Embed Size (px)
Citation preview

27
Chapter Two
PROVISION AND PROVIDERS OF HEALTH SERVICES
This chapter gives an overview of the development of health provision starting by facility-based health services delivery, including hospitals and ambulatory care facilities. A particular attention is given to the distribution of services as a determinant of equitable accessibility, while analyzing the role of the public sector in this regard. The health delivery system is in general curative-oriented and technology-driven, except for Primary Health Care (PHC) that is emphasized as community-based services oriented towards promotion and prevention. PHC is considered by the MOPH as a strategy that involves the NGO sector to provide for the poor an affordable alternative to the expensive private ambulatory care. Vertical public health programs are also tackled as necessary interventions that complement and empower PHC, while targeting specific populations and health conditions. The public-private mix at all levels of health care and the remarkable input of the non-profit sector required a particular attention. Finally, this chapter examines human resources development that has a particularly important impact on health provision.
1- HOSPITAL CARE
The role of government in providing hospital care in Lebanon was subject to a vivid debate in the early 1990s. Private services were

28considered expensive and inequitably distributed, whereas public hospitals, that were part of the organizational structure of the MOPH were hopelessly inefficient. Public provision proponents put forward the un-affordability of costly private care in light of the prevailing economic situation and the necessity of ensuring equitable accessibility, as a rationale for government intervention in remote areas. Opponents argued that better regulation may create incentives for private investment in underserved areas while containing cost through better control of demand and supply. As usual, a technical difference is settled according to political interests. Most often the political decision is rather made prior to the technical debate which is then sought only to provide arguments justifying the decision.
1.1 Public Hospitals Development The provision of health services by the Government has
witnessed a meaningful decline during the long years of civil strife and socioeconomic disturbances that have hit the financial and institutional capacities of the public sector. By the end of the civil war, only half of the 24 public hospitals were left operational, with an average number of active beds not exceeding 20 per hospital. The government 1993 reconstruction plan aimed at rehabilitating and building public hospitals in order to have at least one in each district. Whereas building public hospitals in underserved districts such as Akkar, Dnieh, Hermel, Rachaya, and Hasbaya was technically justified; those built in Zahleh, Saida, Tripoli and most of Mount Lebanon districts had no rational justification and merely served political and confessional interests. Nevertheless, the distribution of public hospitals and beds (table II-1) ended up being more equitable than the private ones (table II-2).
Table II-1: Distribution of public hospitals and beds by mohafazat
Beirut ML SL Nab NL Bekaa Total Hospitals 2 6 3 5 7 5 28 Beds 595 430 235 365 455 470 2550
The total cost incurred in construction and equipment amounted to 320 million USD covering a total number of 30 hospitals with a capacity of 2700 beds. The initial investment cost was only the tip of the iceberg, as the government had to deal with increasing operational

29costs recurring every year. Nevertheless, whether a public hospital was worth the investment in a district rather than another was totally irrelevant considering the prevailing public sector inefficiency. The main challenge was how to improve medical, paramedical and most of all, managerial functions in order to provide quality and cost-effective public services. This is an example of how to bear the consequences of self-interested political decisions and find ad hoc solutions. Public hospitals autonomy was sought as a mean to free hospital managers from the public administration bureaucracy. The needed law was drafted but was subject to lengthy negotiations and reviews by finicky bureaucrats who slowed down the procedure. MOPH was racing to obtain the issuance of this law even as massive building work was ongoing. The law was issued in 1996 and was subsequently subjected to several modifications, whereas the applications decrees had to come successively during the following years. This law enhanced tremendously the performance of public hospitals by granting them financial and managerial autonomy and flexibilities for better procurement and recruitment of qualified personnel. The law proved to be vital for the development of public hospitals, giving them the opportunity to be not only complementary but also competitive with the private sector.
Currently, all public hospitals have acquired an autonomous administration board appointed by government decrees, except for the Tyr hospital, located inside the Palestinian refugee camp, and run by an Army officer. Twenty two of these hospitals are currently operational and the remaining is expected to open before the end of 2008.
The administrative and financial autonomous status allows the hospital�s Administration Board to set up contracts with financing agencies including the MOPH. The hospitalized uninsured patient pays 5% of the bill, in comparison to 15% paid in private hospitals and the MOPH reimburses 85%. The public hospital prices are thus 10 percent lower than those of the private. The contracting of the MOPH with its own hospitals is an interesting financing modality where the financial risk is shifted down to the hospital management level. Financial breakeven is a condition for survival. This creates incentives for developing policies to attract patients and reduces transfer as compared

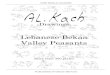
30to the old system�s reverse incentives that prevailed before the implementation of the law of autonomy. The share of public hospitals in admissions has been increasing to exceed, in 2008, 30% of the total admissions on the account of the MOPH.
Fig II-1: MOPH-subsidized admissions to public and private hospitals
It is worth mentioning that the MOPH does not provide any preferential treatment to public hospitals and respects the patient�s freedom in choosing the physician and the hospital. A public hospital is strictly not allowed to select patients nor to impose extra fees. Being less expensive and more equitably distributed than the private, public hospitals are contributing to resolving both cost and equity problems and are expected to play a gate-keeping role through a well-defined referral system.
1.2 Private Hospitals
The private hospital sector development was relatively less affected by the civil disturbances and continued to grow both in number and capacity to represent more than 90% of the total number of hospital beds in the 1990s. This percentage decreased later with the opening of new public hospitals to 80%. However, investment in
27.27
72.73
14.11 18.32
85.8981.68
0
10
20
30
40
50
60
70
80
90
100
2005 2006 2007
PublicPrivate

31private hospitals continued irrespective of the public sector rebuilding plan.
A number of smaller private hospitals are owned by physicians who are considered eminent figures in their community. Most large hospitals often belong to philanthropic or religious congregations, and have a determining role inside the powerful "Association of Private Hospitals". The business community has become increasingly involved in obtaining shares in existing hospitals or investing in new ones. This development in hospital ownership has led to further growth of the sector in an unregulated manner, which has worsened the pre-existing oversupply and induced a greater demand and use of in-patient health services.
Private providers have been investing in areas allowing profit maximization. Poorer regions were not attractive, and remained for a long time relatively underserved, thus exacerbating the inequity problem. Nonetheless, regional discrepancies started becoming less striking by the end of 1990s, as private investment in hospitals increased along with government projects in most of the previously deprived districts. However, the highest availability of beds remains in Beirut and surrounding localities of Mount Lebanon (table II-2).
Table II-2: Distribution of private hospitals according to bed capacity by mouhafazat (2007)
Less than 100 beds 100-200 beds More than 200 beds Total # hosp # hosp # hosp # hosp Beirut 15 4 4 23Mount Lebanon 43 12 1 56North Lebanon 24 3 1 28South Lebanon Nabatieh
219
20
10
249
Bekaa 23 5 0 28Total 135 26 7 168
The MOPH attempts to rationalize the supply distribution remain unavailing in the absence of pertinent legislations. The MOPH disposes of a database on the availability and distribution of health facilities and equipment, within a geographic information system (GIS). This database is known as the �Carte Sanitaire� and it was developed as a tool to control the supply. The law project proposed by

32Ta
ble
II-3
: Dist
ribu
tion
of M
OPH
con
trac
ted
hosp
itals
and
allo
cate
d bu
dget
by
mou
hafa
zat
Tota
l Leb
anon
Con
trac
ts w
ith M
OPH
Y
earl
y ce
iling
(100
0 LB
P)
Perc
ent a
lloca
tion
# ho
sp
(%)
2000
20
02
2007
*
Bei
rut
23
(13.
7)
22
8 11
28
.248
.000
13
.4
Mou
nt L
eban
on
56
(33.
3)
50
23
43
61.8
85.2
00
29.4
N
orth
Leb
anon
28
(1
6.7)
22
17
25
45
.547
.200
21
.6
Sout
h Le
bano
n 24
(1
4.3)
19
11
15
30
.904
.800
14
.7
Nab
atie
h 9
(5.4
) 4
5 9
10.9
21.2
00
5.2
Bek
aa
28
(16.
7)
23
12
22
33.1
51.2
00
15.7
To
tal
168
(100
.0)
140
76
125
210.
657.
600
100.
0 *
Incl
udin
g pu
blic
hos
pita
ls
Tabl
e II
-4: P
er c
apita
allo
catio
n of
MO
PH h
ospi
taliz
atio
n bu
dget
by
moh
afaz
at (L
BP)
Popu
latio
n*
MO
PH B
udge
t Allo
catio
n/ye
ar
2007
**
Per
capi
ta a
lloca
tion
Bei
rut a
nd M
ount
Leb
anon
1
,892
,073
90
,133
,200
,000
48
,000
N
orth
Leb
anon
76
8,70
9 45
,547
,200
,000
59
,000
So
uth
and
Nab
atie
h 62
3,04
3 41
,826
,000
,000
67
,000
B
ekaa
47
1,20
9 33
,151
,200
,000
70
,000
Le
bano
n (to
tal)
3,75
5,03
4 21
0,65
7,60
0,00
0 56
,000
* H
ouse
hold
s Sur
vey
2004
. CAS
** D
ecre
e N
o. 2
2/1
Janu
ary
2007
, MO
PH

33
the MOPH to link licensure of new health care facilities to open geographical locations on the Carte Sanitaire is still �on freeze� in the Council of Ministers.
Whereas inequitable accessibility may partially result from disparities in regional availability of hospital services, it is mostly related to variations in the insurance coverage and the ability to pay among the population. These inequalities were somewhat compensated through more equitable MOPH budget allocation to contracted hospitals as shown in table II-3.
The MOPH aims at providing equal accessibility for the uninsured by contracting with providers in all regions, while trying to adjust per capita allocation of budget between regions according to needs (table II-4). This proved to have, as shall be explained later, an important impact on the accessibility of the poor to hospital services.
Efficiency has been a major concern since the 1990�s1. The majority of private hospitals (135 out of 168) are general and multidisciplinary with less than a 100-bed capacity, and are still encountering difficulties in achieving economies of scale while offering acute care of appropriate quality. Imposing extra fees on MOPH patients was and is still not an uncommon practice.
The availability of �high-tech� services and heavy equipment in relation to the population size is comparable with, and sometimes exceeds, those of Developed Countries. Oversupply in hospital beds and equipment lead to a smaller market share per service and thus to a higher cost per unit. This occurs despite the supplier-induced demand and unnecessary increase in volume, and the consequent inflated bills.
Behind the rapid and continuing growth of private hospitals and their oversized equipment during the eighties and nineties, lie financial incentives generated by contracts with public funds. This explains why long-stay hospitals lacking such incentives, do not attract the private
1Van Lerberghe, W; Ammar,W; Mechbal, A.H. De l�impasse à la réforme: La crise du secteur de santé au Liban. Studies in Health Services Organization and Policy, 2,1997.

34for-profit sector and remain strictly the domain of religious congregations and philanthropic associations. Twenty hospitals with 3600 beds belong to this category which includes elderly homes and geriatric services, rehabilitation and long term physiotherapy, mental health and other chronic conditions. These services are under-priced with a per diem-based reimbursement from MOPH and Ministry of Social Affairs (MOSA.)
Table II-5: Availability of "high-tech" services and heavy equipment (2005)
Lebanon OECD** Number of units Units per million* Units per million
Open heart surgery departments 22 5.7 Cardiac catheterization laboratories 32 8.3 3.3Dialysis centers 55 14.2 5.2Organ Transplant centers 5 1.3 Bone marrow transplant units 3 0.8 Specialized burns centers 1 0.3 In-Vitro Fertilization centers 12 3.1 Radiotherapy 8 2.1 6.2Lithotripsy 31 8.0 2.2CT scan 104 26.9 20.6PET scan 3 0.8 0.6MRI 38 9.8 9.8Sources:* Ministry of Public Health. 2007 and Syndicate of Private Hospitals, 2007 ** Organization for Economic Co-operation and Development (OECD), Health data, 2007
The Ministry of Public Health has been struggling to improve the quality of hospital care and to establish hospital regulation mechanisms. The most successful experience in this domain was the use of accreditation as a tool to improve quality and at the same time to rationalize MOPH contracting with hospitals. The classification system that ranked hospitals according to their capacity, technology advances and level of hotel services, shifted with the beginning of this decade to an accreditation system that focuses more on process and performance.
Over the past 8 years, external auditing of hospitals against explicit quality standards has been promoting, a culture of quality improvement, while providing financing agencies with objective criteria for selecting hospitals. The MOPH was to a large extent capable of restricting contracts to accredited hospitals despite all

35pressures. Table II-3 shows the important decrease in number of contracted hospitals in 2002 compared to 2000 as a result of linking contracting to accreditation. The argument that the MOPH policy would be detrimental for the poor as peripheral hospitals are not prepared for accreditation was refuted by the auditing results as shown in table II-6.
Table II-6: Accreditation of private hospitals by mohafazat (December 2006)
A B C D Total (%) Beirut 3 2 5 1 11 (18.4) Mount Lebanon 11 3 11 14 39 (35.0) North Lebanon 4 2 10 3 19 (20.4) South Lebanon 1 2 13 21 18 (17.5) Bekaa 3 2 7 4 16 (15.5) Total 22 11 46 24 103 (100.0)
This topic as well as other regulation mechanisms such as hospitals performance assessment and control of supply would be developed more in depth later on. Nevertheless, the hospital sector in Lebanon operating in a market economy environment, still needs further regulatory measures in order to improve its efficiency and limit its disproportionate growth.
2-AMBULATORY CARE
Outpatient care is provided by a multitude of health facilities ranging from physicians in solo practice to multidisciplinary polyclinics. High technology is also invading outpatient facilities, including medical laboratories, radiology and other non-invasive diagnostic centers, physiotherapy and dental care clinics, as well as a wide range of same-day treatment clinics, such as dermatology and cosmetic clinics using laser techniques.
It is worth mentioning that these out-patient facilities are beyond any effective control. The practice license provided to medical and paramedical professionals allows them to open a center and to acquire any kind of equipment they deem necessary to provide services within their competencies. Except for medical laboratories, radiology, and physiotherapy, out-patient facilities as such are not subject to licensing.

36
Tabl
e II
-7: M
edic
al fa
cilit
ies l
icen
ses:
dist
ribu
tion
by ty
pe a
nd r
egio
n (M
OPH
, Dec
.200
7)
Bei
rut
Mou
nt L
eban
on
Nor
th L
eban
on
Sout
h Le
bano
n N
abat
ieh
Bek
aa
Tota
l Pr
ivat
e ho
spita
ls*
21
(11.
1%)
64
(33.
9%)
34
(18.
0%)
24
(12.
7%)
10
(5.3
%)
36
(19.
0%)
189
(100
%)
Publ
ic h
ospi
tals
2 (6
.7%
) 6
(20.
0%)
7 (2
3.3%
) 4
(13.
3%)
6 (2
0.0%
) 5
(16.
7%)
30
(100
%)
Disp
ensa
ries
13
6 (1
2.5%
) 40
2 (3
7.1%
) 21
9 (2
0.2%
) 11
3 (1
0.4%
) 63
(5
.8%
) 15
2 (1
4.0%
) 10
85
(100
%)
Imag
ing
cent
ers*
* 27
(1
2.9%
) 87
(4
1.6%
) 38
(1
8.2%
) 22
(1
0.5%
) 8
(3.8
%)
27
(12.
9%)
209
(100
%)
Med
ical
la
bora
tori
es**
45
(1
5.6%
) 10
2 (3
5.3%
) 37
(1
2.8%
) 30
(1
0.4%
) 16
(5
.5%
) 59
(2
0.4%
) 28
9 (1
00%
)
Path
olog
y la
bora
tori
es *
* 6
(15.
4%)
13
(33.
3%)
7 (1
7.9%
) 8
(20.
5%)
1 (2
.6%
) 4
(10.
3%)
39
(100
%)
Bloo
d ba
nks *
**
5 (2
0.0%
) 10
(4
0.0%
) 5
(20.
0%)
2 (8
.0%
) 0
(0.0
%)
3 (1
2.0%
) 25
(1
00%
) D
enta
l la
bora
tori
es
41
(12.
9%)
163
(51.
1%)
37
(11.
6%)
37
(11.
6%)
12
(3.8
%)
29
(9.1
%)
319
(100
%)
Phys
ioth
erap
y ce
nter
s 73
(1
6.6%
) 20
8 (4
7.2%
) 83
(1
8.8%
) 37
(8
.4%
) 13
(2
.9%
) 27
(6
.1%
) 44
1 (1
00%
)
Pros
thet
ic &
or
thot
ic
wor
ksho
ps
3 (1
0.0%
) 15
(5
0.0%
) 6
(20.
0%)
5 (1
6.7%
) 0
(0.0
%)
1 (3
.3%
) 30
(1
00%
)
*
Incl
udin
g lo
ng-s
tay
hosp
itals
**
Incl
udin
g th
ose
insi
de a
nd o
utsi
de h
ospi
tal f
acili
ties
***
Excl
udin
g Le
bane
se R
ed C
ross
tran
sfus
ion
cent
ers

37During the civil war years of 1975-1990, a big number of
dispensaries were licensed, belonging to Non Governmental Organizations (NGOs) and political forces, filling the gap caused by the absence of the public sector. Their services were most of the time limited to the distribution of donated medicines. These dispensaries have been able to survive mostly by relying on the support of MOSA and international donors, and on the collection of fees for service. The decline in international donations and the lack of volunteers in the after-war period have forced many to increase patients� charges. Most of the NGOs facilities were single room understaffed dispensaries with irregular working hours. Only a few were well staffed health centers with modern equipment, such as EKG, US and X-ray machines, and medical laboratories. Medical personnel were available on a part-time basis, and the presence of qualified licensed nurses was uncommon.
Over the 15 years following the end of the civil war, almost all of the dispensaries operating in the country have been receiving vaccines free-of-charge from the MOPH, and most of them have been benefiting from the MOPH-YMCA joint program on drugs for chronic illnesses, in return for a nominal contribution.
According to the 1997 Households Living Conditions Survey, twenty six per cent of interviewed households declared seeking services from public and NGOs dispensaries, which represented the only affordable option for the most deprived2. More evidence shows a continuous increase of this percentage with the enlargement of the PHC network under the leadership of the MOPH3.
The ambulatory care benefits� package varies according to the insuring agency. Among the insured population 15.7% and 60.8% declared not being covered for medical consultations and dental care respectively. Considering the number of uninsured4, almost 60% and 80% of the population respectively do not receive any reimbursement
2Central Administration of Statistics. 1997 Households Living Conditions. 3Reports analysis, PHC monitoring system, MOPH. 4Center Administration for Statistics. 2001. National Households Health Expenditures and Utilization Survey 1999.

38for medical consultation and dental care, which highlights further the need for services provided by the PHC network.
3- COMMUNITY BASED HEALTH SERVICES
3.1 The Role of NGOs
During the years of the civil strife, UN agencies played a major role in conducting essential health programs in joint coordination with NGOs. Activities of NGO�s centers depended heavily on the availability of drugs. MOPH and UNICEF used those donated drugs as incentives to encourage preventive programs among NGOs.
When the MOPH regained leadership over these programmes in the early 1990�s, new incentives were introduced through contractual agreements5. Programs are now run through a network composed of MOPH, MOSA, and NGOs� PHC centers, that covers the whole country.
NGOs have been contributing successfully to joint preventive programs carried out by the MOPH and UN agencies, such as the diarrhea and respiratory infection prevention programs of the 1990s. NGOs actively participate to the activities of the Expanded Program for Immunization (EPI), AIDS control and reproductive health programs.
In addition to the provision of services, some NGOs play a meaningful supporting role in the health system by conducting surveys or training workshops, or by providing logistical support through purchasing, stocking and distributing essential drugs to a vast network of PHC centers, thus ensuring the follow-up of chronically ill patients6.The contract with the Lebanese Red Cross (LRC) for car accidents and emergency transportation is another example of cost-effective services provided through a contractual relationship with an NGO.
5Ammar, W. Health Care Market in Lebanon: Government-NGO Cooperation. Paper prepared for WHO and presented at the Seminar on New Partnerships for Health Development in Developing Countries: The Contractual Approach, a Policy Tool, Geneva 1998.
6Ammar, W., 2003. Health System and Reform in Lebanon. Beirut: WHO.

39
3.2 The Primary Health Care Network A first National Conference on Primary Health Care was held
in Lebanon in 1991. It was inspired by the Alma Ata declaration on �Health for All� in 1978. This was the starting point of a series of consultative meetings held by the MOPH with all stakeholders that led to the elaboration of the PHC National Strategy. A comprehensive assessment of health centers and dispensaries, operating all over the country, was conducted in 1996. The purpose was to identify those able to provide a comprehensive minimal package of PHC services including prevention activities. Among more than 800 facilities, only 29 health centers (19 NGOs, 8 MOPH and 2 MOSA) were selected to form the nucleus of a National Network that evolved to encompass 86 centers in 2005, 109 in 2006 to reach 120 centers in 2007. To this end, the MOPH had to deploy important efforts in many directions including the development of guidelines and health education materials, training activities, developing incentives through contractual agreements, purchasing and distribution of vaccines, drugs, medical supplies and sometimes equipment. In addition, the MOPH used international donations to build and equip 28 health centers that are currently run by NGOs and municipalities, and to transform 5 public rural hospitals into advanced PHC centers.
Each health center has a defined catchment area with an average of 30,000 inhabitants, with some exceptions in under populated rural areas where the number of potential beneficiaries should however not be lower than 15000. The center provides general medical care including pediatrics, cardiology, reproductive health and oral health. Efforts are put on the integration of mental health in the package and to emphasize home care. The center should also play an important role in immunization, school health, health education, nutrition, environmental health and water control. Provision of vaccines, essential drugs and other kinds of support are linked to the pattern of activities that are regularly reported to the MOPH and are subject to analysis, evaluation, and feedback. It is worth mentioning that the PHC centers in the MOPH network do not differentiate between �insured� and �uninsured� in terms of nominal fees. The MOPH policy is to provide an alternative to all those who seek affordable essential services through its network.

40
The MOPH has learned from its experience with private hospitals to avoid perverse incentives generated by linking reimbursement to the volume of services. The ministry�s contracting with NGOs has been a success because it did not involve money transactions for purchasing services. The approach adopted focused on encouraging NGOs to improve the community health status while benefiting from the ministry�s assistance in medical paramedical and management training, in providing vaccines, essential drugs, medical and educational supplies, and from other in kind deliverables.
PHC targets horizontally a whole community using a polyvalent care-givers team and through well established relationships within the health system�s hierarchy. Vertical heath programs on the other hand, focus on disease or service-related objectives and may target a specific age group or sex or region. Clinical guidelines, training programs and education material are developed by one national team of specialized staff that serves all the PHC centers involved with the program. Therefore, the PHC horizontal approach and vertical programs cross cut and complement each other. The vertical approach allows however shifting emphasis between and within programs objectives according to changing priorities.
4- VERTICAL HEALTH PROGRAMS
4.1 Expanded Immunization Program
The Expanded Program for Immunization (EPI) is financed and led by the MOPH. UNICEF, MOSA and NGOs are active partners. Immunization is routinely conducted in almost all health centers and dispensaries operating in the country. The National Calendar includes vaccinations against poliomyelitis (OPV), diphtheria, tetanus, pertussis (DTP), measles mumps, rubella (MMR). The hepatitis B vaccine (Hep. B) was introduced in 1998 and became with the Hemophylus influenza B vaccine (Hib) a part of the Penta vaccine (DPT, Hib, Hep. B) since mid 2006. The number of centers involved in EPI activities has reached in 2007 a total of 109 public and 540 NGOs centers. This partnership has successfully achieved the targeted objectives of the program, as shown in table II-8. The objectives were set however, in

41considering that private for-profit physicians� clinics cover around 50% of the immunization activities. This should be subject to reassessment especially that wide district variations probably exist in terms of public private mix.
Table: II-8: Immunization coverage reached by routine activities in 2006 and 2007
Vaccine Under one year population
Number reached Coverage*
2006 2007 2006 2007 DTP 3 65405 30100 33918 46% 57% OPV 3 65405 29980 33984 46% 57% MCV1** 65405 31763 35998 48.5% 55% Hep B 3 65405 30100 33918 46% 52%
* Only immunization coverage reached through the public and NGOs facilities. ** MCV= measles containing vaccine.
In addition to routine vaccinations, the EPI program started implementing since 1995 National Immunization Days (NID), twice a year. Table II-9 shows the coverage achieved over the last 3 consecutive years based on district health officers reporting.
Table II-9: Achieved coverage through National Immunization Days as reported by districts� officers
Year Target 0-59 months Number reached Percent coverage reached 1995 375,000 359,605 95%
1999 375,000 365,212 97%
2005 324,215 297,410 92%
2006 335,000 321,212 97%
2007(1) 84,079 81,611 97%
(1) 2007 campaign was a Sub-National campaign targetting the Qadas bordering Syria (Hermel, Baalbeck, Zahleh, West Bekaa, Rashaya, Akkar).
Immunization coverage assessment studies however, provide evidence that at least in remote areas the coverage is far from being ideal, as important disparities exist among and within districts.
The last confirmed indigenous case of polio in Lebanon in the 1990s was reported in 1994. Since then, however one locally infected case

42was reported in 2003. The virological culture and genotyping confirmed an infection caused by wild poliovirus type 1 (PV1), South Asia (SOAS) genotype. Epidemiological investigation indicated that the father of the index case was probably the vehicle of the virus, as he had recently travelled to India.
In 2006, measles� outbreak occurred, with 905 reported cases and 2 deaths. Consequently, the EPI technical committee re-introduced in 2006 the monovalent measles vaccine at 9 months to improve the measles national coverage. Considering that two significant measles outbreaks have occurred in the country over the past five years, and in line with the global commitment in eliminating measles and controlling rubella by year 2010, the Ministry of Public Health, conducted a measles and rubella (MR) Catch-up Campaign in spring 2008 targeting around 900,000 children aged 9 months to 14 years. The MOPH experience in this catch-up campaign is worth emphasizing for its relevance for both the regional and the country levels (Box II-1).
As the deadline for achieving the Millennium Development Goals is coming close, the MOPH has to overcome the variability caused by vaccinations conducted in the private sector. It had to find a way to guarantee effective immunization coverage. Setting nominal checklists of target children was thought to be an effective approach, its feasibility is still, however, under the test of time, as it would be explained in chapter six.
Along the same line, the MOPH has developed in 2006 a software to monitor the cold chain temperature. The system was designed to archive, and real-time monitor temperatures of different locations of vaccines stocks. The system archives all temperature values at any set sequence, and could be accessed by computer dial-up connection. It also generates dial up voice message in any alarm case, alerting four ministry officials and a technical person, specifying the location of the breakdown and keeps alarming until corrective measures are taken.

43
Box II-1: The 2008 Measles and Rubella (MR) catch-up campaign
This catch-up campaign gathered the highest number of stakeholders ever reached in Lebanon. In addition to traditional collaboration with other ministries, the NGOs and the scientific societies, the association of private schools and the syndicate of specialized nurseries were also actively involved. Two hundred vaccination teams were organized with licensed trained personnel, to cover some 1,400 public and 2,000 private schools across the country.
WHO- EMRO recommendation was to vaccinate all children of the target age-group irrespective of the child�s immunization status and measles illness. As for most EMR countries, previous history of vaccination and disease is impossible to assess during the campaign. The MOPH was reluctant to comply in the absence of scientific evidence on the added value of additional injection of vaccine for those who have already completed their vaccination on one hand, and the usual non-compliance of private schools on the other. Upon the insistence of WHO and in light of an encouraging meeting held with the association of private schools, the MOPH finally agreed to adopt the EMRO strategy. However, during the campaign school directions showed tremendous resistance to comply, and insisted on having the consent of the parents who, in turn, needed to refer to treating physicians. A tremendous effort was put to contact schools� directors and physicians in order to convince them to accept �a useless additional injection� to children, they were sure had already completed their vaccination. Needless to say this effort would have been better channeled to fill the vaccination gaps in poor city suburbs and remote villages. Obviously such a campaign could never, in the Lebanese context, reach its set targets. This experience is worth mentioning to highlight the importance of adapting interventional strategies to the national context, as they depend on many local factors such as mothers� education, her knowledge about her child�s vaccination and her ability to provide a correct answer. Other factors include the importance of the private sector�s role in both education and health, and, most importantly, how stringent can the health authority be in imposing controversial health measures. What happened next is also informative: A WHO
procedure of evaluation for a campaign, that we knew had failed, and we even knew the reasons behind its failure!
expert came to assess the campaign, and we had to undertake a usual

44
4.2 Tuberculosis Control Program The MOPH takes full charge of tuberculosis patients including
non-Lebanese legal residents. Services are provided through 8 TB centers and include diagnostic, therapeutic, close follow-up and prevention activities.
In 1998, the TB program started implementing the Directly Observed Treatment Strategy (DOTS). The average number of one thousand cases treated yearly in the early nineties, has been going down to 700 in 1998 to reach 570 active TB cases in 2001, and 473 cases in 2007. Twenty five percent of TB patients in 2007 were non-Lebanese, 54% females and 46% males, and 3 cases were HIV positive. DOTS approach is currently widespread, and an active surveillance system is in place. The recovery rate has reached 91% of treated patients.
Table II-10: Distribution of TB cases by age group (2007)
0-4 5-14 15-24 25-34 35-44 45-54 55-64 65+ Total (%) Pulmonary / Smear positive
0 1 29 49 26 17 14 7 143 (30.23)
Pulmonary / Smear negative
10 7 29 32 18 8 7 7 118 (24.95)
Extrapulmonary 6 16 59 61 22 20 15 13 212 (44.82) Total 16 24 117 142 66 45 36 27 473 (100.00)
4.3 Reproductive Health Program
The Reproductive Health Program was launched by MOPH in September 1998, in collaboration with UNFPA and MOSA. Its activities include providing health centers with supplies and drugs, medical equipment, as well as training and to some extent physical rehabilitation. By year 2000, 430 centers had been included in the program, of which 86 had adequate equipment, including 10 with ultrasound machines, and 42 were physically rehabilitated. Sixteen training workshops have been held, whereby 420 health professionals and health workers received training. Currently, 183 centers have been selected as �Centers Of Excellence� (COE), to provide higher standard reproductive health (RH) services in all districts.

45Table II-11: Distribution of centers benefiting from the reproductive health
program by mohafazat (2006)
Region MOPH Run by NGO
NGOs MOPH MOSA Muni-cipalities
Total (%)
Beirut 1 12 1 2 0 16 (8.74) Mount Lebanon 10 17 2 11 2 42 (22.95) North Lebanon 2 19 5 7 0 33 (18.03) South Lebanon 3 8 3 15 0 30 (16.40) Nabatieh 4 23 2 1 0 29 (15.85) Bekaa 8 16 2 7 0 33 (18.03) TOTAL 28 97 14 41 2 183 (100.00)
In addition to offering quality medical services, the COE addresses RH determinants such as unsafe sexual behavior and sexual dysfunction. The scope of services includes: prevention, early detection and treatment of STDs and HIV, basic antenatal, postnatal and post partum care, menopause and post menopause counseling and treatment; family planning activities and adolescent counseling and care. Normative tools such as clinical protocols and management guidelines have been developed and training sessions conducted. A monitoring system is in place with regular reporting, data analysis and feedback.
4.4 National AIDS Control Program
This program was launched by MOPH and WHO in 1989. In the 1990s, a yearly MOPH budget of over 400 million LP was devoted to this program, as a trust fund managed by WHO. This provided better disbursement flexibility and allowed the program to undertake nation-wide preventive and educational campaigns largely covered by the media. NGOs and especially youth associations are actively involved in anonymous testing and counseling activities. The trust fund was reduced in 2000, to 100 million USD, as the MOPH started in 1998 allocating more funds for purchasing multi-therapy drugs. However, the program was capable to mobilize financial resources from international donors.
In this regard, a national HIV/AIDS monitoring, surveillance and evaluation system was established with the World Bank

46
Tabl
e II
-12:
Chr
onic
illn
esse
s dru
gs p
rogr
am: d
istri
butio
n of
hea
lth c
ente
rs a
nd b
enef
icia
ries
by
type
and
reg
ion
Reg
ion
NG
Os
Cen
ters
M
OPH
Cen
ters
M
OSA
ce
nter
s M
OSA
subs
idise
d
NG
Os C
ente
rs
Tota
l num
ber
of
cent
ers
Num
ber
of
bene
ficia
ries
B
eiru
t 37
1
1 1
40
2557
4 M
ount
Leb
anon
15
3 5
3 11
17
2 39
706
Nor
th L
eban
on
66
2 1
6 75
28
898
Sout
h Le
bano
n 81
3
11
1 96
36
557
Bek
aa
47
3 4
3 57
27
110
TOTA
L 38
4 14
20
22
44
0 15
7845
So
urce
: You
ng M
en C
hris
tian
Asso
ciat
ion
(YM
CA)
200
7.
Tabl
e II
-13:
Epi
dem
iolo
gica
l pro
file
of b
enef
icia
ries
and
thei
r di
stri
butio
n by
co-
mor
bidi
ty a
nd m
ultip
le
ther
apy
in%
(N=
157,
845
patie
nts i
n 20
07)
Epid
emio
logi
cal P
rofil
e D
iagn
osis
C
ardi
ovas
cula
r H
yper
tens
ion
Dia
bete
s H
yper
lidid
emia
Ep
ileps
y O
ther
s B
enef
icia
ries %
34
.6
16.4
14
.3
13.8
6.
4 14
.5
Co-
mor
bidi
ty
N
o. o
f Illn
esse
s 1
2 3
4 5
6Pa
tient
s %
43.2
30
.9
16.7
6.
8 2.
0 0.
5 M
ultip
le T
hera
py
Dru
gs p
er p
resc
riptio
n 1
2 3
4 5
6
Patie
nts %
30
.9
24.3
18
.2
12.3
7.
3 7.
0 So
urce
: You
ng M
en C
hris
tian
Asso
ciat
ion
(YM
CA)
200
7.

47Institutional Development Fund. This system involved 350,000 USD in 2006 and is currently operational.
The program received also 200,000 USD from the UN Office for Drugs and Crime in 2007, to increase access to prevention and care services for drug use and HIV/AIDS in the prison settings. UNAIDS approved a budget of 40,000 USD for reinforcing voluntary counseling and testing services during 2008. So far, the program has been successfully achieving the set objectives for these grants.
The program, in collaboration with UNICEF is currently working on the identification and promotion of successful models for a comprehensive response to HIV/AIDS, especially for vulnerable young populations.
Ninety two new HIV cases were notified in 2007, making a cumulative number of 1057 cases recorded since 1989, with 82% males, most of them between 31 and 50 years. Seventy percent got infected through sex, namely heterosexual relations (56% of all cases). The mother to child transmission accounts for 2.2% of all cases. Since 1999, only 3 cases of blood transfusion HIV infection were reported and occurred outside the country.
4.5 Medication for Chronic Illnesses Program This program is financed and supervised by MOPH, while
purchasing, storage, and distribution of drugs are delegated to YMCA. Drugs are dispensed by public and NGOs� health centers to chronically ill indigent patients. The social and financial status of beneficiaries and their families is assessed by professional social assistants. By the year 2007, 440 centers have been affiliated with the program, while the cumulative number of beneficiaries has reached 157,845 patients. The total budget of this program is over 10 billion L.P. including 3.9 billion paid yearly by MOPH for procurement of drugs. It is to be noted that during the July-August 2000 war, 57 additional dispensaries joined the program to meet the needs of the chronically ill displaced persons.
The program is also an important source of information on morbidity and prescribing behavior. The beneficiaries� epidemiological

48profile shows that 34.6% live with cardiovascular conditions, 14.3% with diabetes, 16.4% are treated for hypertension, 13.8% have hyperlipidemia and 6.4% are epileptic cases. Twenty six percent are suffering from 3 diseases or more, and 26.6% are treated with more than 3 drugs.
4.6 School Health Program School Health is a joint Program between WHO, the MOPH
and the Ministry of Education (MOE), and is implemented in close cooperation with the Orders of Physicians and Dentists. It involves three components: The first relates to healthy school environmentwhich includes water control and sanitation, safe accessibility, and general safety measures of the building and the playground. It includes also the inspection of food and beverages sold inside the school and in the surroundings that influence unhealthy lifestyles and eating habits. The second tackles the promotion of healthy lifestyles through the integration of health education in the curriculum, and the promotion of extracurricular health activities. And the third is the medical caredimension that includes routine check-ups, immunization, oral health and others.
Guidelines to standardize the medical exam have been developed and 470 school doctors trained. A referral system is established by linking schools to neighboring PHC centers network for medical and oral health care. An assessment of the school health environment is also planned according to international standards, and shall be followed by interventions to improve resources for environmental safety such as filtration of drinking water, lighting and ventilation. A school health inspection guidebook has been produced and a training for health inspectors is being conducted. Teachers have been trained on health e-learning in schools and IT equipments procured to 10 private, 20 public and 10 UNRWA schools.
In addition to ongoing school health activities, a Global School Health survey was conducted and revealed interesting features that would impact the program�s activities for the coming years (box II-2).

49
Box II-2: Global School-Based Student Health Survey*
A Global School Health Survey was conducted in October 2005, targeting students in grades 7-9 in 100 schools across Lebanon. The survey included questions on alcohol and other drug use, dietary behaviors, hygiene, mental health, protective factors, violence and unintentional injuries, and attitudes towards sexual and reproductive health and HIV related knowledge. Surprisingly, 20% of students had never heard of HIV/AIDS, and 19.5% had at least one drink containing alcohol in the month proceeding the survey. Almost 40% of students felt sad or hopeless in the last 12 months to the extent of being unable to carry out their usual activities. In relation to violence, 40% of students had been physically attacked by a parent, and 25% by a teacher.
*WHO Country Report. Lebanon, 2005.
4.7 School-based Oral Health Program In June 2006, the MOPH adopted a five-year strategic plan
after a large consultation process that included the MOE, the two Orders of Dentists and the NGO sector, with the participation of WHO and UNICEF. In 2006, the program focused on developing education materials and training of the MOE health educators. A dental check-up was performed by 560 dentists on 195,633 students in public schools. Results were alarming: 82% had gum and dental problems and 76% needed treatment. In 2007, workshops were organized to train health educators on teaching oral hygiene and tooth brushing techniques. A second oral check-up campaign was launched targeting 166,691 public school students, and confirmed previous observations. The results of the two campaigns were discussed with MOE and school directors, and communicated to the parents. More than 100,000 tooth brushes and toothpastes were distributed. In 2008, the program launched the �Fluor rinse Campaign� that targeted 30,000 students of the elementary grade-four classes in public schools. Children mouthwashed on a daily basis with fluoride solution, under supervision. This campaign will be repeated targeting the same cohort of students for 3 consecutive years.
4.8 Non Communicable Disease Program
The MOPH has been facing the increasing incidence of NCD, mainly through secondary prevention activities provided through the national PHC network. Patients with chronic diseases such as diabetes

50and hypertension, are regularly followed up and provided with needed essential drugs. Expensive drugs are also dispensed for free by the MOPH drug warehouse to patients suffering from cancer, renal failure, epilepsy, multiple sclerosis, mental illness and other chronic conditions. The program aims at establishing a link with the MOPH coverage of needed episodic hospitalization of the chronically ill that include diabetic complications, heart attacks, strokes, dialysis and others, in order to ensure a continuum of care.
Nevertheless, the MOPH has to intervene in primary prevention as well, since this remains the most cost-effective control measure. Facing financial constraints as well as the scarcity of qualified human resources, the MOPH decided to launch a common NCD preventive program, knowing that most chronic illnesses share the same risk factors related to lifestyles and eating habits, and respond therefore to the same preventive measures and awareness campaigns.
Unfortunately, all efforts put and the progress made in treating the chronically ill at the PHC level as well as secondary and tertiary care, contrast with modest achievements on the promotion and prevention fronts. The MOPH and its partners are lagging behind the powerful commercial and media forces promoting unhealthy life style and advertising for harmful products. On the other hand, even though Lebanon had signed and ratified the Framework Convention on Tobacco Control (FCTC), little progress was made at the legislative level, and any serious policy measure has yet to be taken.
5-HUMAN RESOURCES FOR HEALTH
As an almost universal problem of the developing world, regional discrepancies and imbalance in human resources still exist in Lebanon. The most meaningful component of this imbalance has been the surplus of physicians, accompanied by a shortage of nurses. By 2007, physicians registered in the two existing Orders represented more than 3 per 1000 inhabitants. In that same year, all categories of nurses did not reach two per 1000 inhabitants7. These figures are striking for their impact on both cost and quality of care. However,
7 Order of Nurses, 2007

51having a look on the licenses delivered by the MOPH to medical and paramedical professionals, we can satisfactorily notice that while all professions are keeping almost a constant trend, all categories of nurses� licenses have been increasing during this decade (table II-14). However, one in five of the nurses who receive a bachelor of science in nursing migrates out of Lebanon within one or two years of graduation8.
5.1 Physicians
During the 1990s, the number of physicians grew by 8.3% per year, in comparison with a population growth rate of 1.6%9. The number of registered physicians had exceeded 11,000 in 2007, of which more than 70% were registered as specialists. The physician-to-population ratio is currently 6.5 per thousand in Beirut, and less than 1.8 per thousand in the Bekaa. The ratio of hospital beds per physician is 1.3, while this ratio is between 2 and 3 in most countries, and 2.3 globally10.
Medical graduates have to pass the Colloquium exam carried out by the Ministry of Education (MOE) in order to get the MOPH license to practice. Medical practice is not allowed before registration in one of the two existing Orders of Physicians. Currently, 9,900 physicians are registered in the Order of Physicians of Lebanon in Beirut, and 1,286 in the Order of Physicians of the North.
The proportion of physicians registered in Lebanon who are practicing abroad is unknown and was estimated by the National Provider Survey as falling somewhere between 15 and 20%11.
8 El-Jardali F., et al. Migration of Lebanese nurses: A questionnaire survey and secondary data analysis. International Journal of Nursing Studies. October 2008, 45 (10), pp. 1490-1500.
9Daher, M; Husseini, H; Kasparian, R; Kasparian, C. 1998. La Démographie Médicale au Liban: pléthore, féminisation et rajeunissement. Journal Médical Libanais, 46 (1): 43-46,
10World Health Organization. World Health Statistics 2008. 11 Ammar, W., 2003. Health System and Reform in Lebanon. Beirut: WHO

52Fig II-2a: Physicians Registered Fig II-2b: Physicians Registered
from 1950 through 2000 from 2001 through 2007
Source: Lebanese Order of Physicians (LOP)
In principle, physicians residing in North Lebanon register in the Order of the North, and those residing in all other regions, register in the Order of Lebanon located in Beirut. However, this is not a rigid rule, and political alliances may influence some physicians� decisions in this respect. Electoral purposes may lie behind the registration of physicians from the North in the politically more influential Order of Beirut, whereas the reverse may be explained by the lower enrollment fee in the Order of the North.
Fellowships and grants to study medicine abroad especially in the former Soviet Union and Arab countries have contributed to the tremendous rise in the number of physicians. Besides its effect on over supply, the multiplicity of graduating countries has an impact on quality of care. It is particularly hard to reach a consensus on common standards and clinical protocols among physicians with wide educational background variations.
0
1000
2000
4000
5000
6000
7000
8000
9000
10000
200019901980197019601950
3000
8000
9000
10000
11000
12000
13000
14000
15000
16000
18000
2001 2002 2003 2004 2005 2006 2007
17000

53
Tabl
e II
-14:
Dist
ribu
tion
of p
hysic
ians
by
mou
hafa
zat a
nd sp
ecia
lty (2
007)
Mou
hafa
zat
Surg
ical
Sp
ecia
lties
M
edic
al
Spec
ialti
es
Pedi
atri
cs
Gen
eral
pra
ctic
e To
tal
spec
ialti
es
Tota
l (%
)
Bei
rut
801
944
278
767
2,790
2,632
(23.
53)
Mou
nt L
eban
on
1,504
1,550
445
1,454
4,953
4,804
(42.
95)
Nor
th L
eban
on
400
379
238
452
1,469
1,494
(13.
36)
Sout
h Le
bano
n 517
397
175
319
1,408
1,382
(12.
35)
Bek
aa
317
218
78274
887
874
(7.8
1)To
tal
3,539
3,488
1,214
3,266
11,507
11,186
(1
00.0
0)So
urce
: Ord
ers o
f Phy
sici
ans.
Tabl
e II
-15:
Phy
sicia
ns r
egis
tere
d in
the
Leba
nese
Ord
er o
f Phy
sicia
ns b
y co
untr
y of
gra
duat
ion
(200
7)
G
ener
al P
ract
ition
ers
Sp
ecia
lists
G
radu
atio
n C
ount
ry /
Reg
ion
n %
n %
Le
bano
n
3945
40
.0
20
10
27.7
Ea
ster
n Eu
rope
3085
31
.4
19
52
26.9
W
este
rn E
urop
e
1405
14
.3
22
21
30.6
A
rab
Cou
ntrie
s
1103
11
.2
27
5 3.
8 N
orth
Am
eric
a
59
0.6
69
2 9.
5 O
ther
s
243
2.5
10
5 1.
5 To
tal
9840
10
0.0
72
55
100.
0 So
urce
: Leb
anes
e O
rder
of P
hysi
cian
s (LO
P).

54
5.2 Dentists
The Order of Dentists was established in 1949, but was split in 1966 into two Orders, similar to the two Orders of Physicians. There are currently 4366 dentists registered in the Order of Dentists of Lebanon, of whom 3708 are currently practicing in the country, and another 615 registered in the Order of Dentists of North Lebanon.
Table II-16: Distribution of dentists by Mohafazat in 1994, 2000 and 2007 and ratio per 100,000 population (2007)
1994 2000 2007 n (%) n (%) n (%) %000
Beirut 828 (28.7) 1045 (25.7) 966 (21.2) 24.74 Mount Lebanon 1331 (46.2) 1798 (44.3) 2018 (44.5) 13.44 North Lebanon 270 (9.4) 450 (11.1) 634 (13.9) 8.25 South Lebanon 233 (8.1) 347 (8.5) 633 (13.9) 10.16 Bekaa 43 (1.5) 233 (5.7) 297 (6.5) 6.30 Unspecified 178 (6.2) 188 (4.6) 0 (0) Total 2883 (100) 4061 (100) 4548 (100) 12.11
Source: Orders of Dentists.
In 1994, Doughan and Doumit12, reported a high concentration of dentists in Beirut and Mount Lebanon. Regional discrepancies still prevailed in 2007 as 86% of the specialty dentists (surgery, restorative and aesthetic dentistry,�) are concentrated in Beirut and Mount Lebanon13. This reflects the financial preference of dentists for the more affluent regions of the country, especially that dental care is not as extensively covered by insurance agencies as medical care.
Graduates from universities in Lebanon made up 45% of the pool of dentists, and 58% of the specialized dentists in 2007. The Saint Joseph University and the Lebanese University graduate each some 40 new dentists yearly, while graduates from abroad, mainly Eastern Europe, France and Arab countries, return to Lebanon at the rate of almost 150 every year.
12Doughan, B; Doumit, M. Oral Health in Lebanon: A Situation Analysis, 1994.
13Order of Dentists 2008 report.

55Dentists face a similar situation as physicians in terms of
oversupply and multiplicity of educational backgrounds.
Table II-17: Distribution of specialized dentists by country of specialty (2007)
n %
Lebanon 377 57.7 Romania 45 6.9 Ex-USSR 104 15.9 France 32 4.9 Syria 21 3.2 Egypt 9 1.4 Bulgaria 7 1.0 Other countries 59 9.0 Total 654 100.0 Source Orders of Dentists, 2007.
5.3 Pharmacists
The current number of registered pharmacists at the order of Pharmacists is 4667 of whom 3562 are in practice. The total number of pharmacies licensed by MOPH has reached 1940 by 2007. Numbers of pharmacists and pharmacies have grown from 1995 to 2000 by 46% and 64% respectively, while the growth from 2001 till 2006 was only 23% for pharmacists and 24% for pharmacies.
Table II-18: Evolution of the number of licensed pharmacists and pharmacies (2001-2007)
2000 2001 2002 2003 2004 2005 2006 2007 Pharmacists 3414 3626 3492 3707 3950 4227 4446 4667
Pharmacies 1445 1512 1575 1629 1700 1778 1868 1940
Source: Order of Pharmacists.
Pharmacies are better distributed by mohafazat than medical and dental clinics as a result of regulations� enforcement. The 1994 Pharmacy Practice Law specifies a minimum distance between pharmacies to be respected in providing new licenses. This distance is 200 meters in crowded cities and 300 meters in rural areas. This should have more significant impact on the distribution within rather than between districts and mohafazat. The less meaningful discrepancies in pharmacies distribution in comparison to other health facilities

56provides a typical example of the impact of supply regulation on the equitable distribution of health services.
Table II-19: Pharmacists and pharmacies per 10,000 inhabitants and by mouhafazat (2007)
Pharmacies* Drugstores* n (%) %oo n
Beirut 207 (10.7) 5.3 4 Mount Lebanon 896 (46.2) 5.97 12 North Lebanon 297 (15.3) 3.86 2 South Lebanon 201 (10.4) 5.01 1 Nabatieh 114 ( 5.8) 5.14 0 Bekaa 225 (11.6) 4.77 1 Total 1940 (100.0) 5.17 20
*According to MOPH database, only from 2001 till 2007, drugstores are wholesalers.Source: - Order of Pharmacists (2007). - MOPH Department of Pharmacy (2007).
5.4 Nurses
Traditionally, the shortage of nurses used to result from the unattractive professional status, and the short career life, as many single nurses preferred to quit the profession after getting married. Unsuitable working conditions contributed as well to career instability. Within this context, the creation of the Order of Nurses in 2002 gave a sense of belonging to a body that stands for the nurses rights and safeguards professional standards. The revision of the salary scale in public hospitals under the �Law of Autonomy� led to a better financial status for nurses. The improved competitiveness of governmental hospitals vis-à-vis the private sector in terms of nurses� recruitment, contributed in turn to salary increases also in most private hospitals.
A National Nursing Survey was conducted in 2004, with 6439 respondents between 17 and 64 years of age, with a mean of 31.92 years. Of nurses, 83% were females and 57.8% were single. Compared to a 1994 study14, this survey revealed that a higher percentage of nurses continued to work after marriage. This probably reflects, in addition to the growing financial need, improved working conditions and professional status. Non-Lebanese nurses practicing in Lebanon
14Mansour, A, and Akhatcharian, R. Nursing workforce in Lebanon 1994. Unpublished Study Report.

57accounted for 5.3%. This percentage is probably underestimated due to the fact that most non-Lebanese nurses working without permit declined to complete the survey questionnaire for fear of legal consequences.
Table II-20: Distribution of diplomas among participants in the 2004 National Nursing Survey
Diploma n % No diploma / no formal education 595 10.1 Brevet Pratique (BP)* 961 16.3 Baccalaureate Technique (BT)* 1516 25.8 Technicien superieur (TS)* 994 16.9 Bachelor of Science (BS)** 1426 24.2 Higher degrees** 394 6.7 Total 5886 100
* Vocational education diploma ** University diploma
The survey also showed that 63.6% and 38.6% of respondents have consecutively less than 10 and 5 years of work experience. More than 90% of nurses work in hospitals and 5% in PHC centers, the remaining have an administrative job (1.3%), or an academic career (1.1%), or are working in schools (0.7%) and nurseries (0.3%). The ratio of head nurses to attending nurses, 1 to 5, is comparable to most of the industrialized countries. Of the nurses 93% have full time jobs, 54% earn less than 600,000 LBP (400 USD) per month and those earning more than 1,500,000 LBP (1000 USD) do not exceed 2%.
In 2007, 3233 nurses graduated with a university degree, 2100 nurses with a TS degree (Technique Superieur), 1598 nurses with a BT degree (Baccalaureate Technique) with a total of 6931 nursing personnel15. The ratio of qualified nurses to population is one to 560 compared to one per 1600 persons in 200216.
The nursing education program that the MOPH implemented with the Lebanese University, and the formation of the Order of Nurses
15Société de Recherche Santé et Environnement (SRSE). In collaboration with Amal Mansour and Fouad Ziadeh. Nursing workforce in Lebanon 2004. Unpublished Study Report. 16 Ammar, W., 2003. Health System and Reform in Lebanon. Beirut: WHO

58and Midwifery in 2002, have played an important role in improving the nursing status.
Table II-21: Distribution of nurses by mohafazat (2007)
Mohafazat n % Beirut 665 9.6 Mount Lebanon 2028 29.3 North Lebanon 1535 22.1 South Lebanon 627 9.0 Nabatieh 872 12.6 Bekaa 1204 17.4 Total 6931 100.0
Source: Order of Nurses, 2007
The Faculty of Public Health (FPH) at the Lebanese University (LU), in addition to the BS degree, has designed special master-equivalent degrees to fill certain identified gaps in the paramedical professions. Between the years 2000-2006, a total of 246 such degrees were granted, of whom 41 DESS in intensive care, 35 DESS in operating rooms, 13 DEA in public health, 50 DESS in hospital administration and 106 DESS in community health.
In addition to the FPH at the LU and the already existing nursing schools at AUB, USJ, and Balamand University, more than five additional university nursing schools were established since 2000. Nursing technical institutes are spread all over the country to prepare technical nurses at the BT and TS levels. Other nursing programs exist but are mostly hospital-based.
Table II-22 shows the numbers of nurses and other paramedical personnel who graduated from the Lebanese University between 2000 and 2006. The overall national impact is illustrated in figure II-3 revealing that the category of nurses with university degree is the one that has increased the most.
The ratio of hospital beds to nurses probably exceeded 2 in 2008, which compares well with a ratio ranging from less than 1 to 1.5 beds per nurse in most Western European countries17. As a result of the
17 WHO. World Health Statistics 2008.

59
Fig II-3: Licenses issued by the MOPH for nurses and midwives by category, 1994-2007.
Table II-22: Lebanese University: Public Health Faculty graduates (2000-2006)
00-01 01-02 02-03 03-04 04-05 05-06 Total (%) Nursing 169 187 151 180 222 208 1117 (45.02)
MedicalLaboratory
74 65 63 77 75 67 421 (16.97)
Physiotherapy 39 55 39 42 43 55 273 (11.00)
Midwifery 63 59 34 66 59 45 326 (13.14)
SocialAssistance
21 24 20 49 63 61 238 (9.59)
Orthophony 11 12 9 12 11 11 66 (2.66)
Ergotherapy 10 8 - 8 7 7 40 (1.61)
Total 387 410 316 434 480 454 2481 (100.00)
0
200
400
600
800
1000
1200
1400
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Midw ivesNurses (BT)Nurses (TS, BS)Nurse aids

60
development of the nursing profession hiring of non-registered nurse "auxiliaries" has become quite unjustified in most hospitals.
6- CONCLUSION
Regulation of the supply of human resources could not have a significant impact unless it targets the admission of entrants to universities and technical schools. The most common approach, that proved to be effective in selecting a limited number of students, is the numerus clausus. Restrictive measures of this kind cannot be implemented in Lebanon for two main reasons. First, because it is considered culturally and politically as an unacceptable interference with personal freedom of career choice. Second, because an important number of Lebanese health professionals are yearly graduating from foreign universities, and can hardly be subjected to national control mechanisms. Lebanese Diaspora, that counts more than the number of residence, is particularly out of reach in this regard.
In the absence of an up stream control, down stream measures such as licensing requirements and the colloquium exam have meaningless effect on the supply volume of concerned professionals. Incapable of playing a meaningful role in reducing oversupply, the MOPH was only able to focus on addressing shortages, particularly that of nurses. MOPH interventions in financing university education programs, in conducting training, in creating and supporting the Nurses� Order and in improving their financial and work conditions, had a remarkable impact on promoting the nursing profession. Fig II-4 illustrates how in a liberal health system, where government control is ineffective, oversupply can only be partially adjusted by market mechanisms (the slightly declining medical practitioners curve), whereas the regulation authority may intervene and have a significant impact by filling specific gaps (the mounting curve of nurses production).
Finally, As a result, Lebanon�s indicators related to health care provision are comparable to developed countries. Physicians, pharmacists, dentists and hospital beds ratios to population, are close to those of most OECD countries. However, two striking differences

61prevail: the availability of high-tech equipment is much higher, while despite all efforts, nurses to population ratio remains much lower in Lebanon compared to OECD countries (table II-22).
Fig II-4: Licenses provided to medical practitioners, dentists and nurses 1994-2007
Table II-23: Health Resources compared to Selected OECD countries (2006)
Physicians per 1000
population
Nurses per 1000
population
Pharmacists per 1000
population
Dentists per 1000
population
CT Imaging Scanners
perMillion
MRI Imaging Scanners
perMillion
Hospital Beds per
1000population
Canada 2.1 9.9 0.7 0.6 10.8 4.9 3
UK 2.3 9.2 0.5 0.5 7.0 5 3.7
Spain 3.4 7.4 0.9 0.5 13.3 7.7 2.8
Germany 3.4 9.6 0.6 0.8 15.4 6.6 6.6
France 3.4 7.5 1.1 0.7 7.5 3.2 3.8
Lebanon 2.9 1.8 1.2 1.1 27.0 9.8 3.5
0
200
400
600
800
1000
1200
1400
1600
1800
2000
2200
2400
2600
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Nurses (all categories)
Medical practitioners
Dentists









![FSD3000 Poliisibarometri 2014 · 2020. 7. 10. · 1015 100.0 100.0 9. 2. Muuttujat [BV6] Kunnan kokoluokka Kysymysteksti Kunnan kokoluokka Frekvenssit selite arvo n % v. % Helsinki](https://img.pdfslide.net/doc/110x75/60c80b56ca6ffd47741c8090/fsd3000-poliisibarometri-2014-2020-7-10-1015-1000-1000-9-2-muuttujat-bv6.jpg)



![Breakout by Race / Ethnicity [Weighted] - CCSSE · Total 7,861 100.0 25,667 100.0 1,138 100.0 50,617 100.0 234,634 100.0 74,299 100.0 18,695 100.0 4g. Worked with classmates outside](https://img.pdfslide.net/doc/110x75/5ac86cc17f8b9a6b578c1ca7/breakout-by-race-ethnicity-weighted-7861-1000-25667-1000-1138-1000-50617.jpg)