-
Chapter 20: Pancreatic Disease in Adults
Mary Phillips (Guildford), Irantzu Arregui-Fresneda
(Southampton),
Sinead Duggan (Dublin), Kathryn Freeman (Sheffield), Laura
McGeeney (Cambridge)
The Royal Surrey County Hospital NHS Foundation Trust
Regional Hepato-Pancreatico-Biliary Unit (Surrey and Sussex)
-
Pancreatic Disease
• Developing Guidelines • Content • Future work
-
Developing the Guidelines
• ‘ New’ Dietetic speciality • Regionalisation of services in
2003-5 • 22 x specialist centres:
– Severe cases acute and chronic pancreatitis – Pancreatic
resection
• Annual meetings of NIGPS at the Pancreatic Society of Great
Britain and Ireland est. 2008
• Dozens of requests for help with patient management
• Issues with pancreatic enzyme use within dietetics
-
Literature....
71% response rate from 31 specialist centres (prior to
completion of centralisation of services.)
-
Post operative feeding
-
Type of feed and pre-op assessment
-
Is there a concern about nutrition?
• 37.5% of readmissions due to malnutrition / dehydration
(Grewal et al, 2011)
• 65-68% patients malnourished prior to surgery (Wigmore et al,
1997, Schnelldorfer & Adams, 2005, Jo et al, 2006)
• Concern over undiagnosed DM and PEI prior to surgery.
-
Implications of malnutrition
• Poor wound healing (Gupt & Ihmaidat, 2003) • Readmissions
(37.5% Grewal et al, 2011) • Increased risk of pancreatic fistula
(Kanda et al, 2011) • Chest infection (Gupt & Ihmaidat, 2003) •
Reduced performance status (Barber et al, 1999) • Increased
morbidity in PD (25.7% - 37%, Crucitti et al, 1998) • Increased
mortality in PD (8.1% to 18.5%, Crucitti et al, 1998) • Prolonged
length of stay (Garth et al, 2010)
-
Pancreatic Enzyme Replacement Therapy (PERT)
-
Funding!
-
Duggan S.N., Smyth N.D., O’Sullivan M., Feehan S., Ridgway P.F.
& Conlon K.C. (2012) A transatlantic survey of nutrition
practice in acute pancreatitis. J Hum Nutr Diet.
doi:10.1111/j.1365-277X.2012.01256.x
-
253 Dietitians responded from UK, Ireland and Canada
-
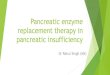
Timing of nutritional support
Is feeding being delayed in obese patients? Early enteral
feeding is recommended, but only
48.7% (DGH) / 64.8% (University Hospital) aimed to do so.
-
Benefit of feeding in the first 48 hours
Petrov M.S, Pylypchuk R.D, Uchugina A.F, A systematic review on
the timing of artificial nutrition in acute pancreatitis. British
Journal of Nutrition 2009;101:787-793
-
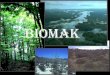
Route of feeding
-
Barriers to feeding
-
Awareness of national / international literature
-
PENG guide
• Acute Pancreatitis – Requirements; feeding routes,
• Chronic Pancreatitis – Requirements; micronutrients
• Pancreatic Cancer – operable and palliative – Duodenal
stents
• Pancreatic Enzyme Replacement Therapy (PERT)
-
Requirements in AP Nutrient Requirements 1,2
Energy 15-25kcal/kg in early stage of complicated disease
25-35kcal/kg in stable disease / recovery phase
Protein 1-1.5 g/kg/day
Fat 30% of total energy
Carbohydrates 50% of total energy
Feed Type Peptide feeds are likely to be required in patients
with extensive
disease 1,2,8
Some patients may tolerate standard polymeric feeds15
Monitoring As per Chapter 6: Monitoring, plus:
Triglycerides 1,16
Blood Glucose 1
Pain, especially if associated with EN
-
Management of Complications Post Op Complications Dietetic
Management
Delayed gastric emptying:
(nausea, vomiting, early
satiety)
Pro-kinetics, good blood glucose control, small frequent meals
and snacks. In practice
patients often have NJ feeding or TPN followed by gradual
reintroduction of liquids / soft
moist diet.
Pancreatic leak/ fistula No specific dietary changes required.
Some units use NJ feeding and NBM to reduce
stimulation of pancreatic enzymes.
Chyle leak Replace fluid and electrolytes losses. Nutrition can
be provided by TPN, EN with an MCT
feed, a minimal fat oral diet or an oral MCT diet.
Dumping syndrome (in the
presence of partial
gastrectomy)
Smaller, more frequent meals, limiting fluid consumption during
meals, eating fewer simple
carbohydrates, eat more complex carbohydrates and foods high in
soluble fibre, laying down
after eating
Weight loss See below
Micronutrient deficiency (due to
poor intake or malabsorption)
Individual micronutrient or multivitamin/mineral
supplementation. PERT if required
Diabetes (especially if blood
sugars are deranged before
resection) 34
Insulin, tablets or diet treated as appropriate. Anecdotally,
diabetes is more common after a
distal pancreatectomy than after pancreatico-duodenectomy
-
Where now.....
• NICE guidelines – Acute Pancreatitis – Chronic Pancreatitis –
Pancreatic Cancer
• Multi-centre trials to strengthen evidence • Education
sessions in surgical / gastroenterology
conferences • Work with pharmacy regarding PERT PGD’s and
prescribing
-
We would like to thank • PENG for supporting the development
of
this chapter • Abbott Healthcare for financially
supporting our annual meeting
-
Thank you Any Questions?
Chapter 20: Pancreatic Disease in AdultsPancreatic
DiseaseDeveloping the GuidelinesLiterature....Post operative
feedingType of feed and pre-op assessmentIs there a concern about
nutrition?Implications of malnutritionPancreatic Enzyme Replacement
Therapy (PERT)Funding!Slide Number 11Slide Number 12Slide Number
13Timing of nutritional supportBenefit of feeding in the first 48
hoursRoute of feedingBarriers to feedingAwareness of national /�
international literaturePENG guideRequirements in APManagement of
ComplicationsWhere now.....Slide Number 23Slide Number 24