Embed Size (px)
Citation preview
300 Northwest 70th Avenues, Suite 102 • Plantation, Florida 33317
(954) 723-0057 Phone • (954) 723-0353 Fax email: [email protected]
Challenges in Pulmonary and Critical Care: 2015
No ve m be r 21 , 20 15
C le ve la n d C lin ic Flo rid a W e sto n , FL
Course Director Franck Rahaghi, MD, MHS, FCCP
Program Evaluation January 5, 2015

2
In November 2015, the National Association for Continuing Education (NACE) sponsored a CME activity, Challenges in Pulmonary and Critical: 2015, in Weston, FL. This educational activity was designed to provide an update in the prevention, diagnosis, and management of pulmonary disease to pulmonologists, hospitalists, and other health care providers who treat patients with pulmonary diseases. Current findings in pulmonary research in topics such as Pulmonary Hypertension, Idiopathic Pulmonary Fibrosis, Alpha One Anti-trypsin Deficiency, Lung Cancer, Pathology of Pulmonary Diseases, COPD, Palliative Care and Sarcoidosis were presented. In planning this CME activity, the NACE performed a needs assessment. A literature search was conducted, national guidelines were reviewed, survey data was analyzed, and experts in each therapeutic area were consulted to determine gaps in practitioner knowledge, competence or performance. Two hundred sixty three healthcare practitioners registered to attend Challenges in Pulmonary and Critical: 2015 in Weston, FL. One hundred fifty six healthcare practitioners actually attended this conference. Each attendee was asked to complete and return an activity evaluation form prior to the end of the conference. One hundred forty seven completed forms were received. The data collected is displayed in this report. CME ACCREDITATION The National Association for Continuing Education is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The National Association for Continuing Education designates this live activity for a maximum of 8 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. National Association for Continuing Education is approved as a provider of nurse practitioner continuing education by the American Association of Nurse Practitioners. AANP Provider Number 121222. This program has been approved for 8.0 contact hours of continuing education (which includes 1.25 hours of pharmacology).

Response Frequency Percent Response Frequency PercentWhat is your specialty? What is your professional degree?
Mean: - Mean: 3.58MD 62 42.47 Primary Care 59 40.41DO 7 4.79 Endocrinology 1 0.68NP 30 20.55 Rheumatology 1 0.68PA 7 4.79 Pulmonology 33 22.60RN 7 4.79 Cardiology 5 3.42Other 33 22.60 Gastroenterolog
y3 2.05
No Response 1 0.68 No Response 7 4.79What is your professional degree? Other:ResponseCTRRTRespiratory Therapist Cardiac SonographerRRTRespiratory TherapistRTRRTMSN/FNP StudentRTRTRRTRTRTRTRRTRTRTRTRTRTRTRRTRRTLPNRRTMPHMBA, CPCI, CPCRRTRRTRRTR. PharmacistRespiratoryRT
Integrated Item Analysis Report
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference
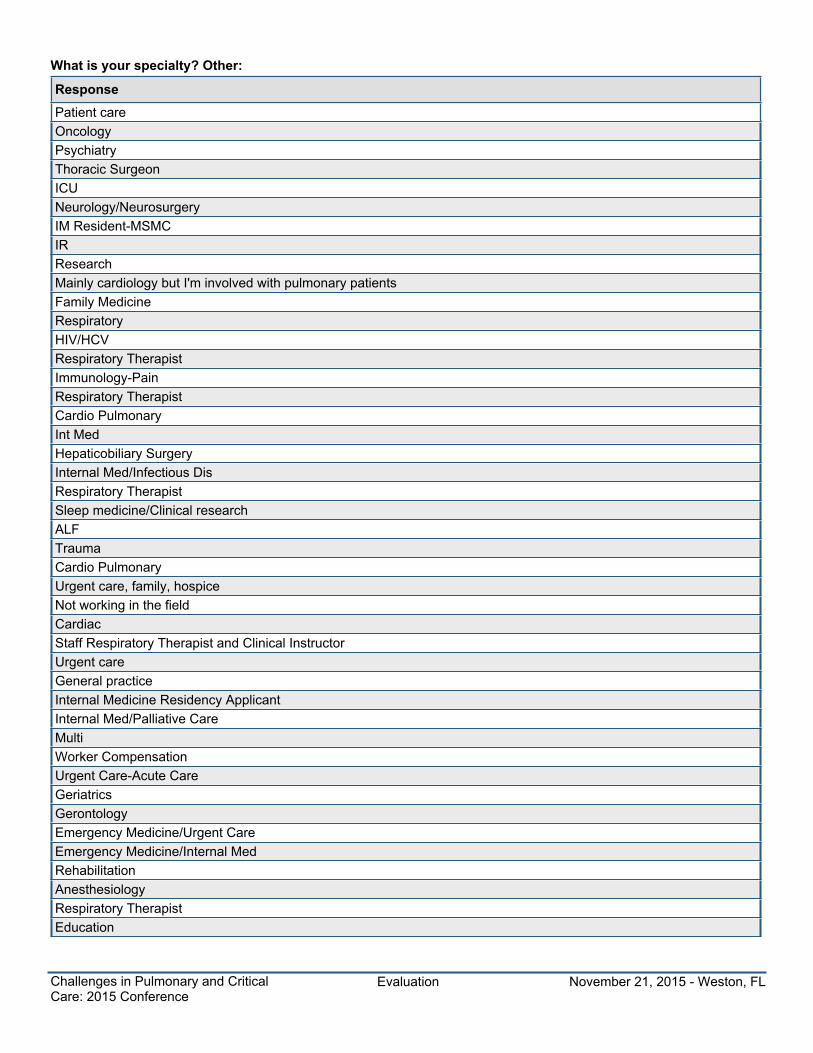
What is your specialty? Other:ResponsePatient careOncologyPsychiatryThoracic SurgeonICUNeurology/NeurosurgeryIM Resident-MSMCIRResearchMainly cardiology but I'm involved with pulmonary patientsFamily MedicineRespiratoryHIV/HCVRespiratory TherapistImmunology-PainRespiratory TherapistCardio PulmonaryInt MedHepaticobiliary SurgeryInternal Med/Infectious DisRespiratory TherapistSleep medicine/Clinical researchALFTraumaCardio PulmonaryUrgent care, family, hospiceNot working in the fieldCardiacStaff Respiratory Therapist and Clinical InstructorUrgent careGeneral practiceInternal Medicine Residency ApplicantInternal Med/Palliative CareMultiWorker CompensationUrgent Care-Acute CareGeriatricsGerontologyEmergency Medicine/Urgent CareEmergency Medicine/Internal MedRehabilitationAnesthesiologyRespiratory TherapistEducation
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference

Response Frequency Percent Response Frequency Percent
Upon completion of this activity, I can now: Discussthe appropriate strategy for the diagnosis of idiopathicpulmonary fibrosis (IPF); recognize prognosticfeatures for individual IPF patients; discussappropriate pharmacotherapeutic options forindividual IPF patients; and appreciate the optimaltiming for referral of IPF patients.
Upon completion of this activity, I can now: Discussthe pathophysiology of pulmonary arterialhypertension (PAH); explain the workup of patientssuspected of having PAH; discuss the evolution ofgoals in trials; list therapeutic options in themanagement of patients with PAH; and discusseffective use of targeted treatment options for PAH.
Mean: 1.19 Mean: 1.27Yes 113 77.40 Yes 103 70.55Somewhat 24 16.44 Somewhat 38 26.03Not at all 1 0.68 Not at all 0 0.00No Response 8 5.48 No Response 5 3.42
Response Frequency Percent Response Frequency Percent
Upon completion of this activity, I can now: Describenew advances in treatment of Lung Cancer; discussthe data behind Lung Cancer screening andrequirements for starting to screen; and describe thepatient selection for Lung Screening.
Upon completion of this activity, I can now: Reviewthe etiology of AATD; discuss how to change youroffice flow to incorporate testing for AATD andutilization of ancillary staff and the pulmonaryfunction lab; and explain treatments for AATD.
Mean: 1.28 Mean: 1.22Yes 106 72.60 Yes 113 77.40Somewhat 32 21.92 Somewhat 28 19.18Not at all 4 2.74 Not at all 2 1.37No Response 4 2.74 No Response 3 2.05
Response Frequency Percent Response Frequency Percent
Upon completion of this activity, I can now: Identifythe pathological features of Pulmonary Diseases;describe Novel tests and stains available topathologists; and discuss the special cooperative roleof Pulmonary Pathologists.
Upon completion of this activity, I can now: Describeour current understanding of the pathophysiology andthe epidemiology of Sarcoidosis; examine the state ofthe art in the methodology for diagnosis ofSarcoidosis; and review our current understanding ofthe treatments considered, including biologics andmineralocorticoid receptor agonists.
Mean: 1.25 Mean: 1.30Yes 104 71.23 Yes 96 65.75Somewhat 32 21.92 Somewhat 37 25.34Not at all 1 0.68 Not at all 2 1.37No Response 9 6.16 No Response 11 7.53
Response Frequency Percent Response Frequency Percent
Upon completion of this activity, I can now: Describethe concept of Palliative Care; discuss the palliativecare medical literature that applies to pulmonarydiseases; and identify which pulmonary patients toconsider for palliative care and when.
Upon completion of this activity, I can now:Understand clinical assessment of COPD patients indeveloping an effective individualized plan of care;implement guideline directed care for patients withCOPD; discuss effective pharmacologic therapies anddelivery options to reduce COPD; discussexacerbations while improving quality of life; andrecognize the impact of comorbidities such asdiabetes and cardiovascular disease in themanagement of patients with COPD.
Mean: 1.17 Mean: 1.20Yes 106 72.60 Yes 98 67.12Somewhat 22 15.07 Somewhat 23 15.75Not at all 0 0.00 Not at all 1 0.68No Response 18 12.33 No Response 24 16.44
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference

Response Frequency Percent Response Frequency Percent
Overall, this activity was effective in enhancing myconfidence in caring for patients with the condition(s)presented.
Overall, I would rate this activity as…
Mean: 1.32 Mean: 1.39Excellent 104 71.23 Strongly Agree 92 63.01Very Good 37 25.34 Agree 50 34.25Good 3 2.05 Neutral 3 2.05Fair 1 0.68 Disagree 0 0.00Poor 0 0.00 Strongly
Disagree0 0.00
No Response 1 0.68 No Response 1 0.68
Response Frequency Percent Response Frequency Percent
As a result of this activity, I have learned newstrategies for patient care:
Overall, this activity was effective in improving myknowledge in the content areas presented:
Mean: 1.31 Mean: 1.46Strongly Agree 102 69.86 Strongly Agree 87 59.59Agree 40 27.40 Agree 45 30.82Neutral 2 1.37 Neutral 10 6.85Disagree 0 0.00 Disagree 0 0.00StronglyDisagree
0 0.00 StronglyDisagree
0 0.00No Response 2 1.37 No Response 4 2.74As a result of this activity, I have learned new strategies for patient care. List these strategies:ResponseWhat about the cost of the treatment. No one mention this issue and is importantImproved diagnostic. Use of vaccinesTo apply the acquired knowledge in whateverGreat talks. Medicine vs all about Research and further advancement of current trends. I will implement thesestrategiesNABetter and easy early for approach to Dx/TxRefer all COPD to pulm for Alpha 1 testingNon Physician- RT- I have a better understanding of the information presentUnderstanding and Dx. COPD pt with treatment optionsBetter patient care and follow up. New testimonials available. When to refer complex patients. Review old patientsstrategy/ new patient strategyScreening for COPD with dephNewer diagnosis and treatment meansHow to approach patients who are "healthy" but should follow screening tests for lung cancer. Differentiate diagnosisfrom PFT resultsMake sure more of my patients see pulmonologist. Continue due diligence in my assessments to hopefully not missthese disordersEarly intervention and treatmentPre-screening remotely and in officeAlpha, Antitripsine deficiency should be screening in all COPD. Usual Interstitional PNA does not affect upper lobe andmiddle lobe (on in again testing no evidence of the disease). Lung Cancer screening > 55 yo > 30 smoking (LRCTscan)Identify and diagnose different pathology. Appropriate referralNew drugs available for Tx of sarcodosis, COPD
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference

As a result of this activity, I have learned new strategies for patient care. List these strategies:ResponseRequested CT for Lung Cancer screening more frequently gives Tx for AATD for stabilized patients yet Cortico ids isthe gold standard treatment for SorcordoTo learn more ways of treating incurable diseases and more guidelines about higher risk patientsPathophysiology. Treatment. S+SBetter understanding pul HT and IPF. Alpha 1 (AATD). Lung Ca. Sarcoid. COPD. PalliativeWho to treat and when to treatSpecific testing is importantScreening for lung cancer. More vigilant looking for Alpha-1 anti-trypsin deficiencyDx and Tx strategies. Current guidelines. Future outlookAlpha 1Better skills in cancer screening Alpha 1 Antitrypsin diagnosis. CT2 X-ray needing editing on Dx and relevant ont of Vilnnew treatment on lifetimeAdequate screening and managementCombination with Ambrisentan- Tadalfil best Tx for PAH. IV Augmentation therapy of 4 drugs is optimal Tx for AATDEarly low dose CT for Lung Ca. AAT testingVarious ways and techniques to interpret, diagnose and treat lung diseasesNew treatmentsVery educationalAble to understand diagnostic of pulmonary diseaseManagementAssessment of COPD. Palliative care discussion. Discuss/ management of Hydropathic Pulmonary FibrosisIn-depth evaluation first then treatDiagnostic tests. Mortality rates. Treatment med plansDiscuss more openly palliative care with patientsTest every symptomatic COPD pt for Alpha 1Creating templates and protocols for COPD. Goal oriented approach to pulm HTN ptsVery resourcefulApply CT guided biopsy in lung cancerDiagnostic lookupCurrently on medical disability but did learn a lot that I would use when I return to workforce shortlyDiagnosing and treatmentTo use better knowledge in screen and Dx and Tx. Teach/ education pt with risk for Resp disease. To refer to specialistas early as possibleCheck Alpha-1- AT level and genotypeMore A-1-AT geneticsBeryllium is very similar to sarcoidoan and sarcordion not all patient's need to be treatedIncrease AATD testing, Careful eval for any ILD/ UIP dxI hope the MD's will use some of theseMore comprehensive/ extensive differential diagnosis. Different Dx tests- such as Lous disease CT scan vs IXR, HR CTin pulmonary visionWill look at COPD patients in a new wayTest all COPD pts for Alpha 1 antitrypsin enzyme deficiency. Screening for Sarcoid in appropriate pts (more =)previously. Use of low dose CT to screen patients who are at risk for lung cancer (w/in 15 yrs)Ex: the work up of patients suspected of having PAH. Strategy for Dx of IPFDiagnosis allgorithmsWill screen for L.C.
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference

As a result of this activity, I have learned new strategies for patient care. List these strategies:ResponseI will try to improve my dropusfile screening and assessment in all my pts with pulmonary dzNew methods for Dx and Rx for Lung Ca, Sarcoidosis, Pathology with IPF, HistoDiagnostic workup. Timely referralsPrecise diagnostic tests. Appropriate medications based on diagnosis with test resultsFor example: All patients with COPD should be tested for AATD. Best screening for Lung cancer is low dose CT. LABA/LAMA decrease COPD exacerbationHow to screen for AAT. Manage Sarcoid, etc.Better screening/ treatmentScreening for AAT. Screening for Lung CancerUtilize PFT in guidance for AATD testing. V/Q scan use to R/O thrombolytic related PAHTest COPD for Alpha 1 deficiencyBest practice. New meds and interventions. Screening best practiceDo testing on broader scale of patients with ages for Alpha-1 antitrypsin defWhen Dx IPF- one of the gold standard on Radiology scan is "honey combing". Every COPD pt should be screened forAlpha-1. Low dose CT af chest more precise than x-ray for pts with hx af smoking whose never had annual CXRDiagnostic test and referral to specialist. Include palliative care options and patient/ family education of choices withrationaleAssessment, treatmentAs a direct patient care Resp. Therapist- I will and have suggested my patients see a Pulmonologist for A1 testingWorkup for PAH. Incorporate testing for AATDNew treatments for PAH, AAT testing, SARCOIDIdentifying ACOS and recognizing benefit of ICS/LAMA combo. Use of PDEY inhibitors in very severe/ severe COPD w/wet cough (chronic bronchitis). Initial combo therapy in DAHWork-up for reinfected PAH patients. Early referral of unexpected IPF pts. AATD testing in COPD pts. Lung cascreening. Pt referral (early). COPD Tx guidelinesEarly diagnosis of lung caPreventative strategies for lung cancer. Symptoms and management of pulmonary HTNTo reduce the chance of multiple organ failure. Measures to improve pulmonary functionVery helpful in practice and improve patients careTherapeutic options in management of patients. Recognize co-morbidities in management of patients
Response Frequency Percent Response Frequency Percent
When do you intend to implement these newstrategies into your practice?
How likely are you to implement these new strategiesin your practice?
Mean: 1.73 Mean: 1.91Very likely 84 57.53 Within 1 month 78 53.42Somewhat likely 32 21.92 1-3 months 25 17.12Unlikely 4 2.74 4-6 months 4 2.74Not applicable 21 14.38 Not applicable 31 21.23No Response 5 3.42 No Response 8 5.48
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference

Response Frequency Percent Response Frequency Percent
In terms of delivery of the presentation, please rate theeffectiveness of the speaker: Felipe Martinez, MD -IPF:
In terms of delivery of the presentation, please rate theeffectiveness of the speaker: Abubakr Bajwa, MD - PH:
Mean: 4.75 Mean: 4.68Excellent 109 74.66 Excellent 105 71.92Very Good 25 17.12 Very Good 30 20.55Good 2 1.37 Good 6 4.11Fair 2 1.37 Fair 1 0.68Unsatisfactory 0 0.00 Unsatisfactory 0 0.00No Response 8 5.48 No Response 4 2.74
Response Frequency Percent Response Frequency Percent
In terms of delivery of the presentation, please rate theeffectiveness of the speaker: Jinesh Mehta, MD - LungCancer:
In terms of delivery of the presentation, please rate theeffectiveness of the speaker: Franck Rahaghi, MD -Alpha-1:
Mean: 4.82 Mean: 4.81Excellent 117 80.14 Excellent 115 78.77Very Good 23 15.75 Very Good 18 12.33Good 1 0.68 Good 2 1.37Fair 0 0.00 Fair 0 0.00Unsatisfactory 0 0.00 Unsatisfactory 1 0.68No Response 5 3.42 No Response 10 6.85
Response Frequency Percent Response Frequency Percent
In terms of delivery of the presentation, please rate theeffectiveness of the speaker: Pablo A. Bejarano, MD -Pathology:
In terms of delivery of the presentation, please rate theeffectiveness of the speaker: Franck Rahaghi, MD -Sarcoidosis:
Mean: 4.86 Mean: 4.73Excellent 109 74.66 Excellent 95 65.07Very Good 16 10.96 Very Good 23 15.75Good 1 0.68 Good 2 1.37Fair 0 0.00 Fair 2 1.37Unsatisfactory 0 0.00 Unsatisfactory 0 0.00No Response 20 13.70 No Response 24 16.44
Response Frequency Percent Response Frequency Percent
In terms of delivery of the presentation, please rate theeffectiveness of the speaker: Nydia Martinez Galvis,MD - Palli:
In terms of delivery of the presentation, please rate theeffectiveness of the speaker: Anas Hadeh, MD - COPD:
Mean: 4.81 Mean: 4.75Excellent 90 61.64 Excellent 78 53.42Very Good 17 11.64 Very Good 19 13.01Good 2 1.37 Good 3 2.05Fair 0 0.00 Fair 0 0.00Unsatisfactory 0 0.00 Unsatisfactory 0 0.00No Response 37 25.34 No Response 46 31.51
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference

Response Frequency Percent Response Frequency Percent
To what degree do you believe that the subject matterwas presented fair, balanced, and free of commercialbias? Felipe Martinez, MD - IPF:
To what degree do you believe that the subject matterwas presented fair, balanced, and free of commercialbias? Abubakr Bajwa, MD - PH:
Mean: 4.86 Mean: 4.87Excellent 120 82.19 Excellent 124 84.93Very Good 18 12.33 Very Good 15 10.27Good 1 0.68 Good 2 1.37Fair 0 0.00 Fair 0 0.00Unsatisfactory 0 0.00 Unsatisfactory 0 0.00No Response 7 4.79 No Response 5 3.42
Response Frequency Percent Response Frequency Percent
To what degree do you believe that the subject matterwas presented fair, balanced, and free of commercialbias? Jinesh Mehta, MD - Lung Cancer:
To what degree do you believe that the subject matterwas presented fair, balanced, and free of commercialbias? Franck Rahaghi, MD - Alpha-1:
Mean: 4.90 Mean: 4.90Excellent 128 87.67 Excellent 127 86.99Very Good 12 8.22 Very Good 12 8.22Good 1 0.68 Good 1 0.68Fair 0 0.00 Fair 0 0.00Unsatisfactory 0 0.00 Unsatisfactory 0 0.00No Response 5 3.42 No Response 6 4.11
Response Frequency Percent Response Frequency Percent
To what degree do you believe that the subject matterwas presented fair, balanced, and free of commercialbias? Pablo A. Bejarano, MD - Pathology:
To what degree do you believe that the subject matterwas presented fair, balanced, and free of commercialbias? Franck Rahaghi, MD - Sarcoidosis:
Mean: 4.87 Mean: 4.85Excellent 111 76.03 Excellent 105 71.92Very Good 14 9.59 Very Good 16 10.96Good 0 0.00 Good 1 0.68Fair 1 0.68 Fair 0 0.00Unsatisfactory 0 0.00 Unsatisfactory 0 0.00No Response 20 13.70 No Response 24 16.44
Response Frequency Percent Response Frequency Percent
To what degree do you believe that the subject matterwas presented fair, balanced, and free of commercialbias? Nydia Martinez Galvis, MD - Palli:
To what degree do you believe that the subject matterwas presented fair, balanced, and free of commercialbias? Anas Hadeh, MD - COPD:
Mean: 4.88 Mean: 4.86Excellent 99 67.81 Excellent 93 63.70Very Good 12 8.22 Very Good 13 8.90Good 1 0.68 Good 1 0.68Fair 0 0.00 Fair 0 0.00Unsatisfactory 0 0.00 Unsatisfactory 0 0.00No Response 34 23.29 No Response 39 26.71
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference

Response Frequency Percent Response Frequency Percent
Future CME activities concerning this subject matterare necessary:
Which statement(s) best reflects your reasons forparticipating in this activity:
Mean: - Mean: 1.59Topics covered 119 81.51 Strongly agree 71 48.63Location/easeof access
91 62.33 Agree 60 41.10Faculty 60 41.10 Neutral 11 7.53Earn CMEcredits
110 75.34 Disagree 1 0.68StronglyDisagree
0 0.00No Response 1 0.68 No Response 3 2.05What topics would you like to see offered as CME activities in the future?ResponseCardiac Disease signs and symptoms, Evidence based approach to treatment, PharmacologyUse of diagnostic tool, Side effects of new vaccinesSameRheumatology, Gastroenterology, DermatologyAsthma advancements, New medicine tech.NeurologyAnyBronchial thermoplastyAsthma, Ventilator managementAsthma- Medical management for children- mechanical devicesAsthma/ COPD overlap symptoms, Sepsis syndrome update, Case presentations- complex cases, PneumoniaHypothyroidism, AsthmaUlcerative colitis, Crohn's diseaseCardiac, CHF presentations and CU surgeryObamacare, now what? How to make Medical Boards more Physician friendly rather than punitiveAlzheimer's DiseaseAsthma inavative therapyProstate cancer, MDRTBPsychological aspects of patients with chronic pulmonary diseaseHypertension, DementiaN/ASarcoidosisPulmonary Hypertension.All current relevant topics in healthcareLiver Disease, HIV, NeurologyMechanical VentilationTx's of COPD and pt with Pulmonary Hypertension for the Respiratory TherapistVent managementEmphasizing Preventative Medicine, Adherence to treatment in Diabetes Mellites, Morbid Obesity, Quitting smokingCystic FibrosisCOPD mechanical ventilationSleep medicine, Occupational Lung diseases
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference

What topics would you like to see offered as CME activities in the future?ResponseUpdate of anti-hypertension medicationsHow to deal with Seniors Alzheimers and Dementia when they get hostile and in 1 min forget they ate or took showeretc. Frustration for the caregiver please, guidelines neededDiabetes, Womens health, Sexually transmitted diseases, Prostate diseasesAsthma, MigraineSepsis campaign, Neuro ICU Herrodynamics, HanodynamicsPulmonary rehabMore GI topicsIntegrative medicineIf it's not related to this topic- then Colon CA, Autism in children, Rare breast cancerSamePulmonary Emboli/ DVT what other work up NEEDED, beside treatmentTB, HIVHypothyroidContinue lung disease topic cover- ie pneumonia, cr, new guidelines cover as well as hospice and palliative careEmersion Rx in Arthritic, Pulmonary effect of 911 (WTC responders)Cardiovascular risk reduction, Advanced Cardiology, Cancer preventionPulmonary Medicine, Congestive Heart failure, DM, Primary Care topics, Rheumatological topicsDermatology Review and updateLung Nodules, Lung cancers, Infections common/ uncommon- Biopsies using navigation/ cryo options, New Asthmabiologies (IL4, IL5, IL13), Reducing re-hospitalization tactics for PNA, COPDObesityGI, Polyps, ObesityInterventional pulmonary medicine/ proceduresENT Disorders, tx plan, GI DisordersCOPD, Asthma, Pulmonary CarcinomaNew technology/ advances in Ventilator managementHIVAcute Chest Syndrome, Sickle cell DiseasePain related to COPDCOPD- acute and chronic managementMore radiology topicsHIVRheumatology, Hematology Oncology, Radiation Oncology, NeurologyNeurologic muscle diseasesWorker compensationAllergy induced asthma and common variable immunodeficiency, cough variant asthmaHematologyObesityManagement of Cardiopulmonary patients, COPD, etc. Meganica ventilationOccupational hazards as related to pulmonary effectsStem cell and pulmonary patient, Also nano technology how close are we to improvement in medicineMetabolic topics, Mental disorders, Immunology disordersAbdominal pain in female and male in Emergency medicineElectronic health records, ICD10, Health education methodsGastro-intestinal
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference

What topics would you like to see offered as CME activities in the future?ResponsePsychological- mental illness due to Pulm Diagnosis. Dr. Martinez touched on this- besides empathy, sympathy. Andhow to deal as careworkers with these patientsBronchial AsthmaAlzheimersObesity, Skin disordersWomen's health, Gyn/ OBModes of ventilation, APRV on flakkaDiabetesSimilar practical and important topics
Additional comments:ResponseThanks. Excellent faculty and waterExcellent courseOkVery informative. Thank youThis was a very excellent conference, educational and up to date. Current information in Diagnosing and Treating ptwith Pulmonary disease. Great Histology slides on different Lung Diseases. Looking forward for next year conference.Please have hot tea if possible on next conference. Thank youExcellent courseVery educational (reinforced info). I enjoyed the conference. Please provide hot water for hot tea. Not everyoneconsume coffee. ThanksThank you for inviting meGreat conferenceExcellent conferenceNoneHave the speakers "repeat the question." Have long desks for us to learn on and take notes, rather than just chairs. Dr.Bejarano- accent hard to understandVery good conferenceThanksExcellent organizationThank you to NACE and all the Doctors and speakers for this and future seminarsThis was a little over my expertiseThank youThey try to states the meaning of Pneumonics, as this can decrease the quality of an excellent presentation as we needto go to the web to figure it outThat was a great and effective lectureVery good conferenceThanksAnas Hadeh is a terrible speakerMore education from the speakers, less case studies and Q/A. Information is too technical at times. Make it moreunderstandable to the audience. Each session is too long in timeNice to see much less research and more clinical. Dementia was well organized and simplified. I liked how the ppt waslaid out. Good to see ppt and lectures free from commercial biasI enjoyed this conference. Too bad not enough chairs with talks available for everyone, but this was okayHeartfelt thank you for all Faculty, staffs and sponsor who make this CE conference possible
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference

Additional comments:ResponseLast former too more conferenceChange your TVs to 1080 (They're awful)Excellent program! ThanksHave enough food for the people attending the conferenceExcellent lecturesGreat conferenceWhen sending acceptance to conference (via email) attach maps and directions to center, parking instructions, etc. tohelp those who are not familiar with location and/or centerThe guideline provided include power point and some graphicAs always, great lecturesVery educational and knowledgeable topicsGreat activity, very organizedToo detailed for 10 MDExcellent presentations. Thanks a lotAlways with distinguished speakers. Great lecturesConsider including an ARAP on your speaker panelNoneExcellent and very relevant topics scope and update. Excellent speakers available for questions. Thank youLong overdueGreat seminar. Thank you for the invitationVery informative
Evaluation November 21, 2015 - Weston, FLChallenges in Pulmonary and CriticalCare: 2015 Conference










![57 F1 742, Federal Reporter - Public.Resource.Org › pub › us › case › reporter › F › 0057 › 0057.f1.0742.pdf742:']. nOER.u. QPQRTElt, vol. 57.i.T})js ·.~~~~nt]dQesnot](https://img.pdfslide.net/doc/110x75/60dd651e2c0b615a0667b025/57-f1-742-federal-reporter-a-pub-a-us-a-case-a-reporter-a-f-a-0057.jpg)

















![094-0057-20 [Unlocked by Www.freemypdf.com]](https://img.pdfslide.net/doc/110x75/577c83031a28abe054b32f1f/094-0057-20-unlocked-by-wwwfreemypdfcom.jpg)
