Embed Size (px)
Citation preview

Cerebrospinal Fluid Immunoreactive Substance P and Somatostatin in Neurological Patients with Peripheral and Spinal Cord Disease
H. CRAMER*, N. R&LER*, K. RISSLER”, M. C. GAGNIEU** and B. RENAUD**
*Department of Neurology, University of Freiburg, 7800 Freiburg, F. t?. G. * * Hopital Neurologique and Universitk Claude Bernard, 69394 Lyon, France.
Abstract-We have measured substance P-like (SPLI) and somatostatin-like (SLI) immunoreactivities in cerebrospinal fluid of 49 patients with peripheral (polyneuropathy, lumboischialgia) and spinal cord disease and in 16 control patients. The patient groups showed significantly higher CSF SPLI levels than controls while the mean SLI levels were unchanged.
Fractionated sampling of CSF (total volume 30ml) in 20 patients with various neurological diseases showed no significant differences between early and late fractions for SLI. In contrast, lumbar-cisternal concentration gradients were negative for SPLI, total protein and IgG, and positive for the dopamine metabolite homovanillic acid and the serotonin metabolite 5-hydroxyindolacetic acid. This suggests that SPLI may be released into the lumbar CSF from lower levels of the neuraxis, presumably the spinal cord and spinal ganglia, whereas SLI stems from diffuse CSF secretion without spinal preponderance.
Introduction
Recent investigations with immunohistochemistry and radioimmunoassay have revealed a wide and uneven distribution of a number of neuropeptides in the central nervous system. Increasing evidence suggests that these bioactive compounds are important in normal neuronal interplay and may be critically involved in a number of neurological diseases (for review see 1, 2). Among the newly discovered neuropeptides, substance P (SP) is one of the best candidates for a neurotransmitter role in the brainstem (3) and in the spinal cord (4-6). It
Date received 10 March 1988
Date accepted 13 May 1988
is highly concentrated in the dorsal horn and in cell bodies of primary sensory afferents (7, 8). Also somatostatin (SST), a hypothalamic neuropeptide discovered in 1968 (9) and identified in 1973 (10) is present in these structures (3, 5, 8, 11). Its concentrations and flow in peripheral nerves has been shown to vary with functional changes (12). Both SP and SST are involved in nociception (13). Antagonistic roles of these two peptides were suggested in pain afferences (14,15). Pain-eliciting effects of intrathecally administered SP in rats (16) contrast with analgesic properties of intrathecal somatostatin in animals and man (17, 18). Together, these findings have raised our interest in possible alterations of SP and somatostatin in the
119

120 NtllKOI’El”IlDtS
cerebrospinai fluid (CSF) of neurological patients with spinal cord and peripheral nervous disease. Since the origin of the peptides in the CSE is a matter of controversy (19-23) we also studied the concentration of the neuropeptides in fractionated consecutive samples of CSF in a number of neuro- logical patients with various diagnoses.
Group III. 17 patients with lumboischialgia and radicular motor-sensory deficit due to interverte-
bral disc protrusion were studied. 3 patients were medication-free, the others received peripheral analgesics and benzodiazepines (diazepam or tetrazepam).
Patients and Methods
Patients
Group 1. Sixteen non-medicated patients without cerebral or spinal disorders and major pain com- plaints were used as controls. The patients pre- sented with diffuse hyperaesthesia and paraes- thesia (5), psychosomatic complaints (3), incom- plete idiopathic facial paresis in remission (2), gonarthrosis (2), otomastoiditis without intra- cranial complication (1) and subfebrile tempera- ture (2). In all cases a suspected meningitis or other organic nervous system pathology was ex- cluded by thorough clinical examination, CSF analysis, EEG and CT scan. Their age and sex distribution is given in Table 1.
Group IV. 19 patients with spinal cord disease were investigated. Two patients had spinal ischemia with tetraplegia and incomplete trans- verse myelitis, respectively, one paraneoplastic and two cervical compressive myelopathy due to intervertebral disc protrusion, four had spinal tumors (meningeomas, cavernous hemangiomas according to WHO classification). Four cases were diagnosed as having amyotrophic lateral sclerosis and two carcinomatous meningeosis. Four patients had spinal pyramidal lesions (spastic para- paresis or incomplete transverse myelitis) of un- determined origin.
Group II. 13 patients with polyneuropathy were studied. The etiologies were: one diabetic, two alcoholic, two toxic (due to vincristin for treatment of lymphogranulomatosis, resorchine for malaria prophylaxis), two dysimmune, two hereditary, one pressure sensitive. In three cases the cause of the polyneuropathy remained undetermined. Two patients showed sensory deficit only, three had solely motor impairment, eight patients had com- bined motor-sensory deficits. Five of the 13 patients complained of painful sensations.
Group V. This group of 20 patients with various diagnosis was used to investigate any occurring craniolumbar gradients of SPLI and SLI in com- parison to gradients of proteins and momoamine metabolites. The group consisted of 3 male and 17 female patients (mean age 48.2 rfr 4.2 S.E.M. years). Four female patients were diagnosed as having multiple sclerosis with severe cerebellar or spinal disturbance, three had infections of CNS (one lymphocytic meningitis, two borreliosis). One patient had Pick’s disease, one senile dementia of Alzhiemer’s type, both diagnoses based on clinical criteria. One patient had normal pressure hydrocephalus, two of four patients with vascular disease showed marked dementia of the multi-infarct type. Four patients had peripheral nervous disease (trigeminal neuropathy, lumbois-
Table 1 Clinical Data and CSF Levels of Total Protein, Substance P-Like (SPLI) and Somatostatin-Like (SLI) Immunoreactivity in Patients with Peripheral and Spinal Cord Disease and in Controls -
Group Number Sex (FIM)
I Control 16 12/4 II Lumboischialgia 17 918 III Polyneuropathy 13 716 IV Spinal cord 19 1 l/8
* significant p < 0.05 vs. control Wilcoxon test ** significant P < 0.01 vs. control Wilcoxon test
Mean age +- S.E.M.
37.9 f 3.8 52.1 i 2.2 52.3 + 5.3 57.6 + 2.8
rota1 protein (mgidl)
30.2 + 2.3 40.1 + 2.9 40.5 * 4.4 60.1 t 13.5
SPLl (fmoliml)
9.0 5 0.6 13.7 F 1.6* 12.7 + 0.9** 14.1 * 1.3**
SLI ~fmolirn/J
43.X t 2.0 45.3 F 3.6 39.4 + 3.6 46.8 k 4.2

NEl’ROLO(~lCAL PATIENTS WITH PERIPHERAL AND SPINAL CORD DISEASE 121
Table 2 Level of Substance P-Like (SPLI) and Somatostatin-Like (SLI) Immunoreactivities. Total Protein, IgG, Homovanillic Acid (HVA) and 5Hydroxyindoleacetic Acid (5HIAA) in Three Successive Fractions of Lumbar CSF (8-10ml each) of 20 Patients (group V).
Substance Fraction I Fraction II Fractron III
SPLI
( fmol/ml)
SLI ( fmol/ml)
total protein (mg/dl) IgG Imgidl) HVA (nmol) 5-HIAA (nmol/l)
12.4 + 1.1 10.0 + 0.9 Y.0 + 0.6**
44.5 + 4.7 43.3 f 4.1 44.5 + 4.7
45.1 * 4.2 38.8 + 3.2** 35.Y + 3.0**
4.16 k 0.64 3.53 ? 054** 3.26 + 0.52**
335.6 i 48.3 510.6 + 71.9** 560.2 * 69.4”’
142.3 f 18.8 209.9 f 24.5** ‘18.0 + 18.0**
* significant p < 0.05 vs. fraction I Wilcoxon test *’ significant p < 0.01 vs. fraction II Wilcoxon test
chialgia. alcoholic polyneuropathy and peroneal
neuralgia). One patient had a chordoma of the cranial base without cerebral involvement and one depression.
Methods
In the standard procedure 8-10ml CSF was sub- tracted after lumbal puncture at the L 3/4 or L 4/5 interspace. CSF was distributed in aliquots for examination of cell count and total protein con- tent, and for high pressure liquid chromatography assay of homovanillic acid and $hydroxyindo- leacetic acid and radioimmunoassay of neuropep- tides. In the 20 patients of group V with a study of peptide gradients the procedure was extended with collection of 3 equal fractions of 8-10ml CSF. Routine laboratory examination of cell count and glucose content was performed on the first fraction only while all fractions were subjected to measure- ments of total protein, IgG, immunoreactivity for SP and somatostatin, homovanillic acid (HVA) and 5hydroxyindoleacetic acid (5HIAA).
Substance P-like immunoreactivity (SPLI) and somatostatin-like immunoreactivity (SLI) were determined by specific radioimmunoassay as de- scribed (24, 25).
HVA and 5-HIAA were analysed using re- versed-phase high pressure liquid chromatography coupled with electrochemical detection as de- scribed (26). IgG levels were determined by an
immunochemical nephelometric method (ICS system Beckman), total protein levels by the method of Biuret.
As statistical tests for significance, the Wilcoxin two sided signed rank test and the Wilcoxin two sample test were used. Correlations were estab- lished by linear regression on a Hewlett-Packard HP 9825 A.
Results
The control patients (Group I, Table 1) showed a mean lumbar CSF SLPI concentration of 9.0 f 0.6 fmol/ml and SLI of 43.8 * 2.0 fmoY1. The mean SPLI concentrations were significantly increased in patients with spinal cord disease to 157%. in patients with polyneuropathy to 141% and in patients with lumboischialgia to 152% of control values (Table 1). In contrast no significant changes were seen for SLI.
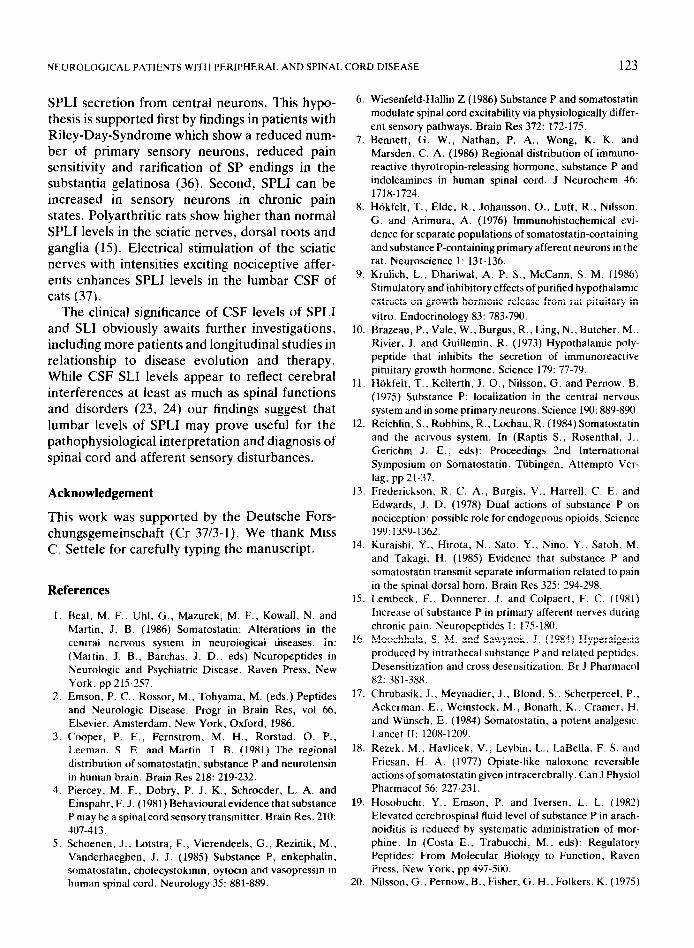
The results of the fractionated sampling are shown in Table 2 and the figure. No gradient for SLI was found, while levels of SPLI decreased significantly from the first to the last fraction parallel tot the diminution of total protein and IgG concentrations. In contrast, a positive concentra- tion gradient appeared for HVA and 5-HIAA.
Discussion
SPLI and SLI levels of control patients in this study are similar to those reported earlier (19-22,24,27,

122 N~~~KOPEPTIDES
SLI
ET SPLI
“Y I II 111 FRACTION
Figure Comparison of metabolite levels in successive frac- tions (8-10ml each) of CSF (fraction I = 100%) in patients of group V. Substance P-like immunoreactivity = SPLI, somato- statin-like immunoreactivity = SLI, total protein = PROT. immunoglobulin G = IGG, homovanillic acid = HVA. 5- hydroxyindoleacetic acid = 5-HIAA.
28). Several lines of evidence suggest that SPLI and SLI i.n the CSF are related to SPLI and SLI in nervous structures. Nilsson et al. (21) found no relationship between plasma and CSF concentra- tions of SPLI, Meisenberg et al. (29) observed no SLI gradients between blood and CSF, and Lund- qvist et al. (30) found CSF SLI unchanged when high doses of somatostatin were infused iv. Since CSF in general is virtually devoid of peptide degrading enzymes (1) the pattern of immunoreac- tivity in the CSF hypothetically reflects directly the pattern of the immunoreactivity released from nervous tissue.
Although numerous studies have shown stimu- lus dependent release of SP and SST from nervous tissue in vitro, there is little known about the sites of entry of these neuropeptides into the CSF. The absence of a crania-caudad CSF gradient for SLI, confirmed in this study, has suggested that SLI is released diffusely from the central nervous system (23). As for SPLI Nutt et al. (28) were unable to demonstrate a concentration gradient in human CSF while Hosobuchi et al. (19) found that cisternal SPLI levels were lower than lumbar levels in patients with arachnoiditis and chronic back pain. In this study we compared SPLI and SLI levels of consecutive CSF fractions systematically
with levels of two monoamine metabolites well known for their predominantly supraspinal origin and positive lumbar-cisternal concentration gradi- ents (31-34) and with total protein and IgG content which show consistently higher levels in caudal segments of the CSF space (35). The uncovered gradient for SPLI which is similar to that of protein and IgG deserves further comment. Since a greater concentration of proteins in the lumbar sac as compared to the cisternal and ventricular levels in explained by the greater blood-CSF perme- ability of albumin in the former compartment (8) the similar gradient for SPLI could be the result of SPLI transport from blood into CSF. A contribu-
tion of extraneuronal SPLI to CSF levels, thus, cannot be excluded and could be supported by the fact that SP is less water soluble than somatostatin and might penetrate blood-CSF barriers and get enriched in the CSF by a trapping mechanism. However, as mentioned, no correlation between plasma and CSF SPLI concentrations was ob- served and plasma SPLI did not co-chromatograph with substance P (21). Moreover, in this study. no correlation between CSF SPLI and total protein was observed in lumbar CSF. Therefore, a more marked release of SPLI from caudal segments of the spinal cord and spinal ganglia, compared to more cranial segments, remains an alternative explanation of the observed gradient, deserving further studies.
The increased levels of lumbar SPLI in patients with spinal cord disease and peripheral nervous disease including polyneuropathy and lumbois- chialgia suggests an increased release of SPLI form nervous tissues in these conditions. High SPLI levels in our patients with polyneuropathy are in contrast to the results of Nutt et al. (28) who found decreased SPLI levels in this disease. This discrep- ancy may be due in part to differences of technique and difference of patient selection. In Nutt’s study three of nine patients showed SPLI values below the detection limit of their assay system. 7 of the 9 patients had decreased pain perception and hyper- algesia was reported in none. However, in our study at least 5 of 13 patients with polyneuropathy and all patients with lumboischialgia complained of painful sensations. Hypothetically, hypalgesia due to spinal deafferentiation might decrease CSF SPLI, whereas hyperalgesia may cause increased
NF-UR~L~OICALPATIENTSWITHPERIPHERALANDSPINALC~RD DISEASE 123
SPLI secretion from central neurons. This hypo- thesis is supported first by findings in patients with Riley-Day-Syndrome which show a reduced num- ber of primary sensory neurons, reduced pain sensitivity and rarification of SP endings in the substantia gelatinosa (36). Second, SPLI can be increased in sensory neurons in chronic pain states. Polyarthritic rats show higher than normal SPLI levels in the sciatic nerves, dorsal roots and ganglia (1.5). Electrical stimulation of the sciatic nerves with intensities exciting nociceptive affer- ents enhances SPLI levels in the lumbar CSF of cats (37).
The clinical significance of CSF levels of SPLI and SLI obviously awaits further investigations, including more patients and longitudinal studies in relationship to disease evolution and therapy. While CSF SLI levels appear to reflect cerebral interferences at least as much as spinal functions and disorders (23, 24) our findings suggest that lumbar levels of SPLI may prove useful for the pathophysiological interpretation and diagnosis of spinal cord and afferent sensory disturbances.
Acknowledgement
This work was supported by the Deutsche Fors- chungsgemeinschaft (Cr 37/3-l). We thank Miss C. Settele for carefully typing the manuscript.
References
1.
2.
3.
4.
5.
Beal, M. F.. Uhl. G., Mazurek, M. F., Kowall. N. and Martin, J. B. (1986) Somatostatin: Alterations in the central nervous system in neurological diseases. In: (Martin. J. B., Barchas. J. D., eds) Neuropeptides in Neurologic and Psychiatric Disease. Raven Press, New York. pp 215-257. Emson, P. C., Rossor, M., Tohyama, M. (eds.) Peptides and Neurologic Disease. Progr in Brain Res, vol 66. Elsevier. Amsterdam, New York, Oxford, 1986. Cooper, P. E., Fernstrom, M. H., Rorstad. 0. P., Leeman, S. E. and Martin, J. B. (1981) The regional distribution of somatostatin, substance P and neurotensin in human brain. Brain Res 218: 219-232. Piercey, M. F., Dobry, P. J. K., Schroeder, L. A. and Einspahr, F. J. (1981) Behavioural evidence that substance P may be a spinal cord sensory transmitter. Brain Res. 210: 407-413. Schoenen, J., Lotstra, F., Vierendeels, G., Rezinik, M., Vanderhaeghen, J. J. (1985) Substance P, enkephalin, somatostatin. cholecystokinin, oytocin and vasopressin in human spinal cord. Neurology 35: 881-889.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
Wiesenfeld-Hallin 2 (1986) Substance P and somatostatin modulate spinal cord excitability via physiologically differ- ent sensory pathways. Brain Res 372: 172-175. Bennett, G. W., Nathan, P. A., Wong, K. K. and Marsden. C. A. (1986) Regional distribution of immuno- reactive thyrotropin-releasing hormone, substance P and indoleamines in human spinal cord. J Neurochem 46: 1718-1724. Hokfelt. T., Elde. R., Johansson, O., Luft, R., Nilsson. G. and Arimura, A. (1976) Immunohistochemical evi- dence for separate populations of somatostatin-containing and substance P-containing primary afferent neurons in the rat. Neuroscience 1: 131-136. Krulich, L., Dhariwal, A. P. S., McCann, S. M. (1986) Stimulatory and inhibitory effects of purified hypothalamic extracts on growth hormone release from rat pituitary in
vitro. Endocrinology 83: 783-790. Brazeau, P.. Vale, W., Burgus, R., Ling, N.. Butcher, M.. Rivier, J. and Guillemin, R. (1973) Hypothalamic poly- peptide that inhibits the secretion of immunoreactive pituitary growth hormone. Science 179: 77-79. Hokfelt, T.. Kellerth, J. O., Nilsson, G. and Pernow. B. (1975) Substance P: localization in the central nervous system and in some primary neurons. Science 190: 889-890. Reichlin, S., Robbins, R., Lochau. R. (1984) Somatostatin and the nervous system. In (Raptis S., Rosenthal, J.. Gerichm J. E., eds): Proceedings 2nd International Symposium on Somatostatin. Tiibingen, Attempt0 Ver- lag, pp 21-37. Frederickson. R. C. A., Burgis, V., Harrell. C. E. and Edwards, J. D. (1978) Dual actions of substance P on nociception: possible role for endogenous opioids. Science 199:1359-1362. Kuraishi. Y., Hirota, N., Sato, Y., Nino. Y.. Satoh. M. and Takagi. H. (1985) Evidence that substance P and somatostatin transmit separate information related to pain in the spinal dorsal horn. Brain Res 325: 294-298. Lembeck. F., Donnerer. J. and Colpaert. F. C. (1981) Increase of substance P in primary afferent nerves during chronic pain. Neuropeptides 1: 175-180. Moochhala, S. M. and Sawynok. J. (1984) Hyperalgesia produced by intrathecal substance P and related peptides. Desensitization and cross desensitization. Br J Pharmacol 82: 381-388. Chrubasik. J.. Meynadier. J., Blond. S.. Scherpereel. P., Ackerman. E.. Weinstock, M., Bonath, K.. Cramer. H. and Wunsch. E. (1984) Somatostatin. a potent analgesic. Lancet II: 1208-1209. Rezek. M.. Havlicek, V., Leybin. L.. LaBella, F. S. and Friesan. H. A. (1977) Opiate-like naloxone reversible actions of somatostatin given intracerebrally. Can J Physiol Pharmacol 56: 227-231. Hosobuchi, Y., Emson. P. and Iversen, L. L. (1982) Elevated cerebrospinal fluid level of substance P in arach- noiditis is reduced by systematic administration of mor- phine. In (Costa E.. Trabucchi. M.. eds): Regulatory Peptides: From Molecular Biology to Function, Raven Press, New York, pp 497-500. Nilsson. G., Pernow. B., Fisher. G. H.. Folkers. K. (1975)

124 NELIKOPEPTIDES
Presence of substance P-like immunoreactivity in plasma from man and dog. Acta Physiol Stand 94: 542-544.
21. Nilsson. G., Pernow, B., Fisher, G. H. and Folkers. K. (1977) Radioimmunological determinations of substance P. In (v Euler. U. S., Pernow. B., eds): Substance P. Raven Press. New York. pp 41-48.
22. Rubinow, D. R.. Gold. P. W., Post, R. M., Ballenger, J. C. and Cowry, R. W. (1984) Somatostatin in patients with affective illness and in normal volunteers. In (Post R. M., Bellenger, J. C., eds): Neurobiology of Mood Disorders, Williams and Wilkins, Baltimore/London, pp 369-387.
23. Soerensen, K. V., Christensen, S. E., Hansen, A. P., Ingerslev, J., Pedersen, E. and Orskov, H. (1981) The origin of cerebrospinal fluid somatostatin: hypothalamic or disperse central nervous system secretion? Neuroendo- crinology 32: 335-338.
24. Cramer, H., Schaudt. D., Rissler, K., Strubel, D., Warter, J. M. and Kuntzmann. F. (1985) Somatostatin-like immu- noreactivity and substance P-like immunoreactivity in the CSF of patients with senile dementia of Alzheimer type, multinfarct syndrome and communicating hydrocephalus. J Neuro1232: 346-351.
25. Rissler, K., Cramer, H., Schaudt, D., Strubel, D. and Gattaz, W. F. (1986) Molecular size distribution of soma- tostatin-like immunoreactivity in the cerebrospinal fluid of patients with degenerative brain disease. Neurosci Res. 3: 213-225.
26. Gagnieu, M. C., Menouini-Foray, V., Guardiola, P.. Quincy, R. and Renaud, B. (1984) Liquid chromatogra- phic determination of homovanillic acid, 5-hydroxyindo- leacetic acid and probenecid levels in human cerebrospinal fluid during probenecid test. Clin Chim Acta 139: l-12.
27. Henning, K., Wallasch, T. H. M.. Przuntek, H. (1986) Determination of beta-endorphin and substance P in small volumes of human cerebrospinal fluid. J Neural Transm 67: 105-112.
28. Nutt, J. H.. Mroz, E. A.. Leeman, S. E., Williams, A. C..
Engel. W. K. and Chase. T. N. (lY80) Substance P in human cerebrospinal fluid: Reductions in peripheral neuropathy and autonomic dysfunction. Neurology 30: 1280-1285.
29. Meisenberg, G. and Simmons. W. H. (1983) Minireview. Peptides and the blood-brain-barrier. Life Sci 32: 261 I- 2623.
30. Lundqvist, G., Gustavsson, S.. Elde. R., Arimura, A.. (1980) A radioimmunosorbent assay for plasma somato- statin. Clin Chim Acta 101: 183-191.
31. Garelis, E. and Sourkes. T. L. (1973) Sites of origin in the central nervous system of monoamine metabolites measured in human cerebrospinal fluid. J Neural Neuro- surg Psychiat 36: 625-629.
32. Portig. P. J. and Vogt. M. (1969) Release to the cerebral ventricles of substances with possible transmitter function in the caudate nucleus. J Physiology 204: 687-715.
33. Post, R. M., Goodwin, F. K.. Gordon. E. and Watkin. D. M. (1973) Amine metabolites in human cerebrospinal fluid: Effects of cord transection and spinal block. Science 179: 897-899.
34. Wood, J. H. (1980) Sites of origin and concentration gradients of neurotransmitters, their metabolites and cyclic nucleotides in cerebroapinal fluid. In (Wood, J. H.. ed): Neurobiology of Cerebrospinal fluid. I. Plenum Publishing Corporation, New York. pp. 53-62.
35. Fishman. R. A., Ransohoff, J.. Ossermann, E. F. (1958) Factors influencing the concentration gradient of protein in cerebrospinal fluid. J Clin Invest 37: 1419-1424.
36. Pearson. J.. Brandeis, L. and Cuello, A. C. (1982) Depletion of substance P-containing axons in substantia gelatinosa of patients with diminished pain sensitivity. Nature 295: 61-63.
37. Jessel1.T. M.. Mudge. A. W., Leemann. S. E. andYaksh. T. L. (1979) Release of substance P and somatostatin. in vivo, from primary afferent terminals in mammalian spinal cord. Proc Sot Neurosci 5. 611.





























