Embed Size (px)
Citation preview
Celiac disease in Turkey
Aydan KansuZarife Kuloğlu
Ankara University School of Medicine Pediatric Gastroenterology, Hepatology and Nutrition
MEDICEL MeetingNaples
September 15-16 2010
Turkey Population:72.561.312 0-14 year:18.859.334 Estimated CD (children): 188.593
TPGHAN (about 100 members) Pediatric Gastroenterology Departments:30
Celiac society Ankara İstanbul İzmir Diyarbakır
Epidemiology Ertekin V. J Clin Gastroenterol 2005;8:689-91
6-17 y, 1263, ttg IgA Seropositivity.1/115 Biopsy proven CD:1/158
Demirçeken F. Turk J Gastroenterol 2008;19:14-21 2-18 y, 1000, ttg IgA
Seropositivity.1/100 Biopsy proven CD:1/111
Epidemiology Dalgıç B and Turkish Celiac Disease
Study Group. ESPGHAN 2010, İstanbul
6-17 y, 13 073 652 Two-stratified Cluster sampling, 20190, 62 cities ttG IgA, ttg IgG, EMA Ig A, same pathologist
Epidemiology
Epidemiology
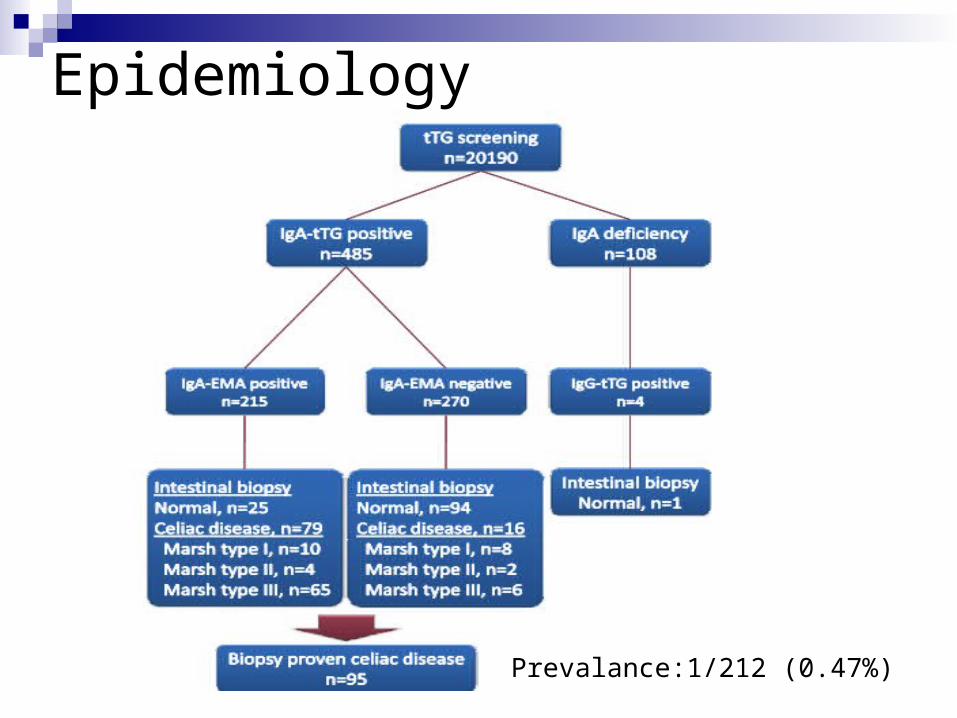
Prevalance:1/212 (0.47%)
HLA types Tüysüz B. Tissue Antigens 2001;6:540-2
55 CD&50 control HLA DQA1, DQB1 (PCR –SSP) HLA A10501, HLA DQB102 alles in than control
Kuloğlu Z, Turk J Pediatr 2008;50:515-20
75 CD (45 classic form: 6.7±3.8 y&30 atypical 9.3±4.3y) 100 healthy renal Tx donors
HLA typing: Serologically (standart lymphotoxicity techniques) Control group: HLA A29, B51, CW5, DR14, Dr16, DQ1
CD: HLA B13, CW7, B8, DR7, DR17, DQ2 was higher than control HLAB35, DR11, DQ7:classical type HLA B8: Atypical type
Clinical Presentation
109 patients, 8.8±4.6 y 60.6% Classical type 37.6% atypical 1.8% silent
Sx: Diarrhea (53.2%), FTT, short stature, abdominal pain
PE: paleness (40.4%), underweight (34.8%), short stature (31.2%)
Lab IDA (81.6%), zinc def (64.1%), PT(35.8%), transaminase(24.7%) Ig A deficiency (9.1%), ab (+) (8%), BMD (28/52), EEG abnormality (4/38) HLA DQ2 and/orDQ8:91%
Abdominal distention, IDA, PT , hypoalbuminemia, transaminase more frequent in classical type than atypical form
Clinical Presentation
Altuntaş B. Acta Pediatr Jpn 1998;40:457-60 47 short statured patients (without GIS symptoms) Bx proven CD:55%
Altuntaş B. Acta Pediatr Jpn 1998;40:597-9 9 patients, ALT Liver Bx: fibrosis, nonspecific reaction Duodenal Bx: CD
Clinical Presentation
32 CD (16 recent diagnosis&16 GFD) 100 healthy control
BMD, Ca, P, ALP, PTH (baseline&12 mo) Dual energy radiograph bone densitometer, L1-4, g/cm2
BMD& BMC were lower in CD than control
Osteoporosis was common in recent diagnosis
1 year later BMD values in patients with recent diagnosis significantly increased
After 1 year osteopenia was resolved
Clinical Presentation
50 with FMF ( questioned, examined, IgA, AGA IgA, AGA IgG, EMA IgA, bx) 1 EMA (+), bx normal
17 with CD (questioned, examined, lab, mutation analysis for MEFV) MEFV mutation:23.5%
No assosication between CD and FMF
Clinical Presentation Sarı S. Dig Dis Sci 2009;54:830-2
101 autoimmune thyroiditis 103 healthy Bx proven CD:4.9%
Dalgıç B. J Child Neurol 2008;21:6-7 70 epilepsy&103 control Bx proven CD: 1.8%
Alehan F. Cephalalgia 2009;28:945-9 73 migraine&147 control Bx proven CD:-
Kalaycı AG. Acta Paediatr 2005;8:678-81 135 IDA &223 control Biopsy proven CD:4.4%
Clinical Presentation Selimoğlu MA. J Clin Gastroenterol 2007;7:667-70
126 CD AST(51.6%), ALT (35.7%), CK (39.7) Myopathy?
Polat TB. Dig Liver Dis 2008;40-182-187 45 CD&30 control Subclinical systolic dysfunction of the left ventricule
Follow-up Aydoğdu S. Dig Dis Sci 2009;10:2183-87
34 CD, followed for at least four years GFD leads to rapid increase in WSDS and HSDS
in patients < 5 y Increase in HSDS is highest in patients 5-10 y Age at diagnosis is the major factor for WSDS and HSDS
at follow-up
Early diagnosis and strict GFD are essential for long-term growth
Leptin&Ghrelin&Nitric oxide
Ertekin V. J Clin Gastroenterol 2006;10:906-9 19 CD&16 control Serum leptin level is affected in CD, is not related to
histopathology, is responsive to GFD
Selimoğlu MA. JClin Gastroenterol 2006;3:191-4 36 CD&10 healthy Ghrelin is increased in CD and is responsive to GFD
Ertekin V. J Clin Gastroenterol 2005;39:782-85 41 CD&14 control NO level is high in CD non adharent to GFD
Conclusion CD is common in Turkey
CD is a well known disease among pediatric gastroenterologists
Rising awareness is needed among pediatricians and in primary care and also among society
Serologic diagnostic tools are needed to be available routinely
Wheat is basic nutrient in Turkish cousine, therefore adherance to GFD may be difficult
GFD products are not widely accessible
Financial support of the state for GFD is not enough





























