Embed Size (px)
Citation preview

www.wjpps.com Vol 8, Issue 6, 2019.
1465
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
CHALLENGES IN DEVELOPMENT OF COLON DRUG DELIVERY
SYSTEM WITH RESPECT TO DISSOLUTION STUDIES
Anchal Gaur1, Dr. Ashu Mittal*
2, Debaprasad Ghosh and Dr. Jagannath Sahoo
Department of Pharmaceutics, KIET School of Pharmacy, Ghaziabad.
ABSTRACT
Colon drug delivery has gained increased importance not only for the
treatment of local diseases associated with colon but also for its
potential for delivery of proteins and therapeutic peptides. Local
delivery allows topical treatment of inflammatory bowel disease,
Crohn‟s disease, Ulcerative colitis. However, treatment can be made
effective if drugs can be targeted directly into colon, thereby reducing
systemic side effects. New technologies have been developed for colon
targeting and to overcome the problem of previous methods. Oral
dosage forms are the most preferred delivery route for colon- specific
delivery due to their convenience. A broad range of in vitro systems is available, from static
monocompartmental to dynamic multicompartmental models. However, these models require
a compromise between technological complexity and biological significance. Further efforts
and technological innovations are still needed to improve in vitro models and meet growing
demands in the areas of health. This review highlights about the challenges in development of
colon drug delivery system with respect to dissolution studies. Oral delivery of drugs in the
colon is valuable in the treatment of diseases of colon where by high local concentration can
be achieved while minimizing side effects.
KEYWORDS: Colon targeted drug delivery, Dissolution, Colon products, Colon
technology.
INTRODUCTION
Colon targeted drug delivery has been the focus of numerous studies in recent years due to its
potential to improve treatment of local diseases affecting the colon, while minimizing
systemic side effects. Some examples of disease states which impact the colon include
Crohn‟s disease, Ulcerative colitis, Irritable Bowel Syndrome.[1,2]
The delivery of drugs to the
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 7.421
Volume 8, Issue 6, 1465-1491 Review Article ISSN 2278 – 4357
Article Received on
20 April 2019,
Revised on 10 May 2019,
Accepted on 31 May 2019,
DOI: 10.20959/wjpps20196-14051
*Corresponding Author
Dr. Ashu Mittal
Department of
Pharmaceutics, KIET School
of Pharmacy, Ghaziabad.

www.wjpps.com Vol 8, Issue 6, 2019.
1466
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
colon via gastrointestinal tract requires protection of a drug from being released in stomach
and small intestine. Drugs, which are destroyed by stomach acid and metabolized by
pancreatic enzymes, are protected. Sustained release of drugs into colon can be useful in
treatment of certain diseases.
The colon is most suitable site for absorption of peptides and protein drugs for following
reasons:[3]
1. Less intensity of digestive enzymes.
2. Proteolytic activity of colon mucosa is less than that observed in small intestine, thus
colon targeted drug delivery system protect peptide and protein drugs from hydrolysis,
and enzymatic degradation in duodenum and jejunum, and releases drug into colon,
which leads to greater bioavailability.[4]
3. And finally, because colon has a long residence time which is up to 5 days and
responsible for enhancement of absorption.[5]
4. Oral route is most convenient and preferred route but other routes for CDDS may be used.
Rectal administration offers shortest route for targeting drugs to colon.[6]
5. The reactions carried out by this gut flora are azoreduction and enzymatic cleavage i.e.
glycosides.
1.1 ADVANTAGES
1. Colon is ideal site for delivery of agents to treat local diseases of colon.
2. Required small drug quantities due to locality targeting.
3. Reduces dosage frequency. Hence lower cost of expensive drugs.
4. Reduced incidence of side effects and drug interactions.
5. Colon is an attractive site where poorly absorbed drug molecules may have an improved
bioavailability.
6. Improve patient compliance.
7. Bypass first pass metabolism.
8. Reduce gastric irritation caused by many drugs like NSAIDS.
9. Flexibility in design.
10. Ulcerative colitis, and Crohn‟s disease are currently treated with glucocorticoids, and
other anti-inflammatory agents.
1.2 DISADVANTAGES
1. Multiple manufacturing steps.
www.wjpps.com Vol 8, Issue 6, 2019.
1467
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
2. Incomplete release rate.
3. Bioavailability of drug is low.
4. Resident microflora could also affect colonic performance via metabolic degradation of
drug.
5. Dose loading is low.
6. Excipients are required in higher quantity.
7. Large no. of process variables.
8. Need of advanced technology.
9. Skilled personal needed for manufacturing of colonic drug delivery system.[7,8]
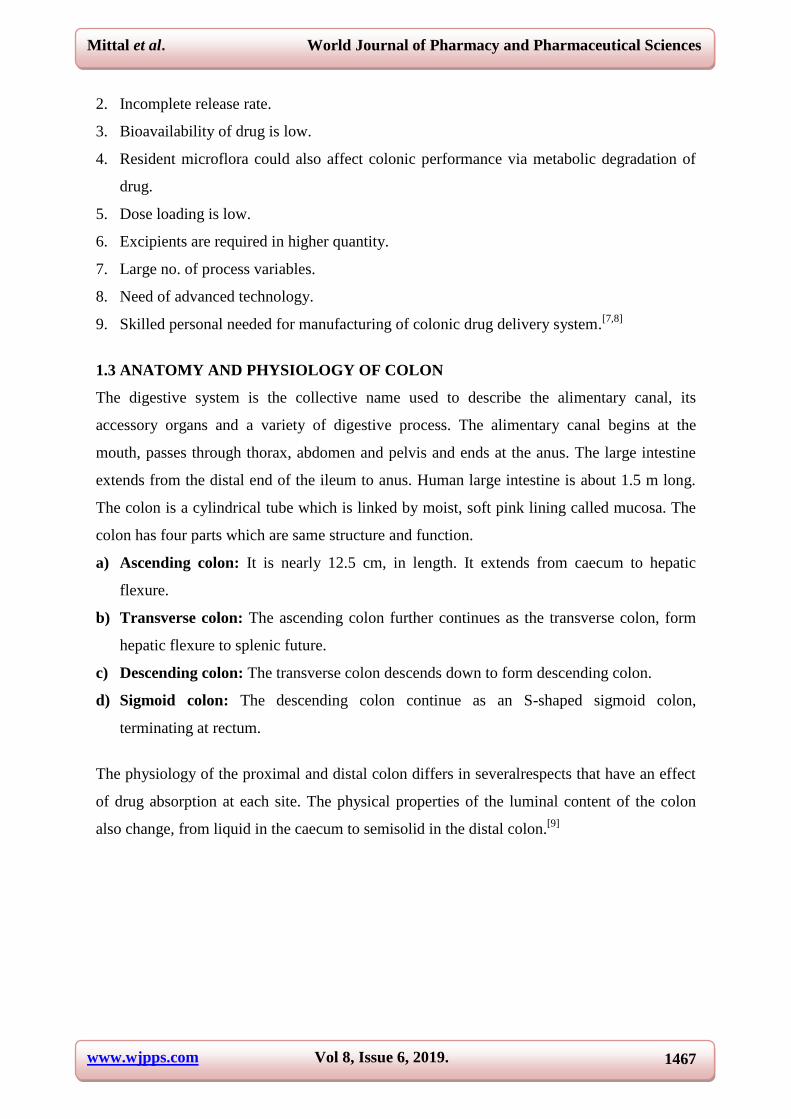
1.3 ANATOMY AND PHYSIOLOGY OF COLON
The digestive system is the collective name used to describe the alimentary canal, its
accessory organs and a variety of digestive process. The alimentary canal begins at the
mouth, passes through thorax, abdomen and pelvis and ends at the anus. The large intestine
extends from the distal end of the ileum to anus. Human large intestine is about 1.5 m long.
The colon is a cylindrical tube which is linked by moist, soft pink lining called mucosa. The
colon has four parts which are same structure and function.
a) Ascending colon: It is nearly 12.5 cm, in length. It extends from caecum to hepatic
flexure.
b) Transverse colon: The ascending colon further continues as the transverse colon, form
hepatic flexure to splenic future.
c) Descending colon: The transverse colon descends down to form descending colon.
d) Sigmoid colon: The descending colon continue as an S-shaped sigmoid colon,
terminating at rectum.
The physiology of the proximal and distal colon differs in severalrespects that have an effect
of drug absorption at each site. The physical properties of the luminal content of the colon
also change, from liquid in the caecum to semisolid in the distal colon.[9]
www.wjpps.com Vol 8, Issue 6, 2019.
1468
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Figure 1: Anatomy of Colon.
1.4 FUNCTIONS OF COLON
Create suitable environment for colonic microorganisms.
Storage reservoir of fecal matter.
Expulsion of the contents of the colon.
Absorption of potassium and water from the lumen.[10]
Table 1: Length of different parts in colon.
Sr.No. Large Intestine Length (cm)
1. Cecum 6-9
2. Ascending colon 20-25
3. Descending colon 10-15
4. Transverse colon 40-45
5. Sigmoid colon 35-40
6. Rectum 12
7. Anal Canal 3
2) COLON PRODUCTS IN MARKET
MARKETED pH DEPENDENT SYSTEMS
DRUG USED
DISEASE POLYMER USED
DOSAGE
FORM DISEASE
Tegaserod
maleate
Eudragit L 100, Eudragit
S 100 Tablet
IrritableBowel
Syndrome.[11]
Prednisolone Eudragit L 100, Eudragit
S 100 Tablet Ulcerative collitis.
[12]
www.wjpps.com Vol 8, Issue 6, 2019.
1469
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
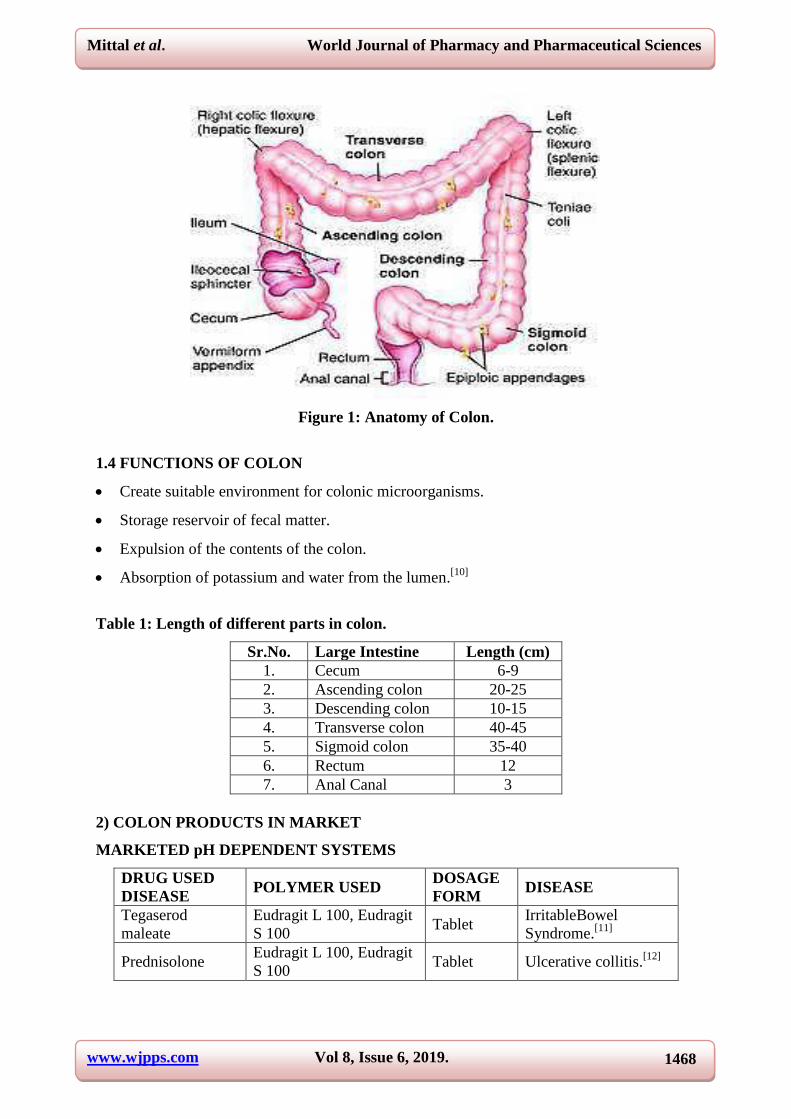
MARKETED TIME DEPENDENT SYSTEMS
DRUG POLYMER USED DOSAGE
FORM LAG TIME
Diltiazem
hydrochloride
Hydroxypropylmethylecellulo
se acetate succinate
(HPAMCAS)
Press coated
tablets
Lag time can be
upto 2-9h in pH
6.8.[13]
Mesalamine HPMCK-100M, HPMCK-4M,
HPMC E15, HPMC E15. Tablets Lag time of 10h.
[14]
MARKETED MICROBIALLY CONTROLLED SYSTEMS
DRUG USED POLYMER USED DOSAGE FORM DISEASE
Valdecoxib
Guar Gum and
Sodium Starch
Glycholate
Tablet Inflammatory
bowel disease.[15]
5- fluorouracil Pectin Tablet Colon cancer.[16]
Metronidazole Sesbania Gum Matrix Tablet Intestinal
Amoebiasis.[17]
NOVEL FORMS OF NATURAL POLYSACCHARIDES USED
DRUG POLYSACCHARIDE DOSAGE FORM
Diclofenac Sodium Chitosan Microspheres
Insulin Chitosan Capsules
Indomethacin Pectin Matrix Tablet
Dexomethasone Guar Gum Matrix Tablet
Indomethacin Chondroitin Sulphate Matrix Tablet
Theophylline Locust- BeanGum Film.[18]
MARKETED PRESSURE CONTROLLED RELEASE SYSTEM
DRUG USED POLYMER USED DOSAGE FORM DISEASE
Caffeine as test drug Ethyl Cellulose Capsule Healthy male
human volunteer
Glycyrrhizin PEG, labrasole Capsule To improve its
bioavailability.[19]
MARKETED HYDROGEL BASED SYSTEM
DRUG USED POLYMER USED APPROACH
USED
METHOD OF
PREPARATION
Satranidazole Chitosan pH sensitive Cross linking
method.[20]
5-fluorouracil
Hydroxyethylmethacrylate,
Methacryloyloxy
azobenzene (MAB)
Degradation by
azoreductase Polymerisation.
[21]
www.wjpps.com Vol 8, Issue 6, 2019.
1470
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
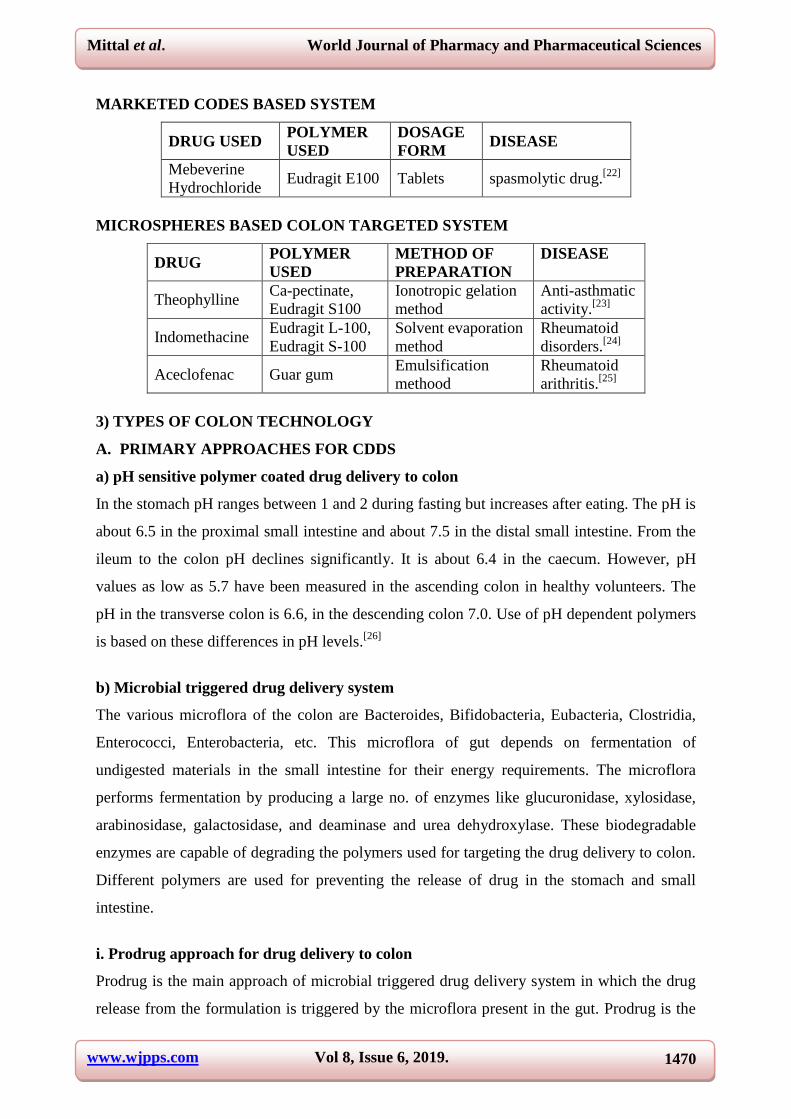
MARKETED CODES BASED SYSTEM
DRUG USED POLYMER
USED
DOSAGE
FORM DISEASE
Mebeverine
Hydrochloride Eudragit E100 Tablets spasmolytic drug.
[22]
MICROSPHERES BASED COLON TARGETED SYSTEM
DRUG POLYMER
USED
METHOD OF
PREPARATION
DISEASE
Theophylline Ca-pectinate,
Eudragit S100
Ionotropic gelation
method
Anti-asthmatic
activity.[23]
Indomethacine Eudragit L-100,
Eudragit S-100
Solvent evaporation
method
Rheumatoid
disorders.[24]
Aceclofenac Guar gum Emulsification
methood
Rheumatoid
arithritis.[25]
3) TYPES OF COLON TECHNOLOGY
A. PRIMARY APPROACHES FOR CDDS
a) pH sensitive polymer coated drug delivery to colon
In the stomach pH ranges between 1 and 2 during fasting but increases after eating. The pH is
about 6.5 in the proximal small intestine and about 7.5 in the distal small intestine. From the
ileum to the colon pH declines significantly. It is about 6.4 in the caecum. However, pH
values as low as 5.7 have been measured in the ascending colon in healthy volunteers. The
pH in the transverse colon is 6.6, in the descending colon 7.0. Use of pH dependent polymers
is based on these differences in pH levels.[26]
b) Microbial triggered drug delivery system
The various microflora of the colon are Bacteroides, Bifidobacteria, Eubacteria, Clostridia,
Enterococci, Enterobacteria, etc. This microflora of gut depends on fermentation of
undigested materials in the small intestine for their energy requirements. The microflora
performs fermentation by producing a large no. of enzymes like glucuronidase, xylosidase,
arabinosidase, galactosidase, and deaminase and urea dehydroxylase. These biodegradable
enzymes are capable of degrading the polymers used for targeting the drug delivery to colon.
Different polymers are used for preventing the release of drug in the stomach and small
intestine.
i. Prodrug approach for drug delivery to colon
Prodrug is the main approach of microbial triggered drug delivery system in which the drug
release from the formulation is triggered by the microflora present in the gut. Prodrug is the

www.wjpps.com Vol 8, Issue 6, 2019.
1471
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
inactive form of an active parent drug that undergoes enzymatic transformation to release the
active drug. These prodrug molecules get hydrolysed in the presence of the enzymes released
by the microflora.
a) Azo bond conjugate
Sulfasalazine is used for treatment of Inflammatory Bowel Diseases. It is 5-amino salicylic
acid (5-ASA) prodrug. 85% of oral dose of Sulfasalazine reaches to colon unabsorbed, where
it is reduced by anaerobic environment into 5-ASA and Sulphapyridine. Various studies are
conducted on Sulphapyridine which lead to formation of other prodrug like Olsalazine, 4-
amino Benzoyl-beta-alanine. Mutual azo prodrug of 5-amino salicylic acid with histidine was
synthesized by coupling L-Histidine with Salicylic acid, for targeted drug delivery to
inflamed gut tissue.[27]
b) Glucuronide conjugate
Glucuronide and sulfate conjugation is major mechanisms for inactivation and preparation for
clearance of a variety of drugs. Bacteria of the lower gastrointestinal tract secrete
glucuronidase that glucouronidate a variety of drugs in the intestine. Since the
glucuronidation process results in the release of active drug and enables its reabsorption,
glucuronide prodrugs would be expected to be superior for colon targeted drug delivery.[28]
c) Cyclodextrin conjugates
The hydrophilic and ionisable Cyclodextrins can serve as potent drug carriers in the
immediate release and delayed release formulations, while hydrophobic cyclodextrins can
retard release rate. The hydrophilic and ionisable Cyclodextrins can serve as potent drug
carriers in the immediate of water. Methotrexate prodrugs of α- and γ-Cyclodextrins were
synthesized and result established the primary aim of masking the ulcerogenic potential of
free drug, by using 12-fold dose of the normal dose of methotrexate and equivalent doses of
the ester.[29]
c) Timed released systems
Time controlled release system such as sustained or delayed release dosage forms are also
very promising drug release systems. However, due to potentially large variations of gastric
emptying time of dosage forms in humans, in these approaches, colon arrival time of dosage
forms cannot be accurately predicted, resulting in poor colonical availability.[30]
www.wjpps.com Vol 8, Issue 6, 2019.
1472
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Disadvantages of this system are
(i) Gastric emptying time varies markedly between subjects or in a manner dependent on
typeand amount of food intake.
(ii) Gastrointestinal movement, especially peristalsis or contraction in the stomach would
resultin change in gastrointestinal transit of the drug.
(iii) Accelerated transit through different regions of the colon has been observed in patients
with the IBD, the carcinoid syndrome and diarrhea and the ulcerative colitis.
That is since the transit time of dosage forms in the small intestine is less variable i.e.about
3±1 hour. The time-release function (or timer function) should work more efficientlyin the
small intestine as compared the stomach.
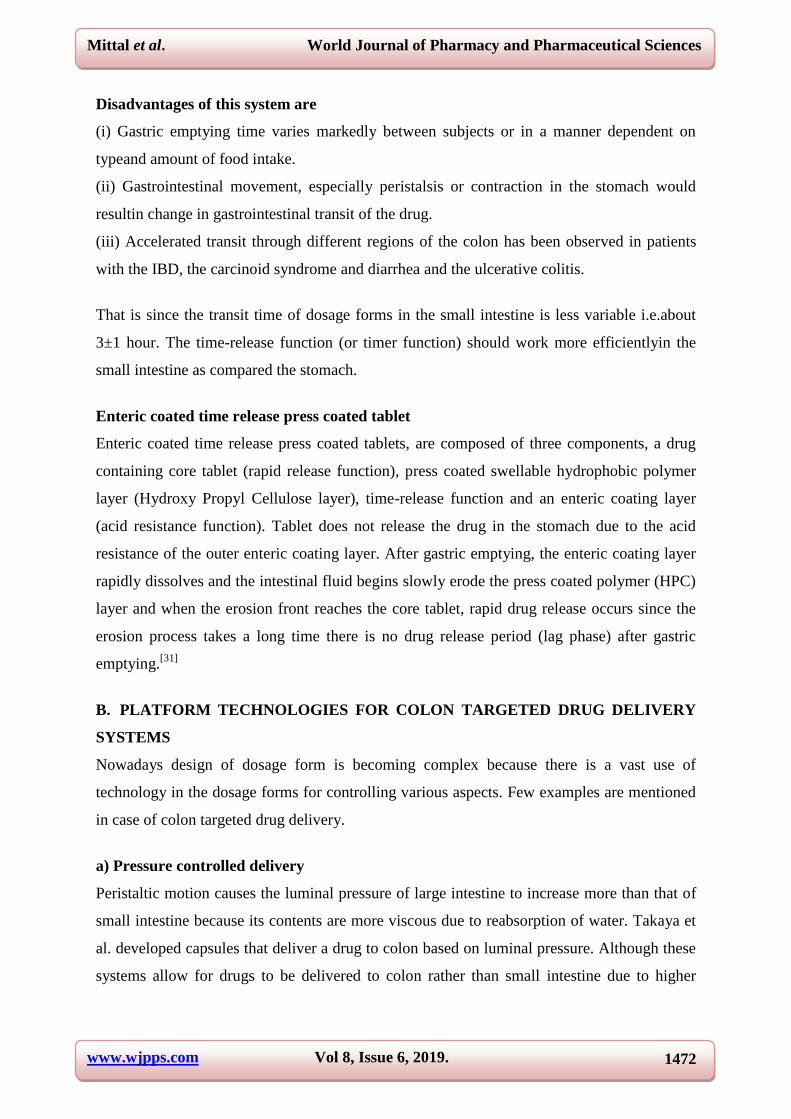
Enteric coated time release press coated tablet
Enteric coated time release press coated tablets, are composed of three components, a drug
containing core tablet (rapid release function), press coated swellable hydrophobic polymer
layer (Hydroxy Propyl Cellulose layer), time-release function and an enteric coating layer
(acid resistance function). Tablet does not release the drug in the stomach due to the acid
resistance of the outer enteric coating layer. After gastric emptying, the enteric coating layer
rapidly dissolves and the intestinal fluid begins slowly erode the press coated polymer (HPC)
layer and when the erosion front reaches the core tablet, rapid drug release occurs since the
erosion process takes a long time there is no drug release period (lag phase) after gastric
emptying.[31]
B. PLATFORM TECHNOLOGIES FOR COLON TARGETED DRUG DELIVERY
SYSTEMS
Nowadays design of dosage form is becoming complex because there is a vast use of
technology in the dosage forms for controlling various aspects. Few examples are mentioned
in case of colon targeted drug delivery.
a) Pressure controlled delivery
Peristaltic motion causes the luminal pressure of large intestine to increase more than that of
small intestine because its contents are more viscous due to reabsorption of water. Takaya et
al. developed capsules that deliver a drug to colon based on luminal pressure. Although these
systems allow for drugs to be delivered to colon rather than small intestine due to higher
www.wjpps.com Vol 8, Issue 6, 2019.
1473
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
colonic pressure, reabsorption of water from colon causes its content to be highly viscous
which may become an obstacle for site- specific delivery.[32]
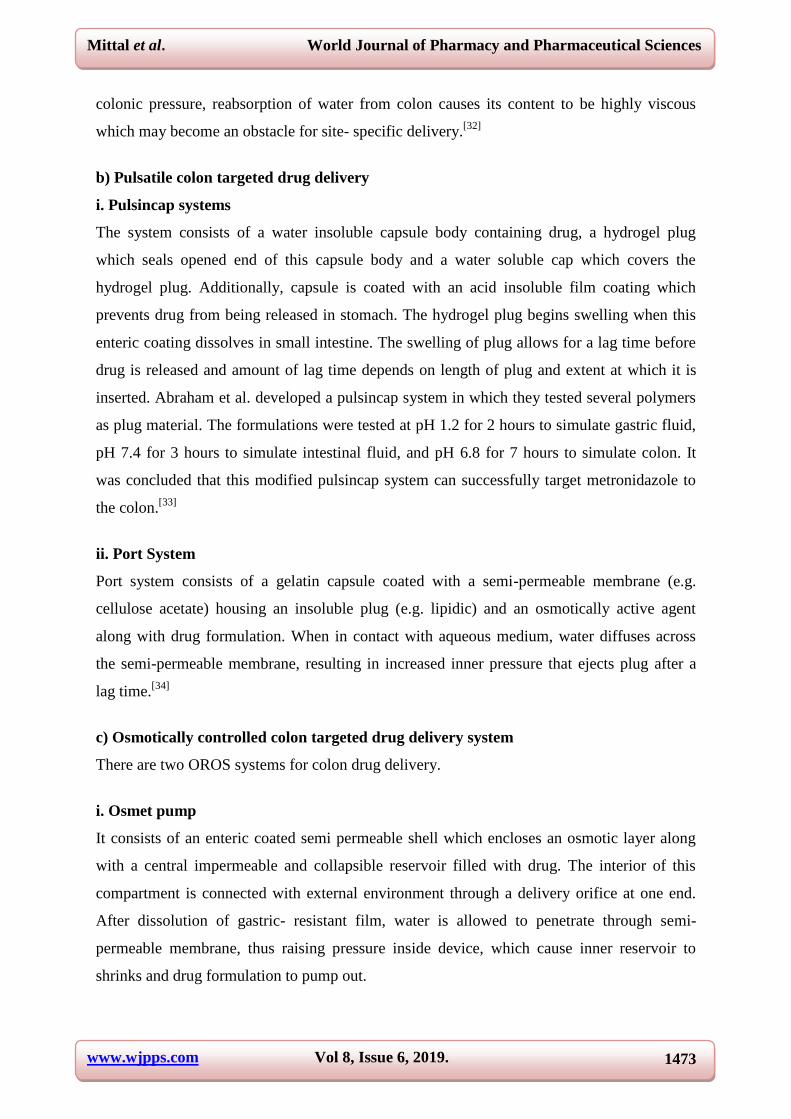
b) Pulsatile colon targeted drug delivery
i. Pulsincap systems
The system consists of a water insoluble capsule body containing drug, a hydrogel plug
which seals opened end of this capsule body and a water soluble cap which covers the
hydrogel plug. Additionally, capsule is coated with an acid insoluble film coating which
prevents drug from being released in stomach. The hydrogel plug begins swelling when this
enteric coating dissolves in small intestine. The swelling of plug allows for a lag time before
drug is released and amount of lag time depends on length of plug and extent at which it is
inserted. Abraham et al. developed a pulsincap system in which they tested several polymers
as plug material. The formulations were tested at pH 1.2 for 2 hours to simulate gastric fluid,
pH 7.4 for 3 hours to simulate intestinal fluid, and pH 6.8 for 7 hours to simulate colon. It
was concluded that this modified pulsincap system can successfully target metronidazole to
the colon.[33]
ii. Port System
Port system consists of a gelatin capsule coated with a semi-permeable membrane (e.g.
cellulose acetate) housing an insoluble plug (e.g. lipidic) and an osmotically active agent
along with drug formulation. When in contact with aqueous medium, water diffuses across
the semi-permeable membrane, resulting in increased inner pressure that ejects plug after a
lag time.[34]
c) Osmotically controlled colon targeted drug delivery system
There are two OROS systems for colon drug delivery.
i. Osmet pump
It consists of an enteric coated semi permeable shell which encloses an osmotic layer along
with a central impermeable and collapsible reservoir filled with drug. The interior of this
compartment is connected with external environment through a delivery orifice at one end.
After dissolution of gastric- resistant film, water is allowed to penetrate through semi-
permeable membrane, thus raising pressure inside device, which cause inner reservoir to
shrinks and drug formulation to pump out.
www.wjpps.com Vol 8, Issue 6, 2019.
1474
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
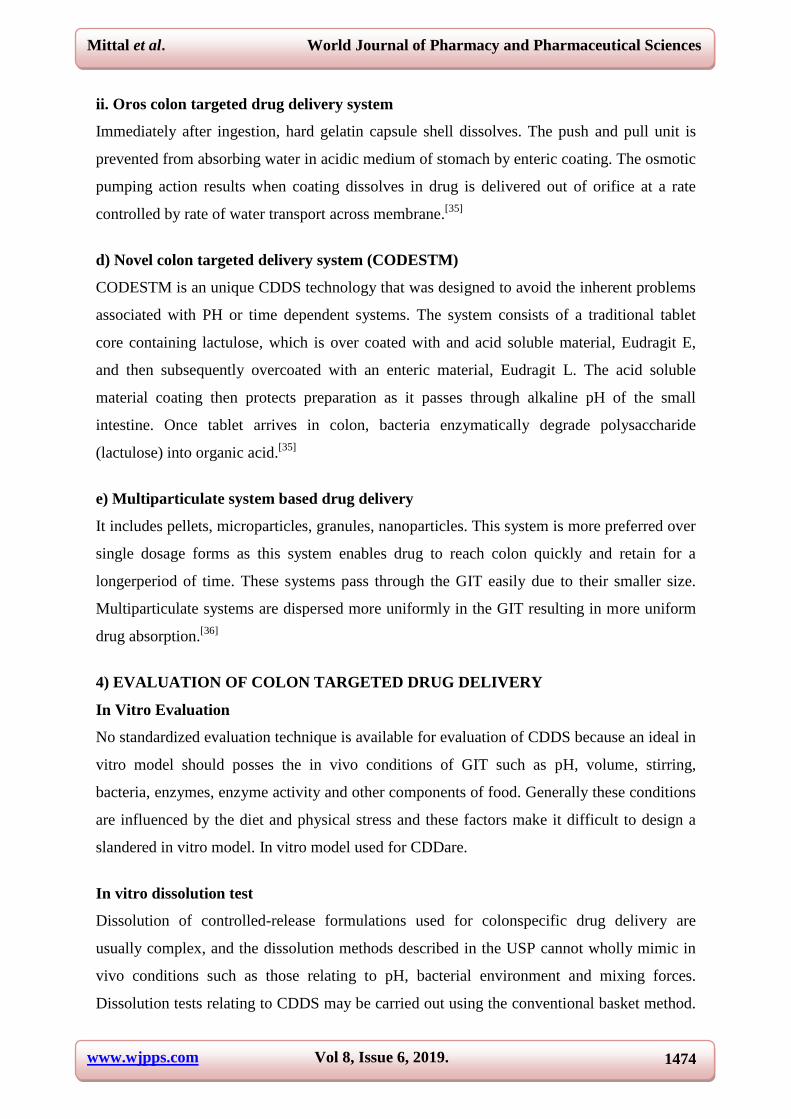
ii. Oros colon targeted drug delivery system
Immediately after ingestion, hard gelatin capsule shell dissolves. The push and pull unit is
prevented from absorbing water in acidic medium of stomach by enteric coating. The osmotic
pumping action results when coating dissolves in drug is delivered out of orifice at a rate
controlled by rate of water transport across membrane.[35]
d) Novel colon targeted delivery system (CODESTM)
CODESTM is an unique CDDS technology that was designed to avoid the inherent problems
associated with PH or time dependent systems. The system consists of a traditional tablet
core containing lactulose, which is over coated with and acid soluble material, Eudragit E,
and then subsequently overcoated with an enteric material, Eudragit L. The acid soluble
material coating then protects preparation as it passes through alkaline pH of the small
intestine. Once tablet arrives in colon, bacteria enzymatically degrade polysaccharide
(lactulose) into organic acid.[35]
e) Multiparticulate system based drug delivery
It includes pellets, microparticles, granules, nanoparticles. This system is more preferred over
single dosage forms as this system enables drug to reach colon quickly and retain for a
longerperiod of time. These systems pass through the GIT easily due to their smaller size.
Multiparticulate systems are dispersed more uniformly in the GIT resulting in more uniform
drug absorption.[36]
4) EVALUATION OF COLON TARGETED DRUG DELIVERY
In Vitro Evaluation
No standardized evaluation technique is available for evaluation of CDDS because an ideal in
vitro model should posses the in vivo conditions of GIT such as pH, volume, stirring,
bacteria, enzymes, enzyme activity and other components of food. Generally these conditions
are influenced by the diet and physical stress and these factors make it difficult to design a
slandered in vitro model. In vitro model used for CDDare.
In vitro dissolution test
Dissolution of controlled-release formulations used for colonspecific drug delivery are
usually complex, and the dissolution methods described in the USP cannot wholly mimic in
vivo conditions such as those relating to pH, bacterial environment and mixing forces.
Dissolution tests relating to CDDS may be carried out using the conventional basket method.
www.wjpps.com Vol 8, Issue 6, 2019.
1475
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
Parallel dissolution studies in different buffers may be undertaken to characterize the
behavior of formulations at different pH levels. Dissolution tests of a colon- specific
formulation in various media simulating pH conditions and times likely to be encountered at
various locations in the gastrointestinal tract. The media chosen were, for example, pH 1.2 to
simulate gastric fluid, pH 6.8 to simulate the jejunal region of the small intestine, and pH 7.2
to simulate the ileal segment. Enteric-coated capsules for CDDS have been investigated in a
gradient dissolution study in three buffers. In vitro test for intactness of coatings and carriers
in simulated conditions of stomach and intestineDrug release study in 0.1 N HCl for 2 hours
(mean gastric emptying time) Drug release study in phosphate buffer for 3 hours (mean small
intestine transit time).
In-Vitro dissolution Studies
The in-vitro dissolution studies were carried out using USP dissolution apparatus type II in
different medium.
Preparation of reagents & solutions
Preparation of 0.1 N HCl
0.1N HCl was prepared by diluting 8.5 ml of concentrated hydrochloric acid to 1000 ml with
distilled water.
Preparation of pH-6.8 phosphate buffer
28.80 g of disodium hydrogen phosphate & 11.45g of potassium hydrogen phosphate were
dissolved in water & volume was made up to 1000 ml.
Preparation of pH-7.4 phosphate buffer
2.38 g of disodium hydrogen phosphate, 0.19 g of potassium dihydrogen phosphate & 8.0 g
of sodium chloride were dissolved in water & volume was made up to 1000 ml. Adjust the
pH if required.[37]
Preparation of pH 6.8 phosphate buffer with 4%w/v rat caecal contents
Male Wistar rats weighing 105-150 gm and maintained on a normal diet were used for the
study. Thirty minutes before the commencement of drug release studies, four rats were killed
by spinal traction. The abdomen were opened, the caecal were traced, ligated at both ends,
dissected and immediately transferred into pH-6.8 phosphate buffer, previously bubbled with
carbon dioxide gas. The caecal bags were opened; their contents were individually weighed,
www.wjpps.com Vol 8, Issue 6, 2019.
1476
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
pooled and then suspended in pH-6.8 phosphate buffer to give 4%w/v dilution. As the
caecum is naturally anaerobic, all these operations were carried out under CO2 gas.[30]
In-
vitro dissolution study was performed by using USP Type II Apparatus (Basket type)
[Electrolab (ETC11L) Tablet Dissolution Tester] at 100 rpm for 2 h in 0.1 N HCl (900 ml).
Then the dissolution medium was replaced with pH 7.4 phosphate buffer (900 ml) and tested
for 3 h as the average transit time of small intestine is 3 h. After 5 h, the dissolution medium
was replaced with pH 6.8 phosphate buffer and tested for next 10 h. At the end of the time
period 10 ml of the sample were taken and analyzed for Nitrofurantoin content as described
previously. A 10 ml fresh and filtered dissolution medium (buffers) was added to make the
volume after each sample withdrawal.
In vitro enzymatic test
For this there are 2 tests:
1. Incubate carrier drug system in fermenter containing suitable medium for bacteria
(Streptococcus faccium or B.ovatus) amount of drug released at different time intervals
determined.
2. Drug release study is done in buffer medium containing enzymes (enzyme pectinase,
dextranase), or rat or guinea pig or rabbit cecal contents. The amount of drug released in
particular time is determined, which is directly proportional to the rate of degradation of
polymer carrier.
In Vivo Evaluation
A number of animals such as dogs, guinea pigs, rats and pigs are used to evaluate the delivery
of drug to colon because they resemble the anatomic and physiological conditions as well as
the microflora of human GIT. While choosing a model for testing a CDDS, relative model for
the colonic diseases should also be considered. Eg. Guinea pigs are commonly used for
experimental IBD model. The distribution of azoreductase and glucouronidase activity in the
GIT of rat and rabbit is fairly comparable to that in the human. For rapid evaluation of CDDS
a novel model has been proposed. In this model the human fetal bowel is transplanted into a
subcutaneous tullel on the back of thymic nude mice, which vascularizes within 4 weeks,
matures and becomes capable of developing of mucosal immune system from the host.[38-42]
5) DISSOLUTION TESTING
Dissolution testing of poorly soluble compounds in immediate- release (IR) solid dosage
forms poses many challenges. These challenges include developing and validating the test

www.wjpps.com Vol 8, Issue 6, 2019.
1477
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
method, ensuring that the method is appropriately discriminatory, and addressing the
potential for anin vivo–in vitrorelationship (IVIVR) or correlation (IVIVC).
A broad range of in vitro systems is available, from static monocompartmental to dynamic
multicompartmental models. However, these models require a compromise between
technological complexity and biological significance. Further efforts and technological
innovations are still needed to improve in vitro models and meet growing demands in the
areas of health.[43]
Need ofin-vitrodissolution testing
a) Characterizing the drug-release mechanism by establishing anin vitrodissolution test
method (or an appropriate alternative method) to measure product performance is particularly
important for poorly soluble compounds.
b) Dissolution testing historically has been a key tool during the development stages of a
compound as well as for commercial manufacturing.
c) For a development compound, dissolution testing is used primarily to help develop and
evaluate new formulations by evaluating the rate of drug release from dosage forms,
evaluating the stability of these formulations, monitoring product consistency, assessing
formulation changes, and establishing IVIVRs or IVIVCs.
d) For a commercial product, dissolution testing is used primarily to confirm manufacturing
and product consistency, to evaluate the quality of the product during its shelf life, and to
assess postapproval changes and the need for bioequivalence studies.[44]
In vitro GSI models
a) Static monocompartmental models
Static models are the most widespread digestive systems. The gastric phase is reproduced by
a pepsin hydrolysis of homogenized food, under fixed pH and temperature, for a set period of
time (pH 1–2, 378℃, 1–3 h). This step may be followed, in the same bioreactor, by an
intestinal phase involving pancreatic enzymes with or without bile (pH 6–7). Most of these
models have been developed for specific applications and are cheap high-throughput tools,
particularly relevant for large prescreening approaches. The United States Pharmacopeia
(USP) apparatus also provides a static, closed environment, widely used to assess dosage
form disintegration and dissolution in a single medium reproducing digestive conditions, both
gastric (Simulated Gastric Fluid) and intestinal (Simulated Intestinal Fluid). However, in this

www.wjpps.com Vol 8, Issue 6, 2019.
1478
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
approach, large volumes of media are often deployed and the mechanical forces (continuous
stirring) are not representative of complex peristaltic movements.[45]
b) Dynamic monocompartmental models
To overcome these limitations, several dynamic gastricmodels have been developed. One
model reproduces, based on in vivo data, the progressive acidification of gastric content by
HCl addition, the time course of pepsin flow rate and gastric emptying.[46]
The Dynamic
Gastric Model(DGM) was designed to take into account the regionspecificity of the stomach.
It is composed of two successive compartments.
(i) The „body‟ where gastric secretions are mixed with food.
(ii) The „antrum‟ where shear forces and stomach grinding are reproduced.
The gastricemptying is regulated by a valve that allows the smallest particles to leave the
stomach, whereas the bigger ones are refluxed into the top chamber to be further digested.
Despite its complexity, the DGM does not accurately reproduce the in vivo peristaltic
forces.[47,48]
The Human Gastric Simulator (HGS), composed of a latex chamber surrounded
by a mechanical driving system, more effectively emulates the peristaltic movements of the
stomach in amplitude, intensity, and frequency.[49]
c)Dynamic bi and multicompartmental models
The main bicompartmental models aim to simulate theluminal conditions of the stomach and
proximal smallintestine.[50,51]
Based on in vivo data, these computercontrolledsystems
reproduce the temperature, pH changesin the gastric and duodenal compartments, gastric
emptying, addition of pepsin, pancreatic juice and (or) bile, anddialysis of digestion end
products.[52]
Thesesystems have been mostly standardized and validatedfor specific
applications, such as the study of antacidactivity.[53]
or the survival of probiotics.[54]
To date, the TIM-1 (TNO gastro-Intestinal Model 1) isthe only GSI system characterized as
„full‟, that is, combining multi-compartmentalization and dynamism.[55]
This model is
composed of the stomach and the three parts of the small intestine, the duodenum, jejunum,
and ileum. It integrates key parameters of human digestion: temperature, kinetics of gastric
and intestinal pH, gastric and ileal deliveries, transit time, peristaltic mixing and transport,
sequential addition of digestive secretions, and passive absorption of water and small
molecules through a dialysis system. TIM-1 is so far the system that allows the closest
www.wjpps.com Vol 8, Issue 6, 2019.
1479
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
simulation of in vivo dynamic events occurring within the human GSI lumen. It has been
applied in a large number of nutritional[56,57]
, toxicological[58,59]
, pharmaceutical[60,61]
, and
microbiological[62]
studies.
APPLICATIONS OF DISSOLUTION TESTING
1. In vitro dissolution testing is well established for solid oraldosage forms as both a quality
control test to assess batch-to batch consistency and to predict in vivo drug release profiles
for both immediate and modified release dosage forms.[63,64]
2. Many commonly used inhaled products such as metereddoseinhalers (MDIs), dry powder
inhalers (DPIs) and suspensionsfor nebulization deliver the active pharmaceutical
ingredient(API) to the lung in a solid form. A variety of competing mechanisms exist for the
clearance of aerosol particles after deposition in the airways.[65]
3. In vitro tools have been extensively used to determine thebioaccessibility of ingested
nutrients. Reported studies range from macronutrients[66,67]
to micronutrients such as
vitamins, minerals, or phytoconstituents.[68,69]
4. A variety of dissolution media, usually at pH=6.8–7.4, ranging from simple phosphate-
buffered saline (PBS) to simulated lung fluid (SLF) have been used for dissolution testing of
inhaled products.We use the term „simulated lung fluid‟, which has become customary in the
literature, with an understanding that SLF does not fully simulate the interstitial or epithelial
lung fluid (ELF) given that it will not contain protein components, mucus, etc.[70]
5. The in vitro dissolution of dysprosium lithium borate microspheres using simulated
synovial fluid used for treatment of Rheumatoid Arthritis.[71,72]
6. The synovial fluid was used to evaluate the in vitro bioactive behavior (in vitro bone-
bonding ability) of tissue-engineered osteochondral (bone-cartilage) composite used in the
treatment of lesions of the articular cartilage. The simulated synovial fluid was continuously
circulated in physiological conditions (pH 7.4 and 37 °C) using a peristaltic pump for up to
14 days with anavailable volume of 50 mL of fluid.[73]
7. Vertzoni et al. developed a simulated gastricmedium that more adequately reflects the
physiological conditions of the fasted state .This medium contains pepsin and low amounts of
bile salt and lecithin.[74]
8. The in vitro release ofbovine serum albumin from matrixes made of these modified
starches using the SCoF1.[75]
9. The in vitro release of metronidazole from modified Pulsincap dosage forms targeted to the
colon in a timedependent manner was evaluated using pH 6.8 phosphate buffer.[76]
www.wjpps.com Vol 8, Issue 6, 2019.
1480
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
10. Development of a media simulatingthe physicochemical characteristics of the ascending
colon in the fasted and fed states.[77]
11. Development of a fluidto simulate the contents of the proximal colon. This medium was
used to predict the input profiles of extended-release products containing isosorbide-5-
mononitrate.[78]
12. SS 5 (300 mL) was used to monitor the release of salbutamol sulphate from oral fast
dissolving films using USP Apparatus 2 (paddles).[79]
13. The test method to characterize the dissolution properties of a multitude of formulation
types available for pulmonary delivery.[80]
14. SLF4 was used to evaluate the in vitro release of itraconazole from nebulized
nanoparticle dispersions.[81]
15. SLF5 was used to evaluate the dissolution oftitanium tritide particles used as components
of neutron generators. These particles may be released into the air as aerosols during
fabrication, assembling, and testing of components or in accidental or fugitive releases.[82]
16. The development of a simulated vaginal fluid(SVF1) (Table 12) that models the fluid
properties originating in the vagina, specifically the vaginal secretion found in healthy,
nonpregnant, premenopausal women.The volume of vaginal fluid can be measured in two
ways, the amount of fluid present at any one time or the amount of fluid produced over an
extended time interval.[83]
17. The in vitro release of clindamycin from bioadhesive gelwas performed using 15 mL of
SVF1 in a vertical diffusion cell.[84]
18. The swelling behavior, the mucoadhesion, and the invitro release of nystatin from a
mucoadhesive vaginal delivery were evaluated using SVF1.[85]
19. Simulated Tears 1 in the volume of 8 mL wasused to evaluate the in vitro release kinetic
of poly-anionic oligonucleotide macromolecules from cationic nanoemulsions with potential
use for age-related macular degeneration treatment.[86]
20. Simulated Tears 2 in the volume of 4 mL was used to evaluate drug-loadingefficiency and
in vitro release of pilocarpine fromhydrogels. These hydrogels behave as a drug-depot for
controlled-release applications.[87]
21. Development of in situ forming sodium alginate gels for the extended release of
indomethacin to the eye. They evaluated the in vitro gelation using Simulated Tears 2 and
Simulated Tears 3 and assessed the in vitro release using Simulated Tears 2 (200 mL/2 mL of
sample).[88]
www.wjpps.com Vol 8, Issue 6, 2019.
1481
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
22. The in vitro release of fentanyl from transdermal systems was evaluated using 500 mL of
SSW(60) using USP Apparatus 5 (paddle over disk).[89]
23. Characterization of the corrosion layer of copper–nickel alloysin SSW2, with its pH
adjusted to 6.5 with ammonia.[90]
6) Limitations and challenges in colon targeted drug delivery[91-93]
1. One challenge in the development of colon-specific drug delivery systems is to establish an
appropriate dissolution testing method to evaluate the designed system in-vitro.
2. As a site for drug delivery, the colon offers a near neutral pH, reduced digestive enzymatic
activity, a long transit time and increased responsiveness to absorption enhancers; however,
the targeting of drugs to the colon isvery complicated.
3. Due to its location in the distal part of the alimentary canal, the colon is particularly
difficult to access.
4. In addition to that the wide range of pH values and different enzymes present throughout
the gastrointestinal tract, through which the dosage form has to travel beforereaching the
target site, further complicate the reliability and delivery efficiency.
5. Successful delivery through this site also requires the drug to be in solution form before it
arrives in the colon or, alternatively, it should dissolve in the luminal fluids of the colon, but
this can be a limiting factor for poorly soluble drugs as the fluid content in the colon is much
lower and itis more viscous than in the upper part of the GI tract.
6. In addition, the stability of the drug is also a concern and must be taken into consideration
while designing the delivery system.
7. The drug may potentially bind in a nonspecific way to dietary residues, intestinal
secretions, mucus or faecal matter.
8. The resident microflora could also affect colonic performance via metabolic degradation of
the drug. Lower surface area and relative „tightness‟ of the tight junctions in the colon can
also restrict drug transport across themucosa and into the systemic circulation.
9. The occurrence of physical and chemical interactionswithin and between the shell and fill
components. It is critical to understand these interactions to develop a softgel product that is
stable and provides desired in vitro and in vivo characteristics.[94]
10. USP Apparatus I and II arecommonly used for dissolution testing of commercially
available products of poorly soluble compounds, whereas other apparatus have been used
primarily for development.[95]
www.wjpps.com Vol 8, Issue 6, 2019.
1482
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
11. USP evaluated the scientific rationale for in vitro dissolution tests for inhalation dosage
forms and concluded that there was no compelling evidence that dissolution was “kinetically
and/or clinicallycrucial for currently approved” OIPs.[96]
12. To simulate host responses more accurately, a combinatorialapproach involving in vitro
models and human intestinal cells in culturehas been proposed.[97]
13. Recent studies have also investigated the effectof in vitro digesta on intestinal cell
proliferation and inflammatory pathways to assess the potential anticarcinogenic or anti-
inflammatory properties of ingested substances.[98,99]
14. One of the major challenges in in vitro digestion is tosimulate as accurately as possible
the peristalsis and realistic shape and motility of GSI compartments. Interestingly, newly
developed GSI models should also reproduce the biphasic gastric emptying curves observed
in vivo, where emptying of solid food components presents a linear pattern starting after a lag
phase, whereas emptying of liquids begins immediately in an exponential manner.[100]
15. There are some technical challenges of measuring invitro dissolution of nanoparticles as
sub-micron particles can easily pass through a line filter, which may overestimate the
dissolution rate.[101]
CONCLUSION AND FUTURE SCOPE
A wide range of GSI models has been developed andapplied in many nutrition and health
studies.By usingin vitro dissolution tests, the industry generally seeks to establish in vivo–in
vitro relationships as opposed to invivo–in vitrocorrelations (IVIVCs), because the latter have
poorly defined validation requirements, challenges of predictability, and extensive added cost
with questionable benefit. Dissolution testing is most often used for the in vitroassessment of
the in vivo behavior of a pharmaceutical dosage form, both for development and quality
control. In vivo performance prediction is a valuable tool in drug developmentand regulatory
evaluation. As methods in modeling and simulation for predictions of bioavailability continue
to expand and improve, the role of predictive tools in drug development and review will
assume greater importance. Advisory Panel not to pursue the development of
standardizedmethods for possible compendial use, but will continue to maintain a watching
brief on the possible impact of dissolution- related effects associated with potential new
forms of OIPs, particularly those involving controlled release.
Establishing quantitative in vitro–in vivo relationships between dissolution data and PK, PD
or clinical data and Establishing quantitative in vitro–in vivo relationships between
www.wjpps.com Vol 8, Issue 6, 2019.
1483
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
dissolution data and PK, giving consideration to the appropriate dissolution timescale relative
to mucocilary ormacrophage particulate clearance mechanisms and improving the robustness
and validation of the dissolution apparatus, particularly with regards to drug loading effects
and Using a truly predictive dissolution medium that correctlysimulates dissolution in the
lung and The use of experimental dissolution data within predictive pharmacokinetic models
[e.g., GastroPlus™ Simulations Plus Inc., Lancaster, CA pulmonary module data or the
published Hochhaus model data.
REFERENCES
1. Philip AK, Dabas S, Pathak K. Optimized prodrug approach: A means for achieving
enhanced anti-inflammatory potential in experimentally induced colitis. J Drug Target,
2009; 17: 235241.
2. Oluwatoyin AO, John TF. In vitro evaluation of khaya and albizia gums as compression
coating for drug targeting to the colon. J Pharm Pharmacol, 2005; 57: 63168.
3. Akala EO, Elekwachi O, Chase V, Johnson H, Marjorie L, Scott K. Organic redox
initiated polymerization process for the fabrication of hydrogel for colon specific drug
delivery. Drug Dev Ind Pharm, 2003; 29: 375386.
4. Chourasia MK, Jain S K. Pharmaceutical approaches to colon targeted drug delivery
systems. J Pharm Sci, 2003; 6:3366.
5. Basit A, Bloor J. Prespectives on colonic drug delivery, Business briefing. Pharmtech,
2003; 185190.
6. Watts P, Illum L. Colonic drug delivery. Drug Dev Ind Pharm, 1997; 23: 893913.
7. VS Mundhe, SS Dodiya. Review article: novel approaches for colon targeted drug
delivery. Ind Amer J Pharm Res, 2011; 3: 158-173.
8. P Patel, S Shukla, Dr. P Bharadia, Dr.V Pandya. Colon targeted drug delivery system- a
review. IJUPLS, 2012; 2: 272-291.
9. BK Sarkar, D Jain, A Banerjee, M Parwal. Colon targeted drug delivery system. RJPBCS,
2011; 2: 365-372.
10. A Patel, N Bhatt, Dr.KR Patel, Dr.NM Patel, DR.MR Patel. Colon targeted drug delivery
system: a review system. JPSBR, 2011; 1: 37-49.
11. Zhang S Q, Thumma S, Chen G H, Deng W B, Repka M A and San-Ming Li: In vitroand
in vivoevaluation of tegaserod maleate pH-dependent tablets. European Journal of
Pharmaceutics and Biopharmaceutics, 2008; 69: 247–254.
www.wjpps.com Vol 8, Issue 6, 2019.
1484
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
12. Chauhan C S, Naruka P S, Rathore R S and Badadwal V: Formulation and evaluation of
Prednisolone tablet for colon targeted drug delivery system. Journal of Chemical and
Pharmaceutical Research, 2010; 2: 993-998.
13. Fukui E, Miyamura N, Kobayashi M : An in vitro investigation of the suitability of press-
coated tablets with hydroxypropylmethylcellulose acetate succinate (HPMCAS) and
hydrophobic additives in the outer shell for colon targeting. Journal of control release,
2001; 70: 97-107.
14. Nagaraju R, Swapna Y, Hari babu R and Kaza R: Design and Evaluation of Delayed and
Extended Release Tablets of Mesalamine. Journal of Pharmaceutical Science and
Technology, 2010; 2: 103-110.
15. Verma S, Singh S.K, Mishra D.K, Gupta A and Sharma R: Formulation and Evaluation of
Microbially- triggered tablets of Valdecoxib. International Journal of Drug Delivery
Technology, 2009; 1: 6-11.
16. Dev R K, Bali V, Pathak K : Novel microbially triggered colon specific delivery system
of 5-Fluorouracil : statistical optimization, in vitro, in vivo, cytotoxic and stability
assessment. International Journal of Pharmaceutics, 2011; 411: 142-151.
17. Patel G N*, Patel R B and Patel H R : Formulation and in-vitro evaluation of microbially
triggered colon specific drug delivery using sesbania gum. Journal of Science &
Technology, 2011; 6: 33-45.
18. Ashord M, Fell JT, Attwood D, Sharma H and Woodhead P : An evaluation of pectin as a
carrier for drug targeting to the colon. Journal of Control Release, 1993; 26: 213-220.
19. Shibata N, Ohno T, Shimokawa T, Hu Z, Yoshikawa Y, Koga K, Murakami M and
Takada K:Application of pressure controlled colon delivery capsule to oral administration
of glycyrrhizin in dogs. Journal of Pharmacy and Pharmacology, 2001; 53: 441-447.
20. Bayat A, Dorkoosh F A, Dehpour A R, Moezi L, Larijanj B, Junginger H E and Rafiee-
Tehrani M : Nanoparticles of quarternized chitosan derivatives as a carrier for colon
delivery of insulin : ex vivo and in vivo studies. International Journal of pharmaceutics,
2008; 356: 259-66.
21. Shantha K L, Ravichandran P and Rao K P: Azo polymeric hydrogels for colon targeted
drug delivery. Biomaterials, 1995; 16: 1313-1318.
22. Omar S, Aldosari B, Refai H and Gohary O A: Colon-specific drug delivery for
mebeverine hydrochloride. Journal of drug targeting, 2007; 15: 691-700.
www.wjpps.com Vol 8, Issue 6, 2019.
1485
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
23. Maestrelli F, Cirri M, Corti G, Mennini N and Mura P: Development of Enteric Coated
Calcium pectinate Microspheres intended for colonic Drug Delivery. European Journal of
Pharmaceutics and Biopharmaceutics, 2008; 69: 508-518.
24. Keshavarao K P, Dixit M, Selvum P and Singh D R: Formulation and evaluation of
indomethacine microspheres for colonic drug delivery system. International research
journal of pharmacy, 2011; 2: 181-184.
25. Ravi P, Rao Kusumanchi R M, Mallikarjun V, Babu Rao B and B R N: Formulation and
Evaluation Of Guar gum Microsperes Of Aceclofenac For Colon Targeted Drug delivery.
Journal Of Pharmacy Reasearch, 2010; 3: 1510-1512.
26. Anil k.Philip. Colon Targeted Drug Delivery Systems: A Review on Primary and Novel
Approaches. OMJ, 2012; 70-78.
27. M Sharma, B Joshi, M Bansal, M Goswami. Colon specific delivery system: the local
targeting. IRJP, 2011; 2: 103-107.
28. N Singh, Dr. RC Khanna. Colon targeted drug delivery system- a potential approach. The
Pharm InnJ, 2012; 1: 40-47.
29. PD Kothawade, MA Wagh. Conventional and novel approaches for Colon specific drug
delivery: a review. E-JST, 2011; 2: 33-56.
30. Ankita Patel, Dhruvita Patel, Truptisolanki, Dr. P.D. Bharadia, Mr. V.M. Pandya and Mr.
D.A. Modi. Novel Approaches for Colon Targeted Drug Delivery System. Journal of
Pharmaceutics and Cosmetology, 2011; 1(5): 86-97.
31. Sharma Anuj, Jain K Amit. Colon targeted drug delivery using different approaches Int.
Journal of Pharmaceutical Studies and Research, 2010; 1(1): 60-66.
32. S.Pradeep Kumar, D.Prathibha, R.Parthibarajan, C.Rubina Reichal. Novel Colon specific
drug delivery system:A review,Int. Journal of Pharmacy and Pharmaceutical Sciences,
2012; 4(1): 22-29.
33. Vishal V.Rajguru, Preeti D. Gaikwad, Vidyadhar H. Bankar, Sunil P.Pawar. An overview
on colonic drug delivery system. Int. Journal of Pharmaceutical Sciences Review and
Research, 2011; 6(2): 197-204.
34. Sachin D.Bhalersao, Paresh R.Mahaparale. Different approaches for colon drug delivery
systems: A Review. International Journal of Research and Reviews in Pharmacy and
Applied Science. 2(3):529-549.
35. Bhushan Prabhakar Kolte et al,. Asian Journal of Biomedical and Pharmaceutical
Sciences, 2012; 2(14): 21-28.
www.wjpps.com Vol 8, Issue 6, 2019.
1486
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
36. Ashwini Sopan Bansode, Avinash Bhausaheb Athare, Veena Sanjay Kasture,
P.N.Kendre. Colon targeted drug delivery system: An Overview. Int. Imperial Journal of
Pharmaceutics and Cosmetology, 2012; 2(2): 1-7.
37. Barbare. L, Teresa.C, Federica.B, Isabella.O, Vittorio.2, Eur J Pharm Biopharm, 2003;
55: 199-202.
38. Kinget.R, Kerela.W, Vervoort. L, Mooter.G.V, J Drug Target, 1998; 6: 129-149.
39. Krishnaiah.Y.S.R, Bhaskar Reddy.P.R, Satyanarayana.V, Karthikeyan.R.S. Int J Pharm,
2002; 236(2): 43-55.
40. Wu.B, Chen.Z, Wei.X, Sun.N, Lu.Y, Wu.W. Eur J Pharm Biopharm, 2007; 67: 707–714.
41. Xinmuing Liu, Qingshen Sun, Huajie Wang, Lei Zhang, Jin-Ye Wang, Microspheres of
Corn protein, zein, for an ivermectin drug delivery system Biomaterials, 2005; 26:
109- 115.
42. Klaus Florey, David.W.F, Analytical Profiles of Drug Substances- Ivermectin, Academic
Press-Elsevier, 1st Ed, Vol 17, New Delhi, 2005; 156-184.
43. R.A. Reed, “A Biopharmaceutical Classification System Approach toIn VitroDissolution
Method Development,” presented at the PhRMA Acceptable Analytical Practices
Workshop, Washington, DC, 23-25 September 2003.
44. Food and Drug Administration, Guidance for Industry:Immediate ReleaseSolid Oral
Dosage Forms; Scale-Up and Postapproval Changes: Chemistry, Manufacturing, and
Controls, In Vitro Dissolution Testing, and In Vivo Bioequivalence Documentation(FDA,
Rockville, MD, November 1995).
45. Kong, F. and Singh, R.P.Disintegration of solid foods in humanstomach. J. Food Sci,
2008; 73: R67–R80.
46. Hoebler, C. Development of an in vitro system simulatingbucco-gastric digestion to
assess the physical and chemical changes of food. Int. J. Food Sci. Nutr., 2002; 53:
389–402.
47. Mercuri, A. The effect of composition and gastric conditions on the self emulsification
process of ibuprofen-loaded self-emulsifying drug delivery systems: a microscopic and
dynamic gastric model study. Pharm. Res, 2011; 28: 1540–1551.
48. Vardakou, M.Achieving antral grinding forces inbiorelevant in vitro models: comparing
the USP Dissolution Apparatus II and the Dynamic Gastric Model with human in vivo
data. AAPS Pharm. Sci. Tech, 2011; 12: 620–626.
49. Kong, F. and Singh, R.PA human gastric simulator (HGS) tostudy food digestion in
human stomach. J. Food Sci, 2010; 75: E627–E635.
www.wjpps.com Vol 8, Issue 6, 2019.
1487
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
50. Vatier, J.Interests of the „artificial stomach‟ techniques tostudy antacid formulations:
comparison with in vivo evaluation. Fundam. Clin. Pharmacol, 1998; 12: 573–583.
51. Mainville, I.A dynamic model that simulates the humanupper gastrointestinal tract for the
study of probiotics. Int. J. Food Microbiol, 2005; 99: 287–296.
52. Yvon, M.In vitro simulation of gastric digestion of milkproteins: comparison between in
vitro and in vivo data. J. Agric. Food Chem, 1992; 40: 239–244.
53. Castela-Papin, N.Drug interactions with diosmectite: astudy using the artificial stomach-
duodenum model. Int. J. Pharm, 1999; 182: 111–119.
54. Tompkins, T.A. The impact of meals on a probiotic duringtransit through a model of the
human upper gastrointestinal tract.Benef. Microbes 2011; 2: 295–303.
55. Minekus, M.A multicompartmental dynamic computercontrolledmodel simulating the
stomach and small intestine. ATLA, 1995; 23: 197–209.
56. Blanquet-Diot, S.Digestive stability of xanthophyllsexceeds that of carotenes as studied in
a dynamic in vitro gastrointestinal system. J. Nutr, 2009; 139: 876–883.
57. Krul, C.A.Intragastric formation and modulation of Nnitrosodimethylaminein a dynamic
in vitro gastrointestinal model under human physiological conditions. Food Chem.
Toxicol, 2004; 42: 51–63.
58. Torres-Escribano, S.Comparison of a static and a dynamicin vitro model to estimate the
bioaccessibility of As, Cd, Pb and Hg from food reference materials Fucus sp. (IAEA-
140/TM) and Lobster hepatopancreas (TORT-2). Sci. Total Environ, 2011; 409: 604–611.
59. Brouwers, J.Food-dependent disintegration of immediaterelease fosamprenavir tablets: in
vitro evaluation using magnetic resonance imaging and a dynamic gastrointestinal
system. Eur. J. Pharm. Biopharm, 2011; 77: 313–319.
60. Dickinson, P.A.An investigation into the utility of a multicompartmental,dynamic, system
of the upper gastrointestinal tract to support formulation development and establish
bioequivalence of poorly soluble drugs. AAPS J, 2012; 14: 196–205.
61. Kheadr, E.Study of the physicochemical and biologicalstability of pediocin PA-1 in the
upper gastrointestinal tract conditions using a dynamic in vitro model. J. Appl. Microbiol,
2010; 109: 54–64.
62. Blanquet-Diot, S.Use of artificial digestive systems toinvestigate the biopharmaceutical
factors influencing the survival of probiotic yeast during gastrointestinal transit in
humans. Pharm. Res, 2012; 29: 1444–1453.
63. US FDA CDER. Guidance for Industry: Dissolution testing of immediate release solid
oral dosage forms

www.wjpps.com Vol 8, Issue 6, 2019.
1488
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/
Guidances/ucm070237.pdf, 1997; Accessed 4 Oct 2011.
64. US FDA CDER. Guidance for Industry: Extended release oraldosage forms:
Development, Evaluation and Application of In Vitro/In Vivo
Correlations.http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInfor
mation/Guidances/ucm070239.pdf, 1997; Accessed 4 Oct 2011.
65. Kreyling WG, Scheuch G. Clearance of particles deposited in thelungs. In: Gehr P,
Heyder J, editors. Particle–lung interactions.2nd ed. New York: Marcel Dekker, 2009;
323–75.
66. Gervais, R.Bioaccessibility of fatty acids from conjugatedlinoleic acid-enriched milk and
milk emulsions studied in a dynamic in vitro gastrointestinal model. Int. Dairy J, 2009;
19: 574–581.
67. Kopf-Bolanz, K.A.Validation of an in vitro digestive systemfor studying macronutrient
decomposition in humans. J. Nutr, 2012; 142: 245–250.
68. Blanquet-Diot, S.Digestive stability of xanthophyllsexceeds that of carotenes as studied in
a dynamic in vitro gastrointestinal system. J. Nutr, 2009; 139: 876–883.
69. Anson, N.M.Bioprocessing of wheat bran improves in vitrobioaccessibility and colonic
metabolism of phenolic compounds. J. Agric. Food Chem, 2009; 57: 6148–6155.
70. Bicer EM, Forbes B, Somers G, Blomberg A, Behndig A, MudwayA. Characterising the
composition of human respiratory tract lining fluids in health and disease in Drug
Delivery to the Lungs 22 Proceedings; Edinburgh, UK. Portishead, UK: The Aerosol
Society, 2011; 9: 82–84.
71. Conzone, S. D.; Brown, R. F; Day, D. E.; Ehrhardt, G. J. Invitro and in vivo dissolution
behavior of a dysprosium lithium borate glass designed for the radiation synovectomy
treatment of rheumatoid arthritis. J. Biomed. Mater. Res, 2002; 60(2): 260–268.
72. Conzone, S. D.; Hemrick, J. G.; Day, D. E. Glass formationand chemical durability of
dysprosium lithium borate glasses intended for in vivo radiation synovectomy. Glass Sci.
Technol, 2001; 74(2): 39–45.
73. Malafaya, P. B.; Reis, R. L. Bilayered chitosan-basedscaffolds for osteochondral tissue
engineering: influence of hydroxyapatite on in vitro cytotoxicity and dynamic bioactivity
studies in a specific double-chamber bioreactor. Acta Biomater, 2009; 5(2): 644–660.
74. Vertzoni, M.; Dressman, J.; Butler, J.; Hempenstall, J.;Reppas, C. Simulation of fasting
gastric conditions and its importance for the in vivo dissolution of lipophilic compounds.
Eur. J.Pharm. Biopharm, 2005; 60: 413–417.

www.wjpps.com Vol 8, Issue 6, 2019.
1489
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
75. Chen, L.; Li, X.; Pang, Y.; Lin, L.; Zhang, X.; Yu, L. Resistantstarch as a carrier for oral
colon-targeting drug matrix system. J. Mater. Sci. Mater. Med, 2007; 18: 2199–2203.
76. Abrahanm, S.; Srinath, M. S. Development of modifiedpulsincap drug delivery system of
metronidazole for drug targeting. Indian J. Pharm. Sci, 2007; 69(1): 24–27.
77. Vertzoni, M.; Diakidou, A.; Chatzilias, M.; Soderlind, E.; Abrahamsson, B.; Dressman, J.
B.; Reppas, C. Biorelevantmedia to simulate fluids in the ascending colon ofhumans and
their usefulness in predicting intracolonic drug solubility. Pharm. Res, 2010; 27:
2187–2196.
78. Fotaki, N.; Symillides, M.; Reppas, C. In vitro versuscanine data for predicting input
profiles of isosorbide-5-monohydrate from oral extended release products on a confidence
interval basis. Eur. J. Pharm. Sci, 2005; 24: 115–122.
79. Mashru, R. C.; Sutariya, V. B.; Sankalia, M. G.; Parikh, P. P.Development and evaluation
of fast-dissolving film of salbutamol sulphate. Drug. Dev. Ind. Pharm, 2005; 31: 25–34.
80. Son, Y. J.; McConville, J. T. Development of a standardizeddissolution test method for
inhaled pharmaceutical formulations. Int. J. Pharm, 2009; 382: 15–22.
81. Yang, W.; Tam, J.; Miller, D. A.; Zhou, J.; McConville, J. T.; Johnston, K. P.; Williams
III, R. O. High bioavailability from nebulized itraconazole nanoparticle dispersions with
biocompatible stabilizers. Int. J. Pharm, 2008; 361: 177–188.
82. Cheng, Y. S.; Dahl, A. R.; Jow, H. N. Dissolution of MetalTritides in a Simulated Lung
Fluid. Health Phys, 1997; 73(4): 633–638.
83. Owen, D.H.; Katz, D. F. A vaginal fluid stimulant. Contraception, 1999; 59(2): 91–95.
84. Gupta, H.; Sharma, A. Ion activated bioadhesive in situgel of clindamycin for vaginal
application. Int. J. Drug Deliv, 2009; 1(1): 32–40.
85. Hombach, J.; Palmberger, T. F.; Bernkop-Schnurch, A. Development and in vitro
evaluation of a mucoadhesive vaginal delivery system for nystatin. J. Pharm. Sci, 2009;
98(2): 555–564.
86. Hagigit, T.; Nassar, T.; Behar-Cohen, F.; Lambert, G.; Benita, S. The influence of
cationic lipid type on in-vitro release kinetic profiles of antisense oligonucleotide from
cationic nanoemulsions. Eur. J. Pharm. Biopharm, 2008; 70: 248–259.
87. Anumolu, S. S.; Singh, Y.; Gao, D.; Stein, S.; Sinko, P. J. Designand evaluation of novel
fast forming pilocarpine-loaded ocular hydrogels for sustained pharmacological response.
J. Controlled Release, 2009; 137: 152–159.
www.wjpps.com Vol 8, Issue 6, 2019.
1490
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
88. Pandit, J. K.; Bharathi, D.; Srinatha, A.; Ridhurkar, D. N.; Singh, S. Long acting
ophthalmic formulation of indomethacin: evaluation of alginate gel systems. Indian J.
Pharm. Sci, 2007; 69(1): 37–40.
89. Numata, C.; Teraoka, R.; Matsuda, Y.; Yagi, K.; Hirai, M.;Kitagawa, S. Dose control
study on fentanyl patchusing two types of covering material. Jpn. J. Pharm. Health Care
Sci, 2008; 34(1): 26–31.
90. Colin, S.; Krier, G.; Jolibois, H.; Hachimi, A.; Muller, J. F.; Chambaudet, A.
Characterization of the corrosionlayer of copper-nickel alloys in a synthetic sweatmedium
by FTMS and LAMMA laser. Appl. Surf. Sci, 1998; 125: 29–45.
91. Ardizzone S, Porro G B. Comparative tolerability of therapies for ulcerative colitis, Drug
Saf, 2002; 25(8): 561-82.
92. Ardizzone S, Porro G B. Inflammatory bowel disease: new insights into pathogenesis and
treatment, J Intern Med, 2002; 252(6): 475- 96.
93. Clemett D, Markham A. ColitisFoundation of America, Prolonged-release mesalazine:
ulcerative colitis and Crohn‟s disease, Drugs, 2000; 59: 929–956.
94. Martins GZ, Souza CRF, Shankar TJ and Oliveira WP. Effect ofprocess variables on
fluiddynamics and adhesion efficiency during spouted bed coating of hard gelatin
capsules. Chemical Engineering and Processing, 2008; 47: 2238–2246.
95. B.R. Rohrs,“In VitroDissolution Testing of Poorly Soluble Compounds:Impact of
Formulation Design,” presented at the PhRMA Acceptable Analytical Practices
Workshop,Washington, DC, 23-25 September 2003.
96. Gray VA, Hickey AJ, Balmer P, Davies NM, Dunbar C, FosterTS, Olsson BL, Sakagami
M, Shah V, Smurthwaite MJ, Veranth JM, Zaidi K. The inhalation ad hoc advisory panel
for the USP performance tests of inhalation dosage forms. Pharm Forum, 2008; 34(4):
1068–74.
97. Payne, A.N.Advances and perspectives in in vitro human gut fermentation modeling.
Trends Biotechnol, 2012; 30: 17–25.
98. Frontela-Saseta, C.Evaluation of antioxidant activity andantiproliferative effect of fruit
juices enriched with Pycnogenol(R) in colon carcinoma cells. The effect of in vitro
gastrointestinal digestion. Phytother. Res, 2011; 25: 1870–1875.
99. Laparra, J.M. and Sanz, Y.Bifidobacteria inhibit theinflammatory response induced by
gliadins in intestinal epithelial cells via modifications of toxic peptide generation during
digestion. J. Cell. Biochem, 2010; 109: 801–807.
100. Siegel, J.A.Biphasic nature of gastric emptying. Gut, 1988; 29: 85–89.
www.wjpps.com Vol 8, Issue 6, 2019.
1491
Mittal et al. World Journal of Pharmacy and Pharmaceutical Sciences
101. Jinno, J., Kamada, N., Miyake, M., Yamada, K., Mukai, T., Odomi, M., Toguchi, H.,
Liversidge, G.G., Higaki, K., Kimura, T., Effect of particle size reduction on dissolution
and oral absorption of a poorly water-soluble drug, cilostazol, in beagle dogs. J. Control.
Release, 2006; 111: 56–64.





![Multiparticulate System for Colon Targeted Delivery …...or controlled release in the proximal colon[3]. This might be achieved by the use of specially designed drug delivery system](https://img.pdfslide.net/doc/110x75/5f0d91447e708231d43aff72/multiparticulate-system-for-colon-targeted-delivery-or-controlled-release-in.jpg)