Challenges in Resource Allocation and Health Service Purchasing
Stellenbosch 1 July 2011
Slide 2
Agenda Major Reform of Purchasing for South Africa Strategic
Purchasing Challenges in Contracting and Reimbursement Lessons from
Other Systems South African Challenges
Slide 3
Functions, Objectives and Goals Source: Adapted from Kutzin, J.
(2008). Health financing policy: a guide for decision-makers. WHO
Europe. Additions from healthcare financing workshop, iHEA Beijing
2009. Health system functions Intermediate objectives of health
finance policy Health system goals
Slide 4
Major Reform of Purchasing for South Africa
Slide 5
MoH on NHI Progress, May 2011 We are working around the clock
everyday around this issue of NHI. The problem is that many believe
that NHI is just the release of a document. For us in health, we
know that it also involves an extensive preparation of the health
care system while at the same time preparing a policy document. In
this case the reengineering of the Health Care System is very
vital. Under the present health care system whether public or
private, no national health insurance can ever survive. While it is
very true that the public health care system is bedevilled by very
poor management leading to poor quality of care adding to the very
low resources available in the public health sector, I wish to
categorically state that the present overall health care system
both public and private will be completely re-engineered. Source:
Health Budget Vote Policy Speech, National Assembly, Dr A
Motsoaledi, 31 May 2011
Slide 6
MoH on Re-engineering The reengineering of the Health Care
System will be according to three main streams. The first stream
will be a district based model. In this model a team of 5
specialist or clinicians shall be deployed in each district. These
teams will specifically focus on maternal and child mortality. This
will help us arrive at our Millennium Development Goals. The 2nd
stream is a School Health programme. Will include eye care, dental
and hearing problems and immunisation programmes in schools. Later
contraceptive health, HIV/AIDS, drug and alcohol abuse. The last
stream will be a ward based PHC model which will deploy at least 10
well trained PHC workers per ward. This method is being put to good
use in Brazil and India. Example of TB care pilot which includes
enhanced diagnostics. Source: Health Budget Vote Policy Speech,
National Assembly, Dr A Motsoaledi, 31 May 2011
Slide 7
District Management Team Source: Re-engineering Primary Health
Care in SA, Discussion document, Nov. 2010 The district management
team (DMT) is responsible and accountable for everything that
happens in the district.
Slide 8
Financing and DMTs It is recommended that all funds for the
functioning of the DHS and the associated PHC should be under the
control of the DMT both in terms of budgeting and financial
management. The DMT should use these funds to purchase selected
services from private providers (e.g. doctors, optometrists,
audiologists) where these skills are not available in the public
sector and where there are gaps. With the NHI in mind it is also
recommended that the DMT become the fund holders for any proposed
PHC capitation and become responsible for allocation of budgets to
ensure the necessary services. In the short term they will probably
require provincial support and mentoring for contract management.
Source: Re-engineering Primary Health Care in SA, Discussion
document, Nov. 2010
Slide 9
DMT Reform Questions Current National Treasury allocates budget
to nine provinces. Risk-adjusted allocation from 2011. Province
responsible for facilities and delivery. Some purchasing and
private contracting. Proposed 52 Districts Who allocates budget?
Risk-adjustment to districts? Problematic data issues. What is a
district? DMT responsible for PHC, clinics, community health
centres and district hospitals. Also school health and
environmental health. Presumably province responsible for regional
and tertiary hospitals? Other? Emergency transport?
Slide 10
Strategic Purchasing
Slide 11
WHO on Purchasing, 2000 Purchasing is the process by which
pooled funds are paid to providers in order to deliver a specified
or unspecified set of health interventions. Passive purchasing
implies following a predetermined budget or simply paying bills
when presented. Strategic purchasing involves a continuous search
for the best ways to maximize health system performance by deciding
which interventions should be purchased, how, and from whom. It
involves the use of selective contracting and incentive schemes.
Purchasing uses different instruments for paying providers,
including budgeting. Source: WHO World Health Report 2000
Slide 12
WHO on Purchasing, 2010 Health-care systems haemorrhage money.
While some countries lose more than others, most, if not all, fail
to fully exploit the resources available, whether through poorly
executed procurement, irrational medicine use, misallocated and
mismanaged human and technical resources or fragmented financing
and administration. All countries can look to improve efficiency by
taking a more strategic approach when providing or buying health
services, e.g. decide which services to purchase based on
information on the health needs of the population and link payments
to providers on their performance and to information on service
costs, quality and impact. Source: WHO World Health Report
2010
Slide 13
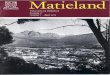
Reimbursement and Risk Fee-for-Service Percentage of Premium
Capitation Per Case Per Diem Provider Risk Fund Risk Low High
LowHigh Source : Garofalo et al, Managed Care Contracting,
1999
Slide 14
WHO on Reimbursement All provider payment mechanisms have
strengths and weaknesses, but particular care should be taken with
fee-for-service payments, which offer incentives to over-service
those people who can pay or who are covered from pooled funds, and
to underservice those who cannot pay. Many alternatives have been
tried. All have advantages and disadvantages. Paying service
providers is a complex, ever-changing process and some countries
have developed a mixed payment system, believing it is more
efficient than a single payment mode. Countries will decide where
they can operate based on their ability to collect, monitor and
interpret the necessary information, and to encourage and enforce
standards of quality and efficiency. Source: WHO World Health
Report 2010
Slide 15
WHO on Waste, Corruption and Fraud Estimated 1025% of public
spending on health linked to procurement is lost each year to
corrupt practices. Experience has shown that to significantly curb
corruption , two complementary strategies need to be applied: a
discipline approach (top-down) based on legislative reforms,
establishing laws, administrative structures and processes needed
to ensure transparent medicine regulation and procurement; and
bottom-up values approach that promotes institutional integrity
through moral values and principles, and tries to motivate ethical
conduct by public servants. Also, accrediting and licensing health
providers, facilities and products (to improve quality), internal
oversight and audit functions. Improved governance requires
intelligence and better use of information, so that breaches of
practice can be identified and changes monitored. Source: WHO World
Health Report 2010
Slide 16
WHO on Fragmentation The bigger the risk pools, the better.
Large pools offer several advantages, notably a greater capacity to
meet the costs of occasional, costly diseases. Small pools are not
financially viable in the long run. Small pools are vulnerable. The
most efficient health systems avoid fragmentation in pooling but
also in channelling funds and distributing resources. Fragmentation
can also be inefficient. Systems with multiple funding channels and
pools, each with its own administrative costs, duplicate effort,
are expensive to run and require coordination. Similarly,
fragmentation in other parts of the system running hospitals,
distributing medicines and equipment, supporting laboratory systems
results in unnecessary waste and duplication. This applies also to
small government-managed pools, such as a district health budget.
In some cases, adequate coverage in poorer districts can be
achieved only when there is direct subsidy from central funding
pools or districts can share costs. Source: WHO World Health Report
2010
Incentives in Building Work Per Uur? Per Muur? Source: Dr
Reinder Nauta, Carecross
Slide 20
Risks Taken Reimbursement Fee-for-Service Percent Premium
Capitation Per Case Per Diem
PriceMarketingFrequencySeverityIntensityActuarial P PI PMFSIA PFSI
PSI Source : Garofalo et al, Managed Care Contracting, 1999
Slide 21
Primary Care Contract Example 1 Medical Scheme Managed Care
Organisation GP Practice Capitation Fee-for-Service PFSI FSI P MA
PMFSIA Transferred
Slide 22
Primary Care Contract Example 1 National Treasury District
Health Board GP Practice Capitation Fee-for-Service PFSI FSI P MA
PMFSIA Transferred
Slide 23
Encouraging entrepreneurial behaviour while protecting core
social values www.euro.who.int/observatory/
Slide 24
Impact of Switching to Retrospective Hospital Payments
Countries with an emerging health insurance model tend to start
with a mixture of retrospective methods of payment and traditional
item-by- item funding of medical facilities. [i.e. fee-for-service]
Insurers in the Czech Republic, Hungary and the Russian Federation
This encouraged hospitals to increase workload and contributed to
higher internal efficiency of hospitals [from command and control].
But structural inefficiency has worsened owing to the growth of
inappropriate admissions and a lack of constraint on using costly
methods of care. Czech Republic: introduction of retrospective
payment system: health expenditure increased by almost 40 per cent
in 2 years. Need for tougher regulatory requirements for health
insurers to use less open-ended provider payment schemes. Source:
Regulating Entrepreneurial Behaviour in European Health
Systems
Payment for Performance
www.euro.who.int/Document/HSF/P4P_Estonia.pdf
Slide 29
Lessons from Other Systems
Slide 30
New Zealand Aotearoa Source: StatsNZ June 2010; WHO Observatory
2009 Total health expenditure: 9.7% of GDP US$ 2,634 per capita pa
Government expenditure 80.2% 71% of private expenditure is OOP
Oldest NHS in the world 1938 4.3 m people 18% aged 60 and over
Unemployment 6% South Island 1.0 m people North Island 3.3 m people
Auckland: 1.5 m
Slide 31
NZ District Health Boards See:
http://www.nationalhealthboard.govt.nz/DHB-Linkshttp://www.nationalhealthboard.govt.nz/DHB-Links
20 District Health Boards Providing directly or funding the
provision of Government funded health care services for the
population of a specific geographical area. Risk-adjustment formula
to allocate funds to DHBs
Slide 32
Health Reform: HBs, AHBs, CHEs, HHSs, DHBs? 1938-1983: Hospital
Boards had a strictly hospital focus; publicly elected (DoH ran
non-hospital public health and some mental health). 1983-1993: Area
Health Boards (AHBs) -hospital and public health services; partly
publicly elected and partly appointed by Government. 1993-1997: 23
Crown Health Enterprises (CHEs), 4 Regional Health Authorities and
Public Health Commission. Publicly owned companies, boards
appointed by Government. 1997: 24 Hospital and Health Services
(HHSs) and Health Funding Authority. Publicly owned companies;
wider range of health and disability service provision; boards
appointed by the Government. 2000: 20 District Health Boards (DHBs)
- very wide responsibilities for publicly funded health and
disability services, including purchasing of services; bodies
corporate owned by the Crown; elected and appointed boards. 2002:
Primary Health Organisations (PHOs) formed. 2009: National Health
Board (NHB) established. Source: http://www.moh.govt.nz and
http://www.health.govt.nz/http://www.moh.govt.nzhttp://www.health.govt.nz/
Slide 33
Improving Health System Performance The question of determining
the appropriate purchasing agent that is, what configuration buys
health services more cost- effectively and according to the needs
and wants of the population it represents has yet to be answered.
ANYWHERE Source: Purchasing to Improve Health System
Performance
Slide 34
Canterbury DHB Canterbury District Health Board (DHB) is the
second largest by population and geographical area (510,000 people
in 2010). Plan, fund, provide healthcare and promote health and
well-being. Largest employer in South Island; over 8,000 staff
employed in 14 hospitals and numerous community bases. 80% of staff
are clinical. Similar number of people employed in delivering
health and disability services, funded either directly or
indirectly by the Canterbury DHB. Over 500 contracts. Primary
health organisations (PHOs) funded by DHBs to support the provision
of essential primary health care services through GPs to those
people enrolled with the PHO. 46 PHOs (countrywide) vary widely in
size, structure; all not-for-profit organisations. GPs in private
practice. Some private hospitals and specialists. Centralised
budget for medicines administered by Pharmac.
Slide 35
NHS Administration The NHS employs 1.4 million staff and has a
budget of 100 billion. [Population 61.8 million in 2009; world's
biggest employer after Indian rail and Chinese Army; half are
clinical staff] Total number of NHS staff increased by around 35%
between 1999 and 2009, but the number of managers increased by 82%.
The NHS today faces great challenges:... It remains stifled by a
culture of top-down bureaucracy For too long, processes have come
before outcomes, as NHS staff have had to contend with 100 targets
and over 260,000 separate data returns to the Department each year.
We will remove unjustified targets and the bureaucracy which
sustains them. We will rebalance the NHS, reducing management costs
by 45% over the next four years : The dismantling of this
bureaucracy will help the NHS realise up to 20 billion of
efficiency savings by 2014. Sources: The Kings Fund, How Many
Managers are there in the NHS? April 2010 Andrew Lansley,
Liberating the NHS announcement July 2010
Slide 36
NHS Accountability
http://www.kingsfund.org.uk/publications/nhs_accountability.html
Accountability in the NHS: Implications of the governments health
reform programme Seeks to inform the debate around the nature of
accountability relationships in the NHS and how these will change
under the reforms. The authors identify five types of
accountability most relevant to health care by scrutiny,
management, regulation, contract and election.
Slide 37
Countries with Risk Adjustment in National Health System
Developed Countries: Australia Canada Denmark Finland Ireland Italy
New Zealand Norway Spain Sweden United Kingdom USA Not an
exhaustive list ! Developing Countries: Brazil Chile Colombia Costa
Rica Cuba Ghana India Indonesia Malaysia Namibia Republic of Korea
Singapore Sri Lanka Taiwan Tanzania Thailand Vietnam Source:
Studies at UCT in 2010
Slide 38
Post-code Lottery The postcode lottery means that waiting times
can range from six months to three years depending on the health
board area. [ 2009] palliative care services had become a postcode
lottery. Two Health Boards had no palliative care strategy .
[Scotland, 2008] Best performing GPs tend to cluster in the
affluent areas of the city, which is reflective of the 'post code
lottery' where those that reside in the affluent wards are able to
demand a better quality of NHS GP services than those that tend to
reside in the deprived wards who tend to suffer in silence Outgoing
health watchdog Ron Paterson has lashed out at New Zealand's
"post-code lottery" public health system, after finding a woman's
access to diagnostic scanning was unfairly delayed. At the heart of
the Gillard Governments [Australian] health reform are an
Independent Hospital Pricing Authority and a National Health
Performance Authority Fixing the hospital postcode lottery is a
matter of life and death [May 2011] Source: Press reports 2008 to
2010
Slide 39
Kings Fund on Variation 2011 Variations in health care in the
NHS are a persistent and ubiquitous problem. But which variations
are acceptable or warranted for example, variations driven by
clinical need and informed patient choice and which are not? The
important question is how to promote good variation and minimise
bad variation. Variations in health care: The good, the bad and the
inexplicable explores the possible causes of variation, shows the
different ways in which variations can be measured, and analyses
variations by PCT. The data itself is not always easy to collect
and analyse. The report outlines the different ways in which
variations can be measured and how these measures can be adjusted
for need age and gender, economic and social characteristics.
Source: Kings Fund, 2011
http://www.kingsfund.org.uk/publications/healthcare_variation.htmlhttp://www.kingsfund.org.uk/publications/healthcare_variation.html
Slide 40
Decentralization in Healthcare Published European Observatory,
2007 www.euro.who.int/__data/assets/pdf_file/0004/.../E89891.pdf
The logic of decentralization is an intrinsically powerful idea:
that smaller organizations, properly structured and steered, are
inherently more agile and accountable than larger organizations.
The recent upsurge in countries reversing the trend and beginning
to recentralize key functions raises new and fundamental questions
about the overall strategy of decentralisation. Is the period of
decentralization of health systems in Europe coming to an end?
Slide 41
Complexities of Decentralization in Europe Many countries have
decentralized, recentralized and then decentralized again in an
on-going cycle, searching for the right balance of efficiency and
responsiveness in their health care system. Looking at the
arguments for and against, in many cases the same reasons are used
to justify movement in opposite directions. These debates are still
current and decentralization is a highly contested process across
Europe. Whatever the nature of the decentralization, it is highly
context- specific Comparison across Europe is difficult given the
complex nature of the arrangements, the importance of the
underlying historical context and the lack of strong evidence.
Source: Euro Observer Spring 2011
Slide 42
South African Challenges
Slide 43
Governance in South Africa The development of proposals for a
District Health System (DHS) have engaged policy discussions within
South Africa for around twenty years.
Slide 44
Defining Decentralization Deconcentration is generally the most
common and limited form of decentralization, and involves the
transfer of functions and/or resources to the regional or local
field offices of the central government agency in question. Within
a deconcentrated system, authority remains within the same
institution (e.g. MoH), but is spread out to the territorially
decentralized instances of this institution. Delegation implies the
transfer of authority, functions, and/or resources to an autonomous
private, semi-public, or public institution. This institution then
assumes responsibility for a range of activities or programs
defined by the central government, often through the mechanism of
contracting. Devolution is the cession of sectoral functions and
resources to autonomous local governments that, in some measure,
then take responsibility for service delivery, administration, and
finance. Source: Classification by Bossert in DBSA report on
Governance, v.d. Heever, February 2011
Slide 45
Governance, Accountability and Decentralisation Source: DBSA
report on Governance, v.d. Heever, February 2011
Slide 46
Financial Systems and Corruption According to the Special
Investigating Unit, it is estimated that 20-25 percent of state
procurement expenditure, amounting to roughly R30 billion a year,
is wasted through overpayment or corruption. Research done by
Municipal IQ revealed serious problems with regard to municipal
finance and intergovernmental fiscal issues. financial auditing and
the investigation of corruption have revealed that weak systems
make it easier for corruption to occur. Improving the overall
capacity and functioning of the public service, particularly in
relation to financial systems and controls, information systems,
and overall management capability might be the single most
effective way of deterring corruption. Source: National Planning
Commission, Diagnostic Overview, 2011
Slide 47
Ghosts in the System Ghost workers (on PERSAL) Ghost social
security beneficiaries (SASSA) Ghost doctors (no qualifications)
Ghost procedures (medical schemes) Ghost taxpayers (SARS, March
2011) Ghost patients?
Slide 48
Budgets and DMTs All available resources need to be harnessed
and focused on improving PHC. The budgets for Programme 2 (district
level services) together with the relevant conditional grants and
other sources of external funding need to be given to the DMT for
their control and responsibility. In addition capital budgets need
to be made available so that the necessary infrastructural
improvements (clinic upgrades, water, electricity, sanitation) and
equipment are made available. It is recommended that the budget for
district level services be ring- fenced based on a formula, largely
based on a capitation fee per person living in the district.
Source: Re-engineering Primary Health Care in SA, Discussion
document, Nov. 2010
Slide 49
Western Cape Health Districts Source: WCDoH Facility Norms
Model Dominance of the City of Cape Town in the province.
Additional districts (not in Census 2001) designated for City for
planning.
Slide 50
Western Cape Districts and Wards Sources: IEC, Census 2001, WC
DoH, ASSA2008
Slide 51
District Numbers and Profile Census 2001 collected data at
District and Sub-district level outside metropolitan areas.
Metropolitan areas treated as one district. Sub-district
populations too uncertain to be used: undercount of 1 in 6;
hot-decking. Census 2011? Every ten years. Voting information
voluntary registration; no-one under voting age. Department of Home
Affairs? Dorrington, 2005: It is quite possible that clinics near
the borders of the health districts also service people from
neighbouring health districts. Registration in each district (with
payments for out-of-area use) would be a highly expensive
administrative system.
Slide 52
In Summary Tension between local responsiveness and post-code
lottery of variable services and quality. How important is equity?
Increased responsiveness AFTER consistent delivery. Need for
managers and strong information systems. Size of risk pools is
critical for financial viability. Contracting is not simple can
easily jeopardise financial soundness. No data at district level
for capitation and risk-adjustment. Devolve fund holding when a
province is well-functioning, not before. And then, only if it
makes sense.
Slide 53
Public Service Performance Addressing the uneven performance of
the public service will not be achieved through multiple new
initiatives but rather through a focused and coordinated approach.
This will require addressing a set of interrelated issues including
instability resulting from repeated changes in policy,
under-staffing and skills shortages, obstacles to building a sense
of professional common purpose in the public service, political
interference, lack of accountability, and insufficient clarity in
the division of roles and responsibilities. Source: National
Planning Commission, Diagnostic Overview, 2011
Slide 54
Heather McLeod The New Zealand Centre for Evidence-based
Research into Complementary and Alternative Medicine (ENZCAM),
University of Canterbury, Christchurch, New Zealand. Extraordinary
Professor, Department of Statistics and Actuarial Science,
University of Stellenbosch [email protected]
www.integratedhealingmbs.com