Embed Size (px)
Citation preview
Cellular Therapy vs Hematopoietic Cellular Therapy vs Hematopoietic Cell Transplantation: Development
of the Cellular Therapy Registryof the Cellular Therapy Registry
Marcelo C. Pasquini, MD, MSq , ,
New08_1.ppt
Outline
What is cellular therapy?Cellular therapy related HCTCellular therapy related HCT
Donor cellular infusionsMesenchymal stromal/stem cells
Cellular therapy for regenerative medicine.Development of the Cellular Therapy RegistryRegistry
Initial concept and implementationData collection
Challenges and strategies.Q&A
New08_2.ppt

Cellular TherapyCellular Therapy
What is Cellular Therapy?
Utilization of cells for treatment of human diseases diseases. Transfusion and Hematopoietic cell transplantation (HCT) are cellular therapies.p ( ) pWhat are the differences?
Transfusion terminally differentiated cells that survive in the recipient for a short period of time.HCT stem and progenitor cells engraft and HCT stem and progenitor cells engraft and replace the recipient’s bone marrow.
Terms and Definitions: Potency
Totipotency: “total potential”. Cells able to differentiate all cells in an organism gincluding extraembryonary tissue. Ex: embryonic stem cells.
Pluripotency: “potential for multiple outcomes”. Cells able to originate cells of different lineages Ex: mesoderm cells different lineages. Ex: mesoderm cells.
Multipotency: cells able to originate l li E h t i ti t several lineages. Ex: hematopoietic stem
cells.
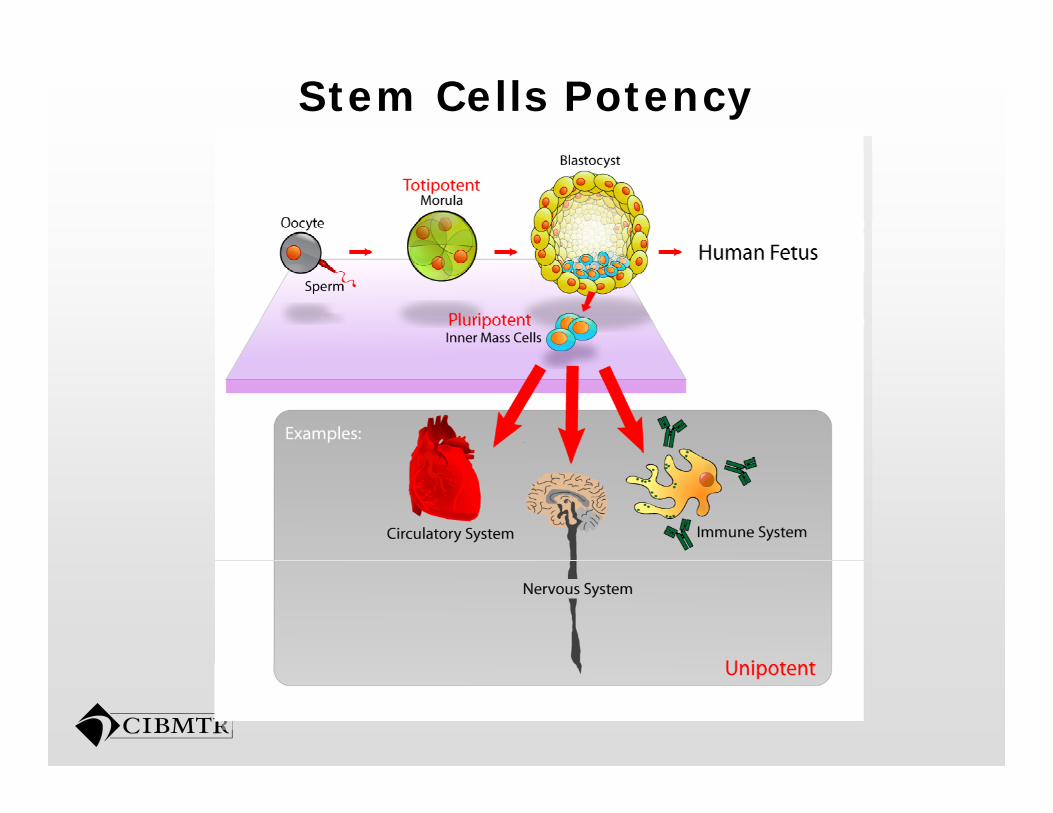
Stem Cells Potency
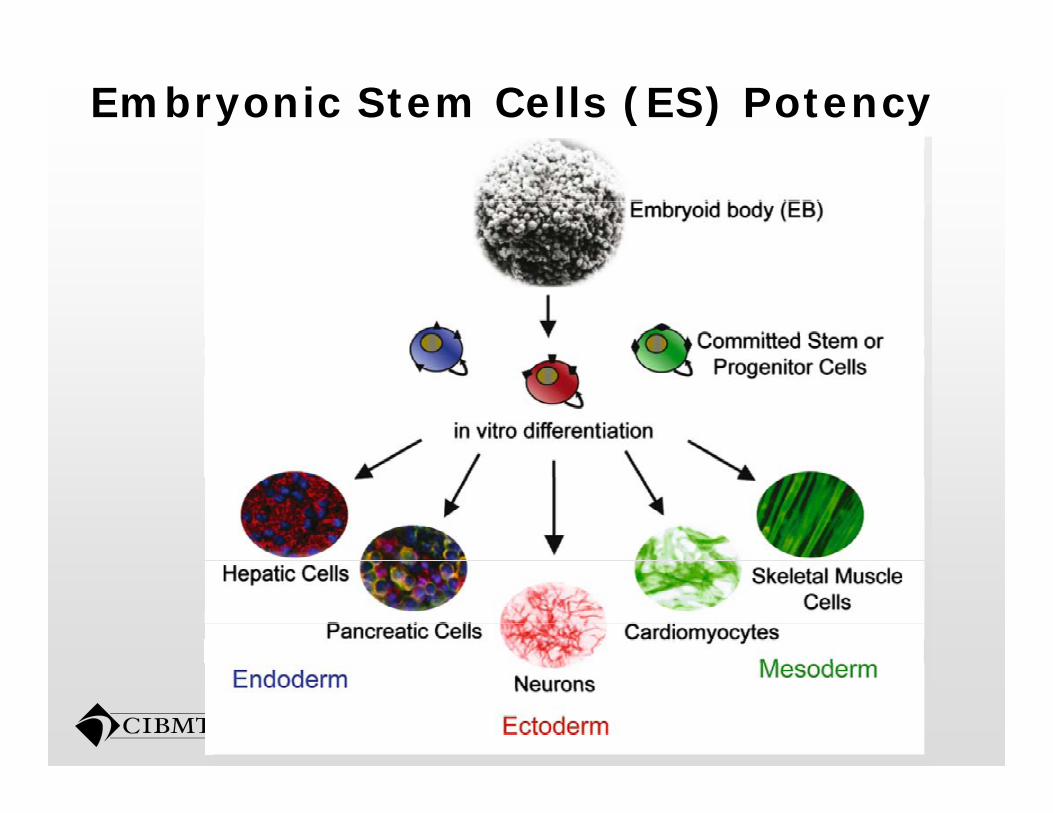
Embryonic Stem Cells (ES) Potency
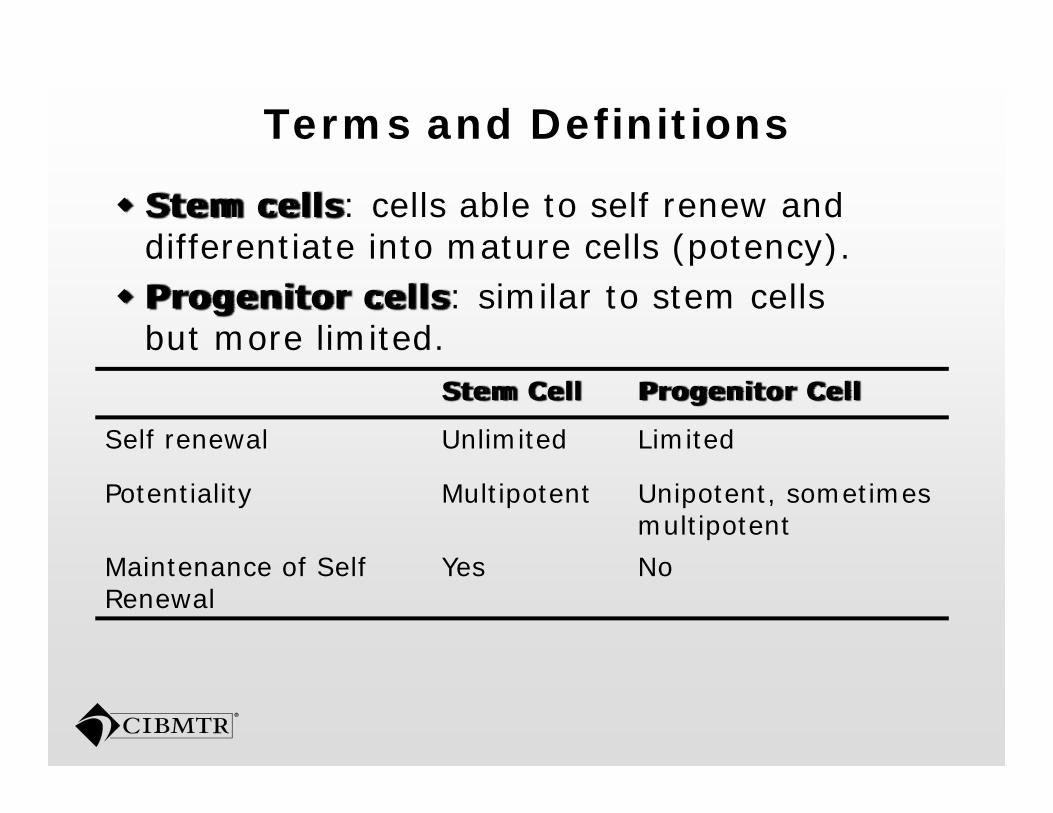
Terms and Definitions
Stem cells: cells able to self renew and differentiate into mature cells (potency)differentiate into mature cells (potency).Progenitor cells: similar to stem cells but more limited.
Stem Cell Progenitor Cell
Self renewal Unlimited Limited
Potentiality Multipotent Unipotent, sometimes multipotent
M i t f S lf Y NMaintenance of Self Renewal
Yes No
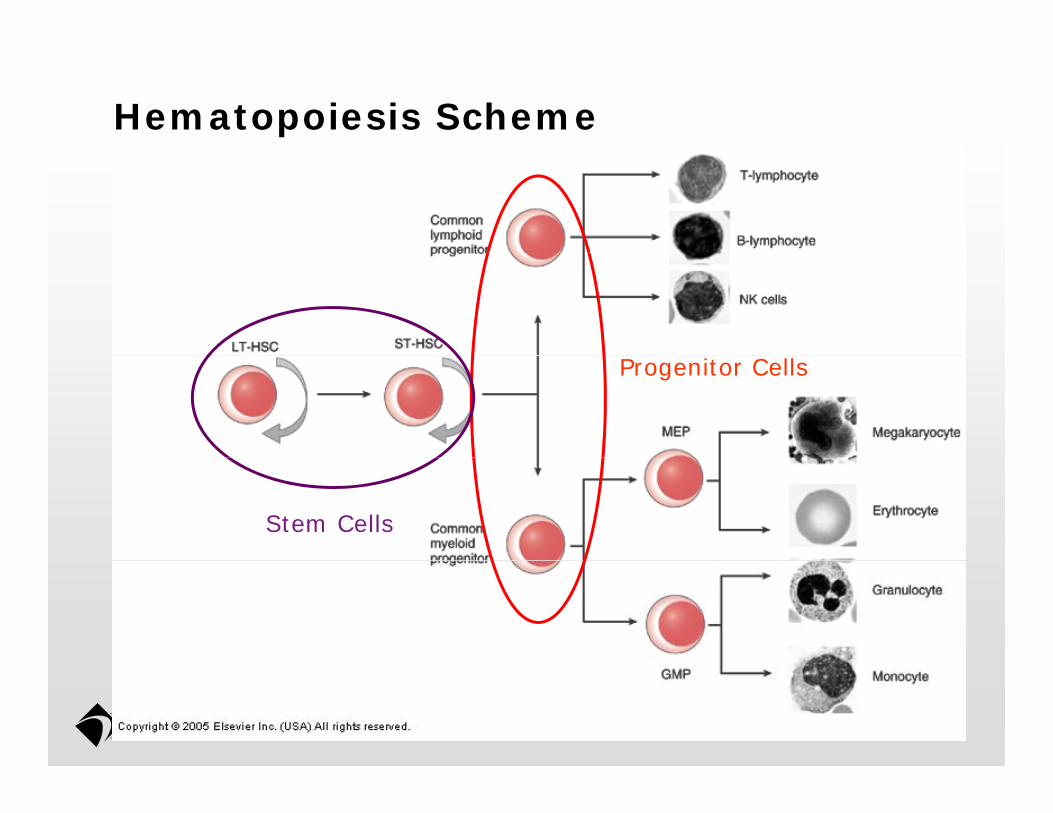
Hematopoiesis Scheme
Progenitor Cells
Stem Cells
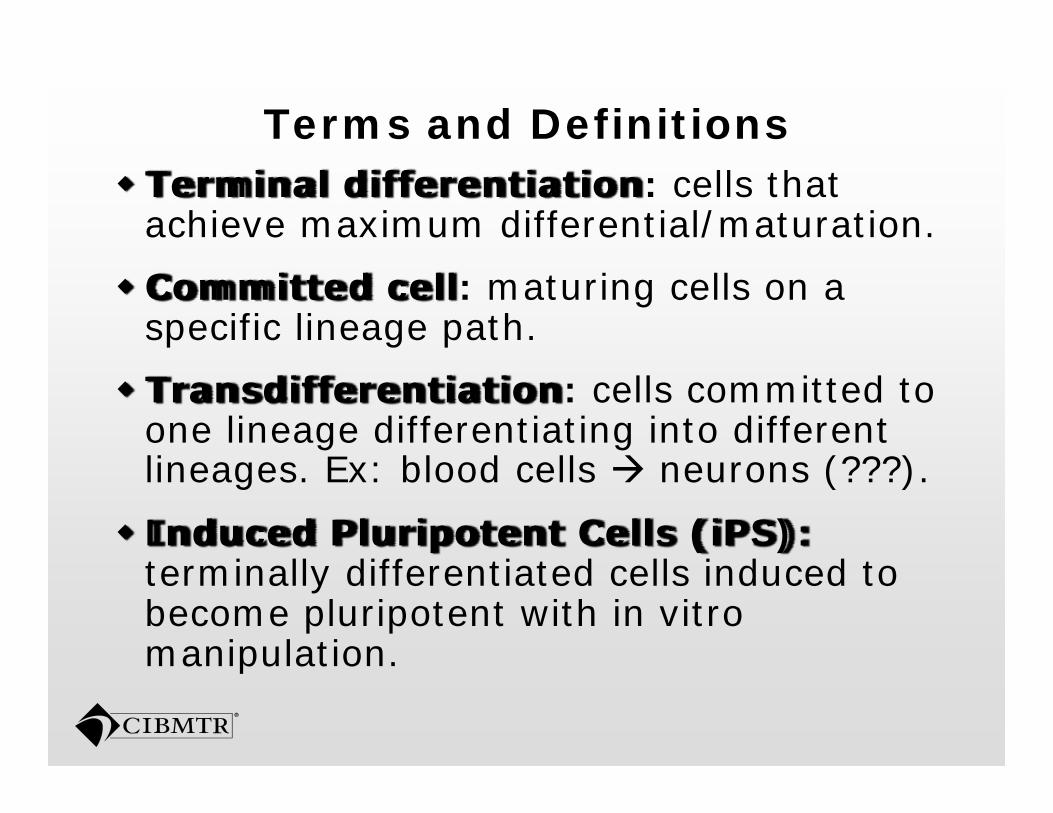
Terms and DefinitionsTerminal differentiation: cells that achieve maximum differential/maturation.
Committed cell: maturing cells on a specific lineage path.
Transdifferentiation: cells committed to one lineage differentiating into different li E bl d ll (???)lineages. Ex: blood cells neurons (???).
Induced Pluripotent Cells (iPS):t i ll diff ti t d ll i d d t terminally differentiated cells induced to become pluripotent with in vitro manipulation.manipulation.
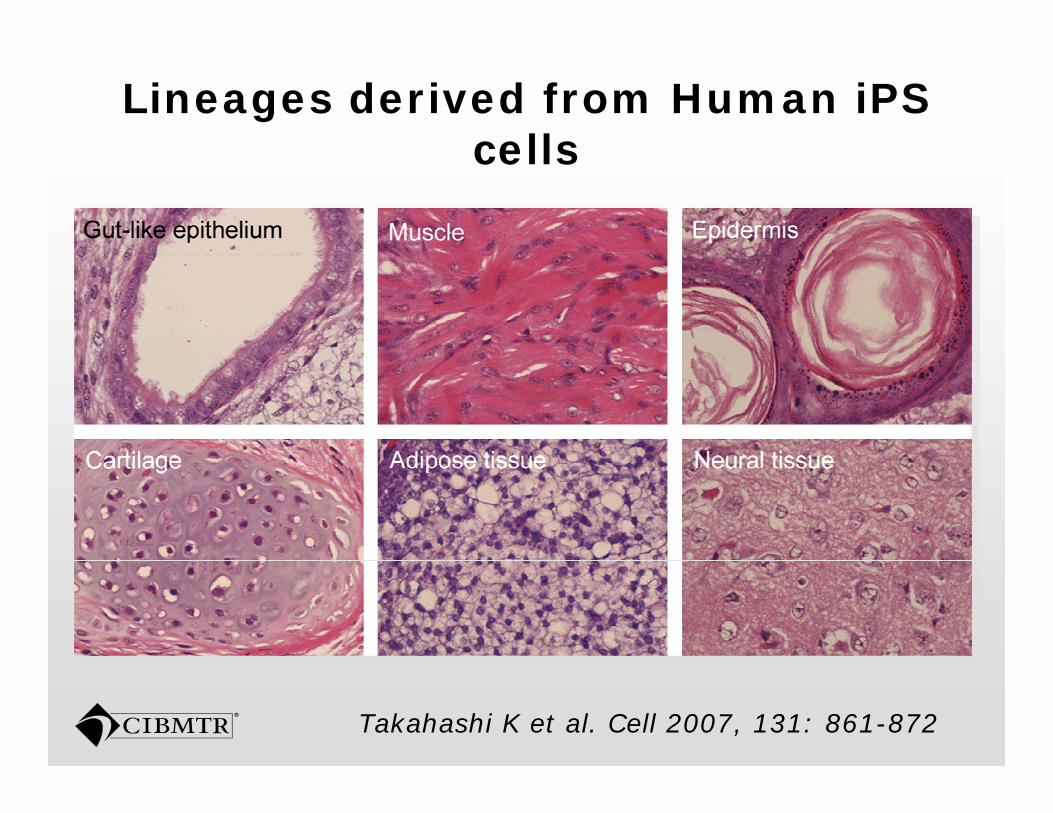
Lineages derived from Human iPS cellscells
Takahashi K et al. Cell 2007, 131: 861-872
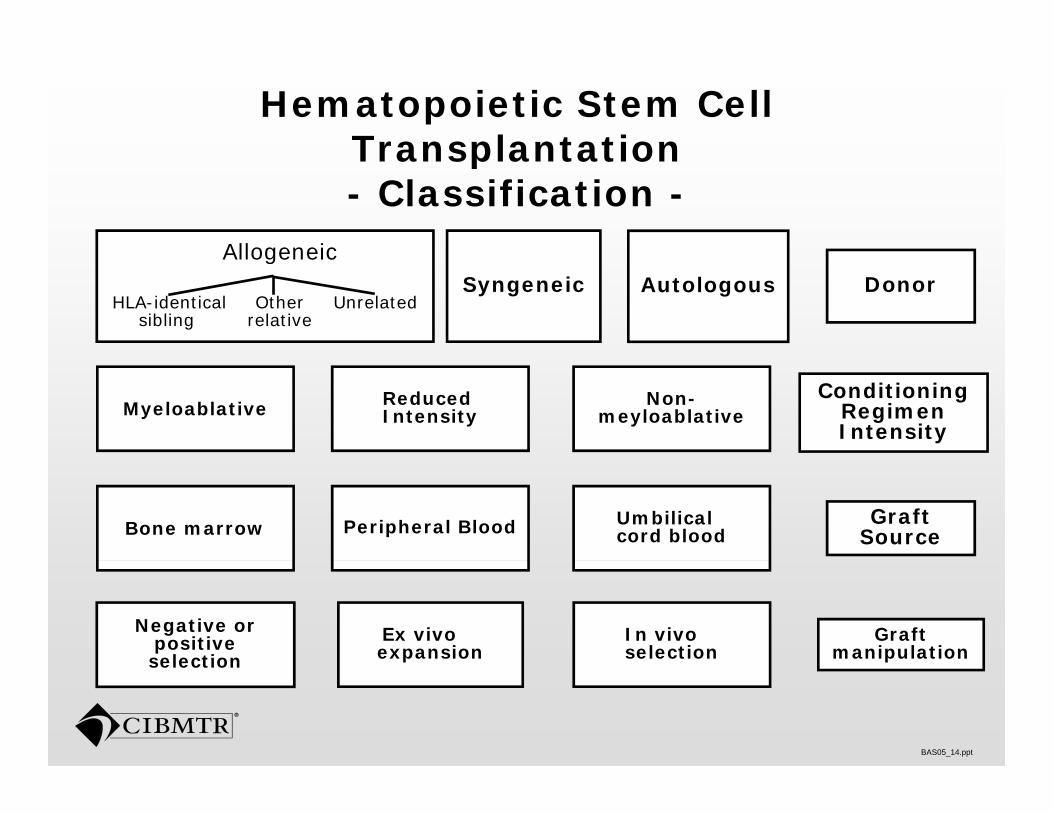
Hematopoietic Stem Cell Transplantation Transplantation - Classification -
AllogeneicAllogeneic
HLA-identical Other Unrelatedsibling relative
DonorSyngeneic Autologous
MyeloablativeConditioning
Regimen Intensity
Reduced Intensity
Non-meyloablative
Bone marrow Graft SourcePeripheral Blood Umbilical
cord blood
Negative or positive selection
Ex vivoexpansion
Graft manipulation
In vivoselection
BAS05_14.ppt
selection
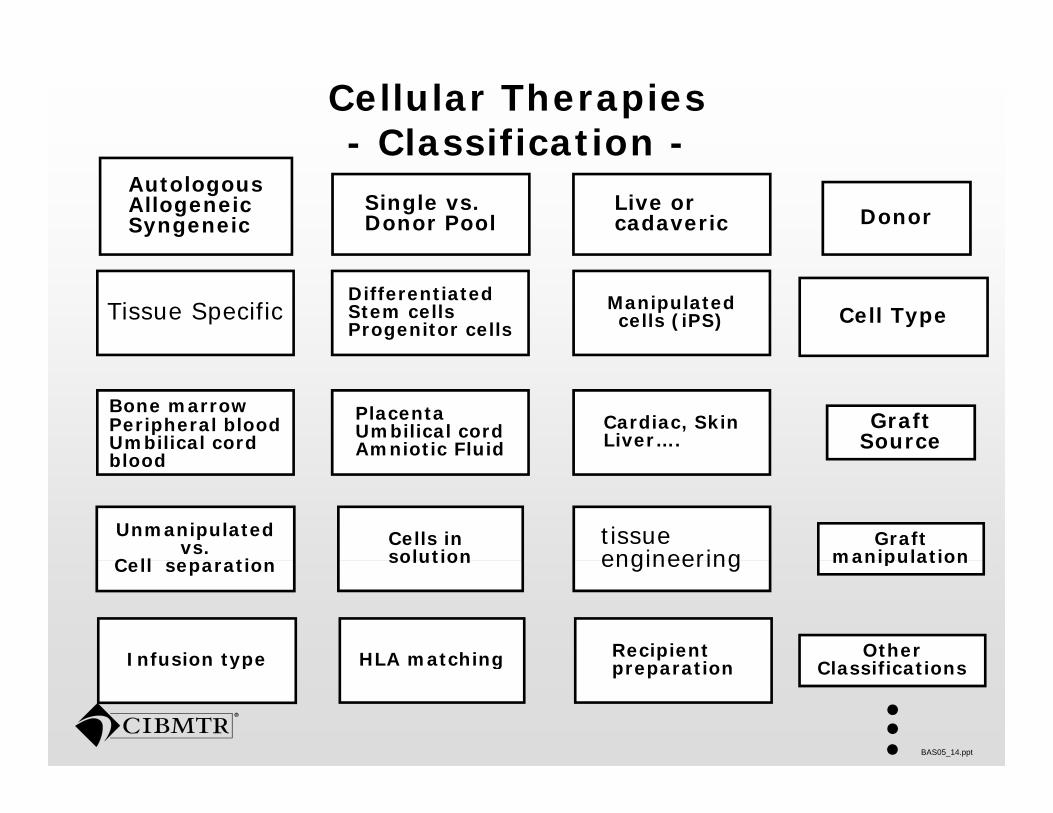
Cellular Therapies - Classification -Classification
DonorSingle vs. Donor Pool
Autologous Allogeneic Syngeneic
Live or cadaveric
Tissue Specific Cell TypeDifferentiated Stem cells Progenitor cells
Manipulated cells (iPS)
Bone marrow Peripheral blood Umbilical cord blood
Graft Source
Placenta Umbilical cord Amniotic Fluid
Cardiac, Skin Liver….
blood
Unmanipulated vs.
C ll ti Cells in solution
Graft manipulation
tissue engineeringCell separation solution manipulationengineering
Infusion type HLA matching Other Cl ifi ti
Recipient ti
BAS05_14.ppt
Infusion type HLA matching Classificationspreparation
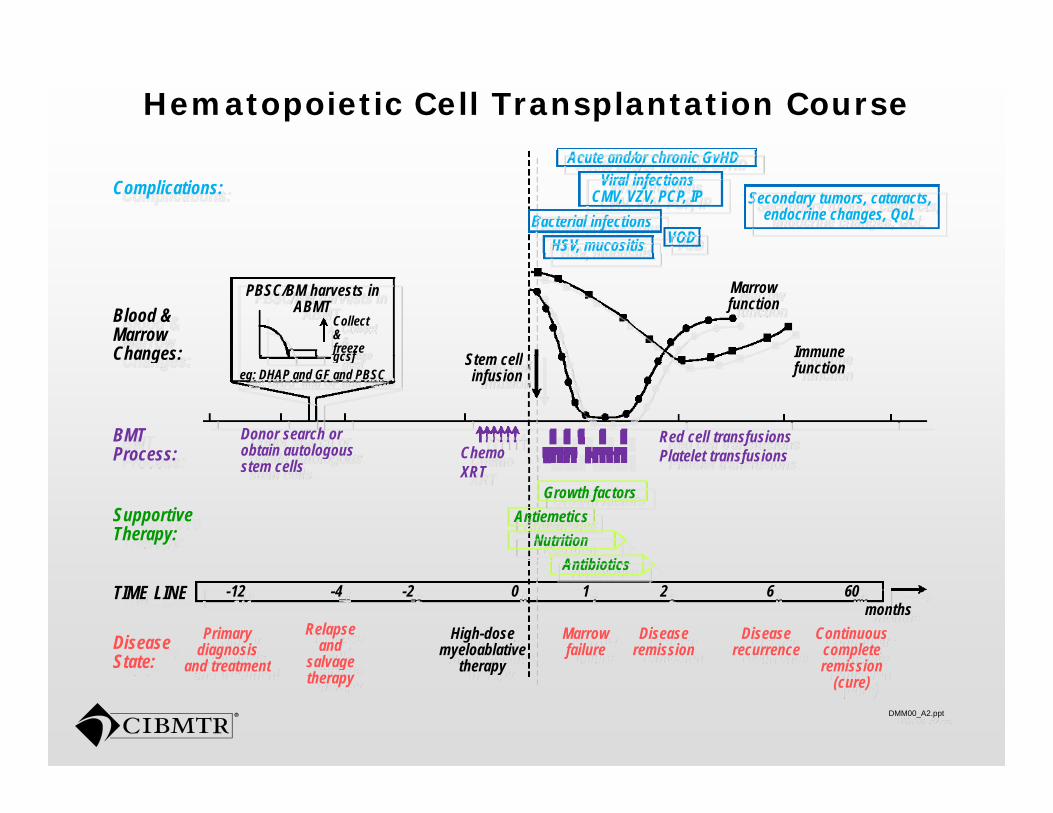
Hematopoietic Cell Transplantation Course
Complications: Secondary tumors, cataracts, endocrine changes, QoL
Acute and/or chronic GvHDViral infections
CMV, VZV, PCP, IPBacterial infections
HSV, mucositis VOD
Blood & Marrow Changes:
PBSC/BM harvests in ABMT
,
St ll
Marrow function
Immune
Collect & freezegcsfChanges:
BMT Process:
Red cell transfusionsPlatelet transfusions
Donor search or obtain autologous Chemo
Stem cellinfusion
Immune functioneg: DHAP and GF and PBSC
gcsf
Process:
Supportive Therapy:
A tibi tiNutrition
AntiemeticsGrowth factors
Platelet transfusionsgstem cells
Chemo XRT
TIME LINE -12 -4 -2 0 1 2 6 60months
Marrowfailure
Diseaseremission
Diseaserecurrence
Continuous complete remission
High-dose myeloablative
therap
Primary diagnosis
and treatment
Relapse and
salvageDisease State:
Antibiotics
DMM00_A2.ppt
remission (cure)
therapyand treatment salvage therapy
State:
Cellular Therapy Course
Multiple infusions along a period of time or single infusions, or implantation.Engraftment or not (depending on potency)Early toxicities
Infusion reactionsInfusion reactionsLate toxicities:
Second malignancies (?)“ d ff ”“Miss-differentiation” GVHDMalignancy Relapseg y p
Milestones are not well defined for all cellular therapies.
Cellular Therapy Related to Hematopoietic Stem Cell Hematopoietic Stem Cell
Transplantation
HCT related Cellular Therapy: Donor Cellular infusions (DCI)Donor Cellular infusions (DCI)
DCI is a common terminology used in the DCI is a common terminology used in the CIBMTR forms.
Related to any cell infusion occurring after a Related to any cell infusion occurring after a HCT without a preparative regimen
The donor most times is the same but it The donor most times is the same, but it does not need to be.
“Off the shelf” MSCs: unknown donorsOff the shelf MSCs: unknown donors
Patients may receive GVHD prophylaxis.
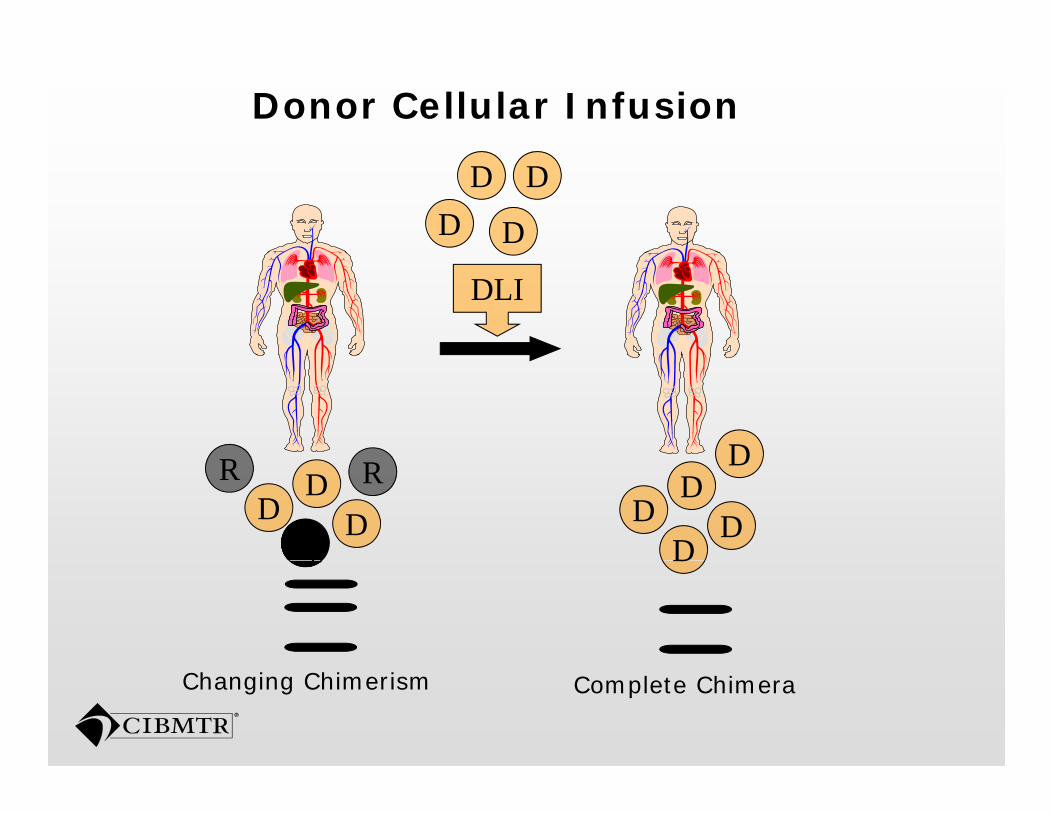
Donor Cellular Infusion
D
D
DD
DLI
D
DRL
RR DD
DD
DD
DL D
Complete ChimeraChanging Chimerism
Indications for DCI
Relapse prophylaxisTreatment of relapse: CML, AML, MM and others. D li i d hi i ( ft f il )Declining donor chimerism (graft failure)Treatment of post transplant malignancy:
PTLD (Lymphoma)PTLD (Lymphoma)
Treatment of Viral Infections Treatment of GVHD (Mesenchymal Stromal Treatment of GVHD (Mesenchymal Stromal Cells)
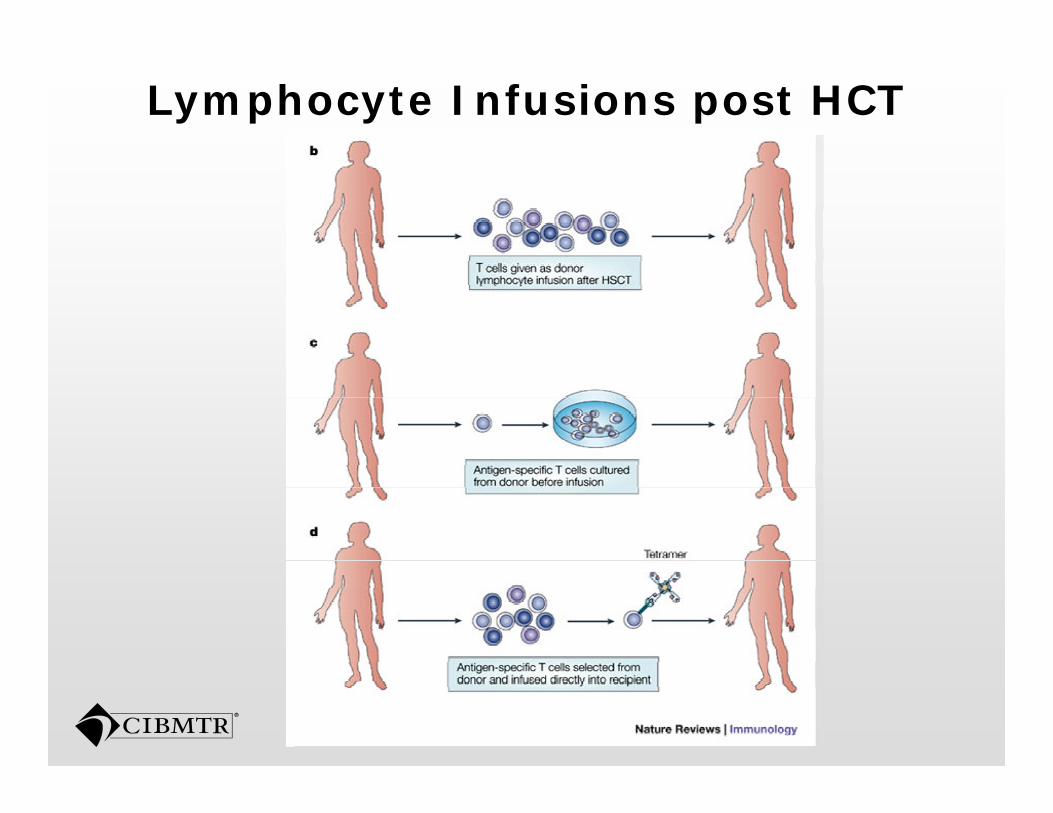
Lymphocyte Infusions post HCT
Cytotoxic T-Cells (CTLs) for viral illnessillness
Ummanipulated lymphocytes:Decrease numbers of viral specific CTLsDecrease numbers of viral specific CTLsPresence of alloreactive T-cell that increase the risk of GVHD and further increase the risk of GVHD and further immunessupression.
Strategies:Strategies:Decrease the content of alloreactive T cells;Development of virus specific CTLs
EBV, Adenovirus and CMV.
Mesenchymal Stem Cells or Mesenchymal Stromal Cells (MSC)Mesenchymal Stromal Cells (MSC)What are these cells?
M h l ll f b l Mesenchymal cells: from embryology are cells from the mesenchima or mesoderm that will give origin to blood, blood vessels, that will give origin to blood, blood vessels, bone and muscle.
Stromal cells: cells from tissue stroma, Stromal cells: cells from tissue stroma, promotes scaffolding and sustain other cells in the tissue.
Mesenchymal Stem cells: cells from the bone marrow that have the capacity to
t b f t d tilgenerate bone, fat and cartilage.
Mesenchymal Stem Cells
Cells with multipotent capacity,
Demonstrate adherence to plastic
Distinct immunophenotypic pattern. p yp p
Bone marrow derived but similar cells are isolated from other tissuesisolated from other tissues.
Multipotent mesenchymal stromal cells is th t i l d i th another terminology used in the
literature and more appropriate for these cells cells.
MSCs in Clinical Medicine
Simple isolation from bone marrow.Normal function is to protect and Normal function is to protect and sustain hematopoietic stem cells.It does not require HLA matchingIt does not require HLA matching.Currently being used for treatment of GVHD due to its effect in inducing GVHD due to its effect in inducing immunetolerance.Other applications under investigation:pp g
Promote engraftment in UCB HCTInflammatory bowel disease, yautoimmune diseases, cardiac diseases.
Cellular Therapy for Regenerative Medicine or Emerging Indication
Cellular Therapy for Regenerative MedicineMedicine
Rapidly evolving field with ramifications to most medical specialtiesto most medical specialtiesUtilize cells for treatment of non-hematologic illnesseshematologic illnessesBone marrow derived cells are most
l d tl commonly used presently. Indications include: cardiovascular,
l i l t i neurological, autoimmune, musculoskeletal among others.
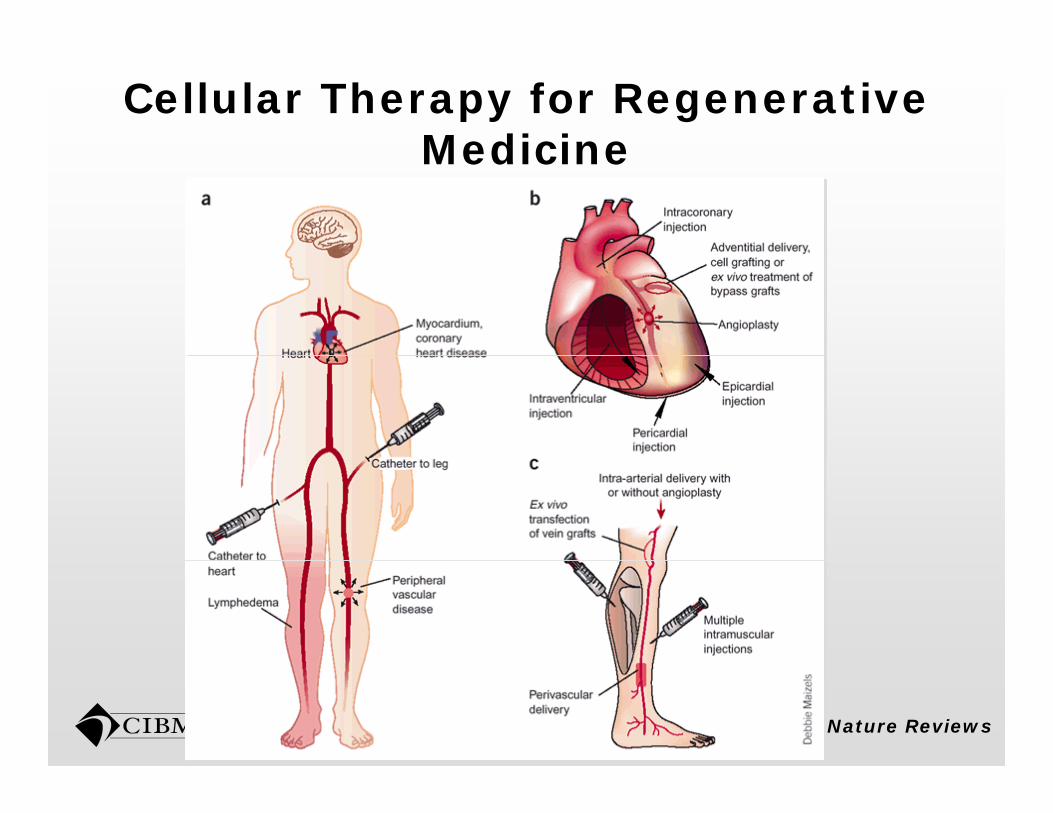
Cellular Therapy for Regenerative MedicineMedicine
Nature Reviews
Cardiac Applications for Cellular therapiestherapies
Indications with largest experience.Treatment for myocardial infarctionTreatment for myocardial infarction.Mainly bone marrow derived cells:
Unmanipulated CD34+selection MSC cardiac Unmanipulated, CD34+selection, MSC, cardiac progenitor cells.
Infusion: intracoronary, intracardiac. Timing: within days from AMI but variable.Outcomes: Ejection fraction, other volume and pressure measurements, survival. Promising outcomes: improvement of EF and
i lsurvival.
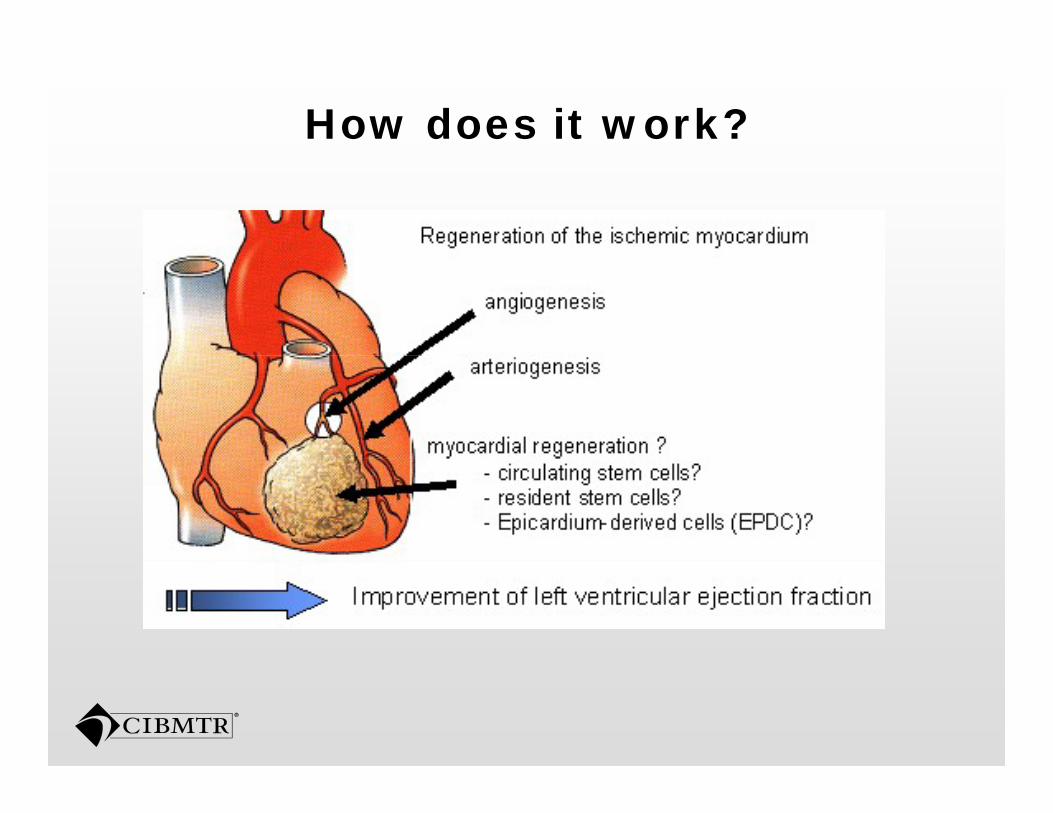
How does it work?
Cellular Therapy for Vascular DiseasesDiseases
Arterial insufficiency and ulcers.C ll t b d i d Cell types: bone marrow derived selected or unmanipulated.
I l i f d h li l i ll Isolation of endothelial progenitor cells (EPCs)
I t t i l i t l i j tiIntrarterial or intramuscular injectionsImprovement in ulcer healing, pain
d i l i d i h and arterial pressure indexes in the treated limb.
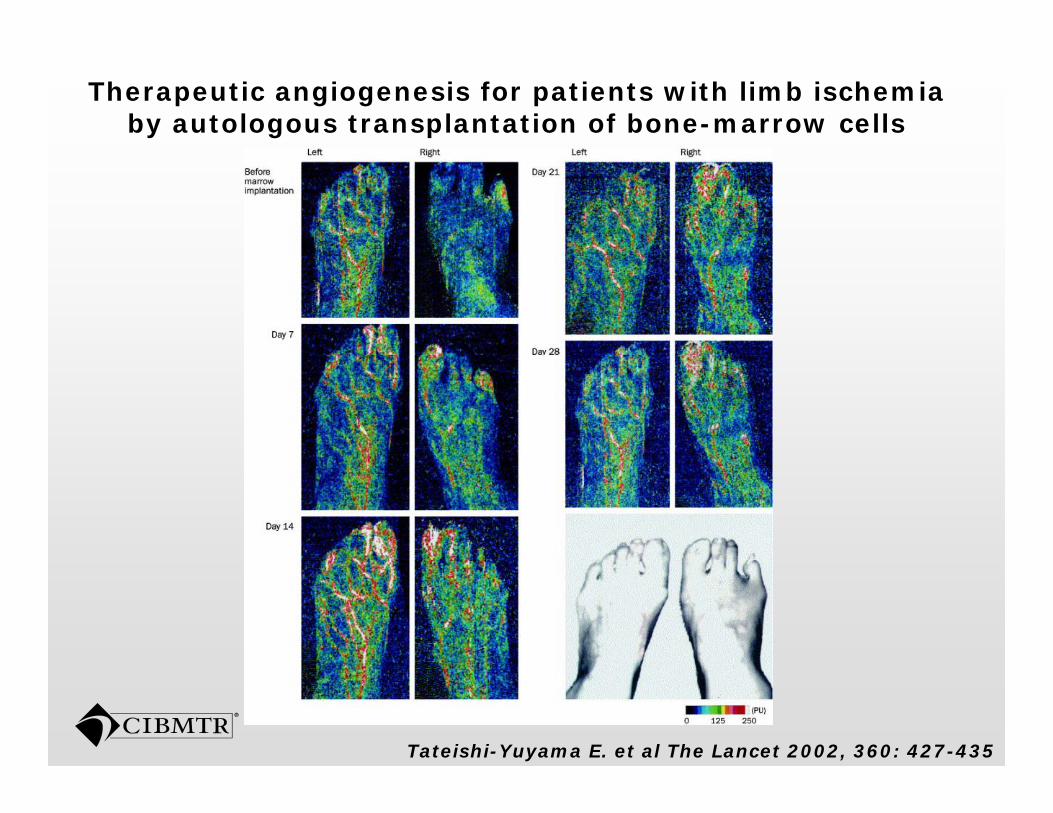
Therapeutic angiogenesis for patients with limb ischemia by autologous transplantation of bone-marrow cells
Tateishi-Yuyama E. et al The Lancet 2002, 360: 427-435
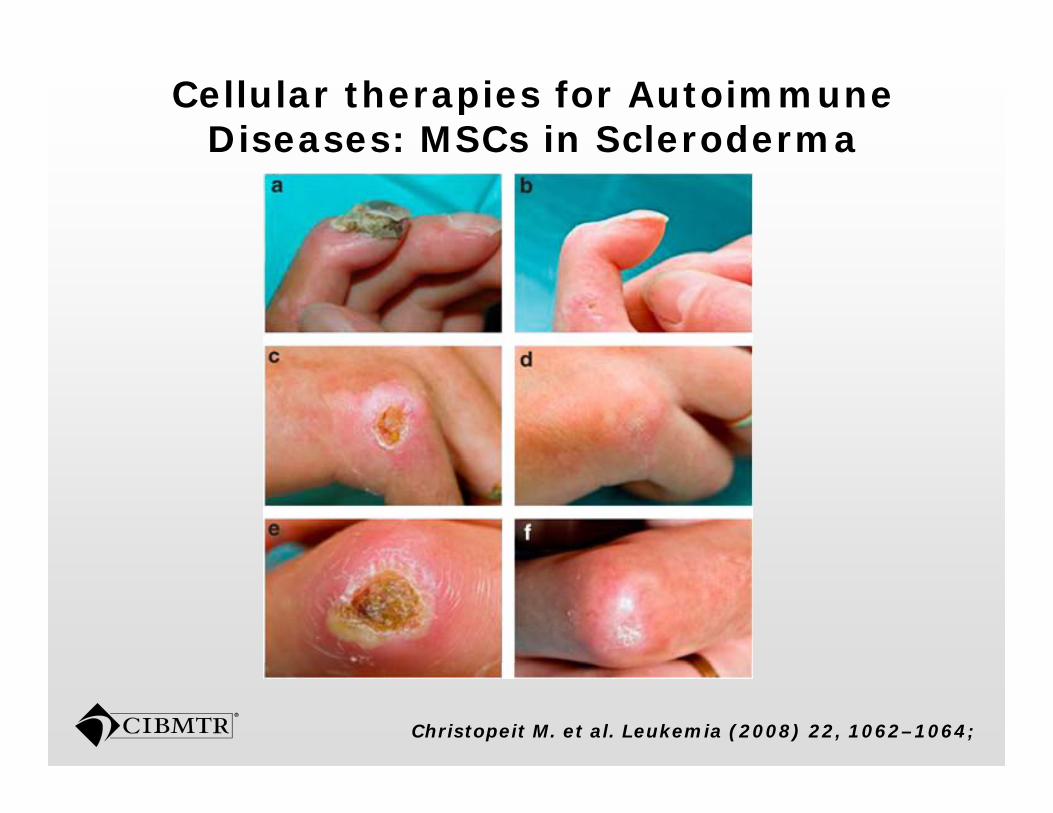
Cellular therapies for Autoimmune Diseases: MSCs in SclerodermaDiseases: MSCs in Scleroderma
Christopeit M. et al. Leukemia (2008) 22, 1062–1064;
Cellular Therapy for Neurologic IndicationsIndications
Parkinson’s disease, stroke, spinal cord injury multiple sclerosisinjury, multiple sclerosis.Stereotatic implantation of cells
d d lMS: standard autologous HCT as salvage after high dose i i immunessupression.
Use of MSC as an anti-inflammatory, remains investigational remains investigational.
Cellular Therapy for Orthopedic IndicationsIndications
Imp o e of onne ti e ti e he lingImprove of connective tissue healing.Application of tissue engineering with h d t l d t ichondrocyte-layered matrices
MSC derived condrocytesSurgical implantation
Other indications being investigatinginvestigating
Crohn’s Disease and ulcerative colitisSystemic Lupus ErythematousSystemic Lupus ErythematousDiabetes mellitus type IRheumatoid ArthritisRheumatoid ArthritisAvascular Necrosis of the FemurA i t hi L t l S l iAmiotrophic Lateral SclerosisMyasthenia gravisA t b l l i h iAcute cerebral vascular ischemiaBad mortgages!!!
Development of the Cellular Therapy Registry
Why a cellular therapy registry? Why should the CIBMTR be involved?should the CIBMTR be involved?
HCT is a type of cellular therapy.Experience with HCT outcomes Experience with HCT outcomes research.Experience in developing and Experience in developing and maintaning large databases.Many cellular therapies are within the Many cellular therapies are within the HCT field.Well established infrastructureNetwork of centers that are starting cellular therapy programs.
SCTODCollect data on outcomes of all allogeneichematopoietic stem cell transplants in the US
Collect data on outcomes of all transplants facilitated by the CW Bill Young Program – even if transplant done outside the UStransplant done outside the US
Include alternative uses of hematopoietic stem cellscells
Core set of data – sufficient to allow center-specific survival and other analysesy
Subset of Report Form data
Establish related donor-recipient specimen p prepository
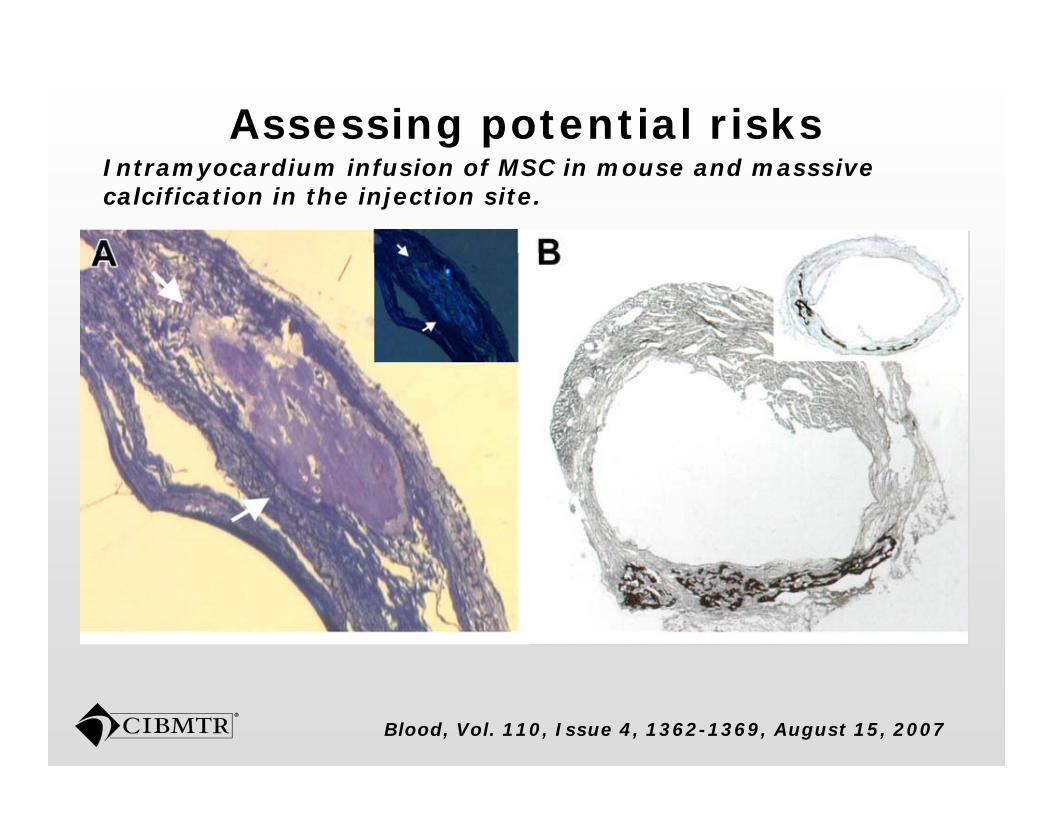
Assessing potential risksIntramyocardium infusion of MSC in mouse and masssive calcification in the injection site.
Blood, Vol. 110, Issue 4, 1362-1369, August 15, 2007
Challenges
Programs on cellular therapy are not the same as HCT, even though same , ginstitution. Beyond hematology and oncology f ldfields.Other specialist might not be i t t d i ll b ti interested in collaboration. Clinical trials with confidential data.Off th h lf d t ith i il Off the shelf products with similar scrutiny as pharmaceutical products.
Cell types being patented Cell types being patented.
Strategy
Develop an interest group within the registry that became the Cellular Therapies Working that became the Cellular Therapies Working Committee (CTWC)Establish a subcommittee to develop a data pcollection tool – CTED.Collaboration with European colleagues.Distribution and implementation of the form.Survey centers involved with cellular th therapy.
Data Collection on Cellular Therapy
Data Collection on Cellular TherapiesTherapies
Incorporate data collection in the same system of CIBMTR formssystem of CIBMTR forms.Separate data collection forms into:
HCT l t d DCIHCT related DCICellular Therapies for regenerative
di imedicine.Any cell for any indication other than replacement of hematopoietic system replacement of hematopoietic system.
HCT-related cellular therapy: DCI
This data is already being collected.Registration level Post TEDRegistration level- Post-TEDResearch
DCI form Baseline follow up form DCI form Baseline follow up form (Combine 2200)
HCT vs DCIHCT vs DCIConditioning regimenWhat was the previous transplantWhat was the previous transplantIndicationType of cells infused yp
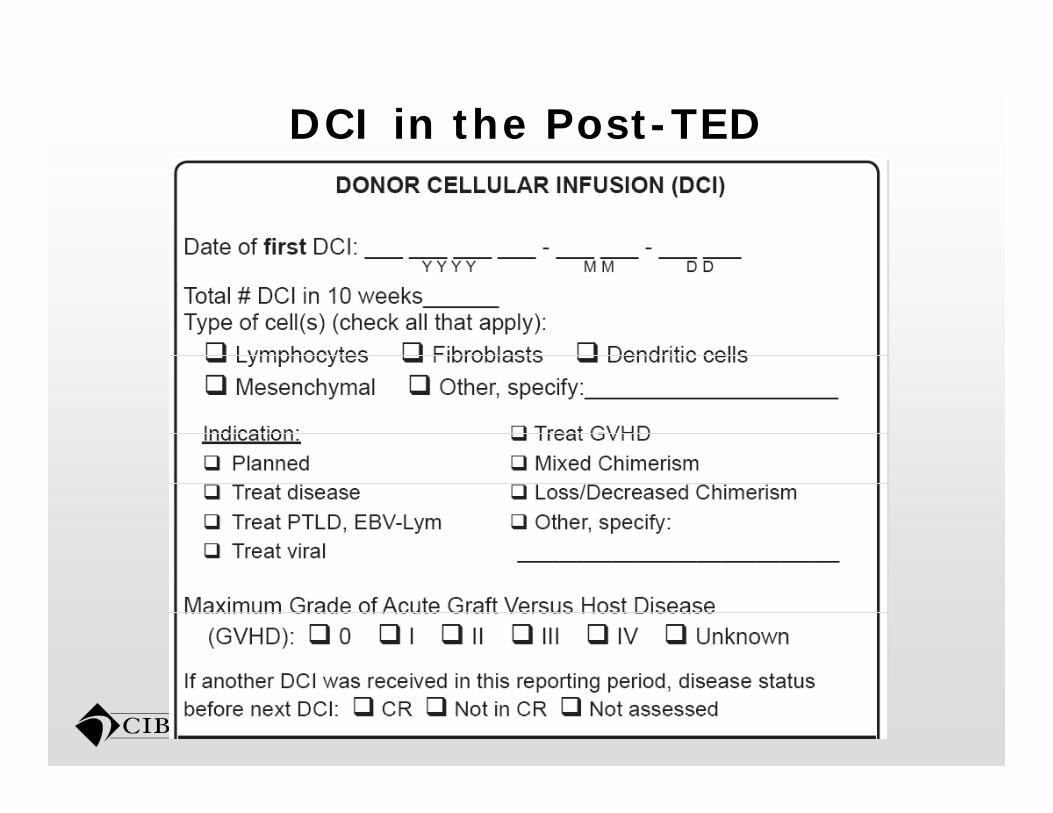
DCI in the Post-TED
Collection of DCI data in ResearchAll DCIs within a 28 day period.
Additional DCIs beyond this period will Additional DCIs beyond this period will require new reporting.
Components:Components:DateNumber of infusionsNumber of infusionsIndication:
Planned treatment of relapse PTLD Planned, treatment of relapse, PTLD, GVHD, viral infection, stable/mixed chimerism, loss of chimerism, other., ,
Collection of DCI data in ResearchComponents (Cont.):
Disease status (primary disease) and date.Disease status (primary disease) and date.Performance statusCells sourceCells sourceType of cells and cells dosesCell manipulationCell manipulation
Collection of Cellular therapy for regenerative medicineregenerative medicine
Extremely broad topic.R i t ti t fRegistration-type form.Collaboration with the EBMT.Start as a non-longitudinal database.Assign an unique ID to all recipients.g q pTrigger to collect the form may be applied different depending on the pp p gcenter.
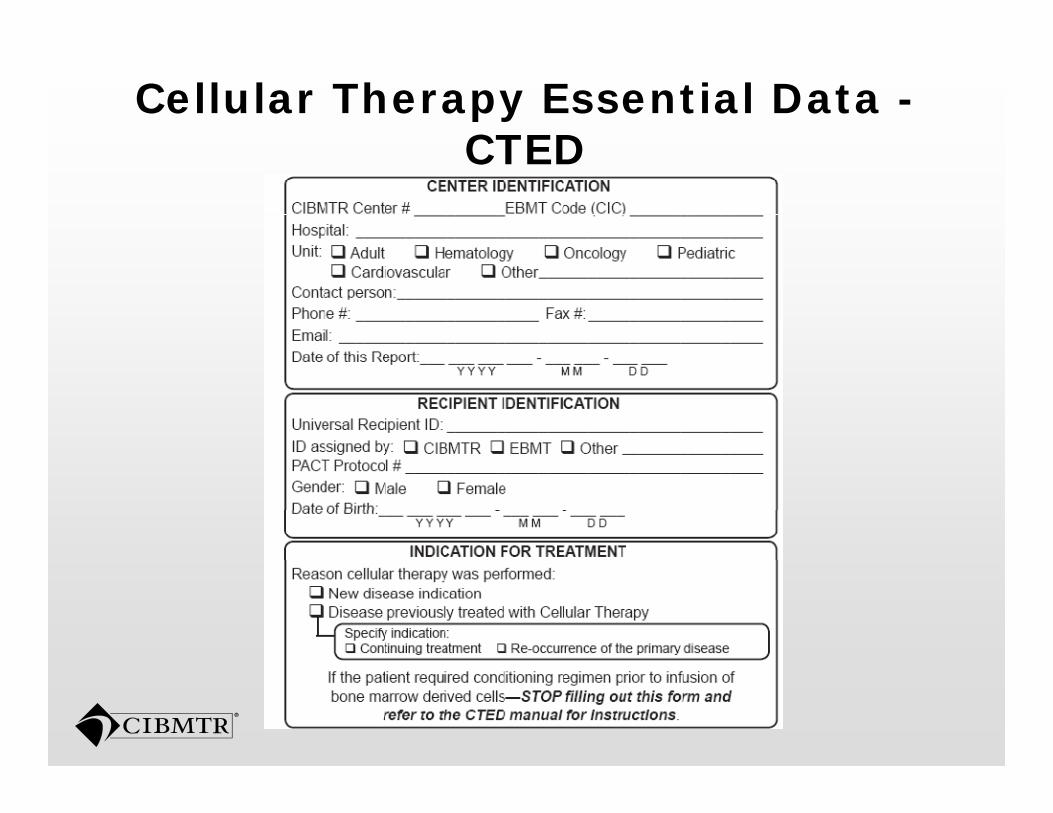
Cellular Therapy Essential Data -CTED CTED
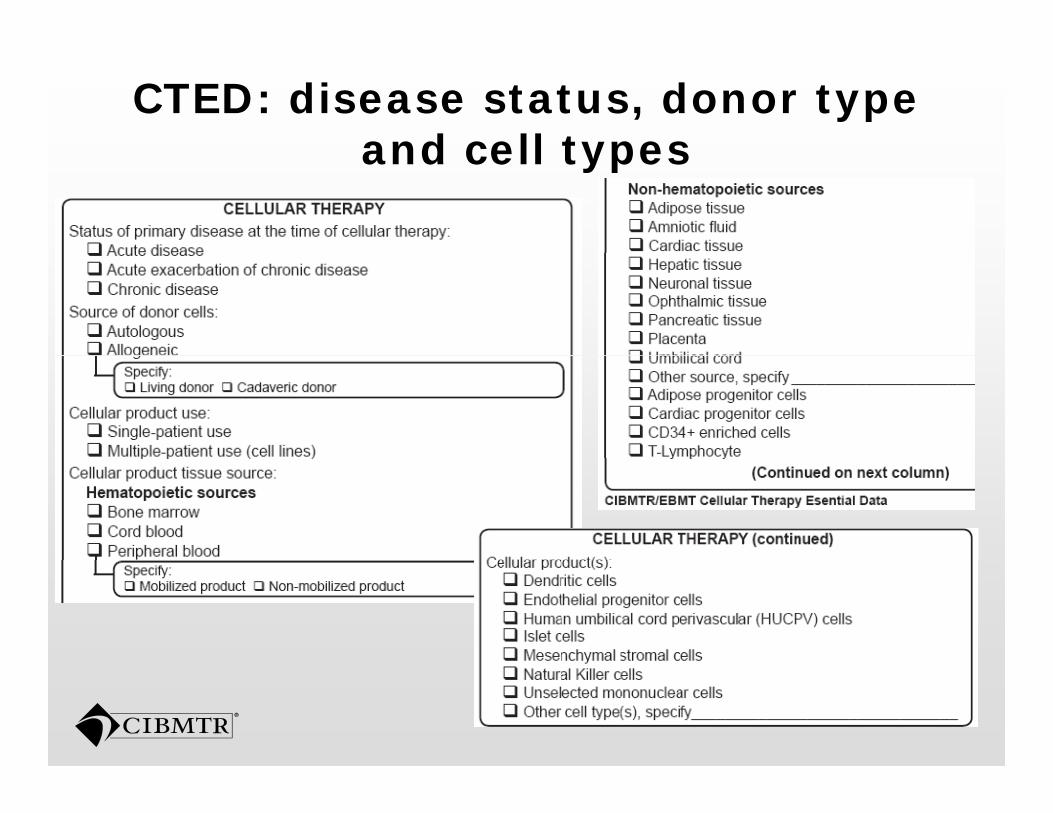
CTED: disease status, donor type and cell typesand cell types
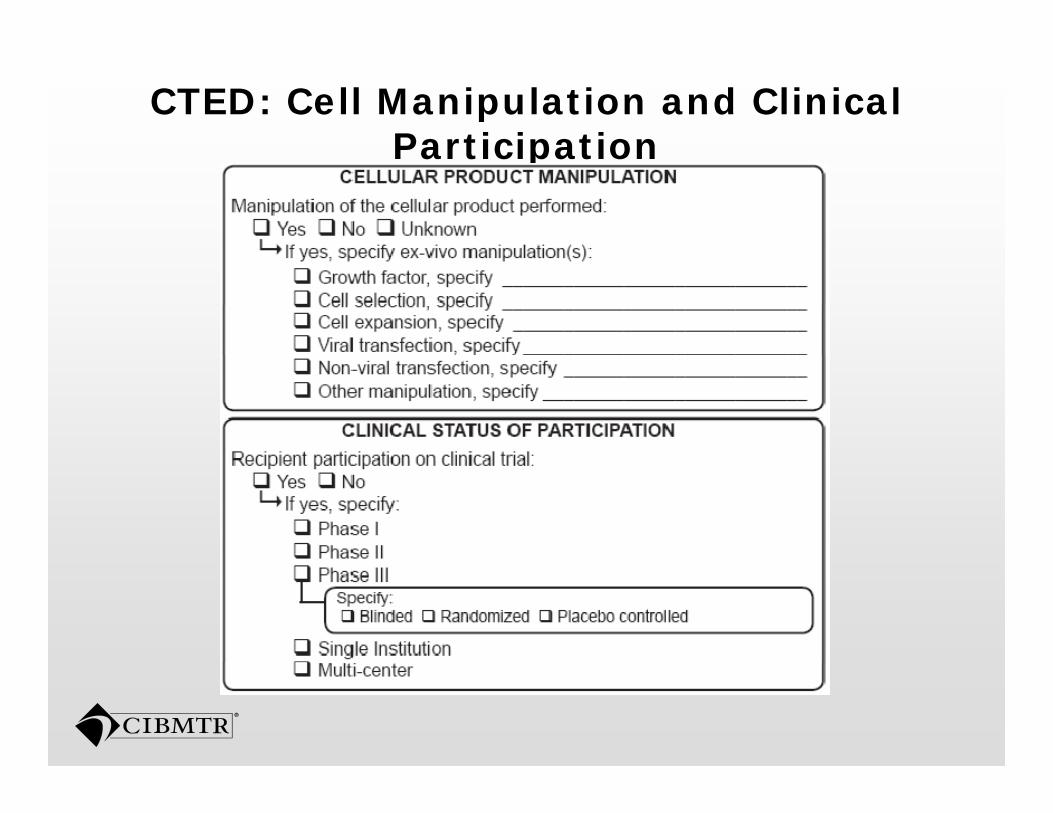
CTED: Cell Manipulation and Clinical ParticipationParticipation
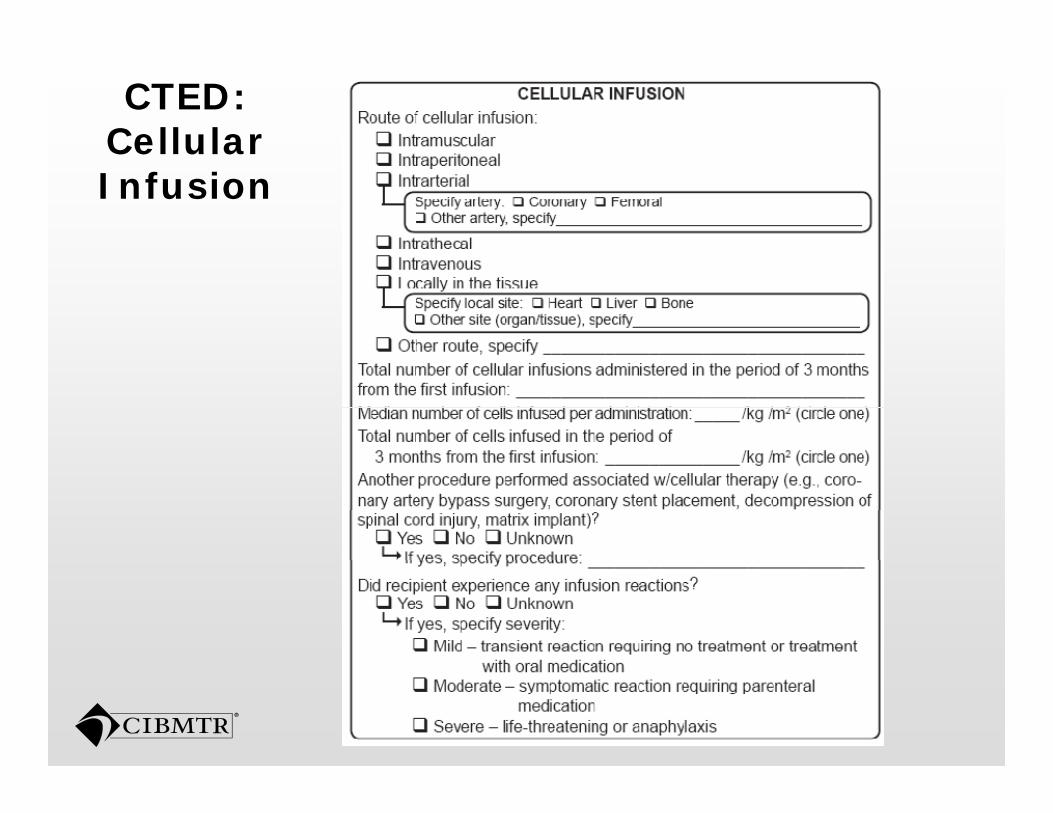
CTED:Cellular Cellular Infusion
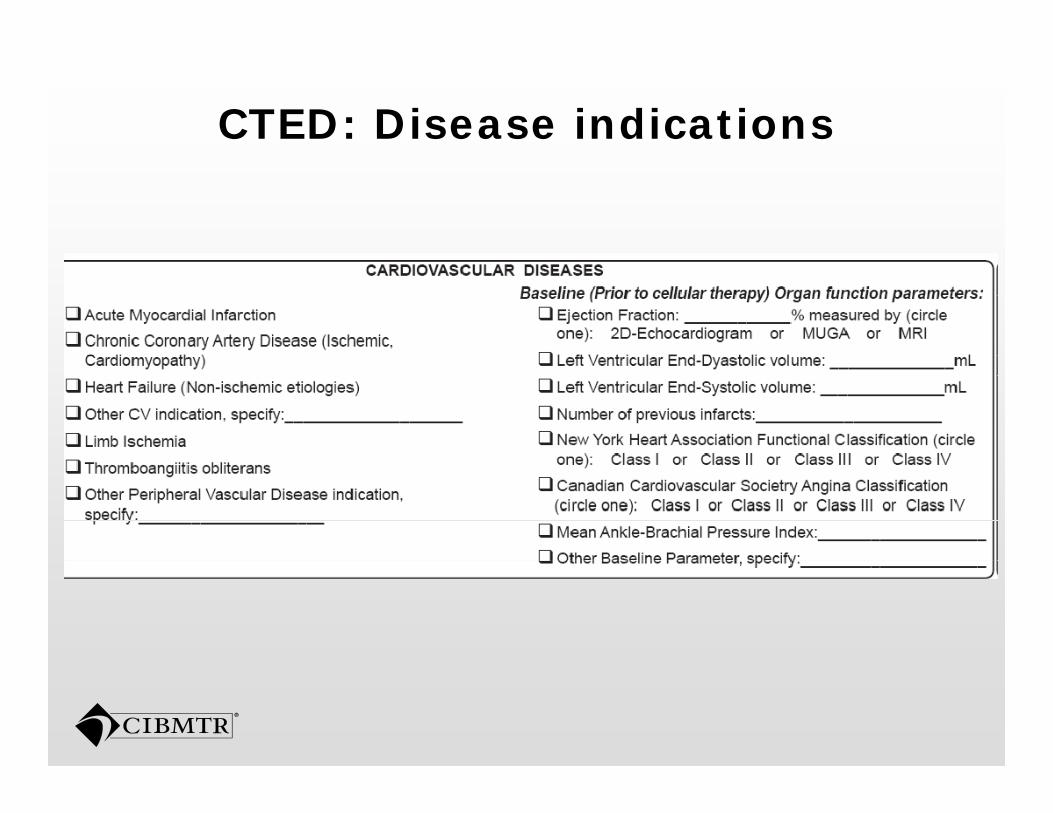
CTED: Disease indications
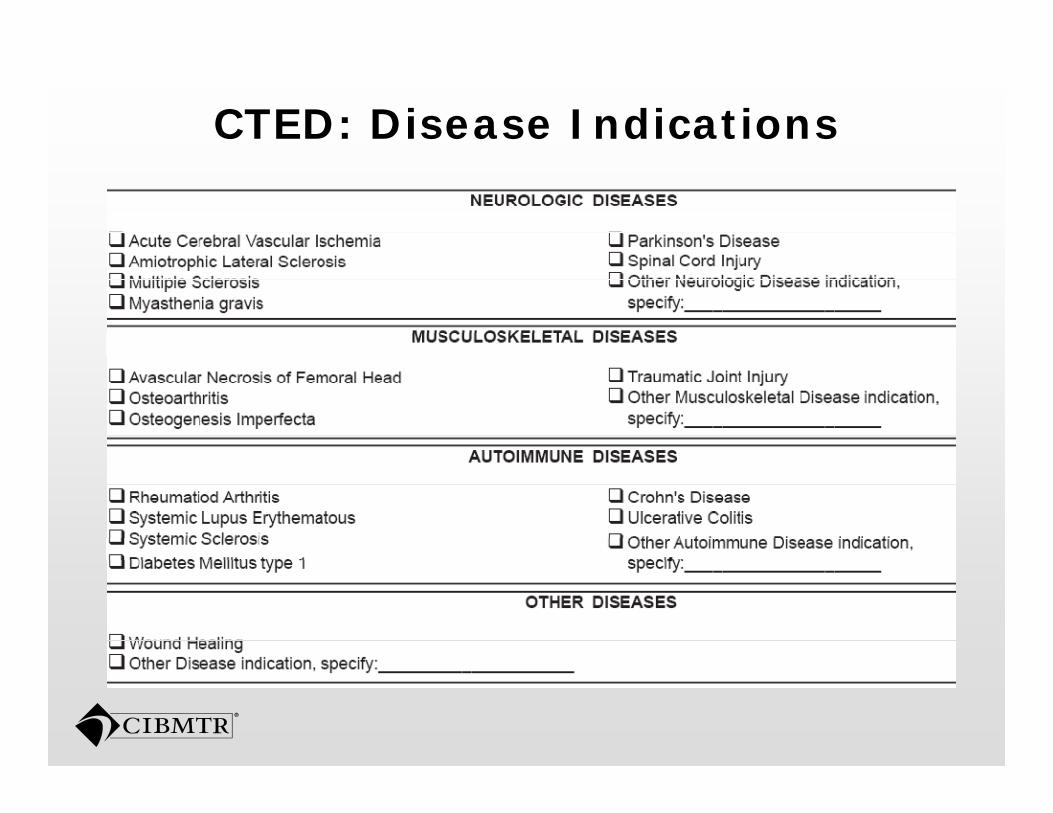
CTED: Disease Indications
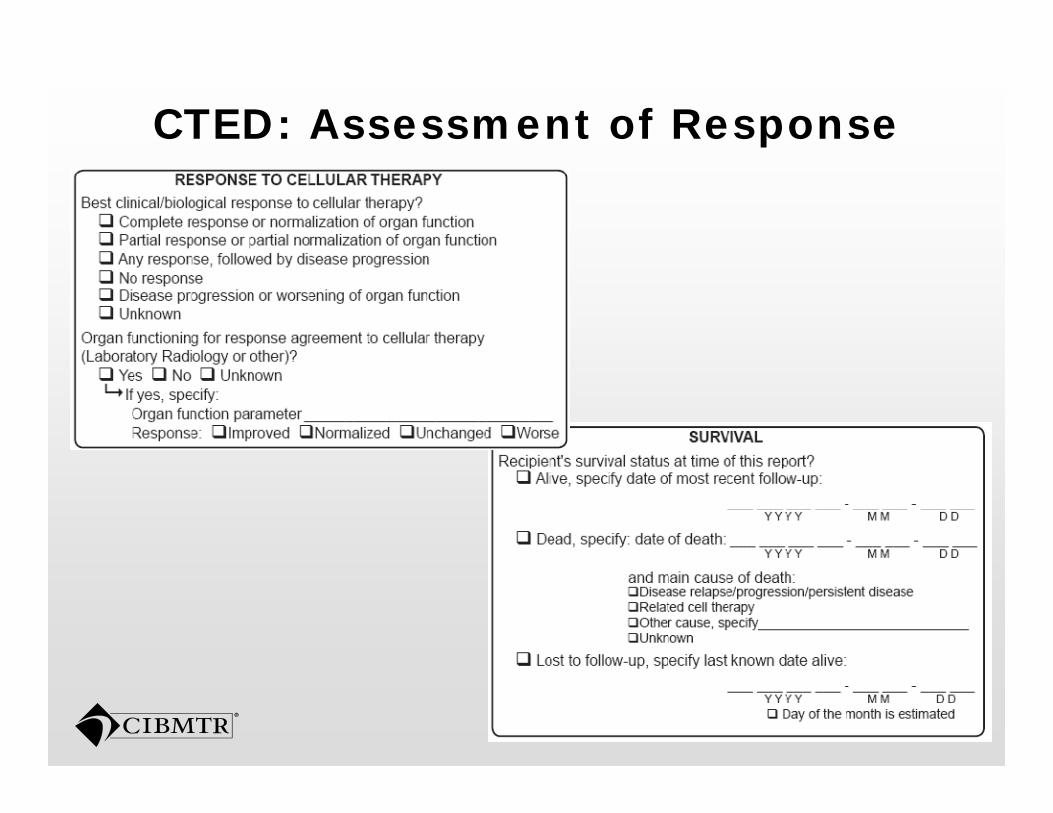
CTED: Assessment of Response
Conclusions
Definitions are important in this emerging fieldemerging field.Not all stem cells are the same, remember the concept of potency and remember the concept of potency and self renewal. R idl h i fi ld ith l t f Rapidly changing field with a lot of promises with clinical data still maturingmaturing.
Conclusions
Importance to set up an infrastructure for data collection for future studiesfor data collection for future studies.
Applying our current forms system to this immense field will be a challenge but we have a good head start already!
Thank you Thank you
Cellular Therapy Working CommitteeCommittee
Leadership:
Armand Keating, MD
Forms SubcommitteeAdrian GeeSergio GiraltArmand Keating, MD
Princess Margaret Hospital, Toronto
Helen Heslop, MD
Sergio GiraltHelen HeslopEdwin HorwitzArmand KeatingHelen Heslop, MD
Baylor College of Medicine, Houston
Joshua Hare MD
Armand KeatingDiane KnutsonKathy LoperMarie MatlackJoshua Hare, MD
University of Miami, Miami
Marie MatlackMarcelo PasquiniPhilip Rowlings
Additional Input from EBMT:Wim FibbeKatarina LeBlanc Al T d llAlan Tyndall
Q&A and Data Managers/Clinical Research Professionals Input