations:AaO2, alveolar-to-arteriolar oxygen; AKA, alcoholic ketoacidosis; ARDS, adult respiratorydistress syndrome; BUN, blood urea nitrogen; CPT, carnitine palmitoyl-transferase; CSF, cerebrospinal fluid;DKA, diabetic ketoacidosis; FFA, free fatty acid; HHS, hyperosmolar hyperglycemic state; IRI, immunoreac-tive insulin; PaO2, arteriolar partial pressure of oxygen; RDKA, recurrent DKA.
A table elsewhere in this issue shows conventional and Systme International (SI) units and conversionfactors for many substances.
Management of Hyperglycemic Crises inPatients With Diabetes
T E C H N I C A L R E V I E W
ABBAS E. KITABCHI, PHD, MD
GUILLERMO E. UMPIERREZ, MDMARY BETH MURPHY, RN, MS, CDE, MBAEUGENEJ. BARRETT, MD, PHD
ROBERT A. KREISBERG, MD
JOHN I. MALONE, MDBARRY M. WALL, MD
R e v i e w s / C o m m e n t a r i e s / P o s i t i o n S t a t e m e n t s
8/2/2019 Ce to Acidosis Diabetic A
2/23
132 DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001
Technical Review
noted in newly diagnosed obese type 2 dia-betic patients (5,26,31). Therefore, the con-cept that the presence of DKA in type 2diabetes is a rare occurrence is incorrect.
The most common types of infectionsare pneumonia and urinary tract infection,accounting for 3050% of cases (Table 4).Other acute medical illnesses as precipitatingcauses include alcohol abuse, trauma, pul-monary embolism, and myocardial infarc-tion, which can occur both in type 1 and 2diabetes (6). Various drugs that alter carbo-
hydrate metabolism, such as corticosteroids,pentamidine, sympathomimetic agents, and- and -adrenergic blockers, and excessiveuse of diuretics in the elderly may also pre-cipitate the development of DKA and HHS.
The recent increased use of continuoussubcutaneous insulin infusion pumps thatuse small amounts of short-acting insulinhas been associated with an incidence ofDKA that is significantly increased over theincidence seen with conventional methodsof multiple daily insulin injections, in spiteof the fact that most of the mechanical prob-lems with insulin pumps have been resolved
(6,3234). In the Diabetes Control andComplications Trial, the incidence of DKA inpatients on insulin pumps was abouttwofold higher than that in the multiple-injection group over a comparable timeperiod (35). This may be due to the exclu-sive use of short-acting insulin in the pump,which if interrupted leaves no reservoir ofinsulin for blood glucose control.
Psychological factors and poor compli-ance, leading to omission of insulin therapy,are important precipitating factors for recur-
rent ketoacidosis. In young female patientswith type 1 diabetes, psychological prob-lems complicated by eating disorders maybe contributing factors in up to 20% of casesof recurrent ketoacidosis (36,37). Factorsthat may lead to insulin omission in youngerpatients include fear of weight gain withgood metabolic control, fear of hypogly-cemia, rebellion against authority, and stressrelated to chronic disease (36). Noncompli-ance with insulin therapy has been found tobe the leading precipitating cause for DKA in
urban African-Americans and medicallyindigent patients (5,26). In addition, a recentstudy showed that diabetic patients withouthealth insurance or with Medicaid alonehad hospitalization rates for DKA that weretwo to three times higher than the rate indiabetic individuals with private insurance
(38). In addition to the above-mentionedprecipitating causes of DKA and HHS, thereare numerous additional medical proceduresand medications that may precipitate HHS.Some of these drugs trigger the developmentof hyperglycemic crises by causing areversible deficiency in insulin action orinsulin secretion (e.g., diuretics, -adrener-gic blockers, and dilantin), whereas otherconditions cause hyperglycemic crises byinducing insulin resistance (e.g., hypercorti-solism, acromegaly, and thyrotoxicosis).Some of the major causes of HHS areincluded in Table 4 (20).
PATHOGENESIS Although thepathogenesis of DKA is better understoodthan that of HHS, the basic underlyingmechanism for both disorders is a reduc-tion in the net effective concentration ofcirculating insulin, coupled with a con-comitant elevation of counterregulatorystress hormones (glucagon, catecho-lamines, cortisol, and growth hormone).Thus, DKA and HHS are extreme manifes-tations of impaired carbohydrate regula-tion that can occur in diabetes. Althoughmany patients manifest overlapping meta-bolic clinical pictures, each condition canalso occur in relatively pure form. Inpatients with DKA, the deficiency in insulincan be absolute, or it can be insufficient rel-ative to an excess of counterregulatory hor-mones. In HHS, there is a residual amount
of insulin secretion that minimizes ketosisbut does not control hyperglycemia. Thisleads to severe dehydration and impairedrenal function, leading to decreased excre-tion of glucose. These factors coupled withthe presence of a stressful condition resultin more severe hyperglycemia than that
Figure 1The triad of DKA (hyperglycemia, acidemia, and ketonemia) and other conditions withwhich the individual components are associated. From Kitabchi and Wall (19).
Table 1Diagnostic criteria for DKA and HHS
DKA
Mild Moderate Severe HHS
Plasma glucose (mg/dl) 250 250 250 600Arterial pH 7.257.30 7.007.24 7.00 7.30Serum bicarbonate (mEq/l) 1518 1015 10 15Urine ketones* Positive Positive Positive SmallSerum ketones* Positive Positive Positive SmallEffective serum osmolality Variable Variable Variable 320(mOsm/kg)
Anion gap 10 12 12 12Alteration in sensoria Alert Alert/drowsy Stupor/coma Stupor/Coma
or mental obtundation
*Nitroprusside reaction method; calculation: 2[measured Na (mEq/l)] glucose (mg/dl)/18; calculaton:(Na) (Cl HCO3
) (mEq/l). See text for details.
8/2/2019 Ce to Acidosis Diabetic A
3/23
seen in DKA. In addition, inadequate fluidintake contributes to hyperosmolarity with-out ketosis, the hallmark of HHS. Thesepathogenic topics will be discussed undervarious subheadings.
Carbohydrate metabolismWhen insulin is deficient (absolute or rela-tive), hyperglycemia develops as a result ofthree processes: increased gluconeogenesis,accelerated glycogenolysis, and impairedglucose utilization by peripheral tissues(3944). Increased hepatic glucose pro-duction results from the high availability ofgluconeogenic precursors, such as aminoacids (alanine and glutamine; as a result ofaccelerated proteolysis and decreased pro-
tein synthesis) (45), lactate (as a result ofincreased muscle glycogenolysis), and glyc-erol (as a result of increased lipolysis), andfrom the increased activity of gluco-
neogenic enzymes. These include PEPCK,fructose-1,6-biphosphatase, pyruvate car-boxylase, and glucose-6-phosphatase,which are further stimulated by increasedlevels of stress hormones in DKA and HHS(4650). From a quantitative standpoint,increased glucose production by the liverand kidney represents the major patho-genic disturbance responsible for hyper-glycemia in these patients, and gluconeo-genesis plays a greater metabolic role thanglycogenolysis (4650,51). Although thedetailed biochemical mechanisms for glu-coneogenesis are well established, themolecular basis and the role of counterreg-ulatory hormones in DKA are the subject ofdebate; very few studies have attempted toestablish a temporal relationship betweenthe increase in the level of counterregula-tory hormones and the metabolic alter-ations in DKA (52). However, studies ofinsulin withdrawal in previously controlledpatients with type 1 diabetes indicate that acombination of increased catecholaminesand glucagon (and a decreased level of freeinsulin) in a well-hydrated individual maybe the initial event (41,43,5356). Fur-thermore, in the absence of dehydration,vomiting, or other stress situations, ketosisis usually mild, while glucose levelsincrease with simultaneous increases inserum potassium (56).
Animal studies have shown that cate-cholamines stimulate glycogen phosphory-
lase via -receptor stimulation and subse-quent production of cAMP-dependentprotein kinase. Decreased insulin in thepresence of an ambient level of glucagon,
which is usually higher in diabetic than innondiabetic individuals, leads to a highglucagon-to-insulin ratio, which inhibitsproduction of an important metabolic regu-lator: fructose-2,6-biphosphate. Reductionof this intermediate stimulates the activity offructose-1,6-biphosphatase (an enzyme thatconverts fructose-1,6-biphosphate to fruc-tose-6-phosphate) and inhibits phospho-fructokinase, the rate-limiting enzyme in theglycolytic pathway (57). Gluconeogenesis isfurther enhanced through stimulation ofPEPCK by the increased ratio of glucagon toinsulin in the presence of increased cortisolin DKA (5759). In addition, the rapiddecrease in the level of available insulin alsoleads to decreased glycogen synthase. Theseinteractions can be summarized as follows:
glucagon/insulin catecholamines cAMP cAMP-dependent proteinkinase fructose-2,6-biphosphate
glycolysis and gluconeogenesis andglycogen synthase
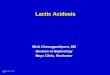
The final step of glucose productionoccurs by conversion of glucose-6-phos-phate to glucose, which is catalyzed byanother rate-limiting enzyme of gluconeo-genesis, hepatic glucose-6-phosphatase,which is stimulated by increased catabolichormones and decreased insulin levels.These metabolic alterations are depicted inFig. 2. Major substrates for gluconeogenesis
are lactate, glycerol, alanine (in the liver),and glutamine (in the kidney). Alanine andglutamine are provided by the process ofexcess proteolysis and decreased protein
DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001 133
Kitabchi and Associates
Table 2Typical total body deficits of waterand electrolytes in DKA and HHS
DKA HHS
Total water (liters) 6 9Water (ml/kg)* 100 100200Na (mEq/kg) 710 513Cl (mEq/kg) 35 515K (mEq/kg) 35 46PO4 (mmol/kg) 57 37Mg2 (mEq/kg) 12 12Ca2 (mEq/kg) 12 12
*Per kilogram of body weight. From Ennis et al. (20)and Kreisberg (24).
Table 3Precipitating factors for DKA
Concomitant Inadequate OtherNumber of cardiovascular insulin treatment New medical
Study location/dates/reference episodes Infections disease or noncompliance onset illness Unknown
Frankfurt, Germany/Petzold 472 19 6 38
et al. (27)Birmingham, U.K./19681972/ 258 28 3 23
Soler et al. (28)Erfurt, Germany/19701971/ 133 35 4 21
Panzram (29)Basel, Switzerland/19681978/ 163 56 5 31
Berger et al. (30)Rhode Island/19751979/Faich 152 43 26 et al. (2)
Memphis, TN/19741985/ 202 38 28 22 10 4Kitabchi et al. (6)
Atlanta, GA/19931994/ 144 28 41 17 10 4Umpierrez et al. (5)
Data are % of all cases. , complete data on these items were not given because total numbers did not reach 100%.
8/2/2019 Ce to Acidosis Diabetic A
4/23
synthesis, which occurs as a result ofincreased catabolic hormones and decreasedinsulin (45,60). In DKA and HHS, hyper-
glycemia causes an osmotic diuresis due toglycosuria, resulting in loss of water andelectrolytes, hypovolemia, dehydration, anddecreased glomerular filtration rate, whichfurther increase the severity of hypergly-cemia (see below). Although increasedhepatic gluconeogenesis is the main mecha-nism of hyperglycemia in severe ketoacido-sis, recent studies have shown a significantportion of gluconeogenesis may be accom-plished via the kidney (51). Decreasedinsulin availability and partial insulin resis-
tance, which exist in DKA and HHS by dif-ferent mechanisms (see below), also con-tribute to decreased peripheral glucoseutilization and add to the overall hypergly-cemic state in both conditions.
Lipid and ketone metabolismThe increased production of ketones inDKA is the result of a combination of
insulin deficiency and increased concentra-tions of counterregulatory hormones, par-ticularly epinephrine, which lead to theactivation of hormone-sensitive lipase inadipose tissue (6164). The increased activ-ity of tissue lipase causes a breakdown oftriglyceride into glycerol and free fatty acids(FFAs). Although glycerol is used as a sub-strate for gluconeogenesis in the liver andthe kidney, the massive release of FFAsassumes pathophysiological predominancein the liver, the FFAs serving as precursors
of the ketoacids in DKA (44,63). In theliver, FFAs are oxidized to ketone bodies, aprocess predominantly stimulated byglucagon. Increased concentration ofglucagon in DKA reduces the hepatic levelsof malonyl-CoA by blocking the conversionof pyruvate to acetyl-CoA through inhibi-tion of acetyl-CoA carboxylase, the first rate-limiting enzyme in de novo fatty acid
synthesis (6366). Malonyl-CoA inhibitscarnitine palmitoyl-transferase (CPT)-I, therate-limiting enzyme for transesterificationof fatty acyl-CoA to fatty acyl-carnitine,allowing oxidation of fatty acids to ketonebodies. CPT-I is required for movement ofFFA into the mitochondria, where fatty acidoxidation takes place. The increased fattyacyl-CoA and CPT-I activity in DKA leads toincreased ketogenesis in DKA (67,68). Inaddition to increased production of ketonebodies, there is evidence that clearance of
134 DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001
Technical Review
Table 4Predisposing or precipitating factorsfor HHS
Acute illnessAcute infection (3260%)
PneumoniaUrinary tract infectionSepsis
Cerebral vascular accidentMyocardial infarctionAcute pancreatitis
Acute pulmonary embolusIntestinal obstructionDialysis, peritonealMesenteric thrombosisRenal failureHeat strokeHypothermiaSubdural hematomaSevere burns
EndocrineAcromegalyThyrotoxicosisCushings syndrome
Drugs/therapy-Adrenergic blockersCalcium-channel blockersChlorpromazine
ChlorthalidoneCimetidineDiazoxideDiureticsEncainideEthacrynic acid
Immunosuppressive agentsL-asparaginaseLoxapinePhenytoinPropranololSteroidsTotal parenteral nutritionPreviously undiagnosed diabetes
From the review by Ennis et al. (20).
Figure 2Proposed biochemical changes that occur during DKA leading to increased gluconeogenesisand lipolysis and decreased glycolysis. Note that lipolysis occurs mainly in adipose tissue. Other eventsoccur primarily in the liver (except some gluconeogenesis in the kidney). Lighter arrows indicate inhib-ited pathways in DKA. F-6-P, fructose-6-phosphate; G-(X)-P, glucose-(X)-phosphate; HK, hexokinase;HMP, hexose monophosphate; PC, pyruvate carboxylase; PFK, phosphofructokinase; PEP, phospho-enolpyruvate; PK, pyruvate kinase; TCA, tricarboxylic acid; TG, triglycerides. From Kitabchi et al. (6).
8/2/2019 Ce to Acidosis Diabetic A
5/23
ketones is decreased in patients with DKA(6971). This decrease may be due to lowinsulin concentration, increased glucocorti-coid level, and decreased glucose utilizationby peripheral tissues (72).
The role of individual counterregula-tory hormones in the process of ketogenesisis reviewed below. Some of the first studiesdemonstrating net ketogenesis by thehuman liver in patients with DKA were donenearly 50 years ago (39). By combining mea-surements of arterial and hepatic venousketone concentrations and estimation ofsplanchnic blood flow in patients with DKA,the liver was demonstrated to produce largeamounts of ketones, and insulin treatmentwas demonstrated to reduce ketone pro-duction promptly. These findings were sub-sequently confirmed and extended withimproved analytical techniques (73). To ourknowledge, rates of ketogenesis have notbeen measured in hyperosmolar nonketoticpatients using either organ balance or iso-topic methods. Subsequent work usingtracer methods (41,74) has demonstratedthat even brief withdrawal of insulin fromtype 1 diabetic patients results in promptdevelopment of ketosis. Insulin withdrawalfrom diabetic patients, however, leads tocomplex changes in circulating concentra-tions of many stress hormones. As a result,it is difficult to dissect the relative contribu-tions of insulin deficiency and stress hor-mone excess in the regulation of ketogenesis.
This is well illustrated in studies examiningglucagon action. Numerous in vitro andsome in vivo studies have demonstrated apotent role for glucagon in the stimulation ofketogenesis. However, some of these studieshave used very high glucagon concentra-tions, and their physiological significancehas been questioned. In a recent study inwhich blood glucose concentrations werecarefully controlled (to eliminate suppressiveeffects of hyperglycemia on lipolysis), alipolytic effect of glucagon was demon-strated (75). Another human study (76)demonstrated modest increases in ketogen-
esis when plasma glucagon was increased ininsulin-deficient subjects. In contrast withthe somewhat equivocal actions of physio-logical or near-physiological concentrationsof glucagon, cortisol appears to have a morepredictable stimulatory action on ketogene-sis (77,78). This may result from both effectson peripheral lipolysis and increased supplyof FFAs, as well as from direct hepatic effects.
Growth hormone may also play aprominent role in ketogenesis. Even mod-est physiological doses of growth hormone
can markedly increase circulating levels ofFFAs and ketone bodies (79,80). Becausethese changes with growth hormoneadministration are observed within 60 min,
increased ketogenesis appears to be theresult of the action of growth hormoneitself rather than locally generated IGF-1. Ithas been reported that in patients with type1 diabetes, the administration of growthhormone leads to significant increases inFFAs, ketone bodies, and glucose concen-trations (81).
Adrenergic stimulation can also increaselipolysis and hepatic ketogenesis. Epineph-rine secretion by the adrenal medulla ismarkedly enhanced in DKA (Table 5). Invitro, epinephrine has a marked effect toincrease lipolysis in adipocytes. In vivo, epi-
nephrine can increase plasma concentra-tions of FFAs, at least when insulin deficiencyis present. In addition, epinephrine facili-tates hepatic ketogenesis directly (82,83).Norepinephrine at concentrations thatapproximate those seen in the synaptic cleftstimulates lipolysis by adipocytes andenhances ketogenesis (84,85).
In addition to the individual effects ofstress hormones, infusion of combinationsof counterregulatory hormones has beenobserved to have synergistic effects when
compared with those seen with single hor-mone infusions (86,87). Indeed, in the set-ting of fixed levels of insulin, infusingmixtures of stress hormones to reach high
physiological/severe stress levels, can pre-cipitate marked increases in lipolysis andketogenesis (44,67). Spontaneous DKA ischaracterized by simultaneous elevations ofmultiple insulin-antagonizing (counterreg-ulatory) hormones (6,8890) in the face ofreduced insulin, which brings about thealtered metabolic profiles seen in DKA.Thus, DKA is analogous to a fasting state,where ketosis is accompanied by elevationsof counterregulatory hormones and reduc-tion of insulin but to a lesser degree than inDKA. The condition in DKA has beenreferred to as a superfasted state (91).
Having suggested that stress hormoneseither singly or in combination are majorcontributors to ketogenesis and the devel-opment of the acidotic state in DKA, thequestion arises whether HHS differs fromDKA with regard to stress hormone secre-tion. There are surprisingly few dataregarding this issue. Reduced concentra-tions of FFAs, cortisol, and growth hor-mone (92) and reduced levels of glucagonhave been demonstrated in HHS relative toDKA (93). In another study, the concentra-
DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001 135
Kitabchi and Associates
Table 5Admission biochemical data in patients with HHS or DKA
Parameters measured HHS DKA
Glucose (mg/dl) 930 83 616 36Na (mEq/l) 149 3.2 134 1.0K (mEq/l) 3.9 0.2 4.5 0.13BUN (mg/dl) 61 11 32 3Creatinine (mg/dl) 1.4 0.1 1.1 0.1pH 7.3 0.03 7.12 0.04Bicarbonate (mEq/l) 18 1.1 9.4 1.43--hydroxybutyrate (mmol/l) 1.0 0.2 9.1 0.85Total osmolality* 380 5.7 323 2.5IRI (nmol/l) 0.08 0.01 0.07 0.01C-peptide (nmol/l) 1.14 0.1 0.21 0.03FFA (nmol/l) 1.5 0.19 1.6 0.16Human growth hormone (ng/ml) 1.9 0.2 6.1 1.2Cortisol (ng/ml) 570 49 500 61.IRI (nmol/l) 0.27 0.05 0.09 0.01C-peptide (nmol/l) 1.75 0.23 0.25 0.05Glucagon (pg/ml) 689 215 580 147
Catecholamines (ng/ml) 0.28 0.09 1.78 0.4Growth hormone (ng/ml) 1.1# 7.9# Gap (anion gap 12) (mEq/l) 11 17
Data are means SEM. From Chupin et al. (95). *According to the formula 2(Na K) urea (mmol/l) glucose (mmol/l); values following intravenous administration of tolbutamide; from Lindsey et al. (93);from Kitabchi and Fisher (23); from Zadik et al. (219) in children with nonketotic hyperglycemia; fromEnnis et al. (20); #from Gerich et al. (92).
8/2/2019 Ce to Acidosis Diabetic A
6/23
tions of glucagon, cortisol, growth hor-mone, epinephrine, and norepinephrinewere measured in patients presenting withacute decompensation of their diabetes(94). Some subjects were hyperglycemicwith little or no ketosis, whereas otherswere frankly ketoacidotic. In this study, noclear-cut differences between hormonal lev-els in DKA and those in HHS could beidentified. However, there were significantpositive correlations between degree ofketonemia and plasma concentrations ofgrowth hormone and FFAs, and there wasa negative correlation with serum C-pep-tide. Glucagon and cortisol concentrationscorrelated well with plasma glucose, butnot with degree of ketonemia. This studypresents correlative data, but does notestablish causal relationships between hor-monal levels and alterations of metabolicpathways; hence, it does not settle the con-troversy of hormonal status in DKA andHHS. In another study, 12 HHS and 22DKA patients showed no differences withregard to FFAs, cortisol, or glucagon (95).This work is of special interest because itdemonstrated that in HHS, both basal andstimulated C-peptide levels were five- tosevenfold higher than those in the DKAgroup. These data are depicted in Table 5and are contrasted with data from otherauthors.
The scarcity of data available in HHSprevents firm conclusions as to whether or
not differences in stress hormone profilescontribute to the less prominent ketosis inthat setting. Available data are consistentwith multiple contributing factors, with themost consistent differences being lowergrowth hormone and higher insulin in HHSthan in DKA (Table 5) (92,95). The higherinsulin levels (demonstrated by high basaland stimulated C-peptide) in HHS provideenough insulin to inhibit lipolysis in HHS(since it takes less insulin for antilipolysisthan for peripheral glucose uptake[67,9698]) but not enough for optimalcarbohydrate metabolism. Although Table 5
shows similar levels of FFAs in HHS andDKA, plasma FFAs may not be reflective ofportal vein FFA levels, which in turn regu-late ketogenesis. It is important to empha-size that studies performed before 1980,which showed similar blood levels ofinsulin in DKA and HHS (99), used assaysthat were not free from interference fromproinsulin. Because patients with DKA andHHS present with an overlapping syn-drome, the differences between DKA andHHS become matters of degree, not funda-
mental pathogenetic differences. However,it is important to remember that hyperos-molarity of severe DKA, which occurs inabout one-third of DKA patients (23), is sec-ondary to fluid losses due to osmotic diure-sis and to variable degrees of impaired fluidintake due to nausea and vomiting; thehyperosmolarity in HHS patients is due tomore prolonged osmotic diuresis and toinability to take fluid. This can be secondaryeither to mental retardation (in certain casesin children) or to chronic debilitation inelderly patients who are unaware of orunable to take adequate fluid (216,217).
Water and electrolyte metabolismThe development of dehydration andsodium depletion in DKA and HHS is theresult of increased urinary output and elec-trolyte losses (25,100,101). Hyperglycemialeads to osmotic diuresis in both DKA andHHS. In DKA, urinary ketoanion excre-tion on a molar basis is generally less thanhalf that of glucose. Ketoanion excretion,which obligates urinary cation excretion assodium, potassium, and ammonium salts,also contributes to a solute diuresis. Theextent of dehydration, however, is typicallygreater in HHS than in DKA. At first, thisseems paradoxical because patients withDKA experience the dual osmotic load ofketones and glucose. The more severedehydration in HHS, despite the lack ofsevere ketonuria, may be attributable to
the more gradual onset and longer durationof metabolic decompensation (102) andpartially to the fact that patients presentingwith HHS typically have an impaired fluidintake. Other factors that may contribute toexcessive volume losses include diureticuse, fever, diarrhea, and nausea and vomit-ing. The more severe dehydration, togetherwith the older average age of patients withHHS and the presence of other comorbidi-ties, almost certainly accounts for thehigher mortality of HHS (102). In addition,osmotic diuresis promotes the net loss ofmultiple minerals and electrolytes (Na, K,
Ca, Mg, Cl, and PO4). Although some ofthese can be replaced rapidly during treat-ment (Na, K, and Cl), others require daysor weeks to restore losses and achieve bal-ance (25,100,101).
The severe derangement of water andelectrolytes in DKA and HHS is the result ofinsulin deficiency, hyperglycemia, andhyperketonemia (in DKA). In DKA andHHS, insulin deficiency per se may alsocontribute to renal losses of water and elec-trolytes because insulin stimulates salt and
water reabsorption in the proximal anddistal nephron and phosphate reabsorp-tion in the proximal tubule (100,101,103).During severe hyperglycemia, the renalthreshold of glucose (200 mg/dl) andketones is exceeded; therefore, urinaryexcretion of glucose in DKA and HHS maybe as much as 200 g/day, and urinary excre-tion of ketones in DKA may be 2030g/day, with total osmolar load of2,000mOsm (103). The osmotic effects of gluco-suria result in impairment of NaCl andH
2O reabsorption in the proximal tubule
and loop of Henle (100). The ketoacidsformed during DKA (-hydroxybutyricand acetoacetic) are strong acids that fullydissociate at physiological pH. Thus,ketonuria obligates excretion of positivelycharged cations (Na, K, NH4
). The hydro-gen ions are titrated by plasma bicarbonate,resulting in metabolic acidosis. The reten-tion of ketoanions leads to an increase inthe plasma anion gap.
The losses of electrolytes and water inDKA and HHS are summarized in Tables 1and 2. During HHS and DKA, intracellulardehydration occurs as hyperglycemia andwater loss lead to increased plasma tonic-ity, leading to a shift of water out of cells.This shift of water is also associated with ashift of potassium out of cells into theextracellular space. Potassium shifts arefurther enhanced by the presence of aci-dosis and the breakdown of intracellular
protein secondary to insulin deficiency(104). Furthermore, entry of potassiuminto cells is impaired in the presence ofinsulinopenia. Marked renal potassiumlosses occur as a result of osmotic diuresisand ketonuria. Progressive volume deple-tion leads to decreased glomerular filtra-tion rate and greater retention of glucoseand ketoanions in plasma. Thus, patientswith a better history of food, salt, and fluidintake prior to and during DKA have bet-ter preservation of kidney function, greaterketonuria, lower ketonemia, and loweranion gap and are less hyperosmolar.
These patients may, therefore, present withgreater degrees of hyperchloremic meta-bolic acidosis (105). On the other hand,diabetic patients with a history of dimin-ished fluid and solute intake during thedevelopment of acute metabolic decom-pensation, plus loss of fluid through nau-sea and vomiting, typically present withgreater degrees of volume depletion,increased hyperosmolarity, and impairedrenal function and greater retention of glu-cose and ketoanions in plasma. The greater
136 DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001
Technical Review
8/2/2019 Ce to Acidosis Diabetic A
7/23
retention of plasma ketoanions is reflectedin a greater increment in the plasma aniongap. Such patients may present withgreater alteration of sensoria, which ismore commonly found in HHS than DKA
(8,102). However, in HHS, as mentionedabove, the inability to take fluid (often inelderly patients) plus other pathogenicmechanisms leads to greater hyperosmo-larity. These pathogenic pathways andtheir relationship to clinical conditions ofDKA and HHS are depicted in Fig. 3.
During treatment of DKA with insulin,hydrogen ions are consumed as ketoanionmetabolism is facilitated. This contributes toregeneration of bicarbonate, correction ofmetabolic acidosis, and decrease in plasma
anion gap. The urinary loss of ketoanions,as sodium and potassium salts, thereforerepresents the loss of potential bicarbonate(106), which is gradually recovered withina few days or weeks (107).
Insulin resistance in hyperglycemiccrisesSoon after insulin therapy became available,the administration of 10 U insulin every 2 hwas reported to be effective for the treatmentof DKA (108,109). In subsequent decades,however, large doses of insulin were recom-mended because two early studies suggestedthat larger doses of insulin were more effec-tive (110,111). In the 1950s and 1960s,two prospective randomized studies com-
pared high-, moderate-, and intermediate-dose insulin therapy in the treatment ofDKA. The results showed no difference inresponse to therapy regardless of insulindose (112,113). In the early 1970s, numer-
ous studies demonstrated that low-dose orphysiological (0.1 U kg1 h1) doses ofinsulin were effective in controlling DKA(114120). None of these studies used ran-domized prospective protocols (121).Between 1976 and 1980, however, numer-ous prospective randomized studies inadults and children demonstrated the effi-cacy of lower or physiological doses ofinsulin by various routes of therapy, which,unlike the high-dose protocol, were associ-ated with a lower incidence of hypokalemia
DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001 137
Kitabchi and Associates
Figure 3Pathogenesis of DKA and HHS.
8/2/2019 Ce to Acidosis Diabetic A
8/23
8/2/2019 Ce to Acidosis Diabetic A
9/23
discharged when stable. Patients withsevere ketoacidosis typically present with abicarbonate level 10 mEq/l and/or a pH7.0, have total serum osmolality 330mOsm/kg, usually present with mentalobtundation (23), and are more likely todevelop complications than are thosepatients with mild or moderate forms ofketoacidosis. Therefore, a classification ofthe severity of DKA appears to be more clin-ically appropriate because it may help withpatient disposition and choice of therapy(see TREATMENT). This classification must becoupled with an understanding of any con-comitant conditions affecting the patientsprognosis and the need for intravenous ther-apy for hydration.
Assessment of ketonuria and ketone-mia, the key diagnostic features of ketoaci-dosis, is usually performed by nitroprussidereaction. However, nitroprusside reactionprovides a semiquantitative estimation ofacetoacetate and acetone levels. This assayunderestimates the severity of ketoacidosisbecause it does not recognize the presenceof-hydroxybutyric acid, which is the mainketoacid in DKA (148). Therefore, if possi-ble, direct measurement of-hydroxybu-tyrate, which is now available in manyhospital settings, is preferable in establishingthe diagnosis of ketoacidosis (149,150).
Diagnostic criteria for HHS includeplasma glucose concentration 600 mg/dl,serum total osmolality 330 mOsm/kg,
and absence of severe ketoacidosis. How-ever, the laboratory profiles of HHS in pre-vious series have shown higher meanvalues of glucose (998 mg/dl) and osmo-lality (363 mOsm/l), with BUN 65 mg/dl,HCO
321.6 mEq/l, sodium 143 mEq/l, cre-
atinine 2.9 mg/dl, and anion gap 23.4 mg/l(100,151). By definition, patients withHHS have a serum pH 7.3, a serumbicarbonate 18 mEq/l, and mild ketone-mia and ketonuria. Approximately 50% ofthe patients with HHS have an increasedanion gap metabolic acidosis as the result ofconcomitant ketoacidosis and/or an
increase in serum lactate levels (151). Table6 provides methods for measurement ofanion gap and serum total and effectiveosmolality from serum chemistries.
In some cases, the diagnosis of DKAcan be confounded by the coexistence ofother acid-base disorders. Arterial pH maybe normal or even increased, depending onthe degree of respiratory compensation andthe presence of metabolic alkalosis fromfrequent vomiting or diuretic use (152).Similarly, blood glucose concentration may
be normal or only minimally elevated in15% of patients with DKA (300 mg/dl),such as in alcoholic subjects or patientsreceiving insulin. In addition, wide vari-ability in the type of metabolic acidosis hasbeen reported. It has been reported that46% of patients admitted for DKA had highanion gap acidosis, 43% had mixed aniongap acidosis and hyperchloremic metabolicacidosis, and 11% had only hyperchlore-mic metabolic acidosis (105).
The majority of patients with hypergly-
cemic emergencies present with leukocyto-sis. Admission serum sodium concentrationis usually low in DKA because of the osmoticflux of water from the intracellular to theextracellular space in the presence of hyper-glycemia. To assess the severity of sodiumand water deficits, serum sodium may becorrected by adding 1.6 mEq to the mea-sured serum sodium for each 100 mg/dl ofglucose above 100 mg/dl (153). Admissionserum potassium concentration is usuallyelevated because of a shift of potassium fromthe intracellular to the extracellular spacecaused by acidemia, insulin deficiency, and
hypertonicity. On the other hand, in HHS,the measured serum sodium concentrationis usually normal or elevated because ofsevere dehydration. In this setting, the cor-rected serum sodium concentration wouldbe very high. Admission serum phosphatelevel in DKA may be elevated despite total-body phosphate depletion.
Pitfalls of laboratory diagnosisIn assessment of blood glucose and elec-trolytes in DKA, certain precautions need to
be taken in interpreting results. Severehyperlipidemia, which is occasionally seenin DKA, could reduce serum glucose (154)and sodium (155) levels, factitiously leadingto pseudohypo- or normoglycemia andpseudohyponatremia, respectively, in labo-ratories still using volumetric testing or dilu-tion of samples with ion-specific electrodes.This should be rectified by clearing lipemicblood before measuring glucose or sodiumor by using undiluted samples with ion-spe-cific electrodes. Creatinine, which is mea-
sured by a colormetric method, may befalsely elevated as a result of acetoacetateinterference with the method (156,157).Hyperamylasemia, which is frequently seenin DKA, may be the result of extrapancreaticsecretion (158) and should be interpretedcautiously as a sign of pancreatitis. The use-fulness of urinalysis is only in the initialdiagnosis for glycosuria and ketonuria anddetection of urinary tract infection. Forquantitative assessment of glucose orketones, the urine test is unreliable, becauseurine glucose concentration has poor cor-relation with blood glucose levels (159,160)
and the major urine ketone, -hydroxybu-tyrate, cannot be measured by the standardnitroprusside method (148).
Differential diagnosisNot all patients with ketoacidosis haveDKA. Patients with chronic ethanol abusewith a recent binge culminating in nausea,vomiting, and acute starvation may presentwith alcoholic ketoacidosis (AKA). In vir-tually all reported series of AKA, the eleva-tion of total ketone body concentration
DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001 139
Kitabchi and Associates
Table 6Calculations from serum chemistries
Anion gapAnion gap = [Na (Cl HCO
3)]
Normal = 79 mEq/l Gap = [patient gap 8]
Average = 8 mEq/lPrimary gap acidosis = anion gap/ HCO3
0.8Primary nongap acidosis = anion gap/ HCO3
0.4Serum sodium correction = add 1.6 mEq sodium for each 100 mg plasma glucose 100 mg/dlto the measured serum sodium value
Total and effective serum osmolalityTotal: 2 [measured serum Na (mEq/l)] glucose (mg/dl) BUN (mg/dl) = mOsm/kg H2O
18 2.8Normal = 290 5
Effective: 2 [measured serum Na (mEq/l)] glucose (mg/dl) = mOsm/kg H2O
18Normal = 285 5
Adapted from Ennis et al. (20).
8/2/2019 Ce to Acidosis Diabetic A
10/23
(710 mmol/l) is comparable to thatreported in patients with DKA (161,162).However, in in vitro studies, the alteredredox cellular state in AKA caused by anincreased ratio of NADH to NAD levelsleads to a reduction of pyruvate and
oxaloacetate, which results in impaired glu-coneogenesis (163). Additionally, low levelsof malonyl-CoA stimulate ketoacidosis andhigh catecholamines, which result indecreased insulin secretion and increasedratio of glucagon to insulin. This sets thestage for a shift in the equilibrium reactiontoward -hydroxybutyrate production(163,164). Consequently, AKA patientsusually present with normal or even lowplasma glucose levels and much higher lev-els of-hydroxybutyrate than of acetoac-etate. The average -hydroxybutyratetoacetoacetate ratio observed in AKA might
be as high as 710:1, as opposed to the 3:1ratio observed in DKA (165). The variablethat differentiates diabetes-induced andalcohol-induced ketoacidosis is the con-centration of blood glucose. Whereas DKAis characterized by hyperglycemia (plasmaglucose 250 mg/dl), the presence ofketoacidosis without hyperglycemia in analcoholic patient is virtually diagnostic ofAKA. Additionally, AKA patients frequentlyhave hypomagnesemia, hypokalemia, andhypophosphatemia, as well as hypocal-
cemia, due to decreased PTH as a result ofhypomagnesemia (165).
Some patients with decreased foodintake (500 kcal/day) for several days maypresent with mild ketoacidosis (starvationketosis). However, a healthy subject is able
to adapt to prolonged fasting by increasingthe clearance of ketone bodies in peripheraltissues (brain and muscle) and by enhanc-ing the kidneys ability to excrete ammo-nium to compensate for the increasedketoacid production (91). Thus, patientswith starvation ketosis rarely present with aserum bicarbonate concentration 18mEq/l and do not exhibit hyperglycemia.
DKA must also be distinguished fromother causes of high anion gap metabolicacidosis, including lactic acidosis, advancedchronic renal failure, and ingestion of suchdrugs as salicylate, methanol, ethylene gly-
col, and paraldehyde. Measuring blood lac-tate concentration easily establishes thediagnosis of lactic acidosis (5 mmol/l)because DKA patients seldom demonstratethis level of serum lactate (122,127,128).However, an altered redox state mayobscure ketoacidosis in diabetic patientswith lactic acidosis (166). Salicylate over-dose is suspected in the presence of mixedacid-base disorder (primary respiratoryalkalosis and increased anion gap meta-bolic acidosis) in the absence of increased
ketone levels. Diagnosis is confirmed by aserum salicylate level 80100 mg/dl.Methanol ingestion results in acidosis fromthe accumulation of formic acid and to alesser extent lactic acid. Methanol intoxica-tion develops within 24 h after ingestion,
and patients usually present with abdomi-nal pain secondary to gastritis or pancre-atitis and visual disturbances that vary fromblurred vision to blindness (optic neuritis).Diagnosis is confirmed by the presence ofan elevated methanol level. Ethylene glycol(antifreeze) ingestion leads to excessiveproduction of glycolic acid. The diagnosisof ethylene glycol ingestion is suggested bythe presence of increased serum osmolalityand high anion gap acidosis withoutketonemia, as well as neurological and car-diovascular abnormalities (seizures andvascular collapse), and the presence of cal-
cium oxalate and hippurate crystals in theurine. Because methanol and ethylene gly-col are lowmolecular weight alcohols,their presence in plasma may be indicatedby an increased (20 mOsm/kg) plasmaosmolar gap, defined as the differencebetween measured and calculated plasmaosmolality. Paraldehyde ingestion is indi-cated by its characteristic strong odor onthe breath. Table 7 also summarizes the dif-ferential diagnosis of various states of comain regard to acid-base balances, etc. (167).
140 DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001
Technical Review
Table 7Laboratory evaluation of metabolic causes of acidosis and coma
Methanol orStarvation Alcoholic ethylene
or high Lactic Uremic ketosis Salicylate glycol Hyperosmolar Hypoglycemicfat intake DKA acidosis acidosis (starvation) intoxication intoxication coma coma Rhabdomyolysis
pH Normal Mild * Normal Normal Mild may be
Plasma glucose Normal Normal Normal or normal Normal or Normal Normal
500 mg/dl 30 mg/dl
Glycosuria Negative Negative Negative Negative Negative Negative Negative Negative
Total plasma Slight Normal Normal Slight to Normal Normal Normal Normal Normal
ketones moderate or slight or slight
Anion gap Slight Slight Normal Normal
or slight Osmolality Normal Normal Normal Normal Normal Normal or
330 slight
mOsm/kg
Uric acid Mild Normal Normal Normal Normal Normal Normal
(starvation)
Miscellaneous May give Serum BUN Serum Serum Myoglobinuria,
false-positive lactate 200 salicylate levels hemoglobinuriafor ethylene 7 mmol/l mg/dl positive positive
glycol
, positive; , negative. *Acetest and Ketostix measure acetoacetic acid only; thus, misleading low values may be obtained because the majority of ketone bodies are-hydroxybutyrate; respiratory alkalosis/metabolic acidosis; may get false-positive or false-negative urinary glucose caused by the presence of salicylate or its metabo-lites; from Bjellerup et al. (220). All other data are from Morris and Kitabchi (167).
8/2/2019 Ce to Acidosis Diabetic A
11/23
TREATMENT
Therapeutic goalsThe therapeutic goals for treatment ofhyperglycemic crises in diabetes consist of1) improving circulatory volume and tissueperfusion,2) decreasing serum glucose andplasma osmolality toward normal levels, 3)clearing the serum and urine of ketones at
a steady rate, 4) correcting electrolyteimbalances, and 5) identifying and treatingprecipitating events (Tables 2 and 3).
MonitoringAs shown in Figs. 4 and 5, monitoring ofserum glucose values must be done every12 h during treatment. Serum elec-trolytes, phosphate, and venous pH mustbe assessed every 26 h, depending on theclinical response of the patient. Foremost,the precipitating factor must be identified
and treated. See Table 7 for a review of thelaboratory evaluation of metabolic causesof acidosis and coma. A flow sheet (Fig. 6)is invaluable for recording vital signs, vol-ume and rate of fluid administration,insulin dosage, and urine output and forassessing the efficacy of medical therapy(6). Figures 4 and 5 represent a successfulprotocol used by the authors for the treat-
ment of DKA and HHS in adult patients.There are some differences in the treat-ment of children with DKA, which aredescribed throughout the following sec-tions. A protocol for the management ofthe pediatric patient with DKA and HHSis shown in Fig. 7.
Replacement of fluid andelectrolytesThe severity of fluid and sodium deficits, asshown in Table 2, is determined primarily
by duration of hyperglycemia, level of renalfunction, and patients oral intake of soluteand water (23,24,44,145,167175). Theseverity of dehydration and volume deple-tion can be estimated by clinical examina-tion (44) using the following guidelines,with the caveat that these criteria are lessreliable in patients with neuropathy andimpaired cardiovascular reflexes:
1. An orthostatic increase in pulse with-out change in blood pressure indicates10% decrease in extracellular vol-ume (i.e., 2 liters isotonic saline).
2. An orthostatic drop in blood pressure(15/10 mmHg) indicates a 1520%decrease in extracellular volume (i.e.,34 liters).
3. Supine hypotension indicates adecrease of20% in extracellular fluidvolume (i.e., 4 liters).
DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001 141
Kitabchi and Associates
Figure 4Protocol for the management of adult patients with DKA. *DKA diagnostic criteria: blood glucose 250 mg/dl, arterial pH 7.3, bicarbonate 15mEq/l, and moderate ketonuria or ketonemia. After history and physical examination, obtain arterial blood gases, complete blood count with differential, uri-nalysis, blood glucose, BUN, electrolytes, chemistry profile, and creatinine levels STAT as well as an electrocardiogram. Obtain chest X ray and cultures as needed.Serum Na should be corrected for hyperglycemia (for each 100 mg/dl glucose 100 mg/dl, add 1.6 mEq to sodium value for corrected serum sodium value).
8/2/2019 Ce to Acidosis Diabetic A
12/23
The use of isotonic versus hypotonicsaline in treatment of DKA and HHS is stillcontroversial, but there is uniform agree-ment that in both DKA and HHS, the firstliter of hydrating solution should be nor-
mal saline (0.9% NaCl), given as quickly aspossible within the 1st hour and followedby 5001,000 ml/h of 0.45 or 0.9% NaCl(depending on the state of hydration andserum sodium) during the next 2 h. State ofhydration can also be estimated by calcu-lating total and effective plasma osmolalityand by calculating corrected serum sodiumconcentration. Total plasma osmolality canbe calculated by the following equation:2(measured Na) (mEq/l) glucose(mg/dl)/18 BUN (mg/dl)/2.8. Total
osmolality, whether calculated or directlymeasured by freezing point depression, isnot equivalent to tonicity, because onlythose solutes that are relatively restricted tothe extracellular space are effective in caus-
ing osmotic flux of water from intracellularto extracellular space. Urea is an ineffectiveosmole; therefore, effective osmolality isdefined as 2(measured Na) (mEq/l) glucose (mg/dl)/18 (45,172). Correctedserum sodium concentrations of 140mEq/l and calculated total osmolality of340 mOsm/kg H
2O are associated with
large fluid deficits (20,23,167171). Cal-culated total and effective osmolalities canbe correlated with mental status, stupor,and coma typically occurring with total
and effective osmolalities of340 and 320mOsm/kg H
2O, respectively (21,23,174).
The presence of stupor or coma in theabsence of such hyperosmolarity demandsprompt consideration of other causes of
altered mental status (145). Severe hyper-tonicity is also more frequently associatedwith large sodium deficits and hypov-olemic shock (21,168174).
The initial goal of rehydration therapyis repletion of extracellular fluid volume byintravenous administration of isotonicsaline (175) to restore intravascular vol-ume; this will decrease counterregulatoryhormones and lower blood glucose (90),which should augment insulin sensitivity(130). The initial fluid of choice is isotonic
142 DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001
Technical Review
Figure 5Protocol for the management of adult patients with HHS. *Diagnostic criteria: blood glucose 600 mg/dl, arterial pH 7.3, bicarbonate 15mEq/l, effective serum osmolality 320 mOsm/kg H2O, and mild ketonuria or ketonemia. This protocol is for patients admitted with mental status change orsevere dehydration who require admission to an intensive care unit. For less severe cases, see text for management guidelines. Effective serum osmolality cal-culation: 2[measured Na (mEq/l)] glucose (mg/dl)/18. After history and physical examination, obtain arterial blood gases, complete blood count with dif-ferential, urinalysis, plasma glucose, BUN, electrolytes, chemistry profile, and creatinine levels STAT as well as an electrocardiogram. Chest X ray and culturesas needed. Serum Na should be corrected for hyperglycemia (for each 100 mg/dl glucose 100 mg/dl, add 1.6 mEq to sodium value for corrected serum value).
Hemodynamic
KPO4) to keep
8/2/2019 Ce to Acidosis Diabetic A
13/23
saline (0.9% NaCl), even in HHS patients orDKA patients with marked hypertonicity,particularly in patients with evidence ofsevere sodium deficits manifested byhypotension, tachycardia, and oliguria. Iso-tonic saline is hypotonic relative to thepatients extracellular fluid and remainsrestricted to the extracellular fluid compart-ment (175). Administration of hypotonicsaline, which is similar in composition tofluid lost during osmotic diuresis, leads togradual replacement of deficits in bothintracellular and extracellular compart-ments (175). The choice of replacementfluid and the rate of administration in HHSremain controversial. Some authoritiesadvocate the use of hypotonic fluid from theoutset if effective osmolality is 320mOsm/kg H2O. Others advocate initial useof isotonic fluid. As outlined in Fig. 5, aninitial liter of 0.9% NaCl over the 1st houris followed by either 0.45 or 0.9% NaCl,depending on the corrected serum sodiumand the hemodynamic status of the patient.
Dextrose should be added to replace-ment fluids when blood glucose concentra-tions are 250 mg/dl in DKA or 300mg/dl in HHS. This can usually be accom-plished with the administration of 5% dex-trose; however, in rare cases, a 10% dextrosesolution may be needed to maintain plasmaglucose levels and clear ketonemia. Thisallows continued insulin administrationuntil ketogenesis is controlled in DKA and
avoids too rapid correction of hypergly-cemia, which may be associated with devel-opment of cerebral edema (especially inchildren) (176). An additional importantaspect of fluid replacement therapy in bothDKA and HHS is the replacement of ongo-ing urinary losses. Failure to adjust fluidreplacement for urinary losses leads to adelay in repair of sodium, potassium, andwater deficits (21,170,176). Overhydration isa concern when treating children with DKA,adults with compromised renal or cardiacfunction, and elderly patients with incipientcongestive heart failure. Once blood pressure
stability is achieved with the use of 1020ml kg1 h1 0.9% NaCl for 12 h, oneshould become more conservative withhydrating fluid (Figs. 4 and 5). Reduction inglucose and ketone concentrations shouldresult in concomitant resolution in osmoticdiuresis of DKA. The resulting decrease inurine volume should lead to a reduction inthe rate of intravenous fluid replacement.This reduces the risk of retention of excessfree water, which contributes to brainswelling and cerebral edema, particularly in
children. The duration of intravenous fluidreplacement in adults and children is48hdepending on the clinical response to ther-apy. However, in a child, once cardiovascularstability is achieved and vomiting hasstopped, it is safer and as effective to pursueoral rehydration.
Insulin therapy
The use of low-dose insulin reemerged inthe 1970s in the U.S. after a prospectiverandomized study using high doses ofintravenous and subcutaneous insulin(total dose 263 45 U) or low-dose insulin(total dose 46 5 U) administered intra-muscularly after aggressive hydrationdemonstrated similar outcomes in the twogroups. Furthermore, significant reductionin hypokalemia and no hypoglycemia weredemonstrated in the low-dose group (122).These findings were confirmed in many
subsequent studies in both adults and chil-dren (23,123128).
An important question raised duringthis period concerned the optimum routeof insulin delivery (17). In one compara-tive study, 45 patients (15 in each of threegroups) were randomly assigned to receivelow-dose insulin intravenously, subcuta-neously, or intramuscularly, with initial
therapy consisting of 0.33 U/kg body wt,as either an intravenous bolus or subcuta-neous or intramuscular injections, fol-lowed by 7 U /h r egu la r in su l inadministered in the same manner (127).Outcome parameters were found to besimilar in the three groups. However, dur-ing the first 2 h of therapy, the groupreceiving intravenous insulin showed agreater decline in plasma glucose andketone bodies. In fact, the group thatreceived subcutaneous or intramuscular
DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001 143
Kitabchi and Associates
Figure 6DKA/HHS flowsheet for the documentation of clinical parameters, fluid and electrolytes,laboratory values, insulin therapy, and urinary output. From Kitabchi et al. (6).
BUN
(e.g., HCO3-)
8/2/2019 Ce to Acidosis Diabetic A
14/23
injections showed an increase rather thana decrease in ketone bodies in the 1st hour.It was of interest that the 10% glucosedecrement, which was defined as anacceptable response in the 1st hour ofinsulin therapy, was achieved in 90% ofthe intravenous group but only in 3040%of the intramuscular and subcutaneousgroups. These groups required second and
third doses of insulin to produce anacceptable glucose decrement. Because 15of the 45 patients had never taken insulin,it was possible to determine their level ofimmunoreactive insulin (IRI) during ther-apy. Insulin levels during 8 h of therapywere measured with the following results:1) the intravenous insulin bolus gave risewithin a few minutes to 3,000 U/ml ofIRI, and 2) a similar amount of insulingiven subcutaneously or intramuscularlybarely doubled the initial level of IRI to
20 U/ml in 1530 min, and it took4 h before the plasma insulin levelreached a plateau at a level of 100 U/ml.In the intravenous protocol, IRI declinedafter the initial peak and plateaued at thesame level as in the intramuscular andsubcutaneous groups, i.e., 100 U/mlin 4 h. The rate of decline in blood glucoseand ketone bodies after the first 2 h
remained comparable in all three groups(88). In a subsequent study, administrationof half the initial dose of insulin as anintravenous bolus and the other half aseither intramuscular or subcutaneousinjections was shown to be as effective inlowering ketone bodies as administrationof the entire insulin dose intravenously(128). Furthermore, it was shown thataddition of albumin to the infusate was notnecessary to prevent insulin adsorptioninto the tubes and containers.
It has been well established that insulinresistance is present in many type 1 (with-out DKA) and most type 2 diabetic patients(44). During severe DKA, there are addi-tional confounding factors, such as stress(elevated counterregulatory hormones),ketone bodies, FFAs, hemoconcentration,electrolyte deficiencies (132), and particu-larly hyperosmolarity, that exaggerate the
insulin resistance state. However, replace-ment of fluid and electrolytes alone maydiminish this insulin resistance by decreas-ing levels of counterregulatory hormonesand hyperglycemia as well as by decreasingosmolarity, making the cells more respon-sive to insulin (90,130). Low-dose insulintherapy is therefore most effective whenpreceded or accompanied by initial fluidand electrolyte replacement.
In the present proposed protocol, wehave used essentially the same insulin regi-
144 DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001
Technical Review
Figure 7Protocol for the management of pediatric patients (20 years) with DKA or HHS. *DKA diagnostic criteria: blood glucose 250 mg/dl, venous pH7.3, bicarbonate 15 mEq/l, and moderate ketonuria or ketonemia. HHS diagnostic criteria: blood glucose 600 mg/dl, venous pH 7.3, bicarbonate 15mEq/l, and altered mental status or severe dehydration. After the initial history and physical examination, obtain blood glucose, venous blood gasses, electrolytes,BUN, creatinine, calcium, phosphorous, and urine analysis STAT. Usually 1.5 times the 24-h maintenance requirements (5 ml kg1 h1) will accomplish asmooth rehydration; do not exceed two times the maintenance requirement. The potassium in solution should be 1/3 KPO4 and 2/3 KCl or Kacetate.
8/2/2019 Ce to Acidosis Diabetic A
15/23
men for both DKA and HHS, but because ofa greater level of mental obtundation inHHS, we have recommended only usingthe intravenous route for HHS (Figs. 4 and5). The important point to emphasize ininsulin treatment of patients with DKA andHHS is that insulin should be used after ini-tial serum electrolyte values are obtainedwhile the patient is being hydrated with 1liter of 0.9% saline. Insulin therapy is theninitiated with an intravenous bolus of 0.15U/kg or 10 U regular insulin, followed byeither intravenous infusion of insulin at arate of 0.1 U kg1 h1 or subcutaneous orintramuscular injection of 710 U/h. How-ever, in children, the initial dose may be 0.1U/kg continuous infusion with or withoutan insulin bolus. Some pediatric endocri-nologists do not use 3 U/h in children.
As noted earlier (26,127), the rates ofabsorption of regular insulin administeredintramuscularly and subcutaneously arecomparable, with the subcutaneous routebeing less painful. However, an intravenousroute should be used exclusively in the caseof hypovolemic shock due to poor tissueperfusion. As depicted in Figs. 4 and 5, theinsulin rate is decreased to 0.050.1 U kg1 h1 when blood glucose reaches250300 mg/dl. A 5% or, rarely, a 10%solution of dextrose is added to the hydrat-ing solution at this time to keep blood glu-cose at its respective level (by adjusting theinsulin rate) until the patient has recovered
from DKA (i.e., HCO3 18 mEq/l, aniongap 12, and pH 7.3) or HHS (osmolal-ity 315 mOsm/kg and patient is alert).Blood glucose monitoring every 60 min willindicate whether this is sufficient to producea consistent reduction in blood glucose. Ifblood glucose fails to decrease at a rate of5070 mg dl1 h1, the patients volumestatus should be reassessed to ensure ade-quate volume repletion. An additional fac-tor that may contribute to the failure ofblood glucose to decline is an error inpreparation of the insulin infusion mixture,which should be redone with greater care
for the appropriate inclusion of insulin intothe infusion solution. If the infusion con-tinues to be ineffective, the infusion rateshould be increased until the desired glu-cose-lowering effect is produced.
PotassiumTable 2 shows typical potassium deficits,which represent mainly intracellular losses,in both DKA and HHS. Extracellular hyper-osmolarity, secondary to hyperglycemia,causes a shift of water and potassium from
the intracellular to the extracellular space,resulting in normal or elevated serum potas-sium concentrations despite total-bodypotassium deficits of 500700 mEq/l(44,177179). This potassium shift is fur-ther enhanced by insulin deficiency andthe presence of acidosis and acceleratedbreakdown of intracellular protein (180).
Excessive urinary potassium losses,which occur as a result of osmotic diuresiswith increased delivery of fluid andsodium to potassium secretory sites in thedistal nephron, are ultimately responsiblefor the development of potassium deple-tion (177180). Secondary hyperaldos-teronism and urinary ketoanion excretion,as potassium salts, further augment potas-sium losses.
During treatment of DKA and HHSwith hydration and insulin, there is typicallya rapid decline in plasma potassium con-centration as potassium reenters the intra-cellular compartment. However, potassiumreplacement should not be initiated untilthe serum potassium concentration is 5.5mEq/l. We recommend administering one-third of the potassium replacement as potas-sium phosphate to avoid excessive chlorideadministration and to prevent severehypophosphatemia. Others use potassiumacetate to avoid an excessive chloride load.Because hypokalemia is the most life-threat-ening electrolyte derangement occurringduring treatment, in the rare patients
(410%) presenting with hypokalemia(179), potassium replacement should beinitiated before insulin therapy and insulintherapy held until plasma potassium levelsare 3.3 mEq/l. Intravenous potassiumadministration should not generally exceed40 mEq in the 1st hour; thereafter, 2030mEq/h is needed to maintain plasma potas-sium levels between 4 and 5 mEq/l. We rec-ommend electrocardiogram monitoringduring potassium therapy in patients pre-senting with hypokalemia or in patientswith any abnormal rhythms other thansinus tachycardia.
BicarbonateMost current reviews do not recommendthe routine use of alkali therapy in DKAbecause DKA tends to correct with insulintherapy. Insulin administration inhibitsongoing lipolysis and ketoacid productionand promotes ketoanion metabolism.Because protons are consumed duringketoanion metabolism, bicarbonate isregenerated, leading to partial correction ofmetabolic acidosis. Arguments that favor
the use of alkali therapy are based on theassumption that severe metabolic acidosisis associated with intracellular acidosis,which could contribute to organ dysfunc-tion, such as in the heart, liver, or brain.Such organ dysfunction could in turn resultin increased morbidity and mortality.Potential adverse effects of alkali therapyinclude worsened hypokalemia, worsenedintracellular acidosis due to increased car-bon dioxide production, delay of ketoanionmetabolism, and development of paradox-ical central nervous system acidosis (181).
A retrospective review (182) has failedto identify changes in morbidity or mortal-ity with sodium bicarbonate therapy. Afterreviewing the risks and benefits of bicar-bonate therapy, one author concluded thatthe only clear indication for use of bicar-bonate is life-threatening hyperkalemia(183). Another study showed that ketoan-ion metabolism was delayed in the pres-ence of bicarbonate therapy, but nosignificant difference in response betweenthe bicarbonate and no bicarbonate groupswas noted (184). A prospective random-ized study examined the effect of bicar-bonate versus no bicarbonate in two groupsof DKA patients with similar degrees ofacidemia (pH 6.97.14) (185). In somepatients, initial cerebrospinal fluid (CSF)chemistry was measured and comparedwith initial plasma chemistry. It was ofinterest that HCO3 and pH in CSF were
significantly higher than those in plasma ofDKA patients. Conversely, ketones and glu-cose were higher in plasma than in CSF.However, CSF and plasma osmolalitieswere similar, indicating that the blood-brain barrier provided greater protectionagainst acidosis for the brain (185). Fur-thermore, regression analysis of the level oflactate, ketones, pH, bicarbonate, and glu-cose showed no significant difference inthe two groups with regard to slopes ofthese variables during recovery from DKA.It was therefore concluded that adminis-tration of bicarbonate in DKA patients
(with pH of 6.97.14) provided no mea-surable advantage either biochemically orclinically (181,185). However, becausethere were very few in a subclass of patientswho had an admission pH of 6.97.0,additional studies are needed at this level ofacidosis. No prospective randomized stud-ies concerning the use of bicarbonate inDKA with arterial pH values 6.9 havebeen reported. In the absence of such stud-ies, bicarbonate therapy in patients withpH 7.0 seems prudent. As outlined in
DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001 145
Kitabchi and Associates
8/2/2019 Ce to Acidosis Diabetic A
16/23
Fig. 4, a pH of 6.97.0 warrants a dose of50 mmol of intravenous bicarbonate; alarger dose is recommended for a venouspH of6.9 because of the increased sever-ity of acidosis. Bicarbonate should beadministered as an isotonic solution, whichcan be prepared by addition of oneampoule of 7.5% NaHCO
3solution (50
mmol HCO3) to 250 ml sterile H
2O. Add
15 mEq of KCl for each ampoule of bicar-bonate administration (if serum potassiumis 5.5 mEq/l).
Regarding the use of bicarbonate inchildren with DKA, no prospective ran-domized study has been reported. Becausegood tissue perfusion created with the ini-tial fluid bolus reduces the lactic acidosis ofDKA and because organic acid productionis reduced as the result of administeredexogenous insulin, the metabolic acid loadin DKA is reduced enough that it appearsto be unnecessary to add buffer NaHCO
3.
Young people who are at the least risk forcardiovascular failure should not receiveNaHCO
3in their rehydration fluids until
there is some clinical evidence of cardiacfailure. Furthermore, in a recent retrospec-tive study of 147 admissions of severe DKAin children with pH 7.15 (two with6.9), the effect of bicarbonate or no bicar-bonate was compared. This study con-cluded that there was no benefit ofbicarbonate and that use of bicarbonatemay be disadvantageous in severe pedi-
atric DKA (186). There have been sugges-tions that administration of NaHCO3
inchildren with DKA may be associated withaltered consciousness and headache, butno definitive causal relationship has beenestablished. It must be stated, however,that a definitive study on the efficacy ofbicarbonate or no bicarbonate in DKArequires a larger number of patients to pro-vide enough power for conclusive results.Until such a time, we recommend thatadult patients with a pH of6.9 receive100 mmol isotonic bicarbonate with KCland 50 mmol bicarbonate for a serum
bicarbonate of 6.97.0. In children, theuse of bicarbonate must be based on thecondition of the individual patient.
Phosphate therapyPhosphate, along with potassium, shiftsfrom the intracellular to the extracellularcompartment in response to hyperglycemiaand hyperosmolarity. Osmotic diuresis sub-sequently leads to enhanced urinary phos-phate losses (Tables 1 and 2). Because ofthe shift of phosphate from the intracellu-
lar to the extracellular compartment, serumlevels of phosphate at presentation withDKA or HHS are typically normal orincreased (187,188). During insulin ther-apy, phosphate reenters the intracellularcompartment, leading to mild to moderatereductions in serum phosphate concentra-tions. Adverse complications of hypophos-phatemia are uncommon, occurringprimarily in the setting of severe hypophos-phatemia (phosphate 1 mg/dl).
Potential complications of severehypophosphatemia include respiratory andskeletal muscle weakness, hemolytic ane-mia, and worsened cardiac systolic perfor-mance (189). Phosphate depletion mayalso contribute to decreased concentrationsof 2,3-diphosphoglycerate, thus shiftingthe oxygen dissociation curve to the leftand limiting tissue oxygen delivery (190).Controlled and randomized studies havenot demonstrated clinical benefits from theroutine use of phosphate replacement inDKA (187,188). Five days of PO
4therapy
increased 2,3-diphosphoglycerate withouta significant change in the oxygen dissoci-ation curve and resulted in a significantdecrease in serum ionized calcium (187).Similar studies have not been performed inpatients with HHS.
Although routine phosphate replace-ment is unnecessary in DKA, replacementshould be given to patients with serumphosphate concentrations 1.0 mg/dl and
to patients with moderate hypophos-phatemia and concomitant hypoxia, ane-mia, or cardiorespiratory compromise (189).Excessive administration of phosphate canlead to hypocalcemia with tetany andmetastatic soft tissue calcifications (191). InHHS, because the duration of symptomsmay be prolonged and because of comorbidconditions, the phosphate level may belower than in DKA; therefore, it is prudent tomonitor phosphate levels in these patients.
If phosphate replacement is needed,2030 mEq/l potassium phosphate can beadded to replacement fluids and given over
several hours. In such patients, because ofthe risk of hypocalcemia, serum calciumand phosphate levels must be monitoredduring phosphate infusion.
Immediate posthyperglycemic careLow-dose insulin therapy provides a circu-lating insulin concentration of60100U/ml. However, because of the short half-life of intravenous regular insulin, suddeninterruption of insulin infusion can lead torapid lowering of insulin concentration,
resulting in a relapse into DKA or HHS.Thus, numerous publications have empha-sized the need for frequent monitoring dur-ing the posthyperglycemic period (6,19,44,56,137,139,192).
Patients with severe DKA and mentalobtundation should be treated with contin-uous intravenous insulin or, if less severe,with hourly injection of subcutaneousinsulin until ketoacidosis is resolved tomaintain insulin levels at 100 U/ml(124). Criteria for resolution of ketoacidosisinclude blood glucose 200 mg/dl, serumbicarbonate level 18 mEq/l, venous pH7.3, and calculated anion gap 12 mEq/l.Once DKA is resolved, hydrating fluid iscontinued intravenously and subcutaneousregular insulin therapy is started every 4 h.An abrupt discontinuance of intravenousinsulin coupled with a delayed onset of asubcutaneous insulin regimen may lead toworsened control; therefore, some overlapshould occur in intravenous insulin therapyand initiation of the subcutaneous insulinregimen. When the patient is able to eat, amultiple daily injection schedule should beestablished that uses a combination of reg-ular (short-acting) and intermediate orlong-acting insulin as needed to controlplasma glucose. Patients with known dia-betes may be given insulin at the dose theywere receiving before the onset of DKA andfurther adjusted using a multiple dailyinjection regimen. In patients with newly
diagnosed diabetes, the initial total insulindose should be 0.6 U kg1 day1,divided into at least three doses in a mixedregimen including short- and long-actinginsulin, until an optimal dose is established.
Although serum -hydroxybutyratelevels are usually 1.5 mmol/l at resolutionof DKA, we do not recommend routinemeasurement of ketone levels during ther-apy. However, in some patients with pro-longed metabolic acidosis, combineddiabetic and lactic acidosis, or other mixedacid-base disorders, direct measurement of-hydroxybutyrate levels may be helpful.
During treatment of DKA, use of the nitro-prusside test, which measures acetoacetateand acetone levels but not -hydroxybu-tyrate, should be avoided because the fall inacetone and acetoacetate lags behind theresolution of DKA (6).
COMPLICATIONS OF THERAPY
Hypoglycemia and hypokalemiaBefore the advent of low-dose insulin pro-tocols (193), these two complications were
146 DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001
Technical Review
8/2/2019 Ce to Acidosis Diabetic A
17/23
seen in as many as 25% of patients treatedwith large doses of insulin (122). Both com-plications were significantly reduced withlower-dose therapy (122). In spite of this,hypoglycemia still constitutes one of thepotential complications of therapy, the inci-dence of which may be underreported(194). The use of dextrose-containing solu-tions when blood glucose reaches 250mg/dl in DKA and a simultaneous reductionin the rate of insulin delivery should furtherreduce the incidence of hypoglycemia. Sim-ilarly, the addition of potassium to thehydrating solution and frequent monitoringof serum potassium during the early phasesof DKA and HHS therapy should reduce theincidence of hypokalemia.
Cerebral edemaAn asymptomatic increase in CSF pressureduring treatment of DKA has been recog-nized for 25 years (195197). Signifi-cant decreases in the size of the lateralventricles, as determined by echoen-cephalogram, were noted in 9 out of 11DKA patients during therapy (198,199).However, in another study, nine children inDKA were compared with regard to brainswelling before and after therapy, and it wasconcluded that brain swelling is usuallypresent in DKA before treatment is begun(200). Symptomatic cerebral edema, whichis extremely rare in adult HHS or DKApatients, has been reported to occur pri-
marily in pediatric patients, particularly inthose with newly diagnosed diabetes. Nosingle factor has been identified that can beused to predict the development of cerebraledema (201,202). Lowering blood glucosein patients with HHS at a rate of 5070 mg dl1 h1 and adding 5% dextrose to thehydrating solution when blood glucose is300 mg/dl are prudent until moreknowledge on the mechanism of cerebraledema is obtained (203,204). A 20-yearreview of cerebral edema in children withDKA from the Royal Childrens Hospital inMelbourne, Australia, concluded that
although no predictive factors for survivalof cerebral edema were identified, protocolsthat use slow rates of rehydration with iso-tonic fluids should be recommended (205).
Several other reviews have found a cor-relation between the development of cere-bral edema and higher rates of fluidadministration, especially in the first hoursof fluid resuscitation. The most current rec-ommendation is to limit fluid administra-tion in the first 4 h of therapy to 50ml/kg isotonic solution (206,207).
Adult respiratory distress syndromeA rare but potentially fatal complication oftherapy is adult respiratory distress syn-drome (ARDS) (208). During rehydrationwith fluid and electrolytes, an initially ele-vated colloid osmotic pressure is reduced tosubnormal levels. This change is accompa-nied by a progressive decrease in arteriolarpartial pressure of oxygen (PaO
2) and an
increase in alveolar-to-arteriolar oxygen(AaO
2) gradient, which is usually normal at
presentation in DKA (19,175,198). In asmall subset of patients, this may progressto ARDS. By increasing left atrial pressureand decreasing colloid osmotic pressure,excessive crystalloid infusion favors edemaformation in the lungs (even in the presenceof normal cardiac function). Patients withan increased AaO2 gradient or those whohave pulmonary rales on physical examina-tion may be at an increased risk for devel-opment of this syndrome. Monitoring ofPaO
2with pulse oximetry and monitoring of
AaO2
gradient may assist in the manage-ment of such patients. Because crystalloidinfusion may be the major factor, we advisethat such patients have lower fluid intake,with addition of colloid administration fortreatment of hypotension unresponsive tocrystalloid replacement.
Hyperchloremic metabolic acidosisHyperchloremic normal anion gap meta-bolic acidosis is present in 10% of
patients admitted with DKA; however, it isalmost uniformly present after resolution ofketonemia (105,209,210). This acidosishas no adverse clinical effects and is grad-ually corrected over the subsequent2448 h by enhanced renal acid excretion.The severity of hyperchloremia can beexaggerated by excessive chloride adminis-tration (211) because 0.9% NaCl contains154 mmol/l of both sodium and chloride,which is 54 mmol/l in excess of the 100mmol/l of chloride in serum. Furthercauses of nonanion gap hyperchloremicacidosis include 1) loss of potential bicar-
bonate due to excretion of ketoanions assodium and potassium salts;2) decreasedavailability of bicarbonate in proximaltubule, leading to greater chloride reab-sorption; and 3) reduction of bicarbonateand other buffering capacity in other bodycompartments. In general, hyperchloremicmetabolic acidosis is self-limiting withreduction of chloride load and judicioususe of hydration solution (212,213). Serumbicarbonate that does not normalize withother metabolic parameters should alert
the clinician to the need for more aggres-sive insulin therapy or further investigation.
RESOURCE UTILIZATION INDKA The process of health carereform demands cost-efficient modes ofdelivering optimal care. The choice of man-agement site (intensive care unit, step-down unit, or general medical ward)therefore becomes a critical issue. Unfortu-nately, there are no randomized prospectivestudies that have evaluated the optimal siteof care for either DKA or HHS. Given thelack of such studies, the decision concern-ing the site of care must be based onknown clinical prognostic indicators andon the availability of hospital resources.
Recent studies that have emphasizedthe use of standardized written guidelinesfor therapy have demonstrated mortalityrates 5% in DKA and 15% in HHS(6,9,10,1216,214). The majority of deathshave occurred in patients 50 years of agebecause of concomitant life-threatening ill-nesses, suggesting that further majordecreases in mortality rates may not beattainable based on treatment of DKA alone(9). As stated earlier, similar outcomes oftreatment of DKA have been noted in bothcommunity and training hospitals, andoutcomes have not been altered by whetherthe managing physician is a family physi-cian, a general internist, a house officerwith attending supervision, or an endocri-
nologist (1416), so long as standard writ-ten therapeutic guidelines are followed.The response to initial therapy, which
would preferably be in the emergencyward, can be used as a guideline for choos-ing the most appropriate hospital site forfurther care. All patients with hypotensionor oliguria refractory to initial rehydrationand those patients with mental obtunda-tion or coma with hyperosmolarity (effec-tive osmolality 320 mOsm/kg H
2O)
should be considered for admission to step-down or intensive care units in order toreceive continuous intravenous insulin
therapy. In the absence of indications forhemodynamic monitoring, the majority ofsuch patients can be managed in lessexpensive step-down units rather thanintensive care units after the initial emer-gency room evaluation and care (19,215).
Options of site of care for DKApatients with less mental obtundation andno hypotension following initial rehydra-tion are based primarily on the availabilityof hospital resources. Those patients whoare mildly ketotic can be effectively man-
DIABETES CARE, VOLUME 24, NUMBER 1, JANUARY 2001 147
Kitabchi and Associates
8/2/2019 Ce to Acidosis Diabetic A
18/23
aged on a general medical ward, assumingthere are 1) sufficient nursing staff to allowfrequent monitoring of vital signs andhourly administration of subcutaneousinsulin and2) on-site blood glucose mon-itoring equipment and rapid turn-aroundtime for routine laboratory services. Con-tinuous intravenous insulin therapy is notgenerally recommended for use in generalmedical wards unless appropriately trainedpersonnel are available. DKA patients witha mild condition who are alert and able totolerate oral intake may be treated in theemergency room and observed for a fewhours before discharge.
Given the known high mortality rateof HHS, the frequent presence of seriousconcomitant illnesses, and the usuallyadvanced age of HHS patients, it is rea-sonable that all such patients be admittedto either step-down or intensive care units.
PREVENTION The two major pre-cipitating factors in the development ofDKA are inadequate insulin treatment(including noncompliance) and infection.In many cases, these events may be pre-vented by better access to medical care,including intensive patient education andeffective communication with a health careprovider during acute illnesses.
Goals in the prevention of hypergly-cemic crises precipitated by either acute ill-ness or stress have been outlined (216).
These goals included controlling insulindeficiency, decreasing excess stress hor-mone secretion, avoiding prolonged fastingstate, and preventing severe dehydration.Therefore, an educational program shouldreview sick-day management with specificinformation on administration of short-act-ing insulin, including frequency of insulinadministration, blood glucose goals duringillness, means to suppress fever and treatinfection, and initiation of an easilydigestible liquid diet containing carbohy-drates and salt. Most importantly, thepatient should never discontinue insulin
and should solicit professional advice earlyin the course of the illness.Success with such a program depends
on frequent interaction between the patientand the health care provider and on thelevel of involvement that the patient or fam-ily member is willing to take to avoid hos-pitalization. The patient/family must bewilling to keep an accurate record of bloodglucose, urine ketones, insulin administra-tion, temperature, respiratory and pulserate, and body weight. Indicators for hospi-
talization include 5% loss of body weight,respiratory rate 36/min, intractable eleva-tions in blood glucose, mental statuschange, uncontrolled fever, and unresolvednausea and vomiting. A group of investiga-tors reported on the successful preventionof recurrent DKA (RDKA) in a pediatricpopulation with the introduction of a hier-archical set of medical, educational, andpsychosocial interventions in a lowersocioeconomic group (217). Insulin omis-sion was documented in 31 out of 44patients (70%) with a history of RDKA andin 13 of the 44 with inadequate education(30%). After initiation of the program, theepisodes of RDKA were reduced to 2.6episodes per 100 patient-months, com-pared with the initial number of 25.2episodes before the program (P 0.0001).RDKA ceased with or without psychother-apy. The authors concluded that RDKA iscausally related to a variety of social andeconomic problems, but its preventionrequires recognition that its proximate causein certain groups is omission of insulin.There is therefore a need for a support sys-tem to ensure adherence (217). In addition,an education program directed towardpediatricians and school educators that pro-moted the signs and symptoms of diabeteswas shown to be effective in decreasingketoacidosis at the onset of diabetes (218).
As previously mentioned, many of theadmissions for HHS are nursing home res-
idents or elderly individuals who becomedehydrated and are unaware or unable totreat the increasingly dehydrated state. Bet-ter education of care givers as well aspatients regarding conditions, procedures,and medications that may worsen diabetescontrol, use of glucose monitoring, andsigns and symptoms of newly onset dia-betes could potentially decrease the inci-dence and severity of HHS.
Beyond the educational issues, recentreports on DKA in urban African-Americantype 1 diabetic patients showed that themajor precipitating cause of DKA was dis-
continuance of insulin (67%). Reasons forstopping insulin included economic rea-sons (50%), lack of appetite (21%), behav-ioral reasons (14%), or lack of knowledgeabout how to manage sick days (14%) (26).Because the most common reason for inter-rupted insulin is economic in nature,changes in the health care delivery systemand in the access patients have to care andmedications may be the most effectivemeans of preventing DKA in this popula-tion. The investigators showed that of 56
DKA admissions, only two patients tried tocontact the diabetes unit for assistance (26).Similarly, a study of hyperglycemic crises inan urban black population demonstratedthat socioeconomic barriers, such as a lowliteracy rate, limited financial resources,and limited access to health care, mightexplain the continuing high rates of admis-sion for DKA in this group of patients (5).
Hospitalizations for DKA in the pasttwo decades have increased in some areasand declined in o