Embed Size (px)
Citation preview

PROTECTINGTHE NATION’S
HEALTHIN AN ERA OF
GLOBALIZATIONCDC’s Global
Infectious DiseaseStrategy
Department ofHealth and Human Services
Centers for Disease Controland Prevention

DEPARTMENT OF HEALTH AND HUMAN SERVICESTommy G. Thompson, Secretary
CENTERS FOR DISEASE CONTROL AND PREVENTIONJeffrey P. Koplan, M.D., M.P.H., DirectorDavid Fleming, M.D., Deputy Director for Science and Public HealthStephen B. Blount, M.D., M.P.H., Director, Office of Global Health
National Center for Infectious DiseasesJames M. Hughes, M.D., Director
National Center for HIV, STD, and TB PreventionHarold Jaffe, M.D., Acting Director
National Immunization ProgramWalter A. Orenstein, M.D., Director
Epidemiology Program OfficeStephen B. Thacker, M.D., M.Sc., Director
Public Health Practice Program OfficeEdward L. Baker, M.D., M.P.H., Director
The following CDC staff members prepared this report.Scott F. Dowell, M.D., M.P.H., National Center for Infectious DiseasesAlexandra M. Levitt, Ph.D., National Center for Infectious Diseases
With input from the Global Infectious Diseases Strategy Working Group
Jay McAuliffe, M.D., Office of Global HealthKenneth Castro, M.D., National Center for HIV, STD, and TB PreventionEugene McCray, M.D., National Center for HIV, STD, and TB PreventionStephen Cochi, M.D., M.P.H., National Immunization ProgramStephen Hadler, M.D., National Immunization ProgramMark White, M.D., Epidemiology Program OfficeMichael Malison, M.D., M.P.A., Public Health Practice Program Office

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Atlanta, Georgia, 2002

For additional copies of this booklet, write to
Office of Health CommunicationNational Center for Infectious DiseasesCenters for Disease Control and PreventionMailstop C-141600 Clifton Road, NEAtlanta, GA 30333Fax: 404-371-5490
or visit the website: www.cdc.gov/globalidplan.htm

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 3
Preface 5
Executive Summary 6
INTRODUCTION 11
International Cooperation To Combat Infectious Diseases 15
U.S. Investment in Global Public Health 16
Protecting the health of U.S. citizens at home and abroad 18
Furthering U.S. humanitarian efforts 19
Providing economic and diplomatic benefits 19
Enhancing security 19
CDC’s Role in Promoting Global Public Health 20
An evolving mission 22
VISION FOR THE FUTURE 24
PARTNERSHIPS AND IMPLEMENTATION 26
PRIORITIES AND OBJECTIVES 28
1 International Outbreak Assistance 28
2 A Global Approach to Disease Surveillance 33
3 Applied Research on Diseases of Global Importance 38
4 Application of Proven Public Health Tools 44
5 Global Initiatives for Disease Control 48
6 Public Health Training and Capacity Building 53
List of Boxes 59
Acronyms 60
Appendix A: Global Health Websites 62
Appendix B: Diplomatic Forums That Address Emerging 64
Infectious Disease Issues
Appendix C: Examples of International Outbreak Assistance 65
Appendix D: WHO Collaborating Centres Based at CDC 67
Appendix E: Regional and Disease-Specific Surveillance Networks 68
Acknowledgments 71
References 72
TABLE OFCONTENTS


Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 5
Since 1994, CDC has been engaged in a nationwide effort to revitalizenational capacity to protect the public from infectious disease. Progress con-
tinues to be made in the areas of disease surveillance and outbreak response;applied research; prevention and control; and infrastructure-building and train-ing. These efforts are intended to provide protection against endemic diseaseslike tuberculosis and hepatitis C, as well as against whatever new or drug-resist-ant diseases arise.
Although safeguarding U.S. health is a domestic goal, its achievement requiresinternational action and cooperation. This is because U.S. health and globalhealth are inextricably linked. As the AIDS epidemic has illustrated, a diseasethat emerges or reemerges anywhere in the world can spread far and wide. Withincreased rates of air travel and international trade, infectious microbes havemany opportunities to spread across borders, whether carried by businessmenand tourists, by mosquitos that “hitchhike” on airplanes, or by exotic animalsimported as pets or livestock. Microbes have additional opportunities for spreadon international shipments of fruits, meats, fish, or vegetables.
The international dimension of the effort to combat infectious diseases is reflect-ed in CDC’s growing international role. Whenever a new, highly dangerous,drug-resistant, or reemerging disease is detected anywhere on the globe, U.S. cit-izens, as well as foreign governments, have come to rely on CDC to provideassistance and public health information. Established diseases such asHIV/AIDS, tuberculosis, and malaria, as well as vaccine-preventable diseasessuch as polio, demand increasing attention and resources as well. This increasedinternational engagement has stimulated CDC to rethink its infectious diseasepriorities, keeping in mind that it is far more effective to help other countriescontrol or prevent dangerous diseases at their source than try to prevent theirimportation.
This document, Protecting the Nation’s Health in an Era of Globalization:CDC’s Global Infectious Disease Strategy, represents an important advance indefining CDC’s evolving global mission and in considering how CDC and itsinternational partners can work together to improve global capacity for disease surveillance and outbreak response. We look forward to working with our manypartners throughout the nation and the world as we put this strategy into practice.
Jeffrey P. Koplan, M.D., M.P.H.DirectorCenters for Disease Control and Prevention
PREFACE

6 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Itis not possible to adequately pro-tect the health of our nation with-
out addressing infectious disease prob-lems that occur elsewhere in theworld. In an age of expanding air trav-el and international trade, infectiousmicrobes are transported across bor-ders every day, carried by infected peo-ple, animals, and insects, and con-tained within commercial shipmentsof contaminated food. “Old” diseasessuch as malaria, measles, and food-borne illnesses are endemic in manyparts of the globe, and new diseasessuch as acquired immunodeficiencysyndrome (AIDS; caused by the humanimmunodeficiency virus (HIV))—aswell as new forms of old diseases suchas multidrug-resistant tuberculosis(TB)—can emerge in one region andspread throughout the world.
Moreover, unforeseen disease prob-lems continue to appear. Recent exam-ples include vancomycin-resistantinfections of Staphylococcus aureus inthe United States and Japan, avianinfluenza in Hong Kong, a new diseasecalled Nipah virus encephalitis inMalaysia, and outbreaks of denguefever in Texas and West Nile encepha-litis in New York. Increased CDCengagement in efforts to improve glob-al disease surveillance and outbreakresponse will help us detect new or un-usual diseases of any kind and respondto health emergencies of any kind—including both naturally occurring andintentionally caused outbreaks.
Left unchecked, today’s emergingdiseases can become the endemic dis-
eases of tomorrow. This is what hap-pened with HIV/AIDS, which spreadfrom a remote part of Africa to allother continents 20 years ago, and isnow entrenched all over the world,necessitating a major internationalcontrol effort.
Because U.S. and internationalhealth are inextricably linked, the ful-fillment of CDC’s domestic mission—to protect the health of the U.S. popu-lation—requires global awareness andstrategic thinking. This document,Protecting the Nation’s Health in anEra of Globalization: CDC’s GlobalInfectious Disease Strategy, describeshow CDC and its international part-ners can collaborate to prevent theemergence and spread of infectiousdiseases.
U.S. Investment in Global Public Health
The United States must participatemore fully in combating infectious dis-ease threats around the world. Theseefforts will yield multiple benefits:
• Protecting the health of U.S. citi-zens at home and abroad. Control-ling disease outbreaks as well asdangerous endemic diseases wher-ever they occur prevents those dis-eases from spreading international-ly, saving lives and dollars. U.S.citizens cannot be adequately pro-tected from diseases such asmeasles, HIV/AIDS, and tuberculo-sis if our public health efforts arerestricted to persons residing withinour borders.
EXECUTIVE SUMMARY

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 7
er nations, damaging their econom-ic, social, political, military, andeducational infrastructures, andcreating vast numbers of orphans.The recent intentional releases ofbiologic agents in the United Stateshave also intensified internationalconcerns about bioterrorism. Dueto the ease and frequency of moderntravel, an intentionally-caused out-break that begins anywhere in theworld can quickly become an inter-national problem. A contagiousbioterrorist agent such as smallpoxcan spread rapidly from person toperson and from country to coun-try. A noncontagious agent such asanthrax can be spread by unexpect-ed methods, including internationalmail. The United States must beprepared to work with othernations to prevent illness and deathscaused by acts of bioterrorism.
Although the United States partici-pates in health projects in many partsof the world, much more can be done,at relatively low cost, with politicalwill, national leadership, and a clearlyarticulated global strategy.
CDC’s Role in PromotingGlobal Public Health
CDC, which is dedicated to the pre-vention and control of disease and thepromotion of health, works by invita-tion in many different jurisdictions,including U.S. states and cities andother nations. Throughout its history,CDC has provided international lead-ership in public health, serving as atechnical consultant to the World
• Furthering U.S. humanitarian ef-forts. The potential for savinghuman lives by preventing infec-tious diseases overseas is tremen-dous. Every year, an estimated threemillion infant and child deaths areprevented by vaccination and otherpreventive health measures. Manyfamilies and communities, includ-ing refugees and displaced people,also benefit from internationalinvestigations that lead to promptcontrol of outbreaks.
• Providing diplomatic and economicbenefits. Because health is an area ofconcern for all nations, internationalprojects that address infectious dis-ease issues can open avenues ofcommunication and ease tensionsbetween the United States and othernations. Improvements in globalhealth will also enhance the U.S.economy and contribute to globalprosperity. Reductions in diseaseburden will promote economicgrowth in nations that representgrowing markets for U.S. products.Investments in global health willalso reduce U.S. healthcare costs bydecreasing the number of cases ofimported diseases and by eradicat-ing diseases currently included inchildhood vaccination programs.
• Enhancing security. Slowed eco-nomic growth fueled by poor healthand disease can impede democraticdevelopment and political transi-tions in poor and former commu-nist nations, contributing to mili-tary conflicts and humanitarianemergencies. The HIV/AIDS pan-demic is already destabilizing poor-
Health Organization (WHO) and min-istries of health on projects that addressinfectious disease problems related toendemic diseases, wars, famines, orother disasters. Many of these projectshave been funded and coordinated bythe U.S. Agency for InternationalDevelopment (USAID). CDC has alsosupported research and public healtheducation on diseases of regional orinternational importance, providedresources and leadership for the small-pox eradication effort, and establishedlong-term collaborative research part-nerships with several developingnations. While considerable effort hasbeen devoted to these internationalactivities, CDC’s primary focus hasremained on domestic health.
In recent years, however, CDC’soverseas role has expanded rapidly.Global polio eradication (http://www. cdc.gov/nip/global) and HIV/AIDS con-trol programs (http://www.cdc.gov/ nchstp/od/gap) have led to substantialinvestments of CDC personnel andfinancial resources, as have a succes-sion of complex international emer-gencies. Between 1990 and 2000,CDC provided outbreak assistance onan ad hoc basis to nations in Asia,Africa, Europe, and Latin America tohelp investigate outbreaks of un-known, highly dangerous, and highlyinfectious diseases, and provided diag-nostic support for hundreds of localinvestigations around the globe.
Although there are no formal struc-tures and designated resources forinternational outbreak response, U.S.citizens—as well as foreign govern-ments—have come to rely on CDC toprovide outbreak assistance and pub-

8 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
lic health information whenever a newor reemerging disease threat is detect-ed anywhere on the globe. Oubreakassistance by CDC would also berequired if an intentionally caused out-break occurred at home or abroad.
CDC’s growing presence overseaspresents new opportunities and newchallenges. This document—developedin consultation with public and privatesector partners, at home and abroad—represents an active effort to furtherdefine CDC’s evolving global mission.It considers how CDC and its interna-tional partners can work together overthe long term to improve the capacityto detect, control, and prevent infec-tious diseases. CDC’s ongoing effortsto strengthen U.S. domestic publichealth infrastructure are critical to thesuccess of these international collabo-rations.
Six Priority Areas
Protecting the Nation’s Health in anEra of Globalization: CDC’s GlobalInfectious Disease Strategy definesCDC’s global infectious disease priori-ties in six areas, selected in consulta-tion with global public health part-ners. In looking towards the future,CDC envisions increased activity andprogress in each area:
1. International Outbreak Assistance.
An underlying principle of the globalstrategy is the recognition that interna-tional outbreak assistance is an inte-gral function of CDC. Supporting thisfunction will require augmenting,updating, and strengthening CDC’sdiagnostic facilities, as well as itscapacity for epidemiologic investiga-tion overseas. In the future, CDC mustalso be prepared, as a matter of rou-tine, to offer follow-up assistance aftereach acute emergency response. Suchfollow-up will assist host-country min-istries of health to maintain control ofnew pathogens when an outbreak isover.
2. A Global Approach to Disease Surveillance.
In the years ahead, regional surveil-lance networks should expand, inter-act, and evolve into a global “networkof networks” that provides earlywarning of emerging health threatsand increased capacity to monitor theeffectiveness of public health controlmeasures. CDC will help stimulate thisprocess by providing technical assis-tance, evaluating regional progress,and working with many partners tostrengthen the networks’ telecommu-nications capacities and encourage theuse of common software tools andharmonized standards for diseasereporting.
3. Applied Research on Diseases of Global Importance.
A research program on diseases thatare of global importance, includingsome that are uncommon in the Unit-ed States, is a valuable resource, bothfor humanitarian reasons and becauseof the dangers represented by someimported diseases. CDC’s laboratori-ans, epidemiologists, and behavioralscientists will maintain an activeresearch program to develop tools todetect, diagnose, predict, and elimi-nate diseases of global or regionalimportance. When a new diseasethreat is reported anywhere in theworld, CDC’s laboratorians and fieldinvestigators will be available to helpanswer questions about disease trans-mission, treatment, control, and pre-vention.
4. Application of Proven Public Health Tools.
There is often a long delay between thedevelopment of a new public healthtool and its widespread use. CDC willintensify efforts to couple appliedresearch with research on ways to pro-mote the use of newly developed toolsfor disease control (“implementationresearch”). CDC will help identify themost effective tools and activelyencourage their international use,applying expertise and resources inlaboratory research, public health pol-icy, program management, and healthcommunications to overcome scientif-ic, financial, and cultural barriers.

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 9
5. Global Initiatives for Disease Control.
CDC will make sustained contribu-tions to global initiatives to reduce theprevalence of HIV/AIDS in young peo-ple by 25% and reduce deaths fromtuberculosis and malaria by 50% by2010. CDC will also work with theGlobal Alliance for Vaccines andImmunization to reduce infant mortal-ity through enhanced delivery and useof new and underutilitzed vaccinesagainst respiratory illnesses and otherchildhood diseases. CDC and its part-ners will also consult on future inter-national priorities for disease control,elimination, and eradication efforts—as well on monitoring for antimicro-bial resistance and planning for pan-demic influenza—and help evaluateprogress through the collection andanalysis of disease surveillance data.
6. Public Health Training and Capacity Building.
CDC will encourage and support theestablishment of International Emerg-ing Infections Programs (IEIPs) indeveloping countries—centers ofexcellence that integrate disease sur-veillance, applied research, prevention,and control activities. The IEIP siteswill partner with Field EpidemiologyTraining Programs (FETPS) and otherinstitutions to strengthen nationalpublic health capacity and providehands-on training in public health.Over time, they may help to strength-en capacity in neighboring countries aswell as within the host country.
Implementation of specific objectivesin these six areas will help realizeCDC’s vision of a world in which U.S.citizens and people throughout theworld are better protected from infec-tious diseases.
Partnerships and Implementation
CDC’s global infectious disease strate-gy was prepared by the National Cen-ter for Infectious Diseases, in collabo-ration with other CDC centers andoffices, including the Office of GlobalHealth, the National Center for HIV,STD, and TB Prevention, the NationalImmunization Program, the Epidemi-ology Program Office, and the PublicHealth Practice Program Office. Manyglobal health organizations and agen-cies provided consultation and assis-tance during its development.
The strategy will be implementedincrementally over the next five years,as funds become available, beginningwith the highest priorities for 2001-2002 (Box 1). As CDC carries out thisstrategy, it will coordinate with foreigngovernments, international organiza-tions (including WHO, the Joint Unit-ed Nations Programme on AIDS[UNAIDS], and the United NationsChildren’s Fund [UNICEF]), otherU.S. agencies (including USAID, the
National Institutes of Health [NIH],the Food and Drug Administration[FDA], the Department of Defense[DoD], the Department of State, theDepartment of Veterans Affairs[DVA], the U.S. Department of Agri-culture [USDA], the National Oceanicand Atmospheric Administration[NOAA], and the National Aeronau-tics and Space Agency [NASA]), pro-fessional societies, research institu-tions, and schools of public health,medicine, nursing, and veterinary sci-ence. CDC will also participate ininternational coalitions that supportdisease eradication efforts and otherregional and global health initiatives.These coalitions may include nationaland local nongovernmental organiza-tions, community-based and faith-based organizations, and communitiesof color. Other implementation part-ners will include pharmaceutical andbiotechnology companies, non-gov-ernmental organizations that addresshealth problems, and developmentagencies, development banks, founda-tions, and other organizations thataim to reduce poverty by reducing theincidence of endemic diseases. Websiteaddresses for selected organizationsand health publications and reportsreferred to in this document are pro-vided in Appendix A.

Box 1
Implementation Priorities, 2001-2002
International Outbreak Assistance Dedicate specific resources—epidemiologic, diagnostic,and logistic—to international outbreak investigations.
A Global Approach to Disease Surveillance Work with WHO and other partners to provide techni-cal assistance to regional networks in Africa, Asia, andLatin America that can fill gaps in global disease sur-veillance and become components of a global networkof networks.
Applied Research on Diseases of Global Importance Establish two or more long-term, on-site research col-laborations in developing countries to test new strate-gies for disease control and prevention.
Application of Proven Public Health ToolsWork with a developing-country partner to launch ademonstration project that employs three or moreproven public health tools to prevent and control infec-tious diseases, depending on local priorities.
Global Initiatives for Disease Control Work with foreign ministries of health and WHO tocomplete the eradication of polio and guinea worm dis-ease.
10 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Help implement HIV/AIDS control programs on allcontinents through CDC’s Global AIDS Program.
Work with the Roll Back Malaria partnership to helpimplement and monitor disease control and preventionprograms in areas with high rates of transmission.
Work with the Stop TB Initiative to improve global sur-veillance, prevention, and medical management of TB,including multidrug-resistant TB, in areas with highrates of transmission.
Establish population-based surveillance centers to mon-itor the impact of vaccine use on diseases targeted bythe Global Alliance for Vaccines and Immunization.These surveillance centers may become the nuclei offuture International Emerging Infections Program sites.
Public Health Training and Capacity BuildingEstablish the first International Emerging InfectionsProgram as a partnership among a ministry of health,CDC, a Field Epidemiology Training Program, and oneor more local universities or medical research institutes.An initial priority will be to establish training in fieldepidemiology, applied laboratory science, and publichealth management.

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 11
INTRODUCTION Itis not possible to adequately pro-tect the health of our nation with-
out addressing infectious disease prob-lems that are occurring elsewhere inthe world. In an age of expanding airtravel and international trade, infec-tious microbes are transported acrossborders every day, carried by infectedpeople, animals, and insects (Box 2),and contained within commercial ship-ments of contaminated food (Box 3).“Old” diseases such as malaria,measles, and foodborne illnesses areendemic in many parts of the globe,and new diseases such as acquiredimmunodeficiency syndrome (AIDS;caused by the human immunodeficien-cy virus (HIV))—as well as new formsof old diseases such as multidrug-resist-ant tuberculosis (TB)—can emerge inone region and spread throughout theworld.
Old diseases, as well as new ones,can travel. For example, between July1999 and January 2000, 56 people insouthern Texas fell ill with denguefever, a mosquitoborne tropical diseaseendemic to South and Central Ameri-ca and parts of Asia. Seventeen ofthose people acquired their illness inthe United States. In 1999, two BoyScouts in New York State acquiredmalaria—eliminated as an endemicdisease problem in the United States ahalf century earlier—from mosquitosat a summer camp in a rural area ofSuffolk County. In August and Sep-
tember, 1999, six people in the north-eastern United States and a Canadianvisiting New York City died from WestNile encephalitis, a viral disease alsotransmitted by mosquitos. The WestNile virus, which is carried by migra-tory birds in Asia, Africa, and Europe,had never before been reported in theWestern Hemisphere.
These outbreaks present new chal-lenges for U.S. public health agenciesat the local, state, and federal levels.They also remind us that millions ofpeople live in tropical areas wheremosquitoborne diseases like malariaand dengue are a fact of everyday life.
Because U.S. and international healthare inextricably linked, fulfillingCDC’s domestic mission—to protectthe health of the U.S. population—requires global awareness and strate-gic thinking. This document, Protect-ing the Nation’s Health in an Era ofGlobalization: CDC’s Global Infec-tious Disease Strategy, describes howCDC and its international partnerscan collaborate to prevent the emer-gence and spread of infectious dis-eases.
The urgency of the situation is illus-trated by the emergence of unforeseendisease problems in recent years. Theseinclude multidrug-resistant Streptococ-cus pneumoniae throughout the worldand vancomycin-resistant Staphylo-coccus aureus in the United States and

12 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Box 2
Infectious Diseases Do Not Recognize Borders
From a public health point of view, domestic and inter-national health are inextricably linked. Examples of dis-ease spread from continent to continent include
• HIV/AIDS—This disease apparently emerged in cen-tral Africa in the 1950s or earlier1 and spread throughmost of Africa, Asia, Europe, and the Americas dur-ing the 1970s and 1980s.
Because the AIDS virus weakens an individual’simmune defenses, an individual with HIV/AIDS maybecome coinfected with malaria, tuberculosis (TB), orpathogens that cause diarrhea or pneumonia.
• TB—During the 1980s, this age-old scourge, whichhad been nearly eliminated in the West by antibiotictreatment, reemerged–sometimes in a multidrug-resistant form—in cities around the world, includingin the United States. By 2000, approximately 46% ofnewly identified U.S. TB cases originated in othercountries.
The spread of TB has been hastened by lack of publichealth surveillance for this disease and by the concur-rent HIV/AIDS epidemic.
• Malaria—Although malaria was eliminated in theUnited States as an endemic disease by the 1960s(through swamp-draining and vector control pro-grams), approximately 1,500 cases of malaria arereported in the United States each year. One-halfoccur in U.S. travelers to malaria-endemic countriesand the other half occur among foreign nationals whoenter the United States already infected.
Over the past 15 years, more than 80 people in theUnited States were infected by local transmissionwithin our borders. In other countries, the spread ofmalaria has been augmented by the spread of anti-malarial drug resistance, and many parasite strainsare increasingly resistant to preventive antimalarialdrugs taken by travelers.
• West Nile encephalitis—This mosquitoborne viral dis-ease carried by migratory birds in Asia, Africa, andEurope, caused 79 cases of encephalitis and 7 deathsin the northeastern United States in 1999.
Because the West Nile virus had never before beendetected in the Americas—and because it had beenmentioned by an Iraqi defector as an organism ofinterest to the Iraqi bioweapons program—it wasspeculated that a strain of West Nile virus isolated inNew York City might have been deliberately engi-neered and disseminated to harm U.S. citizens. How-ever, the scientific evidence suggests that the outbreakwas caused by a naturally occurring viral strain.2
• Vibrio cholerae O1, El Tor biotype—A virulent strainof cholera has caused an ongoing pandemic that haslasted 40 years and affected more than 75 countries.
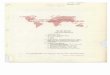
Geographic extent of the Latin American cholera epidem-
ic over time, since its beginning in January 1991. Linesrepresent the advancing front of the epidemic at differenttimes. Since 1995, most Latin American countries havereported diminishing numbers of cases. Cholera has notyet reached the Caribbean.
Adapted from: Tauxe RV, Mintz ED, Quick RE. Epidemic cholera in the New
World: translating field epidemiology into new prevention strategies. Emerg-
ing Infectious Diseases 1:141-6, 1995.

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 13
Beginning in 1961, Vibrio cholerae O1, El Tor bio-type spread from Indonesia through most of Asia intoeastern Europe and Africa. From North Africa itspread to the Iberian Peninsula and into Italy in 1973.In the late 1970s, small outbreaks occurred in Japanand in the South Pacific.
In January, 1991, epidemic cholera appeared in Peruand spread rapidly through most of Latin America,causing over 1,000,000 cases by 1994. This was thefirst time in 100 years that a cholera pandemic hadreached the New World.
• Salmonellosis—A multistate outbreak carried by con-taminated mangoes grown in Brazil caused 79 casesof Salmonella Newport infections in 13 states in1999.
The outbreak was detected and investigated usingPulseNet, the U.S. early warning system for food-borne diseases (page 36). PulseNet linked 78 cases in22 states by comparing the molecular fingerprints ofthe isolates. Once mangoes were implicated as thecommon exposure for these cases, FDA traced thesource of the mangoes back to a single farm in Brazil.The mangoes had been dipped in warm water in anew process designed to kill fruit-fly larvae beforeexportation. Unfortunately, the processing water mayhave been contaminated with Salmonella.
• Coccidioidomycosis—Outbreaks caused by Coccid-ioides immitis, a soil-dwelling fungus common in aridand semiarid parts of the Western Hemisphere, werereported in 1996 in Washington State and in 2000 inPennsylvania.
The outbreaks occurred among church missiongroups who visited endemic regions of northern Mex-ico to undertake construction projects. Infected indi-viduals experienced a severe influenzalike disease
Box 2
with fever, chills and cough. Fungal disease was notinitially suspected.
• Influenza spread on cruise ships—A 1997 outbreak ofthe A/Sydney strain of influenza occurred among peo-ple on a cruise that made stops in Canada and NewEngland.
The A/Sydney strain had been isolated in Australiatoo late in the year to be included in the vaccine for-mulated for the fall/winter flu season in the NorthernHemisphere. Therefore, the cruise ship passengershad not been immunized against it.
• Measles—Fifty-six of the 87 cases of measles identi-fied in the United States in 2000 were traced toimportations of the virus from outside our borders.Twenty-six were direct importations, 18 were second-ary cases, and 8 involved viruses whose DNAsequences suggested a foreign origin.
Comprehensive surveillance and genetic sequencingof all identified strains of the virus allow for tracingof the outbreak strains to the country of origin. Thefinding that indigenous measles transmission can beinterrupted in the United States is an important impe-tus for supporting a global measles elimination cam-paign.
• Polio—Eliminated from the Western Hemispheresince 1991, paralytic polio was again identified inHaiti and the Dominican Republic in 2000, andattributed to waning immunization coverage rates inthose countries.
Unless immunization coverage can be strengthened inother neighboring countries, diseases thought nolonger to be a risk for U.S. children may be importedby travelers.

14 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Box 3
Factors That Facilitate the International Spread of Foodborne Disease
• Globalization of the food supply, particularly of per-ishable foods, like fresh produce U.S. citizens can now eat fresh fruits and vegetables allyear round, produced in both Northern and SouthernHemispheres. However, some fresh foods may be con-taminated during picking, packaging, transport, ordelivery. CDC and FDA are working together to reducethe risk to U.S. consumers.
• The development of new food production industriesin developing nations to meet the needs of the exportmarket This includes growing nonindigenous fruits and veg-etables that may be susceptible to contamination byindigenous microbes. For example, raspberries wererecently introduced into Guatemala with U.S. supportas a potentially valuable commercial crop. Some of theexported raspberries were found to be contaminatedwith Cyclospora, a waterborne protozoan parasite notpreviously associated with foodborne disease.Cyclospora outbreaks associated with these raspber-ries were reported in the United States and Canada.
• Centralized processing of human and animal foods,followed by widespread distribution If an ingredient used in an animal feed, for example, iscontaminated with a strain of Salmonella, that strain
can be quickly disseminated to food animals aroundthe world. Or, if ground beef is contaminated with E.coli O157:H7 at a factory, hamburgers sold at fast-food restaurants in many locations (as well as pack-ages of frozen meat sold at grocery stores) may trans-mit infection.
• Expanded U.S. market for “ethnic” foods There is increased familiarity with—and preferencesfor—foods from different countries, due to interna-tional travel by U.S. citizens, the growing ethnicdiversity of our population, and our many immigrantcommunities. A recent outbreak of typhoid fever wasassociated with imported frozen mamey fruit pulp,popular among Central Americans living in Florida.Outbreaks of gastroenteritis caused by antibiotic-resistant Salmonella have occurred in people who atetraditionally-prepared Mexican cheese made fromraw milk and sold informally.
• Increased international travel International tourists and business travelers oftendevelop “traveler’s diarrhea,” caused by foodbornebacteria that generally do not affect local adults,most of whom have acquired immunity from repeat-ed childhood exposures.
Japan (Box 4), avian influenza inHong Kong (Box 5), a new diseasecalled Nipah virus encephalitis identi-fied in Malaysia, as well as the intro-duction of West Nile encephalitis intoNorth America (Box 2).
Windows of opportunity for dis-ease control may also close. For exam-ple, had smallpox not been eradicatedbefore the global HIV/AIDS epidemic,one of the world’s crowning public
health successes might have beenimpossible to achieve. There is nowevidence that immune suppressionsuch as that caused by HIV/AIDS maylead to a lack of response to smallpoxvaccination or (in some cases) to dis-seminated vaccinal infection that maybe life-threatening.
Left unchecked, today’s emergingdiseases can become the endemic dis-eases of tomorrow. This is what hap-
pened with HIV/AIDS, which emergedin a remote part of Africa during the1970s, spread throughout the worldduring the 1980s, and is now en-trenched on all continents, creatingwidespread devastation. During the2000s, HIV/AIDS has become the tar-get of a major international controleffort (Box 6).

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 15
Box 4
International Spread of AntimicrobialResistance
Drug-resistant pathogens are a growing menace to allpeople, regardless of age, sex, or socioeconomic back-ground. They endanger people in affluent, industrialsocieties like the United States, as well as those in lessdeveloped nations. Many pathogens of internationalimportance are becoming resistant to standard thera-pies, including bacteria that cause pneumonia, earinfections, and meningitis (e.g., Streptococcus pneu-moniae); food and waterborne infections (e.g., Sal-monella and Shigella); sexually transmitted diseases(e.g., Neisseria gonorrhoeae); the human immunode-ficiency virus that causes AIDS; and the parasitesthat cause malaria (Plasmodium spp.). Other exam-ples of clinically important microbes that are rapidlydeveloping drug-resistance include Mycobacteriumtuberculosis; bacteria that cause skin, bone, lung, andbloodstream infections (e.g., Staphylococcus aureus)and urinary tract infections (e.g., Escherichia coli);and pathogens transmitted in health care settings(e.g., enterococci and Klebsiella).
CDC is working with many partners to helpimprove global capacity to detect and control drug-resistant infections. These efforts include workingwith WHO to provide quality control and proficien-cy testing for clinical laboratories in support of sur-veillance for emerging resistance problems. CDC isalso working with FDA, NIH, USAID, DoD, USDA,and other U.S. agencies to develop Part II of the U.S. Public Health Action Plan to Combat Antimi-crobial Resistance (http://www.cdc.gov/drugresis-tance/actionplan), which will serve as a blueprint forU.S. government activities to address internationalantimicrobial resistance issues. U.S. agencies andtheir partners will implement this blueprint in thecontext of WHO’s Global Strategy for the Contain-ment of Antimicrobial Resistance (http://www.who. int/emc/globalstrategy/strategy.html).
International Cooperation ToCombat Infectious Diseases
The United States must participatemore fully in combating infectious dis-ease threats around the world. Theurgency of expanding our contribu-tions to infectious disease control wasemphasized by an interagency work-ing group of the National Science andTechnology Council3 (http://www. ostp.gov/CISET/html/toc.html).
There has also been an outpouringof interest in infectious disease issuesin other nations, both in the developedand the developing world (AppendixB). In July 2000, at the summit meet-ing in Okinawa the Group of EightIndustrialized Nations pledged toreduce deaths from infectious diseasesin poor countries, agreeing to a set of time-limited objectives (http://usinfo.state.gov/topical/econ/group8/summit00). The aim is to reduce theprevalence of HIV/AIDS among youngpeople by 25%, and reduce the number of deaths due to TB and tomalaria by 50% by 2010. These goalsare based on global health initia-tives endorsed by the World HealthOrganization (WHO) in its effort toaddress “diseases of poverty” in devel-oping countries (Box 6). Anothermajor initiative, spearheaded by theGlobal Alliance for Vaccines andImmunization (GAVI; http://www. vaccinealliance.org/), aims to increasedeveloping country access to new andunderutilitzed vaccines against hepati-tis B, Haemophilus influenzae type b,and yellow fever, and to improve deliv-ery of traditional childhood vaccinesagainst measles and other diseases.

16 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Our confidence that nations cancome together to improve globalhealth is reinforced by the success ofthe effort to eradicate smallpox, theinterruption of measles transmission inthe Americas, and the substantialprogress made toward the worldwideeradication of polio (Box 7) andguinea worm disease.
U.S. Investment in Global Public Health
Promoting international cooperationto address emerging infectious diseasesis a natural role for the United States,whose scientists and business leadersare important members of the biomed-ical research and telecommunicationscommunities that provide the technicaland scientific underpinning for infec-tious disease surveillance and control.The United States can continue to leadfrom its strengths in medical scienceand technology to help protect Ameri-can and global health.
Moreover, our nation now has awindow of opportunity to make pub-lic health investments that will payincreasingly valuable dividends in theyears to come. As noted in the 1997Institute of Medicine report, America’sVital Interest in Global Health4
(http://www.nap.edu/books/0309058341/html), investments in internationalefforts to detect, control, and preventinfectious diseases can yield multiplebenefits:
Box 5
Avian Influenza in Hong Kong
Influenza viruses are constantly mutating and evolving,and new strains keep emerging. Because few people haveimmunity to a new strain—and because influenza spreadseasily from person to person—new strains can travelquickly around the world. If a strain is particularly viru-lent, it may cause a pandemic, like the 1918-19 “Spanishflu,” which killed 20 million people, including 500,000Americans.
The WHO International Influenza Surveillance Net-work, which includes 110 laboratories throughout theworld (including a CDC-based WHO Collaborating Cen-tre), gathers influenza isolates on all continents and collectsdata on new strains that have the potential for pandemicspread. In 1997, the government of Hong Kong made useof this network to identify a dangerous strain of avianinfluenza transmitted from chickens to humans that infect-ed 18 persons and killed 6. The authorities feared that thestrain (H5N1) might recombine with a human strain andbecome capable of human-to-human transmission andinvited a CDC team to assist with control of the outbreak.Transmission stopped after the government of Hong Kongordered the destruction of all chickens in Hong Kong thatmight be carrying the virus (see also Box 15).
This episode suggests that it may be possible to preventinfluenza pandemics before they begin, or to mitigate theglobal impact of an influenza pandemic through earlyidentification of a virulent strain and formulation of astrain-specific vaccine. What is required is continued inter-national vigilance and cooperation (i.e., a global network)and—at the national level—the political will and resourcesto act on epidemiological and diagnostic evidence. Had theWHO network not been in place, or had the Hong Konggovernment been unable or unwilling to act, a virulenthybrid chicken/human strain of influenza for which virtu-ally all people lack immunity—and for which there is novaccine and few drug treatments—might have caused amassive global pandemic.

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 17
Box 6
Global Health Initiatives
Four major global health initiatives were launchedbetween 1998 and 2000:
• Roll Back Malaria, a global strategy to reduce deathsfrom malaria by increasing access to prompt andeffective treatment (including protective intermittenttherapy for pregnant women) and prevention tools(including insecticide-treated bednets); by facilitatingrapid response to malaria outbreaks; and by develop-ing new products for the prevention and treatment ofmalaria.
• Stop TB, a global strategy to stop the spread of TBaround the world. One of its objectives is to promoteimplementation of the directly observed therapyshort-course strategy (DOTS). The effective imple-mentation of DOT in NYC, in response to the epi-demic in the late 1980s and early 1990s, has servedas a model in this country and around the world.
• International Partnership Against AIDS in Africa, aUNAIDS-led effort to mitigate the effects of thegrowing HIV/AIDS epidemic. In 1999, as part of thiseffort, the U.S. government launched the Leadershipand Investment for Fighting an Epidemic (LIFE) Ini-tiative, which provides support to the hardest-hitcountries for reducing HIV transmission, improvingtreatment of HIV/AIDS and opportunistic infections,
and strengthening national capacities to collect dis-ease surveillance data and manage nationalHIV/AIDS programs. The Global AIDS Program is the CDC component of the LIFE Initiative (seeBox 21).
• Global Alliance for Vaccines and Immunization(GAVI), a global effort to strengthen childhoodimmunization programs and bring a new generationof recently licensed vaccines into use in developingcountries. These include vaccines against hepatitis B,childhood meningitis, yellow fever, and respiratoryinfections, which are the leading cause of death inchildren under age five. Substantial resources for thispurpose have been pledged by the Bill and MelindaGates Foundation and the governments of Norway,Netherlands and the United States.
Targets for Disease Reduction These targets for disease reduction were endorsed at theGroup of Eight Industrialized Nations Summit in Oki-nawa in July 2000:
HIV/AIDS: 25% reduction in prevalence in youngpeople by 2010
TB: 50% reduction in deaths by 2010 Malaria: 50% reduction in deaths by 2010

18 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Box 7
The World Health Organization Global Polio Laboratory Network
Ascertaining whether a disease is still present in a given area (and, therefore, that further prevention efforts are needed) is a crit-ical part of any disease eradication effort. The WHO Global Polio Laboratory Network uses molecular techniques to determinewhether wild-type polio is circulating in areas undergoing eradication efforts. Since the worldwide campaign began, cases ofpolio have declined by 99% (from 350,000 cases to less than 3,000), and the number of countries in which polio is endemic hasdecreased from 125 to 20.
CDC began training Network virologists in 1986, soon after the Pan American Health Organization declared its goal of elimi-nating polio from the Americas. CDC will continue to train Network virologists for several more years, as new diagnostic meth-ods are developed to meet the stringent surveillance criteria necessary to obtain certification of global polio eradication.
Protecting the health of U.S. citizensat home and abroad. Seeking to con-trol disease outbreaks as well as dan-gerous endemic diseases wherever theyoccur prevents those diseases fromspreading internationally, saving livesand dollars. In addition, CDC’s sup-
port for outbreak investigations pro-vides U.S. scientists with opportunitiesto focus on new or drug-resistantpathogens and consider how best tocontrol, prevent, and treat them before they arrive on our shores. Out-breaks and endemic diseases in other
countries also endanger U.S. travelersabroad.
In terms of U.S. health, it is farmore effective to help other countriescontrol or prevent dangerous diseasesthan try to prevent their importation,because it is neither efficient nor feasi-
Specialized Reference LaboratoryRegional Reference LaboratoryNational/Sub-national LaboratoryProposed National Laboratory

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 19
ble to examine each person who entersor returns to the United States for evi-dence of infection, or to examine allimported goods for evidence of con-tamination. Some infections areasymptomatic, and some infected indi-viduals may enter the country duringthe incubation period of a disease (thetime between infection and theappearance of symptoms). Thus, dis-eases such as measles and TB continueto be imported.
Furthering U.S. humanitarian efforts.Disease prevention is an investment inthe young people of the world and inour collective future. Every year, mil-lions of infant and child deaths areprevented by vaccination and otherpreventive health measures. Manyfamilies and communities also benefitfrom international investigations thatlead to prompt control of outbreaks.These include communities of re-fugees and displaced persons, whomay be especially vulnerable to infec-tious diseases (see Box 13). CDC isalso a major contributor to globalefforts to eradicate polio (http://www. cdc.gov/nip/global) and dracunculia-sis (guinea worm disease; http://www. cdc.gov/ncidod/dpd/parasites/guinea-worm and http://www.cartercenter. org/guineaworm.html).
The potential for saving humanlives by preventing infectious diseasesoverseas is tremendous. For example,an additional three million deathscould be prevented annually by widerworldwide use of childhood vaccines.Although the United States partici-pates in international health projects
in many parts of the world, much morecan be done, at relatively low cost, withpolitical will, national leadership, and aclearly articulated global strategy.
Investing in global health is an areain which global humanitarian needsand U.S. national interests coincide.For example, U.S. efforts to help thestates of the former Soviet Unionrebuild their collapsing public healthinfrastructures5 will also help preventthe resurgence of dangerous diseases(e.g., polio, diphtheria, and drug-resistant TB) that can spread to theAmericas. Similarly, U.S. efforts tohelp China improve surveillance fornew strains of influenza may be crucialin preventing or controlling the nextinfluenza pandemic (see Box 5).
Providing economic and diplomaticbenefits. Improvements in globalhealth can also enhance the U.S. econ-omy in direct and indirect ways.Domestic health care costs can bereduced by decreasing the number ofcases of imported diseases and byeradicating diseases currently includedin childhood vaccination programs.For example, the U.S. saved $3 billionafter investing $32 million in smallpoxeradication, and promises to gain evengreater cost savings if the global polioeradication effort is successful. More-over, a reduction in the infectious dis-ease burden in other countries helpsimprove the economic well-being ofdeveloping nations, which representthe fastest growing markets for U.S.products.
Organizations concerned with eco-nomic development, including the
World Bank and the World TradeOrganization (www.worldbank.organd www.who.int.inf-pr-2000/en/note 2000-wha02.html), have concludedthat disease reduction efforts are a nec-essary part of global developmentstrategies (Box 8). Infectious diseasescan sap the strength of a nation’s work-force and deplete its medical resources,making it more difficult to participatein the global economy. Promotingpolitical stability and sustainable devel-opment in developing nations is amajor goal of U.S. foreign policy.
Because health is an area of concernfor all nations, international projectsthat address infectious disease issuescan open avenues of communicationand ease tensions between the UnitedStates and other nations (Box 9).Investments in global health can alsohelp advance specific U.S. foreign pol-icy objectives, such as improving bilat-eral relationships with Vietnam,China, and the Palestinian Territories,and converting biological weaponsplants in the Russian Federation andthe newly independent states of theformer Soviet Union to peaceful uses.
Enhancing security. Security experts,including members of the U.S. Nation-al Intelligence Council6 (http://www. cia.gov/cia/publications/nie/report/nie99-17d.html) are concerned that largeoutbreaks like the HIV/AIDS pandem-ic may destabilize poorer nations.Slowed economic growth fueled bypoor health and disease in developingand former communist countries maychallenge democratic development andpolitical transitions and contribute to

20 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
humanitarian emergencies and mili-tary conflicts.
The recent intentional releases ofbiologic agents in the United Stateshave also intensified international con-cerns about bioterrorism. Due to theease and frequency of modern travel,an intentionally-caused outbreak thatbegins anywhere in the world canquickly become an international prob-lem. A contagious bioterrorist agentsuch as smallpox can spread rapidlyfrom person to person and from coun-try to country. A noncontagious agentsuch as anthrax can be spread byunexpected methods, including inter-national mail. The United States mustbe prepared to work with othernations to prevent illness and deathscaused by acts of bioterrorism.
CDC’s Role in Promoting Global Public Health
As its name implies, CDC is dedicatedto the control and prevention of dis-ease. The agency grew out of efforts tocontrol malaria in the southern UnitedStates and today retains a critical rolein addressing domestic infectious dis-ease threats. CDC is known in theUnited States for
• Working with state and local publichealth agencies to conduct diseasesurveillance
• Providing national leadership intimes of public health crisis
Box 8
Infectious Diseases and Economic Development
Infectious diseases like malaria and HIV/AIDS act asa massive societal brake, slowing both economic andhuman development.
Each year, malaria slows economic growth in sev-eral sub-Saharan African countries by as much as1.3% per person per year.7 Besides interfering withindividuals’ abilities to earn a living or attend school,malaria affects national economies by impedingtrade, foreign investment, and commerce. It alsointerferes with children’s mental and physical devel-opment and may encourage population growth whenparents decide to have bigger families, knowing thatsome of their children may die young. According toone estimate,8 if malaria had been eliminated 35 yearsago, Africa’s current annual gross domestic productwould be $400 billion, rather than $300 billion—aloss that is nearly five times greater than all develop-ment aid provided to Africa last year.
According to a World Bank report,9 HIV/AIDSmay subtract an additional 1% a year from GDPgrowth in some sub-Saharan African countries, dueto the continuing loss of skilled and unskilled work-ers in the prime of life. In South Africa, for example,HIV/AIDS may depress GDP by as much as 17% overthe next decade, which is a dangerous burden for ayoung democracy. The HIV/AIDS pandemic is desta-bilizing several other hard-hit nations, damaging theireconomic, social, political, military, and educationalinfrastructures, and creating vast numbers oforphans.

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 21
• Diagnosing rare, highly dangerous,and previously unknown diseases
• Responding rapidly to requests foroutbreak assistance
• Researching public health issuesand translating the findings intopractical tools for disease controland prevention
• Using surveillance data to drivepublic health action and informstrategic planning
• Integrating epidemiologic and labo-ratory expertise to address infec-tious disease problems
• Implementing programs for diseaseprevention and control
• Training public health workers
CDC works by invitation in many dif-ferent jurisdictions, including U.S.states and cities and other nations.Throughout its history, CDC has alsoprovided international leadership inpublic health, serving as a technicalconsultant to WHO and ministries ofhealth on projects that address infec-tious disease problems related toendemic diseases, wars, famines, orother disasters. Many of these projectswere funded and coordinated by theU.S. Agency for International Devel-opment (USAID). Through the FieldEpidemiology Training Programs (seeBox 24), the Epidemic Intelligence Ser-vice (http://www.cdc.gov/epo/dapht/ eis), and other programs, CDC has
Box 9
International Disease Control EffortsCan Create New Alliances
Mutual interest in addressing an outbreak or anongoing infectious disease problem may provide theimpetus for collaborations with countries who havenot historically cooperated with the United States onpublic health projects, or with countries whose rela-tionship to the United States is uncertain. One exam-ple is Hong Kong during the transfer of sovereigntyfrom the United Kingdom to China (see Box 5).
At times, concern about disease outbreaks may besufficiently strong to allow national antagonisms tobe set aside in the interests of disease control. Duringthe outbreak of Marburg hemorrhagic fever in 1998,for example, an international investigative team waspermitted to enter a contested part of the Democrat-ic Republic of the Congo. Similarly, an internationalguinea worm eradication team sponsored by theCarter Center received safe passage in southernSudan in 1995, due to a specially negotiated cease-firebetween the government of Sudan and rebel forces.Moreover, a polio eradication team was allowed tooperate in civil war–torn Sri Lanka during 2 “Days ofPeace for National Immunization” that were separat-ed by 30 days of warfare. Three decades earlier, dur-ing the height of the Cold War, the United States andthe Soviet Union agreed on the need to provide coor-dinated financial and technical support to the small-pox eradication effort.

22 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
also supported research and publichealth education on diseases ofregional or international importance.CDC helped lead the smallpox eradi-cation effort in the 1960s, and estab-lished collaborative research stations(see Box 10) in Côte D’Ivoire,Guatemala, and Kenya in the 1980sand in Guinea, Botswana, Thailand,and Uganda in the 1990s. Althoughconsiderable effort has been devotedto these international activities, CDC’sprimary focus has remained ondomestic health.
An evolving mission. In recent years,CDC’s overseas role has expandedrapidly. Global polio eradication andHIV/AIDS control programs have ledto substantial investments of CDCpersonnel and financial resources, ashave a succession of complex interna-tional emergencies. Between 1990 and2000, CDC provided rapid responseteams to nations in Asia, Africa,Europe, and Latin America to help
investigate outbreaks of unknown,highly dangerous, and highly infec-tious diseases (Appendix C), and pro-vided diagnostic support for hundredsof local investigations around theglobe. Some of these investigationsinvolved epidemic diseases and othersinvolved diseases that afflict refugeesand other displaced persons. In manycases, CDC epidemiologists served asmembers of WHO-coordinated inves-tigative teams supported by CDC-based WHO Collaborating Centrelaboratories (Appendix D). In additionto helping with outbreak control,CDC provides on-going public healthconsultation by placing resident advi-sors and assignees with key partneragencies and by working with coali-tions of national groups on emerginginfectious disease issues.
CDC’s growing presence overseaspresents new opportunities and newchallenges. This document, Protectingthe Nation’s Health in an Era of Glob-alization: CDC’s Global Infectious
Disease Strategy, represents an activeeffort to further define CDC’s evolvingglobal mission. It was developed inconsultation with public and privatesector partners at home and abroad. Itconsiders how CDC and its interna-tional partners can work together overthe long-term to improve capacity todetect, control, and prevent infectiousdiseases. This document builds on twoongoing efforts. First, it augments andamplifies the international componentof the 1998 CDC plan PreventingEmerging Infectious Diseases: A Strat-egy for the 21st Century10 (http:// www.cdc.gov/ncidod/emergplan).CDC’s ongoing efforts to strengthenU.S. domestic public health infrastruc-ture are critical to the success of ourinternational collaborations. Second,it fits within the larger framework ofCDC’s efforts to improve internationalhealth, as described in Working withPartners To Improve Global Health:A Strategy for CDC and ATSDR11
(http://www.cdc.gov/ogh/pub/strategy. htm).

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 23
Box 10
Examples of CDC’s Long-term Research Collaborations Overseas
CDC manages research collaborations (sometimesreferred to as “field stations”) in Côte D’Ivoire,Guatemala, Uganda, Guinea, Kenya, Botswana, andThailand, and is establishing long-term collaborativeprojects that may form the basis for a permanent centerin Vietnam. In general, CDC provides core funding forthe field stations, and USAID and other donors provideadditional support for both core activities and specialprojects.
The field station in Kenya is a collaborative effortbetween CDC and the Kenya Medical Research Institute(KEMRI). Most of the research takes place in westernKenya, in an area of intense, year-round malaria trans-mission and high incidence of HIV/AIDS. Major studieshave
• Demonstrated that presumptive malaria treatment ofpregnant women decreases the number of low birth-weight babies born.
• Demonstrated that use of insecticide-impregnatedbednets reduces mortality among children less than 2years of age in areas of high transmission.
• Provided critical information about the immuneresponse to malaria that is being used to design vac-cines.
The field station is also studying the impact of coinfec-tion with HIV and malaria, particularly in pregnancy.Other ongoing activities concern the development ofimmunity to vaccines among HIV-positive children,defining local spectrum of diarrheal diseases and antimi-crobial resistance among diarrheal pathogens, andaddressing the consequences of coinfection with HIVand schistosomiasis.
The field station in Guatemala–the Medical Ento-mology Research and Training Unit/Guatemala, orMERTU/G, is integrated into the Universidad del Valleand works closely with the Guatemalan Ministry ofHealth. MERTU/G has helped evaluate national pre-vention and control efforts related to malaria andonchocerchiasis. Research on leishmaniasis has led toimproved clinical treatment regimens, and research onfoodborne and waterborne diseases such as cholera hasled to improved prevention methods. To reduce deathsdue to Chagas disease—a significant health problem inGuatemala—the Guatemalan Ministry of Health andMERTU/G are conducting nationwide surveys to deter-mine prevalence and risk factors; supporting field andmolecular studies of the triatomine insect that carriesthe disease; and evaluating blood bank practices thatmay contribute to transmission through blood transfu-sions.
Future Directions: Capacity Building The field stations have provided valuable opportunitiesfor CDC scientists to participate in long-term, on-siteresearch on selected diseases of importance in develop-ing countries. Expansion of the field stations andstrengthened ties with local ministries of health wouldfacilitate additional opportunities to investigate endem-ic diseases, respond to new or emerging diseases, andprovide a stable training center for epidemiologists andlaboratory scientists from CDC and the local region. Aspart of CDC’s global strategy, one of the existing fieldstations may also provide the nucleus of the first Inter-national Emerging Infections Program (page 53).

Applied Research on Dis-eases of Global Importance.
CDC’s laboratorians, epidemiologists,and behavioral scientists will maintainan active research program to developtools to detect, diagnose, predict, andeliminate infectious diseases of globalor regional importance. When a newdisease threat is reported anywhere inthe world, CDC’s laboratorians andfield investigators will be available tohelp answer questions about diseasetransmission, treatment, control, andprevention.
Application of Proven Public Health Tools.
The worldwide burden of infectiousdiseases will be significantly reducedas currently available tools with docu-mented efficacy are rapidly dissemi-nated to the most severely affectedpopulations. Research discoveries willbe translated into practical treatments,vaccines, diagnostic tests, and diseaseprevention strategies that are ready foruse by ministries of health and publichealth agencies. CDC’s resources willbe effectively marshaled to assist itspartners in applying these tools inmany countries, saving millions oflives.
Global Initiatives for Disease Control.
Sustained global efforts will reduce theprevalence of HIV/AIDS in young peo-ple by 25% and reduce deaths fromTB and malaria by 50% by 2010.Infant mortality will be reduced in the
24 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
This document defines CDC’s glob-al infectious disease priorities in
six areas, keeping in mind the intimaterelationship between international andU.S. health, selected in consultationwith global public health partners. Inlooking towards the future, CDC envi-sions increased activity and progress ineach area:
International OutbreakAssistance.
CDC will maintain the capacity toidentify and investigate a broad spec-trum of human diseases and serve asan internationally recognized resourcethat helps maintain global awarenessof new and emerging threats.
A Global Approach to Disease Surveillance.
Regional and disease-specific surveil-lance and response networks willincrease in number and geographicalarea until they cover all parts of theworld and monitor all infectious diseases of regional or global impor-tance. The networks will link up witheach other and evolve into a global“network of networks” that providesearly warning of new health threats—including drug-resistant diseases—andincreased capacity to monitor theeffectiveness of public health controlmeasures.
VISION FORTHE FUTURE
1
2
3
4
5

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 25
poorest countries through enhanceddelivery and use of vaccines againstrespiratory illnesses and other child-hood diseases. Polio and dracunculia-sis will be eradicated worldwide,paving the way for future efforts toeliminate such diseases as measles,lymphatic filariasis, onchocerchiasis,Chagas disease, trachoma, rubella,and hepatitis B.
Public Health Training andCapacity Building.
An interconnected group of Interna-tional Emerging Infectious DiseasePrograms (IEIPs) will integrate diseasesurveillance, laboratory studies, andprevention activities, and providehands-on public health training in dis-ease detection, program management,
and outbreak investigation. The IEIPsites will partner with Field Epidemi-ology Training Programs (FETPS) andother institutions to perform popula-tion-based research on transmission ofendemic and emerging diseases andconduct emergency surveillance when-ever a new threat appears. The long-term goal of the IEIPs will be to devel-op sustainable, in-country humancapacity to participate in national andregional efforts for disease surveillanceand outbreak response.
Implementation of specific objectivesin these six areas will help realizeCDC’s vision of a world in which U.S.citizens and all people everywhere arebetter protected from infectious dis-eases.
6

26 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
This plan was prepared by CDC’sNational Center for Infectious
Diseases, in collaboration with othermajor CDC centers and programsinvolved in addressing emerging infec-tious diseases. These include the Officeof Global Health, the National Centerfor HIV, STD, and TB Prevention, theNational Immunization Program, theEpidemiology Program Office, and thePublic Health Practice Program Office.CDC has also worked with globalorganizations and agencies to developthis strategy. Website addresses provid-ing additional information about part-ner organizations and health publica-tions and reports referred to in thisdocument are provided in Box 2 andthroughout the text of the document.
The strategy will be implementedincrementally over the next five years,as funds become available, beginningwith the highest priorities for 2001-2002 (Box 1). As CDC carries out thisstrategy, it will coordinate with foreigngovernments, international organiza-tions (including WHO, the Joint Unit-
ed Nations Programme on AIDS[UNAIDS], and the United NationsChildren’s Fund [UNICEF]), otherU.S. agencies (including USAID, theNational Institutes of Health [NIH],the Food and Drug Administration[FDA], the Department of Defense[DoD], the Department of VeteransAffairs [DVA], the U.S. Department ofAgriculture [USDA], the NationalOceanic and Atmospheric Administra-tion [NOAA], and the National Aero-nautics and Space Agency [NASA]),professional societies, research institu-tions, and schools of public health,medicine, nursing, and veterinary sci-ence.
CDC will also participate in inter-national coalitions that support dis-ease eradication efforts and otherregional and global health initiatives.These coalitions may include nationaland local nongovernmental organiza-tion (NGOs; e.g., Rotary Internation-al and CARE), community-based andfaith-based organizations, and com-munities of color. In addition, CDCwill work closely with groups thatconduct or promote regional diseasesurveillance, such as the CaribbeanEpidemiology Center (CAREC), theAsia-Pacific Economic Cooperation(APEC; see also Appendix E), and the Training in Epidemiology and Pub-lic Health Interventions Network(TEPHINET).
PARTNERSHIPS AND IMPLEMENTATION

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 27
Other implementation partnersinclude
• Pharmaceutical and biotechnologycompanies that develop vaccines,drugs, and rapid diagnostic tests
• NGOs that address related healthproblems (e.g., maternal and childhealth, environmental health, occu-pational health, and chronic illness-es)
• Development agencies, develop-ment banks, foundations, and otherorganizations that aim to reducepoverty by reducing the incidenceof endemic diseases
As emphasized in CDC’s Work-ing with Partners To Improve Glo-bal Health: A Strategy for CDC andATSDR11 (http://www.cdc.gov/ogh/ pub/strategy.htm), CDC’s collabora-tive work overseas will be based onfive approaches:
• CDC’s activities will be rooted insound science, bioethical principles,and local needs.
• The primary modality for actionwill be through partnerships withother institutions.
• CDC will work in technical areas inwhich it has established expertiseand capability.
• CDC will pursue long-term bilater-al relationships, because of theirenhanced productivity.
• CDC will ensure that it has theworkforce and administrativemechanisms required for full imple-mentation of the infectious diseasestrategy.

28 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
When a new, highly dangerous, orreemerging disease is detected
anywhere on the globe—whether in adeveloping or industrialized country,in a close ally or a “nation of con-cern”—U.S. citizens, as well as foreigngovernments, often rely on CDC toprovide outbreak assistance and pub-lic health information. CDC is unusu-al among public health institutions inits comprehensive capacity to identifya wide range of infectious bacteria,viruses, fungi, parasites, and rickettsia.
In past years, however, maintainingthis capacity has not always been apriority. Attempts have been made tocut costs by reducing support for lab-oratory expertise on diseases that arecurrently uncommon in the United
PRIORITIES ANDOBJECTIVES
Priority Area 1: International Outbreak Assistance
Outbreak of Ebola hemorrhagic fever,
Uganda, 2000. The isolation ward of GuluMunicipal Hospital, Gulu, Uganda, duringan outbreak of Ebola hemorrhagic fever inOctober 2000. There is no known drugtreatment or vaccine for this disease, whichis transmitted person-to-person throughcontact with infected bodily fluids and hasa case-fatality ratio of 50–90%.
At the invitation of the Ugandan Min-istry of Health, CDC sent several teams ofscientists to Gulu to participate in a multi-national WHO-coordinated response team.The response team helped bring the epi-demic under control by providing assis-tance and consultation to help rapidly iden-tify cases, provide safe care, and interruptthe spread of the virus.
Photographer: Daniel Bausch, Division of Viral and Rick-
ettsial Diseases, National Center for Infectious Diseases,
CDC
States, including zoonotic diseases likeplague and leptospirosis. However,CDC’s repeated experience with out-breaks of diseases once thought to bearchaic or obscure—including a 1994outbreak of plague in India, a 1995outbreak of a virulent pulmonaryform of leptospirosis in Nicaragua,and a 2000 outbreak of leptospirosisin Malaysian Borneo among athletesat an international competition (Box11)—has underscored the value ofhaving a comprehensive, integratedability to identify and investigate mosthuman diseases and to recognize newthreats. However, gaps remain inCDC’s repertoire of diagnostic tools insuch areas as diseases caused by prions(e.g., new variant Creutzfeldt-Jakob

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 29
disease, the human consequence ofinfection with bovine spongiformencephalopathy, or “mad cow dis-ease”), and some areas requireupgrading to remain effective (e.g.,leptospirosis, yellow fever, diphtheria,anthrax, and helminthic diseases).
CDC frequently collaborates on inter-national outbreak investigations con-ducted in partnership with hostnations. CDC participation occurs onan ad hoc basis, in response torequests for assistance from foreigngovernments or WHO. There is noformal structure for this activity, norare there designated resources. Anunderlying principle of the globalstrategy is the recognition that interna-
tional outbreak assistance is an inte-gral function of CDC. Supporting thisfunction will require augmenting,updating, and strengthening CDC’sdiagnostic facilities, including labora-tories that participate in the WHOCollaborating Centre network, as wellas capacity for epidemiologic investi-gation overseas, including field logis-tics and data management.
Outbreak follow-up. In the future, aspart of the global strategy, CDC willroutinely offer to assist host-countryministries of health and WHO inassessing the public health situation inthe aftermath of a major outbreak. Ifrequested, CDC will send a dedicated
prevention team to revisit the out-break site and suggest additionalstrategies to improve disease surveil-lance and outbreak response. Theteam will share clinical and epidemio-logic outbreak data with healthauthorities and work to strengthenlocal laboratories. The team may alsosponsor local workshops or confer-ences to consider lessons learned fromthe outbreak, review local hospitalresources, and discuss long-term sur-veillance efforts. These follow-upefforts will help maintain mutuallybeneficial relationships and researchpartnerships between CDC, WHO,and local health authorities (Box 12and Priority Area 2).
Box 11
An Outbreak of Leptopirosis Affecting Athletes from 26 Countries Reported bythe GeoSentinel Disease Surveillance System
In September 2000, several athletes returning home fromthe EcoChallenge-Sabah 2000 multisport expeditionrace in Malaysian Borneo fell ill with leptospirosis,apparently contracted while swimming in a contaminat-ed river. Leptospirosis causes severe fever, headache,chills, muscle pain, and cramps. Left untreated, it canlead to kidney and liver failure, meningitis, and death.
Three clinics that participate in GeoSentinel, the glob-al surveillance network of the International Society ofTravel Medicine (Appendix E), reported a cluster ofacute febrile illness among Eco-Challenge racers andhelped identity its cause. A clinic in London, England,reported four instances of suspected leptospirosis andqueried other GeoSentinel sites for similar cases. Clinicsin New York City and Toronto responded with reportsof five more cases among the same group of athletes, and
all communicated their findings to CDC. Further eval-uation indicated that all cases were clinically compati-ble with leptospirosis.
Leptospirosis is contracted by coming into contactwith or swallowing water contaminated with animalurine. During the 12-day Eco-Challenge race, approxi-mately 300 athletes from 26 countries sailed on openocean and then bicycled and hiked through torrentialjungle rain and mud. After that, the racers swam andcanoed in a storm-swollen river and waded throughcaves filled with bat guano. Analysis by CDC suggestedthat participating in the river swim was significantlyassociated with illness. At least 44% of the 155 U.S.participants were affected. Additional cases of lep-tospirosis were identified in athletes from several othercountries as well.

30 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Box 12
Follow-up Activities in the Aftermath of the 1994 Plague Outbreak in India
In September, 1994, rumored outbreaks of bubonic andpneumonic plague in western India caused widespreadpanic and extensive disruptions in international traveland trade. The Indian Ministry of Health authorized aninvestigation by a WHO international team that includ-ed scientists from CDC, the Russian Federation, and bythe WHO South East Asia Regional Office. The work ofthis team was severely compromised by the inability ofIndian laboratories to confirm plague cases by usingstandard diagnostic methods.
The lack of diagnostic capabilities arose because theIndian Ministry of Health, a former world leader inplague vaccines and diagnosis, believing that plague nolonger existed in the country, had allowed its laboratorydiagnostic infrastructure to deteriorate. At the sugges-tion of WHO, the government of India invited CDCteam members to return to conduct field training exer-cises with Indian epidemiologists and hold workshops inplague microbiology at India’s National Institute forCommunicable Diseases (NICD). Later that year, micro-biologists from NICD, the All-India Institute of MedicalScience, and the Haffkine Institute in Bombay came toCDC’s laboratory in Fort Collins, Colorado, as visitingscientists to learn techniques for confirming infectionwith Yersinia pestis (the causative agent of plague), pro-cedures for preparing standardized diagnostic reagents,
and new and advanced molecular methods for identify-ing and characterizing Y. pestis strains.
The relationships that developed among U.S. andIndian scientists during the 1994 outbreak and subse-quent collaborations had lasting scientific and diplo-matic effects. During the Cold War, India had main-tained few contacts with the U.S. public healthcommunity, preferring to collaborate with Russianhealth officials, who (up until 1989) had sent regularshipments of plague diagnostic reagents to NICD.After 1994, however, India was more open to publichealth collaboration with the United States. For exam-ple, the Indian Ministry of Health worked closely withCDC when it renovated and modernized its nationalplague laboratory during the late 1990s, and also whenit reorganized and computerized its national communi-cable disease surveillance system. The Indian Ministryof Health also played an active role in two regional andtwo global workshops on plague organized by WHOand CDC between 1996 and 2000.
International contacts made during the 1994 plagueoutbreak also led to working relationships with theKazakh Institute for Research on Plague Control inAlmaty, Kazakhstan, the Chinese Academy of Preven-tive Medicine in Beijing, and the Institute of EndemicDiseases Control and Research in Yunnan, China.
Objectives for Priority Area 1
Dedicate Resources to Interna-tional Outbreak Assistance
• Facilitate CDC participation ininternational outbreak investiga-tions by
- Developing standard operatingprocedures for responding togovernments’ requests for out-break assistance, in coordinationwith WHO
- Identifying and purchasingequipment and reagents andincreasing capacity for logisticalsupport
- Establishing standard proce-dures for distributing and track-ing specimens for efficient testingat more than one CDC laborato-ry when the cause of an outbreakis unknown.
- Maintaining an inventory ofCDC personnel with expertise in
diseases of regional or globalimportance
- Maintaining a registry of diseasespecialists outside of CDC whohave expertise in diseases ofregional or global importance(“Active Reserves”)
- Developing research protocolsthat might be used during out-break investigations for con-trolled trials of drug treatmentsor other public health interven-tions (see Priority Area 3)

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 31
- Strengthening the capacity ofdeveloping countries to identifyoutbreaks and to request WHO,CDC, or other outside assis-tance as needed
Strengthen Diagnostic Capacity
• Strengthen CDC laboratories (in-cluding CDC-based WHO Collabo-rating Centres) that can identifydiseases that are rare or unknown,drug-resistant, or highly dangerous.
This effort will include strength-ening CDC’s capacity to identifyanimal diseases that can affecthumans, working in conjunctionwith USDA and other partners.
• Strengthen national public healthlaboratories in developing coun-tries by providing diagnostic refer-
ence reagents, laboratory manuals,and training opportunities for labo-ratory scientists.
Strengthen InvestigativeCapacity at CDC
• Rebuild CDC’s capacity to respondto international outbreaks.
• Maintain and expand epidemiolog-ic expertise in a wide range of path-ogens, helping to create a new gen-eration of experts in infectious dis-ease prevention and control.
• Strengthen international collabora-tion during investigations, workingwith many partners, including
- WHO Global Alert and Re-sponse Network (Box 14; h t t p : / / w w w. w h o . i n t / e m c -documents/surveillance/docs/whocdscsr2003.pdf and
Box 13
Outbreaks Among Refugees in Kosovo and the Sudan
rodent excrement and carcasses containing the bacteriaFrancisella tularensis. The epidemic was halted by insti-tuting simple sanitation measures.
Louseborne Relapsing Fever in the Sudan In April, 1999, epidemiologists from CDC assistedWHO in investigating an apparent outbreak of hemor-rhagic fever in southern Sudan among seminomadictribes displaced by famine, civil war, and intertribalstrife. The causative agent proved to be the spirocheteBorrelia recurrentis, which is transmitted by body lice.The outbreak affected about 20,000 people and causedabout 2,000 deaths before the diagnosis was establishedand disease control measures were implemented.
Tularemia in Kosovo In April and May, 2000, an epidemiologist and ecologistfrom CDC joined a WHO-led investigation of an out-break of tularemia among displaced persons returningto damaged homes and farms in rural Kosovo. The ill-ness, which affected 500 to 1,000 people, was charac-terized by fever, severe sore throat, enlarged lymphnodes in the neck, and abscess formation.
The people who fled from Kosovo in March 1999had left behind unharvested crops and homes withunprotected stocks of food. Over the following months,the local populations of field mice and domestic ratsincreased exponentially. Returning refugees became illafter ingesting food and water contaminated with
h t t p : / / w w w. w h o . i n t / e m c -documents/surveillance/docs/whocdscsr2002.pdf).
- European Programme for Inter-vention Epidemiology Training(EPIET;http://www.epiet.org/epiet).
- U.S.-Mexico Border Infectious Disease Surveillance system(BIDS;http://www.r10.tdh.state.tx.us/obh/bids.htm).
- Training Programs in Epidemiol-ogy and Public Health Interven-tions Network (TEPHINEThttp://asclepius.ic.gc.ca/tephinet/.
• Improve coordination among theDepartment of State, CDC, stateand local agencies during investiga-tions of infectious disease threats atU. S. ports of entry.

32 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Box 14
WHO and CDC: Collaboration on International Outbreak Assistance
• Ensure that the United States isprepared to assist in investigationsof international bioterrorist inci-dents.
• Continue to work with WHO andother partners to investigate epi-demics that occur among refugeesand displaced persons (Box 13).
Strengthen Control Efforts
• Strengthen CDC’s capacity to pro-vide prompt and effective epidemiccontrol, by assigning epidemiolo-gists to help monitor disease spreadoverseas, laboratory scientists toprovide rapid diagnostic testing,and social and behavioral scientiststo design and implement communi-ty education and mobilizationefforts.
WHO and CDC work in close partnership to help con-trol outbreaks that involve diseases of unknown cause,diseases with high fatality rates, and diseases that arelikely to spread across borders:
• As an international entity, WHO is a critical partnerin opening doors to U.S. scientists, facilitating U.S.participation in international efforts to identify newthreats and contain potential pandemics. WHO alsoplays a special role in international press manage-ment, encouraging nations to share outbreak infor-mation while helping to minimize false rumors thatcause damage to the trade and tourism industries ofaffected countries.
• CDC provides WHO with technical guidance, includ-ing diagnostic and epidemiologic support. Because
WHO does not maintain laboratory resources of itsown, it relies upon an international network of Col-laborating Centres that includes more than 30 diag-nostic laboratories located at CDC (Appendix D)
At the present time, WHO is strengthening itsability to facilitate international outbreak responseefforts, as well as to support global health initiativesthat address infectious diseases (see Box 6). As partof this effort, WHO is establishing a Global Alertand Response Network to promote prompt report-ing of disease outbreaks and help coordinate offersof outbreak assistance—e.g., supplies, consultation,or on-site support—from public and private sectorpartners.
• Support efforts to provide suppliesduring outbreak emergencies bypartners such as FDA, WHO,NGOs, pharmaceutical companies,multinational corporations, andother members of the private sector.
Offer Follow-Up
• Offer to conduct follow-up activi-ties at the site of an outbreak, incollaboration with ministries ofhealth, WHO, InternationalEmerging Infections Programs(IEIPs; page 53), and existingnational or donor-supported dis-ease control programs. Activitiesmay include
- Sharing data to guide ongoingcontrol programs
- Improving infection controlpractices
- Building laboratory capacity
- Establishing ongoing surveil-lance for the outbreak pathogen
- Implementing long-term preven-tion strategies through the appli-cation of proven health tools (seealso Priority Area 4)

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 33
Stimulated in part by the AIDSpandemic, national and interna-
tional groups, including the NationalScience and Technology Council in1995 and the Group of Eight in 1997,have called for the establishment of aglobal system for disease surveillanceand outbreak response. U.S. agenciesare working with international part-ners to help achieve this goal.
Despite advances in public healthtelecommunications, however, theglobal implementation of this goal hasnot been straightforward. Notableprogress has been made at the regionallevel, with the establishment of suchinternational programs as the Carib-bean Epidemiology Center’s diseasesurveillance network, the Amazon andSouthern Cone networks in SouthAmerica, the Integrated Disease Sur-veillance and Epidemic Preparednessand Response Project in Africa, theMekong Basin Disease Surveillancesystem in Southeast Asia, and theInternational Circumpolar Surveil-lance system in Alaska, Canada,Greenland, and the circumpolarregions of Europe. These and other
Priority Area 2: A Global Approach to Disease Surveillance
fledgling networks (Appendix E) rep-resent pioneering attempts to workacross borders to enhance detectionand control of outbreaks of knowndiseases while maintaining the flexibil-ity to recognize new disease problems.The networks are testing many differ-ent approaches (e.g., syndromic sur-veillance, laboratory-confirmed dis-ease-specific surveillance, hospital- based surveillance, and district-levelsurveillance), depending on localneeds, cultural preferences, and humanand technological resources.
In the years ahead, regional diseasesurveillance networks will grow innumber and geographical scope. In thelong run, regional and disease-specificnetworks should expand, interact, andevolve into a global “network of net-works” that helps ensure early warn-ing of new and reemerging threats andincreased capacity to monitor theeffectiveness of public health controlmeasures
CDC can stimulate this process byproviding technical assistance, evalu-ating regional progress, and workingwith WHO, other U.S. agencies, andother interested groups to strengthenthe networks’ telecommunicationscapacities and encourage the use ofcommon software tools and harmo-
nized standards for disease reporting.CDC can also help revise the Interna-tional Health Regulations, whichdescribe internationally-reportable di-seases and syndromes. In addition,CDC will encourage linkages betweenregional networks and veterinary sur-veillance systems that monitor illness-es and epidemics among agriculturaland feral animals. Several major out-breaks of zoonotic diseases (diseasesof animals that also affect humans)involving agricultural animals haveoccurred in recent years (Box 15).CDC will also support disease surveil-lance efforts in tropical or heavilyforested areas that are likely sources ofhuman infection with unknownzoonotic or vectorborne diseases.
CDC’s priorities in global surveil-lance will be balanced with the priori-ties of collaborating countries, andCDC’s programs will be coordinatedwith the ongoing efforts of develop-ment agencies and NGOs that builddisease surveillance capacity at thenational level. CDC can best supportboth national and regional efforts by providing state-of-the-art diagnos-tic and epidemiologic tools; by devel-oping surveillance standards andguidelines, and by creating new meth-ods for predicting disease risk. CDC can also increase training oppor-tunities by helping establish new or expanded Field EpidemiologyTraining Programs (FETPs), Public

34 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Disease surveillance personnel at the
Caribbean Surveillance System
(CARISURV) of the Carribean Epidemi-
ology Center (CAREC). CARISURV is anelectronic disease surveillance systemthat serves 21 nations: Anguilla,Antigua & Barbuda, Aruba, Bahamas,Barbados, Belize, Bermuda, British Virgin Islands, Cayman Islands,Dominica, Grenada, Guyana, Jamaica,Montserrat, Netherlands Antilles, St.Kitts & Nevis, St. Lucia, St. Vincent &Grenadines, Suriname, Trinidad &Tobago (host country), Turks & Caicos Islands.
CARISURV employs computer-based modules to:
• Track cases of measles as part ofPAHO’s campaign to eliminatemeasles in the Americas
• Track cases of HIV/AIDS • Track cases of unusual or unex-
plained diseases reported byCAREC's Physician-Based SentinelSurveillance system
• Compile weekly reports of notifiablediseases
• Maintain a database of deathscaused by infectious agents
• Help provide distance-learning courses for public health and medical personnel
A new module that facilitates hotel-based disease surveillance is underdevelopment.
CDC and the Walter Reed Army Instituteof Research have worked with CAREC toprovide CARISURV members with bioin-formatics training, technical support,computer equipment, and public health software, including thePublic Health Laboratory InformationSystem (PHLIS) for reporting laboratory- confirmed cases of infectious disease.PHLIS was originally developed at CDCfor use by U.S. state health depart-ments.
Information Services Unit, CAREC.
Health Schools Without Walls(PHSWOW; http://www.tulane.edu/ ~phswow/), and Sustainable Manage-ment Development Programs (PriorityArea 6, Boxes 16 and 24).
The surveillance data gathered bythe regional networks will be used notonly to detect outbreaks but also toevaluate global health initiatives (Pri-ority Area 5) and to drive nationalpublic health programs and decision-making. Disease surveillance data arecrucial, for example, in assessing theeffectiveness of vaccination programsand the risk factors for underimmu-nization in a given area.
Objectives for Priority Area 2
Facilitate Regional DiseaseSurveillance
• Work with WHO and other part-ners to identify gaps in global dis-ease surveillance by conducting ahealth situation analysis.
• Provide technical and materialassistance to regional networks thatcan fill global gaps in disease sur-veillance.
• Host meetings that bring the lead-ers of regional surveillance net-works together on a periodic basisto exchange experiences and meth-ods and facilitate collaboration.
• Develop surveillance modules thatcan facilitate standardization ofdisease reporting among regionaldisease surveillance networks.

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 35
Box 15
Agricultural Costs of Controlling Zoonotic Diseases Carried by Food Animals
When a dangerous animal-borne disease spills over intothe human population, a government may be forced toslaughter large numbers of food animals as a controlmeasure, despite considerable economic costs.
This happened in 1999 when Malaysian healthauthorities were faced with an outbreak of encephalitisamong farm workers that had a nearly 50% mortalityrate. The cause of the outbreak turned out to be a pre-viously unknown paramyxovirus called the Nipah virus,which is carried by swine. To control the outbreak, mil-lions of pigs were slaughtered within a few weeks, severe-ly harming the Malaysian meat industry. Two yearsbefore, a similar precautionary measure was taken by thegovernment of Hong Kong, which arranged the culling ofall 1.6 million chickens on Hong Kong Island and theNew Territories to prevent chicken-to-human transmis-sion of a virulent avian form of influenza (Box 5).
The costs of measures to control the outbreak ofbovine spongiform encephalopathy (BSE, or “mad cowdisease”) in the United Kingdom and continentalEurope, and the related outbreak of an invariably fatalhuman neurodegenerative disease (new variantCreutzfeldt-Jakob disease [nvCJD]) have also been high.Ingestion of beef containing the causative agent of BSE(a prion) can result in the development of nvCJD manyyears later. The export of live cattle and cattle products(other than milk) from the UK has been temporarilybanned by the European Commission, and trade inthese products has been affected on a global basis. Gov-
ernment officials have come under fire, and consumersacross Europe have changed their eating habits due toconcern over the spread of BSE. Control measures,including the slaughter of affected cows, have thus farcost the U.K. government an estimated 3.5 billionpounds (about 5 billion U.S. dollars).
The rapidly spreading outbreak of foot-and-mouthdisease in Great Britain and continental Europe in 2001threatens to dwarf the economic costs of the BSE epi-demic and devastate the centuries-old British livestockindustry. Foot-and-mouth disease does not infecthumans but can be spread by travelers who have con-taminated soil on their shoes or clothing or who carrycontaminated food products. The St. Patrick’s Dayparade in Ireland was cancelled due to concerns aboutspreading the virus, and the British army has been draft-ed to help bury the carcasses of animals slaughteredbecause of potential exposure to the disease. Officialscredit high-quality animal health surveillance andimportation restrictions for the absence of foot-and-mouth disease in the United States, but remain con-cerned because similar measures have failed to containthe spread of the disease in continental Europe.
These examples demonstrate the potential impact aninfectious disease outbreak can have on commerce aswell as on human and animal health. If the UnitedStates were forced to destroy a significant number ofcattle, sheep, pigs, or chickens to control an epidemic,the costs might easily rise into the billions.

36 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Modules may cover sentinel diseasesurveillance, disease-specific sur-veillance, and syndromic diseasesurveillance.
• Help WHO strengthen WHO coun-try and regional offices by provid-ing CDC scientists, as needed, toassist with national and regionaldisease surveillance efforts.
• Assign epidemiologists and labora-tory scientists from CDC to DoDlaboratories in Indonesia, Kenya,and Thailand, in addition to thosealready in Egypt and Peru, to sup-port DoD efforts to help strengthenregional disease surveillance (Ap-pendix E).
• Engage nontraditional partners,such as medical missionary organi-zations and multinational corpora-tions, in regional disease surveil-lance activities, particularly inregions that lack adequate publichealth infrastructures.
Use State-of-the-Art Tools
• Work with DoD, USAID, develop-ment banks, foundations, and otherpartners to provide public healthagencies in developing countrieswith hardware (e.g., hand-heldcomputers for field use), specializedsoftware (e.g., EPI INFO 2000,PHLIS, and LITS+), and reliableInternet access to facilitate partici-pation in regional infectious diseasenetworks and training activities.
• Work with many partners to pro-vide regional networks with field-friendly diagnostic tests (e.g., dip-sticks).
• Work with WHO and other part-ners to develop laboratory stan-dards for diagnostic testing anddata standards for disease and syn-drome reporting.
Promote New Paradigms forGlobal Disease Surveillance
• Establish mechanisms for regularinformation exchange between vet-erinary and agricultural organiza-tions and public health agencies onnew and re-emerging animal dis-eases that might affect humans.
• Work with NOAA, NASA, DoD,NIH, the National Science Founda-tion, and many other partners tocreate models that predict the riskof zoonotic and vectorborne diseaseby integrating climatic, environ-mental, veterinary, entomologic,and epidemiologic data. CDC canplay a major role in providing epi-demiologic data.
• Encourage the use of molecularmethods for microbial subtypingand outbreak detection, such asPulseNet methods for the detectionof foodborne disease outbreaks (seeSurveillance for Foodborne andWaterborne Diseases).
Strengthen WHO’s Disease-Specific Global SurveillanceNetworks
• Provide technical assistance toWHO-sponsored networks thatmonitor specific diseases of globalimportance, such as polio, measles,influenza, and TB (Appendix E).
• Work with WHO to help establisha global network for surveillanceand control of plague, using theWHO Influenza Surveillance Net-work as a model.
• Work with WHO and other part-ners to help draft a new set of Inter-national Health Regulations (IHR)that includes a set of international-ly-reportable diseases or diseasesyndromes.
Facilitate Surveillance forFoodborne and WaterborneDiseases
• Improve global surveillance forfoodborne and waterborne diseasesby
- Establishing sentinel surveillancesites for foodborne and water-borne disease at InternationalEmerging Infections Programs(IEIPs; page 53).
- Working with PAHO and FDAto expand PulseNet—the U.S.early warning system for food-borne diseases—into a regionalsystem for detecting outbreaks offoodborne disease throughout

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 37
the Americas. PulseNet com-pares the molecular fingerprintsof bacterial isolates from manydifferent sources. It can trace thesource of an outbreak to ship-ments of contaminated foodbought and consumed at differ-ent geographic locations. (SeeBox 2.)
- Establishing a mechanism for theregular exchange of surveillanceinformation on foodborne dis-eases (e.g., salmonellosis, shigel-losis, and E. coli O157:H7 infec-tion), including PulseNet finger-printing data, with EuropeanUnion partners.
• Seek WHO approval for establish-ing a CDC-based WHO Collabo-
rating Center for Salmonella Sur-veillance that provides support toWHO’s Global Salmonella Surveil-lance system (Global Salm-Surv).
Facilitate Surveillance forAntimicrobial Resistance
• Provide technical assistance to helpimplement WHO’s Global Strategyfor the Containment of Antimicro-bial Resistance (http://www.who. int/emc/globalstrategy/strategy.html).
• Work with other U.S. agencies todraft and implement Part II of theU.S. Public Health Action Plan ToCombat Antimicrobial Resistance(Box 4), which will consider therole of the U.S. Government in
addressing global resistance prob-lems, such as the spread of mul-tidrug-resistant TB.
• Increase the number of regionallaboratories that conduct state-of-the-art testing for drug resistance,working through the WHO Exter-nal Quality Assurance System andthe WHO Collaborating Centre forAntimicrobial Resistance and usingthe new WHO/CDC laboratorymanual for standardized suscepti-bility testing.
• In collaboration with WHO, theEuropean Union, and other part-ners, explore the possibility ofestablishing an expert workinggroup that sets international stan-dards for detecting and reportingdrug-resistant threats.
Box 16
A Growing Community of International Public Health Leaders
By fostering contacts between CDC staff and scientistsfrom other countries (during outbreak investigations,scientific conferences, training courses, and disease pre-vention projects), CDC is helping build an internationalcommunity of epidemiologists and laboratory scientistswho are prepared to respond to emerging infectious dis-ease threats, whenever and wherever they arise. Oftenlinked by e-mail, as well as by phone and fax, these indi-viduals are part of an informal network that shares out-break alerts and research data and provides assistanceand consultation during infectious disease emergencies.
In addition to these informal exchanges, CDC offersformal training programs in epidemiology (e.g., throughField Epidemiology Training Programs, the PublicHealth Schools Without Walls, and the Epidemic Intel-ligence Service), laboratory diagnostics (e.g., throughfellowships and disease-specific training workshops),and public health management (e.g., through the Sus-tainable Management Development Program) that sup-port the development of public health leaders aroundthe world.

38 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
CDC’s researchers have a dual role.They not only identify the
microbes, risk factors, and epidemio-logic conditions that lead to outbreaks,but also conduct applied research onways to detect, prevent, and controlthem. Maintaining a comprehensivediagnostic and investigative capacitygoes hand-in-hand with maintaining abroad-based research program onendemic and epidemic diseases thatincludes studies in applied epidemiolo-gy, microbiology, and behavioral andsocial science.
A research program on diseases thatare uncommon in the United States isa valuable resource, both for humani-tarian reasons and because of the dan-gers represented by some imported dis-eases. Had scientists begun to study“slim disease”—now known asAIDS—when the syndrome was de-scribed in central Africa in the late1970s,12 the world health communitymight have learned much earlier howHIV is acquired and what can be doneto prevent its spread.
An in-depth knowledge of a widerange of infectious pathogens can alsofacilitate the identification and charac-terization of new microbes that emergein the United States. One example con-cerns hantavirus pulmonary syndrome(HPS), an often-fatal disease first iden-tified in 1993 in the Four Cornersregion of the United States. In 1993hantavirus research was a low priority
Priority Area 3: Applied Research on Diseases of Global Importance
Life cycle of West Nile virus. West Nile encephalitis—which is carried by birds inAsia, Africa, and Europe and spread to humans by mosquito bite—has been rec-ognized as a U.S. health threat since 1999. CDC is working with colleagues in Aus-tralia, the Czech Republic, France, Israel, Romania, and Russia to study the epi-demiology, ecology, and pathogenesis of the West Nile virus and find ways toprevent and control its transmission.
From the CDC website: http://www.cdc.gov/ncidod/dvbid/westnile/birds&mammals.htm
in the United States, because han-tavirus-associated disease had neverbefore been recognized in the WesternHemisphere. However, a few laborato-ries supported by DoD had continuedto collect information on a hantaviraldisease called Korean hemorrhagicfever or hemorrhagic fever with renalsyndrome (HFRS) that killed a signifi-cant number of United Nations troopsduring the Korean Conflict. Because ofthese HFRS studies, the CDC out-
break team in Four Corners wasarmed with sophisticated serologicand molecular tools that allowed themto diagnose HPS in a short time.Because it was known that the HFRShantavirus is transmitted by rodents,the team rapidly honed in on the ani-mal reservoir of the HPS virus andprovided disease prevention guidelinesto the people in the area.
Several fundamental precepts inform CDC’s infectious disease

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 39
research collaborations with othercountries. First, the overriding purposeof CDC’s research work overseas is tolead the way in demonstrating howindividuals and governments can bestprevent and control disease. Second, itis important for CDC to help strength-en international research capacity bysupporting extramural research athome and abroad, through collabora-tions, cooperative agreements, andpeer-reviewed grants. Third, CDC’sresearch activities must be rooted inbioethical principles, respecting theneeds and rights of human researchsubjects. Fourth, CDC must strive toengage new research partners, in addi-tion to its traditional partners at uni-versities and schools of public health.Research collaborators may includescientists from private companies,NGOs, and other U.S. agencies (e.g.,NIH, FDA, DoD, NASA, NOAA, andUSDA).
Long-term, on-site research collabora-tions are especially important, becauseit is often very difficult to study newand hazardous pathogens while anoutbreak is in progress. Long-termpartnerships with in-country researchinstitutions may be mutually benefi-cial, facilitating collaborative fieldresearch and clinical studies, providingopportunities for technology transferand training, and building internation-al friendships and trust within the sci-entific and public health communities.
Objectives for Priority Area 3
Strengthen Overseas ResearchCollaborations by EstablishingIEIPs
• Establish an inventory of existingand potential sites for long-term,on-site research collaborations toaddress infectious disease problemsof regional importance. The inven-tory should evaluate:
- How the site might fill geo-graphical and disease-specificresearch gaps
- The site’s potential as a centerfor research training
- Opportunities to engage multi-ple partners, including in-country partners (e.g., publichealth agencies and universities)and U.S. agency partners (e.g., NIH and DoD)
- Opportunities to leverageresources and ensure sustainability
• Create International EmergingInfections Programs (IEIPs), usingthe information from the inventorydescribed above. (See also PriorityArea 6.)
Conduct Research on Vector-borne and Zoonotic Diseases
• Support the development of field-friendly diagnostic tests for thedetection of zoonotic and vector-borne disease, as well as new meth-ods for animal and vector control.
• Support research on the epidemiol-ogy, ecology, and pathogenesis ofvectorborne and zoonotic diseasesof current international concern,including malaria, West Nile fever,dengue fever, Nipah virus ence-phalitis, rabies, Q fever, leishmania-sis, typhus, plague, and Chagas dis-ease.
• Search for the animal or insectreservoirs of Ebola and Marburghemorrhagic fevers, workingthrough the CDC-based WHO Col-laborating Centre for Viral Hemor-rhagic Fevers and collaboratingwith the South African NationalInstitute of Virology and other part-ners.
• Investigate the relationship betweenenvironmental conditions and theemergence of zoonotic and vector-borne diseases.

40 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Conduct Vaccine Research
• Encourage and support the devel-opment and evaluation of vaccinesagainst diseases of global healthimportance (Boxes 17 and 18).
• Support research on ways todecrease the cost of expensive vac-cines like conjugate Haemophilusinfluenzae type b and pneumococ-cal vaccines in developing countries(e.g., administering them less fre-quently or in lower doses).
• Help define the epidemiology andpublic health burden (illness, mor-tality, and cost) of vaccine-prevent-able diseases in developing coun-tries, and monitor the decliningburden of disease associated withwidespread vaccination. (See alsothe next section.)
Conduct Research in Supportof Global Initiatives for Disease Control
• Encourage and support basicresearch to improve our under-standing of the genetics, physiology,and pathogenesis of parasites, bac-teria, and viruses that cause illness-es targeted by global initiatives fordisease control.
Box 17
CDC’s Role in the Development of Vaccines Against Diseases of Global Importance
CDC supports the vaccine development goals of the Global Alliance forVaccines and Immunization (GAVI), the International AIDS Vaccine Ini-tiative, the DHHS Blueprint for TB Vaccine Development, and the Malar-ia Vaccine Initiative. Over the next 5 years, CDC will work with NIH,FDA, USAID, DoD, and many other public and private partners to helpdevelop:
• A multistage vaccine against malaria, as part of the Malaria VaccineInitiative, funded by the Bill and Melinda Gates Children's VaccineProgram
• A DNA-based vaccine against HIV/AIDS, in collaboration with theEmory Vaccine Center in Atlanta, Georgia
• Strain-specific vaccines against dengue and dengue hemorrhagic fever,in collaboration with Mahidol University in Salaya, Nakhonpathom,Thailand
• Conjugate vaccines against meningococcal meningitis group A, in col-laboration with WHO and the Bill and Melinda Gates Children's Vac-cine Program
• An Ebola vaccine, in collaboration with NIH
• Third generation vaccines against Streptococcus pneumoniae usingproteins common to all pneumococcal serotypes. (Second generationconjugate vaccines are currently under evaluation [see Box 18].)
CDC vaccine researcher working in a biosafety level 4
(BSL-4) containment facility. BSL-4 laboratories are usedfor work on infectious agents for which there are no cur-rent vaccines or treatments (e.g., Ebola virus).

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 41
• Help develop and evaluate
- Tools and strategies to preventtransmission of TB, malaria, andHIV/AIDS
- Treatments for drug-resistantcases of TB, malaria, andHIV/AIDS
- Improved methods for the detec-tion of TB, HIV/AIDS-relatedopportunistic infections, andearly-stage HIV infections
• Assess the impact of coinfectionwith HIV and malaria and withHIV and TB on disease controlefforts.
Conduct Research on Food-borne and Waterborne Diseases
• Evaluate diagnostic strategies forfoodborne and waterborne infec-tions that are common in develop-ing countries, but for which currentdiagnostic procedures are slow,expensive, or difficult.
• Conduct targeted research studiesin sentinel IEIP sites (page 53) todetermine the sources of, and riskfactors for, specific foodborne andwaterborne infections so thatappropriate prevention measurescan be developed.
• In collaboration with WHO andothers, assess the efficacy, safety,and utility of vaccination to preventselected foodborne and waterborneinfections (e.g., typhoid fever) incombination with other preventionstrategies. (See also Conduct Vac-cine Research.)
Box 18
CDC’s Role in the Evaluation of Vaccines AgainstDiseases of Global Importance
Over the next 5 years, CDC will work with many different partners tohelp implement:
• Phase III trials in Thailand of an HIV vaccine based on the glycopro-tein-20 antigen developed by the VaxGen company
• Studies to evaluate the effectiveness of 7-valent pneumoccocal conju-gate vaccines on
- Herd immunity among Native American communities that havehigh rates of invasive disease. This is a phase III, cluster-randomizedtrial of conjugate pneumococcal vaccine conducted in collaborationwith Johns Hopkins School of Public Health.
- Nasopharyngeal carriage of pneumococci in Alaska
- Invasive pneumococcal disease throughout the United States, usingthe Active Bacterial Core Surveillance (ABCs) system.
• Phase III trial in the Gambia of a 9-valent conjugate pneumococcalvaccine against all-cause mortality and acute-respiratory-infection-specific mortality, conducted in collaboration with the MedicalResearch Council-Gambia, USAID, NIH, the Bill and Melinda GatesChildren’s Vaccine Program, and WHO’s Vaccine Development, Vac-cines and Biologicals program.
• USAID-supported Phase I trials of two vaccines against Schistosomia-sis mansoni, conducted by the Schistosome Vaccine Development Project, a partnership involving the Government of Egypt, CDC,NIH/NIAID, NAMRU-3, academic centers, and private industry.
• A multisite rotavirus vaccine trial in Southeast Asian countries using anattenuated human rotavirus vaccine produced in India.

42 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Conduct Research on Diseasesof Pregnant Women and Newborns
• Develop point-of-care diagnosticmethods suitable for use in prenataland obstetric healthcare settings indeveloping countries and providequality assurance programs fortheir use.
• Field test new treatments and pre-vention measures, such as
- Drug combinations for the treat-ment or prophylaxis of malariain infants and in pregnantwomen, for use in areas in whichchloroquine-resistance is com-mon.
- Simple and inexpensive regimensfor the treatment and preventionof HIV/AIDs that can be admin-istered to mothers and babiesduring labor and the first weekof life.
• Explore ways to extend the benefitsof intrapartum or neonatal prophy-laxis (e.g., for prevention ofHIV/AIDS and hepatitis C infec-tion) to pregnant women with littleor no prenatal care.
• Explore the effectiveness of perina-tal application of topical antimicro-bial agents in preventing neonatalsepsis and tetanus.
• Assess the relationship betweenparticular maternal infections andlow birthweight or preterm babies.
Conduct Research on Antimicrobial Resistance
• Encourage and support the devel-opment of drug susceptibility testsand surveillance systems to detectemerging resistance problems.
• Evaluate the impact of new vac-cines (such as the conjugate pneu-mococcal vaccines) on the controlof antimicrobial resistance andinfection. (See also Conduct Vac-cine Research.)
• Determine how disease preventionprograms that include mass chemo-therapeutic treatments can be opti-mized to minimize potential for theemergence of drug resistance.Examples include the use of prazi-quantel to prevent schistosomiasis,albendazole to prevent lymphaticfilariasis, ivermectin to preventonchocerchiasis, azithromycin toprevent trachoma, trimethoprim-sulfamethoxazole to prevent AIDS-associated opportunistic infections,and nevirapine or zidovudine toprevent mother-to-child transmis-sion of HIV/AIDS.
• Encourage efforts by WHO andother partners to
- Evaluate the quality of commer-cially available antibiotic stocksand determine whether low-potency stocks are hastening theemergence of drug-resistantstrains of pneumococci, Myco-bacterium tuberculosis, Plas-modium spp., Neisseria gonor-rhoeae, or other pathogens.
- Determine whether antibioticspurchased over the counter indeveloping countries (and oftenused in subtherapeutic doses) arehastening the emergence of drugresistance.
FDA supports these efforts.
Conduct Research on Healthcare-Acquired (Nosocomial) Infections
• Develop methods for identifyingnosocomial infections and reducingtheir transmission in hospitals withlimited resources for infection con-trol.
• Provide technical assistance to hos-pital staff in assessing risk factorsfor acquiring
- Mycobacterium tuberculosis(e.g., transmitted from patientsto health care workers or toother patients).
- Nosocomial respiratory andenteric infections (e.g., inade-quate barrier nursing practices)
- Nosocomial bloodborne infec-tions (e.g., re-use of medicaldevices or surgical equipment)

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 43
Conduct Research on Infectious Causes of Chronic Diseases
• Conduct research on infectiousagents of international importancethat cause or may cause chronic dis-eases (e.g., hepatitis B and C virus-es and hepatocellular carcinoma,Helicobacter pylori and peptic ulcerdisease or gastric carcinoma,Chlamydia pneumoniae and car-diovascular disease, and humanpapillomaviruses and cervical can-cer)
Conduct Research on SexuallyTransmitted Diseases
• Study the contribution of herpessimplex virus type 2 infection andother genital ulcer diseases on HIVtransmission, and devise appropri-ate intervention strategies.
• Develop more standardized diag-nostic reagents and assays forsyphilis to enhance the capacity tocontrol neonatal syphilis world-wide.
• Monitor the development of antimi-crobial resistance among strains ofChlamydia trachomatis and deviseappropriate alternative treatments.

44 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Priority Area 4: Application of Proven Public Health Tools
Another major priority for CDC isto translate research innovations
into practical public health tools andensure that they are disseminatedwidely and rapidly for the benefit ofpeople all over the world. Examplesof public health tools that have had amajor impact on global infectious dis-ease control are antibiotics, childhoodvaccines, oral rehydration therapy,and vitamin supplements.
There is often a long delay betweenthe development of a new publichealth tool and its widespread imple-mentation. A country may lack themeans to buy a new medical productor it may lack a public health deliverysystem and trained workers to admin-ister it. There may be low demand,because the public is not informedabout a new drug or vaccine, or lowpolitical interest, because the nationalgovernment is not convinced that thedrug or vaccine will be cost-effective.
CDC can use its experience in dis-ease surveillance to demonstrate thevalue of public health tools to min-istries of health and finance and to thepublic, using pilot studies, demonstra-tion projects, and health educationcampaigns (Box 19). For example,CDC will continue to work withUSAID, WHO, and other partners todemonstrate that mechanisms for theprevention or control of malaria (via
vector control, chemotherapy,and insecticide-treated bed-nets) are ready for national orregional implementation,pending the availability ofresources and political com-mitment (see Priority Area 5).CDC can also help develop-ment agencies, NGOs, andother partners address prob-lems related to public healthtraining and to drug or vac-cine delivery (see also PriorityArea 6).
As part of the global strategy,CDC will intensify efforts tocouple applied research withresearch on ways to promote the useof newly developed tools for diseasecontrol (“implementation research”).CDC will help identify the most effec-tive tools and actively encourage theirinternational use, applying expertiseand resources in laboratory research,public health policy, program manage-ment, and health communications toovercome scientific, financial, and cul-tural barriers.
Examples of new tools with thepotential for significant worldwideimpact include point-of-use disinfec-tion and safe water storage to preventwaterborne diseases; auto-disable(one-use) syringes to prevent blood-borne transmission of hepatitis B andC viruses and HIV; and diethylcarba-mazine and albendazole therapy toeliminate lymphatic filariasis.
Bednets protect children from malaria. Nightly use ofinsecticide-impregnated bednets13 reduces childhoodmortality by 20–30%, and use in one village protectschildren in neighboring villages by reducing thenumber of infectious mosquitos. Nevertheless, bed-nets are used by fewer than 10% of persons at risk,due to lack of knowledge, unavailability of bednets,and other logistical constraints.
Objectives for Priority Area 4
Promote Effective Drug Use
• Conduct implementation researchand demonstration projects to pro-mote the use of therapeutic drugssuch as
- Ivermectin to eliminate oncho-cerchiasis in West Africa andCentral America
- Diethylcarbamazine and alben-dazole or mebendazole therapyto eliminate lymphatic filariasisin the Americas
- Single-dose azithromycin toeliminate blinding trachoma inendemic regions in Africa, Mid-dle East, Asia, and CentralAmerica

Box 19
Narrowing the Interval Between the Invention andUse of an Effective Public Health Tool
In the past, the time between the development of a new public health tooland its widespread use was often extremely long. For example, the tetanustoxoid vaccine, developed in 1926 and used to protect soldiers duringWorld War II, was not widely administered to children in industrializedcountries until the 1940s and 1950s, and did not reach high levels of cov-erage in developing countries until the mid-1980s, a 60-year interval.
Today, this gap is narrowing. After the hepatitis B vaccine was licensedin 1981, universal infant hepatitis B vaccination projects were initiated inmany countries, including five U.S.-affiliated Pacific islands where HBVinfection is highly endemic and HBV-induced chronic liver disease is aleading cause of death. After a decade of successful demonstration proj-ects, routine childhood hepatitis B vaccination was recommended by theWorld Health Assembly for all countries. During the 1990s, more than100 countries (including the United States) implemented hepatitis Bimmunization programs, although lack of financing hindered vaccine usein the poorest countries. In 2000, financial assistance for the purchase ofhepatitis B vaccine became available through The Vaccine Fund, and theGlobal Alliance for Vaccines and Immunization (GAVI) targeted hepatitisB vaccine for universal introduction into developing countries by 2007.
The history of the hepatitis B vaccine provides a good example of howthe gap in time between introduction and widespread use of a new pub-lic health tool can be shortened through strategic planning, a rapidsequence of efficacy studies and demonstration projects, active advocacyand funding. As future vaccines and other public health innovations aredeveloped, it should be possible to narrow the gap further. CDC can playan important role in this area.
A man being immunized against hep-
atitis B virus. Expanded use of thehepatitis B vaccine will decrease mor-tality from cirrhosis, liver failure, andhepatocellular carcinoma, which isthe 4th leading cause of cancer deathworldwide.
Adapted from: Centers for Disease Control and
Prevention. Preventing emerging infectious dis-
eases: Addressing the issue of vaccine develop-
ment and use. Atlanta, GA: U.S. Department of
Health and Human Services, 2001.
Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 45
- Single-dose nevirapine to pre-vent perinatal HIV transmission.(See also Priority Area 5.)
- Praziquantel to treat schistoso-miasis
• Promote the widespread use of thedirectly observed therapy short-course strategy (DOTS) to treat TB.(See also Priority Area 5.)
Improve Immunization
• Use CDC resources to strengthenroutine immunization services andto encourage the introduction ofnew and underutilized vaccines,including vaccines against hepatitisB, yellow fever, Haemophilus in-fluenzae type b, and other child-hood diseases. (See also PriorityArea 5.)
Promote the Use of ProvenDisease Prevention Strategies
• Work with ministries of health andPAHO to encourage the adoptionof vector control measures to elim-inate Chagas disease from CentralAmerica and reduce morbidity andmortality from dengue and denguehemorrhagic fever (http://www.cdc.gov/ncidod/dpd/parasites/chagasdisease and http://www.cdc. gov/ncidod/dvbid/dengue).
• Work with private and public sec-tor partners to promote widespreadimplementation of CDC’s SafeWater System, which uses point-of-use disinfection and safe water stor-age to prevent cholera, dysentery,and other waterborne diseases (Box20; http://www.cdc.gov/safewater).

Box 20
CDC’s Safe Water System
46 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
In the future, the elements of the Safe Water Systemmay also be used to promote:
• Safe preparation of foods and beverages by streetvendors
• Safe preparation of medications, such as oral rehy-dration solutions to treat cholera
• Safe preparation of formula for use by HIV-infectedwomen who choose not to breast-feed their infants
• Handwashing and improvements in hygiene
• The addition of nutritional supplements to drinkingwater
In the poorest, least industrialized nations, diarrhealdiseases caused by contaminated food and water remaina leading cause of death in childhood. Many of thesedeaths could be prevented by simple sanitation meas-ures.
With assistance from ministries of health, fundingfrom USAID and Rotary International, and specialexpertise from nongovernmental organizations and theprivate sector, CDC has developed a sustainable way toimprove the safety of household drinking water. Thecomponents of CDC's sate water system, as implement-ed in pilot projects in Zambia, include
• Water disinfection. Population Services International(PSI) has marketed a locally produced disinfectantsolution for water treatment (CLORIN) to commu-nities in the southern, eastern, and western regions ofZambia. A CDC case-control study documented a65% reduction of risk of cholera in Zambian house-holds that use CLORIN.
• Safe storage of water. CDC, the Procter and GambleCompany, and Rotary International have con-tributed to the design of a narrow-mouthed vessel forsafe storage of water. The mold for the new vesselwas shipped to South Africa in January 2000, wherevessels have been produced for use in Zambia,Madagascar, Kenya, Côte d’Ivoire, and Pakistan.
• Social marketing. PSI has trained public health work-ers in Lusaka, Kitwe, and Ndola, Zambia, on how toinvolve their communities in the safe-water effort.
USAID has increased funding for the safe water projectin Zambia to permit nationwide coverage within thenext few years, and the CARE/CDC Health Initiative isfunding similar projects in western Kenya and inAntananarivo, Madagascar. Each CARE/CDC HealthInitiative project will target a population of 200,000people and combine the methods of the Zambian proj-ect with the community organizing techniques of CARE.
A safe water storage vessel employed by participants in an
ongoing Safe Water System implementation project in Homa
Bay, Kenya, initiated in October 2000 in collaboration with
CARE Kenya. The vessel was designed to eliminate a majorsource of diarrheal disease contamination that results whenhands, cups, ladles, or other objects are dipped into openbuckets to remove water for drinking. Because the local popu-lation in Homa Bay preferred to use vessels made of clayrather than plastic, CDC and CARE Kenya incorporated a nar-row mouth, lid, and spigot into traditional clay pots to ensuresafe water storage. The use of plastic vessels with similar char-acteristics, in combination with water disinfectants, hasreduced diarrheal diseases by 30–50% in communities in Zam-bia, Pakistan, and Bolivia.14
Photographer: Bobbie Person, Office of Health Communication, National Center
for Infectious Diseases, CDC

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 47
Disseminate Diagnostic Tests
• Work through the WHO Collabo-rating Centre laboratory networkto provide proven diagnosticreagents for the detection of endem-ic diseases to national public healthlaboratories and regional surveil-lance networks. (See Priority Area1.)
• Work with WHO and donor agen-cies to provide national publichealth laboratories with state-of-the-art laboratory tests that measureantimicrobial resistance in Myco-bacterium tuberculosis and othercommon bacterial pathogens, aswell as in malaria parasites and in the AIDS virus. (See Priority Area 5.)
• Work with ministries of health totransfer technology for molecularsubtyping of common bacterialpathogens (e.g., PulseNet tech-niques; page 36) to national publichealth laboratories for use in detect-ing outbreaks of foodborne dis-eases).
• Work with WHO and ministries ofhealth in central African countriesto provide training in hospital bar-rier nursing practices that preventnosocomial spread of viral hemor-rhagic fevers like Ebola and Mar-burg.
• Continue to support the Safe injec-tion Global Network (SIGN) andwork with development agenciesand other partners to promote safeinjection practices to prevent thespread of hepatitis B and C,HIV/AIDS, and other bloodbornediseases.
• Work with the Roll Back Malariapartnership to promote the use ofinsecticide-impregnated bednets forthe prevention of malaria and othermosquitoborne diseases. (See Prior-ity Area 5.)
• Work with ministries of health andWHO to provide public health edu-cation and mobilize communities touse proven public health tools.
Use Surveillance Data ToDirect Public Health Policy
• Work with ministries of health andministries of finance, WHO, andNGOs to
- Conduct disease surveillance toassess national public healthneeds and recommend specificpublic health tools to addressthem.
- Demonstrate the use of specificsurveillance methods for detect-ing outbreaks, for evaluatingpublic health programs, and fordriving public health decision-making.
• Work with global partners to evalu-ate the progress of global initiativesto combat malaria, TB, AIDS, andvaccine-preventable diseases. (SeePriority Area 5.)

48 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Dr. Gro Bruntland, Director-General of WHO, has said that
“solutions, like problems, have to beglobal in scope.” In accord with thisidea, WHO is helping to coordinatemajor global initiatives to reducedeaths from malaria, TB, andHIV/AIDS—diseases that contributeto poverty and economic stagnation.This approach was endorsed by theGroup of Eight Industrialized Nationsat the Okinawa summit in July 2000.WHO is also helping to coordinateglobal initiatives to increase develop-ing-country access to vaccines againstacute respiratory diseases, yellowfever, hepatitis B, and other diseases,through the Global Alliance for Vac-cines and Immunization (GAVI;http://www.vaccinealliance.org).
Although these global initiativeshave clearly stated goals and are sup-ported by multiple private and publicsector partners (Box 6), the details of
Priority Area 5: Global Initiatives for Disease Control
Children from villages hard-hit by AIDS. Thirteen million children in sub-Saharan Africa have lost one or both parents to AIDS, and the number isexpected to reach 40 million by 2010.15 The number of AIDS orphans is alsogrowing in Asia and Latin America.
Global efforts are underway to help these children and prevent furtherdevastation from HIV/AIDS and other infectious diseases. These global ini-tiatives involve complex alliances among public and private groups, healthand trade experts, and national and international donor organizations.
Photographer: Bobbie Person, Office of Health Communication, National Center for Infectious
Diseases, CDC
their implementation are still underdiscussion. Previous efforts to eradi-cate malaria by using a narrowapproach to vector control ended infailure. Because no proven vaccinesare yet available against malaria, TB,or AIDS, “one-shot” solutions are notfeasible, and it will be necessary toemploy multiple control strategies,including behavioral interventionsthat require a high degree of coopera-tion and trust in affected communities.The incidence of TB, HIV/AIDS, andacute respiratory infections is high inpoor, war-torn, or post-Communistcountries in which public health infra-structures have deteriorated. More-over, emerging drug resistance compli-cates the treatment and control ofeach of these diseases.
A new priority for CDC will be to ele-vate the level of its participation in these and other global initiatives
(Box 6). CDC and its partners will alsoconsult on future international priori-ties for disease control, elimination,and eradication efforts—as well as forantimicrobial resistance monitoringand pandemic influenza preparednessplanning—and help evaluate progressthrough the collection and analysis ofdisease surveillance data.
Increased participation in globalhealth initiatives will require long-term partnerships with host countries,as well as improved coordination withpublic health partners throughout theworld. CDC will build on its strengthsin disease surveillance, laboratory sci-ence, and program evaluation to assistdevelopment agencies, internationalorganizations, NGOs, and develop-ment banks that support internationalprograms to strengthen healthcare sys-tems and control disease. As a partnerin the Global AIDS alliance (Boxes 6

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 49
Box 21
The Global AIDS Program
Thirty-six million people worldwide have been infected with HIV, thevirus that causes AIDS, and more than 21.8 million have died. Eighty-five percent of all AIDS deaths have occurred in the countries of sub-Saharan Africa. In at least five of these countries, more than 20% ofadults are HIV-positive. Infection rates are also climbing in parts of Asia,Latin America, the Caribbean, and the former Soviet Union countriesand Eastern Europe. Only a concerted global effort coordinated byWHO and led by the United States and other industrialized countries canstop this pandemic.
Through the Global AIDS Program (GAP), CDC is working withUSAID and other DHHS agencies to assist ministries of health. In 2001,the program targeted 17 of the hardest-hit African countries (Angola,Botswana, Côte d’Ivoire, the Democratic Republic of the Congo,Ethiopia, Kenya, Malawi, Mozambique, Namibia, Nigeria, Rwanda,Senegal, South Africa, Tanzania, Uganda, Zambia, and Zimbabwe), aswell as India, Brazil, Cambodia, Guyana, Haiti, Thailand, and Vietnam.GAP’s mission is to implement the U.S. Leadership and Investment forFighting an Epidemic (LIFE) Initiative, which is the U.S. contribution tothe International Partnership Against AIDS in Africa and to AIDS effortson other continents.
The goals of the Global AIDS program are to
• Reduce HIV transmission through primary prevention of sexual,mother-to-child, and bloodborne transmission
• Improve community and home-based care and treatment ofHIV/AIDS, sexually transmitted infections, and opportunisticinfections
• Strengthen national capacities to collect and use surveillance dataand manage national HIV/AIDS programs
Additional information on the Global AIDS Program is available athttp://www.cdc.gov/nchstp/od/gap
and 21), for example, CDC has a special opportunity to work withUNAIDS and USAID to implementHIV/AIDS control programs on allcontinents (http://www.unaids.org/ africapartnership/files/mrpretoria.doc).As a partner in Roll Back Malaria(http://www.rbm.who.int), Stop TB(http://www.stoptb.org), and GAVI,CDC can contribute to the SharedAgenda for Health in the Americas(http://wbln0018.worldbank.org/external/lac/lac.nsf)16 developed by PAHO,the Inter-American DevelopmentBank, and the World Bank.
Increased participation in globalhealth initiatives also will requireadditional staff to work on projectsoverseas, as well as to provide diag-nostic support from CDC laboratoriesin the United States. Full participationin GAVI, for example, will requireincreased programmatic support andtechnical expertise in acute respiratorydiseases, yellow fever, hepatitis B, andmeningococcal meningitis. Thereremains a shortage of U.S. and worldexpertise in many infectious diseaseareas. (See also Priority Area 6.)
CDC staff will also continue towork with ministries of health, WHO,PAHO, USAID, and other partnerson disease elimination or eradicationcampaigns. In addition, CDC staffwill help further efforts to reduce ill-ness and death from acute respiratorydiseases and diarrheal diseases,

50 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
which—in addition to HIV/AIDS, TB,and malaria—are the leading infec-tious causes of death, worldwide.CDC will also continue to conductapplied research to improve ourunderstanding of the genetics, physiol-ogy, and pathogenesis of microbesthat cause illnesses targeted by globalinitiatives for disease control. (See Pri-ority Area 3.)
Objectives for Priority Area 5
Establish a Solid Foundationfor Global Initiatives
• Expand the cohort of public healthprofessionals at CDC who haveinternational expertise and can pro-vide support for global initiatives tocombat infectious diseases. (Seealso Priority Area 6)
• Help suggest international priori-ties for current and future globalinitiatives for disease control.Future initiatives might includeantimicrobial resistance monitor-ing, pandemic influenza prepared-ness planning, and campaigns tocontrol or eliminate measles, lym-phatic filariasis, onchocerchiasis,trachoma, rubella, neonatal teta-nus, or hepatitis B.
• Provide technical assistance tonational health authorities in publichealth management of diseases tar-geted by global health initiatives,working through the SustainableManagement Development Pro-gram and other mechanisms. In
some countries this will includeintegrating specialized HIV, TB, andSTD surveillance programs intonational surveillance and laboratoryservice systems for infectious dis-eases.
• Improve coordination among CDCpersonnel who work overseas in thesame country or region.
Enhance Support for DiseaseControl, Elimination, and Erad-ication Programs
• Help complete the eradication ofpolio by 2005. The global effort toeradicate polio is led by WHO, inpartnership with an internationalcoalition that includes CDC, RotaryInternational, UNICEF, and thegovernments of many countries(http://www.cdc.gov/nip/global).The WHO Global Polio Labora-tory Network (Box 7), which usesmolecular techniques to determinewhether wild-type polio is circulat-ing in areas undergoing eradicationefforts, should be expanded toinclude monitoring for other vac-cine-preventable diseases, such asmeasles and rubella.
• Help complete the eradication ofdracunculiasis, working in partner-ship with the Carter Center’s Glob-al 2000 Program, UNICEF, WHO,and other groups (http://www.cdc.gov/ncidod/dpd/parasites/guineaworm and http://www.carter-center.org/guineaworm.html).
• Work with PAHO to complete theelimination of indigenous (i.e., non-
imported) cases of measles in theAmericas, and work with WHO,UNICEF, the UN Foundation,USAID, the American Red Cross,the International Federation of RedCross and Red Crescent Societies(IFRC), and other partners toreduce by 50% by 2005 the nearly900,000 annual measles deathsworldwide.17
Participate in the Roll BackMalaria Initiative
• Contribute to Roll Back Malaria(RBM; http://www.rbm.who.int)through full endorsement andactive promotion of RBM strategicsin malaria-endemic countries insub-Saharan Africa, Southeast Asia,and the Americas. Although RBMstrategies vary by region and bylocal malaria transmission dynam-ics, 90% of the world’s malaria is insub-Saharan Africa, where thestrategies for malaria preventionand control include
- Prompt effective case manage-ment of malaria illness
- Prevention of malaria and itsconsequences in pregnancy,through prophylaxis or preven-tive intermittent treatment regi-mens with an effective anti-malarial drug
- Widespread use of insecticide-treated bednets, particularly byyoung children and pregnantwomen
- Prompt recognition and manage-ment of malaria epidemics

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 51
• Conduct operations research on
- Antimalarial drug efficacy andthe management and preventionof antimalarial drug resistance
- Malaria prevention in pregnancy
- Transmission reduction throughthe use of insecticide-treated bed-nets and other strategies
- Malaria assessment in complexemergencies, such as outbreaksthat occur among refugees oroutbreaks that occur after hurri-canes or other natural disasters
- Malaria diagnostics
- Social attitudes and practicesthat facilitate or hinder the effec-tiveness of malaria control pro-grams
- Malaria surveillance, monitor-ing, and evaluation strategies
• Provide technical assistance to theAfrican Integrated Malaria Initia-tive (http://www.usaid.gov/regions/ afr/abic/sddev/sddspr96/sddspr96.htm; see also Appendix A), aUSAID-sponsored initiative thatenhances integrated malaria treat-ment and prevention in Kenya,Malawi, Zambia, and Benin by pro-moting the use of interventions inthe home (e.g., insecticide-impreg-nated bednets), in healthcare facili-ties (e.g., chemoprophylaxis), andamong pregnant women (e.g., pro-tective intermittent chloroquinetherapy, as recommended by theUSAID Safe Motherhood Initiative).During 2001, the African Integrat-ed Malaria Initiative will be extend-
ed to the Democratic Republic ofthe Congo, Nigeria, Senegal, andUganda.
• Assist ministries of health in malar-ia control efforts and in the moni-toring and evaluation of antimalar-ial drug efficacy. CDC is currentlyworking on national malaria con-trol programs in Kenya, Tanzania,Peru, and Nepal.
Strengthen the Stop TB Program
• Contribute to Stop TB (http://www. stoptb.org) by
- Assigning an epidemiologist toWHO’s Stop TB secretariat
- Providing technical assistance tofacilitate the use of the directlyobserved therapy short-coursestrategy (DOTS) for TB. (Seealso Priority Area 4)
- Strengthening TB treatment pro-grams in LIFE Initiative/GlobalAIDS Program countries (seebelow)
- Supporting demonstration proj-ects on the medical managementof drug-resistant TB
- Providing technical assistance toimprove hospital TB control anddetect hospital and communityoutbreaks in communities withhigh HIV prevalence
- Assigning a medical officer to theInternational Union Against TBand Lung Diseases (IUATLD) totrain a cadre of international TBexperts, as a joint effort withUSAID and WHO
- Providing technical assistanceand laboratory support to imple-ment global antituberculosisdrug resistance surveys
• Consult with ministries of health inRussia, Vietnam, and other coun-tries on training issues related to TBdiagnosis and treatment.
• Conduct operations research on
- TB surveillance, program man-agement, and program evalua-tion strategies
- Multidrug-resistant TB treat-ment approaches and evaluationstrategies
- Treatment strategies for latentTB among persons with HIVinfection
- Factors that improve adherenceto antituberculosis therapy
- New diagnostic methods, drugs,and vaccine for TB
Expand the LIFE Initiative andOther International Efforts ToAddress HIV/AIDS
CDC will work with foreign ministriesof health and public and private sectorpartners in countries targeted by theLIFE Initiative/Global AIDS Program(Boxes 6 and 21; http://www.cdc.gov/nchstp/od/gap) to
• Prevent primary transmission ofHIV by
- Expanding voluntary counselingand testing programs for youthand other vulnerable popula-tions

52 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
- Building large-scale programs toreduce mother-to-child transmis-sion
- Strengthening programs toreduce bloodborne HIV trans-mission
- Strengthening medical manage-ment of sexually transmittedinfections (STIs)
- Supporting and strengtheningnational education and mobi-lization efforts for disease pre-vention
• Improve community and home-based care and treatment by
- Expanding and strengtheningTB prevention and care
- Enhancing care and treatment ofHIV/AIDS and AIDS-relatedopportunistic infections
- Exploring the innovative use ofantiretroviral therapy
• Build public health and medicalinfrastructure by
- Expanding and strengtheningsurveillance for HIV, STIs, andTB
- Providing laboratory support fordiagnosis and surveillance ofHIV, STIs, TB, and opportunis-tic infections, as well as for HIVscreening of blood supplies
- Expanding and strengtheningpublic health information sys-tems
- Providing training in managingand implementing HIV treat-ment and prevention programs(see also page 55).
- Enhancing evaluation of HIV/ AIDS prevention and care pro-grams.
Support Global Vaccine Initiatives
• Help GAVI partners (http://www.vaccinealliance.org/) develop andimplement strategies to strengthenroutine immunization services andmonitor their effectiveness.
•Provide assistance to GAVI inassessing the burden of hepatitis B,yellow fever, Haemophilus influen-zae type b, pneumococcus, rota-virus, meningococcus A, measles,and congenital rubella syndrome indeveloping countries and use thisinformation to design, implement,and evaluate immunization pro-grams against these infections.
• Support efforts by GAVI partners—including pharmaceutical compa-nies, foundations and developmentbanks—to develop and evaluatenew vaccines that are needed indeveloping countries, and to pro-mote their availability. (See also Pri-ority 3.)

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 53
CDC’s growing visibility as aninternational outbreak consultant
has also led to increased participationin efforts to build global public healthcapacity. Although CDC is not a devel-opment agency, CDC has traditionallyassisted USAID with the public healthand research components of develop-ment projects (Box 22) and has con-sulted with private foundations anddevelopment banks on efforts tostrengthen public health infrastruc-tures (Box 23). Over the past decade,CDC has also helped strengthenhealthcare systems in developingcountries, working with hospitaladministrators and physicians toimprove infection control practicesand ensure safe blood supplies. CDChas also managed overseas field sta-tions that facilitate on-site collabora-tive research on diseases of regionaland global importance (Box 10). Inaddition, several foreign scientistsenroll each year in CDC’s Epidemic
Priority Area 6: Public Health Training and Capacity Building
Presentation of certificates: Workshop on HIV/AIDS Epidemi-
ology, Surveillance, and Prevention, May 2000, Nha Trang
City, Khanh Hoa Province, Vietnam. Since Vietnam and UnitedStates renewed diplomatic relations, Vietnamese and U.S. sci-entists and public health workers have collaborated on work-shops, training courses, and research projects that buildnational capacity to detect and prevent HIV/AIDS, TB, malaria,typhoid fever, influenza, hospital-acquired infections, plague,and dengue and dengue hemorrhagic fever.
Photographer: Nguyen Thi Thu Hong, HHS/CDC/Hanoi
Intelligence Service and the EmergingInfectious Disease Laboratory Fellow-ship Program, which is a joint effortbetween CDC and the Association ofPublic Health Laboratories (APHL).
In recent years, in the aftermath ofoutbreaks and other infectious diseasecrises, CDC has responded to requestsfrom more than 80 foreign govern-ments for epidemiologic, laboratory,or research assistance to ensure pre-paredness for future emergencies.However, most of these efforts—which included training courses,research collaborations, program eval-uations, health education campaigns,and the provision of laboratory refer-ence support—were limited in scopeand duration and were not integratedinto a larger effort to build publichealth capacity.
As part of the global strategy, CDCwill propose the establishment of aseries of International Emerging Infec-tions Programs (IEIPs) in developing
countries—centers of excellence thatwill integrate disease surveillance,applied research, prevention, and con-trol activities. Each site will representa partnership between a ministry ofhealth and CDC, with additional part-nerships involving local Field Epidemi-ology Training Programs (FETPs) andone or more local universities or med-ical research institutes. The IEIP siteswill build on existing CDC overseasactivities to strengthen national publichealth capacity and provide hands-ontraining in public health. Over time,they may have a regional as well as anational impact on health.
The IEIPs will be broad-based pub-lic health collaborations between theministry of health of the host countryand CDC, with both parties contribut-ing resources and reaching agreementon the priorities of the program. Eachsite will be built on existing CDC fieldcapacity in that country. Some IEIPsmay be based at research institutions

54 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
where CDC has long-standing collab-orations. Others may be based at CDCfield stations or adjacent to other U.S.institutions abroad, such as NIH’sTropical Medicine Research Centersor DoD’s overseas laboratories. Eachsite will maintain close ties with WHOcountry and regional offices, and, ifpossible, will collaborate with one ofthe Field Epidemiology Training Pro-grams (FETPs) that CDC has helpedestablish in more than 16 countries(Box 24).
The IEIPs will be modeled in parton the U.S. Emerging Infections Pro-gram (EIP; http://www.cdc.gov/ncidod/osr/EIP.htm) whose nine sitesconduct population-based surveil-lance, provide emergency outbreakassistance, invest in cutting-edgeresearch, and address new problemswhenever they arise. Because the EIPsites combine specialized epidemiolog-ic and laboratory expertise, they areable to go beyond the routine func-tions of local health departments toaddress important issues in infectiousdiseases and public health. For exam-ple, when “mad cow disease” wasreported in the United Kingdom in1996, the EIP surveillance sites wereable to reassure the U.S. public withina short time that the disease had notspread to the United States.
Like the domestic EIPs, the Interna-tional EIP sites will perform multiplefunctions, including research onendemic diseases and emergency sur-veillance when a new threat appears.
Box 22
USAID and CDC: Collaboration on Capacity Building
The U.S. Agency for International Development (USAID) and CDC arelongstanding partners in the effort to combat emerging diseases overseas.Twenty years ago, CDC and USAID collaborated with WHO and otherpartners to eradicate smallpox. Today, CDC and USAID are helping erad-icate polio; reduce deaths from malaria, HIV/AIDs, TB, and acute respi-ratory infections; and improve global surveillance for emerging threats.
In many countries, CDC partners with USAID on evaluations of infec-tious disease problems related to wars, famines, or other disasters, as wellas on development projects that involve epidemiologic or diagnosticresearch. CDC also helps implement USAID-supported programs in thefour key areas of USAID’s emerging infectious disease initiative:
• Antimicrobial resistance: Developing and implementing strategies andinterventions for detecting, studying, and containing emerging resist-ance problems.
• TB: Working for a sustainable reduction in the incidence of TB amongkey populations in selected countries through by the introduction ofdirectly observed therapy short-course strategy (DOTS; see Box 6).
• Malaria: Improving the diagnosis and treatment of malaria; promotingeffective preventive strategies; addressing the challenges of malaria inpregnancy; containing malaria outbreaks; responding to malaria dur-ing complex emergencies; slowing the emergence and spread of drug-resistant malaria; and accelerating the development of tools for malar-ia control.
• Disease surveillance and response: Improving public health capacity toobtain and use good quality data for disease surveillance and effectiveresponse to infectious diseases.
As part of the global strategy, CDC will intensify its efforts to workwith USAID to develop mutually reinforcing ways of working together atthe country level to maximize the impact of U.S. investments in globalhealth.

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 55
They will also provide disease surveil-lance data to ministries of health andfinance to help assess the burden ofspecific diseases and evaluate the cost-effectiveness of national public healthprograms. Also like the EIPs, the IEIPswill incorporate preexisting sites (e.g.,U.S. institutions, public health agen-cies, research institutions, and non-governmental organizations); use thesites in an integrated fashion; andestablish an international steeringcommittee to provide guidance forcore projects conducted at all of theIEIP network sites. Areas in whichIEIP sites might play an especiallyimportant role are in surveillance fordrug-resistant forms of malaria, TB,pneumonia, and dysentery. All of thesites will be linked by electronic com-munications to keep health expertsaround the world in close contact withone another.
The long-term goal of the IEIPs willbe to develop sustainable, in-countrycapacity for disease surveillance, out-break investigation, and research ondiseases of regional or global impor-tance by fostering the next generationof international public health leaders(Box 16). The implementation of thisgoal will require extensive scientific,human, and financial resources fromboth private and public sources, aswell as sustained efforts over manyyears. However, the costs will be lowin relation to potential benefits, interms of both human health andincreased global prosperity.
Objectives for Priority Area 6
Establish International Emerging Infections Programs (IEIPs)
• Help create International EmergingInfections Programs (IEIPs) that
- Train local scientists and CDCpersonnel
- Provide diagnostic and epidemi-ologic resources when outbreaksoccur
- Serve as platforms for regionalinfectious disease control activi-ties
- Conduct public health researchof global importance
- Disseminate proven health tools
Expand Training in Epidemiology, Public HealthManagement, and LaboratoryDiagnostics
• Increase training opportunities forforeign scientists in epidemiology,public health management, andstate-of-the-art laboratory tech-niques. For example, CDC will pro-vide training in
- PulseNet’s methods for finger-printing strains of foodbornebacteria (page 36)
- Methods for identifying food-borne viruses
- Drug susceptibility testing ofpathogens of public healthimportance
- DPDx, an Internet-based systemto help confirm diagnoses of par-asitic diseases
- International public health man-agement
- Managing and implementingHIV treatment and preventionprograms in Global AIDS Pro-gram countries (see page 52)
• Work through TEPHINET andother mechanisms to provide tech-nical assistance to health authoritiesin countries that are establishing orexpanding national schools of pub-lic health, new Field EpidemiologyTraining Programs (FETPs), newSustainable Management Develop-ment Programs, or the Rocke-feller Foundation-supported PublicHealth Schools Without Walls(PHSWOW). TEPHINET is a pub-lic health network network thatlinks FETP and PHSWOW staff.
• Help increase the number of publichealth workers in developing coun-tries who are trained in vaccinework by
- Encouraging training efforts byforeign governments, founda-tions, and donor organizations(e.g., the WHO public healthtraining project in Lyon, France)
- Incorporating training compo-nents into such projects as theU.S.-India Vaccine Plan, theEgyptian Schistosomiasis Vac-cine Development Project, andthe HIV vaccine trials in Kenyaand Côte D’Ivoire (Box 18)

56 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
- Training national and regionalhealth workers in vaccine pro-gram planning, monitoring, andevaluation as part of GAVI’seffort to improve routine immu-nization services and to intro-duce new and underutilized vac-cines into developing countries
• Provide training opportunities thatincrease international expertise inthe detection and treatment of pre-natal and perinatal infections.
• Expand the cohort of public healthprofessionals at CDC who haveinternational infectious diseaseexpertise, by
Box 23
The World Bank and CDC Sign a Memorandum of Understanding
Infectious diseases are not just a result of, but also acause of, poverty (see Box 8). In recognition of this fact,the World Bank, a leading global development lender,signed a memorandum of understanding with CDC inFebruary 2001, to intensify joint efforts to prevent andcontrol diseases that take a heavy toll in developingcountries.
Under the agreement, CDC and the World Bank willcollaborate on a broad range of global health activities,related to nutrition, maternal and child health, endemicdiseases such as HIV/AIDS, TB, and malaria, publichealth, health surveillance, health policy and statistics,research, and healthcare technology. Over the next year,for example, CDC will transfer technical experts to theWorld Bank to help design, implement, and evaluateprojects to control the spread of malaria in Africa andpromote worldwide use of vaccines against many child-hood diseases.
The memorandum will also facilitate previouslyestablished collaborations between the World Bankand CDC, including an ongoing project to upgrade thesurveillance infrastructure for infectious diseases inArgentina and Brazil, from the local to the nationallevel. That effort includes
• Training public health workers in epidemiology,management, and laboratory science
• Establishing electronic reporting networks and sen-tinel sites for disease surveillance
• Enhancing laboratory capacity
• Strengthening outbreak response
• Instituting measures to prevent the spread of TBand other priority diseases
- Creating an inventory of CDCstaff to identify gaps in interna-tional expertise
- Developing an internationalinfectious disease training pro-gram or seminar series for CDCstaff, in collaboration with pub-lic health and medical schools
- Establishing an exchange pro-gram that enables visiting scien-tists from other countries towork at CDC and vice versa
- Working with the Association ofSchools of Public Health and theAssociation of Teachers of Pre-ventive Medicine to increase the
number of graduate courses thatcover global infectious diseaseissues
• Expand opportunities for trainingin-hospital infection control andclinical surveillance by providing
- Train-the-trainer courses in hos-pital epidemiology
- Technical assistance to hospitalstaff in designing and implement-ing programs to reduce transmis-sion of nosocomial pathogens

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 57
Box 24
Applied Field Epidemiology Training Programs
For more than 20 years, CDC has collaborated withministries of health around the world to establish FieldEpidemiology Training Programs (FETPs) for specialistsin epidemiology. These programs are modeled on theEpidemic Intelligence Service, CDC’s primary appliedepidemiology training program, which was founded in1951. Canada established a field epidemiology trainingprogram in 1975, and Thailand launched one in 1980,in collaboration with CDC and WHO. CDC partnerswho have helped establish other FETPs include theWorld Bank (Brazil), PAHO (a regional FETP in CentralAmerica), and USAID (Egypt, Jordan, Peru, Philippines,and Central America).
CDC has also provided consultants to Public HealthSchools Without Walls (PHSWOW), which helps post-graduate-level public health per-sonnel attain the epidemiologic,managerial and leadership com-petencies required to runincreasingly decentralized healthsystems. The PHSWOWs arefunded by the Rockefeller Foun-dation with technical supportfrom Tulane University. Thefirst PHSWOW was launched inZimbabwe in 1993 at the Uni-versity of Zimbabwe; the sec-ond in Uganda in 1994 at Mak-erere University; and the third inGhana in 1995 at the Universityof Ghana. In 1997, Vietnamstarted a PHSWOW in collabo-ration with the Hanoi School ofPublic Health.
As of 2000, in addition to EIS, there were 27Applied Epidemiology Training Programs, including 20FETPs, 4 PHSWOWs, and 3 other Applied Epidemiol-ogy Training Programs (the European Programme for Intervention Epidemiology Training [EPIET], theWHO Global Health Leadership Officers Programme[GHLOP], and the WHO/AFRO Programme d’Epi-demiologie Pratique [PEP]). Of 19 programs over 4years old, 18 (95%) continue to produce graduates.Thus far, it is estimated that the 27 Applied Epidemiol-ogy Training Programs have trained more than 900international public health leaders in epidemiology andoutbreak investigation. Approximately 420 more arecurrently in training.
0
5
10
15
20
25
30
1950 1955 1960 1965 1970 1975 1980 1985 1990 1995 2000
Year
Num
ber o
f Pro
gram
s
Number of Applied Epidemiology Training Programs 1950–2001.

58 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
- Consultation to USAID andother donor organizations oninfectious disease projects thatbuild infrastructure to improvethe provision of prenatal andperinatal care in developingcountries.
Enhance Availability of Guide-lines and Other Publications
• In collaboration with WHO andinternational experts, draft region-al health care guidelines on thejudicious use of antibiotics, includ-ing antibiotics that are purchased
over-the-counter. Regional healthcare guidelines can be used tomount public health educationcampaigns on antibiotic usage tohelp retard the development ofdrug resistance.
• Provide consultation to ministriesof health in developing nationalguidelines for
- Hospital infection control,including prevention of hospital-acquired pneumonia, TB, HIV/ AIDS, and other nosocomialinfections of local concern.
- Management of exposures tobloodborne pathogens like HIVand hepatitis B and C.
• Disseminate new information oninfectious disease issues throughthe Morbidity and Mortality Week-ly Report (MMWR), the EmergingInfectious Diseases journal, and theCDC website.

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 59
LIST OF BOXES Box 1: Implementation Priorities, 2001-2002
Box 2: Infectious Diseases Do Not Recognize Borders
Box 3: Factors That Facilitate the International Spread of Foodborne Disease
Box 4: International Spread of Antimicrobial Resistance
Box 5: Avian Influenza in Hong Kong
Box 6: Global Health Initiatives
Box 7: The World Health Organization Global Polio Laboratory Network
Box 8: Infectious Diseases and Economic Development
Box 9: International Disease Control Efforts Can Create New Alliances
Box 10: Examples of CDC’s Long-term Research Collaborations Overseas
Box 11: An Outbreak of Leptopirosis Affecting Athletes from 26 CountriesReported by the GeoSentinel Disease Surveillance System
Box 12: Follow-up Activities in the Aftermath of the 1994 Plague Outbreakin India
Box 13: Outbreaks Among Refugees in Kosovo and the Sudan
Box 14: WHO and CDC: Collaboration on International Outbreak Assistance
Box 15: Agricultural Costs of Controlling Zoonotic Diseases Carried byFood Animals
Box 16: A Growing Community of International Public Health Leaders
Box 17: CDC’s Role in the Development of Vaccines Against Diseases ofGlobal Importance
Box 18: CDC’s Role in the Evaluation of Vaccines Against Diseases ofGlobal Importance
Box 19: Narrowing the Interval Between the Invention and Use of an Effective Public Health Tool
Box 20: CDC’s Safe Water System
Box 21: The Global AIDS Program
Box 22: USAID and CDC: Collaboration on Capacity Building
Box 23: The World Bank and CDC Sign a Memorandum of Understanding
Box 24: Applied Field Epidemiology Training Programs

60 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
AFRIMS Armed Forces Research Institute of Medical Science,Bangkok, Thailand
AIDS acquired immunodeficiency syndrome
AIMI African Integrated Malaria Initiative
AMREF African Medical and Research Foundation
APEC Asia-Pacific Economic Cooperation
APHL Association of Public Health Laboratories
ATSDR Agency for Toxic Substances and Disease Registry
BIDS U.S.-Mexico Border Infectious Disease Surveillance system
CAREC Caribbean Epidemiology Center
DoD Department of Defense
DOTS directly observed therapy short-course strategy
DVA Department of Veterans Affairs
ELISA enzyme-linked immunosorbent assay
EPI Expanded Programme on Immunization
EPIET European Programme for Intervention Epidemiology Training
EIP Emerging Infections Program
EWORS Early Warning Outbreak Recognition System
FDA Food and Drug Administration
FETP Field Epidemiology Training Program
GAP Global AIDS Program
GAVI Global Alliance for Vaccines and Immunization
GHLOP WHO Global Health Leadership Officers Programme
HIV human immunodeficiency virus
HIV/AIDS human immunodeficiency virus infection/acquired immunodeficiency syndrome
HFRS hemorrhagic fever with renal syndrome
HPS hantavirus pulmonary syndrome
IFRC International Federation of Red Cross and Red Crescent Societies
IHR International Health Regulations
IPAA International Partnership Against AIDS in Africa
IUATLD International Union Against TB and Lung Diseases
KEMRI Kenya Medical Research Institute
LIFE Leadership and Investment for Fighting an Epidemic initiative
LITS Laboratory Information Tracking System
ACRONYMS

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 61
MERTU/G Medical Entomology Research and Training Unit/Guatemala
NAMRU-2 Naval Medical Research Unit No. 2, Jakarta, Indonesia
NAMRU-3 Naval Medical Research Unit No. 3, Cairo, Egypt
NASA National Aeronautics and Space Agency
NGO nongovernmental organization
NIH National Institutes of Health
NMRCD Naval Medical Research Center Detachment, Lima, Peru
NOAA National Oceanic and Atmospheric Administration
PacNET Pacific Public Health Surveillance Network
PAHO Pan American Health Organization
PEP WHO/AFRO Programme d’Epidemiologie Pratique
PHLIS Public Health Laboratory Information System
PHSWOW Public Health Schools Without Walls
RBM Roll Back Malaria initiative
SIGN Safe Injection Global Network
STD sexually transmitted diseases
STI sexually transmitted infections
TB tuberculosis
TEPHINET Training in Epidemiology and Public Health InterventionsNetwork
UNAIDS Joint United Nations Programme on AIDS
UNESCO United Nations Educational, Scientific, and Cultural Organization
UNICEF United Nations Children’s Fund
USAID United States Agency for International Development
USAMRU-K United States Army Medical Research Unit, Nairobi, Kenya
USDA United States Department of Agriculture
WHO World Health Organization
WHO/AFRO World Health Organization Regional Office for Africa
WHO/EMRO World Health Organization Regional Office for the EasternMediterranean

62 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
APPENDIX AGLOBAL HEALTH WEBSITES
Organization Publication Web AddressCarter Center Guinea Worm Eradication Program http://www.cartercenter.org/guineaworm.html
Center for Strategic and Contagion and Conflict: Health as a http://www.csis.org International Studies Global Security Challenge
Centers for Disease Control and Prevention The HIV/AIDS Collaboration, http://www.hac.or.th/CDC and The Ministry of Public Health Thailand
Centers for Disease Control and Prevention Global Polio Eradication Initiative http://www.cdc.gov/nip/global
Centers for Disease Control and Prevention Guinea Worm Disease Fact Sheet http://www.cdc.gov/ncidod/dpd/parasites/guineaworm
Centers for Disease Control and Prevention Global AIDS Program http://www.cdc.gov/nchstp/od/gap
Centers for Disease Control and Prevention Working with Partners to Improve Global http://www.cdc.gov/ogh/pub/strategy.htmHealth: A Strategy for CDC and ATSDR
Centers for Disease Control and Prevention International Health Data Reference http://www.cdc.gov/nchs/data/ihdrg99.pdfGuide, 1999
Centers for Disease Control and Prevention U.S.-Mexico Border Infectious http://www.r10.tdh.state.tx.us/obh/bids.htmDiseases Surveillance
Centers for Disease Control and Prevention Preventing Emerging Infectious http://www.cdc.gov/ncidod/emergplanDiseases: A Strategy for the 21st Century
Centers for Disease Control and Prevention Biological and ChemicalTerrorism: http://bt.cdc.gov/documents/btstratplan.pdfStrategic Plan for Preparedness and Response
Centers for Disease Control and Prevention Protecting the Nation’s Health in an Era http://cdc.gov/globalidplan.htmof Globalization: CDC’s Global InfectiousDisease Strategy
Council on Foreign Relations and Why Health Is Important to http://www.cfr.org//public/pubs/Kassalow_Health_ Milbank Memorial Fund U.S. Foreign Policy Paper.htm
Department of Defense Global Emerging Infections System http://www.geis.ha.osd.mil
Department of Health and Human Services DHHS Global Health Website http://www.globalhealth.gov
Bill and Melinda Gates Foundation www.gatesfoundation.org
Global Alliance for Vaccines and Immunization http://www.vaccinealliance.org/
Institute of Medicine Emerging Infections from the Global to http://www4.nationalacademies.org/iom/iomhome.nsfLocal Perspective
Institute of Medicine America’s Vital Interest in Global Health http://www.nap.edu/books/0309058341/html
Joint United Nations Programme for AIDS (UNAIDS) http://www.unaids.org
National Institute of Allergy and Global Research Plan for HIV/AIDS, http://www.niaid.nih.gov/publications/globalhealth /Infectious Diseases, National Institutes Malaria, and Tuberculosis global.pdfof Health
National Intelligence Council The Global Infectious Disease Threat http://www.cia.gov/cia/publications/nie/report/and Its Implications for the United States nie99-17d.html

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 63
Organization Publication Web AddressNational Science and Technology Infectious Disease—A Global Health http://www.ostp.gov/CISET/html/toc.htmlCouncil, Committee on International Science, ThreatEngineering, and Technology, Working Group on Emerging and Reemerging Diseases
Rockefeller Foundation Program on Health Equity http://www.rockfound.org/display.asp?context=3& SectionTypeID=18
Roll Back Malaria http://www.rbm.who.int
Safe injection Global Network http://www.injectionsafety.org
Stop TB Initiative http://www.stoptb.org
United Nations Foundation http://www.unfoundation.org
United States Agency for International Development Infectious Disease Strategy http://www.usaid.gov/pop.health/ID/index/html
World Bank, Pan- American Health Organization, Shared Agenda for Health in the Americas http://wbln0018.worldbank.org/external/lac/lac.nsfand Inter- American Development Bank
World Bank World Development Report 2000/2001 http://www.worldbank.org/poverty/wdrpoverty/report
World Health Organization Removing Obstacles to Healthy Development http://www.who.int/infectious-disease- report/index-rpt99.html
World Health Organization WHO Antimicrobial Resistance Infobank http://oms2.b3e.jussieu.fr/arinfobank
World Health Organization WHO Report on Global Surveillance of http://www.who.int/emc- documents/surveillance/Epidemic-prone Infectious Diseases docs/whocdscsrisr2001.ht ml/Tableofcontents/about.htm
World Health Organization Overcoming Antimicrobial Resistance http://www.who.int/infectious-disease-report/2000/index.html
World Health Organization Global Strategy for the Containment http://www.who.int/emc/globalstrategy/of Antimicrobial Resistance strategy.html
World Health Organization The World Health Report 2000 http://www.who.int/whr/2000/en/report.htm
World Health Organization, Rotary International, Global Polio Eradication Initiative http://www.polioeradication.orgCenters for Disease Control and Prevention, United Nations Children Fund (UNICEF)
World Health Organization, UNICEF, UNAIDS, Health a Key to Prosperity http://www.who.int/inf-new/World Bank, United Nations Educational, Scientific, and Cultural Organization (UNESCO), United Nations Population Fund

64 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Emerging infectious diseases are a topic of discussion at many high-level international meetings, including
Group of Eight Industrialized Nations (G8)a
http://usinfo.state.gov/topical/econ/group8
Asia-Pacific Economic Cooperation (APEC)b
http://www.apecsec.org.sg
Common Agenda with Japanhttp://www.mofa.go.jp/region/n-america/us/agenda
Transatlantic Agenda with the European Unionhttp://www.eurunion.org/partner/agenda.htm
U.S.-Mexico Binational Commissionhttp://www.r10.tdh.state.tx.us/obh/bids.htm
The Arctic Councilhttp://www.arctic-council.org
a. The Group of Eight Industrialized Nations includes: Canada, France, Germany, Italy, Japan, the Russian Federation, the United States, and the United Kingdom.
b. The economies of the Asia-Pacific Economic Cooperation include Australia, Brunei, Canada, Chile, China, Hong Kong China, Indonesia, Japan, Republic of Korea, Malaysia,Mexico, New Zealand, Papua New Guinea, Peru, the Philippines, Russia, Singapore. Chinese Taipei, Thailand, the United States, and Vietnam.
c. The Arctic Council includes: Canada, Finland, Greenland/Denmark, Iceland, Norway, Russia, Sweden, and the United States.
APPENDIX BDIPLOMATICFORUMS THATADDRESSEMERGINGINFECTIOUS DISEASE ISSUES

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 65
APPENDIX CEXAMPLES OF INTERNATIONAL OUTBREAK ASSISTANCE
During the 1990s, CDC participated in numerous outbreak investigations inother countries, sometimes as part of an international WHO team and
sometimes in direct response to a request from an affected nation. These inves-tigations included
1990 Japanese encephalitis in Saipan
1990 Epidemic dysentery in Burundi
1991 Hepatitis E in Kenya and Somalia
1991-92 Epidemic dysentery in Zambia
1991 Cholera in Bolivia, Ecuador, El Salvador, Guatemala, and Peru
1991 Cholera in Brazil
1991 Polio in Romania
1991 Polio in Bulgaria
1992 Polio in Jordan
1992-96 Diphtheria in Ukraine
1993-96 Diphtheria in Russia
1993 Polio in Namibia
1993 Polio in Uzbekistan
1994 Dengue in Nicaragua
1994 Plague in India
1994-95 Measles in Palau, Guam, and the Federated States of Micronesia
1995 Diphtheria in Georgia, Kyrgyzstan, Kazakhstan, Uzbekistan, and Turkmenistan
1995 Leptosporosis in Nicaragua
1995 Ebola fever in the Democratic Republic of the Congo (then Zaire)
1996 Epidemic dysentery in South Africa
1996 West Nile encephalitis in Romania
1996 Typhoid fever in Tadjikistan
1996 E. coli O157:H7 infection in Japan
1996 Polio in Albania
1997 Polio in Turkey
1997 Botulism in Argentina
1997 Cholera in Kenya
1997 Avian influenza in Hong Kong
1997 Rift Valley fever in Kenya
1997 O’nyong-nyong fever in Uganda

66 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
1997 Nosocomial HIV-associated multidrug-resistant TB in Argentina
1997 Multidrug-resistant TB in Colombia
1998 Measles in Romania
1998 Bolivian hemorrhagic fever in Bolivia
1999 Louseborne relapsing fever in southern Sudan
1998 Plague in Ecuador
1998 Dengue in Palau
1998 Dengue in Yap
1998 Amebiasis in the Republic of Georgia
1998-99 Influenza outbreaks on cruise ships (U.S.-Canada)
1999 Dengue fever on U.S.-Mexico border
1999 Epidemic poststreptococcal glomerulonephritis in Brazil
1999 Typhoid fever in Nauru
1999 Nipah virus encephalitis in Malaysia
1999 Marburg fever in the Democratic Republic of the Congo
1999 Polio in Angola
1999 Measles in Costa Rica
1999-2000 Hantavirus pulmonary syndrome in Panama
2000 Polio in the Democratic Republic of the Congo
2000 Tularemia in Kosovo
2000 Cholera in Pohnpei State, Federated States of Micronesia
2000 Rift Valley fever in Saudi Arabia and Yemen
2000 Ebola hemorrhagic fever in Uganda
2000 Measles in Haiti, Dominican Republic, Bolivia
2000 Polio in Haiti and the Dominican Republic
2000 Measles in Zambia
2000 Diphtheria in Latvia
2000 Dengue hemorrhagic fever in El Salvador

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 67
APPENDIX DWHO COLLABORATING CENTRES (WHOCCS)BASED AT CDC
WHOCC for Antimicrobial Resistance WHOCC for Arthropod-Borne Viruses in the Western Hemisphere WHOCC for Clostridium botulinum WHOCC for Dengue and Dengue Hemorrhagic FeverWHOCC for Research, Training, and Eradication of Dracunculiasis WHOCC for HIV/AIDs WHOCC for Reference and Reagents for Human Immunoglobulin Subclasses WHOCC for Foodborne Disease Surveillance WHOCC for Surveillance, Epidemiology, and Control of Influenza WHOCC for Evaluating and Testing New Insecticides WHOCC for Leptospirosis WHOCC for Control and Elimination of Lymphatic Filariasis WHOCC for Malaria Control in Africa WHOCC for Production and Distribution of Malaria Sporozoite ELISAs WHOCC for Mycoses in North America WHOCC for Reference and Research on Plague Control WHOCC for Poliovirus and Enterovirus Surveillance WHOCC for Reference and Research on Rabies WHOCC for Respiratory Viruses Other Than Influenza WHOCC for Rickettsial Diseases WHOCC for ShigellaWHOCC for Smallpox and Other Poxvirus Infections WHOCC for Reference and Research in Syphilis Serology WHOCC for Viral Hemorrhagic Fevers WHOCC for Reference and Research on Viral Hepatitis
Tentative WHO Approval:
WHOCC for Lyme Borreliosis WHO/PAHO Collaborating Center for Rotavirus and the Agents of
Viral Gastroenteritus WHOCC for Public Health Systems and Practice
Proposed New Centers:
WHOCC for Cysticercosis WHOCC for Molecular Identification and Typing of Insect Disease Vectors WHOCC for Measles Virus Diagnostics (also serves as the PAHO
Regional Measles Reference Laboratory) WHOCC for Prevention and Control of Epidemic Meningitis WHOCC for Prevention and Control of Mycobacterium ulcerans (Buruli ulcer)WHOCC for Insecticide ResistanceWHOCC for Infectious Disease PathologyWHOCC for Salmonella Surveillance WHOCC for Streptococcus WHOCC for Vibrio cholerae O1 and O139

68 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
A. Regional Networks for Disease Surveillance & Outbreak Response
Africa
• Integrated Disease Surveillance and Epidemic Preparedness and ResponseProject, led by WHO/AFRO
• International Disease Survey for diseases of epidemic potential (e.g., menin-gitis, yellow fever, cholera, measles, and polio), supported by USAID
Other disease surveillance activities in Africa: The disease surveillance component of UNAIDS’ International PartnershipAgainst HIV/AIDS in Africa (IPAA) monitors progress in reducing infectionrates and deaths from HIV/AIDS, TB, and opportunistic infections.
As part of USAID’s African Integrated Malaria Initiative (AIMI), CDC helpsministries of health in Benin, Kenya, Malawi, and Zambia monitor progress inreducing illness and deaths from malaria. During 2001, AIMI surveillance activ-ities will also be conducted in collaboration with the ministries of health of theDemocratic Republic of the Congo, Nigeria, Senegal, and Uganda.
The U.S. Army Medical Research Unit in Nairobi (USAMRU-Kenya) is coor-dinating an effort to enhance surveillance for HIV/AIDS, malaria, yellow fever,and enteric illnesses in east Africa. Partners include ministries of health in Kenyaand Uganda. the Kenya Medical Research Institute (KEMRI), the African Med-ical and Research Foundation (AMREF), and CDC’s Kenya Field Station.
The Americas and the Caribbean
• Amazon Basin Network Includes 7 laboratories from 5 nations
• Southern Cone Network Includes 8 laboratories from 6 nations
• Caribbean Epidemiology Center (CAREC) disease surveillance system Includes the 21 members of CAREC
• Middle America Network
• U.S.-Mexico Border Infectious Disease Surveillance System
• U.S./Canada International Circumpolar Surveillance project to enhance sur-veillance for invasive bacterial infections among indigenous peoples in sub-arctic regions of northern Canada and Alaska. This project is conducted inassociation with the International Circumpolar Surveillance project in Europe(see: Europe).
Other disease surveillance activities in the Americas and the Carribean: The U.S. Naval Medical Research Center Detachment (NMRCD) in Lima iscoordinating an effort to enhance surveillance for malaria, yellow fever, dengue,and other hemorrhagic fevers in South America. Planners include ministries of
APPENDIX EREGIONAL AND DISEASE-SPECIFICSURVEILLANCE NETWORKS

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 69
health of Peru, Ecuador, and Bolivia, WHO/PAHO, and CDC. An epidemiolo-gist from CDC is currently stationed at NMRCD.
Asia
• Mekong Delta Surveillance Network. Includes China (Yunan), Cambodia, Laos, Thailand, Myanmar, and Vietnam
• Pacific Public Health Surveillance Network (PacNet) Includes 20 Pacific Islands
• Early Warning Outbreak Recognition System (EWORS) A collaboration between the Indonesian Ministry of Health and U.S. NavalMedical Research Unit No. 2 (NAMRU-2). It currently involves hospitalsthroughout Indonesia and is expanding to include hospitals in Cambodia.
Other disease surveillance activities in Asia: Disease Surveillance and Electronic Networking are two of six “pillars” in astrategy to fight HIV/AIDS and infectious diseases endorsed at the 2001 summitmeeting of the Asia Pacific Economic Cooperation (APEC). (The other pillarsare: Outbreak Response, Capacity Building, Partnering Across Sectors, andPolitical and Economic Leadership.) As part of this effort, work has beguntoward the creation of an Asia-Pacific network of networks that will knit togeth-er existing electronic infectious disease networks and facilitate timely transmis-sion of public health information across APEC economies. The cooperative sys-tem will build on existing APEC projects that enhance surveillance for influenza,E. coli O157 infection, dengue, and dengue hemorrhagic fever.
The first International Emerging Infectious Program (IEIP) was established inBangkok in September 2001, as a collaboration between CDC and the Ministryof Health of Thailand. This IEIP site will serve as a resource for infectious dis-ease surveillance networks in Asia.
The United States participates in binational projects to improve disease sur-veillance with Vietnam, Thailand, and Cambodia. These collaborations arecoordinated by CDC, the Armed Forces Research Institute of Medical Science(AFRIMS-Thailand) in Bangkok, and NAMRU-2 in Jakarta. For example, anepidemiologist from CDC stationed at NAMRU-2 and a satellite laboratory inPhnom Pen is working with the Cambodian Ministry of Health to establish aschool of public health. An epidemiologist from CDC has also been assigned toChina to facilitate collaborative projects that address the prevention and controlof viral hepatitis, which is a mjor public health concern in China.
Europe
• E.U.’s EnterNet system for surveillance of international foodborne outbreaks
• International Circumpolar Surveillance project to enhance monitoring ofinvasive bacterial infections in the circumpolar regions of Europe (Iceland,

70 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
Greenland [Denmark], Norway, Sweden, Finland and Russia). This project isconducted in association with the U.S./Canada International CircumpolarSurveillance project (see: The Americas and the Caribbean).
The Middle East
• WHO Middle East Initiative to enhance disease surveillance in Israel and thePalestinian territories
Other disease surveillance activities in the Middle East: The U.S. Naval Medical Research Unit No. 3 (NAMRU-3) in Cairo is coordi-nating a collaborative effort to enhance surveillance for diseases of importancein the Middle East (e.g., meningitis, influenza, acute febrile illnesses, and antibi-otic-resistant enteric organisms). Partners include the Egyptian Ministry ofHealth and Population, health authorities in Yemen, Pakistan, and the Palestin-ian Territories, WHO/EMRO, and CDC. An epidemiologist from CDC is cur-rently stationed at NAMRU-3.
B. Selected Global Networks for Infectious Disease Surveillance &Outbreak Response
• WHO Influenza Surveillance Network
• WHO Global Network for Polio Eradication/Measles Elimination
• WHO Supranational Reference Laboratory Network for AntituberculosisDrug Resistance
• WHO Global Salmonella Surveillance (Global Salm-Surv)
• WHO Global Alert and Response Network (see Box 14)
• Surveillance in support of the worldwide eradication of guinea worm disease
• Surveillance for vaccine-preventable diseases under the Expanded Programmeon Immunization (EPI)
• GeoSentinel, the global surveillance network of the International Society ofTravel Medicine
Includes 26 travel and tropical medicine clinics, 15 in the United States, 2 inthe United Kingdom, 2 in Australia, and 1 each in Canada, Germany, Israel,Italy, Nepal, New Zealand, and Switzerland
As mentioned above, the first International Emerging Infectious Program (IEIP)was established in 2001 in Thailand. As new IEIP sites are founded (see page 53),they will provide technical assistance to local disease surveillance networks andbecome members of a global IEIP network.

Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy 71
Fred Angulo, Felice Apter, Ray Arthur, Judith Bale, Daniel Bausch, David
Bell, Sue Binder, Stephen Blount, Queta Bond, Joel Breman, Jennifer Brooks,
Bruce Brown, Donald S. Burke, Jay Butler, Gail Cassell, Martin Cetron,
Mitchell Cohen, Stephen Corber, Kenneth Castro, Patrick S. Chong, Gary G.
Clark, Stephen Cochi, Daniel Colley, Carol Crawford, Nils Daulaire,
Jonathan Davis, David T. Dennis, Frances L. de Peyster, Deborah Deppe,
Lynn DiFato, Cedric Dumont, Laura Efros, Judith F. English, Charles Erics-
son, David Fleming, Anna Flisser, Julie Gerberding, Jerry Gibson, Jesse
Goodman, Thomas Gomez, Duane Gubler, Richard Guerrant, Stephen
Hadler, Wendy Hall, Margaret Hamburg, Walter Hierholzer, David Hey-
mann, Allen Hightower, Nguyen Thi Thu Hong, Don Hopkins, James
Hospedales, Harold Jaffe, Stephanie James, William Jarvis, Warren Johnson,
Gregory Jones, Marsha Jones, Bradford Kay, Robert Keegan, Richard
Keenlyside, Patrick Kelley, Keith Klugman, Christopher E. Laxton, James W.
LeDuc, Michael Levine, Arthur Liang, Scott Lillibridge, Lavinia M. Limon,
Earl Long, Michael Malison, Eric Mast, Alison Mawle, Jay McAuliffe,
Patrick J. McConnon, Eugene McCray, Joseph McDade, John McGowan,
Martin Meltzer, Eric Mintz, Thomas Monath, Melinda Moore, Anthony
Moulton, Stephen Ostroff, Mark Papania, Alan Parkinson, Anthony Perez,
Robert Perry, Bradley Perkins, Bobbie Person, Francisco Pinheiro, Gabriel
Ponce de Leon, Robert Quick, Rosemary Ramsey, Arthur Reingold, Joy
Riggs-Perla, Nancy Rosenstein, Ronald St. John, Anne Schuchat, Ben
Schwartz, Larry Slutsker, Carol Snarey, Richard Steketee, Mary Grace
Stobierski, Charles Stokes, Susan Stout, Robert Tauxe, Ralph Timperi,
Laura Trent, Juli Trtanj, Mark Walkup, J. Todd Weber, Mark White, Gillian
Woollett, Michael Zeilinger.
ACKNOWLEDGMENTS

72 Protecting the Nation’s Health in an Era of Globalization: CDC’s Global Infectious Disease Strategy
1. Zhu T, Korber B, Nahmias AJ, Hooper E, Sharp PM,Ho DD. An African HIV-1 sequence from 1959 andimplications for the origin of the epidemic. Nature1998;391:594-7.
2. Lanciotti RS, Roehrig JT, Duebel V, et al. Origin ofthe West Nile virus responsible for an outbreak ofencephalitis in the northeastern United States. Science1999;286:2333-7.
3. Working Group on Emerging and Re-emerging Infec-tious Diseases. Committee on Science, Engineering,and Technlogy (CISET), National Science and Tech-nology Council. Infectious Disease—A Global HealthThreat. Washington, DC: U.S. Government PrintingOffice, 1995.http://www.ostp.gov/CISET/html/toc.html
4. Institute of Medicine. America’s Vital Interest inGlobal Health. Washington, DC: National AcademyPress, 1997.http://www.usaid.gov/pop_health/id/index.html
5. Garrett L. Betrayal of Trust: The Collapse of GlobalPublic Health. New York: Hyperion, 2000.
6. The global infectious disease threat and its implica-tions for the United States. National Intelligence Estimate (NIE 99-17D). January 2000.http://www.cia.gov/cia/publications/nie/report/nie99-17d.html
7. Gallup JL, Sachs, JD. The economic burden of malar-ia. Harvard Center for International DevelopmentWorking Paper No. 52, July 2000.http://www.cid.harvard.edu/cidwp/052.htm/
8. World Health Organization Press Release WHO/28,25 April 2000. Economic costs of malaria are manytimes higher than previously estimated. Joint reportissued by the World Health Organization, HarvardUniversity, and the London School of Hygiene andTropical Medicine at the African Summit on RollBack Malaria in Abuja, Nigeria, April, 2000.http://www.who.int/inf-pr-2000/en/pr2000-28.html
REFERENCES
9. World Bank. Confronting AIDS: Public Priorities in aGlobal Epidemic. New York: Oxford University Press.1997.
10. Centers for Disease Control and Prevention. Prevent-ing Emerging Infectious Diseases: A Strategy for the21st Century. Atlanta, GA: U.S. Department of Healthand Human Services, 1998. http://www.cdc.gov/nci-dod/emergplan
11. Centers for Disease Control and Prevention. Workingwith Partners To Improve Global Health: A Strategyfor CDC and ATSDR, Atlanta, GA: U.S. Departmentof Health and Human Services, 2000.http://www.cdc.gov/ogh/pub/strategy.pdf
12. Quinn TC, Mann JM, Curran JW, Piot P. AIDS inAfrica: an epidemiologic paradigm. Science1986;234:956-63.
13. Lengeler C. Insecticide-treated bednets and curtains forpreventing malaria (Cochrane Review). In: TheCochrane Library, Issue 3, 2001. Oxford: Update Software.
14. Quick RE, Venczel LV, Mintz ED, et al. Diarrhea pre-vention in Bolivia through point-of-use disinfectionand safe storage: a promising new strategy. Epidemiol-ogy and Infection: 1999;122:83-90.
15. U.S. Agency for International Development andUNAIDS. Children on the Brink—2000.Http://www.usaid.gov/pubs/hiv_aids/childrenreport.pdf
16. Shared Agenda for Health in the Americas, Pan Ameri-can Health Organization, Inter-American DevelopmentBank, and the World Bank. Http://wbln0018.world-bank.org/external/lac/lac.nsf
17. Global Measles Mortality Reduction and RegionalElimination: Strategic Plan, 2001–2005.WHO/UNICEF, November 2000.Http://www.unicef.org/newsline/01pr26.htm

For additional copies of this booklet, write to
Office of Health CommunicationNational Center for Infectious DiseasesCenters for Disease Control and PreventionMailstop C-141600 Clifton Road, NEAtlanta, GA 30333Fax: 404-371-5490
or visit the website: www.cdc.gov/globalidplan.htm
Suggested CitationCenters for Disease Control and Prevention. Protecting the National’s Health in an Era ofGlobalization: CDC’s Global Infectious Disease Strategy. Atlanta, GA: U.S. Department ofHealth and Human Services, 2001.

Department of Health & Human ServicesCenters for Disease Control and Prevention (CDC)Atlanta, GA 30333
Official Business
Penalty for Private Use $300
RETURN SERVICE REQUESTED
First Class MailPostage Fees Paid
PHS/CDCPermit No. G-284