Embed Size (px)
Citation preview

105
CHAPTER FIVE
THE INTEGRATED CHILD DEVELOPMENT SCHEME (ICDS) AND
ITS IMPLEMENTATION
The Chapter on ICDS and its implementation begins with a brief introduction of the scheme
and then proceeds to know its process of administration and ways of functioning. The chapter
next talks about involvement of ICDS staff in the programmes by bringing in their job
responsibilities and trainings received by them. The chapter later puts in detail description of
the activities carried out under the scheme. The most crucial part of the current chapter that is
the factors affecting the implementation of the activities of ICDS is discussed meticulously
by the researcher, in order to bring in the nuances at the system level and the field level.
Lastly the chapter also unearths the underlying expectations and experiences of community
from ICDS, which the researcher believes should be heard by the people at policy level to
make the programmes suitable and acceptable for the community.
5.1 The Introduction of ICDS Scheme
5.1.1 About the ICDS Scheme
The ICDS (Integrated Child Development Services) scheme is based on the core themes like
addressing the nutritional and development needs of children. It primarily covers the
nutrition, education, development and health needs of children between 0-3 years of age and
3-6 years of age and also includes adolescent girls and pregnant and lactating mothers, as its
target groups. The services offered to the 0-3 age group of children are THR (Take home
Ration), immunization, health check-up, referral services at the AWCs (Anganwadi Centres).
The other group of children falling in the age group of 3-6 are admitted at AWC and every
day they are provided with supplementary food and are engaged in non-formal education.
They are immunised periodically, health check-up is done once in three months and receive
referral services when they fall sick. The immunisation provided to the 0-6 children, covers
vaccinations of six preventable diseases like polio, diphtheria, pertusis, tetanus, tuberculosis,
and measles. The health check-ups are carried out to identify sick and malnourished children,
which need immediate medical attention. When such children are identified they are referred
to the respective PHC (Primary Health Centre) or Subcentres.

106
Similarly, the adolescent girls mainly belonging to the below poverty line and from SC/ST
background are identified for supplementary food by the scheme. They receive food in noon
at the AWC of their village. At a time, two such girls receive supplementary food from the
AWC for a period of 6 months. In addition to this, the girls also receive education about
health, nutritional, personal hygiene and reproductive health. The pregnant and lactating
mothers receive immunisation and relevant information about health and nutrition through
education sessions. They are also instructed about new-born care, personal hygiene and
family planning by the ANMs (Auxiliary Nursing Midwives) and AWWs (Anganwadi
Workers) at the AWCs.
5.1.2 Mandate to reduce malnutrition
The ICDS has been traditionally engaged with the issue of nutrition, and hence the
component of supplementary food occupies a great significance. However in the context of
high prevalence of malnutrition in the state, the activity of supplementary food is not enough
and there is no other provision or initiative from the department to reduce the level of
malnutrition. The Take Home ration (THR) is primarily given on the principle that various
age groups along the human life cycle, should be provided with the required food, energy and
vitamins. In all, though the activities under ICDS address the issue of malnutrition, it is still
short of mandate and vision for reducing malnutrition. As noted by the CDPO (Child
Development Project Officer),
“…we are the nodal agency for supplementary food and nutrition among
children…but for reducing malnutrition, we would like other sectors to work as
well…”
5.1.3 Administrative Structure
At the village level, the AWC is manned by the Anganwadi worker (AWW) and she is
assisted by AW helper. At the block level, the ICDS project is headed by CDPO. The CDPO
is assisted by the ACDPO (Assistant Child Development Project officer). The project is
divided in to BITs and each BIT is headed by an ICDS supervisor. Depending on the size of
the block, the number of BITS is formed and each BIT has around 25 AWCs to be facilitated
and monitored. The personnel under ICDS are supported by their counterparts from other
sectors at their respective levels. At the field level, AWWs coordinate with the ANMs and
ASHAs (Accredited Social Health Activists). Similarly the ICDS supervisors coordinate with

107
ANMs and medical officers, to carry out the nutritional and health related activities
seamlessly. Following figure 5.1 is showing the organogram of the ICDS scheme at the
Thane district
Figure 5.1 The Organogram of the ICDS Scheme
Deputy CEO, Women and Child Development (Class I officer)
(At Zilla Parishad level)
CDPO (Class II officer)
(At Taluka level, 13 Talukas in Thane District)
Mukhaya Sevika (ICDS supervisor)
(BIT level group of 25 AWCs, each BIT has one ICDS supervisor)
Anganwadi Worker (AWW)
(At the village level)
Source: ICDS Office, Jawhar
As can been seen from the figure 5.1, at the district level, the charge of administration is with
the CEO of WCD (Women and Child Development Department). There are total 13 taluka in
the thane districts, and at the taluka level, ICDS projects are managed by the CDPOs. The
CDPOs are helped by the ICDS supervisors, at the BIT level. The region under an ICDS
projects are divided into BITS, where each BIT has around 25 AWCs to be implemented and
monitored. In the villages, AWCs are operated by the AWWs, under the supervision of ICDS
supervisors.
5.1.4 Monitoring
During the frequent interaction with the CDPO office, it was learnt by the researcher that
every month the office sends all the relevant reports completed according to components and
target groups. These reports coming from all the ICDS projects, helps the CEO of WCD, to
check on the efficiency and effectiveness of the scheme, as implemented in the district of
Thane. At the state level, the state has to send the consolidated reports on the 17th day of the
following month to the ministry. Further the data on health services and food services
pertaining to the malnourished children are monitored by the Divisional level Secretary in the
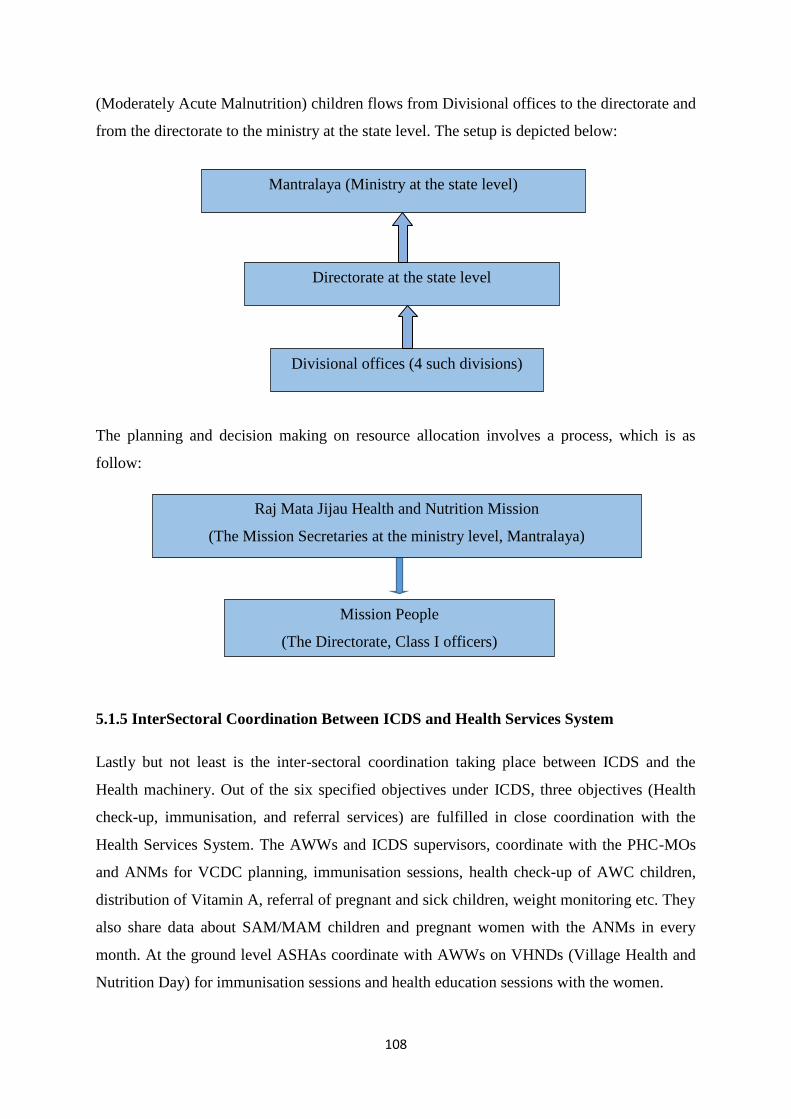
state of Maharashtra. The data about the SAM (Severely Acute Malnutrition) and MAM
108
(Moderately Acute Malnutrition) children flows from Divisional offices to the directorate and
from the directorate to the ministry at the state level. The setup is depicted below:
The planning and decision making on resource allocation involves a process, which is as
follow:
5.1.5 InterSectoral Coordination Between ICDS and Health Services System
Lastly but not least is the inter-sectoral coordination taking place between ICDS and the
Health machinery. Out of the six specified objectives under ICDS, three objectives (Health
check-up, immunisation, and referral services) are fulfilled in close coordination with the
Health Services System. The AWWs and ICDS supervisors, coordinate with the PHC-MOs
and ANMs for VCDC planning, immunisation sessions, health check-up of AWC children,
distribution of Vitamin A, referral of pregnant and sick children, weight monitoring etc. They
also share data about SAM/MAM children and pregnant women with the ANMs in every
month. At the ground level ASHAs coordinate with AWWs on VHNDs (Village Health and
Nutrition Day) for immunisation sessions and health education sessions with the women.
Mantralaya (Ministry at the state level)
Directorate at the state level
Divisional offices (4 such divisions)
Raj Mata Jijau Health and Nutrition Mission
(The Mission Secretaries at the ministry level, Mantralaya)
Mission People
(The Directorate, Class I officers)

109
5.1.6 Eligibility and Selection Of ICDS Staff
Speaking about eligibility and selection of ICDS staff, the CDPO, Jawhar mentioned that, in
case of selection of AWWs, a committee consisting of two Non-official members, the CDPO,
and Medical officer of PHC is constituted at the block level. The committee then scans the
applications, calls the suitable candidates for interview, and recruit the appropriate candidates
as AWWs. The ICDS supervisors (Mukhya Sevika) are selected by the office of CEO, WCD,
Zilla Parishad. The CDPOs are appointed through two mechanisms: first 50 percent is
through promotion from ACDPO, done through the Directorate (Mantralaya) and another 50
percent is through the MPSC (Maharashtra Public Service Commission).
5.2 The ICDS at Jawhar and Mokhada
5.2.1 Infrastructural Facilities at Jawhar and Mokhada
Table 5.1 Number of Villages, Population and Availability of AWCs under ICDS in Jawhar
Block
Sr. No Primary healthcentre
Total AWCs Totalvillages
TotalHamlets
Population
1 Sakur Jawhar-1: 135 33 85 32856
2 Nandgaon 19 64 23587
3 Jamser Jawhar-2: 170 29 110 34881
4 Sakhershet 30 90 35579
Total 305 111 349 126903
Source: THO office, Jawhar, 2013
As can be seen from the Table 5.1, there are two ICDS projects namely ICDS project Jawhar
one with 135 AWCs and ICDS project Jawhar two with 170 AWCs. The ICDS project one
works with two PHCs that is Sakur and Nandgoan PHCs. Similarly the ICDS project two
works with Jamser and Sakhershet PHCs.
Continued…
110
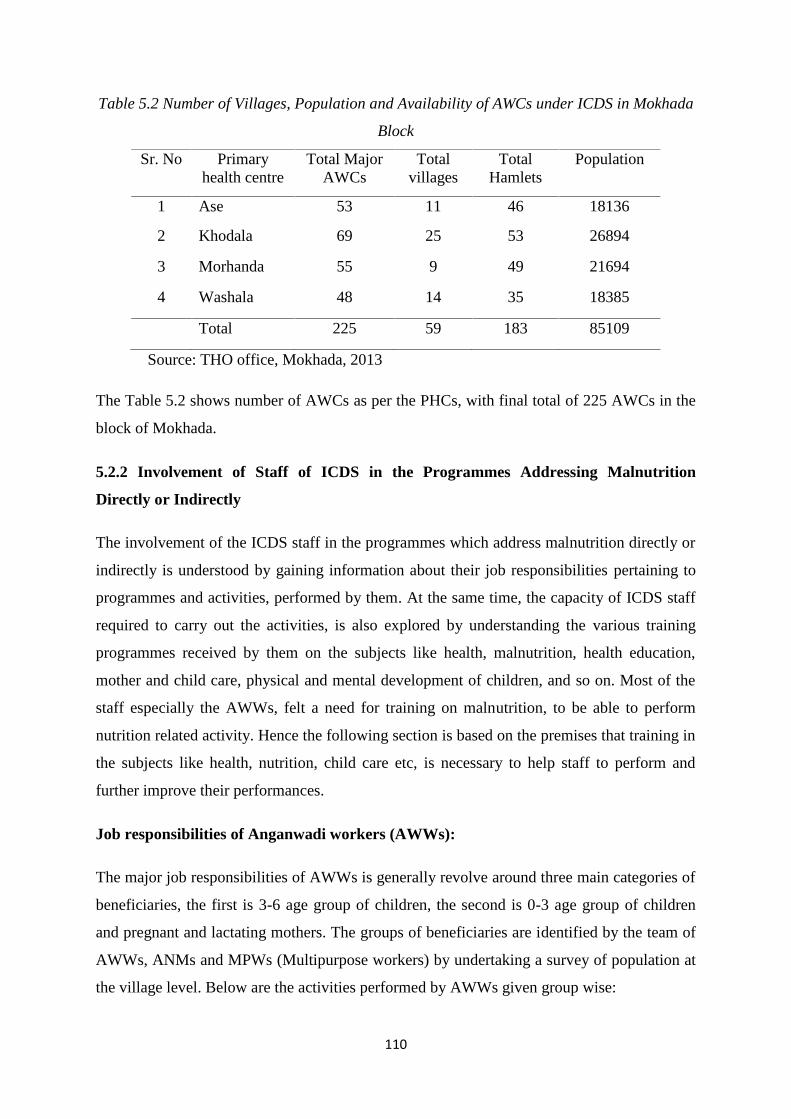
Table 5.2 Number of Villages, Population and Availability of AWCs under ICDS in Mokhada
Block
Sr. No Primaryhealth centre
Total MajorAWCs
Totalvillages
TotalHamlets
Population
1 Ase 53 11 46 18136
2 Khodala 69 25 53 26894
3 Morhanda 55 9 49 21694
4 Washala 48 14 35 18385
Total 225 59 183 85109
Source: THO office, Mokhada, 2013
The Table 5.2 shows number of AWCs as per the PHCs, with final total of 225 AWCs in the
block of Mokhada.
5.2.2 Involvement of Staff of ICDS in the Programmes Addressing Malnutrition
Directly or Indirectly
The involvement of the ICDS staff in the programmes which address malnutrition directly or
indirectly is understood by gaining information about their job responsibilities pertaining to
programmes and activities, performed by them. At the same time, the capacity of ICDS staff
required to carry out the activities, is also explored by understanding the various training
programmes received by them on the subjects like health, malnutrition, health education,
mother and child care, physical and mental development of children, and so on. Most of the
staff especially the AWWs, felt a need for training on malnutrition, to be able to perform
nutrition related activity. Hence the following section is based on the premises that training in
the subjects like health, nutrition, child care etc, is necessary to help staff to perform and
further improve their performances.
Job responsibilities of Anganwadi workers (AWWs):
The major job responsibilities of AWWs is generally revolve around three main categories of
beneficiaries, the first is 3-6 age group of children, the second is 0-3 age group of children
and pregnant and lactating mothers. The groups of beneficiaries are identified by the team of
AWWs, ANMs and MPWs (Multipurpose workers) by undertaking a survey of population at
the village level. Below are the activities performed by AWWs given group wise:

111
For 3-6 years of children:
The AWWs have to run Anganwadi from 9.00 am to 1.30 pm every day except on Sundays.
At Anganwadi, they provide breakfast in morning at 9 am and hot cooked food at 12.00 pm.
The meal is generally prepared by the Self-help groups associated with the AWCs. Secondly
they impart non-formal education by way of conducting plays, games, dance, songs, through
which they try to introduce alphabets (of Marathi), environment (tree, sun, moon etc),
hygiene (washing hands after toilets etc), and so on. Thirdly they also are responsible for
conducting sessions of immunisations, health check-ups, and distribution of vitamin A and
De-worming tablets to the children belonging to the age group of 0-6, in coordination with
the health staff of the attached PHC.
For 6 months-3 years of children:
The major responsibility of AWWs with regard to this age group is to ensure that the group
receive their share of THR (Take Home ration) regular every month as per the prescription.
During the season of migration, the AWWs try to give away the packets to the families as
they are not supposed to stock the materials. However this is not possible as many times
families leave before informing to AWWs. Due lack of instructions in this regard, many
AWWs are clueless about what they should do with the packets.
For the pregnant and lactating mothers:
The packets of THR are also distributed to the pregnant and lactating mothers. The AWWs
prepares the list of ANC (Ante Natal Care and PNC (Post natal Care) mothers and distribute
the THR packets to them. While distributing, the AWWs educate them about the ways to
cook the materials and to be eaten.
Arranging immunisation and health check-up sessions:
Every month the AWWs organise immunisation sessions for children 0-6 years old and
ANC/PNC mothers at AWCs in coordination with ANMs. The RBSK (Rashtriya Bal
Swasthya Karyakram) team has started conducting health check-up of the children. The team
informs the AWWs in advance about the day and accordingly the AWWs make children
ready to get checked by the team on that particular day.
Weighing of children:

112
It is prime responsibility of the AWWs to weigh the children falling in the age group of 0-6
years, in order to monitor their growth. The weighing of children takes place on three days of
a month. Since the days are fixed and known to women in advance, they bring their children
to the AWCs. The AWWs are helped by the AW helpers in this task.
Preparing periodic reports:
The AWWs have to carry out heavy reporting work. As mentioned by them, there are at least
14 registers of different programmes and activity, to be maintained by them on monthly
basis. The ICDS supervisors pay visits and check whether registers are being maintained by
the AWWs. Many of them have found report writing as a time consuming and tedious job to
do. The list of the registers/reports is as follow:
Attendance Register
Stanik Aahar (supplementary food given at AWCs)
Immunisation records
Health check up
Remark book
Take Home Ration (THR)
VCDC register
Mata Samiti
Gradation register (to record weight, height and gradation of children)
Education materials
Masik Aahwal (Monthly Progress Report)
SAM/MAM list
Details of Credit bill of SHG (Shelf Help Groups).
Interaction with the community:
The AWWs have to conduct different type of home visits as per the target groups like
ANC/PNC mothers, SAM and MAM children, adolescent girls etc. In addition to this, they
also arrange meetings with mothers at AWCs, wherein they inform about child health,
nutrition, personal hygiene, immunisation, breastfeeding etc. Besides, they wear the role of
AWWs all 24 hours in a day. As they are part of the community, they happen to meet
women at market places, at festivals, marriages etc, wherein they also enquire about their
health, their children health and if needed give suggestions to them.

113
Training received by AWWs:
Foundation course:
Most of the AWWs had received the basic training upon joining as AWWs. The training is
called as ‘Payabhooth’, meaning the ‘foundation’. The training basically equips the AWWs
to conduct all the AWCs activities as described above. For example, the foundation course,
consist of training on Non-formal Education, wherein, they are taught ways to conduct Non-
formal education through songs, stories, pictures, games etc. After training, they are tested on
activities and evaluated on their performances. They are issued certificates, indicating
completion of the basic course. Thereafter, they keep receiving refresher training, known as
‘Ujalni varg’, wherein things are revised for them and they are also informed about new
things/changes if any.
Training on Malnutrition:
Several AWWs told that they did not receive any specific training on malnutrition from their
department as such. However, few years back, the resource persons from the Rajmata
mission, had taught them about the type of food (special food made with flours of sprouted
wheat and cereals) and their preparation, to be served to SAM/MAM children during VCDCs
(Village Child Development Centre). They were also taught the different recipes of the
special food that should be taught to mothers, so that they would also provide the same food
to the children at their homes. After this, there was no refresh training about malnutrition
being arranged for them. Therefore on regular basis, they were orientated by the CDPOs and
the ICDS supervisors time and again, about issues like weighing of children, identifying
malnourished children and giving gradations to them.
During monthly meetings organised at PHCs with the health staff, the AWWs used to be
briefed by the MOs and ANMs about malnutrition. Any health issue related with malnutrition
or malnourished children are also sometimes discussed in the monthly meetings with the
ANMs and MOs. Through such discussions, they come to know more about malnutrition and
ways to prevent it.
In addition, they were also educated by the ICDS supervisors, about the way to monitor the
intake of food by the children over the period of VCDC. During VCDCs, children are not
able to finish the served food. Initially they eat half of the bowl, or 1/3rd of the bowl and

114
slowly increase their intake. The AWWs are required to monitor the food intake of children
on daily basis and make a note of it. This helps them to check if the children have increased
their food intake over the period during VCDC.
Mother and child care:
In the foundation course, the AWWs are also told about the way to conduct delivery, how to
keep the place clean for delivery, how to wrap a baby after birth, how to identify pneumonia,
how to educate mothers about breastfeeding immediately just after the birth and the regular
breastfeeding and so on.
Training for using machines to weigh children:
A new electronic machine has been introduced to weigh the children. The AWWs have got
the demonstrations from the makers of the machines. It is an automatic machine, wherein the
AWWs need to feed in the basic things like date of birth, height, weight and sex of a child
and get the gradation of it accordingly. In the month of April, 2013, such demonstration was
held for them at a rotary club. The machines have been distributed to all AWWs of the area.
Few AWWs have started using the machines and have found it easy to use. However many
have reported that they cannot recharge it on every weekend due to non-availability of
electric power. Secondly on occasion of a break down, the machine cannot be repaired
immediately as, they have to wait for the technicians from Mumbai to come and fix it.
Health of adolescent girls:
The AWWs have received orientation in the health of adolescent girls, in order to address the
problems of young girls at the AWCs level. The AWWs are mainly involved in giving away
sessions on menstrual cycle, personal hygiene, reproductive health etc. The adolescent boys
are also being educated by the MPWs and HAs.
Reports writing:
There are 14 registers to be maintained by the AWWs. Many times, there come some changes
in the way of reporting or in the format of reports or addition of new report. The ICDS
supervisors, during monthly meetings explain the changes and new addition of reports to the
AWWs, in order to facilitate their report writing.

115
Several orientations and training on many ongoing issues: Being AWWs, they get to deal
with many on-going issues. The issues are as varied as, reproductive health, maternal health,
adolescent health, malnutrition among children and women, new born care etc. They keep
receiving orientations on various matters. This help them to deal with the issues at the village
level and to serve as a strong link with other sectors like health, water, sanitation etc.
Job responsibilities of ICDS supervisors:
Under the capacity of ICDS supervisors, their job responsibilities consist mainly of
supervision of all the activities carried out at AWC level. The supervisory role is performed
by paying visits to AWCs on regular days and as well on weighing days, immunisation days,
VCDCs, health check-ups and Mata Baithak. In a month they are supposed to visit at least 12
AWCs. During AWC visit they observe the distribution of food, immunisation, weighing of
children, gradations given to children (SAM/MAM/Normal), reports maintained by AWWs
and so on. They also see, whether the AWC is clean and surrounding area is also being kept
clean.
They need to prepare their ATP (Advance Travel Plan) for carrying out such visits to AWCs.
The plan is generally prepared by 20th of every month, indicating all the AWC visits,
meetings, programmes to be carried during 1st to 30th of the next month. The plan is then
submitted to the CDPO office for approval. If there is any sudden change in programmes,
then the ATP is altered accordingly with the permission of ACDPO/CDPO.
They also help AWWs in conducting Mata Baithak with the community women, health
education to adolescent girls etc. On their visits, they demonstrate preparation of food, to the
SHGs who is providing food to the AWCs. During sessions with the women, they mainly
focus on food and the right way to cook food, because wrong cooking does away with lots of
vitamins/ nutrients from the food. Secondly they focus on health education which include
personal hygiene, environmental hygiene, and preventive health so that children would not
fall ill. They also address any query about health and food from the gathered women. All
such programmes are taken into considerations while preparing the ATPs.
They help in generating the list of SAM/MAM and sit with the ANMs or MO for planning of
VCDC and CTC (Child Treatment Camps). During VCDCs, they make visits to AWCs to
oversee the distribution of food, quality of food, administration of medicine if any and
weighing of children.

116
Sometimes they also accompany AWWs to house visits, if there is a case which needs extra
counselling or emergency. However, they don’t visit field every day and devote two days in a
week that is Monday and Tuesday, for paper/report work. They also attend monthly meetings
with all the AWWs and share the data and information on SAM/MAM, new birth/death,
immunisation, institutional deliveries etc.
Next most important part of their job responsibilities is that, they prepare the consolidated
Monthly Progress Report (MPR) and submit to the higher authorities. The MPR is a summary
of all the activities carried out at the AWC level in a period of one month. Nowadays it is
done online by login into the given website.
Training received by ICDS supervisors:
The ICDS supervisors are provided a basic training on all 6 objectives of ICDS. The training
mainly includes subjects like nutritious food, pre-school education, health check-up, referrals
services etc. From the blocks of Jawhar and Mokhada, most of the ICDS supervisors, have
undergone this training. In addition, to this basic course, they are also trained time to time on
any new change, or addition of a new component. They also have to take refresher courses,
whenever organised for them. The training of ICDS supervisors mainly takes place at the
district level, Thane. Given the number of ICDS supervisors, in the district, the various
training programmes are organised in a phase wise manner, thus aiming to cover all the
supervisors over a period of time.
Job responsibilities of Child Development Project Officer (CDPO):
The CDPO is mainly responsible for overseeing the operation of the ICDS project, in both
physical and financial aspect. He/she has to deal with the day today functioning of ICDS
supervisors, coordinate with the Zilla Parishad and Women and Child development
department at the district level. Similar at the ground level he/she has to work with a close
coordination with the BDO (Block Development Officer), THOs (Taluka Health Officer) and
Gram Panchayat. He/she has to involve the MOs and THO (if possible), in selection process
of AWWs. He/she does pay visits to AWCs along with ICDS supervisors, whenever possible
and /or needed. He/she is also responsible for the data generated at the CDPO office and
shared with upper authorities and with other sectors.

117
Training received by the CDPOs:
The CDPOs are trained for one month by the RDD (Rural Development department) and
WCD (Department of Women and Child Development). All the training expenses are bore by
the government. The YASHADA, Pune, trains all Class I, II and III officers, including the
CDPOs. There are also refresh trainings for CDPOs, which is mainly for shorter period, say
of 5/7 days. However no specific training on Malnutrition, have ever been planned for the
CDPOs. The CDPOs have received orientation about the Rajmata Jijau Health and Nutrition
Mission, when it was initiated and needed to be implemented through the machinery of
ICDS. In similar fashion, they receive orientation at the district level, about new changes and
additions.
5.3 Routine Programmes Undertaken By ICDS in the Blocks of Jawhar and Mokhada
5.3.1 Description of the Group Specific Activities as they are carried out under ICDS in
Jawhar and Mokhada
Group 1: Children of 3-6 years of age:
Supplementary food served to the children falling in 3-6 years of age group at AWCs:
For the 3-6 years of children, nutritious food is provided twice in a day at the AWC. In the
morning, when the children start gathering they are given snacks to eat like biscuits, ladoos,
mixtures of puffed rice etc. At 12.00 in the noon, hot meal is served, which generally consist
of cooked rice with vegetables and cereals. The food is prepared and supplied by the
‘Bachhat gut’, that is the SHGs. The SHG is formed by the women belonging to BPL families
and SC/ST community. They supply food to the associated AWC/s on 25 days in a month,
excluding all Sundays. The ICDS scheme has prescribed a weekly chart of food to be served
to the children in order to fulfil their nutritional needs. The chart is given and explained to the
SHGs. They accordingly prepare and serve the food to the AWCs at 12.00 pm.
Continued…

118
Table 5.3The Weekly Schedule of Food Given at AWCs
Weekly –Schedule of food provided at AWC
Days Day 1 Day 2 Day 3 Day 4 Day 5 Day 6
9 am Chivada orLadoo (ofsoya beansmixture)
Chivada orLadoo (ofsoya beansmixture)
Chivada orLadoo (ofsoya beansmixture)
Chivada orLadoo (ofsoya beansmixture)
Chivada orLadoo (ofsoya beansmixture)
Chivada orLadoo (ofsoya beansmixture)
12 pm RiceKhichadi
RiceKhichadi
Usal(sprouts)
Usal(sprouts)
WheatShira
WheatShira
The Table 5.3 displays the food chart which needs to be followed. As per the food chart,
children are to be served twice, first at 9 am and during the second time hot meal is given at
12 pm. The hot meal is made of rice, vegetables, sprouts and wheat. The same hot meal is
also served to the adolescent girls.
The SHGs generate credit bills at end of every month, upon submission of which to the ICDS
office, they are reimbursed for their monthly expenses. The bills are reimbursed at the rate of
Rs.5.92 per child and Rs.5.98 per adolescent girls. The SHGs get rice and wheat at lesser rate
from the Government ration shops, which is used to prepare food for the children of AWCs.
Activities taken with children at AWC:
The Anganwadi is conducted between 9 am to 2 pm on all days except Sundays, and during
summer season that is in a month of May, Anganwadi is held between 8.30 am to 1.30 pm. In
the morning at 9 am, as children start gathering at AWC, attendance is taken and breakfast is
served to them. After breakfast, activities like games, storytelling, songs etc are taken with
children. Through such activities, the AWWs try to impart non-formal education. Along with
this, outdoor games are also conducted for at least 30 minutes. One of the AWWs said that
she also indulge children in picture readings. She showed all the pictures, she had hung on
the wall.
All such activities get wind up by 12:30 pm and after which, food is served to children. In
addition to the children, two adolescent girls identified by the AWWs come to AWC and eat
their food. The same food prepared for children is given to the adolescent girls as well. They
come, eat and go. At 1:30 pm, AWC is closed for the day and children are sent off. From
1:30 till 2:00 pm, the AWWs work on the various reports.

119
Group 2: Children of 0-3 years:
Take Home Ration (THR):
This group of children do not attend AWC and hence are given THR every month. The THR
consists of one packet of ‘Shira’, one packet of ‘Upma’ and one packet of ‘Setupeeth’. These
are fortified food materials distributed by the Maharashtra State, WCD department. Every
month, the AWWs give THR to the eligible children. According to the prescription provided
on the packets, in a day, a child should receive minimum 120 gms of ‘Shira’, 120 gms of
‘Upma’ and 130 gms of ‘Setupeeth’. Each month 3 packets of ‘Shira’, ‘Upma’, and
‘Setupeeth’ per child are given to the children. Every alternate month, regular three and one
additional packet, thus total 4 packets per child is distributed by the AWWs.
For the children falling between 0-3 years of age, Take Home Ration (THR) is distributed per
month. The THR for the children consist of:
1. Sheera (Wheat + Jaggery + Soya beans + Sugar) 936 gm
2. Upma (fine grinded wheat) 880 gms
3. Sethepeeth 1170
4. Additional sheera 1500 gms
In case of malnourished children, regular three and additional 1 packet of Sheera of 1500
gms, thus total 4 packets are given in one month and in subsequent month regular three and
additional 2 packets of Sheera, total 5 packets, per child is given. However this is not the
uniform pattern across all the AWCs. At few AWCs, the malnourished children would
receive two additional packets of Sheera of 1500 gms every month.
The packets of THR meant for children 0-3 years, pregnant and lactating mothers are
distributed on the immunisation days, or on, ‘Mata Baithak’ days. As per the official
instructions, the AWWs are not supposed to keep the undistributed packets at AWCs, if
found so, it would be understood that she has not given the packets to few beneficiaries and
might be stocking them for any other personal use.
Health services for 0-3 and 3-6 age group of children:
Immunisation: The immunisation session is arranged once in a month at AWC. It is held
on the village health and nutritional day. The ANM from the PHC comes on the

120
predefined day in a week and administer immunisation to the children. The AWW helper
and ASHA go around in the village, and visit houses having small children. They ask the
mothers to send the children to AWCs for immunisation. On the same day, the ANM and
AWW give health and nutritional education to the mothers of children, pregnant women
and lactating mothers. The ANMs and AWWs also demonstrate different ways of
cooking THR, to the gathered mothers.
The Health Check-up: The health check-up of all children between 0-6 years of age is
conducted once in 3 months. The Medical officer from the respective PHC comes along
with ANMs and conducts out the health check-up. Any sick child is found, is provided
with medicine or referred to PHC/RH as per the condition/diagnosis. On such days, the
PHC-MOs and ANMs are assisted by the AWWs and Helpers. They make sure that all
children from all the age groups are gathered at AWC for the health check-up. For regular
illnesses like cough, fever, dysentery, stock of medicines is provided to AWWs.
The government has introduced RBSK to address the issues related with child health. It
focuses on early diagnosis of all possible illnesses and timely medical interventions. The
team is constituted of expert doctors who visits AWCs and conducts health check-up of
all children gathered at AWCs. The program has thus replaced the old practise of health
check-ups of children being carried out by the PHC-MOs. The team comes, does it job
and goes away. As a result, the intimate contacts between the beneficiaries and doctors
are slowly vanishing. The subsequent visit of the team falls approximately after 6 months,
which is a long gap, as far as follow up is concerned. The AWWs also are unaware of the
way to contact the team in case of some emergency, during this gap. The PHC-MOs,
although comparatively nearer and available, cannot act in emergencies, as he has been
oblivious about the illnesses and diagnosis of the children. This situation creates a great
vacuum as far as timely and regular treatment of children is concerned.
Growth Monitoring: Every month on 15th, 16th and 17th, children between 0-6 are
weighed and categorised in to SAM, MAM, and Normal. Three days are kept with a view
that, since mothers are away for work, they would be able to make at least on any one of
these days. Since the days are fixed, the ICDS supervisors also make a note about it in
their Advance Travel plan, and try to visit the AWCs, on these weighing days. The
AWWs are helped by the helpers in this activity. It was also seen at few places, that
ASHAs were also helping AWWs in the weighing the children at AWCs.
The children are weighed and accordingly, the list of SAM/MAM children is prepared
and shared with the ANMs, ICDS supervisors in the end of every month. This

121
consolidated list of all AWCs then goes up from the ICDS office to the DHO (District
Health officer) and is considered while deciding the number of VCDC to be organised.
On weighing days, mothers are also made aware of increase/decrease in weight of
children and accordingly they are advised by the ANMs and AWWs. Few of the AWWs
have reported that nowadays, especially young and educated mothers have started taking
interest in weight monitoring of their children.
Group 3: Pregnant and Lactating mothers:
Take Home Ration (THR):
The THR is distributed per month to the pregnant women and lactating mothers. The
pregnant women start getting THR from the first month of conception and the lactating
mothers keep getting THR till first six months after the birth of a child.
The THR for pregnant women and lactating mothers consist of
1. Sukadi: 1170 gms (for 9 days)
2. Upma: 1040 gms (8 days)
3. Sheera : 1120 gms (8 days)
The pregnant women on an average should consume 130 gms of upma and 140 gms of sheera
every day. And accordingly they get the packets for total 25 days.
Monthly check up of pregnant and lactating mothers:
On the VHND day (Village Health and Nutrition Day), immunisation is carried out for the
pregnant women, weight is checked and health is monitored. Any problem if identified, then
the woman is referred to the PHC or to the Cottage hospital/Rural hospital located at Jawhar
and Mokhada respectively. This day is also called as ANC clinic day by the ANMs.
Group 4: Adolescent girls:
Every AWC has to identify two adolescent girls from the SC/ST communities who also
belong to the BPL families, for supplementary food. It was observed that every AWC, the
researcher visited have had identified such two girls from their villages. The food cooked for
the children of AWC is also served to the adolescent girls on daily basis. They come, eat the
food and go back to their work. The idea behind this is that, the adolescent girls especially
from poor SC/ST families are found malnourished, physically weak and anaemic. They are

122
also married off early and start bearing children from an early age. As a result, they tend to
give birth to low weight children, which later become vulnerable and tend to fall into the
cycle of malnutrition. Since many of these girls are drop out from schools, they miss the mid–
day-meal served at schools. In this backdrop, they are selected and provided food for at least
6 months, after which another set of two girls is identified. During the period while they are
associated with the programme, they are also taught about personal hygiene, nutritional diet,
health issues and reproductive health.
5.3.2 Common activities for all groups
Educational sessions with the mothers:
Educational sessions with mothers are treated as a major activity by the AWWs, during
which they give advices and suggestions on mother and child care. The sessions are normally
arranged on immunisation day, ANC clinic day, THR distribution day or on weighing days.
Most of the times, the sessions are jointly held with ANMs or with LHVs (Lady Health
Volunteers). The VCDC also has a scope to conduct educational sessions with the mothers.
However, to help improve the interaction with the mothers, during VCDCs, there was no
special fund being allotted to AWWs to develop an educational tool or aid, which could be
demonstrated to the mothers. Recently, the ‘Mata baithak’, has started where Rs 200/- is
given to AWWs for refreshments to be served to the women attending ‘Mata baithak’. It is
being promoted as a meeting with mothers where they would be educated about child care,
malnutrition and so on. At the same time, the mothers would have a chance to see how things
are being run at AWC. Earlier, it was difficult to gather women for such meetings, as they
were always busy and had no incentives to attend meetings with AWWs/ANMs. However,
due to refreshment being served during meetings, there is a hope that more women would
turn up for the meetings. Few of the AWWs mentioned that they organise Mata Baithak on
the day of distribution of THR, where they sure that more women would turn up to collect the
THR packets.
In case, if such sessions with the mothers have not been organised or have had few mothers
attending them, then the AWWs while around in village, when happen to meet the mothers,
try to convey the message to them in informal ways. This indicates that AWWs are generally
seen and accepted as one among them by the community with whom they are often engaged
in informal interactions. They enjoy close proximity and faith of community as compared to

123
other staff like Supervisors, ANMs, and MPWs, which are seen as the government people
and someone who are outsiders.
Home visits (for all the group of beneficiaries of ICDS):
Most of the AWWs said that they have to carry out five different home visits. Firstly, home
visits to ANC mother is made to educate/inform them about early registration, institutional
delivery, and immunisation and secondly they visit to lactating mothers, to educate them
about way to hold baby, way to breastfeed and about new born care. The third kind of visit is
for the malnourished children, wherein they tell to mothers about food, what and how to cook
and eat. The fourth type of home visit is carried out for the adolescent girls, to educate them
about the personal hygiene, health issues etc. The fifth home visit is for imparting lessons on
personal and environmental hygiene to the general population. When asked about whether
they are able to visit all these people on daily basis, most of the AWWs replied that it is not
possible to visit homes every day, as they are too occupied with their AWC work especially
the report writing work. After they release children, they sit half an hour more to do reporting
work. And in afternoon if they go, they seldom find people in houses. They have to visit
people in evening, once they are back from work, which is again not possible, unless and
until it is important.
5.3.3 Other few experiments of the government
A new pilot project, based on Hyderabad model is being planned to implement in the
area. Under the project, supplementary food will be provided to the pregnant women
every day. In order to carry out this activity a team consisting of AWW, ANM, Panchayat
member and ASHA has been envisaged. The pregnant women will get one full meal a day
comprising of ‘Chapati’ (Wheat bread), rice, pulses, vegetables and eggs. The pilot
project is being supported by the UNICEF (United Nation International children
education Funds). If the project found successful, the Mission will discuss about it with
the government.
Another program of 1000 days was held between 14th October 2012 and 9th April 2013 in
Jawhar block. The activities carried out under the programme were VCDCs, health check-
up and distribution of medicines and health education about food. The main groups of
beneficiaries were, children between 0-2 years and ANC and PNC mothers. The basic
aim of the programme was to cover the period, when a child is conceived, is born and

124
attains 2 years with all the necessary food, health and immunisation services. However
the food was not given during the programme because the grant received for the said
programme was not sufficient.
There is a supply of ‘Khauti’, every year to the people belonging to BPL, which is
distributed during the rainy season. It includes, pepper, oil, rice and wheat. It is given
through the, ‘Adivasi Vikas Prakalp’ (Tribal Development Department). The families
with malnourished children get double ‘Khauti’. Because of this, there are parents who
often complain about not declaring their children as ‘Malnourished’, because they would
have also gotten double Khauti, had their children been declared malnourished. Hence
they prefer to keep their children malnourished, with a hope to receive double Khauti.
5.4 Factors Identified at the System Level Affecting the Implementation of ICDS
Activities
5.4.1 Factors at the System Level Affecting the Implementation
There are problems with the ways programmes are implemented in the concerned blocks,
which are caused by the system apathy. Following are the factors, identified by the
researcher, on basis of information shared by the ICDS staff, which were found causing
hindrances in the implementation of activities of ICDS.
Low attendance at AWCs: Low attendance at AWCs is the common problem as cited by the
most of the AWWs. At any given day, out of 15/20 children registered at an AWC, only 9/10
children are present. The AWWs explained various reasons, due to which they have less
children attending the AWCs. Some children are kept at homes to help in house chores or to
baby sit their younger siblings. “…and the 5/6 years old are kept at home to babysit the
smaller ones, when their parents are away at work…hence many times they don’t come to
AWC” mentioned one AWW from Mokhada block. Secondly many mothers don’t send their
children due to the fact that ‘Khichadi’ is being offered every day, as explained by one of the
AWWs, from Jawhar block,
“…we have to go and call the mothers to send their children…some mothers say
that, what we give at AWCs just a plain Khichadi…why would we send our children
just for Khichadi…”
One of the AWWs, who did not have the AWC buildings said that, her children find it
difficult to walk all the way to helper’s house every day, hence they don’t come on few days.

125
Many of them added that at the time when Katkari community migrate, their children do not
come for 7/8 months. In this regard, one AWW added that,
“…since my population is less, there are few children at AWC…that too some of them
don’t come when they migrate out with their parents for work...”
Most of the AWWs, also said that in rainy season also the attendance of AWCs is affected
very badly, as children don’t wade through the overflowing streams and rivulets, to reach to
AWCs. Another set of reason is children often fall sick, during rainy season due to which
they don’t come to AWCs. One AWW from Jawhar also stated that due to private nursery
available at Jawhar, the children of little well-off families don’t come to AWCs.
During their home visits, when the AWWs tell mothers to send their children, they get to hear
these very reasons. Most of the AWWs, said that children coming to AWCs are often not
clean, not bathed and never wear washed clothes. Majority of children are not fed at homes
and often come to AWCs with empty stomachs. The AWWs are also shocked to see that few
children consume alcohol (easily available at homes) before coming to AWCs. All these
factors make children prone to illnesses and malnutrition.
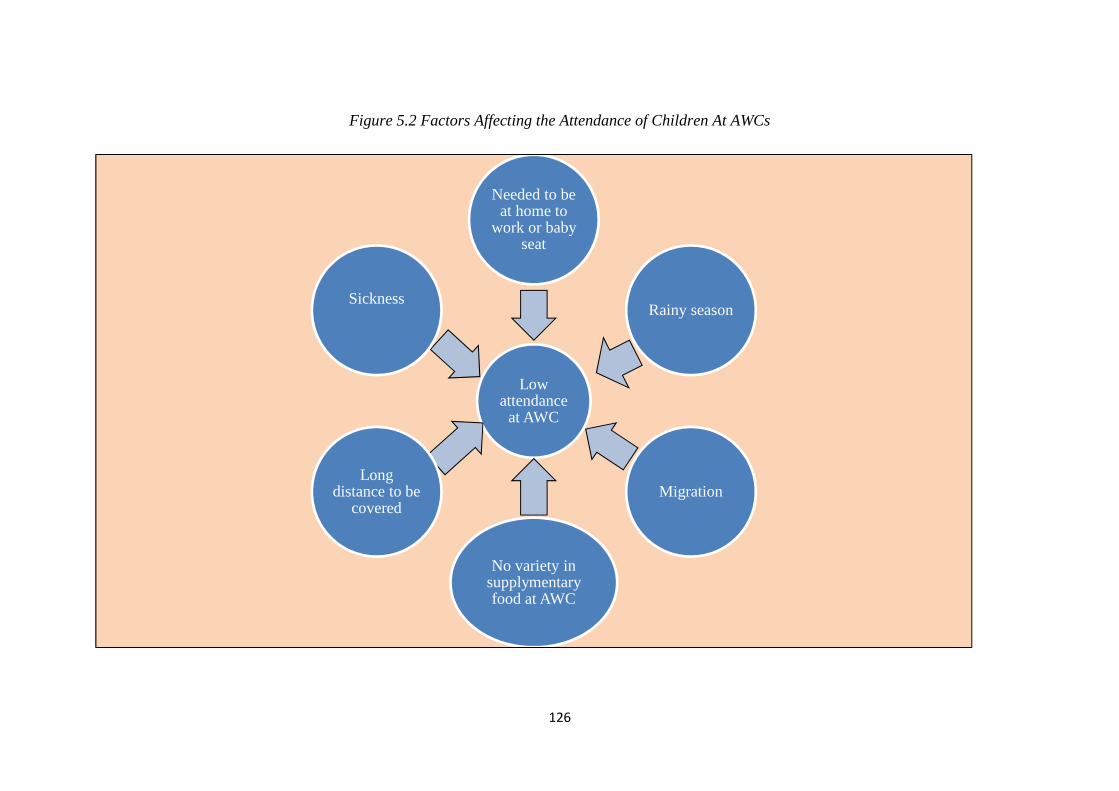
The following figure 5.2 depicts the various factors for low attendance of children at AWCs.
As can be seen, the factors like sickness, long distance to travel, rainy season, migration,
absence of variety of food at AWCs etc make the children less enthusiastic or unable to
attend AWCs on regular basis.
Continued…
126
Figure 5.2 Factors Affecting the Attendance of Children At AWCs
Lowattendance
at AWC
Needed to beat home to
work or babyseat
Sickness
Longdistance to be
covered
No variety insupplymentaryfood at AWC
Migration
Rainy season

127
Basic responsibility of identifying SAM/MAM children lies on AWWs: The AWWs at the
village level identify the SAM/MAM children from the age group of 0-6. Three days in a
month is allotted for weighing, where the children from the village are weighed and
accordingly put into the SAM, MAM and normal category. It is thus the responsibility of the
AWWs to do the correct categorisation of children. When new method, the anthropometric
measurements, was introduced, most of the AWWs lost the confidence of applying the
method correctly. Some AWWs said that they get more number of SAM/MAM children if
the anthropometric measurement is applied. Many were still confused that by what method,
the list of SAM/MAM children should be prepared every month. Some of them have started
to make 3 different lists as per weight to height, weight as per age and as per the
anthropometric measurements, and leave the decision to the supervisors, to select whichever
list they want. One AWW from Jawhar, vented out her concern,
“…every time they change the parameter to decide the underweight children…we are
confused…the young lot understand quickly…but we older don’t understand things
now that easily…”
As per the rules, the list has to be corrected and approved by the supervisors and/or MOs.
One MO from Jawhar block, said though initially they were involved in finalising the list,
however in recent times they do not get time to work on it and most of the time they rely on
the lists prepared by the AWWs. The list of SAM/MAM children serve as the basic premises
for VCDC and CTC, where these children are admitted and treated for malnutrition. When
the method of identification of SAM/MAM children itself is flawless, then the whole purpose
of VCDC and CTC is lost, in the initial stage.
The introduction of the new automatic machine to weigh children, due to lack of training, is
turning out to be a problem for majority of the AWWs, following is the statement from one
such AWW, from Jawhar block, “…the new weighing machine is difficult…many details to
be feed in like DOB, weight, height etc…I need more training in this…”
Problem with Take Home Ration (THR): The THR is given to children from the age group
of 0-3 years. The SAM/MAM children, from this age group are given extra packets every
month. However as mentioned by majority of AWWs and ICDS supervisors, to monitor
intake of THR on daily basis by paying home visits, is challenging, as it would call for a
stand against a norm of cooking same food for every members of the family. The THR meant

128
for the SAM/MAM children is being cooked and eaten by all in the family. One AWW from
Mokhada block commented on this situation,
“… in our visits we often find that THR is also eaten by the other family
members…what to do there is no mechanism to stop this…we cannot be rude with
people and tell them not to eat every time…”.
In the similar way, another AWW from Mokhada, spoke about the same problem,
“…We are told to distribute THR to the children 0-3 and ANC/PNC mothers…we go
and check whether they are eating…but we cannot go every times due to other house-
visits and writing work at AW…”
The common reason cited for these behaviours of people is that the THR provides a break to
people, from their routine and stable food of rice and raggi bread and the tasteless curry,
which is often made without any spices and oil. During the time, when families migrate, they
completely miss THR for a period of 6/7 months. The SAM/MAM children is largely
affected due to the norm of cooking same food for everyone and secondly because of
migration. There were also incidences of people throwing away the packets, if they dislike
the taste of it.
Lack of infrastructure, staff, and resources: It was observed that out of 12 AWCs visited,
during the study, almost 6 AWCs did not have the AWC buildings. These AWCs were then
conducted at the helper’s houses out in their veranda. During rainy season, children would sit
on the semi wet carpets/mattress on the muddy ground, as water would easily slip into the
veranda. Most of the children would not even attend the AWCs. In one of the villages, the
helper’s house was far at the outskirt, as a result many children would not go to AWC. The
helpers, when asked, that whether they would continue giving out their verandah on rent for
AWC, most of them were not sure, as the rent to be received from the system was getting
delayed, without a proper reason.
Low attendance of children also affected the VCDC, because many children would not come
due to rains, no proper sitting arrangements and also due to the long distance to be travelled
to the helpers’ houses. The ‘Bal Kopra’ a food corner, arranged during VCDC, was also
missing from the VCDCs, as VCDCs were organised out in the verandah.

129
When asked about any efforts from them to have AWCs constructed for them, most of them
replied that their proposal is in process, and is taking time. One AWW from Jawhar
expressed,
“…the proposal of the AW building is in the process…meanwhile AWC is conducted
here at the Helper’s house…we make children sit out in the verandah…in rainy
season it becomes quite messy…we are waiting for the AWC building…”
Similar experiences was shared by another AWW from Mokhada block,
“…We have been after the Gramsevak to start constructing our AWC building...it’s
been sanctioned...but he says that 4 lakh is too less for constructing the
building…that’s why the delay is…God knows when the AWC building would come
up…”
Lack of staff to carry out the activities is another major problem, being faced by the system.
For instance, in the block of Jawhar, 12 posts of AWWs were vacant, similarly one post of
ICDS supervisor was vacant. One of the ICDS supervisors indicated that, ““…there is one
post of ICDS supervisor vacant, so all the 25 AWCs coming under that post have been given
to me to supervise…in total I have around 45 AWCs to be monitored in a month, which is not
humanly possible…so sometimes some AWCs are paid visit after two months…I cannot help
it…what to do…?”. From this one can infer that, the staff has to work extra for the vacant
posts, which affect the work assigned to them. From the other staff, it was clear that they are
not able to complete home visits and AWCs visits, as per the monthly target.
At the Mokhada block, there was no CDPO and the CDPO of Jawhar was given the
additional charge of CDPO for the ICDS project at Mokhada. The CDPO, was about to retire,
and there was a talk to promote the ACDPO to the post of CDPO of Jawhar, but about the
CDPO post of Mokhada there was still no clarity. The CDPO said that inadequate staffs do
affect the functioning of the ICDS project. He stated that he was struggling to manage with
the limited staff. He added that whenever anything new scheme/programmes related with
mother, children, nutrition is initiated the responsibility for their implementation is given to
the ICDS projects only. He further added that, the ICDS projects at Jawhar and Mokhada
were not given adequate office spaces. In the preceding week, there was a meeting of all
AWWs being called by the ICDS supervisors, to inform them about a new change in the THR

130
scheme (THR to be distributed through SHGs). Due to lack of space, the meeting was
organised at the PHC.
Migration of the Katkari community and no tracking system to trace for the
community of services: The children mainly from the Katkari community miss the
Anganwadi for about 6/7 months, as they migrate with their families to towns. During this
period they are not able to avail the supplementary education, health check-ups, De-worming
and Vitamin A tablets, weighing per month. They miss the possibility of being identified as
SAM/MAM and miss on the possibility of being admitted to VCDC. During rainy seasons
that from June-September, when they are back to villages they do not attend the AWCs
regularly, due to various reasons like:
They have fallen sick at the work places, where they have not received proper food and
medical care
In absence of AWC buildings, no sitting arrangement at helpers house.
The houses of Helpers or the AWCs being located at long distance, or across the river
which become the obstacles in attending AWCs on daily basis
Negligence from the parents due to other issues like poverty, work, alcoholism etc.
Similarly the other age group of 0-3, who do not attend AWCs, also miss on THR,
immunisation and possible health care in case of any illnesses. Immunisation is an important
thing especially for this age group, which is missed altogether, when they are away.
If given a thought one can realise that the children from Katkari community are deprived of
food and medical care all throughout the year. The MO from the Mokhada block explained
that in a year, from November to May, the community migrate, where the children are not
cared enough by the parents. During June-September, when children are back, they succumb
to the monsoon diseases and remain absent from the AWCs/VCDC/CTC. If this is the
scenario, then it is highly impossible to break these children away from the vicious cycle and
it would serve no purpose, even though programmes like VCDC and CTC are organised.
Most of the time AWWs and the ICDS supervisors do not have the knowledge of work place
and hence are not able to arrange the immunisation services to children, neither can refer the
children to the VCDC being organised at a place, where families have migrated. They have
done this, only when they have known the places where people have migrated. One AWW
from the Jawhar block, had made a good rapport with the contractors, who take the families
131
to towns for work. She keeps in touch with the contractors and find out the location of
people. She then arranges services of immunisation and ANC check-up for people at their
work places. This is something commendable and not all AWWs undertake such extra
efforts.
The Role of the ICDS supervisors: The ICDS supervisor has around 25 AWCs to monitor,
wherein she needs to oversee the functioning of AWC in entirety. She does this, by paying
visits to the AWCs, where she facilitates, guides and supervises the AWWs. However due to
time constraints and long distance, most of the ICDS supervisors do not get to visit all the
AWCs. Secondly the AWWs at many places, were not comfortable seeking help from the
supervisors on each occasion of query and doubt. The responsibility for the major tasks like
identifying SAM/MAM children, conducting VCDC, meetings with mothers, arranging Mata
Baithak, doing follow up of SAM/MAM children etc lies on AWWs, with a little role for the
ICDS supervisors. At the project level also (that is at the block level), they are only supposed
to consolidate all the MPRs collected from the AWWs and submit to the office, with no other
no major responsibilities. Sometimes they are also involved in the administrative work if
demanded so by the CDPO. This explains a scenario, where the role of ICDS supervisors
although is big, but their actual participation is quite low.
Another important aspect is the strict hierarchy which is visible between the ICDS
supervisors and AWWs. As a result it is often seen, the ICDS supervisors blaming AWWs for
their poor performance and lack of initiatives; whereas, the AWWs are seen expressing a
need for greater support from the ICDS supervisors. The following narrations throw a clear
light on the situation,
“…they don’t understand things easily…we have to repeat things many times...only
few AWWs are smart and motivated…sometimes it’s tough to deal with them and we
have to shout..” (ICDS supervisor, Jawhar block)
“… we don’t have platform to place our queries and doubts...we come into contacts
only with the supervisors…in case of emergency we call them and ask…they are good
but sometimes behave bossy with us..” (AWW, Mokhada block)
This calls for a change in operation, according to which both the AWWs and ICDS
supervisors could be assigned similar responsibilities at least in few yet crucial areas like

132
identification of SAM/MAM, engagement with community through educational sessions,
joint home visit etc.
Low morale of AWWs: Most of the AWWs are from the local communities and lack
exposure to the outside world. Majority of them are educated only till 9th or 10th standard and
the younger ones, joined in last 5-10 years are little more educated. Given this, they fail to
understand the intricacies of the functioning of the system and its rules and procedures. The
system keep on introducing new rules, new programmes with predefined protocols, new
reporting formats, and setting of new targets for which they find difficult to adjust with. They
are required to fill up 14 different reports on the monthly basis, which they find time
consuming and feel pressurised to complete the reporting work, on time. One AWW, from
Mokhada cited an example that in the MPR (Monthly Progress Report), they have to fill the
data till 25th of a month and any incidence happening after 25th, is recorded in the next month.
Whereas, into the registers of birth and death, entries are made from beginning of month till
the end of month. In events like child death happening after 25th, get recorded in the
Birth/death register but not in the MPR. In the end when the numbers do not match, then they
are held accountable for the data discrepancies.
On being informed by the supervisors, that their AWCs is in the list for VCDC, the AWWS
go and encash the cheques, go to the market and purchase the required raw material like oil,
sugar, wheat, cereal, peanuts, jaggery and start preparation accordingly. In doing so, they
don’t get help from ASHAs or ANMs, they do all by themselves, with the help of helpers.
In addition, they being close to the community, they carry the responsibility of serving a
crucial link to the various other sectors like health, education, PRIs like gram panchayat and
so on. They have to be present at gramsabha, monthly meetings at PHCs, meetings of
VHSNC (Village Health Sanitation Nutrition Committee) etc. At field, as part of their work,
they need to provide required coordination to the ANMs, ASHAs, MPWs, community leaders
and PRI members.
Most of the AWWs were complaining about the low salary and they have been demanding
increments in their salary and change in the retirement scheme. At the time of retirement,
they should get an amount as a final settlement or a pension scheme should be initiated. To
their dismal, they are still struggling to get this approved from the government, through the
platform of their union.

133
Thus, due to the fact that they have to manage things at all fronts, while tolerating the apathy
of system, the seniors most AWWs have lost zeal to work and was just waiting to get retired,
while the younger ones were also not much enthusiastic about their work and future.
The following figure 5.3 shows that system level problem like inadequate support from ICDS
supervisors, low salary and no increment, heavy reporting work etc together affect the morale
of the AWWs adversely. As a result many of them are seen less motivated and struggling
with the job and its demands.
Continued…

134
Figure 5.3 Factors at System Level Leading to Low Morale Among AWWs
Low moraleof AWWs
Inadequatesupport/guidanc
e from ICDSsupervisor
Lesseducation and
limitedexpoure to theouside world
Lessknowledgeabout rules
and regulationof the system
Heavyreprting work
Low salary/no increment/no retierment
scheme
have to dealwith multiplesatke holders
(NGOs, helathstaff, gramme
sevak andcommunity
people)

135
Issues with Self Help Groups: The hot meal served at AWCs is provided by the SHGs. The
SHGs are formed by the women who belong to SC/ST community and economically fall in
the BPL (Below Poverty Line). The system reimburses the monthly expenditure incurred by
the groups, at the rate of Rs.5.92 per child, per day and Rs. 5.98 per adolescent girl per day.
The SHGs are supposed to get the materials at the lower costs from the government ration
shops. The weekly chart of food is given to the groups, so as to receive food accordingly.
Most the AWWs complained that they don’t receive food as per the chart, and it mostly
cooked rice that is ‘Khichadi’ that the SHGs provide. Even the children attending AWCs are
bored by eating plain khichadi, every day. There are families who do not send children to
AWCs, primarily because of the reason that the AWCs serve only Khichadi and nothing else.
The AWWs said that even after having told them repeatedly, the women of the group still do
not adhere to the weekly chart.
The SHG members, on the other hand, had their own issues. Most of them said that they do
understand the importance of nutritious food but they are helpless. They complained that
their credit bills are not reimbursed for months and months together and also the rate at
which money is given is also very less. In that rate it is not possible to cook vegetables and
cereals by using oil and ghee. In such situation, it becomes very difficult for them to follow
the chart and prepare nutritious food for the children of AWCs. Their concern is also seen to
be felt by the AWWs, which is evident from one narration, coming from Jawhar block,
“…my SHG does not give variety of food...as they say...money is too less for vegetables and
dals…it is actually true”. Few of the SHGs members said that few rationing shops have also
stopped giving them materials on credit. When they visit the ICDS offices to check on their
reimbursement, they are not given any concrete answers by the authorities. The CDPO,
speaking about the matter said that the reimbursement process is often stuck at the upper
level, and at many times, even he is not able to do anything to ensure timely reimbursement.
At many places, it was observed that several SHGs were discontinuing and closing down
primarily due to this reason. The AWWs are left haywire, looking for new SHGs. This can be
understood, through a narration of an AWW from Mokhada block,
“… The SHG told me to look for another SHG, as they are finding it difficult to
continue because they have not been paid for the last 3/4 months...the authority tells
them that they themselves have not received the money then how they would
reimburse them…the money is irregular and also very less..”

136
The active SHGs also do not want to take additional AWCs, if they are already providing to
one/few, on the ground that they will not be able to afford extra AWCs in such situation.
5.4.2. Factors at the community level affecting the implementation of ICDS
The AWWs face the wrath of people, if their children are not identified as SAM/MAM and
admitted at VCDC and CTC. As recollected by one AWW, she had to face the verbal abuses
of one such parent. The people feel that they have been deprived of their rights and been
cheated by the government. The parents fail to recognise the difference between the
SAM/MAM and normal children, and don’t relate with a fact that VCDC and CTC is only for
few and not for all, especially when all of them are facing the same problems of poverty and
day to day struggle for survival. At the same time, the staffs have a pressure from the system
to show the reducing number of SAM/MAM month by month.
As compared with ANMs, LHVs and MPWs, the AWWs enjoy the trust of people, since she
is from the community and one of them. The ANMs, LHVs and MPWs are from other places
and struggle to gain the acceptance from the people. As a result, the community does not take
their help/advices/information seriously. This adds up to the difficulties being faced by the
LHVs, ANMs, and MPWs, at the field level.
The network of AWCs is quite dense, and the ICDS supervisors find it difficult to cover all
the AWCs as per the monthly target. According to the explanation by an ICDS supervisor in
Mokhada block, some AWCs are located deep down the valley on the slopes of mountains,
while few are on the top of mountains and others just across the rivers. These AWCs are
difficult to reach and hence are visited once in two or three months.
Almost every staff struggle with the Katkari community, first of all they don’t send their
children regularly to AWCs and at homes also they don’t treat them at priority basis. Second
major problem is discontinuity in their utilisation of services. Once they migrate, they cease
to be the beneficiaries of services like, hot meals served at AWCs, growth/weight monitoring,
immunisation, ANC clinic, institutional deliveries, THR for small children and ANC/PNC
mothers, VCDC, CTC, home visits, and educational sessions on health, hygiene and nutrition.
The following figure 5.4 summarises all the discussion done so far and explains how the
identified factors at the system and community level affect the implementation of activities of
ICDS. From the figure it is clear that issues like low morale of AWWs, migration, filed level

137
challenges, lack of infrastructure issues with SHGs are some of the major factors which
influence the implementation of programmes and activities of ICDS.
Continued…

138
Figure 5.4 Factors and their Inter-Linkages Affecting the Implementation of Activities under ICDS
Implementation of ICDS
Lowattendance
at AWC Responsibility of
identifyingSAM/MAMon AWWs
Lack ofinfrastructur
e/ staff/resources
Migrationand no
trackingsystem
Field levelchallenges
Lowmorale ofAWWs
Issues withSHGs
Limitedrole ofICDS
supervisor
Limitedmoniteringin case of
THR

139
5.5 Perceptions and Experiences of the Community about ICDS
The community being the observant and also the participant in the role of ‘beneficiary’ do
carry certain perceptions derived from their experiences with the system. This section covers
the perceptions and experiences of the community about ICDS and its services.
Irregular conduct of AWC: The women during FGDs complained that some of the AWCs
in their villages are not held regularly. One woman from Jawhar FGDs, said that, her village
is very small of just 30/40 houses and they have an AWC situated at the outskirt of the
village. She said that the teacher calls the children at her home, as they do not have the AWC
building. The children are left alone to play with each other while she does her household
work. The Khichadi is also not given on every day. Therefore she prefers to not send her
children to that far and for no use. She said that her neighbour also does not send her children
to AWC. Few women from Mokhada block, during FGD, mentioned about the AWC where
their children go. One from them, said that during rainy season, the river start overflowing
and difficult to cross over. In addition the AWC is located up at the top of a hill, where their
hamlet is situated and for the AWW to reach there a distance of 5/6 Km needs to be travelled.
Therefore during rainy season, the teacher does not come and hold the AWC. Their children
therefore are left at home and do not get their Khichadi.
No variety of food: Many women reported that their children just receive plain Khichadi,
with no oil and vegetables in it. One woman said that earlier children would get vegetables,
but nowadays they just get to eat plain yellow rice. Other women also expressed that children
sometimes don’t eat the Khichadi every day, they bring it to homes. When asked about this to
the AWWs, they explained that it is because the SHGs don’t make variety of food and just
provide Khichadi every day. One mother of a SAM child put a point across that,
“...When the government cannot give us vegetables, eggs, and fruits every day, in
spite of having so much money then how could the government expect us to do so at
homes, when we have to struggle for even the basic things...”
Another woman from Mokhada, also echoing the similar thought, said that the AWWs keep
telling them about proper food to be given to children and they put forward the same
argument to them. A weekly chart of food prepared by the system, with an aim to provide
nutritious food to the children during their growing years, is thus seems to be a failing affair.
Following is one such narration of a katkari woman, from Jawhar FGDs,

140
“….At AWC, the children eat rice only and no dals and eggs…at homes we mainly
eat rice and nacchani (ragi)…and nothing else…vegetables also we can afford only
on few days that too when they are available….we cook and share the same food
with everyone at home…what different we can cook and when should we cook…for
the whole day we are out for work...before going to work, we do prepare food and
tell children to take and eat, when they feel hungry and also feed the younger
ones… but we can’t sit at home and watch whether they have eaten or not…”
NO AWC buildings:
“…Children don’t have proper place to sit, we take our children only on
immunisation day and weighing days to the AWC…”
This was the common experience shared by majority of women, who did not have the AWC
building in their villages. Almost, 50% of the women attending FGDs did not have AWC
buildings in their villages. They further added that, at the houses of helpers and at some places
at the houses of AWW, Anganwadi is conducted. But they keep children out in the verandah
and don’t let them inside. During rains, the verandah is full of water. One woman from
Jawhar FGDs, described the situation of the AWC of her village,
“… In rains when the verandah is full of water, they just spread out a carpet outside,
for the children to sit…the carpet gets wet in no time…they put a plastic sheet over
the verandah, which in heavy rains get torn up...somehow they make the children
stand in one corner…give them khichadi and let them off…”
One woman from Jawhar said that in her village the helper house is far off, and hence she
does not send her child there every day. Another few women also expressed the same thing.
They said, children like to stay around their houses and play instead of going there.
Children go there for weighing and immunisation, when sister comes: Most of the
women, from the Mokhada block, said that their children do go to AWC, but are not sure
whether they go regularly. But they do take their children to the AWCs along with other
women of the villages to do immunisation and weighing of the children. They do so because
the AWHs or ANMs go home and ask them to go to AWCs. Few women said that they don’t
miss the weighing days, because their children get packets from the AWCs. One such woman
from Mokhada FGDs narrated a story of her sister, wherein her sister from another village did
not take her children to the AWC for weighing in last months. As a result her children were

141
not provided with the packets from their AWC. Therefore the woman stays at home during
weighing days. When asked about sending children regularly to AWC, she said that her elder
son baby sit her two younger daughters and those younger daughters are too young to go to
AWC. She was also not sure that whether her son is admitted into the AWC or not. But she
does remember that her son some days goes to AWC with other children from the
neighbourhood and some days not.
Children go to AWCs to get food and packets, when we migrate, we don’t get: Most of
the women from Katkari community participating in FGDs, from both the blocks, said that
their children go to AWCs. That way they get to eat something at the AWC and the family
also get packets of food. They further added that the teacher (AWWs) keep telling them to
prepare, ‘Upma’ and ‘Ladoo’, and give to the younger children at homes, but, upma tastes
salty and they prefer to make ‘Bhakaris’ (Indian Roti) out of it. The women said that the
bhakaris so made is eaten by everyone in the house. One woman went on to say that, she at
least makes such bhakaris, twice in a week for all.
Most of them expressed their concern that when they go to Vikramgad and Bhiwandi, for
work, they miss getting such packets. As two women argued that, the AWWs don’t give the
stock for another six months, whereas they get ‘Khauti’ (Ration from Tribal development
department to be used during rainy season) for 6/7 months from the government, during rainy
seasons. Similarly, they argued why they cannot get the packets as well. They finally said that
they need such packets more so ever at the working sites than when they are at villages in
their homes.
Below is the piece of the narration given by a woman from Mokhada FGDs,
“…Out of three/four, we don’t like one packet...it’s very salty…the rest we cook and
prepare…we make bhakaris more than upma and ladoo…during meeting at AWC,
when we go for immunisation, the sister and AW teacher tells us about how to cook
and all…but we cook our way…this month all packets are over...next month we will
travel to Bhiwandi for work, we might not get packets…we will return when farming
work will start…till then no packets…”
AWWs come home to take children for food, weighing and immunisation: Most of the
woman were familiar with the AWWs and were able to tell that the AWWs visit their homes
and ask about their children. Especially, the woman from Jawhar block, were able to
remember that AWWs come to their home to tell them about weighing, immunisation, Mata

142
Baithak and so on. Only few were not able to remember, the last time they had met AWWs
of their villages. This was, as explained by them, might be due to the fact that they must have
been away for work and someone else from their homes must have dealt with AWWs. Many
of the women knew their AWWs very well, even her family members and her parents and in-
laws as well. Most of the women said that they listen to AWWs and try to support her in her
activities also. One woman from Jawhar FGDs, said that,
“…earlier we used to be away at work and could not come to meetings…nowadays,
in a meeting, the sister and AWWs also come…and they give us tea and biscuit and
tell us about health, food, children, doctors, medicines and cleanliness...I like to
attend meetings of our AWW now…”
They call us for meetings, but I am at work: While speaking about their participation in
the meetings with AWWs, ANMs and ASHAs, many of the women agreed that since they are
at work, they cannot come and attend the meetings. Even when the ASHAs, AWWs go and
visit their homes, they are not available at homes. However, wherever possible, when they
happen to meet AWWs or sister, then they do tell them about immunisation, referrals, care of
SAM child, about next meeting etc. The women from Konkana tribe, were however able to
attend the meetings, as most of them were at homes and did not have to go out for work. Few
of the women from Konkana, nonetheless, mentioned that they had to go to fields during
farming days, to take food for all those working on farms and also to help and oversee the
work of labourers. Therefore when they become busy in those days, they miss few of the
meetings at AWCs. As narrated by one of the Konkana woman from Jawhar FGDs,
“…we have quite a large field…we grow rice, nacchani and vegetables…during
farming days my husband, brother-in-laws and mother-in-law, all go to field…I have
to wake up early in morning…finish cooking and pack the food and take it to field for
all of them…later I have to stay with them to help them and also join them in
overseeing the labourers…sometimes I cook for the labourers also and take food for
them as well…my mother-in-law says that, this way we can retain labourers or else
they would go somewhere else...in evening, when we are back, I have to again cook
for all…”
Few women from the Mokhada block said that, since most of the AWWs from their areas
knew that, they have every Tuesday off at the brick kilns, farms etc, they keep such meetings
on Tuesdays or they visit them on Tuesdays. But however few others mentioned that, since

143
Tuesday happens to be a weekly bazaar day, they go to have weekly ration and vegetables and
the staffs seldom finds them at homes.
Summary
In the backdrop of high prevalence of malnutrition in the blocks of Jawhar and Mokhada, one
saw the various programmes being implemented under ICDS projects. The highlight of
programmes being implemented by ICDS is that it has schemes and activities for all age
groups and target groups. For instance, for the age group of 0-3, the ICDS projects in Jawhar
and Mokhada distributed Take Home Rations (THR), conducted immunization sessions and
Health check-ups. Similarly the children were also considered for growth monitoring and
referral services. For the age group of 3-6, Anganwadis were conducted, wherein they were
given non-formal education and supplementary food. Similarly the pregnant and lactating
mothers were being provided with THR and immunization and the adolescent girls were
provided with supplementary food and health education.
In order to implement these activities, the staffs of ICDS were assigned roles and
responsibilities. From the job responsibilities of the staff, it was understood that they were
supposed to undertake certain tasks at facility level that is at AWC and at the same time they
at the community level like educational sessions, home visits, visits to AWCs by the
supervisor staff etc. Almost all were required to do the reporting work with several registers
and forms to be filled periodically. The supervisory staffs like ICDS supervisors have the
additional responsibility of serving as an important link between the field staff and the
system.
To facilitate the staff to carry out their tasks, they have been provided with various training
time and again by the system. It was seen in the chapter that almost every staff interviewed
under the study had been through certain kind of trainings. However it was learnt that there
was no training being provided specifically on malnutrition, except the training conducted by
Rajmata Jijau mission.
At the state policy level ICDS is assigned the task of implementing the Rajmata mission, thus
creating a blur line of authority and responsibility between the ICDS and the mission. For
example, the VCDC is being implemented by the ICDS machinery but funded by the HSS.
None of the staff from either of these departments were sure that whether this arrangement
would remain unchanged in future as well.

144
Moving further it is observed in the discussion, that most of the AWCs receive low
attendance of children. Secondly the SHGs were not able to provide the supplementary food
as per the chart to AWCs due to financial constraints. The credits bills of SHGs were not
being released on time, with delays of three/four months. Few of the SHGs were shutting
down primarily because of this reason.
When it comes to issues pertaining to staff, it came out during analysis that most of the
AWWs were having low morale. The factors that were identified as the reasons for this low
morale were, low salary/no increment, heavy reporting work, less knowledge about rules and
procedures of the system and inadequate support and guidance from the ICDS supervisors.
In the end, while analysing the factors responsible for affecting the implementation of the
ICDS activities like THR and conduct of anganwadi several factors came to light, for
examples, low attendance at AWCs, putting off the responsibility of identifying SAM/MAM
on AWWs, limited role of ICDS supervisors, limited monitoring in case of THR, lack of
infrastructure/staff/resources, field level challenges, low morale of AWWs and issues with
SHGs.
At the community level, the utilisation of such programmes remains low, this is preciously
because, of low priority assigned to children by the community. Secondly, the socio-cultural
barriers preventing them from accessing the programmes and thirdly availability of no time
and resources with the community to access the programmes and follow the advices given by
the staff and fourth reason is the geographical barriers because of difficult terrain, between
the staff and community.
Most of the women complained about non-availability of staff at field on continuous basis
and non-availability of facility like AWC buildings. There were complaints from them about
limited quantity of food during VCDCs. The women were also disturbed to receive non-
practical advices from the staff, for instances, cooking nutritious and separate food for
children, staying at CTC with children taking leave from work and attending meetings at
AWCs.
After having analyzed the programmes being implemented by HSS and ICDS, one came to
know that the poor implementation is accompanied by the low utilisation of programmes and
services by the community. This deadly combination creates a worrisome picture, calling an
urgent need of the system people, to rectify all the gaps and facilitate and improve the
implementation. At the same time, it is needed to introduce or enhance the educational and

145
IEC components of the programmes addressing malnutrition, to sensitize people about the
issue and gain their faith, in order to enhance acceptability and utilisation of services.





























