Embed Size (px)
Citation preview

CHAPTER 8
REVISION OF THE, FAILED IMPIANT ARTFIROPTASTY
Jobn V. Vanore. DPM
First metatarsophalangeal (MTP) joint implantarthroplasty has been practiced by foot surgeons fornow ilrore than 30 years."' Implants ancl surgicaltechniques have evolved but as with any surgicalprocedure complications may occlir. Implantarlhroplasty involr,es the implantation of non-biologic materials into human hosts r'vith theexpectation of mechanical joint propefiies r;r.'ith aminimum of wear. This ideal situation certainly canbe expected to have difficulties and at times failureof the procedure may occllr.
The orthopedic and podiatric literature is
replete u,ith case reports of first MTP joint implantcomplicatiolls.lr'1;21 As in any problematic sttr54ery,
the surgeon should give consrderabie thought as tou.hy the original arthroplasty failed, n'hat is the pre-sent problem both from the patient's point of viewand his o\l'n perception and n'hat is most likely toprovide the patient with a painfree and clurablerevision. Revision ancl surgeon's choices of repairr,r.ill certainly vary both u.ith his experience andwillingness of the patient to cornply with surgicalprocedures and postoperative rnolbidity ancl
disability. There is a wide range of surgical alterna-tives from simple implant removal, re-implantation,revisionary ar-throclesis rvith bone grafting, bonegraft substitlltes. bone plates, ancl external fixationthat may be considered. Occasionally, amputationmay be the most expeclitious treatment alternatirre.\When performing revisionaty liurgeryl there is an
increased likelihood of subsequent comphcations.For this reason) surgeons may perform "simple"procedures or the patient may not want to undergctmore a:lgressive or risky proceclures. Each actionhas its own group of compliczrtions and these mustbe considered by both surgeon and patient duringdiscussions of the problematic implant.
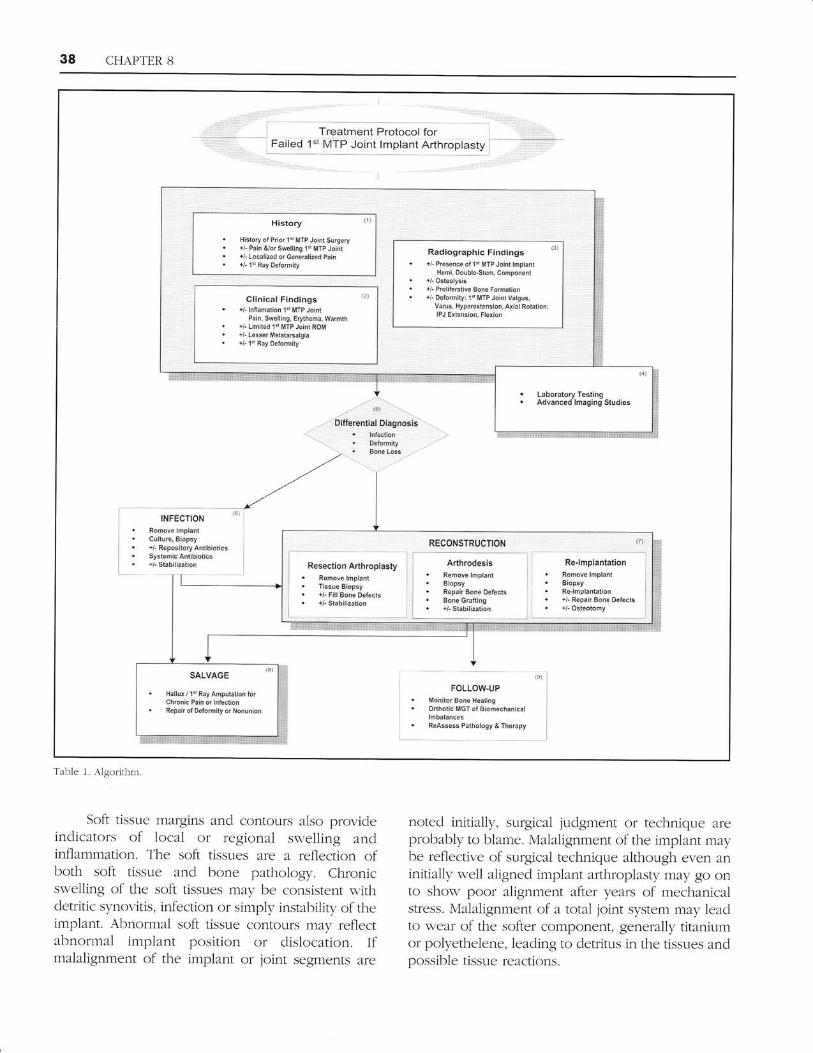
TREATMENT PROTOCOL FOR THEFAILED FIRST MTP JOINT IMPI-{NT
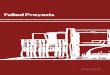
As with any clinical problem, evaluation and assess-
ment of the pathology mllst precede treatment(Figure 1). A comprehensive history ancl physicaleramination is the initial cor-rrse of the treating
physician. The history (Node 1) shouid includedocumentation of the prior surgical interventionsinch-rding dates of occurrence and postoperativecolrrse. The patient may have had an uneventfulpostoperative course and not suffered any r,tntoward
effects until years later. Syrnptoms may be quitestriking or milcl and limited. The patient may presentr,vith or without complaints of pain ancl swelling inand around the first MTP joint. The patient maycomplain of generalized fr;refbot pain or a ftinctionalinabiliry, such as inability to wear regular shoes
comfortably. The patient may no longer be able tcr
perform the same work cluties as prior to surgery.
Many implant procedures were performed fordeformities including hallux valgus and recumence ofdeformity certainly may be a presentinll concern onthe part of the patlent.
Physical examination of the patient (Noc1e 2)
includes identification of the pathology as well as
the normal findings. Patients may present withchronic joint srvelling, tenderness, pain on range ofmotion, Iimitation of ioint motion, defbrmity of thefirst ray or remainder of the foot, subcutaneousbony prominences, soft tissue masses) or lesser
metatarsalgia. Patients may also present rvithsymptoilrs that are totaily unrelated to the priorimplzrnt arthroplasty yet at titnes the subsequenttreating physician may initiate patient clissatisfaction
with discussion of the appropriateness or quality ofthe implant arlhroplasty.
As with most musculoskeletal problems, theinitial evaluration of the patient generally includesradiographic examination (Node 3). Radiographsdocument the type of arthroplasty and generallythe type of implant utilizecl, the resulting deformityancl any concomitant bone or soft tissLle reactions.Obviously, radiographs must be correctly inter-preted and the observed images evaluated by thosef-amiliar with the pathology of implant arthroplasty.
Radiolucency is generally indicative of looseningbe it a mechanical phenomenon or osteolysissecondary to implant debris or infection. Osteolysis
can be a very troublesome problem leading to chronicpain and instability of the implant within bonyconf-ines. Cystic erosions have occurred and may be
the r-esu1t of bone resotption to parlicular debris.
38 CHAPTER 8
Radlographic Findings (3)
. ,, aresoe ol td $tT? Jaint tnp,*tHei, Dqble.St6, Cospo.er{
. +/" Ost€olysis
. a/- Pslif.€tive 3one Fomaiio&
. +l Oeteity: ld irTF Jolnt Vrigrs,Varus, llyretertsnsigc, Axial Rot tionlIPJ Ext&sion, F'sxis
Ctinical Flndings{l- latlabetion 1s [iTP Joint
Pain, Sweltirg, lrrthena, ltsrrl*hil" Limikd 1d lt{TP Joint no!,+l Lser lueata6dgia{- 1s Ray oelomi{r
. LabqatoryT€cling" Advanced lmging Stldies
Resection A(,:roplasty. Aerck lmplant. Tl$ug 3iopsy. +FillB6!aD€fe*. il. Stabilizrlion
Re'tmplantatio*. ReGove lsplanl. Biopsy. Re.tmplanlali.r. +l- Repai. gee tetsc{sr *l-Clsteotoey
lNFgcT,olt
FOLLOW.UPMonito. B@e HetirgOdhoti. lrcl ot Bioa6.harica,letalane.ReAssess Pat*ology & Tho.aly
SALVASE
Hallrx , 1"' Ray Anpllation b.Ctlronic Pain gr hteclionieparr ot tefomity oi No.sio!
Table 1. Algorithm.
Soft tissue margins and contours also provideindicators of local or regional swelling andinflammation. The soft tissues are a reflection ofboth soft tissue and bone pathology. Chronicswelling of the soft tissues may be consistent withdetritic synovitis, infection or simply instability of theimplant. Abnormal soft tissue contours may reflectabnormal implant position or dislocation. Ifmalalignment of the implant or joint segments are
noted initially, surgical judgment or technique areprobably to blame. Malalignment of the implant maybe reflective of surgical technique although even aninitially well aligned implant afihroplasty may go onto show poor alignment after years of mechanicalstress. Malalignment of a total joint system may leadto wear of the softer component, generally titaniumor polyethelene, leading to detritus in the tissues andpossible tissue reactions.

CFL{PTER 8 39
Nerv bone fbrmation at either sicle of theresected bone surfzrces may occurl ectopic boneformation. Excessive bony proliferation is associatedclinically with limitation of motion. Prior to threemonths postoperatively, an aseptic periostealreaction may be noted predominantly along themetatarsal likely associated with periosteal boneformation as a result of the surgical dissection. Ofcollrse, in each case, infection must be exch,rded.
Nlost complications are chronic in natr'tre
although occasionzrlly acute symptoms may beseen. Findings must be correlated and additionallaborzrlory testing or advanced imaging stucliesperformed. Basic testing may reveal lymphocytosis,or elevated seclimentation rates inclicate infectionor osteomyelitis. The patient may have a history ofa draining wound, may be multiple wound culturesand treated with antibiotics. A11 information maybe relevant and may indicate areas of furtherinvestigation. Aclvanced imaging stticlies such as
bone scans and MR imaging may further elucidatepathology. The serotech bone scan utilizes(99m)Tc-1abe1ed leukocltes and is the raclionuclideprocedure of choice for detecting most infections.
DIFFERENTIAL DIAGNOSIS
Pathology of the implant arthroplasty has beendetailed with a variety of complications includinginfection, cleformity, soft tissue ancl bone reactions,
and biomechanical pathology (Node 5). The workupof the patient should allow- the cletermination of thepathology at hand. The treatment plan is formr-rlatecl
w'ith appropliate discttssion and informed consentof the patient. Implant revision may be necessary orsimple obseruation ancl perioclic evaluationperformed until symptoms flare or the patientw-illing to proceeci n'ith further treatment.
REVISION OF THE FAII.E,DINTERPO SITIONAL IMPLANT
Revision of an interpositional implant may vary fromthe sirnple to the complex and this is an importantdeterminant of patient morbidity ancl sllccess.
Implant revision may be necessary due to chronicpain, recurrent deformity, or various soft tissue orbony reactions, such as, detritic synovitis or osteoiy-sis. The patient may experience chronic joint painand swelling, deformity or lateral metatarsalgia.'6'2i
The diagnosis of infectron, be it acute or
chronic osteomyelitis or a foreign-body ceneteredinfection, is the most immecliate factor thatinfluences treatment decisions. Infection of an
implant arthroplasty may be very subtle and not at
al1 the typical red, hot swollen joint that might beexpected. A chronic draining wound may aidcliagnosis but usr-rally not present. The patient mayhave had prior intermittent therapeutic courses ofantibiotics with recurrent minor er),thema or limitedperiafticr-rlar swel1ing. If the diagnostic work-upindicates a deep infection, the site requires cultureand biopsy (Node 6). Generally, this is done as asr.rrgical incision and clrainage and sequestrectomy.
The implant is best removed parlicularly in thepresence of loosening and purulence. The treatmentof a foreign-bocly centered inf-ection requires theremoval of the implant. Culture should includeaerobic, anaerobic and fungus wound cultures.
Tissne biopsy aicls diagnosis particularly bone inosteomyelitis.
-Wounds may be m'.rnaged open for a period oftime or the wound may be closed over repositoryantibiotic beads, be it polymethylmethacrylate orcalcium sulfate. Systemic antibiotics are administeredper usual standards and consultation with infectiousdisease may be considered. In the presence ofsignificant bone resection and osseous instzrbility,
stabilizzrtion of the first ray with an external fixatormay also be considered. Alternatives for reconstlalc-
tion will be much like any other revisionaryarlhroplasty (Node 7). Irr the presence of chronicosteomyelitis or a flail toe, the patient's mostexpedient treatment may be that of amputation(Node B)
Most implant problems are not infectious innature but a combination of deformity with soft tis-st-re or osseous reactions seconclary to the implant.Surgical reconstruction (Node 7) may consist ofconversion of the implant arthroplasty to a 1)
resection arthroplasty, 2) arthrodesis, or 3) insertionof another implant. Bone loss and deformity are
amon5a the most important determinates ofsurgical decisions. Racliographically, the quality ofthe remaining bone, presence of osteolysis, orcystic erosions may influence the revising surgeonschoice of procedure. In all cases, the implantgenerally requires removal. Tissues should bebiopsied and cultures considered. The reconstrLlc-
tion must be tailored not only to the clinicalfindings but the patient must be willing to complywith the postoperative regime required for the
40 CHAPTER 3
proposed proceclllre. The situation may arise whenan amplrtation is selected. The patient may be quitee1der1y, sedentary or simply not willing to complywith the prospect of maybe multiple adclitionalprocedures and amputzrtion may be considered.
Reconstruction with resection arthroplastywould involve removal of the impl:rnt, filling of anybone defects and osseolls stabilization. Stabilizationfor a period postoperatively helps to maintainhallucal position and may be accomplished by a
variety of techniqr-res from simply intramedullaryKirschnel wire to use of external fixatron.
Reconstruction s,.ith revisionary arthroclesis isprobably the most viable altelnative fbr patientswith a failecl first MTP joint implant arthroplasry.Arthrodesis allows for a durable reconstruction br,rthas deflnite requirements of bone grafting,stabilization and long-term disability to allow non-weightbearing and successful bone union. Thepostoperative collrse may be quite extended withthe use of bone grafts, various forms of fixation andthe potential for subsequent complications.
Reconstrlrction with replacement of a newimplant may be relatively straight fonr,,arcl or quite
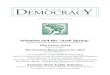
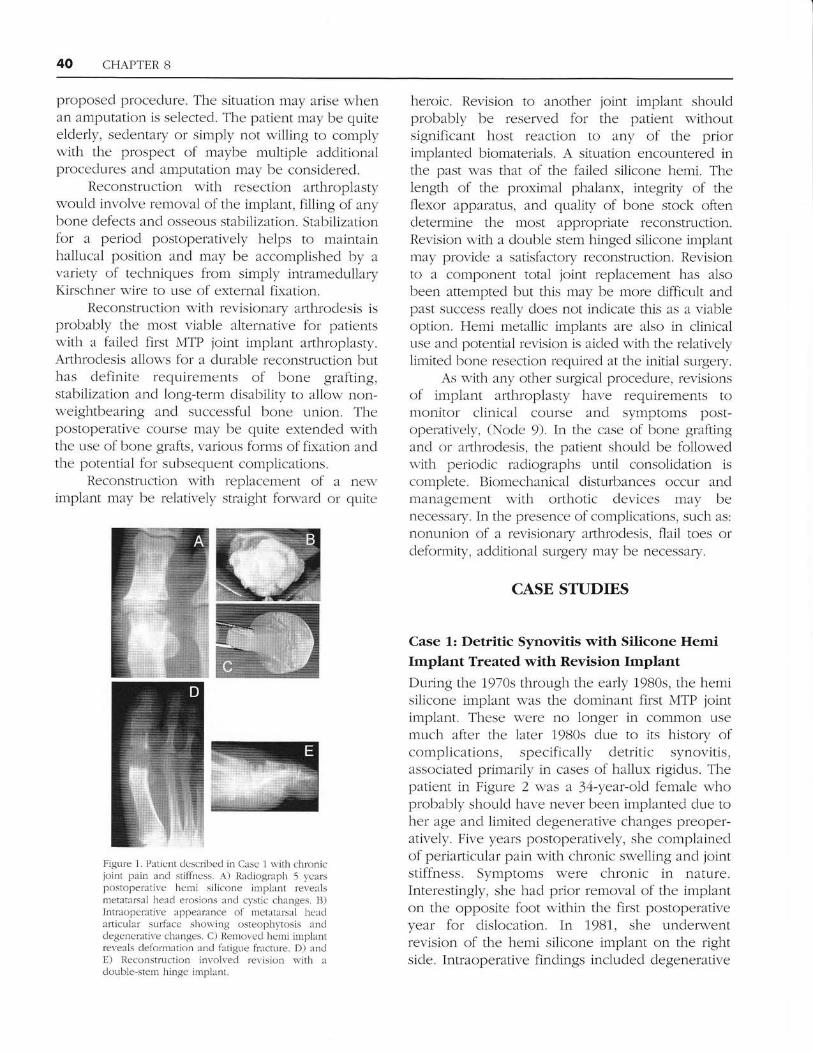
Figure 1. Paticnt clcscribed in Casc 1 nith chronicjoint pain and stifll.ress. A) Radiograph 5 ,vcarspostoperative hcmi silicone implant revealsmetatars:1i heacl erosions and cystic changes. B)Intraoperative appearance of metatalsal heaclarticrLl:rr sUrface sl-ron'ing osteophytosis ancldegenerative changes. C) Rernoted hcmi implantreveals clelbrrn:rtion ancl flLtigne fracture. D) anclE) Iteconstruction involr,ecl revision $iith aclouble stem hinge implant.
heroic. Revision to zrnother joint implant shouldprobably be reserued for the patient withoutsignificant host reaction to any of the priorimplanted biomaterials. A sitr-ration encounterecl inthe past was that of the failed silicone hemi. Thelength of the proximal phalarr, integrity of theflexor apparatlls, and quality of bone stock oftencletermine the most appropriate reconstr-r:ction.Revision with a double stem hinged silicone implantmay provide a satisfactory reconstruction. Revisionto a component total joint replacement has alsobeen attempted but this may be more clifficr-rlt andpast success really cloes not indicate this as a viableoption. Hemi metallic implants are also in clinicalLlse and potential revision is aided with the relativelylimited bone resection required at the initial surgery.
As with any other surgical procedure) revisionsof irnplant arthroplasty have requirements tomonitor clinical course and symptoms post-operativeiy, (Node 9). In the case of bone graftingand or arthrodesis, the patient should be fbllowedwith periodic radiographs r:ntil consolidation iscomplete. Biomechanical distr-rrbances occur andmanagement with orthotic devices may benecessary. In the presence of complications, such as:
nonunion of a revisionary arthroclesis, flai1 toes orclefbrmiry, additional surfaeryr nray be necessaq/.
CASE STUDIES
Case 1: Detritic Synovitis with Silicofle HemiImplant Treated with Revision ImplantDuring the 1970s through the early 1980s, the hemisilicone implant was the dominant first MTP jointimplant. These were no longer in common usemuch after the later 1980s due to its history ofcomplications, specifically detritic synovitis,associatecl primarily in cases of hailux rigidus. Thepatient in Figr.rre 2 was a J4-yeer-o1d female u,-hoprobably should have never been implanted due toher age and limited degenerative changes preoper-atively. Five years postoperatively, she complaineclof periarticular pain w-ith chronic swelling and jointstiffness. Symptoms were chronic in natlrre.Interestingly, she had prior removal of the implanton the opposite foot within the first postoperativeyear for dislocation. In 1981, she underwentrevision of the hemi silicone implant on the rightside. Intraoperative findings included degenerative
CHAPTER 8 41
changes of the first metatarsal head u.ith implantcleformation and fracture but limited inflammatoryresponse to pafticulate silicone. Revisionary arthro-plasty to a double-stem hinged silicone implant wasperfornred. Her immecliate postoperatirre course wasunremarkable but long-term, she developedIirnitation of first metatarsophalangeal joint motionand lesser metatarsalgia that required ofihoticdevices for relief. She also sustained permanentlimitzrtion of activities ancl work capabilities.
Actua11y, many patients with these implantsdid have goocl results with excellent range ofmotion but the problems of detritic synovitis lezrd
to a backlash with meclicolegal implications. Therewere problems with this implant as many of theseimplants were used in a broad range of patientsand pathology. Patients with halltlx valgus seemedto fair the best while those with hallux rigidus ancl
halh-rx r.arus often encountered complications.
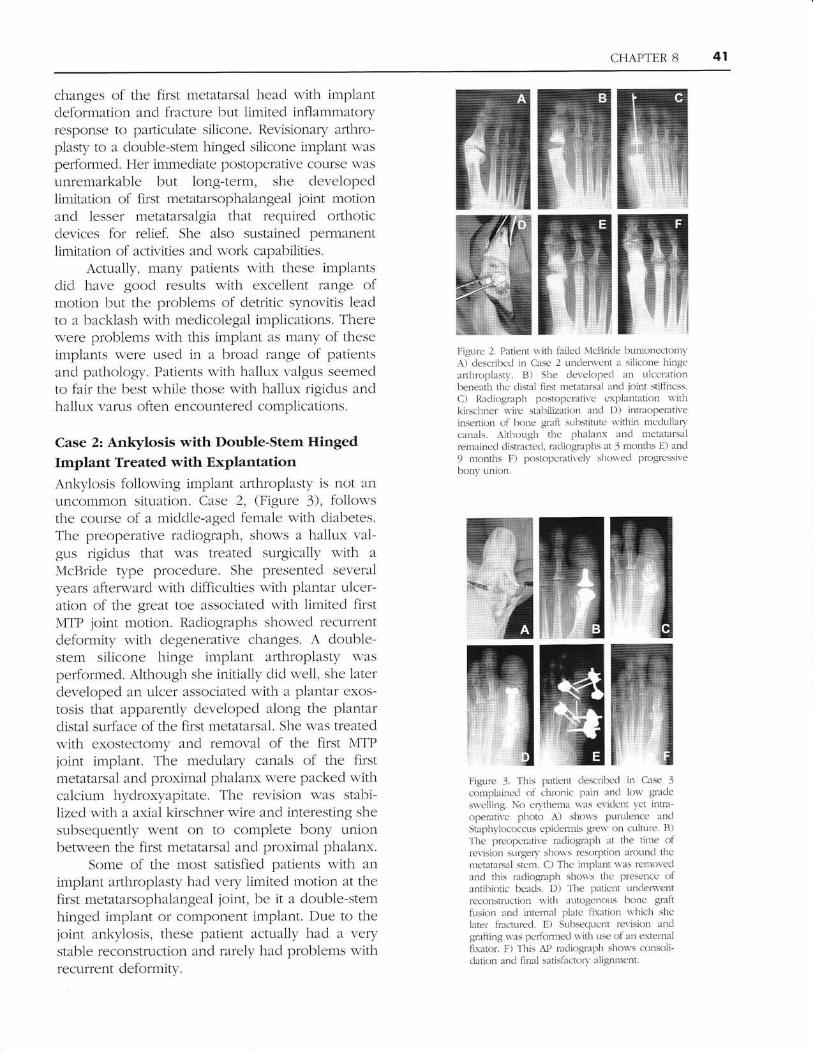
Case 2z Ankylosis with Double-Stem HingedImplant Treated with ExplantationAnkylosis follou,'ing implant arthroplasty is not an
Llncommon situation. Case 2, (Figr-rre 3), followsthe course of a micldle-aged female with diabetes.Tl-re preoperative radiograph, shou.s a halh-rx val-grls rigiclus that was treated surgically with a
McRride type procech:re. She presented severalyears afterrvard with difficulties with plantar ulcer-ation of the great toe associated with limited firstMTP joint rnotion. Radiographs show-ed recllrrentdeformity with degenerative chzrnges. A double-stem silicone hinge implant arthroplasty wasperformed. Although she initially did n e11, she laterdeveloped an ulcer associated with a plantar exos-tosis that apparently developed along the plantardistal surface of the first metatarsal. She n'as treatedwith exostectomy and removal of the first MTPjoint implant. The medulary canals of the firstmetatarsal and ploximal phaianx were packed withcalcium hydroxryapitate. The revision w'as stabi-lized witl-r a axial kirschner n'ire and interesting shesubsequently went on to cornplete bony unionbetween the first metatarsal and proximal phalanx.
Some of the most s2ltisfied patients u,ith animplant arthroplasty had very limited motion zrt thefirst metatarsophalangeal joint, be it a clouble-stemhinged implant or component implant. Due to thejoint ankylosis, these patient actl-lally had a verystable reconstruction and rarely had problems withrecrrrrcnt delorrnity.
Figurc 2. Patient s,ith failecl NlcBricie bllnionccton.IyA) clescribccl in Case 2 ltnclem'ent :r silicone hingearthropl:rsty. B) She cleve lopecl an uiccrationbeneath thc clistal first lrehtxrsal ancL joint stiffness.
C) Racliograph postopcr:ltive cxplantltion \\'ithkirschner wire stairilization ancl D) intraopel':1tive
insefiion of lnne graft substitutc urithin mcclullarvc:rn:rls. ALthough tfic phalanx and net:rtarsairemaircd clistrectecl. radiographs :rt 3 months E) and
9 months F) postopemtirely shorved progrcssivebonr. union.
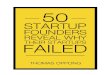
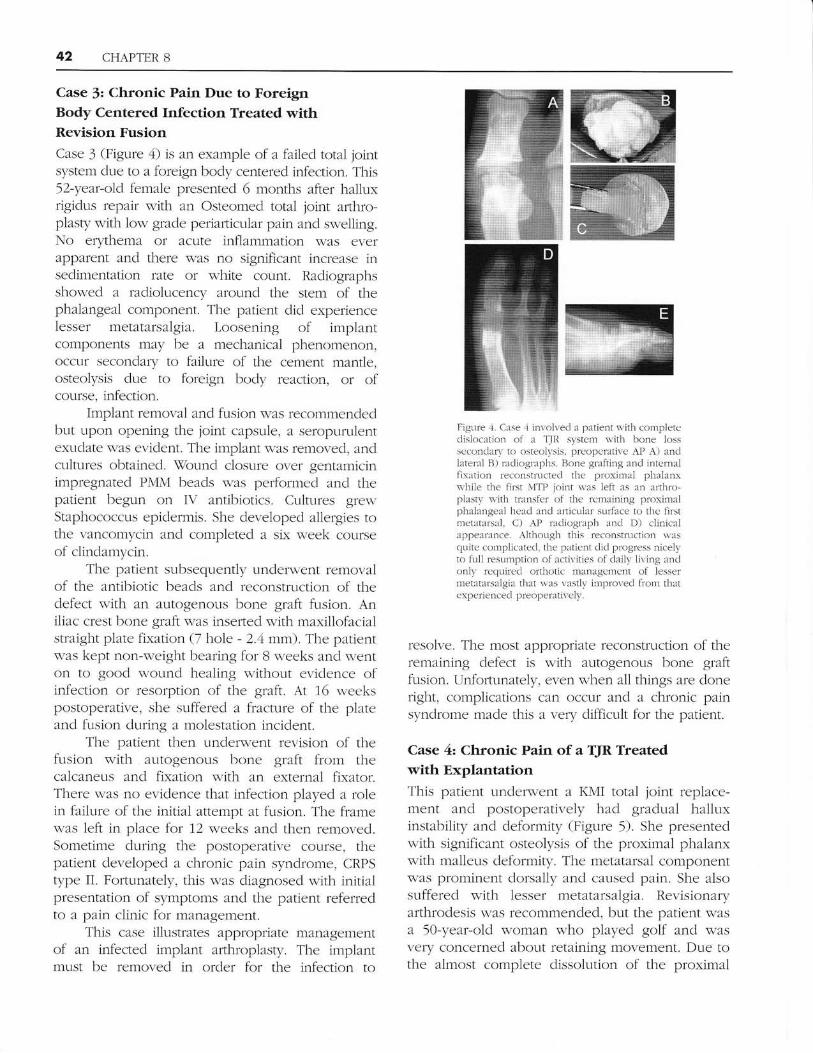
Figure I. Ttris patient clesclibccl in Case 3
complaincd of chonic pain ancl lon. gracle
sq,cllir-rla. No crnthema t'as eviclent yet inffa-operative photo A) shcx's pr-nulence andStaphl.iococcr.rs epiclen'nis gre\\'I on cultr-rre, B)'lhe preopcrattve racliogr:rph at the time ofrer.isior surgery sholls rcsoqrtion alound themetatarsrl stcm. C) The :intpl:rnt l.'as removecland tfils mdiograph shon's the presencc ofantibiotic bcads. D) 'lire paticnt unclem'entreconstruction l.ith autosicnots bonc gmlllusion rncl internal plate fkation n'hich she
later fi'acturecl. E) StLbsequcnt rcr,ision andgraftir-rg *as perlorrned with rtse of an erternalfix:ltor. F) l'his AP racliograph shows consoli-clation and final satjsfactory,' :lligntnent.
42 CHAPTER 8
Case 3: Chronic Pain Due to ForeignBody Centered Infection Treated withRevision FusionCase 3 (Figure 4) is an example of a failed total jointsystem due to a foreign body centered infection. This52-year-old female presentecl 6 months after hallurrigidr-rs repzrir with an Osteomed total joint arthro-plasty witl-r low grade periafiicular pain and su,,elling.No erythema or acute inflammation was everapparent and there was no significant increase insedimentation rate or white count. Radiographsshow.ed a radiolucency around the stem of thephalangeal component. Tl-re patient did experienceIesser metatarsalgia. Loosening of implantcomponents may be a mechanical phenomenon,occur secondary to failure of the cement mantle,osteolysis due to foreign body reaction, or ofcourse, infection.
Implant removal and fusion was recommendeclbut upon opening the joint capsule, a seropurulentexudate was errident. The implant was removed, andcultures obtained. \7ound closure over gentamicinimpregnated PMM beads was performed and thepatient begun on IV antibiotics. Cultures E{rewStaphococcus epidermis. She developed allergies tothe vancomycin and completed a sk week courseof clinclamycin.
The patient subsequently underw-ent removalof the antibiotic beads and reconstftlction of thedefect u,ith an autogenous bone graft fusion. Aniliac crest bone graft was inserted with maxillofacialstraight plate fixation (7 hole - 2.4 mm'). The patientwas kept non-weight bearing for B weeks and wenton to good wound healing without evidence ofinfection or resorption of the graft. At 16 weekspostoperative, she suffered a fracture of the plateand fusion during a molestation incident.
The patient then under-urent revision of thefr-rsion with autogenous bone graft from thecalcaneus and fixation with an external firator.There was no evidence that infection played a rolein failure of the initial attempt at fusion. The framenas left in place for 12 weeks and then removecl.Sometime during the postoperative collrse, thepatient developed a chronic pain syndrome, CRPStype Ii. Fortunately, this was diagnosed with initialpresentation of symptoms and the patient referredto a pain clinic for management.
This case illustrates appropriate managementof an infected implant afihroplasty. The implantmust be removed in order for the infection to
Figure 4. Case ,1 involved 21 patient \\,ith conrplelcdislocatior-r ol a TJll syste m with bone lossscconclary to osteolt.sis. preoperative AP A) andlaterai R) racliogr:rphs. Rone gr:rfting ancl intcrnalfixation reconstructed thc proxirlal phal:rms,-hi1e the flrst NITP ioint \1,as lelt as :rn arthro-pLasty s'ith trarsfel of lhe rcmaining proximalph:rlangeal head and :rrticrLlar surface to thc firstme tat.rrsal, C) AP radiogr':Lph anci D) clinicalappear:1nce. Although this reconstruction wascl,ritc complicatecl, the patient ilid progress nicelyto full resrLmption of :rctivities of d:rilr' living anclonlt, recluirecl orthotic manaEacmcnt of lessermetatirl'salgia that rvas vastly improved fiom th'.rtcxperienceci preoperativcly.
resolve. The most appropriate reconstruction of theremaining defect is with autogenous bone graftfusion. Unforlunately, even when all things are doneright, complications can occr-lr and a chronic painsyndrome made this a very difficult for the patient.
Case 4z Chronic Pain of a TJR Treatedwith ExplantatiotrThis patient underwent a I(MI total joint replace-ment and postoperatively had gradual ha1luxinstahility and deformity (Figure 5). She presentedwith significant osteolysis of the proximal phalanxwith maller-rs deformity. The metatarsal componentwas protninent dorsally and caused pain. She alsosuffered with lesser metatarsalgia. Revisionaryarthrodesis was recommended, but the patient wasa 50-year-o1d woman who played golf and wasvery concerned about retaining movement. Due tothe zrlmost complete dissolution of the proximal
CHAPTER 8 43
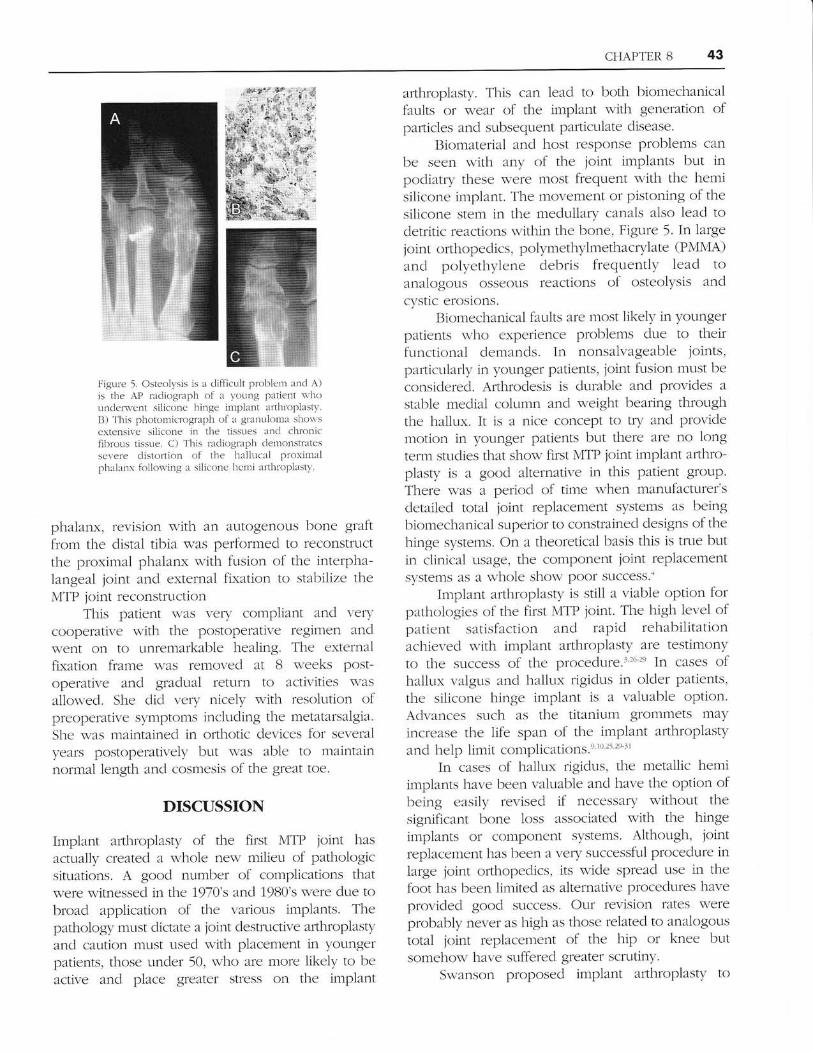
F-igule 5. Osteolysis is a clifllcult problem and A)js the AP r:Lcliograph of a yor:ng prtient s'hounclem'cnt silicone hinge implent :rrthroplastr-.B) 'l his photomicrogr:rph of a grzrnuloma shot'sextensi\.e silicone rn the tissues rncl chronicfibrous tissue. C) T'his racliograPh .lernonstratesscvere distortiot-r of the h:rl1ucal proxirnalphal:Lnx firllowing a silicone hcmi :rrthloplastv.
phalanx, revision with an auto5aenous bone graftfrom the distal tibia was performed to reconstrLlct
the proximal phalanx s,'ith fusion of the interpha-langeal joint and external fixatron to stabilize theMTP joint reconstrLiction
This patlent was very compliant ancl verycooperative \\,ith the postoperative regimen ands,,ent on to unremarkable healing. The externalfixation frame \vas removed 21t B weeks post-operative and gradllal fetllrn to activities \-asa1lowed. She dicl very nicely with resolution ofpreoperative symptoms including the metatarsalgia.
She was maintained in ofihotic clevices for severalyears postoperatively but was able to meintainnorlnal length 21nd cosmesis of the greal toe.
DISCUSSION
Implant arthroplasty of the first MTP joint has
actllally created a whole new' milieu of pathologicsituations. A goocl number of complications thatwere witnessecl in the 1970's and 1980's srere dlle tobroad application of the various irnplants. Thepathology musl dictate a joint destrtlctive arthroplastyand caution must used with placement in yotlngerpatients, those under 50, who are more likely to be
active and place greater stress on the implant
arthroplasty. This can lead to both biomechanicalfaults or wear of the implant with generation ofpafiicles ancl subsequent particttlate disease.
Iliomaterizrl and host response problems can
be seen with any of the joint implants but inpocliatry these were most frequent \\'ith the hemisilicone implant. The movement or pistoning of thesilicone stem in the mec1ullary canals also lead todetritic reactions within the bone, Figure 5. In largejolnt orthopedics, polymethylmethacrylate (PMMA)
and polyethylene debris frequently lead toanalogons osseous reactions of osteolysis andcystic erosions.
Biomechanical faults are most likely in )'oungerpatients who experience problems clue to theirfunctional demancls. In nonsalvageable joints,particularly in younger patients, joint fusion must be
considered. Arthrodesis is durable and provides astable medial column and weight bearing throughthe ha1lux. It is a nice concept to try and providemotion in younger patients but there are no longterm studies that show first MTP ioint implant afihro-plasty is :r goocl alternzrtive in this patient group.
There was a period of time when manufacturer'sdetailecl total joint replacement systems as beingbiomechanical superior to constrained designs of thehinge systems. On a theoretical basis this is true butin clinical usage, the component joint replacementsystems as a whole show poor success.'
Implant arthroplasty is still a viable option forpathologies of the first MTP joint. The l-righ leve1 ofpatlent satisfaction and rapicl rehabilitationachievecl with implant arthroplasty are testimonyto the success of the proceclure.r'2()-2e IL cases ofhal1ux valgr-rs ancl hallr-rx rigiclus in older patients,
the silicone hinge implant is a valuable option.Advzrnces such as the titanium grommets may
increzrse the life span of the implant arthroplastyand help lin'rit complications.e l0252e 31
In cases of hallux rigidus, tl-re metallic hemiimplants have been valuable ancl have the option ofbeing easily revised if necessary without the
significant bone loss associatecl with the hinge
implzrnts or component systems. Although, joint
replacement has been a very successful procedttre in
large joint ofihopeclics, its wide spread use in thefoot has been limited as alternative proceclures have
provided good success. Our revision rates \\'ereprobably never as high as those related to analogottstotal joint replacement of the hip or knee butsomehow have suffered grezlter scrutiny.
Su,'anson proposed implant arthroplasty to
44 CHAPTER 8
improrre cosmesis, improve joint stability, andincrease the likelihood of a reliable degree of jointmotion. Implant arthroplasty as commonlyperformed toclay is not perfbct, but it is a fairlyreliable procedure pafiicularly if the surgeon anclpatient have a clear understanding of the goals andobjectives of the procedr:re.
Finally, if fbot surgeons perform joint implantsurgery, he(she) and the patient shoulcl be wellaware of the potential complications ancl thesurgeon capable of performing, at times,complicated revision surgery.
REFERENCES
1. Albin RK. Weil LS. Flerible implant rrhroplast,v of rhe great roe::rn cvaluation../ An Poclidtr.l: A.r.roc 1971ii 61:967-j5.
2. Cracchiolo A.. Swanson A. Ss,-anson GD. 'I'he arthritic great toenretatarsophalangeal joint: a rer-ics,- of flexible silicone implantarrhroplastv fl'otn tno ntecliciLl centers. C'lin Ortbop 7981;757:64-.).
3. Clacchtolo A. et al.. Afthroplasty of the first metatarsophalangealjoint r,ith a cloublc-stern silicone itnplant. Restrlts in patients s.hohave clegencratir.e joint clisease failure of prcr.ious uper.lrions. orrher,rmatoicl irrrhriris. .J Bane.bint SLu-g Ant 7992:11:512-63.
.ii. GerbertJ. Chang'1.1. Clinical expcrience s.ith t\\.(!colnponcnt firstn]etatllrsel pl-ralangeal jctrnt in-rplants. Clin podiatr ,lIed Stttg1995:12:'i03-13.
j. \loncltrl \,1.. et :11.. In'rplar-rt altlrloplasq,' of thc first rnctatarsopha-langeal joint: :r 12-,ve:rl rctrospe ctive stLlcllr. ./ l.-oot Surg7985;21:273 t).
6. Pf'eiffer WH. et al.. Double stem siliconc implant arthroplasty ofell mclatxl'sophalangeal joints in patients $.ith rheumatoicl:rrthrjtis. Sentin At'tbroplas Ly 1())2;3:76-21.
7. Shenkar \S. Silestic single stem irnplants in tlte treatlnent oflrallrrx rigidrrs. Foctt Anlele Int 7995:76:487 91.
8. Shankar NS, Asaacl SS. Craxford AD. Hingecl silastic irnplants ofthe great rctc. Ctlirt Orthop 1997:272: 227 3/+.
!. Sl'anson AB. clc Groot Srvanson G. LTsc of grommets for fleriblehinge inrplant :rrthroplasty of the grcat toe. Clin C)rthol)1997r340:87 9'i.
10. Su.anson AB, et al. 'I'ltc use of a grommer bone liner for flexiblchingc irrrplant arthroplastlr of the great t,te. Foot Ankle7991:12:719 55.
11. Srvanson AB. Silastic single-sten.i irnplants in the treatment ofhallux rigiclus. Foot Ankle InL 1995;16:E09.
12. Snanson AB. Lumsden RN,I. Snanson GD. Siliconc in-rplantarthroplastl. of thc great toer :r revie\\, of single stem ancl flexiblelrirrge irnplants. Clitl Ofibop 1919:112:30 43.
Vanore J, O'Kcefe RG. Pikscl-rer I. Cllffent statlls of first metrtar-sophalangeal joint implants. Foot Ankle Qudrterl.y 1995;8:721-31.Weil lS, Poll:rk RA. Goller \{rL. Total tirst joint repiacernent infiallrLr r.algus and hallux rigiclus. Long- term results in,18,1 cases.Cl irt Pod krilt 198.ri:1 : 103-29.Yamashina Ntt, N,loatarned F. Peri-articular re:rctions to 11.'ti.roscopicerosion of silicone-polymer implants. Light- and sc;rnningelectron-n-ricroscopic strLdies n'ith energy-dispersi\ e x r.rvanah.sis. Aru .l Surg Pathctl 7985:9:215-9.Y:rnore J, O Keefe R, Irikscher I. Con-rplications of siliconeirrplants in foot slrrgely. Clilt Pocliatry 198,1;1:175-98.Caner.a RG. Postoperrtive clcgcnerative changes of the metatxrsalhead tbllou,ing use of tlie S,i.r,anson rn'rplant: fbur casc repofis../Foot SLIIE 7977 :16:31-7.Dabdoub \i'H, Short I-A. Gtrdas CJ. Aclrte gouty arthritis in a firstmet.ltarsophalangcal joint t'eplacecl u,ith a flexible-l'ringe inrplant:J (il.( Tenurl. J Ftt'l \ttry lOltl 2n l6- o
I-emon B, Pupp GR. IonEl-term cf1icacl, of total SILASTICimplantsr a subjectir.e analysis.,Ilool An.kle Su.rg 1991 ;36:31 l-6.Lernorr RA. Engber WD, N{cBeath AA. A complication of Silastichemi::Lnhroplastl in br-rnion surgely. Foot Ankle 1984;1,252-6.Hetherington \,f. et al. Siliconc implant arthroplastyr a retrospec-tir.c anelysis. ./ Foot Ankle &ug 1c))Jj2:4J$J.N,{cNcamey 'f, ct al. Inguinal lymph nocle tbreign boc\ granr:lo-mas after p1ace1l.iet1t of a silicone rultbcr (Silflex) irnplant of theflrst mctatal'sophalangeal joint. J Rheum cttol. 1996;23:Ut4c)-52.Kitaoka HR, et a1. Salvage of failccl first ntetatarsophalange:rl jorntimplant xrtlroplasty b), irnplant rentor.:Ll ancl s1-novectomv:clinical and biomechanical evalr:ation. Foot Ankle 7992i13:211-50..la1' R\'I. Schoenhaus HD. Complications in irnpl:rnt arthroplastiesfor thc osteoarthritic ioinr../,4nl Podidttl- Assoc 7)82;72:248.lshikalva H. Hanl'rL 'l'. N,Iuras:ls,-a A. The use of gror:nmets forfleriblc hinge toe implants. A case rcport. C'lin Orlhol)1995:316:111-c).Ss anson AR. Lisc t.rf grornments for flexible hinge implant :rrthro-pias6. q,6 dre great toc. Clin Otltop 7997:340:87 9/r.l4oecl<cl tsH. et al. The clouble srentmed silicone-lubber implantlor lheurnatoicl arihritis of the first metatarsophalangeal joint.Lon g-tcrm res u lts. ./ Bozc. Jo i n t S u.rg A n1 7c)92 ;7 I :5 64-l t).
Laird L. Silastic joint arthroplast), of the €jreat toe. A revies. of 228ilnplants using t1're clouble-stemrlecl implant. Clin Orthc)])I9L)0:255:258 72.Sebolcl, EJ. ancl A. Cr:lcchiolo, LIse of titaniurl g1'ommets insiliconc in'rpl:rr-rt arthroplast-v of the h:rlh,rx metrtarsopltalangealjornt. Foctr. Ankle Int 7996. 17(3): p. 145-151.Clayton A{L, Leiclholt JD, Clark N'. Arthropiastv of rhcumatoidnretatarsophalangeal joints: an olltcolre sttdy. Clirt Orthop199 r-;3/+0:48-57.Rrage X4E, Ball ST. Sr-rrgiczLl options for salvagc of end-stagchallr,rx rigidus. l:'oot Ankle Clin, 2002;7:49-73.
15
16
'I it.
tg
1a
14
t7.
23
27
3l
2t)
21
22
21
2i
26
28
l9
30