Embed Size (px)
Citation preview

Cerebral blood flow andmorphological changes after hypoxic-ischaemicinjury in preterm lambs
ENRIQUE HILARIO1, MARI CARMEN REY-SANTANO2, FELIPE GONI-DE-CERIO1,
FRANCISCO JOSE ALVAREZ2, ELENA GASTIASORO2, VICTORIA EUGENIA MIELGO2,
AMALE CABALLERO3, ADOLFO VALLS-I-SOLER4, SONIA GOMEZ-URQUIJO3
& ANTONIA ALVAREZ1
1Department of Cell Biology and Histology, 3Department of Neuroscience, and 4Department of Paediatrics, School of Medicine
and Dentistry, University of the Basque Country, Leioa, Bizkaia, Spain, and 2Research Unit on Experimental Respiratory
Physiology, Hospital de Cruces, 48903 Barakaldo, Vizcaya, Spain
AbstractAim: To evaluate the effect of cerebral hypoxia-ischaemia induced by partial occlusion of the umbilical cord on therelationship of the regional cerebral blood flow and the cerebral cell death in near-term fetal lambs.Methods: Fifteen near-termlambs were assigned to two hypoxic-ischaemic groups with or without life support (3 h), and a healthy one. Hypoxia-ischaemia was induced by partial occlusion of the umbilical cord (60 min). Routine light and electron microscopy, and theTUNEL method for apoptosis were performed. Regional cerebral blood flow was measured by coloured microspheres.Cardiovascular, gas exchange and pH parameters were also evaluated. Results: Both hypoxic-ischaemic groups produced atransient acidosis and a decrease of base excess in comparison to the healthy group. Cortical and cerebellar zones, where theregional cerebral blood flow values were similar to baseline, showed an increased number of oligodendrocyte-like apoptoticcells. In contrast, in the inner zones, where regional cerebral blood flow was increased, the number of apoptotic cells did notincrease. Necrotic neurons were observed in the basal nuclei, mesencephalon, pons and deep cerebellar nuclei.
Conclusion: Our results suggest that regional cerebral blood flow and the presence of apoptotic cells, 3 h after hypoxic-ischemic injury, are correlated.
Key Words: Apoptosis, brain damage, cell death, cellular lesion, perinatal asphyxia
Introduction
The reduction in oxygenation (hypoxia) and/or
blood flow (ischaemia) results in a perinatal asphyctic
event [1]. Cerebral hypoxic-ischaemic (HI) lesion
is one of the major causes of mortality and neuro-
logical morbidity both in the premature and in the
term newborn. Some 2 to 4 of 1000 term live births
suffer asphyxia in the prenatal or intrapartum
periods, representing up to 90% of neonatal HI
lesions [2].
At term, the most frequent intrapartum cause of
neonatal brain injury is asphyxia, which can be divided
into two types [3]. The first is the interruption of the
fetal oxygen supply by some acute obstetric events that
interfere either with the maternal or fetal blood flow
(acute abruption, umbilical cord accident, etc.). In all
cases, the maternal blood flow supply to the placenta is
compromised, and a sudden interruption of fetal
oxygenation is present. The second asphyctic mech-
anism is denominated chronic intrapartum asphyxia
[3]. During labour, each contraction of the uterus
compresses the maternal blood vessels of the placenta,
reducing the maternal blood flow and the oxygen
supply, and probably stopping it altogether. In normal
labour, the fetus is unaffected due to the short duration
of the hypoxia and the presence of a maternal blood
pool within the placenta. However, the intermittent
interruption of the maternal blood supply may be
enough to compromise the fetal acid-base balance in an
abnormal placenta. Thus, the intensity and duration of
HI injury determine the degree of cerebral damage
[4,5], which induce the appearance of a significant
proportion of cells susceptible of undergoing apoptosis
Correspondence: Enrique Hilario, Department of Cell Biology and Histology, School of Medicine and Dentistry, University of the Basque Country, 48940 Leioa,
Vizcaya, Spain. Fax: +34 944648966. E-mail: [email protected]
(Received 14 June 2004; revised 3 January 2005; accepted 17 January 2005)
Acta Pædiatrica, 2005; 94: 903–911
ISSN 0803-5253 print/ISSN 1651-2227 online # 2005 Taylor & Francis Group Ltd
DOI: 10.1080/08035250510031151

that significantly contributes to perinatal cerebral
damage. Moreover, the damage worsens during the
reperfusion phase [6], and continues for hours after
reoxygenation/reperfusion.
In the present work, we use a neonatal model of HI
injury at term in which the injury intensity could be
appreciated and quantified at an early stage. Also, the
injury model used to produce brain damage is similar
to the above related conditions in humans, in which
the decrease of blood flow and hypoxia are due to an
umbilical cord compression. Therefore, although our
study is developed under a less physiological condition
than fetal chronic preparation under spontaneous
behaviour as previously reported [7–12], our model
seems to be close to the clinical situation of asphyxiated
neonates in neonatal intensive care units, and it has
low cost. Also, this model could be used to evaluate
the crucial effect of neuroprotective treatments and
resuscitation techniques (air versus pure oxygen,
surfactant, etc.) to mitigate the HI injury during the
transition from fetal to neonatal life.
The aim of the present work was to study the effect of
cerebral hypoxia-ischaemia induced by partial occlu-
sion of the umbilical cord on the relationship of the
regional cerebral blood flow and the cerebral cell death
in near-term fetal lambs after resuscitation and 3 h of
neonatal life support.
Materials and methods
Animals
The study was carried out on 15 fetal lambs at 86–92%
of gestation (124–133 d of developmental age; term:
145 d). At 120 d (86%) of gestation, the develop-
mental stage of the brain of the fetal sheep is considered
to be similar to that of the full-term newborn infant
[13]. The experimental protocol met European regu-
lations for animal research (EU 86/609), and was
approved by the Experimental Research Committee.
Surgical preparation
Fifteen ewes were used for each experiment and,
independently of multiple gestation, only one fetal
lamb per ewe was used. Sheep were sedated with
xylazine (1 mg/kg) prior to surgery. Anaesthesia was
induced by an intravascular injection of ketamine
hydrochloride (5 mg/kg), and maintained with
continuous infusion of Propofol1 (10 mg/kg/h).
Hydro-electrolyte balance was adjusted by continuous
infusion of Ringer lactate (10 mg/kg/h).
At right lateral recumbent, animals were immedi-
ately intubated with an endotracheal tube (8 mm ID),
and controlled ventilation (CPU1, Omeda, Riverside,
CA, USA) was used to maintain normoxia (16.0–
20.0 kPa with inspired O2 fraction: 0.21–0.60) and
normocapnia (percentage of expired CO2: 4.5–6.0%).
An arterial catheter (Insyte 20GA Catheter, Becton
Dickinson, Drogheda, Ireland) was inserted in a
peripheral artery to monitor arterial pressure.
Fetal lambs were exposed by left laparotomy. The
head was exteriorized and an endotracheal tube (Hi-Lo
Jet Tracheal tube ID 4 mm, Mallinckrodt Medical,
St. Louis, MO, USA) was inserted. Catheters (XRO
umbilical catheter, Vygon, France) were placed in the
right jugular vein (to heart and brain directions), and
the arterial catheter was inserted in the left axillary
artery, advanced through the subclavian artery to place
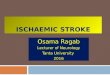
the tip in the brachiocephalic trunk (Figure 1). The left
carotid artery was isolated, and a non-invasive flow
Doppler sensor was allocated to measure cerebral
blood flow in real time (T106, Transonics, Ithaca, FL,
USA).
The umbilical cord was isolated to determine both
venous and arterial flows using non-invasive flow
Doppler sensors (T106, Transonics, Ithaca, FL,
USA). Core temperature was monitored and kept
between 37 and 38�C with a temperature blanket
Figure 1. Regional cerebral blood flow was determined by coloured
microspheres infused in the left subclavian artery. In the ovine animal
model, the left and right subclavian arteries arise from the brachio-
cephalic trunk, which divides equally into left and right carotid
arteries. Arrows represent blood flow through arterial vessels.
LCA/RCA: left and right carotid arteries; DS: Doppler sensor; LSA/
RSA: left and right subclavian arteries; MI: microspheres injection;
C: catheter; BT: brachiocephalic trunk; A: aorta; DA: ductus
arteriosus; PA: pulmonary artery; PT: pulmonary trunk; RA: right
atrium.
904 E. Hilario et al.

(Digiterm S542, JP Selecta, Barcelona, Spain). At this
moment, the basal point (B) was established in all
animals and an arterial blood sample was taken and all
parameters were recorded.
Hypoxic-ischaemic injury
In the hypoxic-ischaemic experimental groups, the HI
injury was induced by partial occlusion of the umbilical
blood flow for 60 min. A rubber occluder was placed
around the umbilical cord, and the flow Doppler
sensor was maintained in the umbilical arteries in order
to continuously measure and display, in real time, the
blood flow. The occluder was properly compressed to
produce a reduction of the umbilical arterial blood flow
lower than 50% of basal value, as the flow Doppler
sensor monitor displayed. During HI injury, fetal
arterial pH, blood gases, mean systemic arterial pres-
sure and heart rate were determined at 15-min inter-
vals. The hypoxic-ischaemic endpoint was established
after 60 min of partial occlusion (HI point), and an
arterial blood sample was taken and all parameters
were recorded. Previous studies have demonstrated
that, at this point, a partial occlusion of the umbilical
cord produces an arterial pH less than 7.1, a 50%
decrease in arterial O2 content (in relation to basal
value) and a base excess less than 715 mmol/l [8].
In animals without HI injury, 60 min after basal
point, an arterial blood sample was also taken and all
parameters were recorded, in order to obtain reference
values for the hypoxic-ischaemic experimental groups
in the statistical study.
Neonatal care
All lambs received i.v. ketamine hydrochloride (8 mg)
and pancuronium bromide (0.4 mg), and then the
umbilical cord was cut. Animals were weighed (SECA
727, Snoqualmie, Germany) and placed in an open
incubator, and the endotracheal tube was connected to
a pressure-limited ventilator (Bourns BP 200, Beard
Med. Sys. Inc., Riverside, CA, USA) with the follow-
ing settings: rate 50 breath/min; peak inspiratory
pressure: 2.9 kPa; positive end-expiratory pressure:
0.5 kPa; inspiratory expiratory ratio 1 : 2; inspired O2
fraction: 1.0; and flow: 10 l/min. Anaesthesia and
paralysis were maintained by a continuous infusion of
ketamine hydrochloride (5 mg/kg/h) and pancuronium
bromide (1 mg/kg/h) in 5% dextrose.
Groups
Lambs were randomly assigned to three different
experimental groups by means of the closed envelope
method. Healthy group: after caesarean section with-
out hypoxia-ischaemia, lambs were managed on
conventional mechanical ventilation for 3 h (n=6) and
sacrificed. Hypoxic-ischaemic control group: after HI
endpoint (60 min of hypoxia-ischaemia), lambs (n=3)
were sacrificed without resuscitation or conventional
mechanical ventilation. Hypoxic-ischaemic injured
group: after 60 min of hypoxia-ischaemia, lambs were
resuscitated and managed on conventional mechanical
ventilation for 3 h (n=6) and sacrificed.
Measurement
Blood samples were obtained from the brachiocephalic
trunk for haematocrit, acid-base balance and gas
exchange. Core temperature, mean systemic arterial
pressure, heart rate and carotid blood flow were also
measured. All parameters were determined and regis-
tered at basal point (B), every 15 min during 60 min of
HI injury, during conventional mechanical ventilation
(1 h) and at 3 h (3 h). Animals were sacrificed by
means of an intravascular overdose of barbiturate.
Necropsy
After sacrifice, the fetal brains were prepared for
regional cerebral blood flow (RCBF) and histopatho-
logical studies. First, carotid arteries were isolated and
catheters were placed to perfuse Ringer lactate solution
at 4�C at a previously registered flow (100–150 ml/
min). After that, the brain was perfused with 500 ml of
4% paraformaline and removed from the skull. The
brain was divided into different cerebral regions in
order to perform RCBF or morphological studies (see
below).
Regional cerebral blood flow
Measurement of RCBF at different intervals was
determined using four coloured microspheres (Dye
Track1, Triton Technology Inc., San Diego, USA),
which were infused through the left subclavian artery
because, in the ovine animal model, the left and right
subclavian arteries arise from the brachiocephalic
trunk which divides equally into the left and right
carotid arteries (Figure 1). The infusion of coloured
microspheres was realized within 30–45 s at B, HI, 1-h
and 3-h intervals as previously described [14]. As
previously mentioned, the flow Doppler sensor and its
monitor display the value of flow at real time, so the
mean carotid blood flow displayed by the monitor
during the 30–45 s of microsphere infusion was used as
a “reference flow” value in the equation below. The
brain was divided into nine cerebral regions: cortical
zones (frontal, parietal, temporal and occipital cortex),
inner zones (thalamus, striatum and hippocampus),
cerebellum and medulla oblongata [9]. Each piece
was weighed and digested with alkali (KOH, 4 M)
during 3 h in a shaking bath at 72�C. The obtained
sample was filtered through a filter of 10-mm pore to
recover the coloured microspheres. Filters were
dried, and dimethylformamide (1.2 ml, Sigma-Aldrich
Cerebral blood flow and cell damage 905

Co. Ltd, Gillingham, UK) was used to extract dye
from the microspheres. To determine the amount of
microspheres per sample, the optical density was
measured by spectrophotometry (HP 8452A, Hewlett
Packard, Silicon Valley, CA, USA) at four different
wavelengths. RCBF was calculated as previously
described [15] as follows: tissue flow=tissue micro-
spheresrreference flow/reference microspheres.
Histology
Fixation quality was scored on a 10-point scale [16].
Thus, 0 corresponds to a bad perfusion, with collapsed
microvessels and the presence of residual erythrocytes,
whereas 10 represents good tissue preservation, in
which residual erythrocytes are not detected, the
microvessels are open and disseminated cell swelling is
absent.
Light and electron transmission microscopy
Brains were placed on a table, and cut into 0.5-cm-
thick consecutive sections. Samples from different areas
were embedded in paraffin wax for light microscopy.
The sections (5-mm thickness) were stained for routine
histological examination with haematoxylin-eosin
(HE), and immunostained for apoptotic studies.
Samples were also obtained for ultrastructural exam-
ination.
Samples processed for transmission electron
microscopy were embedded in Epon by conven-
tional methods. Briefly, tissue blocks of 1 mm3 were
immersed in 2.5% glutaraldehyde in 0.1 M sodium
cacodylate/HCl buffer (pH 7.4) for 2 h. The samples
were then post-fixed in 2% osmium tetroxide in the
same buffer for 2 h and subsequently embedded
in Epon 812 (Fluka, Switzerland). Semithin sections
(1-mm thickness) were stained with Toluidine blue,
and ultra-thin sections (60–80-nm thickness) were lead
stained and observed under the electron microscope.
In HE-stained sections, we evaluated the following
regions and parameters:
(1) Regions: cerebral cortex (frontal, parietal,
temporal, occipital), basal nuclei, hypothal-
amus, thalamus, hippocampus, amygdaloid
body, mesencephalon, pons, cerebellum (cortex
and deep cerebellar nuclei), white matter
(2) Parameters: cell injury (hydropic change,
pyknotic nuclei, etc.), focal necrosis, increase
in cellularity, oedema, microhaemorrhage,
vacuolization.
In situ apoptotic cell labelling
DNA fragmentation was examined on the paraffin
sections using the TUNEL method [17] applying the
ApopTag Apoptosis Kit (Intergene, NY, USA). The
procedure was as follows: brain sections (5-mm thick-
ness) were deparaffined, hydrated and pretreated with
20 mg/ml proteinase K for 30 min at 37�C. Endoge-
nous peroxidase activity was blocked by incubating
slides in 3% hydrogen peroxidase for 15 min. After
washing in PBS and in equilibrating buffer, the sections
were incubated in working strength terminal deoxy-
nucleotidyl transferase enzymes at 37�C for 1 h. The
reaction was halted by stop wash buffer for 10 min.
After several washes in PBS, the reaction was revealed
by peroxidase-diaminobenzidine and finally counter-
stained with methyl green. Involuting mammary gland
sections were used as positive controls for the TUNEL
method.
In each animal, we scanned the presence of apop-
totic figures, did the counting in all consecutive fields
and repeated the procedure in three paraffin sections
(20 mm apart) using a BX50 Olympus microscope.
Only unquestionable apoptotic figures were counted as
such. The amount of apoptosis was expressed as the
number of cells labelled per high power magnification
(high power magnification is meant to imply a r10 eye
piece and a r40 objective).
Statistical analyses
Values are given as mean+standard deviation (SD).
Results were contrasted with a Levene test to confirm
the homogeneity of variance between the different
treatments and a Kolmogorov-Smirnoff test for
normality. One-factor analysis of variance (ANOVA)
with Bonferroni-Dunn’s correction was performed to
assess differences in acid-base balance, base excess,
PCO2, cardiovascular parameters, RCBF and apoptotic
count as a function of group (Statview, Abacus Corp.,
USA).
Cerebral blood flow measurements of the hypoxic-
ischaemic control group were used as references for
the hypoxic-ischaemic injured group to assess the
relationship between RCBF and apoptosis count.
Comparison between parameters was performed by
two-factor ANOVA for repeated measurements as a
function of brain zones and/or groups. A p40.05 was
considered significant.
Results
Physiological data
All animals were alive at the end of the experimental
period. At baseline, all groups demonstrated a mean
systemic arterial pressure of 55+3 mmHg. This value
was maintained without significant changes until the
end of experiment, in all groups. At 3 h, the values
were 55+3 mmHg in the healthy group and
55+4 mmHg in the hypoxic-ischaemic injured group.
Sixty minutes after HI injury, we observed an increase
906 E. Hilario et al.

in the heart rate in all hypoxic-ischaemic animals
(214+11 beats/min; n=9) in comparison to the
healthy group (159+5 beats/min; n=6). However, at
3 h, no difference was observed between the
hypoxic-ischaemic injured group (249+43 beats/min;
n=6) and the healthy one (180+37 beats/min; n=6).
In uteri, all animals showed (Figure 2) an adequate
gas exchange and acid-base balance by means of the
placenta (at baseline, arterial PO2: 4.3+0.3 kPa).
During HI injury, both HI groups showed a significant
decrease of arterial pH (Figure 2a) and base excess
(Figure 2b) in comparison to the healthy group. Only
transient changes in PCO2 (Figure 2c) and hypoxia
(2.7+0.9 vs 4.1+0.1 kPa) were observed. After 3 h,
no differences were shown between the healthy and
injured groups (Figure 2).
Regional cerebral blood flow
Data of RCBF are summarized in Table I. At baseline,
in all animals, the cerebral blood flow in the cortical
regions and in the inner zones of the brain were similar
(198+68 vs 216+112 ml/100 g/min). However, the
blood flow of the cerebellum only represented 11.5%
in comparison to the other zones.
In the healthy group, RCBF did not show significant
fluctuations during the fetal or neonatal period (at 3 h,
cortical RCBF: 170+58 ml/100 g/min; inner RCBF:
106+48 ml/100 g/min; cerebellar RCBF: 24+12 ml/
100 g/min), although inner cerebral blood flow showed
a downwards trend in time.
At the point of HI injury, both hypoxic-ischaemic
groups showed a significant increase in the inner
zones (320+86 vs 160+64 ml/100 g/min), although
changes in cortical and cerebellar RCBF were not
present (Table I). At 3 h, the increase of inner RCBF
was maintained (236+102 vs 106+48 ml/100
g/min). Similarly for the healthy group, neither
the cortical nor cerebellar flow showed significant
differences.
Neuropathological findings
Samples showed a good histological preservation.
Thus, the level of brain fixation corresponds to an 8–9
in the van Reempts’ scale [16].
In both hypoxic-ischaemic groups, mild perivascular
and interstitial oedema was observed; the mesence-
phalon, pons, deep cerebellar nuclei and cerebral
cortex being the most affected zones. Necrotic scat-
tered neurons (Figure 3) were observed in the mesen-
cephalon, pons, deep cerebellar nuclei and basal
nuclei. The ultrastructural study confirms this type of
cell death. Some cells showed a minimum degree of
damage, consisting of mild hydropic changes and
the regrouping of Nissl granules. Areas of necrosis,
haemorrhage or increased cellularity were not
observed.
Quantification of cell death by TUNEL stain
Small and round apoptotic cells were located in both
white and grey matter and not circumscribed to the
Figure 2. (a) Mean basal arterial pH of all animals (open square)
corresponds to baseline point (B). Mean values for both healthy
(open triangles) and hypoxic-ischaemic (open circles) groups are
represented as a function of time (HI, 1-h and 3-h intervals).
Differences at HI point (p50.05) are demonstrated by an asterisk.
Horizontal bars close to x-axis represent chronological sequence of
events. (b) Mean basal base excess of all animals (open square)
corresponds to baseline point (B). Mean values for both healthy
(open triangles) and hypoxic-ischaemic (open circles) groups are
represented as a function of time (HI, 1-h and 3-h intervals).
Differences at HI interval (p50.05) are demonstrated by an asterisk.
Horizontal bars close to x-axis represent chronological sequence
of events. (c) Mean basal PCO2 of all animals (open square) corre-
sponds to baseline point (B). Mean values for both healthy control
(open triangles) and hypoxic-ischaemic (open circles) groups
are represented as a function of time (HI, 1-h and 3-h intervals).
Horizontal bars close to x-axis represent chronological sequence of
events.
Cerebral blood flow and cell damage 907

regions where necrotic neurons were present, which
were negative to apoptag Kit (Figure 4). In some cases,
apoptotic cells were located beside medium- and
large-sized neurons.
Table II summarizes the apoptotic cell count in
different brain areas. In the hypoxic-ischaemic injury
group, TUNEL-positive cells were higher in compar-
ison to both healthy and hypoxic-ischaemic control
ones. This increase was observed in the cerebral cortex,
cerebellum as well as in the pons. In the hypoxic-
ischaemic injury group, a non-significant increase in
the apoptotic cell count was noted in the cerebral basal
nuclei.
Relationship between RCBF and apoptotic cell count
Both parameters demonstrated a relationship as a
function of experimental group (RCBF, p=0.02;
apoptotic count, p=0.0001), but not in regard to brain
zones (RCBF, p=0.11; apoptotic count, p=0.16).
However, a relationship between RCBF and apoptotic
Table I. Regional cerebral blood flow (ml/100 g/min).
Interval
Group
B HI 1 h 3 h
All animals
(n=15)
Healthy
(n=6)
Hypoxic-ischaemic
injury (n=9)
Healthy
(n=6)
Hypoxic-ischaemic
injury (n=6)
Healthy
(n=6)
Hypoxic-ischaemic
injury (n=6)
Frontal cortex 40+12 33+6 66+15 28+4 31+6 37+13 36+5
Parietal cortex 47+8 45+8 57+6 37+5 29+9 42+11 34+10
Temporal cortex 73+66 93+85 69+24 46+13 37+5 63+43 48+28
Occipital cortex 37+9 31+2 64+19 27+4 36+3 32+10 37+14
Mean flow of cortical
zones
198+68 202+88 256+64 138+28 138+14 170+58 152+40
Striatum 54+31 42+30 91+26 36+15 52+12 29+19 49+18
Hippocampus 92+55 67+22 85+29 44+3 66+23 43+13 105+70
Thalamus 90+61 50+16 119+51 42+3 57+18 34+18 81+35
Mean flow in inner
zones
216+112 160+64 320+86a 122+26 176+32a 106+48 236+102a
Medulla Oblongata 72+62 38+13 155+59 24+6 67+18 27+10 112+81
Cerebellum 24+16 18+4 46+27 20+5 27+15 24+12 26+13
Values are given as mean+SD. One-factor analysis of variance (ANOVA) was performed between groups at each interval (B, HI, 1 h and 3 h).a p50.05 vs healthy group.
Figure 3. Presence of neurons showing coagulative changes in the deep cerebellar nuclei of the hypoxic-ischaemic injury group. Cells show
shrinkage and eosinophilia of the cytoplasm (arrows point to cells with more severe damage). Hematoxilin-eosin stain; original
magnificationr100.
908 E. Hilario et al.

count was demonstrated ( p=0.04) as a function of
brain zones and groups.
Discussion
Our results suggest a relationship between regional
cerebral blood flow and histopathological changes in
the fetal lambs. These changes consist of mild peri-
vascular and interstitial oedema with necrotic scattered
neurons and apoptotic oligodendrocyte-like cells.
The morphological changes were more incipient
than grade 1 in the classification of Ikeda et al. [8] in
near-term fetal lambs after 72 h of the HI injury.
However, after 3 h of the HI injury, we observed the
presence of neurons showing coagulative cell changes,
characteristic of cell death [16,18], which corresponds
to a grade 3 of damage in the Ikeda classification. In the
fetal lamb brain, these changes have been previously
reported in the periventricular white matter and in the
parasagital cerebral cortex after 24 h of repetitive cord
occlusion [12], and in the Purkinje cells after 72 h of
severe asphyctic injury [9].
The morphological traits and the localization (both
in grey and in white matter) of the positive TUNEL
cells suggest that these cells could correspond to
oligodendrocyte lineage. Oligodendrocytes are sus-
ceptible to a variety of injurious stimuli induced by
HI injury [1,19], and the intrinsic vulnerability of
oligodendrocyte precursors is considered central to the
pathogenesis of periventricular leukomalacia [20]. The
different mode of cell death observed in neurons and
oligodendrocyte-like cells suggests the activation of a
Figure 4. Presence of two apoptotic figures (arrows) in the basal ganglia of the hypoxic-ischaemic injury group. On the left (arrowhead), a
damaged neuron with a negative stain for TUNEL can also be observed. TUNEL counterstained with methyl green; original
magnificationr400.
Table II. Apoptosis count as a function of different brain regions and experimental groups represented as healthy, hypoxic-ischaemic control
and hypoxic-ischaemic injured groups.
Group
Healthy
(n=6)
Hypoxic-ischaemic control
(n=3)
Hypoxic-ischaemic injury
(n=6)
Parietal cortex 10+4 9+5 79+15a
Temporal cortex 12+2 16+14 82+16a
Basal nuclei 10+2 12+8 41+15
Hypothalamus 20+7 34+11 14+9
Hippocampus 30+3 31+9 23+3
Thalamus 18+3 24+16 24+9
Mesencephalon 39+6 10+1 38+10
Pons 17+10 20+10 55+5a
Cerebellum 27+6 29+10 104+15a
Three sections per zone and animal were evaluated and the mean value+SD expressed as the number of apoptotic cellsr1072 by high-power
microscopic field.a p50.05 vs healthy and hypoxic-ischaemic control groups.
Cerebral blood flow and cell damage 909

different death programme in these cells due to the HI
injury. In this respect, intracellular levels of ATP and
the intensity of the initial insult have been involved in
the fate of cell death by necrosis or apoptosis [5,21].
However, the existence of neuronal subpopulations
and glial cells with a differential sensitivity to asphyxia
or with different abilities to generate ATP via glycolysis
[22] could be also considered.
The fetal lamb model is ideal for the study of cerebral
metabolism and blood flow [7,23,24]. It has been used
in the study of the influence of several physiopa-
thological factors (hypoxia, PCO2 level, acidosis, etc.),
autoregulation and O2 delivery on cerebral blood flow
and on metabolic energy status. Cerebral blood flow is
regulated by the cerebral perfusion pressure and the
cerebrovascular resistance, which is controlled by
arteriolar tone under the influence of blood compo-
nents, blood gases (O2, CO2), pH, etc. [25,26]. In the
fetus, during the initial phase of hypoxia, the increase
of arterial PCO2 and the decrease of arterial PO2 induce
a cerebral vasodilatation. Later, the arterial blood
pressure and the cardiac output decrease with a loss of
cerebral autoregulation and, finally, a change in RCBF
occurs [27]. Also, the alteration of CO2 levels produces
a sudden fall in acid-base balance [28], which also
contributes. In our work, the observed alteration of
CO2, pH, heart rate, etc. could be responsible for the
changes of RCBF during HI injury. Also, we must
consider that the resuscitation and the postnatal
ventilatory management did not affect the auto-
regulation of RCBF, because these parameters were
close to basal (normal) values.
In our study, the cortical and cerebellar zones, where
the RCBF values were similar to baseline, showed an
increased number of apoptotic cells. In contrast, in the
zones where RCBF was increased (inner zones), the
number of apoptotic cells did not increase. Partial
umbilical cord occlusion produces a continuous
decrease of O2 content [8,9] and, consequently, those
brain areas, even with a non-altered flow, but receiving
less O2 content, are susceptible to producing brain cell
injury. In near-term fetal lambs, the failure in perfusion
and/or hypoxia by partial occlusion of the umbilical
flow produces a brain lesion that resembles periven-
tricular leukomalacia findings [8,19]. The differential
distribution between cerebral blood flow and the
apoptotic or necrotic areas observed remains to be
elucidated.
Acknowledgements
We thank Prof. David Hallett for his careful review of themanuscript. This work has been partially supported by grantsfrom Fondo de Investigacion Sanitaria, Ministerio deSanidad (FIS01/0110-1 and FIS01/0110-2), and from theUniversidad del Paıs Vasco (1/UPV075.327-E-14885/2002and 9/UPV00077.327-15330/2003 Hilario). The authorscarried out the work on behalf of the RESPIRA group of
Cooperative Research Networks of Fondo de InvestigacionSanitaria (C03/11).
References
[1] Johnston MV, Trescher WH, Ishida A, Nakajima W. Neuro-
biology of hypoxic ischemic injury in the developing brain.
Pedriatr Res 2001;49:735–41.
[2] Vannucci RC, Perlman JM. Interventions for perinatal
hypoxic ischemic encephalopathy. Pediatrics 1977;100:
1004–14.
[3] Terzidou V, Bennett P. Maternal risk factors for the
fetal and neonatal brain damage. Biol Neonate 2001;79:
157–62.
[4] Walton M, Connor B, Lawlor P, Young D, Sirimanne E,
Gluckman P, et al. Neuronal death and survival in two models
of hypoxic-ischemic brain damage. Brain Res Rev 1999;
29:137–68.
[5] Almeida A, Bolanos JP. A transient inhibition of mitochondrial
ATP synthesis by nitric oxide synthase activation triggered
apoptosis in primary cortical neurons. J Neurochem 2001;77:
676–90.
[6] Jassem W, Fuggle SV, Rela M, Koo DDH, Heaton ND. The
role of mitochondria in ischemia/reperfusion injury. Trans-
plantation 2002;73:493–9.
[7] Szymonowicz W, Walker AM, Cussen L, Cannata J, Yu VY.
Developmental changes in regional cerebral blood flow in fetal
and newborn lambs. Am J Physiol 1988;254:H52–8.
[8] Ikeda T, Murata Y, Quilligan EJ, Choi BH, Parer JT, Doi S,
et al. Physiologic and histologic changes in near-term fetal
lambs exposed to asphyxia by partial umbilical cord occlusion.
Am J Obstet Gynecol 1998;178:24–32.
[9] de Haan HH, Van Reempts JLH, Vles JSH, de Haan J, Hasaart
THM. Effects of asphyxia on the fetal lamb brain. Am J Obstet
Gynecol 1993;169:1493–501.
[10] Mallard EC, Williams CE, Johnston BM, Gluckman PD.
Increased vulnerability to neuronal damage after umbilical cord
occlusion in fetal sheep with advancing gestation. Am J Obstet
Gynecol 1994;170:206–14.
[11] de Haan HH, Gunn AJ, Williams CE, Gluckman PD. Brief
repeated umbilical cord occlusions cause sustained cytotoxic
cerebral edema and focal infarcts in near-term fetal lambs.
Pediatr Res 1997;41:96–104.
[12] Marumo G, Kozuma S, Ohyu J, Hamai Y, Machida Y,
Kobayashi K, et al. Generation of periventricular leukomalacia
by repeated umbilical cord occlusion in near-term fetal sheep
and its possible pathogenetical mechanisms. Biol Neonate
2001;79:39–45.
[13] Raju TNK. Some animal models for the study of perinatal
asphyxia. Biol Neonate 1992;62:202–14.
[14] Alvarez FJ, Gastiasoro E, Rey-Santano MC, Arnaiz A, Larrabe
JL, Gomez MA, et al. Asphyxia in preterm lambs induced by
cord clamping. Effects of MgSO4 on cerebral blood flow an O2
uptake. In: Cabero L, Carrera JM, editors. The perinatal
medicine in the new milenium. Bologna: Monduzzi Editore;
2002.
[15] Heymann MA, Payne BD, Hoffman JI, Rudolf AM. Blood flow
measurements with radionuclide-labeled particles. Progr
Cardiovasc Dis 1977;20:55–78.
[16] Van Reempts JLH. The hypoxic brain: histological and
ultrastructural aspects. Behav Brain Res 1984;14:99–108.
[17] Gravieli Y, Sherman Y, Ben S. Identification of programmed
cell death in situ via specific labeling of nuclear DNA
fragmentation. J Cell Biol 1992;119:493–501.
[18] Wyllie H, Duvall E. Cell injury and death. In: McGee JOD,
Isaacson PG, Wright NA, editors. Oxford textbook of pathol-
ogy. New York: Oxford University Press; 1992.
910 E. Hilario et al.

[19] Rezaie P, Dean A. Periventricular leukomalacia, inflammation
and white matter lesions within the developing nervous system.
Neuropathology 2002;22:106–32.
[20] Back SA, Luo NL, Borenstein N-S, Levine JM, Volpe JJ,
Kinney HC. Late oligodendrocyte progenitors coincide with
the developmental window of vulnerability for human perinatal
white matter injury. J Neurosci 2001;21:1302–12.
[21] Eguchi Y, Shimizu S, Tsujimoto Y. Intracellular ATP levels
determine cell death fate by apoptosis or necrosis. Cancer Res
1997;57:1835–40.
[22] Delgado-Esteban M, Almeida A, Bolanos JP. D-glucose
prevents glutathione oxidation and mitochondrial damage after
glutamate receptor stimulation in rat cortical primary neurons.
J Neurochem 2000;75:1618–24.
[23] Rosenberg AA. Cerebral blood flow and O2 metabolism after
asphyxia in neonatal lambs. Pediatr Res 1986;20:778–82.
[24] Szymonowicz W, Walker AM, Yu VYH, Stewart ML, Cannata
J, Cussen L. Regional cerebral blood flow after hemorrhagic
hypotension in the preterm, near-term, and newborn lamb.
Pediatr Res 1990;28:361–6.
[25] Kjellmer I, Karlsson K, Olsson T, Rosen KG. Cerebral reac-
tions during intrauterine asphyxia in the sheep. I. Circulation
and oxygen consumption in the fetal brain. Pediatr Res
1974;8:50–7.
[26] Whittelaw A, Karlson BR, Haaland K, Dahlin I, Steen PA,
Thoresen M. Hypocapnia and cerebral ischaemia in
hypotensive newborn piglets. Arch Dis Child 1991;66:
1110–4.
[27] Lou HC, Lassen NA, Tweed WA, Johnson G, Jones M,
Palahniuk F. Pressure passive cerebral blood flow and break-
down of the blood-brain barrier in experimental fetal asphyxia.
Acta Paediatr Scand 1979;68:57–63.
[28] Palmer C, Brucklacher RM, Christensen MA, Vannucci RC.
Carbohydrate and energy metabolism during the evolution of
hypoxic-ischemic brain damage in the immature rat. J Cereb
Blood Flow Metab 1990;10:227–35.
Cerebral blood flow and cell damage 911