Embed Size (px)
Citation preview

9/14/2016
1
Ch. 7 – Sensory Physiology
Objectives:
1. Steps to Sensory Perception 2. Categories of Sensory Receptors and Stimuli They Respond To. 3. Somatic Senses versus Special Senses
1. Stimulus – acts on a sensory receptor. 2. Transduction – stimulus causes an action potential in sensory neuron.
3. Conduction – info. about stimulus ascends by sensory neurons through afferent path to brain. 4. Perception – “awareness” and evaluation of the stimuli by the brain.
Part 1: Steps to Sensory Perception

9/14/2016
2
CNS Distinguishes 4 Stimulus Properties:
A. TYPE of stimulus (which receptor activated) see more about receptor types later
B. Stimulus Location – where in body
C. Stimulus Intensity – how strong stimulus is (by number of receptors activated & frequency of APs coming from receptor)
D. Stimulus Duration – how long (duration of APs in sensory neurons)
Somatosensory cortex
1. The Stimulus
4
B. Stimulus Location Ex: 2-point touch discrimination = test of mechanoreceptors for touch in the skin
If stimulus applied to location having high density of sensory receptors, more APs form, brain has better sensory perception. Stimulus needs to hit “center” of receptor. If hits only outer (lateral) edge, stimulation of receptor inhibited (called “lateral inhibition”)
Receptor with more dendrites = bigger response
Lateral inhibition if outer edge of receptor stimulated

9/14/2016
3
C. Stimulus Intensity
Ex. IF small Stimulus
Sensory receptor (= transducer)
Afferent sensory neurons
CNS
Integration, perception
Weak stimulus causes only few APs in receptor
Minimal perception
IF BIG Stimulus
Sensory receptor (= transducer)
Afferent sensory neurons
CNS
Integration, perception
stronger stimulus causes more frequent APs in the receptor.
C. Stimulus Intensity
Greater perception

9/14/2016
4
D. Stimulus Duration how long (duration of APs in sensory neurons)
2 responses to sustained stimulation : Tonic receptors Slow or no adaptation Continuous APs form for duration of stimulus For functions that must be continuously monitored (Ex. Baroreceptors for blood pressure) Phasic receptors Rapid adaptation APs stop if stimulus remains constant Allow body to ignore constant unimportant info.
Ex. Smell, mild temperatures.
Types of Sensory Receptors: A) sensory neuron – the receptor IS an afferent neuron.
B) special receptor cell – intermediate cell senses stimulus, releases neurotransmitter, which stimulates sensory neuron.
2. Stimulus Transduction
AP
AP
Stimulus received by receptor & “transduced” (converted) into a graded AP in sensory neuron.

9/14/2016
5
Stimulus Transduction = Graded AP Response in Sensory Receptor
Stimulus too small
Moderate stimulus
Large stimulus
No AP in receptor
Some APs in receptor
Many APs in receptor
No neurotransmitter released
Neurotrans. released
LOTS of neurotrans. released
Stimulus
Sen
sory
N
eu
ron
AP
! !!!!! X
3. Conduction of Stimulus
Primary sensory neurons - signal from receptor goes to spinal cord or medulla
Secondary sensory neurons signal crosses over (in spinal cord or medulla) to thalamus
Tertiary sensory neurons somatosensory cortex in parietal lobe (post central gyrus)
4. CNS Perception of Stimulus
Left Right
thalamus
medulla
Spinal cord
info. about stimulus ascends by sensory neurons through afferent path to brain

9/14/2016
6
Review • Steps to sensory perception (stim., transduction, conduction, perception)
• Transduction & perception of stimuli based on:
– Type of signal (based on type of receptor stimulated)
– Signal location (are more than one receptor involved)
– Signal strength (stronger stim = more APs in sensory neuron)
– Signal duration (some sensory neurons “adapt”, others don’t)
11
Check syllabus for blank flow
diagram on PNS communication!

9/14/2016
7
Part 2: Categories of Sensory Receptors & Stimuli They Respond To
1. Chemoreceptors – chemicals (taste, smell, pH, and O2, CO2)
2. Thermoreceptors – heat (> 37C) and cold (< 37C)
3. Mechanoreceptors – touch, pressure, vibration. – equilibrium and hearing in inner ear.
4. Photoreceptors – for light (in retina of eye)
5. Proprioceptors – for feedback on movement or stretch (in muscles, joints, tendons, & ligaments)
6. Cutaneous receptors – in skin for touch, pressure, heat, cold, pain.
• Somatic senses = proprioceptors & cutaneous receptors all over body
1. Proprioceptors = Stimuli from skin, muscles, joints, ligaments, and tendons. Sense stretch, movement, body posture. 2. Cutaneous receptors – sense touch, pressure, heat, cold, & pain (mechanoreceptors, thermoreceptors, nocireceptors). Signal conducted to the spinal cord first, crosses over in spinal cord or thalamus, then to somatosensory part of brain.
• Special Senses – Stimuli of smell, taste, sight, and sound.
(olfactory receptors, photoreceptors, mechanoreceptors)
– Have specialized sensory receptors in head
– Signal conducted directly to the brain
Part 3: Somatic Senses versus Special Senses
9/14/2016
8
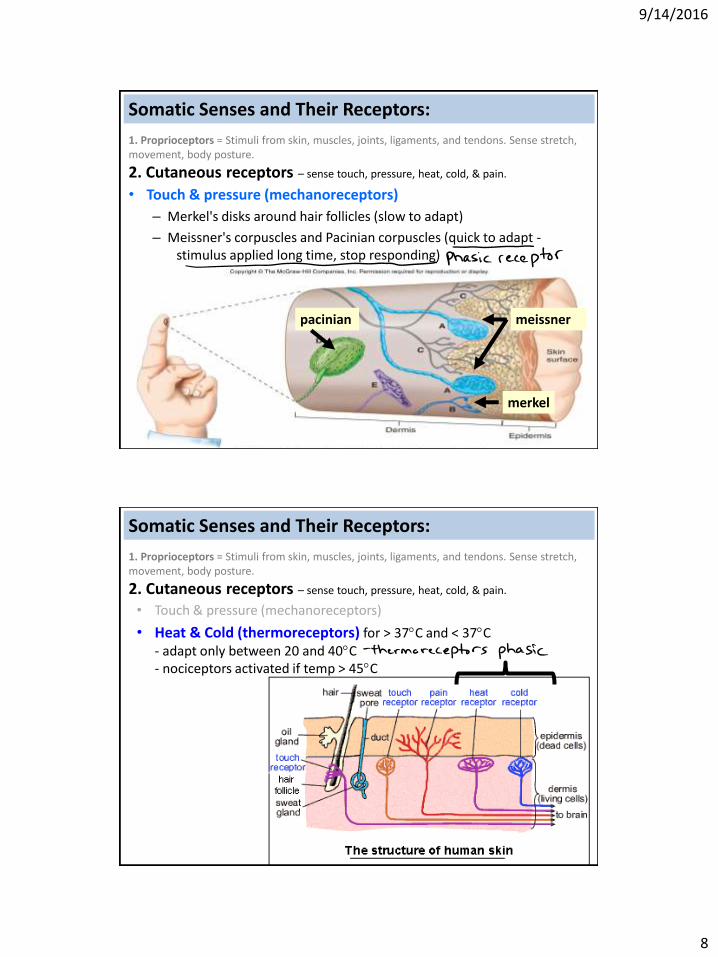
1. Proprioceptors = Stimuli from skin, muscles, joints, ligaments, and tendons. Sense stretch, movement, body posture.
2. Cutaneous receptors – sense touch, pressure, heat, cold, & pain.
• Touch & pressure (mechanoreceptors)
– Merkel's disks around hair follicles (slow to adapt)
– Meissner's corpuscles and Pacinian corpuscles (quick to adapt - stimulus applied long time, stop responding)
pacinian meissner
merkel
Somatic Senses and Their Receptors:
Somatic Senses and Their Receptors:
1. Proprioceptors = Stimuli from skin, muscles, joints, ligaments, and tendons. Sense stretch, movement, body posture.
2. Cutaneous receptors – sense touch, pressure, heat, cold, & pain.
• Touch & pressure (mechanoreceptors)
• Heat & Cold (thermoreceptors) for > 37C and < 37C - adapt only between 20 and 40C - nociceptors activated if temp > 45C

9/14/2016
9
Somatic Senses and Their Receptors:
1. Proprioceptors = Stimuli from skin, muscles, joints, ligaments, and tendons. Sense stretch, movement, body posture.
2. Cutaneous receptors – sense touch, pressure, heat, cold, & pain.
• Touch & pressure (mechanoreceptors)
• Heat & Cold (thermoreceptors)
• Pain (nociceptors)
- Activated by strong, noxious stimulu - 3 categories of pain stimuli: mechanical, thermal, chemical - Might activate 2 pathways: A) Reflex movement (signal to spinal cord then to motor neuron) Body part retracts from stimulus (before you realize it hurt) B) Brain perception - signal goes up to somatosensory cortex (OUCH! you realize it hurt) - signal goes to limbic system & hypothalamus (Emotional Distress)
Referred Pain
Pain in organs is poorly localized
May be displaced if
Multiple 1° sensory neurons converge on single ascending tract in spinal cord
9/14/2016
10
Review • Types of receptors
– Chemoreceptors
– Mechanoreceptors
– Thermoreceptors
– Photoreceptors
– Proprioceptors
– Cutaneous receptors
• Somatic senses versus special senses
– Cutaneous receptors
• Touch & pressure mechanoreceptors
• Heat & cold thermoreceptors
• Nociceptors
19
For “somatic senses”
• Taste (gustation)
• Smell (olfaction)
• Vision
• Hearing (auditory)
• Equilibrium (vestibular)
Special Senses and Their Receptors:

9/14/2016
11
Taste (gustation)
Special Senses and Their Receptors:
- receptors found on taste buds.
- Food / liquid molecules activate different receptors
Sweet (G-protein receptor) -
Sour (ion-gated receptor) – based on H+ ions
Salty (ion-gated receptor) – based on Na+
Bitter (G-protein receptor) – can be toxins
Umami (G-protein receptor) - based on glutamate - pronounced “oo-MAH-mee”
Fig 7.5
Smell (olfaction)
Special Senses and Their Receptors:
• Olfactory receptor neurons on epithelium of upper nasal cavity.
• Odor molecules bind to receptor
• Axons of olfactory neurons form olfactory nerve (Cranial nerve 1)
• Signal to olfactory cortex (temporal lobe)
Fig 7.6

9/14/2016
12
Vision
Special Senses and Their Receptors:
• Light enters pupil •Light bends passing through lens •Light focuses on retina (sensory area with photoreceptors: rods & cones)
• photoreceptors depolarize (form AP) & release glutamate to “bipolar cells” •At retina, image is upside-down & reversed (visual cortex fixes this later) • Retina merges w/optic disk & optic nerve
Vision
• If image on retina not focused, lens changes shape using ciliary muscle (called “accomodation”).
• Relaxation of ciliary muscle = lens gets thinner, to view something far. • Contraction of ciliary muscle = lens gets thicker, to view something close.
Fig. 7-24
Ciliary muscle
lens
9/14/2016
13
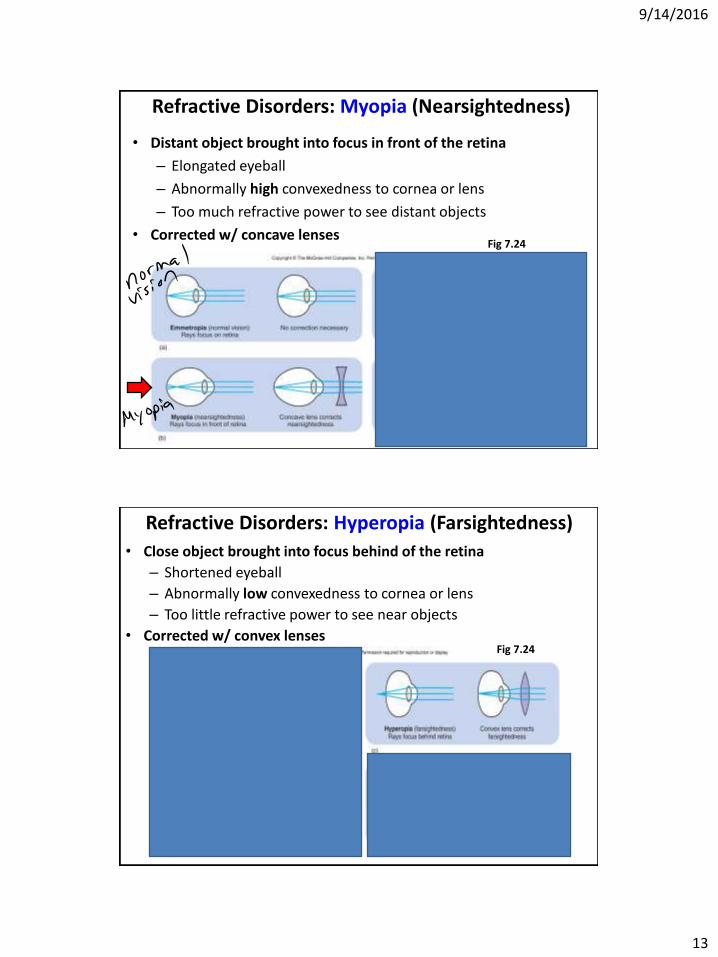
Refractive Disorders: Myopia (Nearsightedness)
• Distant object brought into focus in front of the retina
– Elongated eyeball
– Abnormally high convexedness to cornea or lens
– Too much refractive power to see distant objects
• Corrected w/ concave lenses Fig 7.24
Refractive Disorders: Hyperopia (Farsightedness)
• Close object brought into focus behind of the retina
– Shortened eyeball
– Abnormally low convexedness to cornea or lens
– Too little refractive power to see near objects
• Corrected w/ convex lenses Fig 7.24
9/14/2016
14
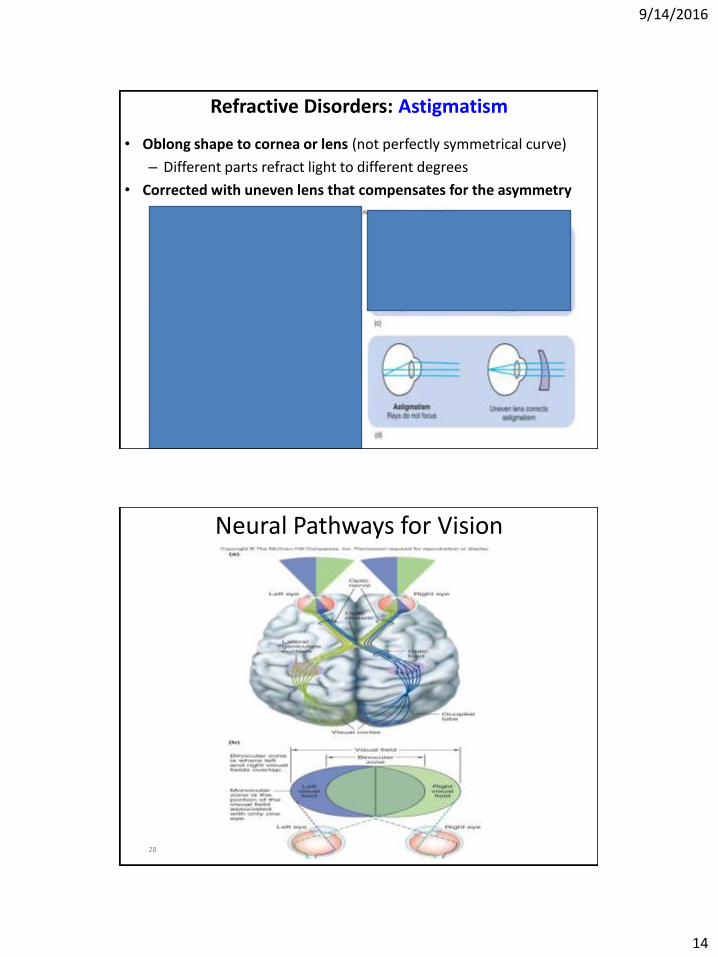
Refractive Disorders: Astigmatism
• Oblong shape to cornea or lens (not perfectly symmetrical curve)
– Different parts refract light to different degrees
• Corrected with uneven lens that compensates for the asymmetry
28
Neural Pathways for Vision

9/14/2016
15
Retinal Cells
• Photoreceptors
–rods and cones
• Bipolar cells
–Neurons that receive neurotransmitter from photoreceptors
–Synapse with ganglion cells
• Ganglion cells
–Neurons that receive neurotransmitter from the bipolar cells
–Conduct APs to CNS (visual cortex of occipital lobe) by the optic nerve.
Photoreceptors • Rods
– More numerous than cones
– Cannot distinguish different colors • Highly sensitive to light
(low light levels detected)
• Low visual acuity (image not as sharp)
• Cones – Found mainly in fovea centralis
– Can distinguish among colors • Low light sensitivity (need more
light to see with cones)
• High acuity (image is sharper)
9/14/2016
16
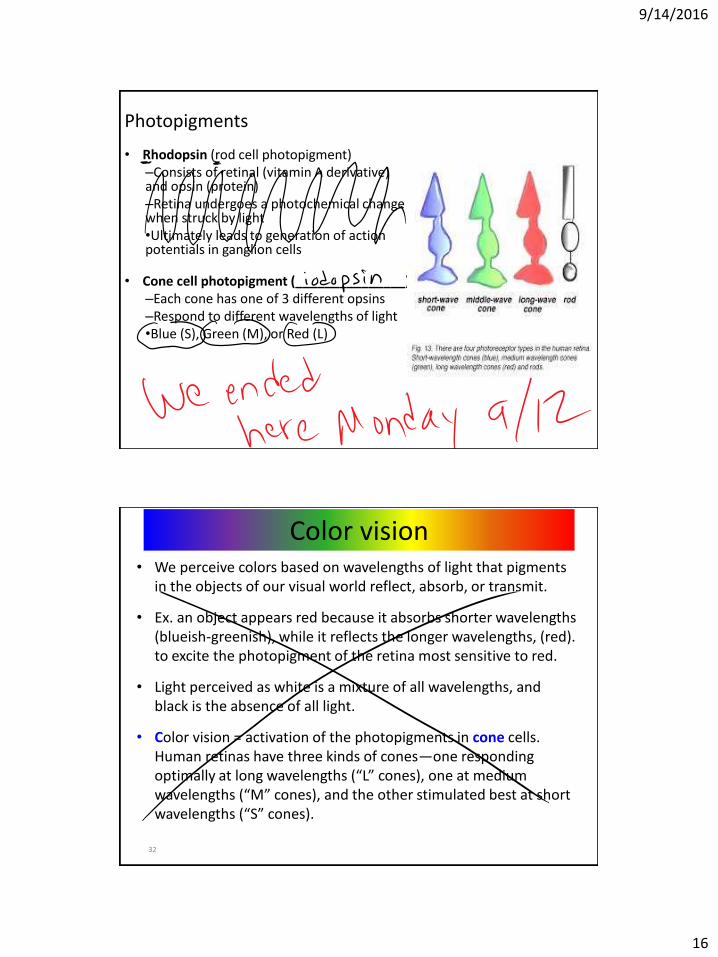
Photopigments
• Rhodopsin (rod cell photopigment) –Consists of retinal (vitamin A derivative) and opsin (protein) –Retina undergoes a photochemical change when struck by light •Ultimately leads to generation of action potentials in ganglion cells
• Cone cell photopigment (_______________) –Each cone has one of 3 different opsins –Respond to different wavelengths of light •Blue (S), Green (M), or Red (L)
32
• We perceive colors based on wavelengths of light that pigments in the objects of our visual world reflect, absorb, or transmit.
• Ex. an object appears red because it absorbs shorter wavelengths (blueish-greenish), while it reflects the longer wavelengths, (red). to excite the photopigment of the retina most sensitive to red.
• Light perceived as white is a mixture of all wavelengths, and black is the absence of all light.
• Color vision = activation of the photopigments in cone cells. Human retinas have three kinds of cones—one responding optimally at long wavelengths (“L” cones), one at medium wavelengths (“M” cones), and the other stimulated best at short wavelengths (“S” cones).
Color vision

9/14/2016
17
33
Color vision
34
• Although each type of cone is excited most effectively by light of one particular wavelength, there is actually a range of wavelengths within which a response will occur.
• Our ability to discriminate color also depends on the intensity of light striking the retina. In brightly lit conditions, the differential response of the cones allows for good color vision. In dim light, however, only the highly sensitive rods are able to respond.
• Though rods are activated over a range of wavelengths that overlap with those that activate the cones, there is no mechanism for distinguishing between frequencies. Thus, objects that appear vividly colored in bright daylight are perceived in shades of gray at night.
Color vision

9/14/2016
18
“Afterimage” or bleaching of photopigments
Black and white afterimage: After viewing black & white image any length of time (~30 seconds), then replace with a white field, see afterimage of the negative of the image that is seen earlier. Color afterimage: After viewing color image ~30 sec, then view white field, image replaced by the complementary color.

9/14/2016
19
Did it look like this?

9/14/2016
20
9/14/2016
21
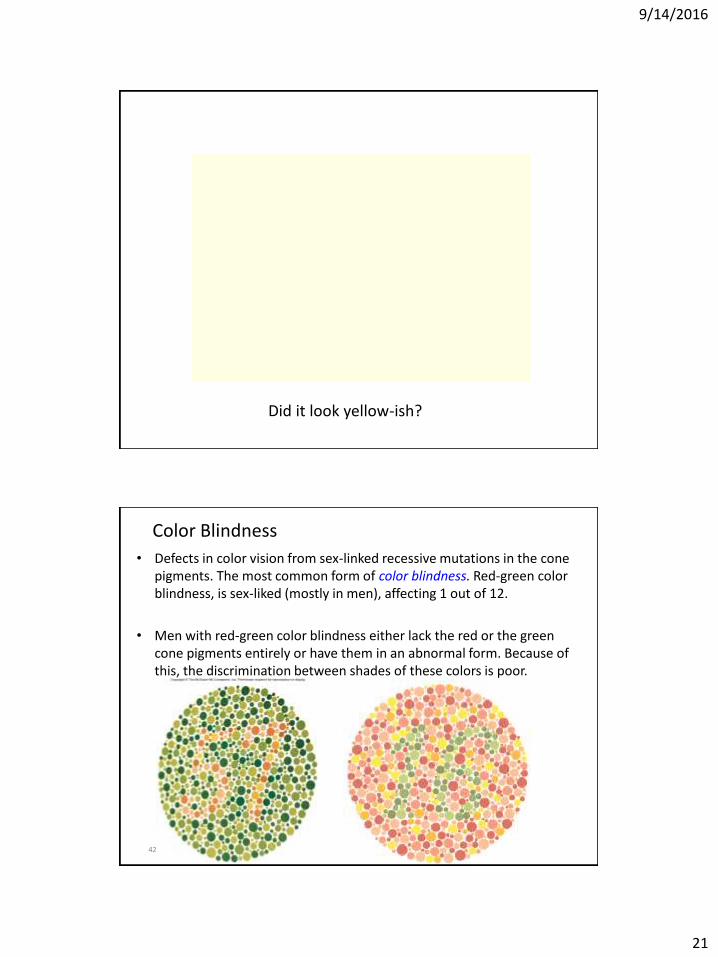
Did it look yellow-ish?
42
Color Blindness
• Defects in color vision from sex-linked recessive mutations in the cone pigments. The most common form of color blindness. Red-green color blindness, is sex-liked (mostly in men), affecting 1 out of 12.
• Men with red-green color blindness either lack the red or the green cone pigments entirely or have them in an abnormal form. Because of this, the discrimination between shades of these colors is poor.

9/14/2016
22
43
Macular Degeneration • The macula lutea = specialized
region of the retina for visual acuity.
• Macular degeneration = defect in this region causing loss of vision in the center of the visual field.
• The most common form of this disease increases with age, occurring in approximately 30% of individuals over the age of 75, and referred to as age-related macular degeneration (AMD).
Review Ear anatomy
– Outer Ear
> Pinna or auricle > External auditory canal > Tympanic membrane (vibrates when struck by sound waves)
Hearing (auditory)
Special Senses and Their Receptors:
Tympanic membrane Fig 7.13

9/14/2016
23
Middle Ear has auditory ossicles: > malleus – near tympanic membrane > incus > stapes – connect to oval window These ossicles
conduct vibration from tympanum to oval window.
Oval window
Vestibular duct (perilymph)
Cochlear duct (endolymph)
Tympanic membrane
Hearing (auditory)
Cochlear branch of Vestibulo-cochlear nerve
Oval window
Vestibular duct (perilymph)
Cochlear duct (endolymph)
Inner Ear (fluid-filled bony labryinth) has:
1. Cochlea (Organ of Corti) – for hearing
2. Otolith organs & Semicircular Canals - for balance (cover later) Cochlea
Tympanic membrane
Hearing (auditory)
Cochlear branch of Vestibulo-cochlear nerve

9/14/2016
24
1. Cochlea (Organ of Corti) for hearing
oval window vibrations travel through “perilymph” & vibrate basilar membrane moves “endolymph” (fluid) in cochlea bends stereocilia on hair cells of cochlear basilar membrane, release neurotransmitter
Oval window
Vestibular duct (perilymph)
Cochlear duct (endolymph)
Basilar membrane
Hearing (auditory)
Cochlear branch of Vestibulo-cochlear nerve
Oval window
Basilar membrane
AP
Vestibulo-cochlear nerve
bends stereocilia on hair cells of cochlear basilar membrane, releases neurotransmitter (glutamate)
Cochlear HAIR CELL

9/14/2016
25
1. has Cochlea (Organ of Corti) for hearing
oval window vibrations travel through “perilymph” & vibrate basilar membrane “endolymph” (fluid) in cochlea (Organ of Corti) bends hair cells on basilar membrane, release neurotransmitter which cause AP in sensory neurons (cochlear branch of vestibulocochlear nerve ) > Signal goes to auditory cortex (temporal lobe) > Brain perceives sound Louder sounds cause more vibrations
Oval window
Vestibular duct (perilymph)
Cochlear duct (endolymph)
Basilar membrane
Hearing (auditory)
Cochlear branch of Vestibulo-cochlear nerve
2 (3) types of Hearing Loss
1. Conduction deafness (read Clinical App Pg 183 & ONLINE) External or middle ear problem Can be helped by hearing aids, which amplify sound waves Many possible causes:
• Cerumen = • Otitis media =
• otosclerosis = hereditary disorder causing progressive deafness due to
overgrowth of bone in the inner ear.
2. Sensory deafness Most common: gradual loss of receptor (hair) cells Or interuption in sound wave conduction between cochlea to auditory cortex
Need cochlear implant
3. Central Not common - damage to ascending neural pathways
Hearing (auditory)

9/14/2016
26
Semicircular canals
Fig 7.13
Balance (vestibular apparatus) Inner Ear (bony labryinth)
1. Cochlea (Organ of Corti)
2. Otolith organs & Semicircular Canals
Balance (vestibular apparatus) Otolith organs (utricle & saccule) have sensory receptors (stereocilia on maculae) that bend with linear movement and head position.
Semicircular canals have ampulla with sensory receptors (stereocilia) for rotational acceleration
Equilibrium also interpreted with input from vision & stretch receptors in muscle

9/14/2016
27
Balance (vestibular apparatus)
Otolith organs (utricle & saccule) have sensory receptors (stereocilia on maculae) that bend with linear movement and head position.
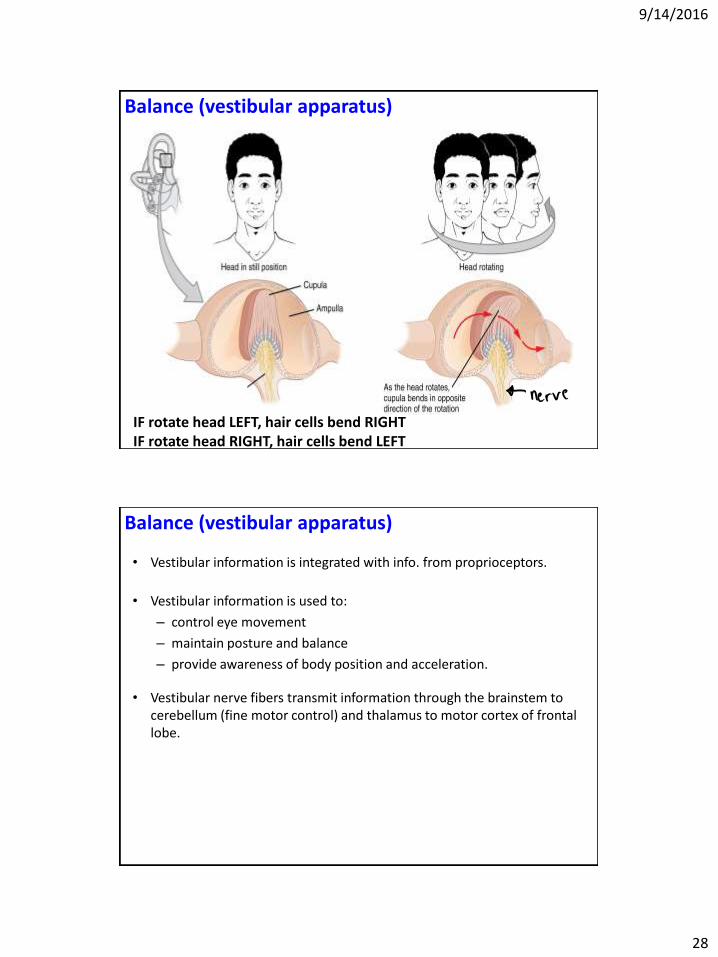
Balance (vestibular apparatus) Fluid-filled Semicircular canals have ampullae with sensory receptors (hair cells with stereocilia) that bend with head rotation. when rotate head, stereocilia of hair cells bend an AP forms, release neurotransmitter, which stimulates vestibular branch of vestibulocochlear nerve.
9/14/2016
28
Balance (vestibular apparatus)
IF rotate head LEFT, hair cells bend RIGHT IF rotate head RIGHT, hair cells bend LEFT
• Vestibular information is integrated with info. from proprioceptors.
• Vestibular information is used to:
– control eye movement
– maintain posture and balance
– provide awareness of body position and acceleration.
• Vestibular nerve fibers transmit information through the brainstem to cerebellum (fine motor control) and thalamus to motor cortex of frontal lobe.
Balance (vestibular apparatus)

9/14/2016
29
Balance (vestibular apparatus)
Cerebellar ataxia – read Clinical App Pg 138 = lack of coordination due to cerebellar damage - Info from vestibular apparatus ascends to cerebellum - Cerebrum needed for fine motor control - Damage leads to errors in speed, force, & direction of movement - Person might move as if drunk (they’re not) - Might reach to grab an object & miss - Might show “intension tremors” (when trying to perform a task,
limb trembles near completion of movement)
https://www.youtube.com/watch?v=5eBwn22Bnio
Balance (vestibular apparatus)
“Vestibular Nystagmus” (vestibulo-ocular reflex) = as your head rotates in a body spin, then stop suddenly, your eyes slowly drift in opposite direction of spin, then eyes dart back to center. This due to fluid in semicircular canals still moving. Continues until fluid stops moving.
https://youtu.be/JaCpG0n6Jas

9/14/2016
30
Review • Taste perception
• Smell perception
• Vision
• Hearing - causes of deafness
• Balance – Vestibular Nystagmus (vestibulo-ocular reflex)
– Cerebellar ataxia
59