Embed Size (px)
Citation preview
Changing Health Changing Health Care Provider Care Provider
Performance: Performance: the the role of effective CME role of effective CME
& CPD& CPD
National Coalition for HP National Coalition for HP Education in GeneticsEducation in Genetics, ,
September 2011September 2011Dave Davis, MDDave Davis, MD
Senior Director, Continuing Education and ImprovementSenior Director, Continuing Education and Improvement
Association of American Medical CollegesAssociation of American Medical Colleges
invisible
invisible
1. What are CME and CPD? Why are they ‘invisible’?
2. The ‘Does CME Work?’ question: the in- vitro perspective
3. Does CME work in the real world? - a look at the in-vivo, clinical care gap and its relationship to the world of genetics education
4. So What? Recommendations to a thoughtful genetics audience: guidelines for the use of CME & CPD
An outline: many questions, little time…
Question #1Question #1Some definitions:
•What do we mean by CME & CPD?
•….by the terms diffusion, implementation?
•….how have we changed in our thinking?
•Later….what is knowledge translation/implementation science?
What do we mean by ‘CPD and CME’?
• educational materials
• formal CME: lectures, small groups, courses
• outreach visits
• opinion leaders
• patient-mediated strategies
• audit/feedback
• reminders (paper, computerized,
interactive, etc)
• comprehensive, QI- or practice-based interventions
• web-based tools, PDAs
(borrowed from EPOC, Cochrane Collaboraitve)
How have we changed…?
Diffusion: distribution of information and the practitioners’ natural unaided adoption of policies and practices
Dissemination: communication of information to clinicians to improve their skills
Implementation: putting a guideline in place, involves effective communication, overcomes barriers by administrative and educational techniques
(after Lomas)...
What do we mean by…?
Question # 2Question # 2“Does CME (CPD) Work?”
The In Vitro Question
(The Sackett question)
Database of Physician Education & Change: www.rdrb.utoronto.ca
The Research and Development Resource Base
- educational, clinical & health services literature
• supported by the
American medical Association, the North American CME organizations, Royal College of Physicians and Surgeons of Canada, the University of Toronto and the Association of American colleges
Now ~25,000 studies

• 12 metropolitan areas, roughly 30 conditions studied, >6,000 patient records examined
• Substandard care noted in 45% of clinical areas (of this, 46% underuse; 11% overuse)
• Little variation by region or by type of condition (chronic, acute), socioeconomic status
• Notable gaps in care in depression, alcohol abuse, diabetes care (about 45%), pneumonia (39%);
• Better care (>50% compliance with recommendations) noted in hypertension, cardiac care, but just
•NOTE: the inviible care gap (undiagnosed, undetected – e.g., smoking cessation, obesity counseling, care gap is HUGE)
www.rdrb.utoronto.cawww.rdrb.utoronto.cawww.rdrb.utoronto.ca
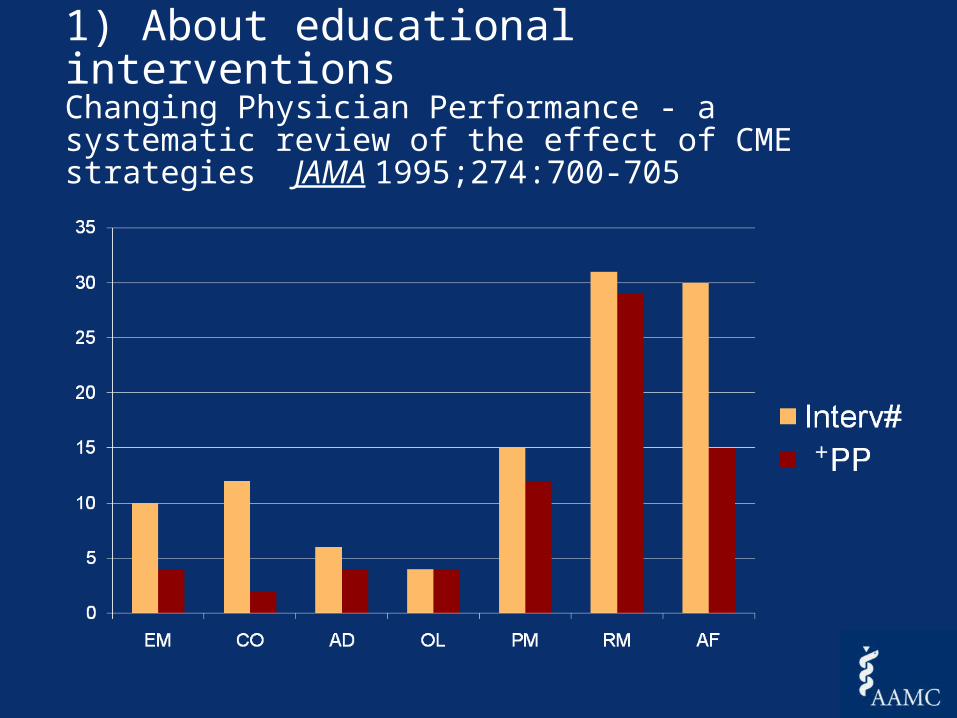
1) About educational interventionsChanging Physician Performance - a systematic review of the effect of CME strategies JAMA 1995;274:700-705
+
Effective• *Interactive Lecturing• *Sequenced Sessions• Accurate needs assessment• Successful education has
three elements – predisposing, enabling, reinforcing
Not so EffectiveDidactic TeachingOne-time only
sessions
The effect of formal CME - conferences, symposia, rounds, meetings, lectures
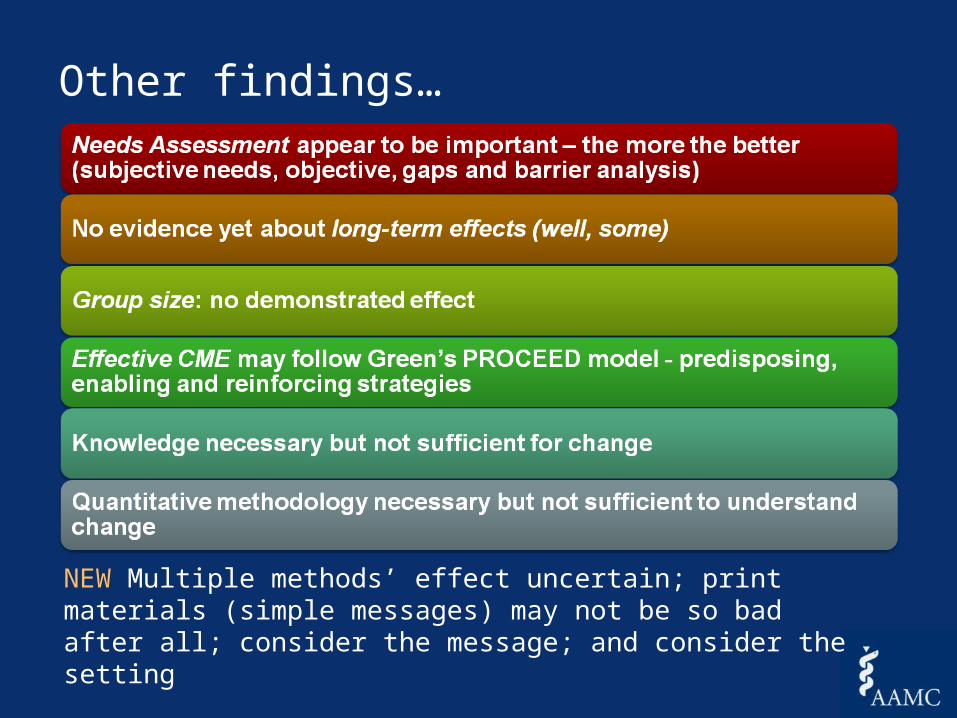
Other findings…
NEW Multiple methods’ effect uncertain; print materials (simple messages) may not be so bad after all; consider the message; and consider the setting
• age
• motivation
• (dis)incentives
• experience
• time
• environment
• training• Emphasis on knowledge• Inability to detect needs,
evaluate performance• ?self-directed learning• ?critical appraisal
The Pathman Model• awareness: of a guideline,
practice innovation, change
• agreement: with the innovation or guideline
• adoption: ‘trying out’ the new practice, irregularly
• adherence: abiding by the new practice on all appropriate occasions Pathman, 1996
2) and about the learner-clinician
The self-assessment question
Davis & co., Davis & co., JAMA JAMA 2006;296:1096-11022006;296:1096-1102
Of 20 comparisons…..
13 demonstrated little, no or an inverse relationship between self and external assessment:• Examples: learning needs, EBM skills, simulated knee
injections• Note: inverse relationships between confidence noted
by Leopold (knee injections), Fox (OSCE misperception) and Parker (knowledge-based FP exam)
7 demonstrated a positive relationship:
• Examples: cultural-linguistic competencies, global performance with dementia patients, comfort with psycho-social issues in family medicine
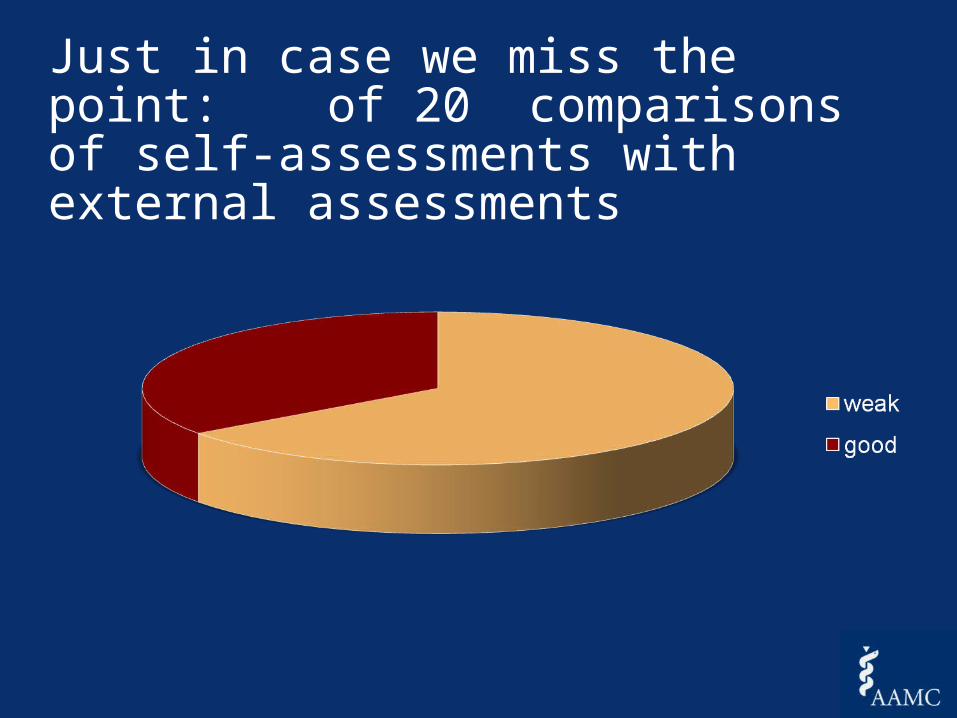
Just in case we miss the point: of 20 comparisons of self-assessments with external assessments
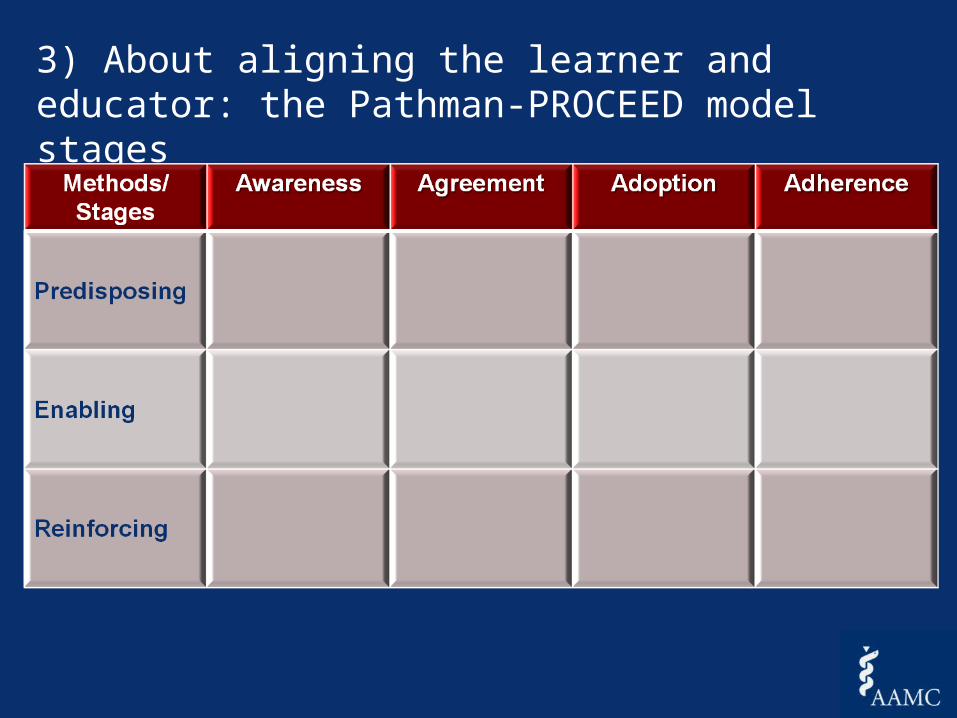
3) About aligning the learner and educator: the Pathman-PROCEED model stages
““Despite the quality of the evidence of CME, it
Despite the quality of the evidence of CME, it
appears to be effective in the acquisition and
appears to be effective in the acquisition and
retention of knowledge, skills, behaviors, and clinical
retention of knowledge, skills, behaviors, and clinical
outcomes” outcomes” AHRQ EB report, Feb 2007
AHRQ EB report, Feb 2007
ACCP, CHEST, 2009
ACCP, CHEST, 2009
3) About the 3) About the cumulative effect of cumulative effect of CCME/CPDCCME/CPD
Does CME/CPD work in the real Does CME/CPD work in the real world? In the world of effectiveness? world? In the world of effectiveness? Why or why not? Why or why not?
The In Vivo Questions The In Vivo Questions
The Clinical Care GapThe Clinical Care Gap
• Overuse
• Underuse
• MisuseChassin, 1998
Question # 3:Question # 3:
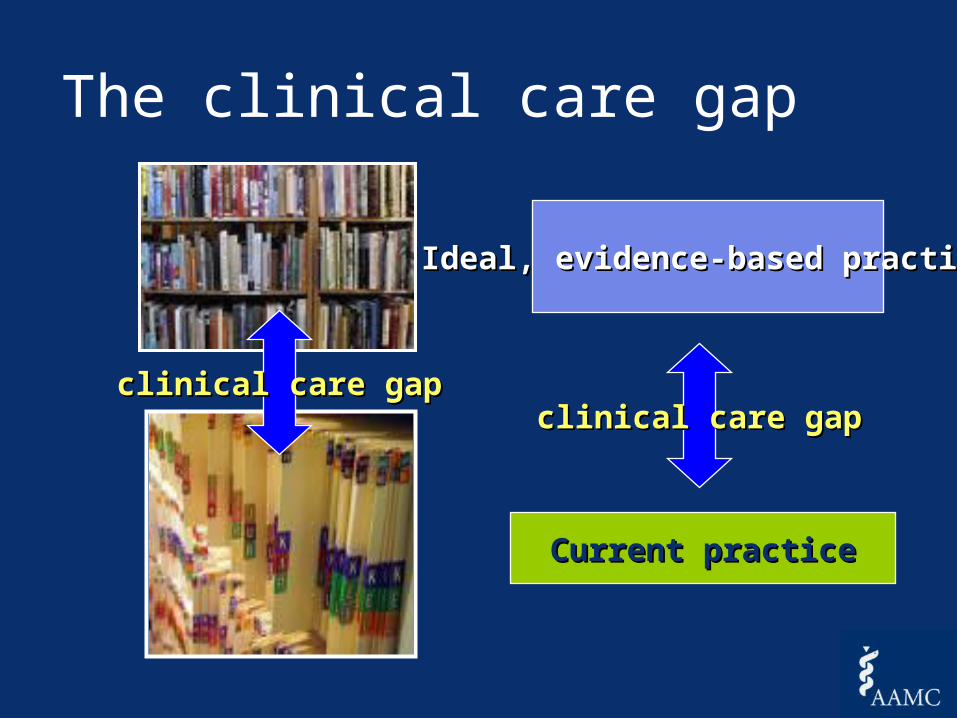
Current practiceCurrent practice
Ideal, evidence-based practiceIdeal, evidence-based practice
clinical care gapclinical care gap
The clinical care gap
clinical care gapclinical care gap
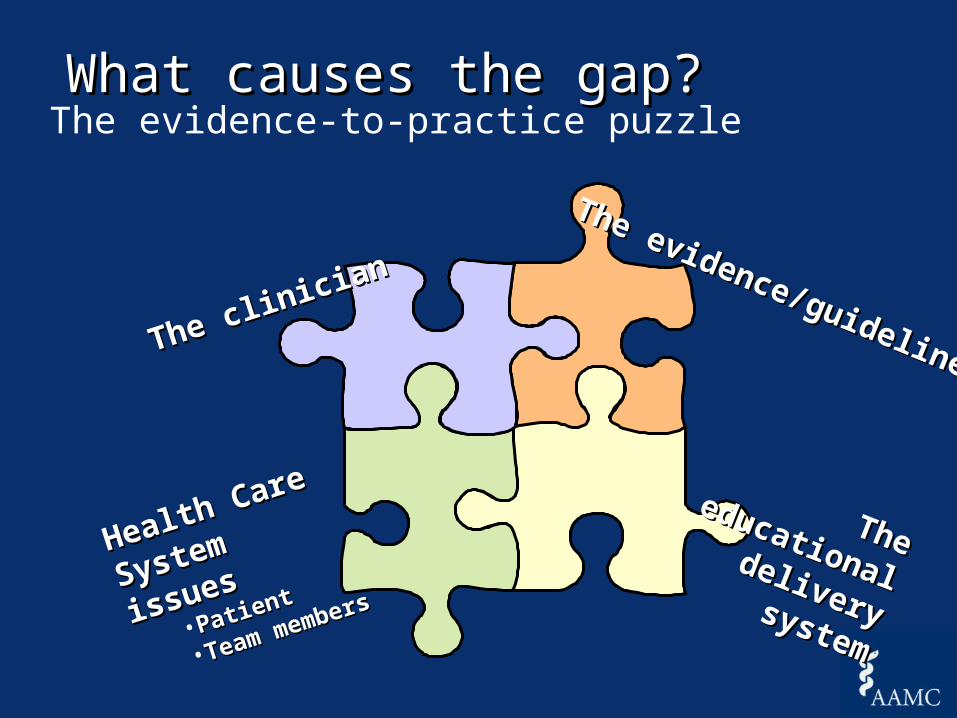
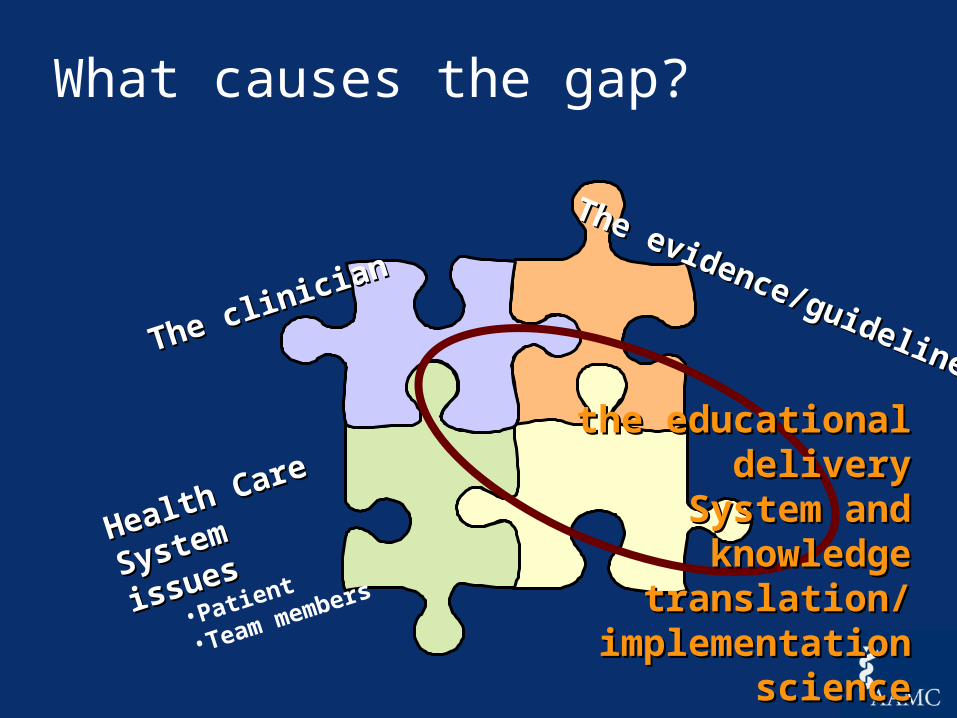
What causes the gap?What causes the gap? The evidence-to-practice puzzle
The educational
The educational deliverydeliverysystemsystem
The clinician
The clinician
The evidence/guideline
The evidence/guideline
Health Care
Health Care
System issues
System issues
•PatientPatient
•Team members
Team members
No time…No, Thursday’s out. How about never-is never good for you?
““Information management is Information management is like having your mouth to a like having your mouth to a
firehose”firehose”
David Naylor, President, University of TorontoDavid Naylor, President, University of Toronto
What causes the gap?
The clinician
The clinician
The evidence/guideline
The evidence/guideline
Health Care
Health Care
System issues
System issues
•Patient
•Team members
the educational the educational deliverydelivery
System and knowledge System and knowledge translation/ translation/
implementation scienceimplementation science
“Knowledge translation is the effective and timely incorporation of evidence-based information into the practices of health professionals in such a way as to effect optimal health care outcomes and maximize the potential of the health system”
– Adapted from the Canadian Institutes for Health Research definition, 2001
Implementation Science is the scientific study of methods to promote the systematic uptake of research findings and other evidence based practice into routine practice thus to improve the quality and effectiveness of health care and services. ..adapted from the NIH, USA
An emerging field; one concept, two terms
Question #4: Question #4: How do CME and CPD play a role in How do CME and CPD play a role in genetics & genetics education genetics & genetics education ?
The guideline process: evidence-to-action
The goal: effective
implementation
Evidence/message
Evidence/message
Development
DevelopmentImplementation
Implementation
Effective CME/PD
‘‘Consideration of clinician learning style, needs
Recommendation #1:
Guideline Development/adaptation
Consider CME/CPD in any evidence development process: from learner and educational perspectives (for example, guard against knowledge overload, consider already-held knowledge)
a.secure buy-in; involve the end-user in guideline development/adaptation
b.employ adult learning principles in guideline statements (format, spacing, language)
c. consider recommending effective educational strategies in the guideline itself
How an we use CME/CPD in evidence/message/guideline development in genetics?
• compatibility• complexity• cost• relative advantage• accessibility• format• patency of evidence, process of development• opportunity; trial-ability
…….educational issues to consider .educational issues to consider within the guideline, evidence itselfwithin the guideline, evidence itself
• Joint body of the Ontario Medical Association and the Ministry of Health and Long term Care, Ontario
• Chooses a topic area; reviews all guidelines in that area; scores them by the Cluzeau/AGREE instrument
• Mounted them on a website
– Quick, 30 second synopsis– Clear language– Appropriate format– Parallel patient synopsis– The apple-score
One attempt to fix the Message:The Guidelines Advisory Committee, Ontario (now the Center for Evidence-based practice)
Recommendation # 2:
Include CME/CPD in any guideline implementation strategy
a)Consider the learner- mode of current learning- stage of awareness-adherence at which clinician-learners exist
b) Consider effective educational strategies
How an we use CME/CPD in genetics education ?
Formal CMELectures, workshops, small groups
Informal education
Audit/Feedback
Reminders
Policy, CQI administrative techniques
Patient Strategies
Multiple Strategies
M&M conferences
Quality-based rounds
Journal Club
Team training
Handover/off rounds
The CPG implementation toolkit
Recommendation # 3:
Consider CME/CPD in a staged fashion, depending on stage of adoption of information, by individuals, groups; use appropriate educational strategies
How can we use CME/CPD in genetics education?
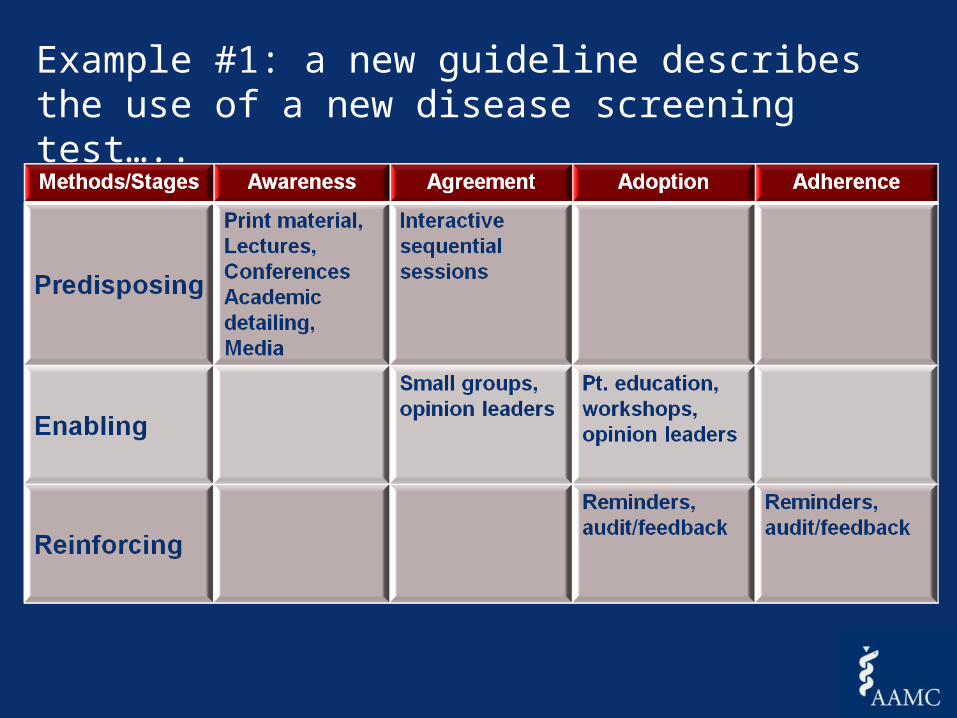
Example #1: a new guideline describes the use of a new disease screening test…..
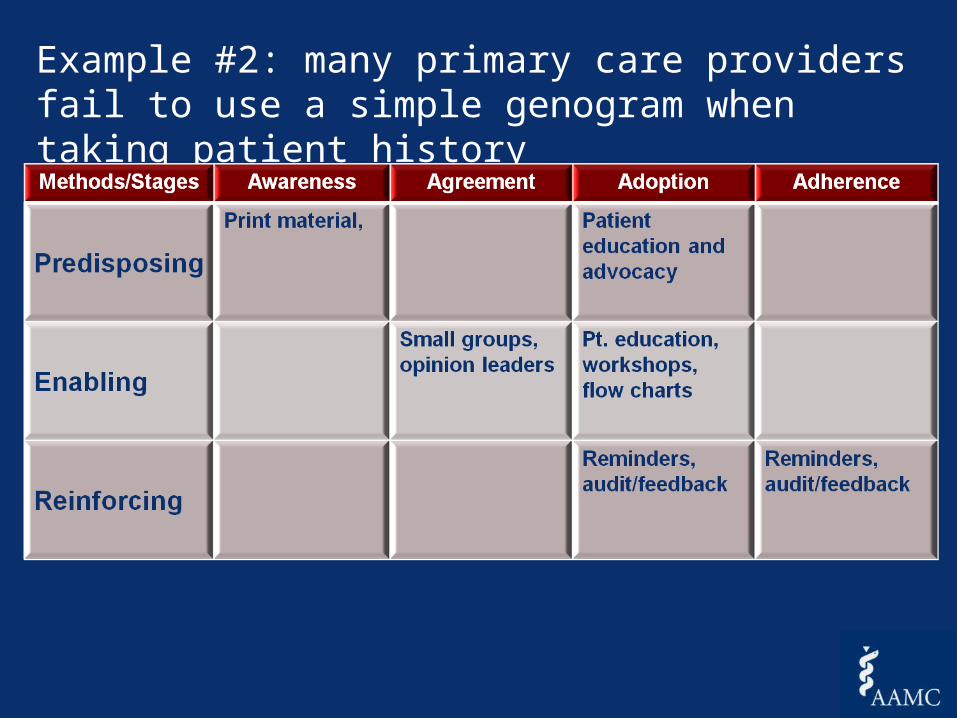
Example #2: many primary care providers fail to use a simple genogram when taking patient history
•Launch, June 2011
•Tools, resources, and support for AAMC members•Collaborative learning sessions•National Faculty Development Initiative•Roughly 250 med schools & teaching hospitals participating
Example #3: a national campaign: a project of the Association of American Medical Colleges
www.aamc.org/bestpractices
• Teach quality and patient safety to the next generation of doctors
• Ensure safer surgery through use of surgical checklists
• Reduce infections from central lines using proven protocols
• Reduce hospital readmissions for high-risk patients
• Research, evaluate, and share new and improved practices.
This list of commitments will grow over time.
Participating medical schools and teaching hospitals have committed to:
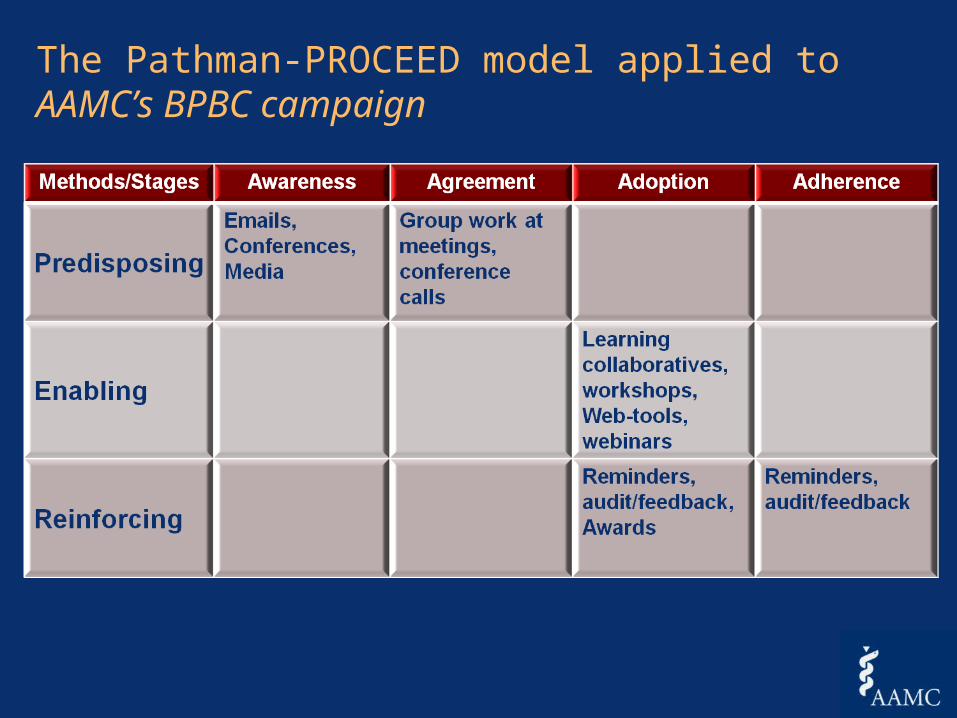
The Pathman-PROCEED model applied to AAMC’s BPBC campaign
• Large and growing body of evidence about the effect of CME/CPD now imbedded in models of change- no longer an invisible (and ineffective) intervention
• Huge clinical care gap, no less so in genetics
• Considerable support for consideration of CME/CPD practices and principles – based on best evidence.
And a few final last words
www.aamc.org/initiatives/CME/ae4Q
www.rdrb.utoronto.cawww.rdrb.utoronto.ca
Dave’s contact info: