Embed Size (px)
Citation preview

Hudson Harris, CIPMHarrisLogic, LLC
Changing the Health Paradigm: Social Navigation and Diversion in Criminal Justice and Healthcare
Karis Grounds
2-1-1 San Diego
Karla Samayoa
2-11 San Diego

Hudson Harris, CIPM
Chief Engagement Officer

The State of Mental Health

911/EMS/Police Jail
Connection Failure ED
Psychiatric HospitalMental Health Event
Mental Health Cycle

Mapping

Clinical
Data Integration
Predictive AnalyticsTechnical
Workflow
Business Intelligence
Project Considerations

Breaking the Cycle

911/EMS/Police Jail
Failure to Connect ED
Psychiatric HospitalMental Health Event
Stella Sequential Intercept
Diversion
Coordination Care
Community BasedWellness

What Happened

25%
100%
$30m
20%
Mental Health Diversion Program
Return on
Investment
Reduction in
Recidivism
Data Metrics
Over 5 Years
Reduction in
Average Daily
Jail Population
Net Revenue
for Program
4:15.5%
Reduction in
Higher Levels
Of Care Costs

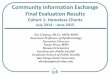
Emergency Department Diversions - Case StudyDallas, Texas from July 2017 Through June 2018
75% 78% 86% 87%
Baylor
Hospital
Methodist
Hospital
Sundance
Hospital
Dallas
Behavioral
Health
100%
75%
50%
0%
25%
Diversions From Higher Levels of Care
84%
13 Area
Hospitals
Regionwide Diversion RateSpread Across 17 Hospitals
82%
Hours Saved53,000
Reduction Bed
Days50%

What’s Next?



Social
Navigation
for Complex
Needs
Karis Grounds Vice President of
Health and
Community Impact
Karla SamayoaDirector of
Enrollment and
Navigation Services

Navigation
Information and
Assistance
Information and
Referrals

Food
Benefits and
Enrollment
Veterans
Courage to Call
Health
Health Navigation
Housing
Housing
Navigation

Transportation
Provider
Income and
benefits Provider
Food Provider Healthcare Provider
Person CenteredModel
Housing Provider

HOUSING STABILITY
FOOD &
NUTRITION
PRIMARY CARE &
PREVENTION
HEALTH MANAGEMENT
SOCIAL & COMMUNITY
CONNECTION
ACTIVITIES OF DAILY
LIVING
LEGAL & CRIMINAL
JUSTICE
FINANCIAL WELLNESS &
BENEFITS
TRANSPORTATION
PERSONAL CARE &
HOUSEHOLD GOODS
UTILITY & TECHNOLOGY
SAFETY & DISASTER
EDUCATION &
HUMAN DEVELOPMENT
EMPLOYMENT
DEVELOPMENT
14 S
ocia
l D
ete
rmin
an
ts o
f H
ea
lth
14 S
oc
ial D
ete
rmin
an
ts o
f
He
alth
/We
lln
ess

Wellness is directly impacted by:
• Poverty
• Health Inequities (Race, Ethnicity, Language)
• Adverse Childhood Events
• Environment
• Genetic Make-up

Risk Indicators:
• Medi-Cal/Unfunded/Underfunded
• Food Insecurity
• Multiple readmissions or ER utilization
• Lack of social supports

Bridging gaps between social and health services
Navigation for Social Needs:

Health Navigation
Shared Understanding: By addressing social needs, health outcomes and condition management will
improve for patient
Shared Goal: Support patients holistically through social and medical connections
Hospital’s Role: Identify at-risk patients with social determinants of health needs and directly refer to
Health Navigation for follow-up
2-1-1’s Role: 2-1-1 Health Navigators receive proactive patient referrals to assess and address risks
of social determinants of health by connecting to resources in the community.

Navigation Details
• Education: Bachelor’s and/or Master’s Degrees in related fields (i.e. psychology, sociology, social work, public health)
• Experience/backgrounds of Navigators: • Bilingual staff (Spanish and English)• Nonprofit organizations throughout San Diego that serve relevant populations (i.e. homeless individuals,
domestic violence victims) • Health education and wellness promotion• Patient advocacy and empowerment • Child welfare services, special education• Behavioral therapy for adults and children with developmental disabilities • Healthcare social work (i.e. skilled nursing facility) • Resource and referral
• Navigators work with clients between 60-100 days, on average (2-3 months)
• Monthly interdisciplinary team case conferences allow for collaboration, support, feedback, and to troubleshoot challenging clients/situations

Screening vs. Assessment
Priority: Providing Medical Care
Secondary: Screening for Specific Social Risks
Example:
• What is your housing situation?
• Have housing, I don’t have housing, I choose not
to answer
• What is the highest level of school that you have
finished?
• Less than high school degree, High school
diploma, more than high school, I choose not to
answer
Social Service Provider
Priority: Addressing complex and interrelated dynamics
Secondary: Accounts for relationship between health and social
Example:
• What is your current housing situation?
• Emergency Shelter, Long-Term Nursing Home, Motel,
Place not meant for human habitation, Safe Haven,
Couch Surfing, Mobile Home, Affordable Housing
• What are your barriers to receiving housing?
• Eviction, Credit History, Cost, Household Size, Issues with
Landlord, Home Repair, Incarceration, Unable to live
independently
• What resources have you access in the past?
• Emergency Shelters, Section 8 Housing, VI-SPDAT/CES,
Rapid Re-housing, HUD/VASH Voucher
Healthcare Provider

Social Determinant of Health
14 Question-Screening
If positive, RRS assessment
and care plan

Risk Rating Scale ToolRisk Rating Scale Tool

Improved Self-EfficacyMore confident in ability to
manage their health
8%
31%
36%
25%
Not Confident
SomewhatConfident
Confident
Very Confident
Reduction on
hospital
readmission
Decrease in
vulnerability risk
rating scaleClient SatisfactionHealth Plan Satisfaction
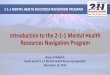
Evidence for Success

Patient Needs
(n =71)
CY 2016-2017:
• 92% decreased vulnerability
• 92% felt confident in the ability to
manage their health
22%
18%
4%
10%
7%
8%
4%
4%
2%
7%
7%
4%
1%
2%
0% 5% 10% 15% 20% 25%
Housing
Food and Nutrition
Utility and Technology
Transportation
Social Community Connection
Financial Wellness
Health Condition Management
Primary Care
Personal Hygiene HH Goods
Human Dev & Education
Employment
Legal
Disaster and Safety
Activities of Daily Living
9.6%
30.0%
211 Patients Comparison Group
Hospital Readmission Rates
Year 1: SDOH Outcomes

Anticipated ROI:• CTI program dramatically reduces preventable hospital readmissions for high-risk, vulnerable
patients
• Avoidable inpatient admissions ~ $17,564 per admission, and ER readmissions ~ $1,3871 ; higher
costs estimated for unfunded population
1Source: American Journal of Managed Care, 2011
Return on Investment

Clinical-CommunityPartnership
• The Value Initiative:
Members in Action:
Managing Risk & New
Payment Modelshttp://www.aha.org/advocacy-
issues/affordability/membersinaction/me
mber-in-action-sharp-grossmont-
hosp.pdf

Levels of Intervention for Complexity of Care
Social Navigation
Medical Care Navigation
Community Information Exchange
Navigating community
resources and access to
services
Connecting to follow-up care
for health condition
Shared record across
agencies for opportunity for
engagement

Lessons Learned:
• Measure outcomes outside of health care costs
• Identify and value organizational champions
• Outcomes tracking with feedback loop to providers
• Tailor interventions and resources for complex health and social
need patients