Embed Size (px)
Citation preview

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
1
Chapter 1
Suspended animation:
concepts of anaesthesia
Introduction
A recent study estimated that 234 million surgical procedures requiring anaesthesia are performed worldwide annually. Anaesthesia is the largest hospital specialty in the UK, with over 12,000 practising anaesthetists, yet in many ways it is the most mysterious. Most non-medical people have only the haziest idea of what anaesthesia involves. The media image is unhelpful. Medical dramas, for example, traditionally paint the surgeon as the hero, and the anaesthetist as a panic-stricken subordinate.
When undergoing an operation, the anaesthetic contributes only a tiny part of the overall risk. Yet, in general, people seem to fear the anaesthetic most of all. Many of my patients express real fears, and ask things like ‘What happens if I don’t go to sleep?’, ‘ What happens if I don’t wake up?’, ‘What happens if I wake up in the middle?’, and ‘How do you know I am really asleep?’
Anaesthesia is both fascinating and rewarding. What I do every day is to suspend the conscious minds of my patients, so that they can undergo painful, invasive surgical procedures of which they remain entirely unaware. The means by which this is brought about still has a hint of magic for me.

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
An
aest
hes
ia
2
In this book, I give a short account of the historical background of anaesthetic practice, a review of anaesthetic equipment, techniques, and medications, and a discussion of how they work. The risks and side effects of anaesthetics will be covered, and some of the subspecialties of anaesthetic practice will be explored.
Concepts of anaesthesia
Many of us have undergone general anaesthesia ourselves, or we may know someone who has. The concept of general anaesthesia is familiar to us, but it is worth having a closer look at the fundamental aspects.
If you observe an adult male under general anaesthesia, he appears to be asleep. He is lying on his back with his eyes closed, not moving. His breathing is slow and regular. His skin is warm and dry. However, if you were to shout his name, or shake him by the shoulder, he would not wake up. Even if you were to cut into his skin with a scalpel, he would not wake up, move, or show any obvious outward response.
Although we often use the word ‘asleep’ to describe someone who is anaesthetized (and I usually use this form of words when talking to patients and colleagues), general anaesthesia is not sleep. In physiological terms, the two states are very dissimilar. The term general anaesthesia refers to the state of unconsciousness which is deliberately produced by the action of drugs on the patient. Local anaesthesia (and its related terms) refers to the numbness produced in a part of the body by deliberate interruption of nerve function; this is typically achieved without affecting consciousness.
What is general anaesthesia?
In the early days of anaesthesia, the mid-19th century, the term etherization was used to describe the state produced by the

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
Susp
end
ed an
imatio
n: con
cepts o
f anaesth
esia
3
inhalation of ether vapour. However, it soon became clear that chloroform and other agents could produce effectively the same state as ether. Clearly, a patient could not be etherized with chloroform. To try to fi nd one word which suffi ced to describe this new state was not easy. Some of the early terms were ‘clumsy, and some of them cacophonous’, such as narcotism , sopor , hebetization , apathization , letheonization , and stupefaction . The American neurologist Oliver Wendell Holmes suggested the term anaesthesia in 1846 in a letter to William Morton, from the Greek meaning ‘without sensation’, and this word, together with its adjective anaesthetic , caught on rapidly. By the time James Young Simpson was publishing his early results with chloroform in 1847, the term was in common use, although ungainly alternative terms such as northria or metaesthesia are still occasionally proposed.
The purpose of inhaling ether vapour was so that surgery would be painless, not so that unconsciousness would necessarily be produced. However, unconsciousness and immobility soon came to be considered desirable attributes of anaesthesia. John Snow, the fi rst doctor to specialize in anaesthesia, wrote in 1872: ‘Ether contributes other benefi ts besides . . . preventing pain. It keeps patients still who otherwise would not be.’ For almost a century, lying still was the only reliable sign of adequate anaesthesia. The state of unconsciousness was considered an advantageous relief from the traumatic experience of surgery.
For nearly a century after the introduction of general anaesthesia, it was provided by a single agent in the majority of cases. Usually, this was ether or chloroform; occasionally, a mixture of the two, or switching from one to the other, was used. Since those agents did what everyone thought was required (they kept the patient unconscious and unmoving), no further consideration was needed. However, the introduction of intravenous agents, muscle relaxants, and other adjuncts led to a discussion of the more specifi c components of general anaesthesia.

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
An
aest
hes
ia
4
In 1926, John Lundy from the Mayo Clinic introduced the term balanced anaesthesia to describe using an array of techniques (such as a sedative premedicant to cause sedation together with general anaesthesia using different agents) to obtain best results. In 1950, Gordon Jackson Rees and Cecil Gray from Liverpool proposed a ‘triad’ of anaesthesia: narcosis (by which they meant ‘unconsciousness’), analgesia, and muscle relaxation, which are often represented on a triangular diagram still taught to students. Crucially, one agent was no longer suffi cient to produce all of these effects, but by using (for example) halothane for unconsciousness, morphine for analgesia, and tubocurarine for muscle relaxation, safe and reliable operating conditions could be produced. The combination of an anaesthetic agent, an analgesic, and a muscle relaxant is still widely used, but the triad model is out of date. For a better model, a more careful consideration of the components of general anaesthesia is required.
Unconsciousness
A few years ago, an anaesthetist friend dislocated his shoulder playing squash. He went to his local emergency department, where he was given a large dose of the analgesic morphine, and a large dose of the sedative midazolam. His shoulder was then put back into joint. He knows he was awake at the time, and he knows that relocation of the shoulder is an extremely painful procedure, despite the morphine. However, due to the effects of the midazolam, which causes transient memory loss, he cannot remember the pain.
What my friend underwent was not general anaesthesia. However, the question he asked me was whether it is ethical to infl ict pain on a patient who does not remember it afterwards, assuming there is no emergency or other urgent reason to do so. After some thought, I replied that I do not think that it is ethical to deliberately infl ict pain on a conscious human being at any time, when alternative courses of action are to hand. Whether that person remembers it afterwards is beside the point.

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
Susp
end
ed an
imatio
n: con
cepts o
f anaesth
esia
5
General anaesthesia provides unconsciousness, but it is reasonable to look closer at what this actually means.
Among many other functions, the conscious mind is responsible for forming both experiences and memories of those experiences. If only one of those functions were interrupted, the mind might form experiences, such as pain, but not memories, and a situation like my friend’s might ensue. However, general anaesthesia temporarily suspends the formation of both experiences (perceptions, awareness) and memories of those experiences.
In addition, general anaesthesia is considered to be a state induced by anaesthetic drugs (the patient cannot make it happen to him- or herself ), and one that is reversible, in the sense of not being permanent: if I were to suffer a head injury, I might cease to form experiences or memories, but this is not general anaesthesia.
Muscle relaxation
Another point on the triad model is muscle relaxation. Cutting into muscle, such as the muscle of the abdominal wall, causes a refl ex spasm of the muscle itself which makes surgery technically more diffi cult, and this reaction is only abolished at very deep planes of anaesthesia. Placing a tube in the trachea is also an extremely stimulating procedure, which can only be performed under very deep anaesthesia. Both these problems can be circumvented by the use of drugs to paralyse the muscles. Anaesthesia need therefore only be deep enough to produce unconsciousness, but paralysis suffi cient for surgical access or intubation can be readily produced by drugs. The term muscle relaxants is used to describe such drugs, which came widely into practice in the 1940s.
However, for many surgical procedures, muscle relaxation is not required. Even without muscle relaxants, a patient under general anaesthesia will not make voluntary movement, even in response

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
An
aest
hes
ia
6
to a painful stimulus such as surgery, and immobility to stimulation is one of the easiest objective signs of general anaesthesia.
But unconsciousness and immobility are not the end of the story. Anaesthesia was fi rst introduced as a means of eliminating pain.
What is pain?
All of us have experienced pain, from our earliest experiences as infants teething or with colic.
The International Association for the Study of Pain (IASP) defi nes pain as ‘an unpleasant sensory and emotional experience resulting from a stimulus causing, or likely to cause, tissue damage, or expressed in terms of that damage’. This is a helpful defi nition, as it incorporates those things which cause pain (actual or potential damage to the body), and the result (an unpleasant sensory experience), as well as the consequences of that result (an unpleasant emotional experience).
The neurophysiology of pain has been extensively studied, and it can be considered to comprise several steps. First, there is the detection of a painful stimulus ( nociception ), which happens by the triggering of specifi c nerve endings called nociceptors in the skin and other organs. Nociceptors produce electrical signals in pain nerve fi bres. These electrical signals are transmitted to the spinal cord by peripheral nerves. The signals may be modifi ed in the spinal cord, but are then transmitted up to the thalamus, a part of the brain which is responsible for integrating sensory signals of all types. From the thalamus, the signals travel to the cortex, the convoluted surface of the brain. At this point, the pain signals are integrated into conscious perception, and it can be stated that pain is being perceived. (Until this point, there were only pain signals.)

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
Susp
end
ed an
imatio
n: con
cepts o
f anaesth
esia
7
However, the process does not end there. The experience of pain triggers powerful emotional consequences, including fear, anger, and anxiety. A reasonable word for the emotional response to pain is ‘suffering’. Pain also triggers the formation of memories which remind us to avoid potentially painful experiences in the future. The intensity of pain perception and suffering also depends on the mental state of the subject at the time, and the relationship between pain, memory, and emotion is subtle and complex.
On their journey through the subconscious parts of the brain, pain signals also trigger physiological responses to stress, by activating what is called the sympathetic nervous system to produce adrenaline (the so-called ‘fi ght or fl ight’ response). The effects of adrenaline are responsible for the appearance of someone in pain: pale, sweating, trembling, with a rapid heart rate and breathing. Additionally, a hormonal storm is activated, readying the body to respond to damage and fi ght infection. This is known as the stress response .
Nociception and pain transmission can be demonstrated in very simple animals, such as fruit fl ies or worms. However, we hesitate to call their experience pain, because we do not consider fl ies and worms to be conscious in the way that humans are.
To come back to our patient, therefore, it might be reasonable to suppose that someone who is unconscious cannot experience pain or suffering, because experiences require a conscious mind.
In fact, even if our patient does not outwardly respond to a surgical incision, he will show signs of registering the stimulus. His heart rate and blood pressure increase. His breathing becomes deeper and more rapid. The hormonal markers of the stress response can be detected in his bloodstream.
Those responses may be abolished by an analgesic such as morphine, which will counteract all those changes. For this reason, it is routine to use analgesic drugs in addition to

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
An
aest
hes
ia
8
anaesthetic ones. But this invites the question: if the patient isn’t aware of the pain, why are painkillers necessary?
The hormonal stress response can be shown to be harmful, especially to those who are already ill. For example, the increase in blood coagulability which evolved to reduce blood loss as a result of injury makes the patient more likely to suffer a deep venous thrombosis in the leg veins. The stress response causes breakdown of fats and proteins to mobilize energy stores: the opposite of the healing response required to build new cells and repair tissues. There is therefore a therapeutic imperative to reducing or treating it. Additionally, a patient with good analgesia intraoperatively is likely to wake up more comfortable than one who has not, so there is a humane benefi t to good intraoperative analgesia. Typical anaesthetic agents are poor at suppressing the stress response, but analgesics like morphine are very effective. Therefore, the optimal confi guration of a general anaesthetic seems to be a general anaesthetic agent to produce unconsciousness, combined with an analgesic to blunt the stress response.
The fridge problem and the formation of memory
As a boy, I remember being puzzled by the question of what happens to the fridge light when the door is closed. Every time I opened the fridge door, no matter how suddenly (to catch it by surprise) or gently (so that the fridge would not notice me), the light was always on. I concluded (wrongly) that the light remained on all the time.
Is there anything which we can measure or detect from outside the fridge, with the door closed, which would tell us if the light were on? It is plain that no light escapes through the door.
Investigation of general anaesthesia poses the same conceptual problem. In this case, the fridge is the patient, and the light is the patient’s consciousness. When the door is open, the patient is conscious, and we can clearly see the light, in the form of the

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
Susp
end
ed an
imatio
n: con
cepts o
f anaesth
esia
9
patient’s interaction with us. When we induce general anaesthesia, we close the door, and we may be left wondering whether the light is somehow still on, however dimly.
One simple solution might simply be to wait until the patient recovers, and ask him what he remembers. The answer is, almost always, that the patient can remember nothing of what happened; in fact, he has no sensation of time having elapsed at all while he was anaesthetized.
By ‘remember’, I mean explicit memory, which is that memory which can be directly called to mind, such as your home phone number. However, there is also the phenomenon of implicit memory, which is memory which cannot be called directly to mind, but nonetheless informs our choices and actions, without our necessarily being aware of it.
Researchers have studied implicit memory formation under anaesthesia using a variety of methods such as free-association word-pair testing, or hypnosis. Early attempts to reveal implicit memory formation under general anaesthesia seemed disquietingly successful, but were methodologically fl awed. To address the issue, a dramatic and compelling study was undertaken by Ben Chortkoff and colleagues in San Francisco. This was essentially a repetition of a 1965 study, but designed to eliminate the fl aws in the earlier work by providing both a control group and investigators who were ‘blind’ to which group the subjects were in. Twenty-one patients were randomized into two groups, anaesthetized, and the following script was played to one of the groups through headphones:
‘Oh, shit, who turned off the oxygen? Who disconnected the
cylinder? Damn it, he’s turning blue. God, his lips are blue. Get that
thing connected again. You got it? OK. I’m going to give him some
more oxygen now.’ A 15-second pause followed, during which the
lungs were infl ated 3 times. ‘Ho boy. OK. He looks better now.
I think we can continue.’

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
An
aest
hes
ia
10
The control group was played a neutral script, but with the same pause and infl ation of the lungs. The following day, each patient was interviewed by a team of three researchers, using questioning and hypnosis to attempt to reveal which script had been heard. The researchers were blind to which script the patients had heard. They were unable to determine which patients had heard the crisis script, and none of the subjects was able to recall the crisis script. Other recent studies designed to investigate implicit memory formation have shown similar results.
Proving that the patient cannot remember things which happened under anaesthesia is not the same as proving that some awareness of those events did not take place at the time. My friend cannot remember having his shoulder relocated, but he believes it was painful at the time. The best evidence we have is that the activity of the brain required to produce consciousness and memory is suppressed very effectively by general anaesthesia.
Arthur Guedel
Arthur Guedel was an American anesthesiologist who was placed in charge of anaesthetic services for the US Army in Vosges, France, during the First World War. The few physician anaesthetists were swamped with cases and could not attend to the thousands of casualties. Guedel trained nurses and orderlies to provide general anaesthesia using ether, and created a wall-chart of the physical signs which took place as an (unpremedicated) patient goes under the infl uence of ether.
It is plain to any observer that someone who starts to breathe ether starts off wide awake (and, in some cases, fi ghting and struggling). Then, after a period, the person begins to become drowsy, then very drowsy, then unrousable, then, if administration is continued, the person will eventually die. There is obviously a relationship between dose and effect. Guedel needed to be able to show when the dose was insuffi cient, satisfactory, or excessive.

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
Susp
end
ed an
imatio
n: con
cepts o
f anaesth
esia
11
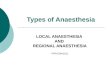
Guedel’s chart is a masterpiece of clarity and simplicity. It uses observations that are easy and quick to learn (such as the size of the pupils and their response to light, or the pattern of respiration) and require no fancy equipment. Guedel taught his technique to many hundreds of people, and used a motorbike to travel around between fi eld hospitals to supervise and teach his pupils.
Guedel was not the fi rst to describe different stages of anaesthesia. John Snow made an attempt many decades earlier, describing fi ve stages. However, Guedel’s stages were easy to differentiate, widely applicable, and very reliable, and became the basis of assessment of anaesthetic depth for the next fi fty years.
1. A chart devised by Arthur Guedel as a simple guide to the stages of anaesthesia, using easily identifi able parameters such as breathing and pupillary responses

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
An
aest
hes
ia
12
The fi rst two Guedel stages can helpfully be compared to the effects of alcohol, which are similar in many ways to the effects of general anaesthetic drugs.
Guedel’s stage 1 resembles mild intoxication with alcohol. The patient is relaxed and sociable, but otherwise behaviour, memory, speech, and refl exes are more or less normal, although the performance of fi ne motor tasks (such as driving) is demonstrably impaired. Alcohol, like general anaesthetic drugs, affects different parts of the brain at different rates.
Guedel’s stage 2 resembles severe intoxication with alcohol. There are several familiar features of this condition. First, there is a profound impairment of the performance of motor tasks. Second, there is behavioural disinhibition. This is because alcohol suppresses the effect of inhibitory pathways in the brain. This makes drunken people much more likely to act violently, to take foolish risks, or to engage in sexual activity which they later regret. Third, severe intoxication with alcohol predisposes to vomiting, as can be seen demonstrated on city streets after the pubs have closed. Fourth, memory can be impaired. People who drink heavily sometimes cannot remember how they got home the night before, or what their behaviour was like during this time.
Further features of stage 2 correspond to a slight preponderance of the sympathetic nervous system: modest dilation of the pupils (although they will react to light), and a slight increase in heart rate and blood pressure. Some refl exes may be slightly enhanced, because the suppression which normally keeps them in check is lost.
Imagine, then, a patient breathing ether. He is terrifi ed, and in dreadful pain from a gangrenous leg. He knows that if the leg is not amputated, he will die. Reluctantly, he starts to breathe the pungent ether vapour. At fi rst, he is able to cooperate, but then he becomes disinhibited, and his will to cooperate fades. He begins to fi ght and struggle with the anaesthetist. A few times, he manages to pull the

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
Susp
end
ed an
imatio
n: con
cepts o
f anaesth
esia
13
mask away from his face, which slows the onset of the ether. A few strong assistants hold him down, but then he vomits copiously, which causes him to choke and inhale his own gastric fl uids.
Guedel’s stage 2 is best defi ned by its most serious problem: disinhibition. Incidentally, fasting the patient before the operation is still routinely practised as a means of attempting to keep the stomach empty. It does not prevent vomiting at the onset of anaesthesia, but it means that the volume in the stomach is as low as possible.
Guedel knew, as many skilled anaesthetists did before him, that stage 2 is the most dangerous stage of anaesthesia. All of the adverse events at induction of anaesthesia occur in stage 2. There are a few additional ones, including coughing, breath-holding, and laryngospasm, a refl ex closure of the vocal cords that can cause the patient to die of an obstructed airway.
(It is diffi cult to get further than stage 2 with alcohol, which is why alcohol is not used as a general anaesthetic agent. Alcohol is not very potent, and must be given orally. Alcohol is also extensively metabolized to poisonous by-products which are responsible for hangover symptoms, but can also be fatal. The lethal dose and the anaesthetic dose of alcohol are therefore quite similar: too similar for it to be contemplated as a sensible choice of agent.)
Despite all these diffi culties, it is possible for a gentle anaesthetist to take a cooperative patient through stage 2 and into the safe stage 3. However, during this time, there must be no interruptions, or any loud noises or other stimuli which the patient might consider threatening. For this reason, until recently it was commonplace for anaesthetic rooms to have a sign on the door saying something like ‘Do not enter while anaesthetic is in progress’. My surgical colleagues usually ask ‘Is it OK to start?’ before they insert the scalpel at the beginning of the case. What they are really asking is: ‘Is this patient safely through stage 2 and

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
An
aest
hes
ia
14
into stage 3?’ Although modern agents are much more forgiving than ether, most anaesthetists still ask for quiet at induction.
Guedel’s stage 3 is the stage of surgical anaesthesia. This is what is meant by use of the term ‘general anaesthesia’ today. In stage 3, the patient will lie still, will not move in response to a painful stimulus, and will display no refl ex activity at all (for example, the eyes will not react to light) but will have adequate preservation of breathing and heartbeat to remain safely alive. Guedel divided stage 3 into four planes, which are of comparatively little relevance to modern clinical practice.
Guedel recognized that too much ether could kill the patient, and defi ned stage 4 as the stage of overdosage with anaesthetic. In stage 4, the patient is on their way to death: the pulse becomes impalpable; the breathing becomes very shallow and irregular, and eventually stops altogether. However, at least at fi rst, all is not necessarily lost. Provided that one recognizes what is going on, and stops giving ether, the patient is still likely to recover.
In fact, stage 4 does not come suddenly and unexpectedly. A vigilant anaesthetist watching the pulse and respiration would notice them declining in plenty of time to avert catastrophe.
Depth of anaesthesia
What Guedel did was to formalize, very effectively, a paradigm which everyone had already adopted: the notion that anaesthesia has ‘depth’.
The idea that anaesthesia has depth is a compelling one, but also controversial. I believe that the adjectives ‘deep’ and ‘light’ as applied to anaesthesia were borrowed from their traditional use in describing natural sleep. Although this makes the metaphor an attractive one because of its seeming familiarity, general anaesthesia is not sleep.

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
Susp
end
ed an
imatio
n: con
cepts o
f anaesth
esia
15
The concept of sleep brings us back to the opening of this chapter, and poses the question: what is the difference between natural sleep and anaesthesia?
Why anaesthesia isn’t sleep: looking at brainwaves
The most complete answer comes from studying the electrical activity of the brain, using the technique of electroencephalography (EEG), which was developed in the 1930s and continually refi ned since. Unfortunately, it is still a somewhat crude method of studying brain activity.
The EEG measures the minute electrical activity of the brain via electrodes placed on the scalp. However, the electrical activity of the brain is not confi ned to the surface: the brain is a solid organ and the deeper parts of the brain produce activity which may not be discernible on the surface at all, although it is likely that the conscious mind is represented in the cortex. EEG signals are extremely weak, and are measured on the microvolt scale, which makes them prone to interference from other sources of electrical signals, such as the heart or muscles, whose signals are approximately a hundred times more powerful.
The EEG waveform is extremely diffi cult to interpret. To an untrained observer, it looks like random squiggles. Played through a loudspeaker, it makes a hiss like a radio tuned to static. Trying to work from this signal to deduce what is happening in the brain is extremely diffi cult. However, certain deductions can be made. Any
One of our commonest phrases is ‘depth of anaesthesia’. We
speak of getting the patient ‘deeper’, of getting him ‘under’, of
getting him ‘down’. All these words imply movement in a vertical
direction; towards the grave.
William Woolf Mushin, 1960

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
An
aest
hes
ia
16
pathological activity, for example the kind that denotes some types of epilepsy, can usually be identifi ed. And some specifi c patterns of activity can be recognized; for example, an awake brain produces a fast, random signal known as the beta rhythm, characterized by the presence of activity with a frequency of 16–25 Hz.
Using EEG analysis, sleep is revealed to be a highly structured process. Humans undergo two different kinds of sleep. It is widely known that one of these produces rapid movements of the eyes, and is known as rapid eye movement (REM) sleep, whereas the other is non-REM (NREM) sleep. REM sleep is when the most vivid and evocative dreams occur but accounts for only 15–20% of sleep time. The two forms of sleep occur as part of a pattern lasting about 90 minutes known as a sleep cycle. It is normal to wake transiently between sleep cycles, and have between three and six complete cycles in a night.
Although our perception of sleep is that it is a period of rest and recharging of the inner batteries, ‘knitting up the ravell’d sleeve of care’, it is clear that sometimes there is considerable cortical activity going on. During REM sleep, for example, the EEG resembles that of the awake individual, with fast, low-amplitude, high-frequency activity.
If we monitor the EEG of someone under general anaesthesia, certain identifi able changes to the signal occur. In general, the frequency spectrum of the signal slows. Some of the features observed seem to resemble those in natural sleep, although the signifi cance of this is not known. Next, the overall power of the signal diminishes. In very deep general anaesthesia, short periods of electrical silence, known as burst suppression, can be observed. Finally, the overall randomness of the signal, its entropy, decreases.
In short, the EEG of someone who is anaesthetized looks completely different from someone who is awake. In contrast to

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
Susp
end
ed an
imatio
n: con
cepts o
f anaesth
esia
17
both wakefulness and REM sleep, anaesthesia is characterized by cortical quiescence. As far as we can tell with the EEG, the cortical function needed to create experiences and memories is signifi cantly affected by general anaesthesia, and this is backed up by other experimental evidence.
For investigation of the functioning brain, EEG has been superseded by more effective methods of investigation, such as functional magnetic resonance imaging (fMRI), which can image the activity of the whole brain in real time during specifi c tasks.
1.0
0.5
0
3 54
6
1
0
Pro
bab
ility
of
nonr
epon
sive
ness
OpioidHypnotic
2
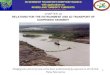
2. A hypothetical response surface. This graph shows the relationship between opioid (analgesic) and hypnotic (anaesthetic) drug concentrations and the probability of non-responsiveness. Point 1: complete responsiveness. Point 2 and the plateau above: no chance of response. The line at 3 shows the relationship between anaesthetic and responsiveness in the absence of opioid. The line at 4 shows the relationship between anaesthetic and responsiveness in the presence of large doses of opioid. Point 5 shows the area of maximum synergy between opioid and anaesthetic. Point 6 shows that, in the absence of anaesthetic, even very high levels of opioid cannot suppress response. The curved line across the middle of the surface is the 50% isobole: and the curved line across the top of the surface, the 95% isobole. These lines denote a 50% and 95% chance of non-responsiveness respectively

OUP CORRECTED PROOF – FINAL, 03/24/12, SPi
An
aest
hes
ia
18
On the other hand, EEG is non-invasive and compact, and a variety of anaesthetic monitors have been developed which measure a localized EEG signal, typically from the forehead, analyse it mathematically, and distil the result into a single number which can be interpreted by the anaesthetist. For example, 90 to 100 could indicate alertness, 70 to 80 sedation, 30 to 50 general anaesthesia, and zero cortical silence. These systems provide an objective measure of the cortical suppression produced by general anaesthesia.
Depth of anaesthesia is no longer considered to be a linear concept, as defi ned by Guedel, since it is clear that anaesthesia is not a single process. It is now believed that the two most important components of anaesthesia are unconsciousness and suppression of the stress response. These can be represented on a three-dimensional diagram called a response surface.
The response surface diagram pictured here is hypothetical. A genuine response surface specifi es the axes more specifi cally. For example, it might show the probability of elevation in blood pressure in response to varying concentrations of isofl urane (an anaesthetic) and remifentanil (an analgesic). True response surfaces are determined experimentally: a very time-consuming process. A complete understanding of anaesthetic effects would require response surfaces comparing every possible combination of anaesthetic drugs against every possible surgical stimulus. Although this is a very large task, considerable inroads are currently being made, and it is highly likely that this work will greatly improve our understanding of the processes of general anaesthesia. Ultimately, our understanding will be limited by the complexity of the brain itself, and the evanescent nature of human experience.