Embed Size (px)
Citation preview

Hindawi Publishing CorporationComputational and Mathematical Methods in MedicineVolume 2013 Article ID 472564 9 pageshttpdxdoiorg1011552013472564
Research Article
CFD Modelling of Abdominal Aortic Aneurysm onHemodynamic Loads Using a Realistic Geometry with CT
Eduardo Soudah1 E Y K Ng2 T H Loong3
Maurizio Bordone1 Uei Pua3 and Sriram Narayanan3
1 Centre Internacional de Metodes Numerics en Enginyeria Biomedical Engineering DepartmentTechnical University of Catalonia CGran Capita sn 08034 Barcelona Spain
2 School of Mechanical and Aerospace Engineering Nanyang Technological University 50 Nanyang Avenue Singapore 6397983Department of General Surgery Tan Tock Seng Hospital 11 Jalan Tan Tock Seng Singapore 308433
Correspondence should be addressed to E Y K Ng mykngntuedusg
Received 2 November 2012 Revised 17 May 2013 Accepted 1 June 2013
Academic Editor Eun Bo Shim
Copyright copy 2013 Eduardo Soudah et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
The objective of this study is to find a correlation between the abdominal aortic aneurysm (AAA) geometric parameters wallstress shear (WSS) abdominal flow patterns intraluminal thrombus (ILT) and AAA arterial wall rupture using computationalfluid dynamics (CFD) Real AAA 3Dmodels were created by three-dimensional (3D) reconstruction of in vivo acquired computedtomography (CT) images from 5 patients Based on 3D AAA models high quality volume meshes were created using an optimaltetrahedral aspect ratio for the whole domain In order to quantify the WSS and the recirculation inside the AAA a 3D CFD usingfinite elements analysis was used The CFD computation was performed assuming that the arterial wall is rigid and the blood isconsidered a homogeneous Newtonian fluid with a density of 1050 kgm3 and a kinematic viscosity of 4 times 10minus3 Pasdots Parallelizationprocedures were used in order to increase the performance of the CFD calculations A relation between AAA geometric parameters(asymmetry index (120573) saccular index (120574) deformation diameter ratio (120594) and tortuosity index (120576)) and hemodynamic loads wasobserved and it could be used as a potential predictor of AAA arterial wall rupture and potential ILT formation
1 Introduction
Most of abdominal aortic aneurysms (AAA) (about 90) arelocated below the level of the renal arteries and are knownas infrarenal aortic aneurysms Infrarenal aortic aneurysmis a pathological enlargement of the aorta in the inferiorthoracic area taking a fusiform shape and may extend intothe iliac arteries The mortality of this pathology is high(15 for ruptured aneurysms) and the current standard ofdetermining rupture risk is based on the anteroposteriordiameter It is known that smaller AAAs that fall below thethreshold of 55 cm diameter may also rupture and yet largerAAAs (diameter gt 55 cm)may remain stable [1ndash3] Howeveroccasionally the AAA diameter is lower than 5 cm and anunexpected ruptured is produced [4] in these cases otherbiomechanical factors [5ndash8] such asWall Shear Stress (WSS)
or geometrical factors [9ndash12] can play an important role in therupture of the aneurysm
To estimate the AAA rupture risk from a biomechanicalpoint of view (material failure) an aneurysm ruptures whenthe stresses acting on the arterial wall exceed its failurestrength According to Laplacersquos law the wall stress on anideal cylinder is directly proportional to its radius andintraluminal pressure Even though an AAA is not an idealcylinder Laplacersquos law still applies and with an increasingaortic diameter the internal pressure increases and so doesthe risk of rupture The increase in internal pressure againstthe aortic walls results in progressive growth of the AAAdiameter and eventually this pressure may overcome theresistance of the aortic wall resulting in rupture [1 2] On theother hand abnormal flow patterns and recirculation developin the AAA sac leading to the formation of the intraluminal
2 Computational and Mathematical Methods in Medicine
thrombus (ILT) [6 13] This phenomenon can provoke theAAA stabilization and start a vicious circle inside the AAA[14] It is reflected by the interaction between the arterial wallstructural remodeling and the forces generated by blood flowwithin the AAA [2 13]Therefore it is apparent that LaplacersquosLaw is insufficient when investigating AAA collapsibilityRather the aneurysm shape has a strong influence on flowpatterns ILT formation wall stress distribution (peak valuesand locations) and consequently its potential rupture [1 15]
The aim of this study is to analyze and to characterize theeffect of wall shear stress and the internal pressure togetherwith the main AAA geometric parameters (maximum diam-eter (119863AMAX) length (119871AAA) AAA proximal neck diameter(119889proximal neck) tortuosity (120576) and asymmetry (120573)) in order toassess its potential rupture Five patient-specific AAAmodelswere created from CT scans A normal descending aorta wasalso simulated to provide a comparison
2 Material and Methods
Five patients with infrarenal aneurysms on followup at TanTock Seng Hospital (Singapore) were included in this studyThe patients chosen for this study were selected with differentsized AAAs in order to cover the different stages of thispathology All the patients participated in this trial analysisvolunteered and provided written informed consent of thestudy This study was reviewed and approved by the EthicsCommittee of the Tan Tock Seng Hospital Singapore Forthe medical image acquisition a computed tomography (CT)Somatom Plus Scanner (AS+) (Siemens Medical Solutions)was used with the following parameters 512 times 512 times 110 pixelspacing 07850785 with a resolution of 1274 pixels per mmand 5mm slice thickness CT scanning was conducted whilethe volunteer was awake in the head first-supine positionusing an endoleak protocol The CT covered the entireabdomen and pelvis and was performed after the administra-tion of intravenous Omnipaque 350 as IV contrast medium
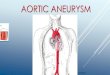
To characterize the structure of the AAA the maingeometrical AAAparameters aremeasured aneurysm length(119871AAA) and maximum diameter of the aneurysm (119863AMAX)(Figure 1(a))The factor which assesses the length (119871AAA) andthe diameter (119863AMAX) of the AAA sac is known as saccularindex (120574) (1) [16] If the saccular index is close to 1 theaneurysm is saccular (spherical) but if it is close to 0 theaneurysm is more fusiform The deformation diameter rate(120594) (1) [17] characterizes the nondeformed abdominal aortadiameter (119889proximal neck) with the maximum diameter of theaneurysm sac 119863AMAX A nonaneurysmal aorta is defined as(119863AMAX = 119889neck)
120573 = 119903119877
120574 = 119863AMAX119871AAA
120594 = 119863AMAX119889proximal neck
120576 = 119871120591 minus 1
(1)
To evaluate the asymmetry (120573) [18] of the aneurysm (1) 119903and 119877 are defined as the radii measured at the midsectionof the AAA sac from the longitudinal 119911-axis to the posteriorand anterior walls respectively as shown in the inset ofFigure 1(b) Thus 120573 = 10 yields an azimuthal symmetryand 120573 = 02 is an AAA for which only the anterior wall isdilated while the posterior wall is nearly flat The tortuosityindex (120576) (1) [19] is the relation between the actual lengths ofthe centerline of the AAA with the length of a hypotheticalhealthy aorta (Figure 1 center)
Based on these indexes and the wide clinical empiricalevidence there are several criteria of the AAA grade How-ever at present there is no clinical consensus to use it Table 1shows the main AAA geometrical characteristics for eachpatient in our study
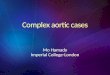
To create the computationalmodel themedical data weresent directly to a personal computer and stored in DigitalImaging and COmmunications inMedicine format (DICOMformat) Figure 2 shows the segmentation workflow Theregion of interest (ROI) analyzed was segmented using thethree-dimensional computer-aided design system DIPPOsoftware [20] The segmented area for each patient startedat the abdominal aorta (approximately in the infra renalarteries) and extended down to the common iliac arteries(Figure 2) The abdominal images were segmented fromCT DICOM images combining two different segmentationprocedures thresholding and level set method (based onsnakes)Thresholding is a nonlinear operation that converts agray-scale image into a binary image where the two levels areassigned to pixels that are below or above the specified thresh-old value The image snake operation creates or modifiesan active contoursnake in a greyscale image The operationiterates to minimize the snakersquos energy which consists ofmultiple components including the length of the snake itscurvature and image gradient [21]
After AAA segmentation we get a 3D volume imageuseful to create a 3D computational model to analyze theblood flow behavior inside the AAA using computationalfluid dynamics (CFD) A mesh sensitivity analysis was per-formed to ensure the accuracy of the simulations using steadytest Depending on the complexity of the AAA model a 3Dmesh consisted of 2000000ndash2500000 tetrahedral elementsUsing the isosurface stuffing algorithm [22] we have obtaineda smooth element and an aspect radio for the whole of themeshes higher than 09 (ideal ratio = 1 for an equilateraltriangle) For the five acquisitions the same medical imageprotocol image processing and volumemesh reconstructionwere used
3 Computational Fluid Mechanics Solver
CFD analysis was performed using BioDyn a friendly userinterface based on the commercial software Tdyn [23] Tdynis a fluid dynamics andmultiphysics simulation environmentbased on the stabilized finite element method that solvedthe Navier-Stokes equations To characterize accurately theblood flow in the AAA a Reynolds number was calculatedfor whole cases Reynolds number is a dimensionless numberthat determinates the dynamic of the fluid Reynolds number
Computational and Mathematical Methods in Medicine 3
Table 1 Patient and AAA geometrical characteristics (119871 120591 119889proximal neck 119903 119877 119863AMAX and LAAA) and all the measurements are expressed incentimeter AAA geometrical indexes (120573 120574 120594 and 120576)
Case SexThoracic aortalength (119871)
Hypotheticthoracic aortalength (120591)
AAA proximalneck
(119889proximal neck)
119903 119877 AAA maxdiameter(119863AMAX)
AAA length(LAAA)
120594 120573 120574 1205761 Male 35994 32044 28 149 245 3945 67 1408 0608 0588 0123
2 Male 3195 3102 17 067 174 2416 41 1421 0388 0589 0029
3 Male 21628 1768 26 102 203 3056 898 1176 0508 0340 0223
4 Male 29355 25526 26 095 307 4031 156 155 0309 0258 0150
5 Male 31034 29624 25 125 125 25 mdash 1 1 mdash 0047
dabdominal_aorta
dproximal neck
ddistal neck
DAMAX
LAAA
L
(a)
R
r
Midsection (DAMAX )
(b)
Figure 1 (a) Main geometrical parameters 119871AAA aneurysm length 119863MAX maximum diameter of the aneurysm 119889proximal neck beginning of theAAA sac 119889distal neck ending of the AAA sac 119889abdominal aorta nondeformed abdominal aorta diameter 119871 is the absolute length of the tortuousvessel and 120591 is the imaginary straight line (b) Schematic visualization of a cross-sectional AAA section where 119903 and 119877 are defined as theradii measured at the midsection of the AAA sac from the longitudinal z-axis to the posterior and anterior walls
is defined as Re = 119880119863] where 119880 is the mean velocity ]is the kinematic viscosity of air and 119863 is the characteristiclength given as the hydraulic diameter 119863 = 4119860119875 for theinlet velocity and here 119860 is the cross-sectional area and 119875 isthe perimeter of the aorta Because the Reynolds number ininlet is low (lt1000) we decided to use a CFD solver for lam-inar flow considering steady homogeneous incompressibleadiabatic and Newtonian fluid However three-dimensionalflow features such as flow separation and recirculation mighttrigger a transition to turbulence at lower Reynolds numbers[9] Based on a preliminary study [6] the effect of theturbulence has been considered to be negligible Followingwe show the Navier-Stokes equations (2)
120588 (120597119906120597119905 + (119906 sdot nabla) 119906) + nabla119901minusnabla sdot (120583nabla119906) = 120588119891 in Ω times (0 119905)
nabla sdot 119906 = 0 in Ω times (0 119905) (2)
where 119906 = 119906(119909 119905) denotes the velocity vector 119901 = 119901(119909 119905) thepressure field and the density (120588) is considered constant with
a value of 1050Kgsdotmminus3 and dynamic viscosity (]) fixed at0004 Pasdots and 119891 the volumetric acceleration The spatial dis-cretization of the Navier-Stokes equations has been done bymeans of the finite elementmethod (FEM) while for the timediscretization an iterative algorithm that can be consideredas an implicit two steps fractional step method has beenused A new stabilisation method known as finite incrementcalculus has recently been developed [24] By considering thebalance of flux over a finite sized domain higher order termsnaturally appear in the governing equations which supply thenecessary stability for a classical Galerkin finite element dis-cretization to be used with equal order velocity and pressureinterpolations The inlet velocity waveform was taken fromthe literature [25] andFigure 3 shows the pulsatilewaveformsused For inlet condition a transient blood flow was imposedin the descendent abdominal aorta The velocity 119880 wascalculated for each patient in order to obtain a total fluidvolumetric flow rate of 500mL for an entire cardiac cycleTheoutlet boundaries were located at the common iliac arterieswhere the pressure follows pulsatile waveforms as defined
4 Computational and Mathematical Methods in Medicine
Figure 2 Workflow of the 3D AAAmodel Obtaining the CT image of the abdominal aorta segmentation of the vessel lumen using thresh-olding and level set method and 3D model of the AAA
in Figure 4(b) It is important to remark that these profilesare not patient-specific data (MR velocity mapping was notperformed on these subjects) which can be a limitation ofthis study In further studies a patient-specific velocity andpressure profile will be used as boundary conditions
Mathematically the boundary conditions can be ex-pressed as in (3a) (3b) and (3c) No-slip condition (vesselrigid wall) was imposed on the surface of the arteries (3a)This choice is motivated by the fact that the physiologicalparameters characterizing the arterial mechanical behaviourof the AAA wall are not well determined This approachhowever reduces the discretization effort considerably inparticular boundary layer gridding and the computationalcost although other approaches consider fluid structureinteraction (FSI) models [13 25ndash28] The inlet velocity isassumed to fully developed their parabolic profile at the inlet(3b) and time-dependent normal traction due to luminalpressure at the outlet (3c) as
119881 = 0 1003816100381610038161003816wall (3a)
119906119911 = 2 (119906 (119905)) (1 minus ( 2119903119889119903 )2) 119906119903 = 01003816100381610038161003816119911=0 (3b)
120591119899119899 = 119899 sdot 119901 (119905) 119868 sdot 119899 (3c)
where 119889119903 is the inner radius of the abdominal aorta 119906119903 isthe Cartesian component of the velocity vector in the ldquo119911rdquodirection and 119906(119905) and 119901(119905) are the time-dependent velocityand pressure waveforms designated in Figure 3 The pressureboundary conditions are given by (3c) where 120591119899119899 is thenormal traction designates at the outlet 119868 is the standardidentity matrix and 119899 designates the normal of the respectiveboundary Figure 4 shows case 4 of the AAA reconstructedmodel and the layers in which our domain is divided in orderto impose the boundary conditions
4 Results
Five models of infrarenal aneurysm with patient-specificgeometry were analyzed using computational fluid dynamicsin order to evaluate the flow patterns wall shear stress andpressure over the aneurysm sac Patients 1 to 4 had infrarenalaneurysms whilst patient 5 is the control case ILT was notfound in any case The unsteady flow simulations were per-formed through twopulsatile cycles to eliminate the influenceof initial transients The results of pressure stress and flow
patterns are shown for the peak systole (02 s) of the secondcardiac cycle
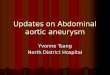
Figure 5 shows the flow patterns velocity streamlinesinside the infrarenal aneurysms sac and three cross-sectionalareas of the AAA (proximal midsection and distal neck)for the five patients studied Note that forward flow pointsdownwards and has a negative value in the adopted coordi-nate system The direction of the flow is from top to bottom(direction 119885 negative) We notice that when the AAA hasasymmetry the velocity streamlines correspondingly showan asymmetric flow pattern inside the AAA sac As shownin [6 7 26 29] the asymmetric flow patterns can providean insight into the mechanism that promotes the thrombusrenewal and possibly enlargement inside the aneurysmRapid decrease in the velocity and regions of very high(or low) hemodynamic stresses gradients may all contributein various ways to the vascular disease primarily via theireffects on the endothelium For example platelets trappedin recirculation zones tend to be deposited in areas of lowshear stress (stenosis) [14] since this and the presence ofvortices cause prolonged contact of the platelets with thesurface in the layer of slow fluid motion [6 19] This effectcan be observed for the pathological cases however in case 4we observe a flow recirculation in the middle section and theasymmetry is low Consequently the flow patterns of theaneurysmnot only depend of the asymmetry of the aneurysmbut also depend of the AAA tortuosity Details of the flowpatterns for the AAAs is shown in Figure 5 (cross-sectionalareas column) From the top to the bottom neck sectionmidsection (maximum diameter in the aneurysm sac) anddistal section We notice that the tortuosity of the AAAprovokes an asymmetric flow patterns in the AAA sac When120576 is high we observe that in the AAA proximal neck sectionthere is a strong irregular flow causing also an irregular flowin the AAA sac meanwhile when 120576 is low this effect doesnot appear From these findings the greater the asymmetryand tortuosity of the AAA the higher the possibility of bloodrecirculation ILT formation and a possible rupture Thusthe importance of geometry in the hemodynamic behaviorof AAAs is supported
Anterior and posterior wall shear stress views are shownin Figure 6 as well as the pressure on the aneurysm sac atthe peak systole The mean WSS in the aneurysm sac of the5 patients varied between 028 (case 5) and 1272 Pa (case 4)with a median of 352 Pa and mean of 574 Pa The areas withWSS values under the mean value have been classified as low
Computational and Mathematical Methods in Medicine 5
09
08
07
06
05
04
03
02
01
00908070605040302010
Time (s)
Vel
oci
ty (
ms
)Inlet velocity prole
(a)
0908070605040302010
Time (s)
16
15
14
13
12
11
10
Pre
ssu
re (
Pa)
Outlet pressure proletimes103
(b)
Figure 3 Boundary conditions for the hemodynamic simulations adapted from [11]
Inlet (descending aorta)
xz y
(a)
Outlet(iliac arteries)
Aortic wall(AAA sac)
x
zy
(b)
Figure 4 Mesh surface different layers are shown aortic wall (dark blue) and inlet (purple) and outlet sections (light blue)
WSS areas (blue) and areas with WSS values higher than themean value as high WSS (red) Analysis of WSS maps forall cases shows that the area of low WSS coincides with thelocation of the recirculation areas (low velocities) and higherWSS values are found in two regions in the neck area and inthe corresponding areawhere the bloodflow jet has an impacton the aneurismal sac The blood flow jet has an impactdirectly on the arterial wall producing higherWSS valuesTheblood flow jet path is provoked by the proximal neck angleconsequently by the AAA tortuosity (see Figure 5) TheseWSS peak values do not influence too much in aneurysmgrowth however in these areas a material failure could beproduced provoked by blood flow jet It is interesting to notethat shear stress levels in all infrarenal aneurysms models arehigher than those in the normal aorta where 120576 is low whichhas a fairly uniform stress shear spatial distributionMaximalvalues are found in the neck region where 120576 is high
Due to the increasing of the internal pressure againstthe aortic walls the AAA diameter grows progressively andeventually it could be able to overcome the resistance of theaortic wall with its breakup This internal pressure is directlyproportional with the aneurysm diameter thereby when thediameter grows the pressure increases High deformationdiameter rate (120594) index could indicate higher internal pres-sure however it should be noticed that the pressure also
depends on the tortuosity index (inversely proportional) andthe flow characteristics (see Figure 5) For instance in case 4even when the section diameter is large the internal pressureis lower than that in case 2 This is originated by a notablypressure drop as a result of the vorticity and flow recirculation(energy losses) in the cases with a high tortuosity index Thiseffect also provokes a pressures gradient between the anteriorand posterior arterial wall in the interior of the AAA sacThese internal high pressure areas inside the sac may indicatethe growth directions of AAA sac
5 Discussions
The objective of this study is to use patient-specific AAAmodels for correlating the geometric indices of the aneurysmwith the hemodynamic loads and eventually with thepotential risk of AAA rupture From a mechanical point ofview AAA ruptures when a maximum stress value over thewall is exceeded The stress peak refers to the mechanicalload sustained by the AAA wall during maximal systolicpressurization In addition it is known that wall stress alonedoes not completely govern failure as an AAA will usuallyrupture when the wall stress exceeds the wall strength Itsvalue depends on arterial systolic pressure the mechanicalproperties and the geometric configuration of the material
6 Computational and Mathematical Methods in Medicine
AAA streamlines AAA sac streamlines details
Cross- sectional
areas
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
3552131574276282368119734157871184
039468078936
0
4654133336167312583320667155103330516670
Cas
e 5
x yz
x yz
x yz
5573949546433523715930966247731858123860619320
x yz
x yz
60112534334675440075333952671620037133580667910
2522222194441666713889111110833330555560277780
|V|
Figure 5 Streamlines details of AAA sac streamline blood flowvelocity and three cross-sectional areas (from the top to the bottom proximalAAA neck and midsection and distal AAA neck) for the five patient studied
under study However the mechanism of arterial wall failuredue to (1) the AAA shape or (2) the pressure distribution isphysically different The first is because of a punctual forceover a wall point and the second is because a consequence
of a pressure distribution over the AAA wall Based on theAAA shape several authors have proposed different criteriafor the AAA collapsibility if the AAAdiameter is higher than55 cm [4] the AAA may rupture or if the asymmetry index
Computational and Mathematical Methods in Medicine 7
WSS anterior WSS posterior Pressure
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
Cas
e 5
High
Low
High
Low
High
Low
High
Low
High
Low
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
37000
37000
37000
37000
37000
33556301112666723222197781633312889944446000
x yz
Figure 6 Anterior and posterior wall shear stress views (high WSS in red and low WSS in blue) and normalized pressure on the aneurysmsac at the peak systole for the five patients
8 Computational and Mathematical Methods in Medicine
factor (120573) is 120573 lt 04 the AAA rupture is high [8] In [10]the AAA collapses when the deformation diameter ratio is120594 gt 33 or if the saccular index is lt06 [11] But depend-ing on the index that is analysed the surgical criteria aredifferent More recently the proposed AAA rupture risk isrelated with the presence of intraluminal thrombus (ILT)[6 26] The intraluminal thrombus plays an important rolein expansion and rupture of advanced aneurysms throughdirectmechanical as well as indirect chemomechanical effects[6] Therefore the AAA dilatation (and a potential rupture)is dependent on the correlation between the geometricalfactor and the hemodynamic load Consequently alternativemethods of AAA rupture assessment are needed
Themajority of these new approaches involve the numer-ical analysis of AAAs using computational fluid dynamics(CFD) to determine the wall shear stress (WSS) distributionsand flow patterns in the aneurysm sac [5 12 13 15 16 30]In our study we did not evaluate the patient-specific wallstrength or the effect of intraluminal thrombus Neverthe-less the AAA cases analyzed provide useful information tounderstanding how hemodynamic loads can affect aneurysmgrowth and possible rupture The pathological cases (cases 1to 4) always present irregular flow in the aneurysm sac nouniform distribution of WSSs and great WSS values in thecurvatures of the aortic vessel These anomalies are propor-tional to the shape of the aneurysm and the angles of twistthat the aorta has Asymmetric flow is always correlated to themodified curvature of the vessel or when some enlargementin the aneurysm is present (high saccular index (120574) andtortuosity (120576) index) The AAA tortuosity could initiate ILTformation and at the same time could provoke arterial wallfailure In a situation where the tortuosity is high and thesaccular index is low the WSS has more effects than thepressure distribution in a possible AAA failure Howeverwhere the AAA is not twisted and the saccular index is highthe pressure effect takes priority In Figure 6 the highest shearstress values are dependent especially on the tortuosity of theAAA The neck angle substantially impacts flow fields caus-ing strong irregular flow patterns in the AAA sac (Figure 5)significantly influencing wall stress distribution (Figure 6)The relationship between these indexes can provide an insightinto themechanism that promotes the thrombus renewal andpossibly enlargement inside the aneurysm
6 Conclusions
To conclude in this work the wall shear stress internalpressure and flow patterns of five patients-specific aortashave been analyzed using a finite element method and theresults have been correlated with the geometrical featuresResults from the patient-specific infrarenal aneurysmmodels(cases 1ndash4) were compared with those of a normal aorta (case5) and it has been found that the normal aorta has a uniformdistribution of the velocity streamlines wall shear stress andpressure compared to that in the pathological cases Maxi-mum wall shear stresses in all infrarenal aneurysm modelsare higher than those in the normal aorta and these valuesare not directly related to the maximum aneurysm diameterproviding evidence that a patient-specific aorta shape analysis
is necessary for a more reliable assessment of the rupturerisk of aortic aneurysms Therefore based on one or twosimple indexes alone to determine the risk of rupture accu-rately is insufficient AAA rupture is a complex situationdepending on themaximum diameter internal pressure wallstress asymmetry saccular index intraluminal thrombusand tortuosity among others Our results demonstrate howthe hemodynamic loads as simulated by computational fluiddynamics (CFD) are influenced by the geometrical factors ofthe aneurysm
Acknowledgment
This project was supported by the NTU-NHG InnovationSeed Grant Project no ISG11007
References
[1] D A Vorp ldquoBiomechanics of abdominal aortic aneurysmrdquoJournal of Biomechanics vol 40 no 9 pp 1887ndash1902 2007
[2] J D Humphrey Cardiovascular Solid Mechanics Cells Tissuesand Organs Springer New York NY USA 2002
[3] J T Powell L C Brown J F Forbes et al ldquoFinal 12-year follow-up of surgery versus surveillance in the UK Small AneurysmTrialrdquoBritish Journal of Surgery vol 94 no 6 pp 702ndash708 2007
[4] S CNicholls J BGardnerMHMeissner andKH JohansenldquoRupture in small abdominal aortic aneurysmsrdquo Journal ofVascular Surgery vol 28 no 5 pp 884ndash888 1998
[5] M L Raghavan and D A Vorp ldquoToward a biomechanical toolto evaluate rupture potential of abdominal aortic aneurysmidentification of a finite strain constitutivemodel and evaluationof its applicabilityrdquo Journal of Biomechanics vol 33 no 4 pp475ndash482 2000
[6] J Biasetti F Hussain and T Christian Gasser ldquoBlood flow andcoherent vortices in the normal and aneurysmatic aortas afluid dynamical approach to intraluminal thrombus formationrdquoJournal of the Royal Society Interface vol 8 no 63 pp 1449ndash1461 2011
[7] C M Scotti and E A Finol ldquoCompliant biomechanicsof abdominal aortic aneurysms a fluid-structure interactionstudyrdquo Computers and Structures vol 85 no 11ndash14 pp 1097ndash1113 2007
[8] D A Vorp M L Raghavan and M W Webster ldquoMechanicalwall stress in abdominal aortic aneurysm influence of diameterand asymmetryrdquo Journal of Vascular Surgery vol 27 no 4 pp632ndash639 1998
[9] E A Finol K Keyhani and C H Amon ldquoThe effect of asym-metry in abdominal aortic aneurysms under physiologicallyrealistic pulsatile flow conditionsrdquo Journal of BiomechanicalEngineering vol 125 no 2 pp 207ndash217 2003
[10] W A Cappeller H Engelmann S Blechschmidt M Wild andL Lauterjung ldquoPossible objectification of a critical maximumdiameter for elective surgery in abdominal aortic aneurysmsbased on one- and three-dimensional ratiosrdquo Journal of Cardio-vascular Surgery vol 38 no 6 pp 623ndash628 1997
[11] K Ouriel R M Green C Donayre C K Shortell J Elliott andJ A DeWeese ldquoAn evaluation of new methods of expressingaortic aneurysm size relationship to rupturerdquo Journal of Vas-cular Surgery vol 15 no 1 pp 12ndash20 1992
[12] T C Gasser M Auer F Labruto J Swedenborg and J RoyldquoBiomechanical rupture risk assessment of abdominal aortic
Computational and Mathematical Methods in Medicine 9
aneurysms model complexity versus predictability of finite ele-ment simulationsrdquo European Journal of Vascular and Endovas-cular Surgery vol 40 no 2 pp 176ndash185 2010
[13] M Bonert R L Leask J Butany et al ldquoThe relationshipbetween wall shear stress distributions and intimal thickeningin the human abdominal aortardquo BioMedical Engineering Onlinevol 2 article 18 2003
[14] D Bluestein L Niu R T Schoephoerster andM K DewanjeeldquoSteady flow in an aneurysm model correlation between fluiddynamics and blood platelet depositionrdquo Journal of Biomechan-ical Engineering vol 118 no 3 pp 280ndash286 1996
[15] M L Raghavan D A VorpM P Federle M S Makaroun andMWWebster ldquoWall stress distribution on three-dimensionallyreconstructed models of human abdominal aortic aneurysmrdquoJournal of Vascular Surgery vol 31 no 4 pp 760ndash769 2000
[16] C Kleinstreuer and Z Li ldquoAnalysis and computer programfor rupture-risk prediction of abdominal aortic aneurysmsrdquoBioMedical Engineering Online vol 5 article 19 2006
[17] J Shum G Martufi E di Martino et al ldquoQuantitative assess-ment of abdominal aortic aneurysm geometryrdquo Annals of Bio-medical Engineering vol 39 no 1 pp 277ndash286 2011
[18] D A Vorp P C Lee D H J Wang et al ldquoAssociation ofintraluminal thrombus in abdominal aortic aneurysm withlocal hypoxia and wall weakeningrdquo Journal of Vascular Surgeryvol 34 no 2 pp 291ndash299 2001
[19] D Bluestein K Dumont M de Beule et al ldquoIntraluminalthrombus and risk of rupture in patient specific abdominalaortic aneurysmmdashFSImodellingrdquoComputerMethods in Biome-chanics and Biomedical Engineering vol 12 no 1 pp 73ndash812009
[20] E Soudah J Pennecot J S Perez M Bordone and E OnateldquoMedical-GiD from medical images to simulations 4D MRIflow analysisrdquo in Computational Vision and Medical ImageProcessing Recent Trends chapter 10 Springer New York NYUSA 1871
[21] E Soudah M Bordone and J S Perez ldquoGmed a platform forimages treatment inside GiD systemrdquo in Proceedings of the 5thConference On Advances And Applications Of GiD Barcelona2010 GiDmdashthe personal pre and postprocessor httpwwwgidhomecom
[22] W E Lorensen and H E Cline ldquoMarching cubes a high reso-lution 3d surface construction algorithmrdquo in Proceedings of the14th Annual Conference on Computer Graphics and InteractiveTechniques (SIGGRAPH rsquo87) pp 163ndash169 1987
[23] M Bordone C Garcıa J Garcıa and E Soudah ldquoBiodyn UserManual TDYN theoretical Backgroundrdquo COMPASSIS 2012httpwwwcompassiscomcompass
[24] E Onate S Idelsohn O C Zienkiewicz and R L Taylor ldquoAfinite point method in computational mechanics Applicationsto convective transport and fluid flowrdquo International Journal forNumerical Methods in Engineering vol 39 no 22 pp 3839ndash3866 1996
[25] Y Papaharilaou J A Ekaterinaris E Manousaki and AN Katsamouris ldquoA decoupled fluid structure approach forestimating wall stress in abdominal aortic aneurysmsrdquo Journalof Biomechanics vol 40 no 2 pp 367ndash377 2007
[26] A-V Salsac S R Sparks J-M Chomaz and J C LasherasldquoEvolution of the wall shear stresses during the progressiveenlargement of symmetric abdominal aortic aneurysmsrdquo Jour-nal of Fluid Mechanics vol 560 pp 19ndash51 2006
[27] C M Scotti J Jimenez S C Muluk and E A Finol ldquoWallstress and flow dynamics in abdominal aortic aneurysms finite
element analysis vs fluid-structure interactionrdquo ComputerMethods in Biomechanics andBiomedical Engineering vol 11 no3 pp 301ndash322 2008
[28] A Borghia N B Wooda R H Mohiaddinb and X Y XualdquoFluid-solid interaction simulationof flow and stress pattern inthoraco abdominal aneurysms a patient-specific studyrdquo Journalof Fluids and Structures vol 24 pp 270ndash280 2008
[29] A Sheidaei S C Hunley S Zeinali-Davarani L G Raguinand S Baek ldquoSimulation of abdominal aortic aneurysm growthwith updating hemodynamic loads using a realistic geometryrdquoMedical Engineering and Physics vol 33 no 1 pp 80ndash88 2011
[30] T Hatakeyama H Shigematsu and T Muto ldquoRisk factors forrupture of abdominal aortic aneurysm based on three-dimen-sional studyrdquo Journal of Vascular Surgery vol 33 no 3 pp 453ndash461 2001
Submit your manuscripts at
httpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
Oxidative Medicine and
Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Parkinsonrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Computational and Mathematical Methods in Medicine
thrombus (ILT) [6 13] This phenomenon can provoke theAAA stabilization and start a vicious circle inside the AAA[14] It is reflected by the interaction between the arterial wallstructural remodeling and the forces generated by blood flowwithin the AAA [2 13]Therefore it is apparent that LaplacersquosLaw is insufficient when investigating AAA collapsibilityRather the aneurysm shape has a strong influence on flowpatterns ILT formation wall stress distribution (peak valuesand locations) and consequently its potential rupture [1 15]
The aim of this study is to analyze and to characterize theeffect of wall shear stress and the internal pressure togetherwith the main AAA geometric parameters (maximum diam-eter (119863AMAX) length (119871AAA) AAA proximal neck diameter(119889proximal neck) tortuosity (120576) and asymmetry (120573)) in order toassess its potential rupture Five patient-specific AAAmodelswere created from CT scans A normal descending aorta wasalso simulated to provide a comparison
2 Material and Methods
Five patients with infrarenal aneurysms on followup at TanTock Seng Hospital (Singapore) were included in this studyThe patients chosen for this study were selected with differentsized AAAs in order to cover the different stages of thispathology All the patients participated in this trial analysisvolunteered and provided written informed consent of thestudy This study was reviewed and approved by the EthicsCommittee of the Tan Tock Seng Hospital Singapore Forthe medical image acquisition a computed tomography (CT)Somatom Plus Scanner (AS+) (Siemens Medical Solutions)was used with the following parameters 512 times 512 times 110 pixelspacing 07850785 with a resolution of 1274 pixels per mmand 5mm slice thickness CT scanning was conducted whilethe volunteer was awake in the head first-supine positionusing an endoleak protocol The CT covered the entireabdomen and pelvis and was performed after the administra-tion of intravenous Omnipaque 350 as IV contrast medium
To characterize the structure of the AAA the maingeometrical AAAparameters aremeasured aneurysm length(119871AAA) and maximum diameter of the aneurysm (119863AMAX)(Figure 1(a))The factor which assesses the length (119871AAA) andthe diameter (119863AMAX) of the AAA sac is known as saccularindex (120574) (1) [16] If the saccular index is close to 1 theaneurysm is saccular (spherical) but if it is close to 0 theaneurysm is more fusiform The deformation diameter rate(120594) (1) [17] characterizes the nondeformed abdominal aortadiameter (119889proximal neck) with the maximum diameter of theaneurysm sac 119863AMAX A nonaneurysmal aorta is defined as(119863AMAX = 119889neck)
120573 = 119903119877
120574 = 119863AMAX119871AAA
120594 = 119863AMAX119889proximal neck
120576 = 119871120591 minus 1
(1)
To evaluate the asymmetry (120573) [18] of the aneurysm (1) 119903and 119877 are defined as the radii measured at the midsectionof the AAA sac from the longitudinal 119911-axis to the posteriorand anterior walls respectively as shown in the inset ofFigure 1(b) Thus 120573 = 10 yields an azimuthal symmetryand 120573 = 02 is an AAA for which only the anterior wall isdilated while the posterior wall is nearly flat The tortuosityindex (120576) (1) [19] is the relation between the actual lengths ofthe centerline of the AAA with the length of a hypotheticalhealthy aorta (Figure 1 center)
Based on these indexes and the wide clinical empiricalevidence there are several criteria of the AAA grade How-ever at present there is no clinical consensus to use it Table 1shows the main AAA geometrical characteristics for eachpatient in our study
To create the computationalmodel themedical data weresent directly to a personal computer and stored in DigitalImaging and COmmunications inMedicine format (DICOMformat) Figure 2 shows the segmentation workflow Theregion of interest (ROI) analyzed was segmented using thethree-dimensional computer-aided design system DIPPOsoftware [20] The segmented area for each patient startedat the abdominal aorta (approximately in the infra renalarteries) and extended down to the common iliac arteries(Figure 2) The abdominal images were segmented fromCT DICOM images combining two different segmentationprocedures thresholding and level set method (based onsnakes)Thresholding is a nonlinear operation that converts agray-scale image into a binary image where the two levels areassigned to pixels that are below or above the specified thresh-old value The image snake operation creates or modifiesan active contoursnake in a greyscale image The operationiterates to minimize the snakersquos energy which consists ofmultiple components including the length of the snake itscurvature and image gradient [21]
After AAA segmentation we get a 3D volume imageuseful to create a 3D computational model to analyze theblood flow behavior inside the AAA using computationalfluid dynamics (CFD) A mesh sensitivity analysis was per-formed to ensure the accuracy of the simulations using steadytest Depending on the complexity of the AAA model a 3Dmesh consisted of 2000000ndash2500000 tetrahedral elementsUsing the isosurface stuffing algorithm [22] we have obtaineda smooth element and an aspect radio for the whole of themeshes higher than 09 (ideal ratio = 1 for an equilateraltriangle) For the five acquisitions the same medical imageprotocol image processing and volumemesh reconstructionwere used
3 Computational Fluid Mechanics Solver
CFD analysis was performed using BioDyn a friendly userinterface based on the commercial software Tdyn [23] Tdynis a fluid dynamics andmultiphysics simulation environmentbased on the stabilized finite element method that solvedthe Navier-Stokes equations To characterize accurately theblood flow in the AAA a Reynolds number was calculatedfor whole cases Reynolds number is a dimensionless numberthat determinates the dynamic of the fluid Reynolds number
Computational and Mathematical Methods in Medicine 3
Table 1 Patient and AAA geometrical characteristics (119871 120591 119889proximal neck 119903 119877 119863AMAX and LAAA) and all the measurements are expressed incentimeter AAA geometrical indexes (120573 120574 120594 and 120576)
Case SexThoracic aortalength (119871)
Hypotheticthoracic aortalength (120591)
AAA proximalneck
(119889proximal neck)
119903 119877 AAA maxdiameter(119863AMAX)
AAA length(LAAA)
120594 120573 120574 1205761 Male 35994 32044 28 149 245 3945 67 1408 0608 0588 0123
2 Male 3195 3102 17 067 174 2416 41 1421 0388 0589 0029
3 Male 21628 1768 26 102 203 3056 898 1176 0508 0340 0223
4 Male 29355 25526 26 095 307 4031 156 155 0309 0258 0150
5 Male 31034 29624 25 125 125 25 mdash 1 1 mdash 0047
dabdominal_aorta
dproximal neck
ddistal neck
DAMAX
LAAA
L
(a)
R
r
Midsection (DAMAX )
(b)
Figure 1 (a) Main geometrical parameters 119871AAA aneurysm length 119863MAX maximum diameter of the aneurysm 119889proximal neck beginning of theAAA sac 119889distal neck ending of the AAA sac 119889abdominal aorta nondeformed abdominal aorta diameter 119871 is the absolute length of the tortuousvessel and 120591 is the imaginary straight line (b) Schematic visualization of a cross-sectional AAA section where 119903 and 119877 are defined as theradii measured at the midsection of the AAA sac from the longitudinal z-axis to the posterior and anterior walls
is defined as Re = 119880119863] where 119880 is the mean velocity ]is the kinematic viscosity of air and 119863 is the characteristiclength given as the hydraulic diameter 119863 = 4119860119875 for theinlet velocity and here 119860 is the cross-sectional area and 119875 isthe perimeter of the aorta Because the Reynolds number ininlet is low (lt1000) we decided to use a CFD solver for lam-inar flow considering steady homogeneous incompressibleadiabatic and Newtonian fluid However three-dimensionalflow features such as flow separation and recirculation mighttrigger a transition to turbulence at lower Reynolds numbers[9] Based on a preliminary study [6] the effect of theturbulence has been considered to be negligible Followingwe show the Navier-Stokes equations (2)
120588 (120597119906120597119905 + (119906 sdot nabla) 119906) + nabla119901minusnabla sdot (120583nabla119906) = 120588119891 in Ω times (0 119905)
nabla sdot 119906 = 0 in Ω times (0 119905) (2)
where 119906 = 119906(119909 119905) denotes the velocity vector 119901 = 119901(119909 119905) thepressure field and the density (120588) is considered constant with
a value of 1050Kgsdotmminus3 and dynamic viscosity (]) fixed at0004 Pasdots and 119891 the volumetric acceleration The spatial dis-cretization of the Navier-Stokes equations has been done bymeans of the finite elementmethod (FEM) while for the timediscretization an iterative algorithm that can be consideredas an implicit two steps fractional step method has beenused A new stabilisation method known as finite incrementcalculus has recently been developed [24] By considering thebalance of flux over a finite sized domain higher order termsnaturally appear in the governing equations which supply thenecessary stability for a classical Galerkin finite element dis-cretization to be used with equal order velocity and pressureinterpolations The inlet velocity waveform was taken fromthe literature [25] andFigure 3 shows the pulsatilewaveformsused For inlet condition a transient blood flow was imposedin the descendent abdominal aorta The velocity 119880 wascalculated for each patient in order to obtain a total fluidvolumetric flow rate of 500mL for an entire cardiac cycleTheoutlet boundaries were located at the common iliac arterieswhere the pressure follows pulsatile waveforms as defined
4 Computational and Mathematical Methods in Medicine
Figure 2 Workflow of the 3D AAAmodel Obtaining the CT image of the abdominal aorta segmentation of the vessel lumen using thresh-olding and level set method and 3D model of the AAA
in Figure 4(b) It is important to remark that these profilesare not patient-specific data (MR velocity mapping was notperformed on these subjects) which can be a limitation ofthis study In further studies a patient-specific velocity andpressure profile will be used as boundary conditions
Mathematically the boundary conditions can be ex-pressed as in (3a) (3b) and (3c) No-slip condition (vesselrigid wall) was imposed on the surface of the arteries (3a)This choice is motivated by the fact that the physiologicalparameters characterizing the arterial mechanical behaviourof the AAA wall are not well determined This approachhowever reduces the discretization effort considerably inparticular boundary layer gridding and the computationalcost although other approaches consider fluid structureinteraction (FSI) models [13 25ndash28] The inlet velocity isassumed to fully developed their parabolic profile at the inlet(3b) and time-dependent normal traction due to luminalpressure at the outlet (3c) as
119881 = 0 1003816100381610038161003816wall (3a)
119906119911 = 2 (119906 (119905)) (1 minus ( 2119903119889119903 )2) 119906119903 = 01003816100381610038161003816119911=0 (3b)
120591119899119899 = 119899 sdot 119901 (119905) 119868 sdot 119899 (3c)
where 119889119903 is the inner radius of the abdominal aorta 119906119903 isthe Cartesian component of the velocity vector in the ldquo119911rdquodirection and 119906(119905) and 119901(119905) are the time-dependent velocityand pressure waveforms designated in Figure 3 The pressureboundary conditions are given by (3c) where 120591119899119899 is thenormal traction designates at the outlet 119868 is the standardidentity matrix and 119899 designates the normal of the respectiveboundary Figure 4 shows case 4 of the AAA reconstructedmodel and the layers in which our domain is divided in orderto impose the boundary conditions
4 Results
Five models of infrarenal aneurysm with patient-specificgeometry were analyzed using computational fluid dynamicsin order to evaluate the flow patterns wall shear stress andpressure over the aneurysm sac Patients 1 to 4 had infrarenalaneurysms whilst patient 5 is the control case ILT was notfound in any case The unsteady flow simulations were per-formed through twopulsatile cycles to eliminate the influenceof initial transients The results of pressure stress and flow
patterns are shown for the peak systole (02 s) of the secondcardiac cycle
Figure 5 shows the flow patterns velocity streamlinesinside the infrarenal aneurysms sac and three cross-sectionalareas of the AAA (proximal midsection and distal neck)for the five patients studied Note that forward flow pointsdownwards and has a negative value in the adopted coordi-nate system The direction of the flow is from top to bottom(direction 119885 negative) We notice that when the AAA hasasymmetry the velocity streamlines correspondingly showan asymmetric flow pattern inside the AAA sac As shownin [6 7 26 29] the asymmetric flow patterns can providean insight into the mechanism that promotes the thrombusrenewal and possibly enlargement inside the aneurysmRapid decrease in the velocity and regions of very high(or low) hemodynamic stresses gradients may all contributein various ways to the vascular disease primarily via theireffects on the endothelium For example platelets trappedin recirculation zones tend to be deposited in areas of lowshear stress (stenosis) [14] since this and the presence ofvortices cause prolonged contact of the platelets with thesurface in the layer of slow fluid motion [6 19] This effectcan be observed for the pathological cases however in case 4we observe a flow recirculation in the middle section and theasymmetry is low Consequently the flow patterns of theaneurysmnot only depend of the asymmetry of the aneurysmbut also depend of the AAA tortuosity Details of the flowpatterns for the AAAs is shown in Figure 5 (cross-sectionalareas column) From the top to the bottom neck sectionmidsection (maximum diameter in the aneurysm sac) anddistal section We notice that the tortuosity of the AAAprovokes an asymmetric flow patterns in the AAA sac When120576 is high we observe that in the AAA proximal neck sectionthere is a strong irregular flow causing also an irregular flowin the AAA sac meanwhile when 120576 is low this effect doesnot appear From these findings the greater the asymmetryand tortuosity of the AAA the higher the possibility of bloodrecirculation ILT formation and a possible rupture Thusthe importance of geometry in the hemodynamic behaviorof AAAs is supported
Anterior and posterior wall shear stress views are shownin Figure 6 as well as the pressure on the aneurysm sac atthe peak systole The mean WSS in the aneurysm sac of the5 patients varied between 028 (case 5) and 1272 Pa (case 4)with a median of 352 Pa and mean of 574 Pa The areas withWSS values under the mean value have been classified as low
Computational and Mathematical Methods in Medicine 5
09
08
07
06
05
04
03
02
01
00908070605040302010
Time (s)
Vel
oci
ty (
ms
)Inlet velocity prole
(a)
0908070605040302010
Time (s)
16
15
14
13
12
11
10
Pre
ssu
re (
Pa)
Outlet pressure proletimes103
(b)
Figure 3 Boundary conditions for the hemodynamic simulations adapted from [11]
Inlet (descending aorta)
xz y
(a)
Outlet(iliac arteries)
Aortic wall(AAA sac)
x
zy
(b)
Figure 4 Mesh surface different layers are shown aortic wall (dark blue) and inlet (purple) and outlet sections (light blue)
WSS areas (blue) and areas with WSS values higher than themean value as high WSS (red) Analysis of WSS maps forall cases shows that the area of low WSS coincides with thelocation of the recirculation areas (low velocities) and higherWSS values are found in two regions in the neck area and inthe corresponding areawhere the bloodflow jet has an impacton the aneurismal sac The blood flow jet has an impactdirectly on the arterial wall producing higherWSS valuesTheblood flow jet path is provoked by the proximal neck angleconsequently by the AAA tortuosity (see Figure 5) TheseWSS peak values do not influence too much in aneurysmgrowth however in these areas a material failure could beproduced provoked by blood flow jet It is interesting to notethat shear stress levels in all infrarenal aneurysms models arehigher than those in the normal aorta where 120576 is low whichhas a fairly uniform stress shear spatial distributionMaximalvalues are found in the neck region where 120576 is high
Due to the increasing of the internal pressure againstthe aortic walls the AAA diameter grows progressively andeventually it could be able to overcome the resistance of theaortic wall with its breakup This internal pressure is directlyproportional with the aneurysm diameter thereby when thediameter grows the pressure increases High deformationdiameter rate (120594) index could indicate higher internal pres-sure however it should be noticed that the pressure also
depends on the tortuosity index (inversely proportional) andthe flow characteristics (see Figure 5) For instance in case 4even when the section diameter is large the internal pressureis lower than that in case 2 This is originated by a notablypressure drop as a result of the vorticity and flow recirculation(energy losses) in the cases with a high tortuosity index Thiseffect also provokes a pressures gradient between the anteriorand posterior arterial wall in the interior of the AAA sacThese internal high pressure areas inside the sac may indicatethe growth directions of AAA sac
5 Discussions
The objective of this study is to use patient-specific AAAmodels for correlating the geometric indices of the aneurysmwith the hemodynamic loads and eventually with thepotential risk of AAA rupture From a mechanical point ofview AAA ruptures when a maximum stress value over thewall is exceeded The stress peak refers to the mechanicalload sustained by the AAA wall during maximal systolicpressurization In addition it is known that wall stress alonedoes not completely govern failure as an AAA will usuallyrupture when the wall stress exceeds the wall strength Itsvalue depends on arterial systolic pressure the mechanicalproperties and the geometric configuration of the material
6 Computational and Mathematical Methods in Medicine
AAA streamlines AAA sac streamlines details
Cross- sectional
areas
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
3552131574276282368119734157871184
039468078936
0
4654133336167312583320667155103330516670
Cas
e 5
x yz
x yz
x yz
5573949546433523715930966247731858123860619320
x yz
x yz
60112534334675440075333952671620037133580667910
2522222194441666713889111110833330555560277780
|V|
Figure 5 Streamlines details of AAA sac streamline blood flowvelocity and three cross-sectional areas (from the top to the bottom proximalAAA neck and midsection and distal AAA neck) for the five patient studied
under study However the mechanism of arterial wall failuredue to (1) the AAA shape or (2) the pressure distribution isphysically different The first is because of a punctual forceover a wall point and the second is because a consequence
of a pressure distribution over the AAA wall Based on theAAA shape several authors have proposed different criteriafor the AAA collapsibility if the AAAdiameter is higher than55 cm [4] the AAA may rupture or if the asymmetry index
Computational and Mathematical Methods in Medicine 7
WSS anterior WSS posterior Pressure
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
Cas
e 5
High
Low
High
Low
High
Low
High
Low
High
Low
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
37000
37000
37000
37000
37000
33556301112666723222197781633312889944446000
x yz
Figure 6 Anterior and posterior wall shear stress views (high WSS in red and low WSS in blue) and normalized pressure on the aneurysmsac at the peak systole for the five patients
8 Computational and Mathematical Methods in Medicine
factor (120573) is 120573 lt 04 the AAA rupture is high [8] In [10]the AAA collapses when the deformation diameter ratio is120594 gt 33 or if the saccular index is lt06 [11] But depend-ing on the index that is analysed the surgical criteria aredifferent More recently the proposed AAA rupture risk isrelated with the presence of intraluminal thrombus (ILT)[6 26] The intraluminal thrombus plays an important rolein expansion and rupture of advanced aneurysms throughdirectmechanical as well as indirect chemomechanical effects[6] Therefore the AAA dilatation (and a potential rupture)is dependent on the correlation between the geometricalfactor and the hemodynamic load Consequently alternativemethods of AAA rupture assessment are needed
Themajority of these new approaches involve the numer-ical analysis of AAAs using computational fluid dynamics(CFD) to determine the wall shear stress (WSS) distributionsand flow patterns in the aneurysm sac [5 12 13 15 16 30]In our study we did not evaluate the patient-specific wallstrength or the effect of intraluminal thrombus Neverthe-less the AAA cases analyzed provide useful information tounderstanding how hemodynamic loads can affect aneurysmgrowth and possible rupture The pathological cases (cases 1to 4) always present irregular flow in the aneurysm sac nouniform distribution of WSSs and great WSS values in thecurvatures of the aortic vessel These anomalies are propor-tional to the shape of the aneurysm and the angles of twistthat the aorta has Asymmetric flow is always correlated to themodified curvature of the vessel or when some enlargementin the aneurysm is present (high saccular index (120574) andtortuosity (120576) index) The AAA tortuosity could initiate ILTformation and at the same time could provoke arterial wallfailure In a situation where the tortuosity is high and thesaccular index is low the WSS has more effects than thepressure distribution in a possible AAA failure Howeverwhere the AAA is not twisted and the saccular index is highthe pressure effect takes priority In Figure 6 the highest shearstress values are dependent especially on the tortuosity of theAAA The neck angle substantially impacts flow fields caus-ing strong irregular flow patterns in the AAA sac (Figure 5)significantly influencing wall stress distribution (Figure 6)The relationship between these indexes can provide an insightinto themechanism that promotes the thrombus renewal andpossibly enlargement inside the aneurysm
6 Conclusions
To conclude in this work the wall shear stress internalpressure and flow patterns of five patients-specific aortashave been analyzed using a finite element method and theresults have been correlated with the geometrical featuresResults from the patient-specific infrarenal aneurysmmodels(cases 1ndash4) were compared with those of a normal aorta (case5) and it has been found that the normal aorta has a uniformdistribution of the velocity streamlines wall shear stress andpressure compared to that in the pathological cases Maxi-mum wall shear stresses in all infrarenal aneurysm modelsare higher than those in the normal aorta and these valuesare not directly related to the maximum aneurysm diameterproviding evidence that a patient-specific aorta shape analysis
is necessary for a more reliable assessment of the rupturerisk of aortic aneurysms Therefore based on one or twosimple indexes alone to determine the risk of rupture accu-rately is insufficient AAA rupture is a complex situationdepending on themaximum diameter internal pressure wallstress asymmetry saccular index intraluminal thrombusand tortuosity among others Our results demonstrate howthe hemodynamic loads as simulated by computational fluiddynamics (CFD) are influenced by the geometrical factors ofthe aneurysm
Acknowledgment
This project was supported by the NTU-NHG InnovationSeed Grant Project no ISG11007
References
[1] D A Vorp ldquoBiomechanics of abdominal aortic aneurysmrdquoJournal of Biomechanics vol 40 no 9 pp 1887ndash1902 2007
[2] J D Humphrey Cardiovascular Solid Mechanics Cells Tissuesand Organs Springer New York NY USA 2002
[3] J T Powell L C Brown J F Forbes et al ldquoFinal 12-year follow-up of surgery versus surveillance in the UK Small AneurysmTrialrdquoBritish Journal of Surgery vol 94 no 6 pp 702ndash708 2007
[4] S CNicholls J BGardnerMHMeissner andKH JohansenldquoRupture in small abdominal aortic aneurysmsrdquo Journal ofVascular Surgery vol 28 no 5 pp 884ndash888 1998
[5] M L Raghavan and D A Vorp ldquoToward a biomechanical toolto evaluate rupture potential of abdominal aortic aneurysmidentification of a finite strain constitutivemodel and evaluationof its applicabilityrdquo Journal of Biomechanics vol 33 no 4 pp475ndash482 2000
[6] J Biasetti F Hussain and T Christian Gasser ldquoBlood flow andcoherent vortices in the normal and aneurysmatic aortas afluid dynamical approach to intraluminal thrombus formationrdquoJournal of the Royal Society Interface vol 8 no 63 pp 1449ndash1461 2011
[7] C M Scotti and E A Finol ldquoCompliant biomechanicsof abdominal aortic aneurysms a fluid-structure interactionstudyrdquo Computers and Structures vol 85 no 11ndash14 pp 1097ndash1113 2007
[8] D A Vorp M L Raghavan and M W Webster ldquoMechanicalwall stress in abdominal aortic aneurysm influence of diameterand asymmetryrdquo Journal of Vascular Surgery vol 27 no 4 pp632ndash639 1998
[9] E A Finol K Keyhani and C H Amon ldquoThe effect of asym-metry in abdominal aortic aneurysms under physiologicallyrealistic pulsatile flow conditionsrdquo Journal of BiomechanicalEngineering vol 125 no 2 pp 207ndash217 2003
[10] W A Cappeller H Engelmann S Blechschmidt M Wild andL Lauterjung ldquoPossible objectification of a critical maximumdiameter for elective surgery in abdominal aortic aneurysmsbased on one- and three-dimensional ratiosrdquo Journal of Cardio-vascular Surgery vol 38 no 6 pp 623ndash628 1997
[11] K Ouriel R M Green C Donayre C K Shortell J Elliott andJ A DeWeese ldquoAn evaluation of new methods of expressingaortic aneurysm size relationship to rupturerdquo Journal of Vas-cular Surgery vol 15 no 1 pp 12ndash20 1992
[12] T C Gasser M Auer F Labruto J Swedenborg and J RoyldquoBiomechanical rupture risk assessment of abdominal aortic
Computational and Mathematical Methods in Medicine 9
aneurysms model complexity versus predictability of finite ele-ment simulationsrdquo European Journal of Vascular and Endovas-cular Surgery vol 40 no 2 pp 176ndash185 2010
[13] M Bonert R L Leask J Butany et al ldquoThe relationshipbetween wall shear stress distributions and intimal thickeningin the human abdominal aortardquo BioMedical Engineering Onlinevol 2 article 18 2003
[14] D Bluestein L Niu R T Schoephoerster andM K DewanjeeldquoSteady flow in an aneurysm model correlation between fluiddynamics and blood platelet depositionrdquo Journal of Biomechan-ical Engineering vol 118 no 3 pp 280ndash286 1996
[15] M L Raghavan D A VorpM P Federle M S Makaroun andMWWebster ldquoWall stress distribution on three-dimensionallyreconstructed models of human abdominal aortic aneurysmrdquoJournal of Vascular Surgery vol 31 no 4 pp 760ndash769 2000
[16] C Kleinstreuer and Z Li ldquoAnalysis and computer programfor rupture-risk prediction of abdominal aortic aneurysmsrdquoBioMedical Engineering Online vol 5 article 19 2006
[17] J Shum G Martufi E di Martino et al ldquoQuantitative assess-ment of abdominal aortic aneurysm geometryrdquo Annals of Bio-medical Engineering vol 39 no 1 pp 277ndash286 2011
[18] D A Vorp P C Lee D H J Wang et al ldquoAssociation ofintraluminal thrombus in abdominal aortic aneurysm withlocal hypoxia and wall weakeningrdquo Journal of Vascular Surgeryvol 34 no 2 pp 291ndash299 2001
[19] D Bluestein K Dumont M de Beule et al ldquoIntraluminalthrombus and risk of rupture in patient specific abdominalaortic aneurysmmdashFSImodellingrdquoComputerMethods in Biome-chanics and Biomedical Engineering vol 12 no 1 pp 73ndash812009
[20] E Soudah J Pennecot J S Perez M Bordone and E OnateldquoMedical-GiD from medical images to simulations 4D MRIflow analysisrdquo in Computational Vision and Medical ImageProcessing Recent Trends chapter 10 Springer New York NYUSA 1871
[21] E Soudah M Bordone and J S Perez ldquoGmed a platform forimages treatment inside GiD systemrdquo in Proceedings of the 5thConference On Advances And Applications Of GiD Barcelona2010 GiDmdashthe personal pre and postprocessor httpwwwgidhomecom
[22] W E Lorensen and H E Cline ldquoMarching cubes a high reso-lution 3d surface construction algorithmrdquo in Proceedings of the14th Annual Conference on Computer Graphics and InteractiveTechniques (SIGGRAPH rsquo87) pp 163ndash169 1987
[23] M Bordone C Garcıa J Garcıa and E Soudah ldquoBiodyn UserManual TDYN theoretical Backgroundrdquo COMPASSIS 2012httpwwwcompassiscomcompass
[24] E Onate S Idelsohn O C Zienkiewicz and R L Taylor ldquoAfinite point method in computational mechanics Applicationsto convective transport and fluid flowrdquo International Journal forNumerical Methods in Engineering vol 39 no 22 pp 3839ndash3866 1996
[25] Y Papaharilaou J A Ekaterinaris E Manousaki and AN Katsamouris ldquoA decoupled fluid structure approach forestimating wall stress in abdominal aortic aneurysmsrdquo Journalof Biomechanics vol 40 no 2 pp 367ndash377 2007
[26] A-V Salsac S R Sparks J-M Chomaz and J C LasherasldquoEvolution of the wall shear stresses during the progressiveenlargement of symmetric abdominal aortic aneurysmsrdquo Jour-nal of Fluid Mechanics vol 560 pp 19ndash51 2006
[27] C M Scotti J Jimenez S C Muluk and E A Finol ldquoWallstress and flow dynamics in abdominal aortic aneurysms finite
element analysis vs fluid-structure interactionrdquo ComputerMethods in Biomechanics andBiomedical Engineering vol 11 no3 pp 301ndash322 2008
[28] A Borghia N B Wooda R H Mohiaddinb and X Y XualdquoFluid-solid interaction simulationof flow and stress pattern inthoraco abdominal aneurysms a patient-specific studyrdquo Journalof Fluids and Structures vol 24 pp 270ndash280 2008
[29] A Sheidaei S C Hunley S Zeinali-Davarani L G Raguinand S Baek ldquoSimulation of abdominal aortic aneurysm growthwith updating hemodynamic loads using a realistic geometryrdquoMedical Engineering and Physics vol 33 no 1 pp 80ndash88 2011
[30] T Hatakeyama H Shigematsu and T Muto ldquoRisk factors forrupture of abdominal aortic aneurysm based on three-dimen-sional studyrdquo Journal of Vascular Surgery vol 33 no 3 pp 453ndash461 2001
Submit your manuscripts at
httpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
Oxidative Medicine and
Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Parkinsonrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Computational and Mathematical Methods in Medicine 3
Table 1 Patient and AAA geometrical characteristics (119871 120591 119889proximal neck 119903 119877 119863AMAX and LAAA) and all the measurements are expressed incentimeter AAA geometrical indexes (120573 120574 120594 and 120576)
Case SexThoracic aortalength (119871)
Hypotheticthoracic aortalength (120591)
AAA proximalneck
(119889proximal neck)
119903 119877 AAA maxdiameter(119863AMAX)
AAA length(LAAA)
120594 120573 120574 1205761 Male 35994 32044 28 149 245 3945 67 1408 0608 0588 0123
2 Male 3195 3102 17 067 174 2416 41 1421 0388 0589 0029
3 Male 21628 1768 26 102 203 3056 898 1176 0508 0340 0223
4 Male 29355 25526 26 095 307 4031 156 155 0309 0258 0150
5 Male 31034 29624 25 125 125 25 mdash 1 1 mdash 0047
dabdominal_aorta
dproximal neck
ddistal neck
DAMAX
LAAA
L
(a)
R
r
Midsection (DAMAX )
(b)
Figure 1 (a) Main geometrical parameters 119871AAA aneurysm length 119863MAX maximum diameter of the aneurysm 119889proximal neck beginning of theAAA sac 119889distal neck ending of the AAA sac 119889abdominal aorta nondeformed abdominal aorta diameter 119871 is the absolute length of the tortuousvessel and 120591 is the imaginary straight line (b) Schematic visualization of a cross-sectional AAA section where 119903 and 119877 are defined as theradii measured at the midsection of the AAA sac from the longitudinal z-axis to the posterior and anterior walls
is defined as Re = 119880119863] where 119880 is the mean velocity ]is the kinematic viscosity of air and 119863 is the characteristiclength given as the hydraulic diameter 119863 = 4119860119875 for theinlet velocity and here 119860 is the cross-sectional area and 119875 isthe perimeter of the aorta Because the Reynolds number ininlet is low (lt1000) we decided to use a CFD solver for lam-inar flow considering steady homogeneous incompressibleadiabatic and Newtonian fluid However three-dimensionalflow features such as flow separation and recirculation mighttrigger a transition to turbulence at lower Reynolds numbers[9] Based on a preliminary study [6] the effect of theturbulence has been considered to be negligible Followingwe show the Navier-Stokes equations (2)
120588 (120597119906120597119905 + (119906 sdot nabla) 119906) + nabla119901minusnabla sdot (120583nabla119906) = 120588119891 in Ω times (0 119905)
nabla sdot 119906 = 0 in Ω times (0 119905) (2)
where 119906 = 119906(119909 119905) denotes the velocity vector 119901 = 119901(119909 119905) thepressure field and the density (120588) is considered constant with
a value of 1050Kgsdotmminus3 and dynamic viscosity (]) fixed at0004 Pasdots and 119891 the volumetric acceleration The spatial dis-cretization of the Navier-Stokes equations has been done bymeans of the finite elementmethod (FEM) while for the timediscretization an iterative algorithm that can be consideredas an implicit two steps fractional step method has beenused A new stabilisation method known as finite incrementcalculus has recently been developed [24] By considering thebalance of flux over a finite sized domain higher order termsnaturally appear in the governing equations which supply thenecessary stability for a classical Galerkin finite element dis-cretization to be used with equal order velocity and pressureinterpolations The inlet velocity waveform was taken fromthe literature [25] andFigure 3 shows the pulsatilewaveformsused For inlet condition a transient blood flow was imposedin the descendent abdominal aorta The velocity 119880 wascalculated for each patient in order to obtain a total fluidvolumetric flow rate of 500mL for an entire cardiac cycleTheoutlet boundaries were located at the common iliac arterieswhere the pressure follows pulsatile waveforms as defined
4 Computational and Mathematical Methods in Medicine
Figure 2 Workflow of the 3D AAAmodel Obtaining the CT image of the abdominal aorta segmentation of the vessel lumen using thresh-olding and level set method and 3D model of the AAA
in Figure 4(b) It is important to remark that these profilesare not patient-specific data (MR velocity mapping was notperformed on these subjects) which can be a limitation ofthis study In further studies a patient-specific velocity andpressure profile will be used as boundary conditions
Mathematically the boundary conditions can be ex-pressed as in (3a) (3b) and (3c) No-slip condition (vesselrigid wall) was imposed on the surface of the arteries (3a)This choice is motivated by the fact that the physiologicalparameters characterizing the arterial mechanical behaviourof the AAA wall are not well determined This approachhowever reduces the discretization effort considerably inparticular boundary layer gridding and the computationalcost although other approaches consider fluid structureinteraction (FSI) models [13 25ndash28] The inlet velocity isassumed to fully developed their parabolic profile at the inlet(3b) and time-dependent normal traction due to luminalpressure at the outlet (3c) as
119881 = 0 1003816100381610038161003816wall (3a)
119906119911 = 2 (119906 (119905)) (1 minus ( 2119903119889119903 )2) 119906119903 = 01003816100381610038161003816119911=0 (3b)
120591119899119899 = 119899 sdot 119901 (119905) 119868 sdot 119899 (3c)
where 119889119903 is the inner radius of the abdominal aorta 119906119903 isthe Cartesian component of the velocity vector in the ldquo119911rdquodirection and 119906(119905) and 119901(119905) are the time-dependent velocityand pressure waveforms designated in Figure 3 The pressureboundary conditions are given by (3c) where 120591119899119899 is thenormal traction designates at the outlet 119868 is the standardidentity matrix and 119899 designates the normal of the respectiveboundary Figure 4 shows case 4 of the AAA reconstructedmodel and the layers in which our domain is divided in orderto impose the boundary conditions
4 Results
Five models of infrarenal aneurysm with patient-specificgeometry were analyzed using computational fluid dynamicsin order to evaluate the flow patterns wall shear stress andpressure over the aneurysm sac Patients 1 to 4 had infrarenalaneurysms whilst patient 5 is the control case ILT was notfound in any case The unsteady flow simulations were per-formed through twopulsatile cycles to eliminate the influenceof initial transients The results of pressure stress and flow
patterns are shown for the peak systole (02 s) of the secondcardiac cycle
Figure 5 shows the flow patterns velocity streamlinesinside the infrarenal aneurysms sac and three cross-sectionalareas of the AAA (proximal midsection and distal neck)for the five patients studied Note that forward flow pointsdownwards and has a negative value in the adopted coordi-nate system The direction of the flow is from top to bottom(direction 119885 negative) We notice that when the AAA hasasymmetry the velocity streamlines correspondingly showan asymmetric flow pattern inside the AAA sac As shownin [6 7 26 29] the asymmetric flow patterns can providean insight into the mechanism that promotes the thrombusrenewal and possibly enlargement inside the aneurysmRapid decrease in the velocity and regions of very high(or low) hemodynamic stresses gradients may all contributein various ways to the vascular disease primarily via theireffects on the endothelium For example platelets trappedin recirculation zones tend to be deposited in areas of lowshear stress (stenosis) [14] since this and the presence ofvortices cause prolonged contact of the platelets with thesurface in the layer of slow fluid motion [6 19] This effectcan be observed for the pathological cases however in case 4we observe a flow recirculation in the middle section and theasymmetry is low Consequently the flow patterns of theaneurysmnot only depend of the asymmetry of the aneurysmbut also depend of the AAA tortuosity Details of the flowpatterns for the AAAs is shown in Figure 5 (cross-sectionalareas column) From the top to the bottom neck sectionmidsection (maximum diameter in the aneurysm sac) anddistal section We notice that the tortuosity of the AAAprovokes an asymmetric flow patterns in the AAA sac When120576 is high we observe that in the AAA proximal neck sectionthere is a strong irregular flow causing also an irregular flowin the AAA sac meanwhile when 120576 is low this effect doesnot appear From these findings the greater the asymmetryand tortuosity of the AAA the higher the possibility of bloodrecirculation ILT formation and a possible rupture Thusthe importance of geometry in the hemodynamic behaviorof AAAs is supported
Anterior and posterior wall shear stress views are shownin Figure 6 as well as the pressure on the aneurysm sac atthe peak systole The mean WSS in the aneurysm sac of the5 patients varied between 028 (case 5) and 1272 Pa (case 4)with a median of 352 Pa and mean of 574 Pa The areas withWSS values under the mean value have been classified as low
Computational and Mathematical Methods in Medicine 5
09
08
07
06
05
04
03
02
01
00908070605040302010
Time (s)
Vel
oci
ty (
ms
)Inlet velocity prole
(a)
0908070605040302010
Time (s)
16
15
14
13
12
11
10
Pre
ssu
re (
Pa)
Outlet pressure proletimes103
(b)
Figure 3 Boundary conditions for the hemodynamic simulations adapted from [11]
Inlet (descending aorta)
xz y
(a)
Outlet(iliac arteries)
Aortic wall(AAA sac)
x
zy
(b)
Figure 4 Mesh surface different layers are shown aortic wall (dark blue) and inlet (purple) and outlet sections (light blue)
WSS areas (blue) and areas with WSS values higher than themean value as high WSS (red) Analysis of WSS maps forall cases shows that the area of low WSS coincides with thelocation of the recirculation areas (low velocities) and higherWSS values are found in two regions in the neck area and inthe corresponding areawhere the bloodflow jet has an impacton the aneurismal sac The blood flow jet has an impactdirectly on the arterial wall producing higherWSS valuesTheblood flow jet path is provoked by the proximal neck angleconsequently by the AAA tortuosity (see Figure 5) TheseWSS peak values do not influence too much in aneurysmgrowth however in these areas a material failure could beproduced provoked by blood flow jet It is interesting to notethat shear stress levels in all infrarenal aneurysms models arehigher than those in the normal aorta where 120576 is low whichhas a fairly uniform stress shear spatial distributionMaximalvalues are found in the neck region where 120576 is high
Due to the increasing of the internal pressure againstthe aortic walls the AAA diameter grows progressively andeventually it could be able to overcome the resistance of theaortic wall with its breakup This internal pressure is directlyproportional with the aneurysm diameter thereby when thediameter grows the pressure increases High deformationdiameter rate (120594) index could indicate higher internal pres-sure however it should be noticed that the pressure also
depends on the tortuosity index (inversely proportional) andthe flow characteristics (see Figure 5) For instance in case 4even when the section diameter is large the internal pressureis lower than that in case 2 This is originated by a notablypressure drop as a result of the vorticity and flow recirculation(energy losses) in the cases with a high tortuosity index Thiseffect also provokes a pressures gradient between the anteriorand posterior arterial wall in the interior of the AAA sacThese internal high pressure areas inside the sac may indicatethe growth directions of AAA sac
5 Discussions
The objective of this study is to use patient-specific AAAmodels for correlating the geometric indices of the aneurysmwith the hemodynamic loads and eventually with thepotential risk of AAA rupture From a mechanical point ofview AAA ruptures when a maximum stress value over thewall is exceeded The stress peak refers to the mechanicalload sustained by the AAA wall during maximal systolicpressurization In addition it is known that wall stress alonedoes not completely govern failure as an AAA will usuallyrupture when the wall stress exceeds the wall strength Itsvalue depends on arterial systolic pressure the mechanicalproperties and the geometric configuration of the material
6 Computational and Mathematical Methods in Medicine
AAA streamlines AAA sac streamlines details
Cross- sectional
areas
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
3552131574276282368119734157871184
039468078936
0
4654133336167312583320667155103330516670
Cas
e 5
x yz
x yz
x yz
5573949546433523715930966247731858123860619320
x yz
x yz
60112534334675440075333952671620037133580667910
2522222194441666713889111110833330555560277780
|V|
Figure 5 Streamlines details of AAA sac streamline blood flowvelocity and three cross-sectional areas (from the top to the bottom proximalAAA neck and midsection and distal AAA neck) for the five patient studied
under study However the mechanism of arterial wall failuredue to (1) the AAA shape or (2) the pressure distribution isphysically different The first is because of a punctual forceover a wall point and the second is because a consequence
of a pressure distribution over the AAA wall Based on theAAA shape several authors have proposed different criteriafor the AAA collapsibility if the AAAdiameter is higher than55 cm [4] the AAA may rupture or if the asymmetry index
Computational and Mathematical Methods in Medicine 7
WSS anterior WSS posterior Pressure
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
Cas
e 5
High
Low
High
Low
High
Low
High
Low
High
Low
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
37000
37000
37000
37000
37000
33556301112666723222197781633312889944446000
x yz
Figure 6 Anterior and posterior wall shear stress views (high WSS in red and low WSS in blue) and normalized pressure on the aneurysmsac at the peak systole for the five patients
8 Computational and Mathematical Methods in Medicine
factor (120573) is 120573 lt 04 the AAA rupture is high [8] In [10]the AAA collapses when the deformation diameter ratio is120594 gt 33 or if the saccular index is lt06 [11] But depend-ing on the index that is analysed the surgical criteria aredifferent More recently the proposed AAA rupture risk isrelated with the presence of intraluminal thrombus (ILT)[6 26] The intraluminal thrombus plays an important rolein expansion and rupture of advanced aneurysms throughdirectmechanical as well as indirect chemomechanical effects[6] Therefore the AAA dilatation (and a potential rupture)is dependent on the correlation between the geometricalfactor and the hemodynamic load Consequently alternativemethods of AAA rupture assessment are needed
Themajority of these new approaches involve the numer-ical analysis of AAAs using computational fluid dynamics(CFD) to determine the wall shear stress (WSS) distributionsand flow patterns in the aneurysm sac [5 12 13 15 16 30]In our study we did not evaluate the patient-specific wallstrength or the effect of intraluminal thrombus Neverthe-less the AAA cases analyzed provide useful information tounderstanding how hemodynamic loads can affect aneurysmgrowth and possible rupture The pathological cases (cases 1to 4) always present irregular flow in the aneurysm sac nouniform distribution of WSSs and great WSS values in thecurvatures of the aortic vessel These anomalies are propor-tional to the shape of the aneurysm and the angles of twistthat the aorta has Asymmetric flow is always correlated to themodified curvature of the vessel or when some enlargementin the aneurysm is present (high saccular index (120574) andtortuosity (120576) index) The AAA tortuosity could initiate ILTformation and at the same time could provoke arterial wallfailure In a situation where the tortuosity is high and thesaccular index is low the WSS has more effects than thepressure distribution in a possible AAA failure Howeverwhere the AAA is not twisted and the saccular index is highthe pressure effect takes priority In Figure 6 the highest shearstress values are dependent especially on the tortuosity of theAAA The neck angle substantially impacts flow fields caus-ing strong irregular flow patterns in the AAA sac (Figure 5)significantly influencing wall stress distribution (Figure 6)The relationship between these indexes can provide an insightinto themechanism that promotes the thrombus renewal andpossibly enlargement inside the aneurysm
6 Conclusions
To conclude in this work the wall shear stress internalpressure and flow patterns of five patients-specific aortashave been analyzed using a finite element method and theresults have been correlated with the geometrical featuresResults from the patient-specific infrarenal aneurysmmodels(cases 1ndash4) were compared with those of a normal aorta (case5) and it has been found that the normal aorta has a uniformdistribution of the velocity streamlines wall shear stress andpressure compared to that in the pathological cases Maxi-mum wall shear stresses in all infrarenal aneurysm modelsare higher than those in the normal aorta and these valuesare not directly related to the maximum aneurysm diameterproviding evidence that a patient-specific aorta shape analysis
is necessary for a more reliable assessment of the rupturerisk of aortic aneurysms Therefore based on one or twosimple indexes alone to determine the risk of rupture accu-rately is insufficient AAA rupture is a complex situationdepending on themaximum diameter internal pressure wallstress asymmetry saccular index intraluminal thrombusand tortuosity among others Our results demonstrate howthe hemodynamic loads as simulated by computational fluiddynamics (CFD) are influenced by the geometrical factors ofthe aneurysm
Acknowledgment
This project was supported by the NTU-NHG InnovationSeed Grant Project no ISG11007
References
[1] D A Vorp ldquoBiomechanics of abdominal aortic aneurysmrdquoJournal of Biomechanics vol 40 no 9 pp 1887ndash1902 2007
[2] J D Humphrey Cardiovascular Solid Mechanics Cells Tissuesand Organs Springer New York NY USA 2002
[3] J T Powell L C Brown J F Forbes et al ldquoFinal 12-year follow-up of surgery versus surveillance in the UK Small AneurysmTrialrdquoBritish Journal of Surgery vol 94 no 6 pp 702ndash708 2007
[4] S CNicholls J BGardnerMHMeissner andKH JohansenldquoRupture in small abdominal aortic aneurysmsrdquo Journal ofVascular Surgery vol 28 no 5 pp 884ndash888 1998
[5] M L Raghavan and D A Vorp ldquoToward a biomechanical toolto evaluate rupture potential of abdominal aortic aneurysmidentification of a finite strain constitutivemodel and evaluationof its applicabilityrdquo Journal of Biomechanics vol 33 no 4 pp475ndash482 2000
[6] J Biasetti F Hussain and T Christian Gasser ldquoBlood flow andcoherent vortices in the normal and aneurysmatic aortas afluid dynamical approach to intraluminal thrombus formationrdquoJournal of the Royal Society Interface vol 8 no 63 pp 1449ndash1461 2011
[7] C M Scotti and E A Finol ldquoCompliant biomechanicsof abdominal aortic aneurysms a fluid-structure interactionstudyrdquo Computers and Structures vol 85 no 11ndash14 pp 1097ndash1113 2007
[8] D A Vorp M L Raghavan and M W Webster ldquoMechanicalwall stress in abdominal aortic aneurysm influence of diameterand asymmetryrdquo Journal of Vascular Surgery vol 27 no 4 pp632ndash639 1998
[9] E A Finol K Keyhani and C H Amon ldquoThe effect of asym-metry in abdominal aortic aneurysms under physiologicallyrealistic pulsatile flow conditionsrdquo Journal of BiomechanicalEngineering vol 125 no 2 pp 207ndash217 2003
[10] W A Cappeller H Engelmann S Blechschmidt M Wild andL Lauterjung ldquoPossible objectification of a critical maximumdiameter for elective surgery in abdominal aortic aneurysmsbased on one- and three-dimensional ratiosrdquo Journal of Cardio-vascular Surgery vol 38 no 6 pp 623ndash628 1997
[11] K Ouriel R M Green C Donayre C K Shortell J Elliott andJ A DeWeese ldquoAn evaluation of new methods of expressingaortic aneurysm size relationship to rupturerdquo Journal of Vas-cular Surgery vol 15 no 1 pp 12ndash20 1992
[12] T C Gasser M Auer F Labruto J Swedenborg and J RoyldquoBiomechanical rupture risk assessment of abdominal aortic
Computational and Mathematical Methods in Medicine 9
aneurysms model complexity versus predictability of finite ele-ment simulationsrdquo European Journal of Vascular and Endovas-cular Surgery vol 40 no 2 pp 176ndash185 2010
[13] M Bonert R L Leask J Butany et al ldquoThe relationshipbetween wall shear stress distributions and intimal thickeningin the human abdominal aortardquo BioMedical Engineering Onlinevol 2 article 18 2003
[14] D Bluestein L Niu R T Schoephoerster andM K DewanjeeldquoSteady flow in an aneurysm model correlation between fluiddynamics and blood platelet depositionrdquo Journal of Biomechan-ical Engineering vol 118 no 3 pp 280ndash286 1996
[15] M L Raghavan D A VorpM P Federle M S Makaroun andMWWebster ldquoWall stress distribution on three-dimensionallyreconstructed models of human abdominal aortic aneurysmrdquoJournal of Vascular Surgery vol 31 no 4 pp 760ndash769 2000
[16] C Kleinstreuer and Z Li ldquoAnalysis and computer programfor rupture-risk prediction of abdominal aortic aneurysmsrdquoBioMedical Engineering Online vol 5 article 19 2006
[17] J Shum G Martufi E di Martino et al ldquoQuantitative assess-ment of abdominal aortic aneurysm geometryrdquo Annals of Bio-medical Engineering vol 39 no 1 pp 277ndash286 2011
[18] D A Vorp P C Lee D H J Wang et al ldquoAssociation ofintraluminal thrombus in abdominal aortic aneurysm withlocal hypoxia and wall weakeningrdquo Journal of Vascular Surgeryvol 34 no 2 pp 291ndash299 2001
[19] D Bluestein K Dumont M de Beule et al ldquoIntraluminalthrombus and risk of rupture in patient specific abdominalaortic aneurysmmdashFSImodellingrdquoComputerMethods in Biome-chanics and Biomedical Engineering vol 12 no 1 pp 73ndash812009
[20] E Soudah J Pennecot J S Perez M Bordone and E OnateldquoMedical-GiD from medical images to simulations 4D MRIflow analysisrdquo in Computational Vision and Medical ImageProcessing Recent Trends chapter 10 Springer New York NYUSA 1871
[21] E Soudah M Bordone and J S Perez ldquoGmed a platform forimages treatment inside GiD systemrdquo in Proceedings of the 5thConference On Advances And Applications Of GiD Barcelona2010 GiDmdashthe personal pre and postprocessor httpwwwgidhomecom
[22] W E Lorensen and H E Cline ldquoMarching cubes a high reso-lution 3d surface construction algorithmrdquo in Proceedings of the14th Annual Conference on Computer Graphics and InteractiveTechniques (SIGGRAPH rsquo87) pp 163ndash169 1987
[23] M Bordone C Garcıa J Garcıa and E Soudah ldquoBiodyn UserManual TDYN theoretical Backgroundrdquo COMPASSIS 2012httpwwwcompassiscomcompass
[24] E Onate S Idelsohn O C Zienkiewicz and R L Taylor ldquoAfinite point method in computational mechanics Applicationsto convective transport and fluid flowrdquo International Journal forNumerical Methods in Engineering vol 39 no 22 pp 3839ndash3866 1996
[25] Y Papaharilaou J A Ekaterinaris E Manousaki and AN Katsamouris ldquoA decoupled fluid structure approach forestimating wall stress in abdominal aortic aneurysmsrdquo Journalof Biomechanics vol 40 no 2 pp 367ndash377 2007
[26] A-V Salsac S R Sparks J-M Chomaz and J C LasherasldquoEvolution of the wall shear stresses during the progressiveenlargement of symmetric abdominal aortic aneurysmsrdquo Jour-nal of Fluid Mechanics vol 560 pp 19ndash51 2006
[27] C M Scotti J Jimenez S C Muluk and E A Finol ldquoWallstress and flow dynamics in abdominal aortic aneurysms finite
element analysis vs fluid-structure interactionrdquo ComputerMethods in Biomechanics andBiomedical Engineering vol 11 no3 pp 301ndash322 2008
[28] A Borghia N B Wooda R H Mohiaddinb and X Y XualdquoFluid-solid interaction simulationof flow and stress pattern inthoraco abdominal aneurysms a patient-specific studyrdquo Journalof Fluids and Structures vol 24 pp 270ndash280 2008
[29] A Sheidaei S C Hunley S Zeinali-Davarani L G Raguinand S Baek ldquoSimulation of abdominal aortic aneurysm growthwith updating hemodynamic loads using a realistic geometryrdquoMedical Engineering and Physics vol 33 no 1 pp 80ndash88 2011
[30] T Hatakeyama H Shigematsu and T Muto ldquoRisk factors forrupture of abdominal aortic aneurysm based on three-dimen-sional studyrdquo Journal of Vascular Surgery vol 33 no 3 pp 453ndash461 2001
Submit your manuscripts at
httpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
Oxidative Medicine and
Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Parkinsonrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Computational and Mathematical Methods in Medicine
Figure 2 Workflow of the 3D AAAmodel Obtaining the CT image of the abdominal aorta segmentation of the vessel lumen using thresh-olding and level set method and 3D model of the AAA
in Figure 4(b) It is important to remark that these profilesare not patient-specific data (MR velocity mapping was notperformed on these subjects) which can be a limitation ofthis study In further studies a patient-specific velocity andpressure profile will be used as boundary conditions
Mathematically the boundary conditions can be ex-pressed as in (3a) (3b) and (3c) No-slip condition (vesselrigid wall) was imposed on the surface of the arteries (3a)This choice is motivated by the fact that the physiologicalparameters characterizing the arterial mechanical behaviourof the AAA wall are not well determined This approachhowever reduces the discretization effort considerably inparticular boundary layer gridding and the computationalcost although other approaches consider fluid structureinteraction (FSI) models [13 25ndash28] The inlet velocity isassumed to fully developed their parabolic profile at the inlet(3b) and time-dependent normal traction due to luminalpressure at the outlet (3c) as
119881 = 0 1003816100381610038161003816wall (3a)
119906119911 = 2 (119906 (119905)) (1 minus ( 2119903119889119903 )2) 119906119903 = 01003816100381610038161003816119911=0 (3b)
120591119899119899 = 119899 sdot 119901 (119905) 119868 sdot 119899 (3c)
where 119889119903 is the inner radius of the abdominal aorta 119906119903 isthe Cartesian component of the velocity vector in the ldquo119911rdquodirection and 119906(119905) and 119901(119905) are the time-dependent velocityand pressure waveforms designated in Figure 3 The pressureboundary conditions are given by (3c) where 120591119899119899 is thenormal traction designates at the outlet 119868 is the standardidentity matrix and 119899 designates the normal of the respectiveboundary Figure 4 shows case 4 of the AAA reconstructedmodel and the layers in which our domain is divided in orderto impose the boundary conditions
4 Results
Five models of infrarenal aneurysm with patient-specificgeometry were analyzed using computational fluid dynamicsin order to evaluate the flow patterns wall shear stress andpressure over the aneurysm sac Patients 1 to 4 had infrarenalaneurysms whilst patient 5 is the control case ILT was notfound in any case The unsteady flow simulations were per-formed through twopulsatile cycles to eliminate the influenceof initial transients The results of pressure stress and flow
patterns are shown for the peak systole (02 s) of the secondcardiac cycle
Figure 5 shows the flow patterns velocity streamlinesinside the infrarenal aneurysms sac and three cross-sectionalareas of the AAA (proximal midsection and distal neck)for the five patients studied Note that forward flow pointsdownwards and has a negative value in the adopted coordi-nate system The direction of the flow is from top to bottom(direction 119885 negative) We notice that when the AAA hasasymmetry the velocity streamlines correspondingly showan asymmetric flow pattern inside the AAA sac As shownin [6 7 26 29] the asymmetric flow patterns can providean insight into the mechanism that promotes the thrombusrenewal and possibly enlargement inside the aneurysmRapid decrease in the velocity and regions of very high(or low) hemodynamic stresses gradients may all contributein various ways to the vascular disease primarily via theireffects on the endothelium For example platelets trappedin recirculation zones tend to be deposited in areas of lowshear stress (stenosis) [14] since this and the presence ofvortices cause prolonged contact of the platelets with thesurface in the layer of slow fluid motion [6 19] This effectcan be observed for the pathological cases however in case 4we observe a flow recirculation in the middle section and theasymmetry is low Consequently the flow patterns of theaneurysmnot only depend of the asymmetry of the aneurysmbut also depend of the AAA tortuosity Details of the flowpatterns for the AAAs is shown in Figure 5 (cross-sectionalareas column) From the top to the bottom neck sectionmidsection (maximum diameter in the aneurysm sac) anddistal section We notice that the tortuosity of the AAAprovokes an asymmetric flow patterns in the AAA sac When120576 is high we observe that in the AAA proximal neck sectionthere is a strong irregular flow causing also an irregular flowin the AAA sac meanwhile when 120576 is low this effect doesnot appear From these findings the greater the asymmetryand tortuosity of the AAA the higher the possibility of bloodrecirculation ILT formation and a possible rupture Thusthe importance of geometry in the hemodynamic behaviorof AAAs is supported
Anterior and posterior wall shear stress views are shownin Figure 6 as well as the pressure on the aneurysm sac atthe peak systole The mean WSS in the aneurysm sac of the5 patients varied between 028 (case 5) and 1272 Pa (case 4)with a median of 352 Pa and mean of 574 Pa The areas withWSS values under the mean value have been classified as low
Computational and Mathematical Methods in Medicine 5
09
08
07
06
05
04
03
02
01
00908070605040302010
Time (s)
Vel
oci
ty (
ms
)Inlet velocity prole
(a)
0908070605040302010
Time (s)
16
15
14
13
12
11
10
Pre
ssu
re (
Pa)
Outlet pressure proletimes103
(b)
Figure 3 Boundary conditions for the hemodynamic simulations adapted from [11]
Inlet (descending aorta)
xz y
(a)
Outlet(iliac arteries)
Aortic wall(AAA sac)
x
zy
(b)
Figure 4 Mesh surface different layers are shown aortic wall (dark blue) and inlet (purple) and outlet sections (light blue)
WSS areas (blue) and areas with WSS values higher than themean value as high WSS (red) Analysis of WSS maps forall cases shows that the area of low WSS coincides with thelocation of the recirculation areas (low velocities) and higherWSS values are found in two regions in the neck area and inthe corresponding areawhere the bloodflow jet has an impacton the aneurismal sac The blood flow jet has an impactdirectly on the arterial wall producing higherWSS valuesTheblood flow jet path is provoked by the proximal neck angleconsequently by the AAA tortuosity (see Figure 5) TheseWSS peak values do not influence too much in aneurysmgrowth however in these areas a material failure could beproduced provoked by blood flow jet It is interesting to notethat shear stress levels in all infrarenal aneurysms models arehigher than those in the normal aorta where 120576 is low whichhas a fairly uniform stress shear spatial distributionMaximalvalues are found in the neck region where 120576 is high
Due to the increasing of the internal pressure againstthe aortic walls the AAA diameter grows progressively andeventually it could be able to overcome the resistance of theaortic wall with its breakup This internal pressure is directlyproportional with the aneurysm diameter thereby when thediameter grows the pressure increases High deformationdiameter rate (120594) index could indicate higher internal pres-sure however it should be noticed that the pressure also
depends on the tortuosity index (inversely proportional) andthe flow characteristics (see Figure 5) For instance in case 4even when the section diameter is large the internal pressureis lower than that in case 2 This is originated by a notablypressure drop as a result of the vorticity and flow recirculation(energy losses) in the cases with a high tortuosity index Thiseffect also provokes a pressures gradient between the anteriorand posterior arterial wall in the interior of the AAA sacThese internal high pressure areas inside the sac may indicatethe growth directions of AAA sac
5 Discussions
The objective of this study is to use patient-specific AAAmodels for correlating the geometric indices of the aneurysmwith the hemodynamic loads and eventually with thepotential risk of AAA rupture From a mechanical point ofview AAA ruptures when a maximum stress value over thewall is exceeded The stress peak refers to the mechanicalload sustained by the AAA wall during maximal systolicpressurization In addition it is known that wall stress alonedoes not completely govern failure as an AAA will usuallyrupture when the wall stress exceeds the wall strength Itsvalue depends on arterial systolic pressure the mechanicalproperties and the geometric configuration of the material
6 Computational and Mathematical Methods in Medicine
AAA streamlines AAA sac streamlines details
Cross- sectional
areas
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
3552131574276282368119734157871184
039468078936
0
4654133336167312583320667155103330516670
Cas
e 5
x yz
x yz
x yz
5573949546433523715930966247731858123860619320
x yz
x yz
60112534334675440075333952671620037133580667910
2522222194441666713889111110833330555560277780
|V|
Figure 5 Streamlines details of AAA sac streamline blood flowvelocity and three cross-sectional areas (from the top to the bottom proximalAAA neck and midsection and distal AAA neck) for the five patient studied
under study However the mechanism of arterial wall failuredue to (1) the AAA shape or (2) the pressure distribution isphysically different The first is because of a punctual forceover a wall point and the second is because a consequence
of a pressure distribution over the AAA wall Based on theAAA shape several authors have proposed different criteriafor the AAA collapsibility if the AAAdiameter is higher than55 cm [4] the AAA may rupture or if the asymmetry index
Computational and Mathematical Methods in Medicine 7
WSS anterior WSS posterior Pressure
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
Cas
e 5
High
Low
High
Low
High
Low
High
Low
High
Low
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
37000
37000
37000
37000
37000
33556301112666723222197781633312889944446000
x yz
Figure 6 Anterior and posterior wall shear stress views (high WSS in red and low WSS in blue) and normalized pressure on the aneurysmsac at the peak systole for the five patients
8 Computational and Mathematical Methods in Medicine
factor (120573) is 120573 lt 04 the AAA rupture is high [8] In [10]the AAA collapses when the deformation diameter ratio is120594 gt 33 or if the saccular index is lt06 [11] But depend-ing on the index that is analysed the surgical criteria aredifferent More recently the proposed AAA rupture risk isrelated with the presence of intraluminal thrombus (ILT)[6 26] The intraluminal thrombus plays an important rolein expansion and rupture of advanced aneurysms throughdirectmechanical as well as indirect chemomechanical effects[6] Therefore the AAA dilatation (and a potential rupture)is dependent on the correlation between the geometricalfactor and the hemodynamic load Consequently alternativemethods of AAA rupture assessment are needed
Themajority of these new approaches involve the numer-ical analysis of AAAs using computational fluid dynamics(CFD) to determine the wall shear stress (WSS) distributionsand flow patterns in the aneurysm sac [5 12 13 15 16 30]In our study we did not evaluate the patient-specific wallstrength or the effect of intraluminal thrombus Neverthe-less the AAA cases analyzed provide useful information tounderstanding how hemodynamic loads can affect aneurysmgrowth and possible rupture The pathological cases (cases 1to 4) always present irregular flow in the aneurysm sac nouniform distribution of WSSs and great WSS values in thecurvatures of the aortic vessel These anomalies are propor-tional to the shape of the aneurysm and the angles of twistthat the aorta has Asymmetric flow is always correlated to themodified curvature of the vessel or when some enlargementin the aneurysm is present (high saccular index (120574) andtortuosity (120576) index) The AAA tortuosity could initiate ILTformation and at the same time could provoke arterial wallfailure In a situation where the tortuosity is high and thesaccular index is low the WSS has more effects than thepressure distribution in a possible AAA failure Howeverwhere the AAA is not twisted and the saccular index is highthe pressure effect takes priority In Figure 6 the highest shearstress values are dependent especially on the tortuosity of theAAA The neck angle substantially impacts flow fields caus-ing strong irregular flow patterns in the AAA sac (Figure 5)significantly influencing wall stress distribution (Figure 6)The relationship between these indexes can provide an insightinto themechanism that promotes the thrombus renewal andpossibly enlargement inside the aneurysm
6 Conclusions
To conclude in this work the wall shear stress internalpressure and flow patterns of five patients-specific aortashave been analyzed using a finite element method and theresults have been correlated with the geometrical featuresResults from the patient-specific infrarenal aneurysmmodels(cases 1ndash4) were compared with those of a normal aorta (case5) and it has been found that the normal aorta has a uniformdistribution of the velocity streamlines wall shear stress andpressure compared to that in the pathological cases Maxi-mum wall shear stresses in all infrarenal aneurysm modelsare higher than those in the normal aorta and these valuesare not directly related to the maximum aneurysm diameterproviding evidence that a patient-specific aorta shape analysis
is necessary for a more reliable assessment of the rupturerisk of aortic aneurysms Therefore based on one or twosimple indexes alone to determine the risk of rupture accu-rately is insufficient AAA rupture is a complex situationdepending on themaximum diameter internal pressure wallstress asymmetry saccular index intraluminal thrombusand tortuosity among others Our results demonstrate howthe hemodynamic loads as simulated by computational fluiddynamics (CFD) are influenced by the geometrical factors ofthe aneurysm
Acknowledgment
This project was supported by the NTU-NHG InnovationSeed Grant Project no ISG11007
References
[1] D A Vorp ldquoBiomechanics of abdominal aortic aneurysmrdquoJournal of Biomechanics vol 40 no 9 pp 1887ndash1902 2007
[2] J D Humphrey Cardiovascular Solid Mechanics Cells Tissuesand Organs Springer New York NY USA 2002
[3] J T Powell L C Brown J F Forbes et al ldquoFinal 12-year follow-up of surgery versus surveillance in the UK Small AneurysmTrialrdquoBritish Journal of Surgery vol 94 no 6 pp 702ndash708 2007
[4] S CNicholls J BGardnerMHMeissner andKH JohansenldquoRupture in small abdominal aortic aneurysmsrdquo Journal ofVascular Surgery vol 28 no 5 pp 884ndash888 1998
[5] M L Raghavan and D A Vorp ldquoToward a biomechanical toolto evaluate rupture potential of abdominal aortic aneurysmidentification of a finite strain constitutivemodel and evaluationof its applicabilityrdquo Journal of Biomechanics vol 33 no 4 pp475ndash482 2000
[6] J Biasetti F Hussain and T Christian Gasser ldquoBlood flow andcoherent vortices in the normal and aneurysmatic aortas afluid dynamical approach to intraluminal thrombus formationrdquoJournal of the Royal Society Interface vol 8 no 63 pp 1449ndash1461 2011
[7] C M Scotti and E A Finol ldquoCompliant biomechanicsof abdominal aortic aneurysms a fluid-structure interactionstudyrdquo Computers and Structures vol 85 no 11ndash14 pp 1097ndash1113 2007
[8] D A Vorp M L Raghavan and M W Webster ldquoMechanicalwall stress in abdominal aortic aneurysm influence of diameterand asymmetryrdquo Journal of Vascular Surgery vol 27 no 4 pp632ndash639 1998
[9] E A Finol K Keyhani and C H Amon ldquoThe effect of asym-metry in abdominal aortic aneurysms under physiologicallyrealistic pulsatile flow conditionsrdquo Journal of BiomechanicalEngineering vol 125 no 2 pp 207ndash217 2003
[10] W A Cappeller H Engelmann S Blechschmidt M Wild andL Lauterjung ldquoPossible objectification of a critical maximumdiameter for elective surgery in abdominal aortic aneurysmsbased on one- and three-dimensional ratiosrdquo Journal of Cardio-vascular Surgery vol 38 no 6 pp 623ndash628 1997
[11] K Ouriel R M Green C Donayre C K Shortell J Elliott andJ A DeWeese ldquoAn evaluation of new methods of expressingaortic aneurysm size relationship to rupturerdquo Journal of Vas-cular Surgery vol 15 no 1 pp 12ndash20 1992
[12] T C Gasser M Auer F Labruto J Swedenborg and J RoyldquoBiomechanical rupture risk assessment of abdominal aortic
Computational and Mathematical Methods in Medicine 9
aneurysms model complexity versus predictability of finite ele-ment simulationsrdquo European Journal of Vascular and Endovas-cular Surgery vol 40 no 2 pp 176ndash185 2010
[13] M Bonert R L Leask J Butany et al ldquoThe relationshipbetween wall shear stress distributions and intimal thickeningin the human abdominal aortardquo BioMedical Engineering Onlinevol 2 article 18 2003
[14] D Bluestein L Niu R T Schoephoerster andM K DewanjeeldquoSteady flow in an aneurysm model correlation between fluiddynamics and blood platelet depositionrdquo Journal of Biomechan-ical Engineering vol 118 no 3 pp 280ndash286 1996
[15] M L Raghavan D A VorpM P Federle M S Makaroun andMWWebster ldquoWall stress distribution on three-dimensionallyreconstructed models of human abdominal aortic aneurysmrdquoJournal of Vascular Surgery vol 31 no 4 pp 760ndash769 2000
[16] C Kleinstreuer and Z Li ldquoAnalysis and computer programfor rupture-risk prediction of abdominal aortic aneurysmsrdquoBioMedical Engineering Online vol 5 article 19 2006
[17] J Shum G Martufi E di Martino et al ldquoQuantitative assess-ment of abdominal aortic aneurysm geometryrdquo Annals of Bio-medical Engineering vol 39 no 1 pp 277ndash286 2011
[18] D A Vorp P C Lee D H J Wang et al ldquoAssociation ofintraluminal thrombus in abdominal aortic aneurysm withlocal hypoxia and wall weakeningrdquo Journal of Vascular Surgeryvol 34 no 2 pp 291ndash299 2001
[19] D Bluestein K Dumont M de Beule et al ldquoIntraluminalthrombus and risk of rupture in patient specific abdominalaortic aneurysmmdashFSImodellingrdquoComputerMethods in Biome-chanics and Biomedical Engineering vol 12 no 1 pp 73ndash812009
[20] E Soudah J Pennecot J S Perez M Bordone and E OnateldquoMedical-GiD from medical images to simulations 4D MRIflow analysisrdquo in Computational Vision and Medical ImageProcessing Recent Trends chapter 10 Springer New York NYUSA 1871
[21] E Soudah M Bordone and J S Perez ldquoGmed a platform forimages treatment inside GiD systemrdquo in Proceedings of the 5thConference On Advances And Applications Of GiD Barcelona2010 GiDmdashthe personal pre and postprocessor httpwwwgidhomecom
[22] W E Lorensen and H E Cline ldquoMarching cubes a high reso-lution 3d surface construction algorithmrdquo in Proceedings of the14th Annual Conference on Computer Graphics and InteractiveTechniques (SIGGRAPH rsquo87) pp 163ndash169 1987
[23] M Bordone C Garcıa J Garcıa and E Soudah ldquoBiodyn UserManual TDYN theoretical Backgroundrdquo COMPASSIS 2012httpwwwcompassiscomcompass
[24] E Onate S Idelsohn O C Zienkiewicz and R L Taylor ldquoAfinite point method in computational mechanics Applicationsto convective transport and fluid flowrdquo International Journal forNumerical Methods in Engineering vol 39 no 22 pp 3839ndash3866 1996
[25] Y Papaharilaou J A Ekaterinaris E Manousaki and AN Katsamouris ldquoA decoupled fluid structure approach forestimating wall stress in abdominal aortic aneurysmsrdquo Journalof Biomechanics vol 40 no 2 pp 367ndash377 2007
[26] A-V Salsac S R Sparks J-M Chomaz and J C LasherasldquoEvolution of the wall shear stresses during the progressiveenlargement of symmetric abdominal aortic aneurysmsrdquo Jour-nal of Fluid Mechanics vol 560 pp 19ndash51 2006
[27] C M Scotti J Jimenez S C Muluk and E A Finol ldquoWallstress and flow dynamics in abdominal aortic aneurysms finite
element analysis vs fluid-structure interactionrdquo ComputerMethods in Biomechanics andBiomedical Engineering vol 11 no3 pp 301ndash322 2008
[28] A Borghia N B Wooda R H Mohiaddinb and X Y XualdquoFluid-solid interaction simulationof flow and stress pattern inthoraco abdominal aneurysms a patient-specific studyrdquo Journalof Fluids and Structures vol 24 pp 270ndash280 2008
[29] A Sheidaei S C Hunley S Zeinali-Davarani L G Raguinand S Baek ldquoSimulation of abdominal aortic aneurysm growthwith updating hemodynamic loads using a realistic geometryrdquoMedical Engineering and Physics vol 33 no 1 pp 80ndash88 2011
[30] T Hatakeyama H Shigematsu and T Muto ldquoRisk factors forrupture of abdominal aortic aneurysm based on three-dimen-sional studyrdquo Journal of Vascular Surgery vol 33 no 3 pp 453ndash461 2001
Submit your manuscripts at
httpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
Oxidative Medicine and
Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Parkinsonrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Computational and Mathematical Methods in Medicine 5
09
08
07
06
05
04
03
02
01
00908070605040302010
Time (s)
Vel
oci
ty (
ms
)Inlet velocity prole
(a)
0908070605040302010
Time (s)
16
15
14
13
12
11
10
Pre
ssu
re (
Pa)
Outlet pressure proletimes103
(b)
Figure 3 Boundary conditions for the hemodynamic simulations adapted from [11]
Inlet (descending aorta)
xz y
(a)
Outlet(iliac arteries)
Aortic wall(AAA sac)
x
zy
(b)
Figure 4 Mesh surface different layers are shown aortic wall (dark blue) and inlet (purple) and outlet sections (light blue)
WSS areas (blue) and areas with WSS values higher than themean value as high WSS (red) Analysis of WSS maps forall cases shows that the area of low WSS coincides with thelocation of the recirculation areas (low velocities) and higherWSS values are found in two regions in the neck area and inthe corresponding areawhere the bloodflow jet has an impacton the aneurismal sac The blood flow jet has an impactdirectly on the arterial wall producing higherWSS valuesTheblood flow jet path is provoked by the proximal neck angleconsequently by the AAA tortuosity (see Figure 5) TheseWSS peak values do not influence too much in aneurysmgrowth however in these areas a material failure could beproduced provoked by blood flow jet It is interesting to notethat shear stress levels in all infrarenal aneurysms models arehigher than those in the normal aorta where 120576 is low whichhas a fairly uniform stress shear spatial distributionMaximalvalues are found in the neck region where 120576 is high
Due to the increasing of the internal pressure againstthe aortic walls the AAA diameter grows progressively andeventually it could be able to overcome the resistance of theaortic wall with its breakup This internal pressure is directlyproportional with the aneurysm diameter thereby when thediameter grows the pressure increases High deformationdiameter rate (120594) index could indicate higher internal pres-sure however it should be noticed that the pressure also
depends on the tortuosity index (inversely proportional) andthe flow characteristics (see Figure 5) For instance in case 4even when the section diameter is large the internal pressureis lower than that in case 2 This is originated by a notablypressure drop as a result of the vorticity and flow recirculation(energy losses) in the cases with a high tortuosity index Thiseffect also provokes a pressures gradient between the anteriorand posterior arterial wall in the interior of the AAA sacThese internal high pressure areas inside the sac may indicatethe growth directions of AAA sac
5 Discussions
The objective of this study is to use patient-specific AAAmodels for correlating the geometric indices of the aneurysmwith the hemodynamic loads and eventually with thepotential risk of AAA rupture From a mechanical point ofview AAA ruptures when a maximum stress value over thewall is exceeded The stress peak refers to the mechanicalload sustained by the AAA wall during maximal systolicpressurization In addition it is known that wall stress alonedoes not completely govern failure as an AAA will usuallyrupture when the wall stress exceeds the wall strength Itsvalue depends on arterial systolic pressure the mechanicalproperties and the geometric configuration of the material
6 Computational and Mathematical Methods in Medicine
AAA streamlines AAA sac streamlines details
Cross- sectional
areas
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
3552131574276282368119734157871184
039468078936
0
4654133336167312583320667155103330516670
Cas
e 5
x yz
x yz
x yz
5573949546433523715930966247731858123860619320
x yz
x yz
60112534334675440075333952671620037133580667910
2522222194441666713889111110833330555560277780
|V|
Figure 5 Streamlines details of AAA sac streamline blood flowvelocity and three cross-sectional areas (from the top to the bottom proximalAAA neck and midsection and distal AAA neck) for the five patient studied
under study However the mechanism of arterial wall failuredue to (1) the AAA shape or (2) the pressure distribution isphysically different The first is because of a punctual forceover a wall point and the second is because a consequence
of a pressure distribution over the AAA wall Based on theAAA shape several authors have proposed different criteriafor the AAA collapsibility if the AAAdiameter is higher than55 cm [4] the AAA may rupture or if the asymmetry index
Computational and Mathematical Methods in Medicine 7
WSS anterior WSS posterior Pressure
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
Cas
e 5
High
Low
High
Low
High
Low
High
Low
High
Low
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
37000
37000
37000
37000
37000
33556301112666723222197781633312889944446000
x yz
Figure 6 Anterior and posterior wall shear stress views (high WSS in red and low WSS in blue) and normalized pressure on the aneurysmsac at the peak systole for the five patients
8 Computational and Mathematical Methods in Medicine
factor (120573) is 120573 lt 04 the AAA rupture is high [8] In [10]the AAA collapses when the deformation diameter ratio is120594 gt 33 or if the saccular index is lt06 [11] But depend-ing on the index that is analysed the surgical criteria aredifferent More recently the proposed AAA rupture risk isrelated with the presence of intraluminal thrombus (ILT)[6 26] The intraluminal thrombus plays an important rolein expansion and rupture of advanced aneurysms throughdirectmechanical as well as indirect chemomechanical effects[6] Therefore the AAA dilatation (and a potential rupture)is dependent on the correlation between the geometricalfactor and the hemodynamic load Consequently alternativemethods of AAA rupture assessment are needed
Themajority of these new approaches involve the numer-ical analysis of AAAs using computational fluid dynamics(CFD) to determine the wall shear stress (WSS) distributionsand flow patterns in the aneurysm sac [5 12 13 15 16 30]In our study we did not evaluate the patient-specific wallstrength or the effect of intraluminal thrombus Neverthe-less the AAA cases analyzed provide useful information tounderstanding how hemodynamic loads can affect aneurysmgrowth and possible rupture The pathological cases (cases 1to 4) always present irregular flow in the aneurysm sac nouniform distribution of WSSs and great WSS values in thecurvatures of the aortic vessel These anomalies are propor-tional to the shape of the aneurysm and the angles of twistthat the aorta has Asymmetric flow is always correlated to themodified curvature of the vessel or when some enlargementin the aneurysm is present (high saccular index (120574) andtortuosity (120576) index) The AAA tortuosity could initiate ILTformation and at the same time could provoke arterial wallfailure In a situation where the tortuosity is high and thesaccular index is low the WSS has more effects than thepressure distribution in a possible AAA failure Howeverwhere the AAA is not twisted and the saccular index is highthe pressure effect takes priority In Figure 6 the highest shearstress values are dependent especially on the tortuosity of theAAA The neck angle substantially impacts flow fields caus-ing strong irregular flow patterns in the AAA sac (Figure 5)significantly influencing wall stress distribution (Figure 6)The relationship between these indexes can provide an insightinto themechanism that promotes the thrombus renewal andpossibly enlargement inside the aneurysm
6 Conclusions
To conclude in this work the wall shear stress internalpressure and flow patterns of five patients-specific aortashave been analyzed using a finite element method and theresults have been correlated with the geometrical featuresResults from the patient-specific infrarenal aneurysmmodels(cases 1ndash4) were compared with those of a normal aorta (case5) and it has been found that the normal aorta has a uniformdistribution of the velocity streamlines wall shear stress andpressure compared to that in the pathological cases Maxi-mum wall shear stresses in all infrarenal aneurysm modelsare higher than those in the normal aorta and these valuesare not directly related to the maximum aneurysm diameterproviding evidence that a patient-specific aorta shape analysis
is necessary for a more reliable assessment of the rupturerisk of aortic aneurysms Therefore based on one or twosimple indexes alone to determine the risk of rupture accu-rately is insufficient AAA rupture is a complex situationdepending on themaximum diameter internal pressure wallstress asymmetry saccular index intraluminal thrombusand tortuosity among others Our results demonstrate howthe hemodynamic loads as simulated by computational fluiddynamics (CFD) are influenced by the geometrical factors ofthe aneurysm
Acknowledgment
This project was supported by the NTU-NHG InnovationSeed Grant Project no ISG11007
References
[1] D A Vorp ldquoBiomechanics of abdominal aortic aneurysmrdquoJournal of Biomechanics vol 40 no 9 pp 1887ndash1902 2007
[2] J D Humphrey Cardiovascular Solid Mechanics Cells Tissuesand Organs Springer New York NY USA 2002
[3] J T Powell L C Brown J F Forbes et al ldquoFinal 12-year follow-up of surgery versus surveillance in the UK Small AneurysmTrialrdquoBritish Journal of Surgery vol 94 no 6 pp 702ndash708 2007
[4] S CNicholls J BGardnerMHMeissner andKH JohansenldquoRupture in small abdominal aortic aneurysmsrdquo Journal ofVascular Surgery vol 28 no 5 pp 884ndash888 1998
[5] M L Raghavan and D A Vorp ldquoToward a biomechanical toolto evaluate rupture potential of abdominal aortic aneurysmidentification of a finite strain constitutivemodel and evaluationof its applicabilityrdquo Journal of Biomechanics vol 33 no 4 pp475ndash482 2000
[6] J Biasetti F Hussain and T Christian Gasser ldquoBlood flow andcoherent vortices in the normal and aneurysmatic aortas afluid dynamical approach to intraluminal thrombus formationrdquoJournal of the Royal Society Interface vol 8 no 63 pp 1449ndash1461 2011
[7] C M Scotti and E A Finol ldquoCompliant biomechanicsof abdominal aortic aneurysms a fluid-structure interactionstudyrdquo Computers and Structures vol 85 no 11ndash14 pp 1097ndash1113 2007
[8] D A Vorp M L Raghavan and M W Webster ldquoMechanicalwall stress in abdominal aortic aneurysm influence of diameterand asymmetryrdquo Journal of Vascular Surgery vol 27 no 4 pp632ndash639 1998
[9] E A Finol K Keyhani and C H Amon ldquoThe effect of asym-metry in abdominal aortic aneurysms under physiologicallyrealistic pulsatile flow conditionsrdquo Journal of BiomechanicalEngineering vol 125 no 2 pp 207ndash217 2003
[10] W A Cappeller H Engelmann S Blechschmidt M Wild andL Lauterjung ldquoPossible objectification of a critical maximumdiameter for elective surgery in abdominal aortic aneurysmsbased on one- and three-dimensional ratiosrdquo Journal of Cardio-vascular Surgery vol 38 no 6 pp 623ndash628 1997
[11] K Ouriel R M Green C Donayre C K Shortell J Elliott andJ A DeWeese ldquoAn evaluation of new methods of expressingaortic aneurysm size relationship to rupturerdquo Journal of Vas-cular Surgery vol 15 no 1 pp 12ndash20 1992
[12] T C Gasser M Auer F Labruto J Swedenborg and J RoyldquoBiomechanical rupture risk assessment of abdominal aortic
Computational and Mathematical Methods in Medicine 9
aneurysms model complexity versus predictability of finite ele-ment simulationsrdquo European Journal of Vascular and Endovas-cular Surgery vol 40 no 2 pp 176ndash185 2010
[13] M Bonert R L Leask J Butany et al ldquoThe relationshipbetween wall shear stress distributions and intimal thickeningin the human abdominal aortardquo BioMedical Engineering Onlinevol 2 article 18 2003
[14] D Bluestein L Niu R T Schoephoerster andM K DewanjeeldquoSteady flow in an aneurysm model correlation between fluiddynamics and blood platelet depositionrdquo Journal of Biomechan-ical Engineering vol 118 no 3 pp 280ndash286 1996
[15] M L Raghavan D A VorpM P Federle M S Makaroun andMWWebster ldquoWall stress distribution on three-dimensionallyreconstructed models of human abdominal aortic aneurysmrdquoJournal of Vascular Surgery vol 31 no 4 pp 760ndash769 2000
[16] C Kleinstreuer and Z Li ldquoAnalysis and computer programfor rupture-risk prediction of abdominal aortic aneurysmsrdquoBioMedical Engineering Online vol 5 article 19 2006
[17] J Shum G Martufi E di Martino et al ldquoQuantitative assess-ment of abdominal aortic aneurysm geometryrdquo Annals of Bio-medical Engineering vol 39 no 1 pp 277ndash286 2011
[18] D A Vorp P C Lee D H J Wang et al ldquoAssociation ofintraluminal thrombus in abdominal aortic aneurysm withlocal hypoxia and wall weakeningrdquo Journal of Vascular Surgeryvol 34 no 2 pp 291ndash299 2001
[19] D Bluestein K Dumont M de Beule et al ldquoIntraluminalthrombus and risk of rupture in patient specific abdominalaortic aneurysmmdashFSImodellingrdquoComputerMethods in Biome-chanics and Biomedical Engineering vol 12 no 1 pp 73ndash812009
[20] E Soudah J Pennecot J S Perez M Bordone and E OnateldquoMedical-GiD from medical images to simulations 4D MRIflow analysisrdquo in Computational Vision and Medical ImageProcessing Recent Trends chapter 10 Springer New York NYUSA 1871
[21] E Soudah M Bordone and J S Perez ldquoGmed a platform forimages treatment inside GiD systemrdquo in Proceedings of the 5thConference On Advances And Applications Of GiD Barcelona2010 GiDmdashthe personal pre and postprocessor httpwwwgidhomecom
[22] W E Lorensen and H E Cline ldquoMarching cubes a high reso-lution 3d surface construction algorithmrdquo in Proceedings of the14th Annual Conference on Computer Graphics and InteractiveTechniques (SIGGRAPH rsquo87) pp 163ndash169 1987
[23] M Bordone C Garcıa J Garcıa and E Soudah ldquoBiodyn UserManual TDYN theoretical Backgroundrdquo COMPASSIS 2012httpwwwcompassiscomcompass
[24] E Onate S Idelsohn O C Zienkiewicz and R L Taylor ldquoAfinite point method in computational mechanics Applicationsto convective transport and fluid flowrdquo International Journal forNumerical Methods in Engineering vol 39 no 22 pp 3839ndash3866 1996
[25] Y Papaharilaou J A Ekaterinaris E Manousaki and AN Katsamouris ldquoA decoupled fluid structure approach forestimating wall stress in abdominal aortic aneurysmsrdquo Journalof Biomechanics vol 40 no 2 pp 367ndash377 2007
[26] A-V Salsac S R Sparks J-M Chomaz and J C LasherasldquoEvolution of the wall shear stresses during the progressiveenlargement of symmetric abdominal aortic aneurysmsrdquo Jour-nal of Fluid Mechanics vol 560 pp 19ndash51 2006
[27] C M Scotti J Jimenez S C Muluk and E A Finol ldquoWallstress and flow dynamics in abdominal aortic aneurysms finite
element analysis vs fluid-structure interactionrdquo ComputerMethods in Biomechanics andBiomedical Engineering vol 11 no3 pp 301ndash322 2008
[28] A Borghia N B Wooda R H Mohiaddinb and X Y XualdquoFluid-solid interaction simulationof flow and stress pattern inthoraco abdominal aneurysms a patient-specific studyrdquo Journalof Fluids and Structures vol 24 pp 270ndash280 2008
[29] A Sheidaei S C Hunley S Zeinali-Davarani L G Raguinand S Baek ldquoSimulation of abdominal aortic aneurysm growthwith updating hemodynamic loads using a realistic geometryrdquoMedical Engineering and Physics vol 33 no 1 pp 80ndash88 2011
[30] T Hatakeyama H Shigematsu and T Muto ldquoRisk factors forrupture of abdominal aortic aneurysm based on three-dimen-sional studyrdquo Journal of Vascular Surgery vol 33 no 3 pp 453ndash461 2001
Submit your manuscripts at
httpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
Oxidative Medicine and
Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Parkinsonrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Computational and Mathematical Methods in Medicine
AAA streamlines AAA sac streamlines details
Cross- sectional
areas
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
3552131574276282368119734157871184
039468078936
0
4654133336167312583320667155103330516670
Cas
e 5
x yz
x yz
x yz
5573949546433523715930966247731858123860619320
x yz
x yz
60112534334675440075333952671620037133580667910
2522222194441666713889111110833330555560277780
|V|
Figure 5 Streamlines details of AAA sac streamline blood flowvelocity and three cross-sectional areas (from the top to the bottom proximalAAA neck and midsection and distal AAA neck) for the five patient studied
under study However the mechanism of arterial wall failuredue to (1) the AAA shape or (2) the pressure distribution isphysically different The first is because of a punctual forceover a wall point and the second is because a consequence
of a pressure distribution over the AAA wall Based on theAAA shape several authors have proposed different criteriafor the AAA collapsibility if the AAAdiameter is higher than55 cm [4] the AAA may rupture or if the asymmetry index
Computational and Mathematical Methods in Medicine 7
WSS anterior WSS posterior Pressure
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
Cas
e 5
High
Low
High
Low
High
Low
High
Low
High
Low
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
37000
37000
37000
37000
37000
33556301112666723222197781633312889944446000
x yz
Figure 6 Anterior and posterior wall shear stress views (high WSS in red and low WSS in blue) and normalized pressure on the aneurysmsac at the peak systole for the five patients
8 Computational and Mathematical Methods in Medicine
factor (120573) is 120573 lt 04 the AAA rupture is high [8] In [10]the AAA collapses when the deformation diameter ratio is120594 gt 33 or if the saccular index is lt06 [11] But depend-ing on the index that is analysed the surgical criteria aredifferent More recently the proposed AAA rupture risk isrelated with the presence of intraluminal thrombus (ILT)[6 26] The intraluminal thrombus plays an important rolein expansion and rupture of advanced aneurysms throughdirectmechanical as well as indirect chemomechanical effects[6] Therefore the AAA dilatation (and a potential rupture)is dependent on the correlation between the geometricalfactor and the hemodynamic load Consequently alternativemethods of AAA rupture assessment are needed
Themajority of these new approaches involve the numer-ical analysis of AAAs using computational fluid dynamics(CFD) to determine the wall shear stress (WSS) distributionsand flow patterns in the aneurysm sac [5 12 13 15 16 30]In our study we did not evaluate the patient-specific wallstrength or the effect of intraluminal thrombus Neverthe-less the AAA cases analyzed provide useful information tounderstanding how hemodynamic loads can affect aneurysmgrowth and possible rupture The pathological cases (cases 1to 4) always present irregular flow in the aneurysm sac nouniform distribution of WSSs and great WSS values in thecurvatures of the aortic vessel These anomalies are propor-tional to the shape of the aneurysm and the angles of twistthat the aorta has Asymmetric flow is always correlated to themodified curvature of the vessel or when some enlargementin the aneurysm is present (high saccular index (120574) andtortuosity (120576) index) The AAA tortuosity could initiate ILTformation and at the same time could provoke arterial wallfailure In a situation where the tortuosity is high and thesaccular index is low the WSS has more effects than thepressure distribution in a possible AAA failure Howeverwhere the AAA is not twisted and the saccular index is highthe pressure effect takes priority In Figure 6 the highest shearstress values are dependent especially on the tortuosity of theAAA The neck angle substantially impacts flow fields caus-ing strong irregular flow patterns in the AAA sac (Figure 5)significantly influencing wall stress distribution (Figure 6)The relationship between these indexes can provide an insightinto themechanism that promotes the thrombus renewal andpossibly enlargement inside the aneurysm
6 Conclusions
To conclude in this work the wall shear stress internalpressure and flow patterns of five patients-specific aortashave been analyzed using a finite element method and theresults have been correlated with the geometrical featuresResults from the patient-specific infrarenal aneurysmmodels(cases 1ndash4) were compared with those of a normal aorta (case5) and it has been found that the normal aorta has a uniformdistribution of the velocity streamlines wall shear stress andpressure compared to that in the pathological cases Maxi-mum wall shear stresses in all infrarenal aneurysm modelsare higher than those in the normal aorta and these valuesare not directly related to the maximum aneurysm diameterproviding evidence that a patient-specific aorta shape analysis
is necessary for a more reliable assessment of the rupturerisk of aortic aneurysms Therefore based on one or twosimple indexes alone to determine the risk of rupture accu-rately is insufficient AAA rupture is a complex situationdepending on themaximum diameter internal pressure wallstress asymmetry saccular index intraluminal thrombusand tortuosity among others Our results demonstrate howthe hemodynamic loads as simulated by computational fluiddynamics (CFD) are influenced by the geometrical factors ofthe aneurysm
Acknowledgment
This project was supported by the NTU-NHG InnovationSeed Grant Project no ISG11007
References
[1] D A Vorp ldquoBiomechanics of abdominal aortic aneurysmrdquoJournal of Biomechanics vol 40 no 9 pp 1887ndash1902 2007
[2] J D Humphrey Cardiovascular Solid Mechanics Cells Tissuesand Organs Springer New York NY USA 2002
[3] J T Powell L C Brown J F Forbes et al ldquoFinal 12-year follow-up of surgery versus surveillance in the UK Small AneurysmTrialrdquoBritish Journal of Surgery vol 94 no 6 pp 702ndash708 2007
[4] S CNicholls J BGardnerMHMeissner andKH JohansenldquoRupture in small abdominal aortic aneurysmsrdquo Journal ofVascular Surgery vol 28 no 5 pp 884ndash888 1998
[5] M L Raghavan and D A Vorp ldquoToward a biomechanical toolto evaluate rupture potential of abdominal aortic aneurysmidentification of a finite strain constitutivemodel and evaluationof its applicabilityrdquo Journal of Biomechanics vol 33 no 4 pp475ndash482 2000
[6] J Biasetti F Hussain and T Christian Gasser ldquoBlood flow andcoherent vortices in the normal and aneurysmatic aortas afluid dynamical approach to intraluminal thrombus formationrdquoJournal of the Royal Society Interface vol 8 no 63 pp 1449ndash1461 2011
[7] C M Scotti and E A Finol ldquoCompliant biomechanicsof abdominal aortic aneurysms a fluid-structure interactionstudyrdquo Computers and Structures vol 85 no 11ndash14 pp 1097ndash1113 2007
[8] D A Vorp M L Raghavan and M W Webster ldquoMechanicalwall stress in abdominal aortic aneurysm influence of diameterand asymmetryrdquo Journal of Vascular Surgery vol 27 no 4 pp632ndash639 1998
[9] E A Finol K Keyhani and C H Amon ldquoThe effect of asym-metry in abdominal aortic aneurysms under physiologicallyrealistic pulsatile flow conditionsrdquo Journal of BiomechanicalEngineering vol 125 no 2 pp 207ndash217 2003
[10] W A Cappeller H Engelmann S Blechschmidt M Wild andL Lauterjung ldquoPossible objectification of a critical maximumdiameter for elective surgery in abdominal aortic aneurysmsbased on one- and three-dimensional ratiosrdquo Journal of Cardio-vascular Surgery vol 38 no 6 pp 623ndash628 1997
[11] K Ouriel R M Green C Donayre C K Shortell J Elliott andJ A DeWeese ldquoAn evaluation of new methods of expressingaortic aneurysm size relationship to rupturerdquo Journal of Vas-cular Surgery vol 15 no 1 pp 12ndash20 1992
[12] T C Gasser M Auer F Labruto J Swedenborg and J RoyldquoBiomechanical rupture risk assessment of abdominal aortic
Computational and Mathematical Methods in Medicine 9
aneurysms model complexity versus predictability of finite ele-ment simulationsrdquo European Journal of Vascular and Endovas-cular Surgery vol 40 no 2 pp 176ndash185 2010
[13] M Bonert R L Leask J Butany et al ldquoThe relationshipbetween wall shear stress distributions and intimal thickeningin the human abdominal aortardquo BioMedical Engineering Onlinevol 2 article 18 2003
[14] D Bluestein L Niu R T Schoephoerster andM K DewanjeeldquoSteady flow in an aneurysm model correlation between fluiddynamics and blood platelet depositionrdquo Journal of Biomechan-ical Engineering vol 118 no 3 pp 280ndash286 1996
[15] M L Raghavan D A VorpM P Federle M S Makaroun andMWWebster ldquoWall stress distribution on three-dimensionallyreconstructed models of human abdominal aortic aneurysmrdquoJournal of Vascular Surgery vol 31 no 4 pp 760ndash769 2000
[16] C Kleinstreuer and Z Li ldquoAnalysis and computer programfor rupture-risk prediction of abdominal aortic aneurysmsrdquoBioMedical Engineering Online vol 5 article 19 2006
[17] J Shum G Martufi E di Martino et al ldquoQuantitative assess-ment of abdominal aortic aneurysm geometryrdquo Annals of Bio-medical Engineering vol 39 no 1 pp 277ndash286 2011
[18] D A Vorp P C Lee D H J Wang et al ldquoAssociation ofintraluminal thrombus in abdominal aortic aneurysm withlocal hypoxia and wall weakeningrdquo Journal of Vascular Surgeryvol 34 no 2 pp 291ndash299 2001
[19] D Bluestein K Dumont M de Beule et al ldquoIntraluminalthrombus and risk of rupture in patient specific abdominalaortic aneurysmmdashFSImodellingrdquoComputerMethods in Biome-chanics and Biomedical Engineering vol 12 no 1 pp 73ndash812009
[20] E Soudah J Pennecot J S Perez M Bordone and E OnateldquoMedical-GiD from medical images to simulations 4D MRIflow analysisrdquo in Computational Vision and Medical ImageProcessing Recent Trends chapter 10 Springer New York NYUSA 1871
[21] E Soudah M Bordone and J S Perez ldquoGmed a platform forimages treatment inside GiD systemrdquo in Proceedings of the 5thConference On Advances And Applications Of GiD Barcelona2010 GiDmdashthe personal pre and postprocessor httpwwwgidhomecom
[22] W E Lorensen and H E Cline ldquoMarching cubes a high reso-lution 3d surface construction algorithmrdquo in Proceedings of the14th Annual Conference on Computer Graphics and InteractiveTechniques (SIGGRAPH rsquo87) pp 163ndash169 1987
[23] M Bordone C Garcıa J Garcıa and E Soudah ldquoBiodyn UserManual TDYN theoretical Backgroundrdquo COMPASSIS 2012httpwwwcompassiscomcompass
[24] E Onate S Idelsohn O C Zienkiewicz and R L Taylor ldquoAfinite point method in computational mechanics Applicationsto convective transport and fluid flowrdquo International Journal forNumerical Methods in Engineering vol 39 no 22 pp 3839ndash3866 1996
[25] Y Papaharilaou J A Ekaterinaris E Manousaki and AN Katsamouris ldquoA decoupled fluid structure approach forestimating wall stress in abdominal aortic aneurysmsrdquo Journalof Biomechanics vol 40 no 2 pp 367ndash377 2007
[26] A-V Salsac S R Sparks J-M Chomaz and J C LasherasldquoEvolution of the wall shear stresses during the progressiveenlargement of symmetric abdominal aortic aneurysmsrdquo Jour-nal of Fluid Mechanics vol 560 pp 19ndash51 2006
[27] C M Scotti J Jimenez S C Muluk and E A Finol ldquoWallstress and flow dynamics in abdominal aortic aneurysms finite
element analysis vs fluid-structure interactionrdquo ComputerMethods in Biomechanics andBiomedical Engineering vol 11 no3 pp 301ndash322 2008
[28] A Borghia N B Wooda R H Mohiaddinb and X Y XualdquoFluid-solid interaction simulationof flow and stress pattern inthoraco abdominal aneurysms a patient-specific studyrdquo Journalof Fluids and Structures vol 24 pp 270ndash280 2008
[29] A Sheidaei S C Hunley S Zeinali-Davarani L G Raguinand S Baek ldquoSimulation of abdominal aortic aneurysm growthwith updating hemodynamic loads using a realistic geometryrdquoMedical Engineering and Physics vol 33 no 1 pp 80ndash88 2011
[30] T Hatakeyama H Shigematsu and T Muto ldquoRisk factors forrupture of abdominal aortic aneurysm based on three-dimen-sional studyrdquo Journal of Vascular Surgery vol 33 no 3 pp 453ndash461 2001
Submit your manuscripts at
httpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
Oxidative Medicine and
Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Parkinsonrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Computational and Mathematical Methods in Medicine 7
WSS anterior WSS posterior Pressure
Cas
e 1
Cas
e 2
Cas
e 3
Cas
e 4
Cas
e 5
High
Low
High
Low
High
Low
High
Low
High
Low
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
33556301112666723222197781633312889944446000
x yz
37000
37000
37000
37000
37000
33556301112666723222197781633312889944446000
x yz
Figure 6 Anterior and posterior wall shear stress views (high WSS in red and low WSS in blue) and normalized pressure on the aneurysmsac at the peak systole for the five patients
8 Computational and Mathematical Methods in Medicine
factor (120573) is 120573 lt 04 the AAA rupture is high [8] In [10]the AAA collapses when the deformation diameter ratio is120594 gt 33 or if the saccular index is lt06 [11] But depend-ing on the index that is analysed the surgical criteria aredifferent More recently the proposed AAA rupture risk isrelated with the presence of intraluminal thrombus (ILT)[6 26] The intraluminal thrombus plays an important rolein expansion and rupture of advanced aneurysms throughdirectmechanical as well as indirect chemomechanical effects[6] Therefore the AAA dilatation (and a potential rupture)is dependent on the correlation between the geometricalfactor and the hemodynamic load Consequently alternativemethods of AAA rupture assessment are needed
Themajority of these new approaches involve the numer-ical analysis of AAAs using computational fluid dynamics(CFD) to determine the wall shear stress (WSS) distributionsand flow patterns in the aneurysm sac [5 12 13 15 16 30]In our study we did not evaluate the patient-specific wallstrength or the effect of intraluminal thrombus Neverthe-less the AAA cases analyzed provide useful information tounderstanding how hemodynamic loads can affect aneurysmgrowth and possible rupture The pathological cases (cases 1to 4) always present irregular flow in the aneurysm sac nouniform distribution of WSSs and great WSS values in thecurvatures of the aortic vessel These anomalies are propor-tional to the shape of the aneurysm and the angles of twistthat the aorta has Asymmetric flow is always correlated to themodified curvature of the vessel or when some enlargementin the aneurysm is present (high saccular index (120574) andtortuosity (120576) index) The AAA tortuosity could initiate ILTformation and at the same time could provoke arterial wallfailure In a situation where the tortuosity is high and thesaccular index is low the WSS has more effects than thepressure distribution in a possible AAA failure Howeverwhere the AAA is not twisted and the saccular index is highthe pressure effect takes priority In Figure 6 the highest shearstress values are dependent especially on the tortuosity of theAAA The neck angle substantially impacts flow fields caus-ing strong irregular flow patterns in the AAA sac (Figure 5)significantly influencing wall stress distribution (Figure 6)The relationship between these indexes can provide an insightinto themechanism that promotes the thrombus renewal andpossibly enlargement inside the aneurysm
6 Conclusions
To conclude in this work the wall shear stress internalpressure and flow patterns of five patients-specific aortashave been analyzed using a finite element method and theresults have been correlated with the geometrical featuresResults from the patient-specific infrarenal aneurysmmodels(cases 1ndash4) were compared with those of a normal aorta (case5) and it has been found that the normal aorta has a uniformdistribution of the velocity streamlines wall shear stress andpressure compared to that in the pathological cases Maxi-mum wall shear stresses in all infrarenal aneurysm modelsare higher than those in the normal aorta and these valuesare not directly related to the maximum aneurysm diameterproviding evidence that a patient-specific aorta shape analysis
is necessary for a more reliable assessment of the rupturerisk of aortic aneurysms Therefore based on one or twosimple indexes alone to determine the risk of rupture accu-rately is insufficient AAA rupture is a complex situationdepending on themaximum diameter internal pressure wallstress asymmetry saccular index intraluminal thrombusand tortuosity among others Our results demonstrate howthe hemodynamic loads as simulated by computational fluiddynamics (CFD) are influenced by the geometrical factors ofthe aneurysm
Acknowledgment
This project was supported by the NTU-NHG InnovationSeed Grant Project no ISG11007
References
[1] D A Vorp ldquoBiomechanics of abdominal aortic aneurysmrdquoJournal of Biomechanics vol 40 no 9 pp 1887ndash1902 2007
[2] J D Humphrey Cardiovascular Solid Mechanics Cells Tissuesand Organs Springer New York NY USA 2002
[3] J T Powell L C Brown J F Forbes et al ldquoFinal 12-year follow-up of surgery versus surveillance in the UK Small AneurysmTrialrdquoBritish Journal of Surgery vol 94 no 6 pp 702ndash708 2007
[4] S CNicholls J BGardnerMHMeissner andKH JohansenldquoRupture in small abdominal aortic aneurysmsrdquo Journal ofVascular Surgery vol 28 no 5 pp 884ndash888 1998
[5] M L Raghavan and D A Vorp ldquoToward a biomechanical toolto evaluate rupture potential of abdominal aortic aneurysmidentification of a finite strain constitutivemodel and evaluationof its applicabilityrdquo Journal of Biomechanics vol 33 no 4 pp475ndash482 2000
[6] J Biasetti F Hussain and T Christian Gasser ldquoBlood flow andcoherent vortices in the normal and aneurysmatic aortas afluid dynamical approach to intraluminal thrombus formationrdquoJournal of the Royal Society Interface vol 8 no 63 pp 1449ndash1461 2011
[7] C M Scotti and E A Finol ldquoCompliant biomechanicsof abdominal aortic aneurysms a fluid-structure interactionstudyrdquo Computers and Structures vol 85 no 11ndash14 pp 1097ndash1113 2007
[8] D A Vorp M L Raghavan and M W Webster ldquoMechanicalwall stress in abdominal aortic aneurysm influence of diameterand asymmetryrdquo Journal of Vascular Surgery vol 27 no 4 pp632ndash639 1998
[9] E A Finol K Keyhani and C H Amon ldquoThe effect of asym-metry in abdominal aortic aneurysms under physiologicallyrealistic pulsatile flow conditionsrdquo Journal of BiomechanicalEngineering vol 125 no 2 pp 207ndash217 2003
[10] W A Cappeller H Engelmann S Blechschmidt M Wild andL Lauterjung ldquoPossible objectification of a critical maximumdiameter for elective surgery in abdominal aortic aneurysmsbased on one- and three-dimensional ratiosrdquo Journal of Cardio-vascular Surgery vol 38 no 6 pp 623ndash628 1997
[11] K Ouriel R M Green C Donayre C K Shortell J Elliott andJ A DeWeese ldquoAn evaluation of new methods of expressingaortic aneurysm size relationship to rupturerdquo Journal of Vas-cular Surgery vol 15 no 1 pp 12ndash20 1992
[12] T C Gasser M Auer F Labruto J Swedenborg and J RoyldquoBiomechanical rupture risk assessment of abdominal aortic
Computational and Mathematical Methods in Medicine 9
aneurysms model complexity versus predictability of finite ele-ment simulationsrdquo European Journal of Vascular and Endovas-cular Surgery vol 40 no 2 pp 176ndash185 2010
[13] M Bonert R L Leask J Butany et al ldquoThe relationshipbetween wall shear stress distributions and intimal thickeningin the human abdominal aortardquo BioMedical Engineering Onlinevol 2 article 18 2003
[14] D Bluestein L Niu R T Schoephoerster andM K DewanjeeldquoSteady flow in an aneurysm model correlation between fluiddynamics and blood platelet depositionrdquo Journal of Biomechan-ical Engineering vol 118 no 3 pp 280ndash286 1996
[15] M L Raghavan D A VorpM P Federle M S Makaroun andMWWebster ldquoWall stress distribution on three-dimensionallyreconstructed models of human abdominal aortic aneurysmrdquoJournal of Vascular Surgery vol 31 no 4 pp 760ndash769 2000
[16] C Kleinstreuer and Z Li ldquoAnalysis and computer programfor rupture-risk prediction of abdominal aortic aneurysmsrdquoBioMedical Engineering Online vol 5 article 19 2006
[17] J Shum G Martufi E di Martino et al ldquoQuantitative assess-ment of abdominal aortic aneurysm geometryrdquo Annals of Bio-medical Engineering vol 39 no 1 pp 277ndash286 2011
[18] D A Vorp P C Lee D H J Wang et al ldquoAssociation ofintraluminal thrombus in abdominal aortic aneurysm withlocal hypoxia and wall weakeningrdquo Journal of Vascular Surgeryvol 34 no 2 pp 291ndash299 2001
[19] D Bluestein K Dumont M de Beule et al ldquoIntraluminalthrombus and risk of rupture in patient specific abdominalaortic aneurysmmdashFSImodellingrdquoComputerMethods in Biome-chanics and Biomedical Engineering vol 12 no 1 pp 73ndash812009
[20] E Soudah J Pennecot J S Perez M Bordone and E OnateldquoMedical-GiD from medical images to simulations 4D MRIflow analysisrdquo in Computational Vision and Medical ImageProcessing Recent Trends chapter 10 Springer New York NYUSA 1871
[21] E Soudah M Bordone and J S Perez ldquoGmed a platform forimages treatment inside GiD systemrdquo in Proceedings of the 5thConference On Advances And Applications Of GiD Barcelona2010 GiDmdashthe personal pre and postprocessor httpwwwgidhomecom
[22] W E Lorensen and H E Cline ldquoMarching cubes a high reso-lution 3d surface construction algorithmrdquo in Proceedings of the14th Annual Conference on Computer Graphics and InteractiveTechniques (SIGGRAPH rsquo87) pp 163ndash169 1987
[23] M Bordone C Garcıa J Garcıa and E Soudah ldquoBiodyn UserManual TDYN theoretical Backgroundrdquo COMPASSIS 2012httpwwwcompassiscomcompass
[24] E Onate S Idelsohn O C Zienkiewicz and R L Taylor ldquoAfinite point method in computational mechanics Applicationsto convective transport and fluid flowrdquo International Journal forNumerical Methods in Engineering vol 39 no 22 pp 3839ndash3866 1996
[25] Y Papaharilaou J A Ekaterinaris E Manousaki and AN Katsamouris ldquoA decoupled fluid structure approach forestimating wall stress in abdominal aortic aneurysmsrdquo Journalof Biomechanics vol 40 no 2 pp 367ndash377 2007
[26] A-V Salsac S R Sparks J-M Chomaz and J C LasherasldquoEvolution of the wall shear stresses during the progressiveenlargement of symmetric abdominal aortic aneurysmsrdquo Jour-nal of Fluid Mechanics vol 560 pp 19ndash51 2006
[27] C M Scotti J Jimenez S C Muluk and E A Finol ldquoWallstress and flow dynamics in abdominal aortic aneurysms finite
element analysis vs fluid-structure interactionrdquo ComputerMethods in Biomechanics andBiomedical Engineering vol 11 no3 pp 301ndash322 2008
[28] A Borghia N B Wooda R H Mohiaddinb and X Y XualdquoFluid-solid interaction simulationof flow and stress pattern inthoraco abdominal aneurysms a patient-specific studyrdquo Journalof Fluids and Structures vol 24 pp 270ndash280 2008
[29] A Sheidaei S C Hunley S Zeinali-Davarani L G Raguinand S Baek ldquoSimulation of abdominal aortic aneurysm growthwith updating hemodynamic loads using a realistic geometryrdquoMedical Engineering and Physics vol 33 no 1 pp 80ndash88 2011
[30] T Hatakeyama H Shigematsu and T Muto ldquoRisk factors forrupture of abdominal aortic aneurysm based on three-dimen-sional studyrdquo Journal of Vascular Surgery vol 33 no 3 pp 453ndash461 2001
Submit your manuscripts at
httpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
Oxidative Medicine and
Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Parkinsonrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 Computational and Mathematical Methods in Medicine
factor (120573) is 120573 lt 04 the AAA rupture is high [8] In [10]the AAA collapses when the deformation diameter ratio is120594 gt 33 or if the saccular index is lt06 [11] But depend-ing on the index that is analysed the surgical criteria aredifferent More recently the proposed AAA rupture risk isrelated with the presence of intraluminal thrombus (ILT)[6 26] The intraluminal thrombus plays an important rolein expansion and rupture of advanced aneurysms throughdirectmechanical as well as indirect chemomechanical effects[6] Therefore the AAA dilatation (and a potential rupture)is dependent on the correlation between the geometricalfactor and the hemodynamic load Consequently alternativemethods of AAA rupture assessment are needed
Themajority of these new approaches involve the numer-ical analysis of AAAs using computational fluid dynamics(CFD) to determine the wall shear stress (WSS) distributionsand flow patterns in the aneurysm sac [5 12 13 15 16 30]In our study we did not evaluate the patient-specific wallstrength or the effect of intraluminal thrombus Neverthe-less the AAA cases analyzed provide useful information tounderstanding how hemodynamic loads can affect aneurysmgrowth and possible rupture The pathological cases (cases 1to 4) always present irregular flow in the aneurysm sac nouniform distribution of WSSs and great WSS values in thecurvatures of the aortic vessel These anomalies are propor-tional to the shape of the aneurysm and the angles of twistthat the aorta has Asymmetric flow is always correlated to themodified curvature of the vessel or when some enlargementin the aneurysm is present (high saccular index (120574) andtortuosity (120576) index) The AAA tortuosity could initiate ILTformation and at the same time could provoke arterial wallfailure In a situation where the tortuosity is high and thesaccular index is low the WSS has more effects than thepressure distribution in a possible AAA failure Howeverwhere the AAA is not twisted and the saccular index is highthe pressure effect takes priority In Figure 6 the highest shearstress values are dependent especially on the tortuosity of theAAA The neck angle substantially impacts flow fields caus-ing strong irregular flow patterns in the AAA sac (Figure 5)significantly influencing wall stress distribution (Figure 6)The relationship between these indexes can provide an insightinto themechanism that promotes the thrombus renewal andpossibly enlargement inside the aneurysm
6 Conclusions
To conclude in this work the wall shear stress internalpressure and flow patterns of five patients-specific aortashave been analyzed using a finite element method and theresults have been correlated with the geometrical featuresResults from the patient-specific infrarenal aneurysmmodels(cases 1ndash4) were compared with those of a normal aorta (case5) and it has been found that the normal aorta has a uniformdistribution of the velocity streamlines wall shear stress andpressure compared to that in the pathological cases Maxi-mum wall shear stresses in all infrarenal aneurysm modelsare higher than those in the normal aorta and these valuesare not directly related to the maximum aneurysm diameterproviding evidence that a patient-specific aorta shape analysis
is necessary for a more reliable assessment of the rupturerisk of aortic aneurysms Therefore based on one or twosimple indexes alone to determine the risk of rupture accu-rately is insufficient AAA rupture is a complex situationdepending on themaximum diameter internal pressure wallstress asymmetry saccular index intraluminal thrombusand tortuosity among others Our results demonstrate howthe hemodynamic loads as simulated by computational fluiddynamics (CFD) are influenced by the geometrical factors ofthe aneurysm
Acknowledgment
This project was supported by the NTU-NHG InnovationSeed Grant Project no ISG11007
References
[1] D A Vorp ldquoBiomechanics of abdominal aortic aneurysmrdquoJournal of Biomechanics vol 40 no 9 pp 1887ndash1902 2007
[2] J D Humphrey Cardiovascular Solid Mechanics Cells Tissuesand Organs Springer New York NY USA 2002
[3] J T Powell L C Brown J F Forbes et al ldquoFinal 12-year follow-up of surgery versus surveillance in the UK Small AneurysmTrialrdquoBritish Journal of Surgery vol 94 no 6 pp 702ndash708 2007
[4] S CNicholls J BGardnerMHMeissner andKH JohansenldquoRupture in small abdominal aortic aneurysmsrdquo Journal ofVascular Surgery vol 28 no 5 pp 884ndash888 1998
[5] M L Raghavan and D A Vorp ldquoToward a biomechanical toolto evaluate rupture potential of abdominal aortic aneurysmidentification of a finite strain constitutivemodel and evaluationof its applicabilityrdquo Journal of Biomechanics vol 33 no 4 pp475ndash482 2000
[6] J Biasetti F Hussain and T Christian Gasser ldquoBlood flow andcoherent vortices in the normal and aneurysmatic aortas afluid dynamical approach to intraluminal thrombus formationrdquoJournal of the Royal Society Interface vol 8 no 63 pp 1449ndash1461 2011
[7] C M Scotti and E A Finol ldquoCompliant biomechanicsof abdominal aortic aneurysms a fluid-structure interactionstudyrdquo Computers and Structures vol 85 no 11ndash14 pp 1097ndash1113 2007
[8] D A Vorp M L Raghavan and M W Webster ldquoMechanicalwall stress in abdominal aortic aneurysm influence of diameterand asymmetryrdquo Journal of Vascular Surgery vol 27 no 4 pp632ndash639 1998
[9] E A Finol K Keyhani and C H Amon ldquoThe effect of asym-metry in abdominal aortic aneurysms under physiologicallyrealistic pulsatile flow conditionsrdquo Journal of BiomechanicalEngineering vol 125 no 2 pp 207ndash217 2003
[10] W A Cappeller H Engelmann S Blechschmidt M Wild andL Lauterjung ldquoPossible objectification of a critical maximumdiameter for elective surgery in abdominal aortic aneurysmsbased on one- and three-dimensional ratiosrdquo Journal of Cardio-vascular Surgery vol 38 no 6 pp 623ndash628 1997
[11] K Ouriel R M Green C Donayre C K Shortell J Elliott andJ A DeWeese ldquoAn evaluation of new methods of expressingaortic aneurysm size relationship to rupturerdquo Journal of Vas-cular Surgery vol 15 no 1 pp 12ndash20 1992
[12] T C Gasser M Auer F Labruto J Swedenborg and J RoyldquoBiomechanical rupture risk assessment of abdominal aortic
Computational and Mathematical Methods in Medicine 9
aneurysms model complexity versus predictability of finite ele-ment simulationsrdquo European Journal of Vascular and Endovas-cular Surgery vol 40 no 2 pp 176ndash185 2010
[13] M Bonert R L Leask J Butany et al ldquoThe relationshipbetween wall shear stress distributions and intimal thickeningin the human abdominal aortardquo BioMedical Engineering Onlinevol 2 article 18 2003
[14] D Bluestein L Niu R T Schoephoerster andM K DewanjeeldquoSteady flow in an aneurysm model correlation between fluiddynamics and blood platelet depositionrdquo Journal of Biomechan-ical Engineering vol 118 no 3 pp 280ndash286 1996
[15] M L Raghavan D A VorpM P Federle M S Makaroun andMWWebster ldquoWall stress distribution on three-dimensionallyreconstructed models of human abdominal aortic aneurysmrdquoJournal of Vascular Surgery vol 31 no 4 pp 760ndash769 2000
[16] C Kleinstreuer and Z Li ldquoAnalysis and computer programfor rupture-risk prediction of abdominal aortic aneurysmsrdquoBioMedical Engineering Online vol 5 article 19 2006
[17] J Shum G Martufi E di Martino et al ldquoQuantitative assess-ment of abdominal aortic aneurysm geometryrdquo Annals of Bio-medical Engineering vol 39 no 1 pp 277ndash286 2011
[18] D A Vorp P C Lee D H J Wang et al ldquoAssociation ofintraluminal thrombus in abdominal aortic aneurysm withlocal hypoxia and wall weakeningrdquo Journal of Vascular Surgeryvol 34 no 2 pp 291ndash299 2001
[19] D Bluestein K Dumont M de Beule et al ldquoIntraluminalthrombus and risk of rupture in patient specific abdominalaortic aneurysmmdashFSImodellingrdquoComputerMethods in Biome-chanics and Biomedical Engineering vol 12 no 1 pp 73ndash812009
[20] E Soudah J Pennecot J S Perez M Bordone and E OnateldquoMedical-GiD from medical images to simulations 4D MRIflow analysisrdquo in Computational Vision and Medical ImageProcessing Recent Trends chapter 10 Springer New York NYUSA 1871
[21] E Soudah M Bordone and J S Perez ldquoGmed a platform forimages treatment inside GiD systemrdquo in Proceedings of the 5thConference On Advances And Applications Of GiD Barcelona2010 GiDmdashthe personal pre and postprocessor httpwwwgidhomecom
[22] W E Lorensen and H E Cline ldquoMarching cubes a high reso-lution 3d surface construction algorithmrdquo in Proceedings of the14th Annual Conference on Computer Graphics and InteractiveTechniques (SIGGRAPH rsquo87) pp 163ndash169 1987
[23] M Bordone C Garcıa J Garcıa and E Soudah ldquoBiodyn UserManual TDYN theoretical Backgroundrdquo COMPASSIS 2012httpwwwcompassiscomcompass
[24] E Onate S Idelsohn O C Zienkiewicz and R L Taylor ldquoAfinite point method in computational mechanics Applicationsto convective transport and fluid flowrdquo International Journal forNumerical Methods in Engineering vol 39 no 22 pp 3839ndash3866 1996
[25] Y Papaharilaou J A Ekaterinaris E Manousaki and AN Katsamouris ldquoA decoupled fluid structure approach forestimating wall stress in abdominal aortic aneurysmsrdquo Journalof Biomechanics vol 40 no 2 pp 367ndash377 2007
[26] A-V Salsac S R Sparks J-M Chomaz and J C LasherasldquoEvolution of the wall shear stresses during the progressiveenlargement of symmetric abdominal aortic aneurysmsrdquo Jour-nal of Fluid Mechanics vol 560 pp 19ndash51 2006
[27] C M Scotti J Jimenez S C Muluk and E A Finol ldquoWallstress and flow dynamics in abdominal aortic aneurysms finite
element analysis vs fluid-structure interactionrdquo ComputerMethods in Biomechanics andBiomedical Engineering vol 11 no3 pp 301ndash322 2008
[28] A Borghia N B Wooda R H Mohiaddinb and X Y XualdquoFluid-solid interaction simulationof flow and stress pattern inthoraco abdominal aneurysms a patient-specific studyrdquo Journalof Fluids and Structures vol 24 pp 270ndash280 2008
[29] A Sheidaei S C Hunley S Zeinali-Davarani L G Raguinand S Baek ldquoSimulation of abdominal aortic aneurysm growthwith updating hemodynamic loads using a realistic geometryrdquoMedical Engineering and Physics vol 33 no 1 pp 80ndash88 2011
[30] T Hatakeyama H Shigematsu and T Muto ldquoRisk factors forrupture of abdominal aortic aneurysm based on three-dimen-sional studyrdquo Journal of Vascular Surgery vol 33 no 3 pp 453ndash461 2001
Submit your manuscripts at
httpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
Oxidative Medicine and
Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Parkinsonrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Computational and Mathematical Methods in Medicine 9
aneurysms model complexity versus predictability of finite ele-ment simulationsrdquo European Journal of Vascular and Endovas-cular Surgery vol 40 no 2 pp 176ndash185 2010
[13] M Bonert R L Leask J Butany et al ldquoThe relationshipbetween wall shear stress distributions and intimal thickeningin the human abdominal aortardquo BioMedical Engineering Onlinevol 2 article 18 2003
[14] D Bluestein L Niu R T Schoephoerster andM K DewanjeeldquoSteady flow in an aneurysm model correlation between fluiddynamics and blood platelet depositionrdquo Journal of Biomechan-ical Engineering vol 118 no 3 pp 280ndash286 1996
[15] M L Raghavan D A VorpM P Federle M S Makaroun andMWWebster ldquoWall stress distribution on three-dimensionallyreconstructed models of human abdominal aortic aneurysmrdquoJournal of Vascular Surgery vol 31 no 4 pp 760ndash769 2000
[16] C Kleinstreuer and Z Li ldquoAnalysis and computer programfor rupture-risk prediction of abdominal aortic aneurysmsrdquoBioMedical Engineering Online vol 5 article 19 2006
[17] J Shum G Martufi E di Martino et al ldquoQuantitative assess-ment of abdominal aortic aneurysm geometryrdquo Annals of Bio-medical Engineering vol 39 no 1 pp 277ndash286 2011
[18] D A Vorp P C Lee D H J Wang et al ldquoAssociation ofintraluminal thrombus in abdominal aortic aneurysm withlocal hypoxia and wall weakeningrdquo Journal of Vascular Surgeryvol 34 no 2 pp 291ndash299 2001
[19] D Bluestein K Dumont M de Beule et al ldquoIntraluminalthrombus and risk of rupture in patient specific abdominalaortic aneurysmmdashFSImodellingrdquoComputerMethods in Biome-chanics and Biomedical Engineering vol 12 no 1 pp 73ndash812009
[20] E Soudah J Pennecot J S Perez M Bordone and E OnateldquoMedical-GiD from medical images to simulations 4D MRIflow analysisrdquo in Computational Vision and Medical ImageProcessing Recent Trends chapter 10 Springer New York NYUSA 1871
[21] E Soudah M Bordone and J S Perez ldquoGmed a platform forimages treatment inside GiD systemrdquo in Proceedings of the 5thConference On Advances And Applications Of GiD Barcelona2010 GiDmdashthe personal pre and postprocessor httpwwwgidhomecom
[22] W E Lorensen and H E Cline ldquoMarching cubes a high reso-lution 3d surface construction algorithmrdquo in Proceedings of the14th Annual Conference on Computer Graphics and InteractiveTechniques (SIGGRAPH rsquo87) pp 163ndash169 1987
[23] M Bordone C Garcıa J Garcıa and E Soudah ldquoBiodyn UserManual TDYN theoretical Backgroundrdquo COMPASSIS 2012httpwwwcompassiscomcompass
[24] E Onate S Idelsohn O C Zienkiewicz and R L Taylor ldquoAfinite point method in computational mechanics Applicationsto convective transport and fluid flowrdquo International Journal forNumerical Methods in Engineering vol 39 no 22 pp 3839ndash3866 1996
[25] Y Papaharilaou J A Ekaterinaris E Manousaki and AN Katsamouris ldquoA decoupled fluid structure approach forestimating wall stress in abdominal aortic aneurysmsrdquo Journalof Biomechanics vol 40 no 2 pp 367ndash377 2007
[26] A-V Salsac S R Sparks J-M Chomaz and J C LasherasldquoEvolution of the wall shear stresses during the progressiveenlargement of symmetric abdominal aortic aneurysmsrdquo Jour-nal of Fluid Mechanics vol 560 pp 19ndash51 2006
[27] C M Scotti J Jimenez S C Muluk and E A Finol ldquoWallstress and flow dynamics in abdominal aortic aneurysms finite
element analysis vs fluid-structure interactionrdquo ComputerMethods in Biomechanics andBiomedical Engineering vol 11 no3 pp 301ndash322 2008
[28] A Borghia N B Wooda R H Mohiaddinb and X Y XualdquoFluid-solid interaction simulationof flow and stress pattern inthoraco abdominal aneurysms a patient-specific studyrdquo Journalof Fluids and Structures vol 24 pp 270ndash280 2008
[29] A Sheidaei S C Hunley S Zeinali-Davarani L G Raguinand S Baek ldquoSimulation of abdominal aortic aneurysm growthwith updating hemodynamic loads using a realistic geometryrdquoMedical Engineering and Physics vol 33 no 1 pp 80ndash88 2011
[30] T Hatakeyama H Shigematsu and T Muto ldquoRisk factors forrupture of abdominal aortic aneurysm based on three-dimen-sional studyrdquo Journal of Vascular Surgery vol 33 no 3 pp 453ndash461 2001
Submit your manuscripts at
httpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
Oxidative Medicine and
Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Parkinsonrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts at
httpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttpwwwhindawicom
Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
Oxidative Medicine and
Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporation
httpwwwhindawicom Volume 2014
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Parkinsonrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom