Embed Size (px)
Citation preview

�
� �
�
Chapter 1
Surgical Anatomy, Embryology, andPhysiology of the Salivary Glands
John D. Langdon, FKC, MB BS, BDS, MDS, FDSRCS, FRCS, FMedSciKing’s College, London, UK
Outline
IntroductionThe Parotid Gland
EmbryologyAnatomyContents of the Parotid Gland
The Facial NerveAuriculotemporal NerveRetromandibular VeinExternal Carotid ArteryParotid Lymph NodesParotid DuctNerve Supply to the Parotid
The Submandibular GlandEmbryologyAnatomy
The Superficial LobeThe Deep LobeThe Submandibular DuctBlood Supply and Lymphatic DrainageNerve Supply to the Submandibular Gland
Parasympathetic InnervationSympathetic InnervationSensory Innervation
The Sublingual GlandEmbryologyAnatomy
Sublingual DuctsBlood Supply, Innervation, and Lymphatic Drainage
Minor Salivary GlandsHistology of the Salivary GlandsControl of Salivation
Salivary Gland Pathology: Diagnosis and Management, Second Edition. Edited by Eric R. Carlson and Robert A. Ord.© 2016 John Wiley & Sons, Inc. Published 2016 by John Wiley & Sons, Inc.
SummaryReferences
Introduction
There are three pairs of major salivary glandsconsisting of the parotid, submandibular, andsublingual glands. In addition, there are numerousminor glands distributed throughout the oral cavitywithin the mucosa and submucosa.
On average, about 0.5 liters of saliva are pro-duced each day but the rate varies throughout theday. At rest, about 0.3 ml/min are produced but thisrises to 2.0 ml/min with stimulation. The contribu-tion from each gland also varies. At rest, the parotidproduces 20%, the submandibular gland 65%, andthe sublingual and minor glands 15%. On stimula-tion, the parotid secretion rises to 50%. The natureof the secretion also varies from gland to gland.Parotid secretions are almost exclusively serous, thesubmandibular secretions are mixed and the sublin-gual and minor gland secretions are predominantlymucinous.
Saliva is essential for mucosal lubrication,speech, and swallowing. It also performs an essen-tial buffering role that influences demineralizationof teeth as part of the carious process. Whenthere is a marked deficiency in saliva produc-tion, xerostomia, rampant caries, and destructiveperiodontal disease ensues. Various digestiveenzymes – salivary amylase – and antimicrobial
1

�
� �
�
2 Chapter 1
agents – IgA, lysozyme, and lactoferrin – are alsosecreted with the saliva.
The Parotid Gland
EMBRYOLOGY
The parotid gland develops as a thickening of theepithelium in the cheek of the oral cavity in the15 mm Crown Rump length embryo. This thicken-ing extends backwards towards the ear in a planesuperficial to the developing facial nerve. The deepaspect of the developing parotid gland producesbud like projections between the branches of thefacial nerve in the third month of intra-uterine life.These projections then merge to form the deeplobe of the parotid gland. By the sixth month ofintra-uterine life the gland is completely canalized.Although not embryologically a bilobed structure,the parotid comes to form a larger (80%) superfi-cial lobe and a smaller (20%) deep lobe joined byan isthmus between the two major divisions of thefacial nerve. The branches of the nerve lie betweenthese lobes invested in loose connective tissue.This observation is vital in the understanding ofthe anatomy of the facial nerve and surgery in thisregion (Berkovitz, et al. 2003).
ANATOMY
The parotid is the largest of the major salivaryglands. It is a compound, tubuloacinar, merocrine,
exocrine gland. In the adult, the gland is composedentirely of serous acini.
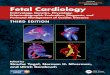
The gland is situated in the space between theposterior border of the mandibular ramus and themastoid process of the temporal bone. The exter-nal acoustic meatus and the glenoid fossa lie abovetogether with the zygomatic process of the tempo-ral bone (Figure 1.1). On its deep (medial) aspectlies the styloid process of the temporal bone. Infe-riorly, the parotid frequently overlaps the angle ofthe mandible and its deep surface overlies the trans-verse process of the atlas vertebra.
The shape of the parotid gland is variable.Often it is triangular with the apex directed inferi-orly. However, on occasion it is more or less of evenwidth and occasionally it is triangular with theapex superiorly. On average, the gland is 6 cm inlength with a maximum of 3.3 cm in width. In 20%of subjects a smaller accessory lobe arises fromthe upper border of the parotid duct approximately6 mm in front of the main gland. This accessorylobe overlies the zygomatic arch.
The gland is surrounded by a fibrous capsulepreviously thought to be formed from the investinglayer of deep cervical fascia. This fascia passesup from the neck and was thought to split toenclose the gland. The deep layer is attached to themandible and the temporal bone at the tympanicplate and styloid and mastoid processes (McMinn,et al. 1984; Berkovitz and Moxham 1988; Williams1995; Ellis 1997). Recent investigations suggestthat the superficial layer of the parotid capsule isnot formed in this way, but is part of the superficialmusculo-aponeurotic system (SMAS) (Mitz and
1 2
5
4
6
3
7
8
9
Figure 1.1. A lateral view of theskull showing some of the bonyfeatures related to the bed of theparotid gland. 1: Mandibular fossa;2: Articular eminence; 3: Tympanicplate; 4: Mandibular condyle; 5:Styloid process; 6: Ramus ofmandible; 7: Angle of mandible;8: Mastoid process; 9: Externalacoustic meatus. Source: SurgicalManagement of the InfratemporalFossa. (J. Langdon, B. Berkovitz &B. Moxham). ISBN 9781899066797.Reproduced with permission of Taylor& Francis Books UK.

�
� �
�
Surgical Anatomy, Embryology, and Physiology of the Salivary Glands 3
Peyronie 1976; Jost and Levet 1983; Wassef 1987;Thaller, et al. 1989; Zigiotti, et al. 1991; Gosain,et al. 1993; Flatau and Mills 1995). Anteriorly,the superficial layer of the parotid capsule is thickand fibrous but more posteriorly, it becomes athin translucent membrane. Within this fascia arescant muscle fibers running parallel with those ofthe platysma. This superficial layer of the parotidcapsule appears to be continuous with the fasciaoverlying the platysma muscle. Anteriorly, it formsa separate layer overlying the masseteric fascia,which is itself an extension of the deep cervicalfascia. The peripheral branches of the facial nerve
and the parotid duct lie within a loose cellularlayer between these two sheets of fascia. Thisobservation is important in parotid surgery. Whenoperating on the parotid gland, the skin flap caneither be raised in the subcutaneous fat layer ordeep to the SMAS layer. The SMAS layer itself canbe mobilized as a separate flap and can be used tomask the cosmetic defect following parotidectomyby reattaching it firmly to the anterior border of thesternocleidomastoid muscle as an advancementflap (Meningaud, et al. 2006).
The superior border of the parotid gland(usually the base of the triangle) is closely molded
1
22
5
4
6
3
7
8
9
10
11
11
1213
14
15
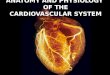
Figure 1.2. The parotid gland andassociated structures. 1: Auriculotem-poral nerve; 2: Superficial temporalvessels; 3: Temporal branch of facialnerve; 4: Zygomatic branch of facialnerve; 5: Buccal branch of facial nerve;6: Mandibular branch of facial nerve;7: Cervical branch of facial nerve; 8:Parotid duct; 9: Parotid gland; 10: Mas-seter muscle; 11: Facial vessels; 12:Platysma muscle; 13: External jugularvein; 14: Sternocleidomastoid muscle;15: Great auricular nerve. Source: Sur-gical Management of the Infratempo-ral Fossa. (J. Langdon, B. Berkovitz& B. Moxham). ISBN 9781899066797.Reproduced with permission of Taylor& Francis Books UK.

�
� �
�
4 Chapter 1
around the external acoustic meatus and the tem-poromandibular joint. An avascular plane existsbetween the gland capsule and the cartilaginousand bony acoustic meatus (Figure 1.2). The infe-rior border (usually the apex) is at the angle ofthe mandible and often extends beyond this tooverlap the digastric triangle where it may lie veryclose to the posterior pole of the submandibularsalivary gland. The anterior border just overlapsthe posterior border of the masseter muscle andthe posterior border overlaps the anterior borderof the sternocleidomastoid muscle.
The superficial surface of the gland is cov-ered by skin and platysma muscle. Some terminalbranches of the great auricular nerve also lie super-ficial to the gland. At the superior border of theparotid lie the superficial temporal vessels with theartery in front of the vein. The auriculotemporalbranch of the mandibular nerve runs at a deeperlevel just behind the superficial temporal vessels.
The branches of the facial nerve emergefrom the anterior border of the gland. The parotidduct also emerges to run horizontally across themasseter muscle before piercing the buccinatormuscle anteriorly to end at the parotid papilla. Thetransverse facial artery (a branch of the superficialtemporal artery) runs across the area parallel toand approximately 1 cm above the parotid duct.The anterior and posterior branches of the facialvein emerge from the inferior border.
The deep (medial) surface of the parotidgland lies on those structures forming the parotidbed. Anteriorly, the gland lies over the massetermuscle and the posterior border of the mandibularramus from the angle up to the condyle. As thegland wraps itself around the ramus it is related tothe medial pterygoid muscle at its insertion on tothe deep aspect of the angle. More posteriorly, theparotid is molded around the styloid process andthe styloglossus, stylohyoid, and stylopharyngeusmuscles from below upwards. Behind this, theparotid lies on the posterior belly of the digas-tric muscle and the sternocleidomastoid muscle.The digastric and the styloid muscles separatethe gland from the underlying internal jugularvein, the external and internal carotid arteriesand the glossopharyngeal, vagus, accessory, andhypoglossal nerves, and the sympathetic trunk.
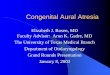
The fascia that covers the muscles in theparotid bed thickens to form two named liga-ments (Figure 1.3). The stylomandibular ligamentpasses from the styloid process to the angle of
Masseter muscle
Stylomandibularligament
Styloid process
Lateral pterygoidmuscle
Medial pterygoidmuscle Superior pharyngeal
constrictor muscle
Stylopharyngeusmuscle
Middle pharyngeal constrictor muscle
Inferior pharyngealconstrictor muscle
Mandibulo-stylohyoidligament
Posterior borderof ramus
Facial vein and artery
Submandibular gland
Figure 1.3. The mandibulostylohyoid ligament andsurrounding anatomy.
the mandible. The mandibulostylohyoid ligament(the angular tract) passes between the angle of themandible and the stylohyoid ligament. Inferiorly,it usually extends down to the hyoid bone. Theseligaments are all that separates the parotid glandanteriorly from the posterior pole of the superficiallobe of the submandibular gland.
CONTENTS OF THE PAROTID GLAND
The Facial NerveFrom superficial to deep, the facial nerve, theauriculotemporal nerve, the retromandibular vein,and the external carotid artery pass through thesubstance of the parotid gland.
The facial nerve exits the skull base at thestylomastoid foramen. The surgical landmarks areimportant (Figure 1.4). To expose the trunk of thefacial nerve at the stylomastoid foramen the dissec-tion passes down the avascular plane between theparotid gland and the external acoustic canal untilthe junction of the cartilaginous and bony canalscan be palpated. A small triangular extension of thecartilage points towards the facial nerve as it exitsthe foramen (Langdon 1998b). The nerve lies about

�
� �
�
Surgical Anatomy, Embryology, and Physiology of the Salivary Glands 5
Parotid gland
Sternocleidomastoidmuscle (SCM)
Posterior belly ofdigastric muscle(PBDM)
Styloid process(palpable through above lying
parotid tissue)
Tip of the mastoidprocess
Measurementsto root of facialnerve:
• 3cm from skin to root
• 4mm from junction of SCM and PBDM to root
Anterior border ofmasseter muscle
Pointer cartilage
3cm
4mm4mm
Figure 1.4. Anatomical landmarks of the extratemporalfacial nerve.
9 mm from the posterior belly of the digastric mus-cle and 11 mm from the bony external meatus (Holt1996). The facial nerve then passes downwards andforwards over the styloid process and associatedmuscles for about 1.3 cm before entering the sub-stance of the parotid gland (Hawthorn and Flatau1990). The first part of the facial nerve gives offthe posterior auricular nerve supplying the auricu-lar muscles and also branches to the posterior bellyof the digastric and stylohyoid muscles.
On entering the parotid gland the facialnerve divides into two divisions, temporofacialand cervicofacial, the former being the larger. Thedivision of the facial nerve is sometimes called thepes anserinus due to its resemblance to the footof a goose. From the temporofacial and cervico-facial divisions, the facial nerve gives rise to fivenamed branches – temporal, zygomatic, buccal,mandibular, and cervical (Figure 1.5). The periph-eral branches of the facial nerve form anastomoticarcades between adjacent branches to form theparotid plexus. These anastomoses are importantduring facial nerve dissection as accidental damageto a small branch often fails to result in any facialweakness due to dual innervation from adjacentbranches. Davis et al. (1956) studied these patternsfollowing the dissection of 350 facial nerves incadavers. The anastomotic relationships betweenadjacent branches fell into six patterns (Figure 1.6).They showed that in only 6% of cases (type VI)is there any anastomosis between the mandibular
Figure 1.5. Clinical photograph of dissected facial nervefollowing superficial parotidectomy.
branch and adjacent branches. This explains why,when transient facial weakness follows facial nervedissection, it is usually the mandibular branch thatis affected.
Auriculotemporal NerveThe auriculotemporal nerve arises from the pos-terior division of the mandibular division of thetrigeminal nerve in the infratemporal fossa. It runsbackwards beneath the lateral pterygoid musclebetween the medial aspect of the condylar neckand the sphenomandibular ligament. It enters theanteromedial surface of the parotid gland passingupwards and outwards to emerge at the superiorborder of the gland between the temporomandibu-lar joint and the external acoustic meatus. Thisnerve communicates widely with the temporofacialdivision of the facial nerve and limits the mobilityof the facial nerve during surgery (Flatau andMills 1995). Further communications with thetemporal and zygomatic branches loop around the

�
� �
�
6 Chapter 1
1
2
3
4
5
1
2
3
3
4
5
ll
1
2
3
4
5
lV
1
2
3
4
5
lll
12
3
4
5
V
12
3
4
5
Vl
l
Figure 1.6. The branching patterns of the facial nerve.
transverse facial and superficial temporal vessels(Bernstein and Nelson 1984).
Retromandibular VeinThe vein is formed within the parotid gland by theunion of the superficial temporal vein and the max-illary vein. The retromandibular vein passes down-wards and close to the lower pole of the parotidwhere it often divides into two branches passingout of the gland. The posterior branch passes back-wards to unite with the posterior auricular vein onthe surface of the sternocleidomastoid muscle toform the external jugular vein. The anterior branchpasses forward to join the facial vein.
The retromandibular vein is an importantlandmark during parotid gland surgery. The divi-sion of the facial nerve into its temporofacial andcervicofacial divisions occurs just behind the retro-mandibular vein (Figure 1.7). The two divisionslie just superficial to the vein in contact with it. Itis all too easy to tear the vein whilst exposing thedivision of the facial nerve!
External Carotid ArteryThe external carotid artery runs deeply within theparotid gland. It appears from behind the poste-rior belly of the digastric muscle and grooves theparotid before entering it. It gives off the posterior
auricular artery before ascending and dividing intoits terminal branches, the superficial temporal andmaxillary arteries at the level of the condyle. Thesuperficial temporal artery continues vertically toemerge at the superior border of the gland andcrosses the zygomatic arch. Within the substanceof the parotid it gives off the transverse facialartery, which emerges at the anterior border of thegland to run across the face above the parotid duct.The maxillary artery emerges from the deep aspectof the gland anteriorly to enter the infratemporalfossa. The maxillary artery gives off the deep auric-ular artery and the anterior tympanic artery withinthe substance of the parotid. All these branchesfrom the external carotid also give off numeroussmall branches within the parotid to supply thegland itself.
Parotid Lymph NodesLymph nodes are found within the subcutaneoustissues overlying the parotid to form the preau-ricular nodes and also within the substance ofthe gland. There are typically 10 nodes within thesubstance of the gland, the majority being withinthe superficial lobe and therefore superficial to theplane of the facial nerve. Only one or two nodes liewithin the deep lobe (Marks 1984; McKean, et al.1985; Garatea-Crelgo, et al. 1993). All the parotidnodes drain into the upper deep cervical chain.

�
� �
�
Surgical Anatomy, Embryology, and Physiology of the Salivary Glands 7
Figure 1.7. The facial nerve and itsrelationship to the retromandibular veinwithin the parotid gland. Source: SurgicalManagement of the Infratemporal Fossa.(J. Langdon, B. Berkovitz & B. Moxham).ISBN 9781899066797. Reproduced withpermission of Taylor & Francis Books UK.
1
25
4
6109
3
78
Parotid DuctThe parotid duct emerges from the anterior borderof the parotid gland and passes horizontally acrossthe masseter muscle. The surface markings of theduct are obtained by drawing a line from the lowestpoint of the alar cartilage to the angle of the mouth(Figure 1.8). This line is bisected and its midpoint isjoined with a straight line to the most anterior pointof the tragus. This line is divided into three equal
parts and the middle section corresponds to theposition of the parotid duct. The duct lies approxi-mately 1 cm below the transverse facial vessels. Theaccessory lobe of the parotid gland, when present,drains into its upper border via one or two tribu-taries. Anastomosing branches between the buccaland zygomatic branches of the facial nerve crossthe duct. At the anterior border of the masseter, theduct bends sharply to perforate the buccal pad of fat

�
� �
�
8 Chapter 1
Figure 1.8. The surface markings for the parotid duct.
and the buccinator muscle at the level of the uppermolar teeth. The duct then bends again to pass for-ward for a short distance before entering the oralcavity at the parotid papilla.
Nerve Supply to the ParotidThe parasympathetic secretomotor nerve supplycomes from the inferior salivatory nucleus in thebrain stem (Figure 1.9). From there, the fibers runin the tympanic branch of the glossopharyngealnerve contributing to the tympanic plexus in themiddle ear. The lesser petrosal nerve arises fromthe tympanic plexus leaving the middle ear andrunning in a groove on the petrous temporal bonein the middle cranial fossa. From here it exitsthrough the foramen ovale to the otic ganglion,which lies on the medial aspect of the mandibu-lar branch of the trigeminal nerve. Postsynapticpostganglionic fibers leave the ganglion to join
the auriculotemporal nerve, which distributes theparasympathetic secretomotor fibers throughoutthe parotid gland. Some authorities suggest thatthere are also some parasympathetic innervationsto the parotid from the chorda tympani branch ofthe facial nerve.
The sympathetic nerve supply to the parotidarises from the superior cervical sympathetic gan-glion. The sympathetic fibers reach the gland viathe plexus around the middle meningeal artery.They then pass through the otic ganglion withoutsynapsing and innervate the gland through theauriculotemporal nerve. There is also sympatheticinnervation to the gland arising from the plexusesthat accompany the blood vessels supplying thegland.
Sensory fibers arising from the connec-tive tissue within the parotid gland merge intothe auriculotemporal nerve and pass proximallythrough the otic ganglion without synapsing. Fromthere the fibers join the mandibular division of thetrigeminal nerve. The sensory innervation of theparotid capsule is via the great auricular nerve.
The Submandibular Gland
EMBRYOLOGY
The submandibular gland begins to form at the13 mm stage as an epithelial outgrowth into themesenchyme forming the floor of the mouth inthe linguogingival groove. This proliferates rapidlygiving off numerous branching processes, whicheventually develop lumina. Initially the developinggland opens into the floor of the mouth posteriorly,lateral to the tongue. The walls of the grooveinto which it drains come together to form thesubmandibular duct. This process commencesposteriorly and moves forwards so that ultimatelythe orifice of the duct comes to lie anteriorly belowthe tip of the tongue close to the midline.
ANATOMY
The submandibular gland consists of a largersuperficial lobe lying within the digastric trianglein the neck and a smaller deep lobe lying withinthe floor of the mouth posteriorly (Figure 1.10).The two lobes are continuous with each otheraround the posterior border of the mylohyoid mus-cle. As in the parotid gland, the two “lobes” are

�
� �
�
Surgical Anatomy, Embryology, and Physiology of the Salivary Glands 9
1
Mylohyoid muscle
Submandibular gland
Sublingual gland
Otic ganglion
Submandibular ganglion
Trigeminal ganglion
Facial nerve ganglion
Inferior ganglion (lX)
Tympanic plexus
lX= Glossopharyngeal nerve
Vll= Facial nerve
V3= Mandibular nerve
Parotid gland
Lesser petrosal nerve
Tympanic nerve
Chorda tympani nerve
Auriculotemporal nerve
Sensory root of facial nerve
Motor root of facial nerve
Trigeminal nerve
Lingual nerve
Medullaoblongata
Parasympathetic nerve fibers
2
3
5
6
lXVll
V3
Pons
4
1
1
2
3
5
6
4
Figure 1.9. The parasympathetic innervations of the salivary glands. The parasympathetic fibers are shown as blue lines.
not true lobes embryologically, as the gland arisesas a single epithelial outgrowth (Langdon 1998a).However, surgically it consists of the two lobes asdescribed previously. It is a mixed seromucinousgland.
The Superficial LobeThe superficial lobe lies within the digastric tri-angle. Its anterior pole reaches the anterior bellyof the digastric muscle and the posterior polereaches the stylomandibular ligament. This struc-ture is all that separates the superficial lobe of thesubmandibular gland from the parotid gland. It
is important to realize just how close the lowerpole of the parotid is to the posterior pole of thesubmandibular gland as confusion can arise if amass in the region is incorrectly ascribed to thewrong anatomical structure (Figure 1.2). Superi-orly, the superficial lobe lies medial to the bodyof the mandible. Inferiorly, it often overlaps theintermediate tendon of the digastric muscles andthe insertion of the stylohyoid muscle. The lobeis partially enclosed between the two layers ofthe deep cervical fascia that arise from the greatercornu of the hyoid bone and is in intimate prox-imity of the facial vein and artery (Figure 1.11).The superficial layer of the fascia is attached to

�
� �
�
10 Chapter 1
Submandibular gland,superficial lobe
(a)
(b)
(c)
Mylohyoid muscle(raphe)
Mylohyoid muscle
Facial vein
Wharton duct
Submandibular gland,deep lobe
Submandibular gland,deep lobe
Tongue
Submandibular gland,superficial lobe
Anterior belly ofdigastric muscle
Anterior belly ofdigastric muscle
Platysma muscle
Figure 1.10. The relationship of the superficial and deep lobes of the submandibular gland. (a) cross-sectional anatomy.(b) The superficial lobe from outside. (c) The relationship of the deep and superficial lobes to the mylohyoid muscle.

�
� �
�
Surgical Anatomy, Embryology, and Physiology of the Salivary Glands 11
Figure 1.11. Superficial dissection of the left submandibu-lar gland. The investing layer of the deep cervical fascia iselevated off of the submandibular gland and the facial veinis identified.
the lower border of the mandible and covers theinferior surface of the superficial lobe. The deeplayer of fascia is attached to the mylohyoid lineon the inner aspect of the mandible and thereforecovers the medial surface of the lobe.
The inferior surface, which is covered by skin,subcutaneous fat, platysma, and the deep fascia, iscrossed by the facial vein and the cervical branchof the facial nerve, which loops down from theangle of the mandible and subsequently innervatesthe lower lip. The submandibular lymph nodeslie between the salivary gland and the mandible.Sometimes one or more lymph nodes may beembedded within the salivary gland.
The lateral surface of the superficial lobe isrelated to the submandibular fossa, a concavity onthe medial surface of the mandible, and the attach-ment of the medial pterygoid muscle. The facialartery grooves its posterior part lying at first deep tothe lobe and then emerging between its lateral sur-face and the mandibular attachment of the medialpterygoid muscle from which it reaches the lowerborder of the mandible.
The medial surface is related anteriorly to themylohyoid from which it is separated by the mylo-hyoid nerve and submental vessels. Posteriorly, it isrelated to styloglossus muscle, the stylohyoid liga-ment, and the glossopharyngeal nerve separating itfrom the pharynx. Between these, the medial aspect
Figure 1.12. Deep dissection of the left submandibulargland. With the submandibular gland retracted, the facialartery is identified in proximity to the facial vein.
of the lobe is related to hyoglossus muscle fromwhich it is separated by styloglossus muscle, thelingual nerve, submandibular ganglion, hypoglos-sal nerve, and deep lingual vein. More inferiorly,the medial surface is related to the stylohyoid mus-cle and the posterior belly of digastric.
The Deep LobeThe deep lobe of the gland arises from the superfi-cial lobe at the posterior free edge of the mylohyoidmuscle and extends forward to the back of thesublingual gland (Figure 1.12). It lies betweenmylohyoid inferolaterally, hyoglossus, and sty-loglossus muscles medially, the lingual nervesuperiorly, and the hypoglossal nerve and deeplingual vein inferiorly.
The Submandibular DuctThe submandibular duct is about 5 cm long inthe adult. The wall of the submandibular ductis thinner than that of the parotid duct. It arisesfrom numerous tributaries in the superficial lobeand emerges from the medial surface of this lobejust behind the posterior border of the mylohy-oid. It crosses the deep lobe, passing upwardsand slightly backwards for 5 mm before runningforwards between the mylohyoid and hyoglossus

�
� �
�
12 Chapter 1
muscles. As it passes forward, it runs between thesublingual gland and genioglossus to open into thefloor of the mouth on the summit of the sublingualpapilla at the side of the lingual frenum just belowthe tip of the tongue. It lies between the lingualand hypoglossal nerves on the hyoglossus. At theanterior border of hyoglossus muscle it is crossedby the lingual nerve. As the duct traverses the deeplobe of the gland it receives tributaries drainingthat lobe.
Blood Supply and Lymphatic DrainageThe arterial blood supply arises from multiplebranches of the facial and lingual arteries. Venousblood drains predominantly into the deep lingualvein. The lymphatics drain into the deep cervicalgroup of nodes, mostly into the jugulo-omohyoidnode, via the submandibular nodes.
Nerve Supply to the Submandibular GlandParasympathetic InnervationThe secretomotor supply to the submandibulargland arises from the submandibular (sublingual)ganglion. This is a small ganglion lying on theupper part of the hyoglossus muscle. There areadditional ganglion cells at the hilum of the gland.The submandibular ganglion is suspended from thelingual nerve by anterior and posterior filaments(Figure 1.13).
Figure 1.13. Clinical photograph showing the relationshipof the lingual nerve to the submandibular gland.
The parasympathetic secretomotor fibers orig-inate in the superior salivatory nucleus and the pre-ganglionic fibers then travel via the facial nerve,chorda tympani, and lingual nerve to the ganglionvia the posterior filaments connecting the ganglionto the lingual nerve. They synapse within the gan-glion and the postganglionic fibers innervate thesubmandibular and sublingual glands (Figure 1.9).Some fibers are thought to reach the lower pole ofthe parotid gland.
Sympathetic InnervationThe sympathetic root is derived from the plexuson the facial artery. The postganglionic fibersarise from the superior cervical ganglion andpass through the submandibular ganglion withoutsynapsing. They are vasomotor to the vessels sup-plying the submandibular and sublingual glands.Five or six branches from the ganglion supply thesubmandibular gland and its duct. Others passback into the lingual nerve via the anterior fila-ment to innervate the sublingual and other minorsalivary glands in the region.
Sensory InnervationSensory fibers arising from the submandibular andsublingual glands pass through the ganglion with-out synapsing and join the lingual nerve, itself abranch of the trigeminal nerve.
The Sublingual Gland
EMBRYOLOGY
The sublingual gland arises in 20 mm embryosas a number of small epithelial thickenings in thelinguogingival groove and on the outer side of thegroove. Each thickening forms its own canal andso many of the sublingual ducts open directly ontothe summit of the sublingual fold. Those that arisewithin the linguogingival grove end up draininginto the submandibular duct.
ANATOMY
The sublingual gland is the smallest of the majorsalivary glands. It is almond shaped and weighsapproximately 4 g. It is predominantly a mucousgland. The gland lies on the mylohyoid and is

�
� �
�
Surgical Anatomy, Embryology, and Physiology of the Salivary Glands 13
covered by the mucosa of the floor of the mouth,which is raised as it overlies the gland to form thesublingual fold. Posteriorly, the sublingual gland isin contact with the deep lobe of the submandibulargland. The sublingual fossa of the mandible islocated laterally and the genioglossus muscle islocated medially. The lingual nerve and the sub-mandibular duct lie medial to the sublingual glandbetween it and the genioglossus.
Sublingual DuctsThe gland has a variable number of excretory ductsranging from 8 to 20. The majority drain into thefloor of the mouth at the crest of the sublingual fold.A few drain into the submandibular duct. Some-times, a collection of draining ducts coalesce ante-riorly to form a major duct (Bartholin’s duct) whichopens with the orifice of the submandibular duct atthe sublingual papilla.
Blood Supply, Innervation, and LymphaticDrainageThe arterial supply is from the sublingual branchof the lingual artery and also the submental branchof the facial artery. Innervation is via the sublingualganglion as described above. The lymphatics drainto the submental nodes.
Minor Salivary Glands
Minor salivary glands are distributed widely in theoral cavity and oropharynx. They are grouped aslabial, buccal, palatoglossal, palatal, and lingualglands. The labial and buccal glands contain bothmucous and serous acini, whereas the palatoglos-sal glands are mucous secreting. The palatal glandsthat are also mucous secreting occur in both thehard and soft palates. The anterior and posteriorlingual glands are mainly mucous. The anteriorglands are embedded within the muscle ventrallyand they drain via four or five ducts near thelingual frenum. The posterior lingual glands arelocated at the root of the tongue. The deep pos-terior lingual glands are predominantly serous.Additional serous glands (of von Ebner) occuraround the circumvallate papillae on the dorsumof the tongue. Their watery secretion is thought tobe important in spreading taste stimuli over thetaste buds.
Histology of the Salivary Glands
The salivary glands are composed of large num-bers of secretory acini, which may be tubular orglobular in shape. Each acinus drains into a duct.These microscopic ducts coalesce to form lobularducts. Each lobule has its own duct and these thenmerge to form the main ducts. The individual lobesand lobules are separated by dense connective tis-sue which is continuous with the gland capsule.The ducts, blood vessels, lymphatics, and nervesrun through and are supported by this connectivetissue.
The acini are the primary secretory organsbut the saliva is modified as it passes through theintercalated, striated, and excretory ducts beforebeing discharged into the mouth and oropharynx(Figure 1.14). The lobules also contain signifi-cant amounts of adipose tissue particularly in theparotid gland. The proportion of adipose tissuerelative to excretory acinar cells increases with age.
In the human parotid, the excretory aciniare almost entirely serous. In the submandibulargland, again, the secretory units are mostly serousbut there are additional mucous tubules and acini.In some areas the mucinous acini have crescentic“caps” of serous cells called serous demilunes. Inthe sublingual gland the acini are almost entirelymucinous, although there are occasional serousacini or demilunes.
The serous cells contain numerous proteina-ceous secretory (zymogen) granules. These gran-ules contain high levels of amylase. In addition, thesecretory cells produce kallikrein, lactoferrin, andlysozyme. In mucous cells, the cytoplasm is packedwith large pale secretory droplets.
Initially the secretory acini drain into inter-calated ducts. These function mainly to conductthe saliva but they may also modify the elec-trolyte content and secrete immunoglobulin A. Theintercalated ducts drain into striated ducts, whichcoalesce into intralobular and extralobular col-lecting ducts. The intercalated duct cells are veryactive metabolically and they transport potassiumand bicarbonate into saliva. They reabsorb sodiumand chloride ions so that the resulting saliva ishypotonic. They also secrete immunoglobulin A,lysozyme, and kallikrein. The immunoglobulin isproduced by plasma cells adjacent to the striatedduct cells and it is then transported through theepithelial lining into the saliva. The main collecting

�
� �
�
14 Chapter 1
Immunoglobulin
LysozymeKallikreinK+
Serousdemilune
Junctions betweenstrated duct cells and cholinergic axon
Junctions betweenintercalated duct cellsand cholinergic axon
Production and secretionof proteinaceousand enzymatic materialswithin secretory vesicles
Production andsecretionof -amylase,perioxidase,prolone-rich proteins
Tight junctions
Flattenedbasal nucleus
Secretory granules
Intercellularsecretorycanaliculus
To interlobular excretory ducts
Cytoplasmicprocesses
Actin myofilaments
Arteriolewith adrenergicnerve terminals Spherical nucleus
Mitochondria
Basal infoldings- increasesurface area
Basal invaginationsand mitochondria
yield striatedappearance
Centrallylocatednucleus Rough ER
Dense apicalmicrofilaments
Desmosomes
Large, spherical,centrally located
nucleus
Microvilli
Secretory endpiece,with adrenergic andcholinergic nerveterminals
Cholinergicaxons
Adrenergicaxons
Intercalated duct cell
Mucous cell
Myoepithelial cell
Striated duct cell
Serous cell
A
A’
B
B’
C
C’
D
D’
Na+
Cl
E
E’
Figure 1.14. Diagram showing the histology of the major components of the salivary glands.
ducts are simple conduits for saliva and do notmodify the composition of the saliva.
Myoepithelial cells are contractile cells closelyrelated to the secretory acini and also much of theduct system. The myoepithelial cells lie betweenthe basal lamina and the epithelial cells. Numer-ous cytoplasmic processes arise from them and
surround the serous acini as basket cells. Thoseassociated with the duct cells are more fusiformand are aligned along the length of the ducts. Thecytoplasm of the myoepithelial cells contains actinmyofilaments which contract as a result of bothparasympathetic and sympathetic activity. Thus,the myoepithelial cells “squeeze” the saliva out

�
� �
�
Surgical Anatomy, Embryology, and Physiology of the Salivary Glands 15
of the secretory acini and ducts and add to thesalivary secretory pressure.
Control of Salivation
There is a continuous low background saliva pro-duction, which is stimulated by drying of the oraland pharyngeal mucosa. A rapid increase in theresting levels occurs as a reflex in response to mas-ticatory stimuli including the mechanoreceptorsand taste fibers. Other sensory modalities such assmell are also involved. The afferent input is viathe salivatory centers, which are themselves influ-enced by the higher centers. The higher centersmay be facilitory or inhibitory, depending on thecircumstances. The efferent secretory drive to thesalivary glands passes via the parasympathetic andsympathetic pathways. There are no peripheralinhibitory mechanisms.
Cholinergic nerves (parasympathetic) oftenaccompany ducts and branch freely around thesecretory endpieces (acini). Adrenergic nerves(sympathetic) usually enter the glands along thearteries and arterioles and ramify with them.Within the glands, the nerve fibers interminglesuch that cholinergic and adrenergic axons fre-quently lie in adjacent invaginations of a singleSchwann cell. Secretion and vasoconstriction aremediated by separate sympathetic axons whereasa single parasympathetic axon may, through serialterminals, result in vasodilatation, secretion, andconstriction of myoepithelial cells.
Secretory endpieces are the most denselyinnervated structures in the salivary glands. Indi-vidual acinar cells may have both cholinergic andadrenergic nerve endings. The secretion of waterand electrolytes, which accounts for the volumeof saliva produced, results from a complex set ofstimuli which are largely parasympathetic. Theactive secretion of proteins into the saliva dependsupon the relative levels of both sympathetic andparasympathetic stimulation.
Although the ducts are less densely inner-vated than secretory acini, they do influence thecomposition of the saliva. Adrenal aldosteronepromotes resorption of sodium and secretion ofpotassium into the saliva by striated ductal cells.Myoepithelial cell contraction is stimulated pre-dominantly by adrenergic fibers, although theremay be an additional role for cholinergic axons.
Summary
• Although embryologically the parotid consistsof a single lobe, anatomically the facial nervelies in a distinct plane between the anatomicalsuperficial and deep lobes.
• There are fixed anatomical landmarks indicat-ing the origin of the extracranial facial nerve asit leaves the stylomastoid foramen.
• The lower pole of the parotid gland is sepa-rated from the posterior pole of the subman-dibular gland by only thin fascia. This can leadto diagnostic confusion in determining the ori-gin of a swelling in this area.
• The relationship of the submandibular salivaryduct to the lingual nerve is critical to the saferemoval of stones within the duct
• Great care must be taken to identify the lin-gual nerve when excising the submandibulargland. The lingual nerve is attached to thegland by the parasympathetic fibers synapsingin the submandibular (sublingual) ganglion.
• The sublingual gland may drain into the sub-mandibular duct or it may drain directly intothe floor of the mouth via multiple secretoryducts.
References
Berkovitz BKB, Langdon JD, Moxham BJ. 2003. The facialnerve and the parotid gland. In: Langdon, JD, Berkovitz,BKB, Moxham, BJ (eds), Surgical Anatomy of theInfratemporal Fossa. London, Martin Dunit, pp. 181–206.
Berkovitz BKB, Moxham BJ. 1988. A Textbook of Head andNeck Anatomy. London, Wolfe.
Bernstein L, Nelson RH. 1984. Surgical anatomy of the extra-parotid distribution of the facial nerve. Arch Otolaryngol110:177–183.
Davis RA, Anson BJ, Budinger JM, Kurth LE. 1956. Sur-gical anatomy of the facial nerve and parotid glandbased on 350 cervicofacial halves. Surg Gynecol Obstet102:385–412.
Ellis H. 1997. Clinical Anatomy, 9th edn. Oxford, Blackwell.Flatau AT, Mills PR. 1995. Regional anatomy. In: Norman JE
deB, McGurk M (eds), Color Atlas and Text of the SalivaryGlands. London, Mosby Wolfe, pp. 13–39.
Garatea-Crelgo J, Gay-Escoda C, Bermejo B, Buenechea-Imaz R. 1993. Morphological studies of the parotid lymphnodes. J Cranio-Maxillo-Facial Surg 21:207–209.
Gosain AK, Yousif NJ, Madiedo G, et al. 1993. Surgicalanatomy of the SMAS: a reinvestigation. Plast ReconstrSurg 92:1254–1263.

�
� �
�
16 Chapter 1
Hawthorn R, Flatau A. 1990. Temporomandibular jointanatomy. In: Norman JE deB, Bramley P (eds), A Text-book and Colour Atlas of the Temporomandibular Joint.London, Mosby Wolfe, pp. 1–51.
Holt JJ. 1996. The stylomastoid area: anatomic-histologicstudy and surgical approach. Laryngoscope 106:396–399.
Jost G, Levet Y. 1983. Parotid fascia and face lifting: a crit-ical evaluation of the SMAS concept. Plast Reconstr Surg74:42–51.
Langdon JD. 1998a. Sublingual and submandibular glandexcision. In: Langdon JD, Patel MF (eds), Operative Max-illofacial Surgery. London, Chapman & Hall, pp. 376–380.
Langdon JD. 1998b. Parotid surgery. In: Langdon JD,Patel MF (eds), Operative Maxillofacial Surgery. London,Chapman & Hall, pp. 386–388.
Marks NJ. 1984. The anatomy of the lymph nodes of theparotid gland. Clin Otolaryngol 9:271–275.
McKean ME, Lee K, McGregor IA. 1984. The distribution oflymph nodes in and around the parotid gland: an anatom-ical study. Br J Plast Surg 38:1–5.
McMinn RMH, Hutchings RT, Logan BM. 1984. A ColourAtlas of Applied Anatomy. London, Wolfe.
Meningaud J-P, Bertolus C, Bertrand J-C. 2006. Parotidec-tomy: Assessment of a surgical technique includingfacelift incision and SMAS advancement. J Cranio-Maxillofacial Surg 34:34–37.
Mitz V, Peyronie M. 1976. The superficial musculo-aponeurotic system (SMAS) in the parotid and cheekarea. Plast Reconstr Surg 58:80–88.
Thaller SR, Kim S, Patterson H, et al. 1989. The submuscularaponeurotic system (SMAS): a histologic and comparativeanatomy evaluation. Plast Reconstr Surg 86:691–696.
Wassef M. 1987. Superficial fascia and muscular layers inthe face and neck: a histological study. Aesthetic PlastSurg 11:171–176.
Williams PL. 1995. (ed.). Gray’s Anatomy, 38th edn.New York, Churchill Livingstone.
Zigiotti GL. Liverani MB, Ghibellini D. 1991. The relation-ship between parotid and superficial fasciae. Surg RadiolAnat 13:293–300.

�
� �
�
Chapter 2
Diagnostic Imaging of Salivary GlandPathology
Pradeep K. Jacob, MD, MBA1 and J. Michael McCoy, DDS2
1Department of Radiology, University of Tennessee at Chattanooga,
College of Medicine, Chattanooga, TN, USA2Departments of Oral and Maxillofacial Surgery, Pathology, and Radiology,
University of Tennessee Medical Center, Knoxville, TN, USA
Outline
IntroductionImaging Modalities
Computed Tomography (CT)CT Technique
Advanced Computed TomographyMagnetic Resonance Imaging (MRI)
MRI TechniqueSpin Echo T1Spin Echo T2Proton Density Images (PD)Gradient Recalled Echo Imaging (GRE)Short Tau Inversion Recovery (STIR)Gadolinium (Gd) ContrastFluid Attenuation Inversion Recovery (FLAIR)Diffusion Weighted Images (DWI)MR Spectroscopy (MRS)Dynamic Contrast Enhanced Magnetic Resonance
ImagingOther Magnetic Resonance Imaging Techniques
Ultrasonography (US)Ultrasound Technique
SialographyRadionuclide Imaging (RNI)Positron Emission
Tomography (PET)Positron Emission Tomography/
Computed Tomography (PET/CT)Diagnostic Imaging Anatomy
Parotid GlandsSubmandibular GlandsSublingual GlandsMinor Salivary Glands
Salivary Gland Pathology: Diagnosis and Management, Second Edition. Edited by Eric R. Carlson and Robert A. Ord.© 2016 John Wiley & Sons, Inc. Published 2016 by John Wiley & Sons, Inc.
Pathology of the Salivary GlandsVascular Lesions
Lymphangioma (Cystic Hygroma)Hemangioma
Acute SialadenitisChronic SialadenitisHIV−Lymphoepithelial LesionsMucous Escape PhenomenaSialadenosis (sialosis)SialolithiasisSjogren SyndromeSarcoidosisCongenital Anomalies
of the Salivary GlandsFirst Branchial Cleft Cyst
Neoplasms – Salivary, EpithelialBenign
Pleomorphic AdenomaWarthin TumorOncocytoma
MalignantMucoepidermoid CarcinomaAdenoid Cystic Carcinoma
Neoplasms – Non-SalivaryBenign
LipomaNeurogenic Tumors
MalignantLymphomaMetastases
SummaryReferences
17

�
� �
�
18 Chapter 2
Introduction
Anatomic and functional diagnostic imaging playsa central role in modern medicine. Virtually allspecialties of medicine to varying degrees dependon diagnostic imaging for diagnosis, therapy, andfollow-up of treatment. Because of the complexityof the anatomy, treatment of diseases of the headand neck, including those of the salivary glands,are particularly dependent on quality medicalimaging and interpretation. Medical diagnosticimaging is divided primarily into two major cat-egories, anatomic and functional. The anatomicimaging modalities include computed tomogra-phy (CT), magnetic resonance imaging (MRI),and ultrasonography (US). Although occasionallyobtained, plain film radiography for the head andneck, including salivary gland disease, is mostlyof historical interest. In a similar manner, the useof sialography has been significantly reduced,although both plain films and sialography are ofsome use in imaging sialoliths. Functional diagnos-tic imaging techniques include planar scintigraphy,single photon emission computed tomography(SPECT), positron emission tomography (PET),and magnetic resonance spectroscopy (MRS), all ofwhich are promising technologies. Recently, the useof a combined anatomic and functional modality inthe form of PET/CT has proved invaluable in headand neck imaging. Previously widely employedprocedures including gallium radionuclide imagingare less important today than in the past.
Imaging Modalities
COMPUTED TOMOGRAPHY (CT)
CT has become indispensable in the diagnosis,treatment and follow-up of diseases of the headand neck. The latest generation of multiple-rowdetector CT (MDCT) provides excellent soft-tissueand osseous delineation. The rapid speed withwhich images can be obtained along with thehigh spatial resolution and tissue contrast makesCT the imaging modality of choice in head andneck imaging. True volumetric data sets obtainedfrom multidetector row scanners allow for excel-lent coronal, sagittal or oblique reformation ofimages as well as a variety of 3-D renderings. Thisallows the radiologist and surgeon to characterizea lesion, assess involvement of adjacent structures
or local spread from the orthogonal projections or3-D rendering. The ability to manipulate imagesis critical when assessing pathology in complexanatomy, such as evaluation of parotid glandmasses to determine deep lobe involvement, facialnerve involvement, or extension into the skullbase. Images in the coronal plane are importantin evaluating the submandibular gland in relationto the floor of mouth. Lymphadenopathy and itsrelationship to the carotid sheath and its contentsand other structures are also well delineated. CT isalso superior to MRI in demonstrating bone detailand calcifications. CT is also the fastest method ofimaging head and neck anatomy. Other advantagesinclude widespread availability of scanners, highresolution images, and speed of image acquisitionalso reduces motion artifacts. Exposure to ionizingradiation and the administration of IV contrast arethe only significant disadvantages to CT scanning.
CT TechniqueThe CT scanner contains a gantry, which holds anX-ray tube and a set of detectors. The X-ray tubeis positioned opposite the detectors and is physi-cally coupled. A “fan beam” of X-rays is producedand passes through the patient to the detectors asthe tube and detector rotate around the patient. Innewer generation of scanners, the multiple rows ofdetectors are fixed around the gantry and only thetube rotates. A table carries the patient through thegantry. The detectors send signals, dependent onthe degree of X-ray attenuation, to a computer thatuses this data to construct an image using complexalgorithms.
For most CT studies (especially in the headand neck) intravenous contrast is administered. IVcontrast is a solution consisting of organic com-pounds bonded with Iodine molecules. Iodine is adense atom with an atomic weight of 127, whichis good at absorbing X-rays and is biocompatible.IV contrast readily attenuates the X-ray beam atconcentrations optimal for vascular and soft tissue“enhancement,” but short of causing attenuationrelated artifacts. Streak artifacts, however, canoccur if the concentration is too high, as seen occa-sionally at the thoracic inlet and supraclavicularregion from dense opacification of the subclavianvein during rapid bolus injection of IV contrast.
CT of the neck should be performed withintravenous contrast whenever possible to opti-mize delineation of masses, inflammatory or

�
� �
�
Diagnostic Imaging of Salivary Gland Pathology 19
Figure 2.1. Axial CT of the neck in soft tissue window with-out contrast demonstrating poor definition between softtissue structures. The blood vessels are unopacified andcannot be easily distinguished from lymph nodes. Note thesialolith (arrow) in the hilum of the left submandibular gland.
infectious changes in the tissues, and enhancevascular structures. Imaging is obtained from thelevel of the orbits through the aortic arch in theaxial plane with breath hold. The images are recon-structed using a computer algorithm to optimizesoft tissue delineation, and displayed in soft tissuewindow and level settings (Figures 2.1 and 2.2). Ina similar manner images are reconstructed usinga computer algorithm to optimize bone details asmore sharp and defined (Figure 2.3). The lungapex is often imaged in a complete neck evalu-ation and displayed using lung window settings(Figure 2.4a). Dedicated CT scans of the chestare beneficial in the postoperative evaluation ofpatients with salivary gland malignancies as lungnodules can be observed, possibly indicative ofmetastatic disease (Figure 2.4b). Multiplanar refor-matted images of the neck are obtained typicallyin the coronal and sagittal planes, (Figures 2.5 and2.6), although they may be obtained in virtuallyany plane desired or in a 3-D rendering.
The Hounsfield unit (H) (named after GodfreyHounsfield, inventor of the CT scanner) is the unitof density measurement for CT. These units areassigned based on the degree of attenuation of
Figure 2.2. Axial CT of the neck in soft tissue window withIV contrast demonstrates improved visualization of struc-tures with enhancement of tissues and vasculature. Notethe small lipoma (arrow) anterior to the left submandibulargland, which distorts the anterior aspect of the gland withslight posterior displacement.
Figure 2.3. Axial CT of the skull base reconstructed ina sharp algorithm and in bone window and level displaydemonstrating sharp bone detail. Note the sharply definednormal right stylomastoid foramen (arrow).

�
� �
�
20 Chapter 2
(a)
(b)
Figure 2.4. Axial CT of the neck at the thoracic inlet inlung windows demonstrating lung parenchyma (a). Axialimage of dedicated CT of chest demonstrating cannon balllesions in a patient previously treated for adenoid cysticcarcinoma of the palate (b). These lesions are represen-tative of diffuse metastatic disease of the lungs, but notpathognomonic of adenoid cystic carcinoma.
the X-ray beam by tissue in a given voxel (volumeelement) and are assigned relative to water (0 H)(Table 2.1). The scale ranges from −1024 H for air,to +4000 H for very dense bone. The images arecreated based on a grayscale from black (−1024H) to white (+4000 H) and shades of gray. Despite
Figure 2.5. Coronal CT reformation of the neck in softtissue window at the level of the submandibular glands.Orthogonal images with MDCT offer very good soft tissuedetail in virtually any plane of interest in order to assessanatomic and pathologic relationships.
Figure 2.6. Sagittal CT reformation of the neck in softtissue window at the level of the parotid gland. Notethe accessory parotid gland (black arrow) sitting atopthe parotid (Stensen) duct (thin white arrow). Also note theretromandibular vein (large white arrow) and external audi-tory canal.