Embed Size (px)
Citation preview

Pediatric Treatment Guidelines
New Guidelines
2007 Edition
Karen Scruggs, MD
Michael T. Johnson, MD
Copyright © 2007 by Current Clinical Strategies Publishing.All rights reserved. This book, or any parts thereof, may notbe reproduced or stored in a retrieval network without thewritten permission of the publisher. The reader is advisedto consult the drug package insert and other referencesbefore using any therapeutic agent. No warranty exists,expressed or implied, for errors and omissions in this text.
Current Clinical Strategies Publishing27071 Cabot RoadLaguna Hills, California 92653Phone: 800-331-8227Fax: [email protected]: www.ccspublishing.com/ccs
Printed in USA ISBN 1-929622-74-0
NeonatologyNormal Newborn Care
I. Prenatal pediatric visitA. The prenatal pediatric visit usually takes place
during the third trimester of the pregnancy. Maternalnutrition, the hazards of alcohol, cigarette smokingand other drugs, and the dangers of passive smok-ing should be discussed. Maternal illnesses andmedications should be reviewed.
Prenatal Pediatric Visit Discussion Issues
Maternal HistoryGeneral health and nutritionPast and present obstetric historyMaternal smoking, alcohol, or drug useMaternal medicationsInfectious diseases: Hepatitis, herpes, syphilis,Chlamydia rubellaMaternal blood type and Rh blood groups
Family HistoryNewborn Issues
Assessment of basic parenting skillsFeeding plan: Breast feeding vs formulaCar seatsCircumcision of male infant
II. DeliveryA. Neonatal resuscitation
1. All equipment must be set up and checked beforedelivery. The infant who fails to breath spontane-ously at birth should be placed under a radiantwarmer, dried, and positioned to open the airway.The mouth and nares should be suctioned, andgentle stimulation provided.
2. The mouth should be suctioned first to preventaspiration. Prolonged or overly vigoroussuctioning may lead to bradycardia and should beavoided unless moderate-to-thick meconium ispresent in the airway.
3. The infant born with primary apnea is most likelyto respond to the stimulation of drying and gentletapping of the soles of the feet. The infant whofails to respond rapidly to these measures isexperiencing secondary apnea and requirespositive pressure bag ventilation with oxygen.
4. Adequate ventilation is assessed by looking forchest wall excursions and listening for air ex-change. The heart rate should be assessed whilepositive pressure ventilation is being applied. Ifthe heart rate does not increase rapidly after
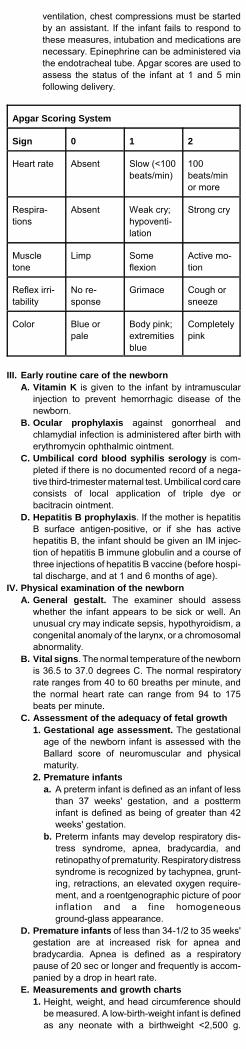
ventilation, chest compressions must be startedby an assistant. If the infant fails to respond tothese measures, intubation and medications arenecessary. Epinephrine can be administered viathe endotracheal tube. Apgar scores are used toassess the status of the infant at 1 and 5 minfollowing delivery.
Apgar Scoring System
Sign 0 1 2
Heart rate Absent Slow (<100beats/min)
100beats/minor more
Respira-tions
Absent Weak cry;hypoventi-lation
Strong cry
Muscletone
Limp Someflexion
Active mo-tion
Reflex irri-tability
No re-sponse
Grimace Cough orsneeze
Color Blue orpale
Body pink;extremitiesblue
Completelypink
III. Early routine care of the newbornA. Vitamin K is given to the infant by intramuscular
injection to prevent hemorrhagic disease of thenewborn.
B. Ocular prophylaxis against gonorrheal andchlamydial infection is administered after birth witherythromycin ophthalmic ointment.
C. Umbilical cord blood syphilis serology is com-pleted if there is no documented record of a nega-tive third-trimester maternal test. Umbilical cord careconsists of local application of triple dye orbacitracin ointment.
D. Hepatitis B prophylaxis. If the mother is hepatitisB surface antigen-positive, or if she has activehepatitis B, the infant should be given an IM injec-tion of hepatitis B immune globulin and a course ofthree injections of hepatitis B vaccine (before hospi-tal discharge, and at 1 and 6 months of age).
IV. Physical examination of the newbornA. General gestalt. The examiner should assess
whether the infant appears to be sick or well. Anunusual cry may indicate sepsis, hypothyroidism, acongenital anomaly of the larynx, or a chromosomalabnormality.
B. Vital signs. The normal temperature of the newbornis 36.5 to 37.0 degrees C. The normal respiratoryrate ranges from 40 to 60 breaths per minute, andthe normal heart rate can range from 94 to 175beats per minute.
C. Assessment of the adequacy of fetal growth1. Gestational age assessment. The gestational
age of the newborn infant is assessed with theBallard score of neuromuscular and physicalmaturity.
2. Premature infantsa. A preterm infant is defined as an infant of less
than 37 weeks' gestation, and a postterminfant is defined as being of greater than 42weeks' gestation.
b. Preterm infants may develop respiratory dis-tress syndrome, apnea, bradycardia, andretinopathy of prematurity. Respiratory distresssyndrome is recognized by tachypnea, grunt-ing, retractions, an elevated oxygen require-ment, and a roentgenographic picture of poorinflation and a fine homogeneousground-glass appearance.
D. Premature infants of less than 34-1/2 to 35 weeks'gestation are at increased risk for apnea andbradycardia. Apnea is defined as a respiratorypause of 20 sec or longer and frequently is accom-panied by a drop in heart rate.
E. Measurements and growth charts1. Height, weight, and head circumference should
be measured. A low-birth-weight infant is definedas any neonate with a birthweight <2,500 g.

Height, weight, and head circumference shouldbe plotted as a function of gestational age on anintrauterine growth chart.
2. Factors that may result in an infant who is smallfor gestational age include chromosomal andother dysmorphic syndromes, congenital infec-tions, maternal hypertension, smoking, uterineanomalies, and multiple gestations.
3. The small-for-gestational age infant is at greaterrisk for cold stress, hypoglycemia, hypocalcemia,and polycythemia.
4. The differential diagnosis for thelarge-for-gestational age infant includes maternaldiabetes and maternal obesity. Thelarge-for-gestational age infant is at risk forshoulder dystocia, birth trauma, andhypoglycemia.
F. Examination of organ systems and regions1. Head, face, and neck
a. The head circumference is measured andplotted, and the scalp, fontanelles, and suturesare examined. Bruising and hematomas of thescalp should be noted. Cephalohematomasare subperiosteal and do not cross suturelines, whereas caputs are subcutaneous anddo cross suture lines.
b. Facial features that suggest a chromosomalanomaly include midfacial hypoplasia, smalleyes, or low-set ears. Fetal alcohol syndromeis suggested by a small upper lip and asmooth philtrum.
c. The eyes should be examined with an oph-thalmoscope to document a red reflex. Theabsence of a clear red reflex is indicative of aretinoblastoma, cataract, or glaucoma.
d. The lips, mouth, and palate are inspectedand palpated for clefts. Nares patency can bedocumented by closing the mouth and occlud-ing one nostril at a time while observing airflow through the opposite nostril.
2. Thorax and cardiovascular systemsa. Chest wall excursions should be observed
and the respiratory rate determined. Thenormal neonatal respiratory rate is 40 to 60breaths per minute.
b. Auscultation of breath and heart sounds.The normal heart rate during the first week oflife may range from 94 to 175 beats per min-ute.
3. Abdomen and gastrointestinal systema. Visual inspection of the abdomen should
assess symmetry and distension.b. Abdominal palpation for masses,
hepatosplenomegaly, or renal masses iscompleted, and the anus should be visuallyinspected.
4. Genitourinary system. The genitalia are exam-ined for ambiguous genitalia, which requiresimmediate endocrinologic and urologic consulta-tion.
5. Musculoskeletal systema. Hip examination may detect developmental
dysplasia. Risk factors for hip dysplasia in-clude a family history, foot deformities, con-genital torticollis, Down syndrome, and breechpresentation. The female to male ratio is 7:1.Ultrasonography is used to evaluate sus-pected hip dysplasia.
b. Fracture of the clavicle occurs in 0.2-3.5% ofvaginal deliveries. Physical findings includelocal swelling and crepitations and an asym-metric Moro reflex. Treatment consists ofmaking a sling by pinning the shirt sleeve ofthe involved side to the opposite side of theshirt.
6. Neurologic systema. The degree of alertness, activity, and muscle
tone should be noted. The head circumferenceis plotted on the growth chart.
b. The posterior midline area should be exam-ined for evidence of neural tube defects.Pilonidal dimples with tufts of hair are evalu-ated with ultrasonography.
V. Common neonatal problemsA. Hypoglycemia
1. Hypoglycemia is common in premature infants,infants who are small for gestational age, infants

of diabetic mothers, and infants who have experi-enced perinatal asphyxia.
2. Hypoglycemia is defined as a blood glucose of<40-45 mg/dL. Hypoglycemic infants require earlyfeedings or IV glucose.
B. Anemia during the newborn period may be causedby hemolytic and congenital anemias, fe-tal-to-maternal hemorrhage, placental abruption,and occult hemorrhage.
C. Bilirubin metabolism1. Hyperbilirubinemia occurs frequently in the nor-
mal newborn because of increased productionand decreased elimination of this breakdownproduct of heme.
2. Initial workup for neonatal hyperbilirubinemiaincludes measurements of total and direct biliru-bin levels, hematocrit, Coombs test, and testingof urine for reducing substances to excludegalactosemia. High levels of bilirubin can causean acute encephalopathy (ie, kernicterus).
D. Gastrointestinal problems1. Ninety-six percent of full-term newborns pass a
meconium stool before 24 hours of age. A de-layed or absent passage of meconium may becaused by meconium plug syndrome,Hirschsprung disease, meconium ileus (cysticfibrosis), or imperforate anus.
2. Bilious vomiting in the newborn is always abnor-mal and usually is caused by an intestinal ob-struction. Vomiting in the newborn also may becaused by inborn errors of metabolism andcongenital adrenal hyperplasia.
E. Urinary problems. Ninety-nine percent of normalfull-term infants will urinate by 24 hours. If urinationhas not occurred within 24 hours, renal ultra-sonography should be done and an intravenousfluid challenge may be given.
References, see page 182.
Neonatal Jaundice
Jaundice is defined by a serum bilirubin concentrationgreater than 5 mg/dL. Clinical jaundice develops in 50% ofnewborns, and breast-fed infants have an increasedincidence of jaundice. Differentiation between physiologicjaundice, which is seen in many infants during the firstweek of life, and pathologic jaundice is essential becausepathologic jaundice is a sign of a more serious condition.
I. PathophysiologyA. Physiologic versus pathologic jaundice
1. Physiologic jaundice is characterized byunconjugated hyperbilirubinemia that peaks bythe third or fourth day of life in full-term newbornsand then steadily declines by 1 week of age.Asian newborns tend to have higher peak biliru-bin concentrations and more prolonged jaundice.Premature infants are more likely to developjaundice than full-term babies.
2. Causes of physiologic jaundicea. Increased bilirubin load due to the high red
blood cell volume in newborns and shortenedblood cell survival.
b. Deficient hepatic uptake and deficient conju-gation of bilirubin.
c. Increased enterohepatic bilirubin reabsorp-tion.
d. Deficient excretion of bilirubin.3. Pathologic jaundice usually appears within the
first 24 hours after birth and is characterized by arapidly rising serum bilirubin concentration (>5mg/dL per day), prolonged jaundice (>7 to 10days in a full-term infant), or an elevated directbilirubin concentration (>2 mg/dL). Conjugatedhyperbilirubinemia never has a physiologic causeand must always be investigated.
II. Clinical evaluation of jaundice in newbornsA. History may reveal abdominal distention, delayed
passage of meconium, lethargy, light colored stools,dark urine, low Apgar scores, poor feeding, weightloss, or vomiting.
B. Physical examination should seek bruising,cephalhematoma, congenital anomalies,hepatosplenomegaly, pallor, petechiae, or small orlarge size for gestational age.

C. Maternal history should assess history ofchorioamnionitis, forceps delivery, vacuum extrac-tion, diabetes, dystocia, or exposure to drugs.Failure to receive immune globulin in a previouspregnancy or abortion that involved risk ofisoimmunization should be sought. Family history ofjaundice, anemia, liver disease, splenectomy, Greekor Asian race, preeclampsia, or unexplained illnessduring pregnancy should be assessed.
III. Laboratory evaluationA. Diagnostic tests include blood group typing of both
mother and infant, a direct Coombs’ test, andmeasurement of serum bilirubin concentration.
B. Ill or premature infants, or those with significantjaundice (serum bilirubin >15 mg/dL) require acomplete blood cell count or hemoglobin,reticulocyte count, blood smear, and direct bilirubinlevel. In infants of Asian or Greek descent, glucose-6-phosphate dehydrogenase (G6PD) should bemeasured.
IV. Differential diagnosis of unconjugatedhyperbilirubinemia
A. Increased bilirubin production1. Fetal-maternal blood group incompatibility is
one cause of increased bilirubin production. Rhsensitization occurs when an Rh-negative motheris exposed to Rh-positive blood cells. Subse-quent Rh-positive fetuses may develophemolysis. Other minor blood group incompatibili-ties also can cause hemolysis and jaundice.
2. ABO incompatibility is the most common type ofisoimmune hemolytic disease. It can occur whenthe mother’s blood group is O and the baby’s is Aor B. This type of hemolysis is relatively mild.
3. G6PD deficiency, a sex-linked disease, is animportant cause of hyperbilirubinemia and ane-mia in infants of Greek and Asian descent.
4. Abnormalities of the red blood cell membrane,such as spherocytosis and elliptocytosis, maycause hyperbilirubinemia. Alpha thalassemia mayoccur in the neonatal period.
5. Hematoma, occult hemorrhage, orpolycythemia (fetomaternal or twin-to-twintransfusion, delayed cord clamping, intrauterinegrowth retardation, or maternal diabetes) maylead to hyperbilirubinemia.
B. Decreased bilirubin excretion1. Delay in intestinal transit time, because bowel
obstruction, increases the enterohepatic circula-tion. Relief of the obstruction results in a declinein bilirubin concentration.
2. Crigler-Najjar syndrome is a rare, inherited,lifelong deficiency of bilirubin excretion. Type I isautosomal recessive. Patients present withextreme jaundice (bilirubin concentration >25mg/dL) and have a very high risk of bilirubinencephalopathy. Type II is autosomal dominant,and it can effectively be treated with phenobarbi-tal.
3. Neonatal hypothyroidism is another cause ofprolonged indirect hyperbilirubinemia.
C. Increased bilirubin production and decreasedexcretion. Sepsis often causes increased break-down of red blood cells and decreased hepaticexcretion of bilirubin. Certain drugs given to thenewborn may also induce hemolysis or decreasebilirubin excretion.
D. Breast feeding is associated with neonatalhyperbilirubinemia. In healthy newborns, the dangerof an elevated bilirubin concentration is minimal, andswitching to formula feeding is unnecessary.
V. Consequences of unconjugated hyperbilirubinemia.Bilirubin encephalopathy (kernicterus) is defined asthe acute and often fatal syndrome characterized byopisthotonos, hypotonia, a high-pitched cry, and lateneurologic sequelae of choreoathetosis, spasticity,upward-gaze paresis, and central hearing loss.
VI. TreatmentA. Low-risk infants with minimal jaundice are ob-
served for an increase in the jaundice intensity or aspread to the baby’s feet (jaundice advances fromhead-to-foot).

Management of Hyperbilirubinemia in the HealthyTerm Newborn
Total serum bilirubin level, mg/dL
Age (H) Considerphototherapy
Phototherapy
Ex-changetransfu-sion ifphoto-therapyfails
Ex-changetransfu-sion andphoto-therapy
<24 ... ... ... ...
25-48 >12 >15 >20 >25
49-72 >15 >18 >25 >30
>72 >17 >20 >25 >30
B. Phototherapy with blue light causesphotoconversion of bilirubin to a water-solubleproduct that is excreted in urine and stool. Bilirubinconcentrations are measured once or twice a dayduring phototherapy, and treatment is discontinuedwhen the bilirubin concentration drops below 12mg/dL.
C. Exchange transfusion therapy. Exchange transfu-sion is used for emergent treatment of markedlyelevated bilirubin and for correction of anemiacaused by isoimmune hemolytic disease.
References, see page 182.
Respiratory Disorders of the New-born
Respiratory distress is a common problem during the firstfew days of life. Respiratory distress may present withtachypnea, nasal flaring, sternal and intercostal retrac-tions, cyanosis, and apnea.
I. Transient tachypnea of the newbornA. Transient tachypnea of the newborn (TTN) usually
presents as early respiratory distress in term orpreterm infants. It is caused by delayed reabsorptionof fetal lung fluid.
B. TTN is a very common, and it is often seen followingcesarean section because babies born by cesareansection have delayed reabsorption of fetal lung fluid.
C. Symptoms of TTN include tachypnea, retractions,nasal flaring, grunting, and cyanosis.
D. Arterial blood gas reveals respiratory acidosis andmild-to-moderate hypoxemia.
E. Chest x-ray often reveals fluid in the interlobarfissures and perihilar streaking. Hyperaeration of thelungs and mild cardiomegaly may be seen; alveolaredema may appear as coarse, fluffy densities.
F. Transient tachypnea of the newborn usually resolveswithin12-24 hours. The chest radiograph appearsnormal in 2-3 days. The symptoms rarely last morethan 72 hours.
G. Treatment of TTN consists of oxygen therapy.Infants will usually recover fully, without long-termpulmonary sequelae.
II. Respiratory distress syndromeA. RDS is a lung disease caused by pulmonary
surfactant deficiency. It occurs almost always inpreterm infants who are born before the lungs areable to produce adequate amounts of surfactant.
B. Respiratory distress usually begins at, or soon after,delivery and tends to worsen over time. Infants willhave tachypnea, nasal flaring, intercostal and sternalretractions, and expiratory grunting.
C. Chest radiography shows diffuse atelectasis, whichappears as reduced lung volume, with homogeneoushaziness or the “ground glass” appearance of lungfields, and air bronchograms.
D. RDS is diagnosed when a premature infant hasrespiratory distress and a characteristic chest radio-graph. The differential diagnosis includes pneumoniacaused by group B streptococci.

E. Ventilatory management 1. Continuous positive airway pressure (CPAP)
improves oxygenation and survival (5-7 cm H2Opressure).
2. For infants exhibiting respiratory acidosis,hypoxemia or apnea, intermittent positive pres-sure ventilation will be required in addition topositive end-expiratory pressure (PEEP).
3. An umbilical or radial arterial line is used tomonitor blood gas levels and blood pressure.
F. Surfactant replacement therapy1. Surfactant therapy reduces mortality by 30-50%
and pneumothorax by 50%.2. Surfactant replacement therapy should be initi-
ated as soon as respiratory distress has beenclinically diagnosed. As long as the infant requiressignificant ventilatory support, Survanta (every 6hours for 4 doses) or Exosurf (every 12 hours for2 doses) should be given.
G. General supportive care. Sepsis and pneumoniaare part of the differential diagnosis of RDS. Pre-sumptive treatment with ampicillin plus gentamicin orcefotaxime usually is given until blood and CSFcultures are negative.
III. Bronchopulmonary dysplasia (BPD, chronic lungdisease)
A. BPD is characterized by hypoxia, hypercarbia, andoxygen dependence that persists beyond 1 month ofage. The chest radiograph shows hyperexpansionand focal hyperlucency, alternating with strands ofopacification.
B. BPD is extremely common among infants who havesevere RDS treated with mechanical ventilation. Theincidence of BPD is inversely proportional tobirthweight. Virtually all babies who develop BPDhave had mechanical ventilation, suggesting animportant role for barotrauma and oxygen toxicity.
C. Respiratory distress syndrome is the most commonpulmonary disease causing BPD. Other neonataldiseases requiring oxygen and mechanical ventila-tion may also cause BPD, including immature lungs,meconium aspiration syndrome, congenital heartdisease, neonatal pneumonia, and aspiration pneu-monia.
D. Signs of BPD include tachypnea and retractions,after extubation. Blood gas measurements showrespiratory acidosis with elevated PaVCO2; in-creased HCO3 indicates metabolic compensation.Higher inspired oxygen concentration is required tomaintain normal oxygenation.
E. Management of bronchopulmonary dysplasia1. Bronchopulmonary dysplasia (BPD), also
known as neonatal chronic lung disease(CLD), is an important cause of respiratoryillness in preterm newborns. Most patientswith BPD gradually improve as healing occursand lung growth continues.
2. Respiratory supporta. Mechanical ventilation. Infants who re-
main ventilator-dependent for severalweeks should be weaned gradually. Smalltidal volumes are preferable to avoid addi-tional mechanical injury. Maintaining apositive end-expiratory pressure of 6 or 7cm H2O may minimize atelectasis. Aslightly prolonged inspiratory duration of0.5-0.6 sec sometimes is needed to pro-mote uniform lung inflation. To facilitateweaning, the arterial carbon dioxide tensionshould be allowed to rise to 55-60 mm Hg,as long as pH is in the normal range. In-fants who can maintain this PCO2 level withspontaneous breathing can be weaned tocontinuous positive airway pressure andthen to supplemental oxygen alone.
b. Oxygen. Supplemental oxygen should beprovided to maintain arterial PO2 above 50-55 mm Hg. Hypoxemia also may increaseairway resistance in infants who have beenweaned from assisted ventilation, supple-mental oxygen can be provided by hood ornasal cannula.
c. Monitoring. Oxygenation should be moni-tored with pulse oximetry. Oxygen satura-tion should be maintained at 92-95 percent.The oxygen concentration (or flow rate bynasal cannula) may need to be increased

during feedings and sleep to maintainadequate oxygenation.
d. In ventilator-dependent infants, capillaryblood gas (CBG) samples should be moni-tored to check PCO2 and pH.
3. Nutrition. Appropriate nutrition must be pro-vided to ensure recovery and growth. Humanmilk or premature formula must be supple-mented to meet these needs.
4. Fluid restrictiona. Fluid intake should be restricted in infants
with BPD to avoid pulmonary edema. How-ever, adequate nutrition must be providedin the reduced volume of feeding. Mostinfants can be managed with modest re-striction of 140-150 mL/kg per day. A pre-mature formula or human milk with addedfortifier is used in preterm infants. Wheninfants reach term postmenstrual age,supplemented human milk or a transitionalformula is used. Additional calories and/orprotein may be added.
b. Growth should be monitored. Protein andmineral intakes should be calculated eachweek to ensure that they are optimal. Se-rum concentrations of calcium, phospho-rus, and alkaline phosphatase are mea-sured weekly or every other week.
5. Diuretics. Pharmacologic therapy may in-clude diuretics.a. Thiazide diuretics. Acute and chronic
administration of diuretics (thiazide and/orspironolactone) improve lung mechanics inpreterm infants with BPD. Diuretics ininfants with evolving or established BPD toachieve acute improvements in pulmonaryfunction are useful.
b. In infants who have pulmonary exacerba-tions attributed to pulmonary edema, or tominimize the circulatory effect of a packedred blood cell transfusion, furosemideshould be given (1 mg/kg per day IV or 2mg/kg per day PO). In infants with severeBPD who appear to have short-term benefitfrom diuretic treatment, a longer course offurosemide (4 mg/kg in two divided dosesPO on alternate days) may be given.
c. In infants three to four weeks old whoremain ventilator-dependent with evolvingBPD, chlorothiazide (10 to 20 mg/kg in twodivided doses, PO) may be used as analternative to furosemide.
d. Serum electrolytes should be measuredone to two days after initiating diuretictherapy, with an increase in dose, and atleast weekly with chronic use. Electrolytesupplements should be administered tocompensate for increased urinary loss.Initial supplementation is 2 to 4 meq/kg perday of sodium chloride and 2 meq/kg perday of potassium chloride, and adjust asneeded.
6. Bronchodilators. Infants with BPD haveincreased airway resistance and may haveepisodes of bronchoconstriction. Inhaled orsubcutaneous administration of beta-2agonists (eg, salbutamol, albuterol,terbutaline) acutely decreases resistance andincreases compliance. The metered doseinhaler (MDI) often is used in infants with BPD.a. Albuterol
(1) In some ventilator-dependent preterminfants with evolving BPD who are twoto three weeks of age, the beta-adrenergic agonist albuterol may im-prove pulmonary function. Albuterol isadministered as one MDI actuation perdose (approximately 0.1 mg) every fourto six hours.
(2) If the infant appears to improve withalbuterol use of a long-acting beta-adrenergic agonist such as salmeterolmay be preferred to avoid adverseeffects that have been associated withchronic use of albuterol. These ad-verse effects include tachycardia,arrhythmias, hypokalemia, and irritabil-
ity.b. Salmeterol is given as one MDI actuation
twice daily. If possible, treatment should bediscontinued gradually as lung functionstabilizes and before hospital discharge.
c. Ipratropium bromide(1) Administration of the anticholinergic
bronchodilator ipratropium bromide(inhaled doses of 25 micrograms/kg) toventilator-dependent preterm infantsimproves respiratory system resistanceand compliance.
(2) Ipratropium can be used for its syner-gistic effect with albuterol in the treat-ment of acute episodes of reactiveairway disease. A combination of in-haled ipratropium bromide andalbuterol (Combivent) may be adminis-tered as one to two MDI actuationsevery four hours, in ventilator-depend-ent infants with BPD.
7. Corticosteroids. Corticosteroids may reduceinflammation and improve lung function ininfants with BPD. Both systemic and inhaledadministration have been used. However,systemic corticosteroid administration is asso-ciated with serious adverse effects and shouldbe avoided if possible.a. Systemic corticosteroids. Systemic
corticosteroids improve lung mechanicsand reduce the need for assisted ventila-tion in infants with established BPD. Sys-temic dexamethasone should be reservedfor the exceptional infant with severe BPDwho cannot be weaned from maximalventilatory and oxygen support.
b. Inhaled corticosteroids. Infants withsevere BPD who are dependent uponsubstantial support with mechanical ventila-tion and high concentrations of supplemen-tal oxygen, may sometimes be treated withinhaled beclomethasone or fluticasone.Beclomethasone (42 µg per puff) orfluticasone (50µg per puff) may be used byMDI connected to the endotracheal tube,and give one to two puffs every 12 hours.
8. Acute exacerbationsa. Infants with severe BPD may have acute
episodes of bronchospasm leading torespiratory decompensation. These may beassociated with viral infections, althoughbacterial pneumonia is uncommon.
b. A chest radiograph should be obtained todetect pulmonary parenchymal changes.Culture and Gram stain should be obtainedof tracheal secretions that are purulent orhave changed in volume or quality. If bac-terial infection is suspected, antibiotictreatment should be initiated while awaitingculture results.
c. Management(1) Treatment should be initiated with
albuterol, which is administered by MDIand spacer (two to four puffs) or bynebulization (0.15 mg/kg in 2 mL sa-line) every 20 minutes for three doses.Either regimen is followed by adminis-tration every one to four hours; thefrequency is decreased as airflow im-proves, or with tachycardia of >200bpm. Another approach is continuousnebulization of albuterol (0.5 mg/kg perhour may be given for one to twohours). Ipratropium should be added ifthe response to albuterol is poor.
(2) If acute bronchospasm occurs in aninfant receiving inhaled corticosteroids,the dose is doubled for 7 to 14 days. Iftreatment with a beta-adrenergic agentand inhaled corticosteroids fails toreestablish stable pulmonary function,a short (five to seven days) taperingcourse of systemic dexamethasone(initial dose 0.25 mg/kg), may be con-sidered. Alternatively, a short course ofprednisone (initial dose 1 mg/kg perday, tapered over five days) may be

tried.9. Monitoring
a. Growth. Patients should be weighed everyone to three days while in the hospital, andlength and head circumference should bemeasured weekly. Nutritional monitoringincludes initial weekly measurement ofblood urea nitrogen, albumin, calcium,phosphorus, and alkaline phosphataseconcentrations. Serum electrolyte concen-trations should be measured every week ininfants on diuretic therapy.
b. Oxygenation(1) Oxygen saturation is monitored contin-
uously with pulse oximetry during hos-pitalization. After discharge, oxygensaturation should be measured for atleast six to eight hours every one totwo weeks, including periods whileawake, sleeping, and feeding.
(2) A target oxygen saturation of 92 to 94percent is adequate to avoidhypoxemia and minimize the risk ofadditional lung injury caused by expo-sure to excessive oxygen concentra-tions. The target saturation should behigher (94 to 96 percent) in infants withpulmonary hypertension.
References, see page 182.
Neonatal Resuscitation
Neonatal resuscitation skills are important because of thepotential for serious disability or death in high-risk infantsand in a few unpredicted full-term, low-risk deliveries.
I. PreparationA. Advanced preparation requires acquisition and
maintenance of proper equipment and supplies.B. Immediate preparation
1. Suction, oxygen, proper-sized face mask and theresuscitation bag should be checked.
2. Appropriately sized ET tubes, cut to 13 cm,should be laid out.
3. Medications should be prepared and an umbili-cal catheter and tray should be prepared.
Neonatal Resuscitation Equipment and Supplies
Suction Equipment
Bulb syringeSuction catheters, 5 (or 6),8, 10 FrMeconium aspirator
Mechanical Suction8 Fr feeding tube and 20 ccsyringe
Bag-and-Mask Equipment
Oral airways, newborn andpremature sizesInfant resuscitation bag witha pressure-releasevalve/pressure gauge to give90-100% O2
Oxygen with flow meter andtubingCushion rim face masks innewborn and premature sizes
Intubation Equipment
Laryngoscope with straightblades, No. 0 (preterm) andNo.1(term newborn). Extra bulbs and batteries forlaryngoscopeEndotracheal tubes, size2.5, 3.0, 3.5, 4.0 mm
Stylet ScissorsGloves
Medications
Epinephrine 1:10,000, 3 ccor 10 cc ampulesNaloxone 0.4 mg/mL,1 mLampulesDextrose 10% in water, 250ccSterile water, 30 cc
Volume expanders-one ormore of these:
Albumin 5% solutionNormal Saline
Ringer’s Lactate solution

Miscellaneous
Radiant warmer and towelsor blanketsStethoscopeAdhesive tape, ½ or 3/4 inchwidthSyringes, 1 cc, 3 cc, 5 cc, 10cc, 20 cc, 50 ccUmbilical arterycatheterization trayCardiotachometer and ECGoscilloscope
Alcohol sponges3-way stopcocks3 Fr feeding tubeUmbilical tapeNeedles, 25, 21, 18 gaugeUmbilical catheters, 3 ½ and5 Fr
II. Neonatal resuscitation proceduresA. During delivery, infant evaluation includes assess-
ment of muscle tone, color, and respiratory effort.B. After delivery, the infant should be placed on a
preheated radiant warmer. The infant should bequickly dried with warm towels. The infant should beplaced supine with its neck in a neutral position. Atowel neck roll under the shoulders may help pre-vent neck flexion and airway occlusion.
C. The upper airway is cleared by suctioning; themouth first, and then the nose, using a bulb syringe.Suctioning should be limited to 5 seconds at a time.
D. If breathing is effective and pulse is >100 beats/min,positive pressure ventilation (PPV) is not needed. Ifcyanosis is present, oxygen should be adminis-tered.
E. Free-flowing oxygen may be given at a rate of 5L/min by holding the tubing 1/2 inch in front of theinfant’s nose, or an oxygen mask may be used.When the infant’s color is pink, the oxygen is gradu-ally discontinued.
F. Positive pressure ventilation should be initiated ifthe infant is not breathing effectively after the initialsteps. Tactile stimulation should be administered bygently slapping the soles of the feet or rubbing theback. If the infant is apneic or gasping, begin PPVwith 100% O2. If the heart rate is <100 beats/min,give PPV immediately by bag-mask.1. Bag-mask ventilation. Ventilations should be
given at a rate of 40-60/min. Visible chest wallmovement indicates adequate ventilation.
2. Endotracheal intubation is initiated if the infantis nonresponsive to bag-mask PPV.
Endotracheal Tube Size and Depth of InsertionFrom Upper Lip
Weight GestationalAge
Size Depth
<1000 g <28 weeks 2.5 mm 7 cm
1000-2000g
28-34 weeks 3.0 mm 8 cm
2000-3000g
34-38 weeks 3.5 mm 9 cm
3000 g ormore
39->40 weeks 4.0 mm 10 cm
G. Evaluation of heart rate1. If the heart rate is >100 beats/min, PPV can be
gradually discontinued after the infant is breath-ing effectively.
2. Chest compressions should be started if theheart rate is <80 beats/min after 15-30 secondsof adequate ventilation.a. Chest compressions are alternated with
ventilations at a ratio of 3:1. The combinedrate should be 120/min (ie, 80 compressionsand 30 ventilations).
b. After 30 seconds, evaluate the response. Ifthe pulse is >80 beats/min, chest compres-sions can be stopped and PPV continueduntil the heart rate is 100 beats/min andeffective breathing is maintained.
3. Epinephrine should be given if the heart rateremains below 80/minute after 30 seconds ofPPV and chest compressions.

Neonatal Resuscitation Medications
Medica-tion
Concentration
Preparation
Dosage Rate/Precautions
Epinephrine
1:10,000 1 mL 0.1-0.3mL/kg IVor ET.May re-peat in 3-5 min ifHR is<80/min
Give rap-idly. Maydilute 1:1with nor-mal salineif given viaET
Volumeexpand-ers
WholebloodAlbumin5%NormalsalineRingerlactate
40 mL 10 mL/kgIV
Give over5-10 minby syringeor IV drip
Naloxone
0.4 mg/mL 1 mL 0.1 mg/kg(0.25mL/kg)IV, ET,IM, SQ
Give rap-idly
Naloxone
1.0 mg/mL 1 mL 1 mg/kg(0.1mL/kg) IV,ET, IM,SQ
IV, ETpreferred.IM, SQaccept-able
Sodiumbicarbonate
0.5mEq/mL(4.2% so-lution) di-luted withsterile wa-ter tomake 0.5mEq/mL
20 mLor two10-mLprefilledsyringes
2 mEq/kgIV
Giveslowly,over atleast 2min.
4. Other medicationsa. Volume expanders. Volume expansion is
indicated for patients who have known orsuspected blood loss and poor response toother resuscitative measures. Albumin 5%,normal saline, or Ringer’s lactate can begiven in boluses of 10 mL/kg over 5 to 10minutes.
b. Sodium bicarbonate is recommendedduring prolonged resuscitation for infantsrefractory to other measures.
c. Naloxone hydrochloride is given to in-fants with prolonged respiratory depressionfollowing narcotic anesthesia given to themother within 4 hrs before delivery.Naloxone is contraindicated in infants ofmothers who are addicted to narcotics.
5. Umbilical vessel catheterization is recom-mended when vascular access is required.The large, centrally located, thin-walled andflat vein is used, and a 3.5 or 5.0 Frradiopaque catheter is inserted into the veinuntil a free flow of blood can be aspirated.
References, see page 182.

General PediatricsDiabetes Mellitus
Diabetes mellitus consists of hyperglycemia caused byinsulin deficiency, impairment of insulin action, or both.Five percent of the population is affected by diabetes, 10%of whom have type 1 diabetes.
I. Classification of diabetes mellitusA. Diabetes mellitus is classified into two types: type 1
and type 2.B. Type 1 diabetes
1. Type 1 diabetes is caused by absolute insulindeficiency. Most cases among children and ado-lescents (95%) result from autoimmune destruc-tion of the beta cells of the pancreas.
2. The peak age at diagnosis is 12 years, and 75-80% of individuals develop type 1 diabetes beforeage 30.
C. Type 2 diabetes is caused by insulin resistance andrelative insulin deficiency. Most type 2 diabetics donot require insulin injections and are obese.
Criteria for Diagnosis of Diabetes
Fasting plasma glucose 126 mg/dL or higherorRandom plasma glucose 200 mg/dL or higher with symptoms
of diabetes (fatigue, weight loss, polyuria, polyphagia,polydipsia)
orAbnormal two-hour 75-g oral glucose tolerance test result,with glucose 200 mg/dL or higher at two hoursAny abnormal test result must be repeated on a subsequentoccasion to establish the diagnosis
II. Management of diabetic ketoacidosisA. DKA can be seen at the time of diagnosis of type 1
diabetes or in the patient who has establisheddisease if diabetes management is inadequate. DKAis caused by insulin deficiency, which leads tohyperglycemia and ketogenesis.
B. Symptoms include polyuria, polydipsia, hyperpneawith shortness of breath, vomiting, and abdominalpain. Hyperosmolar dehydration and acid/base andelectrolyte disturbances occur.
C. Rehydration1. Immediate evaluation should assess the degree
of dehydration by determining capillary refill, skintemperature, and postural heart rate and bloodpressure.
2. Initial fluid resuscitation consists of a 10-mL/kgbolus of 0.9% saline over 30-60 minutes, re-peated if hypovolemic shock persists. Patientsthen should begin to receive maintenance fluidrequirements added to the calculated fluid deficit(>2 y: 30 mL/kg for mild deficit, 60 mL/kg formoderate deficit, 90 mL/kg for severe deficit; <2y: 50 mL/kg for mild deficit, 100 mL/kg for moder-ate deficit, 150 mL/kg for severe deficit). Thesodium concentration of the fluid should provide50% of the sodium deficit in the first 12 hours andthe remainder in the next 36 hours (75 to 125mEq/L sodium chloride).
Laboratory Monitoring During DKA
Blood glu-cose:
At presentation, then hourly byfingerstick with glucose meter
Serum so-dium andpotassium:
At presentation, then at 4- to 6-h inter-vals
Acid/basestatus:
At presentation, then at 2- to 4-h inter-vals. Venous pH and serum carbondioxide
Serum urea nitrogen, complete blood count, acetoneand cultures can be obtained at presentation.
D. Potassium replacement. DKA is associated withtotal body potassium depletion. This deficit shouldbe replaced by infusing potassium chloride at a rate

of 3 mEq/kg per 24 hours after completion of thenormal saline fluid resuscitation. If the patientrequires more than 4 mEq/kg of a potassiuminfusion, 50% can be administered as potassiumphosphate to help prevent hyperchloremic acidosisand hypophosphatemia.
E. Lowering the glucose level1. Regular insulin should be initiated as an intrave-
nous infusion of 0.1 U/kg per hour. The goal oftherapy is to lower the glucose level by 50 to 100mg/dL per hour.
2. Once the glucose level is in the range of 250 to350 mg/dL, 5% glucose should be initiated;when the glucose level is between 180 to 240mg/dL, the infusate can be changed to 10%glucose.
F. Correcting acidosis. Alkali therapy is usually notnecessary to correct the acidosis associated withDKA. If acidosis is severe, with a pH less than 7.1,sodium bicarbonate can be infused slowly at a rateof 1 to 3 mEq/kg per 12 hours and discontinuedwhen the pH exceeds 7.2.
III. Long-term diabetes managementA. Intensive management of diabetes results in a
significant reduction in the development of diabeticcomplications: a 76% reduction in retinopathy, a39% reduction in microalbuminuria, and a 60%reduction in neuropathy.
Target Blood Glucose Range (Preprandial)
Age Glucose Levels (mg/dL)
Infants, tod-dlers
120-220
Preschoolchildren
100-200
School-agechildren
70-150
B. Insulin regimens1. Starting dose of insulin. Most newly diagnosed
patients with type 1 diabetes can be started on0.2 to 0.4 units of insulin per kg. Adolescentsoften need more. The dose can be adjustedupward every few days based upon symptomsand blood glucose measurements.
2. Dosing regimens. Insulin should be provided intwo ways – as a basal supplement with anintermediate- to long-acting preparation and aspre-meal bolus doses of short-acting insulin (tocover the extra requirements after food is ab-sorbed).
3. Monomeric insulins a. Insulin lispro (Humalog) has an onset of
action within 5 to 15 minutes, peak action at30 to 90 minutes, and a duration of action of2 to 4 hours. Insulin lispro is the preferredinsulin preparation for pre-meal bolus doses.
b. Insulin aspart (Novolog) is anothermonomeric insulin. It is a rapid-acting insulinanalog with an onset of action within 10 to 20minutes. Aspart reaches peak concentrationsin 40-50 minutes and has a duration of actionof 3-5 hours. Insulin aspart, like insulin lispro,can be injected immediately before meals,and has a shorter duration of action thanregular insulin. Insulin aspart has a slightlyslower onset and longer duration of actionthan insulin lispro.

Pharmacokinetics of Insulin Preparations
Type ofinsulin
Onsetofaction
Peakofaction
Dura-tionofac-tion
Common pitfalls
Insulinlispro(Humalog)
5 to 15min-utes
45 to75min-utes
2 to 4hours
Hypoglycemia oc-curs if the lag timeis too long; withhigh-fat meals, thedose should beadjusted down-ward.
Insulinaspart(Novolog)
10 to20min-utes
40 to50min-utes
3 to 5hours
Regularinsulin(HumulinR)
30min-utes
2 to 4hours
5 to 8hours
The insulin shouldbe given 20 to 30minutes before thepatient eats.
Insulinglargine(Lantus)
1 to 3hours
5 to 7hours
13 to18hours
Has a constantglucose-loweringprofile withoutpeaks and valleys,allowing it to beadministered onceevery 24 hours.
NPH in-sulin(HumulinN)
1 to 3hours
6 to 12hours
18 to28hours
In many patients,breakfast injectiondoes not last untilthe evening meal;administration withthe evening mealdoes not meet in-sulin needs onawakening.
Lenteinsulin(HumulinL)
1 to 3hours
4 to 8hours
13 to20hours
Loses its effect if itis left in the sy-ringe for more thana few minutes.
Total Daily Insulin Dosage
<5 Years(U/kg)
5-11 Years(U/kg)
12-18 Years(U/kg)
0.6-0.8 0.75-0.9 0.8-1.5
Newly diagnosed patients and those who are in theremission phase may require less insulin.
4. Twice-daily regimens. If the goal is relief fromhyperglycemic symptoms with a regimen that issimple, then twice-daily NPH insulin will beeffective in many patients. Injection of regularplus NPH insulin before breakfast and beforedinner results in four peaks of insulin action,covering the morning, afternoon, evening, andovernight, but the peaks tend to merge.
5. Insulin glargine (Lantus). While NPH insulin isthe insulin most commonly given at bedtime,insulin glargine may be equally effective forreducing HbA1c values and cause lesshypoglycemia.
C. Insulin regimens for intensive therapy of diabe-tes mellitus1. Multiple daily injections. The most commonly
used multiple-dose regimen consists of twice-daily injections of regular and intermediate-acting insulin (NPH).
2. Although a twice-daily regimen improvesglycemic control in most patients, the morningdose of intermediate-acting insulin may not besufficient to prevent a post-lunchtime rise inblood glucose concentrations. The intermediate-acting insulin administered before the eveningmeal may not be sufficient to inducenormoglycemia the next morning unless a largerdose is given, which increases the risk ofhypoglycemia during the night. If necessary, thetwice-daily regimen can be converted into athree- or four-injection program.
3. In contrast to NPH insulin, the time-action profilefor insulin glargine has virtually no peak, whichmay make it the ideal basal insulin for intensiveinsulin therapy in type 1 diabetes.

4. Monomeric insulins, insulin lispro and insulinaspart, may be most useful in patients in whomhigh postprandial blood glucose concentrationsand unexpected high blood-glucose values atother times are problems.
5. Inhaled insulin may become an alternative tomonomeric insulins in the future. It causes a veryrapid rise in serum insulin concentrations (similarto that achieved with subcutaneous insulinlispro). Typical premeal doses consists of 1.5units per kg taken five minutes before a meal.
D. Blood glucose monitoring. Children and adoles-cents should test their blood glucose levels at leastfour times a day, before meals and at bedtime.Quarterly measurement of hemoglobin A1c (HbA1c)assesses glycemic control and reflects the averageblood glucose over the last 120 days.
Assessment of HbA1c Values
HbA1c Values Level of Glycemic Control
HbA1c >10% Poor or minimal
HbA1c 8.0-10.0% Average
<8.0% Excellent or intensive
References, see page 182.
Menstrual Disorders
The median age of menarche is 12.8 years, and thenormal menstrual cycle is 21 to 35 days in length. Bleed-ing normally lasts for 3 to 7 days and consists of 30 to 40mL of blood. Cycles are abnormal if they are longer than8 to 10 days or if more than 80 mL of blood loss occurs.Soaking more than 25 pads or 30 tampons during amenstrual period is abnormal.
I. PathophysiologyA. Regular ovulatory menstrual cycles often do not
develop until 1 to 1.5 years after menarche, and 55-82% of cycles are anovulatory for the first 2 yearsafter menarche. Anovulatory cycles typically causeheavier and longer bleeding.
B. Adolescents frequently experience irregular men-strual bleeding patterns, which can include severalconsecutive months of amenorrhea.
II. AmenorrheaA. Primary amenorrhea is defined as the absence of
menarche by age 16. Puberty is considered delayedand warrants evaluation if breast development (theinitial sign of puberty in girls) does not begin by theage of 13. The mean time between the onset ofbreast development and menarche is 2 years.Absence of menses within 2 to 2.5 years of theonset of puberty should be evaluated.
B. Secondary amenorrhea is defined as the absenceof 3 consecutive menstrual cycles or 6 months ofamenorrhea in patients who have already estab-lished regular menstrual periods.

Differential Diagnosis of Amenorrhea
PregnancyHormonal ContraceptionHypothalamic-related Dis-orders
Chronic or systemic ill-nessStressAthleticsEating disordersObesityDrugs Tumor
Pituitary-related DisordersHypopituitarismTumorInfiltrationInfarction
Ovarian-related DisordersDysgenesisAgenesisOvarian failureResistant ovary
Outflow Tract-related Dis-orders
Imperforate hymenTransverse vaginal sep-tumAgenesis of the vagina,
cervix, uterusUterine synechiae
Androgen ExcessPolycystic ovarian syn-dromeAdrenal tumorAdrenal hyperplasia
(classic andnonclassic)
Ovarian tumorOther Endocrine Disorders
Thyroid diseaseCushing syndrome
C. Amenorrhea with pubertal delay1. Hypergonadotropic hypogonadism is caused
by ovarian failure associated with elevatedgonadotropin levels. An elevated FSH will estab-lish this diagnosis.a. Turner syndrome (XO) may cause ovarian
failure and a lack of pubertal development.Females with Turner syndrome have streakgonads, absence of one of the X chromo-somes, and inadequate levels of estradiol.They do not initiate puberty or uterine devel-opment. This syndrome is characterized byshort stature, webbed neck, widely spacednipples, shield chest, high arched palate,congenital heart disease, renal anomalies,and autoimmune disorders (thyroiditis, Addi-son disease). It may not be diagnosed untiladolescence, when pubertal delay andamenorrhea occur together.
b. Ovarian failure resulting from autoimmunedisorders or exposure to radiation or chemo-therapy may also cause amenorrhea withpube r ta l de lay assoc ia ted wi thhypergonadotropic hypogonadism.
2. Hypogonadotropic hypogonadism is causedby hypothalamic dysfunction or pituitary failure.Low or normal levels of LH and FSH will bepresent, and decreased estradiol levels may bepresent.a. Abnormalities of the pituitary and hypo-
thalamus, and other endocrinopathies (thy-roid disease and Cushing syndrome) maypresent with pubertal delay and low gonado-tropin levels.(1) Amenorrhea may be caused by problems
at the level of the pituitary gland, such ascongenital hypopituitarism, tumor (pitu-i tary adenoma), or infi l trat ion(hemochromatosis).
(2) Prolactin-secreting pituitary adenoma(prolactinoma) is the most commonpituitary tumor. Prolactinomas presentwith galactorrhea, headache, visual fieldscuts, and amenorrhea. Elevated prolactinlevels are characteristic.
(3) Craniopharyngioma is another tumor ofthe sella turcica that affects hypothalamic-pituitary function, presenting with pubertaldelay and amenorrhea.
(4) Other disorders associated withgalactorrhea and amenorrhea includehypothyroidism, breast stimulation, stressassociated with trauma or surgery,phenothiazines, and opiates.
b. Hypothalamic suppression is most com-monly caused by stress, competitive athletics,and dieting (anorexia nervosa).
c. Hypothalamic abnormalities associatedwith pubertal delay include Laurence-Moon-Biedl, Prader-Willi, and Kallmann syndromes.Laurence-Moon-Biedl and Prader-Willi pres-ent with obesity. Kallmann syndrome is asso-ciated with anosmia.
D. Amenorrhea with normal pubertal development1. Pregnancy should be excluded when
amenorrhea occurs in a pubertally maturefemale.
2. Contraceptive-related amenorrhea occurs withdepot medroxyprogesterone (Depo-Provera); itdoes not require intervention; however, a preg-nancy test should be completed.
3. Uterine synechiae (Asherman syndrome)should be suspected in amenorrheic femaleswith a history of abortion, dilation and curettage,or endometritis.
4. Sheehan syndrome (pituitary infarction) issuggested by a history of intrapartum bleedingand hypotension.
5. Other disorders associated with amenorrheaand normal pubertal development. Ovarianfailure, acquired abnormalities of the pituitarygland (prolactinoma), thyroid disease, andstress, athletics, and eating disorders maycause amenorrhea after normal pubertal devel-opment. Polycystic ovarian disease, which isusually associated with irregular bleeding, canalso present with amenorrhea.
E. Genital tract abnormalities1. Imperforate hymen will appear as a membrane
covering the vaginal opening. A history of cyclicabdominal pain is common, and a midline ab-dominal mass may be palpable.
2. Transverse vaginal septum may cause ob-struction. It is diagnosed by speculum examina-tion.
3. Agenesis of the vagina appears as a blind-ended pouch. Normal pubertal development ofbreast and pubic hair occurs, but menarchedoes not occur.
4. Androgen insensitivity (testicularfeminization syndrome) is another commoncause of vaginal agenesis.a. Breast development and a growth spurt
occur, but little if any pubic or axillary hair ispresent. These women have an XY chromo-somal pattern with intra-abdominal or inguinaltestes that produce testosterone, but an X-linked inherited defect of the androgen recep-tor prevents response to testosterone.
b. Female-appearing external genitalia arepresent, but the uterus and vagina are ab-sent. During puberty, breast developmentoccurs because of conversion of androgensto estrogens.
c. The testes are at increased risk for develop-ing tumors and must be removed. Hormonereplacement therapy is provided to initiatepuberty.
F. Polycystic ovary syndrome1. PCO is the most common cause of persistent
irregular menses. Only 70% of patients havepolycystic ovaries on ultrasound. The mostcommon symptom is irregular periods beginningwith menarche; however, intervals ofamenorrhea may also occur. Signs includehirsutism, acne, clitoromegaly, and obesity(50%). Insulin resistance, glucose intolerance,and lipid abnormalities are common.
2. Increased facial hair and midline hair over thesternum and lower abdomen are often present.If hirsutism is severe, an ovarian and adrenaltumor or adrenal enzyme deficiency should beexcluded.
3. PCO is probably an autosomal recessive disor-der that affects ovarian steroidogenesis. Ovula-tion occasionally can occur spontaneously;therefore, amenorrhea secondary to pregnancyalways must be considered.
G. Clinical evaluation of amenorrhea1. Chronic or systemic illness, eating disorders,
and drug use, including hormonal contraception,should be excluded. Tanner staging, pelvicexamina t i on , and poss ib l y pe l v i cultrasonography should be completed.
2. Absence of the uterus, vagina, or both re-quires a chromosomal analysis, which candetermine if the karyotype is XX or XY, and itcan help differentiate between müllerianagenesis and androgen insensitivity.
3. If the anatomy is normal, LH, FSH, and estradiol

are indicated in order to distinguish ovarianfailure from hypothalamic dysfunction. High FSHand LH levels and a low estradiol level areindicators of gonadal dysgenesis (Turner syn-drome) or autoimmune oophoritis. Normal or lowLH, FSH, and estradiol levels indicate hypotha-lamic suppression, central nervous systemtumor, or an endocr inopathy (eg,hypothyroidism).
4. Pregnancy must always be excluded if theindividual is mature pubertally.
5. Free-T4, TSH, and prolactin levels are checkedt o e x c l u d e h y p o t h y r o i d i s m a n dhyperprolactinemia. If the prolactin level iselevated, an MRI is necessary to excludeprolactinoma.
6. Hirsutism and acne are indicative of androgenexcess and PCO. Total testosterone anddehydroepiandrosterone sulfate (DHEAS) levelsare necessary to exclude ovarian and adrenaltumors. A testosterone level >200 ng/dL andDHEAS >700 μg/dL require further investigationto exclude a tumor.
7. A morning 17-hydroxyprogesterone level willscreen for nonclassic adrenal hyperplasia. A 17-hydroxyprogesterone >2 ng/mL is followed by anACTH stimulation test to diagnose 21-hydroxy-lase deficiency.
8. An elevated LH-to-FSH ratio is common withPCO; an ultrasonographic examination maydetect polycystic ovaries.
H. Treatment of amenorrhea1. Anovulation and the resulting lack of progester-
one increases the risk of endometrial hyperpla-sia and endometr ia l cancer. Oralmedroxyprogesterone or an oral contraceptive(OCs) should be prescribed to eliminate thisrisk. Oral progestins can be given cyclically for12 days every month or every third month.
2. PCO is treated with OCs to regulate mensesand to decrease androgen levels. Electrolysisand spironolactone (50 mg tid) can decreasehirsutism.
3. Hypoestrogenic and anovulatory patientswith hypothalamic suppression caused by an-orexia, stress, or strenuous athletics shouldmodify their behavior and be prescribed calciumand hormonal replacement therapy (OCs) toreduce the risks of osteoporosis.
4. Turner syndrome or ovarian failure requiresestrogen and progesterone at a dosage suffi-cient to induce pubertal development, afterwhich time they can be switched to an OC.
III. Abnormal vaginal bleedingA. Abnormal vaginal bleeding is characterized by
excessive uterine bleeding or a prolonged numberof days of bleeding. The most common cause ofabnormal vaginal bleeding in adolescence isanovulation. Abnormal bleeding is common duringthe first 1 to 2 years after menarche becauseanovulatory cycles are frequent.
B. Differential diagnosis of abnormal vaginalbleeding1. Pregnancy, pregnancy-related complications,
sexually transmitted diseases, pelvic inflamma-tory disease, and retained tampons should beexcluded.
2. Vaginal tumors, uterine or cervical carcinoma,and uterine myomas are rare in adolescents.
3. Blood dyscrasias or coagulation defects mayoccasionally be the initial presentation of abnor-mal vaginal bleeding.
4. Hormonal contraceptives are a commoncause of breakthrough bleeding.
C. Clinical evaluation of irregular vaginal bleeding1. Age of menarche, menstrual pattern, amount of
bleeding, symptoms of hypovolemia, history ofsexual activity, genital trauma, and symptoms ofendocrine abnormalities or systemic illnessshould be evaluated.
2. Postural vital signs may suggest hypovolemia. Apelvic examination should assess pelvic anat-omy and exclude trauma, infection, foreign body,or a pregnancy-related complication. Pelvicultrasonography can be used to further assesspelvic anatomy.

Differential Diagnosis of Abnormal Vaginal Bleed-ing
Pregnancy related. Ectopic pregnancy, abortionHormonal contraception. Oral contraceptives, depo-
medroxyprogesteroneHypothalamic-related. Chronic or systemic illness, stress,
athletics, eating disorder, obesity, drugsPituitary related. Prolactinoma, craniopharyngiomaOutflow tract-related. Trauma, foreign body, vaginal tumor,
cervical carcinoma, polyp, uterine myoma, uterine carci-noma, intrauterine device
Androgen excess. Polycystic ovarian syndrome, adrenaltumor, ovarian tumor, adrenal hyperplasia
Other endocrine causes. Thyroid disease, adrenal diseaseHematologic causes. Thrombocytopenia, clotting abnormali-
ties, abnormalities of platelet function, anticoagulantmedications
Infectious causes. Pelvic inflammatory disease, cervicitis
3. Laboratory evaluationa. A pregnancy test and complete blood
count should be completed.b. A history of a very heavy period with
menarche or repeated prolonged or heavymenses warrants a prothrombin time andpartial thromboplastin time to screen forbleeding abnormalities; a bleeding time andvon Willebrand screening panel will identifymore specific coagulation disorders.
c. Signs of androgen excess indicate a needto exclude PCO.
d. Chronic irregular vaginal bleeding man-dates that prolactinoma and endocrineabnormalities (thyroid disease) be excluded.
D. Treatment of irregular vaginal bleeding1. Mild bleeding or shortened cycles associated
with a normal physical examination and normalvital signs requires only reassurance.
2. Mild anemia associated with stable vital signsis treated with a 35 to 50 mcg monophasiccombination OC as follows: One pill QID x 4days. One pill TID x 3 days. One pill BID x 7days. One pill QD x 7-14 days. Stop all pills for7 days and then begin cycling on a low doseOCP QD.
3. The patient should be continued on low-doseOCs for 3 to 4 months before allowing resump-tion of normal cycles. Iron therapy should beincluded.
4. If the hematocrit is <7-8 mg/dL or if vitalsigns are unstable, hospitalization is recom-mended. Intravenous conjugated estrogens(Premarin), 25 mg IV every 4-6 hours for 24hours, will stop the bleeding quickly. Conjugatedestrogen therapy is followed immediately byOCs and iron therapy. Blood transfusion iswarranted only if the patient is severely symp-tomatic. Dilatation and curettage is used as alast resort; however, it is rarely necessary.
5. Antiprostaglandin medications (NSAIDs)decrease menstrual blood loss significantly bypromoting platelet aggregation andvasoconstriction. They do not have the hor-monal side effects of OCs, and they can beused alone in mild cases of abnormal vaginalbleeding.
IV. DysmenorrheaA. Fifty percent of adolescents experience
dysmenorrheaB. Primary dysmenorrhea consists of crampy lower
abdominal and pelvic pain during menses that isnot associated with pelvic pathology. It is the mostcommon form of dysmenorrhea, usually beginning6 months to 1 year after menarche.
C. Secondary dysmenorrhea is defined as painfulmenses associated with pelvic pathology(bicornate uterus, endometriosis, PID, uterinefibroids and polyps, cervical stenosis, ovarianneoplasms). If dysmenorrhea is severe, obstructinglesions of the genital tract should be excluded.Endometriosis is the most common cause (50%) ofchronic pelvic pain in adolescents.
D. Evaluation of dysmenorrhea1. Gynecologic history should determine the
relationship of the pain to the menstrual cycle,severity, and sexual activity.
2. If the pain is mild, easily relieved by NSAIDs,

and the physical examination (including thehymen) are normal, a speculum examination isnot necessary.
3. Severe pain requires a pelvic examination toexclude genital tract obstruction, adnexal and/oruterosacral pain (endometriosis), PID, or amass. Ultrasonography is useful for evaluatingpelvic abnormalities or obstruction.
E. Treatment of dysmenorrhea1. Initial treatment consists of a prostaglandin
synthesis inhibitor, initiated with the onset ofbleeding and continued for as long as painlasts. Gastric irritation can be reduced by takingthe drug with food. a. Mefenamic acid (Ponstel) 500 mg loading
dose, then 250 mg q6h.b. Ibuprofen (Advil) 400-600 mg q4-6h.c. Naproxen sodium (Aleve) 550 mg load,
then 275 mg q6h.d. Naproxen (Naprosyn) 500 mg load, then
250 mg q6-8h.2. Oral contraceptives are also very effective and
can be added if the antiprostaglandin is not fullyeffective.
References, see page 182.
Nocturnal Enuresis
Nocturnal enuresis affects approximately 5 to 7 millionchildren in the United States. Parents may becomeconcerned about nocturnal enuresis when their childreaches 5 to 6 years of age. There is a slight male pre-dominance of 60% for nocturnal enuresis. Etiologic factorsinclude genetics, sleep arousal dysfunction, urodynamics,nocturnal polyuria, psychological components, andmaturational delay.
I. Clinical evaluationA. History
1. A detailed toilet training history and a familyhistory of enuresis should be sought. Otherpertinent details include the onset and pattern ofwetting, voiding behavior, sleep pattern,parasomnias, medical conditions, daytime urinarysymptoms, bowel habits, and psychosocial fac-tors.
2. Urgency or a history of small, frequent voidssuggests bladder instability or small bladdercapacity. Dysuria suggest a urinary tract infection.Polyuria and polydipsia suggest diabetesinsipidus or mellitus. Encopresis suggests consti-pation. Nighttime snoring suggests adenoidalhypertrophy.
B. Physical examination1. Most children who have nocturnal enuresis will
have normal findings on physical examination.Height, weight, and blood pressure should berecorded.
2. A palpable bladder, palpable stool, ectopic ureter,signs of sexual abuse, or abnormal gait should besought. Cremasteric, anal, abdominal, and deeptendon reflexes that reflect spinal cord function allshould be tested.
3. The skin of the lower back should be inspectedfor a sacral dimple, hair patches, or vascularbirthmarks, which indicate spinal dysraphism.Mouth breathing may suggest sleep apnea withassociated enuresis due to adenoidal hypertro-phy.
4. Direct observation of the urinary stream is impor-tant if findings suggest an abnormality. Bladdercapacity can be measured in the office by havingthe child drink 12 oz of fluid on arrival, thenvoiding into a calibrated cup.
C. Laboratory/imaging studies. All children shouldhave urinalysis of a clean-catch midstream urinespecimen. The ability to concentrate urine to 1.015or greater rules out diabetes insipidus and theabsence of glucose rules out diabetes mellitus. Aurine culture should be obtained if the child hasdysuria or an abnormal urinalysis.
II. Treatment A. Nonpharmacologic therapy
1. Motivational therapy. The child should be takenout of diapers or training pants and encouraged to

empty the bladder completely prior to going tobed. The child should participate in morningcleanup. Fluids should be restricted for 2 hoursprior to bedtime.
2. Behavioral therapya. Hypnotherapy involves having the child prac-
tice imagery of awakening to urinate in thetoilet or staying dry all night.
b. Dry-bed training involves waking the childover several nights, and having the child walkto the toilet when voiding is needed. Theeventual goal is to have the child self-awakento void.
c. Enuresis alarms have the highest overall curerate. Alarm systems can be used in combina-t ion wi th behav io ra l therapy orpharmacotherapy. The cure rate may be ashigh as 70% long-term.
B. Pharmacotherapy. Medication for nocturnalenuresis seldom should be considered before 8years of age.1. Imipramine (Tofranil)
a. Imipramine increases bladder capacity andalso may decrease detrusor muscle contrac-tions. The starting dose is 25 mg taken 1 hourbefore bedtime for children ages 6 to 8 yearsand 50 to 75 mg for older children and adoles-cents. The dose may be increased in 25-mgincrements weekly up to 75 mg. Therapy maycontinue from 3 to 9 months, with a slow taper-ing over 3 to 4 weeks. Imipramine is inexpen-sive. The success rate is 15 to 50%.
b. Mild side effects include irritability, dry mouth,decreased appetite, headaches, and sleepdisturbances. Overdose can be lethal.
2. DDAVP (Stimate)a. DDAVP is a synthetic analog of arginine
vasopressin (ADH). It decreases urine volume.The bioavailability is only 1% for the tablet and10% for the nasal spray. The initial dose ofDDAVP is 20 mcg PO or one 10-mcg puff ineach nostril within 2 hours of bedtime. Thedose may be increased in increments of 10mcg every 1 or 2 weeks up to a maximumdose of 40 mcg. Patients may remain onmedication for 3 to 6 months, then shouldbegin a slow decrease of the dose by 10mcg/mo. If oral medication is preferred, thestarting dose is 0.2 mg (one tablet) 1 hourbefore bedtime. If there is no response within1 week, the dose can be titrated by 0.2 mg upto a maximum of 0.6 mg nightly.
b. Side effects of DDAVP are rare and includeabdominal discomfort, nausea, headache, andepistaxis. Symptomatic hyponatremia withseizures is very rare. Contraindications includehabit polydipsia, hypertension, and heartdisease. About 22% become dry with DDAVP.
c. The high initial response rate of DDAVP isattractive for episodic use for summer campand sleepovers.
C. Age-related treatments1. Younger than age 8 years. Motivational and
behavioral methods that assist the child in wakingto void and that praise successful dryness arerecommended.
2. Ages 8 through 11 years. The enuresis alarmgives the best results in terms of response rateand low relapse rate. Intermittent use of medica-tion such as DDAVP can be useful for specialevents.
3. Ages 12 years and older. If use of an enuresisalarm does not stop wetting episodes, continuoususe of medication is justified.
References, see page 182.
Poisoning
Poisoning is defined as exposure to an agent that cancause organ dysfunction, leading to injury or death.Children less than 6 years of age account for 60.8% ofpoisonings.
I. Clinical evaluation of poisoningA. The type of toxin involved should be determined.

The time of the exposure and how much time haselapsed should be assessed.
B. The dose of the toxin should be assumed to be themaximum amount consistent with the circumstancesof the poisoning.
C. Munchausen syndrome by proxy1. Chemical child abuse should be suspected when
childhood poisonings are associated with aninsidious and/or inexplicable presentation (eg,recurrent acidosis, polymicrobial sepsis, recurrentmalabsorption syndrome, factitious hypoglycemia,failure to thrive).
2. The syndrome is referred to as “Munchausensyndrome by proxy” when the abuse is perpe-trated by a caretaker. Agents may include aspirin,codeine, ethylene glycol, fecal material, insulin,ipecac, laxatives, phenothiazines, table salt, andvitamin A.
II. Physical examinationA. The first priority in a severely poisoned child is to
maintain an airway, ventilation, and circulation. B. The vital signs, breath odors, skin, gastrointestinal,
cardiovascular, respiratory, and neurologic systemsshould be assessed.
Physical Findings Associated with Specific Drugsand Chemicals
Symptomor Sign
Agents
Fever Amphetamines, anticholinergics, antihista-mines, aspirin, cocaine, iron, phencyclidine,phenothiazines, thyroid, tricyclic antidepres-sants
Hypother-mia
Barbiturates, carbamazepine, ethanol,isopropanol, narcotics, phenothiazines
Breathodors:
Moth-ballsFruityGarlicBitteralmondPeanuts
Naphthalene, paradichlorobenzeneIsopropanol, acetone, nail polish removerArsenic, organophosphatesCyanideN-3-pyridylmethyl-N-4-nitrophenylurea(VACOR rat poison)
Hyperten-sion
Amphetamines, cocaine, ephedrine, ergotism,norepinephrine, phenylpropanolamine, tricyclicantidepressants (early)
Hypotension
Antihypertensives, arsenic, barbiturates,benzodiazepines, beta blockers, calcium chan-nel blockers, carbon monoxide, cyanide,disulfiram, iron, nitrites, opiates,phenothiazines, tricyclic antidepressants (late)
Tachypnea Amphetamine, cocaine, carbon monoxide,cyanide, iron, nicotine, phencyclidine, salicy-lates
Hypoventilation
Alcohols, anesthetics, barbiturates,benzodiazepines, botulism, chlorinated hydro-carbons, cholinesterase-inhibiting pesticides,cyclic antidepressants, narcotics, nicotine, par-alytic shellfish poisoning, solvents, strychnine
Coma Alcohols, anticonvulsants, barbiturates,benzodiazepines, carbon monoxide, chloralhydrate, cyanide, cyclic antidepressants, hy-drocarbons, hypoglycemics, insulin, lithium,narcotics, phenothiazines, salicylates,sedative-hypnotics, solvents
Seizures Amphetamines, camphor, carbon monoxide,cocaine, gyromitra mushrooms, isoniazid, lead,lindane, nicotine, pesticides, phencyclidine,salicylates, strychnine, theophylline, tricyclicantidepressants
Miosis Narcotics, organophosphates, phenothiazines,phencyclidine
Mydriasis Amphetamine, anticholinergics, antihistamines,atropine, cocaine, phenylpropanolamine,tricyclic antidepressants
Nystagmus Phencyclidine, phenytoin
Peripheralneuropathy
Acrylamide, carbon disulfide, heavy metals

C. Skin examination1. Cyanosis suggests hypoxia secondary to aspira-
tion (eg, hydrocarbon) or asphyxia (eg, apneadue to central nervous system depressants).
2. The adolescent substance abuser may haveneedle tracks along veins or scars from subcuta-neous injections. Urticaria suggests an allergicreaction. Jaundice may signify hemolysis fromnaphthalene mothballs.
D. Cardiovascular effects1. Sympathetic stimulation can cause hypertension
with tachycardia.2. Hypotension is caused by beta adrenergic block-
ade, calcium channel blockade, sympatholyticagents, cellular toxins, psychopharmaceuticalagents, disulfiram-ethanol, and shock associatedwith iron or arsenic.
E. Respiratory effects 1. Tachypnea and hyperpnea may result from
salicylate poisoning. Nervous system stimulantsmay be associated with tachypnea. Cellularpoisons will increase the respiratory rate.
2. Central nervous system depressants maydepress the respiratory drive.
3. Apnea may be associated with toxins causingweakness of respiratory muscles. The respiratoryexamination may reveal poisoning-associatedwheezing (eg, beta-blocker overdose or inhal-ants) or crackles (aspiration pneumonia, pulmo-nary edema).
F. Neurologic examination1. Depressed consciousness, confusion, delirium,
or coma may result from toxins, such as ethanol.Central nervous system stimulants or neurotrans-mitter antagonists produce seizures.
2. Pupils. Dilated pupils can be caused by sympa-thetic stimulation (eg, amphetamine, cocaine).Constricted pupils are caused by parasympa-thetic stimulation (eg, organophosphate pesti-cides) or sympathetic blockade (eg,phenothiazines).
3. Sensorimotor examination may reveal periph-eral anesthesia caused solvents, pesticides, oracrylamide.
4. Neurologic signs of substance abusea. Ethanol, isopropyl alcohol, ethylene glycol,
or methanol can cause an alcoholic state ofintoxication. Amphetamine or cocaine oftencause agitation, euphoria, or paranoia. Lyser-gic acid diethylamide (LSD), mescaline oramphetamines can cause visual or auditoryhallucinations.
b. Benzodiazepines and narcotics (oxycodone)can cause drowsiness, slurred speech, confu-sion, or coma. Phencyclidine (PCP) causesagitation, dissociative delusional thinking,rhabdomyolysis, and rotatory nystagmus. Glueor gasoline sniffing can result in exhilaration,grandiose delusions, irrational behavior, andsudden death from cardiac dysrhythmias.
III. Laboratory assessmentA. Toxic screens
1. The history and physical examination will usuallyprovide enough information to make a diagnosisand begin therapy. Occasionally, toxin screeningof blood and/or urine can confirm the diagnosis.
2. A toxic screen of the blood and urine may includeassays for acetone, acetaminophen, amphet-amines, anticonvulsants, antidepressants, anti-histamines, benzodiazepines, ethanol,isopropanol, methanol, narcotics, neuroleptics, orphencyclidine.
B. Serum osmolarity1. The osmolar gap is derived from the measured
serum osmolality minus the calculated serumosmolality (2 x Na + BUN/2.8 + glucose/18).When exogenous osmoles are present (eg,ethanol, isopropyl alcohol, methanol, acetone, orethylene glycol), the osmolar gap will be ele-vated.
2. Anion gap acidosisa. Lactic acid (eg, in ethanol, isoniazid, iron
poisonings), ketoacids (eg, diabetes, ethanol),or exogenous organic acids may cause ametabolic acidosis.
b. Metabolic acidoses are classified as either

increased anion gap ([Na+ K] - [Cl + HCO3])above 15 mEq/L (ethylene glycol, iron,isoniazid, methanol, or salicylate), or de-pressed anion gap (lithium), or normal aniongap (laxatives, colchicine).
C. Other frequently ordered tests1. Hepatic and renal function should be monitored
because most toxins are detoxified in the liverand/or excreted in the urine. Many poisoningsare accompanied by rhabdomyolysis (elevatedcreatinine phosphokinase levels) from seizures,hyperthermia, or muscle spasms.
2. Urine that fluoresces under Wood lamp exam-ination is diagnostic of antifreeze poisoning.
3. Chest and abdominal radiographs may showradiopacities from calcium tablets, chloral hy-drate, foreign bodies, iodine tablets, phenothi-azine and antidepressant tablets, and en-teric-coated capsules.
4. Serial electrocardiograms are essential withantiarrhythmic drugs, beta- blockers, calciumchannel blockers, lithium, phenothiazines,theophylline, or tricyclic antidepressants.
IV. Diagnostic trialsA. For a few poisons, a “diagnostic trial” of an antidote
can implicate an agent as the cause of a poison-ing.
Diagnostic Trials
Toxin DiagnosticTrial
Route
Positive Re-sponse
Benzo-diazepine
Flumazenil0.02 mg/kg
IV Consciousness im-proves
Digitalis Specific Fabantibodies
IV Dysrhythmia resolves,hyperkalemia im-proves,consciousness im-proves
Insulin Glucose 1g/kg
IV Consciousness im-proves
Iron Deferoxamine40 mg/kg
IM Pink “vin rose” urine
Isoniazid Pyridoxine 5 g IV Seizures abate
Opiate Naloxone 0.1mg/kg
IV Consciousness im-proves
Phenothi-azine
Diphenhydramine 1 mg/kg
IV Dystonia andtorticollis resolve
V. ManagementA. Poison centers can help with the diagnosis and
management of poisonings, and assist in locatingexotic antidotes.
B. Initial management of poisoning involves main-taining an airway, providing ventilatory support,securing vascular access, and initiating resuscita-tion.
C. Decontamination1. Skin, mucous membrane, or eye exposures
should be washed with a stream of lukewarmwater for 15 to 20 minutes. Soap is used todecontaminate skin exposures.
2. Gastric lavagea. Decontamination by lavage is preferred over
emesis in the emergency department be-cause it is controllable. Contraindicationsinclude nontoxic ingestions, ingestions inwhich the substance is already past the stom-ach or absorbed, and caustic or hydrocarboningestions. It is most successful when per-formed within 90 minutes of the ingestion. Fortoxins associated with delayed gastric empty-ing (eg, aspirin, iron, antidepressants,antipsychotics) or for those that can formconcretions (eg, iron, salicylates), lavage maybe beneficial hours later.
b. A large-bore (24-32F) orogastric tube isused, and 100- to 200-cc aliquots of warm,normal saline are infused/withdrawn until nomore pill fragments are detectable in thelavage fluid or until about 2 liters have beenexchanged.
c. Activated charcoal is effective for absorbing

most drugs, but it is ineffective for alcohols,caustics, cyanide, heavy metals, lithium, andsome pesticides.
d. Overdoses of carbamazepine, tricyclic antide-pressants, and procainamide are managedwith multiple doses of charcoal. Contraindica-tions to charcoal include a poisoning whereesophageal endoscopy is contemplated, onein which the toxin is not adsorbed by charcoal,or a poisoning in which the patient has anileus, gastrointestinal hemorrhage, or re-peated retching.
3. Enhanced eliminationa. Multiple doses of charcoal also can enhance
elimination by “gastrointestinal dialysis.”Repetitive doses of charcoal are recom-mended for phenobarbital, salicylate, andtheophylline poisoning.
b. A cathartic, such as magnesium citrate, isrecommended when charcoal is used be-cause charcoal is constipating. Hemodialysisor hemoperfusion can be life-saving for se-vere intoxications.
VI. Specific toxinsA. Acetaminophen (APAP)
1. Single overdoses of greater than 150 mg/kg cancause liver failure. Nausea and abdominal painare common. The patient may vomit repeatedly,be mildly lethargic, or remain asymptomatic. At24 to 36 hours after the ingestion, abdominaltenderness and rising serum transaminaselevels signify onset of hepatitis that peaks inseverity by 96 hours.
2. The Rumack nomogram predicts the likelihoodof hepatitis. The peak concentration is measured4 hours after the ingestion; levels greater than200 mcg/mL at 4 hours are associated with livertoxicity.
3. When acetaminophen has been taken in highdose, or when acetaminophen levels are in therange likely to cause hepatotoxicity,N-acetylcysteine (NAC) is given at a loadingdose of 140 mg/kg, followed by 17 doses of 70mg/kg separated by 4-hour intervals.
4. Once NAC has been started because of onetoxic level, the full course should be given; thereis no need to get repeated APAP concentrations.
B. Alcohols1. Alcohols include ethanol, ethylene glycol, metha-
nol, and isopropyl alcohol. Antifreeze containsethylene glycol, Sterno and windshield wiperfluid contain methanol, jewelry cleaners andrubbing alcohol contain isopropanol.
2. All of the alcohols cause inebriation, loss ofmotor control and coma. Ethylene glycol maycause acidosis, renal failure, and seizures.Methanol may cause metabolic acidosis, sei-zures, and blindness. Isopropyl alcohol canproduce gastritis, ketosis, and hypotension.
3. Concentrations of ethylene glycol or methanol>20 mg/dL require the use of ethanol therapy toblock alcohol dehydrogenase conversion to thetoxic metabolites; hemodialysis is indicated forconcentrations >50 mg/dL. Isopropanol or etha-nol intoxications usually require only closemonitoring with frequent measurements ofserum glucose. Respiratory depression, sei-zures, and coma from ethanol poisoning andlevels >300-400 mg/dL require hemodialysis.
C. Caustics1. Drain cleaners contain sodium hydroxide or
sulfuric acid; toilet cleaners may contain hydro-chloric or sulfuric acids.
2. Laundry or dishwasher detergents may con-tain sodium metasilicate or sodium triphosphate.
3. Signs of caustic ingestion include lip or tongueswelling; burning pain; dysphagia; drooling; andwhitish or red plaques on the tongue, buccal orpalatal mucosa, or in the perioral area. Causticscan cause severe burns to the esophagus orstomach even in the absence of symptoms.
4. Inhalations are managed with humidified oxy-gen. Skin exposures are washed carefully withsoap and water and then treated like any otherburn.
5. Strongly alkaline agents damage the upperesophagus. Hydrochloric, sulfuric (muriatic),

and other acids damage the lower esophagusand stomach.
6. Treatment of caustic ingestions. The childshould be given nothing by mouth, and endo-scopic evaluation should be performed 12 to 24hours after the ingestion. Emesis, lavage andcharcoal are contraindicated.
D. Foreign body ingestion1. Aspirated objects will cause symptoms of
choking, gasping, coughing, cyanosis, wheezing,fever, and poor air entry. While chest radiogra-phy can confirm the diagnosis, a negative filmdoes not rule out aspiration. A foreign bodyrequires immediate removal by bronchoscopy.
2. Ingestion of disc batteries requires removalwhen lodged in the esophagus; those in thestomach or beyond should be followed withrepeated abdominal films every 2 to 3 days toensure passage. Disc batteries that have re-mained in one position for more than 7 days mayrequire surgical removal. Coins or other foreignbodies past the esophagus can be managedwith serial radiographs and parental vigilance fortheir passage.
E. Hydrocarbons1. Aliphatic hydrocarbons include kerosene,
mineral oil, gasoline, and petrolatum. Keroseneand gasoline are capable of causing an aspira-tion pneumonia and CNS depression. Petrola-tum, mineral oil and motor oil do not carry signifi-cant risk of injury. Aliphatic hydrocarbons insmall doses are not harmful if left in the stom-ach. Emesis is contraindicated because of therisk of aspiration; decontamination should beattempted only if a very large dose was taken.
2. Aromatic hydrocarbons, such as xylene ortoluene, are toxic. Aromatic hydrocarbon inges-tions necessitate lavage.
3. Aspiration pneumonia is suggested by gasp-ing, choking, coughing, chest pain, dyspnea,cyanosis, leukocytosis, and fever. A chest radio-graph may not be diagnostic until hours afteringestion.
F. Iron1. Iron is present in many children’s multivitamins,
although the worst cases of iron poisoningusually involve prenatal vitamins, which contain60 mg of elemental iron per tablet. Iron is ametabolic poison and is corrosive to gastricmucosa, resulting in shock.
2. Ferrous sulfate is 20% elemental iron, ferrousfumarate 33%, and ferrous gluconate 11%. Littletoxicity is seen at a dose of elemental iron lessthan 20 mg/kg. Mild symptoms of poisoning areseen at doses of 20-60 mg/kg; moderate-to-severe symptoms at doses of 60 to 100 mg/kg;life-threatening symptoms at doses greater than100 mg/kg; and a lethal dose is 180 to 300mg/kg.
3. Early symptoms include nausea, vomiting,fever, hemorrhagic diarrhea, tachycardia,hypotension, hyperglycemia, and acidosis.Intermediate symptoms (8 to 48 hours afteringestion) may include obtundation, coma,fulminant hepatitis, hypoglycemia, clotting abnor-malities, pulmonary edema, and renal tubulardysfunction.
4. Laboratory findings include a metabolic acido-sis with a high anion gap, an abdominal radio-graph showing radiopaque pills in the stomach,an elevated white blood cell count greater than15,000/mm3, and an elevated blood glucose>150 mg/dL. A serum iron concentration, ob-tained 4 hours after the ingestion, of less than300 mcg/dL is not toxic; 300 to 500 mcg/dL ismildly toxic; 500 to 1000 mcg/dL is moderately toseverely toxic; greater than 1000 mcg/dL is life-threatening.
5. Treatment. Decontamination by lavage shouldbe initiated; charcoal is not effective. Volumeexpansion with intravenous fluids, correction ofelectrolyte/acid-base disturbances, and intrave-nous deferoxamine are recommended.
G. Salicylates1. Aspirin overdoses greater than 150 mg/kg are
toxic. Salicylates are locally corrosive, andtablets can form bezoars near the gastric outlet.

Salicylates stimulate the central respiratorycenter, so that the metabolic acidosis is compen-sated by a respiratory alkalosis.
2. Early symptoms of toxicity include gastrointesti-nal pain, nausea, vomiting, tinnitus, confusion,lethargy, and fever. Respirations often are rapidand deep. Severe poisonings can be associatedwith seizures, coma, and respiratory and cardio-vascular failure.
3. Laboratory findings include hypocalcemia,hypomagnesemia, hypokalemia, andhyperglycemia (early) or hypoglycemia (late).
4. Serum aspirin concentration obtained 2 and 6hours after the ingestion higher than 30 mg/dLare considered toxic, those greater than 70mg/dL are associated with severe symptoms,and those greater than 100 mg/dL are life-threat-ening.
5. Management includes lavage, which may beeffective as long as 4 to 6 hours after the inges-tion. Multiple-dose activated charcoal is effec-tive. Correction of acidemia, hypokalemia, andhypocalcemia are important. Hemodialysis isindicated for serum concentrations greater than100 mg/dL.
References, see page 182.

Developmental Pediatrics
Infant Growth and Development
Infancy consists of the period from birth to about two yearsof age. Advances occur in physical growth, motor develop-ment, cognitive development, and psychosocial develop-ment.
I. Physical growth milestonesA. Birth weight is regained by 2 weeks of age and
doubles by 5 months. During the first few months oflife, this rapid growth continues, after which thegrowth rate decelerates.
Average Physical Growth Parameters
Age Head cir-cumference
Height Weight Dentition
Birth 35.0 cm(13.8 in)
+2 cm/mo (0to 3 mo)
+1 cm/mo (3to 6 mo)
+0.5 cm/mo(6 to 12mo)
Mean = 1cm/mo
50.8 cm(20.0in)
3.0 to 3.5kg(6.6 to7.7 lb)
Regainsbirthweightby 2wk
Doublesbirthweightby 5mo
Centralincisors--6mo
Lateralincisors--8mo
1 year 47.0 cm(18.5 in)
76.2 cm(30.0in)
10.0 kg(22 lb)Triples
birth-weight
Firstmolars--14mo
Canines--19 mo
2years
49.0 cm(19.3 in)
88.9 cm(35.0in)
12.0 to12.5kg(26.4to 27.5lb)
Quadru-plesbirthweight
Secondmolars--24mo
B. Occipitofrontal circumference1. Microcephaly is associated with an increased
incidence of mental retardation, but there is nodirect relationship between small head size anddecreased intelligence. Microcephaly associatedwith genetic or acquired disorders usually hascognitive implications.
2. Macrocephaly may be caused by hydrocepha-lus, which is associated with learning disabilities.Macrocephaly without hydrocephalus is associ-ated with cognitive deficits caused by metabolicor anatomic abnormalities. Fifty percent of casesof macrocephaly are familial and have no effecton intellect. When evaluating the infant withmacrocephaly, the finding of a large head size inone or both parents is reassuring.
C. Height and weight1. Although the majority of individuals who are of
below- or above-average size are otherwisenormal, there is an increased prevalence ofdevelopmental disabilities in these two groups.
2. Many genetic syndromes are associated withshort stature; large stature syndromes are lesscommon. When considering deviation from thenorm, short stature in the family is reassuring.
D. Dysmorphism. Most isolated minor dysmorphicfeatures are inconsequential; however, the pres-ence of three or more indicative of developmentaldysfunction. Seventy-five percent of minor superfi-cial dysmorphisms can be found by examining theface, skin, and hands.
II. Motor development milestonesA. Motor milestones are ascertained from the develop-
mental history and observation. Gross motor devel-opment begins with holding head up, rolling and

progresses to sitting, and then standing, and ambu-lating.
B. Fine motor development1. In the first year of life, the pincer grasp develops.
During the second year of life, the infant learns touse objects as tools during play.
2. Reaching becomes more accurate, and objectsare initially brought to the mouth for oral explora-tion. As the pincer grasp and macular visionimprove, precise manual exploration replacesoral exploration.
C. Red flags in motor development1. Persistent listing to one side at 3 months of age
often is the earliest indication of neuromotordysfunction.
2. Spontaneous frog-legs posturing suggestshypotonia/weakness, and scissoring suggestsspastic hypertonus. Early rolling (1 to 2 months),pulling directly to a stand at 4 months (instead ofto a sit), W-sitting, bunny hopping, and persistenttoe walking may indicate spasticity.
3. Hand dominance prior to 18 months of ageshould prompt the clinician to examine thecontralateral upper extremity for weaknessassociated with a hemiparesis.
III. Cognitive development milestonesA. Language is the single best indicator of intellectual
potential; problem-solving skills are the next bestmeasure. Gross motor skills correlate least withcognitive potential; most infants with mental retarda-tion walk on time.
B. Problem-solving skills1. The 1-year-old child recognizes objects and
associates them with their functions. Thus, hebegins to use them functionally as “tools” insteadof mouthing, banging, and throwing them.
2. Midway through the second year, the child beginsto label objects and actions and categorize them,allowing the child to match objects that are thesame and later to match an object to its picture.
3. Object permanencea. Prior to the infant’s mastery of object perma-
nence, a person or object that is “out of sight”is “out of mind,” and its disappearance doesnot evoke a reaction.
b. The child will progress to finding an object thathas been hidden under a cloth.
c. The next skill in this sequence is the ability tolocate an object under double layers (eg, acube is placed under a cup and then the cupis covered with a cloth).
4. Causality. Initially, the infant accidentally discov-ers that his actions produce a certain effect. Theinfant then learns that actions cause consistenteffects.
C. Language development1. Receptive language skills reflect the ability to
understand language. Expressive language skillsreflect the ability to make thoughts, ideas, anddesires known to others.
2. Prespeech period (0 to 10 months). Receptivelanguage is characterized by an increasing abilityto localize sounds, such as a bell. Expressivelanguage consists of cooing. At 3 months, theinfant will begin vocalizing after hearing an adultspeak. At 6 months of age, the infant adds con-sonants to the vowel sounds in a repetitivefashion (babbling). When a random vocalization(eg, “dada”) is interpreted by the parents as areal word, the parent will show pleasure and joy.In so doing, parents reinforce the repeated use ofthese sounds.
3. Naming period (10 to 18 months). The infant’srealizes that people have names and objectshave labels. The infant begins to use the words“dada” and “mama” appropriately. Infants nextrecognize and understand their own names andthe meaning of “no.” By 12 months of age, someinfants understand as many as 100 words. Theycan follow a simple command as long as thespeaker uses a gesture. Early in the second year,a gesture no longer is needed.
4. The infant will say at least one “real” word (ie,other than mama, dada) before his first birthday.At this time, the infant also will begin to verbalizewith sentence-like intonation and rhythm (imma-ture jargoning). As expressive vocabulary in-

creases, real words are added (maturejargoning). By 18 months, the infant will useabout 25 words.
5. Word combination period (18 to 24 months).Children begin to combine words 6 to 8 monthsafter they say their first word. Early word combi-nations are “telegraphic” (eg, “Go out”). Astranger should be able to understand at least50% of the infant’s speech.
D. Red flags in cognitive development1. Language development provides an estimate of
verbal intelligence; problem-solving provides anestimate of nonverbal intelligence. If deficienciesare global (ie, skills are delayed in both do-mains), there is a possibility of mental retarda-tion.
2. When a discrepancy exists between problem-solving and language abilities, with only languagebeing deficient, the possibility of a hearing impair-ment or a communication disorder should beexcluded. If either language or problem-solvingskills is deficient, the child is at high risk for alearning disability later.
3. All children who have delayed language develop-ment should receive audiologic testing to rule outhearing loss. Deaf infants will begin to babble ontime at 6 months, but these vocalizations willgradually decline thereafter.
IV. Psychosocial developmentA. Emotional development. Emotions are present in
infancy and motivate expression (pain elicits crying).B. Social development
1. Social milestones begin with bonding, whichreflects the feeling of the caregiver for the child.Attachment represents the feeling of the infant forthe caregiver, and it develops within a fewmonths.
2. When recognition of and attachment to a care-giver develops, the simple sight of this person willelicit a smile. The infant becomes more discrimi-nating in producing a smile as he begins todifferentiate between familiar and unfamiliarfaces. The infant learns to use smiling to manipu-late the environment and satisfy personal needs.
3. Temperament represents the style of a child’semotional and behavioral response to situations.
C. Adaptive skill development. Adaptive skills consistof the skills required for independence in feeding,dressing, toileting, and other activities of daily living.Development of adaptive skill is influenced by theinfant’s social environment, and by motor and cog-nitive skill attainment.
D. Red flags in psychosocial development1. Colic may be an early indication of a “difficult”
temperament.2. Delay in the appearance of a smile suggests
an attachment problem, which may be associ-ated with maternal depression. In severe cases,child neglect or abuse may be suspected.
3. Failure to develop social relationships sug-gests autism when it is accompanied by delayedor deviant language development and stereotypicbehaviors.
4. Delays in adaptive skills may indicate overpro-tective parents or an excessive emphasis onorderliness.
References, see page 182.
Toddler Development
Toddlerhood consists of the years from about 1 to 3 yearsof age. Affective development is highlighted by the tod-dler’s striving for autonomy and independence, attachmentto family, and the development of impulse control. Cogni-tive development is characterized by the transition fromsensorimotor to preoperational thought.
I. Growth rate and physical appearanceA. After the rapid growth of infancy, the rate of growth
slows in the toddler years. After age 2, toddlers gainabout 5 lb in weight and 2.5 inches in height eachyear. Growth often occurs in spurts. Between theages of 2 and 2.5 years, the child will have reached50% of his adult height.
B. Growth of the lower extremities often is accompa-

nied by tibial torsion and physiologic bowing of thelegs, which usually corrects by age 3 years. Thepercentage of body fat steadily decreases from 22%at age 1 year to about 15% at age 5 years.
II. Gross motor skillsA. Most children walk without assistance by 18 months.
At 2 years, the stiff, wide-leg gait of earlytoddlerhood becomes a flexible, steady walkingpattern, with heel-toe progression.
Gross Motor Abilities
18 Months
• Walking fast, seldom falling• Running stiffly• Walking up stairs with one hand held• Seating self in a small chair• Climbing into an adult chair• Hurling a ball
24 Months
• Running well without falling• Walking up and down stairs alone• Kicking a large ball
36 Months
• Walking up stairs by alternating feet• Walking well on toes• Pedaling a tricycle• Jumping from a step• Hopping two or three times
III. Fine motor skillsA. The 18-month-old can make a tower of four
blocks. One year later, he can stack eight blocks.Most 18-month-olds will hold the crayon in a fistand scribble spontaneously on paper.
Fine Motor Abilities
18 Months
• Making a tower of four cubes• Releasing 10 cubes into a cup• Scribbling spontaneously• Imitating a vertically drawn line
24 Months
• Building a seven cube tower• Aligning two or more cubes to form a train• Imitating a horizontally drawn line• Beginning circular strokes• Inserting a square block into a square hole
36 Months
• Copying a circle• Copying bridges with cubes• Building a tower of 9 to 10 blocks• Drawing a person’s head
IV. Affective developmentA. Autonomy and independence. Because of im-
proved motor skills, the transition from infancy totoddlerhood is marked increased autonomy andindependence. The toddler may refuse to eatunless allowed to feed himself, and the child mayno longer may be willing to try new foods.
B. Impulse control. Toddlers begin to develop im-pulse control. The 18-month-old may have minimalimpulse control and display several temper tan-trums each day. Most 3-year-olds have somedegree of self-control.
C. Successful toileting usually occurs toward the endof the third year when the child becomes able tocontrol his sphincter, undress, get onto the potty,and has the willingness to participate. Success withconsistent daytime dryness usually is not achieveduntil about 2.5 to 3 years of age.
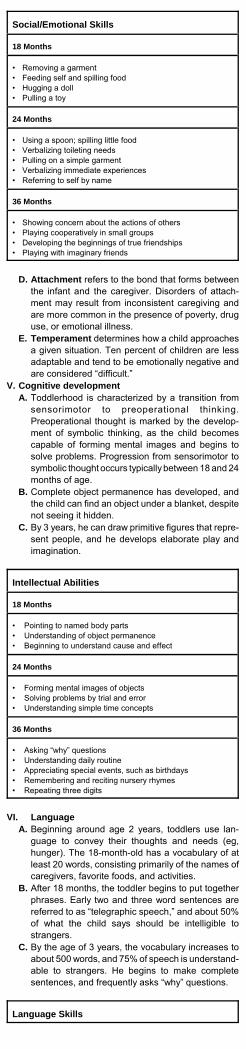
Social/Emotional Skills
18 Months
• Removing a garment• Feeding self and spilling food• Hugging a doll• Pulling a toy
24 Months
• Using a spoon; spilling little food• Verbalizing toileting needs• Pulling on a simple garment• Verbalizing immediate experiences• Referring to self by name
36 Months
• Showing concern about the actions of others• Playing cooperatively in small groups• Developing the beginnings of true friendships• Playing with imaginary friends
D. Attachment refers to the bond that forms betweenthe infant and the caregiver. Disorders of attach-ment may result from inconsistent caregiving andare more common in the presence of poverty, druguse, or emotional illness.
E. Temperament determines how a child approachesa given situation. Ten percent of children are lessadaptable and tend to be emotionally negative andare considered “difficult.”
V. Cognitive developmentA. Toddlerhood is characterized by a transition from
sensorimotor to preoperational thinking.Preoperational thought is marked by the develop-ment of symbolic thinking, as the child becomescapable of forming mental images and begins tosolve problems. Progression from sensorimotor tosymbolic thought occurs typically between 18 and 24months of age.
B. Complete object permanence has developed, andthe child can find an object under a blanket, despitenot seeing it hidden.
C. By 3 years, he can draw primitive figures that repre-sent people, and he develops elaborate play andimagination.
Intellectual Abilities
18 Months
• Pointing to named body parts• Understanding of object permanence• Beginning to understand cause and effect
24 Months
• Forming mental images of objects• Solving problems by trial and error• Understanding simple time concepts
36 Months
• Asking “why” questions• Understanding daily routine• Appreciating special events, such as birthdays• Remembering and reciting nursery rhymes• Repeating three digits
VI. LanguageA. Beginning around age 2 years, toddlers use lan-
guage to convey their thoughts and needs (eg,hunger). The 18-month-old has a vocabulary of atleast 20 words, consisting primarily of the names ofcaregivers, favorite foods, and activities.
B. After 18 months, the toddler begins to put togetherphrases. Early two and three word sentences arereferred to as “telegraphic speech,” and about 50%of what the child says should be intelligible tostrangers.
C. By the age of 3 years, the vocabulary increases toabout 500 words, and 75% of speech is understand-able to strangers. He begins to make completesentences, and frequently asks “why” questions.
Language Skills

18 Months
• Looking selectively at a book• Using 10 to 20 words• Naming and pointing to one picture card• Naming an object (eg, ball)• Following two-directional commands
24 Months
• Using two to three word sentences• Using “I,” “me,” “you”• Naming three picture cards• Naming two objects• Knowing four-directional commands
36 Months
• Using four to five word sentences• Telling stories• Using plurals• Recognizing and naming most common objects
References, see page 182.
Preschooler Development
I. Family relationshipsA. Separation. The average 3-year-old child can
separate easily from parents. Some children cope byadopting a transitional object, usually a soft object,which serves as a symbolic reminder of the parent.
B. Fears and fantasies. Early fantasy, may be indistin-guishable from reality, resulting in a tendency forfears. By the age of 4, children frequently havefrightening dreams that they can state are “not real.”
C. Temper tantrums are characteristic of 2-year-olds,but they should be infrequent by age 5, althoughthere is another peak at 6 years in response to thestresses of schooling.
D. Oppositionality. Preschool children comply withadult requests about 50% of the time. Parents whoare authoritative and firm but also warm, encourag-ing, and rational are more likely to have children whoare self-reliant and self-controlled. A system ofdiscipline should include positive reinforcement fordesired behaviors; consequences for undesiredbehaviors; and interactions that promote the parent-child relationship.
E. Sibling interactions 1. Factors associated with greater sibling rivalry,
include opposite gender, difficult temperament,insecure pattern of attachment, family discord,and corporal punishment. Preschool childrenoften “regress” when a new baby is born, exhibit-ing increased naughtiness, thumb sucking, andaltered toileting.
2. Sibling classes, avoidance of forced interactions,a strong relationship between the older child andthe father, good support for the mother, individualtime with each parent, and talking about the newbaby are helpful.
II. Peer relationshipsA. Play
1. At the age of 2 years, most play is parallel. By theage of 3, children should have mastered aggres-sion and should be able to initiate play with apeer, have joint goals in their play together, andtake turns. Fantasy or pretend play gains promi-nence at about age 3.
2. Pretend friends are very common in children up tothe age of 4. Mastery of aggressive impulsesshould improve after 2 1/2 years of age.

Peer Relationships
2-yearvisit
3-yearvisit
4-yearvisit
5-yearvisit
Amountof inter-action
Parallelplay withpeers,copiesothers,self-talk,solitaryplay, of-fers toy,playsgames
Takes ona role,preferssomefriendsover oth-ers, playsassocia-tively withothers
Interac-tivegames,bestfriend <2y differ-ence,may visitneighborby self,playscoopera-tively withothers
Group offriends
Durationof inter-action
Brieflyalonefromadult,suddenshifts inintensityof activity
20 minwithpeers
Preferspeer playto solitary
Level offantasy
Symbolicdoll, ac-tion fig-ures;mimicsdomesticactivities
Simplefantasyplay; un-familiarmay bemonsters
Elaboratefantasyplay, dis-tinguishes fantasyfrom real-ity, tellsfancifultales
Make-believeand dressup
Imaginaryfriends
May haveone
Common If pres-ent, pri-vate
Favoritetoys/activities
Thingsthatmove,turn, or fittogether;water;books;music;listens tostories
Listens tostories,dressesandundress-es dolls
Sings asong,dances,acts, lis-tens tostories
Rule use Able totaketurns,beginningpropertyrights,“mine,”“rightplaces”
Sharessome
Sharessponta-neously,followsrules insimplegames,facilitywithrules,alter-natelydemand-ing/cooperative
Followsrules ofthegame,followscommu-nity rules
Aggres-sion
Aggres-sive toget things
Negoti-ates con-flicts
Wants topleasefriends
Development of Independence
2-yearvisit
3-yearvisit
4-yearvisit
5-yearvisit
Eating Usesutensils
Spillslittle,pourssome
Helps settable
Helpscook
Dressing Un-dresses,pulls onsimplegarment
Dresseswith su-pervision,unbut-tonssome
Dressesall buttying
Toileting Cleanand dry,but withadult ef-fort andmotiva-tion
Cleanand dryby self-motivatedapproach
Inde-pendent
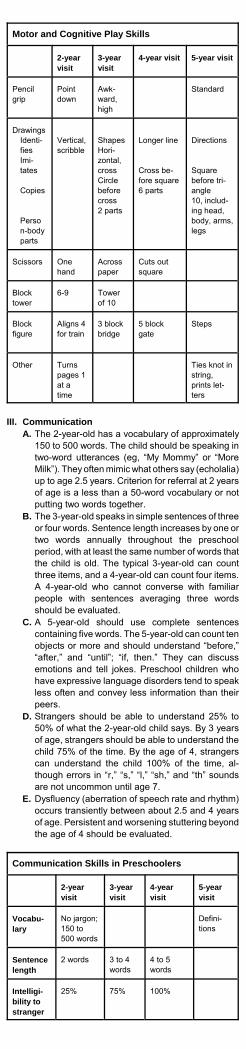
Motor and Cognitive Play Skills
2-yearvisit
3-yearvisit
4-year visit 5-year visit
Pencilgrip
Pointdown
Awk-ward,high
Standard
DrawingsIdenti-fiesImi-tates
Copies
Person-bodyparts
Vertical,scribble
ShapesHori-zontal,crossCirclebeforecross2 parts
Longer line
Cross be-fore square6 parts
Directions
Squarebefore tri-angle10, includ-ing head,body, arms,legs
Scissors Onehand
Across paper
Cuts outsquare
Blocktower
6-9 Towerof 10
Blockfigure
Aligns 4for train
3 blockbridge
5 blockgate
Steps
Other Turnspages 1at atime
Ties knot instring,prints let-ters
III. Communication A. The 2-year-old has a vocabulary of approximately
150 to 500 words. The child should be speaking intwo-word utterances (eg, “My Mommy” or “MoreMilk”). They often mimic what others say (echolalia)up to age 2.5 years. Criterion for referral at 2 yearsof age is a less than a 50-word vocabulary or notputting two words together.
B. The 3-year-old speaks in simple sentences of threeor four words. Sentence length increases by one ortwo words annually throughout the preschoolperiod, with at least the same number of words thatthe child is old. The typical 3-year-old can countthree items, and a 4-year-old can count four items.A 4-year-old who cannot converse with familiarpeople with sentences averaging three wordsshould be evaluated.
C. A 5-year-old should use complete sentencescontaining five words. The 5-year-old can count tenobjects or more and should understand “before,”“after,” and “until”; “if, then.” They can discussemotions and tell jokes. Preschool children whohave expressive language disorders tend to speakless often and convey less information than theirpeers.
D. Strangers should be able to understand 25% to50% of what the 2-year-old child says. By 3 yearsof age, strangers should be able to understand thechild 75% of the time. By the age of 4, strangerscan understand the child 100% of the time, al-though errors in “r,” “s,” “l,” “sh,” and “th” soundsare not uncommon until age 7.
E. Dysfluency (aberration of speech rate and rhythm)occurs transiently between about 2.5 and 4 yearsof age. Persistent and worsening stuttering beyondthe age of 4 should be evaluated.
Communication Skills in Preschoolers
2-yearvisit
3-yearvisit
4-yearvisit
5-yearvisit
Vocabu-lary
No jargon;150 to500 words
Defini-tions
Sentencelength
2 words 3 to 4words
4 to 5words
Intelligi-bility tostranger
25% 75% 100%

2-yearvisit
3-yearvisit
4-yearvisit
5-yearvisit
Grammatic forms
Verbs,some ad-jectivesand ad-verbs
Plurals,pro-nouns
Pasttense
Futuretense
Typicalexamples
Talksabout cur-rent ac-tion, nojargon,namespictures
Tellsownage andsex,countsto 3
Describesrecentexperi-ences,can singsongs,gives firstand lastnames,counts to4, identi-fies gen-der
Counts to10 ormore,recog-nizesletters ofthe al-phabet,knowstele-phonenumberand ad-dress
Fluency Dysfluency common
Dysfluencycom-mon
Somedysfluency
Dysfluencies notexpected
Comprehension
2-yearvisit
3-yearvisit
4-yearvisit
5-yearvisit
Numberstep com-mand
100% for1 withoutgesture
2 3
Numberof bodyparts
Names 1,identifies7
Numberof colors
2named
4 named
Gender Self Self andothers
Ownnames
Refers toself byname
Firstand last
Numberscounted
Says “2"(notcounted)
Countsto 3
10,knowsnumber
Relation-ships
Whichis big-ger,under
Which islonger, 2opposites
Motor development
2-yearvisit
3-yearvisit
4-yearvisit
5-yearvisit
Walksforward
Slightlybent
Swingsarms
Tandemwalks
Walksbackward
10 ft Tandem
Runs Changingdirection
Alter-natingarms
Climbs Out of crib(2.5 y)
Highequip-ment
Jumps Both feetoff floor
26 to 30in frombothfeet
32 in, onefoot leads
Over 10in
Jumpsdown
Step withboth feet
16 in,landson onefoot first
18 in,lands onboth feet
Stairs-up One stepat a time
Withoutrail, al-ternating
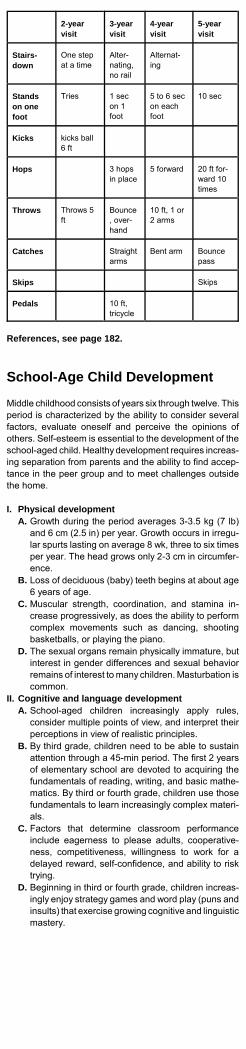
2-yearvisit
3-yearvisit
4-yearvisit
5-yearvisit
Stairs-down
One stepat a time
Alter-nating,no rail
Alternat-ing
Standson onefoot
Tries 1 secon 1foot
5 to 6 secon eachfoot
10 sec
Kicks kicks ball6 ft
Hops 3 hopsin place
5 forward 20 ft for-ward 10times
Throws Throws 5ft
Bounce, over-hand
10 ft, 1 or2 arms
Catches Straightarms
Bent arm Bouncepass
Skips Skips
Pedals 10 ft,tricycle
References, see page 182.
School-Age Child Development
Middle childhood consists of years six through twelve. Thisperiod is characterized by the ability to consider severalfactors, evaluate oneself and perceive the opinions ofothers. Self-esteem is essential to the development of theschool-aged child. Healthy development requires increas-ing separation from parents and the ability to find accep-tance in the peer group and to meet challenges outsidethe home.
I. Physical developmentA. Growth during the period averages 3-3.5 kg (7 lb)
and 6 cm (2.5 in) per year. Growth occurs in irregu-lar spurts lasting on average 8 wk, three to six timesper year. The head grows only 2-3 cm in circumfer-ence.
B. Loss of deciduous (baby) teeth begins at about age6 years of age.
C. Muscular strength, coordination, and stamina in-crease progressively, as does the ability to performcomplex movements such as dancing, shootingbasketballs, or playing the piano.
D. The sexual organs remain physically immature, butinterest in gender differences and sexual behaviorremains of interest to many children. Masturbation iscommon.
II. Cognitive and language developmentA. School-aged children increasingly apply rules,
consider multiple points of view, and interpret theirperceptions in view of realistic principles.
B. By third grade, children need to be able to sustainattention through a 45-min period. The first 2 yearsof elementary school are devoted to acquiring thefundamentals of reading, writing, and basic mathe-matics. By third or fourth grade, children use thosefundamentals to learn increasingly complex materi-als.
C. Factors that determine classroom performanceinclude eagerness to please adults, cooperative-ness, competitiveness, willingness to work for adelayed reward, self-confidence, and ability to risktrying.
D. Beginning in third or fourth grade, children increas-ingly enjoy strategy games and word play (puns andinsults) that exercise growing cognitive and linguisticmastery.

Perceptual, Cognitive, and Language ProcessesRequired for Elementary School Success
Process Description Associated Problems
Perceptual
Visual analy-sis
Ability to break acomplex figureinto componentsand understandtheir spatial rela-tionships
Persistent letter confusion(eg, between b, d, and g);difficulty with basic readingand writing
Proprioception and motorcontrol
Ability to sensebody position byfeel and uncon-sciously programcomplex move-ments
Poor handwriting, requiringexcessive effort
Phonologicprocessing
Ability to perceivedifferences be-tween similarsounding wordsand to breakdown words intosounds
Delayed receptive lan-guage skills; attention andbehavior problems causedby not understanding direc-tion
Cognitive
Long-termmemory
Ability to acquire"automatic" skills
Delayed mastery of thealphabet (reading and writ-ing letters); slow handwrit-ing; inability to progressbeyond basic mathematics
Selectiveattention
Ability to listenand ignore dis-tractions
Difficulty following multistepinstructions, completingassignments, and behavingwell
Sequencing Ability to remem-ber things in or-der; ability to un-derstand time
Difficulty organizing assign-ments, planning, spelling,and telling time
Language
Receptivelanguage
Ability to compre-hend complexconstructions,function words(eg, if, when,only, except),nuances ofspeech, and longblocks of lan-guage (eg, para-graphs)
Difficulty following direc-tions; wandering attention;problems with readingcomprehension; problemswith peer relationships
Expressivelanguage
Ability to recallrequired wordseffortlessly (wordfinding), to con-trol meanings byvarying positionand word end-ings, to constructmeaningful para-graphs and sto-ries
Difficulty expressing feel-ings and using words forself-defense, with resultingfrustration and physicalacting out; struggling dur-ing "circle time" and withlanguage skills.
III. Social and emotional developmentA. School-aged children identify with same-sex par-
ents, adopting them as role models. The parents’moral judgments are internalized as the superego.School-aged children display decreased emotionallability toward parents and an increasing involve-ment in relationships outside of the home.
B. Social and emotional development proceeds inthree contexts: the home, the school, and theneighborhood. The home is the most influential.Milestones of a school child’s increasing independ-ence include the first sleepover at a friend’s houseand the first time at overnight camp.
C. Parents should make demands for effort in schooland extracurricular activities, celebrate successes,and offer unconditional acceptance when failuresoccur. Regular chores provide an opportunity forchildren to contribute to the family, supporting self-esteem. Siblings have critical roles as competitors,loyal supporters, and role models. Sibling relation-ships influence self-image, approach to conflictresolution and interests.
D. The beginning of school coincides with a child’s

further separation from the family and the increas-ing importance of teacher and peer relationships. Inaddition to friendships that may persist for monthsor years, experience with a large number of superfi-cial friendships and antagonisms contributes to achild’s growing social competence. Popularity, animportant part of self-esteem, may be won throughpossessions (having the right toys) as well asthrough personal attractiveness, accomplishments,and social skills.
E. Conformity is rewarded in school-aged children.Some children conform readily and enjoy easysocial success; those who adopt individualisticstyles or have visible differences may be stigma-tized.
F. Dangers such as busy streets, bullies, and strang-ers tax school-aged children’s common sense andresourcefulness. Interactions with peers call onincreasing conflict resolution or pugilistic skills.Children may feel powerlessness in the world, andcompensatory fantasies of being powerful may leadto a fascination with superheroes.
References, see page 182.
Attention-Deficit/Hyperactivity Dis-order
Attention-deficit/hyperactivity disorder (AD/HD) is acondition that appears in early childhood with symptoms ofinattention, hyperactivity, and impulsivity. The symptomsaffect cognitive, academic, behavioral, emotional, andsocial functioning, and persist into adulthood in 70% ofcases. The prevalence of AD/HD between 8 and 10% inschool-aged children. AD/HD occurs two to four timesmore commonly among boys than girls.
I. Clinical features. AD/HD is comprised of three catego-ries of symptoms: hyperactivity, impulsivity, and inatten-tion.A. Core symptoms
1. Hyperactivitya. Hyperactive behavior is identified through
excessive fidgetiness or talking, difficultyremaining seated, difficulty playing quietly, andfrequent restlessness or seeming to be always“on the go.”
b. The hyperactive symptoms typically are ob-served by the time the child reaches fouryears of age and increase during the nextthree to four years. They peak in severitywhen the child is seven to eight years of age,after which they begin to steadily decline. Bythe adolescent years, the hyperactive symp-toms are barely discernible.
2. Impulsivitya. Impulsive behavior, which almost always
occurs in conjunction with hyperactivity inyounger children, is manifested by difficultywaiting turns, blurting out answers, disruptiveclassroom behavior, intruding or interruptingother’s activities, and unintentional injury.
b. The impulsive symptoms typically are ob-served by the time the child is four years ofage and increase during the next three to fouryears to peak in severity when the child isseven to eight years of age. In contrast tohyperactive symptoms, impulsive symptomsusually remain a problem throughout the life ofthe individual.
3. Inattentiona. Inattention may include forgetfulness, being
easily distracted, losing or misplacing things,disorganization, academic underachievement,poor follow-through with assignments or tasks,poor concentration, and poor attention todetail.
b. Inattention typically is not apparent until thechild is eight to nine years of age. Similar tothe pattern of impulsivity, symptoms of inatten-tion usually are a lifelong problem.

B. Diagnostic criteria
DSM-IV Diagnostic Criteria for Attention-Defi-cit/Hyperactivity Disorder
At least six of the following symptoms of inattention orhyperactivity-impulsivity must be evident:
InattentionLack of attention to details or careless mistakes in school-work or other activitiesDifficulty sustaining attention in tasks or play activitiesImpression of not listening when spoken to directlyFailure to follow through on instructions or finish school-work or dutiesDifficulty organizing tasks and activitiesAvoidance or dislike of tasks that require sustained mentaleffort (eg, school
work or homework)Tendency to lose things necessary for tasks or activities(eg, toys, school
assignments, pencils, books)Distractions by extraneous stimuliForgetfulness in daily activities
HyperactivityFidgeting with hands or feet or squirming in seatNot remaining seated when expectedRunning about or climbing excessivelyDifficulty engaging in leisure activities quietlyOften “on the go” or “driven by a motor”Excessive talking
And/Or
ImpulsivityTendency to blurt out answers before questions havebeen completedDifficulty awaiting turnTendency to interrupt or intrude on others (eg, butting intoconversations or
games)
Exclusionary CriteriaA. Some hyperactive-impulsive or inattentive symptoms that
caused impairment must have been present before age 7.B. Some impairment from the symptoms must be present in
two or more settings (eg, at school and at home).C. There must be clear evidence of clinically significant im-
pairment in social, academic or occupational functioning.D. The symptoms do not occur exclusively during the course
of a pervasive developmental disorder, schizophrenia, orother psychotic disorder, and are not better accounted forby another mental disorder.
1. The symptoms must be present in more than onesetting (eg, school and home).
2. The symptoms must persist for at least sixmonths.
3. The symptoms must be present before the age ofseven years.
C. Classification. Three subtypes of AD/HD havebeen identified:
1. The predominantly inattentive type.2. The predominantly hyperactive-impulsive type.3. The combined type.4. Predominantly inattentive. Children with the
predominantly inattentive type of AD/HD (AD/HD-I) usually are diagnosed at 9 to 10 years of age,the age at which symptoms of inattention becomenoticeable.
5. Predominantly hyperactive-impulsive. Childrenwith the predominantly hyperactive-impulsive typeof AD/HD (AD/HD-HI) usually are diagnosed atsix to seven years of age, as symptoms of hyper-activity and impulsivity peak.
6. Combined type of AD/HD (AD/HD-C) usually isdiagnosed at six to seven years of age, as symp-toms of hyperactivity and impulsivity peak.
II. Differential diagnosisA. The symptoms of AD/HD overlap with those of
learning disabilities and behavioral and emotionalproblems, such as depression, anxiety, or posttraumatic stress disorder. These disorders fre-quently coexist with AD/HD.
B. Other conditions to consider in children with symp-toms of inattention, hyperactivity, and impulsivityinclude mental retardation, fragile X syndrome,stressful home environment, inappropriate educa-tional setting, hearing or visual impairment, diabe-tes mellitus, asthma, fetal alcohol syndrome, sleepdisorder, and seizure disorder.

III. Clinical evaluationA. The medical history should include prenatal expo-
sures (eg, drugs, alcohol), perinatal complicationsor infections, central nervous system infection,head trauma, recurrent otitis media, and medica-tions. Family history of similar behaviors is impor-tant because the heritability of AD/HD is 80%.
B. Developmental history should include the onset andcourse of AD/HD symptoms and psychological,medical, and developmental events. Developmentalmilestones, particularly language milestones,school absences, and psychosocial stressors,should be obtained. Parent-child interactionsshould be observed.
C. The examination should include height, weight,head circumference, and vital signs. Dysmorphicand neurocutaneous findings should be noted. Aneurologic examination should be performed. Thechild’s behavior in the office setting should beobserved, although symptoms of AD/HD may notbe apparent in the clinic setting.
D. Family assessment should determine the age ofonset of the symptoms, the duration of symptoms,the settings in which the symptoms occur, and thedegree of functional impairment.
E. School assessment should document the coresymptoms, with an AD/HD-specific behavior check-list and a narrative summary of classroom behaviorand interventions, learning patterns, and functionalimpairment. Copies of report cards and samples ofschool work should be obtained.
F. Rating scales should be completed by parents andteachers for diagnosis, during medication titration,and at regular medication follow-up visits.
G. Comorbid disorders. One-third of children withAD/HD have one or more comorbid conditions,including oppositional defiant disorder, conductdisorder, depression, anxiety disorder, and learningdisabilities.
H. Oppositional defiant disorder (ODD) coexistswith AD/HD in 35% of cases.
I. Conduct disorder coexists with AD/HD in 26% ofcases. DSM-IV criteria for conduct disorder includea repetitive and persistent pattern of behavior inwhich the basic rights of others or major age-appropriate societal norms or rules are violated.
J. Anxiety disorder coexists with AD/HD in 26% ofcases and is more common occurrence in childrenwith the inattentive type of AD/HD.
K. Depression coexists with AD/HD in 18% of casesand occurs more commonly in the inattentive andcombined types.
L. Learning disability coexists with AD/HD rangefrom 20 to 60%.
M. Psychometric testing is not necessary for theroutine diagnosis of AD/HD and does not distin-guish children with and without AD/HD. Nonethe-less, psychometric testing is valuable in narrowingthe differential diagnosis because the core symp-toms of AD/HD can be related to delayed process-ing skills, language disorders, and learning disabili-ties.
IV. Treatment of attention-deficit/hyperactivity disor-der in childrenA. Stimulant medications. Methylphenidate and
dextroamphetamine are the stimulants mostcommonly used to treat AD/HD in children. Thesedrugs have similar efficacy and have mild, usuallyreversible adverse effects.1. Stimulant drugs affect the dopaminergic and
noradrenergic systems, causing the releaseof catecholamines in the central nervoussystem synapses.
2. The response rate for stimulant medication(ie, reduction in hyperactivity or increase inattention is 70 percent. As many as 90 per-cent of children will respond to at least onestimulant.
3. Methylphenidate (Ritalin). Significant reduc-tion in symptoms occurs at doses between0.3 and 0.6 mg/kg. Methylphenidate is avail-able in immediate and sustained releasepreparations.
4. Dextroamphetamine (Dexedrine). Similar tomethylphenidate, both formulations are avail-able in immediate and sustained releasepreparations. The immediate release prepara-

tion of dextroamphetamine-amphetamine hasa duration of as long as six hours.
5. Adverse effects. Many of the side effectsassociated with methylphenidate anddextroamphetamine are mild, of short dura-tion, and reversible with adjustments of dos-ing. Common side effects include anorexia orappetite disturbance (80 percent), sleepdisturbances (3 to 85 percent), and weightloss (10 to 15 percent); less common sideeffects include increased heart rate and bloodpressure, headache, social withdrawal, ner-vousness, and irritability. Deceleration oflinear growth may occur, but adult height isnot affected.
6. Approximately 15 to 30 percent of childrenwho are treated with stimulant medicationsdevelop motor tics, most of which are tran-sient.
Immediate-Release Stimulant Preparations forChildren with Attention-Deficit/HyperactivityDisorder
Medication Initial dos-ing
Dose ad-vancement
Maxi-mumdose
Methylphenidate*MethylphenidateRitalinMethylin (5,10, 20 mgtablets)
5 mg/day x1 day5 mg 2times/day x1 day5 mg 3times/day
Weekly in-crements of5 mg perdose
<25 kg35 mg<25 kg60 mg
Focalin•
(2.5, 5, 10mg tablets)
2.5 mg 2times perday
Weekly in-crements of2.5 to 5 mg
10 mg 2times/day
DextroamphetamineDexedrine(5 mg tab-lets)
Dextrostat(5, 10, mgtablets)
3 to 5years
2.5mg/dayx 1 day.2.5 mg 2times/day
>6 years5 mg x 1day5 mg 2times/day
Weekly in-crements of2.5 mg/dose
Weekly in-crements of5 mg/dose
20 mg
40 mg
Amphetamine-DextroamphetamineAdderall (5,7, 10, 12.5,15, 20, 30mg tablets)
3 to 5years
2.5mg/dayx 1 day2.5 mg 2times/day
>6 years5 mg x 1day5 mg 2times/day
Weekly in-crements of2.5 mg/dose
Weekly in-crements of5 mg/dose
40 mg
*Duration of action: 1 to 4 hours; half-life: 2 to 3 hours•For children >6 years of age
Sustained-release Stimulant Preparations forChildren with Attention-Deficit/HyperactivityDisorder
Medication How sup-plied
Durationof action
Maxi-mumdose
MethylphenidateMethylphenidate SRone-pulsesystem
20 mg tab-lets
8 hours 60 mg
Ritalin-SRone-pulsesystem
20 mg tab-lets
8 hours 60 mg
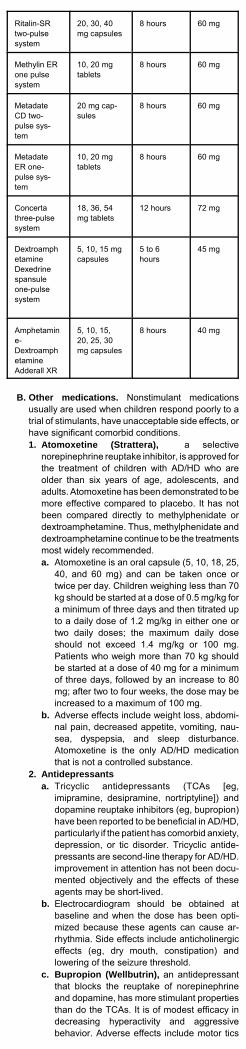
Ritalin-SRtwo-pulsesystem
20, 30, 40mg capsules
8 hours 60 mg
Methylin ERone pulsesystem
10, 20 mgtablets
8 hours 60 mg
MetadateCD two-pulse sys-tem
20 mg cap-sules
8 hours 60 mg
MetadateER one-pulse sys-tem
10, 20 mgtablets
8 hours 60 mg
Concertathree-pulsesystem
18, 36, 54mg tablets
12 hours 72 mg
DextroamphetamineDexedrinespansuleone-pulsesystem
5, 10, 15 mgcapsules
5 to 6hours
45 mg
Amphetamine-DextroamphetamineAdderall XR
5, 10, 15,20, 25, 30mg capsules
8 hours 40 mg
B. Other medications. Nonstimulant medicationsusually are used when children respond poorly to atrial of stimulants, have unacceptable side effects, orhave significant comorbid conditions.1. Atomoxetine (Strattera), a selective
norepinephrine reuptake inhibitor, is approved forthe treatment of children with AD/HD who areolder than six years of age, adolescents, andadults. Atomoxetine has been demonstrated to bemore effective compared to placebo. It has notbeen compared directly to methylphenidate ordextroamphetamine. Thus, methylphenidate anddextroamphetamine continue to be the treatmentsmost widely recommended.a. Atomoxetine is an oral capsule (5, 10, 18, 25,
40, and 60 mg) and can be taken once ortwice per day. Children weighing less than 70kg should be started at a dose of 0.5 mg/kg fora minimum of three days and then titrated upto a daily dose of 1.2 mg/kg in either one ortwo daily doses; the maximum daily doseshould not exceed 1.4 mg/kg or 100 mg.Patients who weigh more than 70 kg shouldbe started at a dose of 40 mg for a minimumof three days, followed by an increase to 80mg; after two to four weeks, the dose may beincreased to a maximum of 100 mg.
b. Adverse effects include weight loss, abdomi-nal pain, decreased appetite, vomiting, nau-sea, dyspepsia, and sleep disturbance.Atomoxetine is the only AD/HD medicationthat is not a controlled substance.
2. Antidepressantsa. Tricyclic antidepressants (TCAs [eg,
imipramine, desipramine, nortriptyline]) anddopamine reuptake inhibitors (eg, bupropion)have been reported to be beneficial in AD/HD,particularly if the patient has comorbid anxiety,depression, or tic disorder. Tricyclic antide-pressants are second-line therapy for AD/HD.improvement in attention has not been docu-mented objectively and the effects of theseagents may be short-lived.
b. Electrocardiogram should be obtained atbaseline and when the dose has been opti-mized because these agents can cause ar-rhythmia. Side effects include anticholinergiceffects (eg, dry mouth, constipation) andlowering of the seizure threshold.
c. Bupropion (Wellbutrin), an antidepressantthat blocks the reuptake of norepinephrineand dopamine, has more stimulant propertiesthan do the TCAs. It is of modest efficacy indecreasing hyperactivity and aggressivebehavior. Adverse effects include motor tics
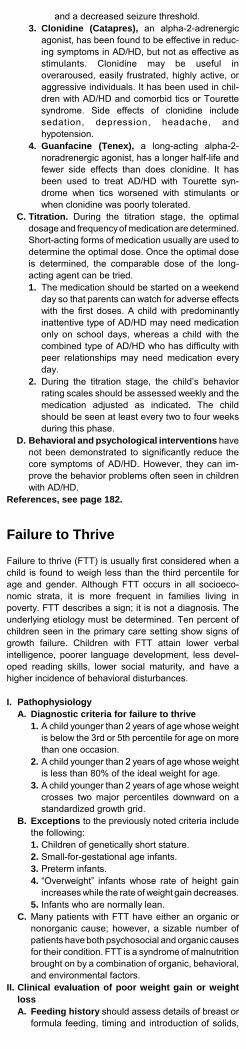
and a decreased seizure threshold.3. Clonidine (Catapres), an alpha-2-adrenergic
agonist, has been found to be effective in reduc-ing symptoms in AD/HD, but not as effective asstimulants. Clonidine may be useful inoveraroused, easily frustrated, highly active, oraggressive individuals. It has been used in chil-dren with AD/HD and comorbid tics or Tourettesyndrome. Side effects of clonidine includesedation, depression, headache, andhypotension.
4. Guanfacine (Tenex), a long-acting alpha-2-noradrenergic agonist, has a longer half-life andfewer side effects than does clonidine. It hasbeen used to treat AD/HD with Tourette syn-drome when tics worsened with stimulants orwhen clonidine was poorly tolerated.
C. Titration. During the titration stage, the optimaldosage and frequency of medication are determined.Short-acting forms of medication usually are used todetermine the optimal dose. Once the optimal doseis determined, the comparable dose of the long-acting agent can be tried.1. The medication should be started on a weekend
day so that parents can watch for adverse effectswith the first doses. A child with predominantlyinattentive type of AD/HD may need medicationonly on school days, whereas a child with thecombined type of AD/HD who has difficulty withpeer relationships may need medication everyday.
2. During the titration stage, the child’s behaviorrating scales should be assessed weekly and themedication adjusted as indicated. The childshould be seen at least every two to four weeksduring this phase.
D. Behavioral and psychological interventions havenot been demonstrated to significantly reduce thecore symptoms of AD/HD. However, they can im-prove the behavior problems often seen in childrenwith AD/HD.
References, see page 182.
Failure to Thrive
Failure to thrive (FTT) is usually first considered when achild is found to weigh less than the third percentile forage and gender. Although FTT occurs in all socioeco-nomic strata, it is more frequent in families living inpoverty. FTT describes a sign; it is not a diagnosis. Theunderlying etiology must be determined. Ten percent ofchildren seen in the primary care setting show signs ofgrowth failure. Children with FTT attain lower verbalintelligence, poorer language development, less devel-oped reading skills, lower social maturity, and have ahigher incidence of behavioral disturbances.
I. PathophysiologyA. Diagnostic criteria for failure to thrive
1. A child younger than 2 years of age whose weightis below the 3rd or 5th percentile for age on morethan one occasion.
2. A child younger than 2 years of age whose weightis less than 80% of the ideal weight for age.
3. A child younger than 2 years of age whose weightcrosses two major percentiles downward on astandardized growth grid.
B. Exceptions to the previously noted criteria includethe following:1. Children of genetically short stature.2. Small-for-gestational age infants.3. Preterm infants.4. “Overweight” infants whose rate of height gain
increases while the rate of weight gain decreases.5. Infants who are normally lean.
C. Many patients with FTT have either an organic ornonorganic cause; however, a sizable number ofpatients have both psychosocial and organic causesfor their condition. FTT is a syndrome of malnutritionbrought on by a combination of organic, behavioral,and environmental factors.
II. Clinical evaluation of poor weight gain or weightlossA. Feeding history should assess details of breast or
formula feeding, timing and introduction of solids,

who feeds the infant, position and placement of theinfant for feeding, and stooling or vomiting patterns.
B. Developmental history should cover gestationaland perinatal history, developmental milestones,infant temperament, and the infant’s daily routine.
C. Psychosocial history should include family compo-sition, employment status, financial status, stress,isolation, child-rearing beliefs, maternal depression,and the caretaker’s own history of possible child-hood abuse or neglect.
D. Family history should include heights, weights,illnesses, and constitutional short stature, inheriteddiseases, or developmental delay.
Causes of Inadequate Caloric Intake
Lack of Appetite! Anemia (eg, iron deficiency)! Psychosocial problems (eg, apathy)! Central nervous system (CNS) pathology (eg, hydro-cephalus, tumor)! Chronic infection (eg, urinary tract infection, acquired
immunodeficiency syndrome)! Gastrointestinal disorder (eg, pain from refluxesophagitis)
Difficulty with Ingestion! Psychosocial problems (eg, apathy, rumination)! Cerebral palsy/CNS disorder (eg, hypertonia, hypotonia)! Craniofacial anomalies (eg, choanal atresia, cleft lip and
palate micrognathia, glossoptosis)! Dyspnea (congenital heart disease, pulmonary disease)! Feeding disorder! Generalized muscle weakness/pathology (eg,myopathies)! Tracheoesophageal fistula ! Genetic syndrome (eg, Smith-Lemli-Opitz-syndrome)! Congenital syndrome (eg, fetal alcohol syndrome)
Unavailability of Food! Inappropriate feeding technique! Inadequate volume of food! Inappropriate food for age ! Withholding of food (abuse, neglect, psychosocial)
Vomiting! CNS pathology (increased intracranial pressure)! Intestinal tract obstruction (eg, pyloric stenosis,malrotation)! Gastroesophageal reflux! Drugs (eg, syrup of ipecac)
III. Physical examinationA. Height, weight, and head circumference should
be plotted on a growth curve. Three measurementsthat are below the 3rd percentile indicate an under-lying organic disease. If all three measurements areconsistently below the third percentile but show thesame rate of increase over a period of time, theinfant probably had intrauterine growth retardation.If the child’s median age for weight is less than themedian age for height, the child may be under-nourished.
B. Dysmorphic features and physical signs ofcentral nervous system, pulmonary, cardiac, orgastrointestinal disorders, or signs of neglect orabuse (poor hygiene, unexplained bruises or scars,or inappropriate behavior) should be sought.
C. Observation of the infant and caretaker. Whilefeeding and playing, the infant may avoid eyecontact or withdraw from physical attention and mayshow a poor suck or swallow, or aversion to oralstimulation. Ineffective feeding technique or inap-propriate response to the infant’s physiologic orsocial cues may be displayed by the caretaker.
D. Diagnostic testing1. Laboratory testing. Tests that will usually
exclude an organic pathology include a completeblood count, urinalysis, urine culture, blood ureanitrogen, creatinine, serum electrolyte levels,and a tuberculin test.
2. Radiologic determination of bone age. If thebone age is normal, it is unlikely that the infanthas a systemic chronic disease or a hormonalabnormality as the cause of poor weight gain.
3. Severe malnutrition requires measurement ofalbumin, alkaline phosphatase, calcium, andphosphorous to assess protein status and tolook for biochemical rickets.
4. Human immunodeficiency virus screening or asweat test may be considered.

E. A feeding evaluation by a nutritionist or an occupa-tional therapist may detect a subtle feeding disor-der.
Causes of Inadequate Calorie Absorption
Malabsorption• Biliary atresia or cirrhosis• Celiac disease• Cystic fibrosis• Enzymatic deficiencies• Food (protein) sensitivity or intolerance• Immunologic deficiency• Inflammatory bowel disease
Diarrhea • Bacterial gastroenteritis• Parasitic infection
Hepatitis
Hirschsprung Disease
Refeeding diarrhea
Causes of Increased Calorie Requirements
Increased Metabolism/Increased Use of Calories• Chronic/recurrent infection (eg, urinary tract infection, tuber-
culosis)• Chronic respiratory insufficiency (eg, chronic lung disease)• Congenital heart disease/acquired heart disease• Malignancy• Chronic anemia• Toxins (lead)• Drugs (eg, excess levothyroxine)• Endocrine disorders (eg, hyperthyroidism,
hyperaldosteronism)
Defective Use of Calories• Metabolic disorders (eg, aminoacidopathies, inborn errors
of carbohydrate metabolism)• Renal tubular acidosis• Chronic hypoxemia (eg, cyanotic heart disease)
IV. Treatment of failure to thriveA. The normal, healthy infant requires an average of
100 kcal/kg of body weight per day. Nutritionalrequirements in children with FTT usually are 150kcal/kg per day.
B. Treatment of infants1. The number of calories per ounce of formula
can be increased by adding less water (13 ozinfant formula concentrate mixed with 10 ozwater provides 24 kcal/oz high-calorie formula)or by adding more carbohydrate in the form ofglucose polymers corn starch or fat in the formof medium-chain triglycerides or corn oil.
2. Once nutritional recovery begins, the infant oftendemands and eats enough food to gain weight.At this point, ad libitum oral feedings are appro-priate.
C. Treatment of older children. Foods can be forti-fied with such items as milk products, margarine,oil, and peanut butter.
References, see page 182.
Speech and Language Development
Language is defined as a symbolic system for the storageand exchange of information. Language consists ofauditory expressive ability (speech), receptive ability(listening comprehension), and visual communication(gestures).
I. Normal speech and language developmentA. Auditory expressive language development
1. In the first 4 to 6 weeks, the earliest soundsconsist of cooing.
2. In the first few months, bilabial sounds begin,consisting of blowing bubbles or the “raspberry.”
3. By 5 months, laughing and monosyllables ap-pear, such as “da,” “ba,” or “ga.”
4. Between 6 and 8 months, infants begin polysyl-labic babbling, consisting of the same syllablerepeated, such as “mamama,” “dadadada.”
5. By 9 months, infants sporadically say “mama” or“dada” without knowing the meaning of these

sounds.6. By 10 months of age, infants use “mama” and
“dada” consistently to label the appropriateparent.
7. By 12 months, infants acquire one or two wordsother than “mama,” or “dada.”
8. During the second year of life, vocabularygrowth velocity accelerates, starting at one newword per week at 12 months of age and increas-ing to one or more new words per day by 24months of age.
9. By 18 to 20 months, a toddler should be using aminimum of 20 words; the 24-month-old shouldhave a vocabulary of at least 50 words.
10. Early during the second year of life toddlersproduce jargon, consisting of strings of differ-ent sounds, with rising and falling, speech-likeinflection. These speech inflection patterns ofare referred to as prosody.
11. By 24 months of age, toddlers are producingtwo-word phrases, such as “want milk!”
12. In the second year of life, pronouns appear(“me” and “you”).
13. Third year. Vocabulary growth velocityreaches a rate of several new words per day.A 30-month-old’s vocabulary should be toolarge for the parent to count (>150 words).
14. By 24 to 30 months, children develop “tele-graphic” speech, which consists of three- tofive-word sentences.
15. By 2 years, the child’s speech should beone-half intelligible; by 3 years, it should bethree-fourths intelligible, and it should becompletely intelligible by age 4 years.
B. Auditory receptive language development1. Newborn infants respond to vocal stimuli by eye
widening or changes in sucking rate.2. The 2- or 3-month-old infant watches and
listens intently to adults and may vocalize back.3. By 4 months of age the normal infant will turn
his head to locate the source of a voice; turningto inanimate stimuli, such as a bell, occurs 1month later.
4. By 7 to 9 months of age, an infant will attendselectively to his own name.
5. By 9 months of age, infants comprehend theword “no.”
6. By 1 year of age, infants respond to one-stepcommands such as “Give it to me.”
7. By 2 years of age, toddlers can follow noveltwo-step commands. (eg, “Put away your shoes,then go sit down”).
8. By 2 years, children will point to objects oncommand and name simple objects on com-mand.
9. By 36 months, a child’s receptive vocabularyincludes 800 words, expanding to 1500-2000words by age 5.
10. By 5 years, children are able to follow three-and four-step commands.
C. Visual language development1. During the first few weeks, the infant will dis-
play alert visual fixation. 2. By 4 to 6 weeks, a social smile appears.3. By age 4 to 5 months, the infant will turn to-
wards a voice.4. By 6 to 7 months, infants play gesture games,
such as patty cake and peek-a-boo.5. Between 8 and 9 months, infants reciprocate
and eventually initiate gesture games.6. By 9 months, infants appropriately wave bye-bye
on command. 7. Between 9 and 12 months, infants express their
desire for an object by reaching and crying.8. By 12 months, infants indicate desired objects
by pointing with the index finger.II. Classification of speech and language disorders
A. Hearing loss1. One infant per thousand is born with bilateral,
severe-to-profound hearing loss. Two childrenper thousand are deafened during the first 3years of life.
2. One-third of congenital deafness is genetic inorigin, one-third is nongenetic, and one-third is ofunknown etiology. The most common nongeneticcause of deafness is fetal CMV infection.
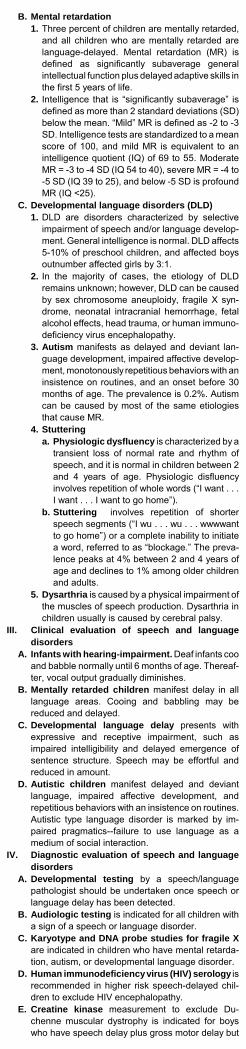
B. Mental retardation1. Three percent of children are mentally retarded,
and all children who are mentally retarded arelanguage-delayed. Mental retardation (MR) isdefined as significantly subaverage generalintellectual function plus delayed adaptive skills inthe first 5 years of life.
2. Intelligence that is “significantly subaverage” isdefined as more than 2 standard deviations (SD)below the mean. “Mild” MR is defined as -2 to -3SD. Intelligence tests are standardized to a meanscore of 100, and mild MR is equivalent to anintelligence quotient (IQ) of 69 to 55. ModerateMR = -3 to -4 SD (IQ 54 to 40), severe MR = -4 to-5 SD (IQ 39 to 25), and below -5 SD is profoundMR (IQ <25).
C. Developmental language disorders (DLD)1. DLD are disorders characterized by selective
impairment of speech and/or language develop-ment. General intelligence is normal. DLD affects5-10% of preschool children, and affected boysoutnumber affected girls by 3:1.
2. In the majority of cases, the etiology of DLDremains unknown; however, DLD can be causedby sex chromosome aneuploidy, fragile X syn-drome, neonatal intracranial hemorrhage, fetalalcohol effects, head trauma, or human immuno-deficiency virus encephalopathy.
3. Autism manifests as delayed and deviant lan-guage development, impaired affective develop-ment, monotonously repetitious behaviors with aninsistence on routines, and an onset before 30months of age. The prevalence is 0.2%. Autismcan be caused by most of the same etiologiesthat cause MR.
4. Stutteringa. Physiologic dysfluency is characterized by a
transient loss of normal rate and rhythm ofspeech, and it is normal in children between 2and 4 years of age. Physiologic disfluencyinvolves repetition of whole words (“I want . . .I want . . . I want to go home”).
b. Stuttering involves repetition of shorterspeech segments (“I wu . . . wu . . . wwwwantto go home”) or a complete inability to initiatea word, referred to as “blockage.” The preva-lence peaks at 4% between 2 and 4 years ofage and declines to 1% among older childrenand adults.
5. Dysarthria is caused by a physical impairment ofthe muscles of speech production. Dysarthria inchildren usually is caused by cerebral palsy.
III. Clinical evaluation of speech and languagedisorders
A. Infants with hearing-impairment. Deaf infants cooand babble normally until 6 months of age. Thereaf-ter, vocal output gradually diminishes.
B. Mentally retarded children manifest delay in alllanguage areas. Cooing and babbling may bereduced and delayed.
C. Developmental language delay presents withexpressive and receptive impairment, such asimpaired intelligibility and delayed emergence ofsentence structure. Speech may be effortful andreduced in amount.
D. Autistic children manifest delayed and deviantlanguage, impaired affective development, andrepetitious behaviors with an insistence on routines.Autistic type language disorder is marked by im-paired pragmatics--failure to use language as amedium of social interaction.
IV. Diagnostic evaluation of speech and languagedisorders
A. Developmental testing by a speech/languagepathologist should be undertaken once speech orlanguage delay has been detected.
B. Audiologic testing is indicated for all children witha sign of a speech or language disorder.
C. Karyotype and DNA probe studies for fragile Xare indicated in children who have mental retarda-tion, autism, or developmental language disorder.
D. Human immunodeficiency virus (HIV) serology isrecommended in higher risk speech-delayed chil-dren to exclude HIV encephalopathy.
E. Creatine kinase measurement to exclude Du-chenne muscular dystrophy is indicated for boyswho have speech delay plus gross motor delay but

who do not have increased deep tendon reflexes.F. Cranial MRI is indicated in the presence of focal
neurologic abnormalities or dysmorphic featuressuggestive of a structural brain abnormality (eg,hypertelorism, midfacial hypoplasia, aberrant hairpatterning).
V. Management of speech and language disorders.The child who has DLD should be referred for speechtherapy. Stuttering requires referral to a speech pathol-ogist. Hearing loss is treated with amplification. Therapyfor autism is directed at enhancing communication andsocial skills.
References, see page 182.

Cardiac Disorders
Heart Murmurs
Ninety percent of children will have an audible heartmurmur at some point in time. Normal murmurs includevibratory and pulmonary flow murmurs, venous hums,carotid bruits, and the murmur of physiologic branchpulmonary artery stenosis. Less than 5% of heart murmursin children are caused by cardiac pathology.
I. Clinical evaluation of heart murmursA. Cyanosis, exercise intolerance, feeding difficulties,
dyspnea, or syncope signify potential cardiac dys-function. Failure to thrive, diffuse diaphoresis,unexplained persistent irritability or lethargy, andatypical chest pain also suggest the possibility oforganic heart disease.
B. The majority of children who have heart murmursare asymptomatic. In early infancy, however, cardiacmalformations may manifest as persistent peacefultachypnea (a respiratory rate greater than 60breaths/min).
C.Family history of a congenital cardiovascularmalformation increases the risk of a cardiac defect,such as with DiGeorge syndrome (type B interruptedaortic arch, truncus arteriosus).
D. Gestational course should be reviewed for expo-sure to teratogens or maternal illnesses. Fetalexposure to lithium may cause Ebstein anomaly ofthe tricuspid valve. Ventricular and atrial septaldefects occur with fetal alcohol syndrome. Transienthypertrophic cardiomyopathy and tetralogy of Fallotare associated with maternal diabetes. Maternalcollagen vascular disease may lead to fetal com-plete heart block.
II. Physical examinationA. Noncardiac malformations. Twenty-five percent of
children who have heart disease have extracardiacanomalies. Diaphragmatic hernia, tracheoesoph-ageal fistula and esophageal atresia, omphalocele,or imperforate anus are associated with congenitalcardiac defects in 15-25% of infants.
B. Cyanotic infants or children, abnormal rate orpattern of breathing, a persistently hyperdynamicprecordium, precordial bulging, or asymmetricpulses should be referred to a cardiologist. Signs ofcongestive heart failure (inappropriate tachycardia,tachypnea, hepatomegaly, abnormal pulse volume)also should prompt referral to a cardiologist.
C. Auscultatory criteria signifying cardiac disease1. Loud, pansystolic, late systolic, diastolic, or
continuous murmurs; an abnormally loud orsingle second heart sound
2. Fourth heart sound or S4 gallop3. Ejection or midsystolic clicks
D. Ventricular septal defect (VSD) is a harshpansystolic murmur of even amplitude that isaudible at the lower left sternal border.
E. Patent ductus arteriosus (PDA) causes a murmurthat is continuous, louder in systole, and located atthe upper left sternal border.
F. Ejection (crescendo-decrescendo) murmurs arecaused by ventricular outflow obstruction. Ejectionmurmurs begin after the first heart sound.
Characteristics of Organic Murmurs
Lesion Shape Timing Loca-tion
OtherFindings
Ventricularseptal de-fect
Plateau Holosystolic
LLSB Apical mid-diastolicmurmur
Mitral re-gurgitation
Plateau Holosystolic
Apex Higherpitchedthan VSDmurmur
Atrialseptal de-fect
Ejection Systolic ULSB PersistentS2 split

Lesion Shape Timing Loca-tion
OtherFindings
Patentductusarteriosus
Dia-mond
Continu-ous
ULSB Boundingpulses
Aortic valvestenosis
Ejection Systolic URSB Ejectionclick
Subvalvular aortic ste-nosis
Ejection Systolic ML-URSB
No ejectionclick
Hypertro-phiccardiomyo-pathy
Ejection Systolic LLSB-apex
LaterallydisplacedPMI
Coarctation Ejection Systolic ULSB-Leftback
Pulse dis-parity
Pulmonaryvalve ste-nosis
Ejection Systolic ULSB Ejectionclick; wideS2 split
Tetralogyof Fallot
Ejection Systolic MLSB Cyanosis
LLSB = lower left sternal border, ULSB = upper left sternal border, URSB =upper right sternal border, MLSB = mid-left sternal border, S2 = secondheart sound, PMI = point of maximal impulse.
III. Differentiation of normal from pathologic murmursA. Criteria for diagnosis of a normal heart murmur
1. Asymptomatic patient.2. No evidence of associated cardiac abnormali-
ties, extracardiac congenital malformations, orsyndromes.
3. Auscultatory features are characteristic of aninnocent murmur.
Normal Murmurs
Type Shape Timing Pitch Loca-tion
OtherFind-ings
Vibra-tory
Ejec-tion
Midsystolic
Low LLSB-apex
Inten-sity<gradeII
Venoushum
Dia-mond
Contin-uous
Me-dium
Subclavicular
Disap-pearsin su-pineposition
Pulmo-naryflow
Flow Sys-tolic
Me-dium
ULSB NormalS2 split
Physio-logicbranchpulmo-naryarterysteno-sis
Ejec-tion
Sys-tolic
Me-dium
Entirechest
Disap-pearsby 4 to6monthsof age
LLSB = lower left sternal border, ULSB = upper left sternalborder, S2 = second heart sound.
IV. Heart murmurs in the newborn infantA. Sixty percent of healthy term newborn infants have
normal heart murmurs. One-third of neonates whohave serious heart malformations may not have adetectable heart murmur during the first 2 weeks oflife. Thirty percent of newborn infants subsequentlydetermined to have heart disease are dischargedfrom the newborn nursery as ostensibly healthy.
B. Persistent peaceful tachypnea should not bedismissed; 90% of infants who have serious car-diac disease have persistent tachypnea after birth.
C. A persistently hyperdynamic precordium sug-gests organic heart disease.
D. Auscultation of the second heart sound. Inhealthy neonates, the second heart sound is splitaudibly by 12 hours of age. A single second heartsound in a quiet neonate indicates: 1) the absence

of one outflow tract valve (aortic or pulmonaryatresia); 2) an abnormal position of the greatvessels (transposition of the great arteries ortetralogy of Fallot); or 3) pulmonary hypertension(ventricular defect, persistent pulmonary hyperten-sion).
References, see page 182.
Chest Pain in Children
Chest pain is the presenting complaint in 6 per 1,000children who present to pediatric clinics. Young childrenare more likely to have a cardiorespiratory cause of theirpain, such as cough, asthma, pneumonia, or heart dis-ease; adolescents are more likely to have pain associatedwith a psychogenic disturbance.
I. Differential diagnosis of chest pain in childrenA. Cardiac disease
1. Cardiac disease is a rare cause of chest pain inchildren. However, myocardial infarction canrarely result from anomalous coronary arteries.Some children will have a pansystolic, continuousor mitral regurgitation murmur or gallop rhythmthat suggests myocardial dysfunction.
2. Arrhythmias may cause palpitations or abnormali-ties on cardiac examination. Supraventriculartachycardia is the most common arrhythmia, butpremature ventricular beats or tachycardia alsocan cause episodes of brief sharp chest pain.
3. Hypertrophic obstructive cardiomyopathy isan autosomal dominant structural disorder;therefore, there often is a family history of thecondition. Children may have a murmur that maybe audible when standing or when performing aValsalva maneuver.
4. Mitral valve prolapse may cause chest painsecondary to papillary muscle or endocardialischemia. A midsystolic click and a late systolicmurmur may be detected.
5. Cardiac infections are uncommon causes ofpediatric chest pain.a. Pericarditis presents with sharp, stabbing
pain that improves when the patient sits upand leans forward. The child usually is febrile;is in respiratory distress; and has a friction rub,distant heart sounds, neck vein distention, andpulsus paradoxus.
b. Myocarditis presents as mild pain that hasbeen present for several days. After a fewdays of fever, vomiting and lightheadedness,the patient may develop pain or shortness ofbreath on exertion. Examination may revealmuffled heart sounds, fever, a gallop rhythm,or tachycardia.
c. Chest radiography will show cardiomegaly inboth of these infections, and the electrocardio-gram will be abnormal. An echocardiogram willconfirm the diagnosis.
B. Musculoskeletal pain1. Musculoskeletal pain is one of the most common
diagnoses in children who have chest discom-fort. Children frequently strain chest wall muscleswhile exercising.
2. Trauma to the chest may result in a mild contu-sion or a rib fracture. The physical examinationwill reveal chest tenderness.
3. Costochondritis is common in children, and it ischaracterized by tenderness over thecostochondral junctions. The pain is sharp andexaggerated by physical activity or breathing.
C. Respiratory conditions1. Severe cough, asthma, or pneumonia may
cause chest pain because of overuse of chestwall muscles. Crackles, wheezes, tachypnea, ordecreased breath sounds are present.
2. Exercise-induced asthma may cause chestpain, which can be confirmed with a treadmilltest.
3. S p o n t a n e o u s p n e u m o t h o r a x o rpneumomediastinum may occasionally causechest pain with respiratory distress. Children withasthma, cystic fibrosis or Marfan syndrome areat high risk. Signs include respiratory distress,decreased breath sounds on the affected side,

and palpable subcutaneous air.4. Pulmonary embolism is extremely rare in
pediatric patients, but it should be considered inthe adolescent girl who has dyspnea, fever,pleuritic pain, cough, and hemoptysis. Oralcontraceptives or recent abortion increase therisk. Young males who have had recent legtrauma also are at risk.
D. Psychogenic chest pain may present with hyper-ventilation or an anxious appearance. A recentstressful event (separation from friends, parentaldivorce, school failure) may often be related tempo-rally to the onset of the chest pain.
E. Gastrointestinal disorders1. Reflux esophagitis often causes chest pain,
which is described as burning, substernal, andworsened by reclining or eating spicy foods. Thiscondition is confirmed with a therapeutic trial ofantacids.
2. Foreign body ingestion may cause chest painwhen the object lodges in the esophagus. Aradiograph confirms the diagnosis.
F. Miscellaneous causes of pediatric chest pain1. Sickle cell disease may cause an acute chest
syndrome.2. Marfan syndrome may cause chest pain and
fatal abdominal aortic aneurysm dissection.3. Collagen vascular disorders may cause chest
pain and pleural effusions.4. Shingles may cause chest pain that precedes or
occurs simultaneously with the rash.5. Coxsackievirus infection may lead to
pleurodynia with paroxysms of sharp chest pain.6. Breast tenderness during puberty or early
breast changes of pregnancy may present aschest pain.
7. Idiopathic chest pain. No diagnosis can bedetermined in 20-45% of cases of pediatric chestpain.
II. Clinical evaluation of chest painA. A history and physical examination will reveal the
etiology of chest pain in most cases. The historymay reveal asthma, previous heart disease, orKawasaki disease. Family history may revealfamilial hypertrophic obstructive cardiomyopathy.
B. The frequency and severity of the pain andwhether the pain interrupts the child’s daily activityshould be determined. Pain that wakes the childfrom sleep is more likely to be related to an organicetiology.
C. Burning pain in the sternal area suggestsesophagitis. Sharp stabbing pain that is relieved bysitting up and leaning forward suggests pericarditisin a febrile child.
D. Mode of onset of pain. Acute onset of pain is morelikely to represent an organic etiology. Chronic painis much more likely to have a idiopathic or psycho-genic origin.
E. Precipitating factors1. Trauma, muscle strain or choking on a for-
eign body should be sought.2. Exercise-induced chest pain may be caused
by cardiac disease or exercise-induced asthma.3. Syncope, fever or palpitations associated with
chest pain are signs of an organic etiology.4. Joint pain, rash or fever may be suggested by
the presence of collagen vascular disease. 5. Stressful conditions at home or school should
be sought.6. Substance abuse (cocaine) or oral contracep-
tives should be sought in adolescents.F. Physical examination
1. Severe distress warrants immediate treatmentfor life-threatening conditions, such aspneumothorax.
2. Hyperventilation may be distinguished fromrespiratory distress by the absence of cyanosisor nasal flaring.
3. Pallor or poor growth may suggest a malig-nancy or collagen vascular disease.
4. Abdominal tenderness may suggest abdominalpain that is referred to the chest.
5. Rales, wheezes, decreased breath sounds,murmurs, rubs, muffled heart sounds orarrhythmias suggest a cardiopulmonary pathol-ogy.

6. The chest wall should be evaluated for bruises(trauma), tenderness (musculoskeletal pain), orsubcutaneous air (pneumothorax orpneumomediastinum).
III. Laboratory evaluationA. A chest radiograph is warranted if the patient has
fever, respiratory distress, or abnormal breathsounds. Fever and cardiomegaly suggestspericarditis or myocarditis.
B. Electrocardiography is recommended if the painwas acute in onset (began in the last 2-3 days) or ifthere is an abnormal cardiac examination (unex-plained tachycardia, arrhythmia, murmur, rub, orclick).
C. Exercise stress testing or pulmonary functiontesting is appropriate for evaluation of cardiacdisease or asthma.
D. Holter monitoring is warranted for syncope orpalpitations.
E. Children with chronic pain, a normal physicalexamination, and no history suggestive of cardiacor pulmonary disease do not require laboratorystudies.
F. Blood counts and sedimentation rates are ofvalue if collagen vascular disease, infection, ormalignancy is suspected.
G. Drug screening may be indicated in the older childwho has acute pain associated with anxiety,tachycardia, hypertension, or shortness of breath.
IV. Management of pediatric chest painA. Emergency department referral is necessary if
the child is in severe distress or has a history ofsignificant trauma.
B. Referral to a cardiologist is recommended forchildren with known or suspected heart disease,syncope, palpitations, or pain on exertion.
C. Musculoskeletal, psychogenic or idiopathic painusually will respond to reassurance, analgesics,rest, and application of a heating pad. If esophagitisis suspected, a trial of antacids may be beneficial.
References, see page 182.
Allergic and DermatologicDisordersAsthma
Asthma is a chronic inflammatory disorder of the airways,causing recurrent episodes of wheezing, breathlessness,chest tightness, and cough.
I. HistoryA. The classic triad of symptoms associated with
asthma consists of cough, shortness of breath, andwheezing. Postnasal drip syndrome can also lead tosymptoms that include cough, wheezing, dyspnea,and/or expectoration of phlegm.
B. There is a parental history of asthma in 50 percentof children with asthma.
Diagnosis of Asthma
Asthma di-agnosis
Days withsymptoms*
Nights withsymptoms
PEF (% per-sonal best)or FEV2 (%predictedbest)
Step 4: se-vere persis-tent
Continual Frequent <60
Step 3: mod-erate persis-tent
Daily >5 times permonth
>60 to <80
Step 2: mildpersistent
>2 times perweek
3 to 4 timesper month
>80
Step 1: mildintermittent
>2 times perweek
<2 permonth
>80
II. Physical examinationA. Widespread, high-pitched, musical wheezes are
characteristic of asthma, although they are notspecific. The presence or absence of wheezing onphysical examination is a poor predictor of theseverity of airflow obstruction in asthma. Wheezingmay be heard in patients with mild, moderate, orsevere airway narrowing; significant airway narrow-ing also may be present without wheezing.
B. Physical findings that suggest severe airflow ob-struction in asthma, including use of the accessory(eg, sternocleidomastoid) muscles of breathing anda pulsus paradoxus.
III. Laboratory testingA. Spirometry, which includes measurement of forced
expiratory volume in one second (FEV1) and forcedvital capacity (FVC), is a useful pulmonary functiontest.1. The FEV1 is the most important spirometric
variable for assessment of airflow obstruction.The FEV1 reflects the average flow rate duringthe first second of forced vital capacity (FVC). Itdeclines in direct and linear proportion withclinical worsening of airways obstruction, and itincreases with successful treatment of airwaysobstruction. The FEV1 can be used for determin-ing the degree of obstruction (mild, moderate, orsevere).
2. Administration of a bronchodilator (eg, Albuterol)by metered-dose inhaler (MDI) is indicatedduring an initial work-up if baseline spirometry.
B. Chest radiograph is almost always normal inpatients with asthma. Its potential value is to detectrare complications and to exclude alternative diag-noses.
C. Tests for allergy1. Allergy skin testing involves prick skin tests.
Drops of antigen-containing solution are placedin parallel rows on each forearm using a panel ofup to 30 different allergens.
2. RAST involves blood measurement of the min-ute quantities of IgE antibody directed at particu-lar antigens. Various panels of antibodies can beordered.
IV. Differential diagnosisA. In children, considerations include foreign body
aspiration, cystic fibrosis, and viral bronchiolitis.

B. In young and middle-aged adults considerationsinclude bronchiectasis, pulmonary embolism,gastroesophageal reflux disease (GERD), andsarcoidosis.
C. In older patients, especially cigarette smokers,considerations include COPD and heart failure.
D. When persistent cough is the presenting complaintand the chest radiograph and lung function arenormal, the differential includes post-nasal drip,GERD, post-viral tussive syndrome, and coughinduced by angiotensin converting enzyme inhibi-tors. With the exception of aspiration, diffuse musi-cal expiratory wheezing is not found in any of theseother causes of persistent cough.
E. Some illnesses are common comorbidities withasthma, including seasonal allergic rhinitis andconjunctivitis (“hay fever”), perennial rhinitis, recur-rent or chronic sinusitis, and post-nasal drip associ-ated with rhinitis or sinusitis.
V. Management of asthmaA. Monitoring. Regular monitoring of the peak
expiratory flow rate (PEFR) should be encouragedin patients with moderate-to-severe asthma. PEFRmeasurement can be used to follow the impact ofany relevant change in therapy upon lung functionand to assess the severity of acute asthmaticexacerbations.
B. Controlling trigger factors. Identifying andavoiding asthma "triggers" are essential in pre-venting asthma flare-ups. Common asthma trig-gers generally fall into the following six categories:allergens; respiratory infections; irritants; chemi-cals; physical activity; and emotional stress. An-nual influenza vaccination is recommended forpatients with asthma.
C. Pharmacologic treatment of intermittentasthma. Patients with mild intermittent asthma aredefined as those who have:1. Symptoms of asthma occurring two or fewer
times per week.2. Two or fewer nocturnal awakenings per month.3. Peak-flow measurements when asymptomatic
that are within the normal range (ie, PEFR >80percent of predicted normal).
4. Short-acting inhaled beta-agonists. Patientswith mild intermittent asthma are best treatedwith an intermittent inhaled beta-2-selectiveadrenergic-agonist. Patients for whom trigger-ing of asthmatic symptoms can be predicted(eg, exercise-induced bronchoconstriction) areencouraged to use their inhaled beta-agonist 10minutes prior to exposure. Inhaled beta-agonists with rapid onset of action, intermediateduration of effect (four to six hours), and beta-2selectivity are recommended.
5. Mast cell stabilizing agents. Mast cell stabiliz-ing agents such as cromolyn (Intal) andnedocromil (Tilade) are alternative medicationsfor prevention of exercise-inducedbronchoconstriction. These medications provideadditive protection when used in combinationwith a beta-agonist. Cromolyn and nedocromilare effective when taken prior to an exposurebut have no ability to relieve asthmatic symp-toms once they have developed.

Stepwise Approach for Managing Asthma
Asthma
Quick relief Long-termcontrol
Medication
Step4:se-vere,persistent
Short-actingbronchodilator as needed:
• Inhaledshort-actingbeta2 agonistor
• Oral beta2
agonist
Dailyanti-inflam-matory medi-cations:• High-dose
inhaledcorticosteroidand
• If needed,add sys-temiccorticoster-oids (0.25to 2 mg perkg per day)and reduceto lowestdosage.
Oralcorticosteroids:Methylprednisone (Medrol),2-mg tablet Prednisolone (Prelone syrup),5 mg per 5 mL (Pediapred liq-uid), 5 mg per 5mL. Prednisone5-mg tablet(Deltasone),5-mg tab(Intensol), 5mg/mL liquid
Step3:mod-erate,per-sistent
Short-actingbronchodilator as needed:• Inhaled
short-actingbeta2 agonistby nebulizeror spacerand facemaskor
• Oral beta2
agonist
Dailyanti-inflam-matory medi-cations, ei-ther: • High-dose
inhaledcorticosteroidor, oncecontrol isestablished
• Low- tomedium-dose in-haled corti-costeroidandlong-actingbronch-odilator (eg,long-actinginhaledbeta2 ago-nist ortheophyllineSR)
Short-actingbeta2 agonistAlbuterol (Airetnebulizer), 2.5mg in 3 mL q4-6h PRN(Proventil-HFAMDI) 2 puffs q4-6h PRN(VentolinRotacaps DPI),1-2 caps q4-6hPRNLong-actingbeta2 agonistSalmeterol(Serevent MDI,SereventDiskus DPI) 2puffs q12h; 1inhalation q12hAlbuterol SR(Volmax tablet,Proventil Repe-tabs) 4-8 mg bidSalmeterol/Fluticasone (AdvairDiskus) 100 μg/50 μg 250 μg/50 μg 500 μg/50 μg1 puff q12h

Stepwise Approach for Managing Asthma
Asthma
Quick relief Long-termcontrol
Medication
Step2:mild,persistent
Short-actingbronch-odilator asneeded: • Inhaled
short-actingbeta2 agonistor
• Oral beta2
agonist
Dailyanti-inflam-matory medi-cations
Inhaledcorticosteroids• Beclomethaso
ne (BecloventMDI) 4-8 puffsbid (VancerilDS MDI) 2-4puffs bid
• Budesonide(PulmicortTurbuhalerDPI)1-2 inha-lations bid.PulmicortRespules,0.25 mg, 0.5mg. 1-2 bid.
• Flunisolide(AeroBid MDI)2-4 puffs bid
• Fluticasone(Flovent), 2-4puffs bid(FloventRotadisk) 1bid.
• Triamcinolone(AzmacortMDI) 4 puffsbid.
Theophylline200 mg, 300mg (SR), 450mg (TR). 100-300 mg bid
Antileukotrienes • Zafirlukast
(Accolate),10-mg tablet, 20 mg bid
• Montelukast(Singulair), 4-or 5-mgchewable tab,10 mg qhs
• Zileuton (ZyfloFlimtab),600-mg tab,600 mg qid
• Cromolyn (In-tal) inhaler, 2-4 puffs tid-qid
• Nedocromil(Tilade) in-haler, 2-4puffs bid-qid
Step1:mild,intermittent
Short-actingbronchodilator as needed<2 times perweek: • Inhaled,
short-actingbeta2 agonistor
• Oral beta2
agonist
No daily medi-cation
Short-actingbeta2 agonistAlbuterol (Airetnebulizer), 2.5mg in 3 mL q4-6h PRN(Proventil-HFAMDI) 2 puffs q4-6h PRN(VentolinRotacaps DPI),1-2 caps q4-6hPRN
Drugs for Asthma
Drug Formulation Dosage
Inhaled beta2-adrenergic agonists, short-acting
AlbuterolProventilProventil-HFAVentolinVentolinRotacaps
metered-doseinhaler (90μg/puff)
dry-powder in-haler (200μg/inhalation)
2 puffs q4-6hPRN
1-2 capsules q4-6h PRN
AlbuterolProventil
multi-dose vialsVentolin NebulesVentolin
nebulized 2.5 mg q4-6hPRN

Drug Formulation Dosage
Levalbuterol -Xopenex
nebulized 0.63-1.25 mg q6-8h PRN
Inhaled beta2-adrenergic agonist, long-acting
Formoterol -Foradil
dry-powder in-haler (12 μg/puff)
1 puff bid.
SalmeterolSereventSerevent Diskus
metered-doseinhaler (21μg/puff)dry-powder in-haler (50μg/inhalation)
2 puffs q12h
1 inhalation q12h
Fluticasone/Salmeterol AdvairDiskus
dry-powder in-haler (100, 250 or500 μg/puff)
1 puff q12h
Inhaled Corticosteroids
BeclomethasonedipropionateBecloventVancerilVanceril Double-Strength
metered-doseinhaler (42μg/puff) (84μg/puff)
4-8 puffs bid
2-4 puffs bid
BudesonidePulmicortTurbuhaler
dry-powder in-haler (200μg/inhalation)
1-2 inhalationsbid
Flunisolide -AeroBid
metered-dosein-haler
(250 μg/puff)
2-4 puffs bid
FluticasoneFlovent
Flovent Rotadisk
metered-doseinhaler(44, 110 or 220μg/puff)dry-powder in-haler (50, 100 or250 μg/inhalation)
2-4 puffs bid(44 μg/puff)1 inhalation bid(100μg/inhalation)
TriamcinoloneacetonideAzmacort
metered-doseinhaler (100μg/puff)
2 puffs tid-qid or4 puffs bid
Leukotriene Modifiers
Montelukast -Singulair
tablets 10 mg qhs
Zafirlukast -Accolate
tablets 20 mg bid
Zileuton - Zyflo tablets 600 mg qid
Mast Cell Stabilizers
CromolynIntal
metered-doseinhaler (800μg/puff)
2-4 puffs tid-qid
NedocromilTilade
metered-doseinhaler (1.75mg/puff)
2-4 puffs bid-qid
Phosphodiesterase Inhibitor
Theophylline Slo-BidGyrocaps, Theo-Dur, Unidur
extended-releasecapsules or tab-lets
100-300 mg bid
D. Treatment of mild persistent asthma1. It is appropriate to begin regular treatment with
anti-inflammatory medications when a patient hasone of the following:
a. Asthmatic symptoms requiring relief with aninhaled bronchodilator more than once perweek.
b. Nocturnal awakenings as often as once everytwo weeks.
c. Observed fluctuations in PEFR of more than 20percent.
2. Inhaled corticosteroids. For adults, the mostfrequently recommended choice of anti-inflamma-tory therapy is an inhaled corticosteroid. Inhaledcorticosteroids are administered twice daily.
a. Use of a spacer device (eg, Aerochamber,Optichamber, Ellipse, or InspirEase) with theinhaled corticosteroids is recommended. Thetriamcinolone acetonide MDI is manufactured

with an attached spacer. The budesonideTurbuhaler is not appropriate for use with aspacer.
b. Oral candidiasis (thrush) is the most commonside effect from the use of inhaledcorticosteroids. This complication is infrequentwhen inhaled corticosteroids are administeredwith spacers and when patients rinse theirmouths with water immediately after use. Hoarsevoice and sore throat are less common sideeffects.
c. Long-term use of inhaled corticosteroids in thedoses recommended for mild asthma is gener-ally well tolerated. Adverse effects related to theeye and to skeletal metabolism are some of themore serious potential consequences of inhaledcorticosteroid use. Suppression of thehypothalamic-pituitary-adrenal axis can alsooccur.
d. Patients receiving regular anti-inflammatorytherapy should continue to use their inhaledbronchodilator as needed for relief of symptomsand prior to exposure to known triggers of theirsymptoms.
3. Leukotriene-modifying agents. Leukotrienes(leukotriene C4, D4 and E4) are potent chemicalmediators of the allergic response in asthma. 5-lipoxygenase enzyme inhibitors block productionof leukotrienes. The leukotriene-receptor antago-nists inhibit the action of leukotrienes at theirreceptor.
a. Zafirlukast (Accolate) is orally administered; itsrelatively long half-life permits twice-daily dosing.Absorption is optimized by ingestion on anempty stomach. The only significant drug inter-action is with warfarin, resulting in an increase inthe prothrombin time. A second member of thisdrug category, montelukast (Singulair) is suitablefor once-daily dosing.
b. Zileuton (Zyflo) inhibits production ofleukotrienes by interfering with metabolism ofarachidonic acid by 5-lipoxygenase. It is admin-istered orally on a QID schedule. A small inci-dence (2 to 4 percent) of hepatic inflammation isassociated with zileuton, leading to the recom-mendation that liver function tests be checkedbefore initiating therapy, monthly for the firstthree months of therapy, and at three- to six-month intervals thereafter. Drug interactionsinclude warfarin (increased prothrombin time)and theophylline (increased serum concentra-tion).
4. Mast cell stabilizing agentsa. The mast cell stabilizing agents, cromolyn and
nedocromil, are alternative choices when initiat-ing regular preventive therapy in mild asthma.These drugs are particularly well suited to use inpatients who refuse to use of any steroid prepa-ration.
b. Cromolyn and nedocromil appear to be some-what less effective than inhaled corticosteroids incontrolling asthma. Treatment with cromolyn andnedocromil requires compliance with a QIDdosing schedule. Patients whose asthma is wellcontrolled with nedocromil taken four times dailycan gradually reduce the dosing schedule totwice daily.
E. Long-acting inhaled beta-agonists. Salmeterol(Serevent) and formoterol (Foradil) are inhaled beta-adrenergic agonists with a duration of action of atleast 12 hours. Twice-daily dosing provides 24-hourbronchodilation. Long-acting beta-agonists are notrecommended as monotherapy for mild asthma. Ashort-acting beta-agonist should be used as needed.
F. Treatment of moderate persistent asthma. Thepresence of any of the following is considered anindication of moderate disease:Daily symptoms of asthma.Daily need for bronchodilator medications.The development of asthmatic attacks that interferewith activity.Nocturnal awakenings more than once per week.PEFR 60 to 80 percent of normal.
1. High-dose inhaled steroid. Fluticasone (Flonase)110 or 220 µg/puff or budesonide (Rhinocort) 200µg/inhalation provides potent topical corticosteroidtherapy for moderate asthma with the convenience

of 2 to 4 puffs twice daily.a. High doses of inhaled corticosteroids (greater
than 1000 to 1500 µg/day) may cause severaladverse systemic effects after long-term use:
(1) Increased intraocular pressure.(2) Cataracts.(3) Growth retardation.(4) Possibly increased bone loss.(5) Hypothalamic-pituitary-adrenal axis suppres-
sion.2. Long-acting inhaled beta-agonists. In patients
requiring dual therapy, combined dry powderformulations allow simultaneous delivery of both acorticosteroid and a long-acting beta-agonist (eg,Advair Diskus, Seretide, Symbicort). The steroiddose is variable (100, 250, or 500 mcg per inhala-tion).
3. Leukotriene-modifying agents. Addition of alipoxygenase inhibitor or leukotriene-receptorantagonist may improve asthma control (andpermit reduction of the dose of inhaledcorticosteroids) in moderate or severe asthma.
4. Long-acting oral bronchodilators. Theophyllineand sustained-release albuterol tablets are effec-tive disease controllers when used in combinationwith regular anti-inflammatory therapy.
a. The major disadvantages of these drugs includethe frequency of side effects, a narrow therapeu-tic window, and relative lack of bronchodilatorpotency
b. Theophylline is a reasonable alternative forpatients who are intolerant of long-acting beta-agonists or who are unable to use a metereddose inhaler properly. Attention to theophyllinepharmacokinetics is essential in order to avoidtoxicity.
G. Treatment of severe asthma. The patient withsevere chronic asthma has frequent asthma exacer-bations as a result of viral illnesses, allergens,exercise, or air pollutants; is usually awakened fromsleep four to seven nights per week; has an FEV1
below 60 percent of predicted; and is unable toachieve normal lung function despite chronic treat-ment with multiple medications, including inhaledsteroids at moderate-to-high dose or continuous,every-other-day or multiple-short courses of oralsteroids. These individuals usually require multiple-controller medications and bronchodilator medica-tions used on a regular basis.
References, see page 182.
Atopic Dermatitis and Eczema
Atopic dermatitis is a chronic inflammation of the skin thatoccurs in persons of all ages but is more common inchildren. Atopic dermatitis affects 10 percent of children.The symptoms of atopic dermatitis resolve by adolescencein 50 percent of affected children.
I. DiagnosisA. Exposure to aeroallergens, irritating chemicals,
foods and emotional stress may worsen the rash.B. Acute lesions are papules and vesicles on a back-
ground of erythema. Subacute lesions may developscales and lichenification. Chronically involved areasbecome thick and fibrotic. Lesions can developsecondary infections with crusting and weeping.Xerosis (dry skin) is characteristic.

Diagnostic Features of Atopic Dermatitis
Major features Pruritus Chronic or relapsing dermatitis Personal or family history of atopic disease Typical distribution and morphology of atopic dermatitis rash: Facial and extensor surfaces in infants and young children Flexure lichenification in older children and adults
Minor features Eyes Cataracts (anteriorsubcapsular) Keratoconus Infraorbital folds affected
Facial pallorPalmar hyperlinearity Xerosis Pityriasis alba White dermatographism Ichthyosis Keratosis pilaris Nonspecific dermatitis of thehands and feet
Nipple eczema Positive type I hypersensitiv-ity skin tests Propensity for cutaneousinfections Elevated serum IgE level Food intolerance Impaired cell-mediated im-munity Erythroderma Early age of onset
C. In infants and young children, pruritus commonly ispresent on the scalp, face (cheeks and chin) andextensor surfaces of the extremities. Older childrenand adults typically have involvement of the flexorsurfaces (antecubital and popliteal fossa), neck,wrists and ankles.
D. Exposure to pollens, molds, mites and animaldander may be important in some patients.
II.TreatmentA. Bathing and moisturizers. Bathing should occur
once daily with warm water for five to 10 minutes.Soap should not be used unless it is needed for theremoval of dirt. A mild cleanser (eg, Dove, Basis,Kiss My Face or Cetaphil) may be used. Afterbathing, patients should apply a moisturizer liberally(eg, Vaseline, Aquaphor, Eucerin, Moisturel, mineraloil or baby oil). Ointments are superior to creams.Lotions are least effective because of their alcoholcontent. To avoid injury to the skin from scratching,fingernails should be cut short, and cotton glovescan be worn at night.
B. Pruritus that is refractory to moisturizers and conser-vative measures can be treated with sedating agentssuch as hydroxyzine (Atarax) and diphenhydramine(Benadryl). Tricyclic antidepressants such asdoxepin (Sinequan) and amitriptyline (Elavil) alsoinduce sleep and reduce pruritus.
C. Systemic corticosteroids should be reserved for usein patients with severe treatment-resistant atopicdermatitis.
D. It is reasonable to use a mild topical steroid initiallyin infants and for intertriginous areas in patients ofany age. If the dermatitis is severe, a more potentsteroid is needed.
Commonly Used Topical Corticosteroids
Preparation Size
Low-Potency Agents
Hydrocortisone ointment, cream, 1, 2.5% (Hytone) 30 g
Mild-Potency Agents
Alclometasone dipropionate cream, ointment, 0.05%(Aclovate)
60 g
Triamcinolone acetonide cream, 0.1% (Aristocort) 60 g
Fluocinolone acetonide cream, 0.01% (Synalar) 60 g
Medium-Potency Agents
Triamcinolone acetonide ointment (Aristocort A),0.1%
60 g
Betamethasone dipropionate cream (Diprosone),0.05%
45 g
Mometasone cream 0.1% (Elocon) 45 g
Fluocinolone acetonide ointment, 0.025% (Synalar) 60 g
Betamethasone valerate cream, 0.1% (Valisone) 45 g
Hydrocortisone valerate cream, ointment, 0.2%(Westcort)
60 g

E. Immunosuppressants and antineoplastics1. Pimecrolimus (Elidel) is a non-steroid cream for
the treatment of mild to moderate eczema.Pimecrolimus has anti-inflammatory activity. Itdoes not cause skin atrophy. Topical applicationis comparable to that of a potent topical steroid.1% pimecrolimus cream is applied twice daily. Itmay be used in children >2 years old. The FDAhas issued warnings about a possible link be-tween the topical calcineurin inhibitors and can-cer.
2. Tacrolimus (Protopic) is more potent thanpimecrolimus in the treatment of severe or refrac-tory atopic dermatitis, with few adverse effects.Tacrolimus is available in 0.1% and 0.03%. Thelower strength may be used in children >2 yearsold. The FDA has issued warnings about apossible link between the topical calcineurininhibitors and cancer.
3. Cyclosporine (Sandimmune) has been effectivein patients with refractory atopic dermatitis. Thecondition returns after the cessation of therapy,although not always at the original level of sever-ity.
References, see page 182.
Contact Dermatitis
Contact dermatitis is an extremely common in the pediatricage group. There are two major forms of contact dermati-tis: irritant and allergic. Common causes of irritant contactdermatitis include overbathing, drooling, prolonged contactwith moisture and feces in the diaper, and bubble baths.
I. Clinical evaluationA. Contact dermatitis usually first appears in infants 2-6
months of age. Infants and children have rashes onthe shoulders, chest, abdomen, and back. Infantsusually also have a rash on the face, scalp andaround the ears. Children older than 18 months oldtend to have rashes on the neck and antecubital andpopliteal fossae. Contact dermatitis usually resolvesby puberty, but it sometimes recurs at times ofstress.
B. Acute lesions are itchy, red, edematous papules andsmall vesicles, which may progress to weeping andcrusting lesions. Chronic rubbing and scratching maycause lichenification and hyperpigmentation.
C. Patch testing is useful for evaluation of persistent,localized reactions. It also may be useful in patientswho have atopic dermatitis and experience a flare orpersistence of disease despite appropriate therapy.
II. Treatment of contact dermatitisA. Moisture. Avoidance of excessive bathing, hand
washing, and lip licking is recommended. Showers orbaths should be limited to no more than 5 minutes.After bathing, patients should apply a moisturizer(Aquaphor, Eucerin, Vaseline) to noninflamed skin.
B. Contact with irritants1. Overuse of soap should be discouraged. Use of
nonirritating soaps (eg, Dove, Ivory, Neutrogena)should be limited to the axilla, groin, hands, andfeet.
2. Infants often have bright red exudative contactdermatitis (slobber dermatitis) on the cheeks,resulting from drooling. A corticosteroid will usu-ally bring improvement.
C. Topical corticosteroids1. Corticosteroid ointments maintain skin hydration
and maximize penetration. Corticosteroid creamsmay sting when applied to acute lesions.
2. Mid- and low-potency topical corticosteroids areused twice daily for chronic, atopic dermatitis.High-potency steroids may be used for flare-ups,but the potency should be tapered after thedermatitis is controlled.
3. Use of high-potency agents on the face, genitaliaand skinfolds may cause epidermal atrophy(“stretch marks”), rebound erythema, and suscep-tibility to bruising.
Commonly Used Topical Corticosteroids

Preparation Size
Low-Potency Agents
Hydrocortisone ointment, cream, 1, 2.5% (Hytone) 30 g
Mild-Potency Agents
Alclometasone dipropionate cream, ointment, 0.05%(Aclovate)
60 g
Triamcinolone acetonide cream, 0.1% (Aristocort) 60 g
Fluocinolone acetonide cream, 0.01% (Synalar) 60 g
Medium-Potency Agents
Triamcinolone acetonide ointment (Aristocort A),0.1%
60 g
Betamethasone dipropionate cream (Diprosone),0.05%
45 g
Mometasone cream 0.1% (Elocon) 45 g
Fluocinolone acetonide ointment, 0.025% (Synalar) 60 g
Hydrocortisone butyrate 0.1% cream, ointment(Locoid)
45 g
Betamethasone valerate cream, 0.1% (Valisone) 45 g
Hydrocortisone valerate cream, ointment, 0.2%(Westcort)
60 g
High-Potency Agents
Amcinonide ointment, 0.1% (Cyclocort) 60 g
Betamethasone dipropionate ointment (Diprosone)0.05%
45 g
Fluocinonide cream, ointment, 0.05% (Lidex) 60 g
4. Allergic reactions to topical corticosteroidsmay occur. Mometasone (Elocon) is the leastlikely to cause an allergic reaction.
D. Antihistamines, such as diphenhydramine orhydroxyzine (Atarax), are somewhat useful forpruritus and are sedating. Nonsedating antihista-mines, such as cetirizine (Zyrtec), loratadine(Claritin) and fexofenadine (Allegra), are helpful.
E. Systemic corticosteroids are reserved for severe,widespread reactions to poison ivy, or for severeinvolvement of the hands, face, or genitals. Predni-sone, 1-2 mg/kg, is given PO and tapered over 10-18days.
References, see page 182.
Diaper Dermatitis
Diaper rash occurs in 50% of infants, with 5% havingsevere rash. The peak incidence is between 9 and 12months of age.
III. Pathophysiology. Breast fed infants have fewerdiaper rashes than formula-fed infants. The frequencyand severity of diaper dermatitis are significantlylower when the number of diaper changes per day iseight or more. Superabsorbent disposable diaperssignificantly reduce the severity of diaper rash whencompared to cloth diapers.
IV. Classification of diaper dermatitisA. Dermatoses related to diaper wearing
1. Irritant diaper dermatitis is the most commonform of diaper dermatitis. It is accentuated on theconvex areas, including the buttocks, lowerabdomen, genitalia, and upper thigh, sparing thecreases. It varies in severity from mild erythema(with or without scales) to papules and maceratedlesions.
a. Management(1) Irritant diaper dermatitis can best be pre-
vented by keeping the skin in the diaper areaprotected from urine and feces by increasingthe frequency of diaper changes and by usingsuperabsorbent disposable diapers.
(2) A low-potency corticosteroid ointment (hydro-cortisone 1%) should be applied four timesdaily with diaper changes. Anticandidalagents such as nystatin (Mycostatin),clotrimazole (Lotrimin), or ketoconazole

(Nizoral) should also be added.(3) Thickly applied barrier creams, such as A&D
ointment, zinc oxide pastes or Vaseline, maybe helpful.
2. Candidal diaper dermatitisa. Candidal diaper dermatitis is characterized by
beefy red plaques with white scales and satel-lite papules and pustules, which almost alwaysinvolve the inguinal creases. It often developsafter an episode of diarrhea. KOH scrapingsmay demonstrate pseudohyphae.
b. Candidiasis is treated with topical nystatin(Mycostatin), clotrimazole (Lotrimin),miconazole (Monistat), or ketoconazole(Nizoral) applied 3-4 times daily. Hydrocortisone1% ointment may help decrease erythema andinflammation and can be applied at the sametime. Oral nystatin (Mycostatin) suspension,four times a day, should be used if repeatedepisodes of candidal dermatitis occur. Themother should be evaluated for candidal infec-tion of the nipples or genital tract. In severecases, oral fluconazole (Diflucan) 3 mg/kg perday as a pulse dose weekly x 2 or for a shortcourse of 5 to 7 days may be of benefit.
References, see page 182.
Dermatophyte Infections
Dermatophytes constitute a group of about 40 fungalspecies that cause superficial infections calleddermatophytoses, ringworm, or tinea.
I. Tinea capitisA. Tinea capitis presents as inflammation with hair
breakage and loss. Inflammatory changes canrange from minimal scaling and redness that resem-bles mild seborrhea to tenderness, redness, edema,purulence, and hair loss (kerion).
B. A hypersensitivity reaction to fungal antigen candevelop, called a dermatophytid or “id” reaction. Idreactions can present with either a dermatitis thatincludes redness, superficial edema involving theepidermis, and scaling or with a “pityriasis rosea-like” reaction that involves red, scaly papules andovoid plaques on the face, neck, trunk, and proximalextremities.
C. Topical antifungals are not effective for hair infec-tion. Griseofulvin is preferred for initial treatment ata starting dose of about 20 mg/kg per day.
D. Selenium sulfide shampoo (Selsun Blue) is used inconjunction with oral antifungals to reduce conta-gion. Tinea capitis is contagious until after 2 weeksof systemic treatment. Dermatophytid reactions canbe treated with topical corticosteroids.
II. Tinea corporis (ring worm) and tinea crurisA. Dermatophyte infection of the body surface is
termed tinea corporis. Tinea cruris describes infec-tion of the upper thigh and inguinal area. Examina-tion reveals red, scaly papules and small plaques.These progressively enlarge to form expandingrings, arcs, or annular patterns.
B. Clearing in previously affected areas produces thetypical “ringworm” appearance. Topical therapy isthe initial treatment approach.
III. Tinea pedis and tinea manuumA. Tinea pedis infection is often interdigital and is
induced by the warmth and moisture of wearingshoes. The web spaces become red and scaly.Fungal infection frequently spreads to involve thesoles of the feet or the palms, with dry scale andminimal redness. Scaling extends to the side of thefoot or hand. Vesicle and blister formation anditching are common.
B. Dermatophyte infection often leads to secondarybacterial infection. A dermatophytid reaction mayoccur, as described for tinea capitis.
C. Dermatophyte hand infection presents as dry scaleon the palm. Infection of just one hand in conjunc-tion with infection of both feet is the most commonpattern.
D. Topical therapy and keeping the involved areas asdry as possible is recommended for hand or foottinea. Oral therapy may be necessary for recalcitrantdisease.

IV. Onychomycosis (tinea unguium)A. Dermatophyte infection of the nail plate is referred to
as onychomycosis, characterized by dystrophy ofthe nail, discoloration, ridging, thickening, fragility,breakage, accumulation of debris beneath the distalaspect of the nail and little or no inflammation.
B. Oral treatment is required to clear infection, butrecurrence is very common.
V. DiagnosisA. Potassium hydroxide (KOH) examination of
scale, hair, or nail is the most rapid diagnosticmethod. A sample of scale, hair, or nail from apossibly infected area is placed on a glass slide,covered with a few drops of 30% KOH, and gentlyheated. The specimen is examined for sporesand/or fungal hyphae.
B. Fungal culture of scale and affected hair or nail canbe accomplished by incubation at room temperaturefor 2 to 3 weeks.
VI. TreatmentA. Oral griseofulvin is effective and safe for treatment
of tinea capitis in children. However, its erratic oralabsorption necessitates doses of about 20 mg/kgper day of the liquid preparation, always adminis-tered with a fatty meal or beverage (such as milk).Ultramicrosize griseofulvin can be administered atthe lower dose of 8 to 10 mg/kg per day.
B. Treatment should be continued for 8 to 12 weeks.Liver function testing is not required whengriseofulvin is used for 6 months or less. Adverseeffects associated with griseofulvin include head-aches and gastrointestinal upset.
Systemic Antifungal Agents
Griseofulvin 20 mg/kg per day of microsize liquid or 7 to 10mg/kg per day of ultramicrosize tablets. Microsize: Cap: 250mg, susp: 125 mg/5 mL, tab: 250, 500 mgUltramicrosize: Tab: 125, 165, 250, 330 mg
Itraconazole (Sporanox) 4 to 6 mg/kg per day. Cap: 100 mg,soln: 10 mg/mL
Terbinafine (Lamisil) 3 to 5 mg/kg per day. Tab: 250 mg
Topical Treatments for Tinea Pedis, Tinea Crurisand Tinea Corporis
Antifungalagent
Prescrip-tion
Cream
Solution orspray
Lotion
Powder
Frequency ofappli-cation
Imidazoles
Clotrimazole 1 percent(Lotrimin,Mycelex)
X X X Twicedaily
Miconazole2 percent(Micatin,Monistat-Derm)
X X X X Twicedaily
Econazole1 percent(Spectazole)
X X Oncedaily
Ketoconazole 2 per-cent(Nizoral)
X X X Oncedaily
Oxiconazole 1 percent(Oxistat)
X X X Oncedaily ortwicedaily
Allylamines
Naftifine 1percent(Naftin)
X X Oncedaily ortwicedaily

Topical Treatments for Tinea Pedis, Tinea Crurisand Tinea Corporis
Antifungalagent
Prescrip-tion
Cream
Solution orspray
Lotion
Powder
Frequency ofappli-cation
Terbinafine1 percent(Lamisil)
X X X Oncedaily ortwicedaily
Butenafine1 percent(Mentax)
X Oncedaily ortwicedaily
C. Itraconazole (Sporanox) is effective and can begiven orally at 3 to 5 mg/kg per day for 4 to 6 weeksor until clearing, followed by a 4-week period off oftherapy. A liquid formulation is available. Cap: 100mg, soln: 10 mg/mL
D. Terbinafine (Lamisil) orally at 3 to 6 mg/kg per dayfor 4 to 6 weeks is effective. Tab: 250 mg
E. Topical antifungals can be used once to twice dailyto clear infections other than tinea capitis andonychomycosis. Newer, more potent topical agentswith once-daily dosing can improve compliance.
F. Hydrocortisone 1% or 2.5% can be added toantifungal therapy to reduce inflammation. Affectedareas should be kept as cool and as dry as possible.
References, see page 182.
Herpes Simplex Virus Infections
HSV is a member of the herpes-virus family, whichincludes varicella zoster virus, Epstein-Barr virus, andcytomegalovirus. Like all herpes viruses, HSV tends toestablish latent infection and eventually it reactivates andbecomes infectious. Most HSV-infected patients haveasymptomatic infections or the symptoms are only mildlyuncomfortable. However, a substantial number of patientsexperience frequent painful recurrences or severe or life-threatening illnesses.
I. Virology and pathogenesisA. Two types of HSV exist: HSV-1 and HSV-2. Both
types can infect any anatomic site.B. HSV-1 may cause asymptomatic infection, oral
lesions, nonoral or non-genital skin lesions, enceph-alitis, neonatal disease, and genital lesions
C. HSV-2 may cause asymptomatic infection, genitallesions, neonatal disease, nonoral, nongenital skinlesions, meningitis, and oral lesions
II. TransmissionA. HSV-1 and HSV-2 are transmitted from person to
person through contact with infected skin lesions,mucous membranes, and secretions. The incubationperiod is 1 to 26 days, and both types may betransmitted in utero or perinatally.
B. Asymptomatic virus shedding may transmit thedisease. Women who have had previous genitalHSV-2 infection shed virus on 2% of days.
C. Oral/facial HSV infections1. HSV-1 infection is extremely common in infants
and children. The most common clinicalmanifestation of primary HSV-1 infection isgingivostomatitis, characterized by fever, mal-aise, myalgia, pharyngitis, irritability, and cer-vical adenopathy. The illness is self-limited andusually of short duration.
2. Recurrent HSV-1 infections are most frequentlycharacterized by oral and lip lesions. Manyindividuals who have oral HSV lesions have noknown history of prior gingivostomatitis.
3. HSV-2 also may cause oral lesions and pharyn-gitis, particularly in sexually active individuals.
D. Genital HSV infections1. Many HSV infections are asymptomatic, but they
can also cause papular, vesicular, or ulcerativelesions with pain, itching, urethral or vaginal dis-charge, and dysuria.
2. Primary infections cause more severe symptomsand signs, including extensive skin lesions, ten-

der inguinal adenopathy, and extragenital le-sions. Primary infections are often associatedwith fever, headache, malaise, abdominal pain,and aseptic meningitis.
3. Eighty percent of persons who have a firstepisode of HSV-2 genital infection will experi-ence a recurrence in the first year. Most patientswho have genital HSV infection have few symp-tomatic recurrences.
E. HSV encephalitis1. HSV encephalitis is the most common viral
infection of the CNS. The incidence peaks at 5to 30 years and at more than 50 years. Ninety-five percent of cases are caused by HSV-1. HSVencephalitis is characterized by acute fever,altered mental status, and focal neurologicsymptoms and signs.
2. Routine CSF findings are not diagnostic. Poly-merase chain reaction (PCR) can detect HSVDNA in CSF. HSV is rarely isolated by culture ofthe CSF.
3. Electroencephalographic (EEG) findings can bediagnostic, with spike and slow wave activitylocalized to the temporal region.
4. CT scan and MRI may reveal localized edemaand hemorrhage suggestive of HSV infection.
5. The prognosis for HSV encephalitis withouttreatment is poor, and even with antiviral ther-apy, substantial morbidity and mortality occurs.Prompt institution of empiric therapy is essentialwhen the clinical diagnosis is suspected.
F. Neonatal HSV infections1. Infection in neonates results from vertical trans-
mission during the peripartum period in 85%; inutero or postpartum transmission rarely occurs.Seventy percent of untreated infants will prog-ress to disseminated or CNS disease. Mostneonatal infections are caused by HSV-2, al-though 30% of cases are caused by HSV-1.Seventy to 80% of infected infants are born tomothers who are unaware that they have genitalHSV infection.
2. Skin, eye, mouth (SEM) disease accounts for45% of peripartum infections. SEM disease mostcommonly presents in the first or second weeksof life with vesicular skin lesions which mayoccur anywhere on the body. Skin lesions havean erythematous base with clear or cloudy fluid.If the infection does not progress to involve theCNS or viscera, SEM disease has a low mortal-ity.
3. Central nervous system disease is manifestas encephalitis, and it accounts for 35% ofperipartum infections.a. Neonatal HSV CNS disease most commonly
presents in the second to third week of life.Only 60% will develop skin lesions during theillness. HSV CNS disease has a 50% mortal-ity if not treated; with treatment, mortality is18%. The diagnosis must be considered inany infant who presents with encephalitis,seizures, apnea, bradycardia, or cranialnerve abnormalities.
b. Cerebrospinal fluid findings are nonspecificand include pleocytosis and increased pro-tein. Early initiation of therapy is critical whenthe diagnosis is suspected.
4. Disseminated disease is characterized byhepatitis, pneumonitis, and disseminatedintravascular coagulation, and it accounts for20% of peripartum infections.a. HSV disseminated disease presents in the
first week of life. Bilateral patchy infiltratesare indicative of pneumonitis. Skin lesionsmay not be present initially.
b. Disseminated HSV disease should be con-sidered in any infant presenting with sepsisthat is unresponsive to antibiotic therapy, orwho has both pneumonitis and hepatitis.
5. Eye infectionsa. HSV is the most common cause of corneal
blindness. HSV keratitis is characterized byconjunctivitis and dendritic lesions of thecornea.
b. Topical steroids are contraindicated becausethey may facilitate spread of infection to thedeep structures of the eyes.

III. Management of perinatal HSV infectionA. The most reliable predictor of the risk of perinatal
transmission is whether a woman has active genitallesions at the time of delivery.
B. A thorough physical examination, including vaginalspeculum exam, at the onset of labor shouldexclude the presence of active genital lesions. IfHSV lesions are found during labor, prompt cesar-ean section is recommended.
C. Management of infants exposed to HSV atdelivery1. Virus cultures of the infant’s conjunctivae, phar-
ynx, skin folds, CSF, and rectum at 24-48 hourscan indicate whether HSV has been transmitted.Infants who are culture positive for HSV fromany site after 24 hours of life are given acyclovir.
2. During the time when HSV-exposed infants arein the hospital, they should be placed in contactisolation. Circumcision is deferred.
IV. Diagnosis of HSV infectionA. HSV-1 and HSV-2 can be isolated by virus culture
from active skin, eye, and genital lesions. In casesof recurrent disease, virus shedding may be toobrief to be detected by virus culture. Herpes sim-plex is rarely is recovered from CSF by culture.
B. Although less sensitive and specific than culture,staining for virus antigens with fluorescent antibod-ies detects HSV more rapidly.
C. PCR is a useful diagnostic procedure for HSVencephalitis, with a sensitivity of 75% and a speci-ficity of 100%.
V. Therapy for HSV infectionsA. Parenteral acyclovir is indicated for severe or
potentially severe infections, such as neonatal HSVinfection, HSV encephalitis, and non-localizedinfections in immunocompromised patients. Oralacyclovir decreases new lesion formation andimproves symptoms in first episode genital HSV.Oral acyclovir has limited effect on the resolution ofrecurrent HSV disease.
B. Topical acyclovir is not effective for skin or orallesions. The ophthalmic solution is useful for HSVkeratitis, in combination with IV acyclovir.
C. Acyclovir (Zovirax) 1. For serious infections, such as neonatal disease
and encephalitis, 5-10 mg/kg IV is given q8h for10 to 21 days. Doses up to 20 mg/kg IV q8h areused for infants who have CNS or disseminatedinfection.
2. Oral acyclovir dosage is 20 mg/kg every 8 hoursor 200 mg five times a day for 7-10 days. Theadult regimen is 400 mg three times a day.
3. S u p p r e s s i o n i s i n d i c a t e d f o rimmunocompromised patients or patients whohave more than 6 genital recurrences a year; 5mg/kg q8h or 400 mg bid. Suppressive therapyis also used for infants who have HSV SEMdisease.
D. Valacyclovir (Valtrex) is an ester of acyclovir thathas better oral absorption; 1 gm orally twice a dayfor 5 days. It has a more convenient dosage sched-ule than acyclovir and is approved for adolescents.
E. Famciclovir (Famvir) has a more convenientdosage schedule than acyclovir and is approved foradolescents. Dosage for first episodes of genitalHSV infection is 250 mg q8h for 5 days, and forrecurrent episodes it is 125 mg twice a day for 5days.
F. Sexually active individuals known to have genitalHSV infection should be advised to use latexcondoms even during asymptomatic periods.
References, see page 182.
Urticaria, Angioedema andAnaphylaxis
Urticaria, angioedema, and anaphylaxis are manifesta-tions of the immediate hypersensitivity reaction. Immediatehypersensitivity is an antibody mediated reaction thatoccurs within minutes to hours of exposure to a particularantigen by an immune individual. Twenty percent of thepopulation will have one of these manifestations, espe-cially urticaria, at some time during life.
I. Pathophysiology

A. Urticaria (or hives) is an intensely itchy rash thatconsists of raised, irregularly shaped wheals. Thewheals have a blanched center, surrounded by a redflare. Antigens, chemicals and physical agents(detergents or ultraviolet light) can cause urticaria.
B. Angioedema is an area of circumscribed swelling ofany part of the body. It may be caused by the samemechanisms that cause hives except that the immu-nologic events occur deeper in the cutis or in thesubmucosal tissue of the respiratory or gastrointesti-nal tract.
C. Anaphylaxis is the acute reaction that occurs whenan antigen is introduced systemically into an individ-ual who has preexisting IgE antibodies.1. The patient has difficulty breathing from constric-
tion of the major airways and shock due tohypotension caused by histamine release.
2. Anaphylactoid reactions are not immunologicallymediated. Mannitol, radiocontrast material, anddrugs (opiates, vancomycin) may degranulatemast cells and cause a reaction that resemblesanaphylaxis.
II. AnaphylaxisA. Causes of anaphylaxis include penicillins, insect
venoms, airborne allergens, foods (peanuts, eggs,milk, seafoods, and food dyes and flavors), antitox-ins to tetanus, and products of animal origin.
B. Symptoms of anaphylaxis include pruritus, injec-tion of the mucous membranes, bronchospasm, andhypotension.
C. Prevention of anaphylaxis. Anaphylaxis is bestprevented by avoidance of the cause. However,anaphylaxis frequently is unanticipated. Individualswith a history of anaphylaxis should be provided withinjectable epinephrine. Short-term desensitizationmay be needed in a patient requiring antibiotictreatment.
D. Treatment of acute anaphylaxis1. Epinephrine in a 1:1000 dilution (1.0 mg/mL)
should be injected at 10-20 min intervals at 0.01mL/kg SQ per dose, with a maximum dose of 0.3mL per dose SQ.
2. Oxygen should be administered (100%, 4 L/min)and the airway should be secured.
3. Albuterol, 0.1-0.2 mL/kg in a 5 mg/mL solution,should be given via nebulizer every 4-6 hours.
4. Administration of diphenhydramine orchlorpheniramine and corticosteroids should beconsidered when a complete response to epi-nephrine does not occur.
III. UrticariaA. Hives most commonly results from ingestion of
foods, food additives, or drugs. These usually causehive formation for only a few hours to two days.
B. Cold urticaria may be induced by exposure to cold,which may result in hypotension after immersion incold water.
C. Cholinergic urticaria is characterized by the ap-pearance of small punctate wheals, surrounded bya prominent erythematous flare. These small papularurtications are pruritic and appear predominantly onthe neck and upper thorax. The lesions often de-velop after exercise, sweating, exposure to heat, oranxiety.
D. Solar urticaria may be caused by various wave-lengths of light (280-500 nm). It is uncommon, andit is treated with sun screens.
E. Chronic urticaria is caused by ingestion of foodsubstances that contain natural salicylates. Sensitiv-ity to the food additive tartrazine yellow No. 5 fre-quently is found in patients with salicylate sensitivity.
F. Exercise urticaria is characterized by hives andbronchospasm after exercise.
G. Genetic deficiencies of complement factor H orfactor I may cause urticaria. Patients who have thesedefects frequently develop severe hives, particularlyafter exposure to cold or hot water or alcohol inges-tion.
H. Treatment of urticaria. Urticaria generally is a self-limiting disorder and usually requires only antihista-mines. Hydroxyzine 0.5 mg/kg is the most effectivetreatment. Diphenhydramine 1.25 mg/kg every 6 hrsis also effective.
IV. Angioedema A. Angioedema is similar to hives, but the reaction
occurs deeper in the dermis. It causes diffusecircumscribed swelling. Angioedema is often ac-

quired, or it may be observed in an inherited diseaseknown as hereditary angioneurotic edema (HANE).
B. Hereditary Angioneurotic Edema (HANE)1. HANE is characterized by episodes of localized
subcutaneous edema of any part of the body.Attacks of severe abdominal cramps and vomitingmay be caused by edema of the bowel wall.Severe attacks of colic may occur during infancy.
2. Laryngeal edema may sometimes progress tototal upper airway obstruction, pulmonary edema,and death. Attacks of palatal and laryngealedema may follow dental trauma or occur duringupper respiratory infections.
3. HANE is inherited as an autosomal dominantdisease. However, about 10% of cases arecaused by new spontaneous mutations, which arepassed to offspring.
4. Prophylaxis against attacks of angioedema canbe achieved with impeded androgens (ie, andro-gens that are only minimally virilizing). Stanozolol,at a dose of 2 mg/day; or danazol, 50-300mg/day, can prevent attacks of angioedema.
C. Acute angioedema does not generally respond toepinephrine, antihistamines, or steroids. Treatmentconsists of supportive therapy with IV fluids, analge-sics, and airway management. Fresh frozen plasmais generally effective.
References, see page 182.

Infectious DiseasesFever Without a Source in Children3 to 36 Months of Age
Most children have a febrile illness before their thirdbirthday. The majority of children have either a self-limitedviral infection or a source of bacterial infection. When thehistory and physical examination cannot identify a specificsource of fever in an acutely ill, nontoxic-appearing childless than three years of age, the illness is called feverwithout a source.
I. Assessment of fever is based upon core temperature,measured rectally. The threshold of fever that indicatesthe need for evaluation in a well-appearing child 3 to 36months of age is 39ºC (102.2ºF).
II. Causes of fever. The vast majority of young childrenwith fever have an infectious cause. Acute fever isdefined as <7 days in duration. The source of infectionmay be a bacterial or viral illness. A. In children 3 to 36 months of age presenting with a
febrile illness, an infectious syndrome, usually avirus, such as croup, bronchiolitis, varicella, orroseola, is identified in 4 percent. A readily identifi-able presumed bacterial illness is diagnosed in 56percent of children. Over 86 percent of these areotitis media.
B. Serious bacterial infectious syndromes in children 3to 36 months of age include meningitis, pneumonia,and cellulitis. Less than one percent have meningi-tis, 30 percent have pneumonia, and 10 percenthave focal soft tissue infections.
C. Pneumonia. Most children with fever and pneumo-nia have an abnormality on physical exam, usuallytachypnea, suggesting respiratory tract disease.Highly febrile young children (<5 years) may haveoccult pneumonia with fever and leukocytosis,without clinical evidence of pneumonia. Twenty-sixpercent of 146 patients with fever >39ºC and WBC>20,000/microL, have pneumonia diagnosed onchest radiograph.
D. Urinary tract infection (UTI) may be the source ofoccult infection in infants and young children withfever.
E. Bacteremia sometimes occurs in a seriously illpatient with meningitis, septic arthritis, or cellulitis.Sepsis is suggested by a child who is ill-appearing,febrile and without a source of infection.
F. Risk factors or bacteremia1. Age 3 to 36 months.2. >39ºC.3. >15,000/microL.
III. EvaluationA. History must include information about oral intake,
irritability or lethargy, cough, vomiting, or change inactivity. Children with pneumonia may have coughor tachypnea, and vomiting without diarrhea canoccur in urinary tract infections. A child with a deepsoft tissue or bone infection may be protecting theaffected area. Underlying medical conditions thatincreases the child’s risk for serious infection includesickle cell disease and urinary tract reflux.
B. The child who has not received three doses of theHib and pneumococcal vaccines is at greater risk foroccult bacteremia than the one who is fully immu-nized.

Clinical and Laboratory Findings in Toxic andNon-toxic Infants and Children
Febrile Infants at Low Risk Toxic Infant or Child
HistoryNo previous hospitaliza-
tions or chronic illnessTerm delivery withoutcomplicationsNo previous antibiotictherapy
Physical ExaminationNontoxic clinical appear-anceNo focal bacterial infection(except otitis media)
Activity, hydration and per-fusion normal
Social SituationParents/caregiver matureand reliableThermometer and tele-phone at child’s home
Laboratory CriteriaWhite blood cell count of5,000-15,000/mm3
Band cell count<1,500/mm3
Normal urinalysis (<5white blood cells/high-power field)
When diarrhea is present,less than 5 white bloodcells/high-power field instool
Slow, irregular or decreasingrespiratory rateHead bobbingStridorParadoxic or abdominalbreathingChest retractionsCentral cyanosisAltered level of conscious-nessFever with petechiaeTachypneaGruntingProlonged expirationNasal flaringPoor muscle tonePoor or delayed capillary refillTachycardia
C. Physical examination. Febrile children who areacutely ill with lethargy, poor perfusion, hypoventila-tion or hyperventilation, and cyanosis have theappearance of being toxic or septic. They areconsidered to have a significant bacterial infectionuntil proven otherwise. Cultures of blood, urine, andCSF should be obtained, fluid and antibiotic therapyinitiated, and admission to the hospital arranged.1. Signs of infection
a. Abnormal vital signs such as tachycardia,tachypnea, or pulse oximetry <95 percent.
b. Lesions in the oropharynx may identify herpesgingivostomatitis (anterior ulcers) orcoxsackie virus (pharyngeal vesicles).
c. Increased work of breathing is indicated bynasal flaring, retractions or use of accessorymuscle, rales or decreased breath sounds.
d. Abdominal tenderness.e. Pain with bone palpation or passive joint
range of motion.f. Skin findings, such as petechiae, cellulitis, or
viral exanthem.D. Laboratory testing
1. WBC and ANC counts. Occult bacteremia issuggested by WBC >15,000/microL and abso-lute neutrophil count (ANC) >10,000/microL.However, 20 percent of patients with occultbacteremia may have a WBC <15,000/microL.
2. Cultures. The definitive diagnosis of a seriousbacterial infection is often made with cultures,although the inherent delay between the initialevaluation of the patient and the availability ofculture results complicates management deci-sions.
3. Blood. Continuously monitored blood culturesystems have decreased the length of time for ablood culture to turn positive.
4. Urine. A clean catch is the preferred method ofurine collection for culture in the child who istoilet-trained. For the diapered child, urineshould be collected by catheterization orsuprapubic aspiration. Bag specimens shouldnot be sent for culture because they are fre-quently contaminated.
5. CSF. Children who are being evaluated for feverwithout a source should be well-appearing and,therefore, not require lumbar puncture. CSFshould be obtained from any patient with sus-pected meningitis.
6. Chest radiograph may be appropriate in pa-tients with tachypnea, respiratory distress, oxy-gen saturation <97 percent, or WBC >20,000-25,000/microL.

IV. ManagementA. Pre-conjugate vaccine strategies
1. Treatment is required for children with WBC>15,000/microL or an abnormal urinalysis withparenteral ceftriaxone, pending blood and/orurine culture results. The prevalence of occultbacteremia and the possibility of missing a caseof meningitis were high enough to justify testingmany children and using broad spectrum antibi-otics.
2. For those children <6 months or those who areincompletely immunized, urinalysis, urine cul-ture, CBC, blood culture, and chest radiographif WBC >20,000-25,000/microL are recom-mended. Patients with WBC >15,000/microLshould receive antibiotic therapy.
V. Recommendations. Children who are ill-appearing orhave unstable vital signs should receive cultures ofblood, urine and, when meningitis is suspected, CSF.Presumptive antibiotic therapy should be initiated. Forchildren 3 to 36 months of age, with fever >39ºC, whoare well-appearing, have no underlying medical condi-tion that would alter susceptibility to infection, and noidentifiable focus of infection should be evaluated asfollows:A. For children <6 months, and for any child <36
months who has not been completely immunized,the following testing and treatment strategies arerecommended: CBC, urinalysis, blood and urinecultures, CXR when WBC >20,000/microL, andantibiotic therapy with parenteral ceftriaxone whenWBC >15,000/microL.
B. Alternatives for children who cannot receiveceftriaxone include clindamycin or a macrolide. Forgirls between 6 and 24 months of age anduncircumcised boys between 6 and 12 months whohave received three doses each of Hib vaccine andPCV7, urinalysis and urine culture should beobtained.
References, see page 182.
Bacterial Meningitis
Therapy should be initiated immediately after the resultsof lumbar puncture (LP) are received or immediately afterLP alone if the clinical suspicion is very high. Should thisprocedure be delayed by the need for cranial imaging,blood cultures should be obtained and antibiotics shouldbe administered empirically before the imaging study,followed as soon as possible by the LP.
I. Pretreatment evaluationA. History. Bacterial meningitis often presents with
fever, vomiting, and nuchal rigidity. Symptomsconsistent with a viral infection of the upper respira-tory tract commonly precede the development ofmeningitis.
B. Older children may complain of headache,photophobia, or neck or back pain. Younger childrenare commonly irritable or lethargic. 20 to 30 percentof children have a seizure prior to diagnosis.
C. Children have a stiff neck, and Kernig andBrudzinski signs may be present. A bulging or tensefontanelle in an infant or a sixth cranial nerve palsysuggests increased intracranial pressure (ICP).Advanced illness is characterized by lethargy,dehydration, or signs of septic shock.
D. Seizure activity should be assessed, and the follow-ing historical information should be obtained beforeantibiotic treatment of presumed bacterial meningitisis instituted:1. Serious drug allergies.2. Vaccines received.3. Recent travel.4. Recent exposure to someone with meningitis.5. Recent infections (especially respiratory and otic
infections).6. Recent head trauma or craniotomy.7. Recent use of antibiotics.8. The presence of a progressive petechial or
ecchymotic rash.E. Blood tests. Initial blood tests should include a
complete blood count with differential and plateletcount, and two sets of blood cultures. Serum electro-lytes, blood urea nitrogen and serum creatinine

concentrations are helpful in planning fluid adminis-tration.
F. CSF examination should be obtained for cell countand differential, glucose and protein concentration,Gram stain, and culture. Cytocentrifugation of CSFenhances the likelihood of detection of bacteria onGram-stained specimens. The CSF Gram stain ispositive in 90 percent with pneumococcal meningitisand in 80 percent with meningococcal meningitis.
G. Characteristic findings include an increased whiteblood cell (WBC) count, usually composed primarilyof neutrophils; an elevated protein concentration;and a low glucose concentration, which may be lessthan 10 mg/dL. Bacterial antigen tests should bereserved for cases in which the initial CSF Gramstain is negative and culture is negative at 48 hours.Polymerase chain reaction (PCR) of CSF and bloodis most helpful for documenting meningococcaldisease in the patient with negative cultures.
H. Children with focal neurologic findings or comashould receive a computer tomographic scan beforeLP.
Cerebrospinal Fluid Findings in Normal and In-fected Hosts
Disorder Color
WBCCount(/mm3)
Gluc-ose(mg/dL)
Pro-tein(mg/dL)
Gram’s Stainandculture
Normalinfant
clear <10 >40 90 negat-ive
Normalchild oradult
clear 0 >40 <40 negat-ive
Bacterialmening-itis
cloudy
200-10000
<40 100-500
usuallypositive
Viralmening-itis
clear 25-1000(<50%PMN)
>40 50-100 negat-ive
Common Etiologic Agents of Meningitis by AgeGroup
Organism 0-3Mont
hs
3-36Month
s
3-21Years
Immuno-
comp-romise
d
Group BStreptococcus
X
Escherichiacoli
X
Listeriamonocytogenes
X
Streptococcuspneumoniae
X X X
Neisseriameningitidis
X X X
Fungus X
Cryptococcus X
Tuberculosis X
Virus X X X X
Note: Haemophilus influenzae no longer is a com-mon pathogen in countries where the conjugatevaccines are used routinely.
I. Neurologic sequelae and steroids. Permanentneurologic sequelae occur in 16 to 36 percent ofchildren who survive an episode of bacterial menin-gitis. A common complication of bacterial meningitisis hearing loss of varying severity.

1. Corticosteroid therapy should be administeredfor H. influenzae type b meningitis. Dexametha-sone for pneumococcal meningitis is recom-mended for infants and children 6 weeks of ageand older.
J. Repeat CSF analysis. Selected infants and chil-dren with bacterial meningitis have a repeat analy-sis of CSF between 24 and 36 hours after initiatingtherapy. Reexamination of CSF is recommended inthe following situations:1. To assure sterilization of the CSF in patients with
resistant organisms, such as pneumococciresistant to cefotaxime or ceftriaxone.
2. When dexamethasone is administered forpneumococcal meningitis, which might interferewith the ability of the physician to assess clinicalresponse such as resolution of fever.
3. When the clinical response to therapy forpneumococcal meningitis is poor despite treat-ment with appropriate agents.
4. Two to three days after the initiation of therapyfor meningitis caused by a Gram negative rod.
5. Repeat CSF cultures should be sterile.II. Empiric therapy
A. From age 1 to 24 months of age, S. pneumoniaefollowed by N. meningitidis are the two most com-mon causes of bacterial meningitis.
B. From age 2 through 18 years, N. meningitidis wasthe most common cause, accounting for more thanone-half of cases, followed by S. pneumoniae.
C. Infants and children with no known immuneproblem. Meningococcus and pneumococcus arethe most likely organisms in immunocompetentinfants and children who have been immunized withthe conjugate H. influenzae vaccine. High doses ofthird-generation cephalosporins, such ascefotaxime (225 to 300 mg/kg per day in three orfour divided doses; maximum dose 12 g per day) orceftriaxone (100 mg/kg per day in one or twodivided doses; maximum dose 4 g per day) plusvancomycin (60 mg/kg per day in four divideddoses) should be started.
Dosages of Antibiotics Administered Intrave-nously to Newborn Infants and Children
Antibiotic Age (Days) Dosage Desired Se-rum Con-centrations(Mcg/mL)
Ampicillin 0-77-30
>30
50mg/kg/doseq8h50-75mg/kg/doseq6h50-75 q6h
Not critical tomeasure
Cefotaxime(Claforan)
0-77-30
>30
50mg/kg/doseq8h50-75mg/kg/doseq6h75 q6h
Not critical tomeasure
Ceftriaxone(Rocephin)
All 80-100mg/kg/dose.At diagnosis,12 h, 24 h,and every 24h thereafter
Not critical tomeasure
Gentamicin 0-77-30
>30
2.5mg/kg/doseq12h2.5mg/kg/doseq8h2.5mg/kg/doseq8h
Peak, 6-10Trough,<2

Antibiotic Age (Days) Dosage Desired Se-rum Con-centrations(Mcg/mL)
Vancomycin 0-77-30>30
15mg/kg/doseq12h15mg/kg/doseq8h15mg/kg/doseq6h
Peak, 30-40Trough, 5-10
D. Children with known immune deficiency1. S. pneumoniae and S. aureus were the two most
common isolates causing meningitis amongchildren with cancer and neutropenia.Cefotaxime or ceftriaxone plus vancomycin givenare empiric coverage. If a Gram negative rod isobserved on Gram stain of the CSF, the additionof an aminoglycoside is recommended.
2. S. pneumoniae and L. monocytogenes are themost likely causes of bacterial meningitis withdefective cell-mediated immunity. In patientswho are at risk for developing listerial infection,high doses of ampicillin (300 to 400 mg/kg perday in four or six divided doses) should be givenalong with cefotaxime or ceftriaxone plusvancomycin until results of cultures return.
E. Patients with recent neurosurgery. In addition tothe usual nosocomial pathogens, coagulase-nega-tive staphylococci (S. epidermidis) and S. aureusare important causes of meningitis after neurosur-gery. Empiric therapy in this setting consists of acombination of vancomycin and a third-generationcephalosporin. An aminoglycoside should be addedif Gram-negative bacilli are noted on CSF Gramstain.
III. Therapy for specific pathogensA. Haemophilus influenzae. Third-generation
cephalosporins such as cefotaxime (200 mg/kg perday in three or four divided doses) and ceftriaxone(loading dose of 75 mg/kg followed by 100 mg/kgper day in one or two divided doses) are effective.Rifampin prophylaxis is indicated for the patient andselected close contacts.
B. Neisseria meningitidis. Meningococcal meningitisis suggested by disease occurring in children andyoung adults, often accompanied by a diffuse,petechial rash. This infection is best treated withpenicillin. A third-generation cephalosporin is aneffective alternative to penicillin. The index patientmay need to take rifampin or ceftriaxone to eradi-cate the organism from the nasopharynx, unlessthe meningitis was treated with ceftriaxone orcefotaxime.
C. Streptococcus pneumoniae is the most commoncause of meningitis in infants and children from 1 to23 months of age. Treatment consists of penicillinfor 10 to 14 days at a dose of 300,000 units/kg perday intravenously every four to six hours. Goodresults are also obtained with cefotaxime.Vancomycin would be administered until thepneumococcal isolate is determined to be suscepti-ble to penicillin or cefotaxime.
D. Listeria monocytogenes, a Gram positive rod, isan important cause of bacteremia and meningitis,particularly in patients with impaired cell-mediatedimmunity. Listeria is treated with ampicillin andgentamicin.
References, see page 182.
Acute Otitis Media
Otitis media is the most frequent diagnosis in sick childrenvisiting physicians’ offices. The disease is most prevalentin infancy. Fluid may persist for weeks to months after theonset of signs of acute otitis media despite treatment.
I. EpidemiologyA. The highest incidence of acute otitis media occurs
between six and 24 months of age. The incidencethen declines with age except for a limited reversalof the downward trend between five and six years of

age, the time of school entry. Acute otitis media isinfrequent in school age children, adolescent, andadults.
B. Risk factors1. Age. The peak age-specific attack rate occurs
between six and 18 months of age. Children whohave had little or no experience with otitis mediaby the age of three years are unlikely to havesubsequent severe or recurrent disease.
2. Sex. Males have a higher incidence of acute otitismedia than females.
II. MicrobiologyA. Bacteria. Most of the bacterial isolates from middle
ear fluid are streptococcus pneumoniae,Haemophilus influenzae, and Moraxella catarrhalis.The conjugate Haemophilus influenzae type b (Hib)vaccine has had little impact on Haemophilus acuteotitis media because more than 90 percent of casesof Haemophilus acute otitis media are due tonontypable strains.
B. Streptococcus pneumoniae is the most importantbacterial cause of otitis media, associated with 25 to40% of cases.
C. Haemophilus influenzae. Nontypable strains of H.influenzae are second in importance in causingacute otitis media, responsible for 10 to 30% ofcases. One-third to one-half of strains of H.influenzae recovered from middle ear fluids producebeta-lactamase.
D. Moraxella catarrhalis has increased in frequency inmiddle ear aspirates of children with acute otitismedia, responsible for 10%. More than 90% ofstrains produced beta-lactamase.
E. Other bacteria. Group A streptococcus is only anoccasional pathogen. Small numbers are identifiedfor Staphylococcus aureus and anaerobic bacteria.Gram-negative bacilli are responsible for 20% ofcases of acute otitis media in the first months of life,but these organisms are rarely present in themiddle-ear effusions of older infants and childrenwith acute otitis media. Pseudomonas aeruginosa isassociated with chronic suppurative otitis media.
F. Viruses. Viral infection is frequently associated withacute otitis media. Sixteen percent of middle-earfluids of children with acute otitis media are associ-ated with viruses, most frequently are respiratorysyncytial virus, rhinoviruses, influenza viruses andadenoviruses.
III. Clinical manifestations. Symptoms of acute otitismedia include otalgia or ear pain, hearing loss, andvertigo. Otalgia is more common in adolescents andadults than in young children.
A. Otorrhea or ear discharge or swelling about the ear(which may indicate disease of the mastoid) arespecific physical findings, if present. Nonspecificsymptoms and signs include fever, irritability, head-ache, apathy, anorexia, vomiting and diarrhea.
IV. Diagnosis. The diagnosis of acute otitis media re-quires evidence of an acute history, signs and symp-toms of middle ear inflammation, and the presence ofmiddle ear effusion.A. The hallmark of establishing the diagnosis is the
demonstration of fluid by pneumatic otoscopy; thefinding of a red tympanic membrane alone is notsufficient to make a diagnosis.
B. Otoscopic examination identifies a tympanicmembrane that is often erythematous due toinflammation, bulges because of the expansion offluid in the middle ear and is immobile because themiddle ear is fluid rather than air filled. Cloudinessis also common.
C. Aspiration of the middle ear fluid is warranted if thepatient with acute otitis media is toxic, has immunedeficits, or has failed prior courses of antibiotics.

V. Treatment and Prevention of Acute Otitis MediaA. Symptomatic therapy
1. Ibuprofen and acetaminophen may improvepain. The topical agent, Auralgan (combinationof antipyrine, benzocaine, and glycerin) im-proves ear pain scores at 30 minutes aftertreatment.
2. First-line antimicrobial therapy. Amoxicillin isthe drug of choice for otitis media because it iseffective, safe, is relatively inexpensive, andhas a narrow microbiologic spectrum. Doublingthe dose to 80 to 90 mg/kg per day divided intotwo doses increases the concentration ofamoxicillin in the middle ear. The increasedconcentrations provide activity against mostintermediate strains of S. pneumoniae andmany of the resistant strains. Only S.pneumoniae that are highly resistant to penicil-lin will not respond to this regimen.
3. Penicillin-allergic patients. In patients whoreport penicillin allergy but who did not experi-ence a Type 1 hypersensitivity reaction (urti-caria or anaphylaxis), cefdinir (14 mg/kg perday in 1 or 2 doses), cefpodoxime (10 mg/kgper day, once daily), or cefuroxime (30 mg/kgper day in 2 divided doses) can be used.
4. A macrolide (erythromycin plus sulfisoxazole,azithromycin, or clarithromycin) is preferred forchildren who have had a Type 1 reaction toamoxicillin or other beta-lactam antimicrobialagents. Erythromycin plus sulfisoxazole([Pediazole] 50 to 150 mg/kg per day dividedinto 4 doses) may be the most effective, but ishas an unpleasant taste. Five days ofazithromycin (Zithromax) 10 mg/kg per day asa single dose on day 1 and 5 mg/kg per day fordays 2 through 5) or clarithromycin ([Biaxin] 15mg/kg per day divided into 2 doses) can beused. Trimethoprim-sulfamethoxazole (Bactrim)may still be useful in regions wherepneumococcal resistance to this combination isnot a concern.
5. Duration of therapya. A 10-day course of an oral antimicrobial is
recommended for the treatment of acuteotitis media. However, a shorter course maybe adequate, and a single dose ofazithromycin has been approved.
b. Ten-day therapy is more effective in patientsunder age 6. A five- to seven-day course ofantibiotics is appropriate for children ages 6and older who have mild to moderate dis-ease.
6. Treatment failures. With antimicrobial therapy,the signs of systemic and local illness usuallyresolve in 24 to 72 hours. Lack of improvementby 48 to 72 hours suggests either anotherdisease is present or the initial therapy was notadequate.a. High-dose amoxicillin-clavulanate (90 mg/kg
per day amoxicillin, with 6.4 mg/kg per day ofclavulanate in two divided doses) is recom-mended. Alternatives include the drugs citedabove for penicillin allergic patients, includ-ing cefdinir, cefpodoxime, and cefuroxime.
b. Ceftriaxone (50 mg/kg IM) is effective for thetreatment of acute otitis media in childrenwho fail amoxicillin. Three consecutive dosesis superior to a single dose. Children shouldbe given the first dose and then observedcarefully for 48 hours, a second or even thirddose should be given if clinical symptomsand signs do not respond to the first injec-tion. Patients who fail amoxicillin-clavulanateshould be treated with a three day course ofparenteral ceftriaxone.

Second-Line Antibiotic Therapy for Acute OtitisMedia
Drug Dosage Comments
Amoxicillin-clavulanic acid(Augmentin)
40 mg/kg ofamoxicillin compo-nent in 3 divideddoses
Diarrhea com-mon
Cefuroxime axetil(Ceftin)
500 mg in 2 divideddoses
Ceftriaxone(Rocephin)
50 mg/kg IM
7. Persistent middle-ear effusion is common afterthe resolution of acute symptoms and is not anindication of treatment failure. Middle-ear effusionmay persist after the onset of acute otitis media in70 to 10% at three months.
8. Chemoprophylaxis should be considered forpatients with three or more episodes of otitismedia in six months and four or more episodes in12 months. Amoxicillin or sulfisoxazole is used atone-half the therapeutic dose administered oncea day during the fall, winter and early spring.
9. Vaccinesa. Conjugate pneumococcal vaccine is recom-
mended for universal immunization of infants toage two years and selective immunization ofchildren two to five years of age. Children withsevere and recurrent episodes of otitis media inthe two- to five-year-old age groups are candi-dates for the conjugate vaccine.
b. Influenza vaccine is now recommended for allinfants 6 to 24 months of age and should begiven in the fall to older children who have hadrecurrent episodes of acute otitis media in thepreceding winter.
10. Surgerya. Tympanostomy tubes have been accepted as
a treatment for chronic otitis media or otitismedia with effusion, their role in the preventionof recurrent acute otitis media is more contro-versial.
b. Adenoidectomy with or without tonsillec-tomy has been documented to be of value inreducing the number of acute episodes forchildren who have recurrences after an initialplacement of tympanostomy tubes. Thesesurgical procedures do not appear to be aneffective primary preventive measure for chil-dren with recurrent acute otitis media.
References, see page 182.
Pneumonia
A lower respiratory tract infection (LRI) develops in one inthree children in the first year of life. Twenty-nine percentof these children develop pneumonia, 15% develop croup,34% tracheobronchitis, and 29% bronchiolitis.
I. Clinical evaluation of pneumoniaA. Cough. Pneumonia usually causes cough that
persists day and night. Patients who cough sponta-neously throughout the office visit are likely to havelower respiratory tract disease.
B. Grunting occurs in 20% of infants who havebronchiolitis or pneumonia. Grunting preventscollapse of narrowed airways and improves oxygen-ation.
C. Chest pain. Pneumonia causes chest pain whenthe infection develops near the pleura. Pneumoniathat involves the diaphragmatic pleura may presentas abdominal pain. Older children may complain ofdiffuse chest or abdominal pain, which is caused bypersistent cough and repeated muscle contraction.
D. Tachypnea. Increased respiratory rate is one of theearliest and most consistent signs of lower respira-tory tract disease.

Abnormal Respiratory Rates by Age
Age Abnormal
<2 months >60 bpm
2-12 months old >50 bpm
>1 year old >40 bpm
E. Retractions of the intercostal spaces may occurwith pneumonia because of decreased complianceor increased airway resistance.
F. Auscultation1. Signs of consolidation include dullness to
percussion and increased transmission of thevoice on auscultation.
2. Crackles are the fine popping sounds that occurwhen previously closed airways open suddenly.They indicate pulmonary parenchymal disease.
3. Wheezing is generated by narrowed airways. Itcan be caused by bronchiolitis, asthma, earlypulmonary edema, subglottic stenosis, or tra-cheal compression.
G. Cyanosis occurs at an oxygen saturation of 67%;however, cyanosis will not manifest in the presenceof anemia. It is not a sensitive predictor of pneumo-nia because significant hypoxemia may be presentbefore cyanosis is visible.
II. Diagnostic evaluation of lower respiratory infec-tionsA. Chest radiograph. A chest radiograph should be
obtained when the child with pneumonia appearsacutely ill.
B. Laboratory tests1. WBC count should be obtained for children who
have significant fever (>38EC in infants, >39ECin children), who appear ill, or who are hos-pitalized.
2. Blood cultures are rarely positive in childrenwith pneumonia. They should be obtained ininfants and children with high fever, ill appear-ance, or upon hospitalization.
3. Bacterial antigen assays of urine by latexagglutination, or antibody tests of blood areindicated when unusual infections are suspectedor when pneumonia is unresponsive to therapy.
4. Nasopharyngeal cultures for viruses andimmunofluorescence studies for viral antigensare obtained when therapy with antiviral agentsis being considered.

Empiric Antibiotic Treatment of Pediatric Pneu-monia
Age group Empiric regimen
NeonateBacterial (notchlamydia)
Ampicillin (for those<2000 g and 0 to
7 days old: 100mg/kg per day in twodivided doses; <2000g and 8 to 28 daysold: 150 mg/kg perday in 3 divideddoses; >2000 g and0 to 7 days old: 150omg/kg per day in 3divided doses; >2000g and 8 to 28 daysold: 200 mg/kg perday in four divideddoses; PLUS
Gentamicin (gestationalage plus weeks
of life - for those <26weeks: 2.5 mg/kg perdose every 24 hours;27-34 weeks: 2.5r/kgper dose every 18hours; 35-42 weeks:2.5 mg/kg per doseevery 12 hours; >43weeks: 2.5 mg/kg perdose every 8 hours)
Viral (herpes simplex) Acyclovir (60 mg/kg perday IV in three divided
doses
One to four monthsBacterial (notchlamydial)
Cefuroxime (150 mg/kgper day IV in three di-vided doses [MAX 4g/day]); ORCeftriaxone (75 to 100mg/kg once daily ORcefotaxime (100 to 200mg/kg per day IV in 4divided doses [MAX 10to 12 g/day]) PLUSclindamycin (30 to 40mg/kg per day IV in 3 or4 divided doses [MAX 1to 2 g/day]) if compli-cated by parapneumoniceffusion
Chlamydial Erythromycin (4o to 50mg/kg per day in fourdivided doses); ORAzithromycin (10 mg/kgon day 1 followed by 5mg/kg daily for 4 moredays [MAX 500 mg onday 1 and 250 mg there-after]);OR Clarithromycin (15mg/kg per day in two di-vided doses [MAX 1g/day])
Four months to fiveyears
Bacterial (notMycoplasmal orChlamydia)
Oral regimensAmoxicillin (80 to 100mg/kg per day PO in 3divided doses [MAX 600mg/day])Parenteral regimens
Ampicillin (150 to 200mg/kg per day IV in 4divided doses [MAX10 to 12 g/day])ORCefuroxime (dosingas above)

Age group Empiric regimen
Older than five yearsMycoplasmal/chlamydialBacterial
E r y t h r o m y c i n ,a z i t h r o m y c i n ,clarithromycin (dosed asabove); OR doxycycline.Ampicillin (dosed as for 4months to 5 years); ORcefuroxime (dosed asabove) + coverage forM y c o p l a s m a o rChlamydia
III. Treatment of Community-Acquired Pneumonia inChildrenA. Neonates
1. Pneumonia is treated with empiric intravenousampicillin (150 mg/kg per day divided every 12hours if meningitis is also suspected and 50 to100 mg/kg every 12 hours if not) and gentamicin(dose based upon gestational age and renalfunction). This regimen will cover the most likelypathogens, group B streptococcus, Listeriamonocytogenes, and Enterobacteriaceae spp.,especially Escherichia coli K1.
2. During the first two weeks of life, herpes simplexvirus (HSV) is a possible cause of pneumonia.Intravenous acyclovir (60 mg/kg in three divideddoses for 21 days) should be considered forsuspected patients.
B. Infants and older children1. Bacterial pneumonia. When bacterial disease
is suspected, the second-generationcephalosporin, cefuroxime (150 mg/kg per dayin three divided doses up to a maximum of 4 to6 g/d), provides good coverage against theusual pathogens.
2. Other possible regimens include: a third-genera-tion cephalosporin, ceftriaxone (75 to 100 mg/kgonce daily up to a maximum dose of 4 g/d) orcefotaxime (100 to 200 mg/kg per day in fourdivided doses up to a maximum of 10 to 12 g/d),for patients three weeks to three months old orampicillin (150 to 200 mg/kg per day in fourdivided doses) for those four months to fouryears old since disease caused by beta-lactamase-producing organisms (eg, Staphylo-coccus aureus and Haemophilus influenzae) isnot likely in this older age group.
3. With the concern for increasing beta-lactamresistance among Streptococcus pneumoniaeisolates and the increasing prevalence ofcommunity-acquired methicillin-resistant S.aureus (MRSA) infections, empiric treatmentwith Clindamycin (30 to 40 mg/kg per day inthree to four divided doses up to a maximum of1 to 2 g/d) is reasonable for complicated casesof community-acquired pneumonia.
4. Since there are reports of antibiotic failures dueto treatment of non-susceptible S. pneumoniaewith beta-lactams and concern for MRSA, se-verely ill patients requiring admission to theintensive care unit should be treated withvancomycin (40 mg/kg per day IV in four divideddoses up to a maximum of 2 to 4 g/d) in additionto a third-generation cephalosporin andazithromycin.
5. Amoxicillin is generally considered the drug ofchoice for the outpatient treatment of patientsyounger than five years of age with community-acquired pneumonia. Because of the increasingprevalence of pneumococcal penicillin-resis-tance, higher doses (80 to 100 mg/kg per dayPO in three divided doses up to a maximum of 2to 3 g/d) are recommended.a. The macrolides are generally recommended
for the outpatient treatment of the older childand adolescent because of the greater likeli-hood of infection due to Mycoplasmapneumoniae and Chlamydia pneumoniae.Doxycycline (4 mg/kg PO per day in twodivided doses up to a maximum of 200 mg/d)is an alternative, especially if a macrolidehypersensitivity exists. Approximately 50percent of S. pneumoniae isolates are now
resistant to the macrolides, so a failure torespond may indicate the need to changetherapy to high-dose amoxicillin or acephalosporin for better pneumococcalcoverage. For the older child admitted to thehospital, addition of a macrolide to the previ-ously suggested antibacterial regimen maybe necessary if M. pneumoniae, C.pneumoniae or legionellosis is suspected.
6. Duration of therapy. Seven to 10 days should beadequate for routine pathogens causing uncom-plicated infection. Switch to oral therapy inpatients who have received parenteral antibiot-ics when the patient has become afebrile for 24to 48 hours and is able to keep down food.
C. Hospitalization. Children who are toxic,hypoxemic, dyspneic, apneic, significantlytachycardic for age, unable to feed, dehydrated, orhave an underlying condition that may be worsenedby the pneumonia require hospitalization. Hospital-ization should be considered for most children lessthan four months of age, unless a viral etiology issuspected and they are relatively asymptomatic.
IV. NeonatesA. Bacterial pneumonia in the first day of life may be
impossible to distinguish from hyaline membranedisease or transient tachypnea of the newborn.Therefore, respiratory distress in newborns shouldbe treated as bacterial pneumonia until provenotherwise. When associated with chorioamnionitis,it is caused most commonly by Escherichia coli orby group B streptococci (GBS). However,Haemophilus influenzae, Streptococcuspneumoniae (pneumococcus), group D strepto-cocci, Listeria, and anaerobes also may be presentin this setting.
B. Infants also may develop bacterial pneumoniatransnatally, secondary to GBS. The onset ofsymptoms tends to occur 12 to 24 hours after birth.
C. Chest radiographs of infants who have bacterialpneumonia may exhibit a diffuse reticular nodularappearance; but, in contrast to hyaline membranedisease, they tend to show normal or increased lungvolumes with possible focal or coarse densities.
D. In the newborn who has bacterial pneumonia, bloodcultures obtained before the initiation of antibioticscommonly grow the offending organism. Cultures ofurine and cerebrospinal fluid should be obtained atthe time of the blood culture.
E. Empiric treatment should be initiated withampicillin 100 mg/kg per day divided every 12 hours(infants <1.2 kg) or every 8 hours (infants >1.2 kg)and cefotaxime 100 mg/kg per day divided every 12hours or 150 mg/kg per day divided every 8 hours(infants >1.2 kg and >7 days old). Gentamicin is analternative. Treatment should be continued for atleast 10 days.
References, see page 182.
Bronchiolitis
Bronchiolitis is an acute wheezing-associated illness,which occurs in early life, preceded by signs and symp-toms of an upper respiratory infection. Infants may have asingle episode or may have multiple occurrences in thefirst year of life.
I. EpidemiologyA. Bronchiolitis occurs most frequently from early
November and continues through April.B. Bronchiolitis is most serious in infants who are less
than one year old, especially those 1-3 months old.Infants at risk include those who are raised incrowded living conditions, who are passively ex-posed to tobacco smoke, and who are not breast-fed.
II. PathophysiologyA. Respiratory syncytial virus (RSV) is the leading
cause of bronchiolitis in infants and young children,accounting for 50% of cases of bronchiolitis requir-ing hospitalization.
B. Infants born prematurely, or with chronic lung dis-ease (CLD), immunodeficiency or congenital heartdisease are at especially high risk for severe RSVillness.

C. RSV is transmitted by contact with nasal secretions.Shedding of virus occurs 1 to 2 days before symp-toms occur, and for 1 to 2 weeks afterwards. Symp-toms usually last an average of 5 days.
D. Parainfluenza viruses are the second-most-frequentcause of bronchiolitis. They cause illness duringautumn and spring, before and after outbreaks ofRSV. Influenza A virus, adenovirus, rhinovirus andMycoplasma pneumonia can all cause bronchiolitis.Rhinovirus and mycoplasma pneumonia causewheezing-associated respiratory illness in olderchildren, while parainfluenza virus and RSV cancause wheezing at any age.
III. Clinical evaluation of bronchiolitisA. Symptoms of RSV may range from those of a mild
cold to severe bronchiolitis or pneumonia. RSVinfection frequently begins with nasal discharge,pharyngitis, and cough. Hoarseness or laryngitis isnot common. Fever occurs in most young children,with temperatures ranging from 38E°C to 40E°C(100.4E°F to 104E°F).
B. Hyperresonance of the chest wall may be present,and wheezing can be heard in most infants withoutauscultation. The wheezing sound is harsh and lowin pitch, although severely affected infants may nothave detectable wheezing. Fine “crackles” areusually heard on inspiration. Substernal and inter-costal retractions are often noted.
C. Cyanosis of the oral mucosa and nail beds mayoccur in severely ill infants. Restlessness andhyperinflation of the chest wall are signs of impend-ing respiratory failure.
IV. DiagnosisA. Infants with bronchiolitis present symptoms of an
upper respiratory illness for several days and wheez-ing during the peak RSV season.
B. Chest radiography typically shows hyperexpansionand diffuse interstitial pneumonitis. Consolidation isnoted in about 25% of children, most commonly inthe right upper or middle lobe.
C. Oxygen saturation values of <95% suggest theneed for hospitalization.
D. Arterial blood gases should be obtained to assessthe severity of respiratory compromise. Carbondioxide levels are commonly in the 30-35 mm Hgrange. Respiratory failure is suggested by CO2
values of 45-55 mm Hg. Oxygen tension below 66mm Hg indicates severe disease.
E. White blood cell count may be normal or elevatedslightly, and the differential count may showneutrophilia.
F. Enzyme-linked immunosorbent assays (ELISA) ofnasal washings for RSV are highly sensitive andspecific.
V. ManagementA. Outpatient management of bronchiolitis is appropri-
ate for infants with mild disease.B. Criteria for hospitalization
1. History of prematurity (especially less than 34weeks).
2. Congenital heart disease.3. Other underlying lung disease4. Low initial oxygen saturation suggestive of respi-
ratory failure (O2 saturation <95%, with a toxic,distressed appearance).
5. Age <3 months.6. Dehydrated infant who is not feeding well.7. Unreliable parents.
C. Before hospitalization, infants should receive anaerosolized beta-adrenergic agent. A few infants willrespond to this therapy and avoid hospitalization. Ifthe response is good, the infant can be sent home,and oral albuterol continued.
D. Hospitalized infants should receive hydration andambient oxygen to maintain an oxygen saturation>92-93% by pulse oximetry.
E. Treatment of bronchiolitis in the hospital1. Racemic epinephrine by inhalation may be
administered as a therapeutic trial. It should becontinued if an improvement in the respiratorystatus is noted. Racemic epinephrine is adminis-tered as 0.5 mL of a 2.25% solution, diluted with3.5 mL of saline (1:8) by nebulization. It is givenevery 20-30 minutes for severe croup, and it isgiven every 4-6 hours for moderate croup.
2. Ribavirin, an antiviral agent, produces modest

improvement in clinical illness and oxygenation.Ribavirin is helpful in severely ill or high-riskpatients. The dosage is 2 gm (diluted to 60mg/mL) aerosolized over 2 hours tid for 3-5 daysusing an oxygen hood. Treatment with ribavirincombined with RSV immune globulin adminis-tered either parenterally or by aerosol is moreeffective than therapy with either agent alone.Corticosteroid use in the treatment of bronchiolitisis not recommended.
Indications for Ribavirin Use in Bronchiolitis
Congenital heart disease,especially cyanoticChronic lung diseaseRenal transplantation, recentAge <6 weeksNeurologic diseasesHeart failure of any causeRSV bronchiolitis and arterialO2 <65 mmHg
Immunodeficiency due tochemotherapyCystic fibrosisSevere combined immunode-ficiencyMultiple congenital anoma-liesCertain premature infantsMetabolic diseasesRSV bronchiolitis and a risingpCO2
VI. Prevention of RSV InfectionsA. Palivizumab (Synagis) is a humanized mouse
monoclonal antibody that is given intramuscularly.Palivizumab is administered intramuscularly in a doseof 15 mg/kg once a month during the RSV season.
Recommendations by the American Academy ofPediatrics for the use of palivizumab (Synagis)and RSV-IGIV:
C Palivizumab (Synagis) or RSV-IGIV prophylaxis should beconsidered for infants and children younger than 2 years ofage with chronic lung disease (CLD) who have requiredmedical therapy for CLD within 6 months before the antici-pated RSV season. Palivizumab is preferred for most high-risk children because of its ease of administration, safety,and effectiveness. Patients with more severe CLD maybenefit from prophylaxis for 2 RSV seasons, especiallythose who require medical therapy.
C Infants born at 32 weeks of gestation or earlier withoutCLD or who do not meet the aforementioned criteria alsomay benefit from RSV prophylaxis. Infants born at 28weeks of gestation or earlier may benefit from prophylaxisup to 12 months of age. Infants born at 29 to 32 weeks ofgestation may benefit most from prophylaxis up to 6months of age. Decisions about duration of prophylaxisshould be individualized according to the duration of theRSV season.
C For patients born between 32 and 35 weeks of gestation,the use of palivizumab and RSV IGIV should be reservedfor infants with additional risk factors.
C Prophylaxis for RSV should be initiated at the onset of theRSV season and terminated at the end of the RSV season.In most areas of the United States, the usual time for thebeginning of RSV outbreaks is October to December, andtermination is March to May, but regional differences occur.
C Palivizumab does not interfere with the response to vac-cines.
References, see page 182.

Pharyngitis
Approximately 30 to 65 percent of pharyngitis cases areidiopathic, and 30 to 60 percent have a viral etiology(rhinovirus, adenovirus). Only 5 to 10 percent of sorethroats are caused by bacteria, with group A beta-hemolytic streptococci being the most common. Otherbacteria that occasionally cause pharyngitis includegroups C and G streptococci, Neisseria gonorrhoeae,Mycoplasma pneumoniae, Chlamydia pneumoniae, andArcanobacterium haemolyticus.
I. Clinical presentation A. Pharyngitis caused by group A beta-hemolytic
streptococci has an incubation period of two to fivedays and is most common in children five to 12 yearsof age. The illness is diagnosed most often in thewinter and spring.
B. Group A beta-hemolytic streptococcal pharyngitisusually is an acute illness with sore throat and atemperature higher than 38.5EC (101.3EF). Constitu-tional symptoms include fever and chills, myalgias,headaches and nausea. Physical findings mayinclude petechiae of the palate, pharyngeal andtonsillar erythema and exudates, and anterior cervi-cal adenopathy.
C. Patients with cough or coryza, are less likely to havestreptococcal pharyngitis. A sandpaperlike rash onthe trunk, which is sometimes linear on the groin andaxilla (Pastia’s lines), is consistent with scarlet fever.
Features of Streptococcal Tonsillopharyngitis
Sudden onsetSore throat (pain on swallow-ing)FeverHeadacheNausea, vomiting, abdominalpain (especially in children)
Marked inflammation ofthroat and tonsilsPatchy discrete exudateTender, enlarged anteriorcervical nodesScarlet fever
Features rarely associated with streptococcaltonsillopharyngitis–suggestive of other etiologies
ConjunctivitisCoughLaryngitis (stridor, croup)
DiarrheaNasal discharge (except inyoung children)Muscle aches/malaise
II. Diagnostic TestingA. Throat culture is the gold standard for the diagnosis
of streptococcal pharyngitis. The sensitivity of throatculture for group A beta-hemolytic streptococci is 90percent. The specificity of throat culture is 99 per-cent.
B. A rapid antigen detection test (rapid strep test) canbe completed in five to 10 minutes. This test has aspecificity of greater than 95 percent but a sensitivityof only 76 to 87 percent.
C. A positive rapid antigen detection test may beconsidered definitive evidence for treatment ofstreptococcal pharyngitis. A confirmatory throatculture should follow a negative rapid antigen detec-tion test when the diagnosis of group A beta-hemolytic streptococcal infection is strongly sus-pected.
Complications of Group A Beta-Hemolytic Strep-tococcal Pharyngitis
Nonsuppurative complications
Rheumatic feverPoststreptococcal glomerulonephritis
Suppurative complications
Cervical lymphadenitisPeritonsillar orretropharyngeal abscessSinusitisMastoiditis
Otitis mediaMeningitisBacteremiaEndocarditisPneumonia
D. The annual incidence of acute rheumatic fever isone case per 1 million population. Suppurativecomplications of streptococcal pharyngitis occur asinfection spreads from pharyngeal mucosa to

deeper tissues.III. Antibiotic Therapy
Selected Antibiotic Regimens for Group A Beta-Hemolytic Streptococcal Pharyngitis
Antibiotic Dose/dosageDosing fre-quency Duration
Penicillin V(Veetids)
Child: 250 mg Two orthree timesdaily
10 days
Adult: 500 mg Two orthree timesdaily
10 days
Penicillin Gbenzathine(Bicillin L-A)
Child: 600,000units
Single injec-tion
--
Adult: 1,200,000units
Single injec-tion
--
Amoxicillin(Amoxil)
Child: 40 mg perkg per day
Three di-vided doses
10 days
Adult: 500 mg Three timesdaily
10 days
Erythromycinethylsuccinate (E.E.S.400)
Child: 40 mg perkg per day
Two to fourdivideddoses
10 days
Adult: 400 mg Four timesdaily
10 days
Erythromycinestolate
Child: 20 to 40mg per kg perday
Two to fourdivideddoses
10 days
Adult: not rec-ommended
-- --
Azithromycin(Zithromax)
Child: 10 mg perkg on day 1; 5mg per kg ondays 2 through5
Once daily 5 days
Adult: 500 mgon day 1; 250mg on days 2through 5
Once daily 5 days
Amoxicillin-clavulanatepotassium(Augmentin)
Child: 40 mg perkg per day
Two orthree di-vided doses
10 days
Adult: 500 to875 mg
Two timesdaily
10 days
Cefadroxil(Duricef)
Child: 30 mg perkg per day
Two divideddoses
10 days
Adult: 1 g Once daily 10 days
Cephalexin(Keflex)
Child: 25 to 50mg per kg perday
Two to fourdivideddoses
10 days
Adult: 500 mg Two timesdaily
10 days
A. Penicillin is the drug of choice for streptococcalpharyngitis. This antibiotic has efficacy and safety,a narrow spectrum of activity and low cost. About 10percent of patients are allergic to penicillin. Curerates are similar for 250 mg of penicillin V giventwo, three or four times daily. The use of intramus-cularly administered penicillin may overcomecompliance problems.
B. Alternatives to penicillin1. Amoxicillin
a. In children, the cure rates for amoxicillin givenonce daily for 10 days are similar to those forpenicillin V. The absorption of amoxicillin isunaffected by the ingestion of food.
b. Amoxicillin is less expensive and has a nar-rower spectrum of antimicrobial activity thanthe once-daily antibiotics. Suspensions of thisdrug taste better than penicillin V suspen-sions, and chewable tablets are available.However, gastrointestinal side effects and skinrash may be more common with amoxicillin.

2. Macrolidesa. Erythromycin is recommended in patients with
penicillin allergy. Because erythromycinestolate is hepatotoxic in adults, erythromycinethylsuccinate may be used. Erythromycin isabsorbed better when it is given with food.About 15 to 20 percent of patients cannottolerate the gastrointestinal side effects oferythromycin.
b. Azithromycin (Zithromax) allows once-dailydosing and a shorter treatment course of fivedays. Azithromycin is associated with a lowincidence of gastrointestinal side effects.
3. Cephalosporins a. A 10-day course of a cephalosporin has been
shown to be superior to penicillin. The overallbacteriologic cure rate for cephalosporins is92 percent, compared with 84 percent forpenicillin.
b. Cephalosporins have a broader spectrum ofactivity than penicillin V. Unlike penicillin,cephalosporins are resistant to degradationfrom beta-lactamase. First-generation agentssuch as Cefadroxil (Duricef) and cephalexin(Keflex, Keftab) are preferable to second- orthird-generation agents.
c. Cephalosporins are reserved for patients withrelapse or recurrence of streptococcal pharyn-gitis.
4. Amoxicillin-clavulanate (Augmentin) is resis-tant to degradation from beta-lactamase pro-duced by copathogens. Amoxicillin-clavulanate isoften used to treat recurrent streptococcal phar-yngitis. Its major adverse effect is diarrhea.
IV. Management IssuesA. Treatment Failure and Reinfection. Patients who
do not comply with a 10-day course of penicillinshould be offered intramuscular penicillin or a once-daily oral macrolide or cephalosporin. Patients withclinical failure should be treated with amoxicillin-clavulanate, a cephalosporin, or a macrolide.
B. Contagion. Patients with streptococcal pharyngitisare considered contagious until they have beentaking an antibiotic for 24 hours. Children shouldnot go back to day care or school until their temper-ature returns to normal and they have had at least24 hours of antibiotic therapy.
References, see page 182.
Acute Conjunctivitis
Conjunctivitis is defined as inflammation of the conjunc-tiva; it is usually caused by infection or allergy. It is oftenreferred to as “pink eye.”
I. EtiologyA. Neonatal conjunctivitis occurs in 1.6-12% of new-
borns. The most common cause is chemical irritationfrom antimicrobial prophylaxis against bacterialinfection, followed by Chlamydia trachomatis infec-tion. Haemophilus influenzae and Streptococcuspneumoniae may also cause infection in newborns.
B. Rarely, gram-negative organisms, such as Esche-richia coli, Klebsiella, or Pseudomonas sp can causeneonatal conjunctivitis. Neisseria gonorrhoeae is anunusual cause of neonatal conjunctivitis because ofthe use of ocular prophylaxis.
C. Herpes simplex can cause neonatalkeratoconjunctivitis; however, it is almost alwaysassociated with infection of the skin and mucousmembranes, or with disseminated disease.
D. In older infants and children, H influenzae is by farthe most common identifiable cause of conjunctivitis,causing 40-50% of episodes. S pneumoniae ac-counts for 10% of cases, and Moraxella catarrhalisis the third most common cause.
E. Adenovirus is the most important viral cause ofacute conjunctivitis. This organism often causesepidemics of acute conjunctivitis. It causes 20% ofchildhood conjunctivitis (most occurring in the falland winter months).
II. Clinical presentationA. In the first day of life, conjunctivitis is usually
caused by chemical conjunctivitis secondary toocular prophylaxis.

B. Three to 5 days after birth, gonococcal conjunctivi-tis is the most common cause of conjunctivitis.
C. After the first week of life and throughout thefirst month, chlamydia is the most frequent cause ofconjunctivitis. Severe cases are associated with athick mucopurulent discharge and pseudomembraneformation.
D. Gonococcal conjunctivitis can present as typicalbacterial conjunctivitis, or as a hyperacute conjuncti-vitis with profuse purulent discharge. There often issevere edema of both lids.
E. In the older infant and child, both viral and bacterialconjunctivitis may present with an acutely inflamedeye. Typically, there is conjunctival erythema, withoccasional lid edema. Exudate often accumulatesduring the night.
F. Many patients who have both adenoviral conjunctivi-tis and pharyngitis also are febrile. The triad ofpharyngitis, conjunctivitis, and fever has beentermed pharyngoconjunctival fever.
III. DiagnosisA. Neonates
1. In cases of neonatal conjunctivitis, a Gram stainand culture should be obtained to exclude Ngonorrhoeae conjunctivitis.
2. Chlamydia trachomatis antigen detection assayshave a sensitivity and specificity of 90%.
B. Infants and older children. Outside the neonatalperiod, a Gram stain is usually not needed unlessthe conjunctivitis lasts longer than 7 days. Thepresence of vesicles or superficial corneal ulcer-ations suggests herpetic keratoconjunctivitis.
IV. Differential diagnosis of conjunctivitisA. Systemic diseases. Most cases of red eye in
children are caused by acute conjunctivitis, allergy,or trauma; however, Kawasaki disease, Lymedisease, leptospirosis, juvenile rheumatoid arthritis,and Stevens-Johnson syndrome may cause con-junctivitis. Glaucoma is a significant cause of a redeye in adults; however, it is rare in children.
B. Allergic conjunctivitis1. Allergic eye disease is characterized by pro-
nounced ocular itching, redness, tearing, andphotophobia. This recurrent disease has seasonalexacerbations in the spring, summer, and fall.Children who have allergic conjunctivitis oftenhave other atopic diseases (rhinitis, eczema,asthma) and a positive family history.
2. Treatmenta. Topical decongestants: Naphazoline 0.1%
(Naphcon), phenylephrine (Neo-Synephrine),and oxymetazoline (OcuClear, Visine LR) maybe used qid, alone or in combination withophthalmic antihistamines, such as antazoline(Vasocon-A) or pheniramine maleate (Naph-Con-A).
b. Topical lodoxamide (Alomide) 0.1% ophthalmicsolution, 1-2 drops qid, is helpful in moresevere cases.
c. Topical corticosteroids are helpful, butlong-term use is not recommended; dexameth-asone (Decadron) 1-2 drops tid-qid.
V. Treatment of acute infectious conjunctivitisA. Gonococcal ophthalmia neonatorum is treated with
ceftriaxone (50 mg/kg/day IV/IM q24h) or cefotaxime(100 mg/kg/day IV/IM q12h) for 7 days.
B. Neonatal conjunctivitis caused by C trachomatis istreated with erythromycin, 50 mg/kg/day PO dividedin 4 doses for 14 days.
C. Bacterial conjunctivitis among older infants andchildren is treated with polymyxin-bacitracin(Polysporin) ointment, applied to affected eye tid.
References, see page 182.
Cat and Dog Bites
Bite wounds account for approximately 1% of all emer-gency department visits: 10% of victims require suturingand 1-2% require hospitalization.
I. PathophysiologyA. Dog bites account for 80-90% of animal bites.
Infection develops in15-20% of dog bite wounds.B. Cat bites account for 15% of animal bites. Cat bites
usually present as puncture wounds, of which 30-
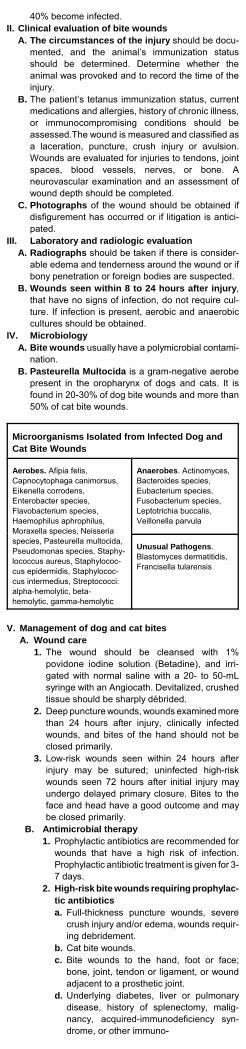
40% become infected.II. Clinical evaluation of bite wounds
A. The circumstances of the injury should be docu-mented, and the animal’s immunization statusshould be determined. Determine whether theanimal was provoked and to record the time of theinjury.
B. The patient’s tetanus immunization status, currentmedications and allergies, history of chronic illness,or immunocompromising conditions should beassessed.The wound is measured and classified asa laceration, puncture, crush injury or avulsion.Wounds are evaluated for injuries to tendons, jointspaces, blood vessels, nerves, or bone. Aneurovascular examination and an assessment ofwound depth should be completed.
C. Photographs of the wound should be obtained ifdisfigurement has occurred or if litigation is antici-pated.
III. Laboratory and radiologic evaluationA. Radiographs should be taken if there is consider-
able edema and tenderness around the wound or ifbony penetration or foreign bodies are suspected.
B. Wounds seen within 8 to 24 hours after injury,that have no signs of infection, do not require cul-ture. If infection is present, aerobic and anaerobiccultures should be obtained.
IV. MicrobiologyA. Bite wounds usually have a polymicrobial contami-
nation.B. Pasteurella Multocida is a gram-negative aerobe
present in the oropharynx of dogs and cats. It isfound in 20-30% of dog bite wounds and more than50% of cat bite wounds.
Microorganisms Isolated from Infected Dog andCat Bite Wounds
Aerobes. Afipia felis,Capnocytophaga canimorsus,Eikenella corrodens,Enterobacter species,Flavobacterium species,Haemophilus aphrophilus,Moraxella species, Neisseriaspecies, Pasteurella multocida,Pseudomonas species, Staphy-lococcus aureus, Staphylococ-cus epidermidis, Staphylococ-cus intermedius, Streptococci:alpha-hemolytic, beta-hemolytic, gamma-hemolytic
Anaerobes. Actinomyces,Bacteroides species,Eubacterium species,Fusobacterium species,Leptotrichia buccalis,Veillonella parvula
Unusual Pathogens.Blastomyces dermatitidis,Francisella tularensis
V. Management of dog and cat bitesA. Wound care
1. The wound should be cleansed with 1%povidone iodine solution (Betadine), and irri-gated with normal saline with a 20- to 50-mLsyringe with an Angiocath. Devitalized, crushedtissue should be sharply débrided.
2. Deep puncture wounds, wounds examined morethan 24 hours after injury, clinically infectedwounds, and bites of the hand should not beclosed primarily.
3. Low-risk wounds seen within 24 hours afterinjury may be sutured; uninfected high-riskwounds seen 72 hours after initial injury mayundergo delayed primary closure. Bites to theface and head have a good outcome and maybe closed primarily.
B. Antimicrobial therapy1. Prophylactic antibiotics are recommended for
wounds that have a high risk of infection.Prophylactic antibiotic treatment is given for 3-7 days.
2. High-risk bite wounds requiring prophylac-tic antibioticsa. Full-thickness puncture wounds, severe
crush injury and/or edema, wounds requir-ing debridement.
b. Cat bite wounds.c. Bite wounds to the hand, foot or face;
bone, joint, tendon or ligament, or woundadjacent to a prosthetic joint.
d. Underlying diabetes, liver or pulmonarydisease, history of splenectomy, malig-nancy, acquired-immunodeficiency syn-drome, or other immuno-

compromising condition.
Prophylactic Antibiotics for Dog and Cat Bites
Outpatient Antibiotics
Cephalexin(Keflex)
Adults: 500 mg qidChildren: 40 mg/kg/d PO qid
Doxycycline(Vibramycin)
Adults: 100 mg bidChildren: 2-4 mg/kg/day, in divideddoses bid
Amoxicillin/clavulanate(Augmentin)
Adults: 500 mg tidChildren: 40 mg amoxicillin/kg/day, individed doses tid
Ceftriaxone(Rocephin)
Adults: 1 g every 24 hours IM or IVChildren: 50 mg/kg/d qd
Penicillin V Adults: 500 mg qidChildren: 50 mg/kg/day, in divided dosesq6-8h
Amoxicillin Adults: 500 mg tidChildren: 40 mg/kg/d, in divided dosestid
Intravenous Antibiotic of Choice
Cefoxitin(Mefoxin)
Adults: 1-2 g q4-8hChildren: 25-50 mg/kg/day, in divideddoses q6h
Alternative Intravenous Antibiotics
Ampicillin/sulbactam (Unasyn)
Adults: 1.5-3.0 g q6h
Ticarcillin-clavulanate(Timentin)
Adults: 3.1 g q6h
Ceftriaxone(Rocephin)
Adults: 1-2 g q24hChildren: 50-100 mg/kg/day, in divideddoses q24h
C. Treatment of infected wounds. Infected bitewounds are treated with amoxicillin/clavulanate (Augmentin). Cellulitis is treated for 10-14 days.
D. Rabies immunoprophylaxis1. The incidence of rabies in persons who have
been bitten by a dog is very low because mostdogs have been vaccinated. An untreated personhas a less than 20% chance of contracting rabiesfrom the bite of a rabid animal. However, if rabiesis contracted, the mortality rate is 100%.
2. Wild animals (raccoons, skunks, bats) are themost common source of rabies. Rabies is trans-mitted when the saliva of an infected animalcomes into contact with the broken skin or mu-cosa of another mammal. The incubation periodranges from 10 days to one year.
3. If rabies infection is suspected, rabies prophy-laxis is administered as follows:a. Rabies immune globulin (RIG), 20 IU/kg, IM
(separate from human diploid cell vaccinebelow).
b. Human diploid cell vaccine (HDCV), 1 cc IM(not gluteal) given on days 1, 3, 7, 14, and 28.
E. Tetanus Immunization. Animal bites should beregarded as tetanus prone, although tetanus infec-tion resulting from cat and dog bites is rare.
References, see page 182.
Peripheral Lymphadenopathy inChildren
Palpable lymph nodes are often found in children becausetheir immune systems are being activated by environmen-tal antigens and the common organisms.Lymphadenopathy is caused by reactive hyperplasia ofundetermined etiology in 50%. Nearly one-third of childrenhave granulomatous diseases, including cat scratchdisease, mycobacterial infections, fungal infections, orLangerhans cell histiocytosis (histiocytosis X). Thirteenpercent have neoplastic diseases, such as Hodgkindisease. Chronic dermatopathic or bacterial infections

comprised the remaining 3 percent of patients. Only 20percent of biopsies will demonstrate a treatable disease.
I. Anatomy and definitions Normal lymph nodes usuallyare less than 1 cm in diameter. Lymph nodes often arepalpable in the inguinal region in healthy individuals,perhaps because chronic trauma and infection arecommon in the lower extremities. Nodes also may bepalpable in the neck (particularly submandibular)because of previous head and neck infections.A. Lymphadenopathy should be classified as localized
(in only one region such as the neck or axilla) orgeneralized (more than one region).
II. Differential diagnosis. Lymphadenopathy can becaused by a vast array of diseases and drugs.A. Localized
1. Cervical. The anterior cervical lymph nodes oftenare enlarged because of a variety of infections ofthe head and neck, or because of a systemicinfection, such as toxoplasmosis and infectiousmononucleosis caused by Epstein-Barr virus orcytomegalovirus. Only one-quarter of patients withenlarged cervical nodes have another seriousdisease, which most often is mycobacterial. Upperposterior cervical lymphadenopathy rarely isassociated with significant diseases in children.
a. Inflamed cervical nodes that develop over a fewdays and progress to fluctuation, especially inchildren, typically are caused by staphylococcaland streptococcal infection. Treatment beginsfirst with a course of antibiotics, often dicloxacillin,but incision and drainage may be indicated.Fluctuant cervical nodes that develop over weeksto months without significant inflammation ortenderness suggest infection with Mycobacteriumtuberculosis, atypical mycobacteria, or Bartonellahenselae, the agent of cat scratch disease.
b. Hard nodes, often associated with cancer inadults, are found infrequently in children. Thenodes involved with Hodgkin disease are rub-bery.
Infectious Etiologies of Cervical Adenitis
Bacterial Viral Fungal/protozoal
Other
Localized Acute
Staphylococcusaureus StreptococcuspyogenesGroup B strepto-coccusAnaerobesFrancisellatularensis
RubellaAdenovi-rusesHerpessimplexvirusMumpsHumanherpesvirus6
ToxoplasmosisHistoplasmosis
Kawasakisyn-dromeRickett-sial pox
Subacute or Chronic
TuberculosisAtypical myco-bacteriaCat-scratch dis-ease
SyphilisActinomycosisNocardiosis
Brucellosis
Generalized
SyphilisTuberculosisScarlet feverTyphoid fever LeptospirosisBrucellosis virus
HIVEpstein-BarrCytomegalovirusMeaslesRubellaVaricellaAdenovirus
Histoplasmosis Toxoplasmosis
Rickett-sialScrubtyphus
Organism Associated with Infectious CervicalLymphadenitis
Neonates
Staphylococcus aureusGroup B streptococcal “cellulitis-adenitis” syndrome
Infancy
As aboveKawasaki syndrome

1 to 4 Years
Staphylococcus aureusStreptococcus pyogenesAtypical mycobacteria
5 to 15 years
Anaerobic bacteriaToxoplasmosisCat-scratch diseaseTuberculosis
Causes of Peripheral Lymphadenopathy
Cause Examples
Infections
Bacterial
Localized Streptococcal pharyngitis; skininfections; tularemia;
plague; cat scratch fever dis-ease; diphtheria; chancroid;rat bite fever
Generalized Brucellosis; leptospirosis;lymphogranuloma
venereum; typhoid fever
Viral Human immunodeficiency virus;Epstein-Barr virus;
herpes simplex virus;cytomegalovirus; mumps;measles; rubella; hepatitis B;dengue fever
Mycobacterial Mycobacterium tuberculosis;atypical mycobacteria
Fungal H i s t o p l a s m o s i s ;coccidiodomycosis; crypto-coccus
Protozoal Toxoplasmosis
Spirochetal Secondary syphilis; Lyme dis-ease
Cancer Metastatic; lymphoma; leukemia
Lymphoproliferative
A n g i o i m m u n o b l a s t i cl y m p h a d e n o p a t h y w i t hdysproteinemiaAutoimmune lymphoroliferativediseaseRosai-Dorfmans’s diseaseH e m o p h a g o c y t i clymphohistiocytosis
Immunologic Serum sickness; drug reactions(phenyutoin)
Endocrine Hypothyroidism; Addison’s dis-ease
Miscellaneous Sarcoidosis; lipid storage dis-eases; amyloidosis;
h is t iocytos is ; chron icgranulomatous diseases;Cast lemans ’ d i sease ;Kikuchi’s disease; Kawasakid isease; in f lammatorypseudotumor; systemic lupuserythematosus; rheumatoidarthritis; Still’s disease;dermatomysositis; Churg-Strauss syndrome

Drugs That Cause Lymphadenopathy
AllopurinolAtenololCaptoprilCarbamazepine
CephalosporinsGoldHydralazine
PenicillinPhenytoinPrimidonePyrimethamineQuinidineSulfonamidesSulindac
Causes of Generalized Lymphadenopathy
Mononucleosis syn-dromesHIV infectionSecondary SyphilisHepatitis BTuberculosisLyme DiseaseMeaslesRubellaBrucellosisTyphoid fever
Systemic lupuserythematosusRheumatoid arthritisStill’s diseaseKawasaki diseaseDermatomyositisAmyloidosisSerum sicknessLeukemiaLymphoma
2. Supraclavicular (or lower cervical)lymphadenopathy is associated with a high risk ofmalignancy (up to 75 percent). Rightsupraclavicular adenopathy is associated withcancer of the mediastinal lymph nodes. Leftsupraclavicular adenopathy (“Virchow’s node”)suggests abdominal malignancy, also most oftena lymphoma.
3. Axillary. The axillary nodes receive drainage fromthe arm, thoracic wall, and breast. Infections,including cat scratch disease, are common causesof axillary lymphadenopathy, although hyperplasticnodes are found in over one-third.
4. Inguinal lymphadenopathy in children usually isassociated with no specific etiology unless thenodes are very large (>3 cm).
5. Epitrochlear. Palpable epitrochlear nodes are notalways pathologic in children, and many biopsiednodes show only hyperplasia. Other causes in-clude infections of the forearm or hand, leukemia,lymphoma, and atypical mycobacterial infections.
B. Generalized lymphadenopathy1. HIV. Nontender adenopathy primarily involving the
axillary, cervical, and occipital nodes develops inthe majority of individuals during the second weekof acute symptomatic HIV infection. The nodesdecrease in size after the acute presentation, buta modest degree of adenopathy tends to persist.
2. Mycobacterial infection can present withlymphadenopathy alone, especially in the neck(scrofula). Mycobacterium avium complex and M.scrofulaceum, account for most cases in children.Nodes typically are nontender, enlarge over weeksto months and can progress to matting and fluctua-tion. Miliary tuberculosis may cause generalizedlymphadenopathy.
3. Mononucleosis is characterized by the triad ofmoderate to high fever, pharyngitis, andlymphadenopathy. Lymph node involvement issymmetric and involves the posterior cervical morethan the anterior chain. Lymphadenopathy alsomay be present in the axillary and inguinal areas,which helps to distinguish infectious mononucleo-sis from other causes of pharyngitis. Nodes arekidney-shaped.
4. Systemic lupus erythematosus. Enlargement oflymph nodes occurs in 50 percent of patients withsystemic lupus erythematosus (SLE). The nodestypically are soft, nontender, discrete, varying insize from 0.5 to several centimeters, and usuallydetected in the cervical, axillary, and inguinalareas.
5. Medications may cause serum sickness that ischaracterized by fever, arthralgias, rash, andgeneralized lymphadenopathy. Phenytoin cancause generalized lymphadenopathy.
III. Diagnostic approachA. History
1. Localizing signs or symptoms suggestive of infec-tion or malignancy.
2. Exposures (eg, cat [cat scratch disease], under-

cooked meat [toxoplasmosis], tick bite [Lymedisease]), travel, high-risk behavior (eg, sexualbehavior, injection drug use).
3. Constitutional symptoms such as fever, nightsweats, or weight loss suggestive of tuberculosis,lymphoma, or other malignancy; fever typicallyaccompanies lymphadenopathy for the majority ofthe infectious etiologies.
4. Use of medications that can causelymphadenopathy.
B. Physical examination1. Location. Palpation of inguinal, cervical, and
axillary nodes, in addition to the liver and spleen,can determine whether it is truly locallymphadenopathy.
2. Size. Abnormal nodes generally are greater than1 cm in diameter. Malignancy is more likely to befound in nodes larger than 2 cm.
3. Consistency. Hard nodes are found in cancersthat induce fibrosis (scirrhous changes) and whenprevious inflammation has left fibrosis. Firm,rubbery nodes are found in lymphomas andchronic leukemia; nodes in acute leukemia tend tobe softer.
4. Fixation. Normal lymph nodes are freely movablein the subcutaneous space. Abnormal nodes canbecome fixed to adjacent tissues (eg, deep fascia)by invading cancers or inflammation. They alsocan become fixed to each other (“matted”).
5. Tenderness suggests recent, rapid enlargementthat has put pain receptors in the capsule undertension. This situation typically occurs with inflam-matory processes, but it also can occur because ofhemorrhage into a node, immunologic stimulation,and malignancy.
C. Diagnostic tests1. Patients with generalized lymphadenopathy should
have a CBC and chest radiograph. If these testsare normal, other considerations include an eryth-rocyte sedimentation rate, serologic test for acuteEBV and CMV infections, PPD, HIV antibodydetermination, RPR, ANA, and heterophile test.
2. Patients with localized (especially cervical)lymphadenopathy can be observed for three tofour weeks and treated empirically with antibiotics(first- or second-generation cephalosporin ordicloxacillin) if nothing else in the history andphysical examination suggests malignancy. Biopsyis appropriate if an abnormal node has not re-solved after four weeks, or immediately in patientswith other findings suggestive of malignancy.
3. Incision and drainage. Fluctuant nodes may benecessary to relieve pain and treat obvious infec-tion.
Treatment of Acute Pyogenic BacterialLymphadenitis
Symptomatic Therapy
1. Apply warm, moist dressings2. Prescribe analgesics3. Incise and drain nodes that have suppuration

Antimicrobial Therapy
Suspected staphylococcal/group A and B streptococcaldisease
Cellulitis or marked enlargement, moderate-to-severesystemic symptoms, or in infants 1 mo of age:IV Nafcillin (Nafcil) 150 mg/kg day ORIV Cefazolin (Ancef) 150 mg/kg/day after aspiration ofnode
Suppuration:IV antibiotics as above and incision and drainage
No prominent systemic symptoms, cellulitis, or sup-puration:
Dicloxacillin (Dynapen) 25 mg/kg/day ORCephalexin (Keflex) 50 mg/kg/day ORClindamycin (Cleocin) 30 mg/kg/day
Suspected anaerobic infection with dental or periodontaldisease, include:
Penicillin V 50 mg/kg/day orClindamycin (Cleocin) 30 mg/kg/day OR
Group A streptococcal infectionAqueous penicillin G 50 000 IU/kg/day IV ORPenicillin V 50 mg/kg/day PO ORCephalexin 50 mg/kg/day PO ORErythromycin ethylsuccinate 40 mg/kg/day PO
Group B streptococcal disease in infantsAqueous penicillin G 200 000 IU/kg/day IV, if sensitive.
References, see page 182.
Intestinal Helminths
Intestinal helminth infestations most commonly affecttravelers, migrant laborers, refugees, children of foreignadoptions, and the homeless. These parasitic infectionsare associated with day-care centers and overseas travel.
I. Clinical evaluationA. Intestinal helminth infections are usually asymp-
tomatic, but serious infections may cause symptomsranging from abdominal discomfort to severe pain.Anorexia, nausea, diarrhea, pruritus, rectal prolapse,bowel obstruction, and death may occur. Hives andeosinophilia may develop, and the worms maysometimes spontaneously exit the body through theanus.
B. Stool examination. Examination of the stool for ovaand parasites is the most important test forhelminthic infection. Stools are collected usingplastic wrap under the toilet seat. Fresh stool mayalso be obtained by rectal examination.
II. EnterobiasisA. The pinworm (Enterobius vermicularis) is the
most common helminth. Pinworms present as analpruritus in irritable children. The disorder tends tooccur in temperate climates. Many patients areasymptomatic. Heavier infections may cause insom-nia, restlessness, vulvovaginitis, loss of appetite,and intractable anal itching.
B. Pinworms are about 10 mm in length. The femaleworm has a pin-shaped tail. At night, worms migratethrough the anus, then deposit their eggs and die onthe perianal skin. Microscopic eggs infest clothing,bedding, and other surfaces, often spreading to theentire family.
C. Pinworms are diagnosed by examining the perianalskin. The stool is usually negative for ova andworms. To obtain the eggs, a tongue blade coveredwith clear tape is placed sticky-side down over theperianal skin in the morning. Specimens are collect-ed on three separate mornings, then taped to glassslides and taken to a laboratory for examination.
D. The elongate, colorless eggs measure 50 to 60 µmand are flattened on one side. Worms may also bevisualized if the anus is examined late at night orearly in the morning.
E. Treatment1. Mebendazole (Vermox), one 100-mg tablet
orally, is safe and effective. A second dose isgiven 10 days later. The entire family is treated.
2. Infested clothing and bedding are washed andfingernails should be kept trimmed, and theperianal area kept clean. Dogs and cats do notspread this infection. Relapses are common.
III. AscariasisA. Roundworms (Ascaris lumbricoides) measure up
to 18 inches in length. The infection is fairly commonin the rural southeastern United States and is fre-quent among immigrants. A. lumbricoides only

infests humans.B. Ascaris eggs reach the soil in feces, and they may
persist in the soil for more than a decade until theyare accidentally consumed. In the gut, worms maycause intestinal obstruction. However, most patientsexperience only vague abdominal discomfort ornausea.
C. Treatment1. Mebendazole (Vermox), 100 mg bid for three
days.2. A follow-up examination of stool for ova and
parasites should be performed in two months.Family screening is recommended.
IV. TrichuriasisA. Whipworm (Trichuris trichiura) infestation is less
common than Ascaris infestation, occurring in thesoutheastern states and in foreign immigrants.
B. Whipworm eggs incubate in the soil. When swal-lowed, they travel to the colon.
C. Adult whipworms are 30-50 µm in length, with athread-like anterior portion. They can live in theintestine and produce eggs for several years, caus-ing mild blood loss and symptoms similar to proctitisand inflammatory bowel disease. Rectal prolapse,diarrhea, loss of appetite, and hives may occur.
D. Treatment of trichuriasis is the same as forascariasis.
V. Less common parasitesA. Hookworms
1. Hookworms develop in the soil from eggs infeces. The larvae are capable of penetrating thebare feet and causing a pruritic rash. The larvaeeventually reach the small intestine.
2. Adult hookworms are about 10 µm in length, witha hooked anterior end, which they use to con-sume 0.03-0.15 mL of blood per day for 10 to 15years. Manifestations include iron deficiencyanemia, chronic fatigue, geophagia, failure tothrive, and depression.
3. Treatment consists of mebendazole as describedabove and iron supplementation.
B. Strongyloidiasis1. Filariform larvae are capable of penetrating intact
skin, persisting for 40 years or more in the smallintestine. It can also be spread in feces or as asexually transmitted disease. Persistent unex-plained eosinophilia in a patient from a regionwhere Strongyloides infection is endemic shouldprompt serologic testing because stool specimensare often negative.
2. Symptoms are usually absent but may includepruritus, pneumonia, abdominal cramping, andcolitis. Treatment consists of thiabendazole(Mintezol).
C. Tapeworms1. Beef tapeworm is transmitted by inadequately
cooked beef, reaching up to 10 to 15 feet inlength in the gut. Diagnosis is made by passageof ribbon-like tapeworm segments or by findingthe eggs in a stool.
2. Pork tapeworm is far more dangerous than T.saginata since its eggs can cause cysticercosis,the invasion of human tissue by larval forms. Insevere cases, the larvae may invade the centralnervous system, causing neurocysticercosis.a. Pork tapeworm is found in immigrants from
Central and South America. Patients withneurocysticercosis frequently present withseizures.
b. This diagnosis should be considered in theevaluation of a patient from Central or SouthAmerica with a new-onset seizure disorder.
3. Dwarf tapeworm is the most common tapewormin the U.S. This tapeworm is 1 inch in length.Ingestion of food contaminated with mouse drop-pings may spread the infection. H. nana infectionmay cycle in immigrant children for years.
4. Fish tapeworm is occasionally transmitted byundercooked fish, especially from the GreatLakes region. It can occasionally causesmegaloblastic anemia.
5. Treatment of all tapeworms consists ofpraziquantel (Biltricide) or niclosamide(Niclocide).
References, see page 182.

Orbital and Periorbital Cellulitis
Periorbital cellulitis is a bacterial infection of the skin andstructures superficial to the orbit; orbital cellulitis is abacterial infection of the orbit.
I. Pathogenesis of periorbital cellulitisA. The most common causes of eyelid redness and
swelling are allergy, trauma, and insect stings orbites. Periorbital cellulitis usually occurs after theskin near the eye has been broken by trauma, aninsect bite, or infection with herpes simplex orvaricella zoster viruses. The organisms that mostfrequently cause periorbital cellulitis followingtrauma are Staphylococcus aureus and Streptococ-cus pyogenes (group A beta-hemolytic strepto-cocci).
B. A bacterial pathogen is identified in only 30% ofcases of periorbital cellulitis, and the pathogen isisolated from the blood in about two thirds of thesecases.
C. Since the introduction of H influenzae type b conju-gate vaccines (HbCV), Hib disease accounts forfewer than 15% of periorbital cellulitis. A child whohas received a second dose of HbCV more than 1week before the onset of eyelid swelling is veryunlikely to have HIB disease.
II. Pathogenesis of orbital cellulitisA. Orbital cellulitis may progress to subperiosteal
abscess, orbital abscess, and cavernous sinusthrombosis.
B. About one-fourth of isolates are S aureus; one-fifth,S pyogenes; one-fifth, HiB; one-tenth, Spneumoniae; one-tenth, anaerobic bacteria; and theremaining 15%, other bacteria.
III. Clinical evaluationA. Periorbital cellulitis usually occurs in children youn-
ger than 2 years of age. Clinical findings include atemperature of 39°C or more and a peripheral whiteblood cell count of greater than 15,000/mm³.
B. Periorbital and orbital cellulitis cause eyelid swelling,with the swelling being unilateral in 95-98% ofcases. Virtually all involved eyelids will beerythematous or violaceous.
C. Signs of trauma or local infection are observed inone-third of patients. When conjunctival inflamma-tion, a purulent discharge, and bilateral lid involve-ment are present, the cause is much more likely tobe conjunctivitis, rather than periorbital or orbitalcellulitis.
D. Globe displacement (proptosis), abnormalmovement (ophthalmoplegia), or pain on move-ment should be sought, and visual acuity should betested.
E. Laboratory evaluation1. White blood cell count greater than 15,000/mm³
suggests bacteremic disease.2. Lumbar puncture should be performed on all
children younger than 1 year of age who have nothad at least two doses of H influenzae B vaccine.
3. Blood culture for bacterial pathogens shouldbe obtained.
IV. TreatmentA. Orbital cellulitis. Children who have signs of orbital
cellulitis should be hospitalized, and antimicrobialtherapy should consist of a third-generationcephalosporin, such as ceftriaxone (50 mg/kg qd IMor IV) or cefotaxime (50 mg/kg/dose q6h IV), plusclindamycin (10 mg/kg/dose q8h IV).
B. Periorbital cellulitis1. Periorbital cellulitis can be managed on an outpa-
tient basis if there is no orbital involvement andthe child does not appear toxic.
2. Ceftriaxone (50 mg/kg, not to exceed 1 g) isgiven IM or IV. If the blood culture remains nega-tive, the child may be started on abroad-spectrum oral agent such asampicillin/clavulanate (Augmentin) or Trimeth-oprim/sulfamethoxazole (Bactrim) to complete a7- to 10-day course of therapy.
References, see page 182.

Tuberculosis
The number of cases of tuberculosis in children youngerthan five years of age in cities has increased 94.3% in thelast four years.
I. Natural history of tuberculosisA. Tuberculosis infection is initiated by the inhalation of
organisms into the lung. During an incubationperiod, that lasts 2 to 10 weeks, the organismsspread to the hilar lymph nodes. This condition isconsidered primary tuberculosis. During the incuba-tion period, the purified protein derivative (PPD) testusually becomes positive.
B. Primary tuberculosis is often completely asymp-tomatic, and the chest radiograph may be only mini-mally abnormal, with hilar adenopathy, and/or smallparenchymal infiltrates. Healed primary tuberculosismay leave calcified deposits in the lung parenchymaand/or hilum.
C. Extrapulmonary disease is more common inchildren than in adults. In children, 25% of tuberculo-sis disease is extrapulmonary. Children and youngadolescents are more likely than adults to havetuberculous meningitis, miliary tuberculosis, adenitis,and bone and joint infections.
D. Reactivation. Children who do not have clinical dis-ease, but who harbor a reservoir of quiescentorganisms may develop tuberculous disease later inlife. Reactivation is most likely to occur duringado lescence , du r ing an ep isode o fimmunosuppression, in the presence of chronicdisease, or in the elderly.
II. Diagnosis of tuberculosis in childrenA. Children exposed to tuberculosis
1. All household contacts of adults with activedisease should be tested by PPD. Thirty to 50%of all household contacts of infectious adults willhave a positive PPD.
2. Children who are known contacts and who arePPD negative, should receive prophylactic ther-apy, usually isoniazid (Laniazid), 10 mg/kg/day.The PPD is repeated in 3 months to check forconversion to a positive PPD test, which wouldindicate infection. If the repeat PPD test remainsnegative, the child is assumed not to be infected,and prophylactic therapy can be discontinued. Ifthe repeat PPD test is positive, the child shouldbe treated for 9 months.
3. Any child with a positive PPD test should beevaluated for active pulmonary andextrapulmonary tuberculosis with a history andphysical examination and posteroanterior andlateral chest radiographs. The source of thechild’s infection should be determined. The sus-ceptibility of the source case’s M. tuberculosisstrain is considered in selecting a prophylactic ortreatment regimen. Contact with the person withcontagious tuberculosis who infected the childmust be prevented until the source case is nolonger infectious.
B. Children at risk for infection1. A PPD test is recommended for children in high-
risk groups. A screening PPD test of 5 tuberculinunits can be placed before a dose of measles-mumps-rubella (MMR) vaccine, simultaneouslywith the MMR vaccine dose, or 6 weeks after theMMR vaccine dose. A false-negative PPD testmay occur within 6 weeks of an MMR vaccination,because of transient immunosuppression fromthe live MMR vaccine.
2. The size of the PPD reaction determined to bepositive varies with the risk of tuberculous infec-tion. The diameter of the induration is measured48 to 72 hours after PPD placement. A positivePPD test requires an evaluation for tuberculousdisease.

Criteria for a Positive PPD Test in Children
Reaction of 5 mm or moreChildren suspected of having tuberculosis (chest x-ray
consistent with active or previously active tuberculo-sis; clinical signs of tuberculosis)
Children in close contact with persons who have knownor suspected infectious tuberculosis
Children with immunosuppressive conditions (HIV infec-tion, corticosteroid therapy)
Reaction of 10 mm or moreChildren younger than 4 years of ageChildren born in, or whose parents were born in, regions
where tuberculosis is highly prevalentChildren frequently exposed to adults who are HIV in-
fected, homeless persons, IV and other street drugusers, poor and medically indigent city dwellers, resi-dents of nursing homes, incarcerated or institutional-ized persons, and migrant farm workers
Children with other medical risk factors (Hodgkin’s dis-ease, lymphoma, diabetes mellitus, chronic renalfailure)
Reaction of 15 mm or moreChildren older than 4 years without any risk factors
3. Previous vaccination with bacille Calmette-Guerin (BCG) vaccine does not change theinterpretation of the PPD test.
4. High tuberculous infection rates occur in South-east Asia, Africa, Eastern Mediterranean coun-tries, Western Pacific countries, Mexico, theCaribbean, and South and Central America.
C. Clinical evidence suggestive of tuberculosis.Tuberculosis must be considered when a childpresents with pneumonia that is unresponsive toantibiotic treatment, “aseptic” meningitis, joint orbone infection, hilar or cervical adenopathy, orpleural effusion.
III. Evaluation of tuberculosis in childrenA. The work-up for a child with a positive PPD test or
suspected tuberculosis includes the following:1. History. Risk factors for exposure to tuberculo-
sis; symptoms of tuberculosis; adult sourcecase.
2. Physical examination. Adenopathy, positiverespiratory system findings, bone or joint dis-ease, meningitis.
3. Diagnostic testsa. Chest x-ray (posteroanterior and lateral).b. Gastric aspirates in children who are too
young to produce a deep sputum samplec. Sputum collection or induction in children
who are able to produce a deep sputumsample.
d. Cultures and smears of appropriate bodyfluids in children with suspectedextrapulmonary tuberculosis.
IV. Treatment of active tuberculosisA. Treatments should be directly observed to ensure
compliance. If possible, the susceptibility results ofthe adult source case should guide the medicationchoice. If the organism may be resistant to one ofthe standard medications, ethambutol (Myambutol[or streptomycin in children too young for visualacuity testing]) should be included.
B. Drug-resistant tuberculosis should be suspected inchildren who are exposed to immigrants from Asia,Africa and Latin America, children who live in largecities, or who are from areas in which isoniazidresistance occurs in more than 4% of cases,children who are homeless, children who havepreviously been treated for tuberculosis, andchildren who are exposed to adults at high risk fortuberculosis.

Treatment Regimens for Active Tuberculosis
Type of Disease Primary Regimen Comments
Pulmonary dis-ease
T w o m o n t h s o fi s o n i a z i d , 1 0 - 1 5mg/kg/day, max 300m g / d a y ; r i f a m p in( R i f a d i n ) , 1 0 - 2 0mg/kg/day, max 600m g / d a y ; a n dpyrazinamide, 20-40mg/kg/day, max 2.0g/day, followed by 4months of daily ortwice-weekly isoniazidand rifampin
Med ica t i o nscan be given 2o r 3t i m e s / w e e kunder directobservation int h e i n i t i a lphase
Extrapulmonarydisease, exceptmeningitis, miliaryd i s e a s e a n dbone/joint disease
Same as for pulmonarydisease
Meningitis, miliaryd isease , andbone/joint disease
Two months of dailyisoniazid, rifampin,pyrazinamide and strep-tomycin, followed by 10months of daily ortwice-weekly isoniazidand rifampin
V. Treatment of latent tuberculosis infectionA. Children with a positive PPD test, but no signs of
active disease, should receive isoniazid for 9months if they are younger than 18 years and for atleast 6 months if they are 18 years of age or older.Exposure to drug-resistant tuberculosis requiresmore specific therapy.
B. The child with tuberculous infection or disease mayreturn to school or child care after drug therapy hasbeen initiated and clinical symptoms have resolved.HIV testing should be completed for any older childor adult with tuberculosis.
References, see page 182.
Urinary Tract Infections in Children
Urinary tract infections (UTI) are a common problem inchildhood, which may lead to renal scarring, hypertension,and end stage renal dysfunction. UTI includes both cystitisand pyelonephritis.
I. Clinical featuresA. Infants and young children with UTI can present
only with fever. The presence of another potentialsource for fever (upper respiratory tract infection,acute otitis media, acute gastroenteritis) does notrule out the possibility of UTI. Other less commonsymptoms of UTI in infants include conjugatedhyperbilirubinemia and failure to thrive.
B. Older children with UTI may have fever, urinarysymptoms (dysuria, urgency, frequency, inconti-nence, macroscopic hematuria), and abdominalpain. Occasionally, older children may present withfailure to thrive, nephropathy, or hypertensionsecondary to prior unrecognized UTIs. Suprapubictenderness and costovertebral angle tendernessmay be present.
Signs and Symptoms of UTI In Children
Newborns Infants and Pre-schoolers
School-Age Chil-dren
JaundiceHypothermiaSepsisFailure to thriveVomitingFever
DiarrheaFailure to thriveVomiting FeverStrong-smellingurine
VomitingFeverStrong-smellingurineAbdominal painFrequencyDysuriaUrgencyEnuresis
C. History. The height and duration of fever, urinarysymptoms, vomiting, recent illnesses, antibioticsadministered, and use of barrier contraceptivemethod should be assessed. The following past

history should be obtained:1. Chronic constipation.2. Chronic urinary symptoms. Incontinence, lack of
proper stream, frequency, urgency, withholdingmaneuvers.
3. Previous UTIs.4. Vesicoureteral reflux (VUR).5. Previous undiagnosed febrile illnesses.6. Family history of frequent UTIs, VUR and other
genitourinary abnormalities.D. Physical examination. Blood pressure, tempera-
ture, suprapubic and costovertebral tenderness, andother sources of fever should be evaluated. Externalgenitalia should be examined for vulvovaginitis,vaginal foreign body, sexually transmitted diseases(STDs), and anatomic abnormalities.
E. Differential diagnosis of a well-appearing infantwith fever without a definite source includes UTI andoccult bacteremia.1. In children vaccinated against Haemophilus
influenzae and Streptococcus pneumoniae, theodds of UTI are much higher than the odds ofoccult bacteremia.
2. The differential diagnosis of an older child pre-senting with urinary symptoms and bacteriuriaincludes nonspecific vulvovaginitis, urinary cal-culi, urethritis secondary to an STD (particularlyChlamydia), and a vaginal foreign body. Patientswith group A streptococcal infection, appendicitis,and Kawasaki disease may present with fever,abdominal pain, and pyuria.
II. DiagnosisA. Decision to obtain urine
1. The presence of two or more of the following fivevariables predicts UTI accurately:a. Age under one year.b. White race.c. Temperature >39ºC.d. Fever for more than two days.e. Absence of another source of fever on history
or examination (ie, absence of upper respira-tory infection, acute otitis media,gastroenteritis).
2. All older girls with urinary symptoms suggestive ofUTI should have a urine specimen obtained forurinalysis and culture.
B. Clean catch specimen is the preferred method ofurine collection in a toilet-trained child. Acatheterized specimen is preferred in the diaperedchild. Suprapubic aspiration also may be used tocollect a specimen in young children. A suprapubicaspirate is recommended when:1. Catheterization is not feasible (eg, penile and
labial adhesions).2. Results from catheterized specimen are inconclu-
sive (eg, repeated contaminated specimen orrepeated low colony counts).
C. Dipstick tests are convenient but may miss somechildren with UTI (sensitivity 88%). Therefore, aurine culture should still be obtained in children withsuspected UTI who have a negative dipstick test. Achild with a positive nitrite test is very likely to havea UTI.
D. Microscopic examination1. The accuracy of microscopic analysis is improved
by using:a. An uncentrifuged specimen.b. A Gram stained specimen.c. A hemocytometer (results reported as
WBC/mm3).2. Examination of urine using these three tech-
niques has been termed an “enhanced urinaly-sis.” In young children, the enhanced urinalysisoffers the best combination of sensitivity andspecificity for predicting a UTI in children. Urineculture should be performed in most patients.
III. Definition of a UTI

Culture Criteria for Significant Bacteruria
Method Colony Count
Suprapubic aspiration Any bacteria
Urethral catheterization >10,000 cfu/mL
Best catch >50,000 cfu/mL
A. A blood culture is not necessary in children over twomonths with UTI. Children less than one month ofage with high fever and a positive urinalysis shouldhave a lumbar puncture performed, since approxi-mately 1 percent with UTI may also have bacterialmeningitis
IV. Imaging. A. Routine imaging is recommended for:
1. Children under five years of age with a febrileUTI.
2. Girls under three years of age with a first UTI.3. Males of any age with a first UTI.4. Children with recurrent UTI5. Children with UTI who do not respond promptly to
therapy.B. Renal ultrasonography can demonstrate the size
and shape of the kidneys, the presence of duplica-tion and dilatation of the ureters, and the existenceof gross anatomic abnormalities.
C. Voiding cystourethrogram is an excellent test toestablish the presence and degree of VUR.Radionuclide VCUG involves catheterization to fillthe bladder with a radioactive liquid and recording ofVUR during voiding. The radionuclide VCUG ismore sensitive than contrast VCUG has a sensitivityof 78 to 91%). The contrast VCUG provides a betteranatomic resolution, which makes it more suited forgrading VUR.
D. Recommendations for imaging1. Routine VCUG for children is recommended
under the age of five years with a febrile UTI,males of any age with a first UTI, girls under theage of three years with a first UTI, and childrenwith recurrent UTI.
2. Routine performance of renal ultrasonography isnot recommended following diagnosis of a firstUTI in children in whom prenatal ultrasonographyhas been performed in a reputable center at >30to 32 weeks of pregnancy. An ultrasound inchildren with a UTI who do not respond promptlyto therapy is recommended.
I. Management, prognosis, and prevention of urinarytract infections in childrenA. Hospitalization. Children who are not responding
to outpatient therapy, who are vomiting and there-fore cannot tolerate oral medication, or who are notable to be adequately followed should be managedas inpatients.
B. Choice of antibiotics. Gram staining of the urinecan aid in the choice of initial antimicrobial therapy.1. E. coli is the most common pathogen causing
UTI, and 50 percent of E. coli are resistant toamoxicillin or ampicillin. First-generationcephalosporins, amoxicillin-clavulanate or ampicillin-sulbactam, andtrimethoprim-sulfamethoxazole (TMP-SMX)should be used with caution because increasingresistance to these antibiotics.
2. Alternatives include second- and third-generationcephalosporins and gentamicin although thesedrugs are not effective in treating enterococcalinfections. Cefixime has been shown to be effec-tive in the treatment of outpatients with UTI.Quinolones are effective and resistance is rare,but safety in children is still unknown.
C. Duration of therapy1. A three-day course of antibiotics is recommended
in older children with their first episode of cystitis(low risk of recurrence or complications). A 10- to14-day course of an antimicrobial is recom-mended for young children and for those withrecurrent or febrile UTIs.

Antibiotic Therapy for Urinary Tract Infectionswith Severe Symptoms
Agent Dosage (mg/kg/day)
Neonate
Ampicillin andGentamicin
7.5 mg/kg/day IV/IM q8h100 mg/kg/day IV/IM q6h
Older Child
Ceftriaxone(Rocephin)
50 mg /kg/day (IM, IV) q24h
Cefotaxime(Claforan)
100 mg /kg/day (IV) q6-8h
Ampicillin/sulbactam(Unasyn)
100-200 mg of ampicillin/kg/day q6h
Gentamicin 3-7.5 mg /kg/day(IV, IM) q8h
Antibiotic Therapy for Urinary Tract Infections with MildSymptoms
Agent Dosage
Cefpodoxime(Vantin)
10 mg/kg/day PO q12h [susp: 50 mg/5mL, 100 mg/5 mL; tabs: 100 mg, 200mg]
Cefprozil (Cefzil) 30 mg/kg/day PO q12h [susp: 125mg/5 mL, 250 mg/5 mL; tabs: 250,500 mg]
Cefixime (Suprax) 8 mg/kg/d PO qd-bid [susp: 100 mg/5mL, tab: 200,400 mg]
Cefuroxime (Ceftin) 125-500 mg PO q12h [125, 250, 500mg]
Amoxicillin/clavulanate (Augmentin)
40 mg of amoxicillin kg/day PO q8h[susp: amoxicillin 125mg/clavulanate/5 mL; tab: amoxicillin250 mg/clavulanate; amoxicillin 500mg/clavulanate]
Trimethoprim/sulfamethoxazole(Bactrim)
6-12 mg/kg/day (trimethoprim) q12h[susp: trimethoprim 40mg/sulfamethoxazole 200 mg/5 mL]
D. Long-term management and follow-up1. Children with recurrent UTI symptoms. Eight
to 30 percent of children with UTI experiencereinfections. Breakthrough UTIs are most com-mon in girls.
2. Prompt diagnosis and treatment of UTI reducesrenal scarring.
3. Low-dose long-term antimicrobial therapy, suchas six to 12 months of TMP-SMX or nitrofuran-toin, should be prescribed for recurrent febrileUTIs and scarring.
4. Children with VUR. The goal of treatingvesicoureteral reflux (VUR) is to prevent progres-sive renal damage. The majority of young chil-dren with VUR have low-grade (grade I to III)VUR, which will resolve spontaneously. Childrenwith grades IV and V VUR and older children areless likely to experience spontaneous resolution.Mild-to-moderate VUR is treated with low-doselong-term antimicrobials until resolution of VUR.Prophylaxis should be discontinued after age fiveto seven years, even if low-grade VUR persists.Prophylaxis consists of TMP-SMX or nitrofuran-toin in half the usual therapeutic doses given atbedtime. One out of every five patients on pro-phylactic nitrofurantoin doses, however, mayexperience GI adverse events. Amoxicillin andcephalosporins are not recommended for prophy-laxis since infection with resistant strains is likelyto emerge.
5. Older children with persistent severe VUR(grades IV and V), and those with lesser degreesof VUR but with progressive scarring while onprophylaxis, should undergo ureteralreimplantation.
6. Children with dysfunctional elimination.Treatment of dysfunctional elimination decreasesUTI recurrence and is associated with fasterresolution of VUR. Treatment of dysfunctional

elimination includes the use of laxatives andtimed voiding (scheduled voids every two to threehours).
References, see page 182.
Viral Laryngotracheitis (Croup)
Acute laryngotracheitis (viral croup) is the most commoninfectious cause of acute upper airway obstruction inpediatrics, causing 90% of cases. The disease is usuallyself-limited. Children in the 1- to 2-year-old age group aremost commonly affected. Viral croup affects 3-5% of allchildren each year. Croup is most common from the latefall to early spring, although cases may occur throughoutthe year.
I. Clinical evaluation of upper airway obstruction andstridorA. Stridor is the most common presenting feature of all
causes of acute upper airway obstruction. It is aharsh sound that results from air movement througha partially obstructed upper airway.1. Supraglottic disorders, such as epiglottitis,
cause quiet, wet stridor, a muffled voice,dysphagia and a preference for sitting upright.
2. Subglottic lesions, such as croup, cause loudstridor accompanied by a hoarse voice and barkycough.
B. Patient age1. Upper airway obstruction in school age and older
children tends to be caused by severe tonsillitisor peritonsillar abscesses.
2. From infancy to 2 years of age, viral croup andretropharyngeal abscess are the most commoncauses of upper airway obstruction.
C. Mode of onset1. Gradual onset of symptoms, usually preceded by
upper respiratory infection symptoms, suggestsviral croup, severe tonsillitis or retropharyngealabscess.
2. Very acute onset of symptoms suggestsepiglottitis.
3. A history of a choking episode or intermittent res-piratory distress suggests a foreign body inhala-tion.
4. Facial edema and urticaria suggestsangioedema.
D. Emergency management of upper airway ob-struction1. Maintaining an adequate airway takes prece-
dence over other diagnostic interventions. If asupraglottic disorder is suspected, a personskilled at intubation must accompany the child atall times.
2. Patients with suspected epiglottitis, severe respi-ratory distress from an obstruction, or suspectedforeign body inhalation should be taken to theoperating room for direct laryngoscopic visualiza-tion and possible intubation.
Causes of Upper Airway Obstruction in Children
Supraglottic Infectious DisordersEpiglottitis Peritonsillar abscess Retropharyngeal abscessSevere tonsillitis
Subglottic Infectious DisordersCroup (viral laryngotracheitis)Spasmodic croupBacterial tracheitis
Non-Infectious CausesAngioedemaForeign body aspirationCongenital obstructionNeoplasmsExternal trauma to neck

Characteristics of selected causes of Upper Air-way Obstruction
Epiglottitis
Laryngotracheo-bronchi-tis(Croup)
Bacte-rialTracheitis
ForeignBody Aspi-ration
History
Inci-dencein chil-drenpre-sentingwithstridor
8% 88% 2% 2%
Onset Rapid, 4-12 hours
Prodrome, 1-7 days
Prodrome, 3days,then 10hours
Acute orchronic
Age 1-6 years 3 mo-3years
3 mo-2years
Any
Season None October-May
None None
Etiol-ogy
Haemophilus in-fluenza
Parainfluenza vi-ruses
Staphylococcus
Many
Pathol-ogy
Inflam-matoryedema ofepiglottisandsupra-glottitis
Edemaandinflamma-tion oftracheaand bron-chial tree
Tracheal-bron-chialedema,necroticdebris
Localizedtracheitis
Signs and Symptoms
Dysphagia
Yes No No Rare
Diffi-cultyswallowing
Yes No Rare No
Drool-ing
Yes No Rare No
Stridor Inspiratory
Inspiratoryand expi-ratory
Inspiratory
Variable
Voice Muffled Hoarse Normal Variable
Cough No Barking Variable Yes
Temperature
Markedlyelevated
Minimallyelevated
Moder-ate
Normal
Heartrate
In-creasedearly
Increasedlate
Propor-tional tofever
Normal
Posi-tion
Erect,anxious,“air hun-gry,” su-pine po-sitionexacer-bates
No effecton airwayobstruc-tion
No effect No effect
Respi-ratoryrate
In-creasedearly
Increasedlate
Normal Increased ifbronchialobstructionpresent

Differentiation of Epiglottitis from ViralLaryngotracheitis
Clinical Feature Epiglottitis Viral Croup
Retractions present present
Wheezing absent occasionally present
Cyanosis present present in severecases
“Toxicity” present absent
Preference forsitting
yes no
II. Epidemiology and etiology of viral laryngotracheitis(Croup) A. Parainfluenza virus type 1 causes 40% of all
cases of laryngotracheitis. Parainfluenza type 3,respiratory syncytial virus (RSV), parainfluenza type2, and rhinovirus may also cause croup.
B. RSV commonly affects infants younger than 12months of age, causing wheezing and stridor.Influenza viruses A and B and mycoplasma havebeen implicated in patients older than 5 years.
III. Clinical manifestationsA. Viral croup begins gradually with a 1-2 day
prodrome, resembling an upper respiratory infec-tion. Subglottic edema and inflammation of thelarynx, trachea, and bronchi eventually develop.
B. Low-grade fever and nocturnal exacerbation ofcough are common. As airway obstruction increasesretractions, develop, restlessness, anxiety, tachycar-dia, and tachypnea may occur.
C. Cyanosis is a late sign. Severe obstruction leads torespiratory muscle exhaustion, hypoxemia, carbondioxide accumulation, and respiratory acidosis.Stridor becomes less apparent as muscle fatigueworsens.
D. Ten percent of croup patients have severe respi-ratory compromise requiring hospital admission, and3% of those children need airway support.
IV. Laboratory evaluation. The diagnosis of viral croupis based primarily on the history and clinical find-ings. When the diagnosis is uncertain or the patientrequires hospitalization, x-rays can be helpful. Theposteroanterior neck radiograph of a patient withviral croup shows symmetrical narrowing of thesubglottic space (“steeple sign”).
V. Inpatient treatment of laryngotracheitisA. The majority of patients who have croup do not
require hospitalization.B. Indications for hospitalization
1. Dusky or cyanotic skin color.2. Decreased air entry on auscultation.3. Severe stridor.4. Significant retractions.5. Agitation, restlessness, or obtundation.
C. Signs that indicate the need for an artificial airwayinclude decreased respiratory effort and decreasedlevel of consciousness. Pulse oximetry may aid inassessing the severity of respiratory compromise.
D. All patients suspected of having viral croup shouldbe given humidified air. Hypoxic or cyanotic patientsrequire oxygen via mask and may require intubation.Oral hydration is essential to help loosen secretions;however, intravenous hydration may become neces-sary in the very ill child.
E. Racemic epinephrine has alpha-adrenergic prop-erties, which decrease subglottic inflammation andedema. Racemic epinephrine is administered as 0.5mL of a 2.25% solution, diluted with 3.5 mL of saline(1:8) by nebulization. It is given every 20-30 minutesfor severe croup, and it is given every 4-6 hours formoderate croup.
F. Corticosteroids reduce subglottic edema andinflammation. Dexamethasone (0.6 mg/kg IM)given one time early in the course of croup results ina shorter hospital stay and reduces cough anddyspnea. Patients who do not require hospitalizationshould not receive steroids.
G. Acetaminophen decreases fever and oxygenconsumption in the febrile patient with croup.
H. Patients with mild viral croup usually are not admit-ted to the hospital and can be treated safely athome. Vaporizers, oral fluids, and antipyretics arethe mainstays of home therapy. The prognosis forcroup is good; however, a subset of children who

have croup will later be identified as having asthma.References, see page 182.
Pelvic Inflammatory Disease
Pelvic inflammatory disease (PID) is an acute infection ofthe upper genital tract in women, involving any or all of theuterus, oviducts, and ovaries. PID is a community-ac-quired infection initiated by a sexually transmitted agent.Pelvic inflammatory disease accounts for approximately2.5 million outpatient visits and 200,000 hospitalizationsannually.
I. Clinical evaluationA. Lower abdominal pain is the cardinal presenting
symptom in women with PID, although the charac-ter of the pain may be quite subtle. The onset ofpain during or shortly after menses is particularlysuggestive. The abdominal pain is usually bilateraland rarely of more than two weeks’ duration.
B. Abnormal uterine bleeding occurs in one-third ormore of patients with PID. New vaginal discharge,urethritis, proctitis, fever, and chills can be associ-ated signs.
C. Risk factors for PID:1. Age less than 35 years.2. Nonbarrier contraception.3. New, multiple, or symptomatic sexual partners.4. Previous episode of PID.5. Oral contraception.6. African-American ethnicity.
II. Physical examinationA. Only one-half of patients with PID have fever.
Abdominal examination reveals diffuse tendernessgreatest in the lower quadrants, which may or maynot be symmetrical. Rebound tenderness anddecreased bowel sounds are common. Tendernessin the right upper quadrant does not exclude PID,because approximately 10 percent of these patientshave perihepatitis (Fitz-Hugh Curtis syndrome).
B. Purulent endocervical discharge and/or acutecervical motion and adnexal tenderness bybimanual examination is strongly suggestive of PID.Rectovaginal examination should reveal the uterineadnexal tenderness.
III. DiagnosisA. Diagnostic criteria and guidelines. The index of
suspicion for the clinical diagnosis of PID should behigh, especially in adolescent women.
B. The CDC has recommended minimum criteriarequired for empiric treatment of PID. These majordeterminants include lower abdominal tenderness,adnexal tenderness, and cervical motion tender-ness. Minor determinants (ie, signs that may in-crease the suspicion of PID) include:1. Fever (oral temperature >101EF; >38.3EC).2. Vaginal discharge.3. Documented STD.4. Erythrocyte sedimentation rate (ESR).5. C-reactive protein.6. Systemic signs.7. Dyspareunia.
C. Empiric treatment for pelvic inflammatory dis-ease is recommended when:1. The examination suggests PID.2. Demographics (risk factors) are consistent with
PID.3. Pregnancy test is negative.
Laboratory Evaluation for Pelvic InflammatoryDisease
• Pregnancy test • Microscopic exam of vaginal discharge in saline• Complete blood counts• Tests for chlamydia and gonococcus• Urinalysis• Fecal occult blood test• C-reactive protein(optional)

IV. Diagnostic testingA. Laboratory testing for patients suspected of
having PID always begins with a pregnancy test torule out ectopic pregnancy and complications of anintrauterine pregnancy. A urinalysis and a stool foroccult blood should be obtained because abnor-malities in either reduce the probability of PID.Blood counts have limited value. Fewer than one-half of PID patients exhibit leukocytosis.
B. Gram stain and microscopic examination of vaginaldischarge may provide useful information. If acervical Gram stain is positive for Gram-negativeintracellular diplococci, the probability of PIDgreatly increases; if negative, it is of little use.
C. Increased white blood cells (WBC) in vaginal fluidmay be the most sensitive single laboratory test forPID (78 percent for >3 WBC per high power field.However, the specificity is only 39 percent.
D. Recommended laboratory tests:1. Pregnancy test.2. Microscopic exam of vaginal discharge in saline.3. Complete blood counts.4. Tests for chlamydia and gonococcus.5. Urinalysis.6. Fecal occult blood test.7. C-reactive protein(optional).
E. Ultrasound imaging is reserved for acutely illpatients with PID in whom a pelvic abscess is aconsideration.
V. Recommendations A. Health-care providers should maintain a low thresh-
old for the diagnosis of PID, and sexually activeyoung women with lower abdominal, adnexal, andcervical motion tenderness should receive empirictreatment. The specificity of these clinical criteriacan be enhanced by the presence of fever, abnor-mal cervical/vaginal discharge, elevated ESRand/or serum C-reactive protein, and the demon-stration of cervical gonorrhea or chlamydia infec-tion.
B. If clinical findings (epidemiologic, symptomatic, andphysical examination) suggest PID empiric treat-ment should be initiated.
Differential Diagnosis of Pelvic InflammatoryDisease
Appendicitis Ectopic pregnancy Hemorrhagic ovarian cystOvarian torsion EndometriosisUrinary tract Infection
Irritable bowel syndrome Somatization Gastroenteritis Cholecystitis Nephrolithiasis
VI. Treatment of pelvic inflammatory disease A. The two most important initiators of PID, Neisseria
gonorrhoeae and Chlamydia trachomatis, must betreated, but coverage should also be provided forgroups A and B streptococci, Gram negativeenteric bacilli (Escherichia coli, Klebsiella spp., andProteus spp.), and anaerobes.
B. Outpatient therapy1. For outpatient therapy, the CDC recommends
either oral ofloxacin (Floxin, 400 mg twice daily)or levofloxacin (Levaquin, 500 mg once daily)with or without metronidazole (Flagyl, 500 mgtwice daily) for 14 days. An alternative is aninitial single dose of ceftriaxone (Rocephin, 250mg IM), cefoxitin (Mefoxin, 2 g IM plusprobenecid 1 g orally), or another parenteralthird-generation cephalosporin, followed bydoxycycline (100 mg orally twice daily) with orwithout metronidazole for 14 days. Quinolonesare not recommended to treat gonorrhea ac-quired in California or Hawaii. If the patient mayhave acquired the disease in Asia, Hawaii, orCalifornia, cefixime or ceftriaxone should beused.
2. Another alternative is azithromycin (Zithromax,1 g PO for Chlamydia coverage) andAmoxicillin-clavulanate (Amoxicillin, 875 mg PO)once by directly observed therapy, followed byamoxicillin-clavulanate (Amoxicillin, 875 mg POBID) for 7 to 10 days.
C. Inpatient therapy1. For inpatient treatment, the CDC suggests either
of the following regimens:a. Cefotetan (Cefotan), 2 g IV Q12h, or
cefoxitin (Mefoxin, 2 g IV Q6h) plusdoxycycline (100 mg IV or PO Q12h)
b. Clindamycin (Cleocin), 900 mg IV Q8h, plusgentamicin (1-1.5 mg/kg IV q8h)
2. Alternative regimens: a. Ofloxacin (Floxin), 400 mg IV Q12h or
levofloxacin (Levaquin, 500 mg IV QD) withor without metronidazole (Flagyl, 500 mg IVQ8h). Quinolones are not recommended totreat gonorrhea acquired in California orHawaii. If the patient may have acquired thedisease in Asia, Hawaii, or California,cefixime or ceftriaxone should be used.
b. Ampicillin-sulbactam (Unasyn), 3 g IV Q6hplus doxycycline (100 mg IV or PO Q12h)
3. Parenteral administration of antibiotics shouldbe continued for 24 hours after clinical re-sponse, followed by doxycycline (100 mg POBID) or clindamycin (Cleocin, 450 mg PO QID)for a total of 14 days.
4. The following regimen may also be used:Levofloxacin (Levaquin), 500 mg IV Q24h,plus metronidazole (Flagyl, 500 mg IV Q8h).With this regimen, azithromycin (Zithromax, 1 gPO once) should be given as soon as the pa-tient is tolerating oral intake. Parenteral therapyis continued until the pelvic tenderness onbimanual examination is mild or absent.
D. Annual screening is recommended for all sexuallyactive women under age 25 and for women over 25if they have new or multiple sexual partners. Aretest for chlamydia should be completed in 3 to 4months after chlamydia treatment because of highrates of reinfection.
E. Additional evaluation:1. Serology for the human immunodeficiency virus
(HIV).2. Papanicolaou smear.3. Hepatitis B surface antigen determination and
initiation of the vaccine series for patients whoare antigen negative and unvaccinated.
4. Hepatitis C virus serology.5. Serologic tests for syphilis.
References, see page 182.
Gastrointestinal DisordersAcute Abdominal Pain
The evaluation of abdominal pain in children is problem-atic because the pain is often difficult to localize, and thehistory in children is often nonspecific.
I. Localization of abdominal painA. Generalized pain in the epigastrium usually comes
from the stomach, duodenum, or the pancreas.B. Periumbilical pain usually originates in small bowel
and colon or spleen. C. Parietal pain, caused by inflammation, is usually
well localized.D. Referred abdominal pain occurs when poorly
localized visceral pain is felt at a distant location.1. Pancreatitis, cholecystitis, liver abscess, or a
splenic hemorrhage cause diaphragmatic irrita-tion, which is referred to the ipsilateral neck andshoulders.
2. Intraabdominal fluid may cause shoulder painon reclining.
3. Gallbladder pain may be felt in the lower back orinfrascapular area.
4. Pancreatic pain often is referred to the posteriorflank.
5. Ureterolithiasis often presents as pain radiatingtoward the ipsilateral groin.
6. Rectal or gynecological pain often is perceivedas sacral pain.
7. Right lower lobe pneumonia may be perceivedas right upper quadrant abdominal pain.
II. Clinical evaluationA. History should include the quality, timing, and type
of abdominal pain.1. Pain of sudden onset often denotes colic,

perforation or acute ischemia caused by torsionor volvulus.
2. Slower onset of pain suggests inflammatoryconditions, such as appendicitis, pancreatitis, orcholecystitis.
B. Colic results from spasms of a hollow viscus organsecondary to an obstruction. It is characterized bysevere, intermittent cramping, followed by intervalswhen the pain is less intense. Colic pain usuallyoriginates from the biliary tree, pancreatic duct,gastrointestinal tract, urinary system, or uterus andtubes.
C. Inflammatory pain is caused by peritoneal irritation,and the patient presents quietly without muchmotion and appears ill. The pain is initially lesssevere and is exacerbated by movement.
D. Vomiting. Usually abdominal pain will precedevomiting. The interval between abdominal pain andvomiting is shorter when associated with colic.Delayed vomiting for many hours is often associatedwith distal bowel obstruction or ileus secondary toperitonitis.
E. Diarrhea. Mild diarrhea with the onset of abdominalpain suggests acute gastroenteritis or early appendi-citis. Delayed onset of diarrhea may indicate aperforated appendicitis, with the inflamed masscausing irritation of the sigmoid colon.
F. Physical examination1. The abdomen should be observed, auscultated,
and palpated for distention, localized tenderness,masses, and peritonitis. The groin must be exam-ined to exclude an incarcerated hernia or ovary,or torsion of an ovary or testicle.
2. Rectal examinationa. Gross blood in the stool suggests ectopic
gastric mucosa, Meckel’s diverticula, or pol-yps.
b. Blood and mucus (currant jelly stool) sug-gests inflammatory bowel disease orintussusception.
c. Melena suggests upper gastrointestinal bleed-ing, necessitating gastric aspiration for blood.
d. Tests for occult blood in the stool should beperformed.
3. Pelvic examinations are mandatory forpostmenarchal and/or sexually active femalepatients. The rectal examination may also beused to evaluate the cervix, uterus, adnexa, andpelvic masses.
4. Fevera. Thoracic disease (eg, pneumonia) may be the
cause of abdominal pain associated with fever.b. Costovertebral angle tenderness with fever
suggests pyelonephritis or a high retrocecalappendicitis.
III. Appendicitis A. Fever, vomiting, irritability, lethargy with right
lower quadrant (RLQ) tenderness and guardingare diagnostic of appendicitis in the very youngpatient until proven otherwise. A mass may be felton rectal exam in 2-7% of younger patients withappendicitis.
B. A WBC >15,000 supports the diagnosis. An ultra-sound of the appendix may be useful.
C. Children older than 2 years old present with aperforated appendix about 30-60% of the time. Thisincidence declines as the age of the child increases.
IV. IntussusceptionA. Intussusception is the most common cause of bowel
obstruction between 2 months and 5 years of age.The most vulnerable age group is 4-10 months old,but children up to 7 years old may be at risk.
B. Intussusception is characterized by vomiting, colickyabdominal pain (85%) with drawing up of the legs,and currant jelly stools (60%). Fever is common.
C. The abdomen may be soft and nontender betweenepisodes of colicky pain, but eventually it becomesdistended. A sausage-shaped mass in the rightupper quadrant (RUQ) may be palpable.
D. Abdominal x-ray. The leading edge of theintussusception is usually outlined with air, which willestablish the diagnosis. Often there are radiographicsigns of bowel obstruction. When the plain abdomi-nal x-ray is normal, intussusception cannot beexcluded without a barium enema.
E. Treatment consists of radiologic reduction, which is

effective in 80-90%. Radiographic reduction iscontraindicated if there is peritoneal irritation ortoxicity.
V. Midgut volvulusA. Midgut volvulus results from the improper rotation
and fixation of the duodenum and colon(malrotation). Obstruction of the superior mesentericartery may cause ischemic necrosis of the gut,which may be fatal.
B. Infants in the first month constitute the majority ofthe cases. Symptoms usually begin about 5 daysbefore diagnosis. The first sign of volvulus is biliousvomiting, followed by abdominal distention and GIbleeding. Peritonitis, hypovolemia, and shock mayfollow.
C. Abdominal x-ray reveals a classic double bubblecaused by duodenal obstruction. Pneumatosisintestinalis or distal bowel obstruction may also beapparent.
D. Infants with rapid deterioration and obstructed loopsof bowel require immediate surgery. If the infant isnot critically ill, an UGI series with water-soluble,non-ionic, isoosmolar contrast will confirm midgutvolvulus. If malrotation or volvulus (beak, spiral orcorkscrew sign) is found, an immediate laparotomyis necessary.
VI. Gallbladder diseaseA. Cholecystitis in children occurs most commonly in
the adolescent female, but it may affect infants whoare only a few weeks of age. Cholecystitis is sug-gested by RUQ pain, back pain, or epigastric pain,radiating to the right subscapular area, biliousvomiting, fever, RUQ tenderness, and a RUQ mass.Jaundice is present in 25-55%, usually in associa-tion with hemolytic disease.
B. Ultrasonography delineates gallstones and is thestudy of choice to screen for gallbladder disease.
C. Radioisotopic scanning evaluates biliary andgallbladder function.
VII. Ectopic pregnancy A. Ectopic pregnancy must be considered in any
postmenarchal, sexually active adolescent withabdominal pain. It is uncommon and usually seen inlate adolescence. Ectopic pregnancy occurs in 0.5-3% of all pregnancies.
B. Signs of ectopic pregnancy include abdominal painin any location, vaginal bleeding, and/oramenorrhea. Nausea and vomiting, other symptomsof pregnancy, and lightheadedness may also bepresent.
C. Abdominal, adnexal, and/or cervical tenderness areoften found on pelvic examination, but occasionallyabdominal tenderness is absent. The cervix may besoft (Godell’s sign) and bluish in color (Chadwick’ssign). The examination may reveal adnexal fullnessand uterine enlargement.
D. Evaluation includes a pregnancy test and ultra-sound. Treatment consists of removal of the ectopicpregnancy by laparoscopy or exploratorylaparotomy.
VIII. Gonadal pain in males A. In males with lower abdominal pain, the scrotum and
its contents must be examined. Testicular torsion isa surgical emergency and must be treated within 6hours of the onset of the pain to save the testicle.
B. Testicular torsion may present as lower abdominalpain, which may be associated with recent trauma orcold. The gonad is tender and elevated in thescrotum, with a transverse orientation. Althoughtesticular torsion may occur at any age, it usuallyoccurs in adolescent males at puberty or shortlyafterwards.
IX. Gonadal pain in femalesA. The leading causes of gonadal pain in females are
ovarian cysts and torsion of uterine adnexal struc-tures.
B. Ovarian cysts are responsible for 25% of childhoodovarian tumors, most commonly in adolescents.Bleeding into the cyst or cystic rupture causes pain,which usually subsides within 12-24 hours. Ultra-sound may show pelvic fluid and the cyst.
C. Torsion of uterine adnexal structures1. Torsion is associated with unilateral, sudden,
severe pain with nausea and vomiting. Thepatient may also have subacute or chronic symp-toms, with intermittent pain for days. The pain isusually diffuse and periumbilical in younger

patients, but in older children and adolescents,the pain may radiate initially to the anterior thighor ipsilateral groin.
2. Fever and leucocytosis are usually present.Physical exam may reveal muscle rigidity andfixation of the mass on pelvic examination.
3. Ultrasound will identify the mass accurately.Surgical exploration may sometimes salvage theovary. Malignant neoplasms may cause torsion in35% of cases.
X. Meckel diverticulum A. Meckel diverticulum are present in 2% of the popula-
tion. It presents as a tender left lower quadrantmass, associated with blood in the stool.
B. Vague abdominal pain with hemoccult positivestools suggests a Meckel diverticulum. Bleeding isseen in 35-40% of childhood cases. A technetiumnuclear scan may confirm the diagnosis.
References, see page 182.
Recurrent Abdominal Pain
Recurrent abdominal pain (RAP) includes any child oradolescent who has recurrent abdominal pain for whichthe family seeks medical attention and explanation. Morethan 90% of the time a “disease” will not be defined andthe family will be left with a “functional” explanation.
I. Epidemiology A. RAP occurs in 10-15% of children between the ages
of 4 and 16 years. About 13-17% of adolescentsexperience weekly pain. The overall incidenceappears to peak at 10 to 12 years. RAP is rareamong children younger than 5 years of age.
Differential Diagnosis of Recurrent AbdominalPain
• Functional abdominal pain• Fecal impaction• Parasitic infection• Partial small bowel ob-
struction- Crohn disease- Malrotation with or with-
out volvulus- Intussusception- Postsurgical adhesions - Small bowel lymphoma - Infection (tuberculosis,
Yersinia)- Eosinophilic
gastroenteritis- Angioneurotic edema
• Ureteropelvic junction ob-struction
• Appendiceal colic
• Dysmenorrhea- Endometriosis- Ectopic pregnancy- Adhesions from pelvic
inflammatory disease• Cystic teratoma of ovary• Musculoskeletal disorders
- Muscle pain- Linea alba hernia- Discitis
• Vascular disorders- Mesenteric thrombosis- Polyarteritis nodosa
• Abdominal migraine• Acute intermittent
porphyria• Psychiatric disorders
Diagnostic Criteria for Functional Abdominal Pain
• Chronicity• Compatible age range, age of onset• Characteristic features of abdominal pain• Evidence of physical or psychological stressful stimuli• Environmental reinforcement of pain behavior• Normal physical examination (including rectal examination
and stool guaiac)• Normal laboratory evaluation (CBC, sedimentation rate,
urinalysis, urine culture, stool ova and parasites)
II. Clinical AspectsA. Functional abdominal pain. The majority of chil-
dren who have RAP are considered to have afunctional etiology, and an organic etiology cannotbe found. The pain occurs in episodes that areperiumbilical, self-limited, unrelated to meals oractivities, and rarely if ever sufficient to awaken thechild from sleep. The growth pattern and findings onthe physical examination are normal. The degree ofinterference with normal activities and school atten-dance are out of proportion to the frequency andseverity of the episodes.
B. Irritable bowel syndrome. Some children whohave RAP manifest characteristics of irritable bowelsyndrome (IBS). The criteria for making this diagno-sis are: 1) abdominal pain relieved by defecation, 2)

more frequent stools at the onset of the pain, 3)altered stool form (hard or loose or watery), 4)passage of mucus, and 5) associated bloating orabdominal distension.
C. Constipation. The most common causes of consti-pation in children are inadequate intake of fruits,vegetables and higher-fiber foods, and an unwilling-ness to evacuate the bowels. The child goes daysbetween bowel movements and the stool is bulkyand hard. Findings on abdominal and rectal exami-nations may confirm the diagnosis; a plain abdomi-nal radiograph may be needed.
D. Inflammatory bowel disease. Ulcerative colitismay present with abdominal pain, hematocheziaand tenesmus. Crohn disease may cause abdomi-nal pain, diarrhea, lethargy, growth and pubertaldelay, and oral, joint, and perirectal involvement.Endoscopy will confirm the diagnosis.
E. Lactose intolerance. Asian, Jewish, Mediterra-nean, and African-American persons are predis-posed to lactase deficiency. Lactose ingestion willcause bloating, loose stools, and cramping abdomi-nal pain. The diagnosis is made by breath hydrogentesting or a therapeutic trial of restriction of milkproducts.
F. Helicobacter pylori-associated peptic ulcerdisease should be suspected when abdominal painis primarily epigastric; when it awakens the childfrom sleep; and when it is associated with anorexia,nausea, recurrent vomiting, anemia, or gastrointesti-nal bleeding. Peptic ulcer disease is very uncom-mon is children; therefore, testing for H pylori shouldnot be part of the preliminary evaluation of a childwho has RAP.
G. Nonulcer dyspepsia is a symptom complex ofepigastric pain, bloating, and discomfort accompa-nied by negative endoscopic and biopsy findings.
H. Abdominal migraine usually is recognized whenepisodes of paroxysmal abdominal pain occur inassociation with nausea and vomiting, sometimeswith associated headache. A strong family history ofmigraine is usually present.
I. Infestation/infection. Infection with Yersiniaenterocolitica and giardia can cause diarrheaassociated with abdominal cramps and pain, butdiarrhea usually is the predominant complaint.
J. Gynecologic conditions. Early menarche,endometriosis, pelvic inflammatory disease, andovarian cyst may cause RAP. These causes can bediagnosed by ultrasonographic examination.
K. Physical and sexual abuse may cause RAP, andsensitive history taking is required to elucidate itspossible role.
III. Clinical assessmentA. The history should assess the location, nature,
frequency of the pain, and associated symptoms.The relationship of the pain to school and so-cial/family stressors is important. Review of systemsshould cover the child’s diet, bowel habits, sleeppatterns, and context in which the pain occurs.
B. The degree to which the pain interferes with thechild’s activities should be defined. Family function,school performance, anxiety, depression, or socialmaladjustment should be assessed. Medication useshould be assessed.
“Red Flags” on History of Recurrent AbdominalPain
• Localization of the pain away from the umbilicus • Pain associated with change in bowel habits, particularlydiarrhea, constipation, or
nocturnal bowel movements • Pain associated with night wakening • Repetitive emesis, especially if bilious • Constitutional symptoms, such as recurrent fever, loss ofappetite or energy • RAP occurring in a child younger than 4 years of age
C. Physical Examination. Height and weight shouldbe recorded and compared to previous growth data.The abdomen should be examined gently andthoroughly while observing the child’s response topalpation. The perianal area should be examined forfissures, skin tags, or signs of sexual abuse. A rectalexamination is not routinely performed.

“Red Flags” on Physical Examination for Recur-rent Abdominal Pain
• Loss of weight or decline in height velocity • Organomegaly• Localized abdominal tenderness, particularly removed from
the umbilicus • Perirectal abnormalities (eg, fissures, ulceration, or skin
tags) • Joint swelling, redness, or heat • Ventral hernias of the abdominal wall
IV. InvestigationsA. Laboratory investigations should usually be limited
to a complete blood count, urinalysis, and examina-tion of a stool specimen for occult blood. In thepresence of diarrhea, a stool for enteric culture andova and parasite examination is indicated.
B. Radiography. A single view of the abdomen can beuseful to confirm constipation.
C. Abdominal ultrasonography can be valuable whenobstructive uropathy hydronephrosis, ovarian cysts,or gall bladder disorders are suspected. Entericduplication also may be revealed by ultrasonography.Ultrasound is appropriate when the pain islateralized, when there are abnormalities on urinaly-sis, or when the pain localizes to the lower quadrantsin a female.
D. Erythrocyte sedimentation rate, serum protein andalbumin levels, and stool for occult blood should beobtained. If IBD is a possible diagnosis. Endoscopyand biopsy will confirm the diagnosis. Upper gastroin-testinal endoscopy with biopsies will confirm thediagnosis when the pattern of pain strongly suggestspeptic ulcer disease.
V. ManagementA. Functional recurrent abdominal pain will be the
diagnosis in the majority of cases. The parentsshould maintain a sympathetic attitude that acknowl-edges the pain but encourages continued activitiesand school attendance. Parents should refrain fromquestioning the child about the pain if the child is notcomplaining. A trial of increasing fiber by dietarymodification may be useful.
B. Psychogenic pain may respond to the interventionof a psychologist or psychiatrist.
C. Constipation requires treatment with regular stoolsofteners, preceded by an enema.
D. Lactose malabsorption. A lactose-free diet forseveral weeks with lactase-treated milk should betried. Ice cream and cheese should be avoided.
E. Enteric infections or infestations require treatmentwith appropriate medications. Abdominal migrainemay warrant a trial of migraine prophylaxis. Prophy-lactic pizotifen, cyproheptadine, propranolol, or ami-triptyline could be considered.
References, see page 182.
Chronic Nonspecific Diarrhea
Diarrhea is considered chronic when it persists for longerthan 3 weeks. Chronic nonspecific diarrhea (CNSD)presents in toddlers between 18 months and 3 years ofage, with frequent, large, watery stools in the absence ofphysical or laboratory signs of malabsorption or infectionand without effect on growth or development. Childrenhave 3 to 6 large, watery bowel movements daily. Thediarrhea spontaneously resolves in 90% of children by 40months of age.
I. PathogenesisA. Factors causing CNSD
1. Excess fluid intake2. Carbohydrate malabsorption from excessive juice
ingestion3. Disordered intestinal motility4. Excessive fecal bile acids5. Low fat intake
B. CNSD occurs when fluid intake exceeds the absorp-tive capacity of the intestinal tract. Malabsorption ofcarbohydrates (sucrose, fructose, sorbitol) in fruitjuices contributes to CNSD.
C. CNSD presents between 18 months and 3 years,with 3-6 large, loose, watery stools per day for morethan 3 weeks.
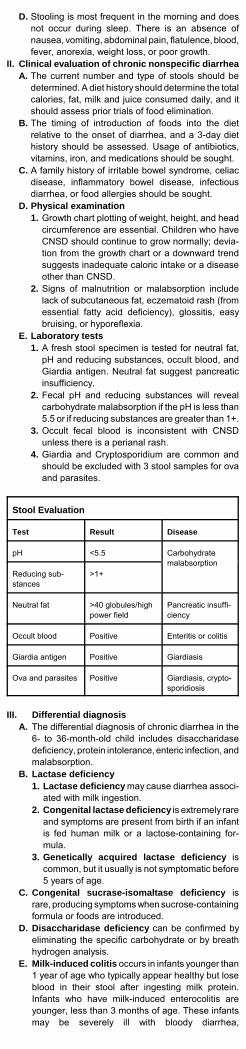
D. Stooling is most frequent in the morning and doesnot occur during sleep. There is an absence ofnausea, vomiting, abdominal pain, flatulence, blood,fever, anorexia, weight loss, or poor growth.
II. Clinical evaluation of chronic nonspecific diarrheaA. The current number and type of stools should be
determined. A diet history should determine the totalcalories, fat, milk and juice consumed daily, and itshould assess prior trials of food elimination.
B. The timing of introduction of foods into the dietrelative to the onset of diarrhea, and a 3-day diethistory should be assessed. Usage of antibiotics,vitamins, iron, and medications should be sought.
C. A family history of irritable bowel syndrome, celiacdisease, inflammatory bowel disease, infectiousdiarrhea, or food allergies should be sought.
D. Physical examination1. Growth chart plotting of weight, height, and head
circumference are essential. Children who haveCNSD should continue to grow normally; devia-tion from the growth chart or a downward trendsuggests inadequate caloric intake or a diseaseother than CNSD.
2. Signs of malnutrition or malabsorption includelack of subcutaneous fat, eczematoid rash (fromessential fatty acid deficiency), glossitis, easybruising, or hyporeflexia.
E. Laboratory tests1. A fresh stool specimen is tested for neutral fat,
pH and reducing substances, occult blood, andGiardia antigen. Neutral fat suggest pancreaticinsufficiency.
2. Fecal pH and reducing substances will revealcarbohydrate malabsorption if the pH is less than5.5 or if reducing substances are greater than 1+.
3. Occult fecal blood is inconsistent with CNSDunless there is a perianal rash.
4. Giardia and Cryptosporidium are common andshould be excluded with 3 stool samples for ovaand parasites.
Stool Evaluation
Test Result Disease
pH <5.5 Carbohydratemalabsorption
Reducing sub-stances
>1+
Neutral fat >40 globules/highpower field
Pancreatic insuffi-ciency
Occult blood Positive Enteritis or colitis
Giardia antigen Positive Giardiasis
Ova and parasites Positive Giardiasis, crypto-sporidiosis
III. Differential diagnosisA. The differential diagnosis of chronic diarrhea in the
6- to 36-month-old child includes disaccharidasedeficiency, protein intolerance, enteric infection, andmalabsorption.
B. Lactase deficiency1. Lactase deficiency may cause diarrhea associ-
ated with milk ingestion.2. Congenital lactase deficiency is extremely rare
and symptoms are present from birth if an infantis fed human milk or a lactose-containing for-mula.
3. Genetically acquired lactase deficiency iscommon, but it usually is not symptomatic before5 years of age.
C. Congenital sucrase-isomaltase deficiency israre, producing symptoms when sucrose-containingformula or foods are introduced.
D. Disaccharidase deficiency can be confirmed byeliminating the specific carbohydrate or by breathhydrogen analysis.
E. Milk-induced colitis occurs in infants younger than1 year of age who typically appear healthy but loseblood in their stool after ingesting milk protein.Infants who have milk-induced enterocolitis areyounger, less than 3 months of age. These infantsmay be severely ill with bloody diarrhea,

hypoproteinemia, and growth failure. Children whohave protein allergies tend to come from familiesthat have allergic histories, and affected childrenmay have eczema, allergic rhinitis, asthma.
F. Giardia or Cryptosporidium enteric infectionsare commonly transmitted by asymptomatic carriersat child care centers. Foul-smelling diarrhea usuallyis associated with abdominal distension and flatus.Diagnosis is confirmed by Giardia antigen in stool orthree stools for ova and parasites.
G. Malabsorption presents with chronic diarrhea,weight loss, poor appetite, weakness and de-creased activity, bloating and flatulence, abdominalpain, and chronic vomiting. The most commoncauses are cystic fibrosis and celiac disease.Chronic diarrhea and failure to thrive warrants asweat test. Screening for celiac disease consists ofa D-xylose absorption test and a serum celiacdisease panel (antigliadin, antiendomysial, andantireticulin antibodies). Celiac disease must beconfirmed by intestinal biopsy.
IV. Management of CNSDA. Fluid intake should be reduced to less than 100
mL/kg/day. Water is substituted for juice to reducethe child’s interest in drinking. Switching from thebottle to the cup also decreases fluid intake.
B. Fat intake is increased to 4 g/kg/day by addingwhole milk to the diet. If lactose intolerance ispresent, low-lactose milk can be used or lactasedrops can be added to milk. Butter, margarine, orvegetable oil are liberally added to foods for childrenless than 2 years of age.
C. Dietary fiber can be increased by consumption offresh fruits and vegetables or by the addition ofbran.
References, see page 182.
Constipation
Constipation is common in infants and children. Theproblem usually resolves after modification of the child’sfluid and dietary regimen.
I. PathophysiologyA. Persistent difficulty with the passage of stool may
lead to impaction, stool withholding, and fecalsoiling.
Conditions Associated With Constipation
Condition Common Causes
Lack of Fecal Bulk High-carbohydrate or high-pro-tein dietUndernutrition
Abnormally Hard Stools Excessive cow milk intake
Abnormally Dry Stools DehydrationInfantile renal acidosisDiabetes insipidusIdiopathic hypercalcemia
Nervous System Lesion Spinal cord lesions
Mechanical Obstruction Anorectal stenotic lesionsIntrinsic and extrinsic massesStricturesAganglionosis (Hirschsprungdisease)
Diseases That ComplicateDefecation
Amyotonia congenitaCerebral palsyHypertoniaHypothyroidism
II. Neonates and infants younger than 1 year of age A. Evaluation of constipation in neonates and
infants1. Inadequate fluid intake, undernutrition, and
excessive cow milk intake should be excludedduring the history.
2. Anal inspection at the time of birth revealsanorectal anomalies in one in every 2,500 livebirths. Anal stenosis accounts for 20% of theseabnormalities. The anus appears very small witha central black dot of meconium, and the infant

must make an intense effort to pass a ribbon-likestool. The abdomen may be distended and stoolcan often be palpated on abdominal examination.
3. Hirschsprung diseasea. Hirschsprung disease accounts for 20-25% of
cases of neonatal obstruction, and it is morecommon in males. Symptoms develop duringthe first month of life in 80%. The majority ofinfants are unable to pass stool normallyduring the first week.
b. Infants with Hirschsprung disease usually failto pass meconium during the first 48 hours oflife. The abdomen is usually distended andtympanitic. Abdominal peristaltic activity maybe visible, and fecal masses may be palpable.The anal canal and rectum are empty of feces.
c. Plain abdominal radiographs reveal gas andstool in the colon above the rectum. Arectosigmoid index (the diameter of the rectumdivided by the diameter of the sigmoid) of lessthan one is consistent with Hirschsprungdisease.
d. When findings from the history, physical, andplain abdominal radiographs suggestHirschsprung disease, contrast examination ofthe unprepared colon should be obtained. Thediagnosis is confirmed by endoscopic biopsy.
B. Management of simple constipation in infants1. Dietary corrective measures are the initial therapy
for infants with simple constipation. Increasingfluid intake and adding carbohydrate sugar to theformula often corrects the problem.
2. Infants that do not respond to dietary measuresare treated with a mineral oil preparation. Routinesuppository administration, enemas, and stimu-lant laxatives should be avoided.
III. Older infants and childrenA. Evaluation
1. Fluid and dietary fiber intake should be assessed.Older children with chronic constipation and stoolwithholding usually also have fecal incontinence.
2. Moveable fecal masses are often appreciated inthe left colon and sigmoid.
3. The lower back should be examined for a deeppilonidal dimple with hair tuft and/or sacralagenesis, suggestive of myelodysplasia. Analinspection may reveal primary anal disease.Normal anal tone found on rectal examinationindicates normal anal innervation. The rectalvault may be filled with inspissated stool.
4. Anteroposterior and lateral x-rays of the abdo-men usually reveal a large rectal/rectosigmoidimpaction with variable amounts of stool through-out the remainder of the colon.
B. Management of chronic constipation1. Distal impaction should be removed with
hypertonic phosphate enemas (Fleet enema).Usually three enemas are administered during a36- to 48-hour period.
2. Mineral oil should be prescribed. The initial doseof mineral oil is 30-75 mL twice daily. Mineral oilis tasteless, and it can be taken with fruit juice,Kool-Aid, or a soft drink. After one month, the oilis tapered by 15 mL (0.5 oz) per dose. Haley’sMO is a mineral oil solution of 1.4 gm/5 mL.
3. The child should sit on the toilet, with proper footsupport, for five minutes after the evening meal totake advantage of the gastrocolic reflex. Abulk-type stool softener (eg, Metamucil) shouldbe initiated when the mineral oil dosage has beentapered to 15 mL twice daily.
References, see page 182.
Gastroenteritis
Acute gastroenteritis consists of diarrheal disease of rapidonset, often with nausea, vomiting, fever, or abdominalpain. It occurs an average of 1.3-2.3 times per yearbetween the ages of 0 and 5 years. Most episodes ofacute gastroenteritis will resolve within 3 to 7 days.
I. Pathophysiology. Gastroenteritis in children is causedby viral, bacterial, and parasitic organisms, althoughthe vast majority of cases are viral or bacterial in origin.

II. Viral gastroenteritisA. All of the viruses produce watery diarrhea often
accompanied by vomiting and fever, but usually notassociated with blood or leukocytes in the stool orwith prominent cramping.
B. Rotavirus is the predominant viral cause of dehy-drating diarrhea. Rotaviral infections tend to pro-duce severe diarrhea, causing up to 70% of epi-sodes in children under 2 years of age who requirehospitalization. Rotavirus infection tends to occur inthe fall in the southwest of the US, then sweepingprogressively eastward, reaching the northeast bylate winter and spring.
C. Norwalk viruses are the major cause of largeepidemics of acute nonbacterial gastroenteritis,occurring in schools, camps, nursing homes, cruiseships, and restaurants.
D. Enteric adenovirus is the third most commonorganism isolated in infantile diarrhea.
III. Bacterial gastroenteritisA. The bacterial diarrheas are caused by elaboration
of toxin (enterotoxigenic pathogens) or by invasionand inflammation of the mucosa (invasive patho-gens).
B. Secretory diarrheas are modulated through anenterotoxin, and the patient does not have fever ormyalgias or tenesmus, or white or red blood cells inthe stool. The diarrhea is watery, often is large involume, and often associated with nausea andvomiting.
C. Invasive diarrhea is caused by bacterialenteropathogens, and is accompanied by systemicsigns, such as fever, myalgias, arthralgias, irritabil-ity, and loss of appetite. Cramps and abdominalpain are prominent. The diarrhea consists of fre-quent passing of small amounts of stool within themucus. Stool examination reveals leukocytes, redblood cells, and often gross blood.
Acute Diarrhea Patterns and Associated Patho-gens
Secretory/enterotoxigenic Inflammatory
Characterized by watery diar-rhea and absence of fecalleukocytes
Characterized by dysentery(ie, fever and bloody stools),fecal leukocytes, and erythro-cytes
Food poisoning (toxigenic)
Staphylococcus aureusBacillus cereusClostridium perfringens
Shigella Invasive E coli SalmonellaCampylobacter
Enterotoxigenic
Escherichia coliVibrio choleraGiardia lambliaCryptosporidiumRotavirusNorwalk-like virus
C difficileEntameba histolytica
IV. General approach to the patient withgastroenteritis
A. Determining and managing the fluid losses,dehydration and electrolyte abnormalities ismore important than ascertaining the specificmicrobiologic cause.
B. History should assess recent antibiotic use, under-lying diseases, other illnesses in the family, travel,untreated water, raw shellfish, attendance at a childcare center, and foods eaten recently.
Clinical Evaluation and Treatment of Acute Diarrhea
Step One--Assess child for degree of dehydration
No dehydration Continue oral hydration and feed-ing
Mild/severe dehydration--------->
Initiate rehydration by oral route(intravenous for severely dehy-drated patients)
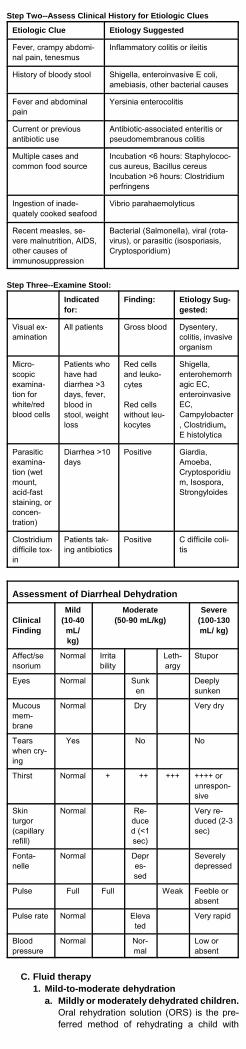
Step Two--Assess Clinical History for Etiologic Clues
Etiologic Clue Etiology Suggested
Fever, crampy abdomi-nal pain, tenesmus
Inflammatory colitis or ileitis
History of bloody stool Shigella, enteroinvasive E coli,amebiasis, other bacterial causes
Fever and abdominalpain
Yersinia enterocolitis
Current or previousantibiotic use
Antibiotic-associated enteritis orpseudomembranous colitis
Multiple cases andcommon food source
Incubation <6 hours: Staphylococ-cus aureus, Bacillus cereusIncubation >6 hours: Clostridiumperfringens
Ingestion of inade-quately cooked seafood
Vibrio parahaemolyticus
Recent measles, se-vere malnutrition, AIDS,other causes ofimmunosuppression
Bacterial (Salmonella), viral (rota-virus), or parasitic (isosporiasis,Cryptosporidium)
Step Three--Examine Stool:
Indicatedfor:
Finding: Etiology Sug-gested:
Visual ex-amination
All patients Gross blood Dysentery,colitis, invasiveorganism
Micro-scopicexamina-tion forwhite/redblood cells
Patients whohave haddiarrhea >3days, fever,blood instool, weightloss
Red cellsand leuko-cytes
Red cellswithout leu-kocytes
Shigella,enterohemorrhagic EC,enteroinvasiveEC,Campylobacter, Clostridium,E histolytica
Parasiticexamina-tion (wetmount,acid-faststaining, orconcen-tration)
Diarrhea >10days
Positive Giardia,Amoeba,Cryptosporidium, Isospora,Strongyloides
Clostridiumdifficile tox-in
Patients tak-ing antibiotics
Positive C difficile coli-tis
Assessment of Diarrheal Dehydration
ClinicalFinding
Mild(10-40
mL/kg)
Moderate(50-90 mL/kg)
Severe(100-130mL/ kg)
Affect/sensorium
Normal Irritability
Leth-argy
Stupor
Eyes Normal Sunken
Deeplysunken
Mucousmem-brane
Normal Dry Very dry
Tearswhen cry-ing
Yes No No
Thirst Normal + ++ +++ ++++ orunrespon-sive
Skinturgor(capillaryrefill)
Normal Re-duced (<1sec)
Very re-duced (2-3sec)
Fonta-nelle
Normal Depres-sed
Severelydepressed
Pulse Full Full Weak Feeble orabsent
Pulse rate Normal Elevated
Very rapid
Bloodpressure
Normal Nor-mal
Low orabsent
C. Fluid therapy1. Mild-to-moderate dehydration
a. Mildly or moderately dehydrated children.Oral rehydration solution (ORS) is the pre-ferred method of rehydrating a child with
dehydration. In most western countries,rotavirus is the most common cause of child-hood diarrhea. In such patients, Pedialyte,Infalyte, Ceralyte, Naturalyte or PediatricElectrolyte is appropriate. ORS should begiven at 50 mL/kg (mild dehydration) or 100mL/kg (moderate dehydration) over a 4-hourperiod. Replacement of stool losses (at 10mL/kg for each stool) and of emesis (esti-mated volume) will require adding appropri-ate amounts of solution to the total.
2. Prevention of dehydrationa. Children who have diarrhea, but not dehy-
drated, may be given glucose-electrolytesolution in addition to their regular diets toreplace stool losses. The well-hydrated childshould continue to consume an age-appropri-ate diet and drink more than the usualamounts of the normal fluids.
b. The diet should emphasize complex carbohy-drates, such as starches, cereal, and freshfruits and vegetables, with no sugary or fattyfoods. Apple juice and soft drinks, such ascola, should be avoided, whereas sportsdrinks, such as Gatorade, are generally welltolerated. If the child is breast fed, breast-feeding should be continued.
3. Severely dehydrated children who are in astate of shock must receive immediate andaggressive intravenous (IV) therapy. When thepatient is stable, hydration may be continuedorally.
4. Intravenous rehydrationa. When intravenous rehydration is required, it
should begin with an isotonic solution (normalsaline, lactated Ringer). Severe dehydrationclinically is associated with a loss of 10-12%of body weight in fluids and electrolytes (100to 120 mL/kg); therefore, this amount plusadditional losses should be infused.
b. Infusion rates of up to 100 mL/min are appro-priate in older children. Infusion rates of 40mL/kg are given over the first 30 minutes,with the remainder of the deficit (70 mL/kg)over the next 2.5 hours, until the calculatedfluid loss has been replenished.
c. For infants, correction should be slower, withinfusion rates no more than 30 mL/kg overthe first hour and the remaining 70 mL/kgover 5 hours.
d. Subsequent maintenance fluids should begiven orally. Oral fluids should be initiated assoon as the patient can drink. They should begiven simultaneously with intravenous fluidsuntil the total fluids administered have replen-ished the calculated deficit.
D. Antibiotic therapy. The effectiveness ofantimicrobial therapy is well established inshigellosis. Shigella is the cause of bacterial dysen-tery and is the second most commonly identifiedbacterial pathogen in diarrhea between the ages of6 months and 10 years. It causes watery diarrheawith mucus and gross blood. Treatment consists ofceftriaxone or cefixime.
E. Refeeding1. Children who have diarrhea and are not dehy-
drated should continue to be fed age-appropriatediets. Fatty foods and foods high in simplesugars, such as juices and soft drinks should beavoided. Well-tolerated foods include complexcarbohydrates (rice, wheat, potatoes, bread,cereals), lean meats, yogurt, fruits, and vegeta-bles. The BRAT diet (bananas, rice, applesauce,toast) does not supply optimal nutrition.
2. Introducing the child’s regular form of milk earlyin the course of therapy is recommended.
F. Antidiarrheal compounds (eg, loperamide,diphenoxylate, bismuth compounds, Kaopectate)should not be used to treat acute diarrhea.
V. Laboratory examinationsA. The presence of blood in the stool, fever, or persis-
tence of the diarrhea for more than 3 days maytrigger a laboratory pursuit of an etiologic agent.
B. Microscopic stool examination. If erythrocytesand white blood cells are present, particularly in thesetting of fever, a bacterial pathogen(Campylobacter, Yersinia, Salmonella, Shigella)

should be suspected. Many red blood cells in theabsence of white blood cells suggests the presenceof Entamoeba.
C. Stool culture should be reserved for individualswhose diarrhea has not responded to fluid andfeeding and for those who have fever and thepresence of leukocytes or red blood cells in thestool.
D. Rotavirus should be suspected in a one-year-oldpresenting in the winter months with a three-dayhistory of vomiting and watery diarrhea with milddehydration. Laboratory evaluation in this setting isgenerally not indicated. If the diagnosis is unclear,stool for viral particles or rotavirus antigen(Rotazyme [R]) may be helpful.
References, see page 182.
Gastroesophageal Reflux
Gastroesophageal reflux (GER) is a common conditioninvolving regurgitation. GER implies a functional orphysiologic process in a healthy infant with no underlyingsystemic abnormalities. The prevalence of GER peaksbetween one to four months of age, and usually resolvesby six to 12 months of age. Regurgitation occurs in 40 to65 percent of healthy infants. Gastroesophageal reflux disease (GERD) is a patho-logic process in infants manifested by poor weight gain,signs of esophagitis, persistent respiratory symptoms, andchanges in neurobehavior. GERD occurs in approximatelyone in 300 infants.
I. Clinical manifestations A. Infants with GER regurgitate without inadequate
growth, esophagitis, or respiratory disease. Infantswith GER are thriving and represent the majority ofinfants who present with this condition.
B. Patients with GERD may manifest persistent regurgi-tation with secondary poor weight gain and failure tothrive. Other infants may manifest signs ofesophagitis, including persistent irritability, pain,feeding problems, and iron deficiency anemia.
II. Diagnostic evaluation. In most cases of GER, nodiagnostic study is required. Although scintigraphy maybest quantify gastric emptying or aspiration, it is not ascommonly used as the upper GI examination (bariumfluoroscopy).
III. Management A. Conservative treatment of GER involves thickened
feedings and positional changes in infants, anddietary modification in children. Healthy infants whoregurgitate may be managed by thickening feedingswith up to one tablespoon of dry rice cereal per 1 ozof formula.
B. Smaller, more frequent feedings are recommendedin older infants and children. Completely upright andprone positioning is beneficial in infants with GERD.Soft bedding materials should be avoided in thissetting. Prone positioning is not routinely recom-mended as first-line management of simple regurgi-tation without evidence of GERD.
C. Pharmacologic management1. H2-receptor antagonists
a. Cimetidine (Tagamet). The recommendedstarting dosage is 10 mg per kg per dose fourtimes daily before meals and at bedtime foreight weeks. Potential side effects includeheadaches, dizziness, diarrhea, andgynecomastia.
b. Ranitidine (Zantac) 1-2 mg per kg per dosetwo to three times daily (2-6 mg per kg perday) is the starting dosage. Potential sideeffects include headaches and malaise, butranitidine has fewer central nervous systemand anti-androgenic side effects.
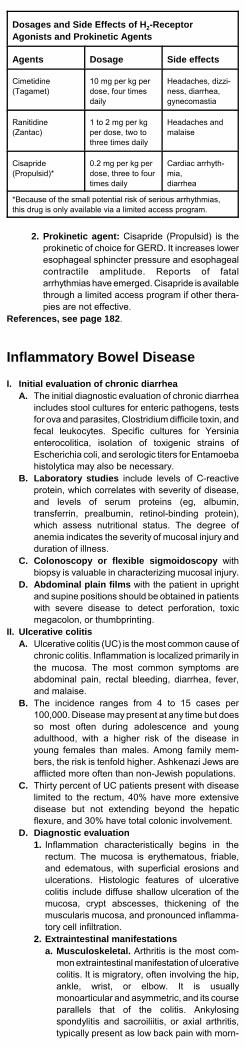
Dosages and Side Effects of H2-ReceptorAgonists and Prokinetic Agents
Agents Dosage Side effects
Cimetidine(Tagamet)
10 mg per kg perdose, four timesdaily
Headaches, dizzi-ness, diarrhea,gynecomastia
Ranitidine(Zantac)
1 to 2 mg per kgper dose, two tothree times daily
Headaches andmalaise
Cisapride(Propulsid)*
0.2 mg per kg perdose, three to fourtimes daily
Cardiac arrhyth-mia,diarrhea
*Because of the small potential risk of serious arrhythmias,this drug is only available via a limited access program.
2. Prokinetic agent: Cisapride (Propulsid) is theprokinetic of choice for GERD. It increases loweresophageal sphincter pressure and esophagealcontractile amplitude. Reports of fatalarrhythmias have emerged. Cisapride is availablethrough a limited access program if other thera-pies are not effective.
References, see page 182.
Inflammatory Bowel Disease
I. Initial evaluation of chronic diarrheaA. The initial diagnostic evaluation of chronic diarrhea
includes stool cultures for enteric pathogens, testsfor ova and parasites, Clostridium difficile toxin, andfecal leukocytes. Specific cultures for Yersiniaenterocolitica, isolation of toxigenic strains ofEscherichia coli, and serologic titers for Entamoebahistolytica may also be necessary.
B. Laboratory studies include levels of C-reactiveprotein, which correlates with severity of disease,and levels of serum proteins (eg, albumin,transferrin, prealbumin, retinol-binding protein),which assess nutritional status. The degree ofanemia indicates the severity of mucosal injury andduration of illness.
C. Colonoscopy or flexible sigmoidoscopy withbiopsy is valuable in characterizing mucosal injury.
D. Abdominal plain films with the patient in uprightand supine positions should be obtained in patientswith severe disease to detect perforation, toxicmegacolon, or thumbprinting.
II. Ulcerative colitisA. Ulcerative colitis (UC) is the most common cause of
chronic colitis. Inflammation is localized primarily inthe mucosa. The most common symptoms areabdominal pain, rectal bleeding, diarrhea, fever,and malaise.
B. The incidence ranges from 4 to 15 cases per100,000. Disease may present at any time but doesso most often during adolescence and youngadulthood, with a higher risk of the disease inyoung females than males. Among family mem-bers, the risk is tenfold higher. Ashkenazi Jews areafflicted more often than non-Jewish populations.
C. Thirty percent of UC patients present with diseaselimited to the rectum, 40% have more extensivedisease but not extending beyond the hepaticflexure, and 30% have total colonic involvement.
D. Diagnostic evaluation1. Inflammation characteristically begins in the
rectum. The mucosa is erythematous, friable,and edematous, with superficial erosions andulcerations. Histologic features of ulcerativecolitis include diffuse shallow ulceration of themucosa, crypt abscesses, thickening of themuscularis mucosa, and pronounced inflamma-tory cell infiltration.
2. Extraintestinal manifestationsa. Musculoskeletal. Arthritis is the most com-
mon extraintestinal manifestation of ulcerativecolitis. It is migratory, often involving the hip,ankle, wrist, or elbow. It is usuallymonoarticular and asymmetric, and its courseparallels that of the colitis. Ankylosingspondylitis and sacroiliitis, or axial arthritis,typically present as low back pain with morn-

ing stiffness.b. Ocular. Episcleritis, uveitis, and iritis may
occur.c. Dermatologic. Abnormalities may include
erythema nodosum, pyoderma gangrenosum,lichen planus, and aphthous ulcers.
d. Hepatobiliary. Manifestations may includehepatic steatosis, primary sclerosingcholangitis (4%), cholelithiasis, andpericholangitis.
e. Miscellaneous. Other complications includenephrolithiasis and a hypercoagulable state.
III. Crohn diseaseA. Crohn disease (CD) is a chronic inflammatory
process, which may involve any portion of thegastrointestinal tract from the mouth to the anus.Inflammation is characterized by transmural exten-sion and irregular involvement of the intestinal tract,with intervening normal tissue (“skip areas”). Mostoften, the distal ileum and proximal colon areinvolved; in about 25% of cases, only the colon isaffected.
B. Crohn disease often has its onset during adoles-cence and young adulthood. It is more common infemales. The overall risk is two to four times higherin first-degree relatives.
C. Fever, abdominal pain, diarrhea, weight loss, andfatigue are common. Rectal bleeding is not asprominent a feature in Crohn disease as it is inulcerative colitis. About 20% of patients haveevidence of perianal disease, such as perirectalfistulas, anal skin tags, anal ulcerations or fissures,or perirectal abscesses. Crohn disease causesextra-intestinal manifestations like those of ulcer-ative colitis.
D. Diagnostic evaluation1. Anemia, caused by chronic blood loss and a
mildly elevated white blood cell count are com-mon.
2. Endoscopic findings include focal ulcerationsand inflammation is interrupted by skip areas.Other features of Crohn disease include rectalsparing, cobblestone appearance, strictures, andileal involvement.
IV. Management of ulcerative colitisA. Mild-to-moderate cases of ulcerative colitis
1. Mesalamine (Asacol) is an oral 5-ASA com-pound used for active ulcerative colitis, andolsalazine sodium (Dipentum) is used for main-tenance therapy. The target dosage for the tabletAsacol (in divided doses) is 2.4 g/day, the cap-sule (Pentasa) 4 g/day, and capsule olsalazine(Dipentum) 1 g/day.
2. Limited left-sided colonic disease orrectosigmoid disease may respond to localtherapy (enemas, suppositories) withcorticosteroids and mesalamine.
3. Rectal preparations of mesalamine (Rowasaenema and suppository) can deliver higherconcentrations to the distal colon for proctitis.Rowasa (4 g) is the only enema preparation of 5-ASA.
4. Balsalazide (Colazal). Balsalazide, a prodrug ofmesalamine (5-aminosalicylic acid) for oraltreatment of mildly to moderately active ulcer-ative colitis. Patients treated with balsalazide aremore likely to achieve a symptomatic remission(88% vs 57%) or a complete remission (62% vs37%), and became asymptomatic in 10 dayscompared to 25 days with delayed-releasemesalamine.
B. Moderately severe cases of ulcerative colitis1. These patients may require rehydration or blood
transfusion. Corticosteroids, a low-residue diet,and local therapy should be initiated.
2. Prednisone usually is started at a dose of 1 to 2mg/kg per day for 1 to 2 weeks. Once the patienthas stabilized, the patient is weaned off thesteroids to alternate-day therapy over 4 to 8weeks; mesalamine (Asacol) is usually started.Hydrocortisone retention enema (Cortenema), iseffective for distal ulcerative colitis.
C. Fulminant ulcerative colitis requires immediatehospitalization. 1. Fluid and electrolyte status must be stabilized
and blood transfusions given as needed. Intrave-nous corticosteroids (methylprednisolone),

broad-spectrum antibiotics (metronidazole, anaminoglycoside, and ampicillin), parenteralnutrition, and bowel rest are initiated.
2. If the patient deteriorates clinically or developscomplications (hemorrhage, toxic megacolon),emergency surgery is performed. If the patienthas not improved for 2 to 4 weeks after maximalmedical therapy, a colectomy should be consid-ered. Surgery is curative for UC.
Treatment of Inflammatory Bowel Disease
Dose/day
Route
Side Effects
5-Aminosalicylic Acid
Mesalamine(Asacol)Mesalamine(Rowasa)
EnemaSupposi-tory
Mesalamine(Pentasa)Olsalazine(Dipentum)Basalazine(Colazal)
30-50mg/kg
2-4 g qd
500 mgbid
50-60mg/kg
20-30mg/kg
2.25 g tid
PO
PR PRPO
PO
PO
Nephrotoxicity
Chills, diarrhea
Local irritation
Nephrotoxicity
Watery diarrhea
Steroids
Prednisone 1-2mg/kg
PO Osteoporosis, hyper-tension, poor growth,obesity, hirsutism,cataracts, adrenalsuppression
Methylprednisolone
0.8-1.6mg/kg
PO Same as for predni-sone
Hydrocorti-sone
Enema
Foam
100 mgQD-BID80 mgQD-BID
PR
PR
Local irritation
Same as enema
Immunosuppressants
6-mercaptopurine
1-1.5mg/kg
PO Pancreatitis, bonemarrow suppression
Azathioprine 1.5-2mg/kg
PO Same as for 6-mercaptopurine
Cyclosporine 2-4mg/kg 4-6mg/kg
IV PO
Nephrotoxicity Hirsutism, hyperten-sion
Antibiotics
Metronidazole 10-20mg/kg
PO/IV
Peripheral neuropa-thy, metallic taste
Miscellaneous
Folic acid 1 mg PO
V. Management of Crohn disease. Treatment is similarto that of ulcerative colitis. Corticosteroids andmesalamine (Asacol) are the mainstays of therapy.Patients with severe colitis, massive weight loss, andsignificant systemic symptoms may need to behospitalized. Prednisone can induce a remission in70% of patients who have small bowel disease.A. Antibiotics (metronidazole and ciprofloxacin) are
useful in mild-to-moderate CD and perianal disease.B. Immunosuppressive agents. Mercaptopurine and
azathioprine are reserved for patients with continu-ous disease activity despite corticosteroid therapy.Cyclosporine may be beneficial in refractory pa-tients.
C. Surgery for Crohn disease is not curative. Indica-tions include obstruction or intractable symptoms.Disease almost always recurs after surgery.
References, see page 182.

Persistent Vomiting
Vomiting is defined as the forceful expulsion of gastriccontents through the mouth. Vomiting can be caused by abenign, self-limited process or it may be indicative of aserious underlying disorder.
I. Pathophysiology of vomitingA. Vomiting is usually preceded by nausea, increased
salivation, and retching. It is distinct from regurgita-tion, which is characterized by passive movement ofgastric contents into the esophagus.
B. Projectile vomiting results from intense gastricperistaltic waves, usually secondary to gastric outletobstruction caused by hypertrophic pyloric stenosisor pylorospasm.
C. Retching often precedes vomiting and is character-ized by spasmodic contraction of the expiratorymuscles with simultaneous abdominal contraction.
II. Clinical evaluation of vomiting
Etiology of Vomiting by Age
Newborn Infant Older Child
Obstruction Malrotationof bowelVolvulusIntestinalatresiaIntestinalstenosisMeconiumileusMeconiumplugHirschsprung diseaseImperforateanusIncarceratedhernia
Pyloric ste-nosis Foreign bod-iesMalrotation(volvulus)Duplicationof alimentarytractIntussusceptionMeckeldiverticulumHirschsprung diseaseIncarceratedhernia
IntussusceptionForeign bod-iesMalrotation(volvulus)MeckeldiverticulumHirschsprung diseaseIncarceratedherniaAdhesions
Gastroin-testinal dis-orders(infecti-ous/inflam-matory)
NecrotizingenterocolitisGastroesophageal refluxParalyticileusPeritonitisMilk allergy
GastroenteritisGastroesophageal refluxPancreatitisAppendicitisCeliac dis-easeParalyticileusPeritonitis
GastroenteritisPeptic ulcerdisease
Infectiousdisorders(nongastro-intestinal)
SepsisMeningitis
SepsisMeningitisOtitis mediaPneumoniaPertussis HepatitisUrinary tractinfection
MeningitisOtitis mediaPharyngitisPneumoniaHepatitisUrinary tractinfection
Neurologicdisorders
Hydrocepha-lusKernicterusSubduralhematomaCerebraledema
Hydrocepha-lusSubduralhematomaIntracranialhemorrhageMass lesion(abscess,tumor)
SubduralhematomaIntracranialhemorrhageBrain tumorOther mass-occupyinglesionMigraineMotion sick-nessHypertensiveencephalopathy
Metabolicand endo-crine disor-ders
Inborn errorsof metabo-lism: Ureacycle de-fects, galac-tosemia, dis-orders oforganic acidmetabolismCongenitaladrenal hy-perplasiaNeonataltetany
Inborn errorsof metabo-lismFructoseintolerance AdrenalinsufficiencyMetabolicacidosis
AdrenalinsufficiencyDiabeticketoacidosis
Renal disor-ders
Obstructiveuropathy Renal insuf-ficiency
ObstructiveuropathyRenal insuf-ficiency
ObstructiveuropathyRenal insuffi-ciency
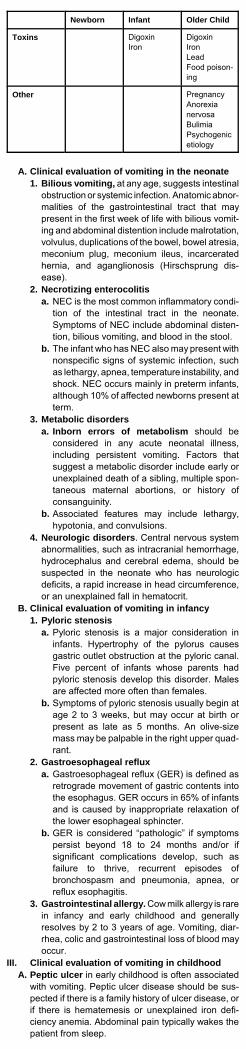
Newborn Infant Older Child
Toxins DigoxinIron
DigoxinIronLeadFood poison-ing
Other PregnancyAnorexianervosaBulimiaPsychogenicetiology
A. Clinical evaluation of vomiting in the neonate1. Bilious vomiting, at any age, suggests intestinal
obstruction or systemic infection. Anatomic abnor-malities of the gastrointestinal tract that maypresent in the first week of life with bilious vomit-ing and abdominal distention include malrotation,volvulus, duplications of the bowel, bowel atresia,meconium plug, meconium ileus, incarceratedhernia, and aganglionosis (Hirschsprung dis-ease).
2. Necrotizing enterocolitisa. NEC is the most common inflammatory condi-
tion of the intestinal tract in the neonate.Symptoms of NEC include abdominal disten-tion, bilious vomiting, and blood in the stool.
b. The infant who has NEC also may present withnonspecific signs of systemic infection, suchas lethargy, apnea, temperature instability, andshock. NEC occurs mainly in preterm infants,although 10% of affected newborns present atterm.
3. Metabolic disordersa. Inborn errors of metabolism should be
considered in any acute neonatal illness,including persistent vomiting. Factors thatsuggest a metabolic disorder include early orunexplained death of a sibling, multiple spon-taneous maternal abortions, or history ofconsanguinity.
b. Associated features may include lethargy,hypotonia, and convulsions.
4. Neurologic disorders. Central nervous systemabnormalities, such as intracranial hemorrhage,hydrocephalus and cerebral edema, should besuspected in the neonate who has neurologicdeficits, a rapid increase in head circumference,or an unexplained fall in hematocrit.
B. Clinical evaluation of vomiting in infancy1. Pyloric stenosis
a. Pyloric stenosis is a major consideration ininfants. Hypertrophy of the pylorus causesgastric outlet obstruction at the pyloric canal.Five percent of infants whose parents hadpyloric stenosis develop this disorder. Malesare affected more often than females.
b. Symptoms of pyloric stenosis usually begin atage 2 to 3 weeks, but may occur at birth orpresent as late as 5 months. An olive-sizemass may be palpable in the right upper quad-rant.
2. Gastroesophageal refluxa. Gastroesophageal reflux (GER) is defined as
retrograde movement of gastric contents intothe esophagus. GER occurs in 65% of infantsand is caused by inappropriate relaxation ofthe lower esophageal sphincter.
b. GER is considered “pathologic” if symptomspersist beyond 18 to 24 months and/or ifsignificant complications develop, such asfailure to thrive, recurrent episodes ofbronchospasm and pneumonia, apnea, orreflux esophagitis.
3. Gastrointestinal allergy. Cow milk allergy is rarein infancy and early childhood and generallyresolves by 2 to 3 years of age. Vomiting, diar-rhea, colic and gastrointestinal loss of blood mayoccur.
III. Clinical evaluation of vomiting in childhoodA. Peptic ulcer in early childhood is often associated
with vomiting. Peptic ulcer disease should be sus-pected if there is a family history of ulcer disease, orif there is hematemesis or unexplained iron defi-ciency anemia. Abdominal pain typically wakes thepatient from sleep.
B. Pancreatitis1. Pancreatitis is a relatively rare cause of vomiting,
but should be considered in the child who hassustained abdominal trauma. Patients usuallycomplain of epigastric pain, which may radiate tothe mid-back.
2. Other factors predisposing to pancreatitis includeviral illnesses (mumps), drugs (steroids,azathioprine), congenital anomalies of the biliaryor pancreat ic ducts , cho le l i th ias is,hypertriglyceridemia, and a family history ofpancreatitis.
C. Central nervous system disorders. Persistentvomiting without other gastrointestinal or systemiccomplaints suggests an intracranial tumor or in-creased intracranial pressure. Subtle neurologicfindings (eg, ataxia, head tilt) should be assessedand a detailed neurologic examination should beperformed.
IV. Physical examination of the child with persistentvomiting
A. Volume depletion often results from vomiting,manifesting as sunken fontanelles, decreased skinturgor, dry mouth, absence of tears, and decreasedurine output.
B. Peritoneal irritation should be suspected when thechild keeps his knees drawn up or bends over.Abdominal distension, visible peristalsis, and in-creased bowel sounds suggests intestinal obstruc-tion.
C. Abnormal masses, enlarged organs, guarding ortenderness should be sought. A hypertrophicpylorus may manifest as a palpable “olive” in theright upper quadrant.
D. Intussusception is often associated with a tender,sausage-shaped mass in the right upper quadrantand an empty right lower quadrant (Dance sign).
E. Digital rectal exam. Decreased anal sphincter toneand large amounts of hard fecal material in theampulla suggests fecal impaction. Constipation,increased rectal sphincter tone, and an empty rectalampulla suggests Hirschsprung disease.
V. Laboratory evaluationA. Serum electrolytes should be obtained when
dehydration is suspected. B. Urinalysis may detect a urinary tract infection or
suggest the presence of a metabolic disorder. C. Plasma amino acids and urine organic acids
should be measured if metabolic disease is sus-pected because of recurrent, unexplained episodesof metabolic acidosis.
D. Serum ammonia should be obtained in cases ofcyclic vomiting to exclude a urea cycle defect.
E. Liver chemistries and serum ammonia andglucose levels should be obtained if liver disease issuspected.
F. Serum amylase is frequently elevated in patientswho have acute pancreatitis. Serum lipase levelsmay be more helpful because it remains elevated fora number of days following an acute episode.
VI. Imaging studiesA. Ultrasonography of the abdomen is the initial
imaging test for suspected pyloric stenosis; however,two-thirds of vomiting infants will have a negativesonogram and will subsequently require an uppergastrointestinal series.
B. Plain radiographs of the abdomen 1. Supine and upright or left lateral decubitus
radiographic views are necessary for detectingcongenital anatomic malformations or obstructivelesions.
2. Air-fluid levels suggest obstruction, although thisfinding is nonspecific and may be seen withgastroenteritis.
3. Free air in the abdominal cavity indicates aperforated viscus. Upright plain films may demon-strate free air under the diaphragm.
C. Upper gastrointestinal series with nonionic,iso-osmolar, water-soluble contrast is indicatedwhen anatomic abnormalities and/or conditions thatcause gastric outlet obstruction are suspected.
D. Barium enema should be performed to detect lowerintestinal obstruction, and it may also be therapeuticin intussusception.
VII. TreatmentA. Initial therapy should correct hypovolemia and

electrolyte abnormalities. In acute diarrheal illnesseswith vomiting, oral rehydration therapy is usuallyadequate for treatment of dehydration.
B. Bilious vomiting and suspected intestinal ob-struction is managing by giving nothing by mouth,and by placing a nasogastric tube connected tointermittent suction. Bilious vomiting requires surgi-cal consultation.
C. Pharmacologic therapy1. Antiemetic agents usually are not required
because most instances of acute vomiting arecaused by self-limited, infectious gastrointestinalillnesses. Antiemetic drugs may be indicated forpostoperative emesis, motion sickness, cytotoxicdrug-evoked emesis, and gastroesophagealreflux disease.
2. Diphenhydramine and dimenhydrinate areuseful in treating the symptoms of motion sick-ness or vestibulitis.
3. Prochlorperazine and chlorpromazine haveanticholinergic and antihistaminic properties andare used to treat vomiting caused by drugs,radiation, and gastroenteritis.
References, see page 182.

Neurologic and RheumaticDisordersFebrile Seizures
Febrile seizures are the most common convulsive disorderof childhood. A febrile seizure is defined as a seizureassociated with fever in infancy or early childhood (usuallybetween 3 months and 5 years of age) without evidence ofintracranial infection or other cause.The problem almost always resolves without sequelae.Only a small minority will develop non-febrile seizureslater. There is no risk of brain damage.
I. Epidemiology. Febrile seizures occur in 2-4% of youngchildren. The most common age of onset is in the sec-ond year of life. Higher temperature and a history offebrile seizures in a close relative are risk factors for thedevelopment of a febrile seizure.A. Recurrence
1. After the first febrile seizure, 33% of children willexperience one or more febrile seizures, and 9%of children who have febrile seizures will have 3or more. The younger the child’s age when thefirst febrile seizure occurs, the greater the likeli-hood of recurrence.
2. Family history of febrile seizures is a risk factor forrecurrence. Short duration of fever before theinitial seizure and relatively lower fever at the timeof the initial seizure are risk factors.
B. Epilepsy. Fewer than 5% of children who havefebrile seizures develop epilepsy. Risk factors for thedevelopment of epilepsy following febrile seizuresinclude suspicious or abnormal development beforethe first seizure, family history of afebrile seizures,and complex first febrile seizure.
II. Pathophysiology. Most febrile illnesses associatedwith febrile seizures are caused by common infections(tonsillitis, upper respiratory infections, otitis media).Children of preschool age are subject to frequentinfections and high fevers.
III. Clinical evaluationA. Febrile seizures usually occur early in the course of
a febrile illness, often as the first sign. The seizuremay be of any type, but the most common is tonic-clonic. Initially there may be a cry, followed by lossof consciousness and muscular rigidity. During thistonic phase, apnea and incontinence may occur.The tonic phase is followed by the clonic phase ofrepetitive, rhythmic jerking movements, which isthen followed by postictal lethargy or sleep.
B. Other seizure types may be characterized by staringwith stiffness or limpness or only focal stiffness orjerking. Most seizures last less than 6 minutes; 8%last longer than 15 minutes.
C. An underlying illness that may require treatmentshould be sought. Symptoms of infection, med-ication exposure, or trauma should be assessed.Family history of febrile or afebrile seizures shouldbe evaluated. A complete description of the seizureshould be obtained from a witness.
D. Physical examination1. The level of consciousness, presence of
meningismus, a tense or bulging fontanelle,Kernig or Brudzinski sign, and any focal abnor-malities in muscle strength or tone should besought.
2. Encephalitis or meningitis must be excluded.E. Laboratory studies should evaluate the source of
fever. A lumbar puncture (LP) is indicated if there isany suspicion of meningitis. CT or MRI are seldomhelpful and are not performed routinely. The electro-encephalogram (EEG) is not helpful in the evalua-tion of febrile seizures because it is not predictive ofrecurrence risk of later epilepsy.
IV. Management of febrile seizuresA. The child should be kept in the emergency depart-
ment or physician’s office for at least several hoursand re-evaluated. Most children will have improvedand be alert, and the child may be sent home if thecause of the fever has been diagnosed and treated.Hospital admission is necessary if the child isunstable or if meningitis remains a possibility.
B. Parental counseling

1. Parents are advised that febrile seizures do notcause brain damage, and the likelihood of devel-oping epilepsy or recurrent non-febrile seizures isvery small. There is a risk of further febrile sei-zures during the current or subsequent febrileillnesses.
2. If another seizure occurs, the parent should placethe child on his side or abdomen with the facedownward. Nothing should be forced between theteeth. If the seizure does not stop after 10 min-utes, the child should be brought to the hospital.
C. Control of fever with antipyretics (acetaminophen)and sponging is recommended, but this practice hasnot been proven to lower the risk of recurrent febrileseizures.
D. Childhood immunizations. Febrile seizures occurmost commonly following a DPT immunizationbecause pertussis provokes fever. The advantagesof vaccines must be weighed against the risk ofpertussis if immunization is postponed.
V. Long-term managementA. Prophylaxis with diazepam or phenobarbital is not
routinely necessary, but is reserved for very youngchildren who have sustained multiple seizuresassociated with focal postictal paralysis.
B. Diazepam may be administered orally and rectallyduring febrile illnesses to prevent recurrences ofseizures. Oral diazepam is given in three divideddoses to a total of 1 mg/kg per day when the child isill or feverish.
References, see page 182.
Seizures
The majority of children with epilepsy have an idiopathicdisorder; the neurological examination and neuroimagingstudies are normal.
I. Clinical evaluation of seizuresA. The first seizure. A child’s first seizure may be
caused by an acute illness, such as a metabolic orinfectious disorder, may be idiopathic and non-recurrent, or may represent the beginning of epi-lepsy.
B. Prognosis after a first seizure. The child who isneurologically normal, has no history of a priorneurological illness, and has an unprovoked seizurewith no evident cause (idiopathic seizure) has a 24percent risk of having another seizure in the nextyear. The recurrence risk increases to 37 percent inchildren in whom the seizure is related to a priorneurological insult (remote symptomatic), such ascerebral palsy, and increases to 70 percent in thenext year in patients who have had two seizures(excluding sequential seizures in 24 hours).
C. Setting in which episodes occur. Most seizuresare random events; however, many nonepilepticsyndromes have characteristic precipitating circum-stances or occur in specific locations. Thus, deter-mining the time of day and the activity in which thechild was engaged prior to the seizure is important.Did the seizures occur only with illness and fever?
D. Behavior immediately prior to the event. On rareoccasions, seizures may be precipitated by environ-mental stimuli, such as sound or an unexpectedtouch. More commonly, no obvious precipitatingcircumstances are present. Thus, obtaining a historyof the events leading up to the seizure is importantbecause they may be more suggestive of a non-seizure diagnosis.
E. What activity was the patient engaged in immedi-ately prior to the seizure? Does the patient mentionany sensory or autonomic symptoms (numbness,visual distortions, auditory or visual hallucinations orillusions, nausea or unusual feelings in the abdomenor chest, an unusual smell or taste, etc) or manifestan alteration in behavior or mood?
F. Are the seizures precipitated by a particular stimu-lus? Seizures rarely are precipitated by mild trauma.
G. Was focal motor activity, such as facial or extremitytwitching, present? These symptoms are consideredan "aura," which is actually the first clinical manifes-tation of the seizure; this information is valuable forlocalizing.
H. Physical description. The physician should obtain
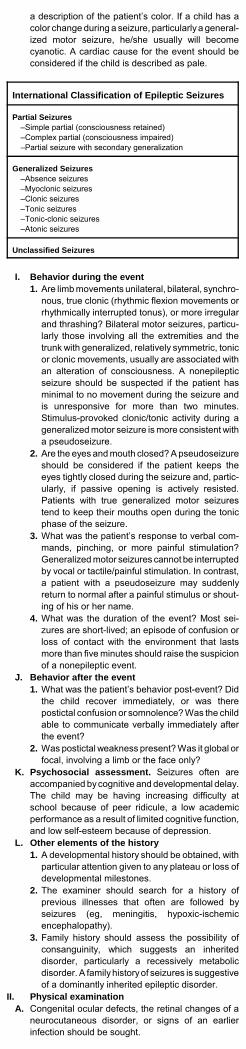
a description of the patient’s color. If a child has acolor change during a seizure, particularly a general-ized motor seizure, he/she usually will becomecyanotic. A cardiac cause for the event should beconsidered if the child is described as pale.
International Classification of Epileptic Seizures
Partial Seizures–Simple partial (consciousness retained)–Complex partial (consciousness impaired)–Partial seizure with secondary generalization
Generalized Seizures–Absence seizures–Myoclonic seizures –Clonic seizures –Tonic seizures–Tonic-clonic seizures–Atonic seizures
Unclassified Seizures
I. Behavior during the event1. Are limb movements unilateral, bilateral, synchro-
nous, true clonic (rhythmic flexion movements orrhythmically interrupted tonus), or more irregularand thrashing? Bilateral motor seizures, particu-larly those involving all the extremities and thetrunk with generalized, relatively symmetric, tonicor clonic movements, usually are associated withan alteration of consciousness. A nonepilepticseizure should be suspected if the patient hasminimal to no movement during the seizure andis unresponsive for more than two minutes.Stimulus-provoked clonic/tonic activity during ageneralized motor seizure is more consistent witha pseudoseizure.
2. Are the eyes and mouth closed? A pseudoseizureshould be considered if the patient keeps theeyes tightly closed during the seizure and, partic-ularly, if passive opening is actively resisted.Patients with true generalized motor seizurestend to keep their mouths open during the tonicphase of the seizure.
3. What was the patient’s response to verbal com-mands, pinching, or more painful stimulation?Generalized motor seizures cannot be interruptedby vocal or tactile/painful stimulation. In contrast,a patient with a pseudoseizure may suddenlyreturn to normal after a painful stimulus or shout-ing of his or her name.
4. What was the duration of the event? Most sei-zures are short-lived; an episode of confusion orloss of contact with the environment that lastsmore than five minutes should raise the suspicionof a nonepileptic event.
J. Behavior after the event1. What was the patient’s behavior post-event? Did
the child recover immediately, or was therepostictal confusion or somnolence? Was the childable to communicate verbally immediately afterthe event?
2. Was postictal weakness present? Was it global orfocal, involving a limb or the face only?
K. Psychosocial assessment. Seizures often areaccompanied by cognitive and developmental delay.The child may be having increasing difficulty atschool because of peer ridicule, a low academicperformance as a result of limited cognitive function,and low self-esteem because of depression.
L. Other elements of the history1. A developmental history should be obtained, with
particular attention given to any plateau or loss ofdevelopmental milestones.
2. The examiner should search for a history ofprevious illnesses that often are followed byseizures (eg, meningitis, hypoxic-ischemicencephalopathy).
3. Family history should assess the possibility ofconsanguinity, which suggests an inheriteddisorder, particularly a recessively metabolicdisorder. A family history of seizures is suggestiveof a dominantly inherited epileptic disorder.
II. Physical examinationA. Congenital ocular defects, the retinal changes of a
neurocutaneous disorder, or signs of an earlierinfection should be sought.
B. The abdominal examination may revealorganomegaly, suggesting a storage disease.
C. Cardiac examination, including an ECG, is neces-sary if concern exists about a cardiogenic cause.Episodes of disturbed neurological function causedby decreased cardiac output (eg, prolonged QTsyndrome or pulmonary hypertension) may closelymimic complex partial seizures.
D. Dysmorphic features should be sought and othercongenital anomalies, body asymmetries, andunusual skull shapes noted.
E. The cutaneous features of tuberous sclerosis, thefacial angioma of Sturge-Weber syndrome, the café-au-lait spots of neurofibromatosis, the nevi of thelinear nevus syndrome, and the swirlinghypopigmentation of Ito syndrome all are character-istic physical findings.
III. Electroencephalogram (EEG). Virtually every childwith recurrent seizures should have an EEG awakeand while sleeping. Obtaining an awake and a sleepEEG and optimizing the timing of the EEGs shouldmaximize the chances of finding epileptiform activity.
A. Sleep. An awake and asleep EEG should be ob-tained. Epileptiform activity may appear in only onestate (usually sleep). In the benign partial epilepsies,focal or multifocal spike and slow wave dischargestypically appear during drowsiness and light sleep.Benign focal epilepsy syndromes may manifestgeneralized EEG discharges as well as aphotoparoxysmal response (epileptiform activityprovoked by repetitive light flashes), which moretypically are seen in the idiopathic generalizedepilepsies. The most striking and diagnostic pattern,however, is the sleep-activated focal spikes.
IV. Laboratory testing and neuroimagingA. Neuroimaging. Most children with recurrent sei-
zures should have an MRI scan, usually without theuse of contrast.
B. Laboratory screening in undiagnosed epilepsy.Routine assessment consists of a serum (and oftenCSF) amino acid analysis, urine for quantitativeorganic acids, serum calcium, glucose, carnitine,ammonia, lactate and pyruvate, routine chromo-somal karyotype (virtually all chromosomal syn-dromes can manifest seizures), and DNA analysisfor fragile X syndrome, particularly in boys andoccasionally in girls with maternal family histories ofmental retardation. More sophisticated geneticanalyses, such as FISH studies, may be needed todiagnose those syndromes missed on routinekaryotype analysis.
V. Treatment of Seizures and Epileptic Syndromesin Children
A. Predictors of recurrence. In children with an idio-pathic seizure, the EEG is the most valuable predic-tor of recurrence. An idiopathic first seizure, therecurrence risk was 41 percent in the first 12 monthsafter the initial seizure if the EEG was abnormalcompared with 15 percent in children with a normalEEG.
B. Treating a child with an idiopathic first seizure isusually not recommended. In children with seizuresthat result from a past injury or insult, the risk ofseizure recurrence is higher.
C. Many parents elect to avoid therapy if the seizuresare infrequent and/or mild. Many patients withbenign partial epilepsy are not treated if seizures arerelatively infrequent. Children with absence seizures,drop attacks, and infantile spasms are virtuallyalways treated.

Epileptic Syndromes and RecommendedAntiepileptic
Syndrome Antiepileptic drug
Localization-related(partial, focal)
1 - CBZ. PB, VPA, TPM,PHT, LTG, OXC2 - GBP, PRM, CRZ,LEV
Generalized epilepsiesAbsence seizures
1 - ESM, VPA, LTG2 - CNZ
Generalized tonic-clonic 1 - CBZ, VPA, PHT, PBTPM2 - LTG
Juvenile myoclonic epi-lepsy
1 - VPA, LMG2 - PRM, CNZ, TPM
Myoclonic absence 1 - VPA, ESM2 - LTG, CNZ, TPM
Infantile spasms 1 - ACTH, prednisone2 - VPA (?), CNZ (?),TPM (?)
Lennox-Gastaut syn-drome 2 - ESM (drop attacks),
FBM
1: First-line drugs2: Second-line drugs
CBZ: carbamazepine; CRZ: clorazepate; CNZ:clonazepam; ESM: ethosuximide; FBM: felbamate;GBP: gabapentin; LEV: levetiracetam; LTG:lamotrigine; OXC: oxcarebazepine; PHT: pheytoin;PB: phenobarbital; PRM: primidone; TPM: topiramate;TGB: tiagabine; VPA: valproic acid (divalproex so-dium)
D. Antiepileptic drug therapy1. Drug dose
a. Most AEDs should be started at about 10 to 25percent of the planned maintenance dose.AEDs with a long half-life can be started atclose to the maintenance dose. If seizures arefrequent, the dose should be increased atintervals not exceeding five half-lives to allowthe serum level to plateau between eachdosage increment.
b. The AED dose should be increased untilseizures stop (regardless of the serum level),unremitting side effects occur, or levels reacha high or supratherapeutic range without asignificant impact upon seizure frequency.
2. Serum levels should be used only as guides totherapy. The therapeutic range is different foreach patient; many achieve seizure control atlevels below the recommended range, whereasothers require levels above the range.
3. Laboratory monitoring is done in all childrenreceiving AEDs, usually at every return visit.
Common Anticonvulsant Drugs
Drug SeizureType
Oral Dose Se-rumLevelmcg/mL
Side Ef-fects andToxicities
Carbamazepine(Tegretol), carba-mazepineXR(TegretolXR)
PartialepilepsyTonic-clonic
Begin 10mg/kg/d.Increase by5 mg/kg/devery wk to20-30mg/kg/d in 2or 3 divideddoses
102 Dizziness,drowsiness,diplopia,liver, dys-function,anemia,leucopoe-nia

Drug SeizureType
Oral Dose Se-rumLevelmcg/mL
Side Ef-fects andToxicities
Clonazepam(Klonopin)
MyoclonicAbsence
Begin 0.05mg/kg/d.Increase by0.05 mg/kgper wk.Maximum,0.2 mg/kg/din 2 or 3 di-vided doses
6.3-56.8
Drowsi-ness, irrita-bility, drool-ing, behav-ioral abnor-malities,depression
Ethosuximide(Zarontin)
AbsenceMyoclonic
Begin 10 to20 mg/kg/din 2 divideddoses; maybe in-creased to50 mg/kg/d
40-160
Drowsi-ness, nau-sea, rarelyblooddyscrasias
Felbamate(Felbatol)
Partialepilepsy Tonic-clonic
600 to 1,200mg/ 2,400 to3,600 mgtwo to threetimes daily
Headache,insomnia,aplasticanemia,hepatitis
Gabapentin(Neurontin)
Partialepilepsy Tonic-clonic
Begin 300mg/d. In-crease by300 mg/devery 3 to 5days. Maxi-mum 900 to1200 mg/din 3 equallydivideddoses
<2 Somno-lence, dizzi-ness.ataxia,headache,tremor,vomiting,nystagmus,fatigue,weight gain
Lamotrigine(Lamictal)
PartialepilepsyTonic-clonicLennox-Gastaut
Begin 2mg/kg/d in 2equal doses.Increase tomainte-nance doseof 5 to 15mg/kg/d.
35433
Severerashes,drowsiness,headache,blurred vi-sion
Topiramate(Topamax)
PartialepilepsyTonic-clonic
Begin 25 to50 mgIncrease to200 to 400mg/day in 2doses
Nephrolithiasis,paresthesias, weightloss
Tiagabine(Gabitril)
Partialepilepsy
Begin 4 mgIncrease to32 to 64 mgin 2-4 doses
Narrowspectrum ofactivity
Oxcarbazepine(Trileptal)
Partialepilepsy
Begin 300 to600 mgIncrease to600 to 2,400mg in 2doses
Hyponatremia
Levetiracetam(Keppra)
Focalepilepsy
Begin 1,000mgIncrease to1,000 to3,000 mg in2 doses
Zonisamide(Zonegran)
Focalepilepsy
Begin 100 to200 mgIncrease to400 to 600mg everyday in 2doses
Nephrolithiasis, weightloss
Pheno-barbital
Tonic-clonic Partialepilepsy
3 to 5mg/kg/d in 1or 2 divideddoses
15-40 Hyperactiv-ity, irritabil-ity, shortattentionspan, tem-per tan-trums, al-tered sleeppattern,Stevens-Johnsonsyndrome,depressionof cognitivefunction

Drug SeizureType
Oral Dose Se-rumLevelmcg/mL
Side Ef-fects andToxicities
Phenytoin(Dilantin)
PartialepilepsyTonic-clonic
5 m 6mg/kg/d in 2divideddoses
293 Hirsutism,gum hyper-trophy, ata-xia, skinrash,StevensJohnsonsyndrome
Primidone(Mysoline)
Tonic-clonicPartialepilepsyMyoclonic
Begin 50mg/d in twodivideddoses.Graduallyincrease to150 to 500mg/d dividedinto 3 equaldoses.
132 Aggressivebehaviorand per-sonalitychangessimilar tothose forphenobar-bital
Sodiumvalproate(Depakote)
Tonic-clonic Absence Myoclonic Partialepilepsy Unclas-sified
Begin 10mg/kg/d.Increase by5 to 10mg/kg perwk. Usualdose, 20 to60 mg/kg/din 2 or 3 di-vided doses.
50-100
Weightgain, alope-cia, tremor,hepato-toxicity
Vigabatrin (Sabril)
Partialepilepsy
Begin 30 to40 mg/kg/d.Increase by10 mg/kgper wk.Maximum,80 to 100mg/kg/d in 2equal doses
1.4-14
Agitation,drowsiness,weight gain,dizziness,headache,ataxia
4. Valproic acid (divalproex) is associated with ahigh incidence of minor elevations of liver en-zymes and serum ammonia.a. The serum gamma glutamyl transpeptidase
(GGT) elevated in 75 percent and alanineaminotransferase (ALT) in 25 percent.
b. Hepatic enzyme elevations greater thanthree times normal should be repeated inseveral weeks and the medications stopped iflevels are increasing rapidly or the child issymptomatic.
5. Carbamazepine. Leukopenia is not uncommonwith carbamazepine, often appearing in the firsttwo to three months of therapy. Severe aplasticanemia or agranulocytosis is rare, occurring intwo per 575,000. Obtain a CBC after the firstmonth of carbamazepine therapy; if the whiteblood count (WBC) or absolute neutrophil count(ANC) is significantly decreased, a repeat studyis done in three to four weeks and may be re-peated again until the counts stabilize. If the ANCfalls below 800 to 1000, the medication should bestopped.
E. Topiramate causes a mild to moderate chronicmetabolic acidosis in two-thirds of children and cancause nephrolithiasis. Complications of chronicmetabolic acidosis include impaired growth andrickets or osteomalacia.1. The serum bicarbonate should be measured at
baseline and monitored periodically thereafter.Dose reduction or drug discontinuation should beconsidered in patients with persistent or severemetabolic acidosis.
F. Ketogenic diet consists of three to four parts fat toone part protein and carbohydrate. The high-fatcontent and relative absence of carbohydrate pro-duces a persistent ketosis, which appears to havean anticonvulsant effect. The level of ketosis can bemonitored daily in the urine and, intermittently, in theserum. The diet suppresses seizure frequency by atleast 50 percent in 40 percent of patients.
G. Epilepsy surgery. Most children achieve reasonablygood seizure control with anticonvulsant medication.Some are refractory despite numerous medicationsand are not candidates for or fail the ketogenic diet.
Surgical interventions should be considered inchildren who have persistent, frequent seizures.Surgical approaches can be divided into relativelynoninvasive (vagal nerve stimulator) and invasive(local resection, lobar or multilobar resection, corpuscallosotomy, hemispherectomy, and multiple subpialtransection) procedures.
H. Vagal nerve stimulation. Many children who failAED therapy and the ketogenic diet are not candi-dates for standard epilepsy surgery. Others mayundergo resective surgery and still have excessivenumbers of seizures. These patients may be candi-dates for vagal nerve stimulation. Approximately 30percent of adults treated in a randomized (high-current stimulation) have a 50 percent or betterseizure reduction.
References, see page 182.
Headache
Chronic or recurrent headaches occur 75% of children by15 years. Migraine is the most common headache syn-drome in children. It is characterized by periodic episodesof paroxysmal headache accompanied by nausea, vomit-ing, abdominal pain, and relief with sleep.
I. Clinical evaluationA. Headaches are characterized as isolated acute,
recurrent acute, chronic nonprogressive, or chronicprogressive. A social and educational history mayidentify significant stresses. Analgesic use should bedetermined.
B. Physical examination should include measurementof growth parameters, head circumference, andblood pressure. The teeth should be examined andsinusitis should be sought. An arteriovenous malfor-mation may cause an asymmetric, machinery-likecranial bruit.
C. Papilledema. The presence of retinal venouspulsation on funduscopy provides evidence ofnormal intracranial pressure. Visual acuity should bemeasured, and a detailed neurologic examination isessential.
D. Investigations. If increased intracranial pressure oran intracranial lesion is suspected, a computedtomographic (CT) head scan should be performed.Magnetic resonance imaging (MRI) may be requiredto diagnose subtle vascular abnormalities orhypothalamo-pituitary lesions.
E. Lumbar puncture may be helpful if pseudotumorcerebri is suspected. However, lumbar puncture mayresult in herniation of the brain in patients who haveobstructive hydrocephalus, an intracranial masslesion, or cerebral edema. Neuroimaging should beperformed prior to the lumbar puncture.
Physical and Neurological Examination of theChild with Headaches
Feature Significance
Growth parameters Chronic illness may affect lineargrowth Hypothalamopituitary dysfunctionmay disturb growth
Head circumference Increased intracranial pressureprior to fusion of the sutures mayaccelerate head growth
Skin Evidence of trauma or aneurocutaneous disorder
Blood pressure Hypertension
Neurologic examination Signs of increased intracranialpressure Neurologic abnormality
Cranial bruits May reflect an intracranialarteriovenous malformation

F. Migraine1. Migraines may be associated with a preceding
aura, which usually involves visual phenomena.The headache is usually unilateral or bilateral,recurrent, throbbing, and associated with nauseaor vomiting. Photophobia or phonophobia iscommon.
2. A family history of migraine is obtained in up to80% of children who have migraine. A familyhistory of motion sickness is common. Migraineepisodes may be triggered by stress, lack ofsleep, excitement, menstruation, or certain foods.
II. Management of migraine headache in childrenA. Abortive treatment
1. NSAIDs and acetaminophen. Early administra-tion of acetaminophen or ibuprofen is helpful.Ibuprofen may provide faster relief thanacetaminophen.a. Acetaminophen is administered in an initial
dose of 10 to 20 mg/kg (one or two 325 mgtablets), with a maximum dose of 1000 mg. Asecond dose of 10 to 20 mg/kg may be givenin two to four hours if symptoms persist.Additional doses may be given at four- to six-hour intervals, but should not exceed threedoses in 24 hours.
b. Ibuprofen is given in a dose of 5 to 10 mg/kgat 4 to 8-hour intervals (maximum 50 mg/kg in24 hours). This dose may be repeated in twoto four hours; no more than three dosesshould be given in 24 hours. Ibuprofen shouldnot be given to patients with abdominal pain,dizziness, or tinnitus.
c. Naproxen (250 mg tablet) can be given tochildren older than 12 years of age. The dosecan be repeated up to three times per day at8- to 12-hour intervals. Naproxen should notbe given to patients with epigastric pain ornausea.
d. Ketorolac can be administered intravenouslyor orally. Intravenous ketorolac successfullytreats migraine in 55 percent. Doses are 0.5mg/kg IV, followed by 1 mg/kg every six hoursor 0.25 mg/kg PO every six hours, up to amaximum of 1 mg/kg per day.
2. Other analgesics. A combination analgesic canbe tried if single analgesics fail to relieve pain inchildren older than eight years of age. Midrinconsists of isometheptene mucate (asympathomimetic agent), dichloralphenazonel (amild sedative), and acetaminophen. The dose foradolescents is two capsules at the onset of theheadache, a third dose one hour later, and afourth capsule 90 minutes later, if needed.
3. Antiemetics. If nausea and vomiting are promi-nent, early use of an antiemetic may relievesymptoms and facilitate sleep. Rectal administra-tion may be preferable.a. Phenothiazines may have additional
antimigraine properties, and have a low inci-dence of acute extrapyramidal reactions. Thedose is 0.25 to 0.5 mg/kg per dose orally,intramuscularly, or rectally; it should not begiven intravenously.
b. Dimenhydrinate also is an effectiveantiemetic. The dose is 1.25 mg/kg orally orintramuscularly every four to six hours.
c. Metoclopramide administered intravenouslyappears to reduce nausea and vomitingassociated with migraine. Its use is reservedfor the emergency department prior to theadministration of dihydroergotamine (DHE).Acute dystonic reactions may occur.
4. Triptans are serotonin agonists with an affinityfor the 5-HT 1b/1d receptor. a. Triptans are widely used in children, although
their use is not approved. Parenteral, oral,and nasal preparations are available.
b. The triptans are highly effective. Sumatriptangiven by the subcutaneous or intranasal routereduces headache severity in 70 percent; oraladministration is effective in 50 percent.Triptans are contraindicated in basilar arteryand hemiplegic migraine because ofvasospasm.
c. Nasal sumatriptan spray is effective andshould be considered for the acute treatmentof migraine in adolescents 12 to 17 years old.Nasal sumatriptan is given to younger chil-dren in an initial dose of 5 mg. If this dose isineffective, 10 mg can be tried. In adoles-cents, a dose of up to 20 mg can be given.
d. Subcutaneous sumatriptan is an effectivetherapy for migraine. After a 6 mg dose,headache is relieved within one or two hours

in 46%.e. Oral sumatriptan is effective and useful in
children. The initial dose in adolescents is 25mg. This may be repeated in 20 minutes if thesymptoms persist. If no improvement occurs,doses up to 50 mg can be used.
B. Prophylactic treatment is used when headachesoccur more than four times per month.1. Cyproheptadine (Periactin) is a histamine and
serotonin antagonist, which is used for migraineprophylaxis. Appetite stimulation with weight gainlimits use. Somnolence occurs. Cyproheptadine(4 to 12 mg at bedtime) is used for prophylaxis inthe younger child.
2. Propranolol is the prophylactic treatment mostcommonly used in children. Chronic therapy withpropranolol reduces the frequency of migraine in60 to 80 percent.a. Propranolol is initiated in a dose of 1 mg/kg in
three divided doses, with a maximum dose of4 mg/kg per day. Heart rate and orthostaticblood pressure should be monitored everythree months. The heart rate should be >60bpm after one minute of exercise.
b. Beta-blockers are contraindicated in childrenwith asthma. They should be used with cau-tion in depression, diabetes, or orthostatichypotension.
3. Valproate decreases headache frequency by 50percent. Side effects include appetite stimulationwith weight gain, gastrointestinal upset, somno-lence, dizziness, and tremor. Additional reportedadverse events include transient hair loss andpolycystic ovary syndrome. Valproate should beused cautiously in children younger than age fiveyears of age because of potential hepatotoxicity.a. Valproate has teratogenic effects. In adoles-
cent females at risk for pregnancy, folic acidalso should be given. Valproate is started in adose of 10 to 15 mg/kg in two divided doses.The dose can be increased in increments of15 mg/kg to a maximum dose of 60 mg/kg perday.
b. Liver function tests and complete blood countshould be monitored every two to threemonths. Thrombocytopenia may occur athigher doses.
c. Serum anticonvulsant concentration shouldbe monitored every three to six months. Areasonable therapeutic range is 50 to 100mg/dL.
4. Amitriptyline is used commonly for migraineprophylaxis in children. A single daily 5 mg oraldose of amitriptyline, given at night, often iseffective. If frequent headaches persist, the doseis advanced slowly by 5 mg increments, with atleast two weeks between changes. The doserarely should exceed 60 mg. Nonspecificelectrocardiographic changes and changes inatrioventricular conduction may occur. Thus, anelectrocardiogram should be obtained.
5. Flunarizine is a calcium channel blocker, whichis unavailable in the United States. Treatmentwith flunarizine 5 mg/day is associated with asignificant reduction in headache frequency.
C. Recommendations1. Abortive treatment begins with either
acetaminophen or ibuprofen. Ibuprofen is givenin an initial dose of 10 mg/kg (maximum dose 50mg/kg). This dose may be repeated in two to fourhours if needed; no more than three dosesshould be given in 24 hours.a. Children with nausea and vomiting should
receive promethazine (Phenergan) 0.25 to 0.5mg/kg rectally and repeat as needed at inter-vals of four to six hours.
b. In children at least five years of age, if analge-sics do not provide relief a trial of sumatriptannasal spray should be initiated. Begin with 5mg; it may be repeated once in four to sixhours if the headache returns. If there is nobenefit, two 5 mg units of nasal spray may begiven together. Similar doses of nasal sprayare used in older children, with a maximum of20 mg.
c. In children older than 10 years without vomit-ing, oral sumatriptan is an option. The initialdose is 25 mg, with a maximum of 50 mg.Other triptans may be tried in patients olderthan 10 years of age who do not respond tosumatriptan: rizatriptan ([Maxalt] 5 mg wafer)or zolmitriptan ([Zomig] 2.5 or 5 mg).
2. Prophylactic treatment is used when head-aches are frequent (more than four times permonth) or if severe and prolonged headache

results in frequent school absences or preventsimportant daily activities.a. In children younger than six years of age,
cyproheptadine (Periactin) is used in a doseof 4 to 12 mg per day, given orally once atbedtime.
b. In older children, propranolol is the first choicein a starting dose of 1 mg/kg in three divideddoses, with a maximum dose of 4 mg/kg perday.
c. If propranolol is not well tolerated, valproate(Depakote) should be used for prophylaxis.Valproate is given primarily to boys older thanfive years of age. This drug should bedavoided in adolescent females because ofweight gain and polycystic ovary syndrome.Valproate is started in a dose of 10 to 15mg/kg in two to three divided doses orally.The dose can be increased in increments of15 mg/kg to a maximum dose of 60 mg/kg perday.
Treatment of Acute Migraine Episodes
Simple analgesics
Acetaminophen Initial dose of 20 mg/kg PO, followedby 10 to 15 mg/kg q 4 h up to a maxi-mum dose of 65 mg/kg per day (maxi-mum, 3,000 mg/day)
Ibuprofen (Advil) 1 to 12 years: 10 mg/kg PO q 4 to 6 h More than 12 years: 200 to 400 mgPO q 4 h; maximum dose 1,200mg/day
Naproxen (Aleve) 5 mg/kg PO q 12 h; maximum dose750 mg/day
Antiemetics
Promethazine(Phenergan)
Initial dose of 1 mg/kg PO (maximum,25 mg); can be repeated at doses of0.25 to 1 mg/kg q 4 to 6 h
Chlorpromazine(Compazine)
1 mg/kg IM for severe attacks
Other Drugs
Sumatriptan(Imitrex)
6 mg SC; may repeat in 1-2 hours;max 12 mg/day Oral: 25-50 mg PO once; may repeatin 2 hoursIntranasal: 5, 10, or 20 mg in one nos-tril; may repeat after 2 hours
Dihydroergotamine(DHE)
0.5 to 1 mg IV over 3 min in children>10 y. Can be repeated q8h. Usedwith metoclopramide.
Prophylactic Agents for Migraine
Amitriptyline(Elavil)
5-10 mg qhs
Propranolol(Inderal)
1 to 4 mg/kg per day; start at low dose andincrease slowly
Valproate(Depakote)
10 to 15 mg/kg in two divided doses; in-creased by 15 mg/kg to a max 60 mg/kgper day
References, see page 182.
Kawasaki DiseaseKawasaki disease (KD) is one of the most commonvasculitides of childhood. The annual incidence is highestamong Asians and Pacific Islanders (32.5/100,000children <5 years of age), intermediate among AfricanAmericans (16.9/100,000 children <5 years) and Hispan-ics (11.1/100,000 children <5 years), and lowest amongCaucasians (9.1/100,000 children <5 years of age). KDshould be considered in any infant with prolonged, unex-plained fever. It is typically a self-limited disorder; however,complications such as coronary artery aneurysm, de-pressed myocardial contractility and heart failure, myocar-dial infarction, arrhythmias, and peripheral arterial occlu-sion may develop.
I. DiagnosisA. Diagnosis requires the presence of fever lasting
five days or more without any other explanation,combined with at least four of the five followingphysical findings:1. Bilateral conjunctival injection.

2. Oral mucous membrane changes, includinginjected or fissured lips, injected pharynx, orstrawberry tongue.
3. Peripheral extremity changes, including ery-thema of palms or soles or edema of hands orfeet (acute phase), and periungual desquama-tion (convalescent phase).
4. Polymorphous rash.5. Cervical lymphadenopathy (at least one lymph
node >1.5 cm in diameter).B. Children who do not meet the criteria may have an
incomplete or atypical form of KD. In addition, somepatients who manifest five or six signs may haveother conditions.
Kawasaki Syndrome: Diagnostic Criteria
I. Fever for >5 days (usually >102EF)II. At least four of five features
A. Bilateral conjunctival injectionB. Cervical adenitis (unilateral >1.5 cm diameter,
non-fluctuant)C. Rash (truncal, perineal accentuation, polymor-
phous but non-vesicular)
D. Inflamed oral mucosae (fissured lips, straw-berry tongue)
E. Hand and feet inflammation (periungual peel-ing around 14-21 days)
III. No alternate diagnosisIV. Fever plus 3/5 criteria are diagnostic when coro-
nary abnormalities are present
II. Laboratory studiesA. Systemic inflammation is manifest by elevation of
acute phase reactants (eg, C-reactive protein[CRP], erythrocyte sedimentation rate, and alpha-1antitrypsin), leukocytosis, and a left-shift in thewhite blood cell count. By the second week ofillness, platelet counts generally rise and mayreach 1,000,000/mm3 (reactive thrombocytosis).
B. KD often presents with a normocytic,normochromic anemia.
C. The urinalysis commonly reveals white blood cellson microscopic examination. Renal involvementmay occur in KD but is uncommon.
D. Elevated transaminase levels or mildhyperbilirubinemia often occur. In addition, aminority of children develop obstructive jaundicefrom hydrops of the gallbladder.
III. Atypical Kawasaki disease. Children suspected ofhaving KD who do not fulfill diagnostic criteria (ie, havefewer than four signs of mucocutaneous inflammation)may have incomplete or atypical KD. Outcomesappear to be comparable to children with completedisease.A. The cardinal manifestation most likely to be absent
in all cases of atypical KD is cervicallymphadenopathy. Adenopathy is missing in up to90 percent of children with atypical disease.
B. Rash may not be manifest in 7 to 10 percent ofchildren with KD.
C. Mucous membrane changes are most characteris-tic of KD and are generally present in more than90 percent of children with any form of the disease.
D. Children with incomplete KD fail to demonstrateperipheral extremity changes in 40 percent ofcases. In comparison, at least 85 percent of thosewith typical KD develop palmar erythema, dorsaledema, or periungual desquamation.
IV. Differential diagnosis. KD is most commonly con-fused with other infectious exanthems of childhood.A. Measles, echovirus, and adenovirus cause
mucocutaneous inflammation but typically haveless evidence of systemic inflammation and lackthe extremity changes seen in KD.
B. Toxin-mediated illnesses, especially beta-hemolytic streptococcal infection and toxic shocksyndrome, lack the ocular and articular involve-ment typical of KD.
C. Drug reactions, such as Stevens-Johnson syn-drome or serum sickness, may mimic KD but withsubtle differences in the ocular and mucosalmanifestations.
V. Initial management. Patients who fulfill the criteria forKawasaki disease are hospitalized and treated withintravenous immune globulin (IVIG) and aspirin. Thosepatients suspected of having atypical disease mayrequire further testing such as slit lamp examinationand echocardiography to confirm the diagnosis.A. Intravenous immunoglobulin should be adminis-
tered at a dose of IVIG 2g/kg, as a single doseover 8 to 12 hours. IVIG should be administered as
soon as a diagnosis of KD is established.B. Aspirin is given as 30 mg/kg/day to >100
mg/kg/day in four divided doses during the acutephase of illness. Subsequently, aspirin is adminis-tered in low doses (3 to 5 mg/kg/day) for itsantiplatelet action. Alternative anti-inflammatoryagents, such as ibuprofen, may be used for pro-longed episodes of arthritis.1. The risks of aspirin include transaminitis, chem-
ical hepatitis, transient hearing loss, and rarelyReye syndrome.
2. Aspirin is continued until laboratory studies (eg,platelet count and sedimentation rate) return tonormal, unless coronary artery abnormalitiesare detected by echocardiography; this phaseof therapy typically is complete within twomonths of the onset of disease.
C. Follow-up. An echocardiogram should be ob-tained early in the acute phase of illness and six toeight weeks after onset to confirm the efficacy oftreatment. Repeated examinations should beperformed during the first two months to detectarrhythmias, heart failure, valvular insufficiency, ormyocarditis. Children with coronary artery abnor-malities receive long-term antithrombotic therapywith aspirin, and regular cardiac evaluation.
D. Vaccinations. The administration of live virusvaccines, including measles and varicella, shouldbe postponed in children who have been treatedwith IVIG. Passively acquired antibodies persist forup to 11 months following IVIG administration, andthey may interfere with vaccine immunogenicity.Patients older than six months of age who requirelong-term aspirin therapy should receive yearlyinfluenza immunization because of the possibleincreased risk of Reye syndrome. They shouldreceive the inactivated vaccine.
References, see page 182.
Juvenile Rheumatoid ArthritisPauciarticular onset juvenile idiopathic arthritis (JIA) isdefined as involvement of fewer than five joints. It is themost common subgroup of JIA, constituting about 50percent of cases of JIA.
I. Clinical presentationA. Pauciarticular JIA affects females more often than
males. The peak incidence of pauciarticular JIA is inthe second and third years. It is less common overfive years of age and rarely begins after age 10. Achild with large joint involvement beginning in theearly teenage years most commonly has aspondyloarthropathy.
B. The typical child with pauciarticular JIA is a girl whois noticed to be limping without complaint. Often thefamily notices that the child “walks funny” in themorning, but after a little while seems fine. The kneeis often swollen.
C. Pauciarticular JIA affects the large joints (knees,ankles, wrists, elbows), but virtually never begins inthe hips. Systemic manifestations (other thanuveitis) are characteristically absent. Thus, fever,rash, or other constitutional symptoms suggest adifferent diagnosis.
D. The involved joints are typically swollen and tenderto compression. They may be warm, but they shouldnot be erythematous. Limitation of motion may notbe present. Long-term complications ofpauciarticular JIA, include uveitis and leg lengthdiscrepancy.
American College of Rheumatology Criteria forDiagnosis of JRA
Diagnostic Requirements For JRA• Documented arthritis of one or more joints for 6 weeks
or longer• Exclusion of other conditions associated with childhood
arthritis- Other rheumatic diseases- Infectious diseases- Childhood malignancies- Nonrheumatic conditions of bones and joints- Miscellaneous conditions
II. Diagnosis. A. The diagnosis of pauciarticular onset JIA is based
upon the presence of arthritis in four or fewer jointsduring the first six months of disease. If a singlejoint is involved, arthritis must be present for atleast three months and multiple alternative causesof arthritis must be excluded. If two or more jointsare involved, arthritis must be present for at least

six weeks, with the elimination of exclusions.
Objective Signs of Arthritis
Joint Swelling- Synovial hypertrophy - Increased amounts of
synovial fluid- Swelling of periarticular
tissuesJoint Pain
- On motion- On palpation (tender-
ness) - At rest
Loss of Joint Motion- Stiffness of joints
Joint WarmthJoint Erythema
B. Laboratory findings1. Antinuclear antibodies (ANAs) are frequently
present in pauciarticular JIA and are associatedwith an increased risk of iridocyclitis. ANAs aretypically present in low or moderate titers in ahomogeneous pattern. Antibodies to dsDNA, Ro,La, Sm, and RNP, and rheumatoid factor shouldbe absent.
2. The erythrocyte sedimentation rate is close tonormal, there is a normal white blood cell countwithout a left shift, and a normal platelet count.
C. Differential diagnosis1. Dactylitis (a swollen finger or toe) may be
pauciarticular, but is more typical of psoriaformarthritis.
2. Children over the age of 9 years with arthritisinvolving the hips or knees and enthesiopathicsymptoms also do not have pauciarticular JIA;t h e s e a r e m a n i f e s t a t i o n s o f aspondyloarthropathy.
3. Children with plant thorn synovitis, septic arthritis,osteomyelitis, or even Lyme disease are mistak-enly diagnosed with pauciarticular JIA. Theseconditions are usually associated with elevatedacute phase reactants. These conditions areoften acutely painful with sudden and dramaticonset, the opposite of pauciarticular JIA.
III. Course and prognosis. Most cases of pauciarticularJIA are benign, resolving within six months. Fifty-fourpercent remit completely. The major morbidity istypically related to the development of uveitis. Recur-rences occur in 20 percent of children. A few childrenwith typical pauciarticular disease evolve into chronicdestructive arthritis. There should not be any systemiccomplications of pauciarticular JIA other than uveitis.
A. Uveitis1. The most serious complication of pauciarticular
JIA, occurring in approximately 20 percent ofchildren, is the development of uveitis oriridocyclitis (inflammation of the anterior uvealtract and the adjacent ciliary body). The subgroupof children with pauciarticular JIA who havedetectable ANAs are at greatest risk of develop-ing iridocyclitis.
2. Uveitis is often initially silent; by the time the childcomplains of pain in the eye or difficulty seeing, itis likely that permanent and irreversible damagehas already occurred. Thus, routine screening isnecessary. Screening must be performed by anophthalmologist and includes a complete slit lampexamination.
B. Leg length discrepancy. There may be significantasymmetric overgrowth when a single knee joint isinvolved, resulting in a leg length discrepancy overtime. Joint injection with glucocorticoids early in thecourse of pauciarticular JIA may prevent leg lengthdiscrepancies. Leg length discrepancies of lessthan 1 cm are probably not important. When theybecome greater, however, proper gait should bemaintained by placing an appropriate lift in theopposite shoe.
IV. Treatment of juvenile rheumatoid arthritisA. Medical therapy. Pauciarticular onset JIA is usually
responsive to nonsteroidal antiinflammatory drugs(NSAIDs) or selective COX-2 inhibitors.Methotrexate and other immunosuppressive drugsare rarely, if ever, required. However, some chil-dren will have disease activity in one or two jointsfor a prolonged period that does not respond toNSAIDs.

NSAID Treatment of Juvenile Rheumatoid Arthri-tis
Ibuprofen(Motrin)
1 to 12 years: 10 mg/kg PO q 4 to 6 h More than 12 years: 200 to 400 mg PO q 4h; maximum dose 1,200 mg/day
Naproxen(Aleve)
5 mg/kg PO q 12 h; maximum dose 750mg/day
B. Intraarticular injection of glucocorticoids may behelpful if only a single joint is involved and therehas been an inadequate response to NSAIDs afterthree or more months of therapy.
C. Etanercept (Enbrel) is a soluble tumor necrosisfactor alpha (TNFa) receptor fusion protein thatbinds TNFa, thereby reducing its activity.Etanercept is best reserved for children with asignificant elevation of the erythrocyte sedimenta-tion rate.
References, see page 182.
Renal and Urologic Disor-dersHematuriaHematuria occurs in about 0.5% and 1% of all children. Itis defined as more than 5 to 10 RBCs per high-powermicroscopic field from a centrifuged midstream voidedurine sample. The urine may be yellow, pink, red, brown,or smoky. Hemoglobin and myoglobin will produce thesame color changes on the dipstick as intact RBCs. Eachurine sample that tests positive for blood by dipstick mustbe examined microscopically to confirm the presence ofintact RBCs.
I. Clinical evaluationA. If microscopic hematuria has been present for 1
month or more, further investigation for the cause isindicated. Vigorous exercise such as jogging or bikeriding may cause hematuria. Abdominal, back orflank pain, especially when associated with bruising,suggests child abuse. Dysuria, urinary frequency,and suprapubic pain or tenderness suggests aurinary tract infection or hypercalciuria.
B. Abdominal pain may be associated with an abdomi-nal mass, nephrolithiasis, or Henoch-Schönleinpurpura. Aspirin, non-steroidal anti-inflammatoryagents, antibiotics, methyldopa, and other drugs cancause hematuria.
C. A history of edema, hypertension, skin rash, pallor,joint swelling or tenderness, abdominal pain, orbloody diarrhea suggests postinfectiousglomerulonephritis, Henoch-Schönlein purpura,lupus nephritis, hemolytic uremic syndrome, orimmunoglobulin (Ig) A nephropathy.
D. If sore throat or pyoderma precedes the hematuriaby 7 to 30 days, poststreptococcal acuteglomerulonephritis must be ruled out. Hematuria witha concurrent upper respiratory infection stronglysuggests IgA nephropathy. Each of these forms ofglomerulonephritis usually is associated withproteinuria and RBC casts.
Evaluation of Hematuria
Patient history, family history, physical examinationExamination of urine for red blood cell casts and crystalsScreening for proteinuria with a dipstickExamination of urine of first-degree relatives for hematuriaUrine cultureUrinary calcium/urinary creatinine; 24-hour urinary calciumexcretionSerum creatinine, C3, streptozyme titerRenal ultrasonographyPlain abdominal film if nephrolithiasis is suspected

Differential Diagnosis of Persistent Hematuria
Without Proteinuria With Proteinuria
Urinary tract infection Urinary tract infection
Hypercalciuria Poststreptococcal acuteglomerulonephritis
Thin basement membranedisease
IgA nephropathy
Sickle cell disease or trait Henoch-Schönlein purpura
Renal cystic disease Membranoproliferativeglomerulonephritis
Nephrolithiasis Lupus nephritis
Renal anatomic abnormali-ties
Alport syndromeHemolytic-uremic syndromeOther forms ofglomerulonephritis
E. A family history of hematuria without renal failuremay be seen with thin basement membrane disease.A family history of hematuria, chronic renal failure,dialysis or renal transplantation with bilateral deaf-ness and ocular abnormalities suggests Alportsyndrome. An audiogram is indicated for childrensuspected of having Alport syndrome.
F. A family history of nephrolithiasis raises the diagnos-tic possibility of nephrolithiasis or hypercalciuria. Afamily history of autosomal dominant polycystickidney disease requires that this disease be ruledout by ultrasound. Sickle cell disease or sickle celltrait in the patient’s family may suggest this diagno-sis.
G. Urinalysis. RBCs from areas of the urinary tractother than glomeruli will be normal in size withsmooth edges (eumorphic). Nonglomerular bleedingusually is associated with normal urinary proteinexcretion and an absence of RBC casts.
Familial Causes of Hematuria
Polycystic kidney diseaseThin basement membrane diseaseSickle cell disease or traitAlport syndrome (hereditary nephritis with deafness)Hypercalciuria with family history of nephrolithiasis
H. Preliminary tests should include a urine culture,blood sickle cell preparation in African-Americanchildren, urinary calcium; urinary creatinine ratio,serum creatinine; C3, and streptozyme titer.Ultrasonography of the kidneys and urinary bladderis recommended to rule out polycystic kidneydisease, tumor, ureteropelvic junction obstruction,and stones.
I. The presence of proteinuria (>1+ on dipstick)strongly suggests glomerulonephritis. The diagnosisof glomerulonephritis demands microscopic inspec-tion of the urinary sediment for RBC casts. RBCsthat have bizarre shapes, blebs, or burrs(dysmorphic RBCs) correlate with a glomerularorigin of the RBC.
J. Proteinuria1. If proteinuria is present on urinalysis, urinary
protein excretion should be measured by a timed12- or 24-hour urine collection or a urineprotein:urine creatinine ratio on a single voidedsample.
2. A complete blood count, C3, C4, antistreptolysin-O titer, streptozyme titer, serum electrolytes,blood urea nitrogen, serum creatinine, serumalbumin, test for lupus erythematosus, hepatitisB screen, and antinuclear cytoplasmic antibodytiter are indicated to clarify the type ofglomerulonephritis. A screening urinalysis onfirst-degree family members is also important.When confirmatory serologic tests arenondiagnostic, a renal biopsy usually is indi-cated.
Renal Structural Abnormalities Associated withHematuria
Polycystic kidney diseaseUreteropelvic junction obstructionVesicoureteral refluxRenal or bladder stones, diverticula or tumorsRenal arteriovenous fistulaForeign bodies

References, see page 182.
Fluids and ElectrolytesDisorders affecting the body fluids and electrolytes aretreated by supplying maintenance requirements, correct-ing volume and electrolyte deficits, and by replacingongoing abnormal losses.
I. DehydrationA. Maintenance fluid and electrolytes
1. Sensible losses, primarily urinary, account for50% of daily fluid requirements. Caloric require-ments for growth can be estimated as equivalenton a kcal-for-mL basis to water requirements.
2. Factors that increase the requirements for calo-ries and water are fever (10% for each degree),physical activity, ongoing gastrointestinal losses,hyperventilation, and hypermetabolic states.
Maintenance Requirements for Fluid and Electro-lytes
BodyWeight
0 to 10kg
10 to 20kg
>20 kg
Water Vol-ume
100 mL/kg 1000 mL +50 mL/kg foreach kg >10kg
1500 mL + 20mL/kg for eachkg >20 kg
Sodium 3 mEq/kg 3 mEq/kg 3 mEq/kg
Potassium 2 mEq/kg 2 mEq/kg 2 mEq/kg
Chloride 5 mEq/kg 5 mEq/kg 5 mEq/kg
3. Abnormal losses, such as those arising fromnasogastric aspiration, prolonged diarrhea orburns, should be measured, and replaced on avolume for volume basis.
B. Estimation of deficit1. Estimation of volume depletion should assess
fever, vomiting, diarrhea, and urine output.Recent feeding, including type and volume offood and drink, and weight change should bedetermined.
Estimation of Dehydration
Degree of Dehy-dration
Mild Moderate Severe
Weight Loss--Infants
5% 10% 15%
Weight Loss--Children
3-4% 6-8% 10%
Pulse Normal Slightly in-creased
Very in-creased
Blood Pressure Normal Normal toorthostatic,>10 mm Hgchange
Orthostaticto shock
Behavior Normal Irritable Hyperirrit-able tolethargic
Thirst Slight Moderate Intense
Mucous Mem-branes
Normal Dry Parched
Tears Present Decreased Absenttears,sunkeneyes
Anterior Fonta-nelle
Normal Normal tosunken
Sunken
External JugularVein
Visible whensupine
Not visibleexcept withsupraclavicular pressure
Not visibleeven withsupraclavicular pres-sure
Skin Capillaryrefill <2 sec
Delayedcapillary re-fill, 2-4 sec(decreasedturgor)
Very de-layed cap-illary refill(>4 sec),tenting;cool, acro-cyanotic ormottledskin
Urine SpecificGravity (SG)
>1.020 >1.020;oliguria
Oliguria oranuria

2. The percent dehydration is used to calculatethe milliliters of body water deficit per kilogramof body weight.
C. Isonatremic dehydration1. The most common cause of dehydration in
infants is diarrhea. Children who have a briefillness and anorexia usually present with iso-tonic dehydration.
2. Oral rehydrationa. Moderate volume depletion should be
treated with oral fluids. The majority of pa-tients who have gastroenteritis can betreated with oral rehydration therapy.
b. Small aliquots of oral hydration solution(Ricelyte, Pedialyte, Resol, Rehydralyte) aregiven as tolerated to provide 50 mL/kg over4 hours in mild dehydration, and up to 100mL/kg over 6 hours in moderate dehydra-tion. Once rehydration is accomplished,maintenance fluid is given at 100 mL/kg perday.
3. Parenteral rehydrationa. Parenteral fluids should be given for severe
volume depletion, altered states of con-sciousness, intractable vomiting, and ab-dominal distention or ileus.
b. The first phase of treatment rapidly expandsthe vascular volume. Intravenous normalsaline or Ringers lactate (10-20 mL/kg)should be given over 1 hour.
c. The next phase of treatment is aimed atcorrecting the deficit, providing mainte-nance, and replacing ongoing abnormallosses. In severe depletion, half of thecalculated deficit is given over the first 8hours and the second half over the next 16hours; maintenance needs are provided.Five percent glucose should be used as thestock solution and NaCl is added accordingto the estimated need.
d. Children who have isonatremic dehydrationrequire 8 to 10 mEq of Na+ per kg of bodyweight for repletion of deficit and 3 mEq/kgper day for maintenance. This Na+ is given ina volume consisting of the calculated main-tenance for water and the estimated waterdeficit. Once urine flow occurs, KCl is addedat a concentration of 20 mEq/L.
D. Hyponatremia and hyponatremic dehydration1. The signs and symptoms of hyponatremia
correlate with the rapidity and extent of the fallin serum Na+ concentration. Symptoms includeapathy, nausea, vomiting, cramps, weakness,headache, seizures, and coma.
2. If the correction of fluid and electrolyte losses isexcessively rapid, the brain may sustain injury.In severe hyponatremia, plasma Na+ concentra-tion should be corrected at no more than 10-12mEq/L/day.
3. Differential diagnosis of hyponatremiaa. Hypovolemia
(1) The most frequent cause of hypovolemichyponatremia is viral gastroenteritis withvomiting and diarrhea. Other causes ofhypovolemic hyponatremia includepercutaneous losses or third spacesequestration of fluid (ascites, burns,peritonitis).
(2) Renal sodium loss (urinary Na+ >20mEq/L) may be caused by diuretics, salt-wasting nephropathy, proximal renaltubular acidosis, and lack of or resis-tance to mineralocorticoid.
b. Euvolemia. The most common cause ofeuvolemic hyponatremia is the syndrome ofinappropriate antidiuretic hormone secre-tion, which is caused by water retention(urinary Na+ is usually >20 mEq/L). Causesinclude tumors, pulmonary disorders, CNSinfection, and certain drugs. Euvolemichyponatremia may also occur in infants fedexcessively diluted infant formula.
c. Hypervolemia. Hypervolemic hyponatremia,associated with edema, may result fromwater retention and excess Na+, as innephrosis, congestive heart failure, cirrho-sis, or renal failure.
4. Management of hyponatremiaa. Hypovolemic patients who have
hyponatremia first require volume repletionwith normal saline, then a solution contain-ing salt is given to correct the Na+ deficit (10to 12 mEq/kg of body weight or 15 mEq/kgin severe hyponatremia) and to provide theNa+ maintenance needs (3 mEq/kg per day)

in a 5% dextrose solution.b. For a serum Na+ concentration of 120 to 130
mEq/L, this amount should be given over a24-hour period. For a serum Na+ concentra-tion <120 mEq/L, the rehydration should bespread out over several days at a rate of 10mEq/day.
c. Symptomatic hyponatremia (headache,lethargy, disorientation) requires urgenttherapy to prevent seizures or coma. (1) Hypertonic saline (3% saline solution)
should be used to raise the serum Na+
by 1 to 2 mEq/L per hour or halfwaytoward normal during the first 8 hours.
(2) A correction using 3% saline over 4hours can be calculated according to thefollowing formula:
Sodium deficit in mEq = (125 - observed[Na+]) x body weight in kg x 0.6
E. Hypernatremia and hypernatremic dehydration1. The hypernatremic patient is usually also
dehydrated. Total body Na+ most commonly isdecreased. Affected patients frequently exhibitlethargy or confusion, muscle twitching,hyperreflexia, or convulsions. Fever is com-mon, and the skin may feel thickened ordoughy.
2. Differential diagnosisa. Diarrhea, which usually results in
isonatremic or hyponatremic dehydration,may cause hypernatremia in the presence ofpersistent fever, anorexia, vomiting, anddecreased fluid intake.
b. Other causes of hypernatremia includewater and Na+ deficit from skin losses orrenal losses, and water losses from centralor nephrogenic diabetes insipidus (DI) ordrugs (lithium, cyclophosphamide).
3. Managementa. Initial therapy requires administration of nor-
mal saline or Ringers lactate to restorecirculating plasma volume. Hypovolemicpatients who have hypernatremia require ahypotonic solution containing salt to restorethe Na+ deficit (2-5 mEq/kg of body weight)and to provide the Na+ maintenance (3mEq/kg of Na+) in a solution containing 20-40 mmol/L of KCl and 5% glucose.
b. For a serum Na+ concentration of 150-160mEq/L, this volume should be given over 24-hours. An elevated serum Na+ concentrationshould be corrected by no more than 10mEq/L per day.
c. For a serum Na+ concentration >160 mEq/L,the rehydration should be spread out overseveral days to lower the Na+ concentrationto 150 mEq/L by 10 mEq/day.
II. Potassium disordersA. Hypokalemia
1. Hypokalemia (serum K+ concentration <3mEq/L) is most frequently caused by gastroin-testinal K+ losses or renal losses (nasogastricsuction, protracted vomiting, diuretics, renaltubular disease). Manifestations ofhypoka lemia inc lude a r rhythm ias ,neuromuscular excitability (hyporeflexia orparalysis, decreased peristalsis, ileus), andrhabdomyolysis.
2. Intracellular K+ concentration can be estimatedfrom the electrocardiogram, which may revealflattened T waves, shortened P-R interval andQRS complex, and eventually U waves.
3. Managementa. In the presence of cardiac arrhythmias,
extreme muscle weakness, or respiratorydistress, patients should receive KCl intrave-nously with cardiac monitoring. Once theserum K+ is stabilized, oral administration ispreferable.
b. If the patient is likely to behypophosphatemic, a phosphate salt shouldbe used. In metabolic alkalosis, KCl shouldbe used; in renal tubular acidosis, a citratesalt should be used.
B. Hyperkalemia1. The most common cause of hyperkalemia (K+
>5.5 mEq/L) is “pseudohyperkalemia” fromhemolysis of the blood sample. This causeshould be excluded by repeating the measure-ment on a free-flowing venous sample. Chil-dren may display hyperkalemia in metabolicacidosis, tissue catabolism, renal failure, vol-ume depletion, or hypoaldosteronism.

2. In salt-losing congenital adrenal hyperplasia,due to complete deficiency of the enzyme 21-hydroxylase, the symptoms in affected maleinfants appear in the first weeks of life andinclude dehydration and failure to thrive to-gether with low serum Na+ and high K+ con-centrations. Affected female infants usually arediagnosed at birth because of ambiguousgenitalia.
3. Manifestations of hyperkalemia include cardiacarrhythmias, paresthesias, muscle weakness,and paralysis.
4. The electrocardiogram demonstrates narrow,peaked T waves and shortened QT intervals atK+ concentrations >6 mEq/L and depressed STsegment and widened QRS complex at K+
concentrations >8 mEq/L.5. Management
a. Emergent therapy to reverse potentially life-threatening hyperkalemia consists of intra-venous calcium. The onset of action is rapid;however, the duration is less than 30 min-utes.
b. Emergent administration of glucose willcause K+ to redistribute to the intracellularspace. Glucose, 0.5 gm/kg, can be givenover 30-60 minutes when EKG changes arepresent.
c. Sodium polystyrene sulfonate (Kayexalate)(1 gm/kg) can be given by high-rectal en-ema or orally. Severe hyperkalemia istreated with hemodialysis.
III. Acid-base disordersA. The pH of the body fluids normally is between 7.35
and 7.45.B. Metabolic acidosis
1. Acidosis results from the addition of acid or theremoval of alkali from body fluids, and it causesa compensatory increase in ventilation (respira-tory alkalosis) and a fall in pCO2. Manifestationsof acidosis include depressed myocardial con-tractility, arrhythmias, hypotension, and pulmo-nary edema.
2. Diagnosisa. Addition of a fixed acid to the extracellular
fluid causes the formation of unmeasuredanions. These unmeasured anions are re-ferred to as the anion gap, which can beestimated as:
Anion gap = Na+ - (Cl +HCO3-) = 10-12 mEq/L
3. Differential diagnosis a. Normal anion gap (hyperchloremic) aci-
dosis(1) This disorder occurs when HCO3
- is lost
from the body, either through the gastro-intestinal tract or the kidneys. Diarrhealfluid is high in HCO3
-, high in K+, and lowin Cl-. Thus, diarrhea causeshypokalemia and hyperchloremic acido-sis.
(2) Failure to excrete acid occurs in mildchronic renal insufficiency and RTA.
b. Increased anion gap acidosis may becaused by diabetic ketoacidosis, lactic acido-sis, ingestion of toxins (aspirin, ethyleneglycol), and renal failure.
4. Treatment of acidosisa. Bicarbonate should be given when plasma
HCO3- is <5 mmol/L. Bicarbonate should be
added to a hypotonic solution and given asa continuous infusion over 1 hour. Theamount to infuse is calculated with the fol-lowing formula:
Amount to infuse in mEq = weight in kg (15-observed [HCO3
-]) x 0.5
b. With severe watery diarrhea, resulting inmoderate-to-severe metabolic acidosis,volume replacement is the primary mode oftherapy.
C. Metabolic alkalosis1. Alkalosis results from a gain of base or a loss of
acid. The common clinical manifestations arelethargy, confusion, neuromuscular irritability,arrhythmias, and seizures.
2. Differential diagnosisa. Causes of metabolic alkalosis include alkali
administration, vomiting, and nasogastricaspiration. In patients with GI loss of acidfrom vomiting, urinary Cl- concentration isusually below 20 mEq/L.
b. Cushing syndrome, Bartter syndrome or

primary aldosteronism may cause metabolicalkalosis.
3. Treatmenta. Therapy consists of identifying and treating
the underlying pathology.b. In mild-to-moderate alkalosis, provision of Cl-
will allow the kidney to excrete the excessbase.
D. Respiratory acidosis1. Respiratory acidosis is induced by an increase
in pCO2, which lowers plasma pH. Causes ofrespiratory acidosis include airway obstruction,and pulmonary disorders.
2. Treatment consists of mechanical ventilationand correction of the underlying disorder.
E. Respiratory alkalosis 1. Respiratory alkalosis is caused by a decrease in
pCO2, secondary to hyperventilation, resulting indizziness, confusion, and seizures.
2. Causes of respiratory alkalosis include hyper-ventilation caused by CNS disorders and panicdisorder. Treatment involves correcting theunderlying disorder. Rebreathing into a bag maydecrease the severity of symptoms.
References, see page 182.
Vesicoureteral RefluxVesicoureteral reflux (VUR) is defined as the retrogradepassage of urine from the bladder into the upper urinarytract. Vesicoureteral reflux occurs in 1 percent of new-borns and 30 to 45% in young children with urinary tractinfection.
VUR predisposes to acute pyelonephritis by allowingbacteria to migrate from the bladder to the kidney.Pyelonephritis may lead to renal scarring, renal injury withsubsequent hypertension, decreased renal function,proteinuria, renal failure, and sometimes end stage renaldisease (ESRD).
I. Grading of VUR based on findings from a contrastvoiding cystourethogram (VCUG).
Grade I - Reflux only fills the ureter without dilation.Grade II - Reflux fills the ureter and the collectingsystem without dilation.Grade III - Reflux fills and mildly dilates the ureterand the collecting system with mild blunting of the calyces.Grade IV - Reflux fills and grossly dilates the ureterand the collecting system. One-half of the calycesare blunted.Grade V - Massive reflux grossly dilates the collect-ing system. All the calyces are blunted with a loss ofpapillary impression and intrarenal reflux may bepresent. There is significant ureteral dilation andtortuosity.
A. Grades I and II are classified as mild reflux, grade IIIas moderate, and grades IV and V as severe.
II. Epidemiology. VUR is present in one percent ofnewborns. The risk of VUR is increased in youngchildren with urinary tract infection, with an incidencethat ranges from 30 to 45%.A. Caucasian children were three times more likely to
have VUR than African-American children. Themaximal grade of reflux Is significantly lower inAfrican-American children.
B. Gender. Girls were twice as likely to have refluxthan boys.
C. Age. Young children and infants (0 to less than 2years of age) are more likely to have VUR than olderchildren.
III. Presentation, diagnosis, and courseA. Prenatal presentation. The presence of VUR is
suggested prenatally by the finding ofhydronephrosis via ultrasonography. VUR is presentin 10 to 40% of all fetuses with prenatally diagnosedhydronephrosis.
B. Postnatal presentation. Postnatal diagnosis ofVUR is usually made after a UTI. Girls are twice aslikely to have VUR after an initial febrile UTI. RoutineVCUG should be therefore performed among thefollowing groups:1. Any male child with a first UTI.2. Girls under the age of three years with a first UTI.3. Any child under five years of age with a febrile
UTI.4. Children with recurrent UTI.5. Children who have a positive RNC on screening.6. Children with other prenatal renal anomaly.7. Children with three urinary tract infections with
unusual organisms.C. Screening of siblings and parents of children
with VUR. Screening of is recommended becauseof the increased familial incidence of VUR.

1. In siblings below two years of age without ahistory of unexplained febrile illnesses or urinarytract infections, a renal ultrasound is recom-mended at three months of age, and aradionuclide cystogram (RNC) is recommendedat six months or at the time of diagnosis of theindex patient.
2. In siblings between two and four years of agewithout a history of unexplained illnesses orurinary tract infections, a RNC is recommended.
3. In siblings above six years of age or parentswithout a history of unexplained febrile illnessesor urinary tract tract infections, a renal ultrasoundis recommended.
4. Siblings with a history of febrile illnesses orrecurrent urinary tract infections, abnormal ultra-sound, or RNC, a VCUG is recommended.
IV. Clinical courseA. Grades I and II. By five years of age, spontaneous
resolution occurrs in 80% of patients.B. Grade III. The oldest group of children 5 to 10 years
of age with bilateral reflux have less than 20%resolution over five years. Children (one to twoyears) with unilateral disease have a 70% resolutionrate.
C. Grade IV. There is a 60% resolution rate for unilat-eral disease and less than 10% resolution rate forbilateral reflux over five years regardless of age atpresentation.
D. Grade V. Spontaneous resolution is rare.E. Renal scarring has been associated with VUR with
30 to 60% of patients having evidence of renalscarring at initial diagnosis of VUR.
V. Management of vesicoureteral reflux
Treatment of Children with Vesicoureteral Reflux
Clinical presenta-tion
Age ofpatient,years
Gradeof reflux
Treatment Comments
Lessthan 1
Allgrades
Antibioticprophylaxis
1 to 5 I and II Antibioticprophylaxis
1 to 5 III and IV Antibioticprophylaxis
If renalscarring or
bilateralreflux,surgeryis op-tional
1 to 5 V Antibioticprophylaxis
If renalscarring or
bilateralreflux,surgeryis op-tional
6 orgreater
I and II Antibioticprophylaxis
If renalscarring or
bilateralreflux,surgeryis op-tional
6 orgreater
III and IV Antibioticprophylaxis
If renalscarring
or bilat-eralreflux,surgeryis op-tional
6 orgreater
V Surgicalrepair
A. Children below one year of age, regardless ofgrade of reflux, should be treated medically be-cause they have a high likelihood of spontaneousresolution. Surgery is a reasonable option if theyhave grade V reflux and renal scarring.
B. All patients with grade I or II reflux, either with

unilateral or bilateral disease, should be treatedmedically as they have high likelihood of sponta-neous resolution.
C. Children between one and five years of age withgrade III or IV reflux, either unilateral or bilateraldisease, should be treated medically. Surgery is areasonable option if there is bilateral reflux andrenal scarring.
D. Children between one and five years of age withgrade V without renal scarring can be treatedmedically. If there is renal scarring, surgery isrecommended.
E. Children six years or older with unilateral grade III-IV reflux without renal scarring can be treatedmedically. If the reflux is bilateral and/or there isrenal scarring, surgical treatment is recom-mended.
F. Children six years or older with grade V refluxshould be treated surgically.
G. Surgery should also be considered if medicaltherapy fails either due to poor compliance, break-through infections due to antibiotic resistance, orsignificant antibiotic side effects.
VI. Follow-upA. Urine cultures are required whenever there are
urinary symptoms suggestive of UTI or unex-plained fever. Surveillance cultures are obtainedevery three to four months.
B. Monitoring of reflux is done by either VCUG orRNC. RNC is the preferred modality as there isless radiation. Yearly evaluation is currently rec-ommended. Patients who have undergone surgicalcorrection require a post-operative VCUG or RNCto document whether the surgery was successful.
C. DMSA scans are recommended in patients withreflux who have an abnormal ultrasound and ininfants who have a febrile urinary infection, dem-onstrated reflux, and a normal ultrasound. Renalultrasound is not as sensitive in detecting renalscars as DMSA scan and has not been as usefulin follow-up.
D. Postnatal. This group of patients are predomi-nantly female and present after an initial febrileillness. The rate of spontaneous resolution isdependent upon age, grade of reflux, and whetherthe reflux is unilateral or bilateral. Medical treat-ment consists of prophylactic antibiotic therapywith trimethoprim-sulfamethoxazole, trimethoprimalone, or nitrofurantoin. One daily dose is adminis-tered at bedtime at one-half the usual dose fortreating an acute infect
E. Patients who are treated medically need to bemonitored in the following manner:1. Mandatory urine cultures are required when-
ever there are urinary symptoms suggestive ofUTI or unexplained fever.
2. Surveillance cultures are obtained every threeto four months.
3. Screening for VUR on a yearly basis with RNC.





























