Embed Size (px)
Citation preview

C H A P T E Rz z z z z z z z z z z z z z z z z z z z z z z z z z z30
Thoracic and Upper Lumbar SpineInjuriesThoracic and Upper Lumbar SpineInjuries
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Mark A. Prevost, M.D.Robert A. McGuire, M.D.Steven R. Garfin, M.D.Frank J. Eismont, M.D.
The primary goals in providing care for patients who havesustained thoracolumbar spinal trauma must includepreservation of life and protection of neurologic function,in addition to restoration and maintenance of alignmentand stability of the spine. Upholding these goals whilemanaging thoracolumbar fractures is both challenging andcontroversial to the spinal surgeon. Many times the bottomline is whether the spine can function as a load-bearingcolumn. If it can, is an orthosis necessary? If not, canstability and alignment be restored with surgical interven-tion? Each of these objectives is best accomplished whenthe treating physician understands the anatomy of thespinal column, appreciates the biomechanics of the injuryand instability, and has an awareness of the expandingtreatment options available for the care of a spine-injuredpatient.104, 105
HISTORICAL BACKGROUNDz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
For physicians taking care of patients with spinal injuries,it is helpful to gain perspective regarding diagnosis andtreatment of these injuries as they have evolved throughtime.
The earliest written record of spinal cord injury is foundin the Edwin Smith Papyrus (3000 BC).35 Later, Egyptianphysicians noted that patients with vertebral trauma oftenhad paralysis of the arms and legs and urinary inconti-nence, thus suggesting an association among vertebralinjuries, spinal cord damage, and loss of function.
Celsus made the next important contribution to thedescription of spinal cord trauma when he distinguishedcervical from thoracolumbar spinal cord injuries. Hereported that fractures of the cervical spine producedrespiratory embarrassment and vomiting whereas traumato the lower portion of the spinal column produced
paralysis of the lower extremities and urinary inconti-nence. He also expanded on Hippocrates’ concept ofmanual extension for reduction of spinal deformities.35
In the 16th century, Ambroise Pare readdressed theproblem of spinal injury.25, 118 He accurately described thesymptoms of cord compression as follows:
Amongst the symptoms are the stupidity, or numbnessor palsy of the arms, legs, fundament and bladder,which take away their sense and motion, so that theirurine and excrements come from them against theirwills and knowledge, or else are wholly suppressed.Which when they happen saith Hippocrates, you mayforetell that death is at hand, by reason that the spinalmarrow is hurt. . . . Having made such a prognostica-tion, you may make an incision so to take forth thesplinters of the broken vertebrae, which driven in pressthe spinal marrow in the nerves thereof.
Modern management of vertebral column traumaarrived with the development of anesthesia and radiogra-phy. In the 1920s, based heavily on principles advocatedby Guttman, emphasis in the treatment of vertebral traumawas placed on closed reduction of fractures.117 Davisproposed a method of reduction in which the patient wasanesthetized and placed in the prone position. Anoverhead pulley suspension raised the lower limbs andproduced marked hyperextension. The physician thenmade a manual thrust over the fractured vertebra in anattempt to realign the fracture. When reduction wasachieved, the patient was immobilized in a plaster jacket.In 1931, Watson-Jones modified this technique by usingtables of different height to hyperextend the spine andobtain reduction.269
Internal fixation of thoracic and lumbar spinal fracturesbegan after the Second World War with the developmentof spinous process plating for unstable fractures.133, 135
875
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 1/69 P 875 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 1/69 P 875 BLACK T

Later, Harrington revolutionized spinal care and rehabili-tation with the introduction of his posterior spinalinstrumentation devices.66 Since then, surgical techniquesand instruments have proliferated and have continued toimprove the ability to anatomically reduce and internallystabilize the injured spinal column.* Neurologic recovery,however, has remained unchanged or only slightly im-proved over the results obtained with postural reductionand nonoperative care.18, 32, 49, 66, 95, 139, 151, 192 At thistime, the major predictable benefits of internal fixation ofspinal fractures are decreased hospital stay, early rehabili-tation, and prevention of deformity.49 However, rootfunction and, in properly selected patients, spinal cordfunction can be dramatically altered and improved withappropriate surgery and stabilization.
ANATOMYz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
The thoracolumbar spine is characterized by a dynamicand complex interaction between the bony vertebralelements, discs, and interconnecting ligaments. It wouldbe impossible to make sound diagnostic and therapeuticdecisions regarding thoracolumbar trauma without a solidunderstanding of this anatomy.
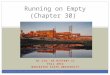
The human spine has 12 thoracic and 5 lumbarvertebrae with interspaced intervertebral discs. Stagnaraand associates studied spinal alignment in healthy personsaged 20 to 29 years without back complaints.259 Widevariation was noted in this healthy population, the range ofthoracic kyphosis being 7° to 63°, with 91% between 18°and 51° (Fig. 30–1A). In the thoracic spine, thisconfiguration is maintained by the wedge-shaped vertebralbodies and discs, which are larger posteriorly thananteriorly. Across the thoracolumbar junction (T10–L2),where most injuries occur, the normal range is reported tobe 0° to 10° kyphosis. In the lumbar spine, the averagelordosis in this same group of normal people was 50°, witha range of 32° to 84°; 92% of these individuals hadbetween 42° and 74° of lordosis259 (see Fig. 32–1B). In thelumbar spine, the discs have an increased height anteriorly,which helps create this lordosis.
White and Panjabi investigated the types of motionpresent throughout the spine273 (Fig. 30–2). The thoracicspine has significantly less flexion-extension motion thanthe cervical or lumbar spines. In the cervical spine fromthe occiput to C7, the average motion between flexion andextension is 13° per level, with a range of 8° to 17°. AtC7–T1 this motion decreases to 9°, and in the thoracicspine from T1 to T6, each level has only 4° of totalflexion-extension motion. From the T6–T7 to the T12–L1levels, flexion-extension motion gradually increases from5° to 12°, in contrast to the average 15° flexion-extensionmotion at each lumbar level (range of 12° to 20°).
The thoracic spine is less capable of bending laterallythan the cervical spine. Lateral bending in the cervicalspine from occiput to C7 averages 8° per level, whereas it
is only about 6° per level from T1 to T10. At the area of theT10–L1 thoracolumbar junction, lateral bending increasesto an average of 8° per level. In the lumbar spine, thismotion decreases to about 6° per level. Much of thethoracic-level rigidity is related to the presence of the ribcage and the costovertebral articulations.216
Axial rotation in the thoracic spine averages 8° from T1to T8 but decreases to approximately 2° per level belowT10. Axial rotation is greater in the thoracic spine than inthe lumbar spine because the facets are aligned in thecoronal plane, as opposed to the more sagittal alignmentthat occurs in the lumbar spine (Fig. 30–3). The transitionregion for facet orientation is the area from T10 to T12.Because of this alteration in facet orientation, the motioncharacteristics of the lower thoracic spine more closelyresemble those of the lumbar spine. In the lumbar spine,the facet joints gradually attain an almost true sagittalorientation at the L4–L5 level. Such alignment providessignificant restriction to rotation and side bending.
The thoracolumbar junction is more susceptible toinjury than are other adjacent portions of the spine.Approximately 50% of all vertebral body fractures and40% of all spinal cord injuries occur from T11 to L2. Thisgreater susceptibility to injury can be explained by thedecrease in rib restraint, changes in stiffness for flexion-extension and rotation, and changes in disc size and shape,which occur relatively acutely in the transitional areabetween the upper thoracic and the midlumbar spine.
The conus medullaris usually begins at T11 and, inmost males, ends at the L1–L2 disc space. The conus infemales frequently stops slightly more proximally. Theconus medullaris can occasionally extend much lower intothe lumbar spine and is often associated with a hypertro-phic filum terminale. The neural elements of the lumbarspine below the L1–L2 disc are usually purely spinal nerverootlets (cauda equina). In addition, an extensive collateralcirculation is located distal to the nerve roots and proximalto the spinal cord, thus making this region less prone tovascular compromise and more likely to recover from aspinal cord injury.218 The thoracic spinal cord hasrelatively poor vascularity and limited collateral circulationwhen compared with the cervical spinal cord and theconus medullaris. Adamkiewicz in 1882 described theblood supply of the spinal cord, including a relativelyconstant medullary artery known as the great medullaryartery or the artery of Adamkiewicz. This artery may beinjured as a result of trauma or thoracic disc herniation orfrom one of the lateral or posterolateral extracavitaryapproaches. Injury to this artery may cause seriousischemic insult to the cord and lead to paralysis. In mostpeople, the artery of Adamkiewicz originates from theintercostal artery on the left side between T10 andT12, where it joins the nerve root sleeve and becomesintradural. The artery then crosses one to three disc spaces,at which point it anastomoses with the anterior spinalartery. Knowledge of this artery and its course is importantduring certain approaches and may explain certainneurologic deficits that may not recover despite adequateanterior decompression.184
The spinal canal in the midthoracic region is consider-ably narrower than in the cervical or lumbar region.86, 237
At the T6 level, the spinal canal has a circular configura-
*See references 8, 22, 23, 27, 51, 63, 64, 76, 80, 87, 93, 107, 131,140, 149, 160, 181–183, 185, 186, 197, 207, 212, 243–245, 262, 264,276, 284.
876 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 2/69 P 876 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 2/69 P 876 BLACK T

tion with a 16-mm diameter. In the middle to lowercervical spine, the canal is 23 × 14 mm, and in thelumbosacral region, it is 26 × 17 mm.183 The small size ofthe thoracic spinal canal must be appreciated for tworeasons. First, because less space is available, even minorspinal column displacement may produce significantspinal cord compression. Second, when consideringreconstruction of the spine, many systems use sublaminarfixation within this already narrowed region of the spinalcanal. Therefore, the patient’s specific injuries, the avail-ability of fixation devices, and spinal anatomy must be
taken into account when selecting instrument shape andsize.
As Dommisse and others have shown, in the thoracicspine the free space between the spinal cord and theborders of the spinal canal is relatively minimal.69
Although the thoracic cord tends to be smaller than thecervical and lumbar enlargements, the free space alsonarrows. In addition and of significance with regard tospinal trauma, the blood supply in the middle and lowerthoracic spine is less abundant than elsewhere in the spinalcord. Adding to the variability is the location of the conus
25.24.23.22.21.20.19.18.17.16.15.14.13.12.11.10. 9.8.7.6. 5.4.3.2.1.
A 7 62
1 2 1 3 4 5 6 7 8 9 10 11 121
12°5 18° 23°5 29° 34°5 40° 45°5 51° 56°5
16
2322
13
30.29.28.27.26.25.24.23.22.21.20.19.18.17.16.15.14.13.12.11.10. 9.8.7.6. 5.4.3.2.1.
A 18 66
1 32 4 5 6 7 8 9 10 11 12
22°8 27°6 32°4 37°2 42° 46°8 51°6 56°4 61°2
16
29
17
2
5
10
7
23
2
8
17
5
1
A
B
FIGURE 30–1. A, Distribution of thoracic kyphosis in 100French people, 43 women and 57 men. B, Distribution oflumbar lordosis in the same group of 100 French people.(A, B, Data from Stagnara, P.; et al. Spine 7:335–342,1982.)
877CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 3/69 P 877 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 3/69 P 877 BLACK T

A B
T12-L1
C D
T5-6
FIGURE 30–3. Rotation in the midthoracic spine andat the thoracolumbar junction. A, The rotation atT5–T6 is represented by the arrow between thespinous processes. The inset shows how the laminaof T5 glides over the posterior elements of T6 withno resistance to rotation. B, After facetectomy, themotion present between T5 and T6 (arrow) isunchanged from A. C, The rotation present betweenT12 and L1 is represented by the arrow between thespinous processes. Because of the sagittal orientationof the facets (inset), rotation is markedly restricted.D, After bilateral facetectomy, motion between T12and L1 (arrow) is markedly increased. The restric-tion from the sagittally oriented facets has beeneliminated.
AXIAL ROTATIONLATERAL BENDINGFLEXION—EXTENSION
0 5 10 0 5 10 0 5 10 15 20
CE
RV
ICA
LT
HO
RA
CIC
LUM
BA
R
DEGREES
Oc—C1
C2—3
C4—5
C6—7C7—T1
T1—2
T3—4
T5—6
T7—8
T9—10
T11—12 T12—L1
L1—2
L3—4
L5—S1
0° 0°
/ /47°
FIGURE 30–2. The motion present ateach level of the spine. (Data frommultiple reviews and from the exper-imental work of White, A.; Panjabi,M. Spine 3:12–20, 1978.)
878 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 4/69 P 878 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 4/69 P 878 BLACK T

medullaris, with terminations in the general populationfollowing almost a bell-shaped curve from the T12 to theL3 level.69
The cord is usually wider in the lateral plane than in theanterior-to-posterior direction. Elliott demonstrated thatthe largest diameter of the cervical enlargement, which is atapproximately C5–C6, was 13.2 mm in the lateral planeand 7.7 mm from anterior to posterior. In the thoracicregion, the smallest measurements were 8 mm laterally and6.5 mm from anterior to posterior, and the lumbosacralenlargement was 9.6 and 8.0 mm, respectively.86 Thesedimensions can be correlated with the space availablewithin the spinal canal. Aebi and Thalgott demonstratedthat the largest area (i.e., the space available in the cervicalcanal) was 24.5 mm laterally and 14.7 mm from anterior toposterior in the thoracic region, thus correlating with thesmall size of the spinal cord at this location.4 The largestspace available was 17.2 mm in the lateral plane and 16.8mm anterior to posterior. At the level of the lumbarenlargement, it was 23.4 mm laterally and 17.4 mm fromanterior to posterior. In general, the cord occupies approx-imately half the space available in each direction. In thethoracic spine, according to Dommisse, the anterior-to-posterior diameter of the spinal canal changes minimally; itaverages approximately 13 mm throughout but increases to15 mm in the lower thoracic spine.69 His measurements ofinterpedicular distance (lateral measurement) averagedabout 15 mm at the smallest point (approximately T6) andincreased to 17 mm at T10–T11.
The morphometry of the pedicles of the thoracic andlumbar spines varies considerably from level to level, aswell as from patient to patient.24, 166, 246, 267, 285 Zindrickand colleagues,286 in an evaluation of 2900 pedicles,determined pedicle isthmus widths and pedicle angles inthe sagittal and transverse planes. In general, pedicleisthmus widths were significantly smaller in the thoracicspine than in the lumbar spine (Fig. 30–4A and B). Thepedicle angles in the transverse plane varied from 27°medial inclination (in a posterior-to-anterior direction) inthe proximal thoracic spine to approximately 1° at T11and −4° at T12. At L1, the angle again inclines medially at11° and gradually increases to approximately 30° at L5(see Fig. 32–4C). In an anatomic study investigating theinternal architecture of thoracic pedicles, Kothe andassociates showed that the medial wall is two to three timesthicker than the lateral wall. This difference in thicknesscould explain the fact that most pedicle fractures related topedicle screw insertion occur laterally.162 An understand-ing of these dimensions and angles is important whenconsidering the use of pedicle screw fixation systems tostabilize thoracic and thoracolumbar spinal injuries.
The flexion axis of the normal thoracic spine and thethoracolumbar junction occurs at the middle to posteriorthird junction of the vertebral body.235, 275 This location ofthe axis results in an anterior compressive force momentarm that is approximately one fourth the length of theposterior tensile force.257 Brown and colleagues in 1957demonstrated that posterior elements fail under tension atapproximately 400 lb.37 This amount of posterior forcecorresponds to a resultant anterior compressive forceof approximately 1200 to 1600 lb. Comprehension ofthis biomechanical principle is essential to gain an
understanding of spinal stability (described later). In thethoracic spine, the human body’s center of gravity isanterior to the spine. As a result, the resting condition inthe thoracic spine and at the thoracolumbar junction is one
25
20
15
10
5
0L5 T9L4 L3 L2 L1 T T T8 T7 T6 T5 T4 T3 T2 T1T
12 11
Spinal level
Tran
sver
se w
idth
(mm
)
A
L5 T9L4 L3 L2 L1 T T T8 T7 T6 T5 T4 T3 T2 T1T
Spinal levelB
20
10
18
16
14
12
8
6
Sag
ittal
wid
th (m
m)
L5 T9L4 L3 L2 L1 T T T8 T7 T6 T5 T4 T3 T2 T1T
Spinal level
40353025201510
505
1015
C
Tran
sver
se a
ngle
(deg
)
10
12 11 10
�
�
�
12 11 10
FIGURE 30–4. Analysis of the morphometric characteristics of the thoracicand lumbar pedicles. A, The transverse width of the pedicle at each levelof the thoracic and lumbar spine is shown. The average pedicle width ofthe lumbar spine ranges from 9 to 18 mm. In the thoracic spine, allpedicles are smaller than 9 mm. B, The longitudinal pedicle width of eachlevel in the thoracic and lumbar spine is represented. It peaks at 17 mmat the T11 vertebra and decreases to 10 mm at T1 and to 14 mm at L5.C, The transverse angle of the pedicles for each level of the thoracic andlumbar spine is shown. The angle is −4° at the T12 vertebra and increasesto 30° at L5 and to 27° at T1. (A–C, Redrawn from Zindrick, M.R.; et al.Spine 12:160–166, 1987.)
879CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 5/69 P 879 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 5/69 P 879 BLACK T

of vertebral body compression and posterior ligamentouscomplex tension. In the thoracic spine, the ribs anterior tothe spinal column and the thick ligaments posteriorly,acting in tension, restrict any further forward flexion in thenormal situation.234 In the lumbar spine, particularly in themore lordotic lower lumbar spine, the center of gravity islocated more posteriorly, and the posterior elements pro-vide approximately 30% of the weight-bearing support.These considerations are important for realignment or formaintenance of alignment after spinal injury.216, 252, 273
One of the important components of thoracolumbarspinal anatomy is the soft tissue that interconnects thebony elements. The complex interaction of ligaments, disc,and musculature allows for both controlled motion andstability of the spine. Trauma to the soft tissues of thethoracolumbar spine can have profound effects on func-tion and stability.
The anterior longitudinal ligament is a strong, broad-based ligament that runs on the anterior aspect of thevertebral body from the atlas to the sacrum. It is firmlyattached to both the ventral aspect of the disc and theperiosteum of the vertebral body. It is a major contributorto spinal stability and limits hyperextension of thevertebral column. The posterior longitudinal ligament alsoruns the length of the spinal column, but it is narrower andweaker than its anterior counterpart. Its primary functionis to limit hyperflexion. The intervertebral disc is com-posed of the anulus fibrosus and the nucleus pulposus.The anulus is formed by concentric bands of fibrocartilagethat run obliquely from one vertebral body to another.This arrangement allows for some motion, yet is one of thestrongest connections between vertebral segments. Thenucleus, which is encased in the anulus, acts as a shockabsorber for axial forces. Of importance in thoracolumbartrauma is that the disc is essentially an avascular structurethat relies on passive diffusion through the end-plates andperipheral aspect of the anulus for nutrition. When thisstructure is disrupted, the potential for healing is limited.
Posteriorly, the lamina are joined by the ligamentumflavum, a broad band of elastic fiber. The spinousprocesses are joined by a weak interspinous ligament anda strong supraspinous ligament. The intrinsic muscles ofthe back include the erector spinae group of muscles(spinalis, longissimus, iliocostalis) and the transversospi-nalis group (rotatores, multifidus, semispinalis). Theintrinsic muscles maintain posture and provide movementof the vertebral column. Any deformity resulting fromtrauma can alter the function of these muscles. In addition,it is important to have an understanding of these musclegroups when considering the various anatomic approachesto the spine described later in this chapter.
MECHANISMS OF INJURYz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Frequently, many complex forces occur at the time ofinjury, each of which has the potential to producestructural damage to the spine.119 Most often, however,one or two forces account for most of the bone orligamentous injuries encountered. The forces most com-monly associated with thoracic, thoracolumbar, and lum-bar spine injuries are axial compression, flexion, lateral
compression, flexion-rotation, shear, flexion-distraction,and extension. Each is discussed from a mechanicalviewpoint, and their effect on the bone-disc-ligamentcomplex of the spine is described.
Axial Compression
Because of the normal thoracic kyphosis, axial loading inthis area usually results in an anterior flexion load on thevertebral body. The resultant spine injuries are discussedunder Flexion.
An axial load in the straight thoracolumbar region (Fig.30–5) often results in pure compressive loading of thevertebral body.156 As described by Roaf, this mechanism
FIGURE 30–5. Axial compression across the straight thoracolumbar regionresults in pure compressive loading of the vertebral body and most oftencauses a thoracolumbar burst fracture.
880 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 6/69 P 880 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 6/69 P 880 BLACK T

produces end-plate failure, followed by vertebral bodycompression.235 With sufficient force, vertical fracturesdevelop through the vertebral body and produce a burstfracture21, 62, 157, 209 (Fig. 30–6). Frederickson and co-workers observed that this fracture then propagatesthrough the midportion of the posterior cortex ofthe vertebral body through the vascular foramina.99
With further loading, centripetal displacement of thebone occurs, frequently with disc fragmentation andposterior disruption. This centripetal force can producefractures at the pedicle-body junction and result inwidening of the interpedicular distance and, particularlyif a flexion component is present, a greenstick fractureof the lamina (see Fig. 30–6). With severe compres-sion, significant disruption of the posterior element mayoccur.
Heggeness and Doherty studied the trabecular anatomyof the thoracolumbar vertebrae and documented a trabec-ular framework that originates from the medial corner ofthe base of the pedicle and extends in a radial fashionthroughout the vertebral body, with thinning of thevertebral cortex near the base of the pedicle at the site of
origin of this trabecular array. Such anatomy may producea site of stress concentration and may explain thetrapezoidal shape of the bony fragments that are frequentlyretropulsed into the spinal canal in burst-type fracturescaused by an axial load130 (Fig. 30–7).
Flexion
Flexion forces (Fig. 30–8) cause compression anteriorlyalong the vertebral bodies and discs, with tensile forcesdeveloped posteriorly. The posterior ligaments may nottear, particularly with rapid loading rates, but posterioravulsion fractures may develop.235 Anteriorly, as the bonefractures and angulation increase, the force is dissipated.With intact posterior ligaments, a stable fracture patternmost often results. Frequently, the middle column remainsintact with no subluxation or retropulsion of bone or discfragments (Fig. 30–9). However, with disrupted poster-ior ligaments and facet capsules, instability may oc-cur.58, 133, 150, 195, 196, 211 If the anterior wedging exceeds40% to 50%, posterior ligamentous and facet joint failure
FIGURE 30–6. A 21-year-old man involved in a motor vehicle accident sustained a burst fracture of L1 and L3. The patient had an incomplete spinal cordinjury. A, A preoperative lateral view shows loss of height predominately at L1. B, A sagittal-cut magnetic resonance image shows compression at bothL1 and L3. C, An axial-cut computed tomographic (CT) scan at L3 shows a retropulsed fragment filling half the canal. D, An axial CT scan at L1 showsa fracture of the lamina and retropulsion of a fragment into canal. E, This injury was stabilized with ISOLA instrumentation combining both pedicle screwsand laminar hooks. Sagittal alignment was maintained. Note the use of a lamina hook at L4 to protect the pedicle screw at that level. F, Postoperativeanteroposterior radiograph showing a cross-connection added for additional stability.
881CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 7/69 P 881 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 7/69 P 881 BLACK T

can be assumed, and late instability with progressivedeformity may occur.271 Flexion-compression injurieswith concomitant middle element failure have a higherpotential for causing mechanical instability, progressivedeformity, and neurologic deficit.146
Lateral Compression
Lateral compression forces produce an injury similar to theanterior wedge compression injuries previously described,except that the force is applied laterally (Fig. 30–10).Lesions may be limited to vertebral body fractures, orassociated posterior ligamentous injury may occur92, 93
(Fig. 30–11). The former are usually stable injuries,whereas the latter may be chronically unstable and lead toprogressive pain and deformity.
Flexion-Rotation
A flexion-rotation injury pattern includes a combination offlexion and rotation forces (Fig. 30–12). As describedpreviously for pure flexion, the predominant injurypattern may be anterior bone disruption. However, asrotational forces increase, the ligaments127, 128, 215 andfacet capsules tend to fail, with subsequent disruption ofboth the anterior and posterior columns. A highly unstableinjury pattern frequently develops, with the posteriorligaments and joint capsules ruptured and the anterior discand vertebral body disrupted obliquely. This mechanismcan result in the classic slice fracture originally describedby Holdsworth.133
In contrast to the cervical spine, pure dislocations areuncommon in the thoracic or lumbar spine174 because ofthe size and orientation of the facets, which require
FIGURE 30–7. A, Line drawing of a coronal and sagittal section from a vertebral body illustrating the trabecular array. B, Computed tomographic imageof a burst injury with a typical trapezoidal-shaped fragment taking origin from the point in the posterior cortex where it thins abruptly. Also note thatthe trapezoidal shape of the fragment roughly parallels the direction of the trabecular arrays. (Line drawing from Heggeness, M.H.; Doherty, B.J. J Anat191:309–312, 1997.)
882 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 8/69 P 882 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 8/69 P 882 BLACK T

distraction in addition to flexion and rotation for disloca-tion to occur. With only a flexion-rotation mechanism ofinjury, fracture of the facets or other posterior elementswill occur more commonly and allow the spine todislocate139, 177, 261 (Fig. 30–13).
Flexion-Distraction
Flexion-distraction lesions were first demonstrated radio-graphically by Chance in 1948,44 but the mechanism ofthis so-called seat belt injury was not fully elucidated untillater.136, 150, 229, 239 In this injury pattern (Fig. 30–14), the
axis of flexion is moved anteriorly (usually toward theanterior abdominal wall), and the entire vertebral columnis subjected to large tensile forces. The bony vertebralelements, discs, and ligaments are torn or avulsed, notcrushed as typically occurs in most spinal injuries. Theseforces can produce a pure osseous lesion, a mixedosteoligamentous lesion, or a pure soft tissue (ligamentousor disc) injury.118 The pure osseous lesion, described byChance, involves a horizontal fracture beginning in thespinous process, progressing through the lamina, trans-verse processes, and pedicles, and extending into thevertebral body (Fig. 30–15). This pure osseous lesionusually occurs in the region of L1–L3, and even though itis acutely unstable, it has excellent potential for healingwith good long-term stability if alignment can be obtained.Combined osteoligamentous or pure soft tissue injuriesmost commonly occur from T12 to L2 and should beconsidered unstable with low spontaneous healing poten-tial (Figs. 30–16 and 30–17).
Flexion-distraction can cause a bilateral facet disloca-tion in the thoracic or thoracolumbar spine173 (see Fig.30–17). The ligaments, capsules, and disc are disrupted,but the anterior longitudinal ligament usually remainsintact; however, it is sometimes stripped off the anterioraspect of the caudal vertebra. If the axis of flexion is farenough anterior and the energy is sufficient, rupture of theanterior longitudinal ligament may occur and result in aseverely unstable injury.150, 256 Generally, this injury is apure distraction rather than a flexion-distraction injury. Ifthe axis of rotation is at the anterior border of the vertebralbodies, compression may occur. The locus of the axis ofrotation changes the nature of the injury.
Shear
A pure shear force (Fig. 30–18) was found by Roaf toproduce severe ligamentous disruption, similar to thecombination of flexion and rotation described previ-ously.235 This force can result in anterior, posterior, orlateral spondylolisthesis of the superior vertebral segmentson those inferior. Traumatic anterior spondylolisthesis ismost common and usually results in a complete spinalcord injury. Occasionally, concomitant fractures throughthe pars interarticularis may occur and result in anautolaminectomy with neural sparing.128 Shear is fre-quently combined with other mechanisms to causecomplex injuries.
Extension
Extension forces (Fig. 30–19) are created when the head orupper part of the trunk is thrust posteriorly; these forcesproduce an injury pattern that is the reverse of that seenwith pure flexion. Tension is applied anteriorly to thestrong anterior longitudinal ligaments and the anteriorportion of the anulus fibrosus, whereas compression forcesare transmitted to the posterior elements (Fig. 30–20).This mechanism may result in facet, lamina, and spinousprocess fractures.96 Avulsion fractures of the anteroinferiorportion of the vertebral bodies may occur, but they are not
FIGURE 30–8. Flexion forces are causing anterior compression of thevertebral bodies and discs and tension in the posterior elements. Thismechanism of injury usually results in a stable compression fracture ofthe vertebral body anteriorly, but as the force continues, posteriorligamentous disruption may occur.
883CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 9/69 P 883 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 9/69 P 883 BLACK T

pathognomonic of extension injuries, as previouslythought. Most of these injuries are stable unless significantretrolisthesis of the upper vertebral body on the lowervertebral body has occurred or they are combined withshear forces.38, 273 Denis and Burkus reported on ahyperextension injury pattern that they termed a lumber-jack fracture-dislocation.60 The mechanism of this injury isa falling mass, often timber, striking the midportion of thepatient’s back. The injury involves complete disruption ofthe anterior ligaments and is an extremely unstable injurypattern.
SPINAL STABILITYz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
The concept of thoracic, thoracolumbar, and lumbarstability after trauma continues to evolve.161 Work byNicoll211 and Holdsworth133 suggested that the posteriorligamentous complex was the major determinant of spinalstability. They considered fracture-dislocations and severeshear injuries with complete disruption of the posteriorligamentous complex to be highly unstable injuries andmost other injuries to be stable. Roaf biomechanicallyconfirmed that gross instability was produced by flexion-rotation forces and shear stress.235
Bedbrook disagreed with the importance given to theposterior ligamentous complex and believed that theanterior disc and vertebral body were the prime determi-nants of stability.18 He cited the lack of instability afterlaminectomy as an example of the relative importance ofthe anterior spinal elements, as opposed to the posteriorstructures, in providing stability.
These two concepts gradually merged into a two-column concept of spinal stability: an anterior weight-bearing column of vertebral bodies and discs and aposterior column of neural arches and ligaments resistingtension.153 It was believed that destruction of either of
these columns was enough to produce instability. Thismodel helped explain the chronic instability often seenafter spinal injuries, especially those that result in akyphotic deformity. However, it was unable to fully explainall cases of acute instability. Experiments had shown thatcomplete section of the posterior elements alone does notresult in acute instability with flexion, extension, rotation,or shear.216, 225, 230, 236 It was necessary to also section theposterior portion of the anterior column to produce acuteinstability, at least in flexion.
Further progress was made when Denis proposed histhree-column model of the spine (Fig. 30–21) to betterreconcile these clinical and biomechanical observations.58
In his classification system, the posterior column iscomposed of the posterior bony arch (including thespinous process, the lamina, the facets, and the pedicles)and the interconnecting posterior ligamentous structures(including the supraspinous ligament, interspinous liga-ment, ligamentum flavum, and facet joint capsules). Themiddle column is composed of the posterior aspects of thevertebral body, the posterior portion of the anulus fibrosus,and the posterior longitudinal ligament. The anteriorcolumn includes the anterior longitudinal ligament, theanterior portion of the anulus fibrosus, and the anteriorvertebral body. Though useful in helping define vertebralcolumn instability, this basic anatomic description of thesupport columns of the spine does not include the spinalcord and spinal nerves. The neural elements, althoughthey do not directly contribute to spinal stability, cannot beforgotten or ignored in stability considerations.138, 139
Denis reviewed his fracture classification system andproposed four categories based on the presence and type ofinstability.58 These categories were stable injuries, mechan-ical instability, neurologic instability, and mechanical andneurologic instability.
Stable injuries include minimal and moderate compres-sion fractures with an intact posterior column, whichprevents abnormal forward flexion. By definition, the
FIGURE 30–9. Radiographs and computed tomographic (CT) scans of a compression fracture in a 48-year-old woman involved in a motor vehicle accident.A, An anteroposterior radiograph of the thoracolumbar junction shows a slight irregularity of the superior end-plate of the body of L1 with minimalinterspinous widening between T12 and L1. B, A lateral radiograph shows loss of height anteriorly and preservation posteriorly at L1. C, A CT scan throughthe body of L1 shows disruption of the cortex anteriorly (black dots) with an intact posterior cortex.
884 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 10/69 P 884 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 10/69 P 884 BLACK T

middle column is intact; it prevents any extrusion of boneor disc into the spinal canal and protects against significantsubluxation. A compression fracture without posteriorcolumn involvement is an example of a stable injury.154
Mechanical instability includes injuries in which two ofthe three columns are injured, thereby allowing abnormalmotion. An example is a severe compression fracture withdisruption of the anterior and posterior columns, whichallows abnormal flexion across an intact middle column.This instability is often associated with pain, but notnecessarily with a neurologic deficit. It is important to
closely evaluate the status of the posterior elements whenevaluating this type of injury. The position of theseelements in relation to each other in the horizontal andvertical planes can give clues regarding flexion androtatory deformity and possible instability. A secondexample is a flexion-distraction injury with disruption ofthe posterior and middle columns; this mechanism causesabnormal flexion with a fulcrum at the intact anteriorcolumn, which functions as a hinge. Chronic instabilityand pain may result, but again, the injury does notnecessarily jeopardize neurologic function. Panjabi andcolleagues performed a biomechanical study on a high-speed trauma model and measured multidirectional flexi-bility. The results of this study supported the three-columntheory of Denis and also showed that the middle columnappears to be the primary determinant of mechanicalstability in the thoracolumbar spine.217
Neurologic instability refers specifically to a burst frac-ture. Denis believed that most of these lesions heal andthat they often become mechanically stable. However, hefound that a neurologic deficit developed in 20% of hispatients with a burst fracture after mobilization as a resultof middle column failure and protrusion of bone into thespinal canal. Neurologic compromise is a strong indicationfor surgical stabilization and decompression. The decom-pression may be accomplished either directly or indirectlyby reduction of deformity and rigid internal immobiliza-tion of the segment. It is generally assumed that injuriessevere enough to cause neurologic deficits are unstable.One’s index of suspicion should remain high whenevaluating these patients.
The typical example of mechanical and neurologicinstability is a fracture-dislocation with disruption of allthree columns and either a neurologic deficit or ‘‘impend-ing neurologic deterioration’’ with the neural elementseither being compressed or ‘‘threatened.’’58
As with the use of any classification system, treatmentfailure may result from rigid adherence to definitionswithout individualizing treatment for each patient.70 Tokeep the use of these definitions in proper perspective,White and Panjabi defined generic clinical instability as‘‘the loss of the ability of the spine under physiologicconditions to maintain relationships between vertebrae insuch a way that there is neither damage nor subsequentirritation to the spinal cord or nerve root and, in addition,there is no development of incapacitating deformity orpain from structural changes.’’273
White and Panjabi273 defined physiologic loads as loadsincurred during normal activity, incapacitating deformity asgross deformity unacceptable to the patient, and incapac-itating pain as discomfort uncontrolled by non-narcoticanalgesics. This definition addresses both the acute and thelate stages of vertebral column trauma. It also drawsattention to the neural elements as a major structure of thespinal column and requires the physician to consider thesestructures, in addition to bones, ligaments, discs, andother soft tissues, as determinants of stability.232 Thoughless specific than Denis’ classification, it requires a basicunderstanding of spinal anatomy, the mechanism of injury,and modes of failure when undertaking treatment.
The preceding discussion should be supplemented witha reminder that instability does not always require surgical
FIGURE 30–10. Lateral compression forces may produce stable lateralwedge compression injuries. They are most often not associated withposterior ligamentous injury.
885CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 11/69 P 885 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 11/69 P 885 BLACK T

treatment. In some cases, prolonged bedrest may be able toachieve the same long-term degree of spinal stability assurgery, and it may be appropriate for the particularcircumstances of an individual patient.
Denis’ Classification of Spinal Injuries
Many classification systems have been designed to describethoracic and thoracolumbar injuries. They may be basedon the mechanism of injury, radiologic/descriptive charac-teristics, or stability. Denis’ three-column concept isfrequently used because it includes each of the injurypatterns most commonly seen and relates them to aspecific mechanism of injury.58
Denis developed his classification system after a reviewof 412 patients with thoracic and lumbar spinal injuries.He divided them into minor and major injuries. Minorinjuries included isolated articular process fractures(0.7%), transverse process fractures (13.6%), spinousprocess fractures (1.7%), and pars interarticularis fractures(1.0%). The four major injury types were compressionfractures (47.8%), burst fractures (14.3%), flexion-distraction (seat belt) injuries (4.6%), and fracture-dislocations (16.3%). Each of these major injuries wasfurther subdivided, depending on the specific radio-graphic findings.
COMPRESSION FRACTURES
By definition, compression fracture injuries are associatedwith fracture of the anterior portion of the vertebral body,but the middle column of the spine is intact (Fig. 30–22).In some cases, the posterior column may be disrupted intension as the upper segments hinge forward on the intactmiddle column. The mechanism of the injury is eitheranterior or lateral flexion.
Compression fractures may be anterior or lateral, withthe former accounting for 89% of this group (see Figs.30–9 and 30–11). Fractures may involve both end-plates(type A, 16%), the superior end-plate only (type B, 63%),the inferior end-plate only (type C, 6%), or a bucklingof the anterior cortex but with both end-plates intact (typeD, 15%).
None of the 197 patients with compression fracturesreported by Denis had a neurologic deficit related to thespinal fracture. Compression fractures with less than 40%to 50% compression and without posterior ligamentousdisruption tend to be stable, low-energy injuries. However,it is still important to assess the patient for noncontiguousspinal fractures.7 A 40% to 50% anterior body compres-sion fracture with the posterior body intact in a physio-logically young individual (with no osteoporosis) stronglysuggests that the posterior ligaments were disrupted.
BURST FRACTURES
Burst fractures are characterized by disruption of theposterior wall of the vertebral body (middle column of thespine), which differentiates them from compression frac-tures (Figs. 30–23 through 30–28). Spreading of theposterior elements may occur and can be seen as awidening of the interpedicular distance on a plain antero-posterior (AP) radiograph of the spine.12
Lamina fractures may also occur (see Fig. 30–6).Cammisa and associates40 found that lamina fractures werepresent on computed tomographic (CT) scans in 50% ofpatients with severe burst fractures, especially in the lowerlumbar spine. In this surgical series, 11 of 30 patients withburst fractures and lamina fractures also had posteriordural tears located at the site of the posterior laminafracture (Fig. 30–29). The incidence was almost 70% inthose with burst fractures, retropulsed bone in the canal,and neurologic injury. The possibility of a dural tear
FIGURE 30–11. Example of a lateral compression fracture. A, An anteroposterior radiograph demonstrates lateral compression with asymmetric loss ofheight. No interspinous process widening is present. B, A lateral radiograph confirms a wedge compression injury with maintenance of height of theposterior portion of the vertebral body. C, A computed tomographic scan through the injured vertebra shows that the injury is limited to the rightanterolateral aspect (arrows), with the remaining cortex intact.
886 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 12/69 P 886 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 12/69 P 886 BLACK T

should be taken into consideration if posterior decompres-sion and stabilization procedures are planned. It shouldnot, however, mandate treatment to routinely repair thedural laceration. Some burst fractures are accompanied byhorizontal fractures of the posterior column. In a retro-spective study by Abe and colleagues, nine patients with athoracolumbar burst fracture and an associated horizontalfracture of the posterior column were studied. They foundthat this type of fracture pattern is not rare; it represented21% of the burst fractures treated by them over an 8-yearperiod. It is best visualized on plain radiographs because itis not easily seen on CT axial cuts. This type of burstfracture differs from flexion-distraction injuries combined
with a burst fracture, which are accompanied by horizon-tal fractures not only in the posterior but also in the middlecolumn. This fracture pattern seems to be more unstablethan burst fractures with no horizontal splitting and mayrequire surgical stabilization to prevent progression ofkyphosis.2
The mechanism of injury for burst fractures is primarilyaxial loading. Axial loading is combined with other forcessuch as flexion (either anterior or lateral) or rotation toaccount for the different fracture patterns seen.
Denis noted that burst injuries can be divided into fivefrequently observed subgroups (Fig. 30–30). One involvesfractures of both end-plates (type A, 24%) and is usuallyseen in the lower lumbar spine. Another involves fractureof only the superior end-plate (type B, 49%) and usuallyoccurs at the thoracolumbar junction. Fracture of only theinferior end-plate is much less common (type C, 7%). Afourth pattern is diagnosed by the presence of a burstfracture of the middle column in combination with arotational injury leading to some degree of lateral sublux-ation or tilt (type D, 15%); this pattern is best seen on aplain AP radiograph. The final subgroup is a burst fractureof the middle column associated with asymmetric com-pression of the anterior column, as seen in a lateralcompression fracture (type E, 5%).
Willen and co-workers verified these injury typesanatomically in autopsy specimens.278 Neurologic deficitswere seen in 47% of the 59 patients studied with burstfractures. There did not appear to be a simple, directrelationship between the extent of spinal canal compro-mise and the severity of neurologic deficit. Willen andcolleagues found increased neurologic damage with type Dfractures, whereas Gertzbein111 found only a weak corre-lation between canal compromise and neurologic deficitin a study of more than 1000 patients with thoracolum-bar spine injuries. Gertzbein thought that most traumato the neural elements probably occurred at the instantof injury. A relationship was, however, found betweenthe location of injury and subsequent neurologic deficit,with the incidence of complete neurologic injury beingsignificantly lower below the thoracolumbar junction(T12–L1).
Burst fractures may be unstable because they representat least a minimum of a two-column injury,154 butadditionally, they may also be accompanied by extensivedisc injury at the levels directly adjacent to the fracture.This possibility has to be considered when deciding ontreatment options.99, 278
FLEXION-DISTRACTION INJURIES
The flexion and distraction mechanism of injury, whichmost commonly occurs in a motor vehicle accident whenthe passenger is using a lap seat belt with no shoulderharness, results in failure of the posterior and middlecolumns in tension with the anterior column serving as thefulcrum (see Figs. 30–15 to 30–17).
Denis divided these injuries into one-level and two-level lesions (Fig. 30–31). A one-level lesion can occurthrough bone, as described by Chance (type A, 47%), or itmay be primarily ligamentous (type B, 11%). Two-levelinjuries involve the middle column by disruption through
FIGURE 30–12. Flexion-rotation forces are much more likely to produceserious spinal injuries than is flexion alone. The combination frequentlydisrupts the posterior ligaments and joint capsules and obliquely disruptsthe anterior disc and vertebral body.
887CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 13/69 P 887 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 13/69 P 887 BLACK T

bone (type C, 26%) or through the ligaments and disc withno middle column fractures (type D, 16%).
One weakness of this classification system is that it doesnot include a category for patients who have distractionfailure of the posterior column with axial load failure of themiddle and anterior columns resulting in a compression orburst fracture. This shortcoming has been noted by severalauthors, who have added additional categories for seat beltinjury.112, 120
In none of the 19 patients with a seat belt injury inDenis’ series did a neurologic deficit related to the spinalfracture develop. In other series, the incidence is alsolow, usually less than 10%.111 Injuries with ligamentous
involvement should be considered acutely and chronicallyunstable, whereas those with significant bone involvementare acutely unstable but may heal well.
FRACTURE-DISLOCATIONS (SHEAR)
Fracture-dislocations are caused by failure of all threecolumns of the spine as a result of compression, tension,rotation, or shear forces (Figs. 30–32 through 30–34).
Three different mechanisms (i.e., three types offracture-dislocation) can occur (see Fig. 30–34). Onepattern (type A) is a flexion-rotation injury, which wasoriginally described by Holdsworth in victims of mining
FIGURE 30–13. This patient sustained a bilateral facet dislocation at T12–L1 as a result of a flexion-distraction/rotation mechanism. A, A lateral radiographshows significant translation of T12 over L1 with maintenance of the integrity (height) of the posterior wall of L1 but some slight comminution of theanterosuperior portion of the body. B, This relationship is well demonstrated on a midsagittal reconstruction of the computed tomographic (CT) scan. C,The characteristic findings on axial images of the CT scan are the double-body image and the empty facet sign (arrows).
888 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 14/69 P 888 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 14/69 P 888 BLACK T

accidents.133 This type may also occur after ejection froma motor vehicle or a fall from a height (Fig. 30–35A). Ashear fracture-dislocation (type B) can be caused by aviolent force directed across the long axis of the trunk. Onesuch example, as described by Denis and Burkus, occurswhen a lumberjack is struck across the midportion of hisback by a falling tree (see Fig. 30–35B).60 Denis’ third type(type C) is a bilateral facet dislocation (see Fig. 30–35C)caused by a flexion-distraction injury. It resembles the seatbelt injury previously described, but with failure of theanterior column. This injury most commonly occurs with
failure of either the anterior intervertebral disc or theanterior vertebral body. The anterior longitudinal ligamentis usually stripped off the inferior vertebral body, therebyallowing significant subluxation to occur.
Denis described 67 patients with fracture-dislocations.Of these patients, 56 had flexion-rotation injuries, 7 hadshear injuries, and 4 had bilateral facet dislocationsresulting from flexion-distraction injuries. All these inju-ries involve significant destruction of each of the threecolumns. This group of injuries was associated with thehighest incidence of neurologic deficit. Of the patientswith flexion-rotation injuries, only 25% were neurologi-cally normal, and 39% had complete spinal cord injuries.All seven patients with shear injuries had completeneurologic deficits. Of the four patients with flexion-distraction injuries, three had incomplete neurologicdeficits, and one was neurologically normal. Other inves-tigators have also reported a significantly higher incidenceof neurologic deficit in patients with fracture-dislocationsthan in those with other injury patterns.111 These injuriesare acutely highly unstable.
‘‘Comprehensive’’ Classification
Various attempts have been made to develop a universalclassification of spinal injuries. In reality, to be effective,such a classification must include structural injury to bothbone and soft tissue, as well as consideration of thepatient’s neurologic status. Gertzbein and colleagues103, 110
formulated a classification system dealing with the struc-tural components of spinal injury, similar to the AOfracture classification used for the extremities. The lesionsare differentiated on the basis of not only the mechanismand radiographic appearance of the injury but also theassociated soft tissue disruption. The classification consistsof well-defined categories based on common morphologiccharacteristics, as well as common primary forces produc-ing the particular injury pattern (Fig. 30–36).
Three main injury types are recognized. Type A injuriesare vertebral body compression fractures (Fig. 30–37).They are caused by axial loading with or withoutadditional flexion forces and are associated with loss ofvertebral height. Type B injuries involve both the anteriorand the posterior elements and are caused by distractiveforces (Fig. 30–38). The hallmark of these injuries iselongation of the distance between portions of the adjacentvertebrae. In type C injuries, anterior and posteriordisruption is present along with associated evidence ofrotational instability, such as offset vertebral bodies,unilateral facet fracture-dislocations, or fractured trans-verse processes (Fig. 30–39).
The three major patterns and their associated subtypesrepresent a continuum of injury severity, from type Alesions, which are axially unstable, to type B lesions, whichhave additional sagittal-plane instability, to type C, withinstability in all three planes. Because the classificationprogresses according to the severity of bony and soft tissuedisruption, as well as stability, it may be used as a guide fortreatment, with injuries more advanced on the classifica-tion being more likely to benefit from surgical treatment.However, it has not been validated as a reproducible
FIGURE 30–14. Flexion-distraction forces across the thoracolumbar spinefrequently produce the typical seat belt injury. The axis of rotation isanterior to the spine, with all the elements of the spine in tension. If thisaxis of rotation is moved posteriorly into the vertebral body, it is possibleto have compressive forces across the anterior vertebral body anddistraction forces across the posterior elements and middle column of thespine.
889CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 15/69 P 889 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 15/69 P 889 BLACK T

FIGURE 30–15. Example of a flexion-distraction injury with disruption through bone. A, An anteroposterior radiograph demonstrates interspinouswidening (arrow) with a fracture line through the lamina of L1 (arrowheads). B, A lateral radiograph confirms the pure osseous lesion, with the fractureline coursing posteriorly through the upper portion of the lamina anteriorly into the vertebral body. C, The injury is better seen on this lateral tomogram,with the fracture line extending through the pedicle. D, The patient was treated operatively with Edwards compression rods from T12 to L2. In thisinstance, the L1 lamina could not be used for anchoring hooks because of the injury to the lamina at this level. E, A lateral radiograph shows reductionof the fracture and restoration of anterior height.
890 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 16/69 P 890 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 16/69 P 890 BLACK T

classification and is unlikely to be validated because of itsextreme complexity.
Other useful classification systems are those describedby Ferguson and Allen92 and by McAfee and co-workers.191, 195, 196 These classification systems focusprimarily on the mechanical forces involved and describethe type of bone or ligamentous injuries associated withthese forces. The American Spinal Injury Association(ASIA) classification system for neurologic injury is themost commonly used objective system currently available.
Because the primary goal of this chapter is to provideclinical guidelines for diagnosing and treating specificinjuries, the more pragmatic classification system of Denisis preferred. For purposes of consistency in this book, anomenclature and classification system consisting of a
combination of mechanistic and descriptive features isused; it is the same for thoracic, thoracolumbar, andlumbar injuries. The first group of injuries consists ofminor injuries, such as avulsion and minor fractures. Thesecond group includes compression fractures, or injuriesgenerated by a combination of flexion and bending thatcan be either stable or unstable, depending on the degreeof anterior compression and ligamentous disruption. Thethird major group represents burst fractures caused by acombination of flexion and axial loading in varyingproportion, and they are easily subdivided by Denis’classification. The fourth group is flexion-distractioninjuries, which are subdivided according to the injuredtissues: the pure bony form is a Chance fracture, the purelyligamentous form is a bilateral facet dislocation, and the
FIGURE 30–16. Example of a combined osseoligamentous flexion-distraction injury at T12. A, A lateral radiograph demonstrates the fracture line coursingthrough the pedicle and traversing the posteroinferior aspect of the body to the T12–L1 disc space. B, A lateral tomogram highlights the path of the fracture(arrowheads). C, An anteroposterior (AP) tomogram clearly demonstrates the fracture through the pars interarticularis. Note the distinctive interspinouswidening with this injury. D, A computed tomographic scan through the upper portion of T12 demonstrates absent inferior T11 facets as a result of thedistraction component. E, This injury was corrected with Edwards compression rodding from T11 to L1, with reduction of the fracture and realignmentof the spine. F, A postoperative AP radiograph confirms reduction of the interspinous widening.
891CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 17/69 P 891 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 17/69 P 891 BLACK T

combination form is either an anterior bony injury withposterior ligamentous disruption or a posterior bonyinjury with anterior discal disruption. The fifth group ofinjuries results from an extension force. The final type iscaused by shear. Clearly, no comprehensive or trulyuniversal system exists because the optimal classificationsystem would have to combine the fracture pattern withinstability and neural status.
OPERATIVE VERSUS NONOPERATIVETREATMENTz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Nonoperative treatment of thoracic and thoracolumbarspine injuries can be extremely effective. The datapresented by Frankel and associates in 1969 remain thestandard against which most treatments and final out-comes are measured.98 Similar excellent results werepublished by Davies and colleagues.56, 139 Postural reduc-tion, as described by Frankel, is still used in someEuropean centers, reportedly with good results.34, 268
A comparison of the results of surgical and nonsurgicaltreatment in the literature is difficult because of thevariations in injury type and differences in severity in thetwo groups, with the surgically treated groups often con-taining patients with more severe injuries.111 Some seriesshow a slight trend toward better neurologic improvementwith surgical treatment, but the statistical significance is
not high.159 Most investigators describing better neuro-logic improvement with surgery have directed their atten-tion at neural decompression through either an anterioror a posterior approach.3, 4, 73, 111, 113, 135, 160, 233, 284
Edwards and Levine described better neurologic recoverythan would be expected with nonoperative treatment byusing the Edwards instrumentation system posteriorlywhile depending on indirect decompression based onimproved fracture reduction.80, 81 Gertzbein, in a study of1019 spine fractures, found no significant improvement inneurologic function with operative treatment.111 In addi-tion, Bravo and co-workers did not find a significantdifference in neurologic improvement in patients treatedwith surgery versus those treated by postural reductionand immobilization.34
Neurologic deterioration can occur during nonopera-tive treatment and was documented in 6 of 33 patientswith burst fractures of the thoracic or thoracolumbarspine.59 Denis and co-workers concluded that surgicaltreatment was a safer treatment option for this specificinjury.59 However, Frankel and associates,98 in their reviewof 371 patients with thoracic or thoracolumbar fractures,found that only 0.5% had neurologic deterioration whentreated by postural reduction and recumbency. Mumfordand co-workers reported a 2.4% incidence of neurologicdeterioration in patients with burst fractures treatednonoperatively.206 If patients do experience neurologicdeterioration during nonoperative treatment, surgicaltreatment, including decompression by an anterior ap-
FIGURE 30–17. Flexion-distraction injury at T12–L1 predominantly disrupting ligamentous structures. A, An anteroposterior radiograph showsinterspinous widening between T12 and L1. B, A lateral radiograph demonstrates the predominantly ligamentous involvement, with the anterior bodiesremaining intact. Note the subluxation of T12 on L1 as a result of the dislocated facets. C, A three-dimensional computed tomographic reconstructionof the injured level shows the dislocated, locked facets. Note the fractured transverse process at L1. D, This patient was operatively managed with an AOinternal fixator from T12 to L1. E, A postoperative lateral radiograph demonstrates reduction and realignment of the injured level.
892 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 18/69 P 892 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 18/69 P 892 BLACK T

proach, is recommended.111 Finally, whether surgicaltreatment or nonoperative treatment is safer depends tosome degree on the experience and preference of thetreating physician and the medical team.
Deformity can be corrected with surgery, but it isunclear whether it is clinically relevant.34, 56, 215 Nicoll211
noted no correlation between deformity and symptoms,whereas Soreff and colleagues258 found a significantcorrelation. McAfee and associates,193 in their review oflate anterior decompression and fusion for thoracolumbarand lumbar injuries, found that residual kyphosis did notinhibit neural improvement. Gertzbein, however, reported
that kyphosis of more than 30° was associated with asignificantly increased amount of back pain at 2-yearfollow-up.111 Edwards and Levine’s data also suggest thatanatomic restoration is important in obtaining goodlong-term results.79–81, 83
Some authors believe that chronic back pain isdiminished in operatively treated patients when comparedwith those treated nonoperatively.111 This improvement inrelief of pain may be a result of better correction andmaintenance of alignment with operative treatment. Inaddition, operative treatment includes fusion of motionsegments with significantly damaged soft tissue elements.These injured tissues often have poor healing potential,
FIGURE 30–19. Extension forces occur when the upper part of the trunkis thrust posteriorly, with the application of anterior tension and posteriorcompression. Most of these injuries are stable unless retrolisthesis of theupper on the lower vertebral body has occurred.
FIGURE 30–18. Shearing requires forces from opposing directions to passthrough the spine at slightly different levels. This mechanism tends toproduce extremely unstable injuries with disruption of all columns of thespine and may produce severe spondylolisthesis with the cephalic spinepositioned anteriorly, posteriorly, or laterally in relation to the caudalportion of the spine.
893CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 19/69 P 893 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 19/69 P 893 BLACK T

and the patient is left with an abnormal motion segmenteven after adequate healing of bone.
Most authors agree that hospitalization time can beshortened by surgical stabilization in patients with paral-
ysis.49, 66, 95, 139, 233 Mobilization and rehabilitation can befacilitated by rigid surgical stabilization, which decreasesthe associated morbidity of prolonged immobilization.However, Gertzbein, in a multicenter spinal fracture study,found the complication rate in surgical patients to be morethan 25%, whereas patients treated nonoperatively had acomplication rate of only 1%.111 The patients treatedsurgically tended to have more severe injuries and a higherincidence of neurologic deficit, both of which increase thelikelihood of complications regardless of treatment type.Place and colleagues compared operative and nonoperativetreatment of patients who sustained spinal fractures withresultant complete spinal cord injuries. The length ofinpatient hospital and rehabilitation stay was 19% less forthe surgically treated group, even though their rate ofcomplications was almost twice as high as that in thenonoperative group.223 At this time, early mobilizationremains the primary predictable advantage of instrumen-tation.
TREATMENT OF SPECIFIC INJURIESz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Minor Fractures
Fractures of the transverse processes usually occur eitherfrom direct trauma or as a result of violent muscularcontraction (avulsion injuries) in response to injury.Isolated fractures of the spinous processes may result froma direct blow over the posterior aspect of the spine.Similarly, fracture of the articular process may occur as aresult of direct trauma. In each of these cases, even thoughthe injury may appear benign, further evaluation isnecessary to be certain that no other associated spinalinjuries are present. Such evaluation is most easilyaccomplished by obtaining a CT scan through the vertebrain question and the adjacent vertebrae. If the CT scan isnegative (no other injuries detected), lateral flexion andextension radiographs should be considered if dynamicinstability is a concern. Once other major injuries to thespine have been excluded, these patients can be mobilizedwith no special brace or activity restrictions, except asneeded for painful symptoms. Transverse process fracturesare painful, and orthotics may be helpful.
Another minor injury is an isolated fracture of the parsinterarticularis at one level, either unilaterally or bilaterally.In Denis’ series, four individuals had this type offracture,58 with all four being the result of a sports injury.If the patient has this injury along with a negative previoushistory of local spine pain (particularly in a young adult orteenager), it can be assumed that this fracture is an acuteinjury that is best treated with immobilization. In thethoracolumbar and upper lumbar regions of the spine, atotal-contact thoracolumbosacral orthosis (TLSO) is ap-propriate. At the L5 level of the spine, it may be necessaryto include one thigh to provide adequate immobilization.
Fractures of the pars interarticularis in the thoracolum-bar or upper lumbar spine in combination with a historyof more severe trauma suggest a major spine injury (e.g.,seat belt injury). This injury can be discerned on thin-cutCT scans with reconstructions of the spine and may also bewell visualized on flexion-extension radiographs if the
FIGURE 30–20. This 26-year-old man was involved in a motor vehicleaccident and sustained an extension injury to the lower part of the spine.A, An anteroposterior radiograph shows a fracture line coursing throughthe lamina of L4 (arrows). Arrowheads point to transverse processfractures. B, A lateral radiograph was unremarkable. C, Computedtomographic scan through the injured body of L4 with multiple fracturelines noted in the posterior column (arrowheads).
894 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 20/69 P 894 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 20/69 P 894 BLACK T

Anterior Middle Posterior
FIGURE 30–21. Denis’ three-columnmodel of the spine. The middlecolumn is made up of the posteriorlongitudinal ligament, the posteriorportion of the anulus fibrosus, andthe posterior aspect of the vertebralbody and disc.
A B
C D
FIGURE 30–22. Denis’ classification ofcompression fractures. These frac-tures may involve both end-plates (A,type A), the superior end-plate only(B, type B), the inferior end-plateonly (C, type C), or a buckling of theanterior cortex with both end-platesintact (D, type D).
895CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 21/69 P 895 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 21/69 P 895 BLACK T

FIGURE 30–23. A 43-year-old man sustained a T12 and L1 burst fracture when a mobile home roof fell on him during a storm. The patient wasneurologically intact. A, A preoperative anteroposterior (AP) radiograph shows approximately 50% loss of height at T12 and L1. B, A preoperative lateralview shows local kyphosis measuring 27°. C, An axial computed tomographic scan shows a minimal burst component at L1. D, This injury was stabilizedwith Synthes USS instrumentation. A pedicle screw was placed in the burst-fractured vertebra of T12 (the pedicles were intact) to act as a fulcrum in thereduction of his 27° of kyphosis. E, Postoperative AP radiograph showing two cross-connectors used for additional stability.
896 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 22/69 P 896 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 22/69 P 896 BLACK T

patient can tolerate the motion. A CT scan, unless the cutsare fine, may not be helpful in determining whether thepars fracture is isolated or a component of a seat belt injurybecause the fracture lines often lie in the transverse planeof the spine and are difficult to visualize with standard CTscanning.33
Compression Fractures
By definition, compression fractures include disruption ofthe anterior column with an intact middle column.Differentiation between a compression fracture and aminimally displaced burst fracture with associated middlecolumn involvement may be subtle. McGrory and col-leagues200 described the use of the posterior vertebralbody angle (PVBA) measured on a lateral plain radiograph.The PVBA is the angle formed by either the superior or theinferior end-plate and the posterior vertebral body wall.An angle greater than 100° for either the superior or theinferior PVBA is considered diagnostic of a burst fracture.A slight decrease in height of the posterior wall incomparison to the vertebra above and below and loss ofthe biconcave contour may also suggest the presence of aburst rather than a compression fracture. Even with carefulscrutiny, 20% or more of subtle burst fractures can bemisdiagnosed on plain radiographs. Therefore, the routineuse of CT scanning for patients with probable compressionfractures is a better method to evaluate the middlecolumn.17 Treatment of these injuries depends on thestatus of the posterior elements, which may or may not bedisrupted. If the anterior column is compressed 40% ormore or if the kyphosis exceeds 25° to 30°, it can beinferred that the ligaments of the posterior column havebeen attenuated to the point that they can no longerfunction normally. Magnetic resonance imaging (MRI) hasbeen shown to be a useful adjunct for identifying the
presence of posterior ligament injury.155 In addition, MRImay be useful in helping differentiate benign from patho-logic compression fractures.9
Nonoperative treatment is adequate in most compres-sion fractures with less than 40% anterior compressionand less than 25° to 30° kyphosis. These patients canusually be managed in a restrictive orthosis, such as atotal-contact TLSO or, occasionally, a Jewett brace. Theycan be allowed to participate in most of their normalactivities while wearing the brace (see Fig. 30–9). Thesepatients should be encouraged to lie in the prone position,which tends to minimize the deformity. They should bediscouraged from lying supine on a soft mattress withmultiple pillows because this position can accentuate thedeformity. Hazel and associates reviewed the long-termoutcome of neurologically intact patients with compres-sion fractures treated nonoperatively. Of the 25 patientsmonitored, 8 had no symptoms, 11 had occasional backpain, 5 needed treatment or modification of activitybecause of frequent pain, and only 1 patient had chronicdisabling back pain.129
The brace should be worn for 3 months or longer.Standing lateral flexion and extension radiographs out ofthe brace should then be obtained. If no abnormal motionis seen through the fractured vertebra or the disc aboveand if significant progression of the deformity has notoccurred, use of the orthosis can be discontinued. Muscleweakness may be significant, and gradual cessation ofbracing over a few weeks may be beneficial, along with amuscle-strengthening program to help support the spine.In those with abnormal motion at the level of injury,continued pain, or progression of deformity to a degreeunacceptable to the patient, surgery may be indicated.Some authors believe that stable fractures in the upper andmiddle thoracic spine do not require brace treatment at allbecause of the inherent stability of the rib cage. Mostauthors tend to be more cautious and usually recommend
FIGURE 30–24. Example of a stable burst fracture (Denis type B) in a 52-year-old man who was neurologically intact. The fracture was treatednonoperatively. A, An anteroposterior radiograph demonstrates loss of height of the body of T12, with minimal interpedicular widening and nointerspinous separation noted. B, A lateral radiograph confirms involvement of the anterior and middle columns with loss of height at both sites. C, Acomputed tomographic scan through T12 demonstrates disruption of the posterior vertebral cortex (arrow) but only minimal displacement of the fragment.The posterior ring remains intact.
897CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 23/69 P 897 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 23/69 P 897 BLACK T

external immobilization at the thoracolumbar junction orin the lumbar spine. Schlickewei and associates249 com-pared a group of patients with stable thoracolumbarinjuries treated by early mobilization with or without abrace. After an average of 2.5-years’ follow-up, they foundgood or excellent results in both groups, without clinicallysignificant differences in progression of deformity betweengroups.
Initial surgical treatment should be recommended if theanterior column is compressed more than 40% or if thekyphosis exceeds 25° to 30°. For those with borderlineindications, surgery could be considered as an option in ayoung patient with a high-energy injury, but it would
probably not be recommended in an elderly patient withmarked osteoporosis and low-energy trauma. In the formercase, the posterior ligaments are much more likely to bedisrupted than in the latter.
Because the posterior elements are disrupted, a poster-ior surgical approach is indicated, and any dual-rodtechnique would be adequate. A distraction system can beused with three-point fixation (e.g., hook-rod system orsegmental fixation systems). If the middle column isdefinitely intact, a compression system can be used (e.g., asegmental fixation system with hooks or screws). Thesurgeon should be aware that a compression system maycause posterior protrusion of an already disrupted disc at
FIGURE 30–25. This 19-year-old man was involved in a fall from an all-terrain vehicle and sustained a burst injury at T12 that resulted in a complete spinalcord injury. A, An anteroposterior (AP) radiograph demonstrates significant loss of height at T12 with interpedicular widening, classically seen with burstfractures. A compression fracture of the superior corner of L2 is also noted (arrow). B, A lateral radiograph shows significant loss of height of both theanterior and middle columns of T12. Small compression injuries at L1 and L2 (arrows) are also seen. C, A computed tomographic scan through T12confirms the presence of a burst fracture with a large retropulsed fragment compromising 80% of the canal and resulting in injury to the conus. D, Apostoperative AP radiograph shows placement of Cotrel-Dubousset instrumentation. A laminar claw configuration was used above and below T12. TwoTexas Scottish Rite Hospital cross-links were used to reinforce the construction. The patient was postoperatively mobilized without a brace. E, Lateralpostoperative radiograph. It would have been better had the upper claw been placed around the T10 lamina to increase the superior lever arm andminimize ‘‘metal stenosis’’ at the site of the retropulsed bone fragment.
898 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 24/69 P 898 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 24/69 P 898 BLACK T

FIGURE 30–26. This 30-year-old man was an unrestrained passenger involved in a motor vehicle accident and was ejected from his car. He sustained anL1 burst fracture with an incomplete spinal cord injury. A, An axial computed tomographic scan through the body of L1 shows a large retropulsed fragmentoccupying most of the spinal canal. B, The patient was treated by anterior corpectomy and decompression at L1. Stability was achieved with the Kanedasystem. C, A 2-year postoperative lateral view shows continued restoration of height and reestablishment of sagittal alignment.
FIGURE 30–27. This 38-year-old man was involved in a motor vehicle accident and sustained a burst fracture of T12. The patient had decreased motorfunction in both lower extremities as well as bladder dysfunction. A, An anteroposterior (AP) radiograph shows collapse of the body and interpedicularwidening. B, A lateral radiograph shows loss of height and segmental kyphosis measuring 28°. C, An axial-cut computed tomographic scan through T12shows a large retropulsed fragment compromising most of the canal. D, A postoperative AP radiograph shows stabilization after corpectomy with a tibiaallograft strut and instrumentation consisting of the University Plate (Acromed). E, A lateral postoperative radiograph shows restoration of height andsagittal alignment with 3° of kyphosis.
899CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 25/69 P 899 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 25/69 P 899 BLACK T

the level of injury and that this protrusion may be largeenough to cause neurologic deterioration. If a compressionconstruct is being considered, the use of intraoperativeevoked potentials is important because it may provideearly documentation of protrusion and allow the surgeonto change the technique or perform a posterolateraldecompression to remove the disc fragment.
The use of anterior surgery is not required for neuraldecompression with these fractures because the middle
column remains intact. However, supplemental anteriorsurgery may occasionally be necessary for patients withmarked anterior destruction to restore bone stock. Thissituation is usually seen in patients with severe osteopeniawho are involved in high-energy injuries. These samepatients may also undergo late collapse with progressivekyphosis and subsequent neurologic deficit. They are besttreated by an anterior approach, although the use ofvertebroplasty has obviated this approach in most cases.146
FIGURE 30–28. Example of a flexion-distraction injury at T12–L1 with an associated burst component of the L1 vertebral body. This patient had anincomplete cord injury. A, Anteroposterior radiograph showing interpedicular widening and increased distance between the posterior spinous processesat T12–L1. B, A lateral radiograph shows the local kyphosis and burst injury at L1. C, A preoperative computed tomographic (CT) scan shows severe canalencroachment from the burst component. D, The patient was treated with ISOLA instrumentation and Edwards sleeves. E, A postoperative lateralradiograph shows good sagittal alignment and reduction of the vertebral body height. F, A postoperative axial CT scan shows partial restoration of thecanal.
900 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 26/69 P 900 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 26/69 P 900 BLACK T

Burst Fractures
By definition, every burst fracture includes disruption ofthe anterior and middle columns, with or withoutdisruption of the posterior column. The type of treatmentdepends on the severity of the injury.150 The three mostimportant factors to be considered are the percentage ofspinal canal compromise, the degree of angulation presentat the site of injury, and the presence or absence of aneurologic deficit.
No strong clinical basis is available to develop aconsensus regarding the best treatment of patients withburst fractures. James and co-workers,141 using a humancadaver L1 burst fracture model, showed that the condi-tion of the posterior column was the most important factorin determining the acute stability of a burst fracture and,therefore, the suitability for nonoperative treatment. Theywent on to review a series of patients with intact posteriorcolumns, but varying degrees of anterior and middlecolumn disruption, and noted that they healed withoutdeformity. Willen and colleagues277 reported on 54patients with thoracolumbar burst fractures treated non-operatively, including patients with neurologic deficit.Most of the deformity occurred on initial mobilization,with little progression of deformity noted at follow-up.Patients with more than 50% loss of height or more than50% canal compromise were found to have significantlyincreased complaints of pain at follow-up. Cantor and
co-workers41 also recommended operative treatment forpatients with evidence of posterior column disruption.Treatment of burst fractures can be logically defined withregard to the goals of surgery. Three parameters determinethese goals: neurologic status, instability, and deformity. Inpatients with neurologic compromise accompanied byinstability, cord compression, marked deformity, or anycombination of these conditions, surgical intervention isthe most appropriate treatment. Nonoperative treatment ofa patient with a neural deficit can be considered in the rareinstance of a stable burst fracture without deformity orresidual cord compression. If the patient is neurologicallyintact and has less than 50% canal compromise and lessthan 30° kyphosis (see Fig. 30–24), nonoperative treat-ment is indicated. Patients with minimal angulation and atwo-column or stable burst pattern should be placed in atotal-contact orthosis with early ambulation as tolerated.41
If the canal compromise is greater than 40% or athree-column injury is present, recumbency for severalweeks should be considered if surgery is not performed;ambulation can then begin in a total-contact TLSO.Surgery is the preferred treatment in patients with morethan 50% canal compromise or more than 30° kyphosis atthe level of injury, even if they do not have any neurologicdeficit.
It should be emphasized that a neurologic deficitincludes not only lower extremity motor and sensorydysfunction but also perineal sensory loss and bowel or
A B
C
FIGURE 30–29. Illustration of the pro-posed mechanism of injury in patientswith burst fractures along with associ-ated laminar fractures and posteriordural tears. A, With axial loading andspreading of the pedicles, a laminarfracture is produced and bone isretropulsed from the vertebral bodyinto the spinal canal. This mechanismof injury may result in protrusion ofthe dura between the laminar fracturefragments. B, As the axial load isdissipated, the laminar fracture frag-ments recoil and may entrap the duraand nerve rootlets. C, If approachedposteriorly, the laminar fracture isdifficult to visualize, and if not care-fully sought, the dura and nerverootlets may be further injured. (A– C,Redrawn from Eismont, F.J.; Green,B.A. J Bone Joint Surg Am 71:1044–1052, 1989.)
901CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 27/69 P 901 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 27/69 P 901 BLACK T

bladder dysfunction. A rectal examination should beperformed to determine whether anal tone is normal withvoluntary contracture. Postvoid residual urine should alsobe checked to be certain that the volume of retained urineis less than 50 mL. Any abnormality in bowel or bladderfunction should be considered a neurologic deficit.
Controversies in the nonoperative treatment of burstfractures include the appropriateness of bedrest and theduration and types of orthosis. However, the duration ofusing a total-contact orthosis should be at least 3 months.During that time, once ambulation is initiated and nochange in alignment is observed on standing lateralradiographs, an increase in activities can be allowed. Someprogressive loss of height of the involved disc space is to beexpected; however, if posterior spinous process wideningis noted or angulation increases to more than 30°,surgical treatment is recommended.141 Mumford andco-workers206 studied 41 patients with thoracolumbarfractures and no neurologic deficit who were treatednonoperatively. The average collapse at follow-up was only
8%, with significant resorption of protruding bone anddiminution in canal compromise (22%). Almost 90% ofpatients had satisfactory work status at last follow-up. Theauthors were unable to correlate residual deformity withsymptoms. Cantor and associates41 reported their resultson 18 neurologically intact patients with burst fracturestreated nonoperatively. They found no prolonged hospitalstay, no significantly increased kyphosis, and little or norestriction of function at follow-up.
If nonoperative treatment is used, prolonged riding inautomobiles and participation in impact activities shouldbe discouraged for 3 to 6 months. The patient should alsobe instructed to avoid marked flexion at the level of injurywhile lying in bed and to avoid lying supine with multiplepillows because this position could increase the deformity.Patients should be encouraged to sleep in the proneposition. If they are unable to understand or follow theseinstructions, either a cast or surgery should be considered.Patients should be instructed to notify the physicianimmediately if any paresthesias, cramping in their lower
A B C
D E
FIGURE 30–30. Denis’ classification of burst fractures. A– C, Types A, B, and C represent fractures of both end-plates, the superior end-plate, and the inferiorend-plate, respectively. D, Type D is a combination of a type A burst fracture with rotation, which is best appreciated on an anteroposterior (AP) radiograph.E, A type E burst fracture is caused by a laterally directed force and hence appears asymmetric on an AP radiograph. The superior or inferior end-plate,or both, may be involved in this fracture.
902 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 28/69 P 902 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 28/69 P 902 BLACK T

extremities, weakness in their legs, or a change in bowel orbladder control develops. Patients should be evaluatedfrequently (1 week, 1 month, 2 months, and 3 monthsafter injury) with standing lateral radiographs to be certainthat the angulation at the level of injury has not increased.After healing appears to be adequate, flexion-extensionradiographs are taken with the patient out of the brace tomake sure that no excessive motion has occurred at thefracture level. If nonoperative treatment fails and eitherprogressive deformity or a neurologic deficit develops,surgical intervention should be initiated. The type ofsurgery is dependent on the method of failure ofnonoperative treatment. If a neurologic deficit develops,anterior decompression should be considered becauseposterior instrumentation performed more than 2 to 3weeks after injury will not adequately reduce the canalcompromise. Similarly, posterolateral decompression maybe difficult as the fragment begins to heal into position.However, if the patient fails nonoperative treatmentbecause of persistent pain or increasing deformity, poster-
ior surgery is usually adequate. If the deformity is partiallycorrected on flexion-extension views, satisfactory reduc-tion of kyphosis can be achieved with posterior instrumen-tation and fusion.
Burst fractures that require operative treatment can beappropriately reduced and stabilized with any system thatallows distraction and three- or four-point fixation. Bymeans of force vectors placed by posterior instrumenta-tion, the ligaments of the middle column can be tightened,thereby reducing the intracanal fragment. Indirect reduc-tion was originally thought to be caused by tensing of theposterior longitudinal ligament, but more recent studiespoint to the annular attachments as being responsible forindirect reduction.39, 99, 127 The most commonly usedposterior systems are currently those that allow segmentalfixation with varying combinations of hooks and screws.Such systems allow variation in the length of the construct,as well as in methods of attachment to the vertebra,depending on the location of the fracture within the spineand the fracture pattern.
A B
C D
FIGURE 30–31. Denis’ classification of flexion-distraction injuries. These injuries may occur at one level through bone (A), at one level through theligaments and disc (B), at two levels with the middle column injured through bone (C), or at two levels with the middle column injured through ligamentand disc (D).
903CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 29/69 P 903 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 29/69 P 903 BLACK T

Zou and colleagues287 studied the use of variousposterior fixation devices for the treatment of burstfractures in a cadaver model. They noted that devicescapable of providing distraction and restoration of sagittalalignment resulted in significantly better canal decompres-sion than did systems that used only distraction. Mannand associates188 compared the Syracuse I-Plate (appliedanteriorly) with the AO Fixateur Interne pedicle screwsystem for the treatment of burst fractures. They foundthat both systems provided adequate stability in patientswithout posterior column disruption. In the presence ofposterior disruption, posterior instrumentation providedsignificantly increased stability. Gurwitz and colleagues122
compared the use of the Kaneda device for anteriorfixation with pedicle screws and a variable spinal plate(VSP) posteriorly for fixation of a corpectomy modelused to simulate a burst fracture. They found that short-segment posterior instrumentation did not adequatelyrestore spinal stability. Farcey and co-workers91 reportedthat posterior fixation does not adequately prevent latecollapse if significant anterior destruction with concomi-tant kyphosis has occurred. They recommended the addi-tion of an anterior strut graft for mechanical reasons, inaddition to posterior instrumentation.
With posterior distraction systems, intraoperativeevoked potentials, posterolateral decompression, and spi-nal sonography may all be used to document and treat anyresidual neural compression that remains after alignmentand stabilization of the fracture. An alternative is to obtainpostoperative CT scans to determine the extent of residual
neural compression and decide whether additional ante-rior decompression and fusion may be necessary (see Fig.30–47). This decision should be predicated on the patient’spostoperative neurologic status with a plateau at a lessdesired or expected level of function. Surgeons whoperform posterior stabilization procedures should beaware that patients who have burst fractures with concom-itant lamina fractures and a neurologic deficit have a 50%to 70% chance that a posterior dural laceration secondaryto the injury is also present.40 Should this complication beencountered, the surgical team should be prepared tomake appropriate repairs.
Burst fractures that require surgery should not betreated with a compression construct, which may increasethe extent of bone retropulsion into the spinal canal. Thisinjury should also not be treated with Luque rods becausethe spine is not protected from axial loading with this typeof fixation and increased retropulsion of bone into thespinal canal is possible.
A neutralization system such as one using plates andscrews may be adequate for the treatment of midlumbarand lower lumbar injuries, if realignment (distractionlordosis) can be obtained. If reduction is achievable,pedicle screw systems allow the surgeon to minimize thelength of the fusion and still provide stability. Althoughthese systems have also been advocated for thoracolum-bar junction injuries, they fail more often in suchapplications, with resultant recurrent deformity and neu-ral compression, particularly if the normal spinal contouris not achieved. If a pedicle screw–based construct with
FIGURE 30–32. A T4–T5 fracture-dislocation resulted in a complete spinal cord injury in a 30-year-old man. A, A computed tomographic scan throughthe injured level demonstrates marked displacement and comminution at T4–T5, with multiple bone fragments within the canal. B, A postoperativeanteroposterior radiograph shows stabilization with a Luque rectangle and sublaminar wires. This instrumentation provided rigid fixation and allowedearly mobilization with minimal external support. The strength of fixation could have been improved with the use of double wires around the laminabilaterally. C, Postoperative lateral radiograph.
904 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 30/69 P 904 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 30/69 P 904 BLACK T

only two-point fixation extending one level above and onelevel below the injury is used at the thoracolumbarjunction, it may be necessary to combine this procedurewith anterior fusion to provide axial support through theinjured vertebra. Such fusion is often not necessary inthe lower and midlumbar spine, in which more weight iscarried through the posterior elements. Insertion ofscrews into the fractured vertebra (if the pedicles areintact) to create three-point fixation and re-create the nor-mal lordosis may obviate the need for concurrent anteriorstabilization.
Anterior decompression and fusion (with instrumenta-
tion) may be performed to treat burst injuries. Thisprocedure is best for patients with significant neuralcompression and neurologic deficit, particularly those withminimal kyphotic deformity. Anterior decompression andfusion should be routinely considered if the injuryoccurred 3 or more weeks previously. The use of thisapproach best ensures adequate neural decompression,and although more residual deformity may remain thanwith most posterior instrumentation systems, it is toleratedby the patient if the anterior fusion is solid. With the useof anterior instrumentation it is possible to obtainadequate correction of deformity, as well as decompression
FIGURE 30–33. This 32-year-old man was involved in a motor vehicle accident and sustained a fracture-dislocation of the thoracic spine and a completespinal cord injury. A, An anteroposterior radiograph demonstrates loss of height at T9, with a minimal rotatory component. B, A lateral radiograph confirmsfracture of the body of T9 with forward subluxation of the body of T8 on T9. Involvement of the posterior wall of T9 appears minimal. C, A computedtomographic scan through the injured level reveals the offset of the T8 vertebra in comparison to T9. The canal compromise is predominantly related tothe malalignment. D, The patient was treated operatively, with instrumentation applied by using the Harrington-Luque technique. Segmental sublaminarwires are used to enhance fixation and allow mobilization with minimal external support. E, A lateral radiograph demonstrates restoration of height andrealignment at the injury level.
905CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 31/69 P 905 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 31/69 P 905 BLACK T

and rigid stabilization in the thoracolumbar, midlumbar,and low lumbar spine.
Laminectomy by itself is never indicated for thetreatment of burst fractures. It cannot relieve the ante-rior neural compression, further destabilizes the spine,and is often associated with an increase in neurologicdeficit.16, 28, 30
Flexion-Distraction Injuries
Flexion-distraction injuries are characterized by disruptionof the posterior and middle columns of the spine intension, whereas the anterior column usually remainsintact and acts as a hinge. The decision to performnonoperative rather than operative treatment dependsprimarily on whether this injury is through bone, asoriginally described by Chance44 (Denis type A), orwhether it also involves significant ligamentous injuries, asseen in atypical Chance fractures (Denis types B, C, andD). A Chance fracture extending only through bone has anexcellent prognosis for healing, although it may beunstable early and difficult to hold in anatomic reductionwithout surgery. Injuries with significant ligamentousdisruption tend to heal in a less predictable fashion andshould be considered unstable both acutely and chroni-cally.
Nonoperative care of a patient with a seat belt injurythrough bone may consist of bedrest for 2 weeks or longer,followed by mobilization in a total-contact TLSO moldedin hyperextension. This orthosis is best molded with thepatient in the prone position or supine on an extensionframe. The patient should be instructed to wear the TLSOand participate in activities as tolerated while wearingthe brace. Frequent evaluation with radiographs taken inthe standing position should be made to ensure that the
deformity has not progressed. After 3 to 4 months, thelevel of injury should be assessed for excess motion withflexion-extension radiographs obtained out of the brace. Ifnonoperative treatment has failed to produce a stable spinewith minimal deformity, surgical treatment consisting ofposterior fusion with a compression system is indicated.Even if treatment is performed late after the injury, thechance of obtaining successful fusion and satisfactoryalignment of the spine is good. Alternatively, early fixationwith compression instrumentation can be considered iffracture-ligament stability or patient compliance is aconcern.
If a seat belt injury is to be treated operatively, aposterior compression system is generally used. Thesystem often needs to extend only one level above and onelevel below the disruption if the laminae are intact.Hook-and-rod or pedicle screw systems can be used.Positioning the patient in the prone position withsupport under the chest and pelvis can often anatomi-cally reduce the fracture. The Luque rod system withsegmental wires is not indicated because it is less able toresist forward flexion unless many levels above and belowthe injury are included in the construct. Anterior decom-pression is not usually appropriate or necessary (unless alarge disc herniation is present at the level) because itremoves the last intact column and further destabilizes thespine.
Fracture-Dislocations
In fracture-dislocations, all three columns of the spine aredisrupted. These injuries have the highest incidence ofneurologic deficit, and most patients should be treatedsurgically. If a fracture-dislocation is present and thepatient is neurologically normal, surgery is performed to
FIGURE 30–34. This 24-year-old man was a victim of a fall from a height that resulted in a fracture-dislocation at L1–L2 and a complete spinal cord injury.A, An anteroposterior radiograph highlights the malalignment at L1–L2 with a significant rotatory component and lateral slip at this level. B, A lateralradiograph confirms the displacement with forward subluxation and overlap at L1–L2. C, A computed tomographic scan through L1–L2 highlights thedisplacement and malalignment resulting in significant canal compromise and spinal cord injury.
906 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 32/69 P 906 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 32/69 P 906 BLACK T

A a b
B a b c
C a b
FIGURE 30–35. Denis’ classification of fracture-dislocation of the spine. A, Type A is a flexion-rotation injury occurring either through bone orthrough the disc. All three columns of the spine are completely disrupted, usually with the anterior longitudinal ligament being the only intactstructure. Commonly, this ligament is stripped off the anterior portion of the vertebral body below. These injuries are usually associated with fracturesof the superior facet of the more caudal vertebra. B, Type B is a shear injury. The type that produces anterior spondylolisthesis of the more cephaladvertebra usually fractures a facet, and that causing posterior spondylolisthesis of the more cephalad vertebra normally does not cause a fracture of the facetjoint. C, Type C is bilateral facet dislocation. This injury is a flexion-distraction injury but with disruption of the anterior column in addition to theposterior and middle columns. This disruption through the anterior column may occur through either the anterior intervertebral disc or the anteriorvertebral body.
907CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 33/69 P 907 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 33/69 P 907 BLACK T

A B C
FIGURE 30–36. Comprehensive classifi-cation of spine injuries. Type A (A) isvertebral body compression. Type B (B) isanterior and posterior element injury withdistraction. Type C (C) is anterior andposterior element injury with rotation.(Redrawn by permission from Gertzbein,S.D. In: Gertzbein, S.D., ed. Fractures ofthe Thoracic and Lumbar Spine. Balti-more, Williams & Wilkins, 1992.)
A1 A2 A3
FIGURE 30–37. Comprehensive classi-fication of type A spinal injuries. Thethree categories of type A fracturesinclude impaction injuries (A1), ofwhich wedge fractures are most com-monly seen; split fractures (A2), ofwhich a pincer fracture is the typicalinjury; and burst fractures (A3). (Re-drawn by permission from Gertzbein,S.D. In: Gertzbein, S.D., ed. Fracturesof the Thoracic and Lumbar Spine.Baltimore, Williams & Wilkins,1992.)
B1 B2 B3
FIGURE 30–38. Comprehensive clas-sification of type B spinal injuries.Flexion-distraction injuries can resultin disruption of soft tissues posteri-orly through the capsule of the facetjoints (B1) or through the bony arch(B2). If distraction and extensionoccur, anterior disruption throughthe disc may often be seen (B3), withor without associated fractures or softtissue injuries of the posterior ele-ments. (Redrawn by permission fromGertzbein, S.D. In: Gertzbein, S.D.,ed. Fractures of the Thoracic andLumbar Spine. Baltimore, Williams &Wilkins, 1992.)
908 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 34/69 P 908 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 34/69 P 908 BLACK T

stabilize the spine and prevent the occurrence of aneurologic deficit while allowing the patient to bemobilized. If a fracture-dislocation is present and thepatient has an incomplete neurologic deficit, surgeryshould be performed to stabilize the spine and decompressthe neural elements. If a fracture-dislocation is present andthe patient has a complete neurologic deficit, surgeryshould be performed to stabilize the spine, shorten thehospital stay, minimize the need for rigid externalimmobilization, and maximize the patient’s potential forrehabilitation.
The surgical management of fracture-dislocations variesaccording to the type of injury. If the patient is neurolog-ically normal or has an incomplete neurologic deficit, it isbest to intubate and turn the patient to the prone positionwhile still awake. The patient’s muscle tone helps stabilizethe spine during turning, and the patient can be quicklymonitored after turning to make certain that neurologicfunction is unchanged. Most patients do not find thismaneuver particularly distressful, provided that they areinformed of it in advance. It makes the turning andpositioning maneuvers safer than logrolling an anesthe-tized patient with a spinal column injury and no inherentability to protect the cord. After positioning has beencompleted and neurologic assessment has been performed,the patient may be anesthetized.
In both flexion-rotation and flexion-distraction injuries,the anterior longitudinal ligament most often remainsintact. These injuries can be reduced with the use of any ofthe previously described distraction systems. If overdis-traction occurs, a shorter central compression systemacting as a tension band can be used between the twodistraction rods, with the system spanning one level aboveto one level below the fracture-dislocation. In many cases,a double-looped 1.20-mm wire passed around the spinousprocesses can prevent overdistraction. In the case offlexion-rotation injury, a compression system by itselfcannot usually provide anatomic realignment. However,with a flexion-distraction injury, it allows excellent fixationand stabilization of the injury. Conversely, in flexion-rotation or flexion-distraction injuries with jumped facets,distraction may be applied to reduce the dislocation. Afterreduction has been achieved with the distraction system, aneutralization system with a plate and screws can be used
to hold the reduction while the distraction component isremoved. The Luque instrumentation system is secureenough to maintain reduction in a flexion-rotation injury,but it may be difficult to achieve anatomic reduction withthis technique because the system does not allow applica-tion or maintenance of distraction. The use of rigidsegmental fixation systems allows better stabilization inthis type of injury.
Shear injuries are the most unstable of the injuriesbecause all three columns are disrupted and all supportingligaments are completely torn.60 Overdistraction is acommon occurrence. The combination of long distractionwith short compression should be considered. An alterna-tive is to reduce these injuries with long distraction andshort local compression, followed by fixation with aplate-and-screw system extending two levels above andtwo levels below the injury. The distraction and compres-sion instrumentation can then be removed. A segmentalclaw with transverse fixation devices or pedicle screws isalso useful. Another possibility is to achieve reduction,again with distraction and compression systems, and thenfix the reduction in situ with Luque rods and segmentalwires. All these approaches provide excellent stability andallow postoperative mobilization of the patient, usuallywith a TLSO.
Primary acute anterior decompression rarely has a rolein fracture-dislocations because the main problem in theseinjuries is usually stability and malalignment. Realignmentby itself frequently decompresses the compromised neuralelements. Anterior decompression may be used in con-junction with posterior instrumentation if adequate de-compression cannot be achieved. This option is particu-larly important in a patient with a partial neurologicdeficit.253
Soft Tissue Injuries
Soft tissue injuries (grades 1 and 2 sprains) involving thethoracic and lumbar spine without complete ligamentousdisruption are diagnosed by exclusion after obtaining adetailed history, performing a thorough physical examina-tion, and ordering appropriate tests. Treatment is symp-tomatic, as for soft tissue injuries that occur elsewhere in
C1 C2 C3
FIGURE 30–39. Comprehensive clas-sification of type C spinal injuries.The common feature of these injuriesis rotation associated with compres-sion (C1), distraction (C2), or rota-tional shear (C3). (Redrawn by per-mission from Gertzbein, S.D. In:Gertzbein, S.D. ed. Fractures of theThoracic and Lumbar Spine. Balti-more, Williams & Wilkins, 1992.)
909CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 35/69 P 909 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 35/69 P 909 BLACK T

the body. Standard physical therapy measures coupledwith short-term bedrest may prove helpful, if necessary, torelieve symptoms. Provided that structural integrity ispresent, gradual mobilization of the patient should beencouraged. The use of analgesics is appropriate, and theuse of nonsteroidal anti-inflammatory drugs may alsoshorten the course of disability and decrease symptoms.Two treatment options to be avoided are prolonged rigidimmobilization and chronic use of narcotic analgesics.
If symptoms of the soft tissue injury persist, the patientshould be reevaluated with the use of plain radiographswith flexion and extension lateral views. If results arenegative, a bone scan or MRI may be performed to rule outan occult spinal fracture or ligamentous injury. If any areais abnormal in the bone scan or MRI, a thin-section CTscan with reconstructions should be obtained. Addition-ally, if the symptoms warrant, MRI can be performed torule out disc herniation or other soft tissue injury.
Disc Injuries
High-energy injuries of the intervertebral discs in thethoracic and thoracolumbar spine are uncommon, butthey can be a significant source of morbidity and causepain or even paralysis. Disc herniations down to theT12–L1 and sometimes the L1–L2 interspaces can involvespinal cord compression, whereas in disc herniationsbelow these levels, compression is limited to the caudaequina. As stated previously, the spinal cord is moresusceptible to injury and less likely to recover onceinjured. This discussion is limited to disc herniations inthe thoracic and thoracolumbar regions.
The classification of disc herniations in the thoracicspine is the same as for herniations in the low lumbarspine. Disc abnormalities are defined as bulging, pro-truded, extruded, or sequestered. A bulging or protrudeddisc is defined as an injury in which the nucleus pulposusmigrates posteriorly but remains confined within theanulus fibrosus. With an extruded disc, the nucleuspulposus ruptures through the anulus fibrosus but is stillconfined anterior to the posterior longitudinal ligament.When a disc is sequestered, the nucleus pulposus hasruptured through the anulus fibrosus, as well as theposterior longitudinal ligament, and lies within the spinalcanal. The thoracic and thoracolumbar regions of the spineare less tolerant than the lumbar spine of any of these discabnormalities. Even a protruded intervertebral disc may besymptomatic because the spinal canal is narrower than inthe cervical and low lumbar regions and the thoracic cordis more susceptible to pressure because of the limitedvascular supply and small space.
Though significantly less common, limbus fractures ofthe lumbar vertebrae must be considered in the differentialdiagnosis of any adolescent or young adult thought to havea traumatic herniated nucleus pulposus. Fracture of thelumbar vertebral limbus consists of a fracture of theperipheral apophyseal ring from either the posterosuperioror the posteroinferior aspect of the vertebra, and thesymptoms are similar to those seen with a herniatednucleus pulposus. Although they were originally thoughtto occur exclusively in the pediatric population, a number
of studies have shown the existence of fragmented,unfused apophyseal rings in adults. Epstein and Epstein88
reported on 27 patients who sustained limbus vertebralfractures at an average age of 32 years and a rangeextending to 44 years of age. Treatment of these lesions isby surgical excision.
Symptoms of thoracic and thoracolumbar disc hernia-tion include pain, paresthesias, and neurologic deficits.The pain may be local and axial at the level of injury, or itmay be radicular in nature, with radiation to the flank,along a rib, or down toward the groin if the disc herniationis at the thoracolumbar junction. Less commonly, painmay involve all areas distal to the spinal cord compression.When this type of dysesthetic pain occurs, significantneural compression and weakness are usually present.
Neurologic findings can include a wide-based, ataxicgait. Sensation may be decreased either in a radiculardistribution or in a distribution involving all regions distalto the level of spinal cord compression. Weakness may bepresent and may follow any of the patterns of spinal cordsyndromes, from a central cord or Brown-Sequard syn-drome to an anterior cord syndrome. On occasion,complete paralysis may also be associated with thoracic orthoracolumbar disc herniation. In addition, abnormalfindings related to rectal tone, perineal sensation, andbladder function may be observed. Subtle changes may bedetected with cystometric evaluation. The reflexes mayrange from normal in patients with minimal spinal cordcompression to marked hyperreflexia with a positiveBabinski sign in patients with significant spinal cordcompression.
Thoracic disc herniation can be detected by MRI (seeFig. 30–52), myelography, or myelography followed by CTscanning (which has the added advantage of demonstrat-ing spinal cord deformity at the level of the discherniation). A CT scan alone is not usually adequate todemonstrate thoracic disc herniation or accurately assessthe extent of spinal cord compression. Plain radiographsare seldom diagnostic. Plain films can, however, be helpfulif the patient has Scheuermann’s disease because thoracicdisc herniation is more likely to develop in these patients.
Appropriate treatment of thoracic and thoracolumbardisc herniation is surgical, provided that the herniation isassociated with incapacitating pain or abnormal neurologicfindings. Surgical approaches to treatment of disc hernia-tion in this region include anterior transthoracic discec-tomy (see Fig. 30–52) with or without fusion, posterolat-eral decompression from a transpedicular approach, and acostotransversectomy approach. Standard laminectomyshould not be used to remove a thoracic or thoracolumbarherniated disc. Because spinal cord manipulation isrequired to remove a disc through a standard posteriorlaminectomy, worsening of the neurologic condition canoccur and has been reported in up to 45% of patientstreated with this approach. The results reported for theanterior transthoracic, costotransversectomy, and postero-lateral transpedicle approaches all show that 80% to 90%of patients improve after surgery, with the remainder beingwithout change or deterioration.83, 170, 187, 216, 219 Becausethe condition is traumatically induced, internal fixationand fusion should be considered, concurrent with thediscectomy.
910 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 36/69 P 910 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 36/69 P 910 BLACK T

Bohlman and Zdelblick31 reviewed 19 patients treatedsurgically for thoracic disc herniation; 8 were treated witha transthoracic approach, and the remaining 11 weretreated with a costotransversectomy approach. Theyconcluded that the transthoracic approach was preferablebecause it greatly improved visualization of the pertinentanatomic structures, including the disc and the neuralelements. All seven patients with paralysis improved afteranterior transthoracic decompression.
Thoracoscopy has been used as a diagnostic tool formany years. It has been successfully used in complexsurgical procedures, including thoracic discectomy. Thepotential benefits of video-assisted thoracoscopic surgeryinclude reduced postoperative pain, improved early shoul-der girdle function, and a shorter hospital stay.171 Reganand associates reported on video-assisted thoracoscopicsurgery performed on 12 thoracic spinal patients, includ-ing 5 discectomies.227 Postoperative CT scans showedadequate spinal cord decompression, and pain wasrelieved in all patients. Huntington and associates under-took a randomized comparison of 30 thoracoscopic and30 open thoracic discectomies for anterior spinal fusion ina live sheep model.137 Their data showed no significantdifference in the amount of disc end-plate resectedbetween the two techniques.
OPERATIVE TREATMENTz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Selection of the instrumentation and type of construct isnot random, nor should it be based entirely on thepreference of the surgeon. All systems have relativestrengths and weaknesses that can be used to advantage.The optimal system and construct for a given fractureshould counteract the deforming forces and maximallydiminish the degree of instability. For example, burstfractures are caused by flexion and axial loading forces, socorrection of deformity and restoration of stability are bestachieved by a system that can impart extension anddistraction. Therefore, neither a Harrington rod nor Luquesegmental instrumentation is optimal for these fractures;the use of segmental fixation with multiple hook or screwfixation is preferable.
Hook-Rod Systems
The Harrington rod system was one of the first rod-hooksystems to treat fractures in the thoracic and the lumbarsegments of the spine.1, 28, 95, 127, 177, 225, 279 Although ithas allowed fracture reduction and spine stabilization, aswell as early rehabilitation, it has little intrinsic stabilityand is mentioned here primarily for historical purposes.*
Reduction of anterior vertebral body fractures isdependent on both distraction and extension (lordotic)forces created by the rods and hooks (see Figs. 30–22 and30–32). With contouring, the rods must achieve three- orfour-point fixation to provide force vectors that pull
posteriorly at the hook sites cephalad and caudad to theinjury while constantly pushing anteriorly toward thefractured vertebra through the lamina and pedicles, eitherat or above and below the level of injury. These vectors areachieved at the expense of increased force at the hook-laminar junction with the use of square-ended Moe rods.61
This three- or four-point fixation translates to vector forcesthat reduce the vertebral body fracture deformity anteri-orly and close the disruption posteriorly. The distractionrod can be used successfully to stabilize and reduce burstfractures, fracture-dislocations, and compression fractureswith associated posterior element disruption. They mayalso be appropriate in flexion-distraction injuries that havea burst component associated with the vertebral bodyinjury. In the latter case, placement of a tension band(spinous process wires or laminar compression rod) maybe necessary posteriorly before application of the distrac-tion force.96
Compression rods fixed to hooks around the laminahave been shown to provide a stronger construct thanpossible with distraction systems when tested againstflexion loading,263 although some authors disagree.222, 242
Rod-hook distraction systems tend to fail by dislodgmentat the rod-hook junction, at the hook-lamina junction, orat the ratchet-rod junction. Compression rods, perhapsbecause they better resist flexion and rotation forces,contribute to failure by fracturing the lamina to which thehooks are attached.82, 170
Many varied recommendations have been made regard-ing the number of spinal segments to instrument, thenumber of spinal segments to fuse,45 and whether theinstrumentation should be removed after the spinal injuryhas healed. Early recommendations were to apply instru-mentation from three levels above the injury to two levelsbelow the injury, fuse all the intervening segments, and notremove the instrumentation unless specific problems oc-cur.66 The optimal length should be determined by thelength of the lever arm necessary to achieve the reduction.14
Rod Sleeve Distraction Instrumentation
The Edwards instrumentation system, which was initiallydesigned for treating spinal trauma, used ratcheteduniversal rods with an outer diameter similar to that of theHarrington distraction rods but with a large core diameter;the system could be used for either distraction orcompression. It is combined with polyethylene rod sleevesand an improved anatomic hook in three sizes rather thanthe standard curved Harrington hooks.79–81, 83, 176
Most burst fractures result from varying degrees of axialcompression and flexion, and the two components of theEdwards system allowed individual adjustment of distrac-tion and extension forces to correct the deformity. The rodprovided distraction across the fracture site, which in mostcases restored vertebral and disc height. The rod sleeves (inthree sizes) were used to generate the central, anteriorlydirected force vector to allow for sagittal plane reduction(Fig. 30–40). Sagittal-plane correction was better thanwith other posterior instrumentation systems because therod sleeves allowed some continued postoperative increasein reduction by gradual accommodation to the spine’s
*See references 1, 51, 67, 71, 72, 96, 101, 142, 143, 145, 152, 200,225, 231, 242, 251, 263.
911CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 37/69 P 911 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 37/69 P 911 BLACK T

normal viscoelastic creep and by constant tensioning of theanterior longitudinal ligament through interoperative bow-ing of the rods within their elastic range.47 In addition, thesleeves produced increased rotational stability by securelywedging between the spinous process and the facet joints.Such wedging improved the overall rotational rigidity ofthe system in comparison to other rod-hook systems.
The results of use of the Edwards system for fracturemanagement in 135 patients treated at a single centerwere reported by Edwards and Levine.81 Postoperativefollow-up results at 1 to 4 years and at 6 to 10 years werereported in 122 of these patients. After partial reductionwith the use of transverse rolls on a Stryker frame,preoperative deformity averaged 14° of kyphosis, 8 mm ofdisplacement, and 68% loss of vertebral body and discheight. The initial study included 61 patients withincomplete paralysis, 41 with complete paralysis, and 33who were neurologically normal. The immediate postop-erative kyphosis was reduced from 14° to −1° (±4°). Atlate follow-up, the kyphosis had increased to 0.5° (±5°).
Vertebral height was restored from 68% preoperatively to96% in the immediate postoperative period and was 90%(±8%) at late follow-up. Translation was similarly reducedfrom 8 mm preoperatively to 0.8 mm (±1.5 mm)immediately after surgery and at late follow-up. For thelast 32 cases in this series, preoperative and postoperativeCT scans of the spinal canal area were performed at thelevel of injury, and findings were compared with those forthe adjacent normal levels. For injuries treated within 2days, rod sleeve reduction increased the canal area from55% to 87% of normal. If surgery was performed between3 and 14 days after injury, the canal area was increasedfrom 53% to 76% of normal.81
Segmental Instrumentation Systems
The use of segmental fixation instrumentation systems hasimproved the treatment of spinal deformities such askyphosis and scoliosis.51 The primary advantage of these
FIGURE 30–40. This 53-year-old man was involved in a motor vehicleaccident and sustained an unstable fracture of his spine. A, A lateralradiograph shows compression of the T10 vertebral body. B, A sagittalcomputed tomographic (CT) reconstruction shows propagation of thefracture through the posterior elements at T9. C, A CT scan through T10reveals a comminuted fracture through the body and posterior elements.The patient was neurologically intact, possibly as a result of disruption ofthe posterior ring, which provided decompression of the canal. CT viewsabove and below T10 revealed laminar fractures at T8 and T9 superiorlyand at T11 inferiorly. D, A postoperative anteroposterior radiographshows stabilization with an Edwards distraction system. Bridging sleevesare positioned superior and inferior to the first intact laminar levels toavoid the fractured posterior elements. E, A lateral postoperative filmconfirms proper positioning of the sleeves over the superior facet points,with realignment and restoration of height at T10. Because of the longinstrumentation, transverse loading devices were used to link the rodsand help solidify the construction.
912 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 38/69 P 912 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 38/69 P 912 BLACK T

systems is that multiple hooks and pedicle screws can beused in both distraction and compression modes, therebyallowing correction of complex deformities and providingstability while maintaining normal sagittal contours. Thissystem is further strengthened with the use of transversetraction devices to convert the system to a rigid rectangle46
(see Figs. 30–25, 30–44, and 30–47). With these systems,increased stability is obtained without the apparentincreased risk of neurologic damage reported with theLuque sublaminar wiring technique.
The role of segmental fixation in the treatment of spinaltrauma continues to evolve. One disadvantage is that thesurgical time required to insert the instrumentation may beslightly greater than with distraction rod systems, espe-cially early in the surgeon’s experience. A second disad-vantage is that a moderate amount of manipulation isrequired when connecting multiple hooks to rods whilesimultaneously reducing the unstable spinal injury. Oneadvantage of segmental fixation is that under certaincircumstances postoperative bracing may be eliminated(especially in the thoracic spine) without jeopardizing thestability and eventual healing of the fusion. Anotherpotential advantage is that these techniques may allowshorter instrumentation length, thus immobilizing fewersegments.222, 272, 280–283
The pattern of hook placement varies from author toauthor, but a few general principles for the constructs maybe used in most cases (Fig. 30–41). Cephalad, a clawconfiguration either at a single level or at adjacent levels isthe mainstay of most constructs (Fig. 30–42). Manydifferent recommendations have been made regarding thelength of instrumentation and configuration of the hooksand pedicle screws. Shufflebarger (personal communica-tion) recommended that the lever arms be of equal lengthabove and below the fracture and stressed the use of adouble lamina claw at both the rostral and caudal extremesof instrumentation. Although in the thoracic spine hewould not hesitate to extend fixation to three levels aboveand two levels below the injury, at the thoracolumbarjunction, he recommended instrumentation two levelsabove and one level below the fracture. However, a shortconstruct should not be used unless the comminution ofthe anterior column is minimal or anterior stability isrestored with a strut graft.
A minimum of three hooks must be used on each rodproximal to the fracture, whether in the thoracic area or atthe thoracolumbar junction. The construct may consist ofat least one single-level claw plus an additional pediclehook below it (augmented claw) or two single-level clawsspaced one segment apart. A bilaminar claw must beplaced distal to the fracture because distal single-levelclaws fail 20% of the time as a result of laminar fracturescaused by the huge force placed on that single level.203 Ifa single-level distal claw is used, it must be augmentedwith an anterior strut.
The claw provides significantly increased holdingpower over a single upgoing hook, thereby allowinggreater potential for correction of deformity while decreas-ing the rate of instrumentation failure. Another advantageof segmental fixation over single hook-rod systems is theability to provide both distractive and compressive forcesover the same construct and thus allow maintenance of
normal sagittal contours. In general, compression main-tains lumbar lordosis, and distraction is used to maintainthoracic kyphosis.197
Pedicle screws placed either above or below a vertebralbody fracture can be used like the rod sleeves of theEdwards system to generate a central, anteriorly directedforce vector to assist in maintaining or creating sagittal-plane reduction (Fig. 30–43).
In fractures at the thoracolumbar junction, where thepedicles are relatively large, a construct of all pediclescrews may be considered. In fractures occurring in thelower thoracic spine, a combination of hooks cephalad tothe fracture and pedicle screws below the fracture may beused. In fractures occurring in the middle and upperthoracic spine, hook constructs are most commonly used.Pedicle screws used in this manner, with adequate fixationabove and below with either a claw configuration oradditional pedicle screws, can improve the overall rigidityof the system and maintain the reduction until fusionoccurs. When treating significant burst fractures withposterior instrumentation, it is important to look at thebiomechanical implications. In a mechanical study byDuffield and colleagues, it was concluded that single-levelposterior instrumentation adjacent to a comminutedsegment will have a finite fatigue life and that anteriorcolumn support equivalent to a healthy motion segmentcan reduce the internal bending moments within animplant to levels that have a low probability of causingfatigue of the implant. They also showed that instrumen-tation of two levels adjacent to a comminuted vertebra asopposed to a single level will reduce the flexion bendingmoment in the implant. These results illustrate the clinicalneed to create load sharing when possible and to selectimplants capable of maintaining reduction and supportingthe spine until fusion has occurred.72 Other studies haveshown the importance of transfixing these constructs withcross-connectors. In a mechanical study of transpedicularspine instrumentation, Carson and associates showed thattransfixing bilevel constructs stabilizes them to all modesof loading and will reduce the excessive increase ininternal components of force and moment associated withlinkage instability.43
Akbarnia and colleagues5 reviewed 67 patients withthoracic and lumbar spine injuries treated at two differentcenters; the range of follow-up was 3 to 26 months.Thirty-nine of these patients had injuries between T11 andL2. Most had instrumentation extending over five to eightvertebral levels, with an average of 10 hooks or screws perpatient. The degree of preoperative and postoperativekyphosis and canal compromise was not detailed in thisreport. The authors stated that alignment was maintainedin 65 patients throughout the duration of follow-up.Fusion was definitely achieved in 31 patients, and twopseudarthroses were performed. It was too early to assessfusion status in the remaining 34 patients. No patient wasneurologically worse after surgery. Complications includedtwo deep wound infections. Hook dislodgment or screwpull-out occurred in five patients, although all five hadfusion at follow-up. In the thoracic spine, these authorsrecommended instrumentation three levels above andthree levels below the injured segment, with claws at theextremes of instrumentation and segmental fixation at the
913CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 39/69 P 913 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 39/69 P 913 BLACK T

intervening levels. In the thoracolumbar spine theyrecommended that fusion extend three levels above andtwo levels below the fracture. In the lumbar spine theysuggested extending the fixation two levels above and onelevel below the injured segment. For both thoracolumbar
and lumbar hook arrangements they recommended thatdouble claws be used superiorly but had varied recom-mendations for the caudal spinal fixation.
Stambough260 reported on 55 patients treated withCotrel-Dubousset instrumentation by a single surgeon,
A
T4
T5
T6
T7
T8
T9
TP/PL
P
P
L
P C
T10
T11
T12
L1
L2
L3
TP/L
P
P
L
LB
T6
T7
T8
T9
T10
T11
L
P
TP
L
P
E
T10
T11
T12
L1
L2
L3
PS
PS
PS
PSD
T10
T11
T12
L1
L2
L3
TP/L
TP/L
L/PS
PS
FIGURE 30–41. Hook and screw placement patterns used with rigid segmental instrumentation systems for the treatment of thoracic and thoracolumbarspine injuries. A, T7 fracture. The instrumentation used is a claw configuration above and below the injury. For a very unstable injury pattern, pediclehooks may be added one level above the injury. B, T9 fracture. An alternative hook pattern can be used in low thoracic fractures. A unilaminar claw isformed with hooks over the top of the transverse process and a pedicle hook at the same level to create a single-level claw, which is then reinforced witha single upgoing hook at the adjacent level to place the upper portion of the construct in two levels rather than three. C, L1 burst fracture. A constructsimilar to that in A may be used. Note that below T10, pedicle hooks are replaced by cephalad-facing lamina hooks. D, In the lumbar spine, where thepedicles are large enough, screws may be substituted for hooks, with the addition of cephalad lamina hooks placed at the distal end of the construct foradditional stability in highly unstable injury patterns. E, Another construct consisting of pedicle screws two levels above and below the fracture to providestability in all planes. Abbreviations: L, lamina hook; P, pedicle hook; PS, pedicle screw; TP, transverse process hook.
914 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 40/69 P 914 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 40/69 P 914 BLACK T

A
D
B
CFIGURE 30–42. Claw configurations used for proximal and distal fixation in rigid segmental instrumentation systems. All these constructs may be usedat single levels or two adjacent levels. A, Transverse process hook with a pedicle hook claw. B, Superior lamina hook with a pedicle hook claw. C,Supralaminar and infralaminar hook claw, useful below T10 where application of pedicle hooks is not recommended. D, Pedicle screw with an infralaminarhook; this is useful in the lumbar spine, where pedicles are large enough to accept pedicle screws. (A– D, Redrawn from Bridwell, K.H.; DeWald, R.L.,eds. The Textbook of Spinal Surgery. Philadelphia, J.B. Lippincott, 1991.)
FIGURE 30–43. This 30-year-old woman was involved in a motor vehicleaccident and sustained a T12 burst fracture without neurologic deficit.A, An anteroposterior radiograph shows minimal loss of height withwidening of the pedicles. B, A lateral radiograph shows approximately30% loss of height and local kyphosis of 8°. The patient was treatedinitially with bedrest and a thoracolumbosacral orthosis. C, Two weeksafter the injury, a repeat lateral radiograph shows greater than 50% lossof height and local kyphosis of 25°.
Illustration continued on following page
915CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 41/69 P 915 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 41/69 P 915 BLACK T

with an average of 48 months’ follow-up. No instances offailure of instrumentation or pseudarthrosis formationwere reported in his series. At final follow-up, deteriora-tion in alignment was minimal in comparison to theimmediate postoperative period.
Argenson and co-workers reported their results in 65patients treated for thoracic or lumbar spine fractures witha follow-up of 6 months or longer.13 They recommendedthat instrumentation extend three levels above and twolevels below the injured segment in the thoracic spine andthe use of pedicular or double laminar hooks (claws) at theextremes of instrumentation with varied intermediateconnections. Forty-nine patients had fractures from T11 toL2. Argenson and co-workers initially extended theinstrumentation two levels above and two levels below thefracture with the use of hooks only and obtainedsatisfactory early results. With shortening of the instru-mentation, they noted considerable problems (e.g., loss offixation in two patients and loss of reduction in fourothers). Their current recommendations are to use pediclescrews one level above and one level below the level offracture, accompanied by pedicle or laminar hooks twolevels cephalad to the fractured vertebra and at the same
level as the caudal pedicle screws. In 12 patients treated inthis fashion, 1 had considerable loss of reduction as aresult of sepsis, whereas the others averaged only 4.3° lossof reduction at follow-up. The earlier results of this groupwith the use of only hooks or only screws resulted in anaverage loss of reduction of 8.6°.
Graziano118 reported his results in 14 patients forwhom he used lumbar pedicle screws and thoracicpedicle–transverse process hook claws in a hybrid Cotrel-Dubousset construct. The pedicle screw fixation was usedone level below the injured segment. Graziano reportedbreakage of only one screw, and increased kyphosisdeveloped in one patient after surgery. This constructoffers the advantages of short-segment fixation in thelumbar spine, where motion preservation is important,while providing a longer fixation span above the level ofinjury, which helps add rigidity to the construct.
In the lumbar spine, Argenson and co-workers13
recommended the use of short instrumentation andpedicle screw fusion one level above and one level belowthe injury, combined with a sublaminar hook at theinferior extent of the instrumentation. Twenty patientswere treated in this fashion, and the average loss of
FIGURE 30–43. Continued. D, The patient was treated operatively withposterior segmental instrumentation with a claw at T9 and pediclescrews at T11 and at L1 and L2. E, A lateral radiograph showsrestoration of height and sagittal alignment at the injury level.
916 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 42/69 P 916 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 42/69 P 916 BLACK T

correction in the first 15 patients was 9°. Even though thisloss of reduction seems significant, the final lordosis at thelevel of injury was −4°, which is very close to normalphysiologic alignment. Complications in this series in-cluded partial fixation loosening in three, broken screws infour, and postoperative infection in eight patients. Theauthors attributed this high infection rate to the increasedduration of surgery associated with the learning curve ofthe surgeon.
Suk and associates265 reviewed their treatment of 18lumbar fractures, including 5 fractures of L1, 2 fractures ofL2, and 1 fracture of L3. They used pedicle screws forfixation, and their average instrumentation extended overtwo segments. This technique contrasts with their previousexperience of using segmental wiring in combination withHarrington distraction rods that spanned almost sixsegments. They found a postoperative kyphosis angle of3.2° with the use of Cotrel-Dubousset instrumentation ascompared with 4.3° for segmentally wired Harringtonrods. Because the follow-up period was longer than 4months in only 11 patients, these results must becategorized as preliminary. McBride recommended thatwhen instrumentation is to be extended to L5, the fusionshould be stopped short (at L4) and the hardware removed9 to 12 months later, as with the ‘‘rod long, fuse short’’technique with Harrington rods.197
The appropriate length of instrumentation was ad-dressed by McKinley and colleagues202 in a review of onlyseven patients monitored for more than 24 months afterCotrel-Dubousset pedicle instrumentation with screws onelevel above and one level below the fractured vertebra.They observed an average loss of 18° of correction (rangeof 8° to 26°) and a significant incidence of screw breakagerequiring reoperation. They concluded that patients withsignificant injury to the anterior and middle columns ofthe spine require anterior corpectomy and fusion toprevent this type of late deterioration if short-segmentCotrel-Dubousset instrumentation with screw fixation isused posteriorly. However, the data supporting thisconclusion were limited, but a similar conclusion was alsoreached by Gereesan.109
Fabris and co-workers reported their results withCotrel-Dubousset instrumentation on nine cases of seatbelt–type injuries of the thoracolumbar spine.90 They useda short compression construct spanning only a singlemotion segment and reported excellent maintenance ofcorrection of deformity and no instrumentation failure.Benzel also described the use of short-segment compres-sion instrumentation for the treatment of burst fracturesafter first reconstructing the vertebral body with a strutgraft.23 The construct consisted of a claw above and a clawbelow the injured segment. It spanned significantly fewermotion segments than typical of traditional constructswhile still maintaining excellent correction of deformity(<2° loss of correction at last follow-up). They noted thatshort constructs functioned best in compression andwarned that short distraction constructs tended to failover time.
In these studies, the recommendations concerningpostoperative use of a TLSO are variable. Akbarnia andcolleagues6 recommended the use of a brace if the patienthad osteoporotic bone or at surgery received less than a
double laminar claw, or its equivalent, both proximally anddistally. Thirty-six of their patients had no immobilization,and 31 used a TLSO or other brace for an average of 4months. Argenson and co-workers13 did not recommendthe use of a postoperative brace for any of their patients,whereas Suk and associates265 treated all their patientswith a postoperative TLSO. In general, the shorter thefixation and the less secure the spine-implant interface, themore likely the authors were to recommend postoperativeTLSO immobilization.
SURGICAL TECHNIQUE
With the patient in the prone position, a midline incisionis made and extended one level further both proximallyand distally than the expected length of instrumentation.The most frequently recommended scheme for instrumen-tation includes fixation two levels above and one levelbelow the injury. Shorter instrumentation is desirable inthe lumbar spine if possible, but it is not as physiologicallyimportant to limit the levels of instrumentation in thethoracic spine.
The construct described is based on a claw configura-tion on the lamina two levels above and one below thelevel of injury (see Figs. 30–41 and 30–43). For the hooksfacing caudad, a laminotomy is performed just cephalad tothe lamina so that the hooks may be placed around thelamina under direct vision. For the hooks directedcephalad, a ligamentum flavum stripper should be in-serted beneath the lamina to prepare the site for hookplacement. In the thoracic spine, thoracic hooks should beused, and in the lumbar spine, lumbar hooks should beused to obtain maximal purchase on the lamina withoutincreasing the chance of neural compression by canalintrusion. The superior portion of the rod should be bentappropriately to conform to the slanting of the lamina inthe sagittal plane and thereby minimize the chance offracture of the lamina and failure of the system. The sameattention should be paid to contouring of the rod at thecaudal lamina.
Additional fixation can be obtained with the use of ahook facing cephalad under the lamina one level abovethe level of injury (see Fig. 30–42A). An alternative tothis system would be the use of instrumentationextending three levels above and two levels below theinjury, along with cephalic and caudal claws. Hooks aredirected cephalad two levels above the level of injuryand caudad one level below the injury. This construct isrelatively safe and extremely rigid. To improve fixation inthe thoracic area, the hooks directed cephalad may bepedicle hooks rather than standard lamina hooks(Fig. 30–44). Additionally, the top hook may be placedon the transverse process, provided that it is of ade-quate size.
Two transverse traction devices should be applied toconnect the rods if space allows. No medial or lateral forceshould be applied to the rods at the time of insertion of thetransverse traction device. The fusion technique shouldinclude decortication of the transverse processes, laminae,and spinous processes within the instrumentation, withcare taken to not weaken any laminae that are directlysupporting hooks.
917CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 43/69 P 917 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 43/69 P 917 BLACK T

Sequential application of segmental instrumentationcan also be used for reduction of dislocations, as well asdefinitive stabilization (Fig. 30–45). A single-rod con-struct is placed in distraction, and distractive forces areapplied until reduction of the dislocation occurs. After thereduction is achieved, the appropriate construct is placedon the contralateral side to stabilize the spine. Finally, thedistraction rod is removed and replaced with a sym-metric construct on the opposite side. Others havedescribed the use of rotational maneuvers, similar to thoseused for correction of scoliosis, to reduce fracture-dislocations.87
For patients treated with instrumentation three levelsabove and two levels below the injury, a circumferentialrigid postoperative brace is necessary. Similarly, wheninstrumentation two levels above and one level below theinjury is used in the lower lumbar spine, where more ofthe weight-bearing forces are carried through the posteriorelements, use of the brace can be eliminated or reduced.The use of a TSLO for mobilization of patients instru-mented two levels above and one level below an injuryat the level of the thoracolumbar junction is advised.In patients with severe anterior comminution andshort posterior instrumentation, anterior corpectomy andstrut fusion will decrease the chance of instrumentationfailure.23, 121, 191, 193
Segmental Sublaminar Wires
The Luque technique was originally used to treat patientswith scoliosis, with the presumed advantage of notrequiring postoperative bracing. It entailed the use of twosmooth, L-shaped stainless steel rods (either 1⁄4 or 3⁄16 inchin diameter) combined with segmental wires. The wireswere made of 16-gauge malleable stainless steel, passedsublaminarly, and twisted around the rods at each level toprovide segmental fixation (see Fig. 30–32). As originallydescribed, no hooks or pedicle screws were used.
This system had two major disadvantages. Manysurgeons noted an increased incidence of neurologicdeficits after passage of the sublaminar wires. Thefrequency of new neurologic deficits decreased as eachsurgeon became more familiar with the technique (thelearning curve).21, 144 This incidence of neurologic deficitalso varied greatly from series to series, from 0% in someto as high as 10% in others.144 Because this increase wasassociated with segmental wiring at the level of the fracturein both cases, these authors recommended against inser-tion of segmental wires in the immediate area of thefracture. The risk of dural impingement may be evengreater during wire removal.116, 210 In 27% of cases,Nicastro and associates210 demonstrated more than 25%canal narrowing with removal of a single wire.
4 mm
3 mm7 mm
4 mm
6 mm
A
C
B
FIGURE 30–44. Placement of thoracic pedicle hooks. A, Appropriate landmarks to remove a piece of inferior articular facet to permit adequate positioningof a pedicle hook. B, A pedicle elevator is inserted into the facet joint, and after engaging the pedicle, placement is checked by moving the vertebra laterallyby lateral translation of the elevator tip. C, The distance between the inferior part of the pedicle and the inferior part of the remaining inferior articularfacet must be equal to the depth of the hook plate from its base to the notch. (A– C, Redrawn from Bridwell, K.H.; DeWald, R.L., eds. The Textbook ofSpinal Surgery. Philadelphia, J.B. Lippincott, 1991.)
918 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 44/69 P 918 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 44/69 P 918 BLACK T

The second major problem with this system was that itwas not able to provide significant axial support to thespine. As originally designed, the L-shaped rods had nomeans to resist sliding axially. Modifications included useof the Harrington outrigger to achieve intraoperativedistraction and, later, modified rods to resist axial collapseby fixation to the lamina and the spinous pro-cesses.8, 71, 92, 93 However, collapse still remains one of themajor weaknesses of this system because the spinousprocesses are the weakest part of the posterior elements.After their prospective study, Ferguson and Allen recom-mended that this system not be used for treating any injuryin which the middle column is disrupted, such as athoracolumbar burst injury, because of the danger of spinalcanal narrowing with axial collapse.92, 93
This inability to provide axial support has been verifiedin laboratory testing. Nasca and co-workers208 instru-mented thoracolumbar swine spines and then subjectedthem to cyclical axial compression loading. The segmen-tally wired L rods allowed three times greater axial
shortening than did Harrington distraction rods (1.5versus 0.5 cm).
To combine the advantages of both systems, a hybridsystem consisting of segmentally wired Harrington distrac-tion rods was developed.100 This system offered theobvious advantage of increased control of translation androtation and maintained an axial distractive force whileminimizing the effect of ligament relaxation and resultanthook cutout (see Fig. 30–32).
Pedicle Screw Fixation Systems
Each of the various pedicle screw fixation systemscurrently in use has different types and sizes of screws,different mechanisms for linking the screws, and differentoptions concerning the ability to compress, distract, orstabilize in situ.*
One of the major advantages of these systems is thatshorter fixation is often possible, frequently with instru-mentation only one level above and one level below theinjured segment (see Fig. 30–18). As discussed previously,the advantages of this short fixation are greatest in thelumbar spine. Fortunately, the larger pedicles allow forsafer placement of pedicle screws in the lower lumbarspine than possible at more proximal levels. Conversely,the benefits of short-segment fixation in the thoracic spineare minimal; one additional level of motion does not affectthe long-term functional results. Proper screw placementin the pedicle is more difficult in the thoracic spine andupper lumbar spine because pedicle size decreases fromcaudad to cephalad.166, 266, 286 In addition, the risk ofserious neurologic deterioration from errant screws isgreater in the thoracic and thoracolumbar spine because ofthe presence of the spinal cord rather than only nerve rootsand rootlets. Vaccaro and co-workers studied 90 screwsplaced in the pedicles of cadaver spines from T4 to T12 byfive experienced spine surgeons.266, 267 They found a 41%incidence of cortical perforation of the pedicle, with 23%of the screws entering the spinal canal. In view of thesepotential risks and benefits, we believe pedicle screwsystems to be most appropriate in the lumbar spine,although they can be used successfully in the thoracicspine when appropriate and when good operative tech-nique is used (Fig. 30–46).
Laboratory data are available for several of thesesystems. Gurr and colleagues121 used a calf spine corpec-tomy model to evaluate different posterior instrumentationsystems in combination with an anterior bone graft. Of thesystems tested, they found that the Cotrel-Duboussetpedicle screw system and the VSP system of Steffee couldbe applied one level above and one level below the defectwith restoration of the spine to original strength in termsof axial loading, forward flexion, and rotation. Thesesystems were significantly superior to the Harringtondistraction system and the Luque segmentally wired L-rodsystem. The limitations of this research, as stated by theauthors, are that the animals were young with uniformly
*See references 3, 4, 6, 22, 52, 54, 55, 57, 64, 65, 67, 79, 108, 109,148, 157, 166, 180, 187, 215, 244, 245, 249, 252, 265, 275, 277,287, 289.
L3
L2
L1
T12
T11
T10
T9
FIGURE 30–45. Use of a unilateral distraction rod for reduction of aT12–L1 fracture-dislocation. Note the placement of the hooks fordefinitive rigid segmental instrumentation on the opposite side of thedistraction instrumentation before application of the distraction. Oncedistraction is achieved, a rod is placed on the opposite side and secured,and then the distraction instrumentation is removed and replaced withrigid segmental instrumentation. If the injury involves disruption of theanterior longitudinal ligament, consideration should be given to place-ment of spinous process wiring at the level of injury before reduction toprevent overdistraction. (Redrawn from Garfin, S.; Northrup, B.E., eds.Surgery for Spinal Cord Injuries. New York, Raven, 1993.)
919CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 45/69 P 919 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 45/69 P 919 BLACK T

FIGURE 30–46. This 50-year-old man fell at work from a height of approximately 16 ft and sustained a T4 burst fracture and multiple posterior elementfractures from C7 to T5. He was neurologically intact. A, A lateral radiograph shows greater than 50% loss of height and local kyphosis. B, A preoperativecomputed tomographic (CT) scan shows approximately 30% canal compromise and disruption of the posterior elements. C, The patient was treatedoperatively with segmental instrumentation involving pedicle screws from T2 to T6. D, A lateral radiograph shows restoration of height and sagittalalignment.
920 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 46/69 P 920 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 46/69 P 920 BLACK T

good-quality bone and the tests were performed immedi-ately after instrumentation, thus allowing no chance toshow the effect of time on loosening or fatigue failure. Inaddition, an anterior bone graft was implanted in eachanimal to provide anterior axial support.
The effect of the rigidity of this instrumentation wasalso investigated in an in vivo animal model.121, 193 Thespine beneath the instrumentation became significantlyosteoporotic, and this effect increased with time. However,the rate and quality of the fusion increased with increasedrigidity of the instrumentation.
The proper length of screw penetration was investigatedby Krag and co-workers.164 Although most of the resis-tance to pull-out is achieved within the pedicle, increasingthe penetration into the vertebral body from 80% to 100%(up to the anterior vertebral cortex) increased resistance toflexion by 54% and to torsion by 24%. However, thisincreased penetration markedly increases the risk of injuryto the vessels immediately adjacent to the vertebral bodies.Pull-out strength also varies significantly with screw de-sign.165, 286 In general, the larger the outer diameter ofthe screw body, the greater the resistance to bending, andlarger thread depth results in greater pull-out strength. Thepitch of the thread was less significant.
Crowe and Gertzbein53 evaluated the AO FixateurInterne in a prospective study involving pedicle fixationone level above and one level below the injury. Theyanalyzed the ability of this system to reduce burst fracturesof the thoracic and lumbar segments of the spine. Theaverage spinal canal cross-sectional area in 25 patients,which had been compromised 54% preoperatively, im-proved to 40% compromise after surgery. This benefit wasmost marked in patients who initially had moderate spinalcanal encroachment (34% to 64%); canal compromise inthis group improved on average from 54% to 31%. Theimprovement was less marked in patients with mild orsevere spinal canal compromise and in those treated more
than 4 days after injury. In view of this modest change of14% over all their patients, it must be questioned whetherthis improvement is significant. It was the authors’conclusion that when canal clearance is essential, anteriordecompression is the treatment of choice. However, Doerrand co-workers68 noted that the Fixateur Interne providedcanal decompression equal to that achieved with Harring-ton rod systems.
Esses and colleagues conducted a prospective, multi-center study on the effectiveness of the Fixateur Interne forthe treatment of thoracolumbar spine trauma.89 Theyreported a mean improvement of 30% in canal compro-mise and a mean correction of 14° in kyphotic deformity.Complications included screw misplacement in sevencases and three cases of broken hardware noted inciden-tally on follow-up radiographs. In no patient did apseudarthrosis develop.
Akbarnia and associates reviewed 61 cases of thora-columbar and lumbar spine fractures treated with the VSPsystem.6 Most of their patients were instrumented onelevel above and one level below the injury. Ninety percentmaintained their reduction, but pseudarthrosis developedin 15%, and 15% had screw breakage or dislodgment.Follow-up was short, averaging only 1 year with a range of2 to 36 months.
Liu and colleagues treated 42 patients by short seg-mental posterior fixation with the AO Fixateur Interne.After an average follow-up of 66.1 months, they showedan average postoperative improvement of 14.2° in theirkyphotic angle with an average loss of 3.3° of correction atfollow-up. Complications were seen in seven patients.Implant failure occurred in six, but no complaints werenoted from these patients. One patient experienced anonunion with screw breakage, which was revised byrepairing the posterior fusion and replacing the instrumen-tation.180
Sasso and Cotler compared Harrington instrumenta-
FIGURE 30–46. Continued. E, A postoperative CT scan shows partial restoration of the canal by ligamentotaxis and correct placement of the pediclescrews (F).
921CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 47/69 P 921 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 47/69 P 921 BLACK T

tion, Luque sublaminar wire instrumentation, and pediclescrew instrumentation in 70 patients with thoracolumbarspine fractures.247 The mean number of levels instru-mented was 6.0, 6.3, and 3.3, respectively. No patientsustained postoperative neurologic injury or deterioration,and complication rates were similar in all three groups. Atlast follow-up, the pedicle screw group had the bestmaintenance of sagittal contours. Markel and Graziano, incomparing Cotrel-Dubousset instrumentation with pediclescrew instrumentation, found a significantly fewer numberof levels fused in patients treated with the latter sys-tems.189
In another study, Cresswell and colleagues comparedthe stability of the AO internal fixation system with theHartshill rectangle and sublaminar wiring in the treatmentof thoracolumbar burst fractures. They reported that bothsystems allowed good initial restoration of anterior andposterior vertebral body height. However, at a 2-yearfollow-up, loss of body height occurred in the Hartshillgroup, whereas body height was significantly bettermaintained in the AO group. They thought that trans-pedicle body grafting, which was performed as part of thetreatment with the AO system, contributed in somemeasure to their success with this system.52
Although most studies have shown excellent initialreduction of deformity with pedicle screw instrumenta-tion, the ability of this instrumentation to maintain thatcorrection has been questioned.107, 248 However, loss ofcorrection is not necessarily associated with a poor clinicalresult or late neurologic deterioration. For example, Carland co-workers42 reported an average correction ofdeformity of 7.4° with pedicle screws, and at last follow-upthe average loss of correction was 6°, which left a finalcorrection of just over 1°. Nevertheless, 97% of theirpatients were satisfied with their result, and 85% of themwent back to work.
Although instrumentation failure would appear to bethe most likely reason for late collapse, such is not usuallythe case. Rather, damage to the discs adjacent to the levelof injury and to supporting soft tissues may be responsible.Because the pedicle screw instrumentation spans fewersegments than the traditional (Harrington, Luque, orCotrel-Dubousset) systems do, it may fail to include all thedamaged motion segments in the fusion, thus allowing forthe occurrence of late deformity.
The initial series describing the use of short-segmentpedicle screw systems had an unacceptable high earlyfailure rate. McLain and associates203 reported on 19patients in whom thoracolumbar fractures were managedwith short-segment pedicle screw instrumentation. Al-though no neurologic or vascular complications occurredin this small group, the rate of early fixation failure wasdisturbingly high (10 of 19 patients), with resultantprogressive deformity and pain. They noted three mainmodes of screw failure: bending, breaking, and pull-out. Asignificant number of screw failures were associated within situ rod bending, which possibly weakened the screwsby prestressing them. Others have reported similarly highrates of early failure of short-segment pedicle screwinstrumentation. However, such failure does not appear tobe a problem when pedicle screw systems are used fordegenerative conditions, possibly because the anterior and
middle columns are intact and, therefore, the instrumen-tation is load sharing. With significant disruption of theanterior and middle columns (i.e., in traumatic injury),most of the load must be borne by the instrumentation,a situation that can lead to failure. Kostuik and col-leagues161 performed a biomechanical study on short-segment pedicle screw instrumentation systems and notedthat the bending moment of the screws increased 300%after disruption of the anterior and middle columns.McCormack and associates198 were able to clinicallypredict patients who were at higher risk for instrumenta-tion failure by classifying the amount of anterior andmiddle column disruption.
A number of alternatives can be used for the preventionof such failures, including reconstruction of the anteriorand middle columns by strut grafting. Ebelke andco-workers76 performed a survivorship analysis of pediclescrew instrumentation in patients with burst fracturestreated with or without additional anterior decompressionand strut grafting. Patients treated by anterior reconstruc-tion had a 100% implant survivorship rate at 22 months,whereas those treated with posterior pedicle screws alonehad an implant survival rate of 68% at 9 months, whichdropped to 50% at 19 months. Other suggestions includethe use of a hybrid hook-claw construct two to threesegments above the level of injury with pedicle screwsbelow.42 This construct is particularly useful at thethoracolumbar junction, where fusion of an increasednumber of motion segments does not result in increasedmorbidity from loss of motion. In a prospective studytreating thoracolumbar injuries with Cotrel-Duboussetsegmental transpedicular fixation two levels above and onelevel below, Katonis and colleagues showed decreasedinstrument failure and sagittal collapse.149 Mermelsteinand associates performed a biomechanical study to analyzethe stability of burst fractures when reinforced withhydroxyapatite cement through a transpedicular approachand stabilized with short-segment pedicle screw instru-mentation. Their results showed that reconstruction withhydroxyapatite cement reduced pedicle screw bendingmoments by 59% in flexion and 38% in extension. Theyconcluded that this technique may improve outcomes inburst fracture patients without the need for an anteriorapproach.204 Finally, the addition of supplemental hooksat the same levels as the pedicle screws, either cephalad,caudad, or both, may significantly decrease failurerates.46, 132 Also, the addition of pedicle screws at the levelof the fracture gives three-point fixation and may preventcollapse, as with the Edwards hook-rod-sleeve construct. Ifthis technique is used, the screws need to be angled awayfrom the fractured end-plates.
It should also be remembered that most screw-platesystems cannot easily provide distraction or anteriorlydirected forces to achieve maximal reduction and preserveanatomic sagittal alignment. Systems that use hooks orscrews (or both) attached to rods are better able to achievethese goals.288
SURGICAL TECHNIQUE
Because many different pedicle screw fixation devices arecurrently available and more are in the process of
922 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 48/69 P 922 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 48/69 P 922 BLACK T

development, this surgical description is general, withemphasis on proper positioning of the pedicle screws. Asstated in the previous section, fixation of one pedicle aboveand one pedicle below the level of injury may be adequate,provided that the anterior fragmentation is minimal. If theanterior comminution is more significant, the alternativesare to extend the instrumentation to two levels above andtwo levels below the injury or plan to perform anteriorcorpectomy and fusion of the fractured vertebra at a laterdate to provide anterior axial support.
The patient is placed in the prone position, and amidline incision is made to expose the spinous processes,laminae, facet joints, and transverse processes of each levelto be instrumented. The orientation of the pedicles isapproximately −4° from sagittal at T12 and 11° fromsagittal at L1, slowly increasing to 30° from sagittal at theL5 level.285 Pedicle diameter similarly varies and isapproximately 8 mm at T12, L1, L2, and L3. It increases toapproximately 1 cm at L4 and almost 1.3 cm at L5. Ahelpful way to assess angulation from the sagittal plane isto measure it on the patient’s CT scan. Pedicle diameter canalso be determined from the CT scan.
The central portion of the pedicle in a cranial-to-caudaldirection can be approximated by passing a line throughthe center of the transverse processes of the vertebral bodybilaterally. This line bisects the midpoint of the pedicles.The midportion crosses the transverse process line in amedial-to-lateral direction at a point defined by a line
drawn through the facet joints244 (Fig. 30–47A). In thelumbar spine, the mammillary process, just lateral to thefacets, is useful to guide entry into the pedicle.
Once the soft tissues have been completely removedand the bone in the area exposed, a high-speed bur can beused to remove the outer cortex over the chosen entrypoint. An awl or 000 curette can then be used to penetratethe pedicle and the vertebral body while maintaining theappropriate inclination from the sagittal plane. Craniocau-dal tilt is best discerned from a lateral scout radiograph.Intraoperative radiography or fluoroscopy can be used toassess the position. If insertion of these screws is basedonly on anatomic landmarks and the experience of thespinal surgeon, the chance of having a screw outside thedesired boundaries of the pedicle may be as high as30%.270 The use of intraoperative radiographs and fluo-roscopy helps decrease this risk. Each hole can be probedwith an angled instrument, such as a nerve hook or depthgauge, in all four quadrants from its anterior to itsposterior extent to be certain that the pedicle has beenentered and the cortex has not been violated. The hole canbe tapped, if necessary, for the instrumentation to be used.The pedicle screws are then inserted.
Regardless of the type of instrumentation, care shouldbe taken to insert the screws with only two to threefingertips on the wrench or screwdriver to avoid strippingthe threads within the pedicle and vertebral body. Becauseof the high risk of vascular and visceral injury, the anterior
A B
FIGURE 30–47. Proper positioning of pedicle screw instrumentation. A, The central portion of the pedicle can be identified by the intersection of two lines.The transverse line bisects the transverse process of each level, and the longitudinal line runs in a cephalad-to-caudal direction and bisects the facet joints.B, A transverse section shows the ideal location for the pedicle screws. It also indicates the proximity of the neural elements to these screws, both withinand outside the spinal canal. The medial-to-lateral inclination of each of these pedicles and screws will vary, depending on the level of the spine (as outlinedin the section of this chapter on anatomy). (A Redrawn from Leona Allison.)
923CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 49/69 P 923 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 49/69 P 923 BLACK T

cortex of the vertebra should not be violated from themidthoracic region to L5, unless it is essential to increasefixation strength, as in an osteoporotic spine. Over thesacrum, it is often necessary to advance one or two threadsthrough the anterior cortex because fixation strengthincreases with bicortical purchase.164
An additional consideration during placement of thesescrews is whether the plate, rod, or pedicle screw itself willviolate an adjacent normal joint. The potential for thiscomplication is determined by the basic design of thepedicle screw fixation device and cannot usually be alteredby the surgeon, so it must be considered when initiallyselecting the pedicle screw instrumentation system.
As with all other instrumentation systems used to treatspinal fractures, achievement of reduction and normalsagittal alignment is one of the primary goals of surgicaltreatment. Both lordosis forces and distracting forces canbe applied through short-segment pedicle screw constructsto achieve these desired outcomes (Fig. 30–48). Radio-graphs in both the AP and the lateral planes should beobtained with the final instrumentation system in place tobe certain that the fracture is adequately reduced, sagittalspinal alignment is satisfactory, and each of the pediclescrews is in the desired position (see Fig. 30–47B).
A useful method for re-creating lordosis is placement ofa screw at the level of injury. When used in conjunctionwith contouring of the rod, excellent three-point fixationmay be achieved. Another method of restoring lordosis isto leave the caudal aspect of the rod angled at approxi-mately 15° up from the cephalad screw (best performedwith screw heads that allow angulation), with the cephaladaspect fixed to the spine. The rod is then forced down toengage the caudal screws. This technique provides distrac-tion and lordosis of the proximal segments.
As with all other instrumentation systems, solid fusionis one of the primary goals of surgery. Adequate careshould be taken to decorticate the transverse processes andthe lateral aspects of the superior facets to increase the
chance of achieving fusion. If the pedicle screw fixationsystem uses plates, it is important that the bone graft beinserted before application of the plates because theprocedure becomes more difficult after the plates havebeen secured in position. Finally, a number of newerinstrumentation systems are made of titanium, whichallows for better postoperative imaging, particularly MRI.77
Posterolateral Decompression
Surgical decompression frequently equates to surgicalreduction when discussing treatment of thoracic andthoracolumbar spine injuries. If complete reduction can beachieved, no other decompression is needed. Edwards andLevine showed that surgical reduction performed within 2days of injury restores the spinal canal area by anadditional 32% whereas surgery performed between 3 and14 days after injury restores only 23%.80, 83 They alsofound that little or no improvement occurs when posteriorinstrumentation is delayed for more than 2 weeks.Crutcher and co-workers54 reported similar results withthe use of a simple Harrington construct and achieved anapproximately 50% reduction in canal clearance. Thefracture pattern influences the adequacy of decompres-sion, with Denis type A fractures having significantly bettercanal clearance by indirect means than Denis type Bfractures. Therefore, with early surgery and better surgicalreduction, the chance of needing any formal neuraldecompression is lessened.
The adequacy of reduction cannot be easily assessed byplain radiography. A postoperative myelo-CT scan is aneffective way to assess for residual neural compres-sion.33, 105 If a significant abnormality is found, anteriordecompression can be performed at a later date.
In addition, if anatomic realignment has been achieved,some resorption of bone from within the spinal canal willoccur over the course of the next year, thereby lesseningthe extent of neural compression.53 Krompinger andcolleagues168 reviewed 29 patients with injuries of thethoracic or lumbar spine treated nonoperatively; 14 hadcanal compromise greater than 25% on initial evaluation.Bone remodeling of the compromised canal was noted in11 of these 14 patients, and canal compromise of less than25% resolved completely in 4 of 8 cases. Similar resultsduring nonoperative treatment of burst fractures have beenreported by others.41 Edwards and associates82 notedcomparable canal fragment resorption in patients treatedwith rod sleeve reduction and fusion, and Sjostrom andcolleagues256 noted resorption of intracanal fragmentsafter the application of pedicle screw constructs andfusion. Willen and co-workers,279 however, reported thatpatients with more than 50% canal compromise rarely hadsignificant resorption. With these factors kept in mind,some patients in whom significant neural compressionremains and is not improved by posterior instrumentationand reduction may still require late operative treatment offractures of the thoracic or thoracolumbar spine. Postero-lateral decompression has also been used at the time ofposterior instrumentation.
The advantage of the posterolateral technique is that itallows stabilization of severe spine injuries, including
FIGURE 30–48. Application of both distraction and lordosis forcesthrough short pedicle screw constructs is necessary to achieve normalsagittal alignment. (Redrawn from Muller, M.E.; Allgower, M., eds.Manual of Internal Fixation, 2nd ed. Heidelberg, Springer-Verlag, 1991.)
924 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 50/69 P 924 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 50/69 P 924 BLACK T

fracture-dislocations, and at the same time allows somedegree of neural decompression without requiring asecond surgical procedure.74 One disadvantage of thistechnique is that it necessarily requires removal ofposterior and posterolateral bone and may thus furtherjeopardize spinal stability and eventual fusion.16 Thesecond major disadvantage is that it is a relatively blindprocedure because the dura and neural elements liebetween the surgeon and the anterior compressive tissue.
The posterolateral technique has been evaluated byGarfin and colleagues.106 In that series, nine patients withburst fractures of the thoracic or lumbar spine were treatedby posterolateral decompression and evaluated with post-operative CT scans. Postoperative CT scanning showedonly one patient with bone remaining in the canal.Hardaker and co-workers126 reported the use of bilateraltranspedicular decompression with posterior instrumenta-tion and fusion for severe burst fractures with an averagecanal compromise of more than 65%. Although anteriordecompression would normally be required for suchextreme amounts of canal compromise, only one patient inthe study underwent an additional anterior procedure.Seventy-seven percent of the patients with a neurologicdeficit had significant improvement, and significant ky-photic deformity had not developed in any patient atfollow-up. Hu and associates135 compared anterior de-compression with transpedicular decompression in pa-tients with incomplete neurologic deficits and found noadditional benefit for anterior vertebrectomy over simpletranspedicular decompression. Both treatments resulted insignificant neurologic improvement when compared witha similar group of patients treated by indirect reductionmaneuvers alone. Others have reported comparable resultswith the use of transpedicular decompression.268 Incontrast, Lemons and colleagues172 compared directdecompression by a posterolateral route with indirectreduction and found no significant differences in improve-ment in canal clearance or neurologic function. Theyconcluded that the posterolateral transpedicular approachis of questionable value for the treatment of burst fractures.
SURGICAL TECHNIQUE
Posterolateral decompression is performed as part of aposterior stabilizing operation in patients with thoracic,thoracolumbar, or lumbar spine injuries. Before theinstrumentation system is applied and before any postero-lateral decompression, the CT transverse sections at thelevel of the injury should be studied to determine whichside of the spinal canal has the more severe neuralcompression. The instrumentation should be inserted firston the side with the smaller amount of neural compressionand corrective forces then applied to reduce the spineinjury. In most cases, these forces include a combination ofdistraction and lordosis with three- or four-point fixationand the force vector directed anteriorly at the level ofinjury.
Attention is then directed to the side of the spine that isfree of instrumentation (Fig. 30–49A). A laminotomy isperformed at the level of maximal neural compression,which is most commonly the area between the pedicles ofthe fractured vertebra. At this level, the adjacent spinous
processes are each trimmed and the intervening ligamen-tum flavum is excised. Five millimeters of adjacent bone isremoved, including portions of the cephalic and caudallaminae, as well as the medial portion of the facet joint atthat level.
The posterior edge of the fracture (anterior to the dura)can be palpated with an angled dural elevator (e.g., Frazierelevator) to assess the degree of residual canal compro-mise. The laminotomy should be extended distally at leastto the inferior edge of the pedicle. Once the medial borderof the pedicle is identified, a power bur is used to drill intothe central portion of the pedicle with all cortices left intact(see Fig. 30–49B). A thin rongeur or curette is then used toremove the medial cortex of the pedicle, with care taken topreserve the nerve root exiting below it (see Fig. 30–49C).A trough is cut 1 cm into the vertebral body anterior to themedial portion of the pedicle that has been thinned.Reverse-angle curettes can be inserted through thisopening, and any bone fragments compressing the anteriorneural elements can be impacted into the vertebral body orbrought out through the lateral trough previously made(see Fig. 30–45D). Mimatsu and co-workers205 havedesigned a variety of impactors specifically for use in thetranspedicular approach. It is possible to extend thisdecompression slightly past midline through this unilateralexposure (see Fig. 30–49E).
If the decompression is adequate on both sides of thecanal, no further decompression is needed. If furtherdecompression is needed on the side that has already beeninstrumented, a second rod is inserted on the side alreadydecompressed, the instrumentation is removed, trans-pedicular decompression is performed on the first side,and the instrumentation is reinserted.
Anterior Transthoracic Decompressionand Fusion
Anterior transthoracic decompression and fusion may beused for the treatment of thoracic and thoracolumbarspine fractures (T2 to L1), either as a single operativeprocedure or in conjunction with a posterior stabilizationprocedure. It is most indicated in patients with maximalanterior neural compression, patients with an incompletespinal cord injury, and those with minimal instability, aswell as for the delayed treatment of injuries, including latepost-traumatic deformities123–125, 131 (see Fig. 30–26).
This transthoracic approach for trauma was firstdescribed by Paul and colleagues,220 and detailed tech-niques along with long-term results of this treatment havebeen published by Bohlman and associates.29, 30 In areview of acute injuries of the upper thoracic spine withparalysis, eight patients were treated by anterior decom-pression and fusion for residual neural compression. Allhad reached a plateau in terms of neurologic recovery atthe time of anterior decompression. Postoperatively, fivepatients were able to walk without aid, two recoveredpartially and were able to walk with crutches and braces,and one patient improved but remained unable toambulate. No patient lost neurologic function as a result ofthis procedure, and solid fusion developed in all patients,even though three had previously undergone laminectomy.
925CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 51/69 P 925 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 51/69 P 925 BLACK T

AB
D
C
E
FIGURE 30–49. Technique of posterolateral decompression of the spinal canal. A, A posterior view of the spine shows the region of exposure and theamount of pedicle resection required to achieve posterolateral decompression. Care should be taken to not cut inferolaterally across the parsinterarticularis. B, The ligamentum flavum has been resected at the level of injury, and the dura has been exposed. Bone is resected laterally up to themedial extent of the pedicle and caudally to the inferior extent of the pedicle. A bur is used to make a hole in the central portion of the pedicle, withthe hole proceeding anteriorly toward the vertebral body. A circumferential rim of cortical bone is left in place. The nerve root is shown medial to thepedicle and exiting below the pedicle. Care should be taken to not injure this nerve root. C, The medial wall of the pedicle is removed with a rongeursuch as a pituitary rongeur. D, A transverse section shows the hole burred down through the pedicle and into the vertebral body. A reverse-angle curetteis used to tap bone out of the spinal canal and into the trough that has been drilled out of the vertebral body. Large bone fragments may also be pulledout through this lateral trough. Care must be taken to not hook the anterior aspect of the dura. E, A transverse section shows the final result afterdecompression. By performing unilateral posterolateral transpedicle decompression, it is usually possible to adequately decompress slightly past themidline.
926 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 52/69 P 926 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 52/69 P 926 BLACK T

None was augmented with any type of instrumentationeither anteriorly or posteriorly. No data were givenconcerning residual angulation at the site of injury.30
Most published series of transthoracic decompressionfor treatment of spinal trauma review either patients withminimal to moderate levels of instability or those who areno longer in the acute stage after their injury. In the lattergroup, some healing with partial stabilization may alreadyhave occurred. Gurr and colleagues121 showed in ananimal corpectomy model that the strength of the spine ismarkedly reduced after corpectomy in comparison to thestrength of an intact spine. This reduction in strength istrue for axial loading, flexion loading, and rotation testing.The addition of an iliac graft still allows three times thedisplacement with axial compression, as well as displace-ment with flexion testing, and torsional stiffness is lessthan one third that of an intact spine. In trauma patientswith significant posterior disruption and an anteriorcorpectomy, additional instability is probably present. Forthis reason, uninstrumented anterior transthoracic decom-pression plus fusion is rarely indicated and should bereserved for patients with significant neural compressionand minimal instability. As the degree of instabilityincreases, it becomes necessary to supplement the anteriordecompression and fusion with either anterior instrumen-tation or posterior stabilization. In severe injuries associ-ated with three-column disruption, some authors recom-mend supplementation of anterior instrumentation withposterior instrumentation and spinal fusion.19, 20 Almostall patients should have postoperative immobilization in aTLSO, except perhaps for those stabilized with rigidposterior segmental fixation devices.
Beginning in the late 1980s, the development of moresophisticated anterior plate systems has improved thequality of anterior fixation in the thoracic and thoracolum-bar spine.15, 158, 167 However, anterior plate fixation to L4,L5, and S1 remains problematic. Most of the currentsystems are based on the principle of two screws per level,with one screw placed posteriorly, parallel to the posteriorcortical wall of the vertebral body, and the second angledobliquely from anterior in the body to posterior. Thistriangular arrangement improves pull-out strength. Inaddition, in most systems an element of compression ordistraction can be applied between the upper and thelower segments of fixation before fixing the bolt or screwto the plate. This technique may improve incorporation ofthe graft anteriorly, as well as the stability of the construct.
Kaneda and associates reported their results in treating150 consecutive patients with thoracolumbar burst frac-tures by anterior decompression and stabilization with theKaneda device (see Fig. 30–26). After a mean follow-up of8 years, radiographs showed a successful fusion rate of93%. Ten patients with a pseudoarthrosis were success-fully managed by posterior spinal instrumentation andfusion. They believe that all their pseudoarthroses oc-curred in patients who had poor placement of the anteriorstrut graft. Kaneda thought that the success of his devicerelied directly on load transmission through a strongtricortical iliac crest graft, with placement of the tricorticalportion beyond the contralateral pedicle. The meanpercent canal obstruction preoperatively was 47% and,postoperatively, 2%. Neurologic function improved by at
least one grade in 95% of patients. Breakage of the implantoccurred in nine patients, with no iatrogenically inducedneurologic deficits. Of the patients who were employedbefore the injury, 96% returned to work. The averagekyphosis was 19° preoperatively, 7° immediately postop-eratively, and 8° at follow-up.147 In a separate report,146
Kaneda and co-workers used the Kaneda device afteranterior decompression in patients with neurologic deficitscaused by post-traumatic kyphosis. All patients reportedexcellent results. Gardner and associates102 used thecontoured anterior spinal plate (CASP) system for a varietyof conditions, including acute burst fractures, and had afusion rate of 100%. McGuire reported 14 unstablethree-column injuries treated by anterior decompressionand stabilization with the University Plate (AcromedCorp.). Radiographically, vertebral height was maintained,and no measurable graft subsidence or kyphosis devel-oped. He reported no hardware failures and one nonuniontreated successfully with a posterior compression con-struct.201 Okuyama and associates reviewed 45 patientswith unstable burst fractures treated by anterior decom-pression and stabilization. They reported 84% with no orminimal pain, a 74% return-to-work rate, and minimalloss of the kyphotic angle until fusion.213 Other recentlypublished studies have also shown similar results withanterior decompression and stabilization for thoracolum-bar burst fractures.115, 190
Most recent studies reporting the results of anteriordecompression and stabilization have used rib or iliac crestbone grafts (or both) for their fusions. Finkelstein andassociates reported the results of a prospective cohortstudy to evaluate the use of cortical allograft bone foranterior spine reconstruction in thoracolumbar fractures.They packed the medullary canal of tibial allografts withautogenous bone from the corpectomy. Twenty-two pa-tients underwent anterior surgery alone, and 14 patientshad both anterior and posterior surgery. In the lattergroup, posterior instrumentation was combined withautogenous bone grafting. They reported an overall fusionrate of 81%, with a trend suggesting that patientsundergoing anterior surgery alone had a higher rate ofnonunion, 5 of 22, than did those undergoing anterior andposterior instrumentation, 2 of 14. In addition, of eightpatients who had loss of correction or loss of stability afteranterior fixation alone, three required revision surgerywith the addition of posterior instrumentation.94
Other authors have noted high complication rates withanterior fixation (30%), as well as significant loss of theinitial deformity correction over time (50%).121 Yuan andco-workers,284 reporting on their results with the SyracuseI-Plate, cautioned that osteoporosis and significant poster-ior column disruption are relative contraindications toanterior fixation.15
SURGICAL TECHNIQUE
The patient should be intubated with a double-lumen tubefor approaches above T10 so that the left and right mainstem bronchi may be ventilated separately; this tube allowsfor later collapse of one lung to provide adequate exposureof the spine. From T10 distally, a single-lumen tube isadequate. For exposure of T10 and above, the patient is
927CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 53/69 P 927 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 53/69 P 927 BLACK T

usually turned to the left lateral decubitus position. Theright side of the chest is chosen as the side for surgery,assuming that the patient does not have any contraindica-tions or exposure-related considerations. This positionavoids any encroachment on the heart and great vessels, aswould be encountered in a left-sided approach, especiallyin the middle and upper thoracic spine regions. A left-sided approach can be chosen if necessary, but prominentinternal fixation should not be used from this side.
Special care should be taken to place a pad just distal tothe patient’s downside axilla to prevent a stretch palsy ofthe brachial plexus. Also, an arm support should be usedto hold the upper part of the arm in a neutral position: 90°forward flexion at the shoulder, neutral abduction adduc-tion, and almost straight at the elbow. Both arms should beadequately protected and padded, especially in the regionof the radial nerve in the posterior aspect of the upper partof the arm and near the ulnar nerve at the elbow. Forwardflexion of more than 90° at the shoulder should be avoidedto minimize the risk of brachial plexus palsy. Tape can besecurely placed across the patient, both at the level of thegreater trochanter and across the shoulder, and thenaffixed to the table. A beanbag placed under the patient isalso useful to help maintain this position.
The patient’s entire right flank, anterior part of thechest, and posterior portion of the torso should beprepared from just inferior to the level of the axilla toinferior to the lateral aspect of the iliac crest. Care shouldbe taken to prepare the skin to the midline anteriorly andbeyond the midline posteriorly. Such preparation mini-mizes the chance of disorientation during the operationand also makes it possible to perform anterior transtho-racic decompression and fusion and posterior instrumen-tation and fusion simultaneously, if necessary.
From T6 through T10, the incision should be madedirectly over the rib of the same number as the fracturedvertebra (Fig. 30–50A) or one level proximal to it. It istechnically easier to work distally than proximally. Removalof a rib one level higher works well, especially if thecorpectomy involves more than one level. For fracturesabove T6, the skin incision should extend over the T6 ribanteriorly and laterally. Posteriorly, it should extend to theinferior tip of the scapula and then curve gently morecephalad, halfway between the medial border of the scap-ula and the midline spinous processes (see Fig. 30–50B).For exposure of T11, T12, or L1, the incision should bemade over the T10 rib to simplify wound closure.
The incision should be made through skin andsubcutaneous tissue down to the deep fascia. From T6through T10, the deep fascia and underlying muscles areincised in line with the skin incision down to the rib,which is stripped subperiosteally on both its outer andinner surfaces. The surgeon should be cautious in the useof electrocautery near the neurovascular bundle. A ribcutter is used to cut the rib at the costovertebral angleposteriorly and at the costochondral junction anteriorly.The remaining inner periosteum is then incised over thelength of the rib bed. For T2–T5, it is important to notethat the long thoracic nerve courses in the midaxillary linefrom the region of the axilla to its innervation of theserratus anterior muscle. Rather than cut this nerve andlose innervation to the more caudal portion of the muscle,it is preferable to detach the serratus anterior muscle from
the anterior chest wall and reflect it cephalad. Thistechnique can be performed to provide exposure up to theT3 rib, with additional exposure achieved by mobilizationof the scapula. Division of the dorsal scapular muscles,rhomboids, and trapezius allows the scapula to be elevatedand displaced laterally from the midline. This maneuveroffers a simple method of gaining a more extensivethoracotomy through the bed of the third rib.
After the chest has been opened, the surgeon shouldplace a hand in the chest in the midlateral line and countthe cephalic and caudal ribs because that is more accuratethan counting the ribs outside the chest wall. The surgeonshould make certain that the rib removed is the rib thatwas planned for removal. It should also be verified that thetotal number of ribs corresponds to that seen on agood-quality AP radiograph of the thoracic spine.
A self-retaining thoracotomy retractor is then insertedover moistened sponges in such a manner that theneurovascular bundle of the cephalic rib and the neurovas-cular bundle from the removed rib are not compressed bythe retractor. The chest retractor is opened slowly tominimize the chance of fracture of adjacent ribs. At thispoint, the lung can be deflated on the ipsilateral side toprovide adequate exposure to the spine.
The spine can be seen and palpated within the chestcavity. It is covered by the relatively thin and translucentparietal pleura. The rib base of the previously resected ribis traced down to its costovertebral junction, and with theknowledge that each rib inserts at the cephalic quarter ofits own vertebra, the levels of each of the vertebral bodiesand discs can be determined. At this point, a spinal needleshould be placed in a disc and a radiograph obtained todefinitively identify the levels.
The parietal pleura is incised halfway between thevertebral neural foramina posteriorly and the anteriorlylocated azygos vein and inferior vena cava. After divisionof the parietal pleura one level above and one level belowthe vertebral body of interest, the segmental vessels areidentified in the midportion of the vertebral body at eachof these three levels. These segmental vessels should beisolated and either tied or ligated with vascular clips. Thevessels should be cut over the anterior third of thevertebral bodies so that they do not interfere with anycollateral flow to the spinal cord, which enters thesegmental vessels near the neuroforamen. With a smallsponge on a clamp or a periosteal elevator, the segmentalvessels and parietal pleura can be swept anteriorly andposteriorly to expose the vertebral bodies and discs in anextraperiosteal fashion. Blunt dissection can then becarried out in this same plane, with a sponge on thesurgeon’s finger used to expose the opposite side of thevertebral body at the site of primary interest. At this time,a malleable or cobra retractor can be inserted between theexposed spine and the parietal pleura that has beendissected anteriorly (see Fig. 30–50C). The retractorprotects the esophagus and great vessels during excision ofthe vertebral body.
Because the rib extends anteriorly over the lateralaspect of the vertebral body, it is necessary to cut it justanterior to the neural foramina. The discs above andbelow the vertebra to be resected can be removed with ascalpel and rongeurs (see Fig. 30–50D). The vertebralbody may then be removed with a rongeur, as well as
928 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 54/69 P 928 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 54/69 P 928 BLACK T

gouges, osteotomes, and power burs (see Fig. 30–50E).Loupe magnification and a headlamp should be used forthis procedure. In the case of an acute fracture with manyloose pieces of bone, a large curette can be used to removethe bulk of the vertebral body. As the posterior margin ofthe vertebral body is approached, red cancellous bonebegins to be replaced by white cortical bone, whichrepresents the posterior cortex of the vertebral body. Ahigh-speed bur may then be used to perforate theposterior cortex at the point of minimal neural compres-sion (see Fig. 30–50F). Another technique to gain accessto the spinal canal is to use a small Kerrison rongeur toenter through the adjacent disc space. Alternatively, onecan begin by removing the pedicle and following thenerve root to the spinal cord. Once a point of entry intothe spinal canal has been made, the remainder of the
posterior cortex of the vertebral body can be removedwith appropriately shaped rongeurs and curettes (see Fig.30–50G and H). Removal is often facilitated with the useof fine-angled curettes to allow the surgeon to push orpull the posterior cortex away from the spinal canal. Thisdecompression should be performed from pedicle topedicle to ensure that no spinal cord compression remains(see Fig. 30–50I). If the bone has been removed and theposterior longitudinal ligament does not bulge anteriorly,the ligament should be removed while at the same timelooking for other disc or bone fragments that may becausing continued compression of the dura. At the end ofthe decompression, the ligament or dura, or both, shouldbe bulging anteriorly.
A trough can be cut into the vertebral bodies throughthe end-plates above and below the area of decompression
A
B
FIGURE 30–50. Technique of anterior transthoracic corpectomy and fusion. A, The patient is placed in a straight decubitus position with theshoulders extended forward 90°, neutral in terms of abduction and adduction, and with the elbows straight. Care is taken to protect the downside brachialplexus by using a pad just distal to the axilla. The dotted line over the rib represents the incision placed one level above that of the spinal fracture. B, Ifthe incision is used to expose the region above the T6 rib, the posterior limb of the incision is extended cephalad halfway between the medial border ofthe scapula and the spinous processes. All the intervening muscles down to the chest wall are divided and tagged for later repair.
Illustration continued on following page
929CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 55/69 P 929 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 55/69 P 929 BLACK T

C
D
FIGURE 30–50. Continued. C, After the thoracic cavity has been entered, a self-retaining chest retractor is inserted. The parietal pleura is incised halfwaybetween the anterior great vessels and the posterior neural foramina, and the segmental vessels are ligated at this same level. The vertebra to be excised,as well as one vertebra above and one vertebra below, is exposed. Extraperiosteal dissection provides the best plane. A malleable retractor is placed onthe opposite side of the spine and connected to the self-retaining chest retractor with a clamp. This malleable retractor serves to protect the great vesselsduring the vertebral corpectomy. D, A scalpel and rongeur are used to remove the discs above and below the level of the vertebral fracture.
930 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 56/69 P 930 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 56/69 P 930 BLACK T

E F
G H
FIGURE 30–50. Continued. E, An osteotome, chisel, or gouge is used to excise the vertebral body back to its posterior cortex. Special care is taken tooriginally position the patient exactly in the straight decubitus position. During resection of the vertebral body with these instruments, each of the cutsis made perpendicular to the floor. These instruments can be used as long as red cancellous bone is encountered. As soon as white cortical bone isobserved, these instruments should no longer be used. F, A high-speed bur can be used to perforate the posterior vertebral body cortex and gain accessto the spinal canal. When the neural compression is significant, a diamond-tipped bur can be used to minimize the chance of dural or neural injury. G,Downbiting 90° Kerrison rongeurs are used to remove bone on the most superficial portion of the vertebral body. H, The bone from the spinal canal onthe far side of the vertebral body is carefully impacted with reverse-angle curettes. Illustration continued on following page
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 57/69 P 931 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 57/69 P 931 BLACK T

J
K
I
FIGURE 30–50. Continued. I, The bone resection at the end of the decompression should extend from the pedicle on one side to the pedicle on the oppositeside. It is easy to underestimate the extent of bone removal necessary to achieve this goal. At the end of the neural decompression, the dura should bulgeanteriorly in a uniform fashion from the end-plate of the vertebra above to the end-plate of the vertebra below and from pedicle to pedicle. If the dura doesnot bulge out concentrically, the surgeon should check for residual neural compression. J, After the corpectomy and resection of the disc above and belowthe level of fracture have been accomplished, a trough is cut into the vertebral body above and below the corpectomy. If any degree of osteoporosis ispresent, the trough should be cut through the cancellous bone up to the next intact end-plate at the superior end of the cephalad vertebra and the inferioraspect of the caudal vertebra. A ridge of bone should be preserved at the posterior aspect of these adjacent vertebrae to prevent migration of the bone graftinto the spinal canal. K, At the end of the neural decompression and fusion, the space between the bone graft and the dura and neural elements should beadequate to minimize the chance of producing any iatrogenic neural compression. This illustration shows three strips of rib being used as bone graft, but asingle, large piece of iliac crest can also be used and may actually provide a stronger anterior strut.
932 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 58/69 P 932 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 58/69 P 932 BLACK T

(see Fig. 30–50J), but creation of a trough can weakenstabilization with the graft and is not routinely recom-mended. Alternatively, all the cartilage can be removedfrom the end-plates, but care must be taken to maintaincortical integrity of the end-plates. Appropriate bone graftis then obtained for insertion across this level of decom-pression. The patient’s own iliac crest may be harvested; atricortical bone graft provides maximal support. Anotheroption, particularly if the injury is associated with minimalinstability and the patient’s rib is of adequate strength, is toimpact three tiers of rib graft into this trough while anassistant pushes on the patient’s gibbus to minimize thedeformity (see Fig. 30–50K). Alternatively, fresh frozencorticocancellous allograft (iliac crest or distal end of thefemur) can be used with good fusion success anteriorly;the use of metal or composite cages filled with autograft isalso another good option. At the end of the decompressionand bone grafting, adequate space should be left betweenthe neural elements and the bone graft (see Fig. 30–50K),and a posterior ridge should be present on the vertebraboth cephalad and caudad to the decompression toprevent migration of the bone graft toward the neuralelements (see Fig. 30–50L and M).
After the corpectomy is completed, an appropriatelysized plate is selected to center the two screws at the levelabove and below the corpectomy as closely as possible onthe adjacent bodies. A template (if supplied) is used toplace the drill holes parallel to the posterior cortex of thevertebral body so that they accept screws or bolts in thatlocation; the screws or bolts are commonly used to providecompression or distraction. Care must be taken toprecisely understand the orientation of the patient on theoperating table and the resulting direction of drilling. Abicortical hole is drilled. It is then depth-gauged to acceptthe proper length screw or bolt. The bolts are screwedtightly into position and may then be used to apply
distraction to the interspace, thereby achieving restorationof body height at the injured level. An appropriately sizedtricortical iliac bone graft can be fashioned to fit into theinterspace. Placement of the graft should be slightly biasedanteriorly in the corpectomy defect. The distraction canthen be released and a plate of proper size selected so thatit does not impinge on the open disc spaces above andbelow the stabilized levels. The plate is placed over thebolts and the nuts provisionally placed on the bolts. Slightcompressive force is applied across the reconstructed level,and the nuts are tightened down to maintain position.Finally, the two anterior screw holes are drilled and thescrews placed into position to complete the construct.
The malleable retractor is removed, and hemostasis isobtained before closure. The parietal pleura is reapproxi-mated with the use of absorbable suture material. One ortwo large chest tubes are inserted. The thoracotomy isclosed with sutures placed above the cephalic rib andbelow the caudal rib, with care taken to avoid theneurovascular bundle immediately beneath the caudal rib.A rib approximator is used to close the chest wall defect,and the pericostal sutures are tied. All the muscles aresutured back to their original positions, including theserratus anterior if it was detached from the chest wall.
If the spine injury was relatively stable and is at a levelof the spine that can be adequately braced with anorthosis, the patient may be mobilized while wearing thebrace. The brace is worn until solid union is demonstratedradiographically. If the spinal fracture was judged to bemoderately or severely unstable, the anterior procedureshould be combined with posterior instrumentation (usu-ally in compression) and fusion to allow early mobiliza-tion. As an alternative, anterior instrumentation can beused to supplement the anterior decompression andfusion, provided that the instability is only moderate (Fig.30–51).
L M
FIGURE 30–50. Continued. A transverse section at the vertebrae above (L) and below (M) the level of the corpectomy should reveal an adequate posteriorrim of cortical bone to prevent migration of the bone graft into the spinal canal and an anterior cortical and cancellous rim of bone to prevent dislodgmentof the bone graft.
933CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 59/69 P 933 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 59/69 P 933 BLACK T

A
B
C
D
E
FIGURE 30–51. Technique for anterior spinal instrumentation after corpectomy. A, After using a depth gauge on the exposed vertebral body, appropriatelysized screw lengths are selected to engage the opposite cortex of the vertebral body. The bolts are placed parallel to the adjacent end-plate to avoid intrusioninto the disc space above or below the corpectomy site. B, Distraction is applied against the bolts to allow easy insertion of the strut graft into thecorpectomy site. C, Determination of the proper length of plate with a template is important to avoid impingement of the superior or inferior disc space.Locking nuts are applied and provisionally tightened. D, Compressive force is applied and the locking nuts tightened down firmly. E, Finally, two anteriorscrews are placed and the nuts are crimped down to prevent possible backing out or loosening. (A– E, Redrawn with permission from Zdeblick, T.A.Z-Plate–ATL Anterior Fixation System: Surgical Technique. Sofamor Danek Group, Inc. All rights reserved.)
934 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 60/69 P 934 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 60/69 P 934 BLACK T

COMPLICATIONSz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
With the correct application of currently available spinalinstrumentation, it is possible to stabilize and anatomicallycorrect most disrupted spinal columns. However, theseprocedures are not risk free and may be associated withmajor complications. This section does not address allcomplications related to spinal surgery, but focuses onthose associated with the treatments described in thischapter. Certain complications such as death, deep veinthrombosis, and pulmonary embolism, though intimatelyrelated to surgery, are not peculiar to spine surgery and aretherefore not discussed here. Other complications such asiliac crest bone graft donor site morbidity are common toall spinal surgeries.134, 169 It cannot be emphasizedstrongly enough that many potential intraoperative com-plications may be avoided, or their severity reduced, bycareful preoperative planning. Accurate identification ofthe mechanism of injury and selection of the appropriateinstrumentation and levels constitute the first critical step.However, despite detailed planning, surgical complicationsmay still occur.
Neurologic Deterioration
Neurologic deterioration can occur before initiation ofdefinitive treatment. Gertzbein111 reported a 3.4% inci-dence of new or increased neurologic deficit after patientswere admitted to trauma centers. He noted, however, thatthis group of patients had a significantly increased returnof neurologic function after initiation of treatment incomparison to those who initially had a neurologic deficit.For patients whose neurologic function deteriorates afterthe initial evaluation, surgical treatment is recommended.In addition, progressive deformity with associated lateneurologic deterioration may develop in fractures man-aged nonoperatively, even if initially stable.114 Neurologicdeficit occurring during or after treatment is one of themost serious complications associated with the surgicaltreatment of spinal injuries. The reported incidence isapproximately 1%.175 Neurologic deterioration may beassociated with overdistraction, overcompression, directinjury resulting from the introduction of instrumentationinto the spinal canal, or loss of position or reduction.
Overdistraction can be reduced to a minimum, or itspossibility anticipated, by careful preoperative assessmentof the mechanism of injury and prediction of the presenceof an intact anterior longitudinal ligament. With thisligament intact and with proper contouring of theposterior instrumentation system to place the spine insome degree of lordosis and the anterior longitudinalligament under tension, overdistraction can usually beavoided. MRI may provide useful information concerningthe status of the anterior longitudinal ligament before anyreduction requiring distraction.36, 155 Neurologic injuryrelated to compression instrumentation can generally beavoided if this construct is used primarily when theposterior cortex of the involved vertebral bodies is intactand the mechanism of injury does not strongly suggest anaccompanying discal injury, which may frequently occurwith flexion-distraction injuries (Fig. 30–52).
Segmental wires, sublaminar hooks, and pedicle screwscan all provide significant intrusion into the spinal canaland transiently or permanently injure or compress thespinal cord or nerve roots. Proper positioning of theinstrumentation and awareness of this complication mayreduce the incidence of occurrence but cannot completelyeliminate it.
During instrumentation, if evoked potentials deterio-rate, if an intraoperative wake-up test is not achievedsuccessfully, or if radiographs show overdistraction orovercompression, the instrumentation system should bealtered. The alteration may be as simple as relieving somedegree of the distraction or compression or removing oneor two segmental wires. Alternatively, it may be necessaryto remove the entire implanted system, insert a differentinstrumentation system, or leave it out altogether. Theinjury pattern, the preceding portion of the procedure, andco-morbid conditions may affect this decision.
Neurologic deterioration observed in the postoperativeperiod may be related to disc herniation, loss of reduction,spinal cord edema, hematoma, or some combination ofthese complications. Immediate study with myelography,CT scanning, or MRI should be considered, and thepatient should be returned to the operating room asnecessary to relieve any neural compression.
INJURY RESULTING FROM INSERTION OFPEDICLE SCREWS
The spinal nerves are particularly susceptible to injury ifthe pedicle is violated medially or inferiorly. In addition, ascrew that is too long can transgress the anterior cortex ofthe vertebral body and injure a major vascular structure.
The risk of neural damage can be minimized if thesurgeon is aware of the spinal anatomy and familiar withthe process of localizing and entering the pedicle. Carefulidentification of the pedicle and proper screw placementunder radiographic control help minimize potential inju-ries. In earlier studies, some authors reported a 10% to20% rate of inaccurate pedicle screw placement, even inwell-controlled environments. This rate reportedly in-creased to as high as 41% in the thoracic spine.254 It mayalso be increased with deformity and instability. Fortu-nately, not all errant screws lead to clinical consequences.
Neural damage can result from direct contact by a screwor by a drill, curette, or tap. Late screw cutout through thepedicle may also result in nerve damage.26 If a postopera-tive radiculopathy is noted, CT evaluation of the screw andbone should be performed, with consideration of screwremoval if the results are positive. However, stability issuesmust also be considered when making these decisions.Rose and associates described a technique involving persis-tently electrified pedicle stimulation instruments, whichcan be used to detect whether the pedicle screws havefractured or broached the cortical bone during placement.This technique may help confirm intraosseous placementof pedicle screws and prevent neurologic injury.240
Kothe and colleagues simulated pedicle fractures in anin vitro model to determine the effect on multidirectionalstability when pedicle instrumentation is used. Aftersimulation of an intraoperative pedicle fracture, the resultsof three-dimensional flexibility testing showed a significant
935CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 61/69 P 935 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 61/69 P 935 BLACK T

decrease in axial rotation and lateral bending stabilityprovided by the instrumentation.163
If screw loosening occurs, loss of correction maydevelop before the fusion heals. Loss of fixation can resultfrom errant placement of a screw, fracture of the pedicle,inadequate purchase of the screw into bone, poor bone
quality, or inadequate screw size.194 Pedicle fracture mayoccur if too large a screw is placed into the pedicle or thescrew is driven out of the pedicular cortex. Sjostrom andassociates255 used CT scans to study the pedicles ofpatients after removal of pedicle screw instrumentationfollowing successful fusion for burst fractures. They found
FIGURE 30–52. A, An anteroposterior (AP) radiograph shows abnormal calcification within the disc spaces at T11–T12 and T12–L1. This finding shouldarouse expectations of detecting a herniated thoracic disc in this symptomatic patient. B, A computed tomographic (CT) scan at T11–T12 documents alarge herniation of a calcified disc fragment with significant compromise of the spinal canal. C, Midsagittal, T1-weighted magnetic resonance imaging (MRI)confirms the significant extent of extrusion of the T11–T12 disc. D, T1-weighted transverse MRI correlates well with the CT scan and again shows thesevere extent of spinal canal compromise. E, T2-weighted transverse MRI best shows the extent of spinal cord compression and actual spinal corddeformation secondary to herniation of the disc. F, This patient was treated by transthoracic T11–T12 discectomy and fusion. G, A follow-up APradiograph confirms satisfactory alignment of the spine.
936 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 62/69 P 936 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 62/69 P 936 BLACK T

that 65% of instrumented pedicles increased in width, asdid 85% of those in which the screw diameter was greaterthan 65% of the diameter of the pedicle. This result,however, may not have clinical consequences. The authorsemphasized the importance of correct screw size to avoidinjury to the pedicle and subsequent loosening of theimplant.
Occasionally, with severe deformity, maximal bone–screw interface strength is required and necessitatesplacement of the screw deep within the vertebral bodyor through the anterior cortex. This situation is morecommon in a patient with an osteoporotic spine than inone with normal bone density. The need for anteriorcortical fixation must be balanced against the risk of injuryto the anterior vascular structures. This problem may behandled by adding screws at other levels or by augmentingthe fixation with polymethyl methacrylate (rarely used intrauma). However, in fractures, alternatives are usuallyavailable, including noninstrumented fusion, bedrest, andalteration of the instrumentation to a system with laminarfixation.
INJURY RESULTING FROM PLACEMENT OFLAMINAR HOOKS
Dislodgment of laminar hooks occurs most commonly inthe lower lumbar segments. However, proximal dislodg-ment also occurs, particularly when the reduction isinadequate and viscoelastic properties are not taken intoconsideration after the initial distraction. If hooks are notproperly seated or are placed into laminar bone rather thandeep to the anterior lamina or if the rod is not properlycontoured, the hooks may cut out, fracture the lamina, orangulate into the underlying neural tissue. The incidenceof neurologic complications after placement of hooks androds is reportedly about 1%. The use of anatomic hookshelps limit some of these problems. Hook dislodgmentmay be associated with excessive force, weak bone, ortechnical errors (e.g., faulty surgical technique, improperimplant selection, improper contouring). Edwards andLevine80 found that dislodgment of distal hooks placedproximal to L4 occurred in only 4% of their large series ofpatients, but that percentage almost doubled at L4 andtripled at L5.
To avoid these complications, the proper instrumenta-tion should be selected, particularly one with a moreanatomic design. Adequate rod contouring or the additionof a rod sleeve is useful to minimize late failure. Excessivebone resection at the laminotomy site should be avoided,particularly at the upper lamina. It is often necessary toremove only a small portion of the superior lamina tosquare the edge before inserting the hook. Excessivenotching leads to the formation of a stress riser andincreases the risk of subsequent fracture. The lateral jointligaments should also be protected, as much as possible,because they help resist lateral hook cutout. Inferiorly, thelaminotomy should not be extended too far laterallybecause the pars interarticularis may be weakened. Manyof the problems with hook dislodgment from the lamina ordislodgment of the rod from the hook have now beeneliminated with the newest generation of segmentalfixation hook-rod systems.
Dural Tears
A dural laceration and concomitant leak of cerebrospinalfluid may result from the injury or from surgery (see Fig.30–24). Intraoperatively, laceration can occur during expo-sure, instrumentation, or decortication. Regardless of thecause, the site of the injury, once identified, should beadequately visualized (with bone removed as necessary)and the dura repaired.83, 84 If primary repair is not possi-ble, muscle or fascia grafting should be performed to closethe defect. In addition, if the seal is less than adequate, alumbar transdural drain can be placed to reduce cerebro-spinal fluid pressure and permit dural healing.
Infections
Infections can occur after spine surgery, but they arerelatively less common than after instrumentation andfusion for degenerative conditions. Infections superficial tothe fascia can be treated with early and aggressivedebridement and either open packing of the wound orclosure over a drainage tube.
Deep infections should also be treated by aggressiveirrigation and debridement as soon as the infection isnoted. If this complication occurs, we attempt to leave thebone graft and the metal instrumentation system in place.After thorough irrigation, outflow tubes are placed deep tothe fascia and all layers are tightly closed. The outflowdrainage system is maintained for at least 4 days untilcultures from the effluent are clear. Inflow-outflow systemscan also be used. They usually require early high flow (upto 500 mL/hr) of saline solution through the system tokeep the tubes patent and functioning. Because superin-fections have been noted to occur after 7 to 10 days, thetubes should be removed after this length of time, even ifculture results are still positive. If the infection persists, theprocedure can be repeated once, again trying to salvage thebone graft, the instrumentation, and the reduction.Occasionally, this treatment fails and it is necessary toremove the metal, the bone graft, or both to help eradicatethe infection. An alternative is to pack the wound open,deep to the fascia, and change the dressing at least daily.
Associated Medical Conditions
Improved medical management has reduced the compli-cations associated with spinal cord injury and is respon-sible for a marked increase in life expectancy. However,head injury, musculoskeletal trauma, and visceral damage,which occur concomitantly in up to 60% of patients withspinal cord injury, often complicate treatment. If thepatient is unconscious at initial evaluation, the diagnosis ofspinal cord injury may be difficult to make. Screeningradiographs of the spine and all long bones below the levelof injury should be performed in all patients with head orspinal cord injury. Additionally, after blunt trauma, asignificant number of spinal cord–injured patients have anassociated abdominal injury and may be unable to feel orcommunicate the underlying problem. Reid and co-workers228 reported a 50% incidence of intra-abdominal
937CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 63/69 P 937 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 63/69 P 937 BLACK T

injury associated with Chance fractures in children andadolescents. Anderson and colleagues10 reported a 66%incidence of hollow viscus lesions associated with seatbelt–type injuries, which climbed to 86% in a pediatricsubset. A perforated viscus with associated peritonitis maygo undetected. Because this complication is responsible forsignificant morbidity and death, peritoneal lavage shouldbe a routine part of the initial evaluation of all patientswith spinal cord injury.
Renal failure is a frequent occurrence in patients withspinal cord injury. A gradual decline in the incidence ofthis problem, particularly as a cause of death, has occurredas a result of advances in bladder drainage techniques(e.g., intermittent catheterization). Once the fluid status(inflow and outflow) is normalized in the acute injurystate, intermittent bladder catheterization should be usedin the management of a neurogenic bladder. After furtherurologic evaluation, individualized treatment may beinstituted. Pulmonary complications, already increased inneurologically injured patients, are further worsened if theanterior transthoracic approach is used.11
Late complications in a spinal cord–injured patient canrelate to painful nonunion of the spine, limited neurologicrecovery of spinal cord or root function (particularlybecause limited recovery leads to persistent nerve compro-mise and pain), and medical complications associated withprolonged bedrest, many of which can be avoided by early,rigid immobilization, as discussed earlier in this chapter. Inparticular, disuse osteoporosis is a common problem inparaplegic patients immobilized for even short periods,and it increases their susceptibility to recurrent injuries.85
Finally, individuals with spinal cord injuries may experi-ence intractable spasticity. For this condition, studies haveshown the efficacy of implantable intrathecal baclofenpumps.65
CONCLUSIONz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
The major objective of any treatment is to construct themost stable environment for the spinal cord, nerve roots,and spinal column to allow neurologic improvement.Although the emphasis in this chapter has been on rigidspinal stabilization, it should be stressed that suchstabilization is only one means of achieving this goal. Itsmajor advantage at this time, in addition to stabilizing andprotecting the spinal cord, is that it allows the patient torapidly initiate rehabilitation. Reversibility of spinal cordinjury remains an unsolved medical and surgical problem.However, rehabilitation has greatly improved the quality oflife of patients with spinal injuries.
Intensive rehabilitation should begin as early as possi-ble, with the major objective being attainment of func-tional independence. The final functional level dependsprimarily on the level and severity of the neurologic deficit.Surgical instrumentation of the spine and effective spinalorthoses permit earlier mobilization of the patient in theacute phase and may allow patients to reach their func-tional level sooner. The best selection of treatment dependson understanding the anatomy, the mechanics of the injuryand the forces involved, and the options that are availableto stabilize and protect the spinal column and cord.
Avoidance of complications associated with the surgicaltreatment of spine injuries requires a thorough knowledgeof the anatomy, an accurate diagnosis, and an understand-ing and experience with the implants chosen.238 However,although complications can be minimized, they cannot beeliminated.
REFERENCES
1. Aaro, S.; Ohlen, G. The effect of Harrington instrumentation on thesagittal configuration and mobility of the spine in scoliosis. Spine8:570–575, 1983.
2. Abe, E.; Sato, K.; Shimada, Y.; et al. Thoracolumbar burst fracturewith horizontal fracture of the posterior column. Spine 22:83–87,1997.
3. Aebi, M.; Etter, C.H.R.; Kehl, T.H.; Thalgott, J. The internal skeletalfixation system. Clin Orthop 227:30–43, 1988.
4. Aebi, M.; Thalgott, J.S. Fractures and dislocations of the thora-columbar spine treated by the internal spinal skeletal fixationsystem. Proc North Am Spine Soc 68, 1987.
5. Akbarnia, B.A.; Crandall, D.G.; Burkus, K.; et al. Use of long rodsand short arthrodesis for burst fractures of the thoracolumbarspine. J Bone Joint Surg Am 76:1629–1635, 1994.
6. Akbarnia, B.A.; Fogarty, J.P.; Tayob, A.A. Contoured Harringtoninstrumentation in the treatment of unstable spinal fractures. ClinOrthop 189:186–194, 1984.
7. Albert, T.J.; Levine, M.J.; An, H.S.; et al. Concomitant noncontig-uous thoracolumbar and sacral fractures. Spine 18:1285–1291,1993.
8. Allen, B.L., Jr.; Ferguson, R.L. The Galveston technique for L-rodinstrumentation of the scoliotic spine. Spine 7:276–284, 1982.
9. An, H.S.; Andreshak, T.G.; Nguyen, C.; et al. Can we distinguishbetween benign versus malignant compression fractures of thespine by magnetic resonance imaging? Spine 20:1776–1782, 1995.
10. Anderson, P.A.; Rivara, F.P.; Maier, R.V.; et al. The epidemiology ofseatbelt-associated injuries. J Trauma 31:60–67, 1991.
11. Anderson, T.M.; Mansour, K.A.; Miller J.I. Thoracic approaches toanterior spinal operations: Anterior thoracic approaches. AnnThorac Surg 55:1447–1452, 1993.
12. Angtuaco, E.J.C.; Binet, E.F. Radiology of thoracic and lumbarfractures. Clin Orthop 189:43–57, 1984.
13. Argenson, C.; Lovitt, J.; Camba, P.M.; et al. Osteosynthesis ofthoracolumbar spine fractures with CD instrumentation. Paperpresented at the Fifth International Congress on CD Instrumenta-tion, Paris, June 1988, pp. 75–82.
14. Ashman, R.B.; Birch, J.G.; Bone, L.B.; et al. Mechanical testing ofspinal instrumentation. Clin Orthop 227:113–125, 1988.
15. Bailey, J.C.; Yuan, H.A.; Fredrickson, B.E. The Syracuse I-Plate.Spine 16(Suppl):120–124, 1991.
16. Balasubramanian, K.; Ranu, H.S.; King, A.I. Vertebral response tolaminectomy. J Biomech 21:813–823, 1978.
17. Ballock, R.T.; Mackersie, R.; Abitbol, J.; et al. Can burst fractures bepredicted from plain radiographs? J Bone Joint Surg Br 74:147–150,1992.
18. Bedbrook, G.M. Recovery of spinal cord function. Paraplegia18:315–323, 1980.
19. Been, H.D. Anterior decompression and stabilization of thora-columbar burst fractures by the use of the Slot-Zielke device. Spine16:70–77, 1991.
20. Been, H.D. Anterior decompression and stabilization of thora-columbar burst fractures using the Slot-Zielke device. Acta OrthopBelg 57:144–161, 1991.
21. Benson, D.R. Unstable thoracolumbar fractures, with emphasis onthe burst fracture. Clin Orthop 280:14–29, 1988.
22. Benson, D.R.; Burkus, J.K.; Montesano, P.X.; et al. Unstablethoracolumbar and lumbar burst fractures treated with the AOFixateur Interne. J Spinal Disord 5:335–343, 1992.
23. Benzel, E.C. Short-segment compression instrumentation for se-lected thoracic and lumbar spine fractures: The short-rod/two-clawtechnique. J Neurosurg 79:335–340, 1993.
24. Berry, J.L.; Moran, J.M.; Berg, W.S.; et al. A morphometric study ofhuman lumbar and selected thoracic vertebrae. Spine 12:362–367,1987.
25. Bishop, W.J. The Early History of Surgery. London, Robert Hale,1960.
938 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 64/69 P 938 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 64/69 P 938 BLACK T

26. Blumenthal, S.; Gill, K. Complications of the Wiltse pedicle screwsystem. Spine 18:1867–1871, 1993.
27. Bohler, J. Operative treatment of fractures of the dorsal and lumbarspine. J Trauma 10:1119–1122, 1970.
28. Bohlman, H.H. Current concepts review: Treatment of fractures anddislocations of the thoracic and lumbar spine. J Bone Joint Surg Am76:165–169, 1985.
29. Bohlman, H.H.; Eismont, F.J. Surgical techniques of anteriordecompression and fusion for spinal cord injuries. Clin Orthop154:57–67, 1981.
30. Bohlman, H.H.; Freehafer, A.; Dejak, J. The results of treatment ofacute injuries of the upper thoracic spine with paralysis. J BoneJoint Surg Am 67:360–369, 1984.
31. Bohlman, H.H.; Zdelblick, T.A. Anterior excision of thoracic discs.J Bone Joint Surg Am 70:1038–1047, 1988.
32. Bradford, D.S.; McBride, G.G. Surgical management of thoracolum-bar spine fractures with incomplete neurologic deficits. Clin Orthop218:201–216, 1987.
33. Brant-Zawadski, M.; Jeffrey, R.B.; Minagi, H.; et al. High resolutionCT of thoracolumbar fractures. AJNR Am J Neuroradiol 3:69–74,1982.
34. Bravo, P.; Labarta, C.; Alcaraz, M.A.; et al. Outcome after vertebralfractures with neurological lesion treated either surgically orconservatively in Spain. Paraplegia 31:358–366, 1993.
35. Breasted, J.H., ed. The Edwin Smith Papyrus. Chicago, Universityof Chicago Press, 1930.
36. Brightman, R.P.; Miller, C.A.; Rea, G.L.; et al. Magnetic resonanceimaging of trauma to the thoracic and lumbar spine. Spine17:541–550, 1992.
37. Brown, T.; Hansen, R.T.; Yorra, A.J. Some mechanical tests on thelumbosacral spine with particular reference to the intervertebraldiscs. J Bone Joint Surg Am 39:1135–1164, 1957.
38. Burke, D.C. Hyperextension injuries of the spine. J Bone Joint SurgBr 153:3–12, 1971.
39. Cain, J.E.; DeJong, J.T.; Dinenberg, A.S.; et al. Pathomechanicalanalysis of thoracolumbar burst fracture reduction: A calf spinemodel. Spine 18:1647–1654, 1993.
40. Cammisa, F.P.; Eismont, F.J.; Green, A.B. Dural laceration occurringwith burst fractures and associated laminar fractures. J Bone JointSurg Am 71:1044–1052, 1989.
41. Cantor, J.B.; Lebwohl, N.H.; Garvey, T.; et al. Nonoperativemanagement of stable thoracolumbar burst fractures with earlyambulation and bracing. Spine 18:971–976, 1993.
42. Carl, A.L.; Tromanhauser, S.G.; Roger, D.J. Pedicle screw in-strumentation for thoracolumbar burst fractures and fracture-dislocations. Spine 17(Suppl):317–324, 1992.
43. Carson W.L.; Duffield R.C.; Arent, M.; et al. Internal forces andmoments in transpedicular spine instrumentation. The effect ofpedicle screw angle and transfixation—The 4R-4bar linkageconcept. Spine 15:893–901, 1990.
44. Chance, G.Q. Note on a type of flexion fracture of the spine. BrJ Radiol 21:452–453, 1948.
45. Chen W.J.; Niu C.C.; Chen, L.H.; et al. Back pain after thoracolum-bar fracture treated with long instrumentation and short fusion.J Spinal Disord 8:474–478, 1995.
46. Chiba, M.; McLain, R.F.; Yerby, S.A.; et al. Short-segment pedicleinstrumentation: Biomechanical analysis of supplemental hookfixation. Spine 21:288–294, 1996.
47. Clark, J.A.; Hsu, L.C.; Yau, A.C.M.C. Viscoelastic behavior ofdeformed spines under correction with halo pelvic distraction. ClinOrthop 110:90–111, 1975.
48. Clohisy, J.C.; Akbarnia, B.A.; Bucholz, R.D. Neurologic recoveryassociated with anterior decompression of spine fractures at thethoracolumbar junction (T12-L1). Spine 17(Suppl):325–328,1992.
49. Convery, F.R.; Minteer, M.A.; Smith, R.N. Fracture dislocation of thedorsal lumbar spine: Acute operative stabilization by Harringtoninstrumentation. Spine 3:160–166, 1978.
50. Cotler, J.M.; Vernace, J.V.; Michalski, J.A. The use of Harringtonrods in thoracolumbar fractures. Orthop Clin North Am 17:87–103, 1986.
51. Cotrel, Y.; Dubousset, J.; Guillaumat, M. New universal instrumen-tation in spinal surgery. Clin Orthop 227:10–23, 1988.
52. Cresswell, T.R.; Marshall, P.D.; Smith, R.B. Mechanical stability ofthe AO internal spinal fixation system compared with that of theHartshill rectangle and sublaminar wiring in the management of
unstable burst fractures of the thoracic and lumbar spine. Spine23:111–115, 1998.
53. Crowe, P.; Gertzbein, S.D. Spinal canal clearance in burst fracturesusing the AO internal fixator. Paper presented at the CombinedMeeting of the Scoliosis Research Society and the European SpinalDeformity Society, Amsterdam, September 1989, pp. 590–591.
54. Crutcher, J.P.; Anderson, P.A.; King, H.A.; et al. Indirect spinal canaldecompression in patients with thoracolumbar burst fracturestreated by posterior distraction rods. J Spinal Disord 4:39–48,1991.
55. Daniaux, H.; Seykora, P.; Genelin, A.; et al. Application of posteriorplating and modifications in thoracolumbar spine injuries: Indica-tions, techniques, and results. Spine 16(Suppl):125–133, 1991.
56. Davies, W.E.; Morris, J.H.; Hill, V. An analysis of conservative(nonsurgical) management of thoracolumbar fractures and fracture-dislocations with neural damage. J Bone Joint Surg Am 62:1324–1328, 1980.
57. Dekutoski, M.B.; Conlan, E.S.; Salciccioli, G.G. Spinal mobility anddeformity after Harrington rod stabilization and limited arthrodesisof thoracolumbar fractures. J Bone Joint Surg Am 75:168–176,1993.
58. Denis, F. The three column spine and its significance in theclassification of acute thoracolumbar spinal injuries. Spine 8:817–831, 1983.
59. Denis, F.; Armstrong, G.W.D.; Searls, K.; et al. Acute thoracolumbarburst fractures in the absence of neurologic deficit. Clin Orthop189:142–149, 1984.
60. Denis, F.; Burkus, J.K. Shear fracture-dislocations of the thoracicand lumbar spine associated with forceful hyperextension (lumber-jack paraplegia). Spine 17:156–161, 1992.
61. Denis, F.; Ruiz, H.; Searls, K. Comparison between square-endeddistraction rods and standard round-ended distraction rods in thetreatment of thoracolumbar spinal injuries: A statistical analysis.Clin Orthop 189:162–167, 1984.
62. Dewald, R.L. Burst fractures of the thoracic and lumbar spine. ClinOrthop 189:150–161, 1984.
63. Dick, W. The ‘‘Fixateur Interne’’ as a versatile implant for spinesurgery. Spine 12:882–900, 1987.
64. Dick, W.; Kluger, P.; Magerl, F.; et al. A new device for internalfixation of thoracolumbar and lumbar spine fractures: The ‘‘FixateurInterne.’’ Paraplegia 23:225–232, 1985.
65. Dickman, C.A.; Yahiro, M.A.; Lu, H.T.C.; et al. Surgical treatmentalternatives for fixation of unstable fractures of the thoracic andlumbar spine: A meta-analysis. Spine 19(Suppl):2266–2273, 1994.
66. Dickson, J.H.; Harrington, P.R.; Erwin, W.D. Results of reductionand stabilization of the severely fractured thoracic and lumbarspine. J Bone Joint Surg Am 60:799–805, 1978.
67. Dodd, C.A.F.; Fergusson, C.M.; Pearcy, M.J.; et al. Vertebral motionmeasured using biplanar radiography before and after Harringtonrod removal for unstable thoracolumbar fractures of the spine.Spine 11:452–455, 1986.
68. Doerr, T.E.; Montesano, P.X.; Burkus, J.K.; et al. Spinal canaldecompression in traumatic thoracolumbar burst fractures: Poster-ior distraction rods versus transpedicular screw fixation. J OrthopTrauma 4:403–411, 1991.
69. Dommisse, G.F. The arteries, arterioles, and capillaries of the spinalcord. Surgical guidelines in the prevention of postoperativeparaplegia. Ann R Coll Surg 62:369–376, 1980.
70. Dorr, L.D.; Harvey, J.P.; Nickel, V.L. Clinical review of the earlystability of spine injuries. Spine 7:545–550, 1982.
71. Dove, J. Internal fixation of the lumbar spine: The Hartshillrectangle. Clin Orthop 203:136–140, 1986.
72. Duffield R.C.; Carson W.L.; Chen L.; Voth B. Longitudinal elementsize effect on load sharing, internal loads, and fatigue life of tri-levelspinal implant constructs. Spine 18:1695–1703.
73. Dunham, W.K.; Langford, K.H.; Ostrowsky, D.M. The managementof unstable fractures and dislocations of the thoracic and lumbarspine. Ala J Med Sci 21:194–204, 1984.
74. Durward, Q.J.; Schweigel, J.F.; Harrison, P. Management of fracturesof the thoracolumbar and lumbar spine. Neurosurgery 8:555–561,1981.
75. Dwyer, A.F. Experience of anterior correction of scoliosis. ClinOrthop 93:191, 1973.
76. Ebelke, D.K.; Asher, M.A.; Neff, J.R.; et al. Survivorship analysis ofVSP spinal instrumentation in the treatment of thoracolumbar andlumbar burst fractures. Spine 16(Suppl):428–432, 1991.
939CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 65/69 P 939 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 65/69 P 939 BLACK T

77. Ebraheim, N.A.; Rupp, R.E.; Savolaine, E.R.; et al. Use of titaniumimplants in pedicular screw fixation. J Spinal Disord 7:478–486,1994.
78. Edwards, C.C. Sacral fixation device design and preliminary results.Paper presented at a meeting of the Scoliosis Research Society,1984.
79. Edwards, C.C.; Levine, A.M. Complications associated with poster-ior instrumentation in the treatment of thoracic and lumbarinjuries. In: Garfin, S., ed. Complications of Spine Surgery.Baltimore, Williams & Wilkins, 1989, pp. 164–199.
80. Edwards, C.C.; Levine, A.M. Early rod-sleeve stabilization of theinjured thoracic and lumbar spine. Orthop Clin North Am17:121–145, 1986.
81. Edwards, C.C.; Levine, A.M. Fractures of the lumbar spine. In:Evarts, C.M., ed. Surgery of the Musculoskeletal System. New York,Churchill Livingstone, 1990, pp. 2237–2275.
82. Edwards, C.C.; Levine, A.M.; Weigel, M.C. Determinants ofneurologic recovery following posttraumatic incomplete paraplegia.Orthop Trans 11:453, 1987.
83. Edwards, C.C.; Rosenthal, M.S.; Gellard, F.; et al. The fate ofretropulsed bone following vertebral body fractures. Orthop Trans13:19, 1989.
84. Eismont, F.J.; Wiesel, S.W.; Rothman, R.H. Treatment of dural tearsassociated with spinal surgery. J Bone Joint Surg Am 63:1123–1136,1982.
85. Elias, A.N.; Gwinup, G. Immobilization osteoporosis in paraplegia.J Am Paraplegia Soc 15:163–170, 1993.
86. Elliott, H.C. Cross-sectional diameters and areas of the humanspinal cord. Anat Rec 93:287–293, 1945.
87. Engler, G.L. Cotrel-Dubousset instrumentation for the reduction offracture dislocations of the spine. J Spinal Disord 3:62–66, 1990.
88. Epstein, N.E.; Epstein, J.A. Limbus lumbar vertebral fractures in 27adolescents and adults. Spine 16:962–966, 1991.
89. Esses, S.I.; Botsford, D.J.; Wright, T.; et al. Operative treatment ofspinal fractures with the AO internal fixator. Spine 16(Suppl):146–150, 1991.
90. Fabris, D.; Costantini, S.; Nena, U. Cotrel-Dubousset instrumen-tation in thoracolumbar seat belt–type and flexion-distractioninjuries. J Spinal Disord 7:146–152, 1994.
91. Farcy, J.C.; Weidenbaum, M.; Glassman, S. Sagittal index inmanagement of thoracolumbar burst fractures. Spine 15:958–965,1990.
92. Ferguson, R.L.; Allen, B.L. A mechanistic classification of thora-columbar spine fractures. Clin Orthop 189:77–88, 1984.
93. Ferguson, R.L.; Allen, B.L. An algorithm for the treatment ofunstable thoracolumbar fractures. Orthop Clin North Am 17:105–112, 1986.
94. Finkelstein, J.A.; Chapman, J.R.; Mirza, S. Anterior cortical allograftin thoracolumbar fractures. J Spinal Disord 12:424–429, 1999.
95. Flesch, J.R.; Leider, L.L.; Erickson, D.L.; et al. Harringtoninstrumentation and spine fusion for unstable fractures andfracture-dislocations of the thoracic and lumbar spine. J Bone JointSurg Am 59:143–153, 1977.
96. Floman, Y.; Fast, A.; Pollack, D.; et al. The simultaneousapplications of an interspinous compressive wire and Harringtondistraction rods in the treatment of fracture-dislocation of thethoracic and lumbar spine. Clin Orthop 205:207–215, 1988.
97. Forsyth, H.F. Extension injuries of the cervical spine. J Bone JointSurg Am 46:1792–1797, 1984.
98. Frankel, H.L.; Hancock, D.O.; Hyslop, G.; et al. The value ofpostural reduction in the initial management of closed injuries ofthe spine with paraplegia and tetraplegia. I. Paraplegia 7:179–192,1969.
99. Fredrickson, B.E.; Edwards, W.T.; Rauschning, W.; et al. Vertebralburst fractures: An experimental, morphologic, and radiographicstudy. Spine 17:1012–1021, 1992.
100. Gaines, R.W.; Breedlove, R.F.; Munson, G. Stabilization of thoracicand thoracolumbar fracture-dislocations with Harrington rods andsublaminar wires. Clin Orthop 189:195–203, 1984.
101. Gardner, V.O.; Armstrong, G.W.D. Long-term lumbar facet jointchanges in spinal fracture patients treated with Harrington rods.Spine 15:479–484, 1990.
102. Gardner, V.O.; Thalgott, J.S.; White, J.I.; et al. The contouredanterior spinal plate system (CASP). Spine 19:550–555, 1994.
103. Garfin, S.R.; Gertzbein, S.D.; Eismont, F. Fractures of the lumbarspine: Evaluation, classification, and treatment. In: Wiesel, S.,
ed. The Lumbar Spine. Philadelphia, W.B. Saunders, 1996,pp. 822–873.
104. Garfin, S.R.; Katz, M.M. The vertebral column: Clinical aspects. In:Nahum, A.M.; Melvin, J., eds. The Biomechanics of Trauma.Norwalk, CT, Appleton-Century-Crofts, 1985, pp. 301–340.
105. Garfin, S.R.; Katz, N.M.; Marshall, L.F. Spinal cord. In: Cales, R.H.;Heelig, R.W., Jr., eds. Trauma Care Systems. Rockville, MD, Aspen,1986.
106. Garfin, S.R.; Mowery, C.A.; Guerra, J.; et al. Confirmation of theposterolateral technique to decompress and fuse thoracolumbarspine burst fractures. Spine 10:218–228, 1985.
107. Garin, D.M.; Leal, C.V.; Granell, J.B. Stabilization of the lowerthoracic and lumbar spine with the internal skeletal fixation systemand a cross-linkage system: First results of treatment. Acta OrthopBelg 58:36–42, 1992.
108. Georgis, T.; Rydevik, B.; Weinstein, J.N.; Garfin, S.R. Complicationsof pedicle screw fixation. In: Garfin, S., ed. Complications of SpineSurgery. Baltimore, Williams & Wilkins, 1989, pp. 200–210.
109. Gereesan, G. Cotrel-Dubousset pedicle fixation in fractures ofthoracic and lumbar spine. Abstract. Paper presented at the SixthInternational Congress on CD Instrumentation, Monte Carlo,September 1989.
110. Gertzbein, S.D. Classification of thoracic and lumbar fractures. In:Gertzbein, S.D., ed. Fractures of the Thoracic and Lumbar Spine.Baltimore, Williams & Wilkins, 1993.
111. Gertzbein, S.D. Scoliosis Research Society: Multicenter spinefracture study. Spine 17:528–540, 1992.
112. Gertzbein, S.D.; Court-Brown, C.M. Flexion-distraction injuries ofthe lumbar spine: Mechanisms of injury and classification. ClinOrthop 227:52–60, 1988.
113. Gertzbein, S.D.; Court-Brown, C.M.; Marks, P.; et al. The neurologicoutcome following surgery for spinal fractures. Spine 13:641–644,1988.
114. Gertzbein, S.D.; Harris, M.B. Wedge osteotomy for the correction ofposttraumatic kyphosis. Spine 17:374–379, 1992.
115. Ghanayem, A.J.; Zdeblick, T.A. Anterior instrumentation in themanagement of thoracolumbar burst fractures. Clin Orthop335:89–100, 1997.
116. Goll, S.R.; Balderston, R.A.; Stambough, J.L.; et al. Depth ofintraspinal wire penetration during passage of sublaminar wires.Spine 13:503–509, 1988.
117. Grantham, S.A.; Malberg, M.I.; Smith, D.M. Thoracolumbar spineflexion-distraction injury. Spine 1:172, 1976.
118. Graziano, G.P. Cotrel-Dubousset hook and screw combinations forspine fractures. J Spinal Disord 6:380–385, 1993.
119. Griffith, H.B.; Gleave, J.R.; Taylor, R.G. Changing patterns offractures of the dorsal and lumbar spine. BMJ 1:891, 1966.
120. Gumley, G.; Taylor, T.K.F. Distraction fractures of the lumbar spine.J Bone Joint Surg Br 64:520–525, 1982.
121. Gurr, K.R.; McAfee, P.C.; Shih, C.M. Biomechanical analysis ofanterior and posterior instrumentation systems after corpectomy: Acalf spine model. J Bone Joint Surg Am 70:1182–1191, 1988.
122. Gurwitz, G.S.; Dawson, J.M.; McNamara, M.J.; et al. Biomechanicalanalysis of three surgical approaches for lumbar burst fracturesusing short-segment instrumentation. Spine 19:977–982, 1993.
123. Guttman, L. History of the National Spinal Injuries Centre, StokeMandeville Hospital, Aylesbury. Paraplegia 5:115–126, 1967.
124. Guttman, L. Spinal Cord Injuries: Comprehensive Management andResearch. Oxford, Blackwell, 1973.
125. Haas, N.; Blauth, M.; Tscherne, H. Anterior plating in thoracolum-bar spine injuries. Spine 16(Suppl):100–111, 1991.
126. Hardaker, W.T.; Cook, W.A.; Friedman, A.H.; et al. Bilateraltranspedicular decompression and Harrington rod stabilization ofsevere thoracolumbar burst fractures. Spine 17:162–171, 1992.
127. Harrington, R.M.; Budorick, T.; Hoyt, J.; et al. Biomechanics ofindirect reduction of bone retropulsed into the spinal canal invertebral fracture. Spine 18:692–699, 1993.
128. Harryman, D.T. Complete fracture-dislocation of the thoracic spineassociated with spontaneous neurologic decompression: A casereport. Clin Orthop 207:64–69, 1986.
129. Hazel, W.A.; Jones, R.A.; Morrey, B.F.; Stauffer, R.N. Vertebralfractures without neurological deficit. A long-term follow-up study.J Bone Joint Surg Am 70:1318–1321, 1988.
130. Heggeness, M.H.; Doherty, B.J. Trabecular anatomy of thoracolum-bar vertebrae: Implications for burst fractures. J Anat 191:309–312,1997.
940 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 66/69 P 940 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 66/69 P 940 BLACK T

131. Herring, J.A.; Wenger, D.R. Segmental spinal instrumentation: Apreliminary report of 40 consecutive cases. Spine 7:285–298, 1982.
132. Hilibrand, A.S.; Moore, D.C.; Graziano, G.P. The role of pedicu-lolaminar fixation in compromised pedicle bone. Spine 21:445–451, 1996.
133. Holdsworth, F.W. Fractures, dislocations, and fracture-dislocationsof the spine. J Bone Joint Surg Am 52:1534–1551, 1970.
134. Hu, R.W.; Bohlman, H.H. Fracture at the iliac bone graft harvest siteafter fusion of the spine. Clin Orthop 309:208–213, 1994.
135. Hu, S.; Capen, D.A.; Rimoldi, R.L.; et al. The effect of surgicaldecompression on neurologic outcome after lumbar fractures. ClinOrthop 288:166–173, 1993.
136. Huelke, D.F.; Kaufer, H. Vertebral column injuries and seat belts.J Trauma 15:304–318, 1975.
137. Huntington, C.F.; Murrell, W.D.; et al. Comparison of thoracoscopicand open thoracic discectomy in a live ovine model for anteriorspinal fusion. Spine 23:1699–1702, 1998.
138. Jackson, R.H.; Quisling, R.G.; Day, A.I. Fracture and completedislocation of the thoracic or lumbosacral spine: Report of threecases. Neurosurgery 5:250–253, 1979.
139. Jacobs, R.R.; Asher, M.A.; Snider, R.K. Thoracolumbar spinalinjuries: A comparative study of recumbent and operative treatmentin 100 patients. Spine 5:463–477, 1980.
140. Jacobs, R.R.; Schlaepfer, F.; Mathys, R.R.; et al. A locking hookspinal rod system for stabilization of fracture-dislocations andcorrection of deformities of the dorsolumbar spine: A biomechanicsevaluation. Clin Orthop 189:168–177, 1984.
141. James, K.S.; Wenger, K.H.; Schlegel, J.D.; et al. Biomechanicalevaluation of the stability of thoracolumbar burst fractures. Spine19:1731–1740, 1994.
142. Jelsma, R.K.; Kirsch, P.T.; Jelsma, L.F.; et al. Surgical treatment ofthoracolumbar fractures. Surg Neurol 18:156–166, 1982.
143. Jodoin, A.; DuPuis, P.; Fraser, M.; et al. Unstable fractures of thethoracolumbar spine: A 10-year experience at Sacre Coeur Hospital.J Trauma 25:197–202, 1985.
144. Johnston, C.E.; Happel, L.T.; Norris, R.; et al. Delayed paraplegiacomplicating sublaminar segmental spinal instrumentation. J BoneJoint Surg Am 68:556–563, 1986.
145. Kahanovitz, N.; Bullough, P.; Jacobs, R.R. The effect of internalfixation without arthrodesis on human facet joint cartilage. ClinOrthop 189:204, 1984.
146. Kaneda, K.; Asano, S.; Hashimoto, T.; et al. The treatment ofosteoporotic-posttraumatic vertebral collapse using the Kanedadevice and a bioactive ceramic vertebral prosthesis. Spine17(Suppl):295–303, 1992.
147. Kaneda, K.; Taneichi, H.; Abumi, K.; et al. Anterior decompressionand stabilization with the Kaneda device for thoracolumbar burstfractures associated with neurological deficits. J Bone Joint Surg Am79:69–83, 1997.
148. Karlstron, G.; Olerud, S.; Sjostrom, L. Transpedicular segmentalfixation: Description of a new procedure. Orthopedics 11:689–700,1988.
149. Katonis, P.G.; Katonis, G.M.; Loupasis, G.A.; et al. Treatment ofunstable thoracolumbar and lumbar spine injuries using Cotrel-Dubousset instrumentation. Spine 24:2352–2357, 1999.
150. Kaufer, H.; Hayes, J.T. Lumbar fracture-dislocation. J Bone JointSurg Am 48:712–730, 1966.
151. Keene, J.S.; Goletz, T.H.; Lilleas, F.; et al. Diagnosis of vertebralfractures. J Bone Joint Surg Am 64:586–595, 1982.
152. Keene, J.S.; Wackwitz, D.L.; Drummond, D.S.; et al. Compression-distraction instrumentation of unstable thoracolumbar fractures:Anatomic results obtained with each type of injury and method ofinstrumentation. Spine 11:898–902, 1986.
153. Kelly, R.P.; Whitesides, T.E. Treatment of lumbodorsal fracture-dislocations. Ann Surg 167:705–717, 1968.
154. Kifune, M.; Panjabi, M.M.; Liu, W. Fracture pattern and instabilityof thoracolumbar injuries. Eur Spine J 4:98–103, 1995.
155. Kerslake, R.W.; Jaspan, T.; Worthington, B.S. Magnetic resonanceimaging of spine trauma. Br J Radiol 64:386–402, 1991.
156. King, A.G. Burst compression fractures of the thoracolumbar spine:Pathologic anatomy and surgical management. Orthopedics 10:1711–1719, 1987.
157. Kinnard, P.; Ghibely, A.; Gordon, D.; et al. Roy-Camille plates inunstable spinal conditions: A preliminary report. Spine 11:131–135, 1986.
158. Kirkpatrick, J.S.; Wilber, R.G.; Likavec, M.; et al. Anterior
stabilization of thoracolumbar burst fractures using the Kanedadevice: A preliminary report. Orthopedics 18:673–678, 1995.
159. Klose, K.J.; Goldberg, M.L.; Smith, R.S.; et al. Neurological changefollowing spinal cord injury: An assessment technique andpreliminary results. Model Sys Sci Digest 3:35–42, 1980.
160. Kostuik, J.P. Anterior fixation for fractures of the thoracic andlumbar spine with or without neurologic involvement. Clin Orthop189:103–115, 1984.
161. Kostuik, J.P.; Munting, E.; Valdevit, A. Biomechanical analysis ofscrew load sharing. J Spinal Disord 7:394–401, 1994.
162. Kothe R.; O’Holleran J.D.; Liu, W.; Panjabi, M.M. Internalarchitecture of the thoracic pedicle. An anatomic study. Spine21:264–270, 1996.
163. Kothe, R.; Panjabi, M.M.; Liu, W. Multidirectional instability of thethoracic spine due to iatrogenic pedicle injuries during transpedicu-lar fixation. A biomechanical investigation. Spine 22:1836–1842,1997.
164. Krag, M.H.; Beynnon, B.D.; Pope, M.H. Depth of insertion oftranspedicular vertebral screws into human vertebrae: Effectupon screw-vertebra interface strength. J Spinal Disord 1:287–294,1988.
165. Krag, M.H.; Beynnon, B.D.; Pope, M.H.; et al. An internal fixator forposterior application to short segments of the thoracic, lumbar orlumbosacral spine. Clin Orthop 203:75–78, 1986.
166. Krag, M.H.; Weaver, D.L.; Beynnon, B.D.; et al. Morphometry of thethoracic and lumbar spine related to transpedicular screw place-ment for surgical spine fixation. Spine 13:27–32, 1988.
167. Krengel, W.F.; Anderson, P.A.; Henley, M.B. Early stabilization anddecompression for incomplete paraplegia due to a thoracic-levelspinal cord injury. Spine 18:2080–2087, 1993.
168. Krompinger, W.J.; Fredrickson, B.E.; Mino, D.E.; et al. Conservativetreatment of fractures of the thoracic and lumbar spine. OrthopClin North Am 17:161–170, 1986.
169. Kurz, L.T.; Garfin, S.R.; Booth, R.E. Harvesting autogenous iliacbone grafts: A review of complications and techniques. Spine14:1324–1331, 1989.
170. Laborde, J.M.; Bahniuk, E.; Bohlman, H.H.; et al. Comparison offixation of spinal fractures. Clin Orthop 152:303–310, 1980.
171. Landreneau, R.J.; Hazelrigg, S.R.; Mack, M.J.; et al. Postoperativepain related morbidity: Video assisted thoracoscopy vs. thoracot-omy. Ann Thorac Surg 56:1285–1289. 1993.
172. Lemons, V.R.; Wagner, F.C.; Montesano, P.X. Management ofthoracolumbar fractures with accompanying neurological injury.Neurosurgery 30:667–671, 1992.
173. Lesoin, F.; Leys, D.; Rousseaux, M.; et al. Thoracic disc herniationand Scheuermann’s disease. Eur Neurol 26:145–152, 1987.
174. Levine, A.; Bosse, M.; Edwards, C.C. Bilateral facet dislocations inthe thoracolumbar spine. Spine 13:630–640, 1988.
175. Levine, A.M.; Edwards, C.C. Complications in the treatment ofacute spinal injury. Orthop Clin North Am 17:183–203, 1986.
176. Levine, A.M.; Edwards, C.C. Lumbar spine trauma. In: Camins, M.;O’Learly, P., eds. The Lumbar Spine. New York, Raven, 1987,pp. 183–212.
177. Lewis, J.; McKibbin, B. The treatment of unstable fracture-dislocations of the thoracolumbar spine accompanied by paraple-gia. J Bone Joint Surg Br 56:603–612, 1974.
178. Lindahl, S.; Willen, J.; Irstam, L. Unstable thoracolumbar fractures:A comparative radiologic study of conservative treatment andHarrington instrumentation. Acta Radiol 26:67–77, 1985.
179. Lindsey, R.W.; Dick, W. The Fixateur Interne in the reduction andstabilization of thoracolumbar fractures in patients with neurologicdeficits. Spine 16(Suppl):140–145, 1991.
180. Liu, C.L.; Wang, S.; Lin, H.J.; et al. AO Fixateur Interne in treatingburst fractures of the thoracolumbar spine. Zhonghua Yi Xue Za Zhi(Taipei) 62:619–625, 1999.
181. Logue, V. Thoracic intervertebral disc prolapse with spinal cordcompression. J Neurol Neurosurg Psychiatry 15:227–241, 1952.
182. Louis, R. Fusion of the lumbar and sacral spine by internal fixationwith screw plates. Clin Orthop 203:18–33, 1986.
183. Louis, R. Surgery of the Spine. New York, Springer-Verlag,1983, p. 78.
184. Lu J.; Ebraheim, N.A.; Biyani, A.; et al. Vulnerability of greatmedullary artery. Spine 21:1852–1855, 1996.
185. Luque, E.R.; Cassis, N.; Ramirez-Wiella, G. Segmental spinalinstrumentation in the treatment of fractures of the thoracolumbarspine. Spine 7:312–317, 1982.
941CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 67/69 P 941 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 67/69 P 941 BLACK T

186. Magerl, F.P. Stabilization of the lower thoracic and lumbar spinewith external skeletal fixation. Clin Orthop 189:125–141, 1984.
187. Maiman, D.J.; Larson, S.J.; Luck, E.; et al. Lateral extracavitaryapproach to the spine for thoracic disc herniations: Report of 23cases. Neurosurgery 14:178–182, 1984.
188. Mann, K.A.; McGowan, D.P.; Fredrickson, B.E. A biomechanicalinvestigation of short segment spinal fixation for burst fractureswith varying degrees of posterior disruption. Spine 15:470–478,1990.
189. Markel, D.C.; Graziano, G.P. A comparison study of treatment ofthoracolumbar fractures using the ACE posterior segmental fixatorand Cotrel-Dubousset instrumentation. Orthopedics 18:679–686,1995.
190. Matsuzaki, H.; Tokuhashi, Y.; Wakabayashi, K.; et al. Rigix platesystem for anterior fixation of thoracolumbar vertebrae. J SpinalDisord 10:339–347, 1997.
191. McAfee, P.C. Biomechanical approach to instrumentation of thora-columbar spine: A review article. Adv Orthop Surg 313–327, 1985.
192. McAfee, P.C.; Bohlman, H.H.; Yuan, H.A. Anterior decompressionof traumatic thoracolumbar fractures with incomplete neurologicaldeficit using a retroperitoneal approach. J Bone Joint Surg Am67:89–104, 1985.
193. McAfee, P.C.; Farey, I.D.; Sutterlin, C.E.; et al. Device-relatedosteoporosis with spinal instrumentation: A canine model. Abstract.Paper presented at a meeting of the International Society for theStudy of the Lumbar Spine, Kyoto, Japan, 1989, p. 20.
194. McAfee, P.C.; Weiland, D.J.; Carlow, J.J. Survivorship analysis ofpedicle spinal instrumentation. Spine 16(Suppl):422–427, 1991.
195. McAfee, P.C.; Yuan, H.A.; Frederickson, B.A.; Lubicky, J.P. The valueof computed tomography in thoracolumbar fractures. An analysis ofone hundred consecutive cases and a new classification. J BoneJoint Surg Am 65:461–473, 1983.
196. McAfee, P.C.; Yuan, H.A.; Lasda, N.A. The unstable burst fracture.Spine 7:365–378, 1982.
197. McBride, G.G. Cotrel-Dubousset rods in surgical stabilization ofspine fractures. Spine 18:466–473, 1993.
198. McCormack, T.; Karaikovic, E.; Gaines, R.W. The load sharingclassification of spine fractures. Spine 19:1741–1744, 1994.
199. McEvoy, R.D.; Bradford, D.S. The management of burst fractures ofthe thoracic and lumbar spine: Experience in 53 patients. Spine10:631–637, 1983.
200. McGrory, B.J.; VanderWilde, R.S.; Currier, B.L. Diagnosis of subtlethoracolumbar burst fractures: A new radiographic sign. Spine18:2282–2285, 1993.
201. McGuire RA; The role of anterior surgery in the treatment ofthoracolumbar fractures. Orthopedics 20:959–962, 1997.
202. McKinley, L.M.; Obernchain, T.G.; Roth, K.R. Loss of correctionand late kyphosis as the result of short segment pedicle fixationwith posterior transpedicular decompression. Abstract. Paperpresented at the Sixth International Congress on CD Instrumenta-tion, Monte Carlo, September, 1989.
203. McLain, R.F.; Sparling, E.; Benson, D.R. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures: Apreliminary report. J Bone Joint Surg Am 75:162–167, 1993.
204. Mermelstein, L.E.; McLain, R.F.; Yerby, S.A. Reinforcement ofthoracolumbar burst fractures with calcium phosphate cement. Abiomechanical study. Spine 23:664–671, 1998.
205. Mimatsu, K.; Katoh, F.; Kawakami, N. New vertebral bodyimpactors for posterolateral decompression of burst fracture. Spine18:1366–1368, 1993.
206. Mumford, J.; Weinstein, J.N.; Spratt, K.F.; et al. Thoracolumbarburst fractures: The clinical efficacy and outcome of nonoperativemanagement. Spine 18:955–970, 1993.
207. Nagel, D.A.; Koogle, T.A.; Piziali, R.L.; et al. Stability of the upperlumbar spine following progressive disruptions and the applicationof individual internal and external fixation devices. J Bone JointSurg Am 63:62–70, 1981.
208. Nasca, R.J.; Hollis, J.M.; Lemons, J.E.; et al. Cyclic axial loading ofspinal implants. Spine 10:792–793, 1985.
209. Nash, C.L.; Schatzinger, L.H.; Browno, R.H.; et al. The unstablestable thoracic compression fracture. Spine 2:261, 1977.
210. Nicastro, J.F.; Hartjen, C.A.; Traian, J.; et al. Intraspinal pathwaystaken by sublaminar wires during removal. J Bone Joint Surg Am68:1206–1209, 1986.
211. Nicoll, E.A. Fractures of the dorsolumbar spine. J Bone Joint SurgBr 31:376–394, 1949.
212. O’Brien, J.P.; Stephens, M.M.; Prickett, C.F.; et al. Nylon sublaminarstraps in segmental instrumentation for spinal disorders. ClinOrthop 203:168–171, 1986.
213. Okuyama, K.; Abe, E.; Chiba, M.; et al. Outcome of anteriordecompression and stabilization for thoracolumbar unstable burstfractures in the absence of neurologic deficits. Spine 21:620–625,1996.
214. Olerud, S.; Karltrom, G.; Sjostrom, L. Transpedicular fixation ofthoracolumbar vertebral fractures. Clin Orthop 227:44–51, 1988.
215. Osebold, W.R.; Weinstein, S.L.; Sprague, B.L. Thoracolumbar spinefractures: Results of treatments. Spine 6:13–34, 1981.
216. Panjabi, M.M.; Brand, R.A., Jr.; White, A.A, 3rd. Three-dimensionalflexibility and stiffness properties of the human thoracic spine.J Biomech 9:185–192, 1975.
217. Panjabi, M.M.; Oxland, T.R.; Kifune, M.; et al. Validity of thethree-column theory of thoracolumbar fractures. A biomechanicalinvestigation. Spine 20:1122–1127, 1995.
218. Parke, W.W.; Gammall, K.; Rothman, R.H. Arterial vascularizationof the cauda equina. J Bone Joint Surg Am 63:53–62, 1981.
219. Patterson, R.H.; Arbit, E. A surgical approach through the pediclefor protruded thoracic discs. J Neurosurg 48:768–772, 1978.
220. Paul, R.L.; Michael, R.H.; Dunn, J.E.; Williams, J.P. Anteriortransthoracic surgical decompression of acute spinal cord injuries.J Neurosurg 43:299–307, 1975.
221. Perot, P.H.; Munro, D.D. Transthoracic removal of midline thoracicdisc protrusions causing spinal cord compression. J Neurosurg31:452–458, 1969.
222. Pinzur, M.S.; Meyer, P.R., Jr.; Lautenschlager, E.P.; et al. Measure-ment of internal fixation device support in experimentally pro-duced fractures of the dorsolumbar spine. Orthopedics 2:28, 1979.
223. Place, H.M.; Donaldson, D.H.; Brown, C.W.; et al. Stabilization ofthoracic spine fractures resulting in complete paraplegia: Along-term retrospective analysis. Spine 19:1726–1730, 1994.
224. Post, J.L.; Green, B.A.; Quencer, R.M.; et al. The value of computedtomography in spinal trauma. Spine 7:417–431, 1982.
225. Purcell, G.A.; Markolf, K.L.; Dawson, E.G. Twelfth thoracic–firstlumbar vertebral mechanical stability of fractures after Harrington-rod instrumentation. J Bone Joint Surg Am 63:71–78, 1981.
226. Purnell, M.; Drummond, D.S.; Keene, J.S.; et al. Hex-nut looseningfollowing compression instrumentation of the spine. Clin Orthop203:172–178, 1986.
227. Regan, J.J.; Mack, M.J.; Picetti, G.G., 3rd; et al. A technical reporton video-assisted thoracoscopy in thoracic spinal surgery. Prelimi-nary description. Spine 20:831–837, 1995.
228. Reid, A.B.; Letts, R.M.; Black, G.B. Pediatric chance fractures:Association with intra-abdominal injuries and seatbelt use.J Trauma 30:384–391, 1990.
229. Rennie, W.; Mitchell, N. Flexion dislocation fractures of the lumbarspine. J Bone Joint Surg Am 55:386–390, 1973.
230. Reuben, M.; Schultz, A.; Denis, F.; et al. Bulging of lumbarintervertebral discs. J Biomech 104:187–192, 1982.
231. Riebel, G.D.; Yoo, J.U.; Fredrickson, B.E.; et al. Review ofHarrington rod treatment of spinal trauma. Spine 18:479–491,1993.
232. Riggins, R.S.; Kraus, J.F. The risk of neurological damage withfractures of the vertebrae. J Trauma 17:126–133, 1977.
233. Rimoldi, R.L.; Zigler, J.E.; Capen, D.A.; et al. The effect of surgicalintervention on rehabilitation time in patients with thoracolumbarand lumbar spinal cord injuries. Spine 17:1443–1449, 1992.
234. Rissanen, P.M. The surgical anatomy and pathology of thesupraspinous and interspinous ligaments of the lumbar spine withspecial reference to ligament ruptures. Acta Orthop Scand46(Suppl):1, 1960.
235. Roaf, R. A study of the mechanics of spinal injuries. J Bone JointSurg Br 42:810, 1960.
236. Roberts, J.B.; Curtiss, P.H., Jr. Stability of the thoracic and lumbarspine in traumatic paraplegia following fracture or fracture-dislocation. J Bone Joint Surg Am 52:1115–1130, 1970.
237. Rockwell, H.; Evans, F.G.; Pheasant, H.C. The comparativemorphology of the vertebral spinal column: Its form as related tofunction. J Morphol 63:87, 1938.
238. Roffi, R.P.; Waters, R.L.; Adkins, R.H. Gunshot wounds to the spineassociated with a perforated viscus. Spine 14:808–811, 1989.
239. Rogers, L.F. The roentgenographic appearance of transverse orChance fractures of the spine: The seat belt fracture. AJR AmJ Roentgenol 111:844–849, 1971.
942 SECTION II • Spine
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 68/69 P 942 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 68/69 P 942 BLACK T

240. Rose, R.D.; Welch, W.C.; Balzer, J.R.; Jacobs, G.B. Persistentlyelectrified pedicle stimulation instruments in spinal instrumenta-tion. Technique and protocol development. Spine 22:334–343,1997.
241. Rosenthal, R.E.; Lowery, E.R. Unstable fracture-dislocations of thethoracolumbar spine: Results of surgical treatment. J Trauma20:485–490, 1980.
242. Rossier, A.B.; Cochran, R.P. The treatment of spinal fractures withHarrington compression rods and segmental sublaminar wiring: Adangerous combination. Spine 9:796–799, 1984.
243. Roy-Camille, R.; Saillant, G.; Berteaux, D.; et al. Osteosynthesis ofthoracolumbar spine fractures with metal plates screwed throughthe vertebral pedicles. Reconstr Surg Traumatol 15:2–15, 1976.
244. Roy-Camille, R.; Saillant, G.; Mazel, C. Plating of thoracic,thoracolumbar, and lumbar injuries with pedicle screw plates.Orthop Clin North Am 17:147–159, 1986.
245. Ryan, M.D.; Taylor, T.K.F.; Sherwood, A.A. Bolt-plate fixation foranterior spinal fusion. Clin Orthop 203:196–202, 1986.
246. Saillant, G. Anatomical study of vertebral pedicles: Surgicalapplication. (In French.) Rev Chir Orthop Reparatrice Appar Mot62:151–160, 1976.
247. Sasso, R.C.; Cotler, H.B. Posterior instrumentation and fusion forunstable fractures and fracture-dislocations of the thoracic andlumbar spine. Spine 18:450–460, 1993.
248. Sasso, R.C.; Cotler, H.B.; Reuben, J.D. Posterior fixation of thoracicand lumbar spine fractures using DC plates and pedicle screws.Spine 16(Suppl):134–139, 1991.
249. Schlickewei, W.; Schutzhoff, G.; Kuner, E.H. FruhfunktionelleBehandlung von Frakturen der unteren Brust und Lendenwirbel-saule mit dem Dreipunktekorsett. Unfallchirurg 94:40–44, 1991.
250. Schmidek, H.H.; Gomes, F.B.; Seligson, D.; et al. Management ofacute unstable thoracolumbar (T11-L1) fractures with and withoutneurological deficit. Neurosurgery 7:30–35, 1980.
251. Shiba, K.; Katsuki, M.; Ueta, T.; et al. Transpedicular fixation withZielke instrumentation in the treatment of thoracolumbar andlumbar injuries. Spine 19:1940–1949, 1994.
252. Shultz, A.; Benson, D.; Hirsch, C. Force deformation properties ofhuman costosternal and costovertebral articulations. J Biomech7:311, 1974.
253. Shuman, W.P.; Rogers, J.V.; Sickler, M.E.; et al. Thoracolumbar burstfractures: CT dimensions of the spinal canal relative to postsurgicalimprovement. AJNR Am J Neuroradiol 6:337–341, 1985.
254. Sim, E. Location of transpedicular screws for fixation of the lowerthoracic and lumbar spine. Acta Orthop Scand 64:28–32, 1993.
255. Sjostrom, L.; Jacobsson, O.; Karlstrom, G.; et al. CT analysis ofpedicles and screw tracts after implant removal in thoracolumbarfractures. J Spinal Disord 6:225–231, 1993.
256. Sjostrom, L.; Jacobsson, O.; Karlstrom, G.; et al. Spinal canalremodelling after stabilization of thoracolumbar burst fractures. EurSpine J 3:312–317, 1994.
257. Smith, W.S.; Kaufer, A. Patterns and mechanisms of lumbar injuriesassociated with lap seat belts. J Bone Joint Surg Am 51:239–254,1969.
258. Soreff, J.; Axdorph, G.; Bylund, P.; et al. Treatment of patients withunstable fractures of the thoracic and lumbar spine. Acta OrthopScand 53:369–381, 1982.
259. Stagnara, P.; Demauroy, J.V.; Dran, G.; et al. Reciprocal angulation ofvertebral bodies in a sagittal plane: Approach to references for theevaluation of kyphosis and lordosis. Spine 7:335–342, 1982.
260. Stambough, J.L. Cotrel-Dubousset instrumentation and thora-columbar spine trauma: A review of 55 cases. J Spinal Disord7:461–469, 1994.
261. Stanger, K.J. Fracture-dislocation of the thoracolumbar spine.J Bone Joint Surg Am 29:107, 1947.
262. Stauffer, E.S. Current concepts review: Internal fixation of fracturesof the thoracolumbar spine. J Bone Joint Surg Am 66:1136–1138,1984.
263. Stauffer, E.S.; Neil, J.L. Biomechanical analysis of structural stabilityof internal fixation in fractures of the thoracolumbar spine. ClinOrthop 112:159–164, 1975.
264. Steffee, A.D.; Biscup, R.S.; Sitkowski, D.J. Segmental spine plateswith pedicle screw fixation: A new internal fixation device fordisorders of the lumbar and thoracolumbar spine. Clin Orthop203:45–53, 1986.
265. Suk, S.I.; Shin, B.O.; Lee, C.S.; et al. CD pedicle screws in thetreatment of unstable lumbar fractures. Paper presented at the FifthInternational Congress on CD Instrumentation, Paris, June 1988,pp. 93–102.
266. Vaccaro, A.R.; Rizzolo, S.J.; Allardyce, T.J.; et al. Placement ofpedicle screws in the thoracic spine: Part I. Morphometric analysisof the thoracic vertebrae. J Bone Joint Surg Am 77:1193–1199,1995.
267. Vaccaro, A.R.; Rizzolo, S.J.; Balderston, R.A.; et al. Placement ofpedicle screws in the thoracic spine: Part II. An anatomical andradiographic assessment. J Bone Joint Surg Am 77:1200–1206,1995.
268. Viale, G.L.; Silvestro, C.; Francaviglia, N.; et al. Transpediculardecompression and stabilization of burst fractures of the lumbarspine. Surg Neurol 40:104–111, 1993.
269. Watson-Jones, R. Fractures and Joint Injuries, 4th ed. Baltimore,Williams & Wilkins, 1960.
270. Weinstein, J.N.; Spratt, K.F.; Spengler, D.; et al. Spinal pediclefixation: Reliability and validity of roentgenogram-based assessmentand surgical factors on successful screw placement. Spine 13:1012,1988.
271. Weitzman, G. Treatment of stable thoracolumbar spine compres-sion fractures by early ambulation. Clin Orthop 76:116–122, 1971.
272. Wenger, D.R.; Carollo, J.J.; Wilkerson, J.A., Jr.; et al. Laboratorytesting of segmental spinal instrumentation versus traditionalHarrington instrumentation for scoliosis treatment. Spine 7:265–269, 1982.
273. White, A.A.; Panjabi, M.M. The basic kinematics of the humanspine: A review of past and current knowledge. Spine 3:12–20,1978.
274. Whitecloud, T.S.; Butler, J.C.; Cohen, J.L.; et al. Complications withthe variable spine plating system. Spine 14:472–476, 1989.
275. Whitesides, T.E. Traumatic kyphosis of the thoracolumbar spine.Clin Orthop 128:78–92, 1977.
276. Wildburger, R.; Mahring, M.; Paszicsnyek, T.; et al. Dorsalstabilization of thoracolumbar spinal instability: Comparison ofthree different implantation systems. Arch Orthop Trauma Surg113:244–247, 1994.
277. Willen, J.; Anderson, J.; Toomoka, K.; et al. The natural history ofburst fractures at the thoracolumbar junction. J Spinal Disord3:39–46, 1990.
278. Willen, J.A.G.; Gaekwad, U.H.; Kakulas, B.A. Acute burst fractures:A comparative analysis of a modern fracture classification andpathologic findings. Clin Orthop 276:169–175, 1992.
279. Willen, J.; Lindahl, S.; Irstam, L.; et al. Unstable thoracolumbarfractures: A study by CT and conventional roentgenology of thereduction effect of Harrington instrumentation. Spine 9:214–219,1984.
280. Williams, E.W.M. Traumatic paraplegia. In: Mathews, D.N., ed.Recent Advances in the Surgery of Trauma. London, ChurchillLivingstone, 1963, p. 171.
281. Wilson, P.D.; Straub, L.R. Lumbosacral fusion with metallic platefixation. Instr Course Lect 9:53–57, 1952.
282. Yosipovitch, Z.; Robin, G.C.; Makin, M. Open reduction of unstablethoracolumbar spinal injuries and fixation with Harrington rods.J Bone Joint Surg Am 59:1003–1013, 1977.
283. Yuan, H.A.; Garfin, S.R.; Dickman, C.A.; et al. A historical cohortstudy of pedicle screw fixation in thoracic, lumbar, and sacral spinalfusions. Spine 19(Suppl):2279–2296, 1994.
284. Yuan, H.A.; Mann, K.A.; Found, E.M.; et al. Early clinicalexperience with the Syracuse I-Plate: An anterior spinal fixationdevice. Spine 13:278–285, 1988.
285. Zindrick, M.R.; Wiltse, L.L.; Doornik, A.; et al. Analysis of themorphometric characteristics of the thoracic and lumbar pedicles.Spine 12:160–166, 1987.
286. Zindrick, M.R.; Wiltse, L.L.; Wiidell, E.H.; et al. A biomechanicalstudy of intrapedicular screw fixation in the lumbosacral spine. ClinOrthop 203:99–112, 1986.
287. Zou, D.; Yoo, J.U.; Edwards, T.; et al. Mechanics of anatomicreduction of thoracolumbar burst fractures: Comparison of distrac-tion plus lordosis. Spine 18:195–203, 1993.
288. Zu, Z.; Maohua, C.; Tianhua, D. Unstable fractures of thoracolum-bar spine treated with pedicle screw plating. Chin Med J (Engl)107:281–285, 1994.
943CHAPTER 30 • Thoracic and Upper Lumbar Spine Injuries
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 69/69 P 943 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h30 10/8/02 39 P 69/69 P 943 BLACK T