Embed Size (px)
Citation preview

Changing Welfare Policies and (Long-term) Care Relations
Prof. Dr. Heinz RothgangCentre for Social Policy Research
University of Bremen
“Relationistic Sociology and Care Relations in a Changing Welfare State”
Workshop of the Research Network “Welfare Societies”July 29th 2011 in Delmenhorst

Prof. Dr. Heinz Rothgang 2
ContentsI. Terminological clarification
II. Action theory: care-giving as a make-or-buy decision
III. The need of long-term care as a new social risk
IV. Welfare State Arrangements in the OECD World
V. Welfare state policies in long-term care
VI. Who cares?
VII. The political issue: How to guarantee future care-giving?

Prof. Dr. Heinz Rothgang 3
ContentsI. Terminological clarification
II. Action theory: care-giving as a make-or-buy decision
III. The need of long-term care as a new social risk
IV. Welfare State Arrangements in the OECD World
V. Welfare state policies in long-term care
VI. Who cares?
VII. The political issue: How to guarantee future care-giving?
Prof. Dr. Heinz Rothgang 4
I. Terminological clarification• Care:
– Care vs. cure– Nursing care vs. social care– Care management vs. case management– Care for
• Children, chronically ill, people with dementia, etc. • People in need of long-term care (=LTC)
• Care relations: – Care-giver vs. cared for – Welfare state agents vis-à-vis care relations
• Welfare state and (long-term) care relation – Changing LTC relations challenge welfare states– Welfare state policies influence care relations

Prof. Dr. Heinz Rothgang 5
ContentsI. Terminological clarification
II. Action theory: care-giving as a make-or-buy decision
III. The need of long-term care as a new social risk
IV. Welfare State Arrangements in the OECD World
V. Welfare state policies in long-term care
VI. Who cares?
VII. The political issue: How to guarantee future care-giving?

Prof. Dr. Heinz Rothgang 6
II. Action theory: Care-giving as a make or buy decision • Care arrangements reach from purely informal to purely
formal care with all kinds of mixed arrangements in-between
• Family chooses arrangements. Determinants are1. Affection (individual care relation)2. Sense of obligation, religious beliefs (culturally) 3. Availability of formal care (national and regional level)4. Opportunity costs (=incentive structure)
• Publicly financed benefits • Prices for formal care • Satisfaction from care-giving• Opportunities to earn in the labour market
• 2, 3, and 4 in particular may change over time– For Germany: § 8 SGB XI defines care-giving as a “gesamt-
gesellschaftliche Aufgabe” moral obligation to care decreases

Prof. Dr. Heinz Rothgang 7
II. Action theory: Care-giving as a make or buy decision (1/3)
Source: Eurofamcare – Final Conference

Prof. Dr. Heinz Rothgang 8
I.2 Action theory: Care-giving as a make or buy decision (2/3)
Quelle: GEK-Pflegereport 2009
Tabelle 1: Regressionsmodelle: Pflegearrangements stationär ambulant Geld
Konstante 54,50 *** 27,24 *** 18,26 *** Vollstationäre Heimplätze je 100 Personen älter 75 Jahre
1,71 *** -0,35 *** -1,36 ***
Beschäftigte in amb. Diensten in VZÄ je 100 Personen älter 75 Jahre
-1,84 *** 4,19 *** -2,34 ***
Arbeitslosenquote -0,66 *** -0,14 ** 0,81 *** Personen je Haushalt -14,83 *** -3,38 * 18,20 *** Agglomerationsraum 0,81 -1,21 * 0,31 Verstädterter Raum 0,36 -0,72 0,36 Kreisfreie Stadt 1,91 ** -0,77 -1,14 Neue Bundesländer 4,40 *** -0,33 -4,07 *** Heimkosten 0,00 * 0,00 -0,00 * Anmerkung: *** P < 0,1 %; ** P < 1 %; * P < 5 % Referenzkategorien: Ländlicher Raum; Kreise; alte Bundesländer

Prof. Dr. Heinz Rothgang 9
83%
60% 59%70% 64% 60%
47%
8%
20% 15%6% 11%
0% 10%
8%20% 26% 24% 25%
40% 33%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
trad.U
S-Milie
une
ues U
S-Milie
u
kons
.MS-M
ilieu
gese
llsch.M
ittelib
erales
MS-M
ilieu
kons
erv.bü
rgerl.M
ilieu
libera
les bü
rg.Milie
u
selber gepflegt nur organisiert nicht beteiligt
Befragte, bei denen ein naher Angehöriger pflegebedürftig wurde(ist) (n=306)
Blinkert / KlieAnnabergstudie 2006
I.2 Action theory: Care-giving as a make or buy decision (3/3)
Prof. Dr. Heinz Rothgang 10
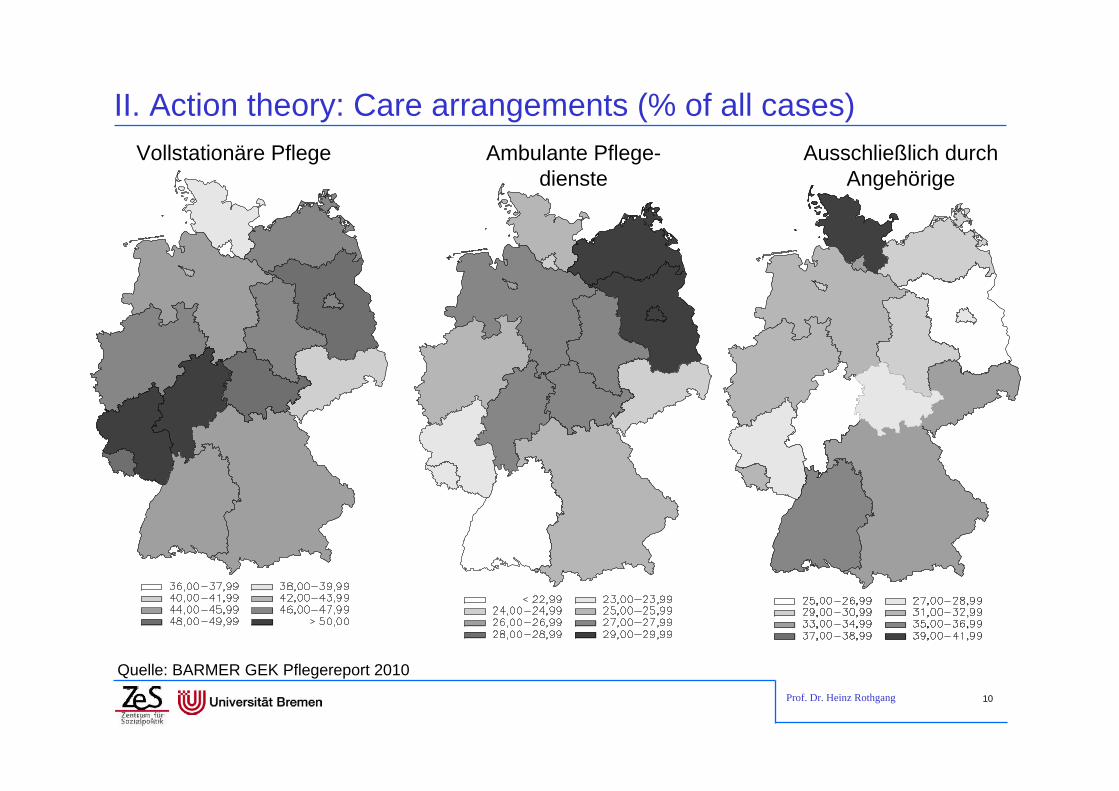
II. Action theory: Care arrangements (% of all cases)
Quelle: BARMER GEK Pflegereport 2010
Ambulante Pflege-dienste
Ausschließlich durch Angehörige
Vollstationäre Pflege

Prof. Dr. Heinz Rothgang 11
II. Action theory: nursing home beds per population
Quelle: GEK Pflegereport 2009

Prof. Dr. Heinz Rothgang 12
II. Action theory: Regional variation in nursing home rates (1/2)Nursing homes rates in level I Nursing home rates in level II
Prof. Dr. Heinz Rothgang 13
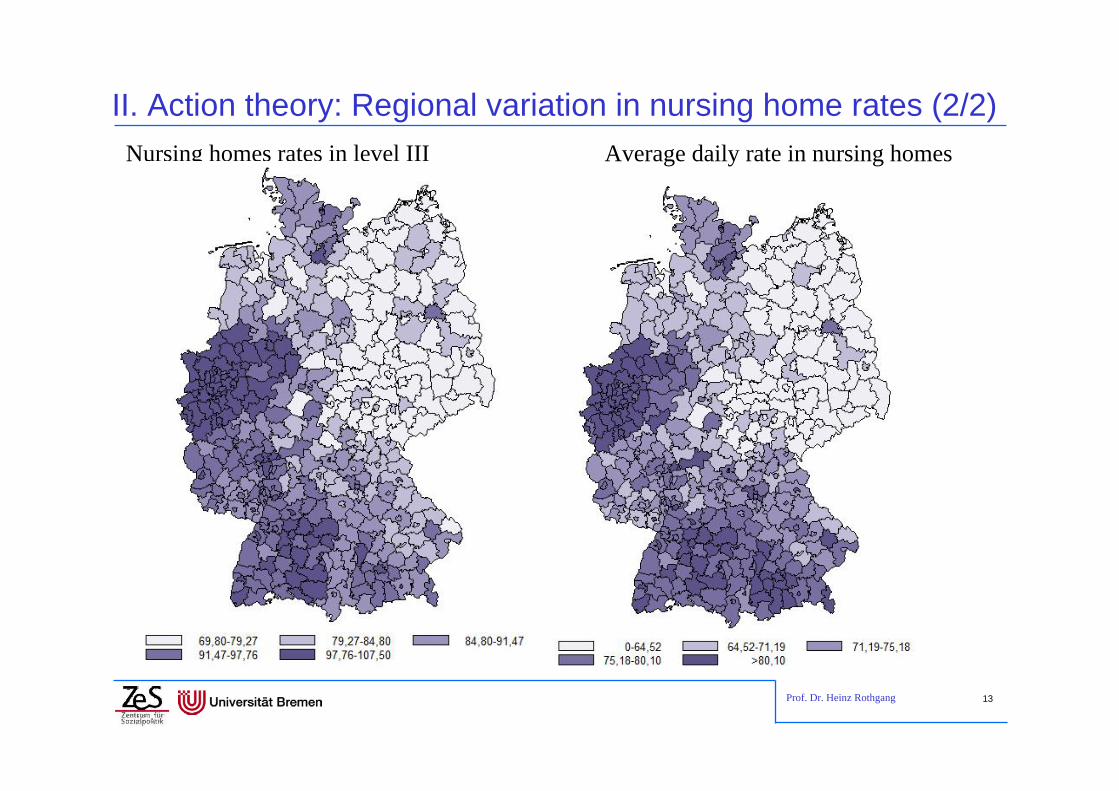
II. Action theory: Regional variation in nursing home rates (2/2)Nursing homes rates in level III Average daily rate in nursing homes

Prof. Dr. Heinz Rothgang 14
ContentsI. Terminological clarification
II. Action theory: care-giving as a make-or-buy decision
III. The need of long-term care as a new social risk
IV. Welfare State Arrangements in the OECD World
V. Welfare state policies in long-term care
VI. Who cares?
VII. The political issue: How to guarantee future care-giving?

Prof. Dr. Heinz Rothgang 15
III. The need of long-term care …… as a new social risk
– Dependency in itself is not new, but • the numbers of dependents has increased• the traditional forms of care-giving seem to loose capacities higher visibility a new problem arises
– Welfare states react (late) constituting a “new” risk• In the EU long-term care was not covered as a risk of its own, thus
the ECJ subsumed it under “health” (Molenaar case 1998)• With few exceptions national legislation only started in the 1990s
… as a new social risk– is relevant for all parts of the population and – has a high quantitative relevance

Prof. Dr. Heinz Rothgang 16
III. The need of long-term care as a social risk
Among the elderly (65+) the risk is at about 10%
Only 2.6% of the total population is in need of long-term care
But: more than half of all those dying in a certain year are in need of long-term care more than half of us will be in need of long-term care
Long-term care is not a fringe risk, but a social risk that should be addressed
Insufficient coverage is an issue for social policy
Share of LTCI beneficiaries among those who died in …
40,3 41,6 43,5 45,4 47
60,2 61,964,3 65 66,7
0
10
20
30
40
50
60
70
80
2001 2003 2005 2007 2009
Jahr
Männer Frauen
Prof. Dr. Heinz Rothgang 17
ContentsI. Terminological clarification
II. Action theory: care-giving as a make-or-buy decision
III. The need of long-term care as a new social risk
IV. Welfare State Arrangements in the OECD World1. Some figures2. Typologies3. The role of women
V. Welfare state policies in long-term care
VI. Who cares?
VII. The political issue: How to guarantee future care-giving?
Prof. Dr. Heinz Rothgang 18
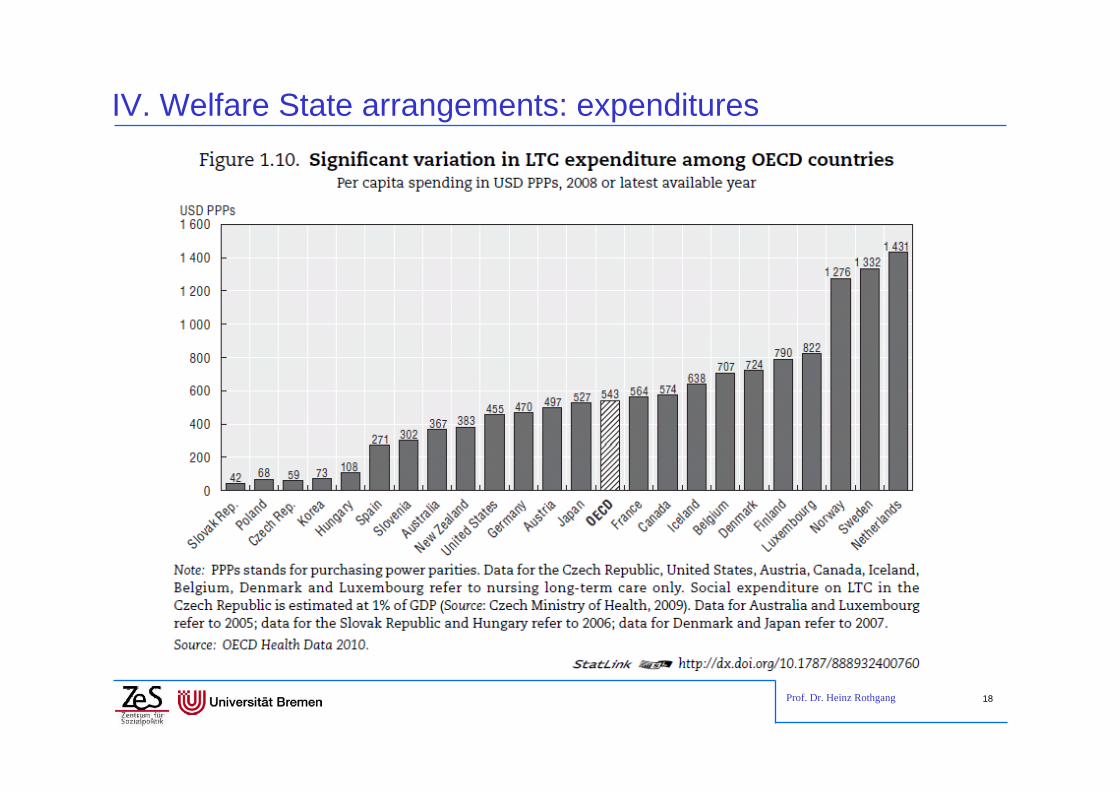
IV. Welfare State arrangements: expenditures

Prof. Dr. Heinz Rothgang 19
IV. Welfare State arrangements: public-private expenditure mix

Prof. Dr. Heinz Rothgang 20
IV. Welfare State arrangements: expenditures to arrangements

Prof. Dr. Heinz Rothgang 21
IV. Welfare State arrangements: Care Arrangements

Prof. Dr. Heinz Rothgang 22
IV. Welfare State arrangements: Typology • There is no well established typology of LTC systems;
Esping-Andersen’s typology is not really useful for LTC
• Attempts for classifications include– Anttonen & Sipilä (1996):
• Scandinavian model of public services • mostly Southern European family care model plus• Central European subsidiary model and • British model of means-testing in the middle
– Bettio & Pantenga (2004): • Southern European countries with much informal and little formal care • Northern European countries with universalistic approach and much
formal care– Timonen (2008):
• three paradigms according to the role of the state, the role of individuals / families and the role of private care provision

Prof. Dr. Heinz Rothgang 23
IV. Welfare State arrangements: Typologies
11
Typology of some EU countries
LTC financing system
Bismarck-Type Beveridge-Type
Type of wel-fare state
Separate LTCI system
No separate LTCI system
Sozial-democratic
Type A Denmark, Finnland,
Sweden
Conservative Type B Austria, Ger-
many, Lu-xembourg,
Netherlandsb
Type C Belgium,
France,a Italy
Liberal Type D United Kingdom, Ireland
Rudimentary Type E: Spanien, Por-tugal, Grie-
chenland

Prof. Dr. Heinz Rothgang 24
IV. Welfare State arrangements: Cash benefits and women • Throughout the OECD informal care-giving is
predominantly female
• Cash benefits – acknowledge informal care-giving but – tend to stabilize gender roles
• Welfare State programmes differ with respect to cash benefits
– Austria: Pflegegeldgesetz (1993) introduced cash benefits as the only type of benefit
– Germany: Pflege-Versicherungsgesetz (1994) introduced the choice between cash benefits and benefits in kind (formal care)
– Japan: LTCI introduced in 2000 does not contain cash benefits as the Japanese feminists heavily opposed to it.

Prof. Dr. Heinz Rothgang 25
ContentsI. Terminological clarification
II. Action theory: care-giving as a make-or-buy decision
III. The need of long-term care as a new social risk
IV. Welfare State Arrangements in the OECD World
V. Welfare state policies in long-term care1. Normative Analysis2. The Introduction of LTCI in Germany
VI. Who cares?
VII. The political issue: How to guarantee future care-giving?

Prof. Dr. Heinz Rothgang 26
V.1 There is a case for mandatory LTC insurance• Private voluntary insurance without a safety net is no
alternative as no civilized society will leave elderly without care if they are in need of care
• Private voluntary insurance besides a – tax-financed – safety net is unlikely to work as private insurance is crowded out– E.g.: in Germany only about 300 thousand insurances has been sold
before mandatory LTCI was introduced– On the other hand: 80% of those in nursing homes relied on means-
tested social assistance
• Means-tested tax-financed social assistance is no solution as– private insurance is discouraged – those who buy insurance are exploited by those who don’t– elderly have to spend down assets and have to live on “pocket money”
Mandatory insurance is useful
Prof. Dr. Heinz Rothgang 27
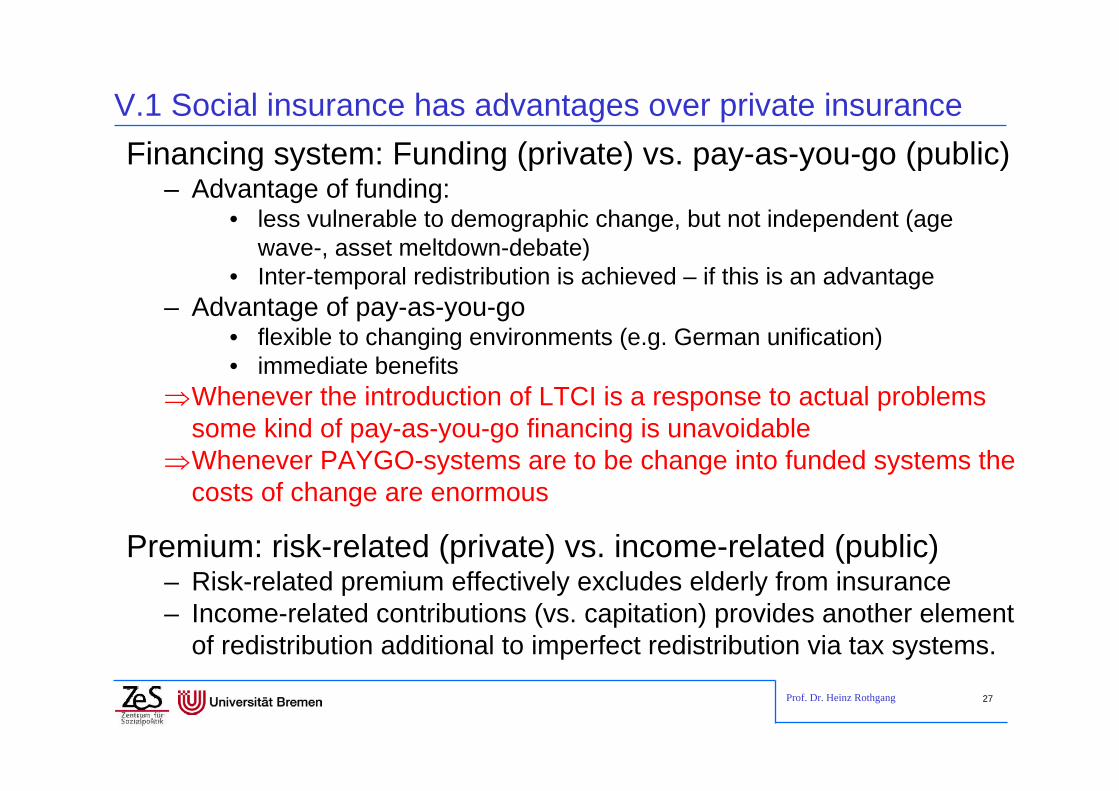
V.1 Social insurance has advantages over private insuranceFinancing system: Funding (private) vs. pay-as-you-go (public)
– Advantage of funding: • less vulnerable to demographic change, but not independent (age
wave-, asset meltdown-debate)• Inter-temporal redistribution is achieved – if this is an advantage
– Advantage of pay-as-you-go• flexible to changing environments (e.g. German unification)• immediate benefits
Whenever the introduction of LTCI is a response to actual problems some kind of pay-as-you-go financing is unavoidable
Whenever PAYGO-systems are to be change into funded systems the costs of change are enormous
Premium: risk-related (private) vs. income-related (public)– Risk-related premium effectively excludes elderly from insurance– Income-related contributions (vs. capitation) provides another element
of redistribution additional to imperfect redistribution via tax systems.

Prof. Dr. Heinz Rothgang 28
V.2 The introduction of LTC insurance (1/4): The Puzzle• LTCI Act was passed 1994 after 20 years of debate:
1. Why was the system introduced at all?– Which problems did the Act address?– Who were the advocates of the reform and why?
2. Why was it introduced at this time? – under a centre-right coalition– in a period of ‘permanent austerity’?
3. Why was it introduced the way it was introduced– with two branches of insurance– with the social insurance following the PAYGO system with capped
benefits etc.?

Prof. Dr. Heinz Rothgang 29
V.2 The introduction of LTC insurance (2/4)• Underlying problem perception
– Demographic change: number of dependent elderly was expected to grow
– Socio-structural change: care capacities of families were expected to decrease
– Increasing numbers of dependent elderly in nursing homes were relying on (means-tested) social assistance
• LTCI was fostered by two distinct discourses – Welfare state discourse:
• German welfare state aims at status maintenance. • It is “unworthy” if citizens with after a normal working life depend on
welfare just because of needing long-term care• High share of welfare recipients was perceived as social scandal
– Fiscal policy discourse• Municipalities were increasingly suffering from high expenditures for
people in nursing homes. Federal states acted as advocates.

Prof. Dr. Heinz Rothgang 30
V.2 The introduction of LTC insurance (3/4)• Course of events
– 1974: report of KDA started welfare state debate on LTC– 1980s: federal states put forward reform proposals triggered by
the fiscal policy debate– 1990s: Fiscal strains due to German reunification. Federal Minster
Blüm advocated introduction of LTC insurance• Blüm advocated insurance though he rejected the idea before• There was also a game for power within government.
LTCI was legitimated by welfare state discourse. The introduction, however, was due to fiscal policy discourse.

Prof. Dr. Heinz Rothgang 31
V.2 The introduction of LTC insurance (4/4)• Reshaping of the welfare state rather than expansion:
– Introduction of LTCI was accompanied by cuts in other welfare state areas
– LTCI marks break with German tradition of service provision according to needs (as in health insurance)
– LTCI Act was shaped in order to prevent any “cost explosion”thereafter
• Tight definition of dependency• Capped benefits (nominally fixed)• Discretionary adjustment of benefits
• Compromise between Christian Democrats and Liberals: two-pillar system with
– Social LTCI as PAYGO system, but– Private mandatory System as funded system
Prof. Dr. Heinz Rothgang 32
ContentsI. Terminological clarification
II. Action theory: care-giving as a make-or-buy decision
III. The need of long-term care as a new social risk
IV. Welfare State Arrangements in the OECD World
V. Welfare state policies in long-term care
VI. Who cares? 1. Care-giving – today2. Care-giving – past developments3. Care-giving – the future
VII. The political issue: How to guarantee future care-giving?

Prof. Dr. Heinz Rothgang 33
VI.1 Care-giving – today
Prof. Dr. Heinz Rothgang 34
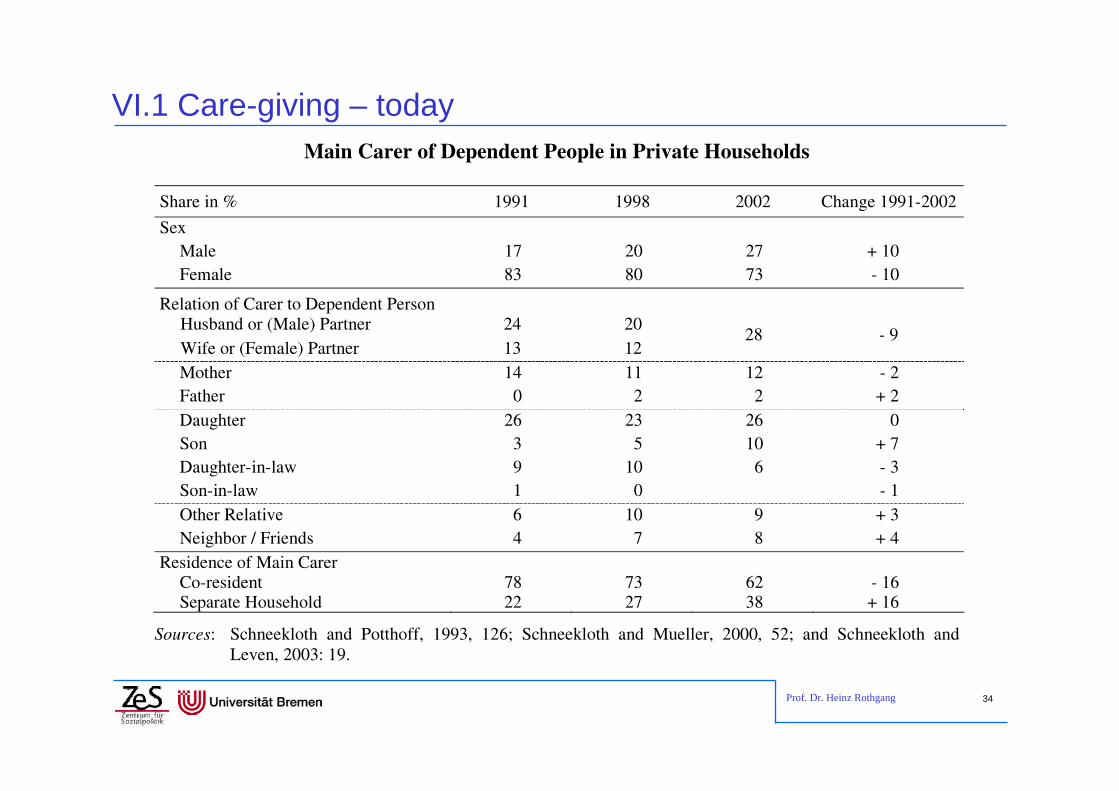
VI.1 Care-giving – todayMain Carer of Dependent People in Private Households
Share in % 1991 1998 2002 Change 1991-2002
Sex Male 17 20 27 + 10 Female 83 80 73 - 10
Relation of Carer to Dependent Person Husband or (Male) Partner 24 20 Wife or (Female) Partner 13 12
28 - 9
Mother 14 11 12 - 2 Father 0 2 2 + 2 Daughter 26 23 26 0 Son 3 5 10 + 7 Daughter-in-law 9 10 6 - 3 Son-in-law 1 0 - 1 Other Relative 6 10 9 + 3 Neighbor / Friends 4 7 8 + 4
Residence of Main Carer Co-resident 78 73 62 - 16 Separate Household 22 27 38 + 16
Sources: Schneekloth and Potthoff, 1993, 126; Schneekloth and Mueller, 2000, 52; and Schneekloth and Leven, 2003: 19.

Prof. Dr. Heinz Rothgang 35
VI.2 Care-giving – past developments (1/3)• Introduction of LTCI triggered expansion of formal sector,
particularly in nursing home care intended effect
• There are huge regional differences in utilizing formal care not intended
• LTCI aims to favour family care over (formal) community care over nursing home care
• There are several measures favouring home care, e.g.– Cash benefits for family care– Pension benefits for informal care-givers– Higher benefits for home care (in level I and II)
• Nevertheless, there has been a trend towards formal care, though the rate of the shift is declining

Prof. Dr. Heinz Rothgang 36
Capacities of formal care
Extramural Care Intramural Care Number of Providers
Employees Whole time equivalents
Number of Nursing homes
Number of beds in nursing
homes 1999 10,820 183,782 56,914 8,859 645,456 2001 10,594 189,567 57,524 9,165 674,292 2003 10,619 200,897 57,510 9,743 713,195 2005 10,977 214,307 56,354 10,424 757,186 2007 11,529 236,162 62,405 11,029 799,059
1999-2001 -2,1 3,1 1,1 3,5 4,5
2001-2003 0,2 6,0 0,0 6,3 5,8
2003-2005 3,4 6,7 -2,0 7,0 6,2
2005-2007 5,0 10,2 10,7 5,8 5,5
1999-2007 6,6 28,5 9,6 24,5 23,8
Source: Statistisches Bundesamt 2008b: 25.
VI.2 Care-giving – past developments (2/3)

Prof. Dr. Heinz Rothgang 37
VI.2 Care-giving – past developments (3/3)
Source: own calculations based on data published by the Federal Ministry of Health
Type of benefits chosen
23,125,4 26,3 26,8 27,5 27,9 28,3 28,7 29,2 29,5 29,6 29,8 29,5 29,0
61,358,1
55,9 54,2 53,0 52,3 52,0 51,5 51,0 50,6 50,3 49,9 49,6 49,0
8,8 9,4 10,0 10,6 10,7 11,0 10,9 10,8 10,8 10,8 10,7 11,0 12,0 13,5
6,9 7,1 7,8 8,4 8,9 8,8 8,8 9,0 9,0 9,1 9,3 9,3 8,9 8,5
0
10
20
30
40
50
60
70
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009Year
Nursing home care cash benefitscombination in kind benefits

Prof. Dr. Heinz Rothgang 38
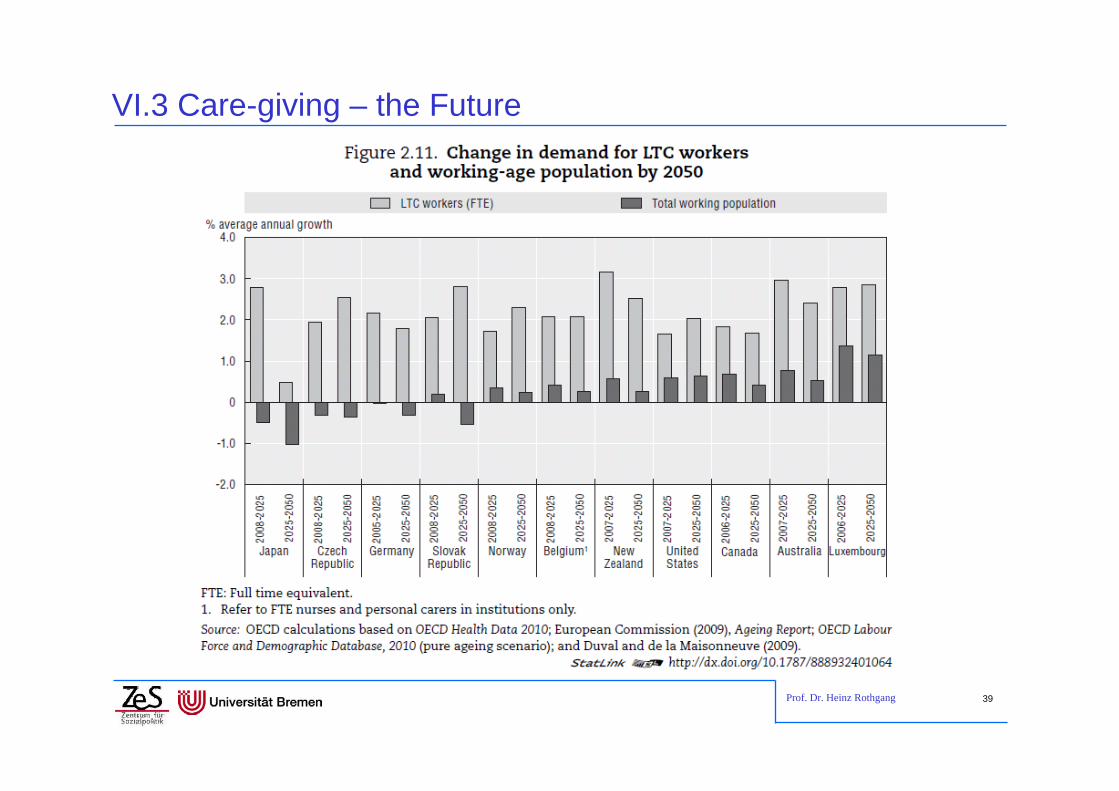
VI.3 Care-giving – the Future• There are good reasons to assume a continuation of this
trend– Demography: Decreasing share of informal caregivers per
dependent elderly– Socio-structural change: Increasing share of 1-person households
among elderly; children live further away – Increase female labour market participation higher opportunity costs of family care-giving
– Declining “duty to care” felt by families
• On the other hand the reservoir of professional care-givers is not growing respectively.
Prof. Dr. Heinz Rothgang 39
VI.3 Care-giving – the Future

Prof. Dr. Heinz Rothgang 40
VI.3 Care-giving – the FutureEntwicklung des Pflegepotenzials je Pflegebedürftigem in NRW - 2002 bis 2040
40
50
60
70
80
90
100
110
2002 2005 2010 2015 2020 2025 2030 2035 2040
Inde
x
Partnerpflegepotenzial je Pfegebed.Kinderpflegepotenzial Szenario 2Kinderpflegepotenzial Szenario 3Pflegepotenzial gesamt Szenario 2Pflegepotenzial gesamt Szenario 3
Abbildung 3: Entwicklung der Indizes für das häusliche Pflegepotenzial je Pflegebedürftigem in Nordrhein-Westfalen 2002 bis 2040 im SzenarienvergleichQuelle: Rothgang 2004.

Prof. Dr. Heinz Rothgang 41
VI.3 Care-giving – the FutureStatus quo
Future
2/3 of all dependent persons are care for in private households
Every 2nd dependent person is cared for without formal care
Informal care is the backbone of care-giving
Relative care potential, i.e. potential informal caregiver per dependent persons, is going to half by 2040
Informal care is going to decline
A new balance of care-giving (‚mixed care arrangements‘) has to be found
• support for informal care-givers
• new role for formalcare (workingtogether with families)
• case management
Growing Expen-diture

Prof. Dr. Heinz Rothgang 42
ContentsI. Terminological clarification
II. Action theory: care-giving as a make-or-buy decision
III. The need of long-term care as a new social risk
IV. Welfare State Arrangements in the OECD World
V. Welfare state policies in long-term care
VI. Who cares?
VII. The political issue: How to guarantee future care-giving?
Prof. Dr. Heinz Rothgang 43
VII. How to guarantee future care-giving?• How to finance LTC?
• How to stabilize informal care?– 2008 reform: counselling, case and care management, additional
benefits for people with dementia, work leave for care-giving– Actual debates
• Reforming the entitlement (new “Pflegebedürftigkeitsbegriff”)• Improve possibilities to combine care-giving and work
• How to find enough professional care-givers– Improving recruitment, retention, and return after childbirth by
• Improving the image of the profession• Improving working conditions and pay
• In order to find the right policy better theories about the care relation and what makes people care might be helpful.
Prof. Dr. Heinz Rothgang 44
The end
Thank you for your attention!
Contact: [email protected]
See also:
Rothgang, Heinz (2010): Social Insurance for Long-Term Care: An Evaluation of the German Model, in: Social Policy and Administration, Vol. 44, No. 4, August 2010, pp. 436–460