Embed Size (px)
Citation preview
CHAPTER I, SECTION-I
Introduction to Cancer
Chapter I, Sec I
1
CANCER
1.1.1 INTRODUCTION
Health is one of the most important domains which we human beings have
focused on in our society. However, cancer is a disease of striking significance in the
world today. It is the second leading cause of death after cardiovascular disease.
According to the International Agency of Research for Cancer (IARC), a 50% increase in
cancer rate within the next 20 years is expected.1 The prevalence of malignant cancers
and mortality due to cancer are also on the increase. This issue is a major concern,
especially in low to middle income countries where over a quarter of disease related
deaths are linked to cancer. 1, 2 With each passing minute, the cancer death toll are rising
and more people are being diagnosed with the disease. According to the World Cancer
report, 10 million new cancer cases are diagnosed annually, with over 7.1 million deaths
due to cancer each year that contribute to 12.6% of the global mortality rate.1 The report
estimates that about 22 million people worldwide are currently living with an oncological
disease. Since 1990, cancer incidence has risen about 19% and cancer mortality has
raised approximately 18% globally within the last decade. These numbers continue to
increase.
Cancer is the generic name for any malignant tumour.3 Hippocrates is credited
with naming the disease carcinos, which is Greek word meaning crab because of the
tumour’s crablike appearance. Later, carcinos was translated into the Latin word cancer.
Cancer is large and complex family of malignancies manifested with uncontrolled and
Chapter I, Sec I
2
undifferentiated cellular growth that replace older cells and affect virtually every organ in
the body. Cancer, a life threatening disease, is characterized by a shift in the controlled
mechanism that governs cell proliferation and differentiation. If this proliferation is
allowed to continue tumour spreading (a process called metastasis-local invasion,
intravasation, transport, extravasation, formation of micrometastasis, colonization) occurs
which can be fatal. Scientific research has elucidated the physiology, cause and treatment
of cancer.
In recent terminology, cancer describes a series of diseases in which abnormal
cells uncontrollably divide, invade other tissues and can spread throughout the body
using the lymph or circulatory systems. It is fundamentally a disease of failure of
regulation of tissue growth.
While there are more than 100 different types of cancer, there are five major categories: 4
Carcinoma is cancer that begins in the tissues that line organs.
Sarcoma is cancer that begins in bone, cartilage, muscle or other connective tissue.
Leukemia is cancer that starts in blood-forming tissue.
Lymphoma and myeloma are cancers of the immune system.
Central nervous system cancers affect the brain and spinal cord.
1.1.2 SYMPTOMS
Symptoms of cancer depend on the type and location of the cancer.5 For example;
lung cancer can cause coughing, shortness of breath or chest pain. Colon cancer often
causes diarrhoea, constipation and blood in the stool. Some cancers may not have any
Chapter I, Sec I
3
symptoms at all. In certain cancers, such as pancreatic cancer, symptoms often do not
start until the disease has reached an advanced stage.
The following symptoms can occur with most cancers:
Chills
Fatigue
Fever
Loss of appetite
Malaise
Night sweats
Weight loss
1.1.3 DIAGNOSIS
Like symptoms, the signs of cancer vary based on the type and locations of the tumour.5
Common tests include the following:
Biopsy of the tumour
Blood tests (which look for chemicals such as tumour markers)
Bone marrow biopsy (for lymphoma or leukemia)
Chest X-ray
Complete Blood Count (CBC)
Computed Tomography (CT) scan
Magnetic Resonance Imaging (MRI) scan
Chapter I, Sec I
4
Most cancers are diagnosed by biopsy. Depending on the location of the tumour, the
biopsy may be a simple procedure or a serious operation. Most patients with cancer
undergo CT scans to determine the exact location of the tumours.
1.1.4 FACTORS RESPONSIBLE FOR CANCER
Cancer causing factors are classified as follows:
1.1.4.1 External factors
a) Chemicals: Exposure to asbestos, benzene, benzidine, cadmium, nickel or vinyl
chloride in the workplace can cause cancer.6
b) Radiation: Radioactive fallout can come from accidents at nuclear power plants or
from the production, testing or use of atomic weapons. People exposed to fallout may
have an increased risk of cancer, especially leukemia and cancers of the thyroid, breast,
lung and stomach.7
c) Infectious organisms: Worldwide approximately 18% of cancers are related to
infectious diseases. This proportion varies in different regions of the world from high of
25% in Africa to less than 10% in the developed world.8
Viruses are usual infectious agents that cause cancer but bacteria and parasites
may also have an effect. A virus that can cause cancer is called an oncovirus. These
include human papillomavirus (cervical carcinoma), epstein-barr virus (B-cell
lymphoproliferative disease and nasopharyngeal carcinoma), kaposi's sarcoma
herpesvirus (kaposi’s sarcoma and primary effusion lymphomas), hepatitis B and
Chapter I, Sec I
5
hepatitis C viruses (hepatocellular carcinoma) and human T-cell leukemia virus-1 (T-cell
leukemias).
Bacterial infection may also increase the risk of cancer, as seen in helicobacter
pylori-induced gastric carcinoma.
Parasitic infections strongly associated with cancer include schistosoma
haematobium (squamous cell carcinoma of the bladder) and the liver flukes, Opisthorchis
viverrini and Clonorchis sinensis (cholangiocarcinoma)
d) Geographical location: Prostate cancer (PCa) occurrence and mortality are well
known to vary greatly in different geographic regions of the world, with low risks of PCa
mortality characteristic of Asia and high risks of PCa mortality characteristic of the US
and Western Europe.9
e) Lifestyle and Environment: Healthy life style behavior for cancer risk reduction
includes:
Diet: Fruits and vegetables contain many antioxidants and phytochemicals, such as
vitamins A, C, E and beta-carotene, which have been shown to prevent cancer.10 Studies
have shown the risk of prostate cancer drops for men who eat tomato products, possibly
because of the phytochemical lycopene. It has been shown that colon cancer declines
among those who drink green tea, which contains antioxidants and phytochemicals and
who regularly, eat soy products and foods rich in selenium, an antioxidant. High-fiber
diets are thought to reduce the risk of colon cancer because the fiber helps move food
Chapter I, Sec I
6
through the lower digestive tract, possibly reducing the contact of any carcinogens with
the bowel lining.
Recommendations of the American Cancer Society to reduce the risk of cancer
include consumption of a mostly plant-based diet, including five or more servings of
fruits and vegetables each day, consumption of whole grains in preference to processed or
refined grains and sugar, limited consumption of high-fat foods and avoiding excessive
use of overheated animal food.
Cessation of smoking and alcohol consumption: Tobacco use has been reported to be
the main cause of 90% of male and 79% of female lung cancers and about 90% of lung
cancer deaths are estimated to be due to smoking.11 The risk of the development of lung
cancer in lifelong smokers is 20-40 times higher than non-smokers. People who use
tobacco products regularly are more likely to develop acute myeloid leukemia (cancer
that starts in blood cells). Cigarette smoke like benzopyrene is carcinogenic. Metabolites
occurring during the activation of carcinogens bind covalently with DNA and DNA
adducts are formed which are regarded as an indicator of cancer risk in smokers. The risk
of individual cancer development is determined by the balance between the metabolic
activation and detoxification of the carcinogens in smoke. Free radicals in cigarette
smoke cause oxidative damage and mutations in DNA which leads to activation of
oncogenes and inhibition of tumour suppressor genes. Drinking small amounts of alcohol
has been shown to offer some protection for people at risk of heart disease, which
normally applies to people over the age of 40. However, heavy consumption of alcohol
Chapter I, Sec I
7
has also been shown to increase the risk of developing cancer of the mouth, pharynx,
larynx, esophagus, liver and breast.
1.1.4.2 Internal factors
a) Inherited mutations: The genetic changes that lead to unregulated cell growth may be
acquired in two different ways. It is possible that the mutation can occur gradually over a
number of years, leading to the development of a 'sporadic' case of cancer. Alternatively,
it is possible to inherit dysfunctional genes leading to the development of a familial form
of a particular cancer type.
Some examples of cancers with known hereditary components include:
Breast cancer - Inheritance of mutant versions of the BRCA1 and BRCA2 genes are
known risk factors.12 Although many, if not most, individuals with breast cancer do not
have detectable alterations in these genes, having a mutant form increases the likelihood
of developing breast cancer.
Colon cancer - Defects in DNA repair genes such as MSH2 are known to predispose
individuals to hereditary non-polyposis colorectal cancer (HNPCC).13
Retinoblastoma - Defects in the Retinoblastoma tumour suppressor gene are known to
cause eye cancer and several other types of cancers.14
b) Hormones: Certain hormones may increase the risk of breast cancer, heart attack,
stroke or blood clots. For example, Diethylstilbestrol (DES) is a synthetic form of the
hormone estrogen that was prescribed to pregnant women to prevent miscarriage,
Chapter I, Sec I
8
premature labor and related complications of pregnancy. Women who took DES during
pregnancy have an increased risk of breast cancer.15
c) Immune conditions: Cancer is an immune-mediated disease. Immune system cells
participate in all stages of tumour genesis and immunosurveillance. Chronic infections
and inflammation associated with limited or polarized immune responses also contribute
to carcinogenesis and tumour progression.16
d) Age: The most important risk factor for cancer is growing older. Most cancers occur in
people over the age of 65.
1.1.5 CELL AND CELL CYCLE
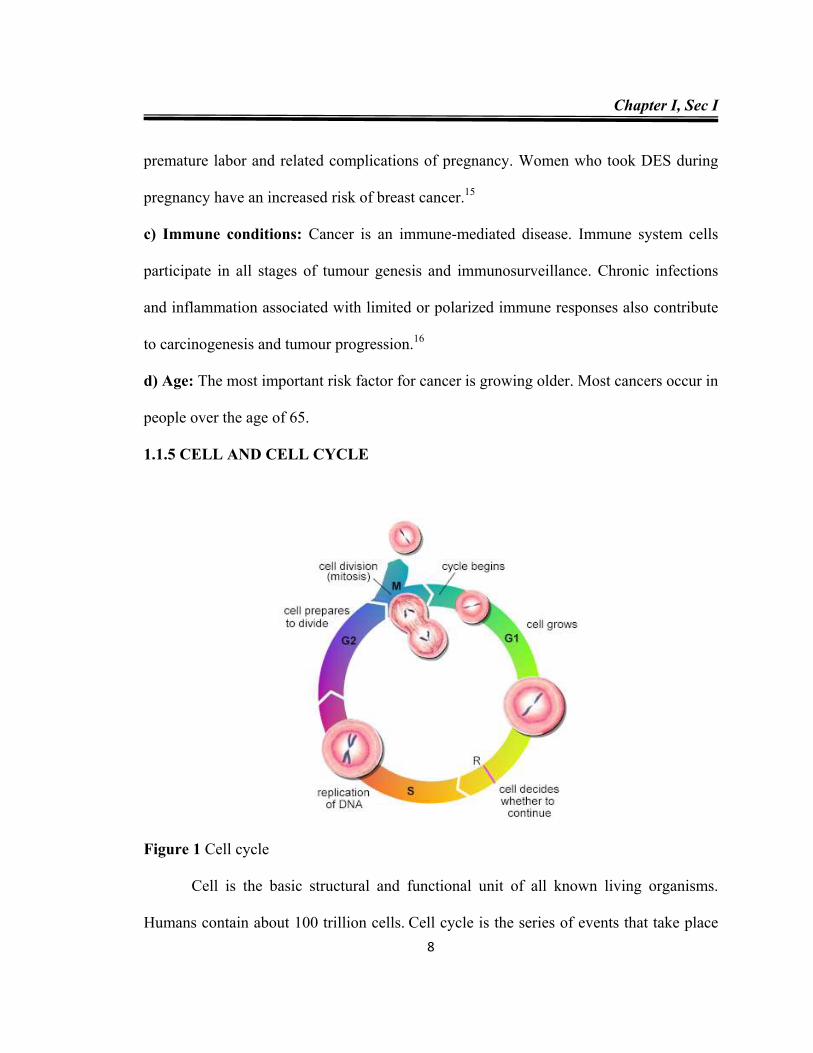
Figure 1 Cell cycle
Cell is the basic structural and functional unit of all known living organisms.
Humans contain about 100 trillion cells. Cell cycle is the series of events that take place
Chapter I, Sec I
9
in a cell leading to its division and duplication. In cells without a nucleus (prokaryotic),
the cell cycle occurs via a process termed binary fission.
In cells with a nucleus (eukaryotes), the cell cycle can be divided in two brief periods:
interphase, during which the cell grows, accumulating nutrients needed for mitosis and
duplicating its DNA, and the mitosis (M) phase, during which the cell splits itself into
two distinct cells, often called "daughter cells". The cell cycle consists of four distinct
phases (Fig 1):17
Gap 1 (G1) phase: Cell grows in size and checks the status of its internal systems. If
everything is functioning normally and any damage to the DNA has been corrected,
the cell moves on through the cycle. If something is wrong and cannot be corrected,
the cell halts its progression through the cycle and may initiate apoptosis and close
down. In the accompanying diagram, R marks the point where restriction of the cycle
can occur.
Synthetic (S) phase: The cell constructs proteins, RNA and DNA replication occurs
during this phase.
Gap 2 (G2) phase: The cell continues to grow and The G2 checkpoint control
mechanism ensures that everything is ready to enter the M phase and divide.
Mitosis (M) phase: Cell growth stops at this stage and cell divide into two cells.
The total length of a cell cycle varies depending on the specialized function of a cell.
Chapter I, Sec I
10
1.1.6 TUBULIN AND MICROTUBULES
Microtubules are key components of the cytoskeleton. They are used as molecular
‘highways’ for transport of materials from one part of the cell to another. Tubulin
heterodimers made up of α- and β-tubulin (50 kDa each in size) are the basic structural
components that constitute microtubules. α- and β-tubulin both have a molecule of GTP
attached to them and are capable of forming heterodimers. These dimers attach to each
other with the hydrolysis of the GTP in the β-tubulin to form chains of alternating α and
β-tubulin called protofilament. Thirteen of these protofilaments come together to form a
tube like structure called microtubule.18 Each dimer in protofilament has directionality as
the β-tubulin and α-tubulin are not identical. The protofilaments arrange themselves in
such a way that the directionality is retained in the microtubule. Thus one end of the
microtubule is called the plus end and the other end is called the minus end. In a free
microtubule, the tubulin dimers keep adding at the plus end and keep falling off at the
minus end. This is called treadmilling.
While formation of the protofilament of the microtubule, the GTP attached to the
β-tubulin undergoes hydrolysis to form GDP. β-tubulin is more stable when it is
associated with a GTP molecule than when it is associated with a GDP molecule.19 So the
formation of microtubule which is driven by GTP hydrolysis leads to destabilization of
its own self. This makes microtubule capable of undergoing catastrophic destruction by
converting GDP to GTP and stabilizing β-tubulin monomers. Thus microtubules in the
cell keep undergoing random cycles of polymerization and de-polymerization.20
Chapter I, Sec I
11
Microtubules are involved in a wide variety of cellular functions such as cell
division, morphology, regulation of motility, signalling and various intracellular
processes.21 They are extremely important in the process of mitosis, during which the
duplicated chromosomes of a cell are separated into two identical sets before cleavage of
the cell into two daughter cells (Fig 2).22 In the mitotic phase of the cell cycle,
microtubules are in dynamic equilibrium with tubulin dimers as tubulin is assembled into
microtubules, which are disassembled to tubulin. Since inhibition of tubulin
polymerization increases the number of cells in metaphase arrest, microtubules are
attractive molecular targets for anticancer therapeutics.
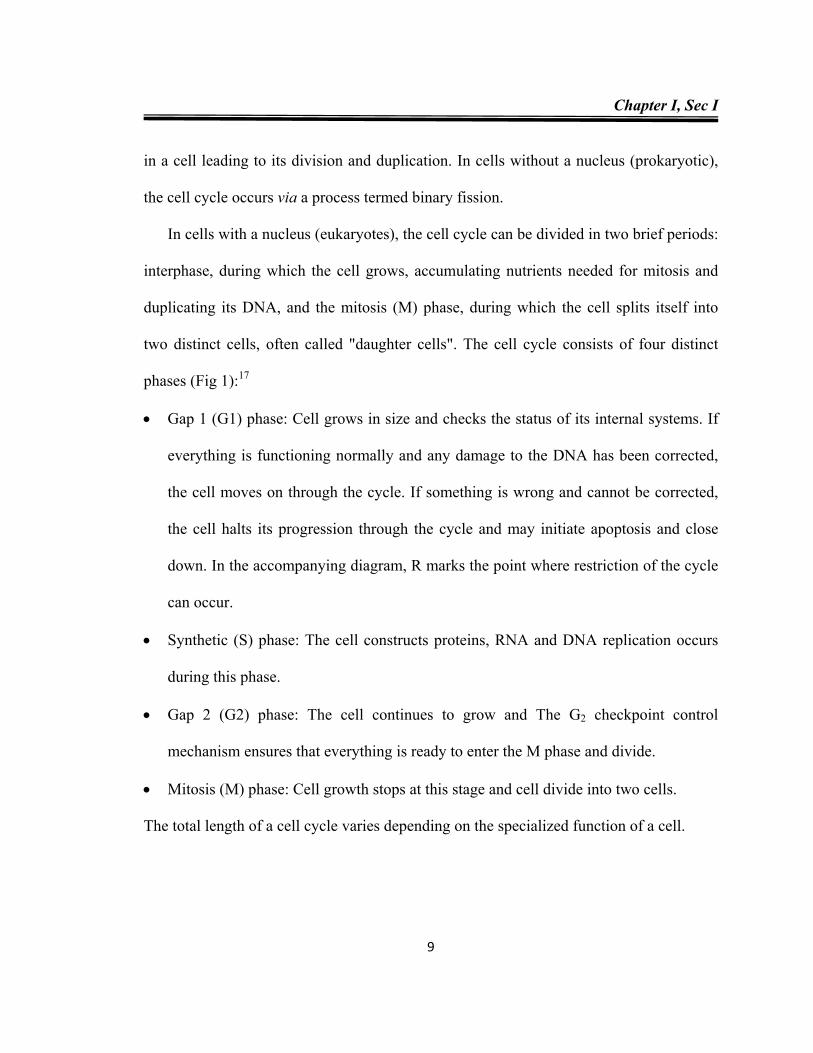
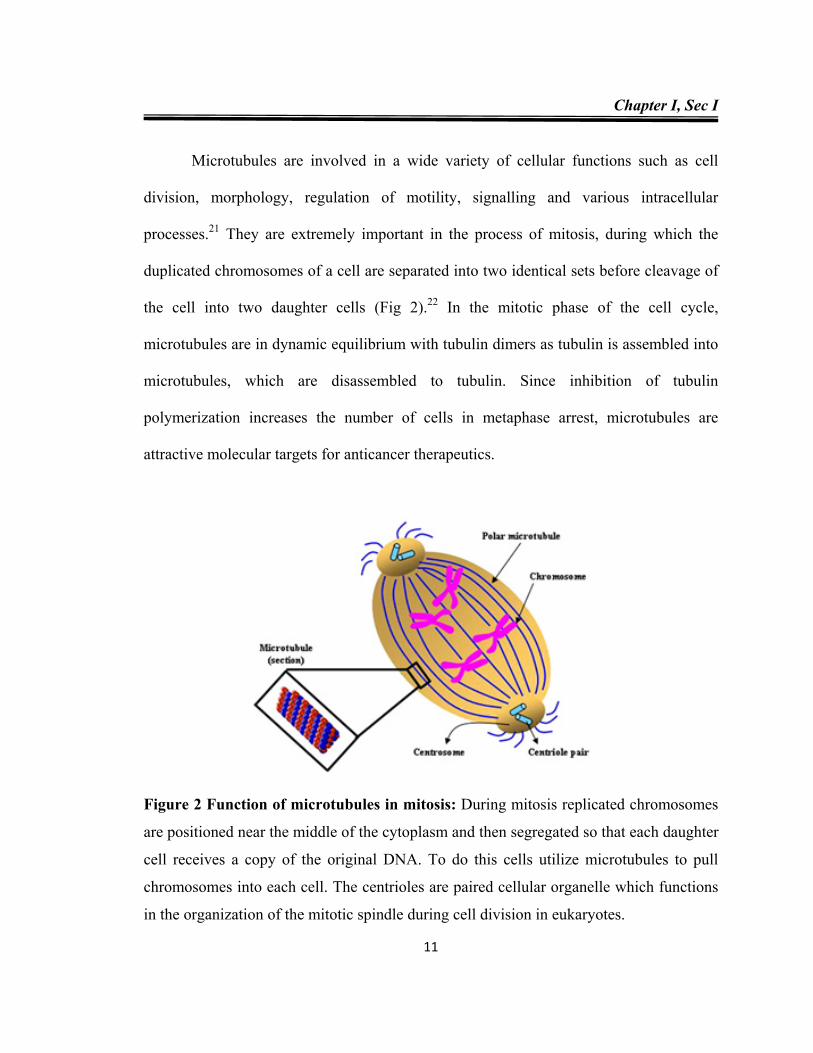
Figure 2 Function of microtubules in mitosis: During mitosis replicated chromosomes
are positioned near the middle of the cytoplasm and then segregated so that each daughter
cell receives a copy of the original DNA. To do this cells utilize microtubules to pull
chromosomes into each cell. The centrioles are paired cellular organelle which functions
in the organization of the mitotic spindle during cell division in eukaryotes.
Chapter I, Sec I
12
1.1.7 CANCER TREATMENTS
In 1846, anesthesia became commonly available to surgeons, resulting in an
increase in the use of surgery as a cancer treatment option.23 As expected, surgery entails
removal of the tumour and often some tissue surrounding or adjacent to the tumour area.
Today treatment selection depends upon the specific form of cancer and its progression.
Current treatment options are sophisticated and widely varied; including targeted therapy,
immunotherapy, hormonal therapy, stem cell or bone marrow transplantation,
hyperthermia, photodynamic therapy, surgery, radiation and chemotherapy, with each
treatment pathway having inherent drawbacks as well as unique benefits. Typically
physicians and cancer professionals describe a cancer based on when the cancer was
detected and how far it has progressed, referred to as staging. Surgery also provides a
means to verify the presence and stage of cancer. One major drawback to surgery is the
fact that sometimes the cancer is widespread and not all of it can be removed. For this
reason and because of the natural cancer cell growth, surgery is usually used in tandem
with an additional form of treatment.
In 1895, cancer treatment was drastically changed when Wilhelm Conrad
Roentgen invented the X-ray, the resulting technology that would give rise to the option
of radiation therapy for cancer treatment. Radiation therapy uses X-rays to target and kill
cancer cells. There are several types of radiation therapy, including internal radiation and
proton therapy; the most common is external-beam radiation therapy in which a machine
positioned outside the patient’s body produces and projects the radiation beam.24 One
Chapter I, Sec I
13
benefit of radiation therapy is that it is a local treatment, affecting the specific part of the
body receiving the therapy. When used in conjunction with surgery, radiation often
proves effective at initially shrinking a tumour to improve the success of subsequent
surgery.
As revolutionary as radiation therapy has been it has many side effects such as
fatigue, mild skin reactions, upset stomach and loose bowel movements.25 Internal
radiation therapy has been cited as causing bleeding, infections and irritation after the
implant is removed.25 These are the short-term side effects, with long-term effects
including the risk of a second cancer, infertility, heart problems, gastrointestinal
problems, lung fibrosis, neurologic problems, thyroid problems or osteoporosis.26
Another cancer treatment, chemotherapy, became available in 1919 when it was
found that a component of mustard gas could reduce white blood cells.27 These
chemotherapeutic drugs halt a cancer cell’s unchecked ability to grow and divide, causing
cell death and reduction of the cancer. Chemotherapy drugs have resulted in more varied
treatment plans using combinations of surgery, radiation and chemotherapy drugs. Side
effects of chemotherapy depend upon the dosage level and how the patient reacts to the
drugs but typically involve fatigue, risk of infection, nausea, vomiting, loss of appetite
and diarrhea. While the side effects of these chemotherapy drugs are usually temporary,
disappearing when the treatment is over, all of the current treatments are physically and
psychologically taxing for the patient; thus, current research focuses on developing more
effective therapeutics with fewer and less severe side effects.
Chapter I, Sec I
14
1.1.8 CHEMOTHERAPY IN CANCER TREATMENT
Chemotherapy is a kind of treatment that uses drugs to attack cancer cells. 28 It is
called a "systemic treatment" since the drug, entering through the blood stream, travels
throughout the body and kills cancer cells at their sites. The drugs may rarely be intended
to have a local effect, but in most cases, the intention is to destroy cancer cells wherever
they may exist in the body. Chemotherapeutic drugs are divided into several categories
based on how they affect specific chemical substances within the cancer cells, which
cellular activities or processes the drug interferes with and which specific phases of the
cell cycle the drug affects. These include:
DNA topoisomerase I and II inhibitors
Apoptosis inducing agents
Antimitotic agents
Antimetabolites
DNA interactive agents and miscellaneous agents
Chemotherapeutic drugs are chemically designed to target cells that are dividing and
growing rapidly. They target the carcinogenic sequence, generally exploiting the rapid
progression of cancer cells throughout the cell cycle. Once they reach the cancer cells,
they act to retard their growth, eventually resulting in their destruction. Chemotherapy
may be given at home, in a clinic or in a hospital. The frequency of chemotherapy can be
daily, weekly, monthly or an on-off schedule depending on the type of drug, the body's
response and the type of cancer. The chemotherapy is decided on the basis of the type of
Chapter I, Sec I
15
cancer. The dosage is calculated on the basis of the patient's body weight and the drug's
toxicity.
Ideal anticancer drugs would eradicate cancer cells without harming normal tissues.
Unfortunately no currently available agents meet this criterion. Two major concerns with
currently available anticancer drugs are their inability to discriminate between normal
and tumour cells and hence unpleasant drug toxicities and development of resistance due
to expression of drug transporters. Thus clinical use of drugs involves a weighing of
benefits against toxicity in a search of favorable therapeutic index. At present more than
50 anticancer drugs has been discovered. They are used in several ways:
Monotherapy or only one drug
Combination chemotherapy or a group of drugs which work together
Combined modality or chemotherapy along with other treatment such as surgery and
radiotherapy
The drugs are delivered to the affected cells in the following forms:
Oral (tablet form, by mouth)
Intravenous or Intramuscular (injected by needle into a vein or muscle)
Intrathecal chemotherapy (injected through a needle in the back)
1.1.9 CLASSIFICATION OF ANTICANCER DRUGS
Chemotherapeutic drugs can be divided into two main classes based on their
action on the cell cycle: cell cycle non-specific and cell cycle specific.
Chapter I, Sec I
16
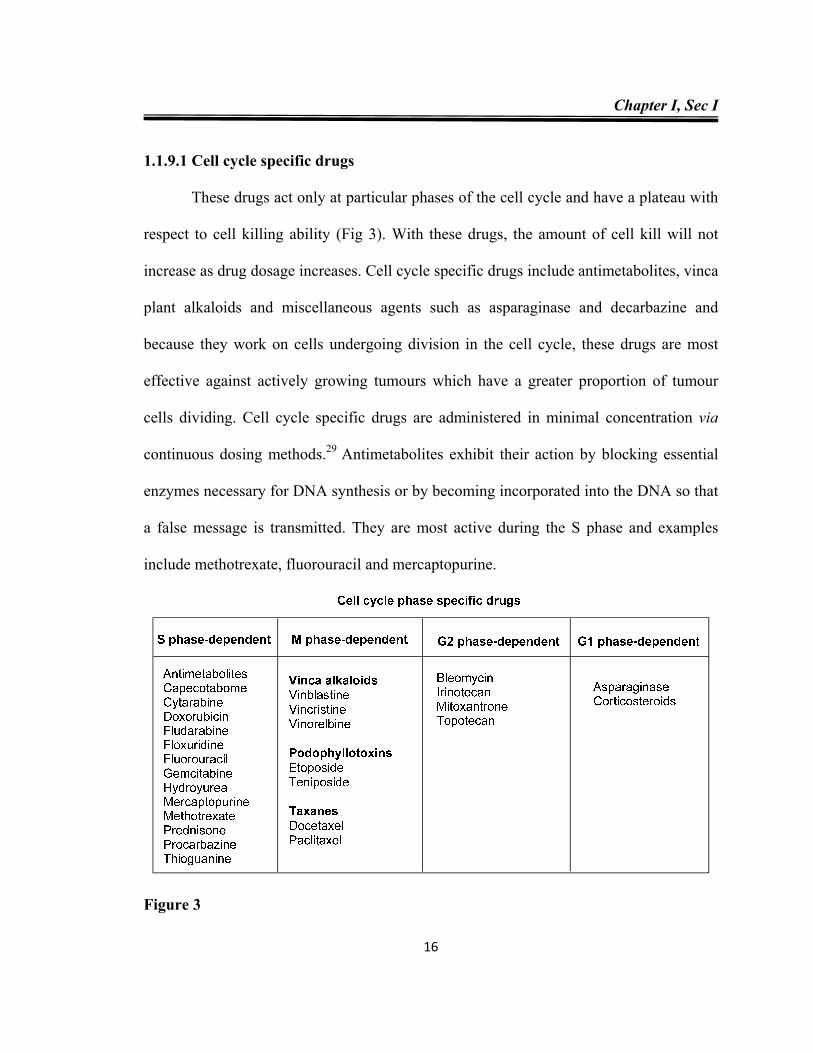
1.1.9.1 Cell cycle specific drugs
These drugs act only at particular phases of the cell cycle and have a plateau with
respect to cell killing ability (Fig 3). With these drugs, the amount of cell kill will not
increase as drug dosage increases. Cell cycle specific drugs include antimetabolites, vinca
plant alkaloids and miscellaneous agents such as asparaginase and decarbazine and
because they work on cells undergoing division in the cell cycle, these drugs are most
effective against actively growing tumours which have a greater proportion of tumour
cells dividing. Cell cycle specific drugs are administered in minimal concentration via
continuous dosing methods.29 Antimetabolites exhibit their action by blocking essential
enzymes necessary for DNA synthesis or by becoming incorporated into the DNA so that
a false message is transmitted. They are most active during the S phase and examples
include methotrexate, fluorouracil and mercaptopurine.
Figure 3
Chapter I, Sec I
17
1.1.9.2 Cell cycle nonspecific drugs
These drugs are active in all phases of the cell cycle and may be effective in large
tumours that have few active cells dividing at the time of administration. Drugs of this
nature are often given as a single bolus injection.30 These have a linear dose-response
curve, which means that the greater the dose of drug that is given, the greater is the
fraction of cells within the tumour that are killed. These drugs are active on cells in either
a dividing or a resting state and include:
Nitrogen mustards - Meclorethamine, Cyclophosphomide, Ifosfamide, Chlorambucil,
Melphalan
Ethylanimine - Thiotepa
Alkyl sulfonate - Busulfan
Nitrosoureas- Carmustine, Lomustine
Triazine derivatives - Dacarbazine
Miscellaneous – L-Asparginase, Cisplatin, Procarbazine
1.1.10 ANTIMITOTIC AGENTS
Chemical compounds targeting microtubules exert their inhibitory effects on cell
proliferation primarily by blocking mitosis, which requires an exquisite control of
microtubule dynamics. Microtubule-targeting drugs are therefore also frequently referred
to as a group of antimitotic drugs and their actions on microtubule stability and dynamic
parameters differ from each other. They interact physically with tubulin by binding to one
Chapter I, Sec I
18
of the three main binding sites: colchicine-, vinblastine- or paclitaxel- binding sites.31
They are usually classified into two main groups:
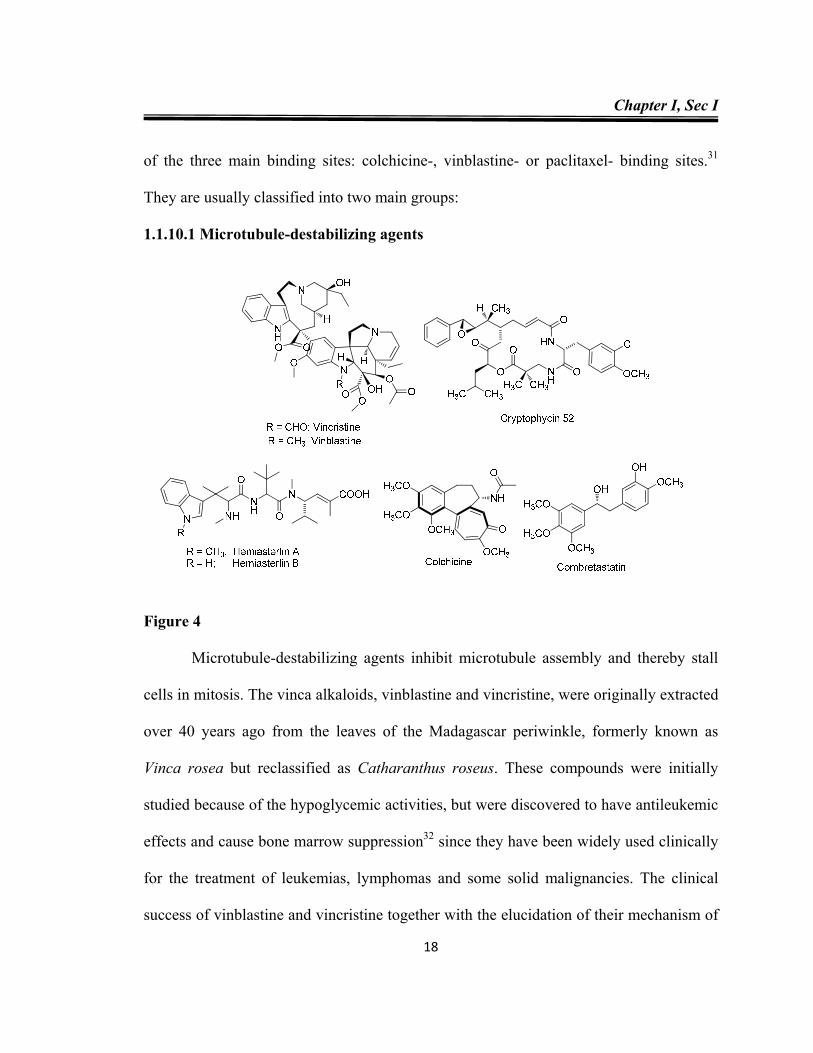
1.1.10.1 Microtubule-destabilizing agents
Figure 4
Microtubule-destabilizing agents inhibit microtubule assembly and thereby stall
cells in mitosis. The vinca alkaloids, vinblastine and vincristine, were originally extracted
over 40 years ago from the leaves of the Madagascar periwinkle, formerly known as
Vinca rosea but reclassified as Catharanthus roseus. These compounds were initially
studied because of the hypoglycemic activities, but were discovered to have antileukemic
effects and cause bone marrow suppression32 since they have been widely used clinically
for the treatment of leukemias, lymphomas and some solid malignancies. The clinical
success of vinblastine and vincristine together with the elucidation of their mechanism of
Chapter I, Sec I
19
action on cellular microtubules, have facilitated the development of several semi-
synthetic derivatives notably vindesine, vinorelbine and vinflunine, which are now used
in the clinic for the treatment of cancer.33 The other microtubule destabilizing agents
include cryptophycin 52, hemiasterlins, estramustine, colchicine and combretastatins (Fig
4).
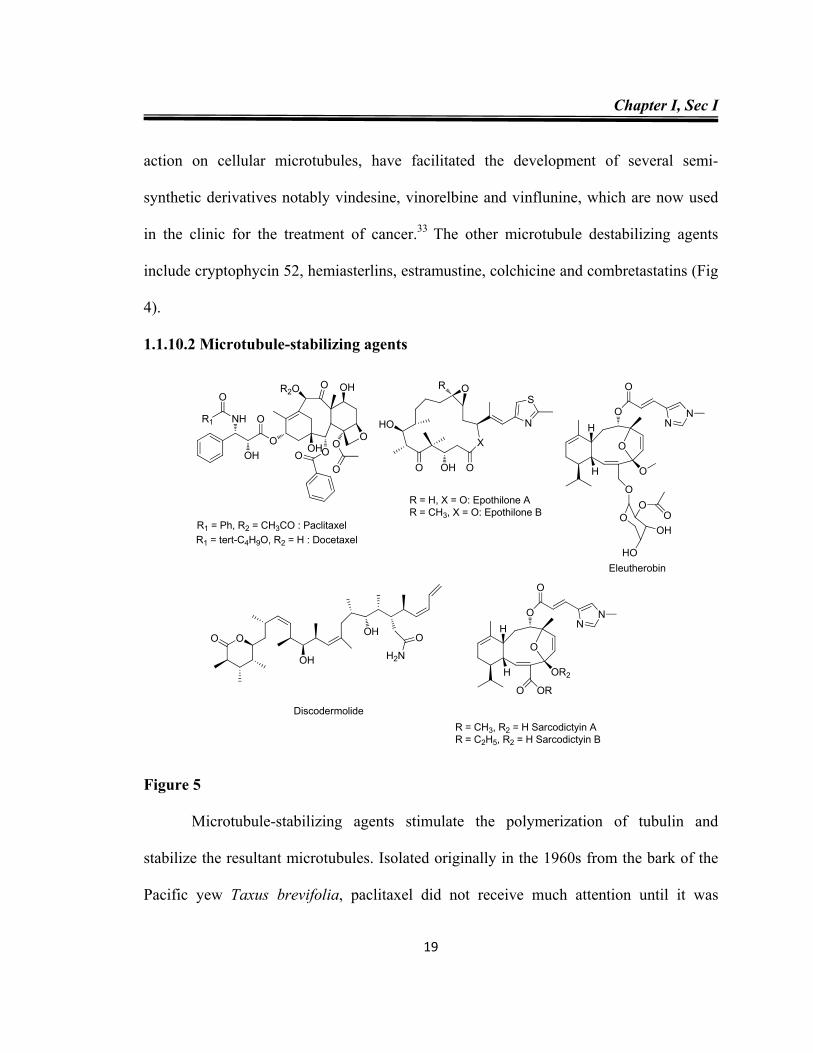
1.1.10.2 Microtubule-stabilizing agents
Figure 5
Microtubule-stabilizing agents stimulate the polymerization of tubulin and
stabilize the resultant microtubules. Isolated originally in the 1960s from the bark of the
Pacific yew Taxus brevifolia, paclitaxel did not receive much attention until it was
O
X
O
OR
N
S
OH
HO
R = H, X = O: Epothilone AR = CH3, X = O: Epothilone B
O
ON
N
O
H
H OR2
ORO
R = CH3, R2 = H Sarcodictyin AR = C2H5, R2 = H Sarcodictyin B
O
O
O
OO
O
OO
OHR2O
OH
NHR1
O
OH
R1 = Ph, R2 = CH3CO : PaclitaxelR1 = tert-C4H9O, R2 = H : Docetaxel
O
ON
N
O
H
H O
O
OO
OOH
HOEleutherobin
OO OH
H2N
O
OH
Discodermolide
Chapter I, Sec I
20
discovered to possess microtubule stabilizing activity.34 This drug is now in widespread
use for the treatment of breast, ovarian, prostate and non-small cell lung cancer, as well
as kaposi’s sarcoma. Its semisynthetic analog, docetaxel, is synthesized from a precursor
isolated from the needles of the European yew Taxus baccata. Docetaxel is more water-
soluble than paclitaxel and is also more active than paclitaxel against cancer cell
proliferation and is now used clinically for the treatment of breast, prostate and non-
small-cell lung cancer.35 The other microtubule-stabilizing agents include epothilones,
eleutherobin, discodermolide and sarcodictyins (Fig 5).
Chapter I, Sec I
21
REFERENCES
1. B. W, Stewart, P. Kleihues, World Health Report 2002: Reducing risks, promoting
healthy life., Geneva, WHO. 2002.
2. J. P, Bond, P. B. Celestino, M. C. Mahoney, C. D. Farrell, J. E. Bauer, J. L. Hastrup,
K. M. Cummings, J cancer educ., 2002 18, 96.
3. www.cancer.org/downloads/STT/ CAFF2007PWSecured.pdf.
4. R. G. McKinnell, R. E. Parchment, A. O. Perantoni, G. B. Pierce, Cambridge
University Press., newyork, 1998, 51.
5. a) J. A. Moscow, K. H. Cowan, Biology of cancer. In L. Goldman, A. I. Schafer eds.
Cecil Medicine. 24th ed. Philadelphia, Pa: Saunders Elsevier; 2011: chap 185. b) M. J.
Thun, A. Jemal, Epidemiology of cancer. In L. Goldman A. I. Schafer, eds. Cecil
Medicine. 24th ed. Philadelphia, Pa: Saunders Elsevier; 2011: chap 183.
6. P. A. Oliveira, A. Colaço, R. Chaves, H. G. Pinto, L. F. P. D. L. Cruz, C. Lopes, An.
Acad. Bras. Ciênc., 2007, 79, 593.
7. A. Frieben, Fortsch. Geb. Roentgenstr., 1902, 6, 106.
8. a) P. Pisani, D. M. Parkin, N. Munoz, J. Ferlay, Biomarkers Prev., 1997, 6, 387. b) D.
M. Parkin. Int. J. Cancer., 2006, 118, 3030.
9. S. Bingham, E. Riboli, Nat. Rev. Cancer., 2004, 4, 206.
10. H. S. Garewal, S. Schantz, Arch. Otolaryngol. Head Neck Surg., 1995, 121, 141.
11. C. L. Vecchia, S. Franceschi, Eur. J. Cancer Prev., 2003, 12, 5.
12. R. L. Milne, Antoniou, Ann. Oncol., 2011, 22, i11
Chapter I, Sec I
22
13. A. K. Rustg, Genes Dev., 2007. 21, 2525.
14. C. J. Sherr, F. McCormick, Cancer Cell, 2002, 2,103.
15. a) J. R. Palmer, L. A .Wise, E. E. Hatch, R Troisi, L. T. Ernstoff, W. Strohsnitter, R.
Kaufman, A. L. Herbst, K. L. Noller, M. Hyer. R. N. Hoover Cancer Epidemiol.
Biomarkers Prev., 2006, 15, 1509. b) M. M. Rubin, Obstet. Gynecol. Surv., 2007, 62,
548.
16. B. F. Zamarron, W. Chen, Int. J. Biol. Sci., 2011, 7, 651.
17. B. Alberts, D. Bray, J. Lewis, M. Raff, K. Roberts, J. D. Watson, Molecular Biology
of the Cell, 5th edn (New York, Garland Publishing, Inc.) 2007.
18. L. Amos, A. Klug, J. Cell Sci., 1974, 14, 523.
19. V. I. Gelfand, A. D. Bershadsky, Annu. Rev. Cell Biol., 1991, 7, 93.
20. H. P. Erickson, E. T. O'. Brien, Annu. Rev. Biophys. Biomol. Struct., 1992, 21, 145.
21. M. A. Jordan, L. Wilson, Nat. Rev. Cancer, 2004, 4, 253.
22. G. F.V. Ismael, D. D. Rosa, M. S. Mano, A. Awada, Cancer Treat. Rev, 2008, 34, 81.
23. http://www.aarp.org/health/conditions-treatments/info-03-2012/history-of-cancer-
timeline.html (Accessed Feb 23, 2013).
24. http://www.cancer.gov/cancertopics/coping/radiation-therapy-and-you/page3
(Accessed Feb 23, 2013).
25. W.D. Bloomer, S. Hellman, New Engl. J. Med., 1975, 293, 80.
26. O. A. Mefty, J. E. Kersh, A. Routh, R. R. Smith, J. Neurosurg., 1990, 73, 502.
27. V.T. DeVita, E. Chu, Cancer Res., 2008, 68, 8643.
Chapter I, Sec I
23
28. A. Desai T. J. Ann, Rev. Cell Dev. Biol., 1997, 13, 83.
29. G. Morgan, Cancer Nurs. Pract., 2003, 2, 27.
30. M. A. Jordan, L. Wilson, Nature Rev., 2004, 4, 253
31. M. N. Islam, M. N. Iskander, Mini-Rev. Med. Chem., 2004, 4, 1077.
32. a) I. S. Johnson, H. F. Wright, G. H. Svoboda, J. Vlantis, Cancer Res., 1960, 20,
1016. b) J. H. Cutts, C. T. Beer, R. L. Noble, Cancer Res., 1960, 20, 1023.
33. A. Duflos, A. Kruczynski, J. M. Barret, Curr. Med. Chem. Anti-Canc Agents, 2002, 2,
55.
34. P. B. Schiff, S. B. Horwitz, Proc. Natl. Acad. Sci. USA, 1980, 77, 1561.
35. Ringel, S. B. Horwitz, J. Natl. Cancer Inst., 1991, 83, 288.
CHAPTER I, SECTION-II
Introduction to Catalysis
Chapter 1, Sec II
24
CATALYSIS
1.2.1 INTRODUCTION
In the early part of the 19th century, when the scientific study of chemistry was just
beginning, it was observed that the occurrence of a number of chemical reactions was
conditional upon the presence of trace amounts of substances that did not themselves take
part in the reaction. In 1836, Swedish scientist J. J. Berzelius conveyed these
observations into the body of chemical knowledge by attributing their action to what he
called their catalytic power, this action he named as catalysis by analogy.1 He assumed
that catalysts possess special powers that can influence the affinity of chemical
substances. The word catalysis comes from Greek word meaning ‘to break down’. Later,
William Ostwald was the first to write down a definition of the catalyst: “a catalyst
accelerates a chemical reaction without affecting the position of the equilibrium.”2
Ostwald recognized catalysis as a ubiquitous phenomenon that was to be explained in
terms of the laws of physical chemistry. While it was formerly assumed that the catalyst
remained unchanged in the course of the reaction, it is now known that the catalyst is
involved in chemical bonding with the reactants during the catalytic process.
Thus catalysis is a cyclic process: the reactants are bound to one form of the
catalyst and the products are released from another, regenerating the initial state. Apart
from accelerating reactions, catalysts have another important property that they can
influence the selectivity of chemical reactions. This means that completely different
products can be obtained from a given starting material by using different catalyst
Chapter 1, Sec II
25
systems. Industrially, this targeted reaction control is often even more important than the
catalytic activity.
Catalysts can be gases, liquids, or solids. Most industrial catalysts are liquids or
solids, whereas the latter react only via their surface. They have been successfully used in
the chemical industry for more than 100 years, examples includes the synthesis of
sulfuric acid, the conversion of ammonia to nitric acid and catalytic hydrogenation. In
fact that 75% of all chemicals are produced with the aid of catalysts; in newly developed
processes, the figure is over 90%. Many organic intermediates and products, synthetic
fibers, pharmaceuticals, dyes, crop-protection agents, resins and pigments can only be
produced by catalytic processes.3 Most of the processes involved in crude-oil processing
and petro-chemistry, such as purification stages, refining and chemical transformations
require catalysts. Manufacturing protocols can be made more economic, green and
sustainable by the design and vigilant use of catalysts.
Catalysis can be broadly divided into two branches: homogeneous and heterogeneous.
1.2.2 HOMOGENEOUS CATALYSIS
A homogeneous catalyst, where the catalyst is in the same phase as the reactants, is
generally accepted by chemists.4 The most attractive property is that all catalytic sites are
accessible because the catalyst is generally a soluble metal complex. Furthermore, it is
possible to tune the chemo-, regio- and enantio-selectivity of the catalyst. Homogeneous
catalysts have a number of other advantages such as high selectivities, better yield and
easy optimization of catalytic systems by modification of ligand and metals. Despite their
advantages and their wide use in a number of applications, many homogeneous catalytic
Chapter 1, Sec II
26
systems have not been commercialized because of the difficulty encountered in
separating the catalyst from the final reaction product. Removal of trace amounts of
catalyst from the end product is essential since metal contamination is highly regulated,
especially by the pharmaceutical industry. Even with the extensive and careful use of
various techniques such as distillation, chromatography or extraction, removal of trace
amounts of catalyst remains a challenge. To overcome the separation problems in
homogeneous catalysis, chemists and engineers have investigated a wide range of
strategies and the use of heterogeneous catalyst systems appears to be the best logical
solution.5
1.2.3 HETEROGENEOUS CATALYSIS
Heterogeneous catalysis involves a reaction in which one or more of the
constituents are in different phases. Thus, a heterogeneous catalyst is normally insoluble
in the reaction medium. From an industrial point of view, heterogeneous catalysts are of
interest for a number of reasons and comparison of the properties of homogeneous and
heterogeneous catalysts are summarized in Table 1. Heterogenization is commonly
achieved by entrapment or grafting of the active species on surfaces or inside the pores of
a solid support, such as silica, alumina or ceria. Although grafting can be achieved by
covalent binding or by simple adsorption of the active catalytic species, covalent binding
is preferred because it is generally sufficiently robust to survive the harsh reaction
conditions; this binding and adsorption process minimizes catalyst leaching and allows
the catalyst to be reused several times.6 A vast majority of the industrial heterogeneous
catalysts are high-surface area solids onto which an active component is dispersed or
Chapter 1, Sec II
27
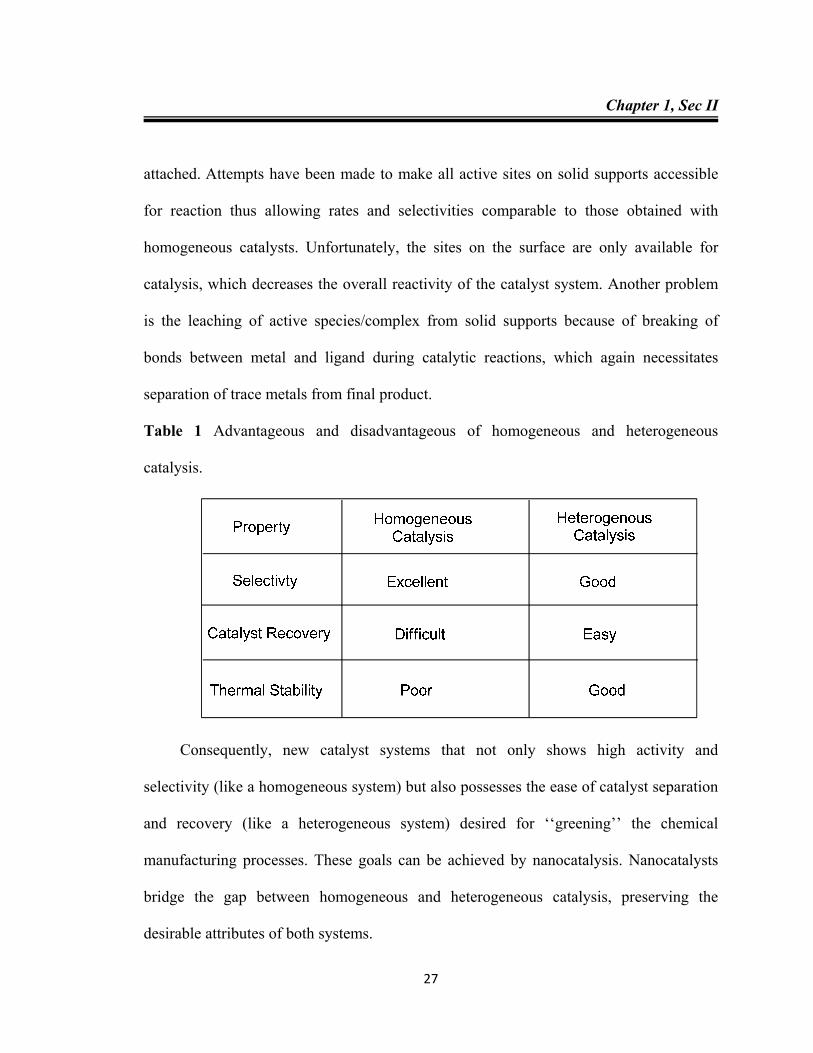
attached. Attempts have been made to make all active sites on solid supports accessible
for reaction thus allowing rates and selectivities comparable to those obtained with
homogeneous catalysts. Unfortunately, the sites on the surface are only available for
catalysis, which decreases the overall reactivity of the catalyst system. Another problem
is the leaching of active species/complex from solid supports because of breaking of
bonds between metal and ligand during catalytic reactions, which again necessitates
separation of trace metals from final product.
Table 1 Advantageous and disadvantageous of homogeneous and heterogeneous
catalysis.
Consequently, new catalyst systems that not only shows high activity and
selectivity (like a homogeneous system) but also possesses the ease of catalyst separation
and recovery (like a heterogeneous system) desired for ‘‘greening’’ the chemical
manufacturing processes. These goals can be achieved by nanocatalysis. Nanocatalysts
bridge the gap between homogeneous and heterogeneous catalysis, preserving the
desirable attributes of both systems.
Chapter 1, Sec II
28
1.2.4 NANOCATALYSIS
One of the most stimulating features of nanotechnology is its potential use in
almost any field. Nanotechnology refers to techniques that offer the ability to design,
synthesize (or manufacture) and control at the length scale ranging from 1 to 100 nm of
the material. The discovery of nanoparticles with varied size, shape and composition has
stretched the limits of technology in ways that scientists would never have dreamt of a
century ago. Nature makes and chemistry reshapes; huge varieties of nanoparticles have
emerged in our daily life, in every field from drugs and electronics to paints and beauty
care products. The evolution from vacuum tubes to diodes and transistors and miniature
chips resulted in smaller and smaller devices with more powerful computing ability. Now
these electric circuits are approaching nano-dimensions and when this realm is entered,
nanocomputers only visible through microscope will appear.7 Among the current
research, application of nanoparticles in catalysis has attracted a lot of attention, because
nanoparticles have a large surface-to-volume ratio relative to bulk materials, they by
offering an attractive alternative to conventional catalysts.8
Nanocatalysis involves a substance or material with catalytic properties that
possesses at least one nanoscale dimension, either externally or in terms of internal
structures. This field is undergoing an explosive development. Nanocatalysis can help
design catalysts with excellent activity, greater selectivity and high stability. These
characteristics can easily be achieved by tailoring the size, shape, morphology,
composition, electronic structure and thermal and chemical stability of the particular
nanomaterial. The nanocatalytic systems are active due to the following reasons:
Chapter 1, Sec II
29
As size decreases, the surface area to volume ratio increases. Therefore, nanocatalysts
are small in size and have an enormous surface area to volume ratio.
The available surface area of the active component of a nanocatalyst is large.
Therefore, it increases contact between the reactant molecules and the catalyst to a
great extent. This enhanced interaction facilitates the heterogeneous catalytic system
and helps to achieve a better reaction rate that is closer to its homogeneous
counterpart.
Easy control of nanocatalysts over size, shape and morphology makes it possible to
rationally design the materials that are specifically needed for a particular catalytic
application. Thus, tuning the properties of a material is easily possible when working
at the nanoscale, which would be difficult with their macroscopic counterparts.
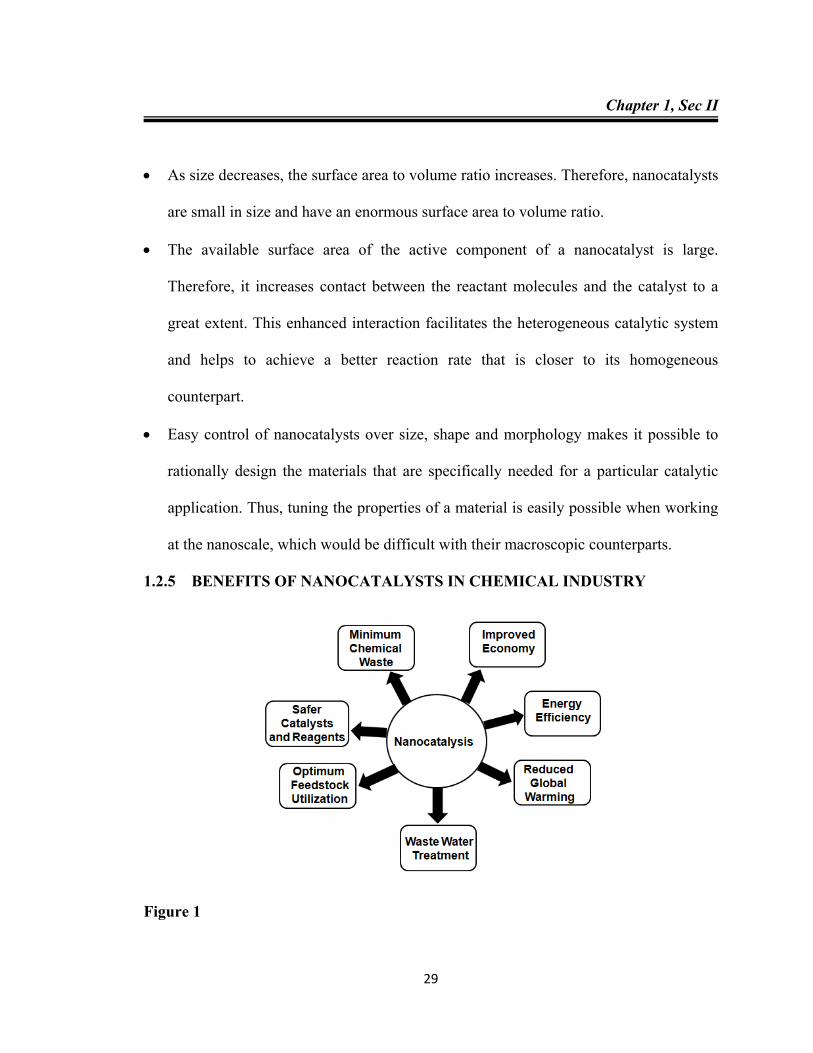
1.2.5 BENEFITS OF NANOCATALYSTS IN CHEMICAL INDUSTRY
Figure 1
Chapter 1, Sec II
30
Increased selectivity and activity of catalysts by controlling pore size and particle
characteristics.
Replacement of precious metal catalysts by catalysts tailored at the nanoscale and use
of base metals, thus improving chemical reactivity and reducing process costs.
Catalytic membranes by design that can remove unwanted molecules from gases or
liquids by controlling the pore size and membrane characteristics.
Thus, nanocatalysts enjoy several advantages over conventional catalyst systems;
however, isolation and recovery of these tiny nanocatalysts from the reaction mixture is
not easy. Conventional techniques (such as filtration) are not efficient because of the
nano size of the catalyst which can lead to the blocking of filters and valve by the
catalyst. This limitation hampers the economics and sustainability of these nanocatalytic
protocols. To overcome this limitation, the use of magnetic nanoparticles has emerged as
a viable solution; their insoluble and paramagnetic nature enables easy and efficient
separation of the catalysts from the reaction mixture with an external magnet.
1.2.6 MAGNETIC NANOPARTICLES (MNPs)
Magnetic nanoparticles are a class of nanostructured materials of current interest,
due largely to their advanced technological and medical applications, envisioned or
realized.6 Among the various magnetic nanoparticles under investigation, magnetic
ferrites nanoparticles are arguably the most extensively studied.9a,e,10 They have been
used in recent years as a versatile support for a variety of heterogeneous catalysts for
diverse classes of organic transformation,11 such as oxidation,11c hydrogenation,11d C-C
coupling,11e asymmetric aldol reaction11f and CO2 cycloaddition reaction11f. Magnetic
Chapter 1, Sec II
31
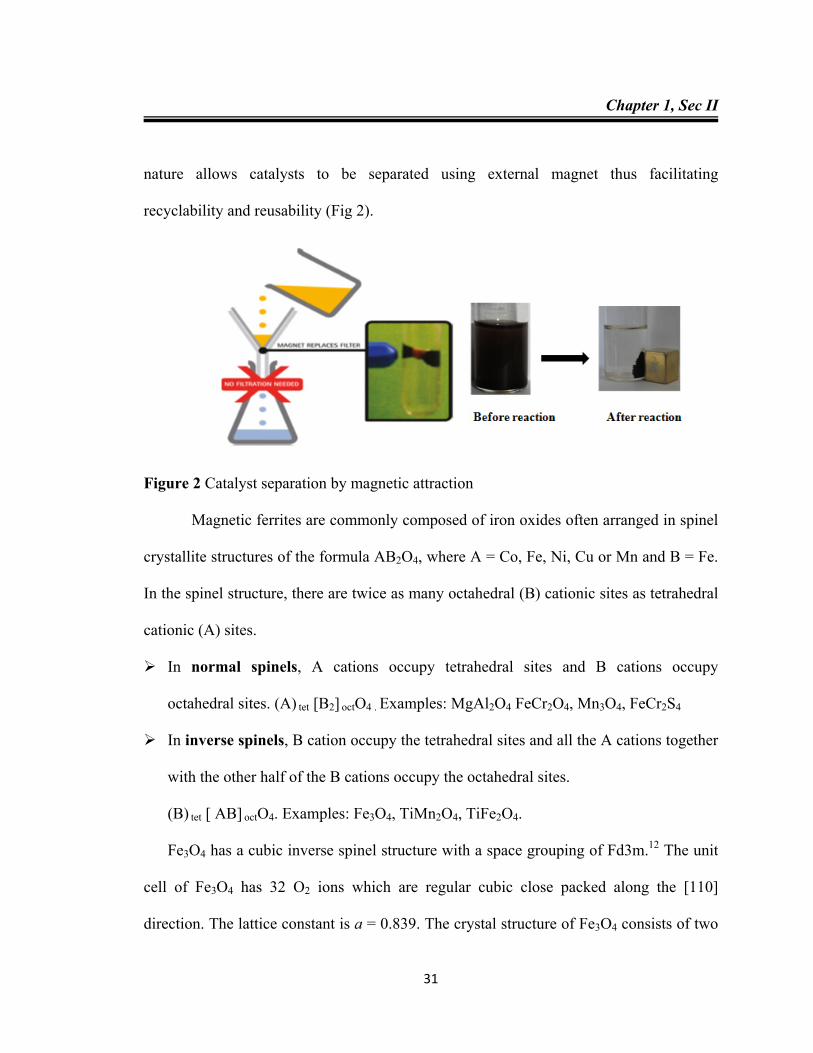
nature allows catalysts to be separated using external magnet thus facilitating
recyclability and reusability (Fig 2).
Figure 2 Catalyst separation by magnetic attraction
Magnetic ferrites are commonly composed of iron oxides often arranged in spinel
crystallite structures of the formula AB2O4, where A = Co, Fe, Ni, Cu or Mn and B = Fe.
In the spinel structure, there are twice as many octahedral (B) cationic sites as tetrahedral
cationic (A) sites.
In normal spinels, A cations occupy tetrahedral sites and B cations occupy
octahedral sites. (A) tet [B2] octO4 . Examples: MgAl2O4 FeCr2O4, Mn3O4, FeCr2S4
In inverse spinels, B cation occupy the tetrahedral sites and all the A cations together
with the other half of the B cations occupy the octahedral sites.
(B) tet [ AB] octO4. Examples: Fe3O4, TiMn2O4, TiFe2O4.
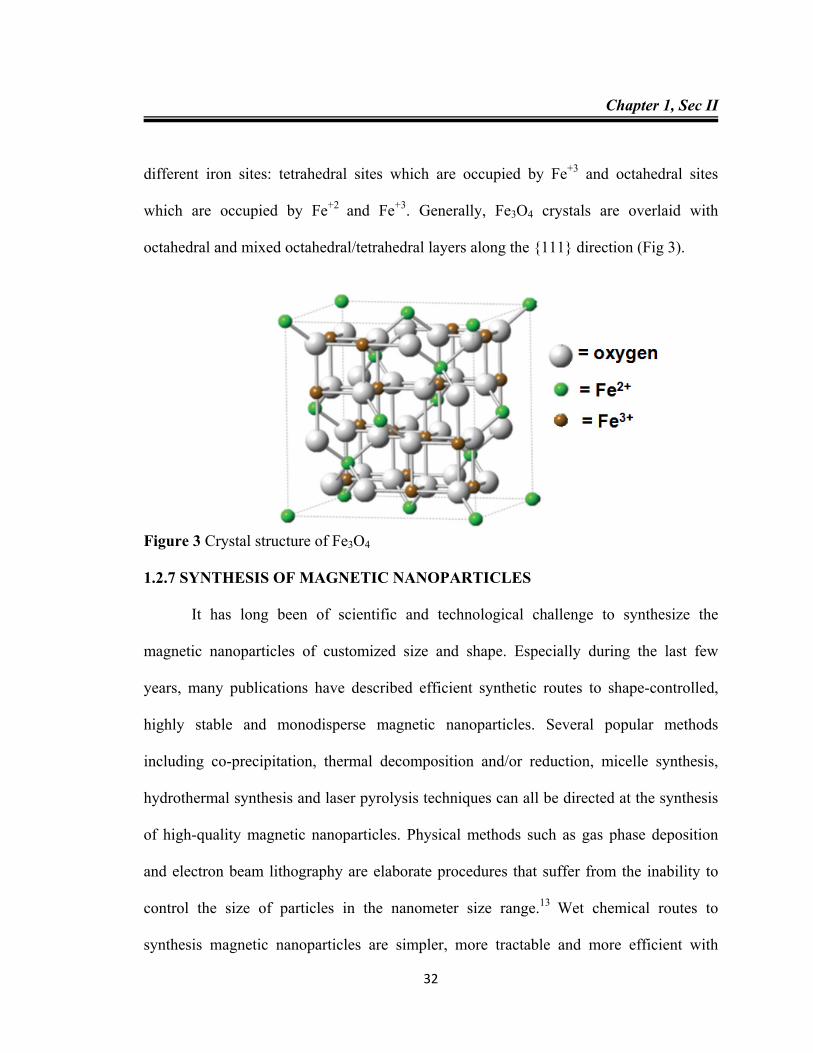
Fe3O4 has a cubic inverse spinel structure with a space grouping of Fd3m.12 The unit
cell of Fe3O4 has 32 O2 ions which are regular cubic close packed along the [110]
direction. The lattice constant is a = 0.839. The crystal structure of Fe3O4 consists of two
Chapter 1, Sec II
32
different iron sites: tetrahedral sites which are occupied by Fe+3 and octahedral sites
which are occupied by Fe+2 and Fe+3. Generally, Fe3O4 crystals are overlaid with
octahedral and mixed octahedral/tetrahedral layers along the {111} direction (Fig 3).
Figure 3 Crystal structure of Fe3O4
1.2.7 SYNTHESIS OF MAGNETIC NANOPARTICLES
It has long been of scientific and technological challenge to synthesize the
magnetic nanoparticles of customized size and shape. Especially during the last few
years, many publications have described efficient synthetic routes to shape-controlled,
highly stable and monodisperse magnetic nanoparticles. Several popular methods
including co-precipitation, thermal decomposition and/or reduction, micelle synthesis,
hydrothermal synthesis and laser pyrolysis techniques can all be directed at the synthesis
of high-quality magnetic nanoparticles. Physical methods such as gas phase deposition
and electron beam lithography are elaborate procedures that suffer from the inability to
control the size of particles in the nanometer size range.13 Wet chemical routes to
synthesis magnetic nanoparticles are simpler, more tractable and more efficient with
Chapter 1, Sec II
33
appreciable control over size, composition and sometimes even the shape of the
nanoparticles. 14
Co-precipitation is a facile and convenient way to synthesize magnetic ferrites
(MFe2O4) nanoparticles.15 In this method they are usually prepared in an aqueous
medium which chemical reaction of formation may be written as Eq. (1). The
nanoparticles are precipitated by the addition of base at a pH levels between 8 and 14,
with a stoichiometric ratio of 2:1 (Fe3+/M2+) in a non-oxidizing oxygen environment. The
size, shape and composition of the MNPs very much depends on the type of salts used
(e.g. chlorides, sulfates, nitrates), M2+/Fe3+ ratio, reaction temperature, pH value, type of
base, also mixing rate, ionic strength of the media, with the addition sequence and
bubbling of nitrogen gas are all important.
M2+ + 2Fe3+ + 8OH¯ → MFe2O4 + 4H2O Eq. 1
1.2.8 PROPERTIES OF MAGNETIC NANOPARTICLES
Ferromagnetic materials are subdivided into areas known as domains.16 In an
unmagnetized sample, the moments of these domains are randomly orientated, but tend to
align themselves in the direction of an external applied magnetic field. As the particle
size approaches a certain minimum critical size, often in the nanoscale range, the
formation of domain walls becomes energetically unfavorable. Changes in magnetization
occur through the rotation of spins rather than through the motion of domain walls.
Particles exhibiting these properties are called single domain. As particle size is
decreased further, spins are affected by thermal fluctuations and the particles become
superparamagnetic. This superparamagnetic property of materials is useful in that
Chapter 1, Sec II
34
individual particles become magnetized only when exposed to an external magnetic field.
Once the external magnetic field is removed, thermal fluctuations again randomize the
magnetic moments of the particles, again resulting in zero net magnetic moment.17
It is this phenomenon of reversible on/off magnetism that makes these
superparamagnetic nanoparticles interesting candidates for catalyst supports. Because
MNPs exhibit no net magnetic moment by themselves, they can be dispersed into
reaction media. Immobilized catalysts on the MNPs can promote reactions in solution
and upon completion, the MNPs and supported catalyst can be easily recovered with an
external magnet. In addition to the novel magnetic recovery method, MNPs also possess
other positive attributes. They exhibit high surface areas (above 200 m2/g) resulting from
the small particle diameters.18 As the diameter of any particle decreases, the surface area
per unit mass increases on the order of 1/D particle. Because MNPs possess only external
surface area, reactions are generally not diffusion limited, unlike porous catalyst supports
or in solid-phase synthesis resins which can suffer from internal diffusion limitations.19
The particles are also thermally and chemically stable under some conditions. In addition,
the particle size provides a large surface area for functionalization which makes them
suitable for catalyst immobilization and dispersible in organic or aqueous solution.
1.2.9 APPLICATIONS OF MAGNETIC NANOPARTICLES
Magnetic nanoparticles with good stability will be of great interest in catalysis
and in biotechnology/biomedicine applications. Such magnetic nanoparticles can be very
useful to assist an effective separation of catalysts, nuclear waste, biochemical products
and cells. 20
Chapter 1, Sec II
35
1.2.9.1 Applications in catalysis
Catalyst recovery and reuse are the two most important features for many
catalytic processes and most heterogeneous systems require a filtration or centrifugation
step and/or a tedious workup of the final reaction mixture to recover the catalyst.
Magnetic nanoparticles are considered as ideal supports for the heterogenization of
homogeneous catalysts since they efficiently disperse catalytic active sites in the reaction
medium. Furthermore, magnetic separation is a “green” process since it avoids the
complications of filtration (such as loss of catalyst, oxidation of sensitive metal
complexes and usage of additional solvents for precipitation steps). Thus, waste and costs
can be greatly reduced.
1.2.9.1.1 Magnetic nanoparticles stabilized with carboxylic- and phosphonic-acid
derivatives
Carboxylic acid sites are predominant among the most common capping agents
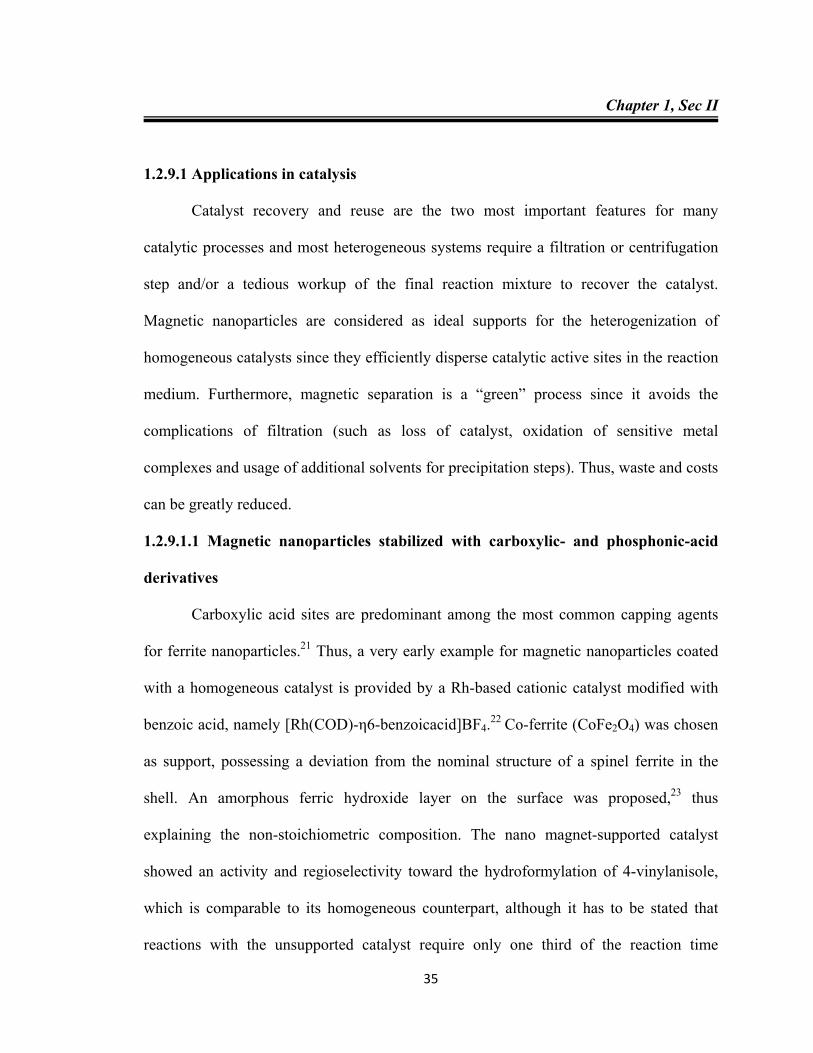
for ferrite nanoparticles.21 Thus, a very early example for magnetic nanoparticles coated
with a homogeneous catalyst is provided by a Rh-based cationic catalyst modified with
benzoic acid, namely [Rh(COD)-η6-benzoicacid]BF4.22 Co-ferrite (CoFe2O4) was chosen
as support, possessing a deviation from the nominal structure of a spinel ferrite in the
shell. An amorphous ferric hydroxide layer on the surface was proposed,23 thus
explaining the non-stoichiometric composition. The nano magnet-supported catalyst
showed an activity and regioselectivity toward the hydroformylation of 4-vinylanisole,
which is comparable to its homogeneous counterpart, although it has to be stated that
reactions with the unsupported catalyst require only one third of the reaction time
Chapter 1, Sec II
36
(Scheme 1). However, the activity is still extraordinarily high relative to catalysts
immobilized on conventional supports, e.g. polymers,24 and shows no loss in activity
upon recycling via magnetic decantation.
Scheme 1
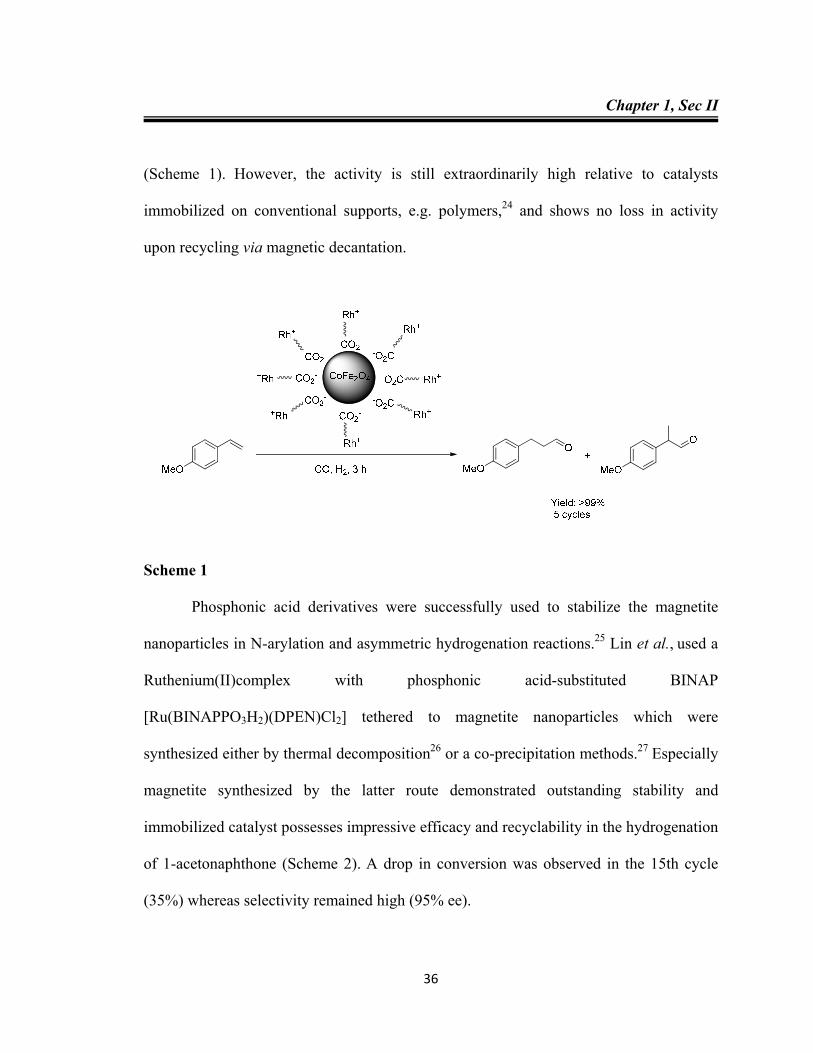
Phosphonic acid derivatives were successfully used to stabilize the magnetite
nanoparticles in N-arylation and asymmetric hydrogenation reactions.25 Lin et al., used a
Ruthenium(II)complex with phosphonic acid-substituted BINAP
[Ru(BINAPPO3H2)(DPEN)Cl2] tethered to magnetite nanoparticles which were
synthesized either by thermal decomposition26 or a co-precipitation methods.27 Especially
magnetite synthesized by the latter route demonstrated outstanding stability and
immobilized catalyst possesses impressive efficacy and recyclability in the hydrogenation
of 1-acetonaphthone (Scheme 2). A drop in conversion was observed in the 15th cycle
(35%) whereas selectivity remained high (95% ee).
Chapter 1, Sec II
37
Scheme 2
1.2.9.1.2 Dopamine stabilized ferrite nanoparticles
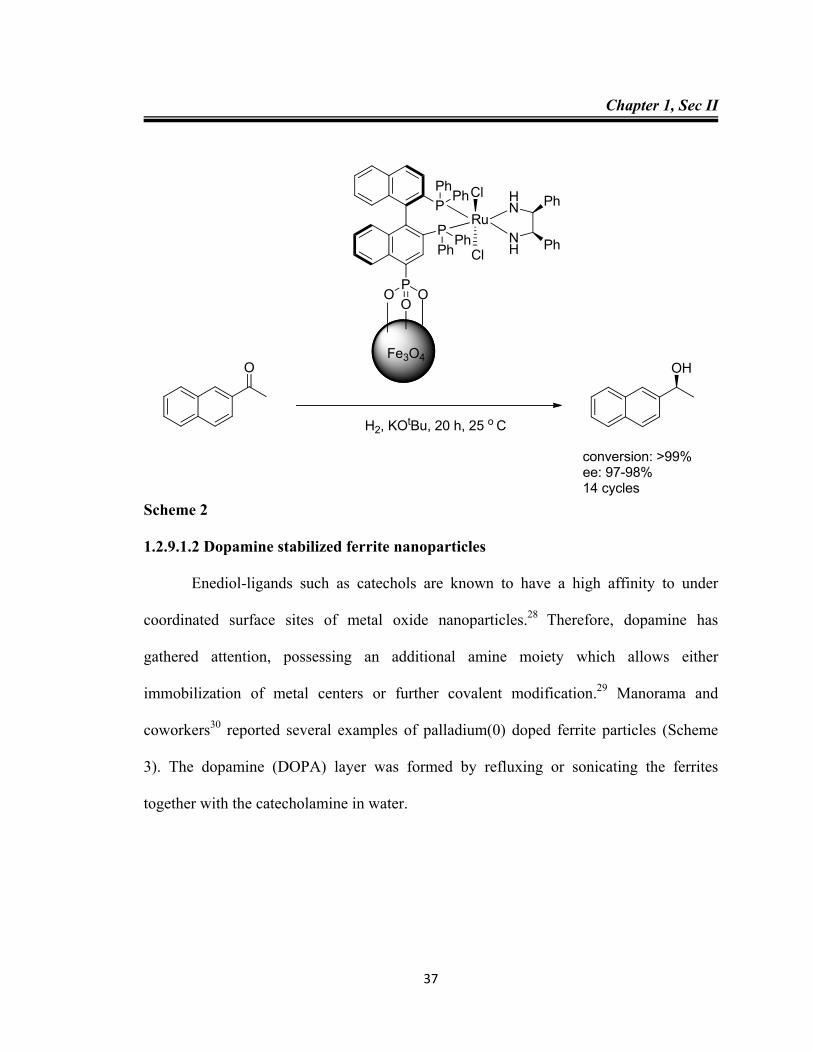
Enediol-ligands such as catechols are known to have a high affinity to under
coordinated surface sites of metal oxide nanoparticles.28 Therefore, dopamine has
gathered attention, possessing an additional amine moiety which allows either
immobilization of metal centers or further covalent modification.29 Manorama and
coworkers30 reported several examples of palladium(0) doped ferrite particles (Scheme
3). The dopamine (DOPA) layer was formed by refluxing or sonicating the ferrites
together with the catecholamine in water.
Fe3O4
PO
OO
PPh
Ph
PPh
PhRu
Cl HN
NHCl
Ph
Ph
O OH
H2, KOtBu, 20 h, 25 o C
conversion: >99%ee: 97-98%14 cycles
Chapter 1, Sec II
38
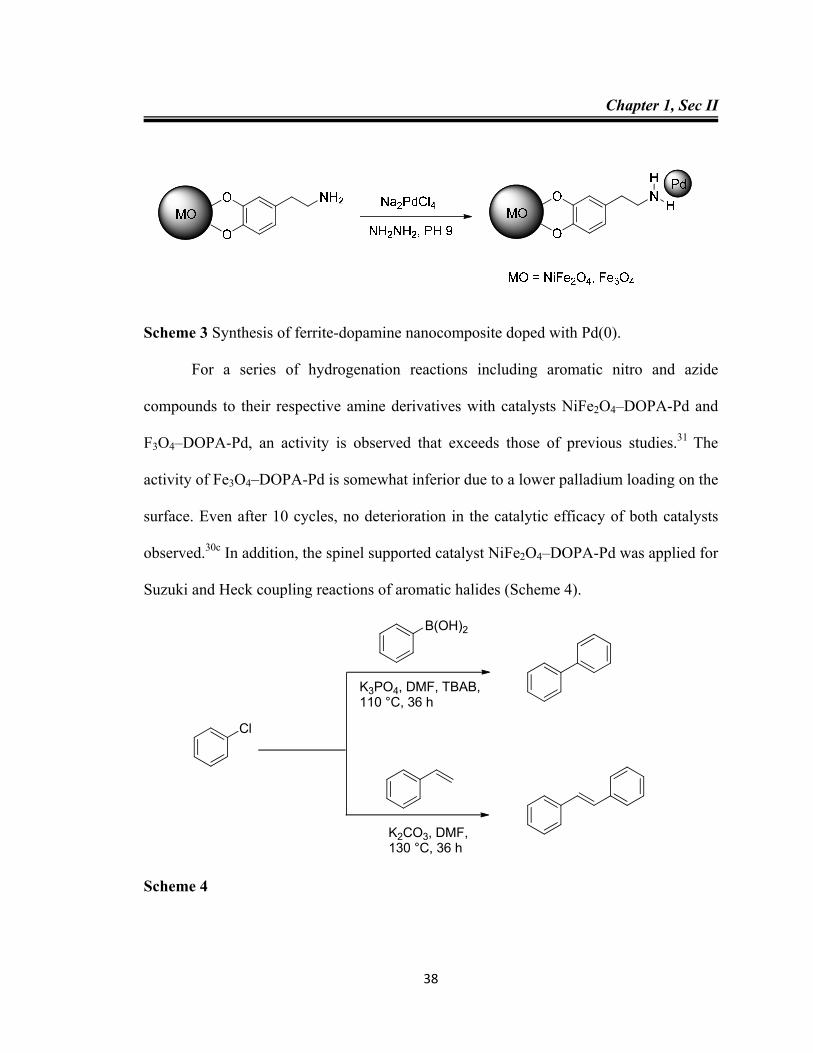
Scheme 3 Synthesis of ferrite-dopamine nanocomposite doped with Pd(0).
For a series of hydrogenation reactions including aromatic nitro and azide
compounds to their respective amine derivatives with catalysts NiFe2O4–DOPA-Pd and
F3O4–DOPA-Pd, an activity is observed that exceeds those of previous studies.31 The
activity of Fe3O4–DOPA-Pd is somewhat inferior due to a lower palladium loading on the
surface. Even after 10 cycles, no deterioration in the catalytic efficacy of both catalysts
observed.30c In addition, the spinel supported catalyst NiFe2O4–DOPA-Pd was applied for
Suzuki and Heck coupling reactions of aromatic halides (Scheme 4).
Cl
K3PO4, DMF, TBAB,110 °C, 36 h
B(OH)2
K2CO3, DMF,130 °C, 36 h
Scheme 4
Chapter 1, Sec II
39
1.2.9.1.3 Silica coated iron oxide nanoparticles
Apart from enediol-ligands, silanes are frequently used to coat ferrites.32 The
deposition and adhesion of silica can be achieved via hydrolysis of a sol-gel precursor to
give shells with a thickness between 2 and 100 nm and because of the strong affinity of
iron oxide surfaces toward silica, no primer is required. An advantage of the silica
coating is that this surface is terminated by silanol groups which can react with various
coupling agents to covalently attach linkers, ligands, metals or complexes.
Nanocomposites of this kind were extensively used for palladium catalyzed cross-
coupling reactions.
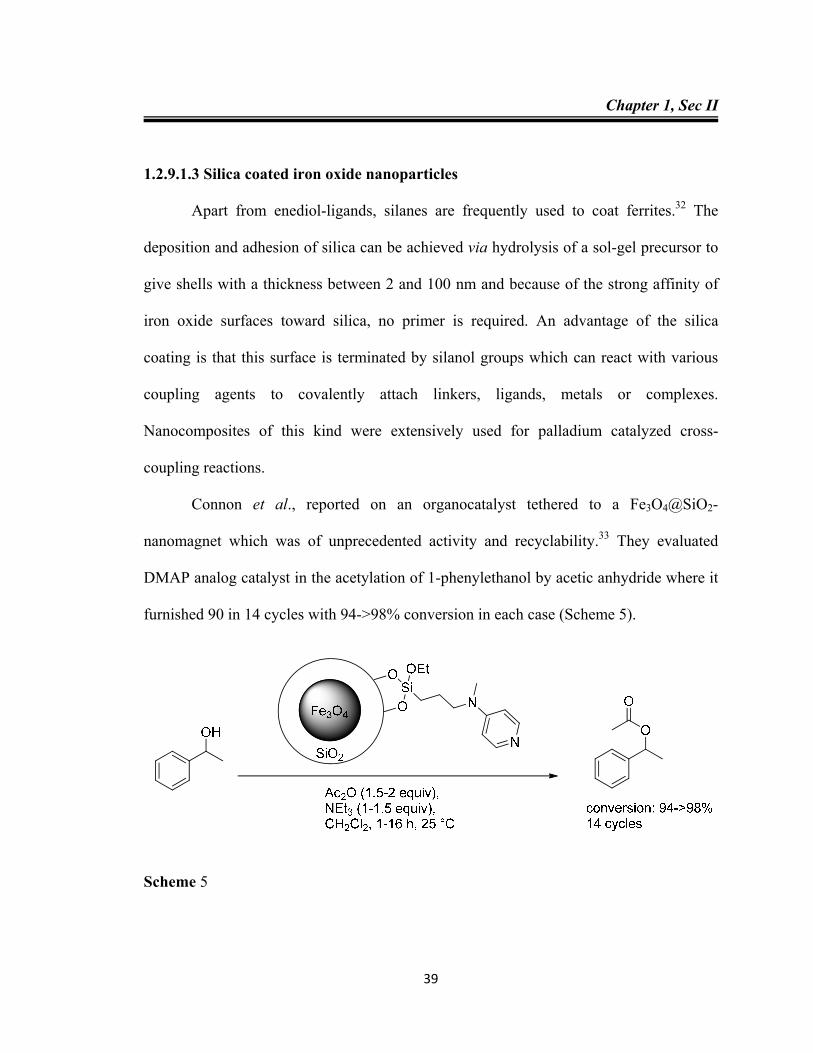
Connon et al., reported on an organocatalyst tethered to a Fe3O4@SiO2-
nanomagnet which was of unprecedented activity and recyclability.33 They evaluated
DMAP analog catalyst in the acetylation of 1-phenylethanol by acetic anhydride where it
furnished 90 in 14 cycles with 94->98% conversion in each case (Scheme 5).
Scheme 5
Chapter 1, Sec II
40
The recovered material was subsequently found to be even active when employed
at loadings as low as 0.2 mol% (79%). The reaction scope was examined by subjecting
recycled catalyst to promote a range of distinct transformations where it acted as a
nucleophilic catalyst. After 30 consecutive cycles, recycled catalyst (0.2 mol%) was still
able to achieve an identical level of conversion (80%) in the acetylation of 1-
phenylethanol.
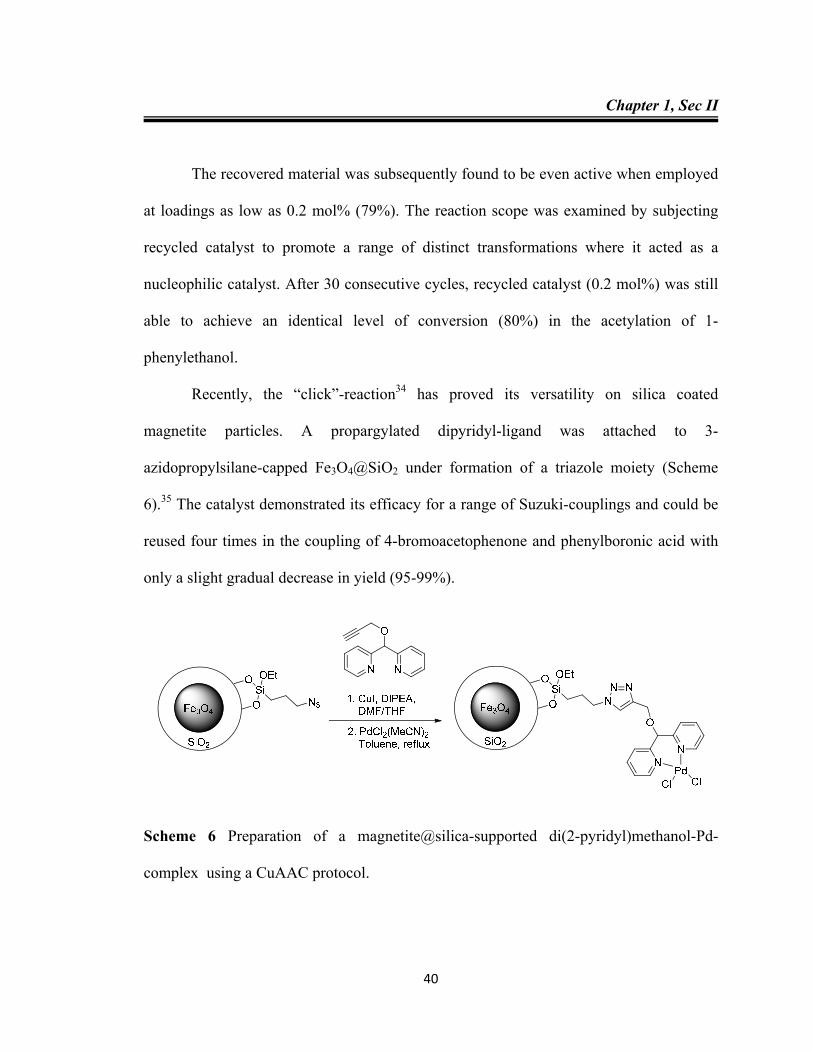
Recently, the “click”-reaction34 has proved its versatility on silica coated
magnetite particles. A propargylated dipyridyl-ligand was attached to 3-
azidopropylsilane-capped Fe3O4@SiO2 under formation of a triazole moiety (Scheme
6).35 The catalyst demonstrated its efficacy for a range of Suzuki-couplings and could be
reused four times in the coupling of 4-bromoacetophenone and phenylboronic acid with
only a slight gradual decrease in yield (95-99%).
Scheme 6 Preparation of a magnetite@silica-supported di(2-pyridyl)methanol-Pd-
complex using a CuAAC protocol.
Chapter 1, Sec II
41
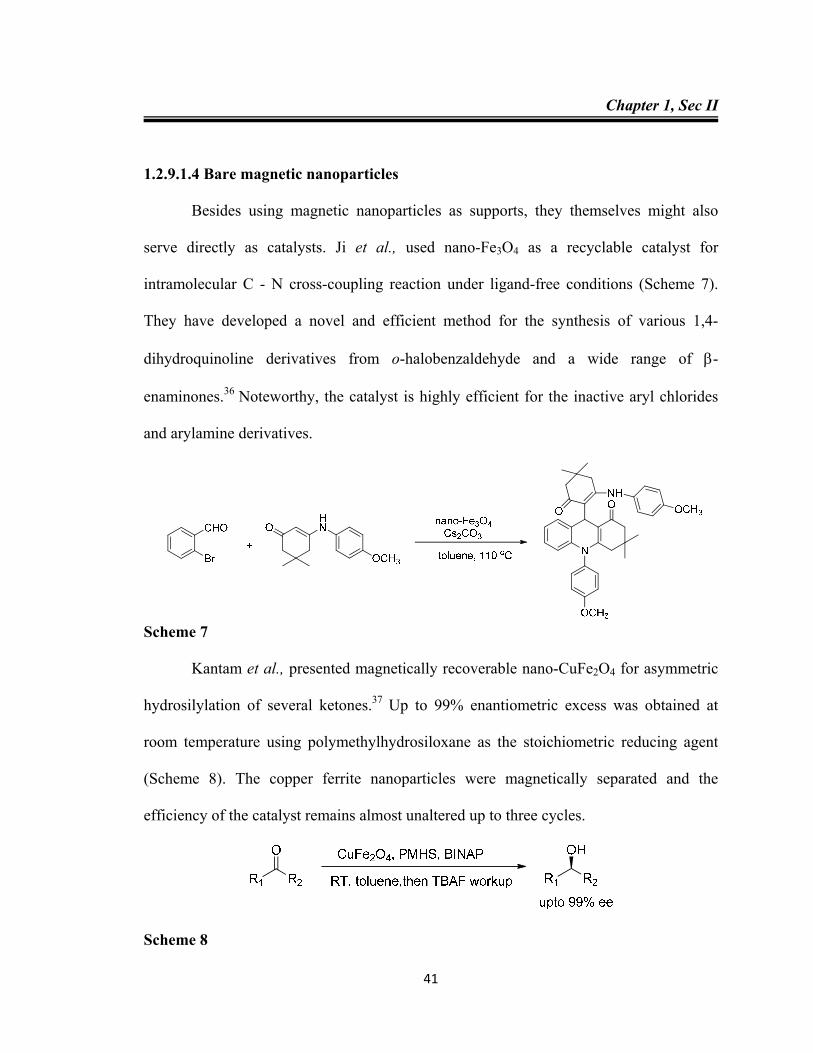
1.2.9.1.4 Bare magnetic nanoparticles
Besides using magnetic nanoparticles as supports, they themselves might also
serve directly as catalysts. Ji et al., used nano-Fe3O4 as a recyclable catalyst for
intramolecular C - N cross-coupling reaction under ligand-free conditions (Scheme 7).
They have developed a novel and efficient method for the synthesis of various 1,4-
dihydroquinoline derivatives from o-halobenzaldehyde and a wide range of -
enaminones.36 Noteworthy, the catalyst is highly efficient for the inactive aryl chlorides
and arylamine derivatives.
Scheme 7
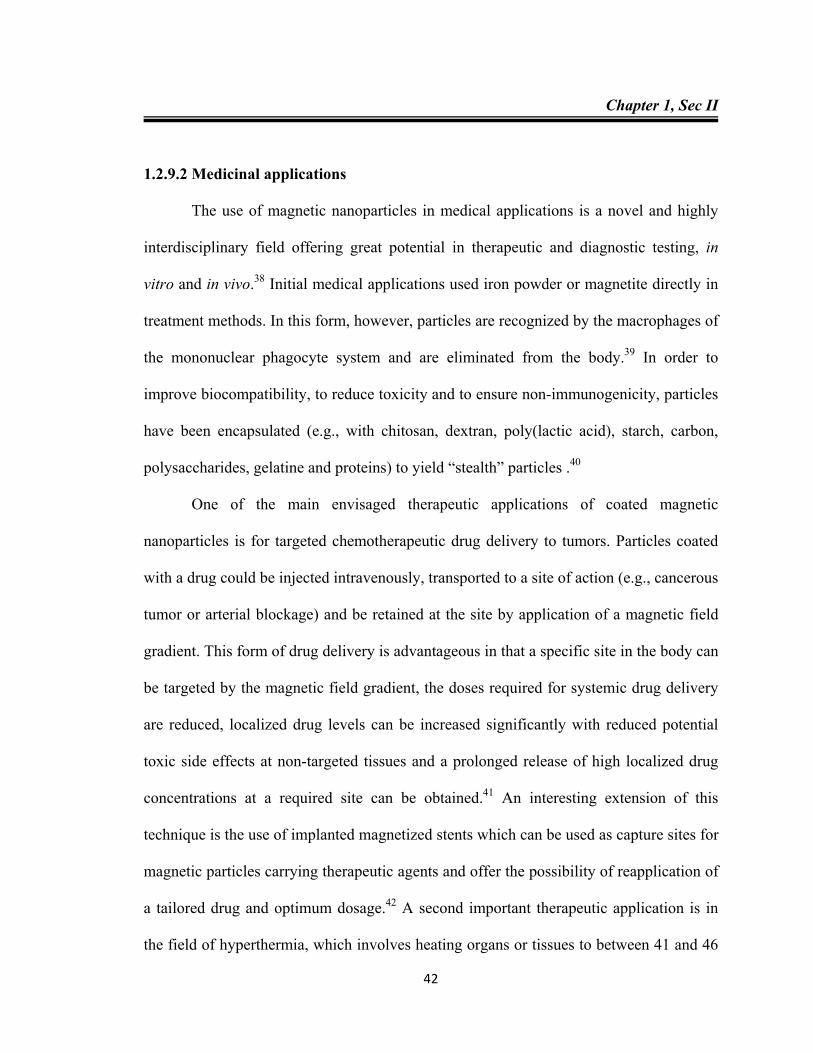
Kantam et al., presented magnetically recoverable nano-CuFe2O4 for asymmetric
hydrosilylation of several ketones.37 Up to 99% enantiometric excess was obtained at
room temperature using polymethylhydrosiloxane as the stoichiometric reducing agent
(Scheme 8). The copper ferrite nanoparticles were magnetically separated and the
efficiency of the catalyst remains almost unaltered up to three cycles.
Scheme 8
Chapter 1, Sec II
42
1.2.9.2 Medicinal applications
The use of magnetic nanoparticles in medical applications is a novel and highly
interdisciplinary field offering great potential in therapeutic and diagnostic testing, in
vitro and in vivo.38 Initial medical applications used iron powder or magnetite directly in
treatment methods. In this form, however, particles are recognized by the macrophages of
the mononuclear phagocyte system and are eliminated from the body.39 In order to
improve biocompatibility, to reduce toxicity and to ensure non-immunogenicity, particles
have been encapsulated (e.g., with chitosan, dextran, poly(lactic acid), starch, carbon,
polysaccharides, gelatine and proteins) to yield “stealth” particles .40
One of the main envisaged therapeutic applications of coated magnetic
nanoparticles is for targeted chemotherapeutic drug delivery to tumors. Particles coated
with a drug could be injected intravenously, transported to a site of action (e.g., cancerous
tumor or arterial blockage) and be retained at the site by application of a magnetic field
gradient. This form of drug delivery is advantageous in that a specific site in the body can
be targeted by the magnetic field gradient, the doses required for systemic drug delivery
are reduced, localized drug levels can be increased significantly with reduced potential
toxic side effects at non-targeted tissues and a prolonged release of high localized drug
concentrations at a required site can be obtained.41 An interesting extension of this
technique is the use of implanted magnetized stents which can be used as capture sites for
magnetic particles carrying therapeutic agents and offer the possibility of reapplication of
a tailored drug and optimum dosage.42 A second important therapeutic application is in
the field of hyperthermia, which involves heating organs or tissues to between 41 and 46
Chapter 1, Sec II
43
°C to obtain tumor cell necrosis.43 The application of an external alternating magnetic
field to nanosized magnetic particles causes heating via hysteresis energy losses .
Superparamagnetic particles are used as magnetic resonance imaging (MRI)
contrast agent in diagnostics applications. MRI may be used to enhance the image
contrast between normal and diseased tissue and/or indicate the status of organ functions
or blood flow. Small superparamagnetic iron oxides (SPIOs) have been developed for
imaging liver metastases and to distinguish loops of bowel from other abdominal
structures.
Medical applications require particles with high saturation magnetization,
exhibiting superparamagnetic behavior and small enough to interact in the region of
interest. Fundamental research must still be performed into areas such as the uniformity
of magnetic particles with an equal probability of magnetic capture and determination of
the fate of the particles in the body. Despite much fundamental research still to be
conducted, the potential for use of magnetic nanoparticles in a variety of biomedical
applications such as for cell separation, lab-on-a-chip applications and for the extraction,
purification and re-injection of patient stem cells after cancer treatment is significant.44
Chapter 1, Sec II
44
REFERENCES
1. G. C. Bond in: Heterogeneous Catalysis: Principles and Applications, Clarendon
Press, Oxford, 1987.
2. B. C. Gates in: Catalytic Chemistry, John Wiley & Sons Inc., New York, 1992.
3. R. A.V. Santen, P. W. N. M. V. Leeuwen, J. A. Moulijn, B. A. Averill, Catalysis: An
integrated approach, 2nd ed, Elsevier: Amsterdam, 1999.
4. a) D. J. C. Hamilton, Science, 2003, 299, 1702. b) R. T. Baker, W. Tumas, Science,
1999, 284, 1477.
5. a) C. Coperet, M. Chabanas, R. P. S. Arroman, J. M. Basset, Angew. Chem. Int. Ed.,
2003, 42, 156. b) J. M. Basset, A. Choplin, J. Mol. Catal., 1993, 21, 95. c) N.
Mizuno, M. Misono, Chem. Rev., 1998, 98, 199. d) F. Lefebvre, J. M. Basset, J. Mol.
Catal. A: Chem., 1999, 146, 3.
6. M. Benaglia, Recoverable and Recyclable Catalysts, John Wiley and Sons, Chichester
2009.
7. B. L. Cushing, V. L. Kolesnichenko, C. J. O. Connor, Chem. Rev., 2004, 104, 3893.
8. a) D. Astruc, Nanoparticles and Catalysis;, Ed.; Wiley-VCH: Weinheim, 2008. b) G.
A. Somorjai, H. Frei, J. Y. Park, J. Am. Chem. Soc., 2009, 131, 16589.
9. a) C. T. Yavuz, J. T. Mayo, W. W. Yu, A. Prakash, J. C. Falkner, S. Yean, L. L. Cong,
H. J. Shipley, A. Kan, M. Tomson, D. Natelson, V. L. Colvin, Science, 2006, 314,
964. b) S. H. Sun, C. B. Murray, D. Weller, L. Folks, A. Moser, Science, 2000, 287,
1989. c) J. Gao, W. Zhang, P. Huang, B. Zhang, X. Zhang, B. Xu, J. Am. Chem. Soc.,
2008, 130, 3710. d) J. Lu, S. H. Yang, K. M. Ng, C. H. Su, C. S. Yeh, Y. N.Wu, D. B.
Chapter 1, Sec II
45
Shieh, Nanotechnology, 2006, 17, 5812. e) Z. Li, L. Wei, M. Gao, H. Lei, Adv.
Mater., 2005, 17, 1001. f) M. K. Yu, Y. Y. Jeong, J. Park, S. Park, J. W. Kim, J. J.
Min, K. Kim, S. Jon, Angew. Chem., Int. Ed., 2008, 47, 5362.
10. a) A. G. Roca, M. P. Morales, K. O’Grady, C. J. Serna, Nanotechnology, 2006, 17,
783. b) Y. H. Zheng, Y. Cheng, F. Bao, Y. S. Wang, Mater. Res. Bull., 2006, 41, 525.
c) C. Lang, D. Schueler, D. Faivre, Macromol. Biosci., 2007, 7, 144. d) P. Majewski,
B.Thierry, Crit. Rev. Solid State Mater. Sci., 2007, 32, 203.
11. a) S. Roy, M. A. Pericas, Org. Biomol. Chem., 2009, 7, 2669. b) R. B. N. Baig, R. S.
Varma, Chem. Commun., 2013, 49, 752. c) V. Polshettiwar, R. S. Varma, Org.
Biomol. Chem., 2009, 7, 37. d) V. Polshettiwar, B. Baruwati, R. S. Varma, Green
Chem., 2009, 11, 127. e) B. Baruwati, D. Guin, S. V. Manorama, Org. Lett., 2007, 9,
5377. f) S. Luo, X. Zhenga, J. P. Cheng, Chem. Commun., 2008, 5719. g) X. Zheng,
S. Luo, L. Zhang, J –P. Cheng, Green Chem., 2009, 11, 455.
12. U. Schwertmann, R. M. Cornell, The Iron Oxides: Structure, Properties, Reactions,
Occurrences and Uses, 2nd edn, WILEY-VCH, Weinheim, 2003. b) U.
Schwertmann, R. M. Cornell, Iron Oxides in the Laboratory, Wiley-VCH, Wienheim,
2000.
13. a) S. Stolnik, L. Illum, S. S. Davis, Adv. Drug Delivery Rev. 1995, 16,195. b) T. T.
Kodas, M. H. Smith, Aerosol processing of materials New York: Wiley-VCH; 1999.
c) C. S Lee, H. Lee, R. M. Westervelt, Appl. Phys. Lett., 2001, 79, 3308. d) A.
Rishton, Y. Lu, R. A Altman, A. C Marley, C. Bian Hahnes, R. Viswanathan, G.
Xiao, W. J. Gallagher, S. S. P Parkin, Microelectron. Eng., 1997, 35, 249.
Chapter 1, Sec II
46
14. a) A. K. Gupta, S. Wells, IEEE Trans. Nanobiosci., 2004, 3, 66. b) A. K. Gupta, A. S.
G. Curtis, Biomaterials, 2004, 25, 3029.
15. a) V. Polshettiwar, B. Baruwati, R. S. Varma, Green Chem., 2009, 11, 127. b) I.
Nedkov, R. E. Vandenberghe, T. Marinova, P.Thailhades, T. Merodiiska, I.
Avramova, Appl. Surf. Sci., 2006, 253, 2589. c) J. E. Tasca, A. Ponzinibbio, G. Diaz,
R. D. Bravo, A. Lavat, M. G. Gonzalez, Top. Catal., 2010, 53, 1087.
16. J. P. Jakubovics, Magnetism and Magnetic Materials, Cambridge University Press,
Cambridge, 1994.
17. A. H. Latham, M. E. Williams, Acc. Chem. Res., 2008, 41, 411.
18. J. Fan, Y. Gao, J. Exp. Nanosci., 2006, 1, 457.
19. A.R. Vaino, K.D. Janda, J. Comb. Chem., 2000, 2, 579.
20. S. Giri, B. G. Trewyn, M. P. Stellmaker, V. S.-Y. Lin, Angew. Chem. Int. Ed., 2005,
117, 5166; Angew. Chem. Int. Ed., 2005, 44, 5038.b) C. Bergemann, D. Muller-
Schulte, J. Oster, L. Brassard, A. S. Lubbe, J. Magn. Magn. Mater., 1999, 194, 45. c)
L. Nunez, M. D. Kaminski, J. Magn. Magn. Mater., 1999, 194, 102.
21. J. Jin, T. Iyoda, C. Cao, Y. Song, L. Jiang, T. J. Li, D. B. Zhu, Angew. Chem. Int. Ed.,
2001, 40, 2135.
22. T. J. Yoon, W. Lee, Y. S. Oh, J. K. Lee, New. J. Chem., 2003, 27, 227.
23. M. H. Sousa, F. A. Tourinho, J. Depeyrot, G. J. da Silva, M. S. F. L. Lara, J. Phys.
Chem. B, 2001, 105, 1168.
24. a) S. C. Bourque, F. Maltais, W. J. Xiao, O. Tardif, H. Alper, P. Arya, L. E. Manzer,
J. Am. Chem. Soc., 1999, 121, 3035. b) S. C. Bourque, H. Alper, J. Am. Chem. Soc.,
Chapter 1, Sec II
47
2000, 122, 956. c) J. K. Lee, T. J. Yoon,Y. K. Chung, Chem. Commun., 2001, 1164.
c) T. Malmström, H. Weigl, C. Andersson, Organometallics, 1995, 14, 2593. d) K.
Nozaki, Y. Itoi, F. Shibahara, E. Shirakawa, T. Ohta, H. Takaya, T. Hiyama, J. Am.
Chem. Soc., 1998, 120, 4051.
25. a) A. Hu, G. T. Yee, W. Lin, J. Am. Chem. Soc., 2005, 127, 12486. b) G. Chouhan, D.
Wang, H. Alper, Chem. Commun., 2007, 4809.
26. S. Sun, H. Zeng, J. Am. Chem. Soc., 2002, 124, 8204.
27. Y. Sahoo, H. Pizem, T. Fried, D. Golodnitsky, L. Burstein, C. N. Sukenik, G.
Markovich, Langmuir, 2001, 17, 7907.
28. T. Rajh, L. X. Chen, K. Lukas, T. Liu, M. C. Thurnauer, D. M. Tiede, J. Phys. Chem.
B., 2002, 106, 10543.
29. C. Xu, K. Xu, H. Gu, R. Zheng, H. Liu, X. Zhang, Z. Guo, B. Xu, J. Am. Chem. Soc.,
2004, 126, 9938.
30. a) B. Baruwati, K. M. Reddy, S. V. Manorama, R. K. Singh, O. Parkash. Appl. Phys.
Lett., 2004, 85, 2833. b) D. Guin, B. Baruwati, S. V. Manorama, J. Mol. Catal. A,
Chem., 2005, 242, 26. c) D. Guin, B. Baruwati, S. V. Manorama, Org. Lett., 2007, 9,
1419. d) B. Baruwati, D. Guin. S. V. Manorama, Org. Lett., 2007, 9, 1419.
31. R. Raja, B. V. Glovko, M. J. Thomas, A. B. Murcia, W. Zhou, S. Xie, G. F. B.
Johnson, Chem. Commun., 2005, 2026.
32. a) Y. Yu, Y. Yin, B. T. Mayers, Y. Xia, Nano Lett., 2002, 2, 183. b) N. Kohler, G. E.
Fryxell, M. Zhang, J. Am. Chem. Soc., 2004, 126, 7206.
Chapter 1, Sec II
48
33. C. A. Dalaigh, S. A. Corr, Y. Gunko S. J. Connon, Angew. Chem. Int. Ed., 2007, 119,
4407.
34. a) C. W. Tornøe, M. Meldal, In American Peptide Symposium; M. Lebl, R. A.
Houghten, Eds, American Peptide Society and Kluwer Academic Publishers: San
Diego, CA, 2001, 263. b) V. V. Rostovtsev, L. G. Green, V. V. Fokin, K. B.
Sharpless, Angew. Chem. Int. Ed., 2002, 41, 2596. c) C. W. Tornøe, C. Christensen,
M. Meldal, J. Org. Chem., 2002, 67, 3057.
35. G. Lu, W. Mai, R. Jin, L. Gao, Synlett, 2008, 9, 1418.
36. X. J. Wu, R. Jiang, Bi. Wu, X. M. Su, X. P. Xu, S. J. Jia, Adv. Synth. Catal., 2009,
351, 3150.
37. M. L. Kantam, J. Yadav, S. Laha, P. Srinivas, B. Sreedhar, F. Figueras, J. Org.
Chem., 2009, 74, 4608.
38. P. Tartaj, In Encyclopedia of Nanoscience and Nanotechnology, Vol. 1, H. S. Nalwa
(Ed.), p. 177, American Scientific Publishers, Stevenson Ranch, CA, 2004.
39. U. O. Häfeli, Int. J. Pharm., 2004, 277, 19.
40. D. Portet, B. Denizot, E. Rump, J. J. Lejeune, P. Jallet. J. Colloid Interface Sci., 2001,
238, 37.
41. C. H. Ahn, J. W. Choi, H. J. Cho. In Encyclopedia of Nanoscience and
Nanotechnology, Vol. 6, H. S. Nalwa (Ed.), p. 815, American Scientific Publishers,
Stevenson Ranch, CA, 2004.
42. a) A. J. Rosengart, M. D. Kaminksi, H. Chen, P. L. Caviness, A. D. Ebner, J. A.
Ritter, J. Magn. Magn. Mater., 2005, 293, 633. b) B. B. Yellen, Z. G. Forbes, D. S.





























