Embed Size (px)
Citation preview

Central East Local Integration Network Hospital Clinical Services PlanBoard Meeting
July 15th, 2008

- 2 -
Today’s Agenda
Project OverviewScope and ObjectivesTeamApproachTimelines
Next Steps
AppendicesProject Goals: Activities and DeliverablesSteering Committee Members
- 3 -
Project Overview

- 4 -
Project Objectives and Scope
The development of a hospital Clinical Services Plan for the Central East LHIN (CE LHIN) will guide the initial steps in creating a “one acute care network” within the CE LHIN. The overarching principles to guide this process, as stated in the Project Charter, include:
Improving quality and safety by grouping together clinical or medical/surgical specialists, their teams and appropriate physical resources.Expanding or creating new programs that would not be viable or sustainable at multiple sites.Creating operational and clinical efficiencies that would allow hospitals to focus on, and improve, their core programs. Create new “centres of excellence” to allow CE LHIN residents to receive services within the LHIN and as close-to-home as possible.
The scope of work is structured around the four goals:
1. Hospital Service Planning and Scenario Modeling
2. Identify Integration Opportunities and New Models of Service
3. Supporting Physician Integration
4. Change Management Strategies
- 5 -
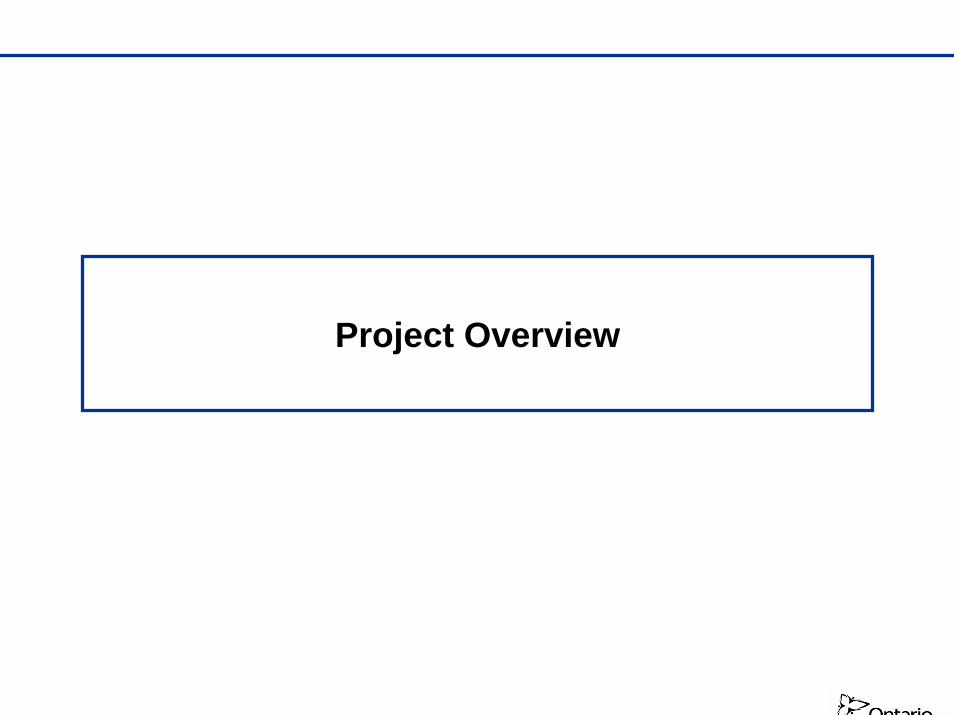
Deloitte and Central East LHIN Project Work Teams
James Meloche Project Lead
PROJECT MANAGEMENT & LEADERSHIP
Lisa PurdyEngagement
Partner
Central East LHIN Clinical Service Plan Steering Committee
Central East LHIN Project
Team
Project TeamAdvisory Panel
Irene PodolakQuality Advisor
Partner
Dr. Dave Matheson - Regional Physician Structure and Credentialing,
Patient Flow, and Paediatrics
Dr. Asim Masood - Emergency and Physician Scheduling Practices
Dr. Daniel Penello - Surgery
Kathy LeBlanc, RN – Regional Service Models
Ann Pottinger, RN – Mental Health
Lynne Golding & Cynthia Heinz, Fasken Martineau DuMoulin – Legal
Advisor
David Cerny, Cohos Evamy –Infrastructure Advisor
Kate Wilkinson - Project Manager
Alan Ruth - Demographic Population Projections
Dr. Dante Morra - Physician Lead, Internal Medicine
Gloria Cardoso - Clinical Support
Kristin Mendoza – Clinical Support
Greg Chow – Data Support
Susan Plewes -Project Manager
Senior Integration Consultants
Decision Support
Communications
Priority Project Leads
Task Group
Task Group
Task Group
Task Group
Task Group
Task Group
Task Group
Task Group
CE CCACProject Sponsor
- 6 -
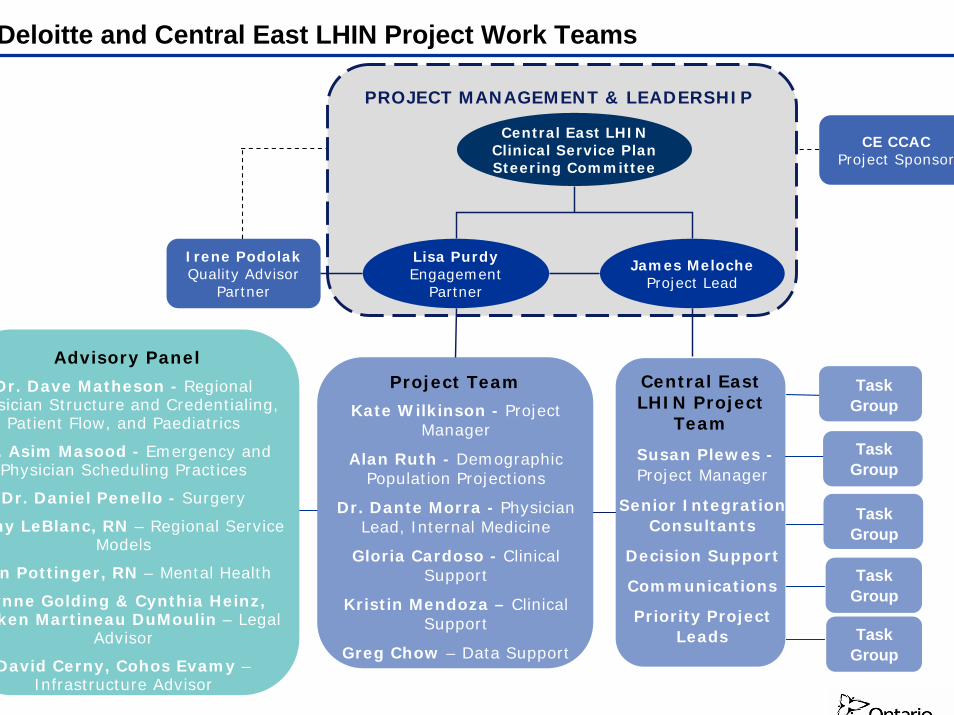
Project Approach
GOAL 4
Action Plan for Implementation
of Viable Integration
Opportunities
Action Plan for Implementation
of Viable Integration
Opportunities
Phase 4.1
GOAL 2
Infrastructure and Financial Requirements to Implement and Operate
Viable Integration
Opportunities
Infrastructure and Financial Requirements to Implement and Operate
Viable Integration
Opportunities
Phase 2.2
Understanding of Current CE LHIN Hospital Service
Utilization Patterns
Understanding of Current CE LHIN Hospital Service
Utilization Patterns
GOAL 1
Base-case Scenario of Future Hospital Service Demand
Base-case Scenario of Future Hospital Service Demand
Phase 1.1 Phase 1.2
Phase 2.1
Service
Model
Options
Phase 1.3
Viable Integration
Opportunities
GOAL 3
Framework for LHIN-wide Physician Credentialing(if Legal and Practical Requirements can be met)Framework for LHIN-wide Physician Credentialing(if Legal and Practical Requirements can be met)
Principles and Guidelines to Build a Framework for a LHIN-wide Surgical/OR and on-call Scheduling System
Principles and Guidelines to Build a Framework for a LHIN-wide Surgical/OR and on-call Scheduling System
Phase 3.1
Phase 3.2
Identify
Integration
Opportunitie
s

- 7 -
Project Timelines
Month
Weeks 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Project Launch
Goal 1: Hospital Services Planning and Scenario Modeling
Phase 1.1 Understanding of Current Central East LHIN Hospital Service Utilization Patterns
Phase 1.2: Baseline Scenario of Future Hospital Service Demand
Phase 1.3: Service Model Options
Goal 2: Identification of Integration Opportunities and New Models of Service Delivery
Phase 2.1: Identify Integration Opportunities
Phase 2.2: Infrastructure and Financial Requirements to Implement and Operate Viable Integration Opportunities
Goal 3: Supporting Physician Integration
Phase 3.1: Framework for LHIN-wide Physician Credentialing
Phase 3.2: Principles and Guidelines to Build a Framework for a LHIN-wide Surgical/OR and on-call Scheduling System
Goal 4: Change Management
Phase 4.1: Action Plan for Implementation of Viable Integration Opportunities
Sept October NovemberJune July August
Kick off meeting
Bed Map & Service Capture Rates
Base-case future demands
Service Model Options
Integration Opportunities
Infrastructure Requirements &
Financial Projections
Credentialing Framework
Scheduling Framework
Action Plan
Month
Weeks 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Project Launch
Goal 1: Hospital Services Planning and Scenario Modeling
Phase 1.1 Understanding of Current Central East LHIN Hospital Service Utilization Patterns
Phase 1.2: Baseline Scenario of Future Hospital Service Demand
Phase 1.3: Service Model Options
Goal 2: Identification of Integration Opportunities and New Models of Service Delivery
Phase 2.1: Identify Integration Opportunities
Phase 2.2: Infrastructure and Financial Requirements to Implement and Operate Viable Integration Opportunities
Goal 3: Supporting Physician Integration
Phase 3.1: Framework for LHIN-wide Physician Credentialing
Phase 3.2: Principles and Guidelines to Build a Framework for a LHIN-wide Surgical/OR and on-call Scheduling System
Goal 4: Change Management
Phase 4.1: Action Plan for Implementation of Viable Integration Opportunities
Sept October NovemberJune July August
Kick off meeting
Bed Map & Service Capture Rates
Base-case future demands
Service Model Options
Integration Opportunities
Infrastructure Requirements &
Financial Projections
Credentialing Framework
Scheduling Framework
Action Plan
Kick off meeting
Bed Map & Service Capture Rates
Base-case future demands
Service Model Options
Integration Opportunities
Infrastructure Requirements &
Financial Projections
Credentialing Framework
Scheduling Framework
Action Plan

- 8 -
Next Steps
1. Develop the base-case for current clinical services utilization within the Central East LHIN - presentation of preliminary results to Steering Committee on July 17th.
2. Conduct key stakeholder consultations and site visits across the LHIN end of July early August.
3. Engage the 5 project task groups in determining program definitions and to further inform the development of service model options for the 5 priority services: Cardiac Services, Vascular Surgery, Thoracic Surgery, in-patient Paediatric and Neonatal Services, and Acute Mental Health and Addiction Services.
4. Identification of key planning assumptions and population projections to identify short-, medium -,and long-term service demands on the CE LHIN hospitals.
Over the next few months, the following activities will occur with the goal of progressing to developing service model options towards the end of the Summer:
- 9 -
Appendix
- 10 -
Goal 1: Hospital Service Planning and Scenario Modeling
- 11 -
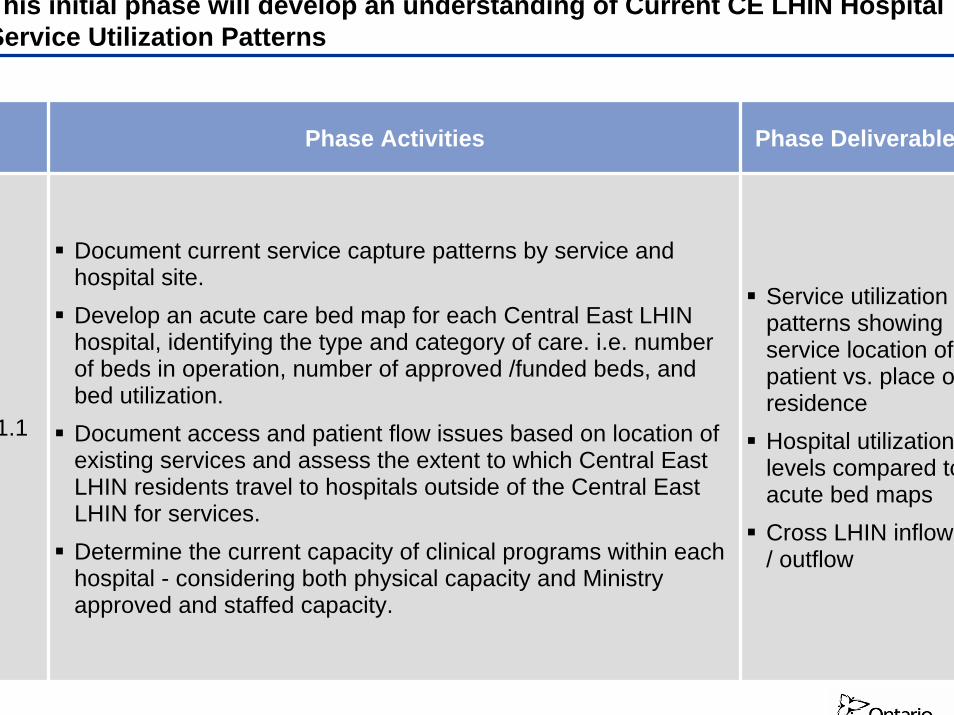
This initial phase will develop an understanding of Current CE LHIN Hospital Service Utilization Patterns
Phase Activities Phase Deliverable
1.1
Document current service capture patterns by service and hospital site. Develop an acute care bed map for each Central East LHIN hospital, identifying the type and category of care. i.e. numberof beds in operation, number of approved /funded beds, and bed utilization.Document access and patient flow issues based on location of existing services and assess the extent to which Central East LHIN residents travel to hospitals outside of the Central East LHIN for services. Determine the current capacity of clinical programs within each hospital - considering both physical capacity and Ministry approved and staffed capacity.
Service utilization patterns showing service location of patient vs. place of residenceHospital utilization levels compared to acute bed mapsCross LHIN inflow / outflow
- 12 -
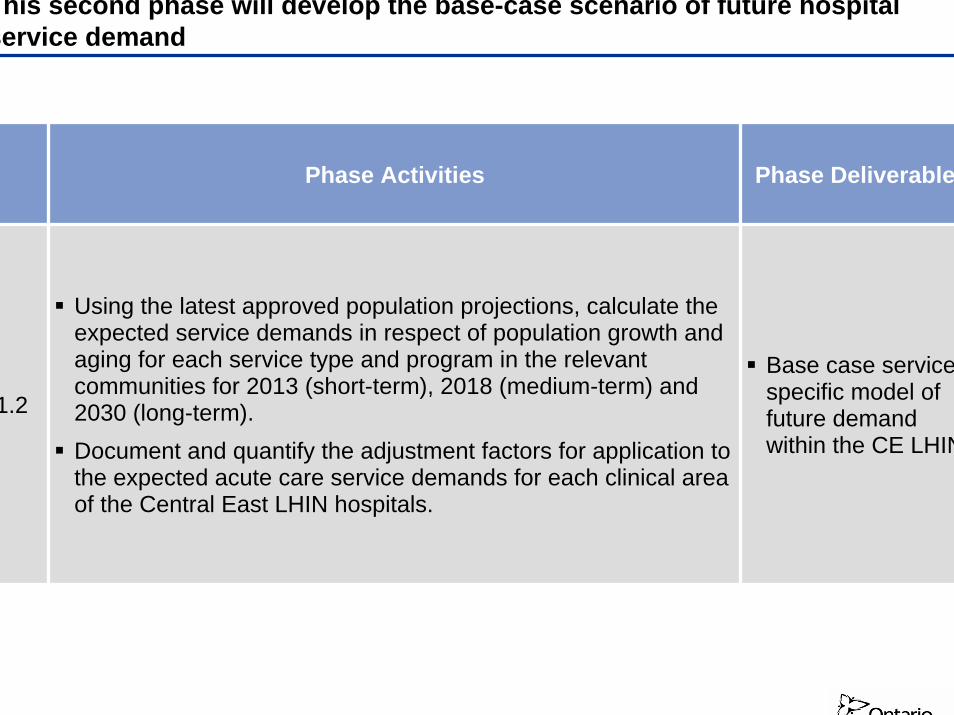
This second phase will develop the base-case scenario of future hospital service demand
Phase Activities Phase Deliverable
1.2
Using the latest approved population projections, calculate the expected service demands in respect of population growth and aging for each service type and program in the relevant communities for 2013 (short-term), 2018 (medium-term) and 2030 (long-term).Document and quantify the adjustment factors for application to the expected acute care service demands for each clinical area of the Central East LHIN hospitals.
Base case service-specific model of future demand within the CE LHIN
- 13 -
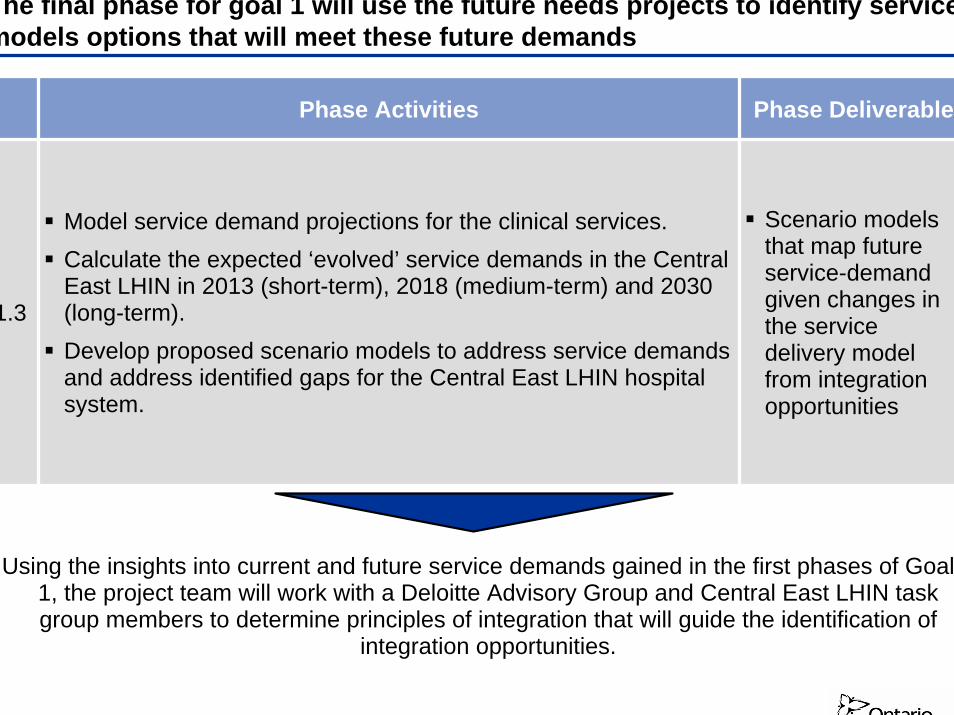
The final phase for goal 1 will use the future needs projects to identify service models options that will meet these future demands
Phase Activities Phase Deliverable
1.3
Model service demand projections for the clinical services.Calculate the expected ‘evolved’ service demands in the Central East LHIN in 2013 (short-term), 2018 (medium-term) and 2030 (long-term).Develop proposed scenario models to address service demands and address identified gaps for the Central East LHIN hospital system.
Scenario models that map future service-demand given changes in the service delivery model from integration opportunities
Using the insights into current and future service demands gained in the first phases of Goal 1, the project team will work with a Deloitte Advisory Group and Central East LHIN task group members to determine principles of integration that will guide the identification of
integration opportunities.
- 14 -
Goal 2: Identification of Integration Opportunities and New Models for Service
Delivery

- 15 -
Phase 2.1 will establish short-term integration opportunities for the five priority areas and develop an understanding of the physical and financial requirements
Phase Activities Phase Deliverable
2.1
Development of short-term integration opportunities in the areas of: Vascular Surgery/Access, Thoracic Surgery, Hospital-based Paediatrics, Cardiac Services (including PCI), Mental Health and Addictions Services (including Children and Family).
After the scenario modeling options are complete, finalize cross-site findings and opportunities for presentation to the ClinicalServices Planning Committee.
Integration opportunities will be explored based on ability to improve quality and increase access to needed hospital services for Central East LHIN residents.
Short, medium and long term integration opportunities
Short term integration opportunities to move forward on

- 16 -
Phase 2.2 will develop an understanding of the physical and financial requirements for those integration opportunities developed in 2.1
Phase Activities Phase Deliverable
2.2
Review current infrastructure capacity, and quantify infrastructure requirements to support short-term integration opportunities, given projected service levels. This includes building, land and large capital equipment.
Building on these assessments, we will have a baseline for capital planning and costing from which to determine infrastructure gaps and the investment required to support new service models.
Create a high-level multi-site modeling plan to demonstrate the development of infrastructure in a phased approach over the next 5 to 10 years that would support the new models of service.Supporting this plan will be an identification of the financial investments and capital expenditures for each phase of the plan.
Development plan of infrastructure requirements to seize short term integration opportunities
- 17 -
Goal 3: Supporting Physician Integration

- 18 -
Goal 3 will develop frameworks to support physician integration through LHIN-wide credentialing and on-call and OR scheduling systems
Phase Activities Phase Deliverable
3.1
Conduct a current state review of physician credentialing processes for each Central East LHIN hospital.
Develop a map of current physician resources within the Central East LHIN with particular reference to: specialty, primary (and secondary) location (s) where they have privileges, and current on-call commitments.
Conduct consultations with key Central East LHIN stakeholders and conduct and external scan (may include regulatory bodies, medical association) to determine activities in other jurisdictions.
Examine the legal and business requirements and constraints for implementing a regional physician credentialing model within Central East LHIN.
A framework for LHIN-wide physician credentialing (pending legal and practical requirements)
3.2
Review relevant documents to assess the current state of surgical/OR and on-call scheduling for each Central East LHIN hospital (e.g. Current and Planned Physician On-call Schedules and Volumes by Specialty).
Conduct consultations with key Central East LHIN stakeholders to gather initial considerations to develop surgical/OR and on-call scheduling system.
Based on the findings from the documentation review and discussions with key stakeholders, develop preliminary principles and guidelines for the dimensions of an application framework.
Principles and guidelines to build a framework for a LHIN-wide Surgical/OR and on-call Scheduling System
- 19 -
Goal 4: Change Management
- 20 -
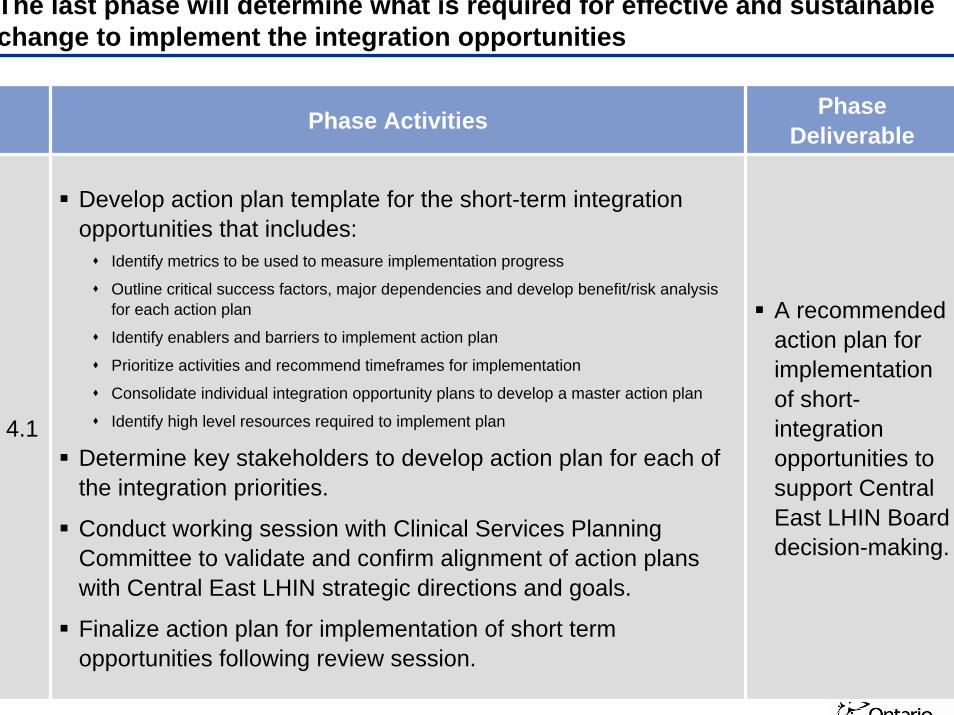
The last phase will determine what is required for effective and sustainable change to implement the integration opportunities
Phase Activities Phase Deliverable
4.1
Develop action plan template for the short-term integration opportunities that includes:
Identify metrics to be used to measure implementation progress
Outline critical success factors, major dependencies and develop benefit/risk analysis for each action plan
Identify enablers and barriers to implement action plan
Prioritize activities and recommend timeframes for implementation
Consolidate individual integration opportunity plans to develop a master action plan
Identify high level resources required to implement plan
Determine key stakeholders to develop action plan for each of the integration priorities.
Conduct working session with Clinical Services Planning Committee to validate and confirm alignment of action plans with Central East LHIN strategic directions and goals.
Finalize action plan for implementation of short term opportunities following review session.
A recommended action plan for implementation of short-integration opportunities to support Central East LHIN Board decision-making.

- 21 -
Steering Committee
- 22 -
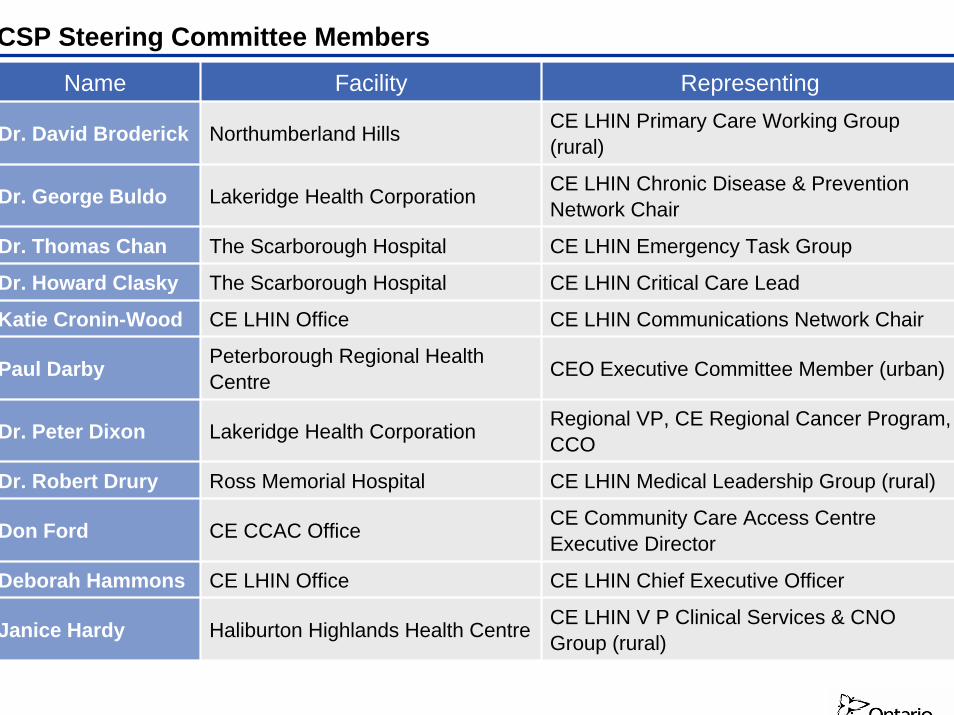
CSP Steering Committee MembersName Facility Representing
Dr. David Broderick Northumberland Hills CE LHIN Primary Care Working Group (rural)
Dr. George Buldo Lakeridge Health Corporation CE LHIN Chronic Disease & Prevention Network Chair
Dr. Thomas Chan The Scarborough Hospital CE LHIN Emergency Task Group
Dr. Howard Clasky The Scarborough Hospital CE LHIN Critical Care Lead
Katie Cronin-Wood CE LHIN Office CE LHIN Communications Network Chair
Paul Darby Peterborough Regional Health Centre CEO Executive Committee Member (urban)
Dr. Peter Dixon Lakeridge Health Corporation Regional VP, CE Regional Cancer Program, CCO
Dr. Robert Drury Ross Memorial Hospital CE LHIN Medical Leadership Group (rural)
Don Ford CE CCAC Office CE Community Care Access Centre Executive Director
Deborah Hammons CE LHIN Office CE LHIN Chief Executive Officer
Janice Hardy Haliburton Highlands Health Centre CE LHIN V P Clinical Services & CNO Group (rural)

- 23 -
CSP Steering Committee Members (cont’)
Name Facility Representing
Kelly Isfan Campbellford Memorial Hospital CEO Executive Committee Member (rural)
Lewis Hooper CE LHIN Office CE LHIN eHealth Steering Committee Chair
Dr. Christopher Jyu The Scarborough Hospital CE LHIN Primary Care Working Group (urban)
Christine Kooy Lakeridge Health CE LHIN VP Clinical Services & CNO Group (urban)
James Meloche CE LHIN Office CE LHIN Senior Director, PICE
Dr. Naresh Mohan Rouge Valley Health System CE LHIN Medical Leadership Group (urban)
Dr. Rosemary Moodie Rouge Valley Health System CE LHIN Paediatrics Lead
Sheila Neuburger Whitby Mental Health Centre CE LHIN Alternate Level of Care Task Group Chair
Dr. John Peto Rouge Valley Health System CE LHIN Seamless Care for Seniors Network
Dr. Peter Prendergast Whitby Mental Health Centre CE LHIN Mental Health & Addiction Network
Chair
Heather Reid Rouge Valley Health System CE LHIN Rehabilitation Task Group Chair
Karen Seymour Peterborough Regional Health Centre
Labour/Unions
Dr. John Wright The Scarborough Hospital Medical Leaders Committee, Council of Academic Hospitals of Ontario
- 24 -
Deloitte, one of Canada’s leading professional services firms, provides audit, tax, consulting, and financial advisory services through more than 6,800 people in 51 offices. Deloitte operates in Québec as Samson Bélair/Deloitte & Touche s.e.n.c.r.l. The firm is dedicated to helping its clients and its people excel. Deloitte is the Canadian member firm of Deloitte Touche Tohmatsu.
Deloitte refers to one or more of Deloitte Touche Tohmatsu, a Swiss Verein, its member firms, and their respective subsidiaries and affiliates. As a Swiss Verein (association), neither Deloitte Touche Tohmatsu nor any of its member firms has any liability for each other's acts or omissions. Each of the member firms is a separate and independent legal entity operating under the names “Deloitte,” “Deloitte & Touche,” “Deloitte Touche Tohmatsu,” or other related names. Services are provided by the member firms or their subsidiaries or affiliates and not by the Deloitte Touche Tohmatsu Verein.
© Deloitte & Touche LLP and affiliated entities.