Embed Size (px)
Citation preview

Chapter 9Chapter 9
Care of the Patient with a
Respiratory Disorder
Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Slide 2Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• External respiration Exchange of oxygen and carbon dioxide between the
lung and the environment
• Internal respiration Exchange of oxygen and carbon dioxide at the cellular
level

Slide 3Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• Upper respiratory tract Nose Pharynx Larynx Trachea
• Lower respiratory tract Bronchial tree
• Bronchioles, alveolar ducts, alveoli

Slide 4Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Mechanics of breathing Thoracic cavity
• Lungs Visceral pleura and parietal pleura
• Respiratory movements and ranges Rhythmic movements of the chest walls, ribs, and
muscles allow air to be inhaled and exhaled
• Regulation of respiration Nervous control—medulla oblongata and pons of the
brain; chemoreceptors—in the carotid and aorta
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology

Slide 5Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Overview of Anatomy and PhysiologyOverview of Anatomy and Physiology
• Respiratory Movements and Ranges Room air when inhaled= 21% Oxygen
• Exhaled air= 16% oxygen Normal Respirations
• Adult= `4-20 bpm
• Newborn= 40-60 bpm
• Early school age child= 22-24 bpm
• Teenager= 20-22 bpm Rate can be affected by many variables
• Sex, age, activity, disease, body temperature, etc.
• Count without patient’s awareness to prevent alteration in breathing pattern

Slide 6Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Assessment of the Respiratory SystemAssessment of the Respiratory System
• Subjective data Shortness of breath, dyspnea, cough
• Objective data Expression, chest movement, and respirations Respiratory distress, wheezes, or orthopnea Adventitious breath sounds
• Sibilant wheezes
• Sonorous wheezes
• Crackles
• Pleural friction rubs

Slide 7Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Laboratory and Diagnostic ExaminationsLaboratory and Diagnostic Examinations
• Chest roentgenogram (CXR)• Computed tomography (CT)• Pulmonary function testing• Mediastinoscopy• Laryngoscopy• Bronchoscopy• Sputum specimen• Cytological studies• Thoracentesis • Arterial blood gases (ABG)• Pulse oximetry

Slide 8Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 9-7Figure 9-7
Fiberoptic bronchoscope.
(A, Courtesy of Olympus America, Melville, New York. B, from Meduri, G.U., et al. [1991]. Protected bronchoalveolar lavage, American Review of Respiratory Disease, 143:855, official journal of the
American Thoracic Society, © American Lung Association.)

Slide 9Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 9-8Figure 9-8
Thoracentesis.
(From Lewis, S.M., Heitkemper, M.M., Dirksen, S.R. [2007]. Medical-surgical nursing: assessment and management of clinical problems. [7th ed.]. St. Louis: Mosby.)

Slide 10Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 9-9Figure 9-9
Portable pulse oximeter with spring-tension digit probe displays
oxygen saturation and pulse rate.
(From Potter, P.A., Perry, A.G. [2009]. Fundamentals of nursing. [7th ed.]. St. Louis: Mosby.)

Slide 11Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Epistaxis Etiology/pathophysiology
• Bleeding from the nose
• Congestion of the nasal membranes leading to capillary rupture
• Primary or secondary Clinical manifestations/assessment
• Bright red bleeding from one or both nostrils
• Can lose as much as 1 liter per hour

Slide 12Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Epistaxis (continued) Medical management/nursing interventions
• Sitting position, leaning forward
• Direct pressure by pinching nose
• Ice compresses to nose
• Nasal packing
• Cautery
• Balloon tamponade

Slide 13Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Deviated septum and nasal polyps Etiology/pathophysiology
• Congenital abnormality
• Injury
• Nasal septum deviates from the midline and can cause a partial obstruction
• Nasal polyps are tissue growths usually due to prolonged inflammation

Slide 14Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Deviated septum and nasal polyps (continued) Clinical manifestations/assessment
• Stertorous respirations (snoring)
• Dyspnea
• Postnasal drip Medical management/nursing interventions
• Pharmacological management Corticosteroids, antihistamines, antibiotics, analgesics
• Nasoseptoplasty
• Nasal polypectomy

Slide 15Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Allergic rhinitis and allergic conjunctivitis (hay fever) Etiology/pathophysiology
• Antigen/antibody reactions in the nasal membranes, nasopharynx, and conjunctiva due to allergens
Diagnostic testing • Allergy testing to determine cause may be helpful
Can be done by skin testing or serum radioallergosorbent test

Slide 16Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Allergic rhinitis and allergic conjunctivitis (continued) Clinical manifestations/assessment
• Edema
• Photophobia
• Excessive tearing
• Blurring of vision
• Pruritus
• Excessive nasal secretions and/or congestion
• Sneezing
• Cough
• Headache

Slide 17Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Allergic rhinitis and allergic conjunctivitis (continued) Diagnostic testing Medical management/nursing interventions
• Pharmacological management Antihistamines Decongestants Corticosteroids Analgesics
• Avoid allergen
• Hot packs over facial sinuses

Slide 18Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 9-3Figure 9-3
Projections of paranasal sinuses and oral nasal cavities on the skull and
face.
(From Thibodeau, G.A., Patton, K.T. [2008]. Structure and function of the body. [13th ed.]. St. Louis: Mosby.)

Slide 19Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Obstructive sleep apnea (OSA) Etiology and pathophysiology
• Characterized by partial or complete upper airway obstruction during sleep
• Apnea refers to the cessation of spontaneous respirations
• Hypopnea is the presence of unusually shallow or slow respirations

Slide 20Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Obstructive sleep apnea (OSA) Clinical manifestations
• Frequent awakening at night
• Insomnia
• Excessive daytime fatigue
• Witnessed apneic episodes
• Loud snoring
• Hypercapnia
• Personality changes
• Irritability

Slide 21Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Obstructive sleep apnea (continued) Complications
• Systemic HTN, cardiac dysrhythmia, heart failure, nocturnal hypoexmia, stroke
Diagnostic tests• Polysomnography (sleep study)
Medical management/nursing interventions• Avoid sedatives
• Avoid alcoholic beverages
• Support groups
• Oral appliances
• nCPAP
• Surgery

Slide 22Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Upper airway obstruction Etiology and pathophysiology
• Precipitated by a recent respiratory event
• Common airway obstructions Choking on food Dentures Aspiration of vomitus or secretions The tongue

Slide 23Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Upper airway obstruction (continued) Clinical manifestations/assessment
• Stertorous respirations
• Altered respiratory rate and character; apneic periods
• Hypoxia; cyanosis
• Wheezing; stridor Medical management/nursing interventions
• Open the airway
• Remove obstruction
• Artificial airway; tracheostomy

Slide 24Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Cancer of the larynx Etiology/pathophysiology
• Squamous cell carcinoma
• Heavy smoking and alcohol use
• Chronic laryngitis
• Vocal abuse
• Family history

Slide 25Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Upper AirwayDisorders of the Upper Airway
• Cancer of the larynx (continued) Clinical manifestations/assessment
• Progressive or persistent hoarseness
• Pain radiating to the ear
• Difficulty swallowing
• Hemoptysis Medical management/nursing interventions
• Radiation
• Surgery Partial or total laryngectomy Radical neck dissection

Slide 26Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Acute rhinitis (common cold) Etiology/pathophysiology
• Inflammation of the mucous membranes of the nose and accessory sinuses
• Virus(es) Clinical manifestations/assessment
• Thin, serous nasal exudate
• Productive cough
• Sore throat
• Fever

Slide 27Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Acute rhinitis (common cold) (continued) Medical management/nursing interventions
• Pharmacological management Analgesic Antipyretic Cough suppressant Expectorant Antibiotic (if infection present)
• No specific treatment
• Encourage fluids

Slide 28Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Acute follicular tonsillitis Etiology/pathophysiology
• Inflammation of the tonsils
• Bacterial or viral infection Clinical manifestations/assessment
• Enlarged, tender, cervical lymph nodes
• Sore throat
• Fever; chills
• Enlarged, purulent tonsils
• Elevated WBC

Slide 29Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Acute follicular tonsillitis (continued) Medical management/nursing interventions
• Pharmacological management Antibiotics; analgesics; antipyretics
• Warm saline gargles
• Tonsillectomy and adenoidectomy Postoperative
o Assess for excessive bleedingo Ice-cold liquids—ice creamo Ice collaro Avoid coughing, sneezing, or vigorous nose blowing

Slide 30Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Laryngitis Etiology/pathophysiology
• Inflammation of the larynx due to virus or bacteria
• May cause severe respiratory distress in children under 5 years old
Clinical manifestations/assessment• Hoarseness
• Voice loss
• Scratchy and irritated throat
• Persistent cough

Slide 31Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Laryngitis (continued) Medical management/nursing interventions
• Pharmacological management Analgesics Antipyretics Antitussives Antibiotics—bacterial
• Viral—no specific treatment, supportive care
• Warm or cool mist vaporizer
• Limit use of voice

Slide 32Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Pharyngitis Etiology/pathophysiology
• Inflammation of the pharynx
• Chronic or acute
• Frequently accompanies the common cold
• Viral, most common
• Bacterial

Slide 33Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Pharyngitis (continued) Clinical manifestations/assessment
• Dry cough
• Tender tonsils
• Enlarged cervical lymph glands
• Red, sore throat
• Fever Medical management/nursing interventions
• Pharmacological management Antibiotics; analgesics; antipyretics
• Warm or cool mist vaporizer

Slide 34Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Sinusitis Etiology/pathophysiology
• Inflammation of the sinuses
• Usually begins with an upper respiratory infection; viral or bacterial
Clinical manifestations/assessment• Constant, severe headache
• Pain and tenderness in involved sinus region
• Purulent exudate
• Malaise
• Fever

Slide 35Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Respiratory InfectionsRespiratory Infections
• Sinusitis (continued) Medical management/nursing interventions
• Pharmacological management Antibiotics Analgesics Antihistamines
• Vasoconstrictor nasal spray (Afrin)
• Warm mist vaporizer
• Warm, moist packs
• Nasal windows

Slide 36Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute bronchitis Etiology/pathophysiology
• Inflammation of the trachea and bronchial tree
• Usually secondary to upper respiratory infection
• Exposure to inhaled irritants Clinical manifestations/assessment
• Productive cough; wheezes
• Dyspnea; chest pain
• Low-grade fever
• Malaise; headache

Slide 37Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute bronchitis (continued) Medical management/nursing interventions
• Pharmacological management Cough suppressants Antitussives Antipyretics Bronchodilators Antibiotics
• Vaporizer
• Encourage fluids

Slide 38Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Legionnaires’ disease Etiology/pathophysiology
• Legionella pneumophila
• Thrives in water reservoirs
• Causes life-threatening pneumonia
• Leads to respiratory failure, renal failure, bacteremic shock, and ultimately death

Slide 39Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Legionnaires’ disease (continued) Clinical manifestations/assessment
• Elevated temperature
• Headache
• Nonproductive cough
• Difficult and rapid respirations
• Crackles or wheezes
• Tachycardia
• Signs of shock
• Hematuria

Slide 40Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Legionnaires’ disease (continued) Medical management/nursing interventions
• Pharmacological management Antibiotics Antipyretics Vasopressors
• Oxygen
• Mechanical ventilation, if necessary
• IV therapy

Slide 41Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Severe Acute Respiratory Syndrome (SARS) Etiology/pathophysiology
• Infection caused by coronavirus
• Spread by close contact between people
• Airborne
• May be spread by touching contaminated objects Clinical manifestations/assessment
• Temperature
• Headache
• Muscle aches
• Mild respiratory symptoms Dry cough and SOB

Slide 42Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Adult respiratory distress syndrome (continued) Diagnostic tests
• Chest radiograph
• Serum antibody testing
• Nasopharyngeal and oropharyngeal swabs Medical management/nursing interventions
• Pharmacological management Antibiotics Antiviral medications
• Respiratory isolation
• Oxygen

Slide 43Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Anthrax Etiology/pathophysiology
• Bacillus anthracis
• Spread by direct contact with bacteria or spores
• Three types: Cutaneous, GI, inhalational Clinical manifestations/assessment
• Cold or flu-like symptoms
• Hemorrhage, tissue necrosis, and lymphedema Medical management
• Antibiotics

Slide 44Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Tuberculosis Etiology/pathophysiology
• Inhalation of tubercle bacillus (Mycobacterium tuberculosis)
• Infection versus active disease
• Presumptive diagnosis Mantoux tuberculin skin test Chest x-ray film Acid-fast bacilli smear 3
• Confirmed diagnosis Sputum culture; positive for TB bacilli

Slide 45Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Tuberculosis (continued) Clinical manifestations/assessment
• Fever
• Weight loss; weakness
• Productive cough; hemoptysis
• Chills; night sweats Medical management/nursing interventions
• Tuberculosis isolation (acid-fast bacilli [AFB])
• Multiple medications to which the organisms are susceptible

Slide 46Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pneumonia Etiology/pathophysiology
• Inflammatory process of the bronchioles and the alveolar spaces due to infection
• Bacteria, viruses, mycoplasma, fungi, and parasites Clinical manifestations/assessment
• Productive cough
• Severe chills; elevated temperature
• Increased heart rate and respiratory rate
• Dyspnea

Slide 47Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pneumonia (continued) Medical management/nursing interventions
• Pharmacological management Antibiotics Analgesics Expectorants Bronchodilators
• Oxygen
• Chest percussion and postural drainage
• Encourage to cough and deep-breathe
• Humidifier or nebulizer

Slide 48Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pleurisy Etiology/pathophysiology
• Inflammation of the visceral and parietal pleura
• Bacterial or viral Clinical manifestations/assessment
• Sharp inspiratory pain
• Dyspnea
• Cough
• Elevated temperature
• Pleural friction rub

Slide 49Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pleurisy (continued) Medical management/nursing interventions
• Pharmacological management Antibiotics Analgesics Antipyretics
• Oxygen
• Anesthetic block for intercostal nerves

Slide 50Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pleural effusion/empyema Etiology/pathophysiology
• Pleural effusion
• Accumulation of fluid in the pleural space
• Empyema—infection Clinical manifestations/assessment
• Dyspnea
• Air hunger
• Respiratory distress
• Fever

Slide 51Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pleural effusion/empyema (continued) Medical management/nursing interventions
• Thoracentesis
• Chest tube with closed water-seal drainage system
• Antibiotics
• Cough and deep-breathe

Slide 52Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Atelectasis Etiology/pathophysiology
• Collapse of lung tissue due to occlusion of air to a portion of the lung
Clinical manifestations/assessment• Dyspnea; tachypnea
• Pleural friction rub; crackles
• Restlessness
• Elevated temperature
• Decreased breath sounds

Slide 53Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Atelectasis (continued) Medical management/nursing interventions
• Pharmacological management Bronchodilators Antibiotics Mucolytic agents Analgesics
• Cough and deep-breathe• Early ambulation• Respiratory treatments
Incentive spirometry; intermittent positive-pressure breathing (IPPB)
Oxygen Chest percussion and postural drainage
• Chest tube

Slide 54Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pneumothorax Etiology/pathophysiology
• A collection of air or gas in the pleural space, causing the lung to collapse
Clinical manifestations/assessment• Decreased breath sounds
• Sudden, sharp chest pain with dyspnea
• Diaphoresis; tachycardia; tachypnea
• No chest movement on affected side
• Sucking chest wound

Slide 55Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 9-13Figure 9-13
Pneumothorax (complete collapse of the right lung).
(From Wilson, S., Thompson, J. [1991]. Respiratory disorders, Mosby’s clinical nursing series. St. Louis: Mosby.)

Slide 56Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pneumothorax (continued) Medical management/nursing interventions
• Chest tube to water-seal drainage system
• Oxygen
• Analgesics
• Encourage fluids

Slide 57Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Lung cancer Etiology/pathophysiology
• Primary tumor or metastasis
• Small-cell, non–small-cell, squamous cell, and large-cell carcinoma
Clinical manifestations/assessment• Hemoptysis
• Dyspnea; wheezing
• Fever; chills
• Pleural effusion

Slide 58Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Lung cancer (continued) Medical management/nursing interventions
• Surgery Most are not diagnosed early enough for curative
surgical intervention Segmental resection Lobectomy Pneumonectomy
• Radiation
• Chemotherapy

Slide 59Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pulmonary edema Etiology/pathophysiology
• Accumulation of serous fluid in interstitial tissue and alveoli
Clinical manifestations/assessment• Dyspnea; cyanosis
• Tachypnea; tachycardia
• Pink or blood-tinged, frothy sputum
• Restlessness; agitation
• Wheezing; crackles
• Decreased urinary output; sudden weight gain

Slide 60Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pulmonary edema (continued) Medical management/nursing interventions
• Pharmacological management Diuretics Narcotic analgesics Nipride
• Oxygen
• Mechanical ventilation, if necessary
• Strict I&O; daily weight
• Low-sodium diet

Slide 61Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pulmonary embolism Etiology/pathophysiology
• Foreign substance in the pulmonary artery Blood clot, fat, air, or amniotic fluid
Clinical manifestations/assessment• Sudden, unexplained dyspnea, tachypnea
• Hemoptysis
• Chest pain
• Elevated temperature
• Increased WBCs

Slide 62Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Pulmonary embolism (continued) Medical management/nursing interventions
• Pharmacological management Anticoagulants Fibrinolytic agents
• Oxygen
• HOB up 30 degrees

Slide 63Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute respiratory distress syndrome (ARDS) Etiology and pathophysiology
• Results from direct or indirect pulmonary injury
• Alveolar capillary membranes are altered resulting increased permeability creating pulmonary edema and hypoxia

Slide 64Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute respiratory distress syndrome (continued) Clinical manifestations
• Respiratory distress
• Changes in level of consciousness
• Tachycardia
• Hypotension
• Decreased urinary output

Slide 65Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute respiratory distress syndrome (continued) Medical management/nursing interventions
• Pharmacological management Corticosteroids Antibiotics Vasodilators Bronchodilators Mucolytics Diuretics Morphine sulfate Neurologic blocking agents Cardiotonic glycosides (digoxin)

Slide 66Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Disorders of the Lower AirwayDisorders of the Lower Airway
• Acute respiratory distress syndrome (continued) Medical management/nursing interventions
(continued)• Oxygen
• Position changes
• Close assessment of vital signs

Slide 67Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)
• Emphysema Etiology/pathophysiology
• The bronchi, bronchioles, and alveoli become inflamed as a result of chronic irritation
• Air becomes trapped in the alveoli during expiration, causing alveolar distention, rupture, and scar tissue
Complication• Cor pulmonale
Right-sided congestive heart failure due to pulmonary hypertension

Slide 68Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
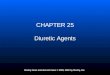
Figure 9-14Figure 9-14
Disorders of the airways in patients with chronic bronchitis, asthma, and emphysema.
(From Lewis, S.M., Collier, I., & Heitkemper, M.M. [1996]. Medical-surgical nursing: assessment and management of clinical problems. [4th ed.]. St. Louis: Mosby.)

Slide 69Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Emphysema (continued) Clinical manifestations/assessment
• Dyspnea on exertion
• Sputum
• Barrel chest
• Chronic weight loss
• Emaciation
• Clubbing of fingers
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 70Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Figure 9-16Figure 9-16
Barrel chest. Note increase in AP diameter.

Slide 71Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Emphysema (continued) Medical management/nursing interventions
• Pharmacological management Bronchodilators; corticosteroids; antibiotics; diuretics
• Oxygen (low-flow)
• Chest physiotherapy
• Humidifier
• Pursed-lip breathing
• High-protein, high-calorie diet
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 72Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Chronic bronchitis Etiology/pathophysiology
• Hypertrophy of mucous glands causes hypersecretion and alters cilia function
• Increased airway resistance causes bronchospasm Clinical manifestations/assessment
• Productive cough
• Dyspnea
• Use of accessory muscles to breathe
• Wheezing
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 73Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Chronic bronchitis (continued) Medical management/nursing interventions
• Pharmacological management Bronchodilators Mucolytics Antibiotics
• Oxygen (low-flow)
• Pursed-lip breathing
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 74Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Asthma Etiology/pathophysiology
• Narrowing of the airways due to various stimuli
• Extrinsic or intrinsic factors
• Influenced by secondary factors
• Antigen-antibody reaction
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 75Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Asthma (continued) Clinical manifestations/assessment
• Mild asthma Dyspnea on exertion Wheezing
• Acute asthma attack Tachypnea Expiratory wheezing; productive cough Use of accessory muscles; nasal flaring Cyanosis
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 76Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Asthma (continued) Medical management/nursing interventions
• Maintenance therapy Serevent inhalant, prophylactic Corticosteroid inhalant Avoid allergens
• Acute or rescue therapy Proventil inhalant; aminophylline IV Corticosteroid and epinephrine oral or subcutaneous Oxygen
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 77Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Bronchiectasis Etiology/pathophysiology
• Gradual, irreversible process that involves chronic dilation of bronchi resulting in loss of elasticity
Clinical manifestations/assessment• Dyspnea; coughing; wheezes and crackles
• Cyanosis; clubbing of fingers
• Fatigue; weakness
• Loss of appetite
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 78Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Bronchiectasis (continued) Medical management/nursing interventions
• Pharmacological management Mucolytic agents Antibiotics Bronchodilators
• Oxygen (low-flow)
• Chest physiotherapy
• Hydration
• Cool mist vaporizer
• Surgery: Lobectomy
Chronic Obstructive Pulmonary Disease (COPD)Chronic Obstructive Pulmonary Disease (COPD)

Slide 79Mosby items and derived items © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
• Nursing diagnoses Airway clearance, ineffective Breathing pattern, ineffective Gas exchange, impaired Anxiety Activity intolerance Nutrition, imbalanced: less than body requirements
Nursing ProcessNursing Process

Chapter 11
Allergy and Respiratory Medications
80Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Chapter 11
Lesson 11.1
81Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Learning Objectives
Identify major antihistamines used to treat breathing problems
Describe the action of antitussive medications List medications used to treat and prevent
asthma attacks
82Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Learning Objectives (cont.)
Describe the major actions and the adverse reactions of the two main categories of bronchodilators
83Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Respiratory System
Upper Respiratory System Oral and nasal cavity, sinuses, pharynx, larynx,
and trachea Lower Respiratory System
Right and left bronchi, right and left lungs, bronchioles, and alveoli
84Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antihistamines
Six Major Groups Action
Compete with histamine for H1 receptor sites to limit its effectiveness
Limits vasodilation, capillary permeability, and swelling
Limits acetylcholine release, which dries secretions in the bronchioles and gastrointestinal system
Sedative effect on the CNS
85Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antihistamines (cont.)
Uses Seasonal allergic rhinitis (SAR) Perennial allergic rhinitis (PAR) Perennial nonallergic rhinitis (PNAR) Relieve symptoms of allergic disorders Adjunctive therapy for anaphylaxis Sedation
86Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antihistamines (cont.)
Adverse Reactions Changes in blood pressure, blurred vision Tachycardia, insomnia, dry mouth, nausea Restlessness, excitability, sedation, tinnitus
Drug Interactions Nursing Process
87Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antihistamines
Life span considerations Pediatrics:
Infants and young children often have anticholinergic side/adverse effects
Paradoxical reactions may occur: increased nervousness, confusion, or hyperexcitability
Elderly More likely to develop side effects such as dizziness,
syncope (fainting), confusion, and extrapyramidal reactions
88Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Question 1
Which of the following is NOT an adverse reaction that may develop from taking antihistamines?
1. Hypertension
2. Hypotension
3. Tachycardia
4. Bradycardia
89Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antitussives
Actions: Depress the cough center in the brain Anesthetize stretch receptors in the respiratory
tract Soothe irritated areas in the throat
Uses: Relief of overactive or nonproductive cough
90Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antitussives (cont.)
Adverse Reactions Constipation, drowsiness, dry mouth, nausea,
postural hypotension Drug Interactions Nursing Process
91Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Question 2
Which of the following is NOT a way that antitussives relieve cough?
1. Act centrally on the cough center in the brain
2. Act peripherally by anesthetizing stretch receptors in the respiratory tract
3. Act locally, primarily by soothing irritated areas in the throat
4. Act systemically to change the expiratory response
92Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Asthma
Asthma is a condition that involves increased inflammation, swelling, and mucus production that lead to bronchiolar constriction. The person is able to breathe air into the lungs but has difficulty breathing out. Wheezing results because the person works to force air out through narrowed, mucus-filled passages during expiration.
The four classes of asthma severity include mild intermittent, mild persistent, moderate persistent, and severe persistent.
93Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

COPD
COPD is a chronic, disabling disorder that causes destruction of alveolar walls. This destruction creates unequal areas of ventilation and perfusion in the body, and oxygen and carbon dioxide exchange is impaired. Patients experience difficulty in expiration.
94Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Asthma and COPD Medications
Prophylactic treatment• Cromolyn sodium
• Nedocromil sodium
Actions:• Slows down destruction of sensitized mast
cells; also may provide hyposensitization (decrease in allergic response)
95Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Asthma and COPD Medications (cont.)
Bronchodilators Sympathomimetics
• Relax smooth muscle of bronchi (dilate)
• Vasoconstriction of blood vessels in body (decreases mucosal and submucosal edema)
• Increase the rate and force of heart contraction
Uses:• Relief of symptoms of bronchospasm in acute or chronic
asthma, bronchitis, and COPD
96Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Asthma and COPD Medications (cont.)
Xanthines• Relax smooth muscle in the bronchi and blood vessels in
the lungs• Directly act on the kidney to produce an increase in
urine production• CNS effects
Uses• Adjunctive therapy for bronchospasm in acute and
chronic bronchial asthma, bronchitis, emphysema• Treatment of neonatal apnea• Acute pulmonary edema
97Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Asthma and COPD Medications (cont.)
Leukotriene Receptor Inhibitors Reduce symptoms of asthma by blocking
receptors for cysteinyl leukotrienes C4, D4, and E4
Uses Treat acute or chronic asthma in patients unable
to take inhaled glucocorticoids
98Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Asthma and COPD Medications (cont.)
Corticosteroids Block reaction to allergens and reduce airway
hyperresponsiveness Inhibit cytokine production, protein activation, and
inflammatory cell migration and activation Uses
Inhaled, long-term asthma control Systemic; often used to get quick control of the
disease when beginning long-term therapy or to speed recovery from severe episodes
99Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Question 3
____________________ is a slowly worsening, disabling disorder that is diagnosed by abnormal tests of expiratory flow.
1. Asthma
2. Bronchitis
3. Chronic obstructive pulmonary disease (COPD)
4. Congestive heart failure100Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Chapter 11
Lesson 11.2
101Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Learning Objectives
Identify at least six medications commonly used as decongestants
Describe the mechanism of action for expectorants
List the major contraindications to the use of nasal steroids
102Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Decongestants
Decongestants Directly affect alpha receptors of blood vessels in
the nasal mucosa, causing vasoconstriction Uses: relieve nasal congestion from allergies and
upper respiratory infections
103Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Expectorants
Expectorants Decrease the thickness of respiratory secretions,
thereby facilitating expectoration Uses: treat productive cough, assist with thick
mucus
104Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Topical Intranasal Steroids
Action Antiinflammatory, reduce nasal congestion
Uses Treatment of allergic, mechanical, or chemically
induced local nasal inflammation or nasal polyps when usual treatment has failed to work
Adverse reactions Asthma, headache, lightheadedness, loss of
sense of smell, nasal irritation and dryness, nausea, nosebleeds, perforation of nasal septum, altered sense of taste and smell
105Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Complementary and Alternative Therapies
Allergy Grape seed, stinging nettle, coleus, vitamin C
Asthma Cordyceps, Tylophora, grape seed, coleus, vitamin C
Cold Arabinoxylane, echinacea, elderberry, astragalus,
goldenseal, grapefruit seed extract, zinc, vitamin C Cough
Ground ivy, thyme, licorice, marshmallow
106Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Chapter 12
Antiinfective Medications
Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc. 107

Chapter 12
Lesson 12.1
108Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Learning Objectives
Identify the major antiinfective drug categories and the organisms against which they are effective
Outline the most important things to teach the patient who is taking antiinfective drugs
109Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Learning Objectives (cont.)
Define "spectrum" and explain what this word means in antiinfective therapy
List some of the most common adverse reactions to medications used to treat infections
110Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Overview
Pathogen Bacteria Fungi Viruses Antimicrobials
111Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antibiotics
Broad-spectrum Narrow-spectrum Adverse reactions
112Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Penicillins
Main antibiotic for years Overuse Penicillin-resistant strains Broad-spectrum drug of choice
113Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Penicillins (cont.)
Action and Uses Interferes with creation of the mucopeptide
cell wall Used to treat multiple infections Overuse and allergies
114Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Penicillins (cont.)
Adverse Reactions Neuropathy
High parenteral doses Skin eruptions GI symptoms Urticaria Laryngeal edema Anaphylaxis
Drug Interactions
115Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Penicillins (cont.)
Nursing Implications and Patient Teaching Assessment
Signs of infection and allergies Diagnosis Planning
10-day regimen Implementation
Route of administration Evaluation Patient Teaching
116Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Tetracyclines
Actions and uses Broad-spectrum antibioticsAdverse Reactions GI upsetNursing Implications Not for pregnant patients or children under 8 years of
age Can cause sensitivity to light (photosensitivity) so
counsel patient about careful sun exposure Take on empty stomach and avoid dairy within 2 hours
of taking drug.
117Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Macrolides
Actions and uses Alternative for pencillinAdverse Reactions GI upsetNursing Implications Check nursing text for drug interactions: there are
several! Advise patient to take with food and drink extra fluids
118Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Sulfonamides
Broad-spectrum antiinfective Bacteriostatic action: inhibits folic acid
synthesis in the cell
119Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Sulfonamides (cont.)
Action and Uses Urinary tract infections Effectively treats multiple microorganisms Preoperative and postoperative therapy for
bowel surgery
120Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Sulfonamides (cont.)
Adverse Reactions
Drug Interactions Potentiate Decrease effectiveness
Nursing Implications and Patient Teaching Contraindications
121Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Broad-Spectrum Antibiotics
Bactericidal or bacteriostatic
122Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Broad-Spectrum Antibiotics (cont.)
Action and Uses Large number of unrelated drugs used to
treat infections caused by a wide range of susceptible organisms
Gram-positive or gram-negative organisms
123Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Broad-Spectrum Antibiotics (cont.)
Adverse Reactions Superinfections Drug interactions are individualized Food interactions Affected organs: auditory nerves, kidneys, and
liver Cross-sensitivityNursing Implications and Patient Teaching
124Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Question 1
____________________ are plant-like organisms growing in irregular masses, without roots, stems, or leaves and without chlorophyll or other pigments involved in photosynthesis.
1. Bacteria2. Fungi3. Viruses4. Parasites
125Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Question 2
____________________ are usually used to treat acute and chronic urinary tract infections, particularly cystitis, pyelitis, and pyelonephritis, when these infections are caused by Escherichia coli or Nocardia asteroides.
1. Penicillins2. Sulfonamides3. Cephalosporins4. Aminoglycosides
126Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Question 3
An organism that causes an infection is a(n):
1. Teratogen.2. Pathogen.3. Allergen.4. Hydrogen.
127Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Chapter 12
Lesson 12.2
128Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Learning Objectives
Identify the major antiinfective drug categories and the organisms against which they are effective
Outline the most important things to teach the patient who is taking antiinfective drugs
List some of the most common adverse reactions to medications used to treat infections
129Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antitubercular Drugs
Overview Underdeveloped nations Risks Etiology: Mycobacterium tuberculosis
130Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antitubercular Drugs (cont.)
Action and Uses Most antitubercular drugs are bacteriostatic;
they have intracellular or extracellular effects that prevent the organism from building new cell walls, thus limiting growth and spread
Some antitubercular drugs are bactericidal Length of treatment Chemoprophylaxis Box 12-1 High-Priority Candidates for
Tuberculosis-Preventive Therapy
131Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antitubercular Drugs (cont.)
Adverse Reactions Common symptoms Toxicity: body sites affected Combination therapy Drug-specific symptoms
132Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antitubercular Drugs (cont.)
Drug Interactions Use of other drugs during therapyNursing Implications and Patient Teaching Assessment Diagnosis
History, chest x-ray, labs Additional patient needs
Planning Length of treatment
Implementation Dose
Evaluation Patient and Family Teaching
133Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antiparasitic Drugs
Amebicides Anthelmintics Antimalarials
134Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Amebicides
Entamoeba histolytica Relationship to traveling Infection sites in the body
135Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Amebicides (cont.)
Action and Uses Destroy invading amoebae Treatment of intestinal and extraintestinal
amebiasis. Drug choice depends on location
136Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Amebicides (cont.)
Adverse Reactions Common: nausea, vomiting, anorexia,
diarrhea, GI distress, hepatic abscess Drug-specific adverse reactions Overdose
137Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Amebicides (cont.)
Drug Interactions Nursing Implications Patient Teaching
138Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Anthelmintics
Helminthiasis: infestation by worms Common infestations:
Pinworms Roundworms Hookworms Tapeworms Whipworms
139Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Anthelmintics (cont.)
Action and Uses Action is drug specific Drugs used:
Thiabendazole Niclosamide and paromomycin Piperazine and pyrantel pamoate Diethylcarbamazine citrate Mebendazole
140Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Anthelmintics (cont.)
Adverse Reactions Drug specific Allergic reaction due to dead microfilaria
141Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Anthelmintics (cont.)
Drug InteractionsNursing Implications and Patient Teaching Assessment Diagnosis Planning Implementation
Preventing transmission Evaluation
142Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antimalarials
Action Interfere with the life cycle of Plasmodium Uses Prevention and treatmentAdverse Reactions Drug-specific: blood dyscrasias, visual and neurologic
changesDrug Interactions Drug-specific: dermatologic, ototoxic, or neurologic
symptoms
143Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.

Antimalarials (cont.)
Nursing Implications and Patient Teaching Assessment
Symptoms Diagnosis Planning
Treatment is strain related Implementation
Loading dose Prevention
Evaluation Laboratory and diagnostic monitoring; eye examination
144Copyright © 2013, 2010, 2006, 2003, 2000, 1995, 1991 by Mosby, an imprint of Elsevier Inc.