Upload
smey204
View
232
Download
0
Embed Size (px)
Citation preview
8/11/2019 Chapter 13 Pharynx
1/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm
Print | Close Windo
Note:Large images and tables on this page may necessitate printing in landscape mode.
Skandalakis' Surgical Anatomy > Chapter 13. Pharynx >
HISTORY
The anatomic and surgical history of the pharynx is shown in Table 13-1.
Table 13-1. Anatomic and Surgical History of the Pharynx
Morgagni 1717 Described the pharyngeal sinus of Morgagni, a space in the nasopharynx between the upper border of the superior constrictor muscle and the
base of the s kull
Rosenmller 1808 Described the lateral pharyngeal recess (fossa of Rosenmller)
Zukerkandl 1882 Described the pharyngeal tonsil
Mikulicz 1886 Reconstructed esophageal and pharyngeal stomas with inverted skin flaps
Beck 1905 Used reversed gastric tube
Jianu 1912
Gavriliu &
Georgescu
1951
Roux 1907 Used jejunum as pedicle graft
Herzen 1908
Vullie t 1911 Used transverse co lon for reconstruct ion
Kelling 1911
Trotter 1913 Reconstructed the posterior and anterior hypopharyngeal wall with horizontal skin flaps
Kirschner 1920 Pioneered gastric transplantation, bringing the stomach to the neck
Wookey 1942 Developed a two-staged repair: doubled a long, full-thickness cervical pedicle flap and sutured it to the pharynx and esophagus, closing the
raw surface; repaired the fistula later by undercutting and suturing the skin margins
Hynes 1950 Performed pharyngoplasty by muscle transplantation, producing a sphincterlike mechanism
Goligher &
Robin
1954 Used left colon for reconstruction via presternal route
Asherson 1954 Performed partial excision of the posterior wall of the pharynx for carcinoma and used the proximal laryngotrachea l tube for reconstruction
Seidenberg
et al.
1959 Developed microvascular technique using jejunum and anastomosing the mesenteric vesse ls to the superior thyroid artery and ante rior facial
vein
Ong & Lee 1960 Performed pharyngogastric anastomosis after esophagopharyngectomy for correction of the laryngopharynx and cervical esophagus
Iskeceli 1962 Experimented with jejunal transplant to the pharynx in experimental animals
Bakamjian 1965 Used deltopectoral flap for pharyngoesophageal reconstruction
Ogura &
Dedo
1965 Used thoracoacromial flap to repair a pharyngostoma
Yamagishi et
al.
1970 Replaced esophagus up to the pharynx with a totally detached isoperistaltic gastric tube
Ariyan 1979 Used pectoralis major muscle flap for pharyngoesophageal reconstruction
McLear et al. 1991 Used jejunal free flap for reconstruction of hypopharyngeal stricture
Anthony et
al.
1994 Performed pharyngoesophageal reconstruction with radial forearm free flap
Wax et al. 1996 Reconstructed the oropharynx with lateral arm free flap
History table compiled by David A. McClusky III and John E. Skandalakis.
References
Missotten FEM. Historical review of pharyngo-oesophageal reconstruction after resection for carcinoma of pharynx and cervical oesophagus. Clin Otolaryngol
1983;8:345-362.
Pigott RW. The results o f pharyngoplasty by muscle transp lantation by W ilfred Hynes. Br J Plast Surg 1993;46:440-442.
Schmidt JE. Medical Discoveries: Who and W hen. Springfield, IL: Charles C. Thomas, 1959.
EMBRYOGENESIS
Normal Development
To understand the anatomy of the pharynx and its associated arteries and nerves and to avoid possible complications related to surgical treatment of
congenital lesions in this relatively inaccessible area, a thorough knowledge of the basic embryologic development of the pharynx is imperative. The pharynx
is a product of differentiation of the embryonic foregut. It occupies a major portion of the foregut in the first few weeks of embryonic development and
precedes the appearance of the more caudal regions. The cranial portion of the foregut transforms from a flat tube into a complicated collection of
structures between the fourth and sixth weeks of embryogenesis.
8/11/2019 Chapter 13 Pharynx
2/40
8/11/2019 Chapter 13 Pharynx
3/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 3
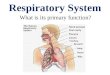
The branchial arch system. The arch system appears in the fourth and fifth gestational weeks as four prominent arches, each consisting of muscular and
cartilaginous components, a nerve, and a n artery. (From Sadler TW. Langman's Med ical Embryology, 8th ed. Philadelphia: Lippincott Williams & W ilkins, 2000; with
permission.)
In the adult pharynx, the eustachian tube and the tonsillar fossa represent derivatives of the first and second branchial pouches respectively. The third
pouch is near the entry of the piriform recess, and the fourth is near the apex. Laryngeal ventricles may be related to the fifth and sixth pouches.
Congenital Anomalies of the Pharynx
Anomalies of the Lateral Branchial Apparatus
Epithelium-lined cysts, sinuses, and fistulas may occur as a result of malfunction in the normal differentiation process of the branchial apparatus.
Understanding the anomalies of the branchial apparatus helps the surgeon predict the location and course of these lesions and surrounding important norma
structures, and thus to avoid their injury at surgery.
First Cleft and Pouch Defects
The fistulas, sinuses, and cysts of the first branchial cleft are intimately related to the external auditory canal and the facial nerve; they are presented in
the chapter on the neck. First pouch defects are rare, but may present as nasopharyngeal cysts (Fig. 13-2). The opening of the sinuses can be near the
eustachian cushion.
Fig. 13-2.
Conge nital cervicoaural fistula or cyst. This is a persiste nt remnant of the ventral portion of the first branchial cleft. The tract may or may not open into the external
auditory canal. (Modified from Skandalakis JE, Skandalakis PN, Skandalakis LJ. Surgical Anatomy and Technique: A Pocket Manua l, 2nd Ed. New York: Springer,
2000; with pe rmission.)
Second Cleft and Pouch Defects
Second cleft and pouch defects may involve the pharynx. Therefore these lesions and their courses are pertinent to understanding the pharynx.
8/11/2019 Chapter 13 Pharynx
4/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 4
COMPLETE FISTULAS
Almost all complete branchial fistulas are derived from the ventral portion of the second cleft and pouch. The external opening is in the lower third of the
neck, anterior to the sternocleidomastoid muscle. The fistula passes through the deep fascia to reach the carotid sheath. Above the hyoid, the tract turns
medially. It passes over and in front of the hypoglossal nerve and between the carotid bifurcation. It enters the pharynx on the anterior face of the
superior half of the posterior tonsillar pillar. Alternatively, the opening can be into the tonsil itself. Figure 13-3 depicts the course of the fistula of the
second branchial cleft and pouch.
Fig. 13-3.
Anomalies of the pharyngeal clefts and pouches. 2, fistulas of the second pharyngeal cleft and pouch. 3, fistula of the third pharyngeal cleft and pouch. 9,
glossopharyngea l nerve. 12, hypog lossal nerve. IC, internal carotid artery; EC, external carotid artery. (Modified from O'Rahilly R, Mller F. Human Embryology &
Teratology, 2nd ed. New York: Wiley-Liss, 1996; with pe rmission.)
SINUSES OPENING INTO THE PHARYNX
Sinuses opening into the pharynx are rarely seen. They usually open into the upper half of the posterior tonsillar pillar or into the tonsil itself.
CYSTS
The cysts of the second pouch may present clinically as a bulging in the posterior tonsillar pillar. Most are encountered in the neck and may extend
between external and internal carotid arteries (Fig. 13-4).
Fig. 13-4.
8/11/2019 Chapter 13 Pharynx
5/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 5
Incomplete closure of the second branchial cleft or pouch may leave cysts. Type I, superficial, at the border of the sternocleidomastoid muscle. Type II, between
the muscle and the jugular vein. Type III, in the bifurcation of the carotid artery. Type IV, in the pharyngeal wall. Types I, II, and III a re of se cond-cleft origin. Type
IV is from the second pouch. M, ste rnocleidomastoid muscle; V, jugular vein; A, carotid artery. (Modified from Skandalakis JE, Gray SW, Rowe JS Jr. Anatomical
Complications in General Surgery. New York: McGraw-Hill, 1983; w ith permission.)
Third Cleft and Pouch DefectsA complete fistula of the third cleft and pouch has never been reported. Such a fistula, theoretically, would pass below the eleventh cranial nerve, over the
superior laryngeal nerve and hypoglossal nerve, and posteromedial to the internal carotid artery. It would then open into the pharynx in the upper part of
the piriform recess (Fig. 13-3).
Internal sinus tracts derived from the third pouch have been reported. They originated from the apex of the left piriform recess in all cases.
Fourth Cleft and Pouch Defects
A complete fistula of the fourth cleft and pouch has not been reported. Theoretically, the route of this fistula (Fig. 13-5) would be from the apex of the
piriform recess, through the cricothyroid membrane (inferior to the cricothyroid muscle), descending into the tracheoesophageal groove and looping around
the artery of the fourth arch, passing cephalodorsal to the carotid, looping over the hypoglossal nerve, descending in the neck, passing through the strap
muscles and platysma, and exiting low in the neck, anterior to the sternocleidomastoid muscle.
Fig. 13-5.
8/11/2019 Chapter 13 Pharynx
6/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 6
The pathway of a fourth b ranchial pouch abnormality. (Modified from Donegan JO. Congenital neck masses . In: Cummings CW (ed). Otolaryngology - Head and
Neck Surgery, 2nd Ed . St Louis: Mosby Year Book, 1993; with permission.)
Surgical Considerations
A thorough understanding of the embryology of the branchial structures is essential for the head and neck surgeon. To aid in the complete surgical excision
of these structures and to avoid complications, it is important to understand their normal course.
First branchial cleft anomalies may come in close proximity to the facial nerve. Therefore, facial nerve identification and dissection is essential to avoid
facial paralysis.
Second branchial cleft anomalies, which are the most common, start in the mid-neck (anterior to the sternocleidomastoid muscle) and course up to the
tonsillar fossa. It is important to remove the entire tract up to the tonsil.
Third branchial cleft anomalies start lower in the neck and pass posteromedial to the internal carotid artery and travel caudally to end in the piriform recess
Fourth branchial cleft anomalies are extremely rare and may present as recurrent thyroiditis. There are no clinical reports of tracts that follow the entire
theoretical course (see section above). Instead most start in the piriform apex, usually the left side, and end after only a short distance in the paratrachea
region.
Direct laryngoscopy is useful for finding the opening of the tract in the apex of the piriform recess (Fig. 13-6). Cannulation of the tract with a Fogartycatheter is helpful for localization of the tract during neck dissection in the left paratracheal region. Identification of the recurrent laryngeal nerve is
important to avoid nerve injury, but may be difficult with previous infection.
Fig. 13-6.
Piriform apex fistula (marked by arrow). (From Jacobs IN, Gray R, Wyly B. Approach to branchial pouch anomalies that cause airway obst ruction during infancy.
Otolaryngol Head Neck Surg 1998;118(5):682-685; with pe rmission.)
Ventral Defects
The embryogenesis and abnormalities of development of the thyroid, parathyroids, and thymus are beyond the scope of this chapter. Information about the
thyroid and parathyroids is included in the chapter on the neck; the thymus is considered in the chapter on the mediastinum. However, the anomalies of the
descent of the medial anlage, the thyroid, are important in the discussion of the pharynx as it pertains to the lingual thyroid because the entire thyroid ma
locate in the oropharynx and cause an obstruction of the airway.
Lingual thyroid refers to the failure of the thyroid to descend to its normal location. This gland may be within the tongue, at the normal location of the
foramen cecum (Figs. 13-7A, B). It is usually the only thyroid tissue present in the patient. Inadvertent excision of the gland may result in permanent
hypothyroidism. Hormonal suppression is usually effective in decreasing the size of the lingual thyroid. Surgery may be selectively used in cases of airway
obstruction or swallowing difficulties refractory to hormonal suppression.
Fig. 13-7.
8/11/2019 Chapter 13 Pharynx
7/40
8/11/2019 Chapter 13 Pharynx
8/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 8
Ectopic thyroid gland. A, Sites a long the pa th of descent of the thyroid from the foramen cecum (lingual thyroid) to the normal location. Hyperdescent to a s ite
benea th the s ternum is also indicated. B, The method o f exposure o f a lingual thyroid gland and the scheme for control of hemorrhage. (Modified from Lemmon WT
Paschal GW Jr. Lingual thyroid. Am J Surg 1941:52;82-85; with permission.)
SURGICAL CONSIDERATIONS
During the normal descent of the thyroid gland portions of the tract may remain (may fail to obliterate). These remnants are known as thyroglossal duct
cysts. The tract starts in the midline neck and extends to the foramen cecum. It is essential to excise the complete tract and incorporate the central body
of the hyoid bone. This is known as a Sistrunk procedure. Failure to excise the central body of the hyoid bone and follow the tract up the foramen cecum
increases the recurrence rate.
Regions of the Nasopharynx
The nasopharynx, oropharynx, and laryngopharynx together form the common aerodigestive tract known as the pharynx (Fig. 13-8). These three separate
regions are, from the surgeon's perspective, quite different and individually complex. Each region is unique with respect to the lesions that arise there, and
each has specific structural and functional considerations. The following pages discuss these three structures.
Fig. 13-8.
8/11/2019 Chapter 13 Pharynx
9/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 9
Alimentary and respiratory system in the head and neck. Medial aspect; sagittal se ction slightly to the right o f the median plane . (Modified from Frick HF, Kummer B
Putz RV (eds). Wo lf-Heidegger's Atlas o f Human Anatomy. Base l, Switzerland: Karger, 1990; w ith permission.)
Development of Nasopharynx
The nasopharynx is full of developmental and morphologic c omplexity. It c ontains:
Pouch of Luschka (pharyngeal bursa) (Fig. 13-9)
Fossa (pharyngeal recess) of Rosenmuller (Fig. 13-8)
Waldeyer's tonsillar ring (Fig. 13-10)
Eustachian (tubal) tonsil (Fig. 13-10)
Luschka's "g land" (the pha ryngeal or third tonsil) (Fig. 13-10)
Eustachian cushion (torus tuba rius) (Fig. 13-8)
Pha ryngeal (extrasellar) hypophysis (Fig. 13-8)
Fig. 13-9.
Pharyngeal bursa and pharyngeal hypophysis as seen in a sagittal section of the head of an infant. (Modified from Hollinshead WH. Anatomy for Surgeons. New
York: Harper & Row , 1968; with pe rmission.)
8/11/2019 Chapter 13 Pharynx
10/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 10
Fig. 13-10.
8/11/2019 Chapter 13 Pharynx
11/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 1
Waldeye r's tonsillar ring. A,sagittal view. B,axial view. (A,Modified from Hollinshead W H. Anatomy for Surgeons . New York: Harper & Row, 1968; B,Modified from
Skandalakis JE, Gray SW, Rowe JS Jr. Anatomical Complications in General Surgery. New York: McGraw-Hill, 1983; with permission.)
Developmental c onsiderations (Fig. 13-11) include:
Rostral tip of the notochord
Hypophysial pouch (Rathke's pouch)
Craniopharyngeal canal
Presphenoid-basisphenoid synchondrosis
Spheno-occipital synchondrosis
Tubotympanic recess
Pneumatization of the superadjacent sphenoid sinus (age 7-8)
Development of the first two pharyngeal pouches on each side
Fig. 13-11.
A,Sagittal section through the cephalic part of a 6-week embryo showing Rathke's pouch as a dorsal outpocketing of the oral cavity and the infundibulum as a
thickening in the floor of the diencepha lon. Band C, Sagittal sections through the developing hypophysis (a remnant of Rathke's pouch) in the 11th and 16th
wee ks of development, respe ctively. Note formation of the pars tuberalis, encircling the s talk of the pa rs nervosa . (Modified from Sadler TW. Langman's Medical
Embryology, 8th ed. Philadelphia: Lippincott Williams & Wilkins, 2000.)
The nasopharynx may also include the adenoids, Rathke's cleft cysts, chordomas, or craniopharyngioma.
Nomina Anatomicarefers to the nasopharynx as the pars nasalis pharyngis, the nasal part of the pharynx. Although the nasopharynx is a part of the
pharynx, remember that it is a purely respiratory passage. Under normal circumstances, it is not a part of the digestive tract, as is the pharynx.
The pharynx arises as the expanded cephalic end of the embryonic foregut (Fig. 13-12). The nasal cavities develop separately from the foregut, arising
from the nasal pits which deepen into nasal sacs. Since the early 1900s, controversies have existed as to whether the nasopharynx should be considered
strictly a part of the nasal cavity, or if it should be regarded as part of the pharynx. From embryogenesis, it is known that some of the original cavity is
taken up into the lower part of the nasal cavities. A portion of the original pharyngeal cavity comes to lie above the level of the definitive palate. It is this
portion of the pharynx that contributes to at least a portion of the nasopharynx and unites with the deepest part of the nasal sacs.
Fig. 13-12.
8/11/2019 Chapter 13 Pharynx
12/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 12
A,Sagittal section through the nasal pit and lower rim of the medial nasa l prominence o f a 6-week embryo. The primitive nasa l cavity is sepa rated from the oral
cavity by the oronasal membrane. B,Similar section as in A,show ing the oronasal membrane breaking down. C,A 7-week embryo with a primitive nasal cavity in
open connection with the oral cavity. D,Sagittal section through the face of a 9-week embryo, showing separation of the definitive nasal and oral cavities by the
primary and s econdary pa late. Definitive choanae are at the junction o f the o ral cavity and the pharynx. (Modified from Sadler TW. Langman's Med ical Embryology,
8th ed. Philadelphia: Lippincott Williams & Wilkins, 2000; with permission.)
The caudal extent of the nasopharynx is above the plane of the soft palate (Fig. 13-8) at the level of the opening of the eustachian tube (derived from the
first pharyngeal pouch). Therefore, the nasopharynx is derived from the embryonic pharynx below the level of the eustachian tube orifice.
Rostral to the eustachian tube orifice, the nasopharynx develops from the deep extension of the nasal cavities. The preceding conclusions are based on th
histology and innervation of the two components of the nasopharynx. The nasal (anterior) nasopharynx possesses the highly vascular respiratory mucosa
that is rich in lymphatics and resembles the nasal cavity. Transition occurs at the level of the eustachian tube, where the posterior nasopharynx has
strat ified squamous epithelium resembling that of the oropharynx.
Congenital Anomalies of the Nasopharynx
Anomalous nasopharyngeal development may be assoc iated with abnormalities of the posterior nasal apertures, including choanal atresia, unilateral or
bilateral (Fig. 13-13), and malformation of the posterior aspect of the skull base. Gross abnormalities such as iniencephaly or anencephaly can also be
assoc iated with nasopharyngeal wall malformations.
Fig. 13-13.
8/11/2019 Chapter 13 Pharynx
13/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 13
Axial CT (computed tomography) showing bilateral choanal atresia. White a rrows indicate at retic plates . V, vomer. (Courtesy Ian N. Jacobs.)
SURGICAL ANATOMY
Surface Anatomy of the Nasopharynx
The nasopharynx extends from the choanae (posterior nasal apertures) (Fig. 13-14) and slopes upward and backward. Its shape follows the slope of media
and lateral boundaries formed by the posterior edges of the vomer and the medial pterygoid plates, respectively (Figs. 13-14, 13-15).
Fig. 13-14.
Base of the skull. (Modified from Frick HF, Kummer B, Putz RV (eds). Wolf-Heidegge r's Atlas of Human Anatomy, Basel, Switzerland: Karger, 1990; with permission.)
Fig. 13-15.
8/11/2019 Chapter 13 Pharynx
14/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 14
Skull, medial aspect; sagittal section s lightly to the left of the median plane. (Modified from Frick HF, Kummer B, Putz RV (eds). Wo lf-Heidegger's Atlas of Human
Anatomy. Basel, Switzerland: Karger, 1990; with permission.)
The anterior plane of the soft palate (Fig. 13-8) produces the lower extent of the nasopharynx. This plane intersects the anterior arch of the atlas in its
posterior extent. This is the narrowest part of the nasopharynx. It is called the isthmus, and it leads to the oropharynx below.
The nasopharynx is just inferior to the sphenoid bone (Fig. 13-15) and the posterior part of the sphenoid sinus. The hypophysial fossa (Fig. 13-15) and
pituitary gland are more cephalad to the sphenoid. The basilar portion of the occipital bone (Fig. 13-15) slopes downward, forming the anterior margin of
the foramen magnum (Figs. 13-14, 13-15), which is located posterosuperiorly to the nasopharynx.
Anterosuperiorly, the vomer articulates with the undersurface of the sphenoid bone (Fig. 13-15). Posterior to this articulation lies the pharyngeal sphenoida
fossa. In this fossa lies the pharyngeal hypophysis (Fig. 13-8). Posterior to it, in the same tissue plane, one finds a collection of lymphoid tissue known as
the pharyngeal tonsil (Fig. 13-8).
Move inferiorly on the posterior wall of the nasopharynx to find the isthmus. Located below the basiocciput (Fig. 13-14) is the anterior arch of the atlas
(Fig. 13-8), and immediately behind it, the dens.
Numerous ligaments are locat ed in this region. The anterior longitudinal ligament is the ligamentous st ructure most closely related to the posterior wall of
the nasopharynx.
The side walls of the nasopharynx are also extremely important. The most prominent structure is the opening of the auditory (eustachian) tube (Fig. 13-
14). This is located just behind the inferior nasal turbinate (concha) (Fig. 13-15). The overhang above and behind the orifice is known as the torus tubarius
(Figs. 13-8, 13-16). This is formed by the bulge of the fibrocartilage of the auditory tube itself. Gerlach's tonsil (eustatchian or tubal tonsil) (Figs. 13-8, 13
10) is a collection of lymphoid tissue located in the mucous membrane over the pharyngeal orifice of the eustachian tube. The fossa of Rosenmuller
(pharyngeal recess) (Fig. 13-8, Fig. 13-17) is located behind the tubal orifice. This is a fairly deep and laterally directed structure. The superior pharyngeal
constrictor (Fig. 13-18) lies in the side wall of the nasopharynx. Dense pharyngobasilar fascia, which is attached to the skull base above and to the
pterygoid plate laterally (Fig. 13-14), is located on the inner aspect of the superior constrictor. The gap in the fascia allows the eustachian tube to pass.
On the outer aspect of the superior constrictor muscle is the weaker buccopharyngeal fascia. It provides a flimsy covering for the wall of the nasopharynx.
Fig. 13-16.
8/11/2019 Chapter 13 Pharynx
15/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 15
8/11/2019 Chapter 13 Pharynx
16/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 16
Pharyngea l cavity, dorsal as pect. The wa ll of the pharynx has been cut a long the mid-dorsal line and opene d. (Modified from Frick HF, Kummer B, Putz RV (eds).
Wolf-Heidegger's Atlas of Human Anatomy. Basel, Switzerland: Karger, 1990; with pe rmission.)
Fig. 13-17.
Pharyngeal cavity, dorsal aspect. The wall of the pharynx has been cut along the middorsal line and opened; the mucous membrane and the superior pharyngeal
constrictor muscle ha ve been partially removed in o rder to expose the different muscles. (Modified from Frick HF, Kummer B, Putz RV (eds). Wo lf-Heidegger's Atlas
of Human Anatomy. Basel, Switze rland: Karger, 1990; with pe rmission.)
Fig. 13-18.
8/11/2019 Chapter 13 Pharynx
17/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 17
Muscular wall of the pharynx, dorsal as pect. (Modified from Frick HF, Kummer B, Putz RV (eds). Wolf-Heidegge r's Atlas of Human Anatomy. Basel, Switzerland:
Karger, 1990; with permission.)
An important feature of the nasopharynx is the development of the first two pharyngeal pouches on either side of this cavity (Fig. 13-8, Fig. 13-9). This
relationship is important with respect t o the development of Waldeyer's ring (Figs. 13-10A & 13-10B). This is an incomplete ring of lymphoid tissue
composed of the pharyngeal tonsil, eustachian tonsil, palatine tonsil, and lingual tonsil.
Lying close to the nasopharynx are two noteworthy embryologic structures: the rostral segment of the notochord and the craniopharyngeal canal (Fig. 13-
11). Tumors (chordoma and craniopharyngioma, respect ively) may arise from these. Both may involve t he nasopharynx.
8/11/2019 Chapter 13 Pharynx
18/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 18
When the nasopharynx is examined indirectly with a mirror or endoscopically, several significant features become apparent. The perichoana with the
posterior tips of the inferior, middle, and superior turbinates (conchae) (Figs. 13-8, 13-16) are readily seen. The posterior vomer sharply divides the
posterior choanae (Fig. 13-14). Enlargement of the turbinates (conchae), adenoids, or polyps, or a mucopurulent nasal discharge can be readily apparent in
this region. Adenoids usually begin to atrophy after thirteen years of age, and if present in an adult, neoplasia should be considered. Enlarged adenoids in
an adult may also raise suspic ion for lymphoepithelial hyperplasia associated with an HIV infect ion. On the exam, juvenile nasopharyngeal angiofibromas c an
be seen as smooth pulsatile masses, which should never be biopsied because the vascularity of the tumor and the brisk bleeding that accompanies biopsy
creates the potential for severe hemorrhage.
Several important landmarks in addition to the torus t ubarius (Fig. 13-16) can be seen when t he nasopharynx is examined during nasopharyngoscopy. The
salpingopharyngeus muscle (Fig. 13-17) is seen to sweep posteriorly and inferiorly from the post erior part of t he torus, forming a raised mucosal fold (Fig.
13-16). The pharyngeal recess previously mentioned is actually formed between the pharyngeal wall and the elevation produced by this fold. Gerlach's tons
underlies this fold. Slight elevation of mucosa in the center of the eustachian tube opening is produced by the underlying levator veli palatini muscle (Figs.13-8, 13-17). Looking at the roof of the nasopharynx, depression in the midline is frequently seen. This concavity is known as the pharyngeal bursa (Fig.
13-8). The mucosa of this bursa is infiltrated by lymphatic nodules at its periphery, which if sufficiently hyperplastic, forms the adenoids. A persistent
remnant of the embryonic notochord in this area may occasionally be seen as a cystic midline nasopharyngeal mass. This is known as the Thornwaldt's cys
and is usually seen later in life.
Residual epithelial elements of Rathke's pouch (Fig. 13-11), an evagination of the stomodeal roof that contributes to the anterior pituitary gland, can give
rise to a craniopharyngioma. These usually occur just superior to the pharyngeal bursa in the midline of the nasopharynx, and may also be present as
nasopharyngeal masses (Fig. 13-9).
Surgical Considerations
Nasopharyngoscopy, whether with direct flexible or rigid telescopes, allows visualization of the structures and landmarks described above. An indirect mirror
exam will also allow excellent visualization of the nasopharynx. However, the latter is limited by the experience of the examiner, the inverted nature of the
mirror image, and the cooperat ion of the patient if the exam is done outside the operat ing room.
The best way to examine the nasopharynx in detail is under general anesthesia with the patient in a supine position. The soft palate (Figs. 13-8, 13-16)
can be retracted by passing catheters through the nares into the oral cavity and out through the mouth. The ends of such catheters are clamped and a
mirror is used by the examiner located at the head of the patient to survey the nasopharynx, denote the structural features, and to perform a variety of
procedures. These procedures include adenoidectomy, biopsies of any areas suspicious for malignancy, removal or marsupialization of polyps and cysts,
cannulation of eustachian tubes, and surgery for nasopharyngeal stenosis (Fig. 13-19). A thorough examination of the three dimensional structure of the
nasopharynx under general anesthesia is essential in planning a surgical repair, such as with laterally-based pharyngeal flaps.
Fig. 13-19.
Severe nasopharyngeal stenosis; complete cicatrix of the nasopharynx. (Modified from McLaughlin KE, Jacobs IN, Todd NW, Gussack GS, Carlson G. Management of
nasopharyngeal and oropharyngeal stenosis in children. Laryngoscope. 107:1322-1331, 1997; with permission.)
Nasopharyngeal examination under general anesthesia is also useful for choanal atresia surgery, although in these cases the catheters cannot always be
passed through the nose; different maneuvers to retract the palate may be necessary.
With respect to malignancies confined to the nasopharynx, it is imperative that a complete nasopharyngeal exam is performed and that the examiner is fully
aware of the normal anatom and variations of the naso har nx. In the case of atients who resent with neck masses su estive of mali nanc a
8/11/2019 Chapter 13 Pharynx
19/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 19
nasopharyngeal exam must always be a part of their head and neck examination. It is also extremely important to examine the nasopharynx of t he pat ients
who present with nasal obst ruction, epistaxis, or serous otitis media. All of these may result from benign or malignant processes in this region. For example
angiofibromas may cause intermittent epistaxis as well as nasal obstruction. A process near the eustachian tube orifice, such as nasopharyngeal carcinoma
or lymphoma, may have unilateral serous otitis media as its only symptom.
Important Anatomic Relationships
Nasopharyngeal walls are c omposed of four layers from inside to outside:
Mucosa
Submucosa or fibrous layer (pharyngobas ilar fascia)
Muscular layer
Buccopharyngeal fascia covering the constrictor muscles
The mucous membrane containing ciliated respiratory and nonciliated c olumnar epithelium is the inner lining. Submucosal connec tive tissue made of
pharyngobasilar fascia is well defined in its attachment to the skull base (Fig. 13-18). External to the superior constrictor muscle is the buccopharyngeal
fascia (Fig. 13-16). Attachment of the nasopharynx to the skull base is extremely important. Significant relationships to the middle cranial fossa, to the
dehiscence between the petrous temporal bone and foramen lacerum (Fig. 13-14), and to the carotid canal are apparent (Fig. 13-14).
The nasopharynx is attached in the midline to the pharyngeal tubercle on the basal surface on the body of the occipital bone (Fig. 13-18). This attachmen
extends bilaterally to the petrous temporal bone (Fig. 13-15), and turning forward, continues to the posterior margin of the medial pterygoid plate (Fig. 13-
14) and the pterygoid hamulus (Fig. 13-15). The fossa of Rosenmuller (Figs. 13-8, 13-17) lies in the roof of the nasopharynx. Because the internal carotid
artery (Fig. 13-20) passes through the foramen lacerum it is close to the nasopharyngeal wall. Expanding masses in the nasopharynx, therefore, can involve
and jeopardize the carotid.
Fig. 13-20.
8/11/2019 Chapter 13 Pharynx
20/40
8/11/2019 Chapter 13 Pharynx
21/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 2
Coronal, slightly oblique section through the middle cranial fossa, showing the cavernous and cerebral portions of the internal carotid artery and cavernous sinus.
Nasopharyngeal lesions may also involve the retropharyngeal or parapharyngeal spaces (Figs. 13-22, 13-23). This can occur since the buccopharyngeal
fascia covering the external surface of the nasopharynx is connected to the prevertebral fascia of the deep layer of the deep cervical fascia. This creates
a space between the two fasc ial layers, known as the retropharyngeal space. Another space located laterally occurs between the buccopharyngeal fascia
and the fascia of the pterygoid muscles. Near the nasopharynx, that space is called the parapharyngeal space. Tumors or infections can invade this space
readily.
Fig. 13-22.
Fascial spaces o f the head and neck region. (Modified from Hollinshea d WH. Anatomy for Surgeons. New York: Harper & Row, 1968; with permission.)
Fig. 13-23.
8/11/2019 Chapter 13 Pharynx
22/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 22
Sagittal view of fascial spaces o f head and neck region. (Based on Hollinshead WH. Anatomy for Surgeons, Vol. 1, 2nd ed. New York: Harper & Row, 1968.)
Important structures that pass between the skull base and the superior constrictor muscles can usually be seen on anatomic specimens. Removing the
mucosa from the medial aspect will reveal the tensor veli palatini (Fig. 13-17) and levator veli palatini muscles, ascending palatine artery, and ascending
pharyngeal artery (Fig. 13-24). The salpingopharyngeus muscle (Fig. 13-17) can also be revealed.
Fig. 13-24.
8/11/2019 Chapter 13 Pharynx
23/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 23
Blood vessels and nerves on the dorsolateral wall of the pharynx, dorsal aspect. The right side especially emphasizes the blood vessels, the left side the nerves.
(Modified from Frick HF, Kummer B, Putz RV (eds). Wolf-Heidegger's Atlas of Human Anatomy. Basel, Switzerland: Karger, 1990; w ith permission.)
The main muscles of the nasopharynx are the tensor and levator veli palatini muscles (Fig. 13-17). These are located in the space between the skull base
and the superior constrictor muscle, which will be described under "Myofascial Framework." This space is sealed by the pharyngobasilar fascia (Fig. 13-18).
These muscles originate from the pterygoid fossa between the lateral and medial pterygoid plates (Fig. 13-14). They insert into the soft palate (Figs. 13-8,
13-16).
The head and neck surgeon must be familiar with several important considerations. The anterior soft palate is tensed by the action of the tensor veli
palatini muscle. This muscle is thought to have an important role in eustachian tube opening and thereby in pressure equalization between the middle ear
and the nasopharynx. Other authors implicate the levator veli palatini in this function.
The levator veli palatini crosses the superior border of the superior constrictor muscle and enters the nasopharyngeal mucosa and the lateral border of the
soft palate. Contraction of the levator veli palatini muscles elevates the soft palate and seals the oral cavity from the oropharynx. This principle is
important when treating patients with velopharyngeal insufficiency and its associated deglutition and speech problems.
Two arteries travel the space below the skull base. These are the ascending pharyngeal, arising from the bifurcation of the internal and external carotid
arteries, and the ascending palatine artery, a branch of the facial artery (Fig. 13-24). These vessels are the main contributors of blood supply to the
nasopharynx.
Although the anatomy of the skull base is beyond the scope of this chapter, familiarity with the location of two structures is important. The foramen
spinosum (Fig. 13-14) is a conduit for the middle meningeal artery (Fig. 13-20). The foramen ovale (F ig. 13-14) provides passage to the mandibular branch
of the trigeminal nerve (Fig. 13-21). These foramina may allow spread of malignancies with origins in the intracranial nasopharynx.
The nasopharynx is relatively insensitive, with the main sensory innervation provided by the branches of maxillary division of the t rigeminal nerve (Fig. 13-
25): the greater and lesser palatine nerves. Cranial nerve IX, the glossopharyngeal nerve (Fig. 13-24), supplies sensory innervation to the mucosal wall as
far superiorly as the eustachian tube. Procedures on the nasopharynx, such as mucosal biopsies and adenoidectomies, however, are relatively painless and
postoperat ive requirements for analgesics are minimal.
Fig. 13-25.
8/11/2019 Chapter 13 Pharynx
24/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 24
Arteries a nd ne rves in the lateral wa ll of the nasal cavity, palate, and infratemporal fossa, medial aspect. (Modified from Frick HF, Kummer B, Putz RV (eds). Wolf-
Heidegger's Atlas o f Human Anatomy. Base l, Switzerland: Karger, 1990; with permission.)
Surgical Considerations
A very important point in a nasopharyngeal surgical procedure, such as adenoidectomy, is the proximity of the atlanto-axial joint (Fig. 13-8). Muscle spasm
or infect ion after surgery may result in at lanto-axial dislocation, known as Grisel's syndrome. Patients with trisomy 21 (Down syndrome) are at higher risk fothis unusual complication.
A variety of benign and malignant neoplasms may occur in the nasopharynx (Tables 13-3 and 13-4). Congenital lesions such as chordomas and
craniopharyngiomas may also be present. Malignancies of the salivary glands as well as melanomas and esthesioneuroblastomas (olfactory neuroblastomas)
may also be found in the nasopharynx.
Table 13-3. Benign Non-Epithelial Tumors, Involving the Nasal Cavity, Paranasal Sinuses, and Nasopharynx 156 Cases
Vascular tumors 81
Capillary hemangioma 30
Cavernous hemangioma 5
Venous hemangioma 3
Benign hemangioendothelioma 3
Angiomatosis 1
Glomus tumor 1
Angiofibroma 38
Osseous and fibro-osseous tumors 52
Osteoma 31
Fibrous dysplasia 9
Ossifying fibroma 7
Osteoblastoma 1
Giant cell tumor 4
Chondroma 7
Myxoma 7
Fibroma 5
Leiomyoma 2
Lipoma 1
Rhabdomyoma 1
Source:Fu YS, Perzin KH. Non-epithelial tumors of the nasal cavity, paranasal sinuse s, and nasopha rynx: a clinicopatho logic study. I. General features and vascular
tumors. Cancer 33:1275-1288, 1974; with pe rmission.
Table 13-4. Malignant Tumors of Nasopharynx from the Mayo Tissue Registry, 1972 to 1981
Tumor Type Number (%)
Squamous cell carcinoma* 120 (71)
Lymphoma 31 (18)
Miscellaneous 18 (11)
Adenocarcinoma 6
Plasma cell myeloma 3
8/11/2019 Chapter 13 Pharynx
25/40
8/11/2019 Chapter 13 Pharynx
26/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 26
Superficial cervical and facial lymph nodes . (Modified from Genden EM, Thawley SE, O'Leary MJ. Malignant neoplasms of the o ropharynx. In: Cummings CW,
Fredrickson JM, Harker LA, Krause CJ, Richardson MA, Schuller DE (eds). Otolaryngology: Head and Neck Surgery, 3rd ed . St Louis: Mosby, 1998; with permission.)
Large primary tumors of the nasopharynx obstruct the choanae and nasal airway and can lead to nasal obstruction as well as to epistaxis. Superior
extension via the foramen lacerum into the cranium can lead to cranial nerve involvement. Most commonly, cranial nerve VI is the first to be involved with
resulting lateral rectus muscle palsy and diplopia. Ophthalmoplegia can oc cur from involvement of c ranial nerves III and IV. High neck and fac ial pain
signifies involvement of cranial nerve V. As the tumor enlarges, cranial nerves VII, IX, X, and XI can be affected (Figs. 13-24, 13-25, 13-27).
Fig. 13-27.
8/11/2019 Chapter 13 Pharynx
27/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 27
A,Sagittal view showing parapharyngeal and retropharyngeal spaces and associated anatomic structures. B,Axial view of the parotid gland and the carotid artery
and o f the peritonsillar, retropharyngeal (space 3), danger (space 4), prevertebral (space 5), and pa rapharyngea l (lateral pha ryngeal) spaces. BPF,
buccopharyngea l fascia; RPS, Retropharyngeal space; DS, Danger s pace; PVS, Prevertebral space; CN, cranial nerve.
The nasopharynx is an extremely complex three dimensional structure with close proximity to the brain, carotid artery, sphenoid sinus, and a variety of
other important structures and nerves (Fig. 13-21). It is involved in breathing, deglutition, and phonation. Hence, it is imperative that a surgeon operating
in this area be thoroughly familiar with the embryologic, anatomic, and physiologic aspects of the nasopharyx. This avoids potentially disastrous
complications.
Oropharynx-Laryngopharynx
The next two regions of the pharynx to be discussed are the oropharynx, continuous with the oral cavity above, and the laryngopharynx, continuous with
the esophagus below. The pharynx is a myofascial framework enclosing the pharyngeal lumen and its contents. The external surfaces of the pharynx make
up the portions of the borders of important deep neck spaces which are involved in various disease processes. Understanding the anatomy and relationship
of the pharynx is important in making sound judgments regarding surgical approaches to the pharynx and adjacent structures.
The following section discusses the anatomy of the pharynx, first describing the myofascial framework. Then we describe the important structures
traversing this framework en route to the pharynx, the structures constituting the oropharynx and laryngopharynx, and the important structures bordering
the pharynx.
Myofascial Framework
The pharyngeal wall is composed of stratified squamous epithelium, which covers the internal surface of the myofascial layer. This layer extends from the
skull base superiorly to the level of the inferior border of the cricoid cartilage inferiorly (Fig. 13-8). This myofascial layer is composed of three paired U-
shaped muscles that open anteriorly: the superior, middle, and inferior pharyngeal constrictor muscles (Figs. 13-18, 13-28). These muscles form a
telescoping structure with the lower muscles overlapping the upper muscles at the inferior border. All three sets of muscles insert posteriorly on a midline
posterior pharyngeal raphe, suspending superiorly from the pharyngeal tubercle of the basiocciput.
Fig. 13-28.
8/11/2019 Chapter 13 Pharynx
28/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 28
Muscles of the tongue, pharynx, and larynx, lateral aspect. (Modified from Frick HF, Kummer B, Putz RV (eds). Wolf-Heidegge r's Atlas of Human Anatomy. Basel,
Switzerland: Karger, 1990; with pe rmission.)
8/11/2019 Chapter 13 Pharynx
29/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 29
These paired pharyngeal constrictor muscles are covered internally and externally by fascial layers. Internally, the constrictor muscles are covered by the
pharyngobasilar fascia, which is thick superiorly and thin inferiorly and covers the muscles the length of the pharynx. Superiorly, the pharyngobasilar fascia
attaches to the pharyngeal tubercle of the occiput (Fig. 13-28), extends along the petrous portion of the temporal bone, and attaches anteriorly to the
medial pterygoid plate (Fig. 13-14) and the pterygomandibular raphe. The upper, thick portion of this fascia suspends the superior constrictor muscle from
the skull base. The external surface of the muscle is covered by the buccopharyngeal fascia. This fascia covers the pharynx at the level of the superior
constrictor muscle and fuses below this level with the middle layer of deep cervical fascia. This third fascia forms the remainder of the external fascial
covering of the pharynx.
The superior pharyngeal const rictor muscles originate from the medial pterygoid plate and pterygomandibular raphe anteriorly. Their fibers extend posteriorl
in a horizontal and slightly superior and inferior direct ion to insert on the posterior midline pharyngeal raphe (Fig. 13-18). These muscles surround the
oropharynx.
The middle pharyngeal constrictor muscles originate anteriorly from the greater and lesser cornua of the hyoid bone (Fig. 13-28). Their fibers extendposteriorly in three separate groups (superior, middle, and inferior) to attach on the posterior midline raphe (Fig. 13-18). The middle constrictors are at the
level bridging the junction between t he lower oropharynx and upper laryngopharynx.
The inferior pharyngeal constrictor muscles are the thickest of the pharyngeal constrictors and the best developed. These arise anteriorly from the oblique
line of the thyroid and cricoid cartilages (Fig. 13-28). They then extend posteriorly in a horizontal, superior, and inferior direction to insert on the posterior
midline raphe. The cephalic portion of the inferior constrictor muscle is termed the cricopharyngeus muscle. The cricopharyngeus muscle forms the upper
esophageal sphincter. It extends from the cricoid cartilage in a horizontal direction and interdigitates with the transverse esophageal muscle layer.
Intervals between the overlapping layers of pharyngeal constrictor muscles are traversed by structures entering the pharynx. The interval between the
superior and middle constrictor muscles is traversed by the stylopharyngeus muscle (Fig. 13-18). This muscle originates from the styloid process and
extends inferiorly and anteriorly in an oblique fashion to attach to the medial aspect of the middle constrictor muscle. The glossopharyngeal nerve supplies
sensory innervation to the base of the tongue and pharynx and also traverses this interspace (Fig. 13-24). The glossopharyngeal nerve and the lingual
artery course together, running deep to the hyoglossus muscle (Fig. 13-28). The stylohyoid ligament, which attaches to the lesser cornu of the hyoid bone
also traverses this interval between the superior and middle pharyngeal constrictor muscles. Lying at the inferior pole of the palatine tonsil, the interval
provides a pathway of extension for an infectious process from the peritonsillar area to the parapharyngeal space, lateral to the superior constrictor muscle
The interval between the middle and inferior pharyngeal constrictor muscles is occupied by the thyrohyoid membrane (Fig. 13-28). The structures traversin
this membrane include the internal laryngeal nerve and superior laryngeal artery and vein (Fig. 13-24). The internal branch of the superior laryngeal nerve
enters the thyrohyoid membrane and supplies sensory innervation to the supraglottic larynx and the piriform recess mucosa. The external branch of the
superior laryngeal nerve continues inferiorly, lateral to the constrictor muscles, and accompanies the superior thyroid vessels (Fig. 13-24) to innervate the
cricothyroid muscle (F ig. 13-28). The internal branch of the superior laryngeal nerve penetrates the thyrohyoid membrane approximately 1 cm inferior and
medial to the greater cornu of the hyoid bone. Infiltration of local anesthetic in this area will create a superior laryngeal nerve block and anesthetize the
laryngopharynx and supraglottic larynx. This is also the area of the t hyrohyoid membrane where an external laryngocele will extend from the endolaryngeal
cavity to t he extralaryngeal space.
The interval between the inferior constrictor muscles and the transverse fibers of the esophageal muscle transmits a neurovascular bundle. This bundle
includes the recurrent laryngeal nerve (Fig. 13-29). This nerve supplies sensory innervation to the glottis and subglottis and motor innervation to the
intrinsic laryngeal muscles except the cricothyroid muscle. Also in this bundle are the inferior laryngeal artery and vein, branches of the thyrocervical trunk
of the subclavian vessels.
Fig. 13-29.
8/11/2019 Chapter 13 Pharynx
30/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 30
Pharyngoesophageal segment showing potential areas of herniation. (Based on Hollinshead WH. Anatomy for Surgeons, Vol. 1, 2nd ed. New York: Harper & Row,
1968.)
The innervation of the pharyngeal muscles is from the pharyngeal plexus (Fig. 13-24). This is composed of the pharyngeal branches of the glossopharyngea
and vagus nerves. The glossopharyngeal nerve supplies only the stylopharyngeus muscle. The vagal contribution supplies all the other muscles, including
the muscles of the soft palate (Fig. 13-30), with the exception of the tensor palatini muscle, which is supplied by the mandibular branch of the trigeminal
nerve (Fig. 13-25). The inferior constrictor muscle also receives innervation from the external branch of the superior laryngeal nerve (Fig. 13-24). The
cricopharyngeus muscle may receive some innervation from the recurrent laryngeal nerve. Sensory innervation of the pharynx is supplied by the
glossopharyngeal nerve through the pharyngeal plexus. This supplies the mucosa of the oropharynx and laryngopharynx with the exception of the piriform
recess mucosa. The piriform recess mucosa receives its innervation from the internal branch of the superior laryngeal nerve, which traverses the submucos
in the anterior wall of the piriform recess (Fig. 13-16).
Fig. 13-30.
Muscles of the s oft palate (cut away to show the levato r veli palatini). (Modified from Hollinshead W H. Anatomy for Surgeons. New York: Harper & Row, 1968; with
permission.)
The vascular supply of the pharyngeal walls is from the ascending pharyngeal artery and the superior thyroid artery, branches of the external carotid artery
(Fig. 13-24). The inferior thyroid artery, a branch of the thyrocervical trunk, also provides arterial supply to the laryngopharynx. The venous drainage of th
pharynx is through the pharyngeal plexus on the posterior surface of the pharynx. This drains into the pterygoid plexus, the superior and inferior thyroid
veins, the facial vein, and directly into the internal jugular vein (Fig. 13-31).
Fig. 13-31.
8/11/2019 Chapter 13 Pharynx
31/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 3
Blood vessels and nerves of the neck, ventrolateral aspect. Parotid gland, sternocleidomastoid muscle, supra- and infrahyoid muscles have been partially removed.
(Modified from Frick HF, Kummer B, Putz RV (eds). Wolf-Heidegger's Atlas of Human Anatomy. Basel, Switzerland: Karger, 1990; w ith permission.)
The lymphatic drainage of the pharynx varies depending on the anatomic level. The posterior drainage is through the retropharyngeal lymph nodes (nodes o
Rouvier), located behind the pharynx at the level of the carotid bifurcation. Drainage of the lateral pharyngeal structures is to the jugulodigastric and
midjugular lymph nodes in the deep jugular chain (Fig. 13-26).
SURGICAL CONSIDERATIONS
Zenker's diverticulum (Fig. 13-32) may form in the area of Killian's dehiscence (Fig. 13-29), an area of weakness between the inferior constrictor muscle an
the f ibers of the cricopharyngeus muscle. It is usually on the left side. This is a pulsion diverticulum. It results from increased intraluminal pharyngeal
pressures above the level of the cricopharyngeus and increased cricopharyngeal muscle pressures. This causes a gradual weakening of this area and
herniation of mucosa and submucosa t hrough the weakened area t o form a diverticulum. This problem is usually remedied by performing a c ricopharyngealmyotomy with or without resection or suspension of the herniated mucosa.
Fig. 13-32.
8/11/2019 Chapter 13 Pharynx
32/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 32
Zenker's diverticulum.
Oropharynx
The oropharynx is a continuation of the oral cavity anteriorly, the nasopharynx superiorly, and the laryngopharynx inferiorly (Fig. 13-8). It is located at
approximately the level of the 2nd and 3rd cervical vertebrae. Its boundaries extend superiorly from the junction of the hard and soft palate (Fig. 13-8, 13-
16) to the inferior margin at the level of the plane of the hyoid bone. Anteriorly, it extends to the junction of anterior and posterior regions of the tongue a
the level of the circumvallate papillae (Fig. 13-16).
The oropharynx contains the:
Soft palate and uvula
Palatine tonsils and tonsillar fossae
Base of tongue
Valleculae
8/11/2019 Chapter 13 Pharynx
33/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 33
Lateral and posterior oropharyngeal walls
SOFT PALATE
The soft palate (Figs. 13-8, 13-16, 13-30) is an essential muscular structure which extends from the level of the hard palate (Fig. 13-8) anteriorly to a
midline protuberance, the uvula, posteriorly. Laterally, the soft palate blends with the tonsillar area. The soft palate prevents nasopharyngeal reflux of air
and food by closing off the oropharynx from the nasopharynx during speech and swallowing.
The soft palate is composed of stratified squamous mucosa which covers a muscular framework of the following five muscles:
Levator veli palatini
Tensor veli palatini
Musculi uvulae
Palatoglossus
P alatopharyngeus
Except for the tensor veli palatini, these muscles are innervated by the vagus nerve to the pharyngeal plexus.
The levator veli palatini muscle (Figs. 13-17, 13-30) forms most of the bulk of the soft palate. It arises from the floor of the petrous portion of the temporal
bone and medial portion of the cartilaginous eustachian tube, medial to the pharyngobasilar fascia. It travels inferomedially in an oblique fashion to fuse wit
the contralateral muscle in the posterior portion of the soft palate.
The tensor veli palatini muscle (Fig. 13-17) is the only soft palate muscle innervated by the mandibular branch of the trigeminal nerve rather than the vagu
nerve. It arises from the medial pterygoid plate (Fig. 13-14), spine of the sphenoid bone, and lateral portion of the cartilaginous eustachian tube, lateral to
the pharyngobasilar fascia. It descends inferiorly to hook around the hamulus of the pterygoid bone (Fig. 13-30) and extends medially as a narrow tendon
to insert on the posterior hard palate as the palatine aponeurosis. This muscle functions to laterally tense the palate and also to open the eustachian tube
orifice. Children with cleft palates have poor function of the tensor veli palatini muscle, due to the muscle's midline dehiscence. This results in poor
eustachian tube opening and chronic middle ear effusions. The eustachian tube dysfunction improves after palatal surgical repair.
The musculi uvulae (Figs. 13-17, 13-30) arise from the posterior hard palate and palatine aponeurosis on each side of the midline, extend posteriorly, and
fuse as they form the uvula (Fig. 13-17). These function to draw the uvula upward and forward. Bifidity or notching of the uvula due to failure of these
muscles to fuse indicates a submucous cleft of the palate. Care should be taken when performing adenoidectomy to avoid postoperative velopharyngeal
insufficiency. Palpation of the palate is necessary to insure absence of submucous clefting even in the absence of a notching of the uvula.
The palatoglossus muscle (Figs. 13-30, 13-33) forms the anterior tonsillar pillar, creating the anterior border of the tonsillar fossa and demarcating the
anterior margin of the lateral oropharynx. It is a thin muscle arising from the inferior portion of the soft palate where it fuses to the contralateral
palatoglossus muscle, and projects inferiorly to attach to the lateral and dorsal tongue. It functions to draw the palate down and to narrow the pharynx.
Fig. 13-33.
8/11/2019 Chapter 13 Pharynx
34/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 34
Bed of the palatine tonsil. (Modified from Hollinshea d WH. Anatomy for Surgeons . New York: Harper & Row, 1968; with permission.)
The palatopharyngeus muscle (Figs. 13-17, 13-30, 13-33) forms the posterior tonsillar pillar and part of the posterior portion of the tonsillar fossa. It arises
as two heads from the hard palate and palatine aponeurosis and more posteriorly from the contralateral palatopharyngeus muscle. The muscle inserts on
the fascia of the lower constrictor muscles. In addition to elevating the pharynx, the palatopharyngeus muscles function to draw the palate down and to
narrow the pharynx.
Blood supply of the soft palate is from the lesser palatine arteries (Fig. 13-25) and branches of the maxillary artery, which travel with the nerve though the
lesser palatine foramen. Sensory innervation is through the lesser palatine branches of the maxillary division of the trigeminal nerve.
TONSILS (PALATINE TONSILS)
The palatine tonsils (Figs. 13-8, 13-10, 13-16, 13-17), commonly referred to as the tonsils, are lymphatic structures containing indentations called crypts.
The tonsils reside in the tonsillar fossa, which is bounded anteriorly by the palatoglossal arch (Fig. 13-16) and posteriorly by the palatopharyngeal arch. Th
arches contain the muscles of their corresponding names and are also referred to as the anterior and posterior tonsillar pillars, respectively (Fig. 13-33).
The tonsillar fossa is bounded superiorly by the soft palate, and inferiorly by the base of tongue mucosa. Tonsillar tissue frequently extends superiorly and
inferiorly into these structures.
Laterally, the tonsil has a capsule that is formed by the pharyngobasilar fascia. A layer of loose connective tissue separates the capsule from the superior
constrictor muscle. This potential space is the peritonsillar space. Spread of infection from the tonsils into this area results in a peritonsillar abscess,requiring transoral aspiration or incision and drainage. Due to the proximity of the medial pterygoid muscle to t he peritonsillar space (the medial pterygoid
muscle is located lateral to the superior constrictor muscle) (Fig. 13-18), peritonsillar abscesses present with trismus and bulging of the tonsil and soft
palate medially and inferiorly.
The inferior pole of the tonsil lies at the level of the interspace between the superior and middle constrictor muscles (Figs. 13-16, 13-18). Extension of a
peritonsillar abscess laterally in this interspace through the buccopharyngeal fascia results in a parapharyngeal space abscess (Fig. 13-34). This results in
more intense trismus because of the direct irritation of the medial pterygoid muscle. This also places the great vessels of the neck at risk due to their
location in the parapharyngeal space. Inferior dissection of infection through the carotid sheath may result in mediastinitis. The glossopharyngeal nerve
(Figs. 13-33, 13-34) also traverses this interspace between the superior and middle constrictor muscles at the inferior pole of the tonsil and is at risk in
deep dissection during a tonsillectomy.
Fig. 13-34.
The vascular supp ly of the pa latine tons il. (Modified from Hollinshea d WH. Anatomy for Surgeons . New York: Harper & Row, 1968; with permission.)
Five branches of the external carotid artery system supply blood to the tonsils. The main supply is inferiorly from the tonsillar branch of the facial artery
(Fig. 13-34). The ascending pharyngeal, dorsal lingual, ascending palatine branch of the facial artery, and descending palatine artery also supply the
tonsils. Lymphatic drainage of the tonsils is primarily to the jugulodigastric lymph nodes (Fig. 13-26).
Sensory innervation of the tonsil is through the glossopharyngeal nerve and from the greater and lesser palatine branches of the maxillary branch of the
trigeminal nerve (Fig. 13-25). The phenomenon of referred otalgia (Fig. 13-35) in cases of tonsillitis, tumors of the tonsil, and after tonsillectomy is
mediated through common projections of the oropharyngeal fibers of the glossopharyngeal nerve and Jacobsen's nerve. Jacobsen's nerve (Figs. 13-24, 13-
35) is the tympanic branch of the glossopharyngeal nerve that innervates the middle ear mucosa.
8/11/2019 Chapter 13 Pharynx
35/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 35
Fig. 13-35.
Pathw ay of referred o talgia from the oropharynx. (Modified from DeSanto LW, Thawley SE, Genden EM. Treatment o f tumors of the oropharynx: Surgical Therapy.
In: Thawley SE, Panje WR, Batsakis JG, Lindberg RD, eds. Comprehens ive Management of Hea d and Neck Tumors, 2nd Ed. Philadelphia: WB Saunders, 1999; with
permission.)
BASE OF TONGUE
The base of tongue (Fig. 13-17) is the posterior one-third of the tongue which lies posterior to the circumvallate papillae (Fig. 13-16) and foramen cecum,
the area of origination of the thyroid gland. It extends posteriorly to the level of the valleculae, and laterally continues with the floor of mouth mucosa at
the inferior pole of the tonsils (Fig. 13-8). The base of tongue contains submucosal lymphatic collections referred to as lingual tonsils, which, together with
the palat ine tonsils and adenoids (pharyngeal and tubal tonsils), form the previously described Waldeyer's ring (Fig. 13-10), a first line of immunologic
defense. This is also an uncommon area of primary lymphoma presentation.
The sensory innervation of the base of tongue is through the glossopharyngeal nerve, which supplies general visceral afferent fibers and special visceral
afferent fibers for taste. Base of tongue musculature is innervated by the hypoglossal nerve (Fig. 13-24). Arterial supply of the base of tongue is through
the lingual arteries. The base of tongue has a rich lymphatic drainage system primarily to the jugulodigastric lymph nodes (Fig. 13-26). Lymphatic drainage
to both sides of the neck is the rule. This necessitates addressing both the ipsilateral and contralateral neck when treating tumors of the base of tongue,
due to the likelihood of bilateral metastases.
The base of tongue extends posteriorly into paired concavities (valleculae) along the base of the lingual surface of the epiglottis (Figs. 13-8, 13-16). The
valleculae are separated in the midline by a median glossoepiglottic fold and bounded laterally by lateral glossoepiglottic folds (pharyngoepiglottic folds) (Fig
13-16), which attach t he epiglottis to the base of tongue.
The remainder of the oropharynx consists of the posterior pharyngeal wall and lateral pharyngeal wall posterior to the posterior tonsillar pillar.
Laryngopharynx (Hypopharynx)
The laryngopharynx is the longest section of the pharynx, extending from the level of the hyoid bone (Fig. 13-8) superiorly to the inferior border of the
cricoid cartilage at the level of the sixth cervical vertebra. It is wider superiorly and narrows inferiorly. The upper part of the laryngopharynx is the most
caudal portion of the common aerodigestive tract. The lower part, including the piriform recessses and postcricoid area, is the beginning of the separated
digestive tract that leads to the esophagus. The laryngopharynx is divided into the following three separate areas (Fig. 13-16):
Posterior pharyngea l wall
Piriform recesses
Pos tcricoid area
The posterior pharyngeal wall extends from the level of the hyoid bone to the inferior border of the cricoid cartilage and is continuous laterally with the
lateral wall of the piriform recesses.
The piriform recessses are funnel-shaped structures that are open posteriorly to the remainder of the pharynx. They are bounded anteriorly and laterally by
the lamina of the thyroid cartilage, and medially by the aryepiglottic fold, arytenoid cartilage, and cricoid cartilage (Fig. 13-8). The superior extent is at the
level of the pharyngoepiglottic fold (Figs. 13-16, 13-17), and the inferior apex is at the level of the cricopharyngeus muscle (Figs. 13-29, 13-32). This apex
approximates the level of the laryngeal ventricle.
The postcricoid area includes the mucosa covering the area from the posterior cricoarytenoid joint superiorly to the inferior border at the cricoid cartilage
(Fig. 13-8). It is continuous laterally with the medial wall of the piriform recessses and inferiorly with the esophagus.
Sensory innervation of the laryngopharynx is from the glossopharyngeal (Fig. 13-24) and vagus nerves. The posterior pharyngeal wall is innervated by the
fibers of the glossopharyngeal nerve through the pharyngeal plexus. The piriform recessses and postcricoid mucosa are innervated by the internal branch of
the superior laryngeal nerve, which runs beneath the mucosa of the anterior piriform recess. Anesthesia of the piriform recesses and larynx can be obtained
by topically anesthetizing the piriform recess mucosa or by percutaneous superior laryngeal nerve block at the thyrohyoid membrane (Fig. 13-28). The
- -
8/11/2019 Chapter 13 Pharynx
36/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 36
. , .
the superior laryngeal nerve, which runs along the lateral border of the inferior constrictor muscle (Fig. 13-24) with the superior thyroid vascular pedicle.
Previously described, the vascular supply to the laryngopharynx is through the superior and inferior thyroid arteries and their branches (Fig. 13-24). The
lymphatic drainage is through the thyrohyoid membrane to jugulodigastric and midjugular lymph nodes (Fig. 13-26), but also involves the
retropharyngeal/peritracheal and periesophageal lymph nodes. Tumors of the laryngopharynx commonly present at an advanced stage because the large
size of the laryngopharynx allows the malignancy to go unnoticed until obstruction occurs late in the disease process. Tumors present with dysphagia,
hemoptysis, voice change due to laryngeal invasion, and commonly as an enlarged metastatic lymph node in the neck. Referred otalgia (Fig. 13-35) is a
common presenting symptom of hypopharyngeal malignancies. This is due t o the common central project ions of the internal branch of the superior laryngea
nerve, which innervates the piriform recess, and Arnold's nerve (the auricular branch of the vagus nerve), which innervates a portion of the posterior
external auditory canal. Therefore, otalgia in the absence of the obvious ear pathology is an indication to carefully examine the upper aerodigestive tract
for pathology.
SURGICAL CONSIDERATIONS
Injury to the external branch of the superior laryngeal nerve can occur in thyroidectomy if the superior thyroid neurovascular pedicle is ligated high. Avoid
injury to the superior laryngeal nerve when clamping the superior thyroid pedicle by observing the following precaution. Ligate the vascular pedicle at the
capsule of the superior pole of the thyroid gland, inferior to the point of divergence of the external branch of the superior laryngeal nerve away from the
vascular pedicle, toward the cricothyroid muscle.
Read an Editorial Comment
Because of the close relationship of the laryngopharynx to the larynx, and the advanced presentation of hypopharyngeal tumors, surgical resection often
involves total or near-total laryngopharyngectomy. The propensity for submucosal extension of disease in the esophagus creates tumors that involve the
inferior apex of the piriform recess and/or the postcricoid mucosa. These often require esophagectomy in addition to total laryngopharyngectomy to ensure
adequate margins of resection in the esophagus. Then total pharyngeal reconstruction can be performed. Use a free jejunal or tubed fasciocutaneous flap in
the case of cervical pharyngeal defects. For pharyngoesophageal defects, use gastric pull-up.
Physical Examination of the Oropharynx and Laryngopharynx
Examination of the oropharynx can easily be performed with the use of tongue depressors. Gentle compression of the middle third of the t ongue inferiorlywith slight anterior traction will allow adequate visualization of the tonsils, anterior base of tongue, soft palate, and posterior pharyngeal wall. For patients
with hyperactive gag reflexes, topical anesthetic can be used to improve visualization. Examination of the base of tongue and valleculae require gentle
anterior retraction of the tongue with a gauze pad and indirect examination with the use of a laryngeal mirror. The mirror is placed superiorly in the
oropharynx with the back of the mirror elevating the soft palate and uvula without contacting the posterior pharyngeal wall to avoid gagging the patient. In
addition to visualization, palpation of the tonsils and base of the tongue with the finger is helpful in detecting mucosal and submucosal abnormalities.
Examination of the laryngopharynx and larynx requires use of a laryngeal mirror or a fiberoptic laryngoscope through the nasal cavity. The larynx and vocal
cord motion should be evaluated. The piriform recesses can best be visualized with the patient phonating. This brings the aryepiglottic folds and arytenoid
cart ilages medial, thereby opening the piriform recesses. The presence of saliva pooling within a single piriform recess should raise suspic ion of a lesion
within that space. The presence of a unilateral paralyzed vocal cord should also raise suspicion of a tumor involving the piriform recess and extending to th
paraglottic space. The posterior pharyngeal wall can also be easily visualized with a mirror or flexible laryngoscope.
The postcricoid area is difficult to visualize with either of these techniques and requires direct laryngoscopy under general or topical anesthesia. The
laryngopharynx, in general, is best visualized with direct laryngoscopy. The laryngoscope is directly inserted into the vallecula. It can then be slid laterally
into the piriform recess, elevating it anteriorly to see the anterior portion of the piriform recess. When the laryngoscope is inserted deeper to the apex of
the piriform recess both the medial and lateral walls can be visualized. The laryngoscope can then be rotated medially into the postcricoid area, by lifting
the larynx anteriorly to open the postcricoid area and esophageal inlet. The laryngoscope is then moved into the contralateral piriform recess. The posterio
pharyngeal wall is also visualized when the larynx is lifted anteriorly by elevating the postcricoid mucosa.
When examining the neck, grasping the thyroid cartilage and moving it from side to side over the top of the cervical spine should produce normal laryngeal
crepitus as the cartilage of the larynx rolls over the bony cervical spine. Absence of this laryngeal crepitus suggests a posterior pharyngeal or postcricoid
mass that is preventing the cartilage-to-bone contact. This portion of the examination should be performed routinely during evaluation of the larynx and
pharynx.
PHARYNGEAL RELATIONSHIP TO DEEP NECK SPACES
The oropharynx has very important relationships to surrounding potential deep neck spaces, including the retrovisceral spaces (Fig. 13-22) and the
parapharyngeal space (lateral pharyngeal space). Although not part of the pharynx, these spaces may be involved with pathology that originates in the
pharynx or encroaches upon the pharynx. Knowledge of the anatomy of these spaces and their relationship to the pharynx is integral to understanding the
surgical approaches to these spaces and the perils and pitfalls of these approaches.
Retrovisceral Space
The area posterior to the pharynx (the retrovisceral space) (Fig. 13-22) can be separated into the following three spaces (Figs. 13-23, 13-27):
Retropharyngea l space
Danger space
Prevertebral space
The retropharyngeal space is bounded by the buccopharyngeal fascia anteriorly and by the alar layer of prevertebral fascia posteriorly. Laterally, it is
continuous with the parapharyngeal space. The parapharyngeal space extends from the skull base superiorly to the level of the tracheal bifurcation
(approximately the level of the fourth thoracic vertebra), where the alar layer of prevertebral fascia fuses with the middle layer of deep cervical fascia. The
retropharyngeal space contains lymph nodes (nodes of Rouvier) in addition to connective tissue. Infections and abscesses in the retropharyngeal space are
usually unilateral in presentation due to the posterior midline attachment of the midline raphe of the superior constrictor muscle to the prevertebral fascia.
The danger space is bounded anteriorly by the alar fascia and posteriorly by the prevertebral fascia. It extends superiorly from the skull base to the
dia hra m inferiorl .
http://windowreference%28%27editorialcomment%27%2C%27editorialcomment.aspx/?aID=70972&comment_aID=71078%27);http://windowreference%28%27editorialcomment%27%2C%27editorialcomment.aspx/?aID=70972&comment_aID=71078%27);8/11/2019 Chapter 13 Pharynx
37/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 37
The prevertebral space is bounded anteriorly by the prevertebral layer of prevertebral fascia, posteriorly by the vertebral bodies, and laterally by the
transverse processes. It extends superiorly from the skull base to the coccyx inferiorly.
Involvement of these spaces with infection may occur from suppuration of retropharyngeal nodes, penetrating injury, or spread from adjacent spaces.
These spaces may be approached either transorally or transcervically.
Parapharyngeal Space (Lateral Pharyngeal Space)
The parapharyngeal, or lateral pharyngeal, space (Figs. 13-27, 13-36) is typically described as an inverted pyramid-shaped space located lateral to the
pharynx. Its superior extent is at the skull base, including a small portion of the temporal bone and a fascial connection from the medial pterygoid plate to
the spine of the sphenoid medially. It extends inferiorly to the level of the greater cornu of the hyoid bone at its junction with the posterior belly of the
digastric muscle. The superior medial border is formed by the fascia of the tensor veli palatini (Fig. 13-27) and medial pterygoid muscles and the
pharyngobasilar fasc ia. Inferiorly, the medial border is formed by the superior constrictor muscle. The anterior border is formed by the pt erygomandibularraphe. The lateral boundaries are the medial pterygoid muscle, the mandible, the deep lobe portion of the parotid gland, and a small portion of the digastric
muscle posteriorly. The posterior border is the prevertebral fascia.
Fig. 13-36.
Frontal view of the parapha ryngeal space. (Modified from Hollinshead WH. Anatomy for Surgeons . New York: Harper & Row, 1968; with permission.)
The parapharyngeal space is divided into a pre- and retrostyloid compartment (Fig. 13-27) by fascia extending from the styloid process to the tensor veli
palatini muscle. The pre-styloid compartment contains lymphatic tissue, the internal maxillary artery, and further branches of the mandibular branch of the
trigeminal nerve. The retrostyloid compartment contains the carotid artery, internal jugular vein, cranial nerves IX, X, XI, and XII, and the cervical
sympathetic chain (Figs. 13-27, 13-36).
Surgical Considerations
Masses or infections in the parapharyngeal space present as a fullness or bulging in the lateral pharyngeal wall, displacing the tonsil medially and/or the soft
palate medially and inferiorly with contralateral deviation of the uvula. Trismus is a frequent finding, especially with parapharyngeal space abscesses or larg
tumors. These are caused by irritation or involvement of the medial pterygoid muscle, which forms the lateral extent of the parapharyngeal space.
8/11/2019 Chapter 13 Pharynx
38/40
5/24/2014 Print: Chapter 13. Pharynx
http://web.uni-plovdiv.bg/stu1104541018/docs/res/skandalakis'%20surgical%20anatomy%20-%202004/Chapter%2013_%20Pharynx.htm 38
, .
or tumors in this space may enter the carotid sheath and place the carotid arteries and the internal jugular vein at risk. Infections may also spread inferiorly
in this space through the mediastinum and the carotid sheath. Drainage of parapharyngeal abscesses or removal of tumors in the parapharyngeal space
should be performed by external approaches to ensure control of the great vessels and major nerves in the retrostyloid compartment. Do this especially in
the case of tumors where the neurovascular structures may be displaced.
Penetrating injuries through the lateral wall of the oropharynx may result in injury to structures in the parapharyngeal space. Injuries that are more posterio
result in damage to the carotid artery, internal jugular vein, or upper cranial nerves. Injuries that are more anterior may result in damage to the parot id
gland, duct, or intraparotid facial nerve. Patients with these types of injuries require observation and serial neurological examinations or carotid arteriogram
to rule out vascular injuries.
We quote Leitner and Johns2on pharyngolaryngectomy for carcinoma of the posterior pharyngeal wall:
Along with neck dissection, we use an extended posterolateral pharyngectomy which includes the primary site, the retropharyngeal lymph nodes, andthe cervical lymph nodes in the resected specimen. T2 and T3 carcinomas can be effectively removed en bloc with the retropharyngeal and neck
dissection specimen. Primary closure has been used in all cases, with minimal functional rehabilitation necessary, and postoperative radiotherapy is
given to the primary site and both sides of the neck.
Sessions et al.3wrote about metastasis in hypopharyngeal cancer:
All treatment plans for hypopharyngeal cancer must consider certain facts: The overwhelming majority of these lesions metastasize to cervical lymph
nodes, and in the case of the posterior pharyngeal wall, bilateral metastasis is the rule rather than the exception; 40% of posterior pharyngeal wall
lesions and probably an equal number of upper pyriform sinus lesions metastasize to t he retropharyngeal nodes; in those patients with c linically
negative necks, the incidence of occult metastasis is substantial; and between 20% and 30% of pyriform sinus lesions, and probably an equal number
of posterior pharyngeal wall lesions, are associated with distant metastasis. Even in the lesser-stage hypopharyngeal lesions, the high rate of
regional metast ases requires inclusion of the neck(s) in all management plans.
HISTOLOGY
From outside to inside, the pharyngeal wall is formed by the buccopharyngeal fascia, muscular layer, fibrous layer, and mucosa.
The buccopharyngeal fascia is a thin layer covering the epimysium and, for all practical purpose s, corresponds to the externa l part of the epimysium.
The muscular layer (superior, middle, and inferior constrictor muscles) and its fibrous network is described previously in connection with the several parts of the
pharynx.
The fibrous layer supports the mucosa that rests on it.
The mucosa of the pharynx may be divided into three pa rts. The anterior portion consists of ciliated and pseudostratified epithelium. The trans itional layer is
columnar epithelium. The posterior layer is non-keratinized stratified squamous epithelium. Several mucous g lands are present.
PHYSIOLOGY
Coordinated movements of the palatal and pharyngeal muscles take place during both swallowing and speech. As previously mentioned the velum (soft
palate and uvula) is instrumental in c losing the nasopharynx during speech.
Certain sounds, such as fricatives, require closure of the nasopharynx by the velum. Closure of the velopharyngeal port (sphincter) is a very complex
sequence of rapid muscle actions. The soft palate elevates toward the posterior pharynx with the levator veli palatini. The muscles of the uvula draw it
upward and forward. The palatoglossus, which forms the anterior tonsillar pillar, narrows the caudal nasopharynx and draws the soft palate down.
Swallowing is a very complex sequence of involuntary events, starting with velopharyngeal closure to prevent reflux. In the first phase of swallowing, the
food bolus enters the mouth and the soft palate tenses and elevates. It is then drawn downward to strip the bolus from the valleculae. The tongue
projects the bolus from the oropharynx into the laryngopharynx.
The three paired constrictor muscles (Figs. 13-18, 13-28) are important in the second phase of swallowing (pharyngeal phase). This is an involuntary phase
that involves the serial contraction of the pharyngeal constrictor muscles in a superior-to-inferior direction to propel a bolus inferiorly.
The cricopharyngeus muscles, unlike the remaining portions of the constrictor muscles, have a tonic level of contraction, allowing them to function as the
upper esophageal sphincter. Relaxation of the cricopharyngeus muscle is necessary to allow the passage of a bolus from the pharynx to the esophagus.
Failure of the cricopharyngeus muscle to relax results in dysphagia. This may be the result of a neuromuscular disease such as amyotrophic lateral sclerosis
polymyositis, myasthenia gravis, multiple sclerosis, Parkinson's disease, or cerebrovascular accidents. Cricopharyngeal achalasia, which may be idiopathic or
the result of gastroesophageal reflux or other etiologies, is failure of the cricopharyngeus muscle to relax.
In the pharyngeal phase of swallowing, the larynx also elevates and moves forward under the base of tongue to aid in protection against aspiration. The
epiglottic folds also move caudal and backward and strip the epiglottic