Embed Size (px)
Citation preview

Chapter 4Chapter 4
Care of the Patient with a
Musculoskeletal Disorder
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 2Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• Functions of the skeletal system Support Protection Movement Mineral storage Hemopoiesis
• Structure of bones Four classifications based on form and shape
• Long, short, flat, and irregular

Slide 3Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
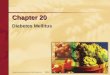
Figure 4-2Figure 4-2
Skeleton, anterior view.
(From Thibodeau, G.A., Patton, K.T. [2005]. The human body in health and disease. [4th ed.]. St. Louis: Mosby.)

Slide 4Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• Articulations (joints) Allow movement and flexibility Hold bones together Three types according to degree of movement
• Synarthrosis—no movement (skull)
• Amphiarthrosis—slight movement (pelvis)
• Diarthrosis—free movement (shoulder)
• Divisions of the skeleton Axial skeleton Appendicular skeleton

Slide 5Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 4-1Figure 4-1
Structure of a freely movable (diarthrotic) joint.
(From Thibodeau, G.A., Patton, K.T. [2008]. Structure and function of the body. [13th ed.]. St. Louis: Mosby.)

Slide 6Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• Under voluntary or involuntary control
• Functions of the muscular system Motion Maintenance of posture Production of heat (85% of body heat)
• Skeletal muscle structure Epimysium (connective tissue covering skeletal muscle)
Perimysium Endomysium
• Both join with epimysium to create tendon• Tendons anchor muscle to bone• Tendon sheaths contain synovial fluid for easy movement

Slide 7Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
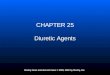
Figure 4-5Figure 4-5
Anterior view of the body.
(From Thibodeau, G.A., Patton, K.T. [2005]. The human body in health and disease. [4th ed.]. St. Louis: Mosby.)

Slide 8Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• Nerve and blood supply Blood vessels provide a constant supply of oxygen
and nutrition, and nerve cells/fibers supply a constant source of information
• Muscle contraction Muscle stimulus—when a muscle cell is adequately
stimulated, it will contract Muscle tone—skeletal muscles are in a constant state
of readiness for action Types of body movements—flexion, extension,
abduction, adduction, rotation, supination, pronation, dorsiflexion, and plantar flexion

Slide 9Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Laboratory and Diagnostic ExaminationsLaboratory and Diagnostic Examinations
• Radiographic studies X-ray Myelogram Nuclear scanning Magnetic resonance imaging (MRI) Computed axial tomography (CT or CAT scan) Bone scan Aspiration/Synovial fluid aspiration
• Endoscopic examination Arthroscopy Endoscopic spinal microsurgery

Slide 10Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Laboratory and Diagnostic ExaminationsLaboratory and Diagnostic Examinations
• Electrographic procedure Electromyogram (EMG)
• Laboratory tests Calcium Erythrocyte sedimentation rate (ESR) Lupus erythematosus (LE) preparation Rheumatoid factor (RF) Uric acid (blood)
http://www.youtube.com/watch?v=k0uSpYd_Ics

Slide 11Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Arthritis Several types; most common RA, rheumatoid
spondylitis, OA, DJD, gout
• Rheumatoid arthritis Etiology/pathophysiology
• Most serious form of arthritis; Chronic, systemic disease
• Most common in women of childbearing age
• Autoimmune disorder, but may also be genetic; smoking greatly increases risk
• May affect lungs, heart, blood vessels, muscles, eyes, and skin
• Chronic inflammation of the synovial membrane of the diarthrodial joints (movable)

Slide 12Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Rheumatoid arthritis (continued) Clinical manifestations/assessment
• Characterized by periods of remission and exacerbation
• Malaise
• Muscle weakness
• Loss of appetite
• Generalized aching
• Edema and tenderness of joints
• Limited range of motion (morning stiffness)
• Can lead to gross deformity and loss of function
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System

Slide 13Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 4-7Figure 4-7
Rheumatoid arthritis of hands.
(From Kamal, A., Brocklehurst, J.C. [1991]. Color atlas of geriatric medicine. [2nd ed.]. St. Louis: Mosby.)

Slide 14Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Rheumatoid arthritis (continued) Diagnostic tests
• Radiography studies show loss of articular cartilage and change in bone structure
• Laboratory tests Erythrocyte sedimentation rate (ESR) (0-15mm/hr) Rheumatoid factor (RF) (0-30 IU/ mL) Latex agglutination test (neg) Synovial fluid aspiration (clear, viscous)

Slide 15Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Rheumatoid arthritis (continued) Medical management/nursing interventions
• Pharmacological management Salicylates, NSAIDs, anti-inflammatory agents, disease-
modifying antirheumatoid drugs
• Rest: 8 to 10 hours of sleep a night
• Exercise: Range of motion two to three times per day
• Heat: Hot packs, heat lamp, and/or hot paraffin
• Rehabilitation
• Joint replacement if needed

SalicylatesAction Analgesic, antipyretic, and antiinflammatory effects Stop the production of prostaglandins; antiplatelet
aggregateUses Treatment of mild to moderate pain; reduces the risk of
myocardial infarctions and stroke, as well as transient ischemic attacks (TIAs) in men
First-line therapy for various forms of arthritis, fever, myalgia, neuralgia, arthralgia, headache, and dysmenorrhea
Systemic lupus erythematosus, acute rheumatic fever
16Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.
Adverse Reactions • Tinnitus, visual disturbances, edema, urticaria, anorexia, epigastric discomfort, and nausea

Salicylates (cont.)
Nursing Implications Assessment, diagnosis, planning,
implementation, and evaluationPatient Teaching Administration time, adverse effects; time for
drug effectiveness; implications for drug interactions and when to contact the healthcare provider; storage and safety; other routes of administration if PO is not tolerated
17Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.
Drug InteractionsAlcohol use increases the chance for GI bleeding; NSAIDs; sulfonamides, sulfonylureas; phenytoin

Acetaminophen
Over-the-counter drug; antipyretic analgesic; no antiinflammatory effect
Action: antipyretic – direct action of the hypothalamic heat-regulating center; blocks pyogenic cytokines through vasodilation and sweating
Use: chronic, nonmalignant pain; osteoarthritis Adverse reactions: rare blood response; liver
toxicity; overdosage can be fatal Drug interactions and hepatotoxicity
18Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Nonsteroidal Antiinflammatory Drugs
Action: unknown; may block prostaglandins; analgesic, antiinflammatory, and antipyretic effects Ex: ibuprofen, indocin, tolectin, naproxen
Uses: rheumatic disease, degenerative joint disease, osteoarthritis, and acute musculoskeletal problems
Adverse reactions: GI most common Drug interactions Nursing implications and patient teaching
19Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Slow-Acting Antirheumatic Drugs - Gold Compounds
Chrysotherapy Action: unknown; interference with biochemical
reactions at the cellular level; inhibit lysosomal enzyme activity; effect on antigen response in rheumatoid arthritis; stops synovitis
Adverse reactions and toxicities –stomatitis; renal and hepatic damage
Dosage and administration -3 months for effect Forms of medication -IM and oral
20Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Slow-Acting Antirheumatic Drugs -Hydroxychloroquine Sulfate
Action: unknown; antimalarial drug; acts to stop antigen formation in the body
Uses Adverse reactions – retinal edema Drug effectiveness – needs 6-12 months
before effects are seen Drug interactions
21Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Slow-Acting Antirheumatic Drugs -
Methotrexate Action: unknown, may affect immune function
to reduce inflammation; alters the way the cells use folic acid
Uses: treatment of cancer and rheumatoid arthritis
Toxicities – do not get pregnant or have immunizations while on this drug
22Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Disease Modifying Antirheumatoid Drugs (DMARDs): - Penicillamine Action: chelating agent Use: rheumatoid arthritis Nursing implications: take 1 hour before or 2
hours after food or drugs Patient and family teaching: treatment
length/drug effectiveness; toxic effects; when to contact healthcare provider; monitoring; brief pain increase following injection; adverse reactions
23Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Disease Modifying Antirheumatoid Drugs (DMARDs): Infliximab
Action/Use: in combination with methotrexate to reduce signs and symptoms of rheumatoid arthritis, Crohn disease, other orthopedic inflammatory or destructive processes
Antibody that binds to proinflammatory enzymes
Adverse reactions: FDA warning; symptoms
24Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Disease Modifying Antirheumatoid Drugs (DMARDs): etanercept
Binds to Tumor Necrosis factor to block normal and immune inflammatory responses
Prevents body’s ability to fight infections Given subq twice weekly Make cause or aggravate systemic lupus
erythematosus
25Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Disease Modifying Antirheumatoid Drugs (DMARDs): Humira
Reduces infiltration of inflammatory cells Adverse: neutropenia Nursing: monitor for infections; hold drug if
infection present
26Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Disease Modifying Antirheumatoid Drugs (DMARDs): azulfidine
Blocks prostaglandin synthesis Adverse: many GI side effects; hepatotoxic Nursing: space doses evenly around the
clock; monitor for bruising, bleeding, itching and jaundice; may discolor urine and skin an orange-yellow color; monitor CBC
27Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Immunosuppresant: Imuran & Cytoxan
Inhibits DNA/RNA protein synthesis May take 12 weeks to see effect Causes GI irritation Monitor for liver impact: bleeding and bruising Avoid pregnancy while taking these drugs
28Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Corticosteroids
Leader of antiinflammatory medications Give with food or milk to prevent GI irritation Causes sodium retention = water retention; I
COME TAPE; fat deposits, hirsutism and diabetes mellitus
Taper off dose per MD instructions
29Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

COX 2 INHIBITOR - CELEBREX
Analgesic and antiinflammatory Risk of GI bleeding; increased risk of MI or
CVA Give with or without food Do not give to patients with sulfa allergy or
asthma Give carefully with Lasix, ACE inhibitors,
warfarin, and lithium
30Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Slide 31Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Ankylosing spondylitis Etiology/pathophysiology
• Chronic, progressive disorder of the sacroiliac and hip joints, the synovial joints of the spine, and the adjacent soft tissues
• Most common in young men
• Strong hereditary tendency Clinical manifestations/assessment
• Pain and stiffness in back; decreased ROM
• Elevated temperature; tachycardia; hyperpnea

Slide 32Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Ankylosing spondylitis (continued) Diagnostic tests
• Hemoglobin, hematocrit, ESR, alkaline phosphatase
• Radiographic Medical management/nursing interventions
• Pharmacological management Analgesics, NSAIDs
• Exercise program: swimming and walking
• Surgery: replace fused joints
• Maintain spine alignment
• Turn, position, and breathing exercises every 2 hours

Slide 33Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Osteoarthritis (degenerative joint disease) Etiology/pathophysiology
• Nonsystemic, noninflammatory disorder that progressively causes bones and joints to degenerate
• Primary Cause is unknown
• Secondary Caused by trauma, infections, previous fractures,
rheumatoid arthritis, stress on weight-bearing joints

Slide 34Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Osteoarthritis (degenerative joint disease) (continued) Clinical manifestations/assessment
• Joint edema, tenderness, instability, and deformity
• Heberden’s nodes – sides of distal joints of fingers
• Bouchard’s nodes – proximal joints of fingers Diagnostic tests
• Radiographic studies
• Arthroscopy
• Synovial fluid examination
• Bone scans

Slide 35Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 4-9Figure 4-9
Heberden’s nodes.
(From Kamal, A., Brocklehurst, J.C. [1991]. Color atlas of geriatric medicine. [2nd ed.]. St. Louis: Mosby.)

Slide 36Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Osteoarthritis (degenerative joint disease) (continued) Medical management/nursing interventions
• Pharmacological management Salicylates, NSAIDs, corticosteroids, glucosamine
supplements
• Exercise balanced with rest
• Heat applications
• Gait enhancers (canes, walkers, etc.)
• Surgery Osteotomy Joint replacement

Slide 37Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Gout (gouty arthritis) Etiology/pathophysiology
• Metabolic disease resulting from an accumulation of uric acid in the blood
• Caused by an ineffective metabolism of purines
• Primary: hereditary factors
• Secondary: use of certain drugs, complication of other diseases, or idiopathic
• Affects men more frequently than women
• Does not occur before puberty in males or before menopause in females

Slide 38Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Gout (gouty arthritis) (continued) Clinical manifestations/assessment
• Excruciating pain, often occurring at night
• Edema
• Inflammation (most common in the great toe)
• Tophi (calculi containing Na urate deposits occurring in periarticular fibrous tissue)
Diagnostic tests• Serum and uric acid level, CBC, ESR
• Radiography studies
• Synovial fluid aspiration

Slide 39Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Inflammatory Disorders of the Musculoskeletal SystemInflammatory Disorders of the Musculoskeletal System
• Gout (gouty arthritis) (continued) Medical management/nursing interventions
• Pharmacological management Colchicine, phenylbutazone (Butazolidin), indomethacin
(Indocin), corticosteroids, allopurinol (Zyloprim), sulfinpyrazone (Anturane)
• Encourage fluid intake
• Monitor intake and output
• Bed rest and joint immobilization
• Dietary restrictions

Antigout Medications Uric acid levels increase; crystal formation Gouty arthritis Relief of pain/ inflammation – acute period Uricosuric agents Probenecid – inhibits renal tubular reabsorption
of uric acid allowing increased excretion – also slows PCN secretion
Allopurinol – decrease production of uric acid Anturane – prevents tophi build up *** ASA inactivates these drugs*****
40Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Uricosuric Agents (cont.)
Adverse reactions: drug-specific symptoms Drug interactions
Salicylates Increased drug effects Acidifying and alkalinizing agents Anticoagulants Hypersensitivity reactions
41Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Uricosuric Agents (cont.)
Nursing implications: assessment, diagnosis, planning, implementation, evaluation
Patient and family teaching: preventing attacks; drug administration; diet and fluid intake; self-monitoring of urine and stools; when to contact the health care provider; colchicine administration; drug interactions
42Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Slide 43Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Other Disorders of the Musculoskeletal SystemOther Disorders of the Musculoskeletal System
• Osteoporosis Etiology/pathophysiology
• Reduction of bone mass
• Most common in women ages 55 to 65
• Contributing factors: immobilization; steroids; high intake of caffeine; diet low in calcium, high in protein; smoking; sedentary lifestyle
Clinical manifestations/assessment• Backache
• Porous and brittle bones
• Dowager’s hump

Slide 44Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Other Disorders of the Musculoskeletal SystemOther Disorders of the Musculoskeletal System
• Osteoporosis (continued) Diagnostic tests
• CBC, serum calcium, phosphorus, alkaline phosphatase, blood urea nitrogen, creatinine level, urinalysis, liver and thyroid function tests
• Radiography studies Medical management/nursing interventions
• Pharmacological management Calcium supplements, vitamin D Estrogen, alendronate (Fosamax)
• Weight-bearing exercises
• Dietary recommendations

Slide 45Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Medications for OsteoporosisMedications for Osteoporosis
• Biphosponates – absorb calcium phosphate crystal into bone; take in am 30 minutes before other meds, sit up for 30 minutes to prevent stomach irritation
• EX Fosamax, Actonel, Aredia, Skelid, Boniva
• Calcitonin – salmon –increases bone mass
• EX: Miacalcin, Fortical
• Estrogen receptor modulator – prevents bone loss and spinal fractures EX Evista
• Parathyroid hormone – prevents sloughing of osteoblasts in spongy bones; increases bone mass
EX: Forteo

Slide 46Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Other Disorders of the Musculoskeletal SystemOther Disorders of the Musculoskeletal System
• Osteomyelitis Etiology/pathophysiology
• Local or generalized infection of the bone and bone marrow
• Staphylococci are the most common cause
• Introduced through trauma (injury or surgery) or via the bloodstream from another site in the body to the bone
• Bacteria invade the bone and degeneration of bone occurs

Slide 47Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Other Disorders of the Musculoskeletal SystemOther Disorders of the Musculoskeletal System
• Osteomyelitis (continued) Clinical manifestations/assessment
• Persistent, severe, and increasing bone pain
• Wound draining purulent fluid
• Signs and symptoms of infection: temperature, tachycardia, and tachypnea
• Edema of affected area Diagnostic tests
• Radiography studies; bone scan
• CBC; ESR; cultures of blood and drainage

Slide 48Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Other Disorders of the Musculoskeletal SystemOther Disorders of the Musculoskeletal System
• Osteomyelitis (continued) Medical management/nursing interventions
• Pharmacological management Antibiotic therapy based upon culture results
• Surgery: removal of necrotic bone
• Absolute rest of affected extremity
• Wound care Irrigate with hydrogen peroxide or antibiotic solution;
cover with sterile dressing
• Drainage and secretion precautions
• Dietary recommendations: high in calories, protein, and vitamins

Slide 49Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Other Disorders of the Musculoskeletal SystemOther Disorders of the Musculoskeletal System
• Fibromyalgia syndrome (FMS) Etiology/pathophysiology
• Musculoskeletal chronic pain syndrome
• Unknown etiology Clinical manifestations/assessment
• Generalized aching/stiffness
• Irritable bowel syndrome
• Tension headache
• Paresthesia of upper extremities
• Sensation of edematous hands

Slide 50Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Other Disorders of the Musculoskeletal SystemOther Disorders of the Musculoskeletal System
• Fibromyalgia syndrome (FMS) (continued) Diagnostic tests
• No specific laboratory or radiographic tests diagnose FMS
Medical management/nursing interventions• Pharmacological management
Tricyclic antidepressants
• Patient education and reassurance
• Exercise
• Relaxation techniques

Slide 51Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Surgical Interventions for Total Knee or Total Hip ReplacementSurgical Interventions for Total Knee or Total Hip Replacement
• Knee arthroplasty (total knee replacement) Replacement of the knee joint Restore motion of the joint, relieve pain, or correct
deformity
• Hip arthroplasty (total hip replacement) Replacement of the hip joint

Slide 52Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 4-11Figure 4-11
A, Tibial and femoral components of total knee prosthesis. B, Total knee
prosthesis in place.
(from Monahan, F.D., et al. [2007]. Phipps’ medical-surgical nursing: health and illness perspectives. [8th ed.]. St. Louis: Mosby.)

Slide 53Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 4-14Figure 4-14
Hip arthroplasty (total hip replacement).

Slide 54Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Surgical Interventions for Total Knee or Total Hip ReplacementSurgical Interventions for Total Knee or Total Hip Replacement
• Arthroplasty Nursing interventions
• Intake and output Drainage from operative drains Oral and intravenous intake Urinary output
• Promote respiratory function Give oxygen 2 to 3 L/min Incentive spirometer; cough and deep-breathe
• Bed rest for 24 to 48 hours
• Change dressing as ordered
• Diet as ordered
• Neurovascular checks and vital signs every 4 hours

Slide 55Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Surgical Interventions for Total Knee or Total Hip ReplacementSurgical Interventions for Total Knee or Total Hip Replacement
• Arthroplasty (continued) Nursing interventions (continued)
• Physical therapy will initiate ambulation and prescribe routine
• Antiembolisim stockings or pneumatic boots/ stockings
• Educate on prophylactic antibiotics before invasive procedures
• Avoid dislocation of prosthesis Avoid adduction and hyperflexion of hip Use toilet riser to prevent hyperflexion of hip

Slide 56Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Fracture of the hip Etiology/pathophysiology
• Most common type of fracture
• Women at higher risk due to osteoporosis when postmenopausal
• Types: intracapsular and extracapsular Clinical manifestations/assessment
• Severe pain at site
• Inability to move the leg voluntarily
• Shortening or external rotation of the leg

Slide 57Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 4-16Figure 4-16
Fractures of the hip.
(from Monahan, F.D., et al. [2007]. Phipps’ medical-surgical nursing: health and illness perspectives. [8th ed.]. St. Louis: Mosby.

Slide 58Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Fracture of the hip (continued) Diagnostic tests
• Radiographic examination
• Hemoglobin Medical management/nursing interventions
• Buck’s or Russell’s traction until surgery
• Surgical repair Internal fixation Neufeld nail and screws, Kuntscher nail Prosthetic implants
o Austin Moore prosthesis, bipolar hip replacement

Slide 59Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Fracture of the hip (continued) Medical management/nursing interventions
(continued)• Postoperative interventions
Wound and drain assessment Vital signs Incentive spirometer and turning every 2 hours Antiembolic stockings; anticoagulation therapy Maintain leg abduction Limit weight-bearing on affected side Chairs and commode seats should be raised to prevent
flexion of hip beyond 60 degrees

Slide 60Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Fracture of the hip (continued) Medical management/nursing interventions
(continued)• Patient teaching for open reduction internal fixation
(ORIF) Assess ability to understand Assist to dangle at bedside No weight on operative side Turn every 2 hours, maintain abduction Physical therapy will instruct as to ambulation and
weight-bearing As patient progresses, encourage continuing ambulation
only with assistance

Slide 61Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Fracture of the hip (continued) Medical management/nursing interventions
(continued)• Patient teaching for hip prosthetic implant
Avoid hip flexion beyond 60 degrees for approximately 10 days; beyond 90 degrees for 2 to 3 months
Avoid adduction of the affected leg beyond midline for 2 to 3 months (maintain abduction)
Maintain partial weight-bearing for approximately 2 to 3 months
Avoid positioning on the operative side

Slide 62Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Other fractures Etiology/pathophysiology
• A traumatic injury to a bone in which the continuity of the tissue of the bone is broken
• Pathological or spontaneous fractures
• Types of fractures: open, closed, greenstick, displaced, complete, comminuted, impacted, transverse, oblique, spiral, Colle’s, and Pott’s

Slide 63Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Other fractures (continued) Clinical manifestations/assessment
• Pain
• Loss of normal function
• Obvious deformity
• Change in the curvature or length of bone
• Crepitus (grating sound with movement)
• Soft tissue edema
• Warmth over injured area
• Ecchymosis of skin surrounding injured area
• Loss of sensation distal to injury

Slide 64Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Other fractures (continued) Diagnostic tests
• Radiographic examination Medical management/nursing interventions
• Splinting to prevent edema
• Body alignment
• Elevation of body part
• Application of cold packs, first 24 hours
• Administration of analgesics
• Assess for change in color, sensation, or temperature
• Observe for signs of shock

Slide 65Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Other fractures (continued) Medical management/nursing interventions
(continued)• Closed (simple)
Closed reduction; immobilization; traction Open reduction with internal fixation device
• Open (compound) Surgical debridement and culture of wound Administration of tetanus toxoid Observation for signs of infection Closure of wound Reduction and immobilization of fracture

Slide 66Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Fracture of the vertebrae Etiology/pathophysiology
• Diving accidents
• Blows to the head or body
• Osteoporosis
• Metastatic cancer
• Motorcycle and car accidents
• Displaced fracture may place pressure on or sever the spinal cord nerves

Slide 67Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Fracture of the vertebrae (continued) Clinical manifestations/assessment
• Pain at site of injury
• Partial or complete loss of mobility or sensation
• Evidence of fracture/fracture dislocation on x-ray Medical management/nursing interventions
• Stable injuries Pain medication, muscle relaxants Back support, brace, or cast
• Unstable fractures Traction (Halo), open reduction

Slide 68Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
FracturesFractures
• Fracture of the pelvis Etiology/pathophysiology
• Falls, automobile accidents, crushing accidents Clinical manifestations/assessment
• Unable to bear weight without discomfort
• Pelvic tenderness and edema
• Signs of shock Medical management/nursing interventions
• Bed rest—More severe fractures may require surgery and/or spica or body cast

Slide 69Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Complications of FracturesComplications of Fractures
• Compartment syndrome Cause
• Progressive development of arterial vessel compression and reduced blood supply to an extremity
Clinical manifestations/assessment• Sharp pain with movement, numbness or tingling in the
affected extremity, cool and pale or cyanotic, slow capillary refill
Medical management/nursing interventions• Fasciotomy (incision into the fascia)
• Can lose the limb if pressure is not relieved

Slide 70Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 4-26Figure 4-26
Compartment syndrome.
(From Beare, P.G., Myers, J.L. [1998]. Adult health nursing. [3rd ed.]. St. Louis: Mosby.)

Slide 71Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Complications of FracturesComplications of Fractures
• Shock Cause
• Blood loss, pain, fear Clinical manifestations/assessment
• Altered level of consciousness, restlessness• Hypotension, tachycardia, and tachypnea• Pale, cool, moist skin
Medical management/nursing interventions• Restore blood volume; shock trousers• IV (blood and/or isotonic solutions)• Oxygen

Slide 72Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Complications of FracturesComplications of Fractures
• Fat embolism Cause
• Embolization of fat tissue with platelets Clinical manifestations/assessment
• Irritability, restlessness, disorientation, stupor, coma, chest pain, and dyspnea
Medical management/nursing interventions• IV fluids
• Steroids, digoxin
• Oxygen
• Will TPA work?

Slide 73Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Complications of FracturesComplications of Fractures
• Gas gangrene Cause
• Severe infection of skeletal muscle by Clostridium Clinical manifestations/assessment
• Pain at site of injury
• Signs of infection; gas bubbles under the skin
• Necrotic skin at site is moist; foul odor from wound Medical management/nursing interventions
• Excision of gangrenous tissue
• Antibiotics; strict aseptic technique

Slide 74Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Complications of FracturesComplications of Fractures
• Thromboembolus Cause
• Blood vessel is occluded by an embolus Clinical manifestations/assessment
• Area tingles and is cold, numb, and cyanotic
• Pulmonary embolus causes a sharp thoracic pain Medical management/nursing interventions
• Anticoagulants

Slide 75Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Complications of FracturesComplications of Fractures
• Delayed fracture healing Healing is delayed but will eventually occur
• Nonunion The ends of the fracture fail to stabilize and heal after
6 to 9 months

Slide 76Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Skeletal Fixation DevicesSkeletal Fixation Devices
• External fixation devices Skeletal pin external fixation
• Immobilizes fractures by the use of pins inserted through the bone and attached to a rigid external metal frame
• Casts/cast brace Made of layers of plaster of Paris, fiberglass, or plastic
roller bandages Stockinette applied, then a sheet of wadding, and
casting material

Slide 77Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Fixator Spica CastFixator Spica Cast

Slide 78Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Nonsurgical Interventions for Musculoskeletal DisordersNonsurgical Interventions for Musculoskeletal Disorders
• Traction The process of putting an extremity, bone, or group of
muscles under tension by means of weights and pulleys to:
• Align and stabilize a fracture site
• Relieve pressure on nerves
• Maintain correct positioning
• Prevent deformities
• Relieve muscle spasms Skeletal or skin as counter weight

Slide 79Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Traumatic InjuriesTraumatic Injuries
• Contusion: A blow or blunt force that causes local bleeding under the skin
• Sprains: Wrenching or hyperextension of a joint
• Whiplash: Injury at cervical spine caused by hyperextension
• Strains: Microscopic muscle tears as a result of overstretching muscles and tendons

Slide 80Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Traumatic InjuriesTraumatic Injuries
• Contusions, sprains, whiplash, strains Medical management/nursing interventions
• Elevate injured area
• Cold compresses for 15 to 20 minutes intermittently for 12 to 36 hours
• Warm compresses for 15 to 30 minutes four times a day after 24 hours
• Compressive dressings and/or splint
• Surgery

Slide 81Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Traumatic InjuriesTraumatic Injuries
• Dislocations Etiology/pathophysiology
• Temporary displacement of bones from their normal position
Clinical manifestations/assessment• Erythema; discoloration
• Edema
• Pain
• Limitation of movement
• Deformity or shortening of the extremity

Slide 82Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Traumatic InjuriesTraumatic Injuries
• Dislocations (continued) Medical management/nursing interventions
• Closed reduction
• Open reduction
• Cold compresses first 24 hours and warm compresses after 24 hours
• Elevate injured extremity
• Elastic bandage
• Immobilize
• Analgesics

Slide 83Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Traumatic InjuriesTraumatic Injuries
• Carpal tunnel syndrome Etiology/pathophysiology
• Compression of the median nerve between the carpal ligament and other structures
• Predisposing factors Obese, middle-aged women Employment in occupations involving repetitious motions
of the fingers and hands

Slide 84Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 4-38Figure 4-38
A, Wrist structures involved in carpal tunnel syndrome. B,
Decompression of median nerve.
(From Thompson, J.M., et al. [2002]. Mosby’s clinical nursing. [5th ed.]. St. Louis: Mosby.)

Slide 85Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Traumatic InjuriesTraumatic Injuries
• Carpal tunnel syndrome (continued) Clinical manifestations/assessment
• Paresthesia (any subjective sensation; pricks of pins)
• Hypoesthesia (decrease in sensation in response to stimulation of sensory nerves)
• Burning pain or tingling in the hands
• Inability to grasp or hold small objects
• Edema of the hand, wrist, or fingers
• Muscle atrophy
• Depressed appearance at the base of the thumb on the palmar side

Slide 86Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Traumatic InjuriesTraumatic Injuries
• Carpal tunnel syndrome (continued) Diagnostic tests
• Physical exam—Tinel’s sign
• Electromyogram
• MRI Medical management/nursing interventions
• Immobilizer for wrist
• Elevate extremity
• ROM exercises
• Hydrocortisone injections
• Surgery

Slide 87Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Traumatic InjuriesTraumatic Injuries
• Herniation of intervertebral disk Etiology/pathophysiology
• Rupture of the fibrocartilage surrounding an intervertebral disk, releasing the nucleus pulposus that cushions the vertebrae above and below
• Lumbar and cervical herniations are most common
• May occur from lifting, twisting, trauma, or degenerative changes

Slide 88Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 4-39Figure 4-39
Sagittal section of vertebrae showing both normal and herniated disks.
(From Thibodeau, G.A., Patton, K.T. [2005]. The human body in health and disease. [4th ed.]. St. Louis: Mosby.)

Slide 89Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Traumatic InjuriesTraumatic Injuries
• Herniation of intervertebral disk (continued) Clinical manifestations/assessment
• Lumbar Low back pain that radiates over the buttock and
numbness and tingling in affected leg
• Cervical Neck pain, headache, and neck rigidity
Diagnostic tests
• CAT scan, myelography, and electromyelography

Slide 90Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Traumatic InjuriesTraumatic Injuries
• Herniation of intervertebral disk (continued) Medical management/nursing interventions
• Pharmacological management Analgesics Muscle relaxants
• Bed rest
• Physical therapy
• Traction
• Surgery Laminectomy, spinal fusion, diskectomy,
chemonucleolysis

Slide 91Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
LaminectomyLaminectomy

Slide 92Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
TumorsTumors
• Tumors of the bone Etiology/pathophysiology
• May be primary or secondary
• Benign or malignant
• Osteogenic sarcoma
• Osteochondroma Clinical manifestations/assessment
• Spontaneous fractures
• Anemia
• Pain especially with weight-bearing
• Edema and discoloration of skin at site

Slide 93Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
TumorsTumors
• Tumors of the bone (continued) Diagnostic tests
• Radiography studies
• Bone scan; bone biopsy
• CBC; platelet count; serum protein levels
• Serum alkaline phosphatase level Medical management/nursing interventions
• Surgery
• Chemotherapy and radiation

Slide 94Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
AmputationAmputation
• Amputation of a portion of or an entire extremity Malignant tumors, injuries, impaired circulation,
congenital deformities, infections
• Postoperative nursing interventions Raise foot of bed to elevate extremity Encourage movement Place in prone position at least two times a day Teach strengthening exercises Elastic wraps to shape residual extremity Assess for respiratory complications Phantom-limb pain is normal

Slide 95Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Nursing ProcessNursing Process
• Assessment Scoliosis
• Lateral curvature of the spine Kyphosis
• A rounding of the thoracic spine
• Hump-backed appearance Lordosis
• An increase in the curve at the lumbar region Blanching test
• Capillary nail refill

Skeletal Muscle Relaxants
Action: reduce muscle tone and involuntary movement without loss of voluntary motor function Centrally acting or direct myotropic blocking
Uses: relief of pain in musculoskeletal and neurologic disorders involving peripheral injury and inflammation; relief of spasticity in chronic conditions
96Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Skeletal Muscle Relaxants (cont.)
Adverse reactions: symptoms Drug interactions: sedatives, narcotic
analgesics, antianxiety agents, hypnotics, alcohol, general anesthetics, MAOIs, and tricyclics Cyclobenzaprine and orphenadrine:
anticholinergic effects that interfere with antihypertensive activity of alpha-adrenergic blockers
97Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.