Embed Size (px)
Citation preview

130
C H A P T E R 6
O U T L I N E
Although the treatment and healing of wounds are some of the oldest subjects discussed in the medical literature, and although there have been numerous advances in understanding the steps involved in wound healing, the exact mechanisms underlying wound healing remain unclear.
TISSUE INJURY AND RESPONSEInjured tissues attempt to restore their normal function and struc-tural integrity after injury. Attempts to restore mechanical integ-rity and to restore barriers to fluid loss and infection and to reestablish normal blood and lymphatic flow patterns are termed wound repair. During wound repair, flawless repair is sacrificed because of the urgency to return to function. In contrast, regeneration, which is the goal of wound healing, is the perfect restoration of the preexisting tissue architecture without scar for-mation; regeneration is achievable only during embryonic devel-opment; in lower organisms; or in certain tissues, such as bone and liver.
All wounds undergo the same basic steps of repair. Acute wounds proceed in an orderly and timely reparative process to achieve sustained restoration of structure and function. A chronic wound stalls during a sustained inflammatory phase and fails to heal.
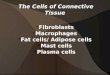
WOUND-HEALING PHASESThe three phases of wound healing are inflammation, prolifera-tion, and maturation. In a large wound such as a pressure sore, the eschar or fibrinous exudate reflects the inflammatory phase, the granulation tissue is part of the proliferative phase, and the contracting or advancing edge is part of the maturational phase. All three phases may occur simultaneously, and the phases may overlap with their individual processes (Fig. 6-1).
Inflammatory PhaseDuring the immediate reaction of the tissue to injury, hemostasis occurs quickly and is rapidly followed by inflammation. This phase represents an attempt to limit damage by stopping bleeding; sealing the wound surface; and removing necrotic tissue, foreign debris, and bacteria. The inflammatory phase is characterized by increased vascular permeability, migration of cells into the wound by chemotaxis, secretion of cytokines and growth factors into the wound, and activation of the migrating cells.
Hemostasis and InflammationBlood vessel injury results in intense local arteriolar and capillary vasoconstriction followed by vasodilation and increased vascular permeability (Fig. 6-2). Erythrocytes and platelets adhere to the damaged capillary endothelium, resulting in plugging of capillar-ies and leading to cessation of hemorrhage. Platelet adhesion to the endothelium is primarily mediated through the interaction between high-affinity glycoprotein receptors and the integrin receptor GPIIb-IIIa (αIIbβ3). Platelets also express other integrin receptors that mediate direct binding to collagen (α2β1) and laminin (α6β1) or indirect binding to subendothelial matrix-bound fibronec-tin (α5β1), vitronectin (αvβ3), and other ligands. Platelet activation occurs by binding to exposed type IV and type V collagen from the damaged endothelium, resulting in platelet aggregation. The initial contact between platelets and collagen requires von Wil-lebrand factor VIII, a heterodimeric protein synthesized by mega-karyocytes and endothelial cells.
Increased Vascular PermeabilityPlatelet binding results in conformational changes in platelets that trigger intracellular signal transduction pathways that lead to platelet activation and the release of biologically active proteins. Platelet alpha granules are storage organelles that contain platelet-derived growth factor (PDGF), transforming growth factor-β (TGF-β), insulin-like growth factor I (IGF-I), fibronectin, fibrin-ogen, thrombospondin, and von Willebrand factor. The dense
Wound HealingMimi Leong, Kevin D. Murphy, Linda G. Phillips
Tissue Injury and ResponseWound-Healing PhasesAbnormal Wound HealingWound DressingsOther TherapiesFetal Wound HealingNew Horizons
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 131
clot and seal the wound. The resulting lattice framework is the scaffold for endothelial cells, inflammatory cells, and fibroblasts to repair the damaged vessel.
Thromboxane A2 and prostaglandin F2α, formed from the degradation of cell membranes in the arachidonic acid cascade, also assist in platelet aggregation and vasoconstriction. Although these activities serve to limit the amount of injury, they can also cause localized ischemia, resulting in further damage to cell mem-branes and the release of more prostaglandin F2α and thrombox-ane A2.
ChemokinesChemokines stimulate the migration of different cell types, par-ticularly inflammatory cells, into the wound and are active par-ticipants in the regulation of the different phases of wound healing. The CXC, CC, and C ligand families bind to G protein–coupled surface receptors called CXC receptors and CC receptors.
Macrophage chemoattractant protein (MCP-1 or CCL2) is induced in keratinocytes after injury. It is a potent chemoattrac-tant for monocytes/macrophages, T lymphocytes, and mast cells. Expression of this chemokine is sustained in chronic wounds and results in the prolonged presence of polymorphonuclear cells (PMNs) and macrophages, leading to the prolonged inflamma-tory response. CXCL1 (GRO-α) is a potent PMN chemotactic regulator and is increased in acute wounds. It is also involved in reepithelialization. Interleukin-8 (IL-8; CXCL8) expression is increased in acute and chronic wounds. It is involved in reepithe-lialization and induces the leukocyte expression of matrix metal-loproteinases (MMPs), which stimulates remodeling. It is also a strong chemoattractant for PMNs and participates in inflamma-tion. Relatively low levels of IL-8 are found in fetal wounds and may be why fetal wounds have decreased inflammation and heal without scars. Expression of the keratinocyte-produced chemo-kine interferon inducible protein 10 (CXCL10) is elevated in acute wounds and chronic inflammatory conditions. It impairs wound healing by increasing inflammation and recruiting lym-phocytes to the wound. It also inhibits proliferation by decreasing
FIGURE 6-1 Schematic diagram of the wound-healing continuum.
Hemostasis 1. Stop bleeding
2. Chemotaxis Inflammatory (reactive)
3. Epithelial migration
4. Proliferation Proliferative (regenerative)
5. Maturation
3. Contraction
4. Scarring
Maturational (remodeling)
5. Remodeling of scar
Inflammation
Connective tissueregeneration
Contracture
Healing Responses
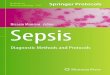
FIGURE 6-2 Time course of the appearance of different cells in the wound during healing. Macrophages and neutrophils are predominant during the inflammatory phase (peak at days 3 and 2, respectively). Lymphocytes appear later and peak at day 7. Fibroblasts are the pre-dominant cells during the proliferative phase. (Adapted from Witte MB, Barbul A: General principles of wound healing. Surg Clin North Am 77:509–528, 1997.)
020 4 6 8 141210 16
Days Postwounding
Rel
ativ
e N
umbe
r of
Cel
ls
Maturation
Proliferation
Inflammation
NeutrophilsMacrophages
Fibroblasts
Lymphocytes
bodies contain vasoactive amines, such as serotonin, that cause vasodilation and increased vascular permeability. Mast cells adher-ent to the endothelial surface release histamine and serotonin, resulting in increased permeability of endothelial cells and causing leakage of plasma from the intravascular space to the extracellular compartment.
The clotting cascade is initiated through the intrinsic and extrinsic pathways. As the platelets become activated, the mem-brane phospholipids bind factor V, which allows interaction with factor X. Membrane-bound prothrombinase activity is generated and potentiates thrombin production exponentially. The throm-bin itself activates platelets and catalyzes the conversion of fibrino-gen to fibrin. The fibrin strands trap red blood cells to form the
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles132
immunoglobulin G (IgG; Fc receptor) and the complement pro-teins C3b and C3bi. As the complement cascade is released and bacteria are opsonized, binding of these proteins to cell receptors on neutrophils allows recognition by the neutrophils and phago-cytosis of the bacteria. When neutrophils are stimulated, they express more CR1 and CR3 receptors, permitting more efficient binding and phagocytosis of these bacteria.
Functional activation occurs after migration of PMNs into the wound site, which may induce new cell surface antigen expres-sion, increased cytotoxicity, or enhanced production and release of cytokines. These activated neutrophils scavenge for necrotic debris, foreign material, and bacteria and generate free oxygen radicals, with electrons donated by the reduced form of nicotin-amide adenine dinucleotide phosphate. The electrons are trans-ported across the membrane into lysosomes, where superoxide anion (O2
−) is formed. Superoxide dismutase catalyzes the forma-tion of hydrogen peroxide (H2O2), which is then degraded by myeloperoxidase in the azurophilic granules of neutrophils. This interaction oxidizes halides, with the formation of byproducts such as hypochlorous acid. The iron-catalyzed reaction between H2O2 and O2
− forms hydroxyl radicals (OH⋅). This potent free radical is bactericidal as well as toxic to neutrophils and surround-ing viable tissues.
Migration of PMNs stops after several days or when wound contamination has been controlled. Individual PMNs survive no longer than 24 hours and are replaced predominantly by mono-nuclear cells. Continuing wound contamination or secondary infection causes complement system activation that provides a steady supply of chemotactic factors and a sustained influx of PMNs into the wound. A prolonged inflammatory phase delays wound healing, destroys normal tissue, and results in abscess formation and possibly systemic infection. PMNs are not essential for wound healing because their phagocytosis and antimicrobial role can be taken over by macrophages. Sterile incisions heal normally without the presence of PMNs.
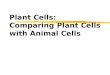
MacrophagesThe macrophage is the one cell that is truly crucial to wound healing by orchestrating the release of cytokines and stimulating many subsequent processes in wound healing (Fig. 6-3). Tissue macrophages are derived from chemotaxis of migrating mono-cytes and appear within 24 to 48 hours of injury. When neutro-phils start to disappear, macrophages appear and induce PMN apoptosis. Monocyte chemotactic factors include bacterial prod-ucts, complement degradation products (C5a), thrombin, fibro-nectin, collagen, TGF-β, and PDGF-BB. Monocyte chemotaxis occurs as a result of the interaction of integrin receptors on the monocyte surface with ECM fibrin and fibronectin. The β integrin receptor also transduces the signal to initiate macrophage phago-cytic activity. Activated integrin expression mediates monocyte transformation into wound macrophages. Transformation results in increased phagocytic activity and selective expression of cyto-kines and signal transduction elements by messenger RNA (mRNA), including the early growth response genes EGR2 and c-fos. Macrophages have specific receptors for IgG, C3b (CR1 and CR3), and fibronectin (integrin receptors) that permit surface recognition and phagocytosis of opsonized pathogens.
Bacterial debris, such as lipopolysaccharide, activates mono-cytes to release free radicals and cytokines that mediate angiogen-esis and fibroplasia. The presence of IL-2 increases free radical release and enhances bactericidal activity. Activity of the free radi-cals is potentiated by IL-2. Free radicals generate bacterial debris,
reepithelialization and angiogenesis and preventing fibroblast migration. Stromal cell–derived factor-1 (SDF-1; CXCL12) is expressed by endothelial cells, myofibroblasts, and keratinocytes and is involved in inflammation by recruiting lymphocytes to the wound and promoting angiogenesis. It is a potent chemoattrac-tant for endothelial cells and bone marrow progenitors from the circulation to peripheral tissues. It also enhances keratinocyte proliferation, resulting in reepithelialization.
Polymorphonuclear CellsThe release of histamine and serotonin leads to vascular permea-bility of the capillary bed. Complement factors such as C5a and leukotriene B4 promote neutrophil adherence and chemoattrac-tion. In the presence of thrombin, endothelial cells exposed to leukotriene C4 and D4 release platelet-aggregating factor, which further enhances neutrophil adhesion. Monocytes and endothelial cells produce the inflammatory mediators IL-1 and tumor necro-sis factor-α (TNF-α), and these mediators further promote endothelial-neutrophil adherence. The increased capillary perme-ability and the various chemotactic factors facilitate diapedesis of neutrophils into the inflammatory site. As the neutrophils begin their migration, they release the contents of their lysosomes and enzymes such as elastase and other proteases into the extracellular matrix (ECM), which further facilitates neutrophil migration. The combination of intense vasodilation and increased vascular permeability leads to clinical findings of inflammation, rubor (redness), tumor (swelling), calor (heat), and dolor (pain). Local tissue swelling is further promoted by the deposition of fibrin, a protein end product of coagulation, and the fibrin becomes entrapped in lymphatic vessels.
Evidence suggests that the migration of PMNs requires sequen-tial adhesive and de-adhesive interactions between β1 and β2 inte-grins and ECM components. Integrin molecules are a family of cell surface receptors that are closely coupled with the cell’s cyto-skeleton. These molecules interact with components of the ECM, such as fibronectin, to provide adhesion and to transduce signal to the interior of the cell.
Integrins are crucial for cell motility and are required in inflam-mation and normal wound healing as well as in embryonic devel-opment and tumor metastases. After extravasation, PMNs, attracted by chemotaxins, migrate through the ECM via transient interactions between integrin receptors and their ligands. Four phases of integrin-mediated cell motility have been described: adhesion, spreading, contractility or traction, and retraction. Acti-vation of specific integrins through ligand binding has been shown to increase cell adhesion and activate reorganization of the cell’s actin cytoskeleton. Spreading is characterized by the develop-ment of lamellipodia and filopodia. Traction at the leading edge of the cell develops through binding of integrin, followed by translocation of the cell over the adherent segment of the plasma membrane. The integrin is shifted to the rear of the cell and releases its substrate, permitting cell advancement. Regulation of integrin function by adhesive substrates offers a mechanism for local control of migrant cells. Within the assembled framework of the ECM, binding sites for integrins have been identified on collagen, laminin, and fibronectin.
The chemotactic agent mediates the PMN response through signal transduction as the chemotaxin binds to receptors on the cell surface. Bacterial products such as N-formyl-methionyl-leucyl-phenylalanine bind to induce cyclic adenosine monophos-phate, but if there is maximal receptor occupancy, superoxide is produced at peak rates. Neutrophils also possess receptors for
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 133
FIGURE 6-3 Interaction of cellular and humoral factors in wound healing. Note the key role of the macro-phage. bFGF, basic fibroblast growth factor; EGF, epidermal growth factor; GAGs, glycosaminoglycans; H2O2, hydrogen peroxide; IFN-γ, interferon-γ; IGF, insulin-like growth factor; IL-1, interleukin-1; IL-6, interleukin-6; KGF, keratinocyte growth factor; O2
−, superoxide; −OH, hydroxyl radical; PDGF, platelet-derived growth factor; PGE2, prostaglandin E2; TGF-β, transforming growth factor-β; TNF-α, tumor necrosis factor-α; VEGF, vascular endothelial growth factor. (Adapted from Witte MB, Barbul A: General principles of wound healing. Surg Clin North Am 77:509–528, 1997.)
which further potentiates the activation of monocytes. Activated wound macrophages also produce nitric oxide (NO), a substance that has been demonstrated to have many functions other than antimicrobial properties.
As the monocyte or macrophage is activated, phospholipase is induced, cell membrane phospholipids are enzymatically degraded, and thromboxane A2 and prostaglandin F2α are released. The macrophage also releases leukotrienes B4 and C4 and 15-hydroxyeicosatetraenoic acid and 5-hydroxyeicosatetraenoic acid. Leukotriene B4 is a potent chemotaxin for neutrophils and increases their adherence to endothelial cells.
Wound macrophages release proteinases, including MMPs (MMP-1, MMP-2, MMP-3, and MMP-9), which degrade the ECM and are crucial for removing foreign material, promoting cell movement through tissue spaces, and regulating ECM turnover. This activity is dependent on the cyclic adenosine monophosphate pathway and can be blocked by nonsteroidal anti-inflammatory drugs or glucocorticoid drugs. Colchicine and retinoic acid appear to decrease collagenase production as well.
Macrophages secrete numerous cytokines and growth factors (Tables 6-1 and 6-2). IL-1, a proinflammatory cytokine, is an acute-phase response cytokine. This endogenous pyrogen causes lymphocyte activation and stimulation of the hypothalamus, inducing the febrile response. It also directly affects hemostasis by inducing the release of vasodilators and stimulating coagulation. Its effect is further amplified as endothelial cells produce it in the presence of TNF-α and endotoxin. IL-1 has numerous effects, such as enhancement of collagenase production, stimulation of carti-lage degradation and bone reabsorption, activation of neutrophils, regulation of adhesion molecules, and promotion of chemotaxis. It stimulates other cells to secrete proinflammatory cytokines. Its effects extend into the proliferative phase, during which it increases fibroblast and keratinocyte growth and collagen synthesis. Studies have demonstrated increased levels of IL-1 in chronic nonhealing wounds, suggesting its role in the pathogenesis of poor wound healing. The early beneficial responses of IL-1 in wound healing appear to be maladaptive if elevated levels last beyond the first week after injury.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles134
Adapted from Rumalla VK, Borah GL: Cytokines, growth factors, and plastic surgery. Plast Reconstr Surg 108:719–733, 2001; and Barrientos S, Stojadinovic O, Golinko MS, et al: Growth factors and cytokines in wound healing. Wound Repair Regen 16:585–601, 2008.IFN-γ, Interferon-γ; IL-1, -2, -4, -6, -8, -10, interleukin-1, -2, -4, -6, -8, -10; PMN, polymorphonuclear cell; TNF-α, tumor necrosis factor-α.
TABLE 6-1 Cytokine Activity in Wound Healing
TYPE OF WOUND
CYTOKINE CELL SOURCE FUNCTION ACUTE CHRONIC
Proinflammatory CytokinesTNF-α PMNs, macrophages Inflammation, reepithelialization, PMN margination and cytotoxicity,
with or without collagen synthesis; provides metabolic substrateIncreased levels Increased levels
IL-1 PMNs, monocytes, macrophages, keratinocytes
Inflammation, reepithelialization, fibroblast and keratinocyte chemotaxis, collagen synthesis
Increased levels Increased levels
IL-2 T lymphocytes Increases fibroblast infiltration and metabolismIL-6 PMNs, macrophages,
fibroblastsInflammation, reepithelialization, fibroblast proliferation, hepatic
acute-phase protein synthesisIncreased levels Increased levels
IL-8 Macrophages, fibroblasts Inflammation, macrophage and PMN chemotaxis; reepithelialization, keratinocyte maturation and proliferation
Increased levels Increased levels
IFN-γ T lymphocytes, macrophages Activates macrophages and PMNs, retards collagen synthesis and cross linking, stimulates collagenase activity
Anti-inflammatory CytokinesIL-4 T lymphocytes, basophils,
mast cellsInhibition of TNF-α, IL-1, IL-6 production; fibroblast proliferation,
collagen synthesisIL-10 T lymphocytes, macrophages,
keratinocytesInhibition of TNF-α, IL-1, IL-6 production, inhibition of macrophage
and PMN activation
Microbial byproducts induce macrophages to release TNF. TNF-α is crucial in initiating the response to injury or bacteria. It upregulates cell surface adhesion molecules that promote the interaction of immune cells and endothelium. TNF-α is detected in a wound within 12 hours and peaks after 72 hours. Its effects include hemostasis, increased vascular permeability, and enhanced endothelial proliferation. Similar to IL-1, TNF-α induces fever, increased collagenase production, reabsorption of cartilage and bone, and release of PDGF as well as the production of more IL-1. However, excessive production of TNF-α has been associated with multisystem organ failure and increased morbidity and mortality in inflammatory disease states, partly through its effects on acti-vating macrophages and neutrophils. Studies have noted elevated levels of TNF-α in nonhealing versus healing chronic venous ulcers. As in the case of IL-1, TNF-α appears to be essential in the early inflammatory response required for wound healing, but local and systemic persistence of this cytokine may lead to impaired wound maturation.
IL-6, which is produced by monocytes and macrophages, is involved in stem cell growth, activation of B cells and T cells, and regulation of the synthesis of hepatic acute-phase proteins. Within acute wounds, IL-6 is also secreted by PMNs and fibroblasts, and increase in IL-6 parallels the increase in the PMN count locally. IL-6 is detectable within 12 hours of experimental wounding and may persist at high concentrations for longer than 1 week. It also works synergistically with IL-1, TNF-α, and endotoxins. It is a potent stimulator of fibroblast proliferation and is decreased in aging fibroblasts and fetal wounds.
IL-8 (also called CXCL8) is secreted primarily by macrophages and fibroblasts in the acute wound, with peak expression within the first 24 hours. Its major effects have already been discussed and include increased PMN and monocyte chemotaxis, PMN degranulation, and expression of endothelial cell adhesion molecules.
Interferon-γ (IFN-γ), another proinflammatory cytokine, is secreted by T lymphocytes and macrophages. Its major effects are macrophage and PMN activation and increased cytotoxicity. It has also been shown to reduce local wound contraction and aid in tissue remodeling. IFN-γ has been used in the treatment of hypertrophic and keloid scars, possibly by its effect in slowing collagen production and cross linking, whereas collagenase (MMP-1) production increases. Experimentally, it has been shown to impair reepithelialization and wound strength in a dose-dependent manner when applied locally or systemically. These findings suggest that administration of IFN-γ may improve scar hypertrophy by decreasing the strength of the wound.
Macrophages also release growth factors that stimulate fibro-blast, endothelial cell, and keratinocyte proliferation and are important in the proliferative phase (see Table 6-2). Macrophage-secreted PDGF stimulates collagen and proteoglycan synthesis. PDGF exists as three isomers—PDGF-AA, PDGF-AB, and PDGF-BB. The PDGF-BB isomer is the only growth factor prep-aration approved by the U.S. Food and Drug Administration (FDA) and is the most widely studied clinically.
TGF-α and TGF-β are released by activated monocytes. TGF-α stimulates epidermal growth and angiogenesis. TGF-β itself stimu-lates monocytes to express other peptides, such as TGF-α, IL-1, and PDGF. TGF-β, which is also released by platelets and fibro-blasts within wounds, exists as at least three isomers—β1, β2, and β3—and its effects include fibroblast migration and maturation and ECM synthesis. TGF-β1 has been shown to play an important role in collagen metabolism and healing of gastrointestinal injuries and anastomoses. In experimental models, TGF-β1 accelerates wound healing in normal, steroid-impaired, and irradiated animals.
TGF-β is the most potent stimulant of fibroplasia, and its strong mitogenic effects have been implicated in the fibrogenesis seen in disease states such as scleroderma and interstitial
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 135
Adapted from Schwartz SI (ed): Principles of Surgery, ed 7, New York, 1999, McGraw-Hill, p 269; and Barrientos S, Stojadinovic O, Golinko MS, et al: Growth factors and cytokines in wound healing. Wound Repair Regen 16:585–601, 2008.
TABLE 6-2 Growth Factors That Affect Wound Healing
TYPE OF WOUND
GROWTH FACTOR CELL SOURCE FUNCTION ACUTE CHRONIC
PDGF Platelets, macrophages, endothelial cells, keratinocytes, fibroblasts
Inflammation; granulation tissue formation; reepithelialization; matrix formation and remodeling; chemotactic for PMNs, macrophages, fibroblasts, and smooth muscle cells; activates PMNs, macrophages, and fibroblasts; mitogenic for fibroblasts, endothelial cells; stimulates production of MMPs, fibronectin, and HA; stimulates angiogenesis and wound contraction
Increased levels Decreased levels
TGF-β (including isoforms β1, β2, and β3)
Platelets, T lymphocytes, macrophages, endothelial cells, keratinocytes, fibroblasts
Inflammation; granulation tissue formation; reepithelialization; matrix formation and remodeling; chemotactic for PMNs, macrophages, lymphocytes, fibroblasts; stimulates TIMP synthesis, keratinocyte migration, angiogenesis, and fibroplasia; inhibits production of MMPs and keratinocyte proliferation; induces TGF-β production
Increased levels Decreased levels
EGF Platelets, macrophages, fibroblasts
Mitogenic for keratinocytes and fibroblasts; stimulates keratinocyte migration
Increased levels Decreased levels
FGF-1 and FGF-2 family Macrophages, mast cells, T lymphocytes, endothelial cells, fibroblasts, keratinocytes, smooth muscle cells, chondrocytes
Granulation tissue formation; reepithelialization; matrix formation and remodeling; chemotactic for fibroblasts, mitogenic for fibroblasts and keratinocytes; stimulates keratinocyte migration; angiogenesis; wound contraction and matrix deposition
Increased levels Decreased levels
KGF (also called FGF-7) Fibroblasts, keratinocytes, smooth muscle cells, chondrocytes, endothelial cells, mast cells
Stimulate proliferation and migration of keratinocytes, increase transcription of factors involved in detoxification of ROS, potent mitogen for vascular endothelial cells; upregulates VEGF, stimulates endothelial cell production of UPA
Increased levels Decreased levels
VEGF Keratinocytes, platelets, PMNs, macrophages, endothelial cells, smooth muscle cells, fibroblasts
Granulation tissue formation; increases vasopermeability; mitogenic for endothelial cells
Increased levels Decreased levels
TGF-α Macrophages, T lymphocytes, keratinocytes, platelets, fibroblasts, lymphocytes
Reepithelialization; increase keratinocyte migration and proliferation
IGF-I Macrophages, fibroblasts Stimulates elastin production and collagen synthesis, fibroblast proliferation
EGF, Epidermal growth factor; FGF-1, -2, -7, fibroblast growth factor-1, -2, -7; HA, hyaluronic acid; IGF-I, insulin-like growth factor I; KGF, keratinocyte growth factor; MMP, matrix metalloproteinase; PDGF, platelet-derived growth factor; PMN, polymorphonuclear cell; ROS, reactive oxygen species; TGF-α,-β, transforming growth factor-α, -β; TIMP, tissue inhibitors of metalloproteinase; UPA, urokinase-type plasminogen activator; VEGF, vascular endothelial growth factor.
pulmonary fibrosis. Enhanced expression of TGF-β1 mRNA is found in keloid and hypertrophic scars. In contrast, fetal wounds have been demonstrated to have a paucity of TGF-β, suggesting that the scarless repair seen in utero occurs because of low or absent amounts of TGF-β. Studies of the three isomers have sug-gested that although TGF-β1 and TGF-β2 play an important role in tissue fibrosis and postinjury scarring, TGF-β3 may limit scar-ring. As the concentration of TGF-β increases in the inflamma-tory site, fibroblasts are directly stimulated to produce collagen and fibronectin, leading to the proliferative phase.
Wound macrophages exhibit different functional phenotypes— M1 (classically activated) and M2 (alternatively activated)—that are at the extremes of a continuum of macrophage function. Lipopolysaccharide and IFN-γ stimulate the differentiation into M1 macrophages that release TNF-α, NO, and IL-6. These mediators are responsible for host defense but at the expense of significant collateral tissue damage. M2 macrophages are
activated by IL-4 and IL-13; suppress inflammatory reactions and adaptive immune responses; and play an important role in wound healing, angiogenesis, and defense against parasitic infec-tions. However, despite their beneficial functions, M2 macro-phages can also be involved in different diseases, such as allergy, asthma, and fibrosis, which is the result of a helper T cell (Th2) response, which is predominated by IL-4 or IL-10. Both pheno-types are important when correctly balanced during the different phases of wound healing. In the inflammatory phase, greater M1 macrophage activity is required for macrophage debris scaveng-ing and invading pathogen destruction. In the proliferative phase, M2 macrophages predominate. The balance between M1 and M2 macrophages is likely disturbed during abnormal wound-healing responses.
Several studies have demonstrated the importance of macro-phages in wound healing by macrophage depletion. Macrophage depletion delays wound infiltration by fibroblasts and decreased
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles136
After injury, the endothelium is exposed to numerous soluble factors and comes in contact with adhering blood cells. These inter-actions result in upregulation of the expression of cell surface adhe-sion molecules, such as vascular cell surface adhesion molecule-1. Matrix-degrading enzymes, such as plasmin and the metallopro-teinases, are released and activated and degrade the endothelial basement membrane. Fragmentation of the basement membrane allows migration of endothelial cells into the wound, promoted by fibroblast growth factor (FGF), PDGF, and TGF-β. Injured endo-thelial cells express adhesion molecules, such as the integrin αvβ3, which facilitates attachment to fibrin, fibronectin, and fibrinogen and facilitates endothelial cell migration along the provisional matrix scaffold. Platelet endothelial cell adhesion molecule-1 (PECAM-1), also found on endothelial cells, modulates their inter-action with each other as they migrate into the wound.
Capillary tube formation is a complex process that involves cell-cell and cell-matrix interactions, modulated by adhesion mol-ecules on endothelial cell surfaces. PECAM-1 has been observed to mediate cell-cell contact, whereas β1 integrin receptors may aid in stabilizing these contacts and forming tight junctions between endothelial cells. Some of the new capillaries differentiate into arterioles and venules, whereas others undergo involution and apoptosis, with subsequent ingestion by macrophages. Regulation of endothelial apoptosis is not well understood.
Angiogenesis appears to be stimulated and manipulated by various cytokines predominantly produced by macrophages and platelets. As the macrophage produces TNF-α, it orchestrates angiogenesis during the inflammatory phase. Heparin, which can stimulate the migration of capillary endothelial cells, binds with high affinity to a group of angiogenic factors.
VEGF, a member of the PDGF family of growth factors, has potent angiogenic activity. It is produced in large amounts by keratinocytes, macrophages, endothelial cells, platelets, and fibro-blasts during wound healing. Cell disruption and hypoxia, hall-marks of tissue injury, appear to be strong initial inducers of potent angiogenic factors at the wound site, such as VEGF and its receptor. VEGF family members include VEGF-A, VEGF-B, VEGF-C, VEGF-D, VEGF-E, and placental growth factor (PlGF). VEGF-A promotes early events in angiogenesis and sub-sequently is crucial to wound healing. It binds to tyrosine kinase surface receptors Flt-1 (VEGF receptor-1, or VEGFR-1) and KDR (VEGF receptor-2, or VEGFR-2). Flt-1 is required for blood vessel organization, whereas KDR is important for endo-thelial cell chemotaxis, proliferation, and differentiation. Animal studies have shown that VEGF-A administration restores impaired angiogenesis found in diabetic ischemic limbs; however, other studies have shown that exogenous VEGF results in vascular leakage and disorganized blood vessel formation. VEGF-C, which is also elevated during wound healing, is primarily released by macrophages and is important during the inflammatory phase of wound healing. Although it works primarily through VEGF receptor-3 (VEGFR-3), which is expressed in macrophages and lymphatic endothelium, it can also activate VEGFR-2, increasing vascular permeability. In vivo administration of VEGF-C in an animal model using an adenoviral vector to genetically diabetic mice resulted in accelerated healing. PlGF is another proangio-genic factor that is elevated after wounding. It is involved in inflammation and expressed by keratinocytes and endothelial cells. It is believed to work synergistically with VEGF, potentiating its proangiogenic function.
Both acidic and basic FGFs (FGF-1 and FGF-2) are released from disrupted parenchymal cells and are early stimulants of
wound fibrosis. Newborn animals that lacked macrophages, mast cells, and functional neutrophils as a result of defective myelopoi-esis healed without scarring at the same speed as wild-type animals if their wounds were protected by antibiotic coverage, suggesting that inflammatory cells are not essential for wound closure. However, several models of specific inducible macrophage deple-tion based on genetically modified mice resulted in a detrimental effect of preinjury depletion of macrophages.1-3 Mice depleted before injury typically showed a defect in reepithelialization, granulation tissue formation, angiogenesis, wound cytokine pro-duction, and myofibroblast-associated wound contraction. Mac-rophage depletion 9 days after injury did not result in any morphologic or biologic differences between control and treat-ment mice, suggesting that macrophages may not be required at later stages of wound healing.2
LymphocytesSignificant numbers of T lymphocytes appear by day 5 after injury and peak on day 7. B lymphocytes appear to be principally involved in downregulating healing as the wound closes. Lympho-cytes stimulate fibroblasts with cytokines (IL-2 and fibroblast-activating factor). Lymphocytes also secrete inhibitory cytokines (TGF-β, TNF-α, and IFN-γ). Antigen-presenting macrophages present bacterial “debris” or enzymatically degraded host proteins to lymphocytes, stimulating lymphocyte proliferation and cyto-kine release. T cells produce IFN-γ, which stimulates the macro-phage to release TNF-α and IL-1. IFN-γ decreases prostaglandin synthesis enhancing the effect of inflammatory mediators, sup-pressing collagen synthesis, and inhibiting macrophage exodus. IFN-γ appears to be an important mediator of chronic nonhealing wounds, and its presence suggests that T lymphocytes are primar-ily involved in chronic wound healing.
Drugs that suppress T-lymphocyte function and proliferation (steroids, cyclosporine, tacrolimus) result in impaired wound healing in experimental wound models, possibly through decreased NO synthesis. In vivo lymphocyte depletion suggests the existence of an incompletely characterized T cell lymphocyte population that is neither CD4+ nor CD8+ that seems to be responsible for the promotion of wound healing.
Proliferative PhaseAs the acute responses of hemostasis and inflammation begin to resolve, the scaffolding is laid for repair of the wound through angiogenesis, fibroplasia, and epithelialization. This stage is char-acterized by the formation of granulation tissue, which consists of a capillary bed; fibroblasts; macrophages; and a loose arrange-ment of collagen, fibronectin, and hyaluronic acid. Numerous studies have used growth factors to modify granulation tissue, particularly fibroplasia. Adenoviral transfer, topical application, and subcutaneous injection of PDGF, TGF-β, keratinocyte growth factor (KGF), vascular endothelial growth factor (VEGF), and epidermal growth factor (EGF) have been tested to increase the proliferation of granulation tissue.
AngiogenesisAngiogenesis is the process of new blood vessel formation and is necessary to support a healing wound environment. After injury, activated endothelial cells degrade the basement membrane of postcapillary venules, allowing the migration of cells through this gap. Division of these migrating endothelial cells results in tubule or lumen formation. Eventually, deposition of the basement membrane occurs and results in capillary maturation.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 137
maturation phase, and new capillaries regress and disappear. These changes alter the appearance of the wound and increase its strength.
EpithelializationThe epidermis serves as a physical barrier to prevent fluid loss and bacterial invasion. Tight cell junctions within the epithelium con-tribute to its impermeability, and the basement membrane zone gives structural support and provides attachment between the epidermis and the dermis. The basement membrane zone consists of several layers: (1) lamina lucida (electron clear), consisting of laminin and heparan sulfate; (2) lamina densa (electron dense), containing type IV collagen; and (3) anchoring fibrils, consisting of type IV collagen, which secure the epidermodermal interface and connect the lamina densa to the dermis.
The basal layer of the epidermis attaches to the basement membrane zone by hemidesmosomes. Reepithelialization of wounds begins within hours after injury. Initially, the wound is rapidly sealed by clot formation and then by epithelial (epidermal) cell migration across the defect. Keratinocytes located at the basal layer of the residual epidermis or in the depths of epithelium-lined dermal appendages migrate to resurface the wound. Epithelializa-tion involves a sequence of changes in wound keratinocytes—detachment, migration, proliferation, differentiation, and stratifi-cation. If the basement membrane zone is intact, epithelialization proceeds more rapidly. The cells are stimulated to migrate. Attach-ments to neighboring and adjoining cells and to the dermis are loosened, as demonstrated by intracellular tonofilament retrac-tion, dissolution of intercellular desmosomes and hemidesmo-somes linking the epidermis to the basement membrane, and formation of cytoplasmic actin filaments.
Epidermal cells express integrin receptors that allow them to interact with ECM proteins such as fibronectin. The migrating cells dissect the wound by separating the desiccated eschar from viable tissue. This path of dissection is determined by the integrins that the epidermal cells express on their cell membranes. Degrada-tion of the ECM, required if epidermal cells are to migrate between the collagenous dermis and fibrin eschar, is driven by epidermal cell production of collagenase (MMP-1) and plasmino-gen activator, which activates collagenase and plasmin. The migrating cells are also phagocytic and remove debris in their path. Cells behind the leading edge of migrating cells begin to proliferate. The epithelial cells move in a leapfrog and tumbling fashion until the edges establish contact. If the basement mem-brane zone is not intact, it will be repaired first. The absence of neighboring cells at the wound margin may be a signal for the migration and proliferation of epidermal cells. Local release of EGF, TGF-α, and KGF and increased expression of their receptors may also stimulate these processes. Topical application of KGF-2 in young and aged animals accelerates reepithelialization. Base-ment membrane proteins, such as laminin, reappear in a highly ordered sequence from the margin of the wound inward. After the wound is completely reepithelialized, the cells become colum-nar and stratified again, while firmly attaching to the reestablished basement membrane and underlying dermis.
Extracellular MatrixThe ECM exists as a scaffold to stabilize the physical structure of tissues, but it also plays an active and complex role by regulating the behavior of cells that contact it. Cells within it produce the macromolecular constituents, including (1) glycosaminoglycans (GAGs), or polysaccharide chains, usually found covalently linked
angiogenesis. FGF-2 provides the initial angiogenic stimulus within the first 3 days of wound repair, followed by a subsequent prolonged stimulus mediated by VEGF from days 4 through 7. There is a dose-dependent effect of VEGF and FGF-2 on angio-genesis. Both TGF-α and EGF stimulate endothelial cell prolif-eration. TNF-α is chemotactic for endothelial cells; it promotes formation of the capillary tube and may mediate angiogenesis through its induction of hypoxia-inducible factor 1 (HIF-1). It regulates the expression of other hypoxia-responsive genes, includ-ing inducible NO synthase and VEGF. HIF-1α mRNA is promi-nently present in wound inflammatory cells during the initial 24 hours, and HIF-1α protein is present in cells isolated from the wound 1 and 5 days after injury in vitro. Data also suggest that there is a positive interaction between endogenous NO and VEGF, with endogenous NO enhancing VEGF synthesis. Simi-larly, VEGF has been shown to promote NO synthesis in angio-genesis, suggesting that NO mediates aspects of VEGF signaling required for endothelial cell proliferation and organization.
TGF-β is a chemoattractant for fibroblasts and probably assists in angiogenesis by signaling the fibroblast to produce FGFs. Other factors that have been shown to induce angiogenesis include angiogenin, IL-8, and lactic acid. Several of the matrix materials, such as fibronectin and hyaluronic acid from the wound site, are angiogenic. Fibronectin and fibrin are produced by macrophages and damaged endothelial cells. Collagen appears to interact by causing the tubular formation of endothelial cells in vitro. Angio-genesis results from the complex interaction of ECM material and cytokines.
FibroplasiaFibroblasts are specialized cells that differentiate from resting mes-enchymal cells in connective tissue; they do not arrive in the wound cleft by diapedesis from circulating cells. After injury, the normally quiescent and sparse fibroblasts are chemoattracted to the inflammatory site, they divide and produce the components of the ECM. After stimulation by macrophage-derived and platelet-derived cytokines and growth factors, the fibroblast, which is normally arrested in the G0 phase, undergoes replication and proliferation. Platelet-derived TGF-β stimulates fibroblast proliferation indirectly by releasing PDGF. The fibroblast can also stimulate replication in an autocrine manner by releasing FGF-2. To continue proliferating, fibroblasts require further stimulation by factors such as EGF or IGF-I. Although fibroblasts require growth factors for proliferation, they do not need growth factors to survive. Fibroblasts can live quiescently in growth factor–free media in monolayers or three-dimensional cultures.
The primary function of fibroblasts is to synthesize collagen, which they begin to produce during the cellular phase of inflam-mation. The time required for undifferentiated mesenchymal cells to differentiate into highly specialized fibroblasts accounts for the delay between injury and the appearance of collagen in a healing wound. This period, generally 3 to 5 days, depending on the type of tissue injured, is termed the lag phase of wound healing. Fibro-blasts begin to migrate in response to chemotactic substances such as growth factors (PDGF, TGF-β), C5 fragments, thrombin, TNF-α, eicosanoids, elastin fragments, leukotriene B4, and frag-ments of collagen and fibronectin.
The rate of collagen synthesis declines after 4 weeks and even-tually balances the rate of collagen destruction by collagenase (MMP-1). At this point, the wound enters a phase of collagen maturation. The maturation phase continues for months or years. Glycoprotein and mucopolysaccharide levels decrease during the
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles138
subsequent decreased adhesion and, as a result, these cells can break away from the primary tumor and metastasize.
An example of the necessary dynamic interactions occurring in the provisional matrix during wound healing is the effect of TGF-β on incisional wounds sealed with fibrin sealant. Fibrin sealant is a derivative of plasma components that mimics the last step in the coagulation cascade. Commercially available fibrin sealant has an approximately 10-fold greater concentration of fibrin than plasma and consequently provides a more airtight, waterproof seal. Fibrin sealant may serve as a mechanical barrier to the early cell-mediated events occurring in wound healing. Supplementation of fibrin sealant with TGF-β has been demon-strated to reverse the inhibitory effects of fibrin sealant on wound healing and increase tensile strength compared with sutured wounds. The increased tensile strength may be a result of improved cell migration into the wound site, more rapid clearance of fibrin sealant, suppression of gelatinase (MMP-9), and enhancement of ECM synthesis in TGF-β–supplemented wounds.
Collagen structure. Collagens are found in all multicellular animals and are secreted by various cell types. They are a major component of skin and bone and constitute 25% of the total protein mass in mammals. The proline-rich and glycine-rich col-lagen molecule is a long, stiff, triple-stranded helical structure that consists of three collagen polypeptide α chains wound around one another in a ropelike superhelix. With its ringlike structure, proline provides stability to the helical conformation in each α chain, whereas glycine, because of its small size, allows tight packing of the three α chains to form the final superhelix. There are at least 20 types of collagen, the main constituents of connec-tive tissue being types I, II, III, V, and XI. Type I is the principal collagen of skin and bone and is the most common. In adults, the skin is approximately 80% type I and 20% type III. In newborns, the content of type III collagen is greater than that found in adults. In early wound healing, there is also increased expression of type III collagen. Type I collagens are the fibrillar, or fibril-forming, collagens. They are secreted into the extracellular space, where they assemble into collagen fibrils (10 to 300 nm in diam-eter), which then aggregate into larger, cable-like bundles called collagen fibers (several micrometers in diameter).
Other types of collagens include types IX and XII (fibril-associated collagens) and types IV and VII (network-forming collagens). Types IX and XII are found on the surface of collagen fibrils and serve to link the fibrils to one another and to other components in the ECM. Type IV molecules assemble into a meshlike pattern and are a major part of the mature basal lamina. Dimers of type VII form anchoring fibrils that help attach the basal lamina to the underlying connective tissue and are especially abundant in the skin.
Type XVII and type XVIII collagens are two of a number of collagen-like proteins. Type XVII has a transmembrane domain and is found in hemidesmosomes. Type XVIII is located in the basal laminae of blood vessels. The peptide endostatin, which inhibits angiogenesis and shows promise as an anticancer drug, is formed by cleavage of the C-terminal domain of type XVIII collagen.
Collagen synthesis. Collagen polypeptide chains are synthe-sized on membrane-bound ribosomes and enter the endoplasmic reticulum (ER) lumen as pro–α chains (Fig. 6-5). These precur-sors have amino-terminal signal peptides to direct them to the ER as well as propeptides at the N-terminal and C-terminal ends. Within the lumen of the ER, some of the prolines and lysines undergo hydroxylation to form hydroxyproline and
to protein in the form of proteoglycans, and (2) fibrous proteins such as collagen, elastin, fibronectin, and laminin.
In connective tissue, proteoglycan molecules form a gel-like ground substance. This highly hydrated gel allows the matrix to withstand compressive force while permitting rapid diffusion of nutrients, metabolites, and hormones between blood and tissue cells. Collagen fibers within the matrix serve to organize and strengthen it, whereas elastin fibers give it resilience, and matrix proteins have adhesive functions.
The wound matrix accumulates and changes in composition as healing progresses, balanced between new deposition and deg-radation (Fig. 6-4). The provisional matrix is a scaffold for cellular migration and is composed of fibrin, fibrinogen, fibronectin, and vitronectin. GAGs and proteoglycans are synthesized next and support further matrix deposition and remodeling. Collagens, which are the predominant scar proteins, are the end result. Attachment proteins, such as fibrin and fibronectin, provide linkage to the ECM through binding to cell surface integrin receptors.
Stimulation of fibroblasts by growth factors induces upregu-lated expression of integrin receptors, facilitating cell-matrix inter-actions. Ligand binding induces clustering of integrin into focal adhesion sites. Regulation of integrin-mediated cell signaling by the extracellular divalent cations Mg2+, Mn2+, and Ca2+ perhaps is caused by induction of conformational changes in the integrins.
A dynamic and reciprocal relationship exists between fibro-blasts and the ECM. Cytokine regulation of fibroblast responses is altered by variations in the composition of the ECM. For example, expression of matrix-degrading enzymes, such as the MMPs, is upregulated after cytokine stimulation of fibroblasts. Collagenolytic MMP-1 is induced by IL-1 and downregulated by TGF-β. Activation of plasminogen to plasmin by plasminogen activator and procollagenase to collagenase by plasmin results in matrix degradation and facilitates cell migration. Modulation of these processes provides additional mechanisms whereby the cell-matrix interaction can be regulated during wound healing. Matrix modulation is also seen in tumor metastasis. Neoplastic cells lose their dependence on anchorage, mediated mainly by integrins; this is probably caused by decreased production of fibronectin and
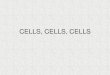
FIGURE 6-4 Wound matrix deposition over time. Fibronectin and type III collagen constitute the early matrix. Type I collagen accumulates later and corresponds to the increase in wound-breaking strength. (Adapted from Witte MB, Barbul A: General principles of wound healing. Surg Clin North Am 77:509–528, 1997.)
020 4 6 8 141210 16
Days Postwounding
Rel
ativ
e A
mou
nts
of M
atrix
Syn
thes
is Maturation
Proliferation
Inflammation
Wound breaking strength
Collagen I
Collagen III
Fibronectin
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 139
Elastic fibers. Tissues such as skin, blood vessels, and lungs require strength and elasticity to function. Elastic fibers in the ECM of these tissues provide the resilience to allow recoil after transient stretching.
Elastic fibers are predominantly composed of elastin, a highly hydrophobic protein (≈750 amino acids long). Soluble tropoelas-tin is secreted into the extracellular space, where it forms lysine cross links to other tropoelastin molecules to generate a large network of elastin fibers and sheets. Elastin is composed of hydro-phobic and alanine-rich and lysine-rich α-helical segments that alternate along the polypeptide chain. The hydrophobic segments are responsible for the elastic properties of the molecule. The alanine-rich and lysine-rich α-helical segments form cross links between adjacent molecules. Although the proposed conforma-tion of elastin molecules is controversial, the predominant theory is that the elastin polypeptide chain adopts a random coil confor-mation that allows the network to stretch and recoil like a rubber band. Elastic fibers consist of an elastin core covered by a sheath of microfibrils, which are composed of several distinct glycopro-teins such as fibrillin. Elastin-binding fibrillin is essential for integ-rity of the elastic fibers.
Microfibrils appear before elastin in developing tissues and seem to form a scaffold on which the secreted elastin molecules are deposited. Elastin is produced early in life, stabilizes, and does not undergo much further synthesis or degradation, with a turn-over that approaches the life span. Age-related modification is a result of progressive degradation as the elastic fibers gradually become tortuous, frayed, and porous. Scanning electron micros-copy shows that, in humans, the elastic meshwork grows largely undistorted during postnatal growth, during which fibers seem to enlarge in synchrony with growth of the tissue. In circumstances not involving a wound, there is little elastin degradation, probably
hydroxylysine. Hydroxylation results in the stable triple-stranded helix through the formation of interchain hydrogen bonds. The pro–α chain then combines with two others to form procollagen, a hydrogen-bonded, triple-stranded helical molecule. In condi-tions such as vitamin C (ascorbic acid) deficiency (scurvy), proline hydroxylation is prevented, resulting in the formation of unstable triple helices secondary to the synthesis of defective pro–α chains. Vitamin C deficiency is characterized by the gradual loss of pre-existing normal collagen, which leads to fragile blood vessels and loose teeth.
After secretion into the ECM, specific proteases cleave the propeptides of the procollagen molecules to form collagen mono-mers. These monomers assemble to form collagen fibrils in the ECM, driven by the tendency of collagen to self-assemble. Cova-lent cross linking of the lysine residues provides tensile strength. The extent and type of cross linking vary from tissue to tissue. In tissues such as tendons, in which tensile strength is crucial, col-lagen cross linking is extremely high. In mammalian skin, the fibrils are organized in a basketweave pattern to resist multidirec-tional tensile stress. In tendons, fibrils are in parallel bundles aligned along the major axis of tension.
Numerous factors can affect collagen synthesis. Vitamin C (ascorbic acid), TGF-β, IGF-I, and IGF-II increase collagen syn-thesis. IFN-γ decreases type I procollagen mRNA synthesis, and glucocorticoids inhibit procollagen gene transcription, leading to decreased collagen synthesis.
Several genetic disorders are caused by abnormalities in colla-gen fibril formation. In osteogenesis imperfecta, deletion of one procollagen α1 allele results in weak, easily fractured bones. Ehlers-Danlos syndrome is a result of mutations affecting type III collagen and is characterized by fragile skin and blood vessels and hypermobile joints.
FIGURE 6-5 Intracellular and extracellular events in the formation of a collagen fibril. A, Collagen fibrils are shown assembling in the extracellular space contained within a large infolding in the plasma membrane. As one example of how collagen fibrils can form ordered arrays in the extracellular space, they are shown further assembling into large collagen fibers, which are visible with a light microscope. The covalent cross links that stabilize the extracellular assemblies are not shown. B, Electron micrograph of a negatively stained collagen fibril revealing its typical striated appearance. ER, Endoplasmic reticulum. (A, From Alberts B, Johnson A, Lewis J, et al [eds]: Molecular biology of the cell, ed 4, New York, 2002, Garland, p 1100; B, Courtesy Robert Horne.)
A
B
Self-assemblyinto fibril
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles140
This binding allows proteoglycans to regulate proteins by (1) immobilizing the protein and restricting its range of action, (2) providing a reservoir of the protein for delayed release, (3) altering the protein to allow more effective presentation to cell surface receptors, (4) prolonging the action of the protein by protecting it from degradation, or (5) blocking the activity of the protein.
Proteoglycans can be components of plasma membranes and have a transmembrane core protein or are attached to the lipid bilayer by a glycosylphosphatidylinositol anchor. These proteogly-cans act as coreceptors that work with other cell surface receptor proteins in binding cells to the ECM and initiating the response of cells to extracellular signaling proteins. For example, the syn-decans are transmembrane proteoglycans located on the surface of many cells, including fibroblasts and epithelial cells. In fibro-blasts, syndecans are found in focal adhesions, where they interact with fibronectin on the cell surface and with cytoskeletal and signaling proteins inside the cell. Mutations leading to inactiva-tion of these coreceptor proteoglycans result in severe develop-mental defects.
The ECM has other noncollagen proteins, such as the fibro-nectins, that have multiple domains and can bind to other matrix macromolecules and cell surface receptors. These interactions help organize the matrix and facilitate cell attachment. Fibronectin is important in animal embryogenesis.
Fibronectin exists as soluble and fibrillar isoforms. Soluble plasma fibronectin circulates in various body fluids and enhances blood clotting, wound healing, and phagocytosis. The highly insoluble fibrillar forms assemble on cell surfaces and are depos-ited in the ECM. The fibronectin fibrils that form on the surface of fibroblasts are usually coupled with neighboring intracellular actin stress fibers. The actin filaments promote assembly of the fibronectin fibril and influence fibril orientation. Integrin trans-membrane adhesion proteins mediate these interactions. The con-tractile actin and myosin cytoskeleton pulls on the fibronectin matrix and generates tension.
Basal lamina. Basal laminae are flexible, thin (40 to 120 nm) mats of specialized ECM that separate cells and epithelia from the underlying or surrounding connective tissue. In skin, the basal lamina is tethered to the underlying connective tissue by special-ized anchoring fibrils. This composite of basal lamina and collagen is the basement membrane.
The basal lamina acts in numerous ways: (1) as a molecular filter to prevent the passage of macromolecules (i.e., in the kidney glomerulus), (2) as a selective barrier to certain cells (i.e., the lamina beneath the epithelium prevents fibroblasts from contact-ing epithelial cells but does not stop macrophages or lympho-cytes), (3) as a scaffold for regenerating cells to migrate, and (4) as an important element in tissue regeneration in locations where the basal lamina survives.
Although composition may vary from tissue to tissue, most mature basal laminae contain type IV collagen, perlecan, and the glycoproteins laminin and nidogen. Type IV collagen has a more flexible structure than the fibrillar collagens; its triple-stranded helix is interrupted, allowing multiple bends.
Laminins generally consist of three long polypeptide chains (α, β, and γ). Mice lacking the laminin γ1 chain die during embryo-genesis because they cannot make a basal lamina. The laminin in basement membranes consists of several domains that bind to perlecan, nidogen, and laminin receptor proteins found on cell surfaces. The type IV collagen and laminin networks are con-nected by nidogen and perlecan, which act as stabilizing bridges. Many of the cell surface receptors for type IV collagen and laminin
because of the hydrophobic nature of elastin, which makes the interior of this highly folded protein inaccessible. As a result of this high degree of three-dimensionality and extensive cross linking, cleavage must be considerable before there is much loss of elasticity. IGF-I and TGF-β stimulate the production of elastin. Glucocorticoids and basic FGF reduce production of elastin in adult skin cells.
Mutations causing a deficiency of elastin protein result in arte-rial narrowing as a consequence of excessive smooth muscle cell proliferation in the arterial wall (intimal hyperplasia). These find-ings suggest that the normal elasticity of an artery is needed to prevent proliferation of these cells. Gene mutations in fibrillin result in Marfan syndrome; severely affected individuals are prone to aortic rupture.
Glycosaminoglycans and proteoglycans. GAGs are un-branched polysaccharide chains composed of repeating disaccha-ride units, a sulfated amino sugar (N-acetylglucosamine or N-acetylgalactosamine) and uronic acid (glucuronic or iduronic). GAGs are highly negatively charged because of the sulfate or carboxyl groups on most of their sugars. Four types of GAGs exist: (1) hyaluronan, (2) chondroitin sulfate and dermatan sulfate, (3) heparan sulfate, and (4) keratan sulfate.
GAGs in connective tissue usually constitute less than 10% of the weight of fibrous proteins. Their highly negative charge attracts osmotically active cations, such as Na+, which causes large amounts of water to be incorporated into the matrix. This results in porous hydrated gels and is responsible for the turgor that enables the matrix to withstand compressive force.
Hyaluronan is the simplest GAG. It is composed of repeating nonsulfated disaccharide units and is found in adult tissues, but it is especially prevalent in fetal tissues. Its abundance in fetal wounds is believed to be a factor in the scarless wound healing seen in fetal tissues. In contrast to the other GAGs, hyaluronan is not covalently attached to any protein and is synthesized directly from the cell surface by an enzyme complex embedded in the plasma membrane.
Hyaluronan plays several different roles because of its large hydration shell. It is produced in large quantities during wound healing, during which it facilitates cell migration by physically expanding the ECM and allowing cells additional space for migra-tion; it also reduces the strength of adhesion of migrating cells to matrix fibers. Hyaluronan synthesized from the basal side of epi-thelium creates a cell-free space for cell migration, such as during embryogenesis and formation of the heart and other organs. When cell migration is finished, the excess hyaluronan is degraded by hyaluronidase. Studies using hyaluronic acid derivative have suggested that these derivatives can accelerate wound healing in burns, surgical wounds, and chronic wounds.4
Proteoglycans are a diverse group of glycoproteins with func-tions mediated by their core proteins and GAG chains. The number and types of GAGs attached to the core protein can vary greatly, and the GAGs themselves can be modified by sulfonation. Because of their GAGs, proteoglycans provide hydrated space around and between cells. They also form gels of different pore size and charge density to regulate the movement of cells and molecules. Perlecan, a heparan sulfate proteoglycan, plays this role in the basal lamina of the kidney glomerulus. Decreased levels of perlecan are believed to play a role in diabetic albuminuria.
Proteoglycans function in chemical signaling by binding various secreted signal molecules, such as growth factors, and modulating their signaling activity. Proteoglycans also can bind other secreted proteins, such as proteases and protease inhibitors.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 141
Stimulated fibroblasts, or myofibroblasts, are found to be a constant feature present in abundance in diseases involving exces-sive fibrosis, including hepatic cirrhosis, renal and pulmonary fibrosis, Dupuytren’s contracture, and desmoplastic reactions induced by neoplasia. The actin microfilaments are arranged lin-early along the long axis of the fibroblast. They are associated with dense bodies that allow attachment to the surrounding ECM. Fibronexus is the attachment entity that connects the cytoskeleton to the ECM and spans the cell membrane in doing so.
MMPs also appear to be important for wound contraction. It has been demonstrated that stromelysin-1 (MMP-3) strongly affects wound contraction. MMPs may be necessary to allow cleavage of the attachment between the fibroblast and the collagen so that the lattice can be made to contract. Different populations of fibroblasts, from different organs, respond to the contraction stimulus in a heterogeneous fashion. It is likely that the stromelysin-1, with the participation of β1 integrins, allows modification of attachment sites between fibroblasts and the col-lagen fibrils. Similarly, cytokines such as TGF-β1 affect contrac-tion by increasing the expression of β1 integrin.
RemodelingThe fibroblast population decreases, and the dense capillary network regresses. Wound strength increases rapidly within 1 to 6 weeks and then appears to plateau up to 1 year after the injury (see Fig. 6-5). Compared with nonwounded skin, tensile strength is only 30% in the scar. An increase in breaking strength occurs after approximately 21 days, mostly as a result of cross linking. Although collagen cross linking causes further wound contraction and an increase in strength, it also results in a scar that is more brittle and less elastic than normal skin. In contrast to normal skin, the epidermodermal interface in a healed wound is devoid of rete pegs, the undulating projections of epidermis that pene-trate into the papillary dermis. Loss of this anchorage results in increased fragility and predisposes the neoepidermis to avulsion after minor trauma.
ABNORMAL WOUND HEALINGIn such a complex series of interweaving events as wound healing, many factors can impede the outcome (Box 6-1). The amount of tissue lost or damaged, amount of foreign material or bacterial inoculation, and length of exposure to toxic factors can affect the time to recovery. Intrinsic factors such as age, chemotherapeutic agents, atherosclerosis, cardiac or renal failure, and location on the body all affect wound healing. Ultimately, the type of scar—whether it is adequate, inadequate, or proliferative—is dictated by the amount of collagen deposition and balanced by the amount of collagen degradation. If the balance is tipped in either direc-tion, the result is poor.
Hypertrophic Scars and KeloidsKeloids and hypertrophic scars are proliferative scars characterized by excessive net collagen deposition (Fig. 6-6). Keloids, by defini-tion, grow beyond the borders of the original wounds and rarely regress with time; they are more prevalent in darkly pigmented skin, developing in 15% to 20% of African Americans, Asians, and Hispanics. There is strong evidence suggesting a genetic sus-ceptibility, including familial heritability, common occurrence in twins, and high prevalence in certain ethnic populations. Shih and Bayat5 suggest a strong multigenetic disposition to keloid
are members of the integrin family. Another important type of laminin receptor is dystroglycan, a transmembrane protein that together with integrins may organize assembly of the basal lamina.
Degradation of the extracellular matrix. Regulated turnover of the ECM is crucial to many biologic processes. ECM degradation occurs during metastasis when neoplastic cells migrate from their site of origin to distant organs via the bloodstream or lymphatics. In injury or infection, localized degradation of the ECM occurs so that cells can migrate across the basal lamina to reach the site of injury or infection. Locally secreted cellular proteases, such as MMPs or serine proteases, degrade the ECM components. Matrix proteolysis helps the cell migrate by (1) clearing a path through the matrix; (2) exposing binding sites, promoting cell binding or migration; (3) facilitating cell detachment so that a cell can move forward; and (4) releasing signal proteins that promote cell migration.
Proteolysis is tightly regulated. Many proteases are secreted as inactive precursors that are activated when required. In addition, cell surface receptors bind these proteases to ensure that they act only on sites where they are needed. Finally, protease inhibitors, such as tissue inhibitors of metalloproteinase (TIMP), can bind these enzymes and block their activity.
Maturational PhaseWound contraction occurs by centripetal movement of the whole thickness of the surrounding skin and reduces the amount of disorganized scar. In contrast, wound contracture is a physical constriction or limitation of function and is a result of the process of wound contraction. Contractures occur when excessive scar exceeds normal wound contraction, and it results in a functional disability. Examples of contractures are scars that traverse joints and prevent extension and scars that involve the eyelid or mouth and cause an ectropion.
Wound contraction appears to take place as a result of a complex interaction of the extracellular materials and fibroblasts that is not completely understood. Using a fibroblast-populated collagen lattice, Ehrlich demonstrated that aborted cell locomo-tion appears to cause bunching and contraction of the collagen fibers. In this in vitro model, trypsinized collagen is populated by fibroblasts that adhere to it in culture. If normal dermal fibroblasts are cultured, they attempt to move but are trapped by the collagen fibers. The tractional forces cause the lattice to bunch and contract.
Numerous studies have shown that fibroblasts in a contracting wound undergo change to stimulated cells, termed myofibroblasts. These cells have function and structure in common with fibroblasts and smooth muscle cells and express alpha smooth muscle actin in bundles termed stress fibers. The actin appears at day 6 after wounding, persists at high levels for 15 days, and is gone by 4 weeks, when the cell undergoes apoptosis. It appears that a stimulated fibroblast develops contractile ability related to the formation of cytoplasmic actin-myosin complexes. When this stimulated cell is placed in the fibroblast-populated collagen lattice, contraction occurs even more quickly. The tension that is exerted by the fibroblasts’ attempt at contraction appears to stimu-late the actin-myosin structures in their cytoplasm. If colchicine, which inhibits microtubules, or cytochalasin D, which inhibits microfilaments, is added to the tissue culture, the result is minimal contraction of the collagen gels. Fibroblasts develop a linear arrangement in the line of tension that, when removed, causes the cells to round up.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles142
human dermal fibroblasts. Hypertrophic scar fibroblasts produce more TGF-β1. In addition, in these scars, collagen synthesis is elevated, whereas collagen degradation is low. MMPs are also affected in these scars: MMP-1 (collagenase) and MMP-9 (gela-tinase, early tissue repair) are decreased, whereas MMP-2 (gelati-nase, late tissue remodeling) is significantly elevated. Blocking TGF-β activity with antibodies decreases scar fibrosis. Growth factors have also been implicated in fibrosis and have been studied as targets for the blockade of fibrosis. IFN-γ, which suppresses collagen synthesis, has been tested clinically in keloid scars and has produced an average 30% reduction in scar thickness.
Prevention of Hypertrophic or Keloid ScarsThe three strategies that reduce adverse scarring immediately after wound closure are tension relief, hydration/occlusion, and use of taping/pressure garments. Wounds with greater tension (perpen-dicular to Langer’s lines), with excessive tension on closure, and in certain anatomic locations (deltoid and sternal) are at a higher risk of adverse scarring. Scarring can be reduced by postsurgical taping of the wound for 3 months. Moisturizing lotions and moisture-retentive dressings (silicone sheets and gels) can reduce the thickness, discomfort, and itching and improve the appear-ance of the scar. After wound healing, water still evaporates more rapidly through scar tissue and may take more than a year to recover to prewound levels. Silicone products may ameliorate evaporative losses and assist hydration of the stratum corneum. These strategies need to be employed soon after initial wound healing. Pressure garments should be used prophylactically in wounds that are wide (e.g., burns); these wounds may take more than 2 or 3 weeks to heal. Garments should be applied as soon as the wound is closed and the patient can tolerate the pressure.7 Avoidance of sun exposure and use of SPF 50+ sunscreens for 1 year postoperatively reduces scar hyperpigmentation and improves clinical appearance.
Linear Hypertrophic ScarsEarly linear scar hypertrophy (e.g., after trauma or surgery) at 6 weeks to 3 months should be treated with pressure therapy. After 6 months, silicone therapy should be continued for as long as necessary if there is further scar maturation. Ongoing hypertrophy may be treated with intralesional corticosteroids (triamcinolone acetonide, 10 to 40 mg/mL) injected into the papillary dermis every 2 to 4 weeks until flat.8 This is the only invasive
formation with a varied inheritance pattern that is predominantly autosomal dominant. Proposed pathways include apoptosis, mitogen-activated protein kinase, TGF-β, IL-6, and plasminogen activator inhibitor-1.
Keloids occur above the clavicles, on the trunk, on the upper extremities, and on the face. They cannot be prevented and are frequently refractory to medical and surgical intervention. Hyper-trophic scars are raised scars within the confines of the original wound and frequently regress spontaneously.
Keloids and hypertrophic scars differ histologically from normal scars. Hypertrophic scars primarily contain well-organized type III collagen, whereas keloids contain disorganized type I and type III collagen bundles.6 Keloids and hypertrophic scars have stretched collagen bundles aligned in the same plane as the epi-dermis, whereas collagen bundles are randomly arrayed and relaxed in normal scars. Keloid scars have thicker, abundant col-lagen bundles that form acellular nodelike structures in the deep dermis with a paucity of cells centrally. Hypertrophic scars, in contrast, contain islands composed of aggregates of fibroblasts, small vessels, and collagen fibers throughout the dermis.5
Hypertrophic scars are often preventable. Prolonged inflamma-tion and insufficient resurfacing, (e.g., burn wounds) promote hypertrophic scarring. Scars perpendicular to the underlying muscle fibers tend to be flatter and narrower, with less collagen formation than when they are parallel to the underlying muscle fibers. Tension appears to signal the formation of activated fibro-blasts resulting in excessive collagen deposition. The position of an elective scar can be chosen to induce a narrower, less obvious healed scar. As muscle fibers contract, the wound edges become reapproximated when they are perpendicular to the underlying muscle and tend to gape if placed parallel to it, leading to greater wound tension and scar formation.
Hypertrophic scars represent a reversible hyperproliferative scar phenotype that regresses when the original stimulus (skin tension, stimulatory growth factors) are removed. Keloids appear to be genetically predisposed and switched on irreversibly by factors such as TGF-β. Expression of the isoforms TGF-β1 and TGF-β2 is increased in human keloid cells compared with normal
InfectionIschemia
CirculationRespirationLocal tension
Diabetes mellitusIonizing radiationAdvanced ageMalnutritionVitamin deficiencies
Vitamin CVitamin A
Mineral deficienciesZincIron
Exogenous drugsDoxorubicin (Adriamycin)Glucocorticosteroids
BOX 6-1 Factors That Inhibit Wound Healing
FIGURE 6-6 Keloids caused by ear piercing.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 143
review of the literature, Ogawa and colleagues13 concluded that the risk of malignancy attributable to keloid radiation therapy is minimal. An additional promising new invasive treatment modal-ity is internal cryotherapy, in which a metal rod is introduced into the keloid and the subsequent extreme cooling leads to tissue necrosis; one study demonstrated a 54% reduction in scar volume without recurrence. Finally, imiquimod 5%, a topical immuno-modulator that stimulates interferon production to increase col-lagen degradation, has been shown, in combination with surgical excision, to result in low keloid recurrence rates (0 to 29%) in some studies but high recurrence rates (89%) in others.14
Although existing strategies for the management of hypertro-phic scars and keloids are broadly similar, the histologic differ-ences between the two scars suggest that, in the future, therapeutic approaches could be developed that are specifically tailored for these different types of scars. However, at the present time, there is no single proven best therapy for the management of these excessive healing scars, and the large number of treatment options reflects this (Table 6-3).8
Chronic Nonhealing WoundsBy definition, chronic wounds are wounds that have failed to proceed through an orderly and timely reparative process to produce anatomic and functional integrity over a period of 3 months. In the United States, it is estimated that 2 to 3 million patients per year are at risk of developing diabetic ulcers, 600,000 patients per year develop chronic leg ulcers secondary to venous insufficiency, and 1 to 3 million patients per year develop pressure ulcers secondary to immobility. These numbers are likely to increase as a result of an aging population and the rising incidence of risk factors for atherosclerotic disease, such as diabetes mellitus and smoking. These wounds are a significant challenge to health care professionals and an immense burden on health care systems and the economy. Patients also report reduced quality of life and social isolation.
Numerous common factors promote adverse wound healing conditions (see Fig. 6-1). Systemic factors, such as malnutrition, aging, tissue hypoxia, and diabetes, contribute significantly to the pathogenesis of chronic wounds. A combination of systemic and localized adverse wound factors collectively overwhelm the normal healing processes, resulting in a hostile wound healing environ-ment (Fig. 6-7).15
Chronic wounds do not occur in animals, and understanding of chronic wounds has come from human studies limited to observation, biopsy, and wound exudate analyses. Chronic wounds have derangements in the various stages of wound healing and have unusually elevated or depressed levels of cytokines, growth factors, or proteinases. Chronic wound fluid, in contrast to acute wound fluid, has been shown to have greater levels of IL-1, IL-6, and TNF-α; levels of these proinflammatory cytokines decreased as the wound healed. An inverse relationship between TNF-α and essential growth factors, such as EGF and PDGF, has been demonstrated.
Chronic wounds typically exhibit powerful proinflammatory stimuli, including bacterial colonization, necrotic tissue, foreign bodies, and localized tissue hypoxia. Tissue edema is significant, and the distance between capillaries is increased, reducing oxygen diffusion to individual cells. Chronic wounds typically have high bacterial counts, which stimulates an inflammatory host response with PMNs expressing reactive oxygen species and proteases resulting in a highly pro-oxidant environment. Disturbed oxidant balance is the likely key factor in the amplification and persistence
management option that has enough supporting evidence to be recommended in evidence-based guidelines. Approximately 50% to 100% of patients respond, and 9% to 50% experience recur-rence.8 Adverse steroid effects include skin atrophy, hypopigmen-tation, telangiectasias,8 and excessive pain during injections. Injections should be limited to the scar itself to minimize adjacent fat atrophy.
Surgical scar revision may be considered for permanent linear hypertrophic scars present after 1 year.9 Simple resection and primary closure may be combined with adjacent tissue undermin-ing, subcutaneous sutures, adjunctive Z-plasty, and postsurgical taping and silicone therapy.
Hypertrophic scars also can be seen in conjunction with a scar contracture. Scar contractures are abnormal shortening of non-matured scars resulting in functional impairment, particularly if the scar is across a joint. Correction of a scar contracture generally requires surgery with Z-plasty, skin graft, or flap to release tension in the scar to restore function and reduce scar hypertrophy.
Widespread Hypertrophic ScarsSevere burns, mechanical trauma, necrotizing infections, wounds requiring more than 2 to 3 weeks to heal, or wounds healed with skin grafting require early application of silicone and compression therapy.7 This therapy should be initiated as soon as the wound is closed and the patient can tolerate the pressure.
The mechanism of action of pressure therapy is poorly under-stood but may involve reduction of wound oxygen tension by occlusion of small blood vessels resulting in a decrease of myofi-broblast proliferation and collagen synthesis. Pressure therapy is believed to act on cellular mechanoreceptors that are involved in cellular apoptosis and linked to the ECM. The increased pressure regulates apoptosis of dermal fibroblasts and diminishes hypertro-phic scarring. In addition, sensory nerve cells transduce mechani-cal pressure into intracellular biochemical and gene expression, synthesizing and releasing different cytokines involved in the physiopathogenesis of proliferative scarring.10
Pressure and silicone therapy should be continued or intensi-fied and combined with selective localized corticosteroid injec-tions in resistant areas. Bleomycin, 5-fluorouracil, and verapamil have been used as adjuncts to corticosteroid therapy.11 Laser therapy, although invasive, is another potentially useful adjunct to reduce scar thickness; resurface scar texture; and treat residual redness, telangiectasias, or hyperpigmentation.
Early surgery is indicated for functional impairment. Burn scar contracture release procedures in the neck and axilla are best performed with flaps to improve functional and cosmetic out-comes further that may not be achievable with skin grafts. Wide-spread large hypertrophic scars may require serial excision or tissue expansion.
KeloidsFirst-line treatments include silicones in combination with pres-sure therapy and intralesional corticosteroid injections. Intrale-sional 5-fluorouracil, bleomycin, and verapamil should be used in accordance with established treatment protocols.8 Refractory cases after 12 months of therapy should be considered for surgical exci-sion in combination with adjuvant therapy. Excision alone results in a high recurrence rate of 50% to 100% and enlargement of the keloid.8 Immediate postoperative electron beam irradiation or brachytherapy with iridium-192 reduces recurrence rates12 but may hypothetically be associated with radiation damage to adja-cent tissues or induction of malignancy. However, in an extensive
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles144
of the inflammatory state in chronic wounds. In addition to direct cell membrane and ECM protein damage, PMN-derived reactive oxygen species, such as superoxide, hydroxyl radicals, and hydro-gen peroxide, can selectively activate signaling pathways leading to activation of transcription factors that control expression of proinflammatory chemokines and cytokines such as IL-1, IL-6,
TNF-α, and proteolytic enzymes such as MMPs and serine pro-teases. Bacterial components, including formyl methionyl pep-tides and extracellular adherence proteins, may also contribute to the upregulation of the inflammatory response.
The amount of normal wound ECM is determined by a dynamic balance among overall matrix synthesis, deposition, and
NA, Not available.
TABLE 6-3 Prevention and Treatment Options for Keloids and Hypertrophic Scars
MODALITY OR TREATMENT OPTION
RESPONSE RATE (%)
RECURRENCE RATE (%) COMMENTS STUDY DESIGN
PreventionPreventive silicone sheeting (postsurgery) 0-75 25-36 Multiple preparations available; tolerated by
children; expensive; avoid on open wounds; poor study design
Review of multiple case studies
Postsurgical intralesional corticosteroid injection (triamcinolone acetonide [Kenalog], 10-40 mg/mL at 6-wk intervals)
NA 0-100 (mean, 50) Patient acceptance and safety; may cause hypopigmentation, skin atrophy, telangiectasia
Review of multiple case studies
Postsurgical topical imiquimod, 5% cream (Aldara)
NA 28 May cause hyperpigmentation, irritation Case study
Postsurgical fluorouracil, triamcinolone acetonide, and pulsed dye lasers (best outcomes)
70 at 12 wk NA Effective; may cause hyperpigmentation, wound ulceration
Clinical trial
First-Line TreatmentCryotherapy 50-76 NA Useful on small lesions; easy to perform; may
cause hypopigmentation, painReview of multiple
case studiesIntralesional corticosteroid injection
(triamcinolone acetonide [Kenalog], 10-40 mg/mL at 6-wk intervals)
50-100 9-50 Inexpensive, requires multiple injections; may cause discomfort, skin atrophy, telangiectasia
Review of multiple case studies
Silicone elastomer sheeting 50-100 NA Multiple preparations available; tolerated by children; expensive; poor study design
Review of multiple case studies
Pressure dressing (24-30 mm Hg) worn for 6-12 mo
90-100 NA Inexpensive; difficult schedule; poor adherence Review of multiple case studies
Surgical excision NA 50-100 Z-plasty option for burns; immediate postsurgical treatment needed to prevent regrowth
Review of multiple case studies
Combined cryotherapy and intralesional corticosteroid injection
84 NA See benefits of individual treatments; may cause hypopigmentation
Case study
Triple-keloid therapy (surgery, corticosteroids, silicone sheeting)
88 at 13 mo 12.5 at 13 mo Tedious; time-intensive; expensive Case study
Pulsed dye laser NA NA Specialist referral needed; expensive; variable results depending on trial (controversial)
Case studies
Second-Line and Alternative TreatmentVerapamil, 2.5 mg/mL, intralesional
injection combined with perilesional excision and silicone sheeting
54 at 18 mo NA Repeated injections; limited experience; may cause discomfort
Clinical trial
Fluorouracil, 50 mg/mL, intralesional injection 2-3 times/wk
88 0 Effective; may cause hyperpigmentation, wound ulceration
Review of multiple case studies
Bleomycin tattooing, 1.5 IU/mL 92, 88 NA Effective; may cause pulmonary fibrosis, cutaneous reactions
Review of case study; control trial
Postsurgical interferon-α2b, 1.5 million IU, intralesional injection bid for 4 days
30-50 8-19 Expensive; may cause pruritus, altered pigmentation, pain
Review of multiple case studies
Radiation therapy alone 56 (mean) NA Local growth inhibition; may cause cancer, hyperpigmentation, paresthesias
Review of multiple case studies
Postsurgical radiation therapy 76 NA Local growth inhibition; may cause cancer Review of multiple case studies
Onion extract topical gels (Mederma) NA NA Limited effect alone, better in combination with silicone sheeting
Prospective case study
Adapted from Juckett G, Hartman-Adams H: Management of keloids and hypertrophic scars. Am Fam Physician 80:253–260, 2009.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 145
expression, resulting in a relative excess of MMP activity. For example, α1-proteinase inhibitor, α2-macroglobulin, and compo-nents of the ECM, such as fibronectin and vibronectin, are down-graded or inactivated within chronic wounds. Growth factors, such as PDGF and VEGF, are also targeted when there is excess protease activity.
Shih and colleagues16 demonstrated that genes such as insulin-like growth factor binding protein 2, collagen type XI alpha 1, inhibin beta A (INHBA), and thrombospondin 1 (THBS1) are dysregulated in chronic wounds. They found INHBA and THBS1 upregulation to be characteristic biomarkers of senescent wounds or wounds that overexpress TGF-β. Both result in significant delays in wound healing.16
degradation. A defining feature of chronic wounds is unbalanced activity, which overwhelms tissue protective mechanisms. Although activated keratinocytes, fibroblasts, and endothelial cells have been shown to increase expression of proteases, incoming neutrophils and macrophages are considered to be the source of proteases, particularly cathepsin G, urokinase-type plasminogen activator, and neutrophil elastase. The expression and activity of gelatinases (MMP-2, MMP-9), collagenases (MMP-1, MMP-8), stromelysins (MMP-3, MMP-10, MMP-11), and membrane-type MMP (MT1-MMP) are upregulated in chronic venous ulcers.
Proinflammatory cytokines are potent inducers of MMP expression in chronic wounds, while also reducing TIMP
FIGURE 6-7 Mechanisms involved in the development and persistence of chronic wounds. Chronic wounds do not adequately complete the “normal” phases of wound healing. A state of chronic inflammation develops as many of the cells recruited to the wound in the proliferative phase of healing adopt a proinflammatory secretory profile. Inflammatory cells, particularly neutrophils and macrophages (M1 phenotype > M2 pheno-type), persist in the wound, creating a highly pro-oxidant, protease-rich environment with an abundance of proinflammatory cytokines such as interleukin-1 (IL-1), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α). The result is a hostile environment with downregulation of protease inhibitors and direct damage to extracellular matrix (ECM), cellular components, and protective growth factors such as platelet-derived growth factor (PDGF) and vascular endothelial growth factor (VEGF). Reactive oxygen species and proteases, such as matrix metalloproteinases (MMP 1, 2, 3, 9, 13), are the most significant deleterious influences. Solid lines indicate upregulation, and dashed lines indicate downregulation. Width of the line is proportional to the effect of the influence. H2O2, Hydrogen peroxide; O2
−, superoxide; TGF-β, transforming growth factor-β. (From Greaves NS, Iqbal SA, Baguneid M, et al: The role of skin substitutes in the management of chronic cutane-ous wounds. Wound Repair Regen 21:194–210, 2013.)
↑ Proteases
MMP 1, 2, 3, 9, 13serine proteases
PDGFVEGF
IL-1αIL-6
TGF-βVEGF
IL-1PDGFTNF-α
O2–, H2O2, etc
↓ Protease inhibitors
Extravasation
Bacterial components
Endothelial cells
Fibroblasts
Neutrophils and macrophages
↑ Reactiveoxygen species
Cell damageand debris
ECM damage(e.g., fibronectin,
vibronectin)
M2 > M1
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles146
tension prevents adequate local tissue perfusion. Under hypoxic conditions, energy derived from glycolysis may be sufficient to initiate collagen synthesis, but the presence of molecular oxygen is critical for post-translational hydroxylation of the prolyl and lysyl residues required for triple-helix formation and cross linking of collagen fibrils. Although mild hypoxia stimulates angiogenesis, this essential step in collagen fibril assembly proceeds poorly when partial pressure of oxygen (PO2) becomes less than 40 mm Hg. Optimal PO2 for collagen synthesis may be present at the periph-ery of the wound, but the center may remain hypoxic.
The role of anemia in wound healing has long been attributed to be predominantly secondary to hypoperfusion. However, studies evaluating colonic anastomoses in a crystalloid-resuscitated hemorrhagic shock model demonstrated altered histologic parameters—decreased white blood cell infiltration, angiogenesis, fibroblast production, and collagen production, all contributing to delayed wound healing.
Tobacco smoking and consumption of tobacco products causes peripheral vasoconstriction and a 30% to 40% reduction in wound blood flow. Elevated levels of serum carbon monoxide inhibit enzyme systems necessary for oxidative cellular metabo-lism. Nicotine also inhibits platelet prostacyclin, promoting plate-let adhesiveness, thrombotic microvascular occlusion, and tissue ischemia. Tobacco use inhibits endothelial cell and fibroblast function, NO synthase activity, VEGF production, fibroblast pro-liferation, collagen synthesis, and vitamin C levels.17 Studies in animals suggested that nicotine cessation for 14 days before flap surgery resulted in similar outcomes to controls, although most clinicians recommend complete smoking cessation in human patients for 4 to 6 weeks before elective procedures.
DiabetesDiabetes mellitus impairs wound healing in several ways. Diabetes-associated large vessel occlusion and end-organ microangiopathy each lead to tissue ischemia and infection. Diabetic sensory neu-ropathy leads to repeated trauma and unrelieved wound pressure. Tissue hypoxia can be demonstrated by reduced dorsal foot trans-cutaneous oxygen tension (TcO2). The thickened capillary base-ment membrane decreases perfusion in the microenvironment, and elevated perivascular localization of albumin suggests increased capillary leak.
VEGF upregulation in patients with diabetes is also impaired.18 Hypoxia is normally a potent upregulator of VEGF, but cells from patients with diabetes do not upregulate VEGF expression in response to hypoxia. Diabetic animals are unable to increase VEGF production after soft tissue ischemia18 because of deficient transactivation by the transcription factor HIF-1α. HIF-1α medi-ates hypoxia-stimulated VEGF expression. With high glucose levels, decreased binding of HIF-1α to its coactivator p300 resulted in decreased HIF-1α functional activity. Covalent binding of the dicarbonyl metabolite methylglyoxal to p300 resulted in modifi-cation of p300 and was responsible for the decreased association of HIF-1α and p300. Administration of deferoxamine, an inhibi-tor of methylglyoxal conjugation, to diabetic mice resulted in normalization of HIF-1α–p300 interaction and transactivation of HIF-1α, with increased neovascularization and enhanced wound healing.
Sensory neuropathy in patients with diabetes predisposes them to repeated trauma. They are susceptible to infection because of an attenuated inflammatory response, impaired chemotaxis, and inefficient bacterial killing. Infection further increases local tissue metabolism, placing an additional burden on the tenuous blood
Other proposed causes for wound chronicity include keratino-cyte hyperproliferation at the periphery resulting in inhibition of fibroblast and keratinocyte migration and apoptosis. Fibroblasts have altered morphologies, slower rates of proliferation, and less responsiveness to applied growth factors. The CD4/CD8 cell ratio is significantly lower in chronic wounds and is likely to be impor-tant in the pathogenesis of diabetic ulcers. Finally, chronic wounds have reduced levels of important growth factors (FGF, EGF, and TGF-β) likely secondary to degradation by excessive proteases or trapping by ECM molecules.
Chronically inflamed wounds are susceptible to neoplastic transformation. Squamous cell carcinoma (Fig. 6-8) was originally reported in chronic burn scars by Marjolin. Chronic osteomyeli-tis, pressure sores, venous stasis ulcers, and hidradenitis may also develop neoplastic change. Biopsies should be performed in cases of chronic wounds that appear clinically atypical. Cutaneous wounds may first exhibit pseudoepitheliomatous hyperplasia—a premalignant condition. Such a diagnosis on biopsy should prompt additional biopsies to exclude squamous cell carcinoma, which may already be present in other areas of the wound.
InfectionWound infection is the most common cause of healing delays. Bacterial counts exceeding 105 organisms per gram of tissue obtained by quantitative biopsy or the presence of virulent organ-isms, typically beta-hemolytic streptococci, would prevent wounds from healing by any means, including flap closure, skin graft placement, or primary suture. Bacterial infection prolongs the inflammatory phase and interferes with epithelialization, wound contraction, and collagen deposition. Bacterial endotoxins stimu-late phagocytosis and release of collagenase, which degrades col-lagen and promotes destruction of surrounding normal tissue. Mechanical and antibiotic treatment is required to decrease the bacterial count, reduce inflammation, and allow wound closure to occur.
Other Causes of Abnormal Wound HealingHypoxiaMolecular oxygen is essential for collagen formation. Ischemia secondary to cardiac failure, arterial disease, or simple wound
FIGURE 6-8 Squamous cell carcinoma in a chronic pressure sore.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 147
partial pressure in the treatment of osteoradionecrosis22-24 via increased capillary density and more complete neovascularization. Hyperbaric treatment of cell cultures resulted in the downregula-tion of nine genes involved in adhesion, angiogenesis, inflamma-tion, and oxidative stress.25 IL-8 mRNA levels were suppressed in endothelial cells with daily HBO therapy.25 HBO therapy is used clinically in patients with chronic diabetic ulcers and wound-healing complications after radiotherapy, and randomized clinical trials demonstrated efficacy when HBO therapy was used in con-junction with standard wound care in cases of recalcitrant, dia-betic, and radiation-induced wounds.26
AgingOlder patients are more likely to experience delayed healing and surgical wound dehiscence. The aging epidermis has fewer Lang-erhans cells and melanocytes and flattening of the dermal-epidermal junction. Keratinocyte proliferation is reduced, and the turnover time is increased by 50%. The dermis has fewer fibro-blasts, macrophages, and mast cells; reduced vascularity; and less collagen and GAGs. There is a quantitative imbalance between collagen production and degradation and a qualitative alteration of the remaining collagen, which has fewer ropelike bundles and shows greater disorganization. Skin elasticity is decreased because of altered elastin morphology. Diminished light touch and pres-sure reduced nociceptive receptors and dermal atrophy increase susceptibility to injury by mechanical forces. Immunosenescence (reduced Langerhans cells and fibroblast activity) impairs wound healing and increases the likelihood of chronic wounds. Micro-vascular disturbances predispose to ischemic ulcers. Finally, there is reduced sebum secretion and vitamin D3 production.27
MMP-2 and MMP-9 are upregulated after experimental wounding in healthy elderly subjects versus younger controls. Decreased reepithelialization, depressed collagen synthesis, im-paired angiogenesis, and decreased growth factors (especially proangiogenic FGF-2 and VEGF) are seen in studies of older animals. The early inflammatory phase appears to be altered in older adults. Impaired macrophage activity (reduced phagocytosis and delayed infiltration) and impaired B lymphocyte activity also have been demonstrated in animal studies. Decreased MMP ac-tivation and decreased TGF-β1 receptor expression in response to hypoxia were demonstrated in keratinocytes isolated from aged donors.
supply, amplifying the risk for tissue necrosis. Lymphocyte and leukocyte function are impaired. Collagen degradation is increased, whereas collagen deposition is impaired. Collagen is brittle sec-ondary to glycosylation in the ECM. In addition, collagen glyca-tion diminishes focal adhesion formation between fibroblast and matrix resulting in decreased fibroblast migration.
Hyperglycemia causes increased advanced glycation end-products, which induce the production of inflammatory mole-cules (TNF-α, IL-1) and interfere with collagen synthesis. High glucose exposure also results in changes in cellular morphology, decreased proliferation, and abnormal differentiation of keratino-cytes. Decreased chemotaxis, phagocytosis, bacterial killing, and reduced heat shock protein expression impair the early phase of wound healing in patients with diabetes. Altered leukocyte infil-tration and wound fluid IL-6 characterize the late inflammatory phases of wound healing in these patients. Growth factors are abnormally expressed, degraded rapidly in wound fluids as a result of increased insulin degrading enzyme activity. Insulin degrading enzyme activity in wound fluid is positively correlated with hemo-globin A1c levels. Elevated MMP and reduced TIMP levels are seen in diabetic wounds in a pattern similar to chronic wounds. Finally, there is increasing evidence that resident cells in chronic wounds undergo phenotypic changes that render them senescent and impair their capacity for proliferation and movement.
Ionizing RadiationIonizing radiation has its greatest effect on rapidly dividing cells in phases G2 through M of the cell cycle. Injury to keratinocytes and fibroblasts impairs epithelialization and formation of granula-tion tissue during wound healing. Radiation injury in endothelial cells results in endarteritis, atrophy, fibrosis, and delayed tissue repair. Repetitive radiation injury results in repetitive inflamma-tory responses and ongoing cellular regeneration. Early side effects include erythema, dry desquamation, skin hyperpigmentation, and local hair loss. Late effects include skin atrophy, dryness, telangiectasia, dyschromia, dyspigmentation, fibrosis, and ulcer-ation.19 The inflammatory and proliferative phases may be dis-rupted by the early effects of radiation. Affected factors include TGF-β, VEGF, TNF-α, IFN-γ, and cytokines such as IL-1 and IL-8. These cytokines are overexpressed after the radiation injury leading to uncontrolled matrix accumulation and fibrosis. NO, which induces collagen deposition, is decreased in irradiated wounds; this may explain the impaired wound strength seen in irradiated wounds. Decreased MMP-1 may contribute to inade-quate soft tissue reconstitution (Table 6-4). Keratinocytes, which are crucial for wound epithelialization, demonstrate a shift in expression from the high molecular keratins 1 and 10 to the low molecular keratins 5 and 14 after radiation injury.
In nonhealing ulcers, keratinocytes display decreased expres-sion of TGF-α, TGF-β1 FGF-1, FGF-2, KGF, VEGF, and hepa-tocyte growth factor (HFG). Expression of MMP-2, MMP-12, and MMP-13 has been shown to be elevated in irradiated human keratinocytes and fibroblasts.20 Fibroblasts play a central role in wound healing through deposition and remodeling of collagen fibers. In irradiated tissue, fibroblasts generate disorganized col-lagen bundles from dysregulation of MMP and TIMP. Because TGF-β regulates MMPs and TIMP, it may be of particular rele-vance to radiogenic ulcers (see Table 6-4).21
Strategies for treating problematic radiogenic ulcers include standard wound care, negative pressure wound therapy, nutri-tional optimization, and optimized blood and oxygen delivery. Hyperbaric oxygen (HBO) therapy may improve tissue oxygen
From Haubner F, Ohmann E, Pohl F, et al: Wound healing after radiation therapy: Review of the literature. Radiat Oncol 7:162, 2012.EGF, Epidermal growth factor; FGF, fibroblast growth factor; IFN-γ, interferon-γ; IL-1, -8, interleukin-1, -8; MMP-1, -2, -12, -13, matrix metalloproteinase-1, -2, -12, -13; NO, nitric oxide; PDGF, platelet-derived growth factor; TGF-β, transforming growth factor-β; TIMP, tissue inhibitors of metalloproteinase; TNF-α, tumor necrosis factor-α; VEGF, vascular endothelial growth factor.
TABLE 6-4 Possible Key Wound-Healing Factors Affected by Radiotherapy With Respect to the Phases of Wound Healing
PHASE OF WOUND HEALING
FACTORS AFFECTED BY RADIATION THERAPY
Inflammation TGF-β, VEGF, IL-1, IL-8, TNF-α, IFN-γProliferation TGF-β, VEGF, EGF, FGF, PDGF, NORemodeling MMP-1, MMP-2, MMP-12, MMP-13, TIMP
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles148
Skin substitutes (discussed later) provide multiple factors that may alter the nature of the wound microenvironment in favor of and allow healing to occur. Split-thickness skin grafting is the surgical substitution of native epidermis and partial dermis to assist wound closure, and it has a strong evidence base from treat-ment of acute burn wounds and chronic nonhealing wounds.28 Skin is harvested from the patient and transferred to an adequately prepared wound bed. The graft provides wound coverage by pro-viding a favorable healing environment through exclusion of pathogenic bacteria and provision of ECM, cells (keratinocytes and fibroblasts), and bioactive molecules (cytokines, chemokines, and growth factors) that facilitate wound repair through a process of “dynamic reciprocity” (Fig. 6-9).15 However, autologous skin grafts occasionally are limited or unavailable. Biologic skin sub-stitutes have been used for many years and include cadaveric skin allografts and porcine and bovine xenografts.28 These grafts are not durable because they do not integrate into the host, and they are associated with rejection and disease transfer. However, they provide adequate temporary wound cover, limiting complications until autologous grafts or other definitive management strategies are available.
WOUND DRESSINGSWound dressings—present since antiquity—evolved very little for many years until 1867, when Lister introduced antiseptic dress-ings by soaking lint and gauze in carbolic acid. Since then, numer-ous more sophisticated products have become available; however, certain characteristics in wound dressings should be considered in the nonsurgical treatment of a wound (Box 6-2). Wound healing is most successful in a moist, clean, and warm environment. Not all dressings can provide all of these characteristics, and not all wounds require all of them; hence, the choice of dressing should match the prevailing wound conditions.
Two concepts that are critical when selecting appropriate dress-ings for wounds are occlusion and absorption. Studies have dem-onstrated that the rate of epithelialization under a moist occlusive
MalnutritionProtein catabolism delays wound healing and promotes wound dehiscence, particularly when serum albumin levels are less than 2.0 g/dL. Protein supplements can reverse this deficiency.
Vitamin deficiencies affect wound healing primarily as a result of their effect as cofactors. Delayed healing can occur 3 months after vitamin C deprivation and can be reversed by supplements of 10 mg/day and no more than 2000 g/day. Deficiency of vitamin A impedes monocyte activation and deposition of fibro-nectin, affecting cellular adhesion, and impairs TGF-β receptors. Vitamin A contributes to lysosomal membrane destabilization and directly counteracts the effect of glucocorticoids. Vitamin K deficiency limits the synthesis of prothrombin and factors VII, IX, and X. Vitamin K metabolism is impeded by antibiotics; patients who have chronic or recurrent infections need to have clotting parameters checked before surgical procedures.
Zinc is a necessary cofactor for RNA polymerase and DNA polymerase. Zinc deficiency impairs early wound healing, but it is rare except with large burns, severe polytrauma, and hepatic cirrhosis. Iron deficiency anemia is a debatable cause of delayed wound healing. Although ferrous ion is a cofactor needed to convert proline to hydroxyproline, reports are conflicting regard-ing the effects of acute and chronic anemia on wound healing. In general, patients should have a well-rounded diet consisting of adequate protein intake and caloric value plus vitamin and mineral supplementation.
DrugsSome exogenously administered drugs directly impair wound healing. Chemotherapeutic agents, such as doxorubicin (Adria-mycin), nitrogen mustard, cyclophosphamide, methotrexate, and bis-chloroethylnitrosourea, are potent wound inhibitors in animal models and interfere with uncomplicated wound healing clinically. They reduce mesenchymal cell proliferation, platelet and inflammatory cell counts, and availability of growth factors, particularly if given preoperatively. Tamoxifen, an antiestrogen, decreases cellular proliferation, with a decrease in wound-breaking strength that is dose dependent and may be secondary to decreased TGF-β production. Glucocorticosteroids impair fibroblast proliferation and collagen synthesis, resulting in decreased granulation tissue formation. Furthermore, steroids stabilize lysosomal membranes. Administration of vitamin A can reverse this particular effect. Diminished wound-breaking strength caused by exogenous steroids is time and dose related. High doses of nonsteroidal anti-inflammatory drugs have been reported to delay healing, but doses in the therapeutic range are unlikely to have an effect.
Treatment of Chronic WoundsThe management of a chronic wound depends on its etiology. Currently available therapies are slow, labor-intensive, and expen-sive without any guarantee of healing if all local and systemic factors are not addressed. Wound-healing research identified key structural proteins and molecules in normal and disordered wound healing as possible targets for future interventions. This research led to the application of topical growth factors to chronic wounds, which, although initially promising, almost universally failed to produce clinically significant improvements in wound healing. The reason for the failure is presumed to be a result of degradation of the growth factors by proteases in the wound fluid. This failure highlighted the complex nature of wound healing, where simply replacing one element is not enough.
FIGURE 6-9 The “dynamic reciprocity” model of wound healing. Inter-actions are dynamic as they vary with time and location within the wound site. Products of any one element influence the actions of the others. Inappropriate downregulation of any one element can result in conversion from an acute to a chronic wound. (From Greaves NS, Iqbal SA, Baguneid M, et al: The role of skin substitutes in the management of chronic cutaneous wounds. Wound Repair Regen 21:194–210, 2013.)
• Biological• Synthetic
• Growth factors• Cytokines
Adult or Neonatal:• Fibroblasts• Keratinocytes
Cells:BioactiveMolecules:
Extracellular Matrix:
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 149
(ConvaTec, Skillman, NJ), Allevyn (Smith & Nephew, Largo, FL), and Curafoam (Kendall Company, Mansfield, MA). Wound healing beneath absorptive dressings appears to be slower than under occlusive dressings, possibly because of wicking of cytokines from the wound bed or decreased keratinocyte migration.
The final class of wound dressings consists of creams, oint-ments, and solutions. This is a broad category that extends from traditional materials, such as zinc oxide paste, to preparations containing growth factors. Various categories include dressings with antibacterial properties such as acetic acid, Dakin’s solution, silver nitrate, mafenide (Sulfamylon), silver sulfadiazine (Silva-dene), iodine-containing ointments (Iodosorb), and bacitracin. Application of these products is indicated when clinical signs of infection are present or if quantitative culture demonstrates more than 105 organisms per gram of tissue.
The number of available wound products is staggering. The surgeon must have information about available dressings to allow effective wound management (Box 6-3).
OTHER THERAPIESHyperbaric Oxygen TherapyWound ischemia is the most common cause of wound-healing failure. HBO therapy uses oxygen as a drug and the hyperbaric chamber as a delivery system to increase PO2 at the target area. HBO therapy is used for myriad disease processes, including bacterial infections, decompression sickness, improvement of split-thickness skin graft take, flap survival and salvage, acute thermal burns, necrotizing fasciitis, chronic wounds, hypoxic wounds, osteoradionecrosis, and radiation injuries.29 Ischemia or tissue hypoxia (PO2 <30 mm Hg) significantly impairs normal metabolic activity and decreases wound healing by impairing fibroblast proliferation, collagen synthesis, and epithelialization. HBO therapy involves inhalation of 100% oxygen at 1.9 to 2.5 atm, which can increase tissue PO2 10 times higher than usual. The higher PaO2 is sufficient to supply the tissue with all its meta-bolic requirements, even in the absence of hemoglobin; this ele-vated level lasts for 2 to 4 hours after termination of HBO therapy and induces synthesis of endothelial cell NO synthase as well as angiogenesis. Oxygen has been reported to stimulate angiogenesis, enhance fibroblast and leukocyte function, and normalize cutane-ous microvascular reflexes.30,31
Evaluation of the vascular supply to the target area is essential, and revascularization before HBO therapy is an essential prereq-uisite to HBO therapy. Patients will likely benefit from adjuvant HBO therapy if improvement in tissue oxygenation can be dem-onstrated in a hypoxic wound while breathing oxygen under hyperbaric conditions.29 Transcutaneous oxygen pressure (TcPO2) is used to assess wound perfusion and oxygenation. A wound TcPO2 less than 35 mm Hg in room air indicates a hypoxic wound. In-chamber TcPO2 of 200 mm Hg or more suggests potential benefit from HBO therapy.
HBO treatments for hypoxic wounds are usually delivered at 1.9 to 2.5 atm for sessions of 90 to 120 minutes each, with the patient breathing 100% oxygen during the treatment. Treatments are given once daily, five to six times per week and should be given as an adjunct to surgical or medical therapies. Clinical evidence of wound improvement should be noted after 15 to 20 treatments.
Complications of HBO therapy are caused by changes in atmospheric pressure and elevated PO2. Middle ear barotrauma, ranging from tympanic membrane hyperemia to eardrum
dressing is twice that of a wound that is left uncovered and allowed to dry. An occlusive dressing provides a mildly acidic pH and low oxygen tension on the wound surface, which is conducive for fibroblast proliferation and formation of granulation tissue. However, wounds that produce significant amounts of exudate or have high bacterial counts require a dressing that is absorptive and prevents maceration of the surrounding skin. These dressings also need to reduce the bacterial load while absorbing the exudate produced. Placement of a pure occlusive dressing without bacte-ricidal properties would allow bacterial overgrowth and worsen the infection.
Dressings can be categorized into four classes: (1) nonadherent fabrics; (2) absorptive dressings; (3) occlusive dressings; and (4) creams, ointments, and solutions (Table 6-5). Briefly, nonadher-ent fabrics are fine-mesh gauze supplemented with a substance to augment their occlusive properties or antibacterial abilities, such as Scarlet Red, a relatively nonocclusive dressing that is impreg-nated with O-tolylazo-O-tolylazo-β-naphthol that is used on skin graft harvest sites in burn care. Xeroform is a relatively occlusive, hydrophobic dressing containing 3% bismuth tribromophenate in a petrolatum base, which helps mask wound odors and has antimicrobial activity against Staphylococcus aureus and Escherichia coli.
Occlusive dressings provide moisture retention, mechanical protection, and a barrier to bacteria. These dressings can be divided into biologic and nonbiologic dressings. Examples of bio-logic dressings are allograft, xenograft, amnion, and skin substi-tutes. An allograft is a graft transplanted between genetically unique humans, whereas a xenograft is a graft, such as pigskin, transplanted between species. Allografts and xenografts are tem-porary dressings; both will be rejected if left on a wound for an extended period. Amnion is derived from human placentas and is another effective biologic wound dressing. Initially, these dress-ings were most often used in the treatment of burn wounds; however, they can be used as a temporary measure in other wounds.
Absorptive dressings are useful for wounds with a significant amount of exudate. Leg ulcers can produce 12 g/10 cm2/24 hours of exudate. Examples include wide-mesh gauze, the oldest of this type of dressing, which loses its effectiveness when saturated, and newer materials, such as foam dressings, which provide the absor-bent qualities for removing large quantities of exudate and have a nonadherent quality to prevent disruption of newly formed granulation tissue on removal. Examples include Lyofoam
Creates a moist environmentRemoves excess exudatePrevents desiccationAllows for gaseous exchangeImpermeable to microorganismsThermally insulatingPrevents particulate contaminationNontoxic to beneficial host cellsProvides mechanical protectionNontraumaticEasy to useCost-effective
BOX 6-2 Characteristics of Ideal Dressing
Adapted from Morin RJ, Tomaselli NL: Interactive dressings and topical agents. Clin Plast Surg 34:643–658, 2007.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles150
TABLE 6-5 Types of Dressings
CATEGORYCOMPOSITION AND CHARACTERISTICS FUNCTION EXAMPLES COMMENTS
Nonadherent fabrics
Fine-mesh gauze with supplement to augment occlusive and nonadherent properties, healing-facilitating capabilities, and antibacterial characteristics
Protection, moist environment Scarlet Red, Vaseline gauze, Xeroform, Xeroflo, Mepitel, Adaptic, Telfa
Scarlet Red, Xeroform, Telfa, Vaseline gauze—hydrophobic, more occlusive; Xeroflo, Mepitel, Adaptic—less occlusive, allow drainage of fluid into overlying dressing layers
AbsorptiveGauze Wide mesh gauze Removing exudates, prevents
macerationWide-mesh gauze Not effective when saturated; can be
used for wound débridement if in contact with wound
Foams Hydrophobic polyurethane sheets
Protection, absorption of exudate Lyofoam, Allevyn, Curafoam, Flexzan, Vigifoam
Advantages—comfortable, can expand and conform to wound, easily removed for cleansing
Disadvantages—need to be replaced as wounds heal, custom shapes are labor-intensive to make, limited protection from bacteria, cannot be used while bathing
OcclusiveNonbiologic Insulation, moisture retention,
protective barrier acts against bacteria
Films Clear polyurethane membranes with acrylic adhesive on one side
See above Tegaderm, Mefilm, Carrafilm, Bioclusive, Transeal, Opsite
Waterproof; permeable to oxygen, carbon dioxide, and water vapor; do not interfere with patient function; allow visualization of wound; nonabsorptive, can leak; require intact skin around wound area; wound contraction may be slowed, removal may disrupt new epithelium
Hydrocolloids Hydrocolloid matrix (gelatin, pectin, carboxymethylcellulose)
As above; absorbs water from wound exudates, swells, liquefies to form moist gel
Duoderm, NuDerm, Comfeel, Hydrocol, Cutinova, Tegasorb
Available as adhesive wafers, paste, powders; similar features as films, but bulkier; more protection, but may interfere more with function
Alginates Cellulose-like polysaccharide fibers derived from calcium salt of alginate (seaweed)
As above; calcium alginate conversion to soluble sodium salt after contact with wound exudates results in hydrophilic gel
Algiderm, Algosteril, Kaltostat, Curasorb, Carasorb, Melgisorb, SeaSorb, Kalginate, Sorbsan
Occlusive environment; various forms—ropes, ribbons, pads
Hydrogels Polyethylene oxide or carboxymethylcellulose polymer and water (80%)
As above; rehydrating agents for dry wounds; little water absorption (high water content)
Vigilon, Nu-gel, Tegagel, FlexiGel, Curagel, Flexderm
Available as gels, sheets, impregnated gauze; occlusive environment
Biologic Similar to nonbiologicsHomograft Derived from genetically
unique humansCadaver skin Temporary dressing; is rejected if left
on wound for extended periodXenograft Interspecies graft (e.g., pig) Pigskin Same as aboveAmnion Human placenta Good biologic dressingSkin substitutes Different compositions Integra, Alloderm, Apligraf,
Biobrane, TranscyteIntegra—bilayered membrane skin
substitute; AlloDerm—acellular cadaveric dermis; Apligraf—living, bilayered, biologic dressing composed of neonatal dermal fibroblasts on collagen matrix
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 151
Adapted from Lionelli GT, Lawrence WT: Wound dressings. Surg Clin North Am 83:617–638, 2003.
TABLE 6-5 Types of Dressings—cont’d
CATEGORYCOMPOSITION AND CHARACTERISTICS FUNCTION EXAMPLES COMMENTS
Creams, Ointments, and SolutionsAntibacterial Different compositions Used to treat infected wounds Acetic acid (gram-negative,
Pseudomonas); Dakin’s solution (broad antibacterial spectrum); iodine-containing antibacterials (Iodosorb, Iodoflex, Betadine; broad antibacterial and antifungal spectrum); silver nitrate (broad antibacterial spectrum); mafenide acetate (Sulfamylon; broad antibacterial spectrum) silver sulfadiazine (Silvadene; broad antibacterial, antifungal, and antiviral spectrum); Acticoat (broad antibacterial spectrum)
Acetic acid—impairs wound healing; Dakin’s—toxic to fibroblasts; iodine-containing solutions—toxic to fibroblasts, impairs wound healing; silver nitrate—treats burns, slows epithelialization, hyponatremia, stains clothes black; mafenide acetate—penetrates eschar, painful application, inhibits reepithelialization, carbonic anhydrase inhibitor; silver sulfadiazine—transient neutropenia, accelerates epithelialization of partial-thickness burns, neovascularization, commonly used for burns; Acticoat—silver-impregnated occlusive dressing, antibacterial activity lasts 3 days
Antibacterial ointments
Different compositions Used to treat infected wounds; soothing to apply; lubricates wound surface; occlusive; antibacterial activity lasts 12 hr
Bacitracin (gram-positive cocci and bacilli); neomycin (gram-negative) polymyxin B sulfate (gram-negative); Polysporin (polymyxin B, bacitracin); Neosporin (polymyxin B, bacitracin, neomycin); triple antibiotic ointment (polymyxin B, bacitracin, neomycin)
Neosporin—increased reepithelialization in experimental wounds by 25% compared with wounds with no dressing
Enzymatic Different compositions; uses naturally occurring enzymes
Removal of necrotic tissue Sutilains (derived from Bacillus subtilis); collagenase (Santyl; derived from Clostridium histolyticum); papain (derived from vegetable pepsin)
Sutilains—digests denatured collagen; collagenase—digests denatured and native collagen; papain—effective against collagen in presence of cofactor containing sulfhydryl group; addition of urea doubles enzymatic action of papain
Other Normal saline wet to dry gauze dressing
Removal of necrotic tissue Nondiscriminating—necrotic and newly formed granulation tissue and epithelium removed; can be painful
perforation, is the most common complication. Pneumothorax (particularly tension pneumothorax) is far less common but potentially life-threatening. Other complications associated with increased PO2 include brain oxygen toxicity, manifested by con-vulsions resembling grand mal seizures; oxygen lung toxicity, resulting from damage from oxygen free radicals to lung paren-chyma and airways and ranging from tracheobronchitis to full-blown respiratory distress syndrome; and transient myopia. Absolute contraindications to HBO therapy are (1) uncontrolled pneumothorax, (2) current or recent treatment with bleomycin or doxorubicin (potential aggravation of cardiac and pulmonary toxicity), and (3) treatment with disulfiram (increases risk of developing oxygen toxicity).
Randomized clinical trials demonstrated that HBO is a useful adjunctive therapy for diabetic ischemic foot ulcers and reduces
the rate of extremity amputation. In addition, the Cochrane Col-laborative in 2004 reviewed HBO therapy for chronic wounds and concluded that HBO therapy reduces the risk of amputation for patients with diabetic foot ulcers and increases the chance of healing at 1 year. These studies are difficult to interpret because of the length of time chronic wounds take to heal and the vari-ability among wounds that cannot be controlled. Furthermore, the Cochrane Collaborative noted that the recommendations were based on small, underpowered studies and that further ran-domized studies were greatly needed to clarify the benefits of this costly therapy. Despite the obvious potential scientific biases, medical insurance companies have decided to support HBO therapy as an adjunct treatment for perfused, chronic, nonhealing lower extremity wounds, provided that the limbs have already undergone revascularization.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles152
Incisional woundThree-layer dressingsOintmentsOcclusive dressings
Partial-thickness wounds (e.g., abrasions, donor sites)No dressing (scab)Impregnated gauzeCreams, ointmentsOcclusive dressings
Full-thickness wounds (e.g., pressure sores)Alginates or hydrogels—rarely applicableCreams, gels (e.g., Silvadene)Wet to dry dressing changesVacuum-assisted closure device
BOX 6-3 Dressing Options for Noninfected Clean Wounds
Despite evidence suggesting potential benefit of HBO therapy on healing chronic wounds, its cost is high. Patients often travel long distances for daily treatments at great cost to themselves and their families. Although reported protocols for treatment of isch-emic limb ulcers vary significantly, most involve a total cost of $15,000 to $40,000. HBO therapy is not recommended as a primary treatment for patients with uncomplicated diabetic or ischemic ulcers; however, in selected more complicated cases, HBO therapy may have a role.32
Negative Pressure–Assisted Wound TherapyOne of the most significant discoveries in wound management in recent decades was the improvement in wounds with negative pressure–assisted wound therapy (NPWT) (Fig. 6-10). With this technology, the surgeon has options in addition to immediate closure of wounds (i.e., adjunctive therapy before or after surgery or an alternative to surgery in extremely ill patients).
Argenta and associates originally described the use of negative pressure to assist in wound closure in 1997. By applying subat-mospheric pressure to wounds, they demonstrated removal of chronic edema, an increase in local blood flow, and stimulation of granulation tissue. This technique may be used on acute, sub-acute, and chronic wounds. Additional studies demonstrated significant improvement in wound depth in chronic wounds treated with NPWT compared with wounds treated with saline wet to moist dressings. In addition, treatment with negative pressure results in faster healing times, with fewer associated complications.
The exact mechanism of the improvement in healing with NPWT has yet to be determined. Many investigators initially believed that the reason for increased wound healing is the removal of wound exudates while keeping the wound moist. As originally hypothesized by Argenta and associates, with NPWT, there is a fivefold increase in blood flow to cutaneous tissues. Further studies showed an increase in capillary caliber and stimulated endothelial proliferation and angiogenesis. It is well known that increased bacterial loads result in slowed wound healing; however, despite increased wound healing with NPWT, it has been shown to result in increased bacterial counts. Other studies suggested that NPWT produces three-dimensional stress within the cells (microstrain) and across the whole area of the wound (mac-rostrain), resulting in changes such as increased cellular prolifera-tion and higher microvessel density. Evidence also suggests that
FIGURE 6-10 Negative pressure–assisted wound closure sponge in place on a patient’s abdomen.
NPWT alters wound fluid composition by removing potentially deleterious proteinases and inflammatory cytokines, such as MMP-1, MMP-2, MMP-9, and TNF-α.
Although the mechanisms responsible for the improvement achieved with NPWT have yet to be clearly elucidated, this treat-ment represents a significant improvement in cost-effectiveness and has decreased length of stay after acute and chronic wounds. There have been reports of a 78% decrease in hospital stay and a 76% decrease in cost with NPWT. This cost decrease and effec-tiveness of wound treatment with NPWT have translated to home health care treatment of Medicare patients.
Clinical benefits of NPWT have been demonstrated in ran-domized controlled trials and include a decrease in wound volume or size, accelerated wound bed preparation, accelerated wound healing, improved rate of graft take, decreased drainage time for acute wounds, reduction of complications, enhancement of response to first-line treatment, increased patient survival, and decreased cost. Trials published more recently have further dem-onstrated the wound-healing efficacy of NPWT. A 16-week, 18-center, randomized clinical trial conducted by Armstrong and Lavery comprising 162 patients with diabetes with larger and more complex wounds than in previous randomized trials found that NPWT healed more wounds after partial foot amputation versus the standard of care (43 [56%] versus 33 [39%]; P = .040). The authors noted that NPWT produced faster wound-healing rates (P = .005) and faster granulation tissue formation rates versus standard of care based on the time needed to complete closure (P = .002). Resource utilization for patients treated with NPWT was evaluated in the same study population. Apelqvist reported that patients randomly assigned to the NPWT group required fewer surgical procedures (including débridement) than the control group (43 versus 120; P < .001), fewer average number of dressing changes (41 [range, 6-140] in the NPWT group versus 118.0 [range, 12-226] in the control group; P < .0001), and fewer outpatient treatment visits (4 [range, 0-47] in the NPWT group versus 11 [range, 0-106] in the control group; P < .05). A cost savings greater than $12,800 resulted compared with standard therapy. Combined with the clinical data, these analyses provide compelling evidence that appropriate use of NPWT is efficacious and cost-effective in achieving healing of properly selected wounds on an inpatient and outpatient basis.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 153
hydroxylase and may explain why there is higher fibroblast activity in fetuses younger than 20 weeks’ gestation.
Collagen synthesis decreases to adult levels after 20 weeks’ gestation, and collagen degradation increases with gestational age. Increased gene expression of MMP-1, MMP-3, and MMP-9 cor-relates with the onset of scar formation in nonwounded fetal skin. These findings suggest that late-gestation fetal rat skin undergoes an adult type of tissue remodeling after wounding that leads to the scarring seen in adult skin.
There are also differences in the components of the ECM of fetal and adult wounds. After injury, fibronectin levels are similar in adults and fetuses, but tenascin, an inhibitor of fibronectin, increases earlier and returns to normal more rapidly in the fetus. Larger amounts of fibronectin in fetal wounds stimulate immedi-ate cell attachment, whereas the more rapid deposition of tenascin in the fetus allows cells to migrate and fully epithelialize the wound more rapidly and decrease wound-healing time.
Hyaluronic acid is persistently elevated in fetal wounds. During gestation, decreasing levels of hyaluronic acid correlate with increasing scarring potential. The unique ECM composition of fetal tissues may influence collagen fibril deposition by facilitating cell mobility and migration, leading to the loose collagen pattern seen in healed fetal wounds as opposed to the dense collagenous pattern seen in adult scars. However, few studies have examined the effect of modifying the ECM components.
In addition, the fetus exhibits a reduced inflammatory response with a lack of neutrophil infiltration and decreased infiltration of endogenous immunoglobulins. The paucity of macrophages and a difference in the temporal appearance of macrophages in fetal wounds may explain differences in growth factor profiles and the reduced inflammatory response. These studies cite a direct correla-tion between increased macrophage recruitment in older fetuses and the development of increased scarring.
Fetal wounds have minimal levels of TGF-β and FGF-2. TGF-β is the growth factor that has been most extensively studied in fetal wound repair. TGF-β1 induces rapid healing and scar formation when added to adult rat wounds and induces inflammation and fibrosis when added to fetal rabbit wounds. TGF-β production may be blunted in hypoxemic conditions, leading to the theory that the decreased oxygen tension in the fetal environment inhibits TGF-β production and results in decreased scar formation. It has been suggested that differential expression of the different TGF-β isoforms, rather than the pres-ence of TGF-β, may be important in explaining the differences in repair.
PDGF also disappears more rapidly in fetal wounds. The paucity of growth factors may be explained by decreased inflam-matory cell recruitment. Normal inflammatory (adult-type) wound healing may have evolved to reduce the risk of infection at the expense of healing quality. Growth factor manipulation to make wounds more fetal-like has failed to result in completely scarless healing and has failed to regenerate dermal appendages. In addition, some inconsistencies in fetal wound healing are not clearly understood. There are differences in species with regard to scarless fetal wound healing, and not all fetal tissues are capable of scarless healing. For example, fetal lamb diaphragm and gastric wounds scar, whereas concurrent skin wounds heal without scarring.
The presence of myofibroblasts and concurrent scar formation suggests that a transition in fibroblast phenotype may contribute to scarring. Excisional wounds in 75-day-gestation fetal lambs showed an absence of scar formation and alpha smooth muscle
FETAL WOUND HEALINGFetal skin wounds heal rapidly without the scarring and inflam-mation characteristic of adult skin wounds. In adult cutaneous healing, dermal appendages (hair follicles, sweat and sebaceous glands) fail to regenerate. In addition, healed adult wounds have densely packed collagen bundles oriented perpendicularly to the wound surface, whereas collagen in uninjured and fetal skin retains a reticular pattern. Fetal wounds reepithelialize faster, with less neovascularization and a faster increase in strength. Fetal wounds differ in inflammatory responses, ECM components, growth factor expression, and biologic responses to growth factor expression. It was thought that fetal wound healing represented ideal tissue repair and that understanding fetal wound healing would provide surgeons the tools to regulate and control the dif-ferent steps in adult wound healing.
Fetal repair depends on gestational age and wound size. The wound size threshold (diameter of excised skin at which 50% of wounds heal without scarring at a given gestational age) appears to be 6 to 10 mm for 60-day-gestation and 70-day-gestation animals and 4 to 6 mm for 80-day-gestation and 90-day-gestation animals. Larger wounds may extend the time to healing and expose wound tissue to a different ECM and growth factor profile. Larger excisional wounds may also stimulate the formation of myofibroblasts resulting in scar formation. The transition from scarless to scarring repair occurs near the end of the second tri-mester. Wounds heal faster in a fetus than in a neonate, and they heal more slowly in adults compared with neonates.
Skin appendages are formed when dermal fibroblasts induce the epithelium to form hair follicles or glands. Wounds created early in gestation heal without scarring and with dermal append-ages, suggesting tissue regeneration versus repair. In contrast, late gestation wounds heal with scarring and without dermal append-ages. The transition from scarless healing to healing without dermal appendages suggests that fetal fibroblasts lose their ability to induce the epithelium to form dermal appendages with advanc-ing gestational age.
Intrinsic differences (oxygen tension of the human fetus) rather than extrinsic differences (amniotic fluid environment) are more likely determinants of whether wounds will heal with scars. Oxygen tension is markedly decreased in fetal sheep (mean PaO2 = 20 mm Hg) compared with adult sheep (mean PaO2 of 116 mm Hg); this is partially compensated by the relative affinity of fetal hemoglobin for oxygen.
The fetal environment, an extrinsic difference between fetal and adult wounds, is characterized by a hyaluronic acid–rich amniotic fluid. The increased number of hyaluronic acid receptors and increased amount of hyaluronic acid may create a permissive environment in which fibroblast movement is facilitated, resulting in the increased rate and efficiency of fetal healing.
Much of fetal wound-healing research has focused on fetal fibroblasts. Fetal fibroblasts appear to have characteristics quite different from adult fibroblasts. Proline hydroxylation is a rate-limiting step in collagen synthesis by dermal cells. Early-gestation fetal human fibroblasts have increased prolyl hydroxylase activity that gradually decreases to adult levels after 20 weeks of gestation. Collagen types I, III, V, and VI appear earlier, and the ratio of type III to type I is greater in fetal wounds, which is consistent with the higher prevalence of type III collagen in normal fetal tissue. Fetal fibroblasts in vitro have higher collagen production than their adult counterparts. This higher collagen production may be secondary to the unique regulatory mechanism for prolyl
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles154
actin expression. Alpha smooth muscle actin appears after 100 days of gestation along with scar formation.
Focus has shifted more recently to multiple pluripotent stem cells, such as epithelial stem cells (EpSCs), mesenchymal stem cells (MSCs), and “small dot” cells, and their role in fetal wound healing. The slowly proliferating EpSCs, which are interspersed throughout the basal layers, are surrounded by more quickly pro-liferating basal cells and their suprabasal progeny to form epider-mal proliferative units. EpSCs are also found within the bulge area of hair follicles and are believed to migrate to the epidermis after injury and differentiate into dermal, vascular, and neural components.
MSCs play a role in regenerative healing, including immuno-modulation, antifibrosis, antiapoptosis, and angiogenesis,33 as well as preventing excessive inflammation. They immunoregulate through multiple independent pathways, including the induction of IL-10 secretion by macrophages.34
“Small dot” cells also have been identified to play a role in fetal wound healing. There is a 20-fold greater increase of these cells in fetal blood than postnatal blood. Fluorescence-labeled “small dot” cells transplanted into a postnatal murine incisional wound model migrated to the wound bed and decreased scarring.35 Further investigations should help to elucidate the importance of these stem cell populations in fetal wound healing and in treating abnormal wound healing (Table 6-6).36
NEW HORIZONSTissue EngineeringIn 1987, the National Science Foundation bioengineering panel defined tissue engineering as “the application of the principles and methods of engineering and the life sciences toward the develop-ment of biologic substitutes to restore, maintain, or improve function.” These principles and methods have been used toward the creation of skin products made of cells, ECM components, or combinations of the two. This tissue-engineered skin has devel-oped and progressed rapidly over the past 20 years, mainly because of the limitations associated with autografts, and may function by providing the cellular or matrix components that could be neces-sary for wounds to heal. These new skin substitutes more accu-rately mimic native tissues to promote sustained healing without rejection. The use of biologic dressings, scaffolds, stem cell therapy, and gene therapy are a few examples of tissue engineering, in which new tissues are created rather than transferred.
Bioengineered skin substitutes can potentially save millions of dollars a year for health care delivery services through reduced spending on dressings and treatment of wound-induced compli-cations, particularly in the treatment of venous, diabetic, and pressure ulcers that form 90% of all chronic wounds. Bioengi-neered skin substitutes act as protective dressings, by limiting bacterial colonization and fluid loss, but they also stimulate healing (Fig. 6-11).15 Their design is variable and dependent on the layer of skin they are designed to replace.
Bioengineered Skin SubstitutesEpidermal replacements are created by expansion of patient-derived keratinocytes in the laboratory.37 These are fragile con-structs that are attached to a carrier material to facilitate application to the wound. Dermal substitutes are based on a structural three-dimensional matrix material, which behaves similar to ECM, and may incorporate cells or bioactive molecules. Provision of these key factors to the wound bed may provide the necessary stimulus
bFGF, Basic fibroblast growth factor; HA, hyaluronan; IL-6, -8, -10, interleukin-6, -8, -10; MSC, mesenchymal stem cell; PDGF, platelet-derived growth factor; TGF-β, transforming growth factor-β; VEGF, vascular endothelial growth factor.
TABLE 6-6 Comparison of Fetal Regenerative Wound Healing Profile With Postnatal Wound Healing
FETAL POSTNATAL
Phenotype Regenerative Scar formation
Growth FactorsbFGF Lower HigherPDGF Lower HigherVEGF Higher LowerTGF-β TGF-β1 Low levels High levels TGF-β2 Low levels High levels TGF-β3 High levels Low levels
Inflammatory ResponseInflammatory cell Minimal High levels leukocytes,
macrophages, mast cells infiltrate
Cytokines Proinflammatory: IL-6,
IL-8Low levels High levels
Anti-inflammatory: IL-10 High levels Low levels
Extracellular MatrixCollagen Histology Fine, reticular weave Thick, ropelike bundles Type III collagen High levels Low levels Deposition Immediate Delayed Cross linking Low levels High levels TGF-β1-stimulated
depositionAbsent Present
Hyaluronan Expression High levels Low levels
Persistent expression Transient expression Molecular weight High Low HA receptors (fibroblast) High levels Low levelsMechanical force Myofibroblast (day 14) Absent PresentStem cells MSC High levels Lower levels Dot cells Present Absent
From Leung A, Crombleholme TM, Keswani SG: Fetal wound healing: Implications for minimal scar formation. Curr Opin Pediatr 24:371–378, 2012.
to rebalance the wound microenvironment in favor of healing. Bilayer materials represent a combination of features seen in epi-dermal and dermal models.
Epidermal SubstitutesThe gold standard epidermal substitute is an autograft derived from split-thickness skin grafting or from cell line bioreactor expansion. Epidermal replacements are created by expansion of patient-derived cells in the laboratory until enough cell mass is generated to be transferred to the wound. Autologous
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 155
FIGURE 6-11 The effect of skin substitutes in the wound bed. Skin substitutes have variable structures and cellular content. They may be cellular or acellular, but both forms induce the influx of endogenous cells, including fibroblasts, keratinocytes, endothelial cells, macrophages, and neutrophils into the wound bed. These cells secrete various cytokines and growth factors that stimulate angiogenesis, extracellular matrix (ECM) deposition, and reepithelialization via the process of dynamic reciprocity. The skin substitute is replaced by native tissues eventually resulting in a healed wound. Solid lines indicate upregulation, and dashed lines indicate downregulation. IL-1, Interleukin-1; IL-6, interleukin-6; KGF-2, keratinocyte growth factor-2; MMP, matrix metalloproteinase; NO, nitric oxide; PDGF, platelet-derived growth factor; TGF-α, transforming growth factor-α; TGF-β, transforming growth factor-β; VEGF, vascular endothelial growth factor. (From Greaves NS, Iqbal SA, Baguneid M, et al: The role of skin substitutes in the management of chronic cutaneous wounds. Wound Repair Regen 21:194–210, 2013.)
VEGF
IL-6NO
PDGFTGF-α
IL-6IL-1
KGF-2IL-6
TGF-β
ECM
Bacteria
NOMMP
SerineProtease
Skin substitute
Endothelial cells
Keratinocytes
Fibroblasts
Neutrophils andmacrophages
VEGF
keratinocytes were first cultured in the laboratory 35 years ago; this progressed into production of cultured epithelial autografts (small sheets of cells two to three layers thick) that were initially used to treat burn victims. Although these grafts are not subject to rejection, there may be a 2- to 3-week delay to generate enough tissue to cover a defect. Epicel, Epidex, Myskin, Bioseed, and Cellspray are epidermal replacements that use autologous keratinocytes.38 Cryoskin and Celaderm contain allogeneic kera-tinocytes. Delivery systems include application as cultured epi-thelial autografts (e.g., Epicel), carrier dressings ranging from bovine collagen to a chemically defined polymer (e.g., Myskin), and conversion into a suspension that can be sprayed onto wound sites (e.g., Cellspray). Limitations of human donor-derived epidermal replacements include (1) need for a well-vascularized dermal bed, (2) low expansion capabilities, and (3) adaptation of phenotypes to in vitro conditions, limiting their ability to form new tissue.
In addition, other epidermal replacements, such as allografts, xenografts, inert membranes (e.g., silicone), and epidermal or bilayer substitutes that do not provide autologous keratinocytes, can provide only temporary wound coverage.28 As a result, these replacements are primarily used for patients with major burns or tissue loss to limit the immediate complications of the injury until definitive coverage can be provided.
Dermal SubstitutesWhen the dermis is destroyed, epidermal substitutes are not enough to ensure wound healing.37 The dermis is essential for skin elasticity and mechanical resistance and epithelial-mesenchymal communications facilitate many complex ex vivo functions of epidermal cells.38 The absence of the dermis has been associated with increased frequency of developing fibrotic conditions.38 Keratinocytes and fibroblasts participate in double paracrine sig-naling: Keratinocytes initiate growth factors in fibroblasts, which
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles156
epidermal layer consists of a silicone membrane that functions as a temporary barrier to prevent dehydration and provide flexible coverage of the wound. The dermal layer is made up of bovine collagen type I and shark chondroitin-6-sulfate. Host cells migrate into the scaffold, degrade the matrix, and replace it with newly synthesized native tissue, such as collagen. Integra is grafted onto the wound bed and when vascularization occurs, the silicone “epidermis” is removed and replaced with either a split-thickness skin graft or tissue-engineered epidermal substitute.
Improved bioengineering techniques later enabled the develop-ment of cellular bilayer substitutes, which contain living kerati-nocytes and fibroblasts and benefit from the angiogenic and inflammatory mediators these cells produce. Apligraf is a bilayered cellular construct that comprises an “epidermal” layer of neonatal human foreskin keratinocytes and a “dermal” layer of bovine-derived collagen matrix seeded with NHFFs. Apligraf, which is indicated for acute and chronic wounds and burns, has been demonstrated to achieve its healing effect through the delivery of cytokines (IFN-α, IFN-β, IL-1, IL-6, and IL-8), growth factors (e.g., PGDF), and ECM components to the wound bed. Because these cellular bilayer substitutes are complex composites contain-ing live cells, they are expensive and difficult to manufacture and have a very limited shelf life.
Evidence for the Use of Skin Substitutes in Chronic WoundsClinical studies examining the effect of skin substitutes on wound healing have looked at many aspects, including immunocompat-ibility, mechanical properties, dermoepidermal junction regenera-tion, and reepithelialization. However, as is often the case with clinical studies on wound healing, many of these studies do not give a complete assessment of their true effect because of their divergent starting wound conditions, differing etiologies, and lack of controls. In many instances, qualitative morphologic examina-tion of regenerated tissue is overlooked in favor of a quantitative assessment of wound closure, such as time to closure. Further-more, much of the evidence is based on low-quality case series and case controls, but there have been a few significant random-ized controlled trials to date that have suggested that skin substi-tutes are useful in accelerating wound healing in chronic wounds, such as diabetic ulcers and venous leg ulcers, and reducing the incidence of osteomyelitis and amputation.
Risks Associated With Skin SubstitutesIn contrast to the use of allografts and xenografts, which can result in graft rejection and transfer of disease from graft to host, modern tissue substitutes have rare instances of rejection. The reasons why rejection is rare in these instances are as follows: (1) Cultured epidermal cells do not express major histocompatibility class II HLA-DR antigens and are not contaminated with Langerhans cells, which are the antigen-presenting cells of the skin; (2) many of these tissue substitutes are acellular, leaving only a protein scaf-fold38; and (3) substitutes that are cellular are populated with fetal cells (e.g., NHFF) that are less likely to trigger an immune response.28
Although there is a small risk of disease transmission to the host of bloodborne pathogens, such as HIV, syphilis, hepatitis B, and hepatitis C, all skin substitutes are rigorously tested to reduce the risk of disease transmission to the host. They all must obtain Human Tissue Act or FDA approval, or both, before clinical application.
Cellular tissue substitutes benefit from the early release of various cytokines and growth factors that accelerate wound
stimulate keratinocyte proliferation.37 Keratinocytes can also control fibroblast differentiation into myofibroblasts. Conse-quently, dermal reconstruction is essential in cases in which no dermis is left on the wound bed.
Dermal substitutes consist of a three-dimensional biomaterial matrix that must behave similar to ECM and must provide a template for host infiltration and a physical support to guide the differentiation and proliferation of cells involved in wound healing. Studies suggest that properties such as matrix elasticity can influence cellular differentiation processes and positioning of specific cell types. The ideal scaffold possesses biocompatibility, biodegradability, and suitable mechanical properties on the macro, micro, and nano scale, with mean pore size of 100 to 200 mm and porosity greater than 90%. Micropore size, shape, distribu-tion, and porosity influence cell intrusion, proliferation, and func-tion. Nanopores play a crucial role in promoting gas and nutrient diffusion through the matrix to support cell survival. Creating a matrix with comparable mechanical properties to the injured tissue is fundamental because its characteristics can mediate ben-eficial cellular activity, especially adhesion, cytoskeletal organiza-tion, and differentiation.
Many dermal tissue substitutes (Oasis, Strattice, and Allo-derm) are rendered acellular to minimize immunogenic responses and provide a scaffold that is repopulated, revascularized, and remodeled with the patient’s own fibroblasts and endothelial cells.38 Acellular dermis has a growing evidence base in the man-agement of chronic wounds and is widely used in plastic and reconstructive surgery because the skin grafts are nonimmuno-genic, are mechanically robust, can be used off the shelf, and have favorable handling characteristics. Other products, such as ICX-SKN, Apligraf, and Orcel, incorporate neonatal human foreskin fibroblasts (NHFFs) or keratinocytes, or both, which are less immunogenic than their adult counterparts, to provide substitutes containing living cells.28,38
There is some clinical evidence to suggest that cellular products may be superior to acellular products in terms of wound healing. The presence of live cells impregnated onto the matrix material ensures that important growth factors can be secreted in sufficient concentrations to replace the growth factors that are absent or downregulated in the wound. Compton and colleagues demon-strated that tissue-engineered dermal matrices combined with seeded cells could lead to true dermal regeneration when they observed in vivo regeneration of organized skin at 35 days using a biodegradable collagen GAG matrix seeded with a suspension of autologous keratinocytes. Yannas also found that dermal sub-stitutes with living dermal fibroblasts resulted in better wound healing with less myofibroblastic activity. In addition, autologous cells were preferable to allogeneic ones, and fibroblasts from dermis produced better results than fibroblasts from adipose tissue. Studies with Dermagraft, which contains NHFFs, yielded good results for patients with chronic wounds of various etiologies by stimulating cellular infiltration, angiogenesis, and epithelializa-tion. Tremblay and colleagues demonstrated that cellular dermal substitutes promoted more rapid vascularization than acellular counterparts (4 days versus 14 days) in a mouse model.
Bilayer SubstitutesBilayer substitutes—available in cellular and acellular varieties—are the most advanced class in terms of structural mimicry of natural skin and are the most expensive available substitutes. Integra, developed in 1981, was the first acellular bilayer and has been used successfully to treat burns and chronic wounds. The
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 157
including bone marrow, skeletal muscle, adipose, and blood. They have been shown to improve acute and chronic wound healing in human and animal models. Although it was thought that the mechanism of action was totally understood, studies have sug-gested that MSCs act through many mechanisms, including cell differentiation, growth factor and cytokine production, immune system modulation, maintenance of the ECM, and wound contraction.
Although differences in gene and cytokine expression can be observed in MSCs derived from different origins,42 a set of core genes are preserved and expressed by all MSCs. MSCs from dif-ferent tissues share properties, allowing identification of these cells as MSCs. There are no data at the present time to suggest that MSCs from one tissue origin should be used preferentially over another for wound-healing applications, although placental-derived MSCs have become a popular target for research. Bone marrow–derived MSCs and placental-derived MSCs showed minimal differences of cell phenotype, differentiation, and immu-nomodulative properties, and similar to other MSCs, placental-derived MSCs are immune-privileged, allowing for allogeneic use.
Multiple mechanisms are involved in MSC-mediated wound healing, including anti-inflammatory and antimicrobial, immu-nomodulative, and tissue reparative activities. MSCs play an important role in mediating each phase of the wound-healing process (Fig. 6-12).43 During the inflammatory phase, MSCs coordinate the effects of inflammatory cells and inhibit the effects of inflammatory cytokines such as TNF and IFN-γ. MSCs also decrease wound infection by secreting antimicrobial factors and by stimulating immune cell phagocytosis. In addition, MSCs promote the transition from the inflammatory to the proliferative phase. In the proliferative phase, MSCs express growth factors such as VEGF, basic FGF, and KGF to promote granulation and epithelialization. Finally, MSCs regulate remodeling of the wound by promoting organized ECM deposition. The benefits of MSCs in wound healing have been demonstrated in several preclinical and clinical studies.
Methods of MSC delivery into the wound include direct injec-tion of a single cell suspension, gel or matrix delivery systems, and synthetic bio-inspired polymers. Recruitment of endogenous MSCs is another method to deliver these cells to the wound. Clinical results using MSCs topically or systemically to enhance the healing of wounds have been promising. Badiavas demon-strated that direct topical application of bone marrow–derived cells to chronic nonhealing wounds can lead to wound closure and rebuilding of tissues. Falanga and colleagues also administered MSCs topically by developing a delivery system using fibrin glue in treating acute and chronic wounds. Bone marrow–derived MSCs, combined with a fibrin spray, were applied topically up to three times. Surgical defects created from excision of nonmela-noma skin cancers healed within 8 weeks, suggesting that MSCs contributed to accelerated resurfacing. Chronic lower-extremity wounds present for longer than 1 year significantly decreased in size or healed completely by 20 weeks. The study also found a correlation between the surface density of MSCs and the reduc-tion in ulcer size.
Systemic administration of MSCs also was observed to promote healing in chronic wounds, particularly when there is an underly-ing condition such as diabetes and other systemic disorders. In a randomized controlled study of 24 patients with nonhealing ulcers of lower extremities by Dash and colleagues, the authors simultaneously administered cultured autologous bone marrow–derived MSCs intramuscularly into the affected limb and topically
healing. However, this beneficial effect may be offset or out-weighed by a proinflammatory macrophage response to their cel-lular content. Two macrophage phenotypes (M1 and M2) were discussed previously.39 The presence of intact cells within implanted scaffolds can be associated with adverse remodeling.40 Sandor and colleagues demonstrated that the presence of cells within a scaffold was associated with increased amounts of proin-flammatory cytokines, increased M1 macrophage polarization, and a poor remodeling outcome in a primate model. Similarly, Brown and colleagues39 found that implantation of a xenogeneic ECM scaffold containing a cellular component resulted in the classic cascade of inflammatory processes with infiltration of pre-dominantly M1 macrophages at 3 days postimplantation, with eventual scar tissue formation in a rat model. When the same scaffold materials were prepared by methods that remove the cel-lular component, the mononuclear cell response was marked by primarily M2 macrophages.39 Other studies also showed that thoroughly decellularized biologic ECM scaffolds promote a host response that is polarized toward the M2 macrophage phenotype and associated with constructive tissue remodeling.39,41
Future of Bioengineered Skin SubstitutesAt the present time, the most advanced skin substitutes cannot fully mimic the properties of normal skin and lack dermal append-ages. They lack glands; pilosity; and specialized cells for the perception of cold, heat, pain, pressure, and vibration.38 Skin pigmentation is discrepant. Future constructs should induce an environment so that wounds heal quickly without scarring or more ideally so that skin regenerates, preserving function and cosmesis. The ideal substitute would be composed of all three components involved in dynamic skin reciprocity—cells, ECM, and bioactive molecules. No FDA-approved products of this type exist at the present time, although a highly porous alginate scaf-fold, seeded with murine myoblasts and impregnated with FGF-2 and HGF, has demonstrated promise in promoting repopulation of native muscle cells in the wound site.
Gene and Stem Cell TherapyGene and stem cell therapy are emerging as promising approaches for the treatment of acute and chronic wounds. Embryonic stem cells were discovered in 1981, and it was quickly recognized that their regenerative properties could potentially be harnessed for treating chronic wounds. However, because of ethical issues, research and their use have been limited. This situation led to the investigation and subsequent discovery of self-renewing multipo-tent adult progenitor cells (MAPCs), which do not have the same ethical limitations.
Whole bone marrow was first investigated as a possible candi-date for cellular therapy because of the ease of harvest and because it is a source of autologous MAPCs. Studies demonstrated that bone marrow can increase vascularity and accelerate closure of chronic wounds. However, because bone marrow is composed of different cell types, including MAPCs, which make up a very small portion of the bone marrow, it is unclear which cell popula-tions are beneficial for wound healing. Isolation of MSCs, a heterogeneous group of MAPCs, from bone marrow and their use in wound-healing studies demonstrated that MSCs result in improved granulation tissue formation and neovascularization compared with whole bone marrow.
MSCs are self-renewing and can differentiate into different mesenchymal lineages, including adipocytes and chondrocytes. They have been isolated in vivo from many different tissues,
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles158
FIGURE 6-12 Mesenchymal stem cell (MSC) roles in each phase of the wound-healing process. HGF, Hepatocyte growth factor; IL-4, interleukin-4; IL-10, interleukin-10; KGF, keratinocyte growth factor; MMPs, matrix metalloproteinases; PDGF, platelet-derived growth factor; TGF-β3, transforming growth factor-β3; TIMP, tissue inhibitors of metalloproteinase; TNF, tumor necrosis factor; VEGF, vascular endothelial growth factor. (From Maxson S, Lopez EA, Yoo D, et al: Concise review: Role of mesenchymal stem cells in wound repair. Stem Cells Transl Med 1:142–149, 2012.)
MSCs in the Wound Healing Phases
Phases
Roles of MSCs
1-3 daysInflammation
• Regulation of inflammation• TNF suppression• IL-10, IL-4 production• Blocking of T-cell proliferation
• Production of VEGF, HGF, and PDGF• Recruitment of keratinocytes, dermal fibroblasts, and host stem cells
• Production of TGF-�3, KGF• Regulation of MMPs/TIMP• Regulation of collagen deposition
2 weeksProliferation
Up to 2 yearsRemodeling
directly onto the ulcer.44 Within 12 weeks, significant improve-ment in pain and a greater decrease in wound size (72% versus 25%) were observed in the MSC-treated group compared with the control group. Clinical benefit of systemic administration of MSCs was also observed in a randomized controlled study con-ducted by Lu and colleagues.45 Briefly, one limb of the patient was injected intramuscularly with cultured autologous bone marrow–derived MSCs or fresh nonculture bone marrow–derived mononuclear cells. The contralateral leg was injected with normal saline as a control for each patient. Compared with control groups, MSC injections and mononuclear cell injections resulted in marked improvement in pain-free walking at 24 weeks and significant increase in ulcer healing rate. Furthermore, the MSC-treated group demonstrated significantly greater increase in ulcer healing rate compared with the group injected with mononuclear cells. Although these studies have shown promising results, there are still numerous areas of future study, including the effect of the source of the MSCs, the benefits of MSCs alone or within a matrix, the timing and frequency of MSC administration, and the number of cells administered.
Although the use of placental-derived MSCs is a popular target for research at the present time, the use of placental tissue for wound treatment started more than 100 years ago. The first reported case series used amnion membrane and chorionic mem-brane as skin substitutes for burns and ulcers. More recently, placental tissue has been studied as an alternative source of MSCs, providing multipotent differentiation and beneficial immunosup-pressive capabilities similar to MSCs derived from other tissues, such as bone marrow–derived MSCs, in terms of morphology, growth, membrane markers, and differentiation potential. MSCs from placenta presented the same morphology and growth char-acteristics as well as markers such as CD105, CD29, and CD44. No expression of the hematopoietic markers CD34, CD45, and HLA-DR was detected. The authors also demonstrated differen-tiation potential of placental MSCs into endothelial and neuronal cells. Other studies confirmed the MSC markers, such as CD44, CD73, CD90, and CD105 membrane markers, in cells derived
from placental membranes. Additional studies demonstrated tri-lineage differentiation capabilities of placental-derived MSCs as well as their lack of immunogenicity and positive immunomodu-latory effects in vitro.
Native placenta tissue cells also provide ECM and numerous growth factors important in wound healing. Analysis of cryopre-served amnion membrane growth factor and growth factor recep-tor content by reverse transcriptase polymerase chain reaction and enzyme-linked immunosorbent assay identified EGF, KGF, HGF, basic FGF, and the family of TGFs. All of these factors are critical in the wound-healing process.
Skin substitutes containing human MSCs have been character-ized to identify critical components necessary for wound healing. A unique feature of these skin substitutes is the presence of viable cells, including MSCs, fibroblasts, and epithelial cells. Fluorescence-activated cell sorting analysis of cells within the skin substitutes reveals the expression of MSC markers, CD105 and CD166, and the absence of CD45, confirming their stem cell identity. Because CD45+ cells are potentially immunogenic, the absence of this antigen indicates a lack of cell-mediated immunogenicity. The number of MSCs present within the skin substitutes is unpub-lished. However, the published cell concentration within placental membranes ranges from 1 to 4 × 104 cells/cm2.46 The viability of cells within the skin substitute is also confirmed, ensuring that functioning cells are delivered at the time of use. Post-thaw, the product’s cell viability must be determined to be greater than 70% before it can be released for clinical use. Although the presence of viable MSCs within the skin substitute is beneficial for wound repair,47,48 it is the combination of viable MSCs, native ECM, and growth factors within the skin substitute that is integral in pro-moting wound repair.
A protein profile of the skin substitute reveals the presence of growth factors needed to carry out the phases of normal healing—inflammatory, proliferative, and remodeling (Table 6-7).43 Several anti-inflammatory and antimicrobial factors are present in the placental-derived MSC–containing skin substitute, including defensins, neutrophil gelatinase-associated lipocalin, interleukin-1
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 159
Skin has also been shown to be a large repository of MAPCs. These MAPCs can arise from the epidermis, dermis, hair follicle bulge, dermal sheath, and dermal papillae. In particular, the hair follicle bulge area is considered an abundant, easily accessible source of actively growing MAPCs. Hair follicle MAPCs have been shown to differentiate into neurons, glial cells, keratino-cytes, and smooth muscle cells. Because of their location, skin-derived MAPCs are present in the wound and are accessible for harvest.
Gene therapy, or the insertion of a gene into recipient cells, has the potential to affect wound healing by recruiting MAPCs to the wound in vivo or through ex vivo modification of MAPCs; the modified cell can then be used for cellular therapy. Gene therapy using vectors has been used experimentally to improve wound healing through overexpression of chemokine genes known to have effects on MAPC homing. Gene therapy allows for the continuous production of the desired protein into the wound by the transduced cells. Direct administration of proteins into the wound could potentially result in degradation of the proteins by wound proteases. Gene therapy–mediated overexpres-sion of HIF-1α and SDF-1α have been used to improve wound healing in a diabetic mouse model.
Although much is still unknown about the use of gene therapy in wound healing, a great deal of research is underway. As more is learned about the molecular biology of wound healing, there will likely be greater use of gene therapy to accelerate wound healing.
The therapy of choice needs to be based on the basics of wound bed preparation and modified according to the character-istics of the wound. Despite the availability of many dressings and alternative therapies, no substantial studies have shown a dif-ference in healing between therapies of the same category. The cost-benefit ratio of some therapeutic modalities is still unclear. A systematic approach that addresses débridement, exudate
receptor antagonist, and several others. These factors help to tran-sition from the inflammatory phase to the proliferative phase of wound healing and to clear infected wounds. Also present are the angiogenic proteins VEGF, basic FGF, and PDGF; the epithelial cell stimulatory proteins KGF and EGF; and the antiscarring proteins TGF-β3, IFN-α2, and HGF. Physiologic levels of growth factors and cytokines are critical to ensure healing of chronic wounds. The unique population of viable cells allows for the sustained release of a cocktail of growth factors, persisting at physiologic levels over extended periods and eliminating the need for frequent reapplication. Functionally, the skin substitutes have been shown to promote cell migration and wound closure in in vitro wound-healing assays.
Further investigation is also needed to elucidate the interac-tions between MSCs and the various immune and wound-healing cell types that are present in the wound bed because these studies would be useful to optimize the timing and dosage of MSC deliv-ery to the wound for maximal efficacy. The use of MSCs as a therapy presents advantages over pharmaceuticals, protein/growth factors, and committed progenitor cells because MSCs are able to interact with the surrounding cell types and biochemical environ-ment to express in a regulated manner the appropriate trophic factors for enhanced dermal wound healing. MSCs will likely emerge as an important therapy to reduce the formation of fibrotic tissue and the appearance of scars after cutaneous injury (Fig. 6-13).49
Bone marrow–derived or whole blood–derived endothelial progenitor cells are endothelial precursors and play a role in angio-genesis and vasculogenesis. These cells improve tissue perfusion by increasing neovascularization. Subsequently, these cells, which can secrete angiogenic factors such as VEGF, are potentially important in the treatment of numerous disease processes, includ-ing wound healing, myocardial infarction, vascular disease, and cancer.
From Maxson S, Lopez EA, Yoo D, et al: Concise review: Role of mesenchymal stem cells in wound repair. Stem Cells Transl Med 1:142–149, 2012.Acrp-30, Adiponectin; Ang-2, angiotensin-2; bFGF, basic fibroblast growth factor; EGF, epidermal growth factor; FGF-7, fibroblast growth factor-7; HB-EGF, heparin-bound epidermal growth factor; HGF, hepatocyte growth factor; IFN-α2, interferon-α2; IGF, insulin-like growth factor; IGFBP-1, -2, -3, insulin-like growth factor binding protein-1, -2, -3; IL-1Ra, interleukin-1 receptor antagonist; KGF, keratinocyte growth factor; LIF, leukemia inhibitory factor; MMP-1, -2, -3, -7, -8, -9, 10, -13, matrix metalloproteinase-1, -2, -3, -7, -8, -9, 10, -13; N-GAL, neutrophil gelatinase-associated lipocalin; PDGF, platelet-derived growth factor; PEDF, pigment epithelium-derived factor; PlGF, placenta growth factor; SDF-1β, stromal cell–derived factor 1β; TGF-α, transforming growth factor-α; TIMP-1, -2, tissue inhibitor of matrix metalloproteinase-1, -2; TPO, thrombopoietin; VEGF, vascular endothelial growth factor.
TABLE 6-7 Functional Classes of Wound-Healing Proteins in Human Mesenchymal Stem Cell–Containing Skin Substitutes
SPECIFIC PROTEINS PRIMARY FUNCTION
MMP-1, MMP-2, MMP-3, MMP-7, MMP-8, MMP-9, MMP-10, MMP-13 Matrix and growth factor degradation, facilitate cell migrationTIMP-1 and TIMP-2 Inhibit activity of MMPs, angiogenicAng-2, HB-EGF, EGF, FGF-7 (also known as KGF), PlGF, PEDF, TPO, TGF-α, IGF Stimulate growth and migrationbFGF, PDGF-AA, PDGF-AB, PDGF-BB, VEGF, VEGF-C, VEGF-D Promote angiogenesis, also proliferative and migration stimulatory effectsTGF-β3, HGF Inhibit scar and contracture formationIFN-α2 Prevent fibrosis by decreasing TGF-β1 and TGF-β2
α2-Macroglobulin Inhibit protease activity, coordinate growth factor bioavailabilityAcrp-30 Regulate growth and activity of keratinocytesIL-1Ra Anti-inflammatoryN-GAL AntibacterialLIF Support of angiogenic growth factorsSDF-1β Recruit cells to site of tissue damageIGFBP-1, IGFBP-2, IGFBP-3 Regulate IGF and its proliferative effects
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles160
Bello YM, Falabella AF, Eaglstein WH: Tissue-engineered skin. Current status in wound healing. Am J Clin Dermatol 2:305–313, 2001.
This article discusses the various skin substitutes available and their uses in wound healing.
Dang C, Ting K, Soo C, et al: Fetal wound healing current per-spectives. Clin Plast Surg 30:13–23, 2003.
This review article discusses the morphologic, cellular, and molecular aspects of scarless fetal wound healing.
Eming SA, Hammerschmidt M, Krieg T, et al: Interrelation of immunity and tissue repair or regeneration. Semin Cell Dev Biol 20:517–527, 2009.
This article reviews the complex role of the immune system in tissue repair and tissue regeneration.
management, and bacterial burden should be the standard of clinical practice and can be accomplished even in situations with limited resources.
SELECTED REFERENCESAlberts B, Johnson A, Lewis J, et al, editors: Cell junctions, cell adhesion, and the extracellular matrix. In The Molecular Biology of the Cell, ed 4, New York, 2002, Garland, pp 1091–1114.
This chapter provides a comprehensive review of matrix and integrin biology and the critical role of these in biologic pro-cesses, including tissue repair.
Barrientos S, Stojadinovic O, Golinko MS, et al: Growth factors and cytokines in wound healing. Wound Repair Regen 16:585–601, 2008.
This article reviews cytokines, growth factors, and chemo-kines in wound healing.
FIGURE 6-13 Mesenchymal stem cells (MSCs) can influence cutaneous regeneration by multiple distinct mechanisms acting on multiple cell types. HGF, Hepatic growth factor; RNS, reactive nitrogen species; ROS, reactive oxygen species. (From Jackson WM, Nesti LJ, Tuan RS: Mesenchymal stem cell therapy for attenu-ation of scar formation during wound healing. Stem Cell Res Ther 3:20, 2012.)
MSCs
Vascular endothelial cells
Keratinocytes
Fibroblasts
Dermal fibroblasts
Fibrocytes
1. Modulate T-cellbiology
6. Directdifferentiation
5. Promoteangiogenesis
4. Inhibit woundhealing fibroblasts
3. Anti-fibrosisfactors (e.g., HGF)
2. Neutralize ROS
ROS
T-cells
RNS
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

CHAPTER 6 Wound Healing 161
7. Engrav LH, Heimbach DM, Rivara FP, et al: 12-Year within-wound study of the effectiveness of custom pressure garment therapy. Burns 36:975–983, 2010.
8. Juckett G, Hartman-Adams H: Management of keloids and hypertrophic scars. Am Fam Physician 80:253–260, 2009.
9. Cooper JS, Lee BT: Treatment of facial scarring: Lasers, filler, and nonoperative techniques. Facial Plast Surg 25:311–315, 2009.
10. Yagmur C, Akaishi S, Ogawa R, et al: Mechanical receptor-related mechanisms in scar management: A review and hypothesis. Plast Reconstr Surg 126:426–434, 2010.
11. Davison SP, Dayan JH, Clemens MW, et al: Efficacy of intra-lesional 5-fluorouracil and triamcinolone in the treatment of keloids. Aesthet Surg J 29:40–46, 2009.
12. Rio E, Bardet E, Peuvrel P, et al: Perioperative interstitial brachytherapy for recurrent keloid scars. Plast Reconstr Surg 124:180e–181e, 2009.
13. Ogawa R, Yoshitatsu S, Yoshida K, et al: Is radiation therapy for keloids acceptable? The risk of radiation-induced carcino-genesis. Plast Reconstr Surg 124:1196–1201, 2009.
14. Cacao FM, Tanaka V, Messina MC: Failure of imiquimod 5% cream to prevent recurrence of surgically excised trunk keloids. Dermatol Surg 35:629–633, 2009.
15. Greaves NS, Iqbal SA, Baguneid M, et al: The role of skin substitutes in the management of chronic cutaneous wounds. Wound Repair Regen 21:194–210, 2013.
16. Shih B, Sultan MJ, Chaudhry IH, et al: Identification of biomarkers in sequential biopsies of patients with chronic wounds receiving simultaneous acute wounds: A genetic, his-tological, and noninvasive imaging study. Wound Repair Regen 20:757–769, 2012.
17. Sorensen LT, Toft BG, Rygaard J, et al: Effect of smoking, smoking cessation, and nicotine patch on wound dimension, vitamin C, and systemic markers of collagen metabolism. Surgery 148:982–990, 2010.
18. Thangarajah H, Yao D, Chang EI, et al: The molecular basis for impaired hypoxia-induced VEGF expression in diabetic tissues. Proc Natl Acad Sci U S A 106:13505–13510, 2009.
19. Hom DB, Ho V, Lee CKK: Irradiated skin and its postsurgi-cal management. In Hom DB, Hebda PA, Gosain AK, editors: Essential Tissue Healing of the Face and the Neck, Shelton, CT, 2009, BC Decker and People’s Medical Publish-ing House, pp 224–238.
20. Goessler UR, Bugert P, Kassner S, et al: In vitro analysis of radiation-induced dermal wounds. Otolaryngol Head Neck Surg 142:845–850, 2010.
21. Haubner F, Ohmann E, Pohl F, et al: Wound healing after radiation therapy: Review of the literature. Radiat Oncol 7:162, 2012.
22. Delanian S, Chatel C, Porcher R, et al: Complete restoration of refractory mandibular osteoradionecrosis by prolonged treatment with a pentoxifylline-tocopherol-clodronate com-bination (PENTOCLO): A phase II trial. Int J Radiat Oncol Biol Phys 80:832–839, 2011.
23. Freiberger JJ, Yoo DS, de Lisle Dear G, et al: Multimodality surgical and hyperbaric management of mandibular osteora-dionecrosis. Int J Radiat Oncol Biol Phys 75:717–724, 2009.
24. Jacobson AS, Buchbinder D, Hu K, et al: Paradigm shifts in the management of osteoradionecrosis of the mandible. Oral Oncol 46:795–801, 2010.
25. Kendall AC, Whatmore JL, Harries LW, et al: Changes in inflammatory gene expression induced by hyperbaric oxygen
Herdrich BJ, Lind RC, Liechty KW: Multipotent adult progenitor cells: Their role in wound healing and the treatment of dermal wounds. Cytotherapy 10:543–550, 2008.
This article provides a comprehensive review of the current state of stem cell therapy in wound healing.
Hunter JE, Teot L, Horch R, et al: Evidence-based medicine: Vacuum-assisted closure in wound care management. Int Wound J 4:256–269, 2007.
This article reviews negative-pressure wound closure using evidence-based medicine.
Juckett G, Hartman-Adams H: Management of keloids and hypertrophic scars. Am Fam Physician 80:253–260, 2009.
This article discusses current evidence-based treatment of keloids and hypertrophic scars.
Kulikovsky M, Gil T, Mettanes I, et al: Hyperbaric oxygen therapy for non-healing wounds. Isr Med Assoc J 11:480–485, 2009.
Negative-pressure wound closure topics and uses are reviewed.
Lionelli GT, Lawrence WT: Wound dressings. Surg Clin North Am 83:617–638, 2003.
This article provides a thorough discussion of classes and uses of wound dressings.
Singer AJ, Clark RAF: Cutaneous wound healing. N Engl J Med 341:738–746, 1999.
This article provides a comprehensive review of the cellular and molecular aspects of wound healing.
REFERENCES1. Goren I, Allmann N, Yogev N, et al: A transgenic mouse
model of inducible macrophage depletion: Effects of diph-theria toxin-driven lysozyme M-specific cell lineage ablation on wound inflammatory, angiogenic, and contractive pro-cesses. Am J Pathol 175:132–147, 2009.
2. Lucas T, Waisman A, Ranjan R, et al: Differential roles of macrophages in diverse phases of skin repair. J Immunol 184:3964–3977, 2010.
3. Mirza R, DiPietro LA, Koh TJ: Selective and specific macro-phage ablation is detrimental to wound healing in mice. Am J Pathol 175:2454–2462, 2009.
4. Voigt J, Driver VR: Hyaluronic acid derivatives and their healing effect on burns, epithelial surgical wounds, and chronic wounds: A systematic review and meta-analysis of randomized controlled trials. Wound Repair Regen 20:317–331, 2012.
5. Shih B, Bayat A: Genetics of keloid scarring. Arch Dermatol Res 302:319–339, 2010.
6. Gauglitz GG, Korting HC, Pavicic T, et al: Hypertrophic scarring and keloids: Pathomechanisms and current and emerging treatment strategies. Mol Med 17:113–125, 2011.
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.

SECTION I Surgical Basic Principles162
biologic scaffolds with and without a cellular component. Biomaterials 30:1482–1491, 2009.
40. Keane TJ, Londono R, Turner NJ, et al: Consequences of ineffective decellularization of biologic scaffolds on the host response. Biomaterials 33:1771–1781, 2012.
41. Valentin JE, Stewart-Akers AM, Gilbert TW, et al: Macro-phage participation in the degradation and remodeling of extracellular matrix scaffolds. Tissue Eng Part A 15:1687–1694, 2009.
42. Hwang JH, Shim SS, Seok OS, et al: Comparison of cyto-kine expression in mesenchymal stem cells from human pla-centa, cord blood, and bone marrow. J Korean Med Sci 24:547–554, 2009.
43. Maxson S, Lopez EA, Yoo D, et al: Concise review: Role of mesenchymal stem cells in wound repair. Stem Cells Transl Med 1:142–149, 2012.
44. Dash NR, Dash SN, Routray P, et al: Targeting nonhealing ulcers of lower extremity in human through autologous bone marrow-derived mesenchymal stem cells. Rejuvenation Res 12:359–366, 2009.
45. Lu D, Chen B, Liang Z, et al: Comparison of bone marrow mesenchymal stem cells with bone marrow-derived mono-nuclear cells for treatment of diabetic critical limb ischemia and foot ulcer: A double-blind, randomized, controlled trial. Diabetes Res Clin Pract 92:26–36, 2011.
46. Bieback K, Brinkmann I: Mesenchymal stromal cells from human perinatal tissues: From biology to cell therapy. World J Stem Cells 2:81–92, 2010.
47. Wolbank S, Hildner F, Redl H, et al: Impact of human amniotic membrane preparation on release of angiogenic factors. J Tissue Eng Regen Med 3:651–654, 2009.
48. Yew TL, Hung YT, Li HY, et al: Enhancement of wound healing by human multipotent stromal cell conditioned medium: The paracrine factors and p38 MAPK activation. Cell Transplant 20:693–706, 2011.
49. Jackson WM, Nesti LJ, Tuan RS: Mesenchymal stem cell therapy for attenuation of scar formation during wound healing. Stem Cell Res Ther 3:20, 2012.
treatment in human endothelial cells under chronic wound conditions. Exp Cell Res 318:207–216, 2012.
26. Thom SR: Hyperbaric oxygen: Its mechanisms and efficacy. Plast Reconstr Surg 127(Suppl 1):131S–141S, 2011.
27. Sgonc R, Gruber J: Age-related aspects of cutaneous wound healing: A mini-review. Gerontology 59:159–164, 2013.
28. Macri L, Clark RA: Tissue engineering for cutaneous wounds: Selecting the proper time and space for growth factors, cells and the extracellular matrix. Skin Pharmacol Physiol 22:83–93, 2009.
29. Kulikovsky M, Gil T, Mettanes I, et al: Hyperbaric oxygen therapy for non-healing wounds. Isr Med Assoc J 11:480–485, 2009.
30. Goldman RJ: Hyperbaric oxygen therapy for wound healing and limb salvage: A systematic review. PM R 1:471–489, 2009.
31. Kuffler DP: Hyperbaric oxygen therapy: An overview. J Wound Care 19:77–79, 2010.
32. Wu SC, Marston W, Armstrong DG: Wound care: The role of advanced wound healing technologies. J Vasc Surg 52:59S–66S, 2010.
33. Wang S, Qu X, Zhao RC: Mesenchymal stem cells hold promise for regenerative medicine. Front Med 5:372–378, 2011.
34. Prockop DJ, Oh JY: Mesenchymal stem/stromal cells (MSCs): Role as guardians of inflammation. Mol Ther 20:14–20, 2012.
35. Kong W, Li S, Lorenz HP: Germ plasm-like Dot cells main-tain their wound regenerative function after in vitro expan-sion. Clin Exp Pharmacol Physiol 37:e136–e144, 2010.
36. Leung A, Crombleholme TM, Keswani SG: Fetal wound healing: Implications for minimal scar formation. Curr Opin Pediatr 24:371–378, 2012.
37. Lazic T, Falanga V: Bioengineered skin constructs and their use in wound healing. Plast Reconstr Surg 127(Suppl 1):75S–90S, 2011.
38. Auger FA, Lacroix D, Germain L: Skin substitutes and wound healing. Skin Pharmacol Physiol 22:94–102, 2009.
39. Brown BN, Valentin JE, Stewart-Akers AM, et al: Macro-phage phenotype and remodeling outcomes in response to
Descargado de ClinicalKey.es desde Universidad Nacional Autonoma de Mexico agosto 09, 2016.Para uso personal exclusivamente. No se permiten otros usos sin autorización. Copyright ©2016. Elsevier Inc. Todos los derechos reservados.