Embed Size (px)
Citation preview

Chapter 3
Non-incineration Treatment Technologies and Trends
Of the still unresolved issues regarding medicalwaste management, one of the most critical is whichtechnologies and controls are most appropriate fortreatment. 1 Clearly, the answer depends on theparticular circumstances of the medical waste gener-ator and the host community for the treatmentfacility. Factors such as the nature (quantity andtypes) of the medical waste, the availability ofpermitted landfill space, local air quality conditions,and other demographic and geographic factors (e.g.,urban v. rural locations) need to be considered whenselecting the most appropriate management strategy.Safety, reliability, and costs of alternative treatmentmethods and the regulatory certainty associated withtheir use also affect selection of treatment alterna-tives. Knowledge of various incineration and non-incineration alternatives can also facilitate adoptionof medical waste policies at all levels of government.
While some States and localities actively encour-age incineration as a preferred method of treatment,others have enacted moratoriums on incinerators tosuspend permitting until further information on thesafety of the option is available or new regulationsgoverning it are completed. Thus, incompletenessand uncertainty characterize regulatory activity formedical waste management.
The dilemma now facing New York State facili-ties, for example, can occur elsewhere dependingupon how a State adopts regulations. Facilities theremust make management decisions regarding whetherto upgrade existing on-site incinerators no later thanthe fall of 1990 in order to be able to meet New YorkState’s new air quality standards by January 1, 1992.At present many facilities are seeking treatmenttechnologies alternative to incineration; however, todate the State Health Department has not developedand implemented standards for the approval oftreatment alternatives. As a result, the State govern-ment is limiting the available treatment technologiesto the previously approved methods of incineration
and autoclaving. This delay in the evaluation andapproval of alternative technologies may preventmany New York State facilities from using them,including technology already approved in otherStates and/or technology which could be moreattractive from both financial and environmentalperspectives (94).
This chapter, based on available information,addresses the variety of available and emergingnon-incineration treatment alternatives, their techni-cal capabilities, and their risks and costs. First,treatment of medical wastes by autoclaving (i.e., aprocess of steam sterilization), the most frequentlyemployed alternative to incineration, is discussed.Then, a number of other alternative treatments areexamined: steam disinfection and compaction; mechani-cal/chemical disinfection; microwaving; irradiation;and other emerging treatment technologies. 2 Chap-ter 4 discusses various incineration options, includ-ing co-incineration and regional incineration, andpollution control issues, as well as risk and costimplications. A comparison of non-incineration andincineration treatment alternatives is included inchapter 6.
Increasingly, questions are raised about the avail-ability and performance of non-incineration treat-ment alternatives for medical wastes. While themajority of medical waste is autoclave or inciner-ated, some medical waste (treated or untreated) islandfilled, including some categories of infectiouswastes. The State of Washington found in its surveyof medical facilities that some infectious wastes areabout as frequently treated by autoclaving as byincineration (139). In addition, other treatmentmethods, including disposal into the sewer system,are not rare. It should be noted again that mosttreatment alternatives some form of solid wastedisposal, usually either incineration or landfilling,will be necessary.
IIt sho~d be not~ tit ~~tment in this repofl refers to a process to render wastes noninfectious, unless otherwise indicated, sucb as ~atment toreduce toxicity of wastes, or treatment to render wastes nonrecognizable.
z~s ~~pter relies on tie Om con~act repo~ ‘‘Medical Waste Treatment Tw~ologies,’ completed by Robert Spurg@ Spurgin & Associates,March 1990. See alSO (30) and (73). It should be noted tht mention of a specific company or treatment technology does not constitute endorsementof it by OTA. OTA tloes not endorse any specific application of the various incineration and nonincineration treatment alternatives.
–27-

28 ● Finding the Rx for Managing Medical Wastes
The viability of alternative technologies hasincreased in recent years due to the increased costof incineration, the difficulty associated withpermitting incinerators, and the perceived desir-ability of reducing dependence on incineratorsgiven concerns over their emissions. A number ofStates (e.g., New Jersey, California, Washington)are attempting to encourage adoption of alternativetechnologies for such reasons. EPA is conductingseveral research projects to evaluate various wastetreatment technologies as required by MWTA (92).
The extent of detail contained in these EPAstudies is not known, but the Agency does report that‘‘most of the treatment technologies are as effective[as incineration] in rendering medical waste nonin-fectious” (141). In addition to the usually highercapital, maintenance, and operating costs of inciner-ation, EPA cites the public perception problems anduncertain regulatory climate associated with inciner-ation as disadvantages of incineration compared toalternative treatment technologies (141). Landfillavailability and other factors, however, will alsoinfluence a medical or health-care facility’s choiceof treatment technology.
Alternative treatment technologies are less capitalintensive and have fewer emission concerns thanincineration processes. Although it is important torecognize that oftentimes more than one treatmenttechnology may be needed to manage all compo-nents of the waste stream (e.g., incineration ofpathological wastes that cannot be autoclave).Further, the nature of emissions and efficacy of newtreatment technologies must be demonstrated.
AUTOCLAVINGHistorically, autoclaving or steam sterilization
has been used as a treatment method in laboratorysettings to sterilize microbiological laboratory cul-tures (104).3 The first commercial steam sterilizationprocess for medical infectious waste was introducedin California in 1978. As incineration requirementswere tightening in California, it became clear thatinsufficient off-site capacity existed to replace
closed on-site incinerators, which would not meetthe State air emission standards (see ch. 5).
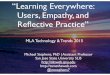
Autoclaving is a process by which wastes areeither sterilized or disinfected prior to disposal in alandfill (114) (see figure 2).4 Autoclaving can be asterilization process if all microorganisms are ex-posed to the steam for a sufficient temperature/pressure/time period to assure their destruction. The routineachievement of sterilization can be monitored byplacing Bacillus stear other mophilus spores into thecenter of a load to be autoclave. If the sporessurvive, then the conditions for sterilization have notbeen achieved; if the spores are destroyed (i.e., failto grow in microbiological media after steamsterilization), then the conditions for sterilizationhave been achieved (given the practical limitationsof this routine test).
If the spores have not been destroyed during steamsterilization, then sterilization has not occurred.However, some level of disinfection of the wastewould likely have resulted. Unfortunately, the levelof disinfection cannot be routinely or practicallymeasured. Sterilization of infectious waste is gener-ally regarded as “overkill” for most waste disposalsituations. Disinfection of infectious waste is proba-bly a more reasonable goal for most infectiouswastes, though some appropriate and measurabledisinfection goal should be established (1 11).
Most steam sterilizers in use for treating infec-tious wastes are of the high-vacuum type (92). In theautoclaving process, bags of infectious waste areplaced in a chamber and steam is introduced for adetermin ed period of time (usually about 15 to 30minutes) and pressure. The use of pressure helpsreduce the required time for disinfection of medicalwastes, yet the amount of time required will still varydepending on the type and volume of waste (141).Steam temperatures are usually maintained at 250‘For slightly higher (to disinfect the waste morequickly and allow for shorter cycle times).
Autoclaving parameters, e.g., temperature andresidence/cycle time, are determinedby the factorsinfluencing the penetration of steam to the entire
sEthylene oxide and other gas sterikation processes are typically used to sterilize processes for medical equipmen~ but are dSO SOmebes used totreat wastes. EPA, however, does not recommend ethylene oxide for treating infectious wastes because of its toxicity and given that other treatmentoptions are available (122).
4st~~ation i5 a Pmwss tit des~oys ~ ~cmorg~5m5 (e.g., Pathogem). Disinfection is a process intended to reduce the n u m b e r o fmicroorganisms or pathogens as low a level as possible, at least below the level at which exposure to a susceptible host could not result in an infectiousdisease. Actual sterilization is not likely to be maintained once wastes leave the autoclave, m is true of incineration ash residue (see studies cited in 134);thus, disinfection is a more accurate term.
Chapter 3-Non-incineration Treatment Technologies and Trends ● 29
Figure 2—Autoclave
SOURCE: AMSCO, Erie, PA.
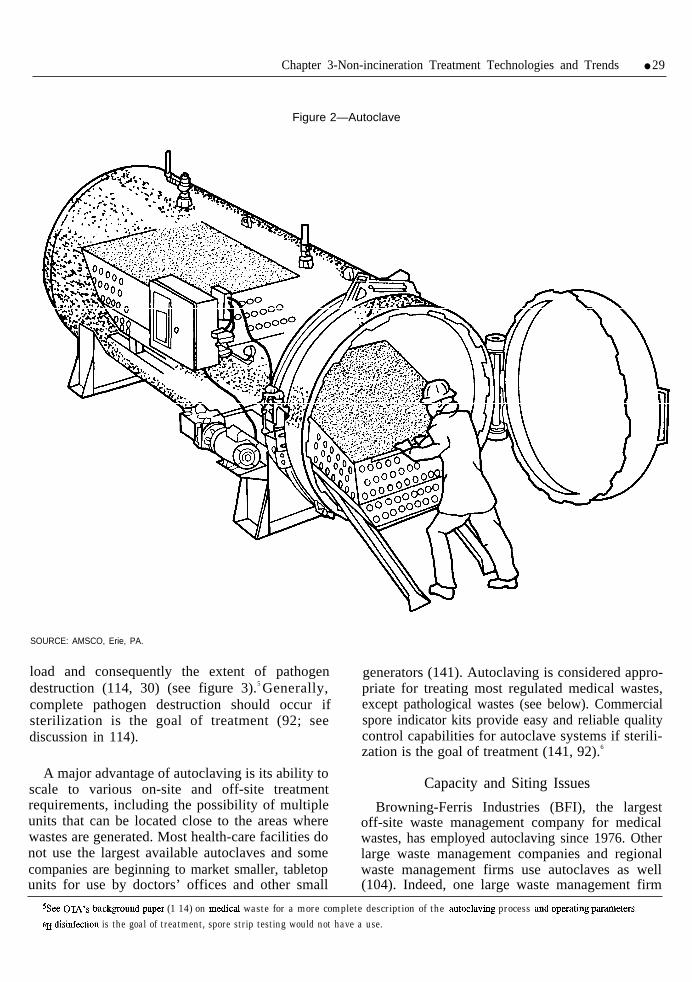
load and consequently the extent of pathogendestruction (114, 30) (see figure 3).5 Generally,complete pathogen destruction should occur ifsterilization is the goal of treatment (92; seediscussion in 114).
A major advantage of autoclaving is its ability toscale to various on-site and off-site treatmentrequirements, including the possibility of multipleunits that can be located close to the areas wherewastes are generated. Most health-care facilities donot use the largest available autoclaves and somecompanies are beginning to market smaller, tabletopunits for use by doctors’ offices and other small
generators (141). Autoclaving is considered appro-priate for treating most regulated medical wastes,except pathological wastes (see below). Commercialspore indicator kits provide easy and reliable qualitycontrol capabilities for autoclave systems if sterili-zation is the goal of treatment (141, 92).6
Capacity and Siting Issues
Browning-Ferris Industries (BFI), the largestoff-site waste management company for medicalwastes, has employed autoclaving since 1976. Otherlarge waste management companies and regionalwaste management firms use autoclaves as well(104). Indeed, one large waste management firm
ssee C)W’S back~o~d paper (1 14) on medic~ waste for a more complete description of the autoclaving process md Operadng P~eters.blf dis~ection is the goal of treatment, spore strip testing would not have a use.

30 ● Finding the Rx for Managing Medical Wastes
Figure 3—Typical Sterilization Destruction Curve
‘F ‘C
250(1 27)
240(1 16)
220(104)
200(93]
180(82
160(71)-
140(60)-
120(49)
100(38)
Temperature
O 5 lb microbiological wastes
● 15 lb microbiological wastes
10 20 30 40 50 60 70 80 90
Time (rein)
SOURCE: William Rutala et al., “Decontamination of Microbiological Wasteby Steam Sterilization,” Applied Environment/ Microbiology,vol. 33, 1982.
reports that it is currently siting more autoclavesthan incinerators. Meanwhile, some hospitals con-tinue to use on-site autoclaves for treating their ownmedical waste. The demand for autoclaving appearsto be increasing across the Nation, as the rest of thecountry begins to experience the shift from heavyreliance on incineration and the increased need foroff-site medical waste treatment that emerged inCalifornia in the late 1970s.
A major advantage of autoclaving is the capacitya single unit can provide without the spatial require-ments associated with incineration systems. Thecapacity of an autoclave is a function of its size andthroughput. 7 For example, an autoclave capable ofdisinfecting 4,000 pounds per hour of medical wastemeasures 8 feet in diameter by 24 feet in length,which means it occupies about as much space as a500-pound-per-hour incinerator (104).
Autoclaving maybe limited in some applicationsbecause wastes that are only autoclave are stillrecognizable-unless they are then shredded orcompacted (see below).8 EPA points out that the‘‘recognizability’ of medical wastes is only an issuein States covered by MWTA and that most Stateshave not found it necessary or practical to adopt sucha requirement (141). The potentially high costs ofrequiring the nonrecognizability of treated wasteshave led some to question the wisdom of a require-ment to address solely an aesthetic concern.
In the past, landfill refusals of autoclave medicalwastes frequently occurred. A variety of reasonsaccount for these refusals, but usually they happenedbecause landfill operators could not easily identifywhether waste had been treated and disinfected.Efforts to use bags that change in some visible wayin response to autoclaving (e.g., that melt in theautoclaving process or have a strip that changescolor) apparently have met with mixed results (104).A nonrecognizability requirement is one solution tothis problem, albeit a potentially costly one.
Another solution is for commercial users to havetheir own private, permitted landfills for disposal.Informal discussions by OTA with a number ofhospital officials across the country indicate, how-ever, that few refusals occur if a hospital worksclosely with landfill operators to explain their wasteprocedures. The State of Washington reports fromits 1989 survey that 86 percent of the hospitalsresponding to the survey have not had a wastecollector or landfill refuse to accept its wastebecause of its potentially infectious nature (139).
For States under the MWTA program, wastesmust be treated and destroyed or rendered nonrecog-nizable to be exempt from the tracking program.This would necessitate that some form of shredding
7~e ~~e of tie autoclave loading hopper and the cycle time needed for disinfection% however, affect and limit autoclave ~ou@Put (63).8Histofic~ly, proble~tic operation has also been a factor leading some hospitals to abandon autoclavfig (1 14). Appmently, re~nt ~Provements
in the technology have minimiz ed some of these concerns. Proper operatio% however, is key to the effective functioning of any treatment technology.

Chapter 3--Non-incineration Treatment Technologies and Trends ● 31
be employed before shipping the autoclave wasteoff-site; otherwise use of the manifest form would berequired to meet the tracking requirements. Anoption for Congress is to amend MWTA (orrelated follow-ens) to allow verified autoclavedwastes to be exempt from manifesting. Thisessentially means modifying the nonrecognizablecriteria of the regulatory program.
Suitability for Different Medical Wastes andAssociated Risks
Some wastes are not suitable for autoclaving.‘‘ Suitability,’ however, is determined by bothtechnical and nontechnical factors. For example,particular pathological wastes are sometimes con-sidered unsuitable for autoclaving (principally foraesthetic reasons, i.e., they will not be renderednonrecognizable). 9 In any case, approximately 90percent of the regulated medical wastes generatedare suitable for autoclaving (104). Autoclaving isconsidered particularly appropriate for microbiolog-ical wastes (e.g., laboratory cultures). In contrast,autoclaves are not suitable for cytotoxic and othertoxic chemical wastes because of the hazardousnature of these wastes. In addition, contaminatedanimal bedding is not autoclave.
To the extent that autoclaving is used for only aportion of medical wastes, then it can be used as asupplement, more than a substitute for incineratingmedical wastes. Yet, if wastes are segregated fortreatment based on their chemical and physicalcharacteristics, it is likely that a smaller fraction ofwaste will require incineration. Additional segrega-tion of the items requiring incineration (or othertreatment) is not usually necessary since thesewastes are generated and/or managed separately .10
Documented health impacts from autoclaving donot exist. It is of critical importance that certainwastes, due to their either hazardous or pathological
nature, not be autoclave. For example, autoclavinghazardous materials such as antineoplastic agents,radioisotopes, solvents, or other toxic wastes couldlead to chemicals being volatilized by the steam andcould result in possible worker exposure betweenprocess cycles. If autoclaves are of a gravity-displacement type, steam “escapes” through an
outlet vent, most of which is condensed and drainedinto the sanitary sewer.11
Potentially, if the waste itself contains traceelements of formalin or other carcinogenic com-pounds, workers could be exposed to the aerosolizedcompounds if they come in contact with the ventingsteam (104). Once again, the importance of separat-ing waste materials for diversion to the mostappropriate treatment method is evident (e.g., in thiscase, hazardous materials to a hazardous wastetreatment option). Further study of emissions fromautoclaves is warranted based on the fact thatinfectious wastes may contain significant levels ofcytotoxic compounds or low level radioactivewastes and concerns that the presence of suchsubstances could lead to emission problems.
A noticeable odor in the steam discharge, de-scribed by one knowledgeable observer as ‘‘muchlike styrofoam cups tossed in a campfire,” is notknown to be harmful (104). Odor-controlling tabletsthat can be added to each autoclave load areavailable. 12 The potential for problems with landfillleachate associated with autoclave waste is notknown, but in general the survival of viruses in solidwaste leachate does not seem to occur.13
Costs and Volume Reduction Issues
Autoclave units are generally not as costly ason-site or off-site incineration alternatives. Anautoclave unit will cost between $30,000 and$100,000 installed (depending on the size of theunit), with annual operating costs at about $0.05 to0.07 per pound plus labor, with an expected equip-
me phrase “pathological wastes” throughout this report refers to wastes of human origin (e.g., tissues, organs, body parts). Pathogens andpathogenetic wastes should be distinguished from pathological wastes (of human origin). Pathogens and pathogenetic wastes are components of themicrobiological waste type (see ch. 1).
~~or exmple, in most hospitis all tissue samples are transferred to pathology for amlysis before disposal and can be collected separately here forincineration.
ll~ese disch~ges t. he s~tw sewer system should be fiocuous ~ their impact although ~ ~dus~~ waste water discharge pefit may berequired by the local sewage distict authority (see ch. 5).
]@TA&d not dete~e Whether these table~ m~kthe odor orac~ly c~gethe chefis~, orwhether their effect makes a differencefrom a h~~health perspective.
13 See litera~e review ~d discussion by ~nberg (1 10), from w~ch the au~or concludes tit reseach hS not esmblished a relationship betweenlandfill leachate and solid waste and disease, and that obtaining evidence of such a relationship is difficult and further research is necessary. Also seerefs. 138, 103, 44.

32 ● Finding the Rx for Managing Medical Wastes
ment lifetime of 10 to 15 years. Landfill costs mustalso be taken into account, but overall this treatmentoption appears less expensive than incineration andmanagement of its ash residue (if it has to be sent toa hazardous waste landfill). The State of Californiaconcluded from its preliminary cost data that auto-claving and other non-incineration alternatives maybe more economical for some small medical facili-ties than retrofitting existing incinerators to meettheir newly proposed air emission control measure(108).
If autoclave waste is not subsequently com-pacted or shredded, there is no significant volumereduction. Yet, given that medical waste representssuch a small percentage of the solid waste stream, itdoes not pose a significant contribution to landfillcapacity problems experienced in some areas of thecountry (and landfill waste cost is usually chargedon a weight rather than a volume basis). Forexample, California reports that if all on-site incin-erators are abandoned for alternative treatmentmethods, the medical waste requiring landfillingwould only represent 0.03 percent of the wastecurrently handled at MSW landfills in the State(108).
AUTOCLAVING ANDCOMPACTION
High-vacuum steam sterilization combined withthe compaction of treated waste began in Californiain 1978 and is increasingly being used in theNortheast and Mid-Atlantic areas of the country. Asof May 1990, over 100 units are in operation. Thistreatment process combines an autoclave with astationary compaction unit intended to handle theregulated medical waste as well as the solid wastefrom a health-care facility (see figure 4). The systemis designed to be used as an on-site treatmentalternative (104, 48, 30).14
The high-vacuum autoclave removes air, whichacts as a steam displacement barrier, and therebyshortens the time for the steam to achieve thenecessary operating temperature (approximately 284°F) and permeate the entire waste load. This meansthat exposure to the waste is faster and the cycle timeis reduced, which is estimated to be between 40 and50 minutes from loading to loading (104).
The disinfected waste is then hydraulically fedinto the solid waste hopper, where it is compactedwith general refuse from the facility and automati-cally fed into the refuse bin or trailer for hauling toa solid waste facility. Operators are not exposed tothe treated medical wastes, reducing the risk ofexposure to sharps, fluids, or other waste items. Aswith most autoclaves, no separate fuel source isusually needed since live steam from existing boilersin the facility’s physical plant can usually power thesystem (104). The compaction process achieves a 60percent reduction of volume of the waste, and higherlevels of up to 80 can be achieved if corrugatedcardboard and other recyclable materials are sepa-rated from the waste to be compacted and landfilled.
The system is increasingly being adopted on theeast coast, even in States covered by MWTA (wherethe autoclaved/compacted waste must be tracked).In New York State, however, the two restrictionsassociated with compacted, autoclave waste havelimited the application and acceptance of thisalternative. First, the New York State Department ofHealth is requiring that the sharps treated in autoclave/compaction units, such as the San-i-pak units, mustbe in compaction-resistant containers to preventspillage and/or exposure to sharps when the com-pacted waste is placed in the landfill. Second, the‘‘recognizability’ of the compacted waste hasresulted in refusal by many local landfills to acceptthe waste (94). As noted above, however, in otherareas of the country such refusals appear lessdifficult to overcome with explanation and demon-stration of the process to landfill operators.
The capital costs are approximately $115,000 to$130,000 for equipment suitable for a 400 bedhospital, with estimates of $35,000 to $60,000 forsite preparation (including utilities, slab, drainage,etc.) (48, 94). Operating costs, according to the solemanufacturer, San-i-pak, range from $0.03 perpound when the solid waste disposal costs are $300per pull (haul) to $0.10 per pound when pull costsrun as high as $1,600. Fuel costs are stated to be$0.003 per pound of steam used (47). The operatingcost estimate includes this steam and electricity cost,as well as repairs and maintenance, the capitalizedcost of the equipment, labor, and bags (48). Thesystems have an expected lifetime of 15 years(similar to that of most incinerators). The operating
laFour sizes of the autoclave and compaction unit are available which will accommodate 1,3,7, or 16 autoclave bags, m=s~ appm~ately 38x44inches each in a given cycle. Some limitti attemp~ have been made for a commercial off-site use of the technology; such use, however, does not appearas practical as the on-site application for which the unit was designed (104).

Chapter 3-Non-incineration Treatment Technologies and Trends ● 33
Figure 4—Autoclave and Compaction Unit
Sterilizerload door(for medicalwastes)
Compactorload door(for othersolidwastes)
(roll-off)interface
Time and
Compactortemperature
controlchart recorder
panel/
Sterilizer
/controlpanel
Ratchet I
jack “eye” Gauges
connector
SOURCE: San-i-pak Pacific, Inc., Tracy, CA.
cost includes hauling costs for infectious and generalwastes, and specially hauled wastes, i.e., chemother-apeutic, radioactive, and pathological wastes (esti-mated to be less than 1 percent of a facility’s totalwaste).
MECHANICAL/CHEMICALDISINFECTION
Chemical agents such as chlorine have been usedas disinfectants for medical products for some time,although the application to large volumes of infec-tious wastes generated by hospitals and laboratoriesis more recent (104). This type of technology, whichhas been available since the mid- 1980s, is referred toas “mechanical/chemical’ because of mechanicalmaceration and chemical disinfection (a result offorcing a reaction that occurs to volatilize wastematerial and expose all of the pathogens to a
chemical disinfectant in a controlled environment);the residue is discharged to the sewer system.15
Chemical disinfection processes, according toEPA, are most appropriate for liquid wastes, al-though they can be used to treat solid wastes (122).The appropriateness of the process for pathologicalwastes is not clear (92). A number of factors shouldbe considered regarding the effective use of chemi-cal disinfection, including: the types and biology ofmicroorganisms in the wastes; degree of contamina-tion; type of disinfectant used (usually sodiumhypochlorite, commonly known as chlorine bleach)and its concentration and quantity; the contact time;mixing requirements; etc. (122). As with othertreatment alternatives, efficacy of the method needsto be demonstrated through the development of abiological testing program and monitoring on aperiodic basis using appropriate indicators in orderfor the system to be adopted and used on a routine
ls~s me of system is also sometimes referred to as “hydropulptig” (see 30).

34 Ž Finding the Rx for Managing Medical Wastes
basis. Test results reported to date find the process,using chlorine bleach, to be an effective disinfectantfor medical wastes contaminated wi th vege tab lebacteria and viruses, but less effective againstspore-formin g bacteria (92).16 No standard protocolhas been developed to evaluate the efficacy of thesystem and to assist in developing standard operat-ing procedures for it (92).
Maceration of the medical waste, involving high-speed hammermill blades and/or shredders, requiresuse of copious amounts of water. To keep the unitfrom overheating as well as to disinfect the waste,water is introduced along with the disinfectant(usually chlorine-based) during the maceration phase.The simultaneous volatilization and introduction ofthe disinfectant is designed to render the wastesnoninfectious. The introduction of water creates aliquid waste, which is discharged to the sewer.17
This means an industrial waste water dischargepermit from the local sewage district may berequired.
According to Research Triangle Institute’s (RTI)contractor report to EPA, “Once the proper operat-ing parameters such as the flow rates for water andchlorine solutions are established the device issimple to operate and requires little training” (92).The nonrecognizable nature of the byproduct of themechanical/chemical treatment process and its abil-ity to treat liquid medical waste before dischargingit to the sewer system are important factors account-ing for the favorable market response to thistreatment alternative. The waste treated by theprocess is rendered nonrecognizable by the shred-ding and pulverizing phases, which are primarily fortreatment efficiency but act to destroy the waste aswell (104).18 This means that the waste meets thenonrecognizability criteria of MWTA and would nothave to be tracked under its manifest system.
Increased concern over the practice of discharginguntreated liquids (e.g., blood and other body fluids)into the sewer system also makes the mechanical/chemical process with its discharge of treated
liquids an attractive alternative. Yet, it is not clearthat this system would reduce any risks that mightexist as a result of direct discharges in a facility ofblood and body fluids into the sewer system (see ch.5). Further, the sewage system contains countlesshuman pathogens from the vast quantity of humanbody waste. Liquid medical waste comprises only aminor fraction of this overall waste flow. Microbio-logically, there is little difference between bloodwaste and fecal/urine waste (except that fecal wasteswould be expected to have a far greater number ofhuman pathogens) (11 1).
The process is designed for on-site use withpossible applications to a variety of medical andhealth-care settings (see figure 5). The frost companyto manufacture such a system (Medical SafeTec.,Inc.) currently offers three machines, one for largerapplications and the other two for laboratory set-tings. A similar system was designed by a companyfor application in the funeral industry. This companyalso has a clinical machine for sharps and plans tooffer over 200 separate machines for a wide varietyof health-care applications. While the one companyis offering a system that would require a largefacility to purchase one unit, the other company ismarketing smaller machines for use throughout thehospital (104).
States such as California and New Jersey, whichare open to innovative technology for medical wastegenerally, are a responsive market for this alterna-tive. Some large generators converted to this system,rather than replacing or retrofitting existing incin-erators (104). Currently, about 40 of the smallerunits are in use, primarily for sharps management.These systems can treat pathological waste (e.g.,formalin-fixed tissue samples) and most other medi-cal wastes. 19 The system is powered electrically withstandard electrical requirements. Sewer connectionis mandatory, and, as noted, a local discharge permitmay be necessary. Concern has been raised over thelevel of metals, organics, and other contaminantsthat may be in the sewage discharge (5).
IGHward and ocwpation~ risk from tie handling, storage, and use of chlorine have been suggested as a potential disadvantage of ~s tec~olog’y(94).
17Repofiedly, systems that shred and disinfect medical wastes that will not require use of copious amounts of water or a sewer dkchge are beingdeveloped (63). One such process will combine conventional shredding technology with the use of special red bags. These red bags have a small seamthat envelops a few grams of formulated powder (a water-activated disinfectant). Treated material is “only slightly moist, no longerrecognizable. . disinfected and volume-rcxiuced” (78).
18A pres~~~g system which is part of the large hammermill, breaks up the waste materials before the ha.mmermill pulverims hem.
lg~e EPA s~tes, however, that these units are not normally recommended for patiOIOgicd waste ~es (141).

Chapter 3-Non-incineration Treatment Technologies and Trends .35
Figure 5-Mechanical/Chemical Disinfection Unit
Negative pressureMepa filter system blower
1
SOURCE: Medical SafeTec, Inc., Indianapolis, IN.
The percentage of dissolved solids in the dis-charge into the sewer is high (up to 10,000 ppm v.300 ppm for residential users), but the manufacturerstates that changes necessary to reduce the level tothat of other points of discharges are now feasible(104). Even so, the liquid effluent contains highconcentrations of substances, e.g., chlorine, that mayrequire pretreatment before being discharged to themunicipal sewer system. It would appear that localpermit levels for sewage discharges would have tobe met.20
Solidwaste
collectioncart
\
designed to control emissions and force air througha series of prefilters and a chlorine-resistant falterbefore discharging it to the atmosphere (141, 5). Theuse of chlorine and the potential impact on sewagedischarges is also raised as a concern with thechemical disinfection process. Further study of theseissues is needed, possibly as part of EPA’s currentresearch on alternative treatment methods.
There are no air quality regulations that arerelevant. Although it is not clear there is a need forany air regulations, given that no known air emis-sions problems have been encountered, little hasbeen reported about the nature of the emissions.There is some concern over the potential forproducing volatile chemicals and/or microbes dur-ing the shredding process, although the system is
The mechanical nature of the equipment, with somany moving parts, means it could require a highlevel of maintenance. This also means there is morepotential occupational exposure. The manufacturersnote that no injuries involving equipment repair ormaintenance have been reported.21 As with anautoclave unit, the space needed for a mechanical/chemical unit is not large and the capacity is thenmainly a factor of the throughput rate for the unit.The smaller units require an area approximately 10
20R~ (92) ~Wo~ tit ~a~te ~eatment effluent from the Medical S~eT& tit has been tested according to the specitlcations published under theClean Water Act for pollutant analysis (40 CFR, Part 136).
21Ye~ ~S ~th o~er ~eatment ~ternatives, it is not clear how fr~uently a~idents are reported (given mncerns OVer pOteIl~ hpiiCtS 011 kMIKZIIICe
pre miums, etc.).

36 ● Finding the &for Managing Medical Wastes
feet by 9 feet and the units with additional capacitywould require areas of 11 feet by 10 feet.
Capital costs are approximately between $40,000and $50,000 (equipment and installation) for thesmaller units and approximately $350,000 for thelarger sized unit. Operating costs are reported to be$0.06 per pound of waste per hour of treatment(104).
MICROWAVEThe application of microwave technology to
disinfect medical waste was introduced in Europeseveral years ago. The technology is from WestGermany and just recently is being marketed in theUnited States (34). The units can be on-site ormobile facilities. The first on-site installation was inNorth Carolina in March 1990. A second commer-cial system began operation shortly after this inCalifornia as a supplemental technology to anexisting regional incinerator (104, 34).
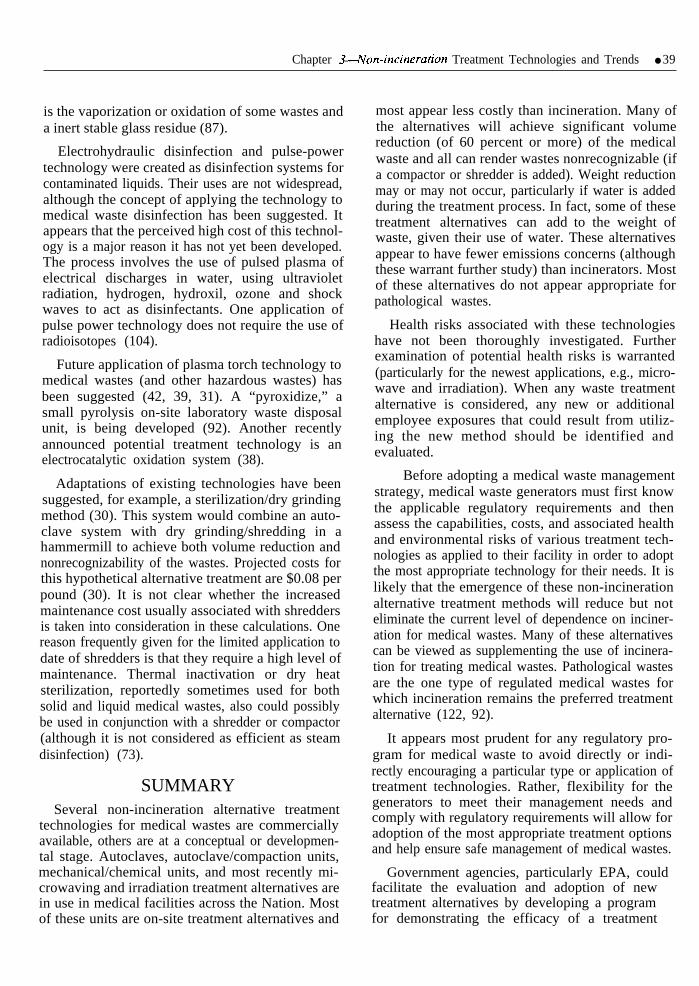
Powered by electricity, the unit shreds the wastein a controlled environment; the waste then entersthe chamber for exposure to the microwaves (seefigure 6). The disinfection process takes placethrough microwave heating, which occurs inside thewaste material (unlike other thermal treatmentmethods which heat wastes externally) and wettingand shredding the waste to facilitate heating andsteam penetration of the waste. The material isdischarged to a storage bin for ultimate disposal.
Computerized controls, as with most other treat-ment technologies, are used to ensure the minimumparameters for disinfection and proper function ofthe equipment. Fire and temperature conditionsnecessary for waste sterilization are the same asthose for autoclaving (92). Studies conducted inGermany by the Institute of Hygiene, University ofGottingen concluded that the process treated ma-terial to a lower level of bacteria content thanordinary household wastes (as reported by ref. 35).Performance tests at a unit operating in the UnitedStates, using a Bacillus subtilis microbiologicalspore test indicator, found the wastes to be treatedunder conditions to render it sterilized (35). Re-search Triangle Institute reports that although themethod is essentially a steam sterilization method, itis necessary to confirm that conditions required forsteam sterilization exist in the microwave process(92).
Photo credit: Vetco Sanitec Corp.,Combustion Engineering, Stamford, CT
Microwave units can be installed on-site or be used asmobile units. Mobile units could facilitate collection of
regulated medical wastes from home health-care settings,doctor offices, and other small generators of medical
wastes. This type of mobile microwave unit has been usedin Berlin, West Germany for several years.
As with autoclaving, approximately 90 percent ofmedical wastes can be treated by this method (it isnot recommended for pathological wastes). The useof electricity averages about $0.02 per pound.Energy use is reportedly lower than that of anincinerator (35). The shredding process results in avolume reduction of 80 percent prior to disposal.Treated wastes are suitable for disposal in a solidwaste landfill. Given that the process is used inEurope with no reported emission problems, itsacceptance is anticipated in the United States (35,104).
The microwave system is designed to be operatedby unskilled labor. All adjustments in wastes levelsand time are preprogrammed into the system (92).Operating and maintenance costs are reported to beapproximately $0.10 or $0.07 per hour, dependingon whether the system is operated 8 hours or 10hours a day, respectively. Capital costs are about$500,000 for a unit (35). It appears that health risksassociated with the unit would primarily be associ-ated with the maintenance of the shredder compo-nent of the system. Potential operator exposure tovolatized chemicals during loading or cleaning/maintenance should be examined, h o w e v e r .
IRRADIATIONA common practice is to treat medical products
with radiation for sterilization purposes (104). Thehigh cost of cobalt used in the process and highoperating costs have discouraged commercial ven-tures from using the technology for medical wastemanagement. In February 1990, however, the first

Chapter 3-Non-incineration Treatment Technologies and Trends ● 37
Figure 6—Mobile Microwave Medical Waste Disinfection Unit\
u
12
o11
II 1‘%31 0)
o- 13
1.2.
3.
4.
5.
6.
7.
8.
9.
Process scheme of a mobile microwave-disinfection unit
Feeding hopper
Feeding crank
Shredder
Connecting hopperwith inspection window
Level sensors
Main conveyor auger
Microwave generators
Temperature holding section
Discharge conveyor auger
SOURCE: Vetco Sanitec Corp., Combustion Engineering, Stamford, CT.
commercial medical waste irradiation facility wasopened in Arkansas, and additional facilities areplanned in California and New Jersey. Questionshave been raised about the actual process of radiat-ing the material and achieving adequate disinfection(104) (see figure 7). Garoma radiation sterilizesinfectious waste by penetrating the waste andinactivating microbial contaminants. T h e i o n i z i n gradiation hydrolyzes the water molecules within the
10.
11.
12.
13.
14.
15.
16.
17.
Temperature sensors
Filter system, 2-stage
Water tank with pumpand spraying connection
Steam generator
Steam connection
Hydraulic aggregate
Room heater
Container
micro organisms and these intermediate hydrolysisproducts interact with the gamma radiation andbiological compounds, are broken down and arerendered noninfectious. The company pursuing thistreatment technology emphasizes that the waste willnot be disposed of as solid waste. Rather, it isshredded, rendering it nonrecognizable, and isshipped to a cement kiln where it is burned as fuel(104).22 Eventually, one such operator of a system
~t should be noted that concerns have also been raised about the practice of burning wastes in cement kilns, which typically are not subject to airemission standards (other than the new source performance standard (NSPS) for particulate matter emissions). The assumption is that these kilns operateat such high temperatures that wastes used as fuels are destroyed without producing harmful emissions. This is an unsettled regulatory issue. It is true,however, that any cement kiln burning MSW would be subject to air emissions standards for MSW incinerators as proposed by EPA in December 1989.

38 ● Finding the Rx for Managing Medical Wastes
Figure 7—irradiation Unit
Cobalt 60 radiation chamber
Infectious waste
SOURCE: Technology Process, Inc.
plans to separate the plastic waste and sell the treatedplastic residues for recycling (92, 101).
The process is highly predictable, according toRTI’s analysis (92). Verification of the conditionsfor disinfection involves using Bacillus pumilis as atest indicator organism. According to RTI, nostudies specifically addressing the efficacy of gammairradiation of medical waste for disinfection (92). Inaddition, film is placed between every few boxes toquantify the amount of radiation each box receives(104).
Again, this treatment method is not recommendedby EPA for pathological wastes. The capacity ofthese units is a factor of the throughput rate. Theunits are an off-site alternative and can manage alltypes of waste, except pathological wastes. Theapproximate operating cost could be $0.15 per
Treated waste
pound. Potential risks of this alternative treatmenttechnology are primarily associated with the possi-bility of radiation exposure to workers.23
OTHER POTENTIALTREATMENT TECHNOLOGIESOther technologies with potential application to
medical waste management are in a conceptual orexperimental stage in their development. Several arementioned here to illustrate the variety of attemptsto develop treatment alternatives for medical wastes.
One technology that has recently been announcedas available and capable of thermally destroyingbiomedical wastes uses an electric molten glassfurnace. At least with other waste types, the wastesare fed into the furnace and are subjected to intenseheat (2,300 ‘F) and air and water vapor. The result
~Worker~ ~pma@ ~ese systems ~~~d ~ve to be @ained according to tie IfJ ~ ‘‘S~nd~ds for Protection Ag&t Radiation” [email protected] would need to be highly trained to ensure the efficient and safe operation of the process.
Chapter 3--IVon-incineration Treatment Technologies and Trends ● 39
is the vaporization or oxidation of some wastes anda inert stable glass residue (87).
Electrohydraulic disinfection and pulse-powertechnology were created as disinfection systems forcontaminated liquids. Their uses are not widespread,although the concept of applying the technology tomedical waste disinfection has been suggested. Itappears that the perceived high cost of this technol-ogy is a major reason it has not yet been developed.The process involves the use of pulsed plasma ofelectrical discharges in water, using ultravioletradiation, hydrogen, hydroxil, ozone and shockwaves to act as disinfectants. One application ofpulse power technology does not require the use ofradioisotopes (104).
Future application of plasma torch technology tomedical wastes (and other hazardous wastes) hasbeen suggested (42, 39, 31). A “pyroxidize,” asmall pyrolysis on-site laboratory waste disposalunit, is being developed (92). Another recentlyannounced potential treatment technology is anelectrocatalytic oxidation system (38).
Adaptations of existing technologies have beensuggested, for example, a sterilization/dry grindingmethod (30). This system would combine an auto-clave system with dry grinding/shredding in ahammermill to achieve both volume reduction andnonrecognizability of the wastes. Projected costs forthis hypothetical alternative treatment are $0.08 perpound (30). It is not clear whether the increasedmaintenance cost usually associated with shreddersis taken into consideration in these calculations. Onereason frequently given for the limited application todate of shredders is that they require a high level ofmaintenance. Thermal inactivation or dry heatsterilization, reportedly sometimes used for bothsolid and liquid medical wastes, also could possiblybe used in conjunction with a shredder or compactor(although it is not considered as efficient as steamdisinfection) (73).
SUMMARYSeveral non-incineration alternative treatment
technologies for medical wastes are commerciallyavailable, others are at a conceptual or developmen-tal stage. Autoclaves, autoclave/compaction units,mechanical/chemical units, and most recently mi-crowaving and irradiation treatment alternatives arein use in medical facilities across the Nation. Mostof these units are on-site treatment alternatives and
most appear less costly than incineration. Many ofthe alternatives will achieve significant volumereduction (of 60 percent or more) of the medicalwaste and all can render wastes nonrecognizable (ifa compactor or shredder is added). Weight reductionmay or may not occur, particularly if water is addedduring the treatment process. In fact, some of thesetreatment alternatives can add to the weight ofwaste, given their use of water. These alternativesappear to have fewer emissions concerns (althoughthese warrant further study) than incinerators. Mostof these alternatives do not appear appropriate forpathological wastes.
Health risks associated with these technologieshave not been thoroughly investigated. Furtherexamination of potential health risks is warranted(particularly for the newest applications, e.g., micro-wave and irradiation). When any waste treatmentalternative is considered, any new or additionalemployee exposures that could result from utiliz-ing the new method should be identified andevaluated.
Before adopting a medical waste managementstrategy, medical waste generators must first knowthe applicable regulatory requirements and thenassess the capabilities, costs, and associated healthand environmental risks of various treatment tech-nologies as applied to their facility in order to adoptthe most appropriate technology for their needs. It islikely that the emergence of these non-incinerationalternative treatment methods will reduce but noteliminate the current level of dependence on inciner-ation for medical wastes. Many of these alternativescan be viewed as supplementing the use of incinera-tion for treating medical wastes. Pathological wastesare the one type of regulated medical wastes forwhich incineration remains the preferred treatmentalternative (122, 92).
It appears most prudent for any regulatory pro-gram for medical waste to avoid directly or indi-rectly encouraging a particular type or application oftreatment technologies. Rather, flexibility for thegenerators to meet their management needs andcomply with regulatory requirements will allow foradoption of the most appropriate treatment optionsand help ensure safe management of medical wastes.
Government agencies, particularly EPA, couldfacilitate the evaluation and adoption of newtreatment alternatives by developing a programfor demonstrating the efficacy of a treatment

40 ● Finding the Rx for Managing Medical Wastes
method. A general protocol for the certification ofapproval of any type of waste treatment technology(e.g., hazardous, solid, medical) could be establishedwith adjustments made for developing appropriatetesting programs (e.g., biological testing of medicaltreatment methods).
Interim approval status might be given while testprotocols and results are developed and/or pilotprojects, perhaps at veterans’ hospitals or othergovernment facilities could be used. Monitoringnew facilities on aperiodic basis, perhaps with somesupporting funding, could facilitate developing ap-
propriate operating parameters and specifications. Aprogram similar to the Superfund Innovative Tech-nology Evaluation Program has been suggested as amodel for a program evaluating new medical wastetechnologies (31, 124).
Such efforts could help ensure that governmentregulatory activity does not create barriers forevaluation and adoption of new technologies. Animportant task for State and Federal regulators thenis to rid the current regulatory system of inconsisten-cies and ambiguities and enable the “market” tomove ahead with optimum management solutions.