Embed Size (px)
Citation preview

Changes in Hemodynamics and Coronary Blood Flow During Left Ventricular Assistance With the Hemopump Norihiko Shiiya, MD, Robin Zelinsky, MD, Philippe H. Deleuze, MD, and Daniel Y. Loisance, MD Centre de Recherches Chirurgicales, CHU Henri Mondor, Creteil, France
The Hemopump, a catheter-mounted left ventricular assist device, has been demonstrated to be effective in supporting patients with potentially reversible cardiac failure. The mechanism of recovery of the hearts with this device is not fully understood. The effects of the Hemopump on hemodynamics and coronary blood flow with and without myocardial ischemia and failure have been studied in 8 anesthetized open-chest dogs. Coro- nary blood flow in the left circumflex artery was assessed with an intracoronary Doppler catheter. Myocardial ischemia was induced by ligation of the left anterior descending and diagonal branches. The effects of maxi-
he Hemopump (Nimbus Medical, Inc, Rancho Cor- T dova, CA) is a recently developed, catheter- mounted, temporary left ventricular assist device. It has been used for patients in cardiogenic shock after acute allograft rejection or acute myocardial infarction, and for patients who failed to be weaned from cardiopulmonary bypass [l]. Initial clinical results are encouraging, show- ing the ability of this pump to facilitate the recovery of the failing hearts. It has also been used for prophylactic left ventricular assistance during high-risk coronary angio- plasty [2].
The understanding of the mechanism of recovery of the failing hearts and the change in coronary blood flow under Hemopump support is essential for better patient management, but limited information is available on this subject [3, 41. With this device, blood is continuously pumped out of the left ventricle into the aorta through a 21F inflow cannula that is positioned in the left ventricle across the aortic valve. Maximum flow of the pump depends on mean aortic pressure (MAP), and is relatively limited (approximately 3.5 L/min at an MAP of 60 mm Hg). These characteristics would make the effects of left ventricular assistance with this device different from those with other left ventricular assist devices. The purpose of the present study was to show the effects of
Accepted for publication Dec 13, 1991.
Presented in part at the Thirty-seventh Annual Meeting of the American Society for Artificial Internal Organs, Chicago, IL, April 25-27, 1991.
Address reprint requests to Dr Loisance, Centre de Recherches Chirurgi- cales CNRS, UA 1431, CHU Henri Mondor, 8, rue du General Sarrad, 94010 Creteil, France.
mum support were compared with those of minimum support. The effects of the Hemopump varied according to cardiac function. When cardiac dysfunction was mild, the Hemopump support slightly reduced myocardial 0, demand (assessed by pressure-work index) by volume unloading. When cardiac dysfunction was severe, total bypass was achieved and myocardial 0, demand de- creased by 45%, owing to both volume and pressure unloading. Coronary blood flow was incompletely auto- regulated, and the ratio of blood flow to 0, demand increased.
(Ann Thorac Surg 1992;53:1074-9)
Hemopump support on hemodynamics and coronary blood flow in the presence and absence of myocardial ischemia and failure.
Material and Methods
Animal Preparation Eight adult mongrel dogs weighing from 20 to 38 kg were anesthetized with intravenous pentobarbital (30 mg/kg), intubated, and mechanically ventilated with 60% oxygen. Anesthesia was maintained with 1% to 2% halothane. All animals received humane care in compliance with the ”Guide for the Care and Use of Laboratory Animals” published by the National Institutes of Health (NIH publication No. 85-23, revised 1985).
A Swan-Ganz catheter was placed through the left jugular vein. A left thoracotomy and a median laparotomy were performed. A microtip pressure catheter (Millar PC-350; Millar Instruments, Inc, Houston, TX) connected to a control unit (Millar TC-100) was placed in the left ventricle through the left atrium. Heparin was adminis- tered intravenously (1 mg/kg). Under fluoroscopic guid- ance, the Hemopump was introduced into the left ventri- cle through a transversal arteriotomy of the infrarenal abdominal aorta. It was the same device as that for human use. A 3F intracoronary Doppler catheter (NuVel 7891; NuMed, Inc, Hopkinton, NY) for coronary blood flow velocity (CBFV) assessment was positioned in the left circumflex coronary artery through a 9F Judkins guiding catheter introduced through a puncture of the abdominal aorta. After the Doppler catheter was positioned, the guiding catheter was withdrawn from the coronary os- tium. The Doppler catheter was connected to a 20-MHz
0 1992 by The Society of Thoracic Surgeons 0003-4975/92/$5.00
Ann Thorac Surg 1992;53:1074-9
SHllYA ET AL 1075 HEMODYNAMICS DURING HEMOPUMP SUPPORT
TCO (Ilmin)
6
5
4
3
2
1
0
SVR (dynrs.ssclcm5)
4Ooo
3ooo
2000
lo00
0
* T
rn co H W
* : p<0.05 **: PGO.01
* * n
- HP1 HP7 HP1 HP7 HP1 HP7 NORMAL ISCHEMIA FAILURE
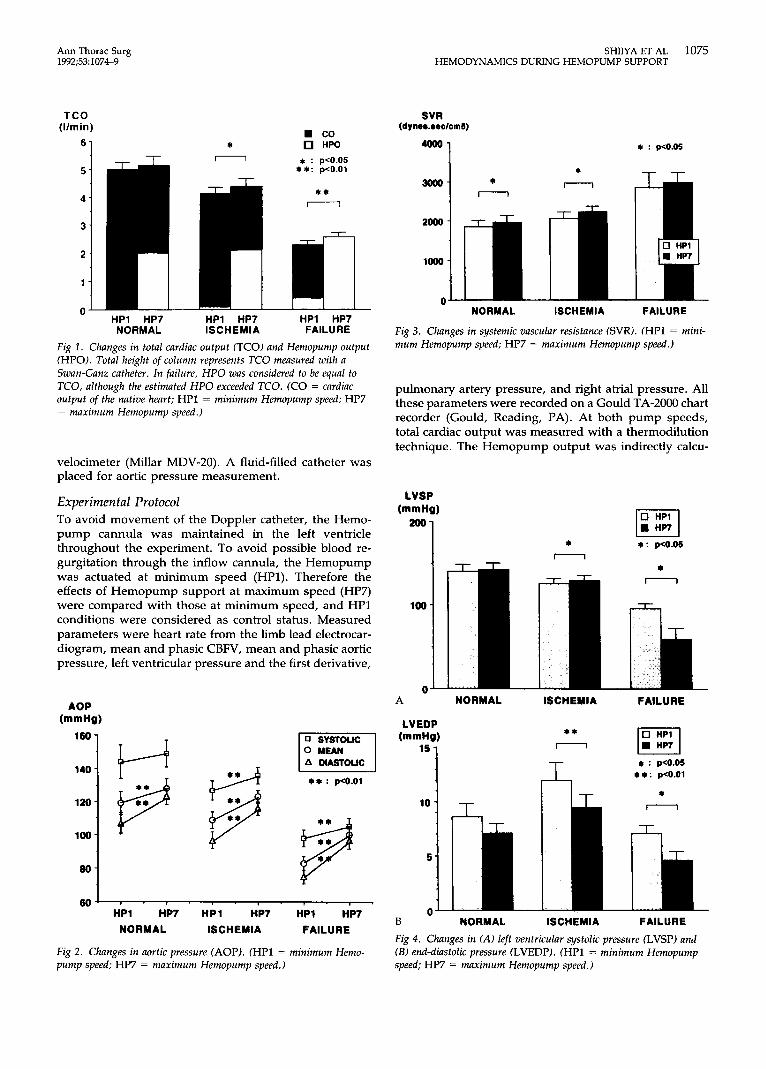
Fig 1. Changes in total cardiac output (TCO) and Hemopump output (HPO). Total height of column represents TCO measured with a Swan-Ganz catheter. In failure, HPO was considered to be equal to K O , although the estimated HPO exceeded TCO. (CO = cardiac output of the native heart; HPl = minimum Hemopump speed; HP7 = maximum Hemopump speed.)
velocimeter (Millar MDV-20). A fluid-filled catheter was placed for aortic pressure measurement.
Experimental Protocol To avoid movement of the Doppler catheter, the Hemo- pump cannula was maintained in the left ventricle throughout the experiment. To avoid possible blood re- gurgitation through the inflow cannula, the Hemopump was actuated at minimum speed (HP1). Therefore the effects of Hemopump support at maximum speed (HP7) were compared with those at minimum speed, and HP1 conditions were considered as control status. Measured parameters were heart rate from the limb lead electrocar- diogram, mean and phasic CBFV, mean and phasic aortic pressure, left ventricular pressure and the first derivative,
-1 HP1 HP7 HP1 HP7 HP1 HP7
NORMAL ISCHEMIA FAILURE
Fig 2. Changes in aortic pressure (AOP). CHPl = minimum Hemo- pump speed; HP7 = maximum Hemopump speed.)
* n
* : pco.05
+ T T
NORMAL ISCHEMIA FAILURE
Fig 3. Changes in systemic vascular resistance (SVR). (HPl = mini- mum Hemopump speed; HP7 = maximum Hemopump speed.)
pulmonary artery pressure, and right atrial pressure. All these parameters were recorded on a Gould TA-2000 chart recorder (Gould, Reading, PA). At both pump speeds, total cardiac output was measured with a thermodilution technique. The Hemopump output was indirectly calcu-
* a: p<0.05
n
100
0 - FAILURE A NORMAL ISCHEMIA
LVEDP ** n Fl
+ : p<0.05 *+: p<0.01
* n 10 -
5 -
0 - B NORMAL ISCHEMIA FAILURE
Fig 4. Changes in (A) left ventricular systolic pressure (LVSP) and (B) end-diastolic pressure (LVEDP). (HPl = minimum Hernopump speed; HP7 = maximum Hemopump speed.)

1076 SHIIYA ET AL HEMODYNAMICS DURING HEMOPUMP SUPPORT
Ann Thorac Surg 1992;53:1074-9
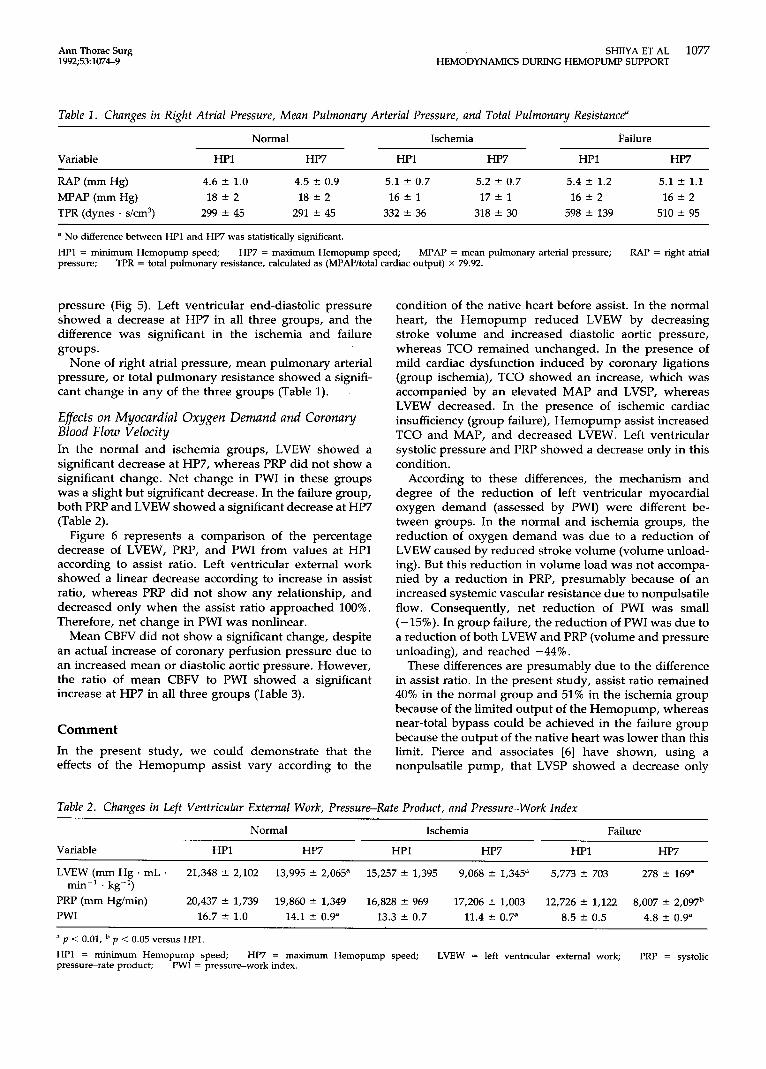
Fig 5 . A representative tracing of electrocardiogram m-w 1 (fCG), coronary blood flow v e l o h y (CBFV), aortic
EcG .LLL\L --\<\, p pressure (AOP), left ventricular pressure (LVP), and its first derivative in 1 dog. Total cardiac output was 2 53 Llmin at HPl A t HP7, AOP increased and separated from LVP, which showed a dramatic de- crease. A brief period of increase in CBFV at the mo- ment of change of pump speed preceded the steady state. (HP1 = minimum Hernopuma speed; HP7 =
8 . I
maximum Hemopump speed.)
L
lated by a computerized algorhythm console of the con- sole itself as a function of MAP.
After the measurements for normal heart were com- pleted, the left anterior descending coronary artery after the first diagonal branch was ligated and measurements were repeated. Then ligations of all the visible diagonal branches were added, and measurements were repeated. In 3 dogs, additional measurements were made after further ligations of the proximal left anterior descending coronary artery (all 3 dogs) and, subsequently, a few proximal marginal branches (2 of 3 dogs). Thus three to five pairs of measurements were made for each dog. Before each coronary ligation, 2 mg/kg of lidocaine was administered intravenously. The interval between coro- nary ligation and measurements was 10 minutes.
Data Analysis Left ventricular pressure-work index (PWI) according to Rooke and Feigl [5] was used to assess the change in left ventricular myocardial oxygen demand. Their original formula was modified to make it match the experimental condition :
MVO2 = KI(LVSP X HR) + K,[(LVSP - 0.2PP)
X (TCO - HPO)/BW] + K3
where MVO, is left ventricular myocardial oxygen con- sumption (mL 0, * min-' * 100 g-'), LVSP is left ventric- ular systolic pressure (mm Hg), HR is heart rate (beats/ min), PP is pulse pressure (mm Hg), TCO is total cardiac output (mL/min) measured by thermodilution technique, HPO is Hemopump output (mL/min), and BW is body weight (kg). The coefficients are: K, = 4.08 x lop4, K, = 3.25 x K3 = 1.43. We also analyzed the two essential components of PWI independently, namely, systolic pres- sure rate product (PRP = LVSP x HR) and left ventricular external work (LVEW = (LVSP - 0.2PP) x (TCO - HPO)/BW).
Statistics The data were expressed as mean 2 standard error of the mean. Statistical analyses were performed with Student's paired t test between data at HP1 and those at HP7. Values of p less than 0.05 were considered to be signifi- cant.
+I&
i--.-----.-
Results Total cardiac output in the control condition was 4.99 5 0.25 L/min in normal hearts (group normal), 3.86 f 0.45 L/min after ligation of the LAD, 3.29 f 0.44 Urnin after ligations of the diagonal branches, and 3.33 f 0.39 L/min after further ligations. Because the effect of each coronary ligation on TCO varied considerably among individual dogs, we divided the data after coronary liga- tion into two groups according to TCO: those in which TCO was greater than 2.99 L/min (ischemia group) and those in which TCO was less than 2.99 L/min (failure group). The borderline value was decided as the mean minus 3 times the standard deviation (lower limit of 99% confidence area) of TCO in normal hearts. As a result, 14 pairs of measurements in 7 dogs were included in the ischemia group and 7 pairs of measurements in 6 dogs were included in the failure group. Total cardiac output at HP1 was 4.13 f 0.23 L/min in the ischemia group and 2.28 f 0.16 L/min in the failure group.
Effects on Hernodynamics Support at HP7 resulted in a significant increase in TCO in the ischemia and failure groups, whereas no significant change was seen in the normal group. The contribution of Hemopump output to TCO (assist ratio) at HP7 was 40% f 3% in the normal group and 51% 2 4% in the ischemia group. In the failure group, this ratio was 104% f 6%; it was more than 87% in an individual dog (Fig 1).
Mean aortic pressure showed a significant increase in all three groups at HP7. This increase was due to an increase of diastolic blood pressure in the normal group, whereas both systolic and diastolic pressures showed a significant increase in the ischemia and failure groups (Fig 2).
Systemic vascular resistance showed an increase at HP7 in all three groups, and the difference was significant in the normal and ischemia groups (Fig 3).
Figure 4 shows the change in left ventricular pressures. Left ventricular systolic pressure did not show a signifi- cant change in the normal group, whereas it showed a significant increase at HP7 in the ischemia group. These changes corresponded to the changes in systolic blood pressure. By contrast, LVSP in the failure group showed a dramatic decrease at HP7, and separated from aortic
Ann Thorac Surg 1992;53 1074-9
SHIIYA ET AL 1077 HEMODYNAMICS DURING HEMOPUMP SUPPORT
Table 1. Changes in Right Atrial Pressure, Mean Pulmonary Arterial Pressure, and Total Pulmonary Resistance"
Variable
Normal Ischemia Failure
HPl HP7 HPl HP7 HPI HP7
5.1 f 1.1 MPAP (mm Hg) 18 f 2 18 f 2 16 f 1 17 f 1 16 f 2 16 f 2 TPR (dynes . s/cm3) 299 f 45 291 f 45 332 f 36 318 f 30 598 f 139 510 f 95
RAP (mm Hg) 4.6 f 1.0 4.5 f 0.9 5.1 2 0.7 5.2 2 0.7 5.4 f 1.2
a No difference between HP1 and HP7 was statistically significant.
HP1 = minimum Hemopump speed; pressure;
HP7 = maximum Hemopump speed; MPAP = mean pulmonary arterial pressure; RAP = right atrial TPR = total pulmonary resistance, calculated as (MPAP/total cardiac output) x 79.92.
pressure (Fig 5). Left ventricular end-diastolic pressure showed a decrease at HP7 in all three groups, and the difference was significant in the ischemia and failure groups.
None of right atrial pressure, mean pulmonary arterial pressure, or total pulmonary resistance showed a signifi- cant change in any of the three groups (Table 1).
Effects on Myocardial Oxygen Demand and Coronary Blood Flow Velocity In the normal and ischemia groups, LVEW showed a significant decrease at HP7, whereas PRP did not show a significant change. Net change in PWI in these groups was a slight but significant decrease. In the failure group, both PRP and LVEW showed a significant decrease at HP7 (Table 2).
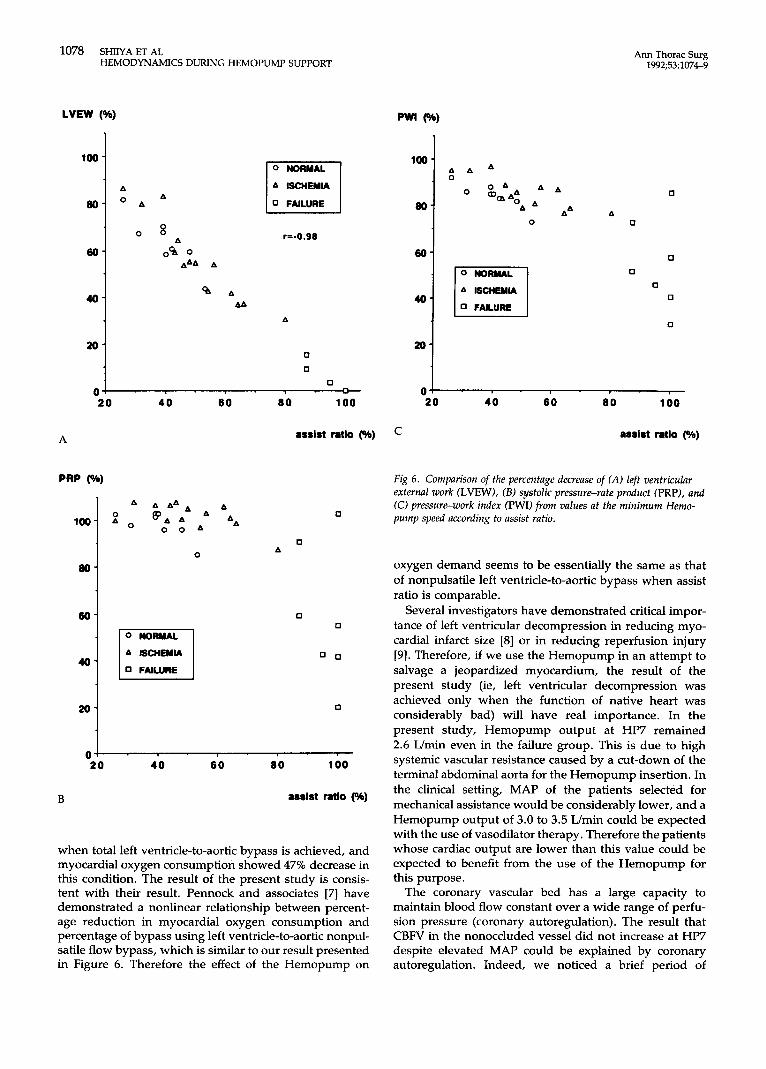
Figure 6 represents a comparison of the percentage decrease of LVEW, PRP, and PWI from values at HP1 according to assist ratio. Left ventricular external work showed a linear decrease according to increase in assist ratio, whereas PRP did not show any relationship, and decreased only when the assist ratio approached 100%. Therefore, net change in PWI was nonlinear.
Mean CBFV did not show a significant change, despite an actual increase of coronary perfusion pressure due to an increased mean or diastolic aortic pressure. However, the ratio of mean CBFV to PWI showed a significant increase at HP7 in all three groups (Table 3).
Comment In the present study, we could demonstrate that the effects of the Hemopump assist vary according to the
condition of the native heart before assist. In the normal heart, the Hemopump reduced LVEW by decreasing stroke volume and increased diastolic aortic pressure, whereas TCO remained unchanged. In the presence of mild cardiac dysfunction induced by coronary ligations (group ischemia), TCO showed an increase, which was accompanied by an elevated MAP and LVSP, whereas LVEW decreased. In the presence of ischemic cardiac insufficiency (group failure), Hemopump assist increased TCO and MAP, and decreased LVEW. Left ventricular systolic pressure and PRP showed a decrease only in this condition.
According to these differences, the mechanism and degree of the reduction of left ventricular myocardial oxygen demand (assessed by PWI) were different be- tween groups. In the normal and ischemia groups, the reduction of oxygen demand was due to a reduction of LVEW caused by reduced stroke volume (volume unload- ing). But this reduction in volume load was not accompa- nied by a reduction in PRP, presumably because of an increased systemic vascular resistance due to nonpulsatile flow. Consequently, net reduction of PWI was small (-15%). In group failure, the reduction of PWI was due to a reduction of both LVEW and PRP (volume and pressure unloading), and reached -44%.
These differences are presumably due to the difference in assist ratio. In the present study, assist ratio remained 40% in the normal group and 51% in the ischemia group because of the limited output of the Hemopump, whereas near-total bypass could be achieved in the failure group because the output of the native heart was lower than this limit. Pierce and associates [6] have shown, using a nonpulsatile pump, that LVSP showed a decrease only
Table 2. Changes in Left Ventricular External Work, Pressure-Rate Product, and Pressure-Work Index
Variable
Normal Ischemia Failure
HP1 HP7 HPI HP7 HP1 HP7
LVEW (mm Hg . mL . 21,348 f 2,102 13,995 2 2,065" 15,257 2 1,395 9,068 f 1,345a 5,773 f 703 278 2 169"
PRP (mm Hg/min) 20,437 f 1,739 19,860 2 1,349 16,828 2 969 17,206 f 1,003 12,726 f 1,122 8,007 2 2,097b PWI 16.7 2 1.0 14.1 2 0.9" 13.3 2 0.7 11.4 2 0.7" 8.5 f 0.5 4.8 f 0.9"
a p < 0.01,
HPl = minimum Hemopump speed; pressure-rate product;
min-' . kg-')
p < 0.05 versus HPI.
HP7 = maximum Hemopump speed; LVEW = left ventricular external work; PRP = systolic PWI = pressure-work index.
1078 SHIIYA ET AL HEMODYNAMICS DURING HEMOPUMP SUPPORT
40-
20-
LVEW (%)
% A AA
A
0
0
Ann Thorac Surg 1992;53:1074-9
40-
20-
A ISCHEMIA
r=-0.90
% A AA
A
0
0
0 0 -
100
a
60
40
20
0
B
A A A A A A A
P o 'AA AA 0 0 1
0
A ISCHEMIA
0 FAILURE
80 100
assist ratio (%)
0
0 A
0 0
0 0
0
40 60 80 100
assist ratio (%)
when total left ventricle-to-aortic bypass is achieved, and myocardial oxygen consumption showed 47% decrease in this condition. The result of the present study is consis- tent with their result. Pennock and associates [7] have demonstrated a nonlinear relationship between percent- age reduction in myocardial oxygen consumption and percentage of bypass using left ventricle-to-aortic nonpul- satile flow bypass, which is similar to our result presented in Figure 6. Therefore the effect of the Hemopump on
rw
80
60
40
20
0
A A A
A& A
A SCHEYIA
0 FAILURE
0
0 0
0
0
0
0
0
- 20 40 6 0 80 100
assist ratio (%) C
Fig 6 . Comparison of the percentage decrease of (A) left ventricular external work (LVEW), ( B ) systolic pressure-rate product (PRP), and (0 pressure-work index (PWI) from values at the minimum Hemo- pump speed according to assist ratio.
oxygen demand seems to be essentially the same as that of nonpulsatile left ventricle-to-aortic bypass when assist ratio is comparable.
Several investigators have demonstrated critical impor- tance of left ventricular decompression in reducing myo- cardial infarct size [8] or in reducing reperfusion injury [9] . Therefore, if we use the Hemopump in an attempt to salvage a jeopardized myocardium, the result of the present study (ie, left ventricular decompression was achieved only when the function of native heart was considerably bad) will have real importance. In the present study, Hemopump output at HP7 remained 2.6 L/min even in the failure group. This is due to high systemic vascular resistance caused by a cut-down of the terminal abdominal aorta for the Hemopump insertion. In the clinical setting, MAP of the patients selected for mechanical assistance would be considerably lower, and a Hemopump output of 3.0 to 3.5 Umin could be expected with the use of vasodilator therapy. Therefore the patients whose cardiac output are lower than this value could be expected to benefit from the use of the Hemopump for this purpose.
The coronary vascular bed has a large capacity to maintain blood flow constant over a wide range of perfu- sion pressure (coronary autoregulation). The result that CBFV in the nonoccluded vessel did not increase at HP7 despite elevated MAP could be explained by coronary autoregulation. Indeed, we noticed a brief period of

Ann Thorac Surg 1992;53: 1074-9
SHIIYA ET AL 1079 HEMODYNAMICS DURING HEMOPUMP SUPPORT
Table 3. Changes in Mean Coronary Blood Flow Velocity and Ratio of Coronary Blood Flow Velocity to Pressure-Work lndex
Normal Ischemia Failure
Variable HPI HP7 HPI HP7 HP1 HP7
CBFV (cds) 15.1 2 1.9 14.5 2 1.8 14.7 f 1.7 14.6 2 1.6 10.2 * 1.5 9.3 f 1.3 CBFVPWI 0.93 f 0.15 1.07 f 0.17" 1.13 f 0.12 1.31 2 0.14b 1.20 2 0.16 1.99 f 0.31"
a p < 0.05, CBFV = mean coronary blood flow velocity; index.
p < 0.01 versus HPI. HPl = minimum Hemopump speed; HP7 = maximum Hemopump speed; PWI = pressure-work
increase in CBFV at the moment of change of pump speed that preceded the steady state at lower CBFV, both in the present study and in the clinical study [4]. Merhige and associates [3] have shown, using tracer microspheres, decreased myocardial perfusion in the nonischemic area that correlates with reduced fractional shortening caused by Hemopump support. However, the blood flow/O, demand ratio (mean CBFV/PWI) showed an increase in the present study, which means that autoregulation was not perfect. Because oxygen consumption is given by the product of blood flow and oxygen extraction, this increase should be accompanied by a reduction in oxygen extrac- tion. Dole and Nuno [lo] have demonstrated that reduc- tion of myocardial oxygen consumption attenuates coro- nary autoregulation. They have concluded that when myocardial oxygen tension is higher than 32 mm Hg, the degree of coronary autoregulation decreases, and an increase in coronary perfusion pressure results in an increase in myocardial blood flow and a decrease in oxygen extraction. The result of the present study is consistent with their result.
Criticism of the Methods In the present study, we used the PWI of Rooke and Feigl [5] as an index of myocardial oxygen demand. We chose it because it can represent mechanical energy expended for performing external work and maintaining pressure at end-systole, and it does not require the measurement of ventricular volume. An increase in stroke volume with no change in LVSP and HR has been demonstrated to result in an increase in myocardial oxygen consumption [5]. Because similar change could be obtained with left ven- tricular assistance, use of the index that involves stroke volume is essential. Other indexes that involve an integral over time can account for the oxygen cost of stroke volume, because large stroke volumes are associated with long systolic periods. However, the change in contractility can also change duration of systole. The PWI has been demonstrated to be much less dependent on catechola- mine-induced changes in contractility [5].
The application of the PWI to damaged heart remains to be validated, because the damaged heart would certainly have an increased basal metabolic demand. Nevertheless, we believe that use of this index in heart failure is not inappropriate in the sense that the PWI represents total mechanical energy expended by left ventricle.
Conclusion The results of the present study suggest that: (1) the effects of Hemopump support vary according to the function of the native heart, (2) when cardiac dysfunction is mild, Hemopump support slightly reduces myocardial oxygen demand by volume unloading, (3) when cardiac dysfunction is severe and total bypass is achieved, He- mopump support decompresses the left ventricle and decreases myocardial oxygen demand by 45%, by both volume and pressure unloading, and (4) coronary blood flow in the nonoccluded vessel is incompletely autoregu- lated, and the ratio of blood flow to oxygen demand increases under Hemopump support.
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Frazier OH, Wampler RK, Duncan JM, et al. First human use of the Hemopump, a catheter-mounted ventricular assist device. Ann Thorac Surg 1990;49:299304. Loisance D, Dubois-Rande JL, Deleuze PH, Okude J, Rosen- Val H, Geschwind H. Prophylactic intraventricular pumping in high risk coronary angioplasty. Lancet 1990;335:438-40. Merhige ME, Smalling RW, Cassidy D, et al. Effect of the Hemopump left ventricular assist device on regional myocar- dial perfusion and function. Reduction of ischemia during coronary occlusion. Circulation 1989;8O(Suppl 3):158-66. Dubois-Rande JL, Zelinsky R, Deleuze P, Geschwind H, Loisance D. Coronary hemodynamics during Hemopump left intraventricular assistance [Abstract]. Circulation 1990; 82(Suppl 3):680. Rooke GA, Feigl €0. Work as a correlate of canine left ventricular oxygen consumption, and the problem of cate- cholamine oxygen wasting. Circ Res 1982;50:273-86. Pierce WS, Aaronson A€, Prophet GA, Williams DR, Wald- hausen JA. Hemodynamic and metabolic studies during two types of left ventricular bypass. Surg Forum 1972;23:176-8. Pennock JL, Pierce WS, Waldhausen JA. Quantitative evalu- ation of left ventricular bypass in reducing myocardial isch- emia. Surgery 1976;79:52%33. Pennock JL, Pae WE, Pierce WS, Waldhausen JA. Reduction of myocardial infarct size: comparison between left atrial and left ventricular bypass. Circulation 1979;59:275-9. Allen BS, Okamoto F, Buckberg GD, Bugyi H, Leaf J. Studies of controlled reperfusion after ischemia: 13. Reperfusion conditions: critical importance of total ventricular decom- pression during regional reperfusion. J Thorac Cardiovasc Surg 1986;92:605-12. Dole WP, Nuno DW. Myocardial oxygen tension determines the degree and pressure range of coronary autoregulation. Circ Res 1986;59:202-15.