Embed Size (px)
Citation preview

CHARACTERIZATION OF LYMPHATIC
VESSELS AND LYMPHATIC ENDOTHELIAL CELLS IN TYPE 2 DIABETES MELLITUS
Structural, morphological and molecular analysis
DOCTORAL THESIS for obtaining the academic degree of
Doctor of Philosophy (Ph.D.)
submitted by Monika Hämmerle, MD within the thematic program: Cell communication in health and disease (CCHD)
supervised by Prof. Dr. Dontscho Kerjaschki & Dr. Brigitte Hantusch
Clinical Institute of Pathology Vienna, August 2012

Acknowledgements
First of all, I would like to thank my supervisors Prof. Dontscho Kerjaschki und Dr. Brigitte
Hantusch for giving me the opportunity to do my PhD in the research laboratory of the Clinical
Institute of Pathology and who supported me throughout the years.
I would like to thank my cooperation partners at the Department of Rheumatology, Carl‐Walter
Steiner, for excellent technical assistence in FACS sorting and at the Department of General
Surgery, Dr. Christoph Neumayer, for guaranteeing me that I could use my material as fresh as
possible. Moreover, I would like to thank Dr. Stefan Thurner and especially Dejan Stokic for
helping me with the bioinformatical data analysis.
I thank all my friends and colleagues from the CCHD PhD program, especially my lab mate Tom
without whom the day would not have been so much fun.
I would like to announce a big thank to Bernhard Höfle, who triggered my enthusiasm for
science.
Last but not least, I would like to thank my family and friends for their incessant support, love
and motivation.
Die Wissenschaft, richtig verstanden, heilt den Menschen von seinem Stolz;
denn sie zeigt ihm seine Grenzen.
Albert Schweitzer

I
Summary
Background ‐ Small vessel disease of kidney, nerves, retina and skin, referred to as
microangiopathy, is a major cause of morbidity in type 2 diabetes mellitus (T2DM). While
characteristic changes in blood capillary walls and endothelial dysfunction of blood vessels are
well studied in type 2 diabetes, examination of lymphatic endothelial cells (LECs) and lymphatic
vessels (LVs) is scarcely done. However, complications seen in type 2 diabetes, e.g. increased
risk for infections, wound healing defects and obesity, may be related to lymphatic dysfunction.
Therefore, we aimed at comprehensively analyzing potential morphological and structural
differences of lymphatic endothelial cells and lymphatic vessels in the skin of type 2 diabetes
mellitus patients. Further, we wanted to identify gene expression signatures that are
deregulated in human dermal lymphatic vessels to define mechanisms that are linked with
microvascular complications observed in type 2 diabetes.
Methods – By immunohistochemistry, basement membranes of lymph vessels were analyzed
and blood and lymph vessel densities of diabetic versus normoglycemic skin was evaluated.
Further, we identified signs of inflammation, e.g. macrophage infiltration and TNFα expression.
We compared the gene expression profiles of ex vivo isolated dermal LECs retrieved from
normoglycemic versus type 2 diabetic patients using microarrays and subsequent intensive
bioinformatical analysis. The up‐ or downregulated expression of selected candidate genes was
confirmed by quantitative real‐time PCR and immunofluorescence stainings. Further, we focused
on two differentially regulated genes and performed macrophage adhesion, transmigration and
chemotatic assays as well as siRNA‐mediated knockdown experiments to identify their specific
function in lymphatic endothelial cells.
Results ‐ Neither prominent alterations in extracellular matrix (ECM) protein deposition, nor
morphological BM changes of lymphatic capillaries and collecting LVs were found in the skin of
T2DM patients. This excluded the occurrence of diabetic lymphangiopathy comparable to that of
blood vessels. However, the evaluation of lymph vessel counts revealed a prominent enhanced
lymph vessel density in type 2 diabetic patient's skin. Further, we traced a strong macrophage
infiltration in the dermis of type 2 diabetic patients. These macrophages produced vascular
endothelial growth factors VEGF‐A and VEGF‐C, as well as the pro‐inflammatory cytokine TNFα.

II
Transcriptomal analysis of ex vivo isolated diabetic versus non‐diabetic LECs resulted in a list of
180 differently expressed genes. Consistent with earlier studies, we identified several genes that
have already been linked to genetic susceptibility for type 2 diabetes, including HP, APOD, HHEX,
CD55, ANXA1, LMNA and FABP4. Essentially, we observed multiple changes related to altered
LEC proliferation, adhesion and migration. Further, in line with increased TNFα abundance, we
observed expression changes of CXCL10, VCAM1, CYR61, CXADR, SDC1 and AQP3. TNFα treatment
of cultured LECs led to deregulated expression of selected genes, recapitulating the array results,
indicating that TNFα is one major contributor to diabetes‐specific gene expression signatures in
lymphatic endothelial cells. CXCL10 was confirmed as one important candidate gene only
expressed in chronically inflamed lymphatic vessels, contributing to adhesion and
transmigration of macrophages and possibly intending to resolute the dermal inflammation.
Further, the fatty acid transporter FABP4 was specifically upregulated in LECs and lymphatic
vessels in type 2 diabetes in comparison to blood endothelial cells (BECs) and blood vessels.
FABP4 was shown to regulate LEC proliferation and permeability in vitro, and pointed out the
crucial role of lymphatic vessels in fatty acid transport and metabolism.
Conclusion ‐ These data reveal gene sets highlighting the dramatically altered milieu skin
lymphatic vessels have to cope with during type 2 diabetes mellitus. Further, we discovered that
skin lymphatics show a chronic subacute inflammatory phenotype characterized by macrophage
recruitment and de novo lymphangiogenesis. We provide evidence for a paracrine crosstalk,
mainly via TNFα and CXCL10, fostering macrophage recruitment to LECs as one
pathophysiological process that might contribute to persistent inflammation and consecutively,
aberrant lymphangiogenesis in the skin.

III
Zusammenfassung
Hintergrund ‐ Mikroangiopathie, eine Erkrankung der kleinen Gefäße der Nieren, der Nerven,
der Retina und der Haut, ist eine häufige Komplikation im Verlauf des Typ 2 Diabetes mellitus.
Während diabetische Veränderungen der Blutgefäße in der Haut sehr gut charakterisiert sind,
ist über mögliche morphologische, strukturelle und molekulare Veränderungen von
Lymphgefäßen wenig bekannt. Trotzdem besteht die Vermutung, dass Komplikationen des
Diabetes wie erhöhtes Infektionsrisiko, Wundheilungsstörungen und Veränderungen des
Fettstoffwechsels auch die Folge einer Lymphgefäßdysfunktion sind. Das Ziel dieser Arbeit war
es, potentielle Veränderungen des Lymphgefäßsystems in der Haut auf morphologischer,
zellulärer und molekularer Ebene zu beschreiben. Darüber hinaus war es das Ziel, deregulierte
Genexpressionsmuster zu erkennen, um sie mit den oben genannten Komplikationen in
Verbindung zu bringen.
Methoden – In dieser Arbeit wird eine umfassende immunhistochemische Analyse der
diabetischen Haut, inklusive einer Analyse der Basalmembranen der Gefäße, der Gefäßdichte
und von Zeichen einer Entzündung, präsentiert. Zusätzlich wurde mit Hilfe der Genechip
Microarray‐Technologie und nachfolgender intensiver bioinformatischen Analyse das mRNA‐
Expressionsprofil der diabetischen im Vergleich zu nicht‐diabetischen Lymphendothelzellen, die
ex vivo aus Patientenhaut isoliert wurden, analysiert. Die Expression wichtiger Kandidatengene
wurde mit Hilfe von quantitativen PCR‐Analysen sowie Immunfluoreszenzfärbungen bestätigt.
Im weiteren Verlauf haben wir funktionell auf zwei Gene fokussiert. Es wurden
Makrophagenadhäsions‐, ‐transmigrations und –chemotaxis‐Experimente durchgeführt, um ihre
Rolle in der Interaktion mit Makrophagen zu analysieren. In siRNA‐mediierten knockdown
Studien wurde versucht, die spezifische Funktion dieser Gene in lymphatischen Endothelzellen
herauszufinden.
Ergebnisse ‐ Signifikante Veränderungen der Basalmembranen von, sowie erhöhte Expression
von Extrazellulärmatrixproteinen rund um diabetische Lymphgefäße konnten nicht gefunden
werden, was die Existenz einer sogenannten diabetischen Lymphangiopathie ausschloss.
Dennoch zeigte ein Vergleich der Lymphgefäßdichte von diabetischer und nicht‐diabetischer
Haut eine signifikant erhöhte Dichte der Lymphgefäße beim diabetischen Patienten. Zusätzlich
konnte in der diabetischen Haut eine starke Infiltration mit Makrophagen nachgewiesen

IV
werden. Diese Makrophagen produzierten vaskuläre Wachstumsfaktoren wie VEGF‐A und
VEGF‐C, sowie das pro‐inflammatorische Zytokin TNFα. Der transkriptionelle Vergleich des
mRNA‐Profils von diabetischen und nicht‐diabetischen Lymphendothelzellen führte zur
Identifikation von 180 differentiell regulierten Genen. Neben Genen, die als mögliche
Suszeptibilitätsgene für die Entwicklung des Typ 2 Diabetes gelten, wie z.B. HP, APOD, HHEX,
CD55, ANXA1, LMNA und FABP4, wurden Transkripte gefunden, die mit der Proliferation von
Lymphendothelzellen, sowie mit der Adhäsion und Migration von inflammatorischen Zellen in
Gefäßen assoziiert sind, was mit dem immunhistochemischen Befund korrelierte. Es wurden
besonders prominente Expressionsunterschiede von CXCL10, VCAM1, CYR61, CXADR, SDC1 und
AQP3 detektiert. Diese konnten durch eine Stimulation von Lymphendothelzellen mit TNFα in
vitro spezifisch rekapituliert werden. CXCL10 wurde als ein wichtiges Chemokin identifiziert, das
wahrscheinlich nur im Rahmen einer Entzündung auf dermalen Lymphgefäßen exprimiert wird
und das eine wichtige Rolle bei der Adhäsion und Transmigration von Makrophagen und damit
möglicherweise bei der Auflösung einer lokalen Entzündung spielt. Es war auch eine
Gensignatur von Lipidtransportern in dLECs dereguliert. Darunter war speziell die Expression
von FABP4 nicht nur in diabetischen Lymphendothelzellen und Lymphgefäßen signifikant
erhöht, sondern grundsätzlich spezifisch für Lymph‐ im Vergleich zu Blutendothelzellen. Ein
Einfuss von FABP4 auf das Verhalten von Lymphendothelzellen, wie endotheliale Proliferation
und Permeabilität wurde gezeigt. Die verstärkte Expression von FABP4 in Lymphendothelzellen
hebt damit die essentielle Rolle der Lymphgefäße im Rahmen des Lipidtransports und
Fettsäurestoffwechsels hervor.
Schlussfolgerung ‐ Diese Arbeit beleuchtet die Genexpressionsveränderungen von
Lymphendothelzellen der Haut im Rahmen des Typ 2 Diabetes mellitus und zeigt mit welchen
metabolischen Veränderungen diese zu kämpfen haben. Die erhöhte Lymphgefäßdichte ist mit
einer starken Makrophagendichte assoziiert, und es scheint hier eine enge Kommunikation
zwischen diesen Zellen, vor allem mittels der Chemokine CXCL10 und TNFα stattzufinden.
Umgestellt: Zusammenfassend lässt sich sagen, dass es über einen parakrinen Mechanismus zu
einer vermehrten Rekrutierung von Makrophagen in der diabetischen Haut kommt, was zu
chronischer Entzündung und in der Konsequenz zu vermehrter Lymphangiogenese führt.
Dadurch konnten wir zeigen, dass dermale Lymphkapillaren aktiv an den bekannten
Phänomenen der verzögerten Wundheilung und persistierenden Entzündungen im Typ 2
Diabetes beteiligt sind.

V
Contents
ACKNOWLEDGEMENTS 1
SUMMARY 1
ZUSAMMENFASSUNG 3
CONTENTS 5
LIST OF FIGURES 9
LIST OF TABLES 11
ABBREVIATIONS 12
1. AIMS AND RESEARCH OBJECTIVES 1
2. THE LYMPHATIC VASCULAR SYSTEM 3
2.1 Embryonic lymphatic vascular development 4
2.2 Lymphatic vessel anatomy and structure 8
2.3 Molecular markers for lymphatic endothelial cells 9
2.4 Lymphatic vascular function 14
2.5 Perspective 16
3. TYPE 2 DIABETES MELLITUS 17
3.1 Hereditary factors in T2DM 17
3.2 Insulin action and resistance 18

VI
3.3 Role of adipose tissue in insulin resistance and type 2 diabetes mellitus 18
3.4 Vascular complications in diabetes mellitus 20
3.5 Skin symptoms and clinical signs of T2DM 21
3.6 Diagnosis of T2DM 22
3.7 Therapy of T2DM 23
4. LYMPHATIC VESSELS, TYPE 2 DIABETES MELLITUS AND LIPID METABOLISM 25
4.1 Lymph vessel morphology in T2DM 25
4.2 Lymph vessels and inflammation 26
4.3 Lymph vessels with special emphasis on lipid metabolism 27
5. DNA MICROARRAYS 28
5.1 Advantages and problems of using DNA microarrays 28
5.2 Application of the microarray technique in T2DM research 29
6. MATERIAL AND METHODS 31
6.1 Patients and skin samples 31
6.2 Antibodies 32
6.3 Buffers and solutions 33
6.4 Micropreparation of lymphatic endothelial cells from human skin 35
6.5 Cell staining procedure for subsequent fluorescent activated cell sorting 35
6.6 Fluorescenceactivated cell sorting 36
6.7 RNA isolation 36
6.8 RTPCR and gel electrophoresis 37
6.9 Sample preparation for microarray experiment 37
6.10 Bioinformatical and statistical analysis 38
6.11 Quantitative Realtime PCR 38
6.12 SDSPAGE and Western Blot 39
6.13 Immunohistochemistry and Immunofluorescence 40
6.14 Evaluation of lymph and blood vessel density and counting of macrophages 40

VII
6.15 Tissue fixation and processing for electron microscopy 41
6.16 Primary Human Dermal Endothelial Cell Culturing 41
6.17 siRNA mediated gene knockdown 42
6.18 LEC Proliferation assay 43
6.19 Protein CoImmunoprecipitation (CoIP) 43
6.20 Chromatin immunoprecipitation (ChIP) 43
6.21 TNFα stimulation of LECs 46
6.22 Scratch wounding assay 46
6.23 Enyzmelinked Immunosorbent Assay (ELISA) 46
6.24 Macrophage adhesion assay 47
6.25 Macrophage transmigration experiment 47
6.26 Agarose spot assay 47
6.27 LEC monolayer permeability assay and TEER measurements 48
6.28 Statistical methods and analysis 48
7. RESULTS AND DISCUSSION 49
7.1 Morphological features of diabetic skin 49 7.1.1 Basement membrane morphology of small blood and lymphatic capillaries in diabetic skin 49 7.1.2 Basement membrane morphology of lymphatic collectors in diabetic skin 53 7.1.3 Increased lymphatic vessel density in the skin of T2DM patients 53 7.1.4 Increased macrophage infiltration in diabetic skin 56 7.1.5 Macrophages produce vascular endothelial growth factors 57 7.1.6 Increased TNFα levels in human diabetic skin 59 7.1.7 TNFα production by CD68+ macrophages 60
7.2 Ex vivo isolation of LECs from human skin 62 7.2.1 Quality control of isolated LECs 62
7.3 Bioinformatical analysis of diabetic versus nondiabetic LEC transcriptomes 67 7.3.1 Identification of deregulated pathways and gene functions using Ingenuity Pathway Analysis 70 7.3.2 Verification of LEC specific genes and comparison with other arrays 84 7.3.3 Diabetic LECs exhibited a distinct gene expression profile compared to diabetic BECs 85 7.3.4 Genes linked to altered lipid transport and metabolism, increased oxidative stress and to the pathogenesis of type 2 diabetes mellitus 87 7.3.5 Identification of a gene signature related to wound healing and tissue repair in dLECs 89 7.3.6 Identification of a gene signature related to increased adhesion of inflammatory cells 91 7.3.7 Deregulated genes associated with cellular host defense 93
7.4 TNFαinduced effects on LEC behavior 96 7.4.1 TNFα responsiveness of LEC genes in vitro 96

VIII
7.4.1 Increased migration of LECs upon TNFα stimulation 99 7.4.2 Macrophage adhesion to LECs is increased by TNFα stimulation 99
7.5 CXC motif chemokine 10 (CXCL10) expression and function in LECs 102 7.5.1 CXCL10 is upregulated and secreted by LECs upon TNFα stimulation 102 7.5.2 CXCL10 mediates macrophage adhesion to LECs 103 7.5.3 CXCL10 induces chemotaxis of macrophages 106 7.5.4 CXCL10 enhances LEC‐transmigration of macrophages 108
7.6 Characterization of Fatty acid binding protein 4 (FABP4) expression and function in LECs 110 7.6.1 FABP4 is specifically expressed in lymphatic endothelial cells 111 7.6.2 FABP4 expression could be specifically knocked down in LECs 112 7.6.3 FABP4 regulates LECs proliferation 113 7.6.4 FABP4 expression increases LEC permeability 114 7.6.5 FABP4 expression regulates PPARγ expression in LECs 114 7.6.6 Possible interactions of FABP4 with PPARγ 115
8. CONCLUSIONS AND FUTURE PERSPECTIVES 118
REFERENCES 124
CURRICULUM VITAE 144

IX
List of Figures Figure 1: Growth of lymphatic vessels in the mammalian embryo: Injection model of
Sabin. 4
Figure 2: Development of the vascular systems. 5
Figure 3: Pathways of how glucotoxicity contributes to diabetic complications in blood vessels.
20
Figure 4: Confirmation of LEC purity used for cell culture experiments. 42
Figure 5: Graphical depiction of the human FABP4 promotor. 45
Figure 6: BM morphology of blood and lymphatic capillaries in human diabetic skin. 50
Figure 7: Laminin expression of diabetic and non‐diabetic LVs and BVs. 51
Figure 8: Collagen IV expression of diabetic and non‐diabetic LVs and BVs. 52
Figure 9: Ultrastructural analysis of LVs. 52
Figure 10: Lymphatic collectors in diabetic skin do not show any morphological changes. 53
Figure 11: LV and BV density in diabetic versus normoglycemic skin. 55
Figure 12: Macrophage infiltration in normoglycemic versus diabetic human skin. 56
Figure 13: VEGF‐C and VEGF‐A expression of infiltratin skin macrophages. 57
Figure 14: Quantitative analysis of VEGF‐C and VEGF‐A production by infiltrating skin
macrophages.
58
Figure 15: TNFα expression in skin. 59
Figure 16: Production of TNFα by macrophages. 60
Figure 17: Fluorescent activated cell sorting of ex vivo isolated LECs and BECs. 63
Figure 18: Exclusion of leukocyte contaminations. 63
Figure 19: Quality control of isolated LECs. 64
Figure 20: Amplification check of RNA isolated from dLECs. 65
Figure 21: Amplification check of RNA isolated from ndLECs. 66
Figure 22: Normalization of microarray chip data. 67
Figure 23: Bioinformatical analysis using Student's t‐test and RVM. 67
Figure 24: Hierarchical cluster analysis. 69
Figure 25: Pathway analysis using IPA. 71
Figure 26: Deregulated cellular functions in dLECs. 71
Figure 27: Confirmation of FABP4, APOD and NOX4 by realtime PCR and 88

X
immunofluorescence.
Figure 28: Confirmation of AQP3, MMP2 and CYR61 expression by realtime PCR and immunofluorescence.
90
Figure 29: Confirmation of VCAM‐1, CXCL10, CXADR and SDC1 expression by realtime PCR and immunofluorescence.
92
Figure 30: Upregulation of CXCL10, VCAM‐1 and CYR61 gene expression of cultured LECs by TNFα stimulation.
97
Figure 31: Downregulation of CXADR, SDC1 and AQP3 gene expression of cultured LECs by TNFα stimulation.
97
Figure 32: Downregulation of FABP4, GALNTL2 and APOD gene expression of cultured LECs by TNFα stimulation.
98
Figure 33: No change of MMP2 and NOX4 gene expression of cultured LECs by TNFα stimulation.
98
Figure 34: Increased migration of LECs after TNFα stimulation. 100
Figure 35: Adhesion of macrophages to primary LECs in vitro. 101
Figure 36: Expression and secretion of CXCL10 in LECs upon TNFα stimulation. 103
Figure 37: CXCL10 is responsible for macrophage adhesion to lymphatic endothelial monolayer.
104
Figure 38: VCAM‐1 is dispensable for macrophage adhesion to lymphatic endothelial monolayer.
105
Figure 39: Secreted CXCL10 is responsible for chemotaxis of macrophages. 107
Figure 40: CXCL10 confers macrophage transmigration. 108
Figure 41: FABP4 is specifically expressed in LECs compared to BECs. 111
Figure 42: siRNA‐mediated knockdown of FABP4 in LECs. 112
Figure 43: FABP4 regulates LEC proliferation. 113
Figure 44: FABP4 expression is not upregulated by lymphangiogenic factors. 113
Figure 45: FABP4 regulates permeability of LEC monolayers. 114
Figure 46: FABP4 regulates PPARγ expression. 115
Figure 47: Co‐Immunoprecipitations of FABP4 and PPARγ. 116
Figure 48: Chromatin immunoprecipitations of PPARγ. 116
Figure 49: Importance of lymphatic vessels in type 2 diabetic skin and the attempt of establish a model showing their contribution, involvement and alterations in the skin of type 2 diabetic patients.
122

XI
List of Tables
Table 1: Structural differences of blood capillaries, lymphatic capillaris and collecting LVs
9
Table 2: Lymphatic specific genes and their knockouts. 13
Table 3: Clinical data of selected diabetic patients and normoglycemic controls. 32
Table 4: Primary antibodies 33
Table 5: Secondary antibodies 33
Table 6: Primers used for RT‐PCR. 37
Table 7: Taqman gene expression assays used for quantitative real‐time PCR. 39
Table 8: Primers used for qPCR to check binding of PPARγ to FABP4 promotor region. 45
Table 9: Genes associated with most deregulated pathways as evaluated by IPA analysis. 72
Table 10: Genes assciated with most deregulated functions as evaluated by IPA analysis. 73
Table 11: Transcript levels of deregulated candidate genes functionally clustered in (A) Inflammatory Response, (B) LEC Adhesion and Migration, (C) LEC growth and Lymphangiogenesis, and (D) Small Molecule Biochemistry.
78
Table 12: Transcript levels of LEC specific genes. No significant differences could be seen for LEC‐specific genes between diabetic LECs (dLECs) and non‐diabetic LECs (ndLECs).
85
Table 13: Gene overlap of diabetic LECs (dLECs) and diabetic BECs (dBECs) 86
Table 14: Transcript levels of deregulated genes already associated with type 2 diabetes. 88
Table 15: Transcript levels of genes associated with wound healing and tissue repair. 90
Table 16: Transcript levels of genes linked to increased adhesion of inflammatory cells. 91
Table 17: Transcript levels of genes associated with cellular host defense. 95

XII
Abbreviations ANGPT2 Angiopoietin 2 AQP3 Aquaporin 3 APC(s) Antigen presenting cell(s) APOD Apolipoprotein d BEC(s) Blood endothelial cell(s) BM Basement membrane BMI Body mass index BV(s) Blood vessel(s) ChIP Chromatin immunoprecipitation CLEC‐2 C‐type lectin‐like receptor 2 CLEVER‐1 Common lymphatic endothelial and vascular endothelial receptor‐1 Co‐IP Co‐immunoprecipitation CRP C‐reactive protein COUP‐TF II COUP transcription factor 2 CXADR Coxsackie and adenovirus receptor CXCL10 Chemokine (C‐X‐C motif) ligand 10 CYR61 Cysteine rich, angiogenic inducer, 61 DARC Duffy antigen/chemokine receptor DAVID Database for Annotation, Visualization and Integrated Discovery DC(s) Dendritic cell(s) ddH2O Double destilled water dLEC(s) Diabetic lymphatic endothelial cell(s) DM Diabetes mellitus EC(s) Endothelial cell(s) ECM Extracellular matrix ER Endoplasmatic reticulum FABP(s) Fatty acid binding protein(s) FACS Fluorescence activated cell sorting FFAs Free fatty acids FITC Fluorescein isothiocyanate FOXC2 Forkhead box protein C2 FPG Fasting plasma glucose GLUT‐4 Glucose transporter type 4 HA Hyaluronic acid HDMEC(s) Human dermal microvascular endothelial cell(s) HUVEC(s) Human umbilical venous endothelial cell(s) ICAM‐1 Interendothelial cell adhesion molecule 1 IFG Impaired fasting glucose IGT Impaired glucose tolerance IL Interleukin IR Insulin resistance IRS Insulin receptor substrate LEC(s) Lymphatic endothelial cell(s) LN(s) Lymph node(s)

XIII
LV(s) Lymph vessel(s) LYVE‐1 Lymphatic vessel endothelial hyaluronan receptor 1 MMP2 Matrix metalloproteinase 2 ndLEC(s) Non‐diabetic lymphatic endothelial cell(s) NEFA(s) Non‐esterified fatty acid(s) nFκB Nuclear factor 'kappa‐light‐chain‐enhancer' of activated B‐cells NO Nitric oxide NOX4 NADPH oxidase 4 NRP2 Neuropilin 2 OGTT Oral glucose tolerance test PAI‐1 Plasminogen activator inhibitor‐1 PAL‐E Pathologische anatomie Leiden‐endothelium PAS Periodic acid‐Schiff PI3K Phosphoinositide 3‐kinase PKC Phosphokinase C PLC2 Phospholipase C gamma 2 PPAR Peroxisome proliferator‐activated receptor gamma PROX‐1 Prospero homeobox protein 1 RMA Robust multi‐array average ROS Reactive oxygen species RVM Relative variance method SDC1 Syndecan 1 SLC Secondary lymphoid tissue chemokine SLP76 SH2 domain‐containing leukocyte protein of 76 kDa SMC(s) Smooth muscle cell(s) SNP(s) Single‐nucleotide polymorphism(s) SOCS Suppressor of cytokine signaling SOX18 SRY (sex determining region Y)‐box 18 SYK Tyrosine kinase SYK T1DM Type 1 diabetes mellitus T2DM Type 2 diabetes mellitus TEER Transendothelial electric resistance TLR4 Toll‐like receptor 4 TNFα Tumor necrosis factor alpha TNFβ Tumor necrosis factor beta VCAM‐1 Vascular cell adhesion molecule 1 VE‐cadherin Vascular endothelial cadherin VEGF Vascular endothelial growth factor VEGFR Vascular endothelial growth factor receptor vWF Von Willebrand factor

1
1. Aims and Research Objectives
The number of patients suffering from type 2 diabetes mellitus (T2DM) is increasing constantly.
Impairment of wound healing and higher frequence of skin infections are common
complications seen in T2DM patients. These symptoms widely rely on pathological changes of
big and small blood vessels which is called macro‐ and microangiopathy, respectively
(Stehouwer and Schaper, 1996). While endothelial dysfunction of blood vessels (BVs) is a well‐
studied situation in T2DM, research on pathological changes of lymphatic vessels (LVs) has
rarely been done. Complications seen in T2DM seem to be not only caused by BV dysfunction. It
was hypothesized that LVs additionally account for these complications, because LV dysfunction
leads to wound healing defects (Saaristo et al., 2006), local inflammation (Rockson, 2001) and
obesity (Harvey et al., 2005). These are conditions often associated with the diagnosis of T2DM.
However, almost nothing is known about potential morphological, structural and functional
changes of lymphatic endothelial cells (LECs) and LVs in T2DM.
The aim of this thesis project was to perform a comprehensive illustration of the morphological,
structural and molecular changes of LVs and LECs in the skin of T2DM patients. To gain insight
into how T2DM alters the lymphatic vasculature and to elucidate functional implications of LVs
in the pathogenesis of the disease, three major research objectives were addressed:
1) Trace potential structural and morphological changes of LVs in the skin of T2DM patients,
including basement membrane changes, vessel density and signs of inflammation.
2) Perform an ex vivo transcriptomal comparison of diabetic versus nondiabetic LECs
isolated from the skin of four type 2 diabetic and four normoglycemic patients.
3) Identification of deregulated functional gene expression patterns of diabetic LECs and
confirmation of association with the pathogenesis of T2DM by in vitro cell culture assays.
The first issue was addressed by extensive histochemical and electron microscopy analyses to
trace morphological alterations of LVs in T2DM, such as altered composition and thickness of
basement membranes, LV shape or dilation, and changes of vacuolisations or organelles in LECs.
Further, we determined the number of BVs and LVs in the skin of T2DM compared to

2
normoglycemic patients and analyzed whether these morphological differences were associated
with signs of inflammation, e.g. immune cell infiltration.
Secondly, in order to discover cellular processes affected in LVs by T2DM, we performed
microarray analyses of ex vivo isolated LECs from diabetic versus non‐diabetic human skin and
compared their transcriptomal profiles. Extensive bioinformatical pathway analysis and
literature search identified gene expression signatures linking LEC biology with T2DM. These
gene clusters contained well known factors as well as gene candidates that were novel in this
context, and they highlighted the role of LECs in processes related to 'inflammation', 'lipid
metabolism' and 'wound healing' as well as 'lymphangiogenesis'.
Thirdly, strong deregulated candidate genes were selected and confirmed by quantitative real‐
time PCR and immunofluorescent stainings on human diabetic and normoglycemic skin. Among
these, C‐X‐C motif chemokine 10 (CXCL10) and fatty acid binding protein 4 (FABP4), were
selected for further functional characterization. CXCL10 was shown to be a chemotactic factor
for macrophages, contributing to the quite uncharted knowledge about the interaction between
lymphatic endothelium and macrophages. Further, the involvement of FABP4 expression in LEC
proliferation and endothelial monolayer permeability was analyzed.
Conclusively, a comprehensive morphological and molecular characterization of LECs and LVs in
the skin of diabetic versus normoglycemic patients is presented and is, to the thesis author’s
knowledge, the first of this kind. The data implicate that lymphatic vessels play a significant
active role in the skin alterations of type 2 diabetes. It is hoped that by identifying patterns of
dLEC gene expressions, new therapeutic targets for this upcoming worldwide epidemic will
become available.

3
2. The lymphatic vascular system
The lymphatic vascular system represents a network of blind‐ended lymph capillaries and
lymphatic collectors which drain the interstitial fluid and transport it back to the blood
vasculature, thereby maintaining tissue fluid homeostasis. Besides, lymphatic vessels are
important regulators of immune cell trafficking and absorption of dietary fats. The existence of
the lymphatic vascular system is indispensable for life and lymphatic dysfunction in individuals
leads to chronic edema and impaired immune response (Tammela and Alitalo, 2010; Alitalo
2011). The lymphatic vasculature was first described by Gaspare Aselli (Aselli, 1627). In 1902,
Florence Sabin proposed a model of lymphatic vasculature development (Sabin, 1902). She
injected ink into pig embryos and showed that lymphatic endothelial cells (LECs) bud from veins
and form primary lymphatic sacs near the junction of the subclavian and anterior cardinal vein.
From these primary lymphatic sacs, LECs form a primitive lymphatic vessel (LV) system by
endothelial sprouting (see Figure 1) surrounding tissues and organs. The thoracic duct, the main
deliverer of lymph fluid, develops from the cisterna chyli, a dilated sac at the lower end of the
thoracic duct, and remains as a final connection to the blood circulation (van der Putte, 1975).
The Sabin model suggests that the LV system arises from the blood vasculature. In 1910, an
alternative model was proposed by Huntington and McClure (1910) who claimed that the
primary lymph sacs are built in the mesenchyme, and only later venous connections are formed.
At least, this theory is true in birds (Schneider et al., 1999).
Until a few years ago the differentiation between blood vessels (BVs) and LVs within tissues was
merely possible according to morphological and histological criteria, e.g. thinner walls of
lymphatics, no basement membranes (BM) and lack of pericytes. However, uncertainty
remained about distinguishing blood endothelial cells (BECs) from LECs. Especially in the last 10
to 20 years progress in this field accelerated dramatically because of the identification of
lymphatic specific markers like vascular endothelial growth factor receptor 3 (VEGFR3,
Kaipainen et al., 1995), Prospero homeobox protein 1 (PROX1, Wigle and Oliver, 1999),
lymphatic vessel endothelial hyaluronan receptor 1 (LYVE1, Banerji et al., 1999) and
podoplanin (Breiteneder‐Geleff et al., 1999). Along with the discovery of these lymphatic specific

4
markers, it became possible to sort and cultivate primary LECs and BECs in vitro. Still, only few
specific markers for LECs are available and most endothelial cell (EC) markers are expressed on
both, BVs and LVs. This affirms the close structural and developmental relationship between the
two vessel systems.
2.1 Embryonic lymphatic vascular development
Due to the importance of the lymphatic vasculature in physiologic and pathological condition,
the development of LVs has been extensively studied. Embryonic blood vessels originate from
mesodermal cells which give rise to hemangioblasts and angioblasts, the precursor cells of all
endothelial cells (ECs; Figure 2 A). Afterwards, angiogenesis occurs that includes formation and
remodeling of new vessels by endothelial sprouting and splitting. LVs originate from the venous
vascular system. They start to develop in the sixth to seventh embryonic week in humans and at
embryonic day (E) 9.0‐9.5 in mice (Tammela and Alitalo, 2010; Oliver, 2004). Oliver (2004) and
colleagues (Oliver and Srinivasan, 2010) suggested a four stage model of the lymphatic
vasculature development: LEC competence, LEC commitment, LEC specification and LV
differentiation and maturation (Figure 2 B). During these steps certain genes are specifically up‐
and downregulated in LECs, each of them important for these distinct stages of development.
Lymphatic endothelial cell competence and commitment
In order to gain a certain competence, cells become able to respond to an initial inducing signal
(Grainger, 1992). The key step for development of LECs is that venous ECs become responsive to
a lymphatic‐inducing signal. Concerning the developmental competence for embryonic veins, it
is believed that the expression of COUP transcription factor 2 (COUPTF II) is important for
development of the venous vascular system by inhibiting Notch‐signaling, which is required for
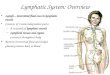
Figure 1: Growth of lymphatic vessels in the mammalian embryo: Injection model of Sabin(Sabin, 1902). Lymphatic ducts growing in the three directions (a) and building of lymphatic sacs(b) from which EC are sprouting to form a primary lymphatic capillary system (c).

5
arterial cell differentiation (You et al., 2005). Further, COUPTF II might be involved in the
repression of lymphatic key transcription factor PROX1 to prevent too early LEC differentiation
(Oliver and Srinivasan, 2010). Earlier, it was suggested that the expression of LYVE1 by some
endothelial cells lining the anterior cardinal vein at E 9.0‐9.5 is important for gaining lymphatic
competence (Jurisic and Detmar, 2009; Cueni and Detmar, 2008; Maby‐El Hajjami and Petrova,
2008). However, the lack of a specific lymphatic phenotype in Lyve1 knockout mice voiced the
concern whether it is really crucial for LEC phenotype development (Luong et al., 2009; Gale et
al., 2007).
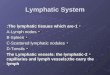
Figure 2: Development of the vascular systems. Scheme of the main steps of blood andlymphatic vascular development starting from the mesodermal angioblasts, which differentiateinto endothelial cells (A). Stepwise development of the lymphatic vascular system (B); modifiedfrom Oliver and Srinivasan (2010).

6
There are speculations that not LYVE1 alone, but another factor is responsible for the initiation
of this important step in venous endothelial cells. This factor was claimed to be SOX18, a
transcription factor which is an upstream regulator of the lymphatic master regulator PROX1.
SOX18 is expressed in a subpopulation of ECs in the anterior cardinal vein and its loss results in
lack of PROX1 expression and termination of lymphatic development. SOX18 might be
transiently required for lymphatic differentiation as it is detected only up to E 14.5 (Francois et
al., 2008). The signal leading to the expression of SOX18 in endothelial cells is still unknown.
However, after gaining lymphatic competence, the cells are able to form a specific cell type
which is dependent on the inducing tissue (Grainger, 1992). This is called lymphatic
commitment and occurs between E 9.0‐10.5 and is characterized by the expression of PROX1.
PROX1 is only expressed in a subpopulation of ECs in the region anterior of the developing
forelimb of mice (Wigle and Oliver, 1999) and it is the most important regulator to confer and
maintain the LEC phenotype (Tammela and Alitalo, 2010).
Lymphatic specification
Lymphatic specification takes place between E 10.5‐11.5. in mice. After formation of LEC
precursor cells, ECs start to bud from the anterior cardinal vein on E 11.0 to build the primary
lymph sacs. This is stimulated by vascular endothelial growth factor C (VEGFC) which is the
most important lymphangiogenic factor (Kukk et al., 1996) and enhancer of lymphatic sprouting
(Saaristo et al., 2002). During lymphatic specification, additionally to LYVE1 and PROX1, other
lymphatic specific markers, e.g. secondary lymphoid chemokine (SLC), podoplanin, VEGFR3 and
Neuropilin 2 (NRP2), are expressed, whereas typical blood vascular markers like CD34 become
downregulated (Kume, 2010; Tammela and Alitalo, 2010; Wigle and Oliver, 1999).
Lymphatic differentiation and maturation
The final step of LEC development is characterized by differentiation and maturation of LECs.
This last stage lasts several days and is a stepwise process (Oliver and Harvey, 2002; Alitalo
2011). LECs are budding and sprouting from the lymph sacs to form a primitive lymphatic
vasculature. Additional lymphatic markers are expressed, e.g. desmoplakin, β‐chemokine
receptor D6 and angiopoietin 2 (ANGPT2) and NFATC1. Shortly before birth, the whole gamut of
lymphatic specific markers that is found in adult LVs is present (Tammela and Alitalo, 2010). A
recent publication claims that besides the well known factors semaphorin3a‐neuropilin‐1
signaling is additionally required for lymph vessel maturation and valve formation (Jurisic et al.
2012).

7
Separation of blood and lymphatic vessels
Important for the formation of an independent and functional LV system is its complete
separation from the blood vasculature. Several genes have been shown to control the separation
process of LVs from BVs: SRC homology 2‐domain‐containing leukocyte protein of 76 kDa (SLP
76) and tyrosine kinase SYK (Abtahian et al., 2003), phospholipase C2 (PLC2) (Ichise et al.,
2009), O‐glycans (Fu et al., 2008) and podoplanin (Uhrin et al., 2010). Slp76/ and Syk/ mice
exhibit vascular malformations, e.g. arteriovenous shunts, abnormal blood‐lymphatic
connections, haemorrhage and blood filled lymphatics (Abtahian et al., 2003). Similar
phenotypes were observed in mice lacking PLC2 (Ichise et al., 2009) or O‐glycans (Fu et al.,
2008). However, the mechanism leading to these misconnections is not absolutely clear. It is
hypothesized that failed platelet aggregation and thrombi formation in the blood‐lymphatic
connector regions are the reason, due to a failure in signaling between C‐type lectin‐like
receptor 2 (CLEC2), SLP76, SYK and podoplanin. CLEC2‐mediated platelet activation is
dependent on the activity of SYK and SLP76 (Suzuki‐Inoue et al., 2006). Moreover it was shown
that podoplanin is a direct interaction partner of CLEC2 expressed on platelets (Suzuki‐Inoue et
al., 2007). Loss of CLEC2‐podoplanin interaction leads to failed platelet activation and
aggregation. Confirmation of this hypothesis was recently provided by Uhrin et al. (2010) and
Bertozzi et al. (2010) who showed that podoplanin is responsible for activation of platelets via
CLEC2, which results in activation of SLP67, and for subsequent closure of blood‐lymphatic
connections. Another important molecule responsible for separation of the two vascular systems
is T‐synthase, a glycosyltransferase, possibly also by regulating podoplanin expression (Fu et al.,
2008).
Development of lymph nodes
Another important feature of lymphatic development is the formation of lymph nodes (LNs)
which begins at around E 12.5 in mice when connective tissue protrudes into lymph sacs.
Incipient clusters of cells were shown to express interleukin‐7‐receptor‐α (IL7Rα) and to be
positive for CD4 and CD45, but negative for CD3 (Mebius, 2003). Via IL7Rα signaling, expression
of lymphotoxin‐α1β2 is induced which is necessary for lymphoid neoangiogenesis. Crucial for
formation of LNs is not only the clustering of CD45+CD4+CD3‐‐cells but also the expression of
adhesion molecules like vascular endothelial growth factor‐1 (VCAM1) which keeps incoming
cells in place for their interaction with hematopoietic and stromal cells. Chemokines expressed
and necessary for the development of LNs are CCL19, CCL21, CXCL12 and CXCL13 (Tammela and
Alitalo, 2010; Mebius, 2003).

8
2.2 Lymphatic vessel anatomy and structure
There are mainly five different compartments of the lymphatic vasculature system: lymphatic
capillaries, lymphatic collectors, lymph nodes, lymphatic trunks and lymphatic ducts, having
diameters ranging between 10µm and 2 mm (Rovenská and Rovenský, 2011; Swartz, 2001). The
LV system starts in the periphery with blind‐ended and thin‐walled lymph capillaries. They have
a diameter of 10‐50µm. The lymph capillaries build a network, the so‐called lymphatic areolas
which finally assemble to bigger collecting LVs. These collecting vessels then assemble to mainly
five main lymphatic trunks: the lumbal, the intestinal, the bronchomediastinal, the subclavian
and the jugular trunk. These trunks in turn pass the lymph into the right and the left thoracic
ducts.
The main LV is the left thoracic duct which drains the lymph fluid from the whole body, except
the upper right body region, and transports it back to the blood vasculature via the left
subclavian vein. The right thoracic duct drains lymph from the upper right body region into the
right subclavian vein (Jeltsch et al., 2003; Fritsch and Kühnel, 2001). Except these two sites
where lymph enters the blood, no connections between the blood and the lymph vascular
system exist. The two vascular systems rather run in parallel and in close proximity to each
other. Along its way, lymph is filtered by passing through LNs where foreign antigens are taken
up and presented by antigen‐presenting cells (APCs) to initiate a specific immune reaction.
Besides, LNs are sites of immigration and reservoir for white blood cells and tumor cells which
gain access to the blood vasculature via high endothelial venules (Swartz and Skobe, 2001).
Lymphatic capillaries, blood capillaries and bigger collecting LVs dispose of eminent structural
differences (summarized in Table 1). In contrast to blood capillaries with narrow and regular
lumina, LVs normally have wide and irregular lumina. The wall of lymphatic capillaries is formed
by a single layer of non‐fenestrated ECs with an incomplete or absent BM (Leak, 1970; Leak and
Burke, 1968, 1966). Small LVs are not covered by pericytes and do not have valves (Alitalo et al.,
2005). Because a BM is mostly absent from lymphatic capillaries, LECs are directly attached to
the extracellular matrix (ECM) with elastic anchoring filaments to prevent collapse of vessels
due to high interstitial pressure. These anchoring filaments, 6‐10nm in diameter, are composed
of emilin‐1 and fibrillin (Danussi et al., 2008; Gerli et al., 2000) and tether the LECs to collagen
fibers (Leak and Burke, 1968, 1966). Lymphatic capillaries show overlapping ECs which build
valve‐like opening structures and hence regulate permeability for interstitial fluid (Trzewik et
al., 2001). The lack of interendothelial tight junctions also contributes to their increased
permeability compared to blood capillaries. Pre‐collecting and collecting lymph vessels are
characterized by a smooth muscle cell (SMC) layer, interendothelial tight junctions and bileaflet
valves (Alitalo et al., 2005). The contractility of the SMCs is important to propulse lymph,
whereas the valves prevent its backflow (Tammela and Alitalo, 2010). The distance between two

9
valves is called the lymphangion (Jeltsch et al., 2003), each of which is a contractile compartment
pumping lymph into the next one. Important proteins for valve formation are integrin α9
(Bazigou et al., 2009) and FOXC2 (Norrmén et al., 2009; Petrova et al., 2004). In functional LVs,
which have separated regularly from BVs, no blood can be found intraluminally.
Blood
capillaries Lymphatic capillaries
Collecting lymphatic vessels
Lumina Regular, narrow Irregular, wide Circular, wide
Endothelial cells Abundant cytoplasm Scant cytoplasm ‐
Overlapping endothelial cells
Absent Present ‐
Valves Absent Absent Present Tight junctions Present Absent Present Cell membrane invaginations and cytoplasmic
vesicles
Scant Abundant ‐
Basement membrane Present Absent Present, but thinnerAnchoring filaments Absent Present Absent
Blood Present Usually absent Usually absentPericytes Present Absent Present
Table 1: Structural differences of blood capillaries, lymphatic capillaris and collecting LVs: based on data from Tammela et al. (2005b), Nathanson (2003), Schmid‐Schönbein (1990) and Gnepp and Green (1979).
2.3 Molecular markers for lymphatic endothelial cells
LECs exhibit a panel of specific markers which are not expressed in BECs. Some EC markers are
expressed on both cell types, e.g. CD31 (PECAM1; platelet and endothelial cell adhesion molecule
1) and vascular endothelial (VE)‐cadherin. Others, like pathologische anatomie Leiden‐
endothelium (PALE) and endoglyx‐1 are only expressed on BECs (Wilting et al., 2002; Christian
et al., 2001). Many studies aimed at characterizing differential gene expression in BECs versus
LECs using transcriptomal and proteomic approaches (Podgrabinska et al., 2002; Hirakawa et
al., 2003; Wick et al., 2007; Roesli et al., 2008), as well as phage display technique (Keller T.M.,
unpublished). Due to the identification of specific lymphatic markers, research in this field
accelerated dramatically in the last 20 years. Table 2 shows a summary of all important
lymphatic specific genes including lymphatic phenotypes in murine gene knockout models. The
four main lymphatic specific markers LYVE1, PROX1, Podoplanin and VEGFR3 are described in
more detail below.

10
Lymphatic vessel endothelial hyaluronan receptor1 (LYVE1)
LYVE1 was discovered as a homologue of the leukocyte hyaluronic acid (HA) receptor CD44
(Banerji et al., 1999), showing a similarity of 51% with CD44. However, LYVE1 expression
differs largely from to the expression of CD44. While CD44 is widely expressed in different cell
types, LYVE1 has a restricted expression pattern in LECs and in some BECs in the papillary
dermis of eczematous and psoriatic skin (Gröger et al., 2007). Like CD44, LYVE1 is a receptor for
HA. Upon stimulation with inflammatory cytokines these receptors are able to bind HA. It was
shown that specific changes in receptor sialylation regulates the functional status and thereby
the binding capacity for HA (Nightingale et al., 2009). Anyhow, LYVE1 is the first lymphatic
specific gene expressed in ECs during lymphatic development. It was suggested that LYVE1
expression is the initial signal for ECs to gain lymphatic competence and to respond to a
lymphatic‐specific signal (Jurisic and Detmar, 2009; Maby‐El Hajjami and Petrova, 2008).
However, Lyve1/ mice fail to exhibit any specific phenotype. They do not show any apparent
defects in embryonic development, lymphangiogenesis and no signs of lymph absorption defects
like chylous ascites or edema (Luong et al., 2009; Gale et al., 2007). The same is true for CD44/
and Lyve1/CD44 double knockout mice. Additionally, they show an unperturbed HA, leukocyte
homeostasis and dendritic cell (DC) migration (Gale et al., 2007). Stimulation of LECs with the
pro‐inflammatory cytokines tumor necrosis factor α (TNFα) and tumor necrosis factor β (TNFβ)
results in an immediate internalization and degradation of LYVE1 expression, which is
completely reversible by withdrawal of cytokines. Nevertheless, uptake of HA or leukocyte
trafficking was not changed in these cells (Johnson et al., 2007), suggesting that some other
receptor compensates for the function of LYVE1 in LECs (Jackson, 2009).
Prosperorelated homeobox 1 (PROX1)
PROX1 is a nuclear transcription factor expressed very early in the development of the
lymphatic vasculature in mice. Around E 9.5, Prox1 is expressed in the subset of ECs which give
rise to the murine LV system (Tammela and Alitalo, 2010). PROX1 was originally cloned by
homology to the Drosophila homeobox gene prospero. It is expressed in a variety of tissues, like
in the central nervous system, lens, heart, liver and pancreas and transiently in skeletal muscle
(Oliver et al., 1993). By generating mice which lack Prox1 expression it could be shown that its
inactivation leads to embryonic lethality. PROX1 is necessary for appropriate lens development
(Liu et al., 2012; Wigle et al., 1999) as well as liver tissue organisation (Sosa‐Pineda et al., 2000).
Moreover, Wigle and Oliver (1999) showed that inactivation of PROX1 completely arrested
lymphatic vascular development by blocking budding and sprouting of LECs. PROX1 is not only
important for LV development but also crucial to establish and maintain the lymphatic
phenotype of ECs. It has been shown that re‐expression of PROX1 in BECs can induce a
lymphatic phenotype of these cells by repressing genes which are associated with the blood

11
vascular phenotype (Hong et al., 2002; Petrova et al., 2002). Conversely, siRNA‐mediated
downregulation of PROX1 in cultured LECs resulted in expression of blood endothelial markers
like CD34 and endoglin, suggesting that LEC identity is reversible (Johnson et al., 2008).
Podoplanin
Podoplanin is a 38kDa protein and was originally discovered in puromycin aminonucleoside
nephrosis (PAN), a rat model of human minimal change nephropathy characterized by a severe
flattening of podocytes and proteinuria at a nephrotic level due to lowered glomerular protein
retention capacity. In PAN, podoplanin expression was downregulated by 70% (Breiteneder‐
Geleff et al., 1997) in the glomeruli and it was shown that podoplanin is necessary for controlling
the shape of podocytes (Matsui et al., 1999), which are the crucial functional filtering cells. By
using inhibitory antibodies to podoplanin, specific features of PAN could be induced (Matsui et
al., 1998). Having observed that endothelial cells were specifically stained with the anti‐
podoplanin antibody, also angiosarcomas were stained and it was shown that podoplanin is a
specific marker for LVs (Breiteneder‐Geleff et al., 1999). Besides its expression in LECs and
podocytes, podoplanin is expressed in various other adult tissues like skeletal muscle, placenta,
lung and heart (Martín‐Villar et al., 2005), myofibroblasts of the breast and salivary glands, in
osteoblasts and mesothelial cells (Ordonez, 2006), alveolar type I cells (Ramirez et al., 2003;
Rishi et al., 1995) and in the basal layer of the human epidermis (Schacht et al., 2005). The first
expression of podoplanin appears around E 10.5‐11.5 in PROX1 positive LEC progenitor cells
(Oliver, 2004). Compared to LYVE1, podoplanin is indispensable for LV development. Schacht et
al. (2003) showed that a homozygous mutation in the podoplanin gene results in lymphatic
pattern defects, whereas BVs appear to be normal. This defect leads to congenital lymphedema,
dilation of LVs and impaired lymph transport. Ramirez et al. (2003) described a podoplanin
knockout mouse which died immediately after birth because of respiratory failure due to a
reduced number of type I alveolar epithelial cells. Furthermore, podoplanin is suggested to be a
ligand for CLEC2, a platelet membrane protein (Suzuki‐Inoue, 2009) and therefore implicated in
the regulation of platelet function. Just recently, Uhrin et al. (2010) confirmed this hypothesis by
providing evidence that podoplanin can induce platelet aggregation and is especially important
for the separation of LVs from BVs during embryonic development. An additional evidence that
podoplanin regulates platelet function is based on the finding that podoplanin‐Fc shedded into
the blood vasculature induced disseminated intravascular coagulation (Cueni et al., 2010a).
Moreover, expression of podoplanin was detected in various epithelial tumors and could be used
as a prognostic factor because of its ability to induce migration, spreading and invasion of tumor
cells (Kapoor, 2012; Fujita and Tagaki, 2012; Cueni et al., 2010b; Wicki and Christofori, 2007;
Wicki et al., 2006).

12
Vascular endothelial growth factor receptor 3 (VEGFR3) and its ligands
VEGFRs belong to the receptor tyrosine kinase superfamily. They are equipped with an
extracellular domain organized into seven immunoglobin‐like folds, a single transmembrane
region, a juxtamembrane domain, a split tyrosine‐kinase domain that is interrupted by a 70‐
amino‐acid kinase insert and a C‐terminal tail (Koch et al., 2011; Olsson et al., 2006). VEGFR3
was one of the first discovered LEC markers. During early development, it is expressed in all ECs,
but it becomes restricted to the lymphatic system during lymphatic vascular development
(Kaipainen et al., 1995), except for BVs in the thyroid, adrenal glands and pancreas (Tammela et
al., 2005a). Additionally, tumor BVs are positive for VEGFR3 (Lymboussaki et al., 1998). Mice
deficient for Vegfr3 die between E 10‐12.5 due to severe cardiovascular failure accompanied by
vascular remodeling defects, pericardial edema and necrosis (Dumont et al., 1998). Two
important ligands for activating and regulating VEGFR activity are VEGF‐C and VEGF‐D
(Tammela and Alitalo, 2010) which both induce migration, proliferation and survival of ECs
(Tammela et al., 2005a). Whereas homozygous deletion of VEGF‐C results in a complete absence
of lymphatic vasculature in mice and heterozygous loss leads to lymphatic hypoplasia
(Karkkainen et al., 2004), loss of VEGF‐D has no effect on lymphatic development and was
suggested to be dispensable (Baldwin et al., 2005). However, blockage of VEGF‐D resulted in
impaired LEC sprouting and migration (Ny et al., 2008). Overexpression of Vegfr3, VegfC or
VegfD stimulated lymphangiogenesis in a plethora of animal models. This mechanism is also
important for tumor progression and LN metastasis. Inhibition of the VegfC/DVegfr3 signaling
reduced LN metastasis in a variety of tumor models (reviewed in Tammela and Alitalo, 2010). A
co‐receptor of VEGFR3 is NRP2 which mediates VEGF‐C‐induced lymphatic sprouting (Xu et al.,
2010). NRP2 is expressed in veins and LVs and may cooperate with VEGFR3 to maximize the
affnity of LECs towards the angiogenic factors VEGF‐C and VEGF‐D. Mice lacking Nrp2 show
selective absence or reduction of small lymphatic capillaries, whereas the collecting vessels
appear to be normal (Yuan et al., 2002).

13
Gene Phenotype Reference Transcription factors
Prox1 No LVs, chylous ascites (‐/‐), adult‐onset
obesity (+/‐) (Wigle and Oliver, 1999; Harvey et al., 2005)
Foxc2
absent valves, abnormal lymphatic patterning, lymphatic dysfunction (‐/‐),
vessel and lymph node hyperplasia (+/‐)
(Kriederman et al., 2003; Petrova et al., 2004; Norrmén et al., 2009)
Sox18 (ragged) lymphedema, chylous ascites (‐/‐) (Pennisi et al., 2000)Adhesion molecules
Integrin α9 chylothorax, lymphedema (‐/‐) (Huang et al., 2000)Growth factors/receptors
Angpt1 hyperplastic LVs (transgenic) (Tammela et al., 2005c)
Angpt2 lymphatic hypoplasia, chylous ascites
(‐/‐) (Gale et al., 2002)
VegfC no LVs (‐/‐), lymphatic hypoplasia, lymphedema, chylous ascites (+/‐) (Karkkainen et al., 2004)
Vegfr3 cardiovascular failure, chylous
pericardium (‐/‐) (Dumont et al., 1998)
Vegfr3 lymphedema (Chy mouse) (Karkkainen et al., 2001)Nrp2 lymphedema, reduction of LVs (‐/‐) (Yuan et al., 2002)
Others
Podoplanin lymphedema, LV dilation, diminished lymphatic transport (‐/‐), blood filled
lymphatics
(Schacht et al., 2003; Uhrin et al., 2010)
Slp76 and Syk abnormal blood‐lymphatic connections
(‐/‐) (Abtahian et al., 2003)
Efnb2 retrograde lymph ow, chylothorax,
absent valves (‐/‐) (Mäkinen et al., 2005)
Lyve1 no lymphatic phenotype (‐/‐) (Gale et al., 2007)
Adrenomedullin lymphedema, abnormal lymphatic
patterning (‐/‐) (Dunworth et al., 2008; Fritz‐
Six et al., 2008) Fiaf dilated intestinal LVs (‐/‐) (Bäckhed et al., 2007)
Table 2: Lymphatic specific genes and phenotypes of their knockouts in mice. PROX‐1, Prospero homeobox protein 1; FOXC2, forkhead box 2; SOX18, sex determining region Y‐related high mobility group box 18; ANGPT1, angiopoietin 1; ANGPT2, angiopoietin 2; VEGF, vascular endothelial growth factor; VEGFR, vascular endothelial growth factor receptor; NRP2, neuropilin 2; SLP‐76, SRC homology 2‐domain‐containing leukocyte protein of 76 kDa; EFNB2, ephrin B2; LYVE‐1, lymphatic vessel endothelial hyaluronan receptor 1; FIAF, fasting‐induced adipose factor; KO, knockout; TG, transgenic.

14
2.4 Lymphatic vascular function
LVs are found throughout the body, except for the brain and avascular or bradytroph tissues like
cornea, cartilage or epidermis. Particularly in the dermis, mesenterium and LNs (Fritsch and
Kühnel, 2001), which are in need of interstitial fluid drainage, the density of lymph vessels is
very high. Adult de novo lymphangiogenesis is normally negligible but may occur during certain
pathological conditions like tissue inflammation, wound healing processes and lymphatic
metastasis (Tammela and Alitalo, 2010; Cueni and Detmar, 2008).
Drainage of interstitial fluid
The most important function of LVs is to drain the interstitial fluid to maintain body fluid
homeostasis. The lymphatic vascular system is a one‐way transport system for fluid, proteins,
lipids and cells forming a milky suspension which is absorbed from the interstitium and
transported back to the blood vasculature. Via valve‐like openings, tissue fluid is taken up and
transported further by active and passive lymphatic pumps and valves (reviewed in
Bridenbaugh et al., 2003). Active lymphatic pumps (intrinsic forces) are only present in larger
collecting vessels and are generated by the contractions of SMCs. The passive lymph pump is
dependent on extrinsic forces produced in the surrounding tissue, e.g. skeletal muscle and
cardiac contraction, respiratory or gastrointestinal peristaltic pressure, and mainly relevant for
lymph capillaries due to the lack of surrounding SMCs. In general, lymph fluid is transported
against a hydrostatic pressure and a protein concentration gradient back to the blood
vasculature mainly by the 'left' thoracic duct. Lymph propulsion in the larger collecting LVs is
dependent on the contraction of SMCs and on systemic forces, like respiration (Schad et al.,
1978), blood pressure (Parsons and McMaster, 1938), exercise (Olszewski et al., 1977) and
massage (Mortimer et al., 1990). The net flow rate of lymph is approximately 100‐500 times less
than blood flow rate (Swartz, 2001). Lymph formation is dependent on interstitial tissue
pressure and tightness of the ECM (reviewed in Swartz, 2001). Fluid movement can be described
by the Starling Equation and is mainly a result of diffusion and filtration and dependent on
hydrostatic and oncotic forces, so called 'Starling forces' (Jackson, 2009). Normally, all forces
together lead to a diffusion or filtration rate of 2 liters of interstitial fluid per day, most of which
is taken up by blind‐ended lymphatic capillaries. Determinants of lymphatic uptake are molecule
size, composition and lipophilicity. It was shown that molecules with sizes up to 1µm can enter
lymphatics freely (Bergqvist et al., 1983). Moreover, cancer drugs enter lymphatic circulation
much faster as in form of colloids than as solutes (Hagiwara et al., 1989) and lipids show higher
uptake rates than hydrophilic substances (Jackson, 1981). Lymphatic and interstitial flow is
further suggested to play important role in tumor antigen presentation and tumor immune
escape (Swartz and Lund, 2012).

15
Uptake and transport of intestinal lipids Implications for lipid metabolism
Lacteals, specialized and blind‐ended lymphatics in the center of each villus are crucial for the
uptake of dietary lipids packed as large lipoprotein particles from the intestine (Schmid‐
Schönbein, 1990). Intestinal lymph is a milky, chylomicron‐rich fluid which is also designated as
'chyle'. The appearance of free chyle in the abdominal or thoracic cavity, chylous ascites or
chylothorax, respectively, is a sign of lymphatic dysfunction (Rockson, 2008). This is seen in
mouse models with mutations in Prox1, Vegfr3, Angpt2 and Sox18. Information about
regulation of uptake of lipids into lacteals is sparse. Additionally, it is not known whether LVs
can actively influence and regulate lipid uptake and transport. Recently, Dixon et al. (2009)
described an in vitro model of the enterocyte‐lacteal interface using differentiated LECs and
Caco‐2 cells. By using a fluorescently labeled fatty acid, it was shown that its transport is
polarized from the enterocytes to the lymphatics through both transcellular and paracellular
pathways. This model highlights not only the importance of lymphatics for lipid uptake but
provides an interesting tool for evaluating drug delivery from the intestine into the circulation.
Interaction with immune cells
LVs serve as the principal conduits for APCs to reach regional LNs and to encounter foreign
antigens. Moreover, they take part in the clearance of leukocytes from sites of inflammation
(Tammela and Alitalo, 2010). An inflammatory condition itself stimulates angiogenesis and
lymphangiogenesis (Alitalo, 2011; Alitalo et al., 2005), e.g. chronic inflammatory diseases like
psoriasis (Halin and Detmar, 2008) or rheumatoid arthritis (Zhang et al., 2007). Pro‐
inflammatory cytokines such as TNFα can induce expression of the lymphangiogenic factor
VEGF‐C, which is mainly produced by macrophages (Baluk et al., 2009, 2005). Thereby, these
cells are able to stimulate lymphangiogenesis (Maruyama et al., 2005). Toll‐like receptor 4
(TLR4) is highly expressed on the surface of LECs and the main mediator of LPS‐induced
activation of NFκB (nuclear factor 'kappa‐light‐chain‐enhancer' of activated B‐cells). Via this
signaling pathway, various chemokines, such as CCL2, CCL5 and CX3CL1 are released, which
contribute to the chemotaxis of macrophages (Kang et al., 2009). On the other hand, migration of
DCs is regulated via CCR7 expressed on DCs and CCL21 expressed on LECs (Förster et al., 2008;
Ohl et al., 2004). In Ccr7‐knockout mice, migration of DCs via LVs to LNs is precluded (Randolph
et al., 2005). Further, pro‐inflammatory cytokines, e.g. TNFα, stimulate the expression of the
leukocyte adhesion molecules inter‐cellular adhesion molecule 1 (ICAM 1), VCAM1 and E‐
selectin on LECs which in turn stimulate DC adhesion and transmigration (Johnson et al., 2007).
CCR10‐positive T‐lymphocytes are especially attracted by a subpopulation of collecting LVs
expressing high levels of CCL27 but low levels of podoplanin (Wick et al., 2008). Moreover,
expression of macrophage‐mannose receptor 1 (MMR1, Marttila‐Ichihara et al. (2008); Irjala et
al. (2001)) and common lymphatic endothelial and vascular endothelial receptor‐1 (CLEVER1,

16
Karikoski et al., 2009; Salmi et al., 2004) regulate lymphocyte traffcking in LVs. However,
detailed knowledge on the specific interaction mechanisms of different immune cell types with
the lymphatic endothelium is still sparse.
Escape route for tumor cells Lymphatic metastasis
Tumors spread either via LVs or BVs to form metastases in regional LNs or distant organs,
respectively. Tumors start to metastasize (i) by induction of peritumoral LV growth and (ii) by
invading the newly formed as well as pre‐existing afferent LVs. Detection of tumor cells within
LNs, especially in the so‐called sentinel LN, is clinically used and important for tumor staging
and therapy (Lyman et al., 2005). However, the mechanism how tumor cells invade into LVs is
poorly understood. Lymphangiogenic factors like VEGFC and VEGFD induce the formation of
new LVs by binding to VEGFR3 (Jeltsch et al., 1997) and were shown to be prominently
upregulated in a variety of tumors (reviewed in Stacker et al., 2002). VEGFC‐induced tumor
lymphangiogenesis and tumor growth could be inhibited by blocking VEGFR3 signaling (He et
al., 2002). Additionally, neutralizing monoclonal antibodies to VEGFC, VEGFD or VEGFR3 were
suffcient to block tumor growth (Stacker et al., 2001). Moreover, chemokines and their
corresponding receptors are suggested to be involved in the interaction of tumor cells with the
lymphatic endothelium, e.g. CCL21 and CCR7 (Shields et al., 2010, 2007). Additionally,
lipoxygenases are implicated in tumor cell invasion of LVs by interendothelial gap formation
(Kerjaschki et al., 2011).
2.5 Perspective
The analysis of LECs from different anatomic sites and pathological situations would allow for a
better understanding of the mechanisms involved in lymphatic vascular growth, function and
repair. Moreover, there is a strong need for the development of novel therapeutics in metabolic
as well as malignant diseases. Still, few studies have investigated the alterations of human
lymphatic endothelial cells in human pathophysiologic situations. Depending on the specific
pathophysiological microenvironment, different molecular repertoires are expected to be
altered, and these could highlight potential disease markers and, consecutively, therapeutic
targets.

17
3. Type 2 diabetes mellitus
There is a dramatic global increase in the prevalence of type 2 diabetes mellitus (T2DM) that will
reach an estimated number of 366 million patients in 2030 (Wild et al., 2004), making it a
workwide epidemic. Diabetes mellitus (DM) describes a metabolic disorder mainly
characterized by abnormal hyperglycemia which leads to subsequent defects in insulin action or
insulin secretion or both, and then being associated with disturbances in fat, protein and
carbohydrate metabolism in the whole body (Alberti and Zimmet, 1998).
3.1 Hereditary factors in T2DM
T2DM is known to be a multifactorial disease. Besides environmental factors, genetic elements
are suggested to contribute to its pathogenesis. Predisposition to the disease is determined by a
combination of both components, meaning that without exposure to certain environmental
factors, development of T2DM in genetically predisposed people does not necessarily occur.
However, a positive family history is a major risk factor for T2DM because 15‐25% of first‐
degree relatives of patients develop diabetes (Pierce et al., 1995). If both parents are affected,
the lifetime risk to develop T2DM is 60% at the age of 60 (Tattersal and Fajans, 1975). The
concordance rate for monozygotic twins reaches 35‐58% and for dizygotic twins it is 17‐20%
(Kaprio et al., 1992; Newman et al., 1987).
A series of genome‐wide linkage scans was performed, which identified new important
candidate genes for the development of T2DM. These are gene variants affecting insulin
secretion, insulin sensitivity, glucagon secretion or adiposity (reviewed in Staiger et al., 2009).
One attractive and consistent candidate gene is peroxisome proliferator‐activated receptor,
encoded by PPARG. Individuals with a prolinealanine change at position 12 show a lower body
mass index and decreased risk for the development of insulin resistance and T2DM (Altshuler et
al., 2000; Deeb et al., 1998). Other genetic polymorphisms linked to development of IR and
T2DM include Gly927Arg in insulin receptor substrate 1 (IRS1) and Gly483Ser in PPAR gamma
coactivator‐1 (PGC1α), which seemed to be not consistent because their initial association could
not be recapitulated (Stumvoll et al., 2005). During the last decade, a lot of single nucleotide
polymorphisms (SNPs) ‐ most of them affecting β‐cell function (Staiger et al., 2009) ‐ could be
identified, which represent potential risk SNPs for the development of T2DM.

18
3.2 Insulin action and resistance
Insulin is a peptide hormone synthesized in the β‐cells of the islet of Langerhans in the pancreas
and central to regulating fat and carbohydrate metabolism in the body. It downregulates the
glucose serum level by inducing glucose uptake into liver, muscle and fat tissue, which is then
stored as glycogen in these tissues. Insulin further stimulates growth and differentiation,
lipogenesis, glycogen and protein synthesis and inhibits lipolysis, proteolysis and glycogenolysis
(Saltiel and Kahn, 2001). Deviation from the balanced interplay between insulin action and
insulin secretion leads to changes in blood glucose levels (Stumvoll et al., 2005). In T2DM,
individuals are characterized by resistance of organs to the actions of insulin, thereby causing a
relative insulin deficiency. Main insulin target organs, i.e. adipose tissue, liver, muscle and
endothelium are affected by insulin resistance (IR, Zeyda and Stulnig (2009); Simonson and
Kendall (2005)). IR is often strongly associated with obesity, disturbances in lipid metabolism
and physical inactivity (Stumvoll et al., 2005). IR is suggested to be the central pathological
mechanism underlying glucose intolerance, dyslipidemia, hypertension, hyperuricemia,
endothelial dysfunction and a pro‐inflammatory, pro‐thrombotic environment (Simonson and
Kendall, 2005).
On a molecular level, IR and T2DM become manifest in all stages of insulin signaling (Pessin and
Saltiel, 2000). These include insulin receptor and kinase activity, the concentration and
phosphorylation of insulin receptor substrate 1 (IRS1) and 2 (IRS2), phosphoinositide‐3‐kinase
(PI3K) activity, glucose transporter translocation, and the activity of intracellular enzymes.
Several gene knockout models with targeted deletion of components of the insulin signaling
pathway were developed to study IR in rodents, e.g. insulin receptor knockout, Irs1 knockout,
Irs2 knockout and glucose transporter 4 (Glut4) knockout (Saltiel and Kahn, 2001). While
single knockouts of genes often did not disturb glucose homeostasis, combinatorial knockouts
did, reflecting the polygenetic nature of T2DM (Saltiel and Kahn, 2001).
3.3 Role of adipose tissue in insulin resistance and type 2 diabetes mellitus
Adipose tissue plays a crucial role in the pathogenesis of T2DM, as it is a very active organ that
releases hormones, cytokines and lipid messengers. Enlarged visceral adipose tissue releases
non‐esterified fatty acids (NEFAs) and inflammatory cytokines, e.g. TNFα and interleukin (IL)‐6
(Rajala and Scherer, 2003; Ravussin and Smith, 2002; Hotamisligil et al., 1995) that contribute to
the so‐called metabolic syndrome. NEFAs have been suggested to contribute to IR by inhibition
of glucose uptake, glucose oxidation and glycogen synthesis and by increasing hepatic

19
gluconeogenesis (Bergman and Ader, 2000). Additionally, NEFAs can activate pro‐inflammatory
signaling pathways (Stumvoll et al., 2005; Itani et al., 2002). TNFα can further enhance
concentrations of circulating NEFAs by stimulating lipolysis and thereby provoking its own
negative effect on the insulin signaling pathway (Hotamisligil, 2000). Further, in the metabolic
syndrome TNFα expression is increased systemically and interferes with insulin signaling by
inhibiting IRS1 phosphorylation and insulin‐stimulated glucose uptake into adipocytes
(Hotamisligil et al., 1994). Conversely, deletion of TNFα improved insulin sensitivity in
genetically obese mice (Hotamisligil, 1999). Similarly, IL‐6 inhibits insulin signaling by
increasing the expression of suppressor of cytokine signaling (SOCS) proteins, which increase
IRS protein degradation (Krebs and Hilton, 2003; Senn et al., 2003).
The finding of increased expression of pro‐inflammatory cytokines in adipose tissue and serum
was the first link between inflammation, obesity and diabetes (Hotamisligil, 2006; Pradhan et al.,
2001). Chronic inflammation in adipose tissue induced by infiltration of macrophages was
described in obese humans and mice and was linked to the development of obesity‐related IR
(Weisberg et al., 2003; Xu et al., 2003). These macrophages were shown to be of an anti‐
inflammatory phenotype but they were capable of producing pro‐inflammatory cytokines, which
contributed to the development of IR (Zeyda et al., 2007; Zeyda and Stulnig, 2007). Further, a
close connection between IR and inflammatory pathways, e.g. NFκB pathway, has been
established (Stumvoll et al., 2005). Alternatively, recent experiments suggested that
endoplasmic reticulum (ER) stress is crucial for the initiation and regulation of inflammation
and insulin action as observed in IR (Hotamisligil, 2010).
Whereas NEFAs and pro‐inflammatory cytokines are upregulated in visceral obesity and T2DM,
the concentration of adiponectin, an adipokine with beneficial metabolic effects is reduced
(Hotta et al., 2000; Hu et al., 1996). Adiponectin potentiates the effects of insulin, namely
decreased hepatic gluconeogenesis, enhanced glucose uptake in skeletal muscle, fatty acid
oxidation and inhibition of lipolysis (Stumvoll et al., 2005). Other cytokines released by
adipocytes and/or the stromal vascular fraction which have been suggested to be of a pro‐
inflammatory phenotype and to be involved in the pathogenesis of T2DM are: leptin, resistin,
visfatin, retinol‐binding protein 4, IL‐1, IL‐18 and monocyte chemotactic protein‐1 (reviewed in
Tilg and Moschen, 2008).
Altogether, these recent findings reflect the multifactorial nature of IR and T2DM and highlight
the importance of adipose tissue inflammation, ER stress and inflammatory cytokine serum
levels in disease pathogenesis.

20
3.4 Vascular complications in diabetes mellitus
Cardiovascular complications are the main cause of increased morbidity and mortality in T2DM.
Adults diagnosed with diabetes have a 2‐ to 4‐fold increased risk for development of
cardiovascular events compared to those without diabetes (Fox et al., 2004). Vascular
complications include micro‐ and macroangiopathy (Schalkwijk and Stehouwer, 2005;
Stehouwer et al., 1997). Microangiopathy is the essential cause of nephropathy, retinopathy and
neuropathy. On the contrary, macroangiopathy mainly affects coronary, carotid and peripheral
arteries and increases the risk for myocardial infarction, stroke and diabetic foot syndrome
(Duby et al., 2004; Goldberg, 2003; Kikkawa et al., 2003; Porta and Bandello, 2002). A huge
clinical trial study published 1995 demonstrated that hyperglycemia plays an important role in
the pathogenesis of microvascular complications in non‐insulin dependent DM (Group, 1995).
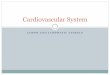
Figure 3: Molecular pathways of how glucotoxicity contributes to diabetic complications in bloodvessels (taken from Calcutt et al. (2009)).

21
There are four major hypotheses about how hyperglycemia can cause diabetic blood vascular
complications (Figure 3) on a molecular level: (i) increased polyol pathway flux, (ii) increased
advanced glycation end‐product (AGE) formation, (iii) activation of protein kinase C (PKC) and
(iv) increased hexosamine pathway flux (Brownlee, 2001). The common element linking these
four mechanisms is the overproduction of reactive oxygen species (ROS) by the mitochondrial
electron‐transport chain (Du et al., 2000; Nishikawa et al., 2000). Besides ROS production,
endothelial dysfunction is characterized by an imbalanced production of vasoconstrictors and
vasodilators with increased production of endothelin and reduced bioavailability of the
vasodilator nitric oxide (NO), increased vascular permeability due to an increased expression of
VEGF, capillary and vascular occlusion due to increased production of TGF‐β and fibronectin,
pro‐inflammatory gene expression and decreased fibrinolysis with increased risk of
thromboembolic events (reviewed in Brownlee, 2001). Important serum biomarkers for diabetic
endothelial dysfunction include increased levels of plasminogen activator inhibitor‐1 (PAI‐1),
sE‐selectin, sVCAM‐1, sICAM‐1, C‐reactive protein (CRP) and TNFα (Schalkwijk and Stehouwer,
2005; Meigs et al., 2004). However, the complete cascade of pathophysiological events that lead
to vascular alterations by T2DM is still unsolved.
3.5 Skin symptoms and clinical signs of T2DM
Patients share common clinical features suggestive for the development of T2DM. These include
obesity, hypertension, dyslipidemia, non‐alcoholic fatty liver and acanthosis nigricans with
brownish hyperpigmentation of the skin. Moreover, many patients show a familiar
predisposition with first or second degree relatives diagnosed with T2DM (Pinhas‐Hamiel and
Zeitler, 2007; Reinehr, 2005). Around 80% of children and adolescents are asymptomatic
(Reinehr, 2005). Symptoms of severe hyperglycemia include polyuria, polydipsia, weight loss,
polyphagia and blurred vision (Association, 2005). Often associated with T2DM is an increased
susceptibility to infections of the urinary and respiratory tract and soft tissue infections (Joshi et
al., 1999).
Additionally, many patients show cutaneous manifestations (van Hattem et al., 2008):
‐ Yellow nails: Yellow discoloration of hallux nail.
‐ Diabetic thick skin: Asymptomatic, measurably thicker skin.
‐ Acrochordons: Small, pedunculated, soft lesions, most often on eyelids, neck, and axillae.
‐ Diabetic dermopathy: Atrophic, scarring, hyperpigmented macules on the extensor
surface of lower legs.
‐ Acanthosis nigricans: Hyperpigmented plaques.

22
‐ Acquired perforating dermatosis: Dome‐shaped papules and nodules with
hyperkeratotic plug.
‐ Calciphylaxis: Localized redness and tenderness, then subcutaneous nodules and
necrotizing skin ulcers appear.
‐ Eruptive xanthoma: Crops of yellow papules with an erythematous halo.
‐ Granuloma anulare: Oval or ring‐shaped lesions with a raised border of skin‐colored or
erythematous papules
The can often precede disease onset by many years. Moreover, T2DM patients suffer from
recurrent and long‐lasting skin infections with colonization of bacteria, viruses and fungi
(Jelinek, 1994). Therefore, it is suggested that there is a disturbed skin microenvironment
caused by an interplay of different mechanisms, including regulatory misconduct in metabolism,
inflammation, angiogenesis etc.
3.6 Diagnosis of T2DM
The preferred test for diagnosis T2DM is the measurement of fasting plasma glucose (FPG),
which is cost‐efficient, easy to do and acceptable to patients (Association, 2007). Alternatively,
one could do a 75‐g oral glucose tolerance test (OGTT), which is more sensitive and more
specific than FPG but hardly reproducible (Association, 2007). The use of HbA1c is not
recommended for diagnosis at this time, but rather for monitoring therapy response
(Association, 2005), while others identified HbA1c as a predictor of T2DM (Pradhan et al., 2007).
Criteria for diagnosis of DM are the following (Association, 2007; Rydén et al., 2007):
1. Symptoms of diabetes (polyuria, polydipsia, unexplained weight loss) and a plasma glucose
>200 mg/dl (11.1 mmol/l) at any time of day.
OR
2. FPG >126 mg/dl (7.0 mmol/l). Fasting is defined as no caloric intake for at least 8 h.
OR
3. 2‐h plasma glucose >200 mg/dl (11.1 mmol/l) during an OGTT.
If hyperglycemia cannot be defined as diabetes, it will be categorized as impaired fasting glucose
(IFG = IFG 100 mg/dl (5.6 mmol/l) to 125 mg/dl (6.9 mmol/l)) or impaired glucose tolerance
(IGT = 2‐h plasma glucose 140 mg/dl (7.8 mmol/l) to 199 mg/dl (11.0 mmol/l)). Both terms are
significant risk factors for the development of manifest diabetes and cardiovascular diseases
(Association, 2007; Rydén et al., 2007). Not only patients with symptoms, but also in
asymptomatic subjects, early diagnosis of T2DM is necessary. Criteria for testing for diabetes in

23
asymptomatic adults, which are at high risk to develop diabetes, are the follow (Association,
2009, 2007; Rydén et al., 2007; Association, 2005):
1. Age >45 years, BMI (body mass index) >25 kg/m2
2. Age >45 years, BMI >25 kg/m2 and additional risk factors:
‐ Physical inactivity
‐ First‐degree relative with diabetes
‐ High‐risk ethnic population
‐ Hypertension (>140/90 mmHg)
‐ HDL (high density lipoproteins) cholesterol level <35 mg/dl and/or triglyceride level
>250 mg/dl
‐ Polycystic ovary syndrome
‐ IGT (impaired glucose tolerance) or IFG (impaired fasting glucose)
‐ Vascular disease
Although complex and expensive, the current gold standard to measure insulin sensitivity is
hyperinsulinemic‐euglycemic clamp (Simonson and Kendall, 2005). IR and T2DM are often
associated with central obesity. This feature can be defined by waist circumference (> 102cm for
men, > 88cm for women), BMI (> 30kg=m2) or waist‐to‐hip‐ratio (> 0:9 in men and > 0:85 in
women). Moreover, it is important to use laboratory measurements of plasma triglycerides,
HDL, cholesterol and CRP (reviewed in Simonson and Kendall, 2005).
3.7 Therapy of T2DM
IR is the basis for the development of overt T2DM. Therefore, the major aim of therapy is to
improve insulin sensitivity of peripheral tissues. This can either be done by life style
modifications or by conventional drug therapy.
1) Life style interventions:
The first step of therapy are lifestyle interventions, including diet, weight loss and physical
activity, which were shown to be effective in preventing the development of T2DM in subjects
with IGT (Tuomilehto et al., 2001), to improve insulin sensitivity in patients with T2DM
(Ostergård et al., 2007) and to reduce cardiovascular risk factors (Stumvoll et al., 2005).
2) Medications:
Thiazolidinediones are a class of drugs which enhance insulin sensitivity, reduce glycemia and
hyperlipidemia, improve vascular function and reduce the inflammatory milieu in T2DM (Yki‐

24
Järvinen, 2004). Thiazolidinediones act as PPAR agonists. They alter adipose tissue metabolism
and lead to redistribution of tissue triglycerides from visceral to subcutaneous stores, thereby
reducing levels of circulating NEFAs (Ye et al., 2004) and hepatic lipid content (Yki‐Järvinen,
2004). Additionally, they are able to reduce pro‐inflammatory cytokines and increase
adiponectin (reviewed in Meriden, 2004). Moreover, they decrease FPG and HbA1c (Balfour and
Plosker, 1999). Important side effects are weight gain, uid retention, edema, hemodilution and
congestive heart failure (Nesto et al., 2004). Therefore, they should be used with caution
especially in patients with pre‐existing cardiovascular diseases (Nissen and Wolski, 2007).
Another treatment option is Metformin (Group, 1998a). It is a potent antihyperglycemic drug
with extrapancreatic effects. It reduces intestinal glucose resorption and hepatic
gluconeogenesis, and increases muscular glucose uptake (Hundal and Inzucchi, 2003;
Kirpichnikov et al., 2002). Metformin has also been shown to have beneficial effects on
cardiovascular risk factors (Hundal and Inzucchi, 2003). Gastrointestinal complaints, e.g.
diarrhea, nausea and vomiting are common side effects (Correia et al., 2008).
Sulfonylurea derivates act by increasing insulin secretion from the pancreatic β‐cell and
reduce the occurrence of micro‐ and macro‐vascular complications (Group, 1998b).
Other treatment options include αglucosidase inhibitors (Chiasson et al., 1998). In the late
stages of disease, when pancreatic insulin secretion is reduced to a level causing absolute insulin
deficiency, treatment is only possible by exogeneous insulin.
Moreover, therapy also includes management of associated cardiovascular risk factors, e.g.
hypertension, coronary artery disease, cerebrovascular disease and diabetic foot syndrome.
However, even more important than therapy, is the early diagnosis and prevention of diabetes in
order to reduce the population's burden of this disease.
However, till now, curative therapy of T2DM is still not available, explaining the necessity of
future research to identify novel biomarkers as well as novel therapy target structures. Here,
especially compartments are interesting, which were fairly neglected in the past, e.g. the
lymphatic vessel system.

25
4. Lymphatic vessels, type 2 diabetes mellitus and lipid metabolism
Research has remained sparse in the field of LV changes in conditions of IR and obesity. While
endothelial dysfunction of BVs is a well‐studied situation, almost nothing is known about
potential involvement and morphological changes of LECs and LVs in T2DM. We hypothesized
that LVs might experience phenotypical and molecular changes due to their important function
in wound healing, immune cell traffcking and fat metabolism (Alitalo, 2011; Tammela and
Alitalo, 2010).
4.1 Lymph vessel morphology in T2DM
Early microscopy studies showed histochemical and ultrastructural changes of LVs in the skin of
patients with T2DM. Thickening of BM, dilatations of intracellular spaces and dislocation of the
lymphatic endothelium were described, all of which affirming the existence of a so‐called
diabetic lymphangiopathy (Kaufmann et al., 1980; Ohkuma, 1979). However, uncertainty
remained as lymphatic capillaries could not be distinguished from blood capillaries without
unambiguous staining of definite lymphatic markers at that time. Later, increased expression of
the lymphatic markers podoplanin and LYVE‐1 was shown for pancreatic lymphatics
concomitant with an increased number of vesicles and protrusions of LECs during insulitis in
T1DM. Additionally, an increased number of DCs and T‐lymphocytes was shown to penetrate the
lymphatic endothelial wall and to infiltrate the pancreatic tissue (Ji et al., 2006; Qu et al., 2003,
2004), indicating an active role of lymphatic vessels during the autoimmune reaction of T1DM.
Skeletal muscle LVs of diabetic compared to non‐diabetic mice showed no changes regarding LV
density, but increased VEGF‐C and VEGF‐D mRNA expression, mainly attributable to an
increased damage of muscle fibers (Kivelä et al., 2007). Moriguchi et al. (2005) evaluated
changes of the lymphatic system in an alloxan‐induced diabetic mouse model. An increased
thoracic duct lymph flow and reduced uptake of dextran into regional LNs was observed. These
changes were reversible by the application of insulin. Overall, these data were pointing towards
an involvement of lymphatic vessels in the pathophysiology of diabetes, yet dependent on the
specific anatomic environment.

26
4.2 Lymph vessels and inflammation
Maruyama et al. (2007) used a corneal inflammation model to evaluate lymphangiogenesis
associated with wound healing in diabetic db/db mice, which show an inactivating mutation of
the leptin receptor. The study claimed reduced lymphangiogenesis in corneal incision wounds of
diabetic mice, which was accompanied by a decreased macrophage infiltration into the wound
region. Both phenomena, decreased lymphangiogenesis and reduced macrophage infiltration,
were detected to be beneficial for corneal wound healing. This group has further shown that
macrophages are able to contribute to the formation of LVs either by production of VEGF‐C,
which drives lymphangiogenesis or by conversion into LYVE‐1/podoplanin expressing cells
which reintegrate into the lymphatic endothelium (Maruyama et al., 2005). On the contrary,
another study showed that treatment of skin wounds of diabetic mice with VEGF‐C accelerated
LV formation associated with faster wound closure (Saaristo et al., 2006). Therefore, de novo
lymphangiogenesis, though versatile, seems to play a role during diabetic skin wound healing.
Further, LVs are essential for proper immunological functioning, especially regarding immune
cell trafficking and antigen delivery. The major cell types transported by the lymph are CD4+
memory T cells and APCs (Angeli and Randolph, 2006). APCs, e.g. DCs migrate via LVs to regional
LNs where they present antigens to naive T‐cells (Randolph et al., 2005). Pro‐inflammatory
cytokines induce the migration of DCs from the skin towards LVs by diminishing the expression
of E‐cadherin (Schwarzenberger and Udey, 1996), which loosens the interaction to surrounding
keratinocytes, and by upregulation of adhesion molecules (Angeli and Randolph, 2006).
Moreover, DCs produce matrix metalloproteinases to digest components of the ECM and BM and
to facilitate their migration throughout the tissue (Ratzinger et al., 2002). Defective lymphatic
function leads to an inefficient clearance of inflammatory cells and pathogens via the lymph and
consequently causes an increased risk for tissue infections (Rockson, 2001). Especially patients
with T2DM are susceptible to all kinds of infections, including skin infections (Muller et al., 2005;
Shah and Hux, 2003). It was shown that the number of peripheral DCs are reduced in T2DM
patients (Seifarth et al., 2008), pointing at reduced immune surveillance.
So far, little is known about the interaction of LECs and inflammatory cells as well as DCs under
hyperglycemic conditions. Cell culture experiments with human umbilical venous endothelial
cells (HUVECs) showed a significant increased adhesion of leukocytes after 24 hours of high
glucose exposure (Morigi et al., 1998). The same effect was seen with the incubation of HUVECs
with sera of diabetic patients (Morigi et al., 1998). Additionally, the expression of adhesion
molecules like ICAM1 and VCAM1 was significantly increased after incubation with high glucose
which was reversible by blocking these molecules (Morigi et al., 1998). Just recently, the
expression of chemokine ligand 27 (CCL27) on podoplanin‐low expressing lymphatic
precollectors was reported. This finding provides one explanation of an exit route for CCR10+ T‐

27
lymphocytes from inflamed tissue to the regional LNs (Wick et al., 2008). Overall, the specific
mechanisms of immune cell recruitment and consecutive migration into and along the LVs are
still poorly understood.
4.3 Lymph vessels with special emphasis on lipid metabolism
Another important function of LVs is the absorption and transport of fat and free fatty acids
(FFAs, Alitalo et al. (2005); Jurisic and Detmar (2009)). Further, there is increasing evidence that
there exists a close relationship between lymphatic function and fat metabolism as well as
adipogenesis (Harvey, 2008; Rosen, 2002):
(i) LNs and LVs are often surrounded by fat tissue (Harvey, 2008).
(ii) LV‐adjacent adipocytes respond to local immune reactions by increasing lipolysis (Pond and
Mattacks, 1998, 1995).
(iii) Chronic stimulation of LNs expands surrounding adipose tissue (Mattacks et al., 2003).
(iv) LN development is necessary for development of associated LN fat pads (Eberl et al., 2004).
(v) Haploinsufficiency in the PROX1 gene, a master regulator of lymphatic development, causes
adult‐onset obesity in mice. Cell culture experiments showed that incubation with lymph of
these obese mice led to a differentiation of 3T3‐L1 preadipocytes to mature adipocytes (Harvey
et al., 2005; Nougues et al., 1988).
(vi) Another indication for the involvement of lymphatics in fat formation is provided by
patients with lymphedema. In the late stages of disease they suffer from severe and irreversible
fibrosis and overgrowth of adipose tissue in the edematous limb (Rockson, 2001).
(vii) Further, it was shown that blood cholesterol levels can influence lymphatic function. Lim et
al. (2009) discovered LV dysfunction and degeneration in ApoE‐/‐ mice fed a high‐fat diet. LV
integrity was disturbed and lymph transport declined, resulting in tissue swelling. Moreover,
lymphatic collectors lacked SMC coverage and had dysfunctional valves (Lim et al., 2009).
Hence, the hypothesis that leakage of lymph or failed removal of tissue fluid and adipogenic
factors may cause adipocyte maturation may be supported by these studies. This in turn would
have therapeutic implications for obesity and lymphedema by promoting lymphatic integrity or
preventing the release of adipogenic factors (Schneider et al., 2005). However, to what extent
lymph vasculature regulates lipid metabolism and adipose tissue formation is still speculative
and needs to be further clarified. Especially, knowing the regulation of uptake and transport of
adipogenic factors from and to the adipose tissue would be of great importance to evaluate
potential contributions of lymphatics to conditions like lymphedema and obesity.

28
5. DNA Microarrays The microarray technology emerged more than a decade ago. It was first described in 1987
(Kulesh et al., 1987) and improved until the first miniaturized microarrays were produced with
10.000 cDNAs spotted on a microscope slide (Schena, 1996; Schena et al., 1995). This technical
progress was appreciated with enthusiasm due to the possibility to detect the expression of a
very high number of genes at once (Lander, 1999; Brown and Botstein, 1999). In principal,
several types of microarrays exist according to the length of the spotted DNA‐probes (Draghici
et al., 2006):
1) cDNA arrays: length of the probe is up to a few thousand base pairs
2) oligonucleotide arrays: short (25‐30mer) or long (60‐70mer) oligonucleotide probes
The probes can either be contact‐spotted, inkjet deposited or directly synthesized on the
substrate (Draghici et al., 2006).
5.1 Advantages and problems of using DNA microarrays
High sensitivity, high accuracy and reproducibility are extremely important for reliable
microarray experiments. The sensitivity is defined as the concentration range (number of mRNA
copies) in which accurate measurements versus background noise are possible. The accuracy is
the degree of conformity of the measured versus its real value. High specificity is the ability that
a probe binds to a unique target sequence (Draghici et al., 2006). Reproducibility is the ability of
an experiment to be accurately reproduced. All these factors may be influenced by a variety of
parameters, including technical handling variations during RNA isolation and amplification,
synthesis of cDNA, washing and hybridization conditions and the amount of DNA bound to the
material (Pollock, 2002). Low starting material is a strong limitation for reliable microarray
experiments. In order to avoid this problem, additional
RNA amplification steps were added (Wick et al., 2004) in this study. Another possible error
could be the source and identity of the cDNA clones used in the array (Pollock, 2002).
Assessment of clone identity for 1189 IMAGE cDNA clones revealed that only 62% showed
sequence identity with the published data (Halgren et al., 2001). An often faced problem is the
variability of obtained results due to the biological complexity of tissues or diseases, e.g. T2DM
or schizophrenia (Miklos and Maleszka, 2004).

29
However, the great advantage of microarrays is that analysis of 47.000 genes (Human Genome
U133 Plus 2.0 Arrays, Affymetrix) is possible at once. Especially, to obtain a first overview of
which genes are deregulated, high‐throughput microarray analyses are indispensable. They
were shown to be very helpful in differentiating normal from tumor cells (Cole et al., 1999).
Additionally, tumor classifications became possible, e.g. for diffuse large B‐cell lymphomas
(Alizadeh et al., 2000), melanomas (Bittner et al., 2000) and breast cancer (Perou et al., 2000,
1999). Moreover, large‐scale genotyping became applicable, e.g. the analysis of SNPs (Fan et al.,
2000).
The possibility to look at thousands of genes at the same time also bears problems, because
bioinformatical analyses often result in a large list of genes. These are often hard to dissect and
to relate to biological processes which are important for the condition analyzed. Additionally,
the outcome of different bioinformatical tests is completely diverse lists of genes. Moreover,
innocent bystander genes often show the greatest differences while the most important genes
are hidden in the bulk of data (Miklos and Maleszka, 2004).
Using different online availabe tools, data can be analysed and genes are annotated according to
their similar biological function and similar localization within the cell. Moreover, sets of genes
can be related to distinct pathways, thereby highlighting the most important cellular processes
within a disease.
5.2 Application of the microarray technique in T2DM research
T2DM is a multifactorial disease integrating environmental factors and genetic elements in its
pathogenesis. Therefore, many parameters can generate expression data retrieved from
microarray experiments. in the context of DM and obesity, different cell types have been
analyzed by genome wide expression analysis to identify deregulated gene expression
signatures. Gene expression analysis of adipose tissue of obese and lean mice provided a wealth
of data and insight into adipocyte function (Nadler et al., 2000; Soukas et al., 2000). Microarray
analysis of aortic ECs in a streptozotocin‐induced model of T1DM unravelled transcripts related
to metabolic dysfunction and inflammation (Maresh and Shohet, 2008). Gene expression profiles
of peripheral blood mononuclear cells of diabetic patients with and without diabetic
nephropathy were analyzed (Moczulski et al., 2007). Proximal tubular cells exposed to high
glucose in vitro were checked for characteristic gene expression patterns (Qi et al., 2007).
Additionally, especially the analysis of SNPs plays an important role in the identification of geno‐
/haplotypes and potential susceptibility genes (Yang et al., 2007). Several hundreds of genes
have been studied for their role in T2DM (van Tilburg et al., 2001). Genome wide‐scans and
analysis of SNPs will help to identify completely new genes and pathways linked to the

30
pathogenesis of the disease (van Tilburg et al., 2001). Although a lot of new information is
generated using these approaches, it has to be kept in mind that T2DM is a complex disease
where it is often hard to integrate gene expression data into the functional context of disease.
Nevertheless, these genetic approaches provide informations that represent the basis of
diagnosis, development of new therapeutic targets and disease prevention. Moreover, they can
contribute to a better understanding of the etiology and pathogenesis of T2DM (van Tilburg et
al., 2001).

31
6. Material and Methods
6.1 Patients and skin samples For ex vivo transcriptomal comparison, LECs were isolated from non‐necrotic, apparently
healthy human skin derived from four type 2 diabetic and four normoglycemic patients. Table 3
shows the clinical characteristics of included patients. The study and the isolation protocol were
approved by the local ethics committee (ethics committee proposal nos. 449/2001; 81/2008).
All included patients gave their informed consent prior to the isolation procedure.
Diabetic patients
In the diabetic group, skin was obtained from leg amputates. Leg amputations were necessary
because of severe vascular side effects of T2DM. All four diabetic patients were diagnosed with
T2DM more than 6 years prior to cell isolation. They suffered from peripheral arterial occlusive
disease (PAOD) and were treated because of hypertension with one or two antihypertensives.
Three out of four patients had an elevated BMI. All patients received insulin for treatment of
T2DM.
Normoglycemic controls
In the non‐diabetic (normoglycemic) group, skin was taken either from leg amputates (2
samples) or from surgical abdominoplasty (2 samples). Leg amputations were necessary either
because of a trauma or an ulcus cruris due to venous insuffciency not related to T2DM. Only one
of the normoglycemic patients had a PAOD and received hypertensive therapy with three
antihypertensives. The BMI of included normoglycemic patients was slightly elevated and was
between 24.7 and 30.4.

32
Diabetic patients
Patient# 1 2 3 4 Age (years) 88 77 56 76
Sex Male Female Male MaleHbA1c (%) 11.4 8.7 12.4 8.7 BMI (kg/m²) 30.8 16.4 26.2 32
PAOD Yes Yes Yes Yes Microangiopathy Yes No Yes yes Hypertension Yes Yes Yes yes Blood pressure
(mmHg) 130/65 120/65 120/70 130/80
Antihypertensive therapy
Yes Yes Yes Yes
Antidiabetic therapy
Yes Yes Yes Yes
Indication for operation
Ulcus cruris Ulcus cruris Ulcus cruris Bypass stenosis
Normoglycemic control patients Patient# 1 2 3 4
Age (years) 35 26 31 84 Sex Female Male Male Male
BMI (kg/m²) 25 30.4 26 24.7PAOD No No No Yes
Microangiopathy No No No No Hypertension No No No Yes
Antihypertensive therapy
No No No Yes
Indication for operation
Cutis laxa abdominis
Cutis laxa abdominis Trauma Ulcus cruris
Table 3: Clinical data of selected diabetic patients and normoglycemic controls. HbA1c: glycated hemoglobin, BMI: body mass index, PAOD: peripheral artery occlusive disease.
6.2 Antibodies The following antibodies were used in immunohistochemistry, FACS and Western blotting:
Name Application Catalogue number
Company
FITC‐conjugated anti‐CD31 FACS* 555445 Becton Dickinson Pharmingen
RPE‐Cy5.1‐conjugated mouse monoclonal anti‐CD45
FACS PM IM2653 Beckman Coulter
IgG fraction of a polyclonal anti‐podoplanin antiserum
FACS, MB†, IF‡,IHC§
Produced in our lab
mouse anti‐CD31 (Clone JC70A)
MB, IF M0823 DAKO Cytomation
mouse monoclonal anti‐laminin alpha‐chain IF M0638 DAKO Cytomation
mouse anti‐CD68 IF, IHC M0876 DAKO Cytomation rabbit anti‐collagen IV IF 20411 Novotec

33
mouse clone 2C3 anti‐Duffy antigen/chemokine receptor gene (DARC)
IHC Kindly provided by Dr. I. Colin, INSERM, Paris
goat anti‐VEGFC IF AF752 R&DAnti‐VEGF‐A IF AF‐293‐NA R&Drabbit anti‐TNF‐α IF ab6671 Abcam mouse anti‐VCAM‐1 IF, CC|| 1244 Immunotech
rabbit anti‐CXADR IF sc‐15405 Santa Cruz (kindly provided by B. Vigl, ETH Zurich)
goat anti‐FABP4 IF AF3150 R&Dgoat anti‐CXCL10 IF, CC AF‐266‐NA R&Drabbit anti‐AQP3 IF ab15117 Abcam rabbit anti‐CYR61 IF ab24448 Abcam
Table 4: Primary antibodies used for * FACS: Fluorescence‐activated cell sorting, † MB: magnetic beading, ‡ IF: Immunofluorescence, § IHC: Immunohistochemistry, || CC: Cell culture experiments and ¶WB: Western blotting.
Name Application Catalogue number
Company
R‐Phycoerythrin donkey anti‐rabbit IgG FACS* 711‐116‐152
Jackson ImmunoResearch
Alexa Fluor 546 goat anti‐mouse IF‡ A11018 Molecular Probes
Alexa Fluor 488 goat anti rabbit
IF A11034 Molecular Probes
Alexa Fluor 546 goat‐anti rabbit
IF A11010 Molecular Probes
Alexa Fluor 488 goat anti‐mouse IF A11017 Molecular Probes
Alexa Fluor 488 donkey anti‐mouse IF A21202 Molecular Probes
Alexa Fluor 594 donkey anti‐goat IF A11058 Molecular Probes
HRP‐conjugated rabbit anti‐mouse
IHC§, WB¶ JZM035046 Axell
HRP‐conjugated goat anti rabbit
IHC, WB SGZ034047 Axell
Table 5: Secondary antibodies used for * FACS: Fluorescence‐activated cell sorting, † MB: magnetic beading, ‡ IF: Immunofluorescence, § IHC: Immunohistochemistry, || CC: Cell culture experiments and ¶WB: Western blotting.
6.3 Buffers and solutions Laemmli sample buffer: 2x concentrate
2 ml 1 M Tris‐HCl (pH 6.8)
4 ml 20% SDS (Sodium dodecyl sulfate; no. 161‐0302, Biorad)
200mM DTT (DL‐Dithiothreitol, for molecular biology; no. D9779‐5G, Sigma)

34
4.7 ml 60% Glycerol (Glycerin 87%; no. 1.04094.1000, Merck)
6.6 mg Bromphenol Blue (3',3",5',5"‐Tetrabromophenolsulfonephthalein; no. B‐8026, Sigma)
9.3 ml Aqua bidestillata
Resolving gel: 10 ml
3.3 ml Aqua bidestillata
4.0 ml 30% Acrylamide mix/Bis Solution (29:1, 3.3%C; no. 161‐0156, Biorad)
2.5 ml 1.5 M Tris‐HCl (pH 8.8)
0.1 ml 10% SDS (Sodium dodecyl sulfate; no. 161‐0302, Biorad)
0.1 ml 10% APS (Ammonium persulfate; no. 161‐0700, Biorad)
0.004 ml TEMED (N,N,N,N'‐Tetra‐methyl‐ethylenediamine; no. 161‐0800, Biorad)
Stacking gel: 5 ml
3.4 ml Aqua bidestillata
0.83 ml 1 M Tris‐HCl (pH 6.8)
0.63 ml 30% Acrylamide mix/Bis Solution (29:1, 3.3%C; no. 161‐0156, Biorad)
0.05 ml 10% SDS (Sodium dodecyl sulfate; no. 161‐0302, Biorad)
0.05 ml 10% APS (Ammonium persulfate; no. 161‐0700, Biorad)
0.005 ml TEMED (N,N,N,N'‐Tetra‐methyl‐ethylenediamine; no. 161‐0800, Biorad)
Electrophoresis buffer: 10 l
144 g Glycine (no. 161‐0718, Biorad)
30g Tris (Tris‐hydroxymethyl‐aminomethan; no. 1.08382.1000, Merck)
50 ml 20% SDS (Sodium dodecyl sulfate; no. 161‐0302, Biorad)
up to 10 l with Aqua bidestillata
Transfer buffer: 10 l
24.58 g Tris (Tris‐hydroxymethyl‐aminomethan; no. 1.08382.1000, Merck)
112.08 g Glycine (no. 161‐0718, Biorad)
2 l Methanol (no. M/4000/17, Fisher Scientific)
TrisBuffered Saline Tween20 (TBST):
6.1 g (50mM) Tris
9 g (150mM) NaCl
up to 1000 ml with Aqua bidestillata
500µl Tween‐20

35
6.4 Micropreparation of lymphatic endothelial cells from human skin Ex vivo isolation of ECs from human skin of diabetic patients and normoglycemic controls was
performed according to a combined enzymatic‐mechanical protocol as previously described
(Wick et al., 2008, 2007; Kriehuber et al., 2001). The whole procedure was conducted on ice.
Around 6‐8 hours after surgical amputation, approximately a ten to ten centimeter piece of skin
was removed and immediately put on ice onto a NIROSTA plate, disinfected with 70% alcohol.
Excessive subcutaneous fat was removed and skin was cut into 2 cm wide stripes for easier
handling. Thereafter, skin was dermatomized with a clamp and a dermatome with a sterile blade
mounted (E.Weck%CO; 10 mm). The dermatomized skin was collected in ice‐cold Iscove's
Modified Dulbecco's Medium (IMDM, InvitrogenTM, no. 21056‐023) and washed several times
with fresh IMDM on a shaker to remove excessive blood and fat. In the meantime, Dispase I
(Roche Applied Science, 10 x 2 mg sterile, no. 04942086001) was reconstituted in 1 ml of aqua
bidestillata (Abd) and further diluted with pre‐warmed PBS (cell culture grade, free of Ca2+ and
Mg2+) to obtain a final concentration of the enzyme of 0.6‐2.4 U/ml. The skin was put into 10 cm
dishes with its epidermal side up and covered with a sterile NIROSTA grid and the Dispase I
solution. The dishes were incubated for at least 60 minutes in an incubator at 37°C/5% C02. The
enzymatic reaction was stopped with pre‐warmed IMDM/10% FCS/1% 500mM EDTA solution.
After 60 minutes, the dermis could be easily removed from the epidermis using two tweezers.
The dermal sheets were put into 10cm dishes containing ice‐cold EBM‐2 medium supplemented
with 5% fetal serum and EGM‐2‐MV SingleQuots R (CC‐4147; Lonza). Thereafter, ECs were
released from the dermal sheets by scraping with an inverted scalpel until the skin fragments
were disaggregated. Released cells were sieved with a cell strainer (70µm pore size, BD
FalconTM, Bedford, USA, no. 352350) positioned on 50 ml tubes. The expected cell loss within
the sieving process was 10‐15%. Released and sieved cells were pelleted at 4°C at 1600 rpm (in
443g) for 8 minutes and resuspended in 20 ml ice‐cold PBS/2%BSA/1mM EDTA and sieved
again.
6.5 Cell staining procedure for subsequent fluorescent activated cell sorting The isolated single cells were stained with antibodies directed to CD45, CD31 and podoplanin.
Cell staining was performed to sort EC populations into LECs (CD31+PDPN+) and BECs
(CD31+PDPN‐) and to exclude contaminations with CD45+ cells, e.g. leukocytes and fibroblasts.
The antibodies were diluted in PBS/2%BSA/1mM EDTA, and incubated for 20 minutes in the
dark. After sieving through a cell strainer, cells were spun down again at 1600 rpm (443g) for 8
minutes, resuspended in 1100µl PBS/2%BSA/1mM EDTA and transferred into micronic tubes

36
for subsequent cell staining. 100µl of cells were used for antibody isotype control staining (tube
B) and transferred into a separate micronic tube. The rest of the cells represented the vast
majority of the cells and the definite sample (tube A).
A three‐step staining procedure was performed with intermediate washing steps and
centrifugation of cells at 1600 rpm for 8 minutes in between:
1. Antipodoplanin antibody (concentration 2.8mg/ml): 1:150 for A; rabbit IgG (concentration
100µg/ml): 1:150 for B
2. Donkey antirabbit IgG PE (R‐phycoerythrin‐conjugated; JacksonImmunoResearch, no. 711‐
116‐152): 1:200 for A and B
3. Mouse monoclonal antiCD31FITC 1:10 (Fluorescein‐Isothiocyanate‐conjugated; BD
Biosciences Pharmingen, no. 555445) and mouse antiCD45PC5 1:100 (RPE‐Cy5.1‐conjugated;
Immunotech, no. IM2653) for A; mouse IgG1FITC 1:10 (Dako Cytomation, no. X0927) and
mouse antiIgG1PC5 1:100 (Immunotech, no. IM2663) for B
After the last washing and centrifugation step, cells were resuspended in EGM‐2MV medium,
transferred on ice and transported to the FACS core facility unit of the General Hospital Vienna.
6.6 Fluorescenceactivated cell sorting After cell isolation and cell staining, flow cytometric isolation was performed on a BD FACSAria
Cell Sorter (Becton Dickinson Immunocytometry Systems, San Jose, CA). The flow rate was set to
10.000 cells per second but normally it was not higher than 3600 cells per second due to lower
cell numbers. Cells were separated into LECs (CD31+PDPN+) and BECs (CD31+PDPN‐) by using
CD45 (=leukocyte marker) as gate and podoplanin and CD31 (=panendothelial marker) for
sorting. One important control for purity of sorted cells was the CD45 negativity, which was
checked in all isolated cell populations after sorting and was shown as a plotted histogram.
Immediately after sorting, cells were lyzed with 350µl of RLT‐buffer/β‐mercaptoethanol and
RNA was isolated.
6.7 RNA isolation The RNA isolation was conducted using QIAshredder (Qiagen, no. 79654) and RNeasy Mini Kit
(Qiagen, no. 74104). The procedure was performed at room temperature according to the
manufacturer's instructions. For RNA isolation, cells were lyzed in 350µl of RLT‐buffer/β‐
mercaptoethanol, transferred to a QIAshredder column and centrifuged for two minutes at
maximum speed (13200 rpm). 350µl of 70% ethanol was added to the flow through (lyzed and
homogenisated cells), transferred to RNeasy mini columns and centrifuged for 30 seconds at

37
maximum speed. Afterwards, a DNase digest was performed: 350µl RW1‐buffer was added to
the column followed by 30 seconds of centrifugation at maximum speed. 80µl DNase I/RDD
buffer (1:8; RNase‐free DNase Set, Qiagen, no. 79254) was added to the RNeasy spin column
membrane and allowed to incubate for 15 minutes at room temperature. Thereafter, 350µl
RW1‐buffer was added and the columns were centrifuged for additional 30 seconds at maximum
speed. 500µl RPE‐buffer was added and the columns were centrifuged for 30 seconds at
maximum speed. This step was repeated twice. Additional two minutes of centrifugation were
added to dry the membrane of the column. Elution of isolated RNA was performed with 40µl
RNase‐free water. The isolated RNA samples were immediately stored at ‐80°C.
6.8 RTPCR and gel electrophoresis RNA of ex vivo isolated dLECs and ndLECs was used for non‐quantitative RT‐PCR to detect
transcripts for actin, keratin and the endothelial markers von Willebrand factor (vWF),
podoplanin and PROX‐1. Results were visualized using standard agarose gel electrophoresis.
Gene Forward Reverse Podoplanin caacgggaacgatgtggaag cgttggcagcagggcgtaac LYVE1 gccaggtgcttcagcctggtg cttcagcttccaggcatcgcacgg Prox1 acaagccgaagcgagaagg aacaagggtggtggctcag vWF cgctccttctcgattattgg ccggacagcttgtagtaccc
Keratin agaccaaaggtcgctactgc agaactgggaggaggagagg Actin atctggcaccacaccttctacaatgagctgcg cgtcatactcctgcttgctgatccacatctgc
Table 6: Primers used for RTPCR.
6.9 Sample preparation for microarray experiment The approximate amount of isolated mRNA per patient sample was 10‐100 ng/µl. Due to this
low amount of starting material and in order to be able to perform a reliable microarray
analysis, RNA was amplified (Wick et al., 2004). Two amplification steps were added using the
MessageAmp® II aRNA Amplification Kit (Ambion Cat.No. AM1751), according to the
manufacturer's instructions. After each amplification step, RNA amount and purity was checked
using the Agilent 2100 Bioanalyzer. Then, 1µg of amplified RNA was biotin‐labeled and purified
using MessageAmpTM II‐Biotin Enhanced Kit (Ambion, Cat.No. AM1791), hybridized to
Affymetrix Gene Chips (Gene Chip R Human Genome U133 Plus 2.0 Arrays, no. 900466,
Affymetrix) and chips were scanned using a Gene Chip® Scanner 3000 7G (Affymetrix). These
arrays represent the expression repertoire of the whole human genome for the analysis of over
47.000 transcripts on one chip.

38
6.10 Bioinformatical and statistical analysis Bioinformatical and statistical analysis was performed as previously described (Wick et al.,
2008, 2007). After background correction and normalization using the robust multi‐array
average (RMA) method, datasets were analyzed by the relative variance method (RVM, Stokić et
al. (2006)) and Student's t‐test to identify genes differentially expressed in diabetic (dLECs)
versus non‐diabetic LECs (ndLECs). Only genes with postnormalization values above the BioB
control were included in the calculations. Further, a p‐value < 0.05 was considered to identify
genes that were significantly different between dLECs and ndLECs. Database for Annotation,
Visualization and Integrated Discovery (DAVID, http://david.abcc.ncifcrf.gov, Huang et al.
(2009)), the NetAffx tool available on the affymetrix website (www.affymetrix.com) and the
online available software IPA (Ingenuity Pathway Analysis, http://www.ingenuity.com) were
used as a source for pathway analysis and information about involvement of genes in biological
processes. In addition, intensive literature research was added to finally group the genes
according to their similar biological function. Cluster analysis and heat map visualization was
done using the open source software programs Cluster 2.11 and Tree View 1.6 (available via
http://bonsai.hgc.jp/~mdehoon/software/cluster/software.htm). Moreover, a comparison of
differentially regulated genes in dLECs and in diabetic BECs (dBECs) from the same patients was
performed in order to gain knowledge on specific reaction patterns of LECs compared to BECs in
T2DM.
6.11 Quantitative Realtime PCR Differential transcript levels of the several LEC specific genes were evaluated by quantitative
real‐time PCR. Quantitative real‐time PCR analyzes were performed on a Chromo4® Real‐time
PCR System (Biorad). 1 µg RNA was transcribed into cDNA using Superscript II Reverse
Transcriptase (Invitrogen, no. 18064‐014). The obtained cDNA was diluted up to 100µl in aqua
bidestillata (Abd). For one reaction 3µl of cDNA plus 6µl of Abd was mixed together with 1µl of
the Taqman gene expression assay plus 10µl of Taqman Gene Expression Master Mix (Applied
Biosystems; no. 4369016).
Taqman gene expression assays were purchased from Applied Biosystems:
Gene Probe number Gene Probe number GAPDH hs99999905_m1 GALNTL2 hs00365065_m1CRIP1 hs00832816_g1 VCAM‐1 hs01003369_m1PDPN hs01089982_g1 CXCL14 hs01557413_m1CD44 hs00153304_m1 APOD hs00155794_m1IGFBP3 hs00181211_m1 PTX3 hs01073991_m1CXADR hs00154661_m1 FABP4 hs00609791_m1

39
AQP3 hs00185020_m1 PPARG hs01115513_m1MMP2 hs00234422_m1 GATA3 hs00231122_m1CCL27 hs00171157_m1 CXCL10 hs00171042_m1CYR61 hs00155479_m1 SDC1 hs00896424_g1 NOX4 hs00418356_m1 PTGS2 hs01573471_m1
Table 7: Taqman gene expression assays used for quantitative realtime PCR.
The following temperature protocol was used: Steps 3 and 4 were repeated 40 times with
intermediate plate reading.
1) 50°C ‐ 00:02:00
2) 95°C ‐ 00:10:00
3) 95°C ‐ 00:00:15
4) 60°C ‐ 00:01:00
Values were calculated applying the ddCt method as described (Pfaffl, 2001) and statistical
analysis was done using Microsoft® Office Excel 2003.
6.12 SDSPAGE and Western Blot Confluent ECs were homogenized in Laemmli sample buffer under shearing of genomic DNA
with an inverted pipette tip. For protein denaturation, samples were heated at 95°C for 5
minutes. 25µl of samples were loaded on a 12% bisacrylamide/acrylamide gel. The resolving gel
and stacking gel were prepared according to Sambrook/Fritsch/Maniatis (Molecular Cloning. A
Laboratory Manual, 2nd edition, 1989). PageRulerTM Prestained Protein Ladder (no. SM0671,
Fermentas Life Sciences), a 3‐color ladder with a mixture of 10 proteins covering a molecular
weight range from 10 to 170 kDa (5µl/well) was used as marker. The gels were run at 120V for
the first 30 minutes and then with 160V until the sample buffer front left the gel. Protein blotting
was done overnight at 24V using nitrocellulose transfer membranes (BA83, Whatman Protran).
Afterwards, the nitrocellulose membrane was dried between 30 minutes and overnight and
blocked with 5% milk powder in TBS‐T. The membrane was washed three times for 10 minutes
in TBS‐T buffer at room temperature (RT) and incubated with indicated antibodies in TBS‐
T/5%BSA for 1 hour at RT or overnight at 4°C (depending on the antibody used). After first
antibody hybridization, the membrane was washed three times for 10 minutes in TBS‐T buffer
and incubated with HRP‐conjugated secondary antibodies for 1 additional hour. Afterwards, the
membrane was washed for 1 hour to reduce background as much as possible. For detecting the
chemoluminescent signal, ECL plus (GE) was used. Exposure times varied between 30 seconds
and 10 minutes depending on the intensity of the signal. Densitometric evaluation was
performed with the LumiImager software.

40
6.13 Immunohistochemistry and Immunofluorescence Human skin was fixed in 4% paraformaldehyde at room temperature or in 20% sucrose at 4°C
overnight for embedding in paraffin or geltol, respectively. For deparaffinization, 2‐5µm sections
were incubated at 60°C for 30 minutes or overnight, subsequently dewaxed in xylene and
rehydrated in a series of descending concentrations of ethanol (100%, 96%, 70%, 50% and
water) to completely remove the paraffin. Antigen retrieval was performed in an autoclave for
60 minutes or in a microwave (600 W, 3 x 5 minutes) in 10mM citrate buffer, pH 6. In the case of
frozen sections, 5µm were cut using a cryotome and used immediately or stored at ‐20 to ‐80°C.
For immunostaining, sections were thawed, dried at room temperature for 10 minutes and fixed
in ice‐cold acetone or 1% paraformaldehyde (PFA) for 20 minutes. Thereafter, the individual
staining procedure was started. Blocking of sections was performed for 20 minutes at room
temperature with 10% goat or donkey serum. Afterwards sections were washed shortly in PBS
and first antibody solution was added. Depending on the first antibody, incubation was done for
1 hour at RT or overnight at 4°C. Next, the sections were washed 3 times 5 minutes in PBS and
secondary antibody dilution was applied. For fluorescence microscopy, fluorescently labeled
secondary antibodies were used. Immunohistochemical stainings were performed by using
either Avidin Biotin Complex (ABC), Alkaline Phosphatase (AP) or Horseradish Peroxidase
(HRP) staining according to standard protocols. Pictures were taken with a VANOX AHBT3
microscope (Olympus) or a laser scanning microscope (LSM 5 Exciter, Zeiss).
6.14 Evaluation of lymph and blood vessel density and counting of macrophages In order to quantify the number of BVs and LVs in skin samples of T2D and normoglycemic
patients, 5µm sections were immunostained with anti‐Duffy antigen/receptor for chemokines
(DARC) and anti‐podoplanin antibodies for visualization of BVs and LVs, respectively. The
number of CD68‐positive macrophages was determined in the dermis of four diabetic and four
non‐diabetic patients by staining with mouse anti‐human CD68 antibody (DAKO Cytomation; no.
M0876). Non‐overlapping fields were captured with an Olympus VANOX AHBT3 microscope at
200x magnification and the number of vessels was counted per medium power field, the number
of CD68‐positive cells was counted per 100µm2. Mean numbers of vessels/macrophages were
calculated per group of patients and the significance of difference was evaluated using paired
Student's t‐test.

41
6.15 Tissue fixation and processing for electron microscopy Dermatomized skin was cut into 1mm2 small pieces and fixed in 4% paraformaldehyde + 0.1%
glutaraldehyde in 0.1 M cacodylate buffer for 24 to 72 hours. Thereafter, skin was washed in
cacodylate buffer 2 times for 10 minutes and contrasted using osmium tetroxide for 2 hours.
After washing in aqua bidestillata and dehydrating in a series of ascending concentrations of
ethanol (70%, 80%, 96%, 100%) the skin was put into 100% propylenoxide for 10‐15 minutes
(twice) and into a 1:1 solution of propylenoxide and embedding medium EPON 812 for
additional 60 minutes. Afterwards, skin was put into pure EPON812 overnight. On the next day,
tissue was poured into fresh resin and this was polymerized at 60°C for two to three days.
Ultrathin sections (80nm) were cut using a Reichert‐Jung Ultracut E Mikrotom and collected on a
copper grid. The grids were stained with uranyl acetate/methanol and lead citrate. Pictures
were taken at different magnifications using a transmission electron microscope (JEOL 1010).
6.16 Primary Human Dermal Endothelial Cell Culturing Human dermal microvascular endothelial cells (HDMECs) were purchased from Promocell (no.
C‐12260). Pure LEC populations were obtained by magnetic bead sorting using the rabbit anti‐
podoplanin antibody. LEC purity was checked by Western blotting for the presence of
podoplanin and CD31 and for the negativity of CD146 as BEC specific marker (Amatschek et al.,
2007). Further, nuclear PROX‐1 as well as podoplanin expression was confirmed by
immunofluorescence stainings on LECs (see Figure 4). Cells were grown in endothelial basal
medium (EBM‐2) supplemented with 5% fetal serum and EGM‐2‐MV SingleQuots (CC‐4147;
Lonza) in an incubator at 37°C and 5% CO2. For all cell culture experiments, LECs were used
between passages 5‐8 and starved overnight in EBM‐2/0.5% FCS, unless otherwise indicated.

42
6.17 siRNA mediated gene knockdown siRNA transfection of LECs was done by using RNAiFect (Qiagen, no. 301605) in 24 well plates.
5*104 LECs were seeded the day before transfection in EGM‐2MV medium containing serum and
antibiotics and incubated at 37°C and 5% CO2. 20 µmol of siRNA (FABP4: nos. s4964 and s4965;
PPARg: nos. s10887 and s10888 from Ambion) was diluted in the appropriate volume of Buffer
EC‐R (supplied within the kit) to give a final volume of 100µl. 6 µl of RNAiFect were added and
samples were incubated for 15 minutes at room temperature to induce complex formation.
300µl of fresh EGM‐2MV medium and 100µl of the complexes were added to the adherent cells.
Medium was replaced after 6 hours to avoid cell toxicity by the transfection reagent. Gene
silencing was monitored after 48 hours using western blot analysis.
Figure 4: Confirmation of LEC purity used for cell culture experiments. Purity of LECs wasconfirmed by western blotting by checking the presence of podoplanin and CD31 and the absenceof CD146. Immunofluorescence double staining with the lymphatic specific markers podoplaninand PROX‐1 and CD31 further confirmed the purity of LECs in vitro.

43
6.18 LEC Proliferation assay 2*104 cells of scrambled or FABP4‐specific siRNA‐transfected LECs were seeded into 24‐well
plates with EGM‐2MV medium. The number of cells was counted every 48 hours and plotted as a
line diagram against time on the y‐axis using Microsoft®Excel 2003.
6.19 Protein CoImmunoprecipitation (CoIP) To show a direct interaction of FABP4 with PPARγ in LECs, co‐immunoprecipitations were
performed using the ProFoundTM Mammalian Co‐Immunoprecipitation Kit (no. 26149, Pierce)
according to the manufacturer's instructions. Both antibodies against FABP4 and PPARγ were
examined for the ability to pull down the antigen together with the other protein. LECs were
stimulated with 20µM rosiglitazone (no. 350‐125‐M025; Enzo Life Sciences) for 24 hours prior
to cell lysis in order to enhance PPARg levels. For immobilization of antibody, 50µg of either
FABP4 or PPAR was coupled to the AminoLink® Plus Coupling Resin. LECs were lyzed with IP
Lysis Buffer (0.5% Triton‐X100 in PBS, 10% protease inhibitor). Lysates were pulled through a
syringe with a 22‐gauge needle, put on the resin and gently mixed overnight at 4°C. The day
after, co‐immunoprecipitates were eluted using 50µl of Elution Buffer (supplemented with 5µl
1M Tris‐HCl pH 9.5) provided within the kit. Eluates were concentrated using centrifugal filter
units (Amicon Ultra ‐ 0.5ml 10k Ultracel®, no. UFC501024, Millipore). 30µl of eluates were
mixed with 6µl of 6x Laemmli sample buffer and applied to the gel for SDS‐PAGE analysis. For
long time storage of resin, 200 µl of 1X Coupling Buffer plus 0.02% sodium azide was added to
the spin columns, which then can be reused up to 10 times.
6.20 Chromatin immunoprecipitation (ChIP) To study activation of the FABP4 promotor by PPARγ ChIP was performed as previously
described (Gal‐Yam et al., 2008).
Cell culturing and antibody coupling:
LECs were seeded into 14 cm dishes, grown to confluence and stimulated with or without 20µM
rosiglitazone for 24 hours. The day before cell harvesting, sheep anti‐mouse IgG magnetic beads
(Dynabeads R M‐280, no. 112.01D, Invitrogen) were washed three times and resuspended with
1 ml of PBS‐BSA (bovine albumin serum, no. A7030, Sigma, 5mg/ml). Beads were incubated with
8µg/ml of anti‐PPARγ antibody (no. ab41928, Abcam) or mouse IgG (ChromPure mouse IgG,
whole molecule; no. 015‐000‐003, JacksonImmunoResearch) overnight at 4°C at 10 rpm.

44
DNA‐protein crosslinking and chromatin isolation:
Confluent cells were collected in EGM‐2MV, pelleted at 1600 rpm for 5 minutes, resuspended in
5 ml EGM‐2MV/1% formaldehyde (no. 47608, Sigma) for DNA‐protein crosslinking and
incubated for 10‐15 minutes. Cells were quenched with 1.37 M glycine for 5 minutes, washed
with 10ml of ice‐cold PBS plus 1% protease inhibitors (complete EDTA‐free, no. 11873580001,
Roche) and centrifuged for 5 minutes at 1600 rpm. Pellet was lyzed in 1ml SDS lysis buffer (1%
SDS, 10mM EDTA, 50mM Tris‐HCl (pH 8.1)) plus 1% protease inhibitors and put on ice for 10
minutes. Chromatin was sonicated 10 seconds for 25 times (100%, continuous, low) and
checked by gel electrophoresis. Therefore, 20µl of chromatin was filled up with H2O, 10µl 5M
NaCl was added and boiled for 15 minutes at 95°C. RNA was digested by adding 1µl RNAse
(DNAse free) and incubation for 30 minutes at 37°C, proteins were digested by adding 1µl
proteinase K (10mg/ml) and incubation for 20 minutes at 45°C. Chromatin was centrifuged at
full speed for 1 minute, supernatant was collected and DNA was purified using a QIAquick
column (Qiagen PCR Purification Kit, no. 28106). DNA concentration was measured by
Nanodrop 2000 (Thermo Scientific) and 2µg of DNA was loaded onto a 2% agarose gel to check
for the size of DNA‐fragments, which should be between 500 and 1000 base pairs for IP
experiments.
Chromatin immunoprecipitation and PCR analysis:
30µg of chromatin was used for IP and diluted 10‐fold with IP dilution buffer (0.01% SDS, 1.1%
Triton X 100, 1.2 mM EDTA, 16.7 mM Tris‐HCl (pH 8.1), 167 mM NaCl) up to 2ml. 80µl of
prepared beads coupled with anti‐PPARγ antibody were added and incubated overnight at 4°C
(10 rpm). On the following day, beads were washed 5 times with 1 ml RIPA buffer (50mM
Hepes‐KOH (pH 7.6), 0.5M Lithiumchloride, 1mM EDTA, 1% NP40, 0.7% Deoxycholic acid,
ddH2O), 2 times with TE (10mM Tris‐HCl (pH=8.0), 1mM EDTA) and eluted with 2 x 200µl
elution buffer (0.1M NaHCO3, 1% SDS). 16µl 5M NaCl was added to de‐crosslink and incubated
for four hours at 65°C. 50µl of input DNA was mixed with 16µl 5M NaCl and 400µl elution buffer.
Thereafter, 8µl EDTA, 16µl 1M Tris‐HCl and 2µl proteinase K were added to both samples and
incubated overnight at 45°C. DNA was recovered by phenol/chloroform extraction and
ethanol/glycogen precipitation and resuspended in 100µl of H2O. Potential PPAR binding sites in
the FABP4 promotor region was identified using SybrGreen quantitative real‐time PCR using
KAPA SYBR FAST qPCR master mix (Kapa Biosystems, no. KM4104). The location of the primers
(see Table 8 for primer sequences and Figure 5 for primer locations) was chosen according to
their proximity to PPARγ responsive elements (PPREs) which are known to be important
binding sites for the transcription factor PPARγ in the FABP4 promotor region regulating FABP4
expression.

45
Gene Forward Reverse FABP41 tttaagccagttcctctgagagg gaggtagaattgatggaccaatggFABP42 aagagtgtatacatacacagtcttga agaatggtaggcaggtttgcFABP43 tcttggcaagccacagtaataaatgc gcacttttgctgtgagatttcccFABP44 gctttgggaagtcattgctgatcc ccacaggatgctatgggagtgaFABP45 gagagggtatgtttcctcttcaacc gtacagcatagacatgcacacaccFABP46 gcagcacatgtgaacaacttctgtc ggtgtgtggtcacaagctaccMYT1 gaaccactggcagagaaagc gggtgagaggtgtcccag
Table 8: Primers used for qPCR to check binding of PPARγ to FABP4 promotor region.
The following temperature protocol was used. Step 2, 3 and 4 were repeated 40 times with
intermediate plate reading. The annealing temperature for the primer pairs FABP4‐1, FABP4‐5
and FABP4‐6 was 59.8°C, for FABP4‐2, FABP4‐3 and FABP4‐4 61.8°C:
1) 95°C ‐ 00:03:00
2) 95°C ‐ 00:00:03
3) 59.8°C or 61.8°C ‐ 00:00:30
4) 72°C ‐ 00:00:01
Figure 5: Graphical depiction of the human FABP4 promotor. Forward and reverse primers are labeled red. Restriction sites of different restriction enzymes are labeled black. PPARresponsive elements (PPREs) and CCAAT‐enhancer‐binding proteins (C/EBP) binding sites are labeled green.

46
6.21 TNFα stimulation of LECs In order to analyze the gene expression responsiveness of LECs to TNFα, cells were starved
overnight in EBM‐2/0.5% FCS and stimulated with or without 1, 10 and 20 ng/ml of TNFα (R&D;
no. 210‐TA‐010) for 6, 12 and 24 hours. In neutralization experiments, LECs were cultured in
EBM‐2/0.5% FCS containing 10 ng/ml TNFα with or without 25µg/ml TNFα antibody (Abcam;
no. ab6671). Altered gene expressions induced by TNFα were checked using subsequent
quantitative real‐time PCR and Western blotting.
6.22 Scratch wounding assay In order to check whether TNFα has an influence on wound closure of LEC monolayers and
therefore also migration of LECs, we starved and stimulated LECs with or without 10ng/ml of
TNFα for 24 hours. Thereafter, an artificial wound was created using a 200µl pipette tip. Non‐
adherent cells were washed away and wound closure was monitored with an inverted live cell
microscope (AxioVert 200M, Zeiss) by taking pictures of the same section every hour for 24
hours. Wound area was measured using AxioVision 4.7 and calculated as amount of wound
closure (in %) from timepoint t=0.
6.23 Enyzmelinked Immunosorbent Assay (ELISA) Supernatants of stimulated LECs were collected and concentrated 20‐fold from 2 ml to
approximately 100µl using centrifugal filter units (Amicon Ultra ‐ 0.5ml 10k Ultracel R, no.
UFC501024, Millipore). 80µl of supernatants were used for coating of 96‐well ELISA plates
overnight and checked for the secretion of CXCL10. Primary anti‐CXCL10 antibody (no. AF‐266‐
NA, R&D Systems) was diluted 1:200 in PBS/1%BSA and 100µl was added to each well. After
incubation for 2 hours at room temperature, the plate was washed three times with 300µl
PBS/0.1% tween‐20 and 100µl of secondary antibody (diluted 1:3500 in PBS) was pipetted to
each well. Secondary antibody solution was incubated for an additional hour at room
temperature. Thereafter, plate was washed and 50µl of substrate solution (3,3',5,5'‐
Tetramethylbenzidine Liquid Substrate, no. T4444, Sigma) was added and incubated for 20
minutes under light protection. The reaction was stopped using Stop Reagent for TMB Substrate
(no. S5814, Sigma). The color development was read at 450nm in a microtiter plate reader
(Synergy HT; Bio‐Tek) within 10 minutes.

47
6.24 Macrophage adhesion assay 5*104 LECs were seeded into 24 well plates, starved overnight in EBM‐2/0.5% FCS and
stimulated with or without 10 ng/ml TNFα for 24 hours. Additionally, LECs were pre‐incubated
with inhibitory antibodies to CXCL10 (no. AF‐266‐NA, R&D Systems) and VCAM‐1 (no. 1244,
Immunotech). THP‐1 macrophages were grown in RPMI‐1640 medium containing 10% FCS (no.
10108, Gibco) and 1% Pen/Strep (no. 15140, Gibco). Before addition to LEC monolayer, THP‐1
macrophages were labeled using Cell trackerTM green CMFDA (1:5000, no. C2925, Invitrogen,
Molecular probes). 5*105 THP‐1 macrophages (+ 10ng/ml PMA (no. P8139, Sigma)) were
diluted in 500µl EBM‐2/0.5% FCS and added to LECs monolayer. After 3 hours, non‐adherent
cells were washed away and adherent THP‐1 cells were photographed using an inverted life cell
microscope (AxioVert 200M, Zeiss).
6.25 Macrophage transmigration experiment 2*104 LECs were seeded on the underside of fibronectin‐coated transwell filters (no. 3421;
Corning) and grown to confluence. Then, cells were starved overnight in EBM‐2/0.5% FCS and
stimulated with 10ng/ml TNFα (with or without an inhibitory antibody to TNFα or CXCL10) for
24 hours. THP‐1 macrophages were grown in RPMI‐1640 medium containing 10% FCS and 1%
Pen/Strep. Before addition to LEC monolayers, THP‐1 macrophages were labeled using Cell
trackerTM green CMFDA (1:5000, no. C2925, Invitrogen, Molecular probes). 5*105 THP‐1 cells (+
10ng/ml PMA) were diluted in 500µl EBM‐2/0.5% FCS and added to the upper chamber.
Fluorescence of transmigrated macrophages was measured in the lower chamber at 1, 3 and 6
hours using a fluorescence plate reader (485‐530nm; Synergy HT, Bio‐Tek).
6.26 Agarose spot assay Wiggins and Rappoport (2010) presented a novel chemotaxis assay based on the invasion of
cells into agarose spots containing chemoattractants. Due to the fact that CXCL10 is secreted by
LECs upon TNFα stimulation, we wanted to know if supernatants containing CXCL10 are
chemotactic for THP‐1 macrophages. Therefore, we applied this assay to our needs. 4% Agarose
solution (no. 18300‐012, Gibco) was shortly boiled and diluted in PBS to obtain a 1% agarose
solution. Thereafter, 20µl of agarose solution was mixed with 20µl of cell culture supernatants,
which was previously concentrated (see above). Two 10 µl‐spots of agarose‐supernatant
solution were pipetted in each well of a 24‐well plate and allowed to cool for 10 minutes at 4°C.
THP‐1 macrophages were labeled using Cell trackerTM green CMFDA (1:5000, no. C2925,

48
Invitrogen, Molecular probes), diluted in RPMI1640/0.5%FCS/1% Pen/Strep, stimulated with
10ng/ml PMA and 500.000 cells were added to each well of the 24‐well plate. After 24 and 48
hours, pictures were taken with an inverted live cell microscope (AxioVert 200M, Zeiss).
6.27 LEC monolayer permeability assay and TEER measurements 2*104 LECs were seeded onto fibronectin coated transwell filters (no. 3421, Costar) and grown
to confluence. Then, cells were starved overnight in EBM‐2/0.5% FCS and 150µl FITC‐dextran
solution (10µg/ml; no. FD70S‐100MG, Sigma) was applied to the upper and 500µl of medium to
the lower chamber. Diffused FITC‐dextran was measured spectroscopically in the lower
chamber at λ=485‐530nm using a fluorescence plate reader (Synergy HT, Bio‐Tek).
Transendothelial electric resistance (TEER) measurements were done using Millicell®‐ERS
electrode (Millipore). Resistance was measured in triplicates and calculated as per cm2 of
transwell filters. Transwell filters without LECs were used as background control and fresh
medium was added to the wells prior to each measurement.
6.28 Statistical methods and analysis Evaluation and compilation of data was carried out by using Microsoft Office Excel® 2003.
Significance was assessed using Student’s T‐Tests after determination of the variance equality
using an F‐Test. Graphics were made using Adobe Illustrator CS3. A p‐value of < 0.05 was
considered as statistically significant. * indicates a p‐value < 0.05, ** indicates a p‐value < 0.01,
*** indicates a p‐value < 0.001.

49
7. Results and Discussion
7.1 Morphological features of diabetic skin
Changes of vessel morphology and structure in T2DM have been reported earlier, especially for
BVs. These include BM thickening due to increased expression and deposition of ECM proteins.
Moreover, important features of tissue morphology in diabetic skin include changes in BV and
LV density as well as associated signs of inflammation.
In the first part of my thesis, I performed an extensive histological examination of dermal
lymphatic capillaries in T2DM skin specimens to trace potential morphological alterations.
7.1.1 Basement membrane morphology of small blood and lymphatic capillaries in diabetic skin
BM thickening is a common well described feature of diabetic BVs. Expression and deposition of
ECM proteins like type IV collagen and laminin is generally increased in DM (Asselot‐Chapel et
al., 1996; Roy et al., 1994, 1996). Around physiological normal LVs, ECM protein expression and
deposition is generally low and, if present, LVs show no regular continuous BM, but a rather
fragmented BM‐like structure (see also section 2.1.4, Vainionpää et al., 2007; Petrova et al.,
2002; Podgrabinska et al., 2002). Especially, the expression of some laminins was shown to be
completely absent from LECs (Vainionpää et al., 2007; Wigle et al., 2002). In order to take a
closer look at potential BM alterations of skin lymphatic capillaries in T2DM, we co‐stained
paraffin sections of human skin of T2DM and normoglycemic patients with the routinely used
Periodic acid‐Schiff (PAS) stain that labels the glycoproteins forming the BM, together with an
anti‐podoplanin antibody. Figure 6 A shows the onionskinned‐like thickening of BM in BVs of
human diabetic skin (black arrow) compared to normoglycemic skin, while LVs were PAS‐
negative both in diabetic and normoglycemic condition (black arrowheads). By staining
consecutive sections of diabetic skin with antibodies directed against podoplanin and smooth
muscle actin (SMA), lymphatic capillaries were identified due to their negativity for smooth
muscle actin (Figure 6 B; Tammela et al., 2005b). Next, we stained frozen sections of human skin
with anti‐laminin antibody to visualize eventual deposition alterations of this ECM protein
(Figure 7). This staining showed a more prominent deposition of laminin in diabetic (Figure 7 A)

50
compared to non‐diabetic BVs (Figure 7 D), whereas laminin was neither expressed in diabetic
(Figure 7 B) nor in non‐diabetic human skin LVs (Figure 7 E).
Moreover, double labeling with antibodies to podoplanin and collagen IV showed similar
amounts of collagen IV expression by both, LVs and BVs, indicating no significant expression
difference between diabetic (Figure 8 A‐C) and normoglycemic skin (Figure 8 D‐F).
Additionally, we performed ultrastructural analysis of LVs using electron microscopy, which
Figure 6: BM morphology of blood and lymphatic capillaries in human diabetic skin. A:Double labeling with PAS and anti‐podoplanin antibody shows thickening of BM of diabetic BVs(black arrow) but PAS negativity for LVs in diabetic and normoglycemic skin (blackarrowheads). B: Staining of consecutive sections of diabetic skin identified SMA‐negative, butpodoplanin‐positive vessels as a lymphatic capillary; Size bar: 20µm.

51
visualizes cellular alterations like membrane and organelle changes at high resolution.
Longitudinal pictures from the LVs confirmed that there are no obvious morphological changes
of lymphatic capillaries in diabetic versus normoglycemic skin and that LVs of diabetic skin do
not dispose of a BM lining (Figure 9). Vielleicht auch noch erwähnen: we did not trace luminal
expansions of LVs or LEC vacuolisations with this detailed technique, indicating no grave lymph‐
edematous condition in the skin specimens.
To conclude, in contrast to early observations tracing modifications of lymphatic vessel basal
lamina in T2DM (Ohkuma, 1979) and aberrant lymphatic vessels newly grown in carcinomas
(Vainionpää et al., 2007), we could not detect laminin and type IV collagen expression in T2DM.
Figure 7: Laminin expression of diabetic and nondiabetic LVs and BVs. A‐F: Double labeling with antibodies against laminin (A, D) and podoplanin (B, E); Merged images: C, F; Upper panel: diabetic skin, lower panel: normoglycemic skin; Size bar: 20µm.

52
Figure 9: Ultrastructural analysis of LVs. Electron microscopy of LVs of diabetic and normoglycemic skin revealed no changes in LEC morphology, e.g. appearance of BM; Lu: vessel lumen; Stars mark endothelial cell layer; Magnification: 10.000x.
Figure 8: Collagen IV expression of diabetic and nondiabetic LVs and BVs. AF:Double labeling with antibodies against collagen IV (A, D) and podoplanin (B, E) to showcollagen IV positive LVs in diabetic (upper panel) and normoglycemic skin (lower panel).Size bar: 20µm.

53
7.1.2 Basement membrane morphology of lymphatic collectors in diabetic skin
In contrast to lymphatic capillaries, the larger collecting LVs are characterized by the presence of
a BM and smooth muscle cell layers (Tammela et al., 2005b). We identified smooth muscle actin
(SMA)‐positive LVs with PAS in order to show whether they are altered in the diabetic condition.
However, similar to lymphatic capillaries, lymphatic collecting vessels did not show any
dramatic BM changes, as it is observed for diabetic BVs (Figure 10).
Overall, from these histological data we conclude that there are neither prominent alterations in
ECM protein deposition, nor morphological BM changes of lymphatic capillaries and collecting
LVs in the skin of T2DM patients. This finding is in contrast to reports by Ohkuma (1979) and
Kaufmann et al. (1980), where histochemical and ultrastructural changes of LVs were described
in the skin of patients with T2DM, namely thickening of BM, dilatations of intracellular spaces
and dislocation of the lymphatic endothelium. All of these changes were accepted as proof for a
diabetic lymphangiopathy. However, it is questionable if the described changes can be attributed
to LVs, as BVs and LVs could not be distinguished at that time due to the lack of specific markers
for lymphatic vessels.
7.1.3 Increased lymphatic vessel density in the skin of T2DM patients
However, the density of dermal capillaries itself might be an indicator of pathologic vessel
alterations, as it was described in lymphedema or acute inflammation (Seyama et al., 2010;
Kerjaschki et al., 2004). Hence, we quantified the density of LVs and BVs in the skin of diabetic
versus normoglycemic patients by immunostaining of paraffin sections using antibodies against
DARC to visualize BVs (Wick et al., 2008) and podoplanin for the detection of LVs (Breiteneder‐
Figure 10: Lymphatic collectors in diabetic skin do not show any morphological changes. A: Labeling of diabetic skin with PAS and anti‐podoplanin antibody; B: Double labeling of consecutive sections of diabetic skin with anti‐SMA and anti‐podoplanin antibodies to identify the indicated vessel as a lymphatic collecting vessel; Size bar: 20µm.

54
Geleff et al., 1999). Figure 11 shows representative images of human diabetic and
normoglycemic skin containing podoplanin‐positive LVs (left panel, black arrows) and DARC‐
positive BVs (right panel). Counting and quantification of LVs revealed a significant higher
number of LVs in diabetic compared to normoglycemic skin (p‐value = 0.04). Similarly, BV
density was slightly increased in diabetic compared to normoglycemic skin, but this was not
significant (p‐value = 0.7).
Under physiological conditions LECs scarcely proliferate. De novo lymphangiogenesis seems to
occur rather upon inflammatory or cancerous signals (Cueni and Detmar, 2008). Hence, we
supposed that the higher LV density in the skin of T2DM patients could be the result of a chronic
inflammatory stimulus present in the dermis. Moreover, higher LV density in diabetic patients
might represent a reaction of the skin and the skin vasculature to a perturbed metabolic
situation. In agreement with studies in human patients with metabolic diseases, enhanced LV
densities were previously detected in pathological situations such as cholesterol‐rich
atherosclerotic lesions (Kholova et al., 2011), and in chronic venous insufficiency ulcers
(Fernandez et al., 2011). In contrast to our findings, a decreased LV density associated with
reduced macrophage number and impaired wound healing was found in skin wounds (Saaristo
et al., 2006) and in a corneal suture model assay (Maruyama et al., 2007) of db/db mice.
However, although established murine models were used, artificial and acute wounds were
created which might not reflect the chronic inflammatory condition of the skin of patients
included in our study. Furthermore, our morphological characterization did not include skin
wounds or skin ulcera but rather (apparently) healthy skin.
Other studies showed that accelerated lymph vessel formation was crucial for resolution of
airway obstruction (Baluk et al., 2005), and to restore gut homeostasis in Crohn’s disease (von
der Weid et al., 2011). However, in chronic inflammation, LVs are suggested to be more
detrimental. Several reports indicate that inflammatory‐driven lymphangiogenesis leads to
dysfunctional vessel formation, representing an overproliferative phenomenon with reduced
lymph drainage capacity and enhanced leakyness (Baluk et al., 2009, Alexander et al., 2010).
Consistent with these findings, in pancreatic island inflammation, blocking of
lymphneoangiogenesis was beneficial for island transplants (Yin et al., 2011). Although some
reports indicate beneficial effects of increased lymphangiogenesis in inflammatory conditions
(Saaristo et al. 2006, Maruyama et al. 2005), other publications report dysfunctional lymphatic
vessels especially in chronic inflammatory diseases leading to prolongation of inflammation
(Alexander et al. 2010; von der Weid et al., 2011). Conclusively, the question whether
exaggerated lymphatic vessel formation might be dysfunctional but still be useful to resolve
inflammation and function as a bystander in tissue remodelling and wound repair in T2D has to
be explored.

55
Our findings also raise the question why BV density was not enhanced in T2DM skin. Consistent
with our observations, recent studies in murine models showed that acute inflammation
strongly enhances lymph vessel density but not that of blood vessels (Kim et al., 2009;
Huggenberger et al., 2011). Further, reduced blood vasculature was observed in diabetic skin
due to hypoxia and ischemia, which regulate VEGF production (Galiano et al. 2004; Enholm et al.,
1997; Thangarajah et al., 2009). Further, CXCL10, which was upregulated in dLECs, is known to
have an inhibitory effect on angiogenesis (Belperio et al., 2000; Bodnar et al., 2009).
Figure 11: LV and BV density in diabetic versus normoglycemic skin. Staining for LVs (black arrows) with anti‐podoplanin antibody and quantification of LV density shows higher LV density in diabetic skin; Right panel: Staining for BVs with anti‐DARC antibody and quantification of BV density reveals slightly elevated but not significantly different number of BVs in diabetic compared to normoglycemic skin; Size bar: 20µm.

56
Overall, our results suggest that lymphatic vessels follow a different proliferative stimulus than
blood vessels in T2D skin, which might be due to significant differences in tissue‐residing factors
and mechanisms that drive lymphangiogenesis versus angiogenesis.
7.1.4 Increased macrophage infiltration in diabetic skin
Considering the above mentioned murine wound healing study in db/db mice (Maruyama et al.,
2005), we evaluated the number of CD68‐ positive macrophages in normoglycemic and diabetic
human skin. Macrophage infiltration, measured as the number of macrophages per 100µm2 was
highly pronounced in diabetic compared to normoglycemic human skin, representing a 3.5‐fold
increase (Figure 12, p‐value < 0.001).
Macrophages produce growth factors which in turn support re‐epithelialization and promote
angiogenesis during wound healing. When they are missing, retarded of wound healing is
observed (Martin & Leibovich, 2005). The process of wound healing is strongly disturbed in
non‐healing diabetic wounds (Mahdavian Delavary et al., 2011). There is retarded wound
healing when macrophages show increased cytokine production and are dysfunctional (Khanna
et al., 2010). Pierce et al. (2001) report macrophage dysfunction which is characterized by the
enhanced production of inflammatory cytokines. Moreover, Zampell et al. (2012) show a more
than 3‐fold increase in macrophage number in lymph stasis, a condition of lymphatic vessel
dysfunction. Anti‐TNFα treatment of skin wounds depleted macrophages and increased wound
healing in diabetic mice (Goren et al., 2007). Hence, increased macrophage infiltration could be a
sign of enhanced production of inflammatory cytokines, but also of their reduced clearance by
newly grown, but dysfunctional lymphatic vessels.
Figure 12: Macrophage infiltration in normoglycemic versus diabetic human skin.Immunohistochemical labeling of human skin sections with anti‐CD68 antibody andquantification of macrophage number per 100µm2; Size bar: 20µm.

57
7.1.5 Macrophages produce vascular endothelial growth factors
As increased macrophage tissue infiltration is a critical sign of skin inflammation, we next aimed
to analyze their potential of production angiogenic and proinflammatory substances, supporting
a pro‐lymphangiogenic and pro‐inflammatory milieu in the skin of T2DM patients.
It is well accepted that macrophages can produce vascular endothelial growth factors (VEGFs),
e.g. VEGF‐A and VEGF‐C, and thereby are able to drive lymphangiogenesis (Machnik et al., 2009;
Kerjaschki, 2006; Maruyama et al., 2005).
Figure 13: VEGFC and VEGFA expression of infiltratin skin macrophages. A: Doublelabeling of human diabetic (upper panel) and normoglycemic (lower panel) skin with antibodiesto CD68 and VEGF‐C showing that macrophages in diabetic and normoglycemic skin are able toexpress VEGF‐C; Size bar: 20µm. B: Double labeling of human diabetic (upper panel) andnormoglycemic (lower panel) skin with antibodies to CD68 and VEGF‐A showing thatmacrophages in diabetic and normoglycemic skin are able to express VEGF‐A; Size bar: 20µm.

58
Therefore, we evaluated VEGF‐C and VEGF‐A expression by infiltrating tissue macrophages in
human diabetic and normoglycemic skin. As shown in Figure 13 A, both, 'diabetic' and
'normoglycemic' macrophages were expressing VEGF‐C, which is a strong lymphangiogenic
factor (Jussila and Alitalo, 2002). Similarly, VEGF‐A production was visible in infiltrating
macrophages of diabetic and normoglycemic skin (Figure 13 B).
Quantitative analysis (Figure 14) revealed that 76% and 90% of macrophages expressed VEGF‐C
in nondiabetic and diabetic skin, respectively (p‐value = 0.11). Further, 85% and 82% of
macrophages expressed VEGF‐A in non‐diabetic and diabetic skin, respectively (p‐value = 0.31).
Due to the fact that there was a highly increased number of infiltrating macrophages in diabetic
skin, which produced these (lymph‐)angiogenic factors, we assumed the generation of a steep
VEGFA and VEGF‐C interstitial tissue gradient, which could be a potent driver of
lymphangiogenesis in the skin of T2DM patients. Due to this result, it is tempting to hypothesize
that increased macrophage infiltration could be directly involved in the generation of the
strongly increased LV density and of the slightly elevated BV number in T2DM skin.
Figure 14: Quantitative analysis of VEGFC and VEGFA production by infiltrating skinmacrophages.

59
7.1.6 Increased TNFα levels in human diabetic skin
In skin diseases, e.g. psoarisis, TNFα expression has been identified as a key agent driving
persistent inflammation, and its expression was mainly assigned to T‐cell and macrophages
(Bonifati and Ameglio, 1999). Further, low grade vascular inflammation and elevated levels of
pro‐inflammatory cytokines are predictive for the development of cardiovascular diseases and
T2DM (Haddy et al., 2003). Especially, TNFα levels are increased in subjects with endothelial
dysfunction, as this pro‐inflammatory cytokine downregulates endothelial NO expression
(Yoshizumi et al., 1993) and causes acute local vascular inflammation (Chia et al., 2003).
Moreover, it is well established that TNFα levels are significantly increased in wounds of
diabetic mice (Goova et al., 2001). In order to trace if TNFα expression is increased in diabetic
skin, we performed respective immunofluorescence stainings. As shown in Figure 15, highly
increased levels of TNFα were detected in the skin of T2DM patients. In particular, diabetic
vasculature (white arrows) and epidermis (white arrowheads) as well as cellular structures in
between exhibited the strongest TNFα expression. These data further strongly suggested a
possible functional role of TNFα in the skin of type 2 diabetic patients.
Figure 15: TNFα expression in skin. Human diabetic (upper panel) and non‐diabetic (lowerpanel) skin was stained with anti‐TNFα antibody. Increased staining could be found invasculature and epidermis of diabetic skin.

60
7.1.7 TNFα production by CD68+ macrophages
Activated macrophages are not only crucial regulators of wound healing processes in diabetic
skin but also an important source of TNFα (Goren et al., 2007). Immunofluorescent double
staining with anti‐CD68 and anti‐TNFα antibody reconfirmed the increased macrophage
infiltration in diabetic (Figure 16 A) compared to normoglycemic skin (Figure 16 B) and showed
that these macrophages expressed TNFα (magnified inlets). It has been shown that macrophages
contribute to diabetes‐associated impaired wound healing mainly by producing TNFα (Goren et
al., 2007). Dysfunction of cutaneous macrophages combined with their reduced efferocytosis
(i.e. their phagocytosis capacity) contributes to impaired resolution of local inflammation and
complicated wound healing (Khanna et al., 2010). Our data suggested that a pro‐inflammatory
milieu in human diabetic skin is generated in part by macrophages via production of TNFα,
which in turn could have a detrimental impact on wound healing processes (Eming et al., 2007;
Goren et al., 2007) as well as migration of immune cells to the afferent LVs (Johnson et al., 2006).
All in all, enhanced levels of dysfunctional macrophages seem to contribute to disturbed skin
wound healing and susceptibility to skin infections, which was underlined by our data.
Figure 16: Production of TNFα by macrophages. Human diabetic (A) and non‐diabetic (B) skin was stained with anti‐CD68 and anti‐TNFα antibody. Increased macrophage infiltration could bedetected in diabetic skin as well as TNFα production by these macrophages (A, lower panel), whereas no expression was found in macrophages of normoglycemic skin (B, lower panel).

61
To summarize the first part of my thesis, the morphological findings we retrieved from the
immunohistochemical analysis of diabetic and normoglycemic skin showed increased lymph
vessel density, accompanied by a strong macrophage infiltration, which produced on one hand,
vascular endothelial growth factors, and, on the other hand the pro‐inflammatory cytokine
TNFα.
However, no dramatic differences where found regarding deposition of extracellular matrix
proteins, including laminin and collagen IV. Additionally, on an ultrastructural level, no BM or
cellular alterations could be traced for LVs in T2DM skin. Similarly to small LVs, also the bigger
collecting LVs showed no significant changes when compared to BVs of T2DM skin, which are
characterized by an increased staining for smooth muscle actin.
Altogether, these findings suggest that, although LV did not exhibit a form of diabetic
lymphangiopathy, as it was reported earlier, the dermis of T2D patients manifests dramatic
tissue remodelling processes characterized by enhanced LV density and increased macrophage
infiltration, supporting the pro‐inflammatory milieu and predisposing for recurrent infections.

62
7.2 Ex vivo isolation of LECs from human skin
Besides the fact that we observed significantly increased lymphangiogenesis associated with
enhanced macrophage infiltration in diabetic skin, there were no strong morphological
differences evident. However, we hypothesized that dermal LECs might reflect the altered load
of metabolites and retarded wound healing of T2DM skin on a molecular level. We expected that
we could answer the question whether complications seen in T2DM skin may be related to LV
malfunction, because this leads to wound healing defects (Saaristo et al., 2006), contributes to
local infection (Rockson, 2001) and has an important impact on lipid transport and metabolism
(Harvey et al., 2005). This potential LV dysfunction, together with signs for enhanced
lymphangiogenesis, should become evident by deregulation of respective gene expression
patterns.
Therefore, the second aim of my thesis was the analysis of the differential transcriptome of LECs
derived from T2DM patients and normoglycemic controls. I isolated LECs from human skin of
four diabetic and four non‐diabetic patients using a combined enzymatic‐mechanical protocol as
previously established and described (Wick et al., 2007, 2008; Kriehuber et al., 2001, see also
Material and Methods). The clinical characteristics of included patients are described in Table 3.
As shown in Figure 17 A, cells were sorted into LECs (CD31+Podoplanin+, green dots) and BECs
(CD31+Podoplanin‐, red dots). Reanalysis after sorting demonstrated the enrichment of CD31‐
and podoplanin‐positive LECs (in %) in the upper right quadrant, suggesting isolation of highly
pure populations of CD31/podoplanin double‐positive cells (Figure 17 B).
7.2.1 Quality control of isolated LECs
In order to exclude leukocyte contaminations, isolated cells were additionally stained with PC5‐
labeled CD45. As shown in Figure 18, the percentage of CD45+ cells after sorting was less than
one percent in all cell preparations, indicating nearly complete absence of leukocytes.
To stay as close as possible to the in vivo situation, immediately after sorting, cells were lyzed,
RNA was isolated and transcribed into cDNA. Using RT‐PCR, non‐diabetic (ndLECs) and diabetic
(dLECs) LECs were shown to be positive for lymphatic markers von Willebrand factor (vWF),
podoplanin and PROX1, but negative for keratin, suggesting exclusion of keratinocytes (Figure
19 A). Quantitative realtime PCR analysis confirmed similar expression levels of podoplanin in
dLECs and ndLECs (Figure 19 B). Altogether, these data confirmed high purity of isolated LEC
populations and exclusion of keratinocyte and leukocyte contaminations.

63
Figure 17: Fluorescent activated cell sorting of ex vivo isolated LECs and BECs. LECs andBECs were sorted by fluorescence using antibodies to podoplanin and CD31. BECs were CD31+and podoplanin‐ (A, red dots), while LECs were double positive for CD31 and podoplanin (A,green dots). B: Post‐sort analysis shows accumulation of double positive LECs in the upper rightquadrant. X‐axis: CD31 (FITC‐labeled) intensities, y‐axis: podoplanin (PE‐labeled) intensities;ndLECs: non‐diabetic LECs, dLECs: diabetic LECs.
Figure 18: Exclusion of leukocyte contaminations. Staining of cell populations with anti‐CD45staining was done in order to exclude leukocyte contaminations. Post‐sort analysis showsexclusion of CD45 positivity in isolated cells.

64
In order to obtain reliable microarray data and due to the low amount of RNA starting material,
two RNA amplification steps were amended (Wick et al., 2004) and checked by Agilent
Bioanalyzer 2100 measurements. Figures 20 and 21 show the Agilent graphs of RNA amounts
before and after two amplification rounds. This analysis further visualized the high quality of the
amplified RNA, excluded the possibility of degradation artefacts and guaranteed sufficient
amounts of RNA for subsequent array hybridization.
Figure 19: Quality control of isolated LECs. A: Using RT‐PCR and gel electrophoresis,transcripts for actin, vWF, keratin, podoplanin and prox1 were detected; ndLEC: non‐diabeticLEC, dLEC: diabetic LEC, +: positive control, ‐: negative control. B: Quantitative realtime PCRconfirmed expression of podoplanin in isolated cells, which showed no significant difference;dLEC: diabetic LEC, ndLEC: non‐diabetic LEC.

65
Figure 20: Amplification check of RNA isolated from dLECs. Left panel: RNA amount of isolated dLECs before amplification; right panel: RNA amount of isolated dLECs after two amplification rounds. The x‐axis of depicted graphs represents the runtime (s), the y‐axis represents the fluorescence units [FU].

66
Figure 21: Amplification check of RNA isolated from ndLECs. Left panel: RNA amount of isolated ndLECs before amplification; right panel: RNA amount of isolated ndLECs after two amplification rounds. The x‐axis of depicted graphs represents the runtime (s), the y‐axis represents the fluorescence units [FU].

67
7.3 Bioinformatical analysis of diabetic versus nondiabetic LEC transcriptomes
Files obtained from GCOS (.cel) were used to analyze significant changes between gene
expression profiles of different patients and groups (Wick et al., 2004, 2007, 2008). Only genes
with postnormalization values above the BioB control were included in the calculations. After
background correction and normalization (Figure 22) using the robust multichip average (RMA)
method, datasets were analyzed using two‐sample t‐test and relative variance method (RVM,
Stokić et al., 2006) (Figure 23). The RVM method was developed to trace gene expression
alterations in small sample entities, and is was successfully tested to identify important
endothelial markers like podoplanin (Stokić et al., 2006). Further, a p‐value < 0.05 was
considered to identify genes significantly different between dLECs and LECs.
Figure 23: Bioinformatical analysis using Student's ttest and RVM. Bioinformatical analysis of diabetic versus non‐diabetic LECs using RVM and t‐test. Both methods in one graph are shown on the right.
Figure 22: Normalization of microarray chip data. Normalization was done by RobustMultichip Average (RMA) using Bioconductor software in R.

68
Further, y‐comparison of LEC‐specific marker genes and of the genes differentially regulated
between dLECs and dBECs from the same patients was performed. Redundant annotation terms
were identified and omitted. All data has been deposited in NCBIs Gene Expression Omnibus and
are accessible through GEO accession number GSE38396
(http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE38396). Gehört schon hierher:
Hierarchical clustering was used to analyze expression profiles of the different samples and was
carried out using Euclidean distance metric and centroid linkage rule analysis with the
GeneSpringGX (Ambion) software. Data were represented as a dendrogram with the closest
branches of the tree representing arrays with similar gene expression patterns. The expression
profiles of the eight different array samples was analyzed, which illustrated a broad similarity
among the four dLEC arrays or the four LEC arrays from normoglycemic controls (ndLECs;
Figure 24).
The t‐test and RVM analysis retrieved a list of 180 genes that were differentially expressed
between dLECs and ndLECs. While 49 genes were upregulated, 131 genes were downregulated
in dLECs compared to ndLECs. This 180 significantly deregulated dLEC candidate genes were
the basis of a gene network that was assumed to be of functional relevance. The Gene Ontology
Browser available on the affymetrix website (www.affymetrix.com) was used as sources to
classify genes according to functionality context. Ingenuity Pathway Analysis (IPA) software
(Ingenuity Systems, Redwood City, CA, USA) was used to identify cellular networks that
statistically fit to a given input gene list and according expression values. The association of
genes with particular functions, pathways and diseases was analyzed according to their scores. A
Canonical pathway analysis identified pathways which were most significant to the input data
set. The significance value associated with functions and pathways is a measure of how likely it
is that genes from the data set file participate in that function. The significance is then expressed
as a p‐value, which is calculated by the right‐tailed Fisher’s exact test. An extensive NCBI GEO
and PubMed ‘in silico’ research was amended to retrieve information on gene expression and
relevance for LEC biology.

69
Figure 24: Hierarchical cluster analysis: LECs derived from four T2DM patients exhibit aunique gene expression pattern. Hierarchical clustering of the four LEC versus four dLEC geneexpression data (A) and of the 180 differentially expressed genes (FC>1.5) (B). Combined entityand condition trees are shown. On the y‐axis, an entity tree was generated by grouping the probesets based on the similarity of their expression profiles. On the x‐axis, a condition tree wasgenerated showing the relationship between the samples.

70
7.3.1 Identification of deregulated pathways and gene functions using Ingenuity Pathway Analysis
In order to identify functional gene patterns offering insight into the role of LECs in T2DM, the
differentially expressed genes were grouped according to their biological functions using the
NetAffx tool as well as Ingenuity Pathway Analysis (IPA). IPA revealed, which canonical
pathways and which gene functions are mainly altered in dLECs versus ndLECs. The top 10 of
the canonical pathways (Figure 25) and gene functions (Figure 26) were visualized using a bar
chart. Genes associated with these pathways and functions are highlighted in the Tables 9 and
10. Combining all in silico analyses, this led to the establishment of four overrepresented themes
in dLECs, comprising (A) defense response and inflammation, (B) tissue remodeling and cell
motility, (C) lymphangiogenesis and cell fate regulation and (D) lipid handling and small
molecule biochemistry (Table 11). Furthermore, the dLEC transcripts were highly enriched for
“plasma membrane” (44 transcripts) and “cell periphery and extracellular space” (71
transcripts) compartments (both P < 0.001), highlighting an extensive modulation of dLEC
molecules at the environmental interface.
Conclusively, these unbiased, computer‐based methods identified a dLEC transcriptome strongly
distinct from that of LECs under physiologic condition. This transcriptome mirrored the
phenotypic changes of T2DM skin on a molecular level and highlighted an involvement of LVs in
T2DM skin alterations. In the following sections, I will present the main candidates of the
deregulated gene themes and will discuss implications of their deregulation in LECs.

71
Figure 25: Pathway analysis using IPA. For the canonical pathway categorization of alteredexpressed genes, IPA software was used to calculate a p‐value (set ≤ 0.05, shown as blue bars) byFishers exact test, determining the probability with which a set of genes is associated with aknown biological function or pathway. The ratio (yellow squares) represents the number ofdifferentially expressed genes from the dataset divided by the total number of genes thatconstitute that canonical pathway.
Figure 26: Deregulated cellular functions in dLECs. Rankings of the top twenty Molecular andCellular Functions.

72
Ingenuity Canonical Pathways
pvalue (log) Ratio Molecules
Fatty Acid Biosynthesis 1,89E+00
3,92E‐02 ACACB, SLC27A3
IGF1 Signaling 1,84E+00 4,9E‐02 JUN, IGFBP3, SFN, CYR61, PRKAR1A
Complement System 1,84E+00 8,33E‐02 SERPING1, C1S, CD55IL10 Signaling 1,80E+00 5,71E‐02 IL1R2, SOCS3, JUN, IL1RN
Acute Phase Response Signaling
1,75E+00 3,93E‐02 SOCS3, SERPING1, HP, JUN, IL1RN, C1S, FGG, MIF
MIFRegulation of Innate Immunity
1,67E+00 6,52E‐02 PLA2G4A, JUN, PTGS2
Role of Macrophages, Fibroblasts and
Endothelial Cells in Rheumatoid Arthritis
1,64E+00 2,79E‐02 IL1R2, SOCS3, VCAM1, HP, JUN, F2RL1, IL1RN, C1S, MMP1,
WNT5A
Leukocyte Extravasation Signaling
1,58E+00 3,57E‐02 VCAM1, CLDN1, EZR, CD44, MMP2, RASSF5, MMP1
LPS/IL1 Mediated Inhibition of RXR
Function 1,57E+00 3,24E‐02
IL1R2, JUN, SLC27A2, FABP4,SLC27A3, PAPSS2, CHST15
VDR/RXR Activation 1,45E+00 5E‐02 CXCL10, IGFBP3, VDR, HSD17B2
Glucocorticoid Receptor Signaling
1,34E+00 2,84E‐02 IL1R2, VCAM1, JUN, HSPA1A, IL1RN, ANXA1, FGG, MMP1
IL8 Signaling 1,30E+00 3,19E‐02 CDH1, VCAM1, NOX4, RND3, MMP2, PTGS2
Atherosclerosis Signaling 1,19E+00 3,54E‐02 PLA2G4A, VCAM1, IL1RN, MMP1Glycosphingolipid Biosynthesis Neolactoseries
1,19E+00 2,9E‐02 GLT8D2, GGTA1
MIFmediated Glucocorticoid Regulation
1,10E+00 5,26E‐02 PLA2G4A, PTGS2
HIF1α Signaling 1,10E+00 3,64E‐02 JUN, SLC2A1, MMP2, MMP1Inhibition of
Angiogenesis by TSP1 1,08E+00 5,56E‐02 JUN, SDC1
Rac Signaling 1,07E+00 3,23E‐02 NOX4, JUN, CD44, IQGAP1
PXR/RXR Activation 1,06E+00 3,3E‐02 SCD, PAPSS2, PRKAR1AOGlycan Biosynthesis 1,05E+00 4,26E‐02 GLT8D2, GALNTL2
Table 9: Genes associated with most deregulated pathways (see Figure 25) as evaluated by IPA analysis.

73
Category pvalue (log) Molecules
Cellular Growth and Proliferation
1,61E‐13‐4,75E‐03
IL13RA2, SERPINB2, CXCL10, GNA15, EZR, SERPINB7, CLCA2, SLC2A1, MT1X, DCN, RRM2, FGFR2, MMP2, ANLN, KRT10,
FGFBP1, AREG, CDH1, CTSB, SPINT2, HHEX, CYR61, UNC5A, PHLDA2, CD55, BCL11B, TGM2, DSG3, JUN, HK2, F2RL1, TFAP2A,
FABP4, KRT2, RASSF5, VDR, CAV2, IGF2BP3, TGFBI, KRT17, MAP7, DEFB1, FOLR1, PLA2G4A, TMEM49, CD44, PTGS2, SFN,
GATA3, CXADR, NEDD9, ID4, CD81, SOCS3, SLC7A11, HSPA1A, GPNMB, BIRC5, FGFR3, CRIP1, CCL27, RORA, POSTN, SERPINB5, PTX3, KRT16, NOX4, H19, RRAD, LMNA, AURKA, IRF6, STC1, RAPGEF2, IL1RN,
IGFBP3, LOX, KIAA0101, ANTXR1, RARRES1, APP, GPC1, ANXA1, S100A8, VCAM1,
TFAP2C, PKP1, TP63, EDNRB, CGA, IL20RB, MST4, TPT1, HOPX, KLRK1, KLF5, TNFRSF19, PRKAR1A, WNT5A
Cellular Movement 2,54E‐11‐5,13E‐03
CD81, SOCS3, IL13RA2, SERPINB2, CXCL10, CCL27, EZR, CXCL14, POSTN, SERPINB5,
LYVE1, KRT16, PODXL, SLC2A1, DCN, ANLN, MMP2, AURKA, KRT10, S100A2, AREG, STC1, CDH1, RND3, IL1RN, CTSB, IGFBP3,
SPINT2, HHEX, CYR61, LY6D, LOX, SERPING1,
CDC20, UNC5A, CD55, RARRES1, IQGAP1, APP, TGM2, JUN, TFAP2A, F2RL1, ANXA1, TOP2A, FABP4, PTPRZ1, S100A8, VDR,
RASSF5, MMP1, NUSAP1, TFAP2C, VCAM1, TP63, SDC1, TGFBI, EDNRB, RACGAP1, CD69, DEFB1, LRRC15, LYPD3, TPT1,
PLA2G4A, HP, KLRK1, KLF5, CD44, PTGS2, GATA3, NEDD9,
WNT5A, PRKAR1A
CellToCell Signaling and Interaction
1,43E‐09‐5,13E‐03
CD81, MRC1, HSPA1A, MMRN1, FGG, SERPINB2, GP‐NMB, CXCL10, FGFR3, CCL27, CXCL14, POSTN, SERPINB5, KRT1, CLCA2, PTX3, KRT16, PODXL, DCN, FGFR2, MMP2, FGFBP1, AREG, STC1, CDH1, RND3, IL1RN, SLC7A2, IGFBP3, CYR61, ANK3, LY6D, LOX, ZDHHC2, SERPING1, CD55, IQGAP1, APP, TGM2, GPC1, DSG3, F2RL1, ANXA1, KRT2, PTPRZ1, S100A8, RASSF5, MMP1, DSC3,
VCAM1, TFAP2C, TP63, SDC1, TGFBI, CD69, PERP, LRRC15, CGA, IL20RB, LYPD3, TPT1, CLDN1, LGALS7B, KLRK1, CD44, PTGS2,
GATA3, NEDD9, CXADR, WNT5A
Tissue Development 1,43E‐09‐5,13E‐03
CD81, C4ORF31, MMRN1, FGG, SERPINB2, GPNMB, CXCL10, FGFR3,

74
POSTN, SERPINB5, CLCA2, PTX3, KRT16, NOX4, PODXL, DCN, FGFR2, MMP2, AREG, IRF6, STC1, CDH1, RND3, IL1RN, IGFBP3, HHEX, DSC1, CYR61, LY6D, ZDHHC2,
SERPING1, CD55, IQGAP1, APP, TGM2, DSG3, JUN, TFAP2A, F2RL1, ANXA1, PTPRZ1, S100A8, RASSF5, DSC3, TFAP2C, VCAM1, SDC1, TP63, TGFBI, KRT17, PERP, OVOL1, PLA2G4A, CLDN1, LGALS7B, KLF5, CD44, PTGS2, GATA3, NEDD9, CXADR, PRKAR1A,
WNT5A
Cellular Development 1,81E‐09‐5,13E‐03
CD81, SOCS3, CSTA, SLC7A11, HSPA1A, IL13RA2, SERPINB2, BIRC5, CXCL10, FGFR3, GNA15, RORA, EZR, POSTN, NOX4, RRAD, DCN, HBA1, BASP1, LMNA, FGFR2, MMP2,
AURKA, KRT10, AREG, STC1, IRF6, BHLHE41, CDH1, RND3, IL1RN, IGFBP3, CTSB, HHEX, DSC1, CYR61, SCD, LOX,
UNC5A, CD55, ANTXR1, BCL11B, SPRR1A, APP, TGM2, GPC1, JUN, F2RL1, TFAP2A, ANXA1, TOP2A, PTPRZ1, FABP4, S100A8, RASSF5, VDR, MMP1, TFAP2C, VCAM1, SDC1, TP63, EDNRB, TGFBI, RACGAP1,
CD69, MAP7, PERP, OVOL1, FOLR1, MST4, TPT1, PLA2G4A, HOPX, KLRK1, KLF5,
TMEM49, CD44, PTGS2, SFN, GATA3, CXADR, ID4, WNT5A, PRKAR1A
Dermatological Diseases and Conditions
6,06E‐09‐5,13E‐03
CD81, SCD, LOX, SOCS3, SERPING1, SRD5A1, CD55, APP, SERPINB2, BIRC5, DSG3, JUN, CCL27, TOP2A, KRT2, S100A8, VDR, KRT1, MMP1, KRT14, KRT16, PKP1, TP63, SDC1, EDNRB, KRT17, C1S, PERP, LMNA, MMP2, KRT10, DSG1, AREG, CDH1, CLDN1, KRT5,
IL1RN, PTGS2, DSC1
Hair and Skin Development and
Function
1,04E‐08‐5,13E‐03
CSTA, SLC7A11, UNC5A, HSPA1A, ANTXR1, SPRR1A, BIRC5, TGM2, DSG3, ANXA1, KRT2, VDR, KRT1, RIPK4, KRT14, KRT16, TP63, EDNRB, TGFBI, KRT17, OVOL1, KRT10,
IL20RB, MST4, AREG, IRF6, KRTDAP, CDH1, CLDN1, KRT5, FOXQ1, PTGS2, SFN, CYR61,
KRT15, TNFRSF19, ID4, WNT5A
Organ Development 1,04E‐08‐5,13E‐03
LOX, SOCS3, BCL11B, SPRR1A, APP, FGFR3, TGM2, RORA, KRT2, VDR, KRT1, RIPK4, KRT14, KRT16, PODXL, VCAM1, TFAP2C, TP63, EDNRB, KRT17, TLL1, FGFR2, MMP2, CGA, OVOL1, KRT10, AREG, IRF6, KRTDAP, HOPX, CDH1, HP, KRT5, CLDN1, FOXQ1, HHEX, PTGS2, SFN, KRT15, CXADR, TNFRSF19, ID4, PRKAR1A, WNT5A
Cell Death 2,82E‐08‐5,13E‐03
CD81, CSTA, SOCS3, SLC7A11, HSPA1A, SERPINB2, BIRC5, CXCL10, FGFR3, CCL27, EZR, SERPINB5, CLCA2, NOX4, SLC2A1, DCN, MT1X, HBA1, RRM2, LMNA, FGFR2, ANLN, MMP2, AURKA, TXNL4B, DSG1, AREG, STC1,
CDH1, RAPGEF2, RND3, IL1RN, CTSB,

75
IGFBP3, CYR61, SCD, RAB25, UNC5A, SRPX, CDC20, PHLDA2, CD55, ANTXR1, BCL11B, SPRR1A, APP, TGM2, AQP3, GPC1, DSG3, JUN, HK2, F2RL1, TFAP2A, ANXA1, TOP2A, PTPRZ1, S100A8, VDR, RASSF5, MMP1, VCAM1, TFAP2C, SDC1, TP63, EDNRB,
TGFBI, CD69, PERP, DEFB1, CGA, SH3BP5, MST4, TPT1, PLA2G4A, CHP2, KLRK1, KLF5,
CD44, PTGS2, SFN, NEDD9, TNFRSF19, ID4,
WNT5A, PRKAR1A
Inflammatory Disease 4,99E‐07‐5,13E‐03
CD81, MRC1, SOCS3, SLC7A11, HSPA1A, IL13RA2, CA12, SNX7, PCDH7, C4ORF31, FGG, SERPINB2, BIRC5, FGFR3, IL1R2,
CXCL10, RORA, CXCL14, POSTN, SERPINB7, IMPA2, SERPINB5, ADAMTS5, CLCA2,
PPP1R14C, ERH, C1S, RRM2, TLL1, LMNA, FGFR2, MMP2, C6ORF142, PAPSS2, AREG, IRF6, CDH1, IL1RN, SLC7A2, IGFBP3, CTSB, TAGAP, DSC1, CPS1, MCTP2, SCD, ZDHHC2, LOX, CDC20, SRD5A1, CD55, ANTXR1, PRR5L, APP, TGM2, JUN, F2RL1, ANXA1, TOP2A, PTPRZ1, KRT2, FABP4, S100A8, VDR, MMP1, VCAM1, SDC1, EDNRB, DST, CD69, SH3BP5, HOPX, PLA2G4A, HP, CD44,
CDH26, PTGS2, GATA3, TN‐ FRSF19, KYNU, WNT5A
Genetic Disorder 6,26E‐07‐3,71E‐03
MRC1, MALAT1, GLT8D2, SLC27A2, IL13RA2, SNX7, CA12, PCDH7, C4ORF31, GALNTL2, FGG, CXCL10, SERPINB7,
SLCO2B1, ACACB, SLC2A1, KLHDC10, DCN, MT1X, HBA1, RRM2, FGFR2, TLL1, ANLN, MMP2, KRT10, S100A2, C6ORF142, DSG1, WFDC5, CDH1, FXYD3, CTSB, SPINT2,
C10ORF58, C13ORF18, CYR61, CPS1, PER2, APOD, ANK3, SH3RF2, SERPING1, SRD5A1, CD55, BCL11B, TGM2, C17ORF67, AQP3, DSG3, HK2, JUN, F2RL1, TFAP2A, TOP2A, FABP4, KRT2, VDR, TRIM29, MMP1, DSC3, TGFBI, KRT17, DST, NLGN4X, SLC39A6, DEFB1, SH3BP5, FOLR1, PLA2G4A, HP,
KRT5, TMEM49, CD44, PTGS2, GATA3, NEDD9, KYNU, ID4, CD81, SOCS3, SLC7A11, HSPA1A, MT1M, CHST15, BIRC5, FGFR3, IL1R2, CRIP1, CCL27, RORA, CXCL14, POSTN, IMPA2, SERPINB5, KRT1, ADAMTS5, RIPK4, PPP1R14C, KRT16, NOX4, H19, RRAD, C1S, BASP1, LMNA, AURKA, PAPSS2, IRF6, RAPGEF2, IL1RN, SLC7A2, IGFBP3, DSC1, HSD17B2, MCTP2, SCD, CYP46A1, LOX, SRPX, CDC20, KIAA0101, ANTXR1, RARRES1, IQGAP1, APP, RGS17, GPC1, PTPRZ1, S100A8, RNF144B, KRT14, ANXA8L2, PKP1, TP63, SDC1, EDNRB,
RACGAP1, MIR155HG, PERP, OVOL1, MT1H,

76
TSPAN8, TPT1, HOPX, CLDN1, KLF5, TNFRSF19, PRKAR1A, WNT5A
Hematological System Development and Function
6,94E‐07‐5,02E‐03
CD81, SOCS3, SERPING1, HSPA1A, CD55, IL13RA2, BCL11B, MMRN1, APP, BIRC5, CXCL10, TGM2, JUN, CCL27, F2RL1, RORA, EZR, ANXA1, CXCL14, TOP2A, FABP4,
S100A8, RASSF5, VDR, MMP1, PTX3, VCAM1, EDNRB, CD69, HBA1, PERP, DEFB1, MMP2,
KRT10, PAPSS2, TSPAN8, TPT1, STC1, HP, IL1RN, SLC7A2, CTSB, CD44, HHEX, PTGS2, DSC1, GATA3,
NEDD9
Immune Cell Trafficking 6,94E‐07‐5,13E‐03
CD81, SOCS3, SERPING1, HSPA1A, CD55, APP, TGM2, CXCL10, F2RL1, CCL27, ANXA1, CXCL14, FABP4, S100A8, RASSF5, PTX3, PODXL, VCAM1, SDC1, EDNRB, CD69, DEFB1, MMP2, KRT10, TPT1, STC1, HP,
IL1RN, SLC7A2, CTSB, CD44, PTGS2, DSC1, NEDD9
Inflammatory Response 2,33E‐06‐5,13E‐03
CD81, SOCS3, SERPING1, HSPA1A, CD55, APP, FGG, TGM2, CXCL10, IL1R2, DSG3, F2RL1, CCL27, ANXA1, CXCL14, FABP4,
S100A8, LYVE1, VDR, PTX3, NOX4, PODXL, VCAM1, EDNRB, CD69, DEFB1, IL20RB, TPT1, STC1, PLA2G4A, HP, IL1RN, KLRK1, SLC7A2, CTSB, CD44, PTGS2, DSC1, GATA3,
NEDD9
Organismal Injury and Abnormalities
1,22E‐05‐5,05E‐03
SOCS3, SCD, SERPING1, SLC7A11, IL13RA2, APP, CXCL10, TGM2, FGFR3, DSG3, F2RL1, ANXA1, POSTN, LYVE1, MMP1, PODXL,
EDNRB, C1S, FGFR2, LMNA, MMP2, MT1H, KRT10, AREG, STC1, HOPX, PLA2G4A, HP, IL1RN, KLRK1, KLF5, CTSB, CD44, IGFBP3,
PTGS2
Cell Morphology 1,41E‐05‐5,13E‐03
ANK3, HSPA1A, ANTXR1, SPRR1A, IQGAP1, APP, TGM2, FGFR3, CXCL10, JUN, GNA15,
TFAP2A, EZR, ANXA1, POSTN, PTPRZ1, VDR, SERPINB5, PTX3, KRT16, NOX4, VCAM1, TP63, SDC1, EDNRB, TGFBI, RRAD, DCN, HBA1, BASP1, MAP7, LMNA, MMP2, STC1, IRF6, CDH1, RND3, KLRK1, KLF5, IGFBP3, CD44, PTGS2, CYR61, GATA3, TNFRSF19,
NEDD9, WNT5A
Tissue Morphology 1,63E‐05‐4,51E‐03
CD81, ANK3, SOCS3, LOX, SERPING1, APP, BIRC5, CXCL10, FGFR3, JUN, TFAP2A, F2RL1, ANXA1, SERPINB7, S100A8, SERPINB5, VDR, CAV2, MMP1, NOX4, VCAM1, H19, TP63, EDNRB, CD69, DCN, MAP7, FGFR2, MMP2, CGA, TPT1, STC1, IL1RN, CD44, IGFBP3, CTSB, PTGS2, SFN,
GATA3, CYR61, NEDD9, WNT5A
Lipid Metabolism 1,73E‐05‐4,41E‐03
PTX3, SCD, CYP46A1, ACACB, SLC27A2,SRD5A1, CGA, APP, IL1R2, GPC1, PLA2G4A,
F2RL1, IL1RN, ANXA1, CTSB, FABP4, S100A8, PTGS2, VDR, CAV2, SLCO2B1, APOD

77
Molecular Transport 1,73E‐05‐3,56E‐03
SCD, ACACB, SLC27A2, CGA, APP, IL1R2, GPC1, PLA2G4A, F2RL1, IL1RN, ANXA1, CTSB, FABP4, S100A8, PTGS2, CAV2,
SLCO2B1, APOD
Small Molecule Biochemistry
1,73E‐05‐4,52E‐03
CYP46A1, SCD, SOCS3, SLC27A2, SRD5A1, APP, IL1R2, GPC1, HK2, F2RL1, RORA, ANXA1, FABP4, S100A8, VDR, CAV2,
SLCO2B1, PTX3, ACACB, SLC2A1, EDNRB, CGA, PLA2G4A, IL1RN, KLRK1, SLC7A2,
CTSB, PTGS2, APOD
Table 10: Genes assciated with most deregulated functions (see Figure 26) as evaluated by IPA analysis.

78
AffyID Accession Gene Gene Description Ratio* Pvalue Molecule / Function†
Cluster A: Inflammatory Response Innate immune and acute phase response208470_s_at NM_005143 HP Haptoglobin 8.43 0.021 Peptidase, acute phase protein 206157_at NM_02852 PTX3 Pentraxin‐related gene 2.80 0.0004 Acute phase protein, regulation of innate immunity 208747_s_at NM_001734.3 C1S Transcribed locus, component 1, s subcomponent 2.76 < 0.05 Complement component, opsonisation
200838_at NM_001908 CTSB Cathepsin B 1.78 0.003 Lysosomal cysteine peptidase, cellular stress and wounding, APP processing
200986_at NM_000062 SERPING1 Serpin peptidase inhibitor, clade G (C1 inhibitor), member 1
1.71 0.004 Peptidase inhibitor, regulates C1S
200602_at NM_000484 APP Amyloid precursor protein 1.54 0.029 Acute phase protein 206785_s_at NM_2260 KLRC2 Killer cell lectin‐like receptor subfamily C, member 2 0.26 < 0.05 Ca‐dependent lectin, defense response regulation 205821_at NM_7360 KLRK1 Killer cell lectin‐like receptor subfamily K, member 1 0.23 < 0.05 MHCI receptor, innate immunity 208155_x_at NM_001468 GAGE1 G antigen 1 0.23 < 0.05 Antigenic peptide, defense response 210397_at U73945 DEFB1 Defensin, beta 1 0.20 0.0003 Antimicrobial peptide, defense response
202917_s_at NM_002964 S100A8 S100 calcium binding protein A8 0.14 0.041 Antimicrobial cytokine, RAGE ligand, inflammatory response
226926_at NM_001035516 DMKN Dermokine 0.13 0.002 Inflammatory protein 218677_at NM_020672 S100A14 S100 calcium binding protein A14 0.11 0.012 Ca2+ and RAGE ligand 230720_at NM_001165032 RNF182 Ring finger protein 182 0.10 < 0.05 MHCI associated antigen‐processing 219612_s_at NM_000509 FGG Fibrinogen gamma chain 0.08 < 0.05 Fibrin monomer, inflammatory marker 204971_at NM_005213 CSTA Cystatin A 0.05 0.012 Cysteine protease inhibitor, regulates CTSB
Wounding and stress response 236843_at NM_001143836 NOX4 NADPH oxidase 4 4.81 0.026 ROS production, oxygen sensor, inflammatory response 222748_s_at AW194729 TXNL4B Thioredoxin‐like 4B 3.77 0.026 Spliceosomal protein 213425_at NM_003392 WNT5A Wingless‐type MMTV integration site family, member 5A 3.64 0.0004 Signaling protein, inflammatory mediator 203060_s_at NM_004670 PAPSS2 3'‐phosphoadenosine 5'‐phosphosulfate synthase 2 3.27 < 0.05 ATP‐binding enzyme, anti‐inflammatory 200799_at NM_005345 HSPA1A Heat shock 70kDa protein 1A 1.88 0.011 Protein folding enzyme, cell stress
210145_at NM_024420 PLA2G4A Phospholipase A2, group IVA (cytosolic, calcium‐dependent)
0.28 < 0.05 arachidonic acid releasing enzyme, pro‐inflammatory
206461_x_at NM_005951 MT1H Metallothionein 1H 0.27 0.014 Zn‐binding protein, anti‐oxidant 204326_x_at NM_002450 MT1X Metallothionein 1X 0.23 0.008 Zn and Ca homeostasis, anti‐oxidant 217546_at NM_176870 MT1M Metallothionein 1M 0.19 < 0.05 Cu and Zn binding 205081_at NM_001311 CRIP1 Cysteine‐rich protein 1 (intestinal) 0.17 0.021 Zn finger protein family, immediate early gene
204748_at NM_000963 PTGS2 Prostaglandin G/H synthase and cyclooxygenase 0.17 0.017 Prostaglandin producing enzyme, inflammatory mediator
Chemotaxis, leukocyte adhesion and extravasation
204533_at NM_001565 CXCL10 Chemokine (C‐X‐C motif) ligand 10 5.16 0.009 Chemokinge ligand, chemotactic for monocytes and T‐cells
203868_s_at NM_001078 VCAM‐1 Vascular cell adhesion molecule 1 4.23 0.001 Integrin receptor, leukocyte adhesion molecule 226017_at NM_138410 CMTM7 CKLF‐like MARVEL transmembrane domain containing 7 1.52 0.038 Chemokine‐like, unknown function 204438_at NM_002438 MRC1 Mannose receptor, C type 1 1.47 < 0.05 Endocytosis glycoprotein, pathogen endopinocytosis 205945_at NM_000565 IL6R Interleukin 6 receptor 0.30 < 0.05 Subunit of the interleukin 6 (IL6) receptor complex

79
205403_at NM_004633 IL1R2 Interleukin 1 receptor, type II 0.26 < 0.05 Cytokine decoy receptor 206172_at NM_000640 IL13RA2 Interleukin 13 receptor, alpha 2 0.22 < 0.05 Chemokine receptor, suppresses T‐cell response
204597_x_at NM_003155 STC1 Stanniocalcin 1 0.21 < 0.05 Pleiotropic homodimeric glycoprotein, anti‐inflammatory
213506_at BE965369
F2RL1 Coagulation factor II (thrombin) receptor‐like 1 0.17 0.010 Receptor for trypsin and trypsin‐like enzymes coupled to G proteins, innate immune response
222484_s_at NM_004887 CXCL14 Chemokine (C‐X‐C motif) ligand 14 0.11 0.0005 Chemokine acting on macrophages and DCs 228575_at NM_144717 IL20RB interleukin 20 receptor beta 0.11 0.049 Coreceptor for IL20, suppresses T‐cell response 212657_s_at U65590 IL1RN Interleukin 1 receptor antagonist 0.08 < 0.05 IL1 antagonist 207955_at NM_006664 CCL27 Chemokine (C‐C motif) ligand 27 0.06 0.006 T‐cell attracting chemokine
Cluster B: LEC Adhesion and MigrationGrowth factors and signaling 204379_s_at NM_000141 FGFR2 Fibroblast growth factor receptor 2 0.30 0.032 FGF receptor signaling, cell growth 203819_s_at NM_006547 IGF2BP3 Insulin‐like growth factor 2 mRNA binding protein 3 0.28 < 0.05 mRNA binder, translational regulator
206100_at NM_001874 CPM Carboxypeptidase M 0.27 < 0.05
Membrane peptidase, controls hormone and growth factor activity
201506_at NM_000358 TGFBI Transforming growth factor, beta‐induced, 68kDa 0.23 < 0.05 Cell‐collagen interactions, inhibits cell adhesion 210095_s_at M31159 IGFBP3 Insulin‐like growth factor binding protein 3 0.22 0.011 Translational repressor, prolongs the half‐life of IGFs
209795_at NM_001781.2 CD69 = CLEC2 CD69 molecule 0.20 < 0.05
Ca dependent lectin superfamily of type II transmembrane receptors
225316_at NM_032793 MFSD2A Major facilitator superfamily domain containing 2 0.19 0.023 multi‐pass membrane protein, supposed tu suppressor
205239_at NM_001657 AREG Amphiregulin 0.17 < 0.05 EGF‐like autocrine growth factor, involved in infection
and inflammation 204268_at NM_005978 S100A2 S100 calcium binding protein A2 0.16 0.03 EF hand Ca binding protein, cell growth, pro‐migratory
203638_s_at NM_005130 FGFBP1 Fibroblast growth factor binding protein 1 0.11 0.025 Carrier protein that releases FGFs from the
extracellular matrix 203074_at NM_001630 ANXA8L2 Annexin A8‐like 2 0.10 0.030 ca‐dependent phospholipid binding, controls migration
204637_at NM_000735.3 CGA Glycoprotein hormones, alpha polypeptide 0.10 < 0.05 Hormone subunit, involved in vascularization, cell death
204379_s_at NM_000142 FGFR3 Fibroblast growth factor receptor 3 0.09 0.031 Fibroblast growth factor receptor, signaling pathway
ECM Proteolysis
235368_at NM_007038 ADAMTS5 ADAM metallopeptidase with thrombospondin type 1 motif, 5 3.24 0.002 Metalloprotease, cartilage aggrecan and proteoglycan
destruction 1555071_at NM_012464 TLL1 Tolloid‐like 1 2.36 < 0.05 Metalloprotease, regulates ECM formation 201069_at NM_00453 MMP2 Matrix metallopeptidase 2 2.14 0.009 degrades type IV coll, vascular remodelling
204475_at NM_002421 MMP1 Matrix metallopeptidase 1 (interstitial collagenase) 0.26 < 0.05 peptidoglycan metabolism, serum levels reduced in t2d,
206421_s_at NM_003784 SERPINB7 Serpin peptidase inhibitor, clade B (ovalbumin), member 7 0.24 < 0.05 serine‐type endopeptidase inhibitor
210715_s_at NM_021102 SPINT2 Serine peptidase inhibitor, Kunitz type, 2 0.15 0.009 inhibits a variety of serine proteases
204489_s_at NM_032330 CAPNS2 Calpain, small subunit 2 0.14 0.039 EF‐hand, calcium binding protein, regulatory unit for ca activated proteases
220051_at NM_006799.2 PRSS21 Protease, serine, 21 (testisin) 0.14 < 0.05 serine protease
204855_at NM_002639 SERPINB5 Serpin peptidase inhibitor, clade B (ovalbumin), member 5 0.13 0.036 serine‐type endopeptidase inhibitor

80
204614_at NM_002575 SERPINB2 Serpin peptidase inhibitor, clade B (ovalbumin), member 2
0.11 0.038 serine‐type endopeptidase inhibitor , uPA inhibitor
242204_at NM_145652 WFDC5 WAP four‐disulfide core domain 5 0.06 0.006 serine‐type endopeptidase inhibitor
ECM adhesion / cell migration
213909_at NM_001135057 LRRC15 Leucine rich repeat containing 15 7.26 < 0.05 membrane protein, might promote migration and invasion
236361_at NM_054110 GALNTL2 UDP‐N‐acetyl‐alpha‐D‐galactosamine:polypeptide N‐acetylgalactosaminyltransferase‐like 2
3.91 0.008
catalyzes O‐linked polysaccharide biosynthesis
1563502_at NM_016353 ZDHHC2 Palmitoyltransferase ZDHHC2 2.77 < 0.05 palmitoyltransferase, tetraspanin stabilization 220037_s_at NM_006691 LYVE1 Lymphatic vessel endothelial hyaluronan receptor 1 2.50 0.036 hyaluronic acid binding, cell motion, cell adhesion. 221447_s_at NM_031302 GLT8D2 Glycosyltransferase 8 domain containing 2 2.13 0.022 glycosyltransferase
210764_s_at NM_001554 CYR61 Cysteine rich protein 61 2.09 0.027 Ecm protein, interacts with several integrins and with heparan sulfate
215446_s_at NM_002317.5 LOX Lysyl oxidase 2.00 0.007 extracellular copper enzyme that initiates the
crosslinking of collagens and elastin 205612_at NM_007351 MMRN1 Multimerin 1 1.75 0.020 elastin microfibril interfacer, integrin ligand
203066_at NM_015892 GALNAC4S‐6ST
Carbohydrate sulfotransferase 14, B cell RAG associated protein
1.68 0.029 hexose biosynthesis, ECM formation
210809_s_at D13665 POSTN periostin, osteoblast specific factor 0.26 0.022 member of the fasciclin family, heparin binding
212014_x_at NM_000610 CD44 CD44 molecule 0.20 0.006 hyaluronic acid binding, vascular integrity, lc extravasation
201893_x_at NM_001920 DCN Decorin 0.19 0.001 proteoglycan, matrix assembly 203824_at NM_004616 TSPAN8 Tetraspanin 8 0.17 0.029 cell surface glycoprotein, integrin binder, cell mobility 204455_at NM_001723 DST Dystonin 0.14 0.008 plakin family protein, hemodesmosomes 201287_s_at NM_002997 SDC1 Syndecan 1 0.12 0.017 surface proteoglycan, cell spreading and adhesion
201141_at NM_002510 GPNMB Glycoprotein (transmembrane) nmb, osteoactivin 0.10 0.004 type I transmembrane glycoprotein, integrin binding, heparin binding
Morphogenesis / cytoskeleton organisation
1569020_at BC020686 NEDD9 Neural precursor cell expressed, developmentally down‐regulated 9 3.57 0.051 lamellipodia, integrin signaling
204955_at NM_006307 SRPX Sushi‐repeat‐containing protein, X‐linked 2.35 0.045 cytoskeletal association, reg. of cell adhesiveness 224694_at NM_032208 ANTXR1 Anthrax toxin receptor 1 0.27 < 0.05 type I transmembrane protein, filopodia organization
202890_at NM_001198608 MAP7 Microtubule‐associated protein 7 0.26 < 0.05 microtubule‐associated protein, cell polarization and differentiation.
223687_s_at NM_017527 LY6K Lymphocyte antigen 6 complex, locus K 0.23 < 0.05 anchored to membrane 206385_at NM_001149.3 ANK3 Ankyrin 3, node of Ranvier (ankyrin G) 0.19 < 0.05 cytoskeletal anchoring at plasma membrane 205014_at NM_031308 EPPK1 Epiplakin 1 0.16 0.028 Intermediate filament cytolinker
225615_at NM_001136265 LOC126917=IFFO2 Intermediate filament family orphan 2 0.16 0.0002 intermediate filaments
201820_at NM_000424 KRT5 Keratin 5 0.12 0.0002 intermediate filaments 206276_at NM_003695 LY6D Lymphocyte antigen 6 complex, locus D 0.09 0.006 leading edges of filopodia, mediates cell adhesion
Cellcell adhesion228863_at AF029343 PCDH17 Protocadherin 17 3.97 < 0.05 Ca‐dependent cell adhesion
233663_s_at NM_177980 CDH26 Cadherin‐like 26 3.18 < 0.05 cadherin domain‐containing protein, Ca2+‐dependent cell‐cell adhesion

81
205534_at NM_001173523 PCDH7 Protocadherin 7 0.27 < 0.05 member of cadherin superfamily 1569003_at NM_030938 TMEM49 Transmembrane protein 49 0.24 < 0.05 Cell‐cell adhesion, induces autophagy of starving cells 226374_at NM_001338 CXADR Coxsackie virus and adenovirus receptor 0.21 0.008 homophilic cell adhesion molecule, Lv permeability
205595_at NM_001944 DSG3 Desmoglein 3 (pemphigus vulgaris antigen) 0.16 0.033 calcium‐binding transmembrane glycoprotein vascular integrity
221854_at AI378979 PKP1 Plakophilin 1 0.15 0.002 member of the arm‐repeat (armadillo) and plakophilin gene, desmosomes
206032_at NM_001941 DSC3 Desmocollin 3 0.13 0.003 desmosomal protein, cell‐cell adhesion 222549_at NM_021101 CLDN1 Claudin 1 0.05 0.002 tight junction protein,
206642_at NM_001942 DSG1 Desmoglein 1 0.05 0.001 desmosomal protein, cell‐cell adhesion, vascular integrity
207324_s_at NM_004948 DSC1 Desmocollin 1 0.04 0.011 desmosomal protein, cell‐cell adhesion
Cluster C: LEC Growth / Lymphangiogenesis Response to stimulus / axon guidance236448_at R37358 UNC5A Unc‐5 homolog A (C. elegans) 6.23 0.013 netrin‐4 receptor, required for axon‐guidance
221933_at NM_020742 NLGN4X Neuroligin 4, X‐linked 4.27 0.012 neuronal cell surface protein involved in cell junction organization
213194_at NM_002941 ROBO1 Roundabout, axon guidance receptor, homolog 1 0.31 < 0.05 immunoglobulin gene superfamily, axon guidance receptor
204469_at NM_002851 PTPRZ1 Protein tyrosine phosphatase, receptor‐type, Z polypeptide 1 0.29 < 0.05 receptor protein tyrosine phosphatase, axonogenesis
202391_at NM_006317 BASP1 Brain abundant, membrane attached signal protein 1 0.09 0.024 transcription corepression molecule, axon guidance
Gprotein coupled receptor signaling
203096_s_at BF439282 RAPGEF2 Rap guanine nucleotide exchange factor (GEF) 2 3.45 0.011 Ras GTPase activating factor, fosters adherence junction formation
220334_at NM_012419 RGS17 Regulator of G‐protein signalling 17 2.63 < 0.05 GTPase activating protein, inhibitor of GPCR signaling 206701_x_at NM_000115 EDNRB Endothelin receptor type B 1.76 0.023 G protein‐coupled receptor, lymph vessel formation 222077_s_at NM_001126103 RACGAP1 Rac GTPase activated protein 1 0.30 < 0.05 negatively regulates Rho‐mediated signals
223322_at BC004270 RASSF5 Ras association (RalGDS/AF‐6) domain family 5 0.26 0.046 binds to activated Ras proteins, integrin signaling, directional ec movement
204803_s_at NM_004165 RRAD Ras‐related associated with diabetes 0.24 < 0.05 small GTPase associated signal transduction, inhibits vascular lesion formation
229723_at NM_054114 TAGAP T‐cell activation GTPase activating protein 0.21 < 0.05 Rho GTPase‐activating protein
212724_at BG054844 RND3 Rho family GTPase 3 0.12 0.023 GTP binding, semaphorin signaling in neurons, stress fiber organization
218186_at NM_020387 RAB25 RAB25, member RAS oncogene family 0.11 0.017 small GTPase protein, tumor suppressor
Other signaling transduction 201811_x_at NM_004844 SH3BP5 SH3‐domain binding protein 5 (BTK‐associated) 1.57 0.020 protein kinase inhibitor activity 203126_at NM_014214 IMPA2 Inositol(myo)‐1(or 4)‐monophosphatase 2 0.26 0.003 PI recycling pathway for signaling 221215_s_at NM_020639 RIPK4 Receptor‐interacting serine‐threonine kinase 4 0.26 0.0004 protein kinase C‐associated kinase 243582_at NM_152550 SH3RF2 SH3 domain containing ring finger 2 0.25 < 0.05 negative regulation of phosphatase activity
211003_x_at NM_0040613 TGM2 Transglutaminase 2 0.22 <0.05 covalent crosslinking of proteins, positive regulation of cell adhesion
226907_at NM_030949.2 PPP1R14C Protein phosphatase 1, regulatory (inhibitor) subunit 14C 0.13 0.004 kinase C‐enhanced PP1 inhibitor
Transcriptional regulators

82
204689_at NM_002729 HHEX Hematopoietically expressed homeobox 2.14 0.003 Homeobox TF, regulator of VEGF signaling 201464_x_at NM_002228 JUN Jun oncogene 1.65 0.018 Virus derived TF, cell growth, promotes ins resistance 204254_s_at NM_000376 VDR Vitamin D (1,25‐ dihydroxyvitamin D3) receptor 0.28 < 0.05 nuclear hormone receptor 222895_s_at NM_138576 BCL11B B‐cell CLL/lymphoma 11B 0.25 < 0.05 Zn‐finger TF, Tu‐suppressor
204653_at BF343007 TFAP2A Transcription factor AP‐2 alpha 0.25 0.016 Homo‐ or heterodimeric TF, neg. regulator of proliferation
221530_s_at NM_030762 BHLHB3 Basic helix‐loop‐helix domain containing, class B, 3 0.24 < 0.05 Transcriptional repressor
205286_at NM_003222 TFAP2C Transcription factor AP‐2 gamma (activating enhancer binding protein 2 gamma)
0.22 0.016 Homo‐ or heterodimeric TF, developmentally regulated
202597_at AU144284 IRF6 Interferon regulatory factor 6 0.21 0.021 Helix‐turn‐helix TF, neg. regulation of proliferation 205251_at NM_022817 PER2 Period homolog 2 (Drosophila) 0.20 0.002 Circadian clock gene 209603_at BC003070 GATA3 GATA binding protein 3 0.16 0.016 Zn‐finger TF
209291_at NM_001546 ID4 Inhibitor of DNA binding 4, dominant negative helix‐loop‐helix protein
0.13 < 0.05 Helix‐loop‐helix protein, repressor of cell proliferation
209212_s_at AB030824 KLF5 Kruppel‐like factor 5 (intestinal) 0.13 0.039 Zn‐finger TF 227475_at AI676059 FOXQ1 Forkhead box Q1 0.11 0.015 Member of FOX gene TFs, TGFb mediator 211597_s_at AB059408 HOPX HOP homeobox 0.04 0.006 homeobox TF, tu suppressor
Cell cycle / mitosis
212086_x_at NM_005572 LMNA Lamin A/C 0.53 0.004 nucl. envelope constituent, associated with lipodystrophy
208079_at NM_198433 AURKA Aurora kinase A 0.28 < 0.05 Mitotic spindle organisation 218039_at NM_016359 NUSAP1 Nucleolar and spindle associated protein 1 0.28 < 0.05 DNA and microtubule binding, cytokinesis 201291_s_at NM_001067 TOP2A Topoisomerase II alpha 170 kDa 0.28 < 0.05 fosters cell cycle progression, mitosis, DNA replication. 202870_s_at NM_001255 CDC20 Cell division cycle 20 homolog 0.27 < 0.05 complexes and activates APC, cell cycle controller 202756_s_at NM_002081 GPC1 Glypican 1 0.25 0.002 cell surface heparan sulfate proteoglycan 222608_s_at NM_018685 ANLN Anillin, actin binding protein 0.22 < 0.05 role during cytokinesis in mitosis
230104_s_at NM_015964 TPPP3 Tubulin polymerization‐promoting protein family member 3 0.18 0.043 microtubule bundle formation, centrosome
amplification 209773_s_at NM_001165931 RRM2 Ribonucleotide reductase M2 polypeptide 0.14 < 0.05 Deoxyribonucleotide synthesis, cell proliferation, 33323_i_at X57348 SFN Stratifin 0.04 0.014 p53 effector, PKC inhibitor
Cell survival / apoptosis / p53 signaling
218499_at NM_016542 RP6‐213H19.1 Serine/threonine protein kinase MST4 0.22 < 0.05 GCK group III family of kinases, cleaved by Casp‐3
202504_at NM_012101 TRIM29 Tripartite motif‐containing 29 0.21 0.006 TF, negatively regulates p53222392_x_at AJ251830 PERP PERP, TP53 apoptosis effector 0.17 0.028 p53 regulated gene
209569_x_at NM_014392 D4S234E=P21
DNA segment on chromosome 4 (unique) 234 expressed sequence, brain neuron cytoplasmic protein 1 0.14 0.015 transcriptional target of p53, pro‐apoptotic
206400_at NM_002307 LGALS7 Lectin, galactoside‐binding, soluble, 7 (galectin 7) 0.05 0.005 p53‐induced, pro‐apoptotic
Cluster D: Small Molecule BiochemistryLipid transport / metabolic process 1554833_at NM_018349 MCTP2 Multiple C2 domains, transmembrane 2 5.14 < 0.05 binds Ca in absence of phospholipids, obesity marker!
220331_at NM_006668 CYP46A1 Cytochrome P450, family 46, subfamily A, polypeptide 1 4.14 < 0.05 Monooxygenase, cholesterol turnover , steroid degradation
235978_at AI766029 FABP4 Fatty acid binding protein 4, adipocyte 3.85 0.006 FFA chaperone, intracell. fa transport 49452_at NM_001093.3 ACACB Acetyl‐CoA carboxylase 3.70 0.014 rate‐limiting enzyme in fatty acid oxidation

83
201525_at NM_001647 APOD Apolipoprotein D 2.64 0.012 lipid transporter glycoprotein
222217_s_at NM_024330 SLC27A3 Solute carrier family 27 (fatty acid transporter), member 3
2.17 0.003 Fa transport and acyl‐CoA activation
205769_at NM_003645 SLC27A2 Solute carrier family 27 (fatty acid transporter), member 2 0.28 < 0.05 acyl‐CoA ligase activity
200832_s_at NM_005063 SCD‐1 Stearoyl‐CoA desaturase 0.23 0.039 rate‐limiting enzyme of monounsaturated fatty acid biosynthesis
205220_at NM_006018 GPR109B G protein‐coupled receptor 109B 0.07 0.042 Anti‐lipolytic signalling receptor
Ion transport / metabolic process 203473_at NM_007256 SLCO2B1
Solute carrier organic anion transporter family, member 2B1 1.76 0.031 anion and PGE transporter, lipid uptake
224209_s_at NM_001242505 GDA Guanine deaminase 0.26 < 0.05 guanine deamination, 214414_x_at NM_000558 HBA1 Hemoglobin, alpha 1 0.26 < 0.05 oxygen transport
209921_at NM_014331 SLC7A11 Solute carrier family 7, (cationic amino acid transporter, y+ system) member 11 0.25 < 0.05 cysteine:glutamate antiporter activity
217528_at NM_006536 CLCA2 Chloride channel, calcium activated, family member 2 0.21 0.042 calcium sensitive chloride conductance protein 204675_at NM_001047.2 SRD5A1 Steroid‐5‐alpha‐reductase, alpha polypeptide 1 0.20 < 0.05 steroid degradation enzyme, lipid metabolism 39248_at NM_004925 AQP3 Aquaporin 3 0.17 0.0004 water + glycerol transporter 225516_at NM_003046 SLC7A2 Solute carrier family 7, member 2 0.12 < 0.05 cationic aa transporter 217564_at NM_001122633 CPS1 Carbamoyl‐phosphate synthetase 1, mitochondrial 0.10 0.018 removal of excess urea from cells 214164_x_at NM_001218 CA12 Carbonic anhydrase XII 0.07 0.011 zn metalloenzyme 204437_s_at NM_000802 FOLR1 Folate receptor 1 (adult) 0.04 0.009 transports 5‐methyltetrahydrofolate into cells 217388_s_at NM_001032998 KYNU Kynureninase 0.02 < 0.05 hydrolase , tryptophan metabolism
Glucose transport / metabolic process
201250_s_at NM_006516 SLC2A1 olute carrier family 2 (facilitated glucose transporter), member 1 0.24 0.049 glucose transmembrane transport
202934_at NM_000189 HK2 Hexokinase 2 0.17 < 0.05 allosteric enzyme of glycolysis
Unknown 228977_at AK090664.1 LOC729680 Uncharacterized LOC729680 2.10 < 0.05 unknown
228875_at NM_001085480.2 C6orf189=FAM162B Family with sequence similarity 162, member B 1.90 0.039 unknown
217966_s_at NM_052966.2 FAM129A=GIG39 Family with sequence similarity 129, member A 1.85 0.031 unknown
229518_at NM_052943.3 FAM46B Family with sequence similarity 46, member B 0.29 0.002 unknown 209255_at NM_014997.3 KIAA0265 Kelch domain containing 10 0.27 < 0.05 unknown 238063_at NM_152680.2 TMEM154 Transmembrane protein 154 0.24 < 0.05 unknown
212992_at NM_138420 C14orf78=AHNAK2 AHNAK nucleoprotein 2 0.23 0.009 unknwon
Table 11: Transcript levels of deregulated candidate genes functionally clustered in (A) Inflammatory Response, (B) LEC Adhesion and Migration, (C) LEC growth and Lymphangiogenesis, and (D) Small Molecule Biochemistry. *Shown are ratios of diabetic (dLECs) versus non‐diabetic (ndLECs) LECs probeset expression. †Statistical significance of that ratio is indicated either as P‐value, or as significant result of RVM analysis, which integrates a P‐value ≤ 0.05. ‡Differentially expressed genes were grouped according to their biological functions (GO annotation) and the top differentially expressed genes were ranked in order, based on their mean fold change differences.

84
7.3.2 Verification of LEC specific genes and comparison with other arrays
In order to additionally control and confirm the purity of LEC preparations, we examined for
expression changes of several LEC‐specific marker genes which were shown to be not
significantly altered between dLECs and ndLECs (Table 12). For example, the transcript level of
podoplanin, which was used for FACS sorting had a fold change (FC) of 1.08 (dLEC/ndLEC) and
was considered to be unchanged between the two groups of cells (see also Figure 18 B).
Expression alterations of established LEC transcripts (e.g. CD44, CCL27, CXADR, CXCL14, LYVE1,
PKP1, APP, EDNRB, FABP4, KRT14, MMRN1) (Podgrabinska et al., 2002; Hirakawa et al., 2003;
Wick et al., 2007; Wick et al., 2008) underlined their specific role in lymphatic vessels and
validated the quality of our approach. dLECs further revealed some overlapping gene expression
changes with hypoxic LECs (Irigoyen et al., 2007), and with LECs derived from skin of
lymphedema patients (Ogunbiyi et al., 2011) and lymph node derived LECs (Malhotra et al.,
2012), pointing towards a similar role of these gene candidates in pathological lymphatic
dysfunction. In contrast to our results, recent studies detected downregulation of key lymphatic
markers PROX1 and VEGFR3 in adipose tissue lymphatics in familial human hyperlipidemia
(Horra et al., 2009) as well as murine skin inflammation (Vigl et al., 2011).
Moreover, we compared our data with data sets derived from LECs in pathological situations
associated with diabetes, inflammation, wound healing and lymphatic dysfunction, though only
few studies have investigated the gene expression changes of human endothelial cells in
pathophysiologic situations (St. Croix et al., 2000; Seaman et al., 2007; Clasper et al., 2008;
Ogunbiyi et al., 2011). Here, we traced some overlaps with gene expression changes in hypoxic
LECs (GALNTL2) (Irigoyen et al., 2007). However, compared to another study using an
experimental model of acute post‐surgical lymphedema, nearly no overlap could be detected
(Tabibiazar et al., 2006). Moreover, only a weak overlap could be detected with VEGFC
responsive genes in LECs (Yong et al., 2005). This points towards a specific role of deregulated
genes in LECs in different pathological conditions.
Overall, our findings indicated that LEC‐specific markers are stable in diabetic skin and that their
expression alterations in LVs of other tissue types might depend on the specific
pathophysiological situation and microenvironment.

85
Gene symbol Gene name FC (dLEC/ndLEC) pvalue
ABCA4 Retinal‐specific ATP‐binding cassette
transporter 0.66 0.58
ANGPT2 Angiopoietin‐2 precursor 1.27 0.31KLHL4 Kelch‐like protein 4 0.95 0.89
LYVE1 Lymphatic vessel endothelial
hyaluronan receptor 1 2.19 0.09
PDPN Podoplanin 1.08 0.70THBS4 Thrombospondin 4 precursor 1.88 0.57VEGFR3 Vascular endothelial cell receptor 3 1.08 0.84
Table 12: Transcript levels of LEC specific genes. No significant differences could be seen for LEC‐specific genes between diabetic (dLECs) and non‐diabetic (ndLECs); FC = fold change.
7.3.3 Diabetic LECs exhibited a distinct gene expression profile compared to diabetic BECs
The mRNA expression analysis of BECs derived from the same four diabetic and normoglycemic
patients revealed a completely diverse set of genes differentially regulated in diabetic BECs
(dBECs). Out of the 180 differentially regulated genes in dLECs, only 19 were also altered in
dBECs (Table 13), which represents an overlap of only 10.5%. This result suggested that a highly
specific gene signature was present in dLECs compared to dBECs and indicated that LVs
undertake completely different tasks than BVs in the skin of T2DM patients.

86
AffyID Gene name Gene description FC
(dLEC/ndLEC) FC
(dBEC/ndBEC) Cell adhesion
210809_s_at POSTN periostin, osteoblast
specific factor 0.26 2.52
206032_at DSC3 desmocollin 3 0.25 0.22212063_at CD44 CD44 0.25 0.23
201141_at GPNMB glycoprotein
(transmembrane) nmb 0.18 0.17
212724_at RND3 Rho family GTPase 3 0.18 0.27206400_at LGALS7 galectin 7 0.05 0.18
Angiogenesis, wound healing
210764_s_at CYR61 cysteine‐rich, angiogenic
inducer, 61 2.09 2.15
204855_at SERPINB5 serpin peptidase inhibitor, clade B,
member 5 0.22
0.19
204614_at SERPINB2 serpin peptidase inhibitor, clade B,
member 2 0.19 0.12
Immune response
208747_s_at C1S complement component 1, s subcomponent 2.75 2.86
222484_s_at CXCL14 chemokine (C‐X‐C motif)
ligand 14 0.18 0.13
Cell growth
205014_at FGFBP1 fibroblast growth factor
binding protein 1 0.11 0.28
204379_s_at FGFR3 fibroblast growth factor
receptor 3 0.09 0.30
Transport 39248_at AQP3 aquaporin 3 0.29 0.26
203473_at SLCO2B1 solute carrier organic anion transporter family, member 2B1
1.76 0.26
Transcription
202597_at IRF6 interferon regulatory
factor 6 0.28 0.30
203074_at ANXA8 annexin A8 0.09 0.26Other
226926_at DMKN Dermokine 0.13 0.22205251_at PER2 period homolog 2 0.20 0.34
Table 13: Gene expression overlap of diabetic LECs (dLECs) and diabetic BECs (dBECs) with documented fold change (FC) between diabetic and nondiabetic cell populations.

87
7.3.4 Genes linked to altered lipid transport and metabolism, increased oxidative stress and to the pathogenesis of type 2 diabetes mellitus
First, we identified expression changes of several genes that have already been genetically
linked to T2DM in humans (see Table 14), including haptoglobin (HP, Quaye et al., 2006), JUN
oncogene (Malhotra et al., 2009), tetraspanin 8 (TSPAN8, Zeggini et al., 2008) apolipoprotein d
(APOD, Vijayaraghavan et al., 1994), hematopoietically‐expressed homeobox protein (HHEX,
Sladek et al., 2007; Saxena et al., 2007), lamin A/C (LMNA, Wegner et al., 2007) and fatty acid
binding protein 4 (FABP4, Chan et al., 2010). Genes additionally crucial for lipid metabolic
processes included FABP4 and APOD. APOD is reported to be a genetic marker for T2DM and
obesity (Vijayaraghavan et al., 1994), to be increased in T2DM myotubes and gestational
diabetes (Navarro et al., 2010; Hansen et al., 2004) and to be involved in defense mechanisms
against oxidative stress (Navarro et al., 2010).
The results indicate that established T2D markers prove valid in the lymphatic vessel
compartment and confirmed their importance as potential biomarkers. However, other markers
very characteristic for T2DM, like PPARγ, did not come up in dLECs, highlighting the multi‐
faceted genetic contribution in this disease. Taken together, these alterations presumably confer
altered adhesive, metabolic and inflammatory properties to type 2 diabetes LECs.
FABP4 is highly and specifically expressed in LECs (Ferrell et al., 2008; Wick et al., 2007 and
unpublished result) and is an important mediator of IR in mice (Uysal et al., 2000). Moreover, its
expression in human umbilical venous endothelial cells (HUVECs) is regulated by VEGF (Elmasri
et al., 2009). NOX4 is a major contributor of reactive oxygen species (ROS) production in
endothelial cells (Goettsch et al., 2009) and a mediator of angiogenesis (Ushio‐Fukai, 2007). We
confirmed FABP4, NOX4 and APOD upregulation by quantitative realtime PCR (Figure 27 A) and
reconfirmed FABP4 protein expression by immunofluorescence (Figure 27 B). Elevated
expression levels of FABP4, NOX4 and APOD in dLECs pointed towards a highly disturbed
metabolic status in the skin of T2DM patients. These lipid handling abnormalities, together with
the downregulation of small molecule transporters (examples) show that LVs are compromised
in their function in T2DM.

88
AffyID Accession
no. Gene symbol
Gene name FC
(dLEC/ndLEC) pvalue
208470_s_at P00738 HP Haptoglobin 8.43 0.0209
235978_at AI766029 FABP4 Fatty acid binding
protein 4, adipocyte
3.85 0.006
201525_at P05090 APOD Apolipoprotein D 2.64 0.0115
204689_at Q03014 HHEX Hematopoietically
expressed homeobox
2.14 0.0027
201464_x_at P05412 JUN Jun oncogene 1.65 0.0182212086_x_at P02545 LMNA Lamin A/C 0.53 0.0042203824_at P19075 TSPAN8 Tetraspanin 8 0.17 0.0285
Table 14: Transcript levels of deregulated genes already associated with type 2 diabetes. Transcript levels of dereguated genes which were published to be genetically associated with type 2 diabetes. FC (dLEC/ndLEC) = fold change between diabetic (dLEC) and non‐diabetic (ndLEC) LECs.
Figure 27: Confirmation of altered expression of FABP4, APOD and NOX4 in dLECs by realtime PCR and immunofluorescence. A: Differential expression of FABP4, APOD and NOX4 was confirmed by quantitative realtime PCR using Taqman ® gene expression assays. B: FABP4 expression was additionally confirmed by double‐labeling of human diabetic and non‐diabetic skin with antibodies to FABP4 and podoplanin; Size bar: 20µm.

89
7.3.5 Identification of a gene signature related to wound healing and tissue repair in dLECs
A huge number of transcripts involved in ECM remodeling and adhesion processes indicated a
major effect of T2DM on LEC growth and migration, pointing at ongoing LV morphogenesis
and/or tissue remodeling (Table 15). There were prominent deregulations of a gene set of
proteases (MMP1, MMP2) and protease inhibitors (SERPINs), and of a gene set of transcripts
involved in formation and binding of ECM components and LEC motility (CYR61, GALNTL2) and
wound repair (AQP3).
Two important genes implicated in angiogenesis, tissue remodeling and wound healing are
cysteine rich protein 61 (CYR61) and matrix metalloproteinase 2 (MMP2), which were found to
be upregulated in dLECs. CYR61 is an ECM protein that mediates wound healing (Chen et al.,
2001) and angiogenesis via integrins (Leu et al., 2002). Further, it is implicated in the
pathogenesis of diabetic retinopathy (You et al., 2009) as a downstream target of advanced
glycation endproducts (Hughes et al., 2007). Additionally, MMP2 expression was shown to
stimulate angiogenesis and wound healing (Slyke et al., 2009; Agah et al., 2004). Furthermore,
we detected downregulation of aquaporin 3 (AQP3), a water and glycerol transporter, which is
also important for cutaneous wound healing by reducing epidermal proliferation and migration
(Hara‐Chikuma and Verkman, 2008). Additionally, chemokine ligand 14 (CXCL14, Maerki et al.,
2009) and defensin beta 1 (DEFB1, Schittek et al., 2008) were downregulated in dLECs. Both
have antimicrobial effects, suggesting a function for LECs of diabetic skin in the regulation of
infections (see Table 15).
We confirmed altered expression of AQP3, MMP2 and CYR61 by quantitative realtime PCR
(Figure 28 A). Further, downregulation of AQP3 protein in diabetic LVs was reconfirmed by
immunofluorescent double staining (Figure 28 B), as well as upregulation of CYR61 (Figure 28
C). MMP2 and CYR61 overexpression in dLECs indicated involvement of LVs in increased tissue
remodeling as observed during wound healing processes and increased lymphangiogenesis.
AQP3 expression was not reported in LECs before but its expression in diabetic LECs
additionally points towards an involvement of LVs in dermal healing processes. Moreover, this
gene could represent a new water and glycerol transporter in LECs (Ishibashi et al., 2009).

90
AffyID Accession
no. Gene symbol
Gene name FC
(dLEC/ndLEC) pvalue
222484_s_at O95715 CXCL14 Chemokine (C‐X C motif) ligand 14 0.11 0.0005
210397_at P60022 DEFB1 Defensin, beta 1 0.20 0.0003
201069_at P08253 MMP2 Matrix
metallopeptidase 2 2.14 0.0085
210764_s_at O00622 CYR61 Cysteine rich protein 61
2.09 0.0271
39248_at Q92482 AQP3 Aquaporin 3 0.17 0.0004
Table 15: Transcript levels of genes associated with wound healing and tissue repair. FC (dLEC/ndLEC) = fold change between diabetic (dLEC) and non‐diabetic (ndLEC) LECs.
Figure 28: Confirmation of altered AQP3, MMP2 and CYR61 expression in dLECs by realtime PCR and immunofluorescence. A: Analysis of differential expression by quantitative realtime PCR using Taqman ® gene expression assays. B, C: AQP3 and CYR61 expression was additionally confirmed by double‐labeling of human diabetic and non‐diabetic skin with antibodies to respective antigen and podoplanin; Size bar: 20µm.
Conclusively, The gene alterations might indicate a stage of increased active reparative
mechanism in T2D skin. and show that lvs play an active role in T2D skin disorder.

91
7.3.6 Identification of a gene signature related to increased adhesion of inflammatory cells
A plethora of genes implicated in cell adhesion and inflammatory processes was altered
significantly in dLECs (Table 16). The most upregulated genes included vascular cell adhesion
molecule (VCAM1) and chemokine (CXC‐motif) ligand 10 (CXCL10), while coxsackie and
adenovirus receptor (CXADR) and syndecan 1 (SDC1) were downregulated. These genes are
mainly responsible for the regulation of immune cell traffcking. VCAM1 was previously reported
to be expressed in LECs upon TNFα stimulation and to be an important regulator of DC adhesion
and migration in vitro and in vivo (Johnson et al., 2006). CXCL10 seems to be a crucial chemokine
in T‐cell and macrophage infiltration (Heller et al., 2006; Dufour et al., 2002) and implicated in
resolution of inflammation (Rahman et al., 2010). CXADR interacts with junctional adhesion
molecule 1 to regulate monocyte, neutrophil and T‐cell migration across junctional connections
(Luissint et al., 2008; Zen et al., 2005) and was previously reported to be specifically expressed
on LECs (Vigl et al., 2009). SDC1 has major tasks in inhibiting leukocyte adhesion to the
endothelium (Götte et al., 2002) and is reported to be downregulated by TNFα (Kainulainen et
al., 1996).
AffyID Accession
no. Gene symbol
Gene name FC (dLEC/ndLEC) pvalue
204533_at P02778 CXCL10 Chemokine (C‐X‐C motif) ligand
10 5.16 0.0093
203868_s_at P19320 VCAM1 Vascular cell adhesion molecule 1
4.23 0.0013
207955_at Q9Y4X3 CCL27 Chemokine (C‐C motif) ligand 27
0.06 0.0058
226374_at P78310 CXADR Coxsackie virus and adenovirus
receptor 0.21 0.0080
201287_s_at P18827 SDC1 Syndecan 1 0.12 0.0165
Table 16: Transcript levels of genes linked to increased adhesion of inflammatory cells. FC (dLEC/ndLEC) = fold change between diabetic (dLEC) and non‐diabetic (ndLEC) LECs.
Differential gene expression of VCAM1, CXCL10, CXADR and SDC1 was confirmed by realtime
PCR and showed that expression ratios matched those retrieved from microarray analysis
(Figure 29 A). Differential gene expression of CXCL10 and CXADR was further approved on
protein level by double‐immunofluorescence stainings of human skin (Figure 29 B and C).
Conclusively, differential expression of VCAM1, CXCL10, CXADR and SDC1 suggested increased

92
adhesion of inflammatory cells to the lymphatic endothelium in the skin of T2DM patients,
possibly as a result of an increased pro‐inflammatory milieu.
Figure 29: Confirmation of altered VCAM1, CXCL10, CXADR and SDC1 expression in dLECs by realtime PCR and immunofluorescence. A: Differential expression of VCAM‐1, CXCL10, CXADR and SDC1 was confirmed by quantitative realtime PCR using Taqman ® gene expression assays. B, C: Differential expression of CXCL10 and CXADR was reconfirmed by double‐labeling of human diabetic and non‐diabetic skin with antibodies to CXCL10, CXADR and podoplanin; Size bar: 20µm.

93
7.3.7 Deregulated genes associated with cellular host defense
The prominent inflammation‐related gene cluster revealed alterations of processes related to
cellular defense, response to infection, chemotaxis/leukocyte adhesion and tissue repair/wound
healing (Table 17).
A group of acute phase and antimicrobial defense response factors contained transcripts of well
described extracellular factors, which previously have been detected as important inflammatory
markers in plasma, lymph fluid or wound tissue. Of note, we detected upregulation of transcripts
for HP (haptoglobin), PTX3 (pentraxin), C1S (complement 1), SERPING1 (serpin peptidase
inhibitor, clade G (C1 inhibitor), member 1) and APP (amyloid precursor protein), and
downregulation of GAGE1 (G antigen 1), DEFB1 (defensin, beta 1), S100A8 (S100 calcium binding
protein A8) and FGG (fibrinogen gamma chain). Further, innate immune response genes KLRC1
(killer cell lectin‐like receptor subfamily C, member 1), KLRK1 (killer cell lectin‐like receptor
subfamily K, member 1) and KYNU (kynureninase) were downregulated. Transcripts for
extracellular inflammatory regulators WNT5A (wingless‐type MMTV integration site family,
member 5A), AREG (amphiregulin) and IL1RN (interleukin 1 receptor antagonist) were
deregulated.
Interestingly, a plethora of membrane‐associated receptors involved in proper inflammatory
signaling, like IL6R (interleukin 6 receptor), IL1R2 (interleukin 1 receptor 2), IL13RA
(interleukin 13 receptor A), and SLC7A2 (solute carrier family 7 (cationic amino acid
transporter, y+ system), member 2) were downregulated. Further, intracellular stress factors
NOX4 (NADPH oxidase 4), HSPA1A (heat shock 70kDa protein 1A), and CTSB (cathepsin B) were
upregulated, while components of arachidonic acid uptake and metabolism (SLCO2B1, PLA2G4A,
PTGS2) were downregulated. These results suggested an extensive involvement of dLECs in skin
infection and host defense.
Many of the transcripts regulated in dLECs have been previously identified in whole tissue
lysates of chronic human skin inflammation, venous ulcers and wounds (de Jongh et al., 2005;
Charles et al., 2008; Roy et al., 2008; Grice et al., 2010), and the emergence of these gene
products might be a specific contribution of lymphatic vessels. We identified overlapping
deregulation of some transcripts described in atopic dermatitis (AREG, CSTA, DEFB1 and S100A8;
de Jongh et al., 2005), for psoriasis, (including CXCL10 and S100A8; Guttman‐Yassky et al., 2008),
nonhealing venous ulcers, (including AQP3 and SFN; Charles et al., 2008), in wound
inflammation, including CXCL10, CYR61, JUN, PTX3, SOCS3 and VCAM1 (Roy et al., 2008), and in
the diabetic wound microbiome, including CXCL10, FABP4, CD55, DEFB1 and S100A8 (Grice et al.,
2010). Several of the secreted factors (HB, C1S, FGG, HP, PTX3) have been previously detected as
inflammatory markers in plasma, lymph fluid or wound tissue. Additionally, some, but generally

94
low overlap was detected when comparing our gene list with a murine skin inflammation model,
including VCAM1, FGFR3, CXCL10 and ADAMTS5 (Vigl et al., 2011).
Downregulation of important inflammatory response genes in dLECs, indicating a prolonged
period of inflammatory disorder in the skin that leads to hampered immune modulatory
functions of dermal lymphatics. Further, these genes indicate that LVs play an active role in skin
wounds and infections by contributing to pathogen modulation. Altogether, these gene
candidates might highlight functional pathways that are involved in recurrent skin infections.
In summary, the dLEC transcriptome highlights the processes, which are also seen on a
morphological level. The findings underline the importance of LVs and LECs in immunological
processes and lipid metabolism and suggest that skin LVs react actively on the multiple,
metabolic as well as inflammatory interstitial burden.
The results in the ‘inflammatory cluster’ indicate a prolonged period of inflammatory disorder in
the skin that leads to hampered immune modulatory functions of dermal lymphatics. The large
number of transcripts involved in ECM remodeling and adhesion processes indicates a major
effect of T2D on LEC growth and migration, pointing at ongoing lymphatic vessel remodeling,
supporting the finding of increased lymphangiogenesis in T2DM skin. Further, a huge number of
positive and negative regulators of cell growth, migration, proliferation and survival and
suggested an activation of cellular differentiation and survival processes in LECs in T2D skin.
Additionally, LECs might deal with the lipid handling abnormalities, as many small molecule
transporters were downregulated, showing that LVs are compromised in their function,
regarding lipid, water and electrolyte transport.
Moreover, the increased expression of TNFα also contributes to dysregulation of genes, mainly
implicated in the clusters ‘cell adhesion’ and ‘inflammatory response’ (see next section).

95
AffyID Accession
no. Gene symbol
Gene name FC
(dLEC/ndLEC) pvalue
206157_at P26022 PTX3 Pentraxin‐related
gene 2.80 0.0004
208747_s_at P09871 C1S Transcribed locus,component 1, s subcomponent
2.76 <0.05
200799_at P08107 HSPA1A Heat shock protein A1A
1.88 0.0106
200838_at P07858 CTSB Cathepsin B 1.78 0.0029
203473_at O94956 SLCO2B1
Solute carrier organic
anion transporter family,
member 2B1
1.76 0.0313
200986_at P05155 SERPING1
Serpin peptidase inhibitor, clade G (C1 inhibitor), member 1
1.71 0.0039
200602_at P05067 APP Amyloid precursor protein
1.54 0.0285
205821_at P26718 KLRK1
Killer cell lectin‐like receptor subfamily C, member 1
0.26 <0.05
204971_at P01040 CSTA Cystatin A 0.05 0.0118236843_at Q9NPH5 NOX4 NADPH oxidase 4 4.81 0.0255
213425_at P41221 WNT5A
Wingless‐type MMTV integration
site family, member 5A
3.64 0.0004
204597_x_at P52823 STC1 Stanniocalcin 1 0.21 < 0.05
206785_s_at Q3KQS7 KLRC2
Killer cell lectin‐like receptor subfamily C, member 1
0.26 <0.05
210397_at P60022 DEFB1 Defensin, beta 1 0.20 0.0003
204748_at P35354 PTGS2 prostaglandin G/Hsynthase and cyclooxygenase
0.17 0.0165
202917_s_at P05109 S100A8 S100 calcium binding protein
A8 0.14 0.0713
212657_s_at P18510 IL1RN Interleukin 1 receptor antagonist
0.08 0.0969
Table 17: Transcript levels of genes associated with cellular host defense. Transcript levels of dereguated genes which are implicated in the process of cellular and host defense. FC (dLEC/ndLEC) = fold change between diabetic (dLEC) and non‐diabetic (ndLEC) LECs.

96
7.4 TNFαinduced effects on LEC behavior
In the final part of my thesis, I aimed to develop a mechanistic link between the observed
morphological changes of T2DM skin, i.e. the enhanced LV and macrophage number, and the
specific gene expression profile of dLECs. In order to establish this link between skin lymphatic
morphology and the dLEC transcriptome, we were looking for a factor possibly bridging the gap
between these two findings.
7.4.1 TNFα responsiveness of LEC genes in vitro
Due to the finding that the highly increased macrophage number in diabetic skin was capable of
producing a local pro‐inflammatory milieu via TNFα, we aimed at investigating whether in vitro
TNFα stimulation of LECs could recapitulate the differential gene expression observed by our
transcriptomal analysis of dLECs versus ndLECs ex vivo. TNFα treatment induced upregulation
of CXCL10, VCAM1 and CYR61 (Figure 30) and downregulation of SDC1, CXADR and AQP3
(Figure 31) as it was identified by the transcriptomal analysis of ex vivo isolated LECs from
T2DM patients. Additionally, treatment with an inhibitory TNFα antibody reversed TNFα
induced expression changes of genes and suggested that differential gene expressions are highly
specific for TNFα. However, expression of FABP4, GALNTL2 and APOD was downregulated,
which is in contrast to the array data (Figure 32). Moreover, no effect could be found on
expression of MMP2 and NOX4 (Figure 33).
We conclude from these data that increased TNFα levels, mainly produced by infiltrating
macrophages, might directly influence the expression of some genes in microvascular LECs.
Hence, we identified TNFα‐driven gene expression as one signaling pathway leading to
differential gene expression in dLECs versus ndLECs. However, TNFα‐driven differential
expression of other genes did not match array data. Therefore, we hypothesize that not only one
predominant but rather the interplay of several phenomena, including epigenetic,
transcriptional, or microRNA‐mediated mechanisms, is crucial for the diabetic metabolic status
and responsible for observed gene expression changes of dLECs versus ndLECs.

97
Figure 30: Upregulation of CXCL10, VCAM1 and CYR61 gene expression of cultured LECs byTNFα stimulation. Primary dermal LECs were cultured in EBM‐2/0.5% FCS and stimulated with10ng/ml TNFα for 24 hours (with or without TNFα inhibitor). TNFα treatment of primary culturedLECs perfectly recapitulated upregulation of CXCL10, VCAM1 and CYR61 as found by microarrayanalysis.
Figure 31: Downregulation of CXADR, SDC1 and AQP3 gene expression of cultured LECs by TNFα stimulation. Primary dermal LECs were cultured in EBM‐2/0.5% FCS and stimulated with 10ng/ml TNFα for 24 hours (with or without TNFα inhibitor). TNFα treatment of primary cultured LECs perfectly recapitulated downregulation of SDC1, CXADR and AQP3 as found by microarray analysis.

98
Figure 32: Downregulation of FABP4, GALNTL2 and APOD gene expression of cultured LECsby TNFα stimulation. Primary dermal LECs were cultured in EBM‐2/0.5% FCSand stimulatedwith 10ng/ml TNFα for 24 hours (with or without TNFα inhibitor). Downregulation of FABP4,GALNTL2 and APOD expression by TNFα treatment is contrary to array results.
Figure 33: No change of MMP2 and NOX4 gene expression of cultured LECs by TNFα stimulation. Primary dermal LECs were cultured in EBM‐2/0.5% FCS and stimulated with 10ng/ml TNFα for 24 hours (with or without TNFα inhibitor). No effect of TNFα could be found on MMP2 and NOX4 expression.

99
7.4.1 Increased migration of LECs upon TNFα stimulation
Interestingly, expression of several genes integrated in the clusters of ‘cell adhesion’ and
‘inflammatory response’ were regulated by TNF‐α and the in vitro stimulation experiments
matched the array data. Therefore, the effect of TNFα on LEC behavior was studied more
detailed.
LVs are able to react to an inflammatory milieu by increasing lymphangiogenesis (Cueni and
Detmar, 2008). TNFα is a pro‐inflammatory cytokine which can stimulate EC migration and
proliferation (Gao et al., 2002). In order to analyze the effect of TNFα on the behaviour of human
primary LECs, we performed an in vitro scratch wound healing assay with and without TNFα
stimulation. Stimulation of LECs seeded into 24‐well plates with 10ng/ml TNFα for 24 hours
significantly increased LEC migration and induced faster wound closure in a scratch wound
assay (Figure 34, p‐value = 0.007).
This data indicated that TNFα might lead to lymph vessel remodeling or enhanced lymph vessel
growth (Baluk et al., 2009) and further corroborated a potential link between increased TNFα
levels and increased LV density in the skin of T2DM patients.
7.4.2 Macrophage adhesion to LECs is increased by TNFα stimulation
Molecular mechanisms which regulate the entry of inflammatory cells from the blood into the
lymphoid tissues during their circulation in the body are well characterized (Miyasaka and
Tanaka, 2004; von Andrian and Mempel, 2003). In contrast, much less is known about the exit
mechanisms of these cells, especially of macrophages, from the surrounding tissues into afferent
lymphatics. However, migration of professional antigen‐presenting cells like lymphocytes, DCs
and macrophages is essential for controlling immune responses (Angeli and Randolph, 2006).
Increased TNFα levels were found in T2DM patients as well as T2DM mouse models.
Additionally, it was shown that endothelial interactions with immune cells are increased during
hyperglycemia (Algenstaedt et al., 2003).

100
Therefore, we tested whether TNFα exerted effects on the interaction between LECs and
macrophages. In vitro stimulation of primary LECs with TNFα led to a massively increased
adhesion of macrophages (p‐value < 0.001). This was highly specific for TNFα as this effect could
be reduced to the amount of adherent macrophages of unstimulated LECs by additional
treatment with an inhibitory anti‐TNFα antibody (Figure 35).
Conclusively, we could show increased macrophage adhesion to LEC monolayers after TNFα
stimulation, indicating massive upregulation of adhesion molecules on LECs responsible for
macrophage adhesion. Similar results were shown for DCs, adhering to and transmigrating
through TNFα‐stimulated LECs, which was dependent on VCAM1 expression (which was also
upregulated in dLECs compared to ndLECs) in vitro and in vivo (Johnson et al., 2006). This fact
indicats that macrophages might undergo enhanced lymphatic traffcking in T2DM.
Figure 34: Increased migration of LECs after TNFα stimulation. Primary dermal LECs werecultured in EBM‐2/0.5% FCS and stimulated with or without 10ng/ml TNFα for 24 hours. Anartificial wound was made in each well. Representative images at timepoints t=0h, t=12h andt=24h and quantification of measured closure of wound area are shown.

101
Figure 35: Adhesion of macrophages to primary LECs in vitro. Primary dermal LECs werestarved overnight in EBM‐2/0.5% FCS and stimulated with or without 10ng/ml TNFα for 24hours (with or without TNFα inhibitor). Increased macrophage adhesion to LECs was detectedupon TNFα treatment, which was reversible with an anti‐TNFα antibody; Size bar: 100µm.

102
7.5 CXC motif chemokine 10 (CXCL10) expression and function in LECs
The array results indicated a prominent upregulation of CXCL10 in dLECs (Table 16), and we
could recapitulate strong upregulation of CXCL10 expression in LECs by TNFa stimulation
(Figure 29). CXCL10 is a small cytokine and is also called interferon gamma‐induced protein 10
(IP‐10). It has fundamental roles in effector T‐cell generation and function (Dufour et al., 2002).
Moreover, it is suggested to be involved in the invasion of immune cells into the brain, thereby
contributing to the pathogenesis of multiple sclerosis (Salmaggi et al., 2002). Additionally,
CXCL10 contributes to airway inflammation in asthma (Medoff et al., 2002) and its upregulation
is accompanied by a delayed resolution of local inflammation (Rahman et al., 2010). CXCL10 is
angiostatic and was shown to lead to apoptosis and dissociation of newly formed BVs (Bodnar et
al., 2009, 2006). In diabetes, CXCL10 leads to beta cell destruction via interaction with TLR4
(Schulthess et al., 2009). Here, we aimed to analyze the functional implications of CXCL10
expression in LECs.
7.5.1 CXCL10 is upregulated and secreted by LECs upon TNFα stimulation
As shown by realtime PCR, CXCL10 was not expressed in unstimulated but dramatically
upregulated in TNFα‐stimulated LECs (see Figure 30). This upregulation could be further
confirmed by Western blotting analysis on a protein level (Figure 36 A). Moreover, we could
show that LECs secrete this chemokine upon stimulation with TNFα using ELISA and Western
blotting of supernatants (Figure 36 B).

103
Figure 36: Expression and secretion of CXCL10 in LECs upon TNFα stimulation. Primary dermal LECs were starved overnight in EBM‐2/0.5% FCS and stimulated with or without 10ng/ml TNFα for 24 hours (with or without TNFα inhibitor). Cells were lysed in Laemmli sample buffer and respective supernatants were collected. A: CXCL10 expression in LECs was checked using western blotting. GAPDH was used as loading control. CXCL10 is not visible in unstimulated but massively upregulated in TNFα‐stimulated LECs. B: Supernatants of stimulated and unstimulated LECs were checked for CXCL10 secretion by ELISA and Western blotting showing secretion of this chemokine by TNFα‐stimulated LECs.
7.5.2 CXCL10 mediates macrophage adhesion to LECs
Due to the fact that CXCL10 was upregulated and secreted upon TNFα treatment, and that TNFα
significantly increased adhesion of macrophages to the LEC monolayers, we hypothesized that
CXCL10 could be one factor responsible for the massively increased macrophage adhesion to
LECs. Therefore, we stimulated primary LECs with 10ng/ml TNFα, with or without an inhibitory
antibody to CXCL10. A massively increased adhesion of THP‐1 macrophages to LECs was found
upon TNFα treatment, which was almost completely abrogated by addition of an inhibitory
CXCL10 antibody (Figure 37, p‐value = 0.04). Conversely, treatment of LECs with TNFα plus an
inhibitory antibody to VCAM1 – which was also upregulated by TNFα treatment and shown to
be responsible for DC adhesion in LECs (Johnson et al., 2006) ‐ did not affect macrophage
adhesion to the lymphatic endothelium (Figure 38, p‐value = 0.65). This suggests that CXCL10 is
an important mediator of macrophage adhesion to lymphatics, possibly only in an inflammatory
condition when TNFα levels are increased and, hence, lead to its secretion by LECs.

104
Figure 37: CXCL10 is responsible for macrophage adhesion to lymphatic endothelialmonolayer. Primary dermal LECs were starved overnight in EBM‐2/0.5% FCS and stimulated withor without 10ng/ml TNFα for 24 hours with or without an inhibitory antibody to CXCL10. Increasedmacrophage adhesion to LECs could be found upon TNFα treatment which was reversed by CXCL10inhibitory antibody; Size bar: 100µm.

105
Figure 38: VCAM1 is dispensable for macrophage adhesion to lymphatic endothelial monolayer. Primary dermal LECs were starved overnight in EBM‐2/0.5% FCS and stimulatedwith or without 10ng/ml TNFα for 24 hours with or without an inhibitory antibody to VCAM1.VCAM1 inhibitory antibody did not change macrophage adhesion to LECs; Size bar: 100µm.

106
7.5.3 CXCL10 induces chemotaxis of macrophages
Having shown that CXCL10 is secreted by LECs upon TNFα stimulation and that CXCL10 is in part
responsible for macrophage adhesion, we asked whether CXCL10 secreted from stimulated LECs
had a chemotactic effect on macrophages. Therefore, we used the supernatants of LECs
stimulated with or without TNFα ‐ with addition of inhibitory antibodies to TNFα and CXCL10 ‐
and performed an agarose spot assay (Wiggins and Rappoport, 2010). As shown in Figure 39,
there was increased migration of macrophages into the agarose spots which contained TNFα (C)
compared to spots lacking TNFα (B). Increased migration induced by TNFα could be significantly
inhibited by an anti‐TNFα antibody (D). Similarly, when using a specific inhibitory antibody to
CXCL10, macrophage migration into the agarose spots could be reduced to the same extent as
with the anti‐TNFα antibody at both timepoints (p‐value = 0.008, E).
Conclusively, CXCL10 was identified as a factor regulated by TNFα in LECs. Our findings suggest
that this chemokine could be responsible for the chemotaxis of macrophages towards LVs.
Additionally, it could be possible that the interaction between lymphatic endothelium and other
inflammatory cells are affected by CXCL10, e.g. T‐cells and DCs, as well as the interaction of LVs
with tumor cells. However, additional experiments by using a recombinant form of CXCL10 are
needed to confirm observed effects on adhesion and chemotaxis of macrophages to LECs.

107
Figure 39: Secreted CXCL10 induces chemotaxis of macrophages. Primary dermal LECs werestarved overnight in EBM‐2/0.5% FCS and stimulated with or without 10ng/ml TNFα for 24hours plus an inhibitory antibody to TNFα and CXCL10. Supernatants were collected andconcentrated for use in an agarose spot assay to measure chemotaxis of macrophages. Migrationarea was evaluated after 24 and 48 hours, respectively. Representative pictures andquantification of migration area (in µm2) shows an increased chemotaxis of macrophages intospots containing TNFα (C) which was specifically inhibited by an inhibitory antibody againstTNFα (D) and CXCL10 (E). PBS (A) and supernatant of LECs not stimulated with TNFα (B) wereused as controls.

108
7.5.4 CXCL10 enhances LECtransmigration of macrophages
Similar to CCL27 in LECs, which was shown to be responsible for the transmigration of
CCR10+T‐lymphocytes (Wick et al., 2008), we hypothesized that CXCL10 could also confer
transmigration of THP‐1 macrophages. Therefore, we performed a transwell migration assay by
culturing LECs on the underside of fibronectin‐coated transwell filters. After having grown to
Figure 40: CXCL10 confers macrophage transmigration. Dermal LECs were grown toconfluence on the underside of fibronectin‐coated transwell filters and stimulated with 10ng/mlTNFα for 24 hours with or without an inhibitory antibody to CXCL10 to show involvement ofCXCL10 in macrophage transmigration. After putting the macrophages into the upper chamber,fluorescence of transmigrated macrophages was measured in the lower chamber after one (A),three (B) and six hours (C). As a control for LEC monolayer permeability, measurement of FITC‐dextran permeability of conuent monolayers showed no difference when stimulated withdifferent substances (D). Conclusively, TNFα stimulation led to enhanced macrophagetransmigration, which could be specifically diminished by an inhibitory CXCL10 antibody.

109
confluence, LEC monolayers were stimulated with TNFα with or without a specific inhibitory
CXCL10 antibody. TNFα significantly enhanced transmigration of macrophages after one, three
and six hours, which was blocked by addition of a specific inhibitory anti‐TNFα antibody. When
adding a blocking anti‐CXCL10 antibody, transmigration of macrophages was significantly
reduced at the 3 hours stimulation timepoint, but only slightly after one and six hours (see
Figure 40 A‐C). The increase of transmigrated macrophage number was not due to increased
permeability of the confluent LEC monolayers, as permeability for FITC‐dextran was unchanged
(Figure 40 D). This indicated that CXCL10 is substantially involved in mediating transmigration
of macrophages through lymphatic endothelium. CXCL10 might regulate transmigration via
binding to CXCR3 expressed on THP‐1 macrophages, which is the counterreceptor for CXCL10
(Singh et al., 2007). Similar to TNFα, CXCL10 could be an important, yet unrecognized regulator
of immune cell trafficking in the context of persistent T2DM skin inflammation.
In summary, we could show that CXCL10 was highly upregulated in T2DM skin, possibly due to
higher levels of TNFα, as it could not be detected in non‐diabetic LECs or LECs not treated with
TNFα. Further, CXCL10 was shown to be secreted by LECs after TNFα‐stimulation. CXCL10
derived from LECs might be crucial not only for macrophage adhesion but also for chemotaxis
and transmigration in a pro‐inflammatory milieu.

110
7.6 Characterization of Fatty acid binding protein 4 (FABP4) expression and function in LECs
Among the metabolically altered genes in dLECs, we detected strong upregulation of FABP4
(Table 14). Fatty acid binding proteins represent a family of lipid chaperones, which facilitate
the transport of fatty acids to different compartments of the cell, including lipid droplets,
endoplasmatic reticulum, nucleus, cytoplasm, peroxisomes or mitochondria (Furuhashi and
Hotamisligil, 2008). Additionally, they are implicated in integrating lipid signaling and
inflammatory pathways. Their expression is highly conserved as they are expressed in different
species from Drosophila melanogaster and Caenorhabditis elegans up to mice and humans
(Makowski and Hotamisligil, 2004). Fatty acid binding protein 4 (FABP4), also called adipocyte
protein 2 (aP2) is mainly expressed in adipocytes, macrophages and DCs. Its expression is highly
regulated by fatty acids, PPARγ‐agonists and insulin (Furuhashi and Hotamisligil, 2008). Its
importance in the pathogenesis of T2DM and IR was demonstrated in Fabp4 knockout mice
(Hotamisligil et al., 1996). FABP4 expression has not been reported in LECs before, although
hints exist that this gene could be important for LEC behavior, as it was reported as a potential
candidate gene involved in lymphedema (Ferrell et al., 2008).

111
7.6.1 FABP4 is specifically expressed in lymphatic endothelial cells
FABP4 was upregulated in dLECs versus ndLECs. Additionally, we found it exclusively expressed
in LECs compared to BECs. This differential expression could be confirmed Western blotting
analysis (Figure 41 A). Additionally, FABP4 could be detected by immunofluorescence in
podoplanin‐positive LECs (Figure 41 B). Moreover, FABP4 co‐localized with podoplanin‐positive
LVs in human skin (Figure 41 C), whereas on a consecutive section, blood vessels stained with
endoglyx‐1 do not show FABP4 expression (Figure 41 D).
Figure 41: FABP4 is specifically expressed in LECs compared to BECs. A: Protein expression analysis of FABP4 in LECs and BECs is shown. GAPDH was used as a loading control. B: Immunofluorescent stainings of LECs with antibodies to podoplanin and FABP4 showed the strong FABP4 expression of LECs. C: Double staining of human skin with antibodies to podoplanin and FABP4 showed FABP4 expression by LVs. D: Double staining of a consecutive section using antibodies to podoplanin and endoglyx‐1, which is highly specific for BVs. This confirms that FABP4 is not expressed on BVs of human skin. Size bar: 20µm.

112
7.6.2 FABP4 expression could be specifically knocked down in LECs
To analyze whether FABP4 knockdown has an impact on cell behavior, LECs were transfected
with FABP4‐specific siRNA and scrambled siRNA as control using RNAiFect. Efficient knockdown
of FABP4 expression was shown by Western blot analysis (Figure 42 A) as well as
immunofluorescent stainings (Figure 42 B).
Figure 42: siRNAmediated knockdown of FABP4 in LECs. LECs were transfected with FABP4‐specific or scrambled siRNA using RNAiFect. Knockdown of FABP4 expression was analyzed byWestern blotting (A) and immunofluorescence stainings (B).

113
7.6.3 FABP4 regulates LECs proliferation
Elmasri et al. (2009) showed that FABP4 expression is induced by VEGF stimulation in HUVECs
and that it is involved in the regulation of HUVEC proliferation. In order to analyze the specific
role of FABP4 in LECs, we comparatively determined the proliferation rate of scrambled versus
FABP4 siRNA‐transfected LECs. As shown in Figure 43, proliferation of LECs was significantly
reduced in FABP4 siRNA‐transfected LECs after 96 and 144 hours (p‐value = 0.04) compared to
LECs transfected with scrambled control siRNA. However, in contrast to the findings of Elmasri
et al. (2009), we did not find induction of FABP4 expression by VEGFs (Figure 44). This suggests
that besides VEGFs other, yet unidentified factors are responsible for highly specific FABP4
expression in LECs and LVs compared to BECs and BVs.
Figure 44: FABP4 expression is not upregulated by lymphangiogenic factors. Cell lysates ofLECs stimulated with VEGF‐A, VEGF‐C and VEGF‐D were analyzed for protein expression ofFABP4. No differences of FABP4 expression were observed. GAPDH was used as a loadingcontrol.
Figure 43: FABP4 regulates LEC proliferation. LECs were transfected with FABP4‐specific or scrambled siRNA using RNAiFect and cells were counted at respective timepoints.

114
7.6.4 FABP4 expression increases LEC permeability
Using these siRNA‐mediated transfection tools, we investigated whether manipulation of FABP4
expression has an impact on LEC‐LEC adhesion and on the stability of inter‐lymphatic
endothelial cell junctions by measuring FITC‐dextran permeability and transendothelial electric
resistance (TEER) of a LEC monolayer. Reduced permeability for FITC‐dextran was measured
when FABP4 expression was knocked down in LECs (Figure 45 A). In concordance with the
reduced permeability, we found increased TEER in FABP4 knockdown LECs compared to
scrambled siRNA transfected cells (Figure 45 B). These data indicate that FABP4, besides its well
established function as a fatty acid transporter in adipocytes, seems to exert important basic
cellular features in LECs.
7.6.5 FABP4 expression regulates PPARγ expression in LECs
It has been shown that peroxisome proliferator activated receptor gamma (PPARγ) regulate
FABP4 expression in adipocytes and fibroblasts (Furuhashi and Hotamisligil, 2008). Hence, we
wanted to know if this concept also applies to LECs. We transfected LECs with FABP4‐ and
PPARγ‐specific siRNAs. As shown in Figure 46, knockdown of FABP4 led to a strong decrease of
Figure 45: FABP4 regulates permeability of LEC monolayers. LECs were seeded onfibronectin (FN) coated transwell filters and grown to confluence. A: FITC‐dextran diffusion wasmeasured using an ELISA reader at λ=485‐530nm in transwells with LEC monolayers transfectedwith FABP4‐specific and scrambled siRNA and in FN coated wells only. B: Transendothelialelectric resistance (TEER) was measured using a manual electrode.

115
FABP4 expression and similarly also PPARγ expression in LECs (A). Conversely, PPARγ
knockdown did not influence FABP4 expression in LECs (B).
This could indicate that FABP4 expression in LECs is driven by a rather solid differentiation‐
dependent transcriptional regulation, while PPARγ is sensitive to the presence of FABP4.
7.6.6 Possible interactions of FABP4 with PPARγ
FABPs serve as shuttle proteins for fatty acids in order to activate PPARs (Wolfrum, 2007),
which then, in concert with retinoic acid receptors, activate so‐called peroxisome‐proliferator‐
responsive element (PPREs) in genes. FABP4 was shown to directly interact with PPARγ in COS‐
7 cells (Tan et al., 2002). By functional analysis of PPRE motifs in genes of fatty acid‐binding
proteins, a direct binding of PPARγ/RXR heterodimers to PPREs in the FABP4 promoter was
demonstrated (Schachtrup et al., 2004). By this way, FABPs activate their own transcription,
regulating a positive feedback‐loop. Moreover, it was shown that treatment with the PPARγ
agonist rosiglitazone upregulated the expression of FABP4 and PPARγ (Cabré et al., 2007; Allen
et al., 2006) and a nuclear translocation of FABP4 occured (Ayers et al., 2007; Gillilan et al.,
2007), thereby possibly stimulating the interaction of FABP4 and PPARγ.
Due to the fact that FABP4 regulated PPARγ expression in LECs (Figure 46), we were interested
to know whether these two genes were interacting directly with each other in LECs. Therefore,
we performed co‐immunoprecipitations with anti‐FABP4 and anti‐PPARγ antibodies,
Figure 46: FABP4 regulates PPARγ expression in LECs but not vice versa. 5x104 LECs wereseeded into 24 well plates and transfected with FABP4‐/PPARγ‐specific siRNA as well asscrambled siRNA using RNAiFect transfection reagent. PPARγ (A) and FABP4 (B) proteinexpression was checked usingWestern blot analysis. GAPDH protein expression served as aloading control.

116
respectively from whole LEC lysates. As shown in Figure 47, we could not detect any direct
interaction between FABP4 and PPARγ in either of the two immunoprecipitates. This finding
does not completely exclude an interaction of these two molecules in LECs. Rather, low amounts
of starting material, too low expression of PPARγ in LECs or too weak or too short interaction
between these proteins could be the limitations of our practical approach.
In order to see whether PPARγ protein binds to PPREs in the promotor region of FABP4 gene,
we performed ChIP assays as previously described (Gal‐Yam et al., 2008).
Figure 47: CoImmunoprecipitations of FABP4 and PPARγ. Co‐immunoprecipitation, usinganti‐FABP4 or anti‐PPARγ antibodies, from the lysates of LECs stimulated with 20µM ofrosiglitazone. The precipitates were analyzed by immunoblotting. Western blots indicate thatproteins are not interacting with each other.
Figure 48: Chromatin immunoprecipitations of PPARγ to show potential interactions withPPREs in the FABP4 promotor region. Chromatin immunoprecipitations of LEC lysatesstimulated with or without 20µM rosiglitatzone for 24 hours. Binding of PPARγ to PPREs waschecked using SybrGreen quantitative real‐time PCR and specific primer pairs. MYT1 primerwas used as negative control.

117
In all of the six potential PPRE sites, except for site 6, no significant enrichment in site
amplification by quantitative PCR could be detected between unstimulated and rosiglitazone‐
stimulated LECs (Figure 48). Site 6 represents a PPRE in the core promotor region of FABP4
very near to the 5'‐UTR and the start codon of the FABP4 gene, suggesting that PPARγ
preferentially binds to this PPRE of endothelial FABP4. The primer for myelin transcription
factor 1 (MYT1) served as a negative control.
In summary, we could show that FABP4 is significantly increased in diabetic LECs. It could serve
as a new specific marker for LECs, as it is not expressed in BECs and BVs of human skin.
Moreover, it significantly influences proliferation and permeability of LECs and influences
PPARγ expression after knockdown. FABP4 could represent one important connector gene
between lipid metabolism and lymphatic vessel functioning, as it was shown that LV dysfunction
lead to lymphedema, which is associated with increased formation of adipose tissue (Rockson,
2001) and increased obesity in mice (Harvey et al., 2005).

118
8. Conclusions and Future Perspectives
A final model for involvement of dermal lymphatic vessels in type 2 diabetes
1. Morphological analysis
During this thesis work, a comprehensive analysis of LVs and LECs in the skin of type 2 diabetic
patients was performed. A morphological as well as molecular characterization is presented. A
great merit is that this work boldly analyzed human tissue specimens, and it addressed a less
studied vascular system in diabetes. While endothelial dysfunction of BVs is a well‐studied
complication in T2DM, research data on how lymphatics may be altered and involved in disease
pathogenesis is barely known so far. However, skin complications associated with diabetes are
not only related to BV but additionally to LV dysfunction. LV malfunctioning may lead to wound
healing defects (Saaristo et al., 2006), increased risk for local infections (Rockson, 2001) and
formation of adipose tissue (Harvey et al., 2005).
Increased lymphatic vessel density was observed in cholesterol‐rich atherosclerotic lesions
(Kholova et al., 2010) and chronic venous insufficiency ulcers (Fernandez et al., 2011) of human
patients, suggesting causal relationships between these diseases. In contrast to newly grown
carcinoma‐associated lymphatic vessels (Vainionpää et al., 2007), we could not detect laminin
and type IV collagen expression alterations, which was consistent with unaltered lymphatic
vessel diameter and absence of hyperplasia. Although a 'so‐called' diabetic lymphangiopathy
was reported earlier (Kaufmann et al., 1980; Ohkuma, 1979), no phenotypical changes of LVs
could be found in the skin of T2DM patients, regardless of their size. We conclude that mostly
due to a completely different assembly of the vessel wall (no regular BM, no SMC coverage),
observed changes are not similar to BV changes in T2DM. Additionally, intraluminal LV pressure
is significantly lower and lymph flow rate is approximately 100‐500 times less than blood flow
rate (Swartz, 2001). However, if intraluminal pressure and lymph flow rate is changed in a
similar way than in BVs in type 2 diabetics (Calles‐Escandon and Cipolla, 2001), this would be an
interesting features to measure, although this is very difficult to conduct in humans.

119
Significantly increased LV and macrophage density was found in the skin of T2DM patients.
Although controversial to previously published studies (Maruyama et al., 2007; Saaristo et al.,
2006), we suggest that this could be an intercorrelating feature, where macrophages regulate LV
density via the expression of VEGFs (Machnik et al., 2009; Maruyama et al., 2005) and possibly
also via TNFα, which has pro‐migratory and proliferative activity. It needs further investigations
to answer the question why there is increased macrophage infiltration in the skin of type 2
diabetic patients. Is it related to ischemia, to hyperglycemia or is it a result of reduced
efferocytosis due to a dysfunction of macrophages which in turn could sustain local
inflammation?
2. The dLEC transcriptome
Extensive bioinformatical and literature analysis of microarray data retrieved a long list of genes
which were dissected into different functional pathways using Ingenuity Pathway Analysis
(IPA). This led to the establishment of four overrepresented themes, comprising (Cluster A)
defense response and inflammation, (Cluster B) tissue remodeling and cell motility, (Cluster C)
lymphangiogenesis and cell fate regulation and (Cluster D) lipid handling and small molecule
transport.
We did not trace downregulation of key lymphatic differentiation markers, as was observed in
obesity and inflammation (Horra et al., 2009; Vigl et al., 2011), and we did not trace deregulation
of transcripts for lymphatic valve and junction proteins (Hämmerling et al., 2006), though
lymphatic vessels were postulated to contribute to obesity due to disrupted integrity (Harvey et
al., 2005). Rather, the overlaps with hypoxic LECs and LECs derived from skin of lymphedema
patients (Irigoyen et al., 2007; Ogunbiyi et al., 2011) emphasized a role of these candidates in
pathological lymphatic dysfunction. Further, overlaps with transcriptomes of whole tissue
lysates from nonhealing venous ulcers (Charles et al., 2008), wound inflammation (Roy et al.,
2008) and diabetic wound microbiome (Grice et al., 2010) might indicate that these specifically
derive from LECs. Therefore, we concluded that lymphatic vessels show stable LEC identity in
type 2 diabetic skin, while they manifest alterations that highlight the specific
pathophysiological microenvironment.
The functional gene sets underlined the emergence of enhanced lymphatic vessel density.
During capillary morphogenesis, LECs have to be released from their quiescent phenotype,
which is triggered by dissolution of the basement membrane and complex changes of their
migratory behaviour. Mature LECs scarcely proliferate and must re‐enter the cell cycle during
growth of new vessels from pre‐existing ones. The huge number of positive and negative
regulators of cell growth, migration, proliferation and survival suggested an activation of cellular
differentiation and survival processes in LECs in T2DM skin. The transcriptional downregulation

120
of GTPase‐activating molecules might indicate relief of a quiescent LEC proliferation state, as it
was described recently for Ras GTPase‐activating RASA1 (Lapinski et al., 2012). dLECs revealed
decrease of p53‐mediated downstream effectors, hence extending their proliferation potential.
Accordingly, p53‐deficient mice show enhanced lymphangiogenesis (Ruddell et al., 2008), and
silencing of p53 signaling improved diabetic wound healing (Nguyen et al., 2010). However, the
master‐regulators dictating the concerted gene suppressions of several gene clusters remain
unknown, suggesting involvement of epigenetic, transcriptional, or microRNA‐mediated
mechanisms. Recent findings point towards such regulatory traits in diabetic endothelial cells
(Pirola et al., 2011; Cayrol et al., 2007; Zampetaki et al., 2010).
3. Mechanistic analysis that brings all findings together
In T2DM, the interstitial space of the dermis contains an overload of fatty acids, glucose, proteins
and adipogenic factors derived from the blood circulation (Tammela et al., 2010). Despite absent
regulation of adipokines or their cognate receptors in dLECs, enhanced lipid levels per se might
contribute to pathological alterations of lymphatic vessels. Dyslipidemia was associated with
dysfunctional lymphatic vessels that lead to chronic inflammatory disorders of the skin (Lim et
al., 2009). Hence, incomplete clearance of interstitial fluid and its contents might lead to
phenotypic changes similar to lymphedema like increased collagen deposition, fibrotic
alterations, and dermal swelling (Alitalo, 2011). Type 2 diabetic skin specimens showed obvious
thickening (own observation), pointing at such alterations. This might be added to the obviously
damaged skin barrier‐immune axis and underlines the paramount importance of initial
lymphatics for maintenance of skin homeostasis.
Though macrophages are essential for physiological wound healing (Mahdavian Delavary et al.,
2011), in type 2 diabetes, their increased influx has been correlated with impaired wound
healing (Wetzler et al., 2000), characterized by expression of pro‐inflammatory cytokines,
especially TNF‐α (Khanna et al., 2010). Here, we show that macrophage infiltration and TNF‐α
production is associated with human dermal pathology as well. Activated macrophages have
been recognized to directly contribute to de novo lymphangiogenesis (Kerjaschki, 2005) by (1)
production of lymphangiogenic factors and (2) conversion into LECs. However, we detected
relatively low enhancement of VEGF‐C levels, which was not significantly different between
diabetic and non‐diabetic skin, corresponding to a poor overlap with VEGF‐C responsive genes
in LECs (Yong et al., 2005), which suggested a minor contribution to the increased lymph vessel
count. Pathologic lymphangiogenesis might be driven by additional mediators such as PDGF‐BB,
HIF or FGF‐2 (Alitalo, 2011), though we did not trace altered expression of these factors or their
cognate receptors in dLECs. Rather, we provide the first confirmation of TNF‐α‐induced gene
deregulation in human LECs in vivo that is strongly correlated with a pro‐migratory LEC

121
phenotype. Accordingly, enhanced TNF‐α levels were shown to drive lymph vessel remodeling
(Baluk et al., 2009).
Besides indications from murine studies (Tammela & Alitalo, 2010), in humans, enhanced lymph
vessel density was correlated with accelerated chronic wound healing (Labanaris et al., 2009)
and restoration of gut homeostasis in Crohn’s disease (von der Weid et al., 2011). However,
several reports indicate that inflammatory‐driven lymphangiogenesis leads to dysfunctional
vessel formation showing reduced lymph drainage capacity (Tammela & Alitalo, 2010). The
active recruitment of macrophages to dLECs via CXCL10 chemotaxis might be indicative of such
impeded clearance, but could also be the prerequisite to lymph vessel integration. In a LPS‐
driven peritonitis model, enhanced numbers of macrophages were closely attached to newly
formed inflammatory lymphatic vessels, then directly incorporating into these (Kim et al., 2009).
It is tempting to speculate that macrophages in human patients´ skin are involved in an
analogous mechanism of lymphatic vessel expansion. This exaggerated macrophage entrapment
and de novo lymph vessel formation could lead to decreased tissue fluid, lipid and immune cell
drainage and, finally, persistent inflammation that altogether hinder skin regeneration. The
question whether exaggerated lymph vessel formation is beneficial for the skin pathology in
type 2 diabetes, has to be explored.
To summarize, we revealed that dLECs contribute to chronic inflammation, decreased defense of
infections, leukocyte recruitment, tissue remodeling and severely altered homeostasis of T2DM
skin. Figure 49 summarizes the effects evoking the altered dLEC properties, including increased
load of metabolites and macrophage influx over time, which lead to molecular alterations in
dermal LECs. LECs in T2DM skin show an unprotected, activated phenotype characterized by
increased inflammatory, migratory, lipid handling and lymphangiogenic capacity and apoptosis
resistance. A paracrine cross‐talk between macrophages and dLECs leads to increased
macrophage recruitment which might be the source of enhanced lymph vessel expansion.
Specifically, TNF‐α is a key mediator of cross talk between proinflammatory macrophages and
LECs. TNF‐α
Conclusively, the analysis of lymphatic endothelial cells from different anatomic sites and
pathological situations allows a better understanding of the mechanisms involved in lymphatic
vascular growth, function and repair, depending on the specific pathophysiological
microenvironment. Transcriptomal comparison led to the identification of a distinct gene
expression profile that characterized lymphatic vascular changes in T2DM on a molecular level,
suggesting that LECs are undergoing major changes during T2DM, including changes in vessel
permeability, lipid transport, proliferation and vessel remodelling. Importantly, the array data
underlined our morphological findings. We could show a correlation between the gene cluster
‘inflammation’ with the increased macrophage infiltration and TNFα expression. Additionally,

122
mediated gene expression alterations in LECs lead to further macrophage recruitment, hence
reinforcing lymph vessel propagation and chronic inflammation.
Figure 49: Importance of lymphatic vessels in type 2 diabetic skin and the attempt of establishing a model showing their contribution, involvement and alterations in the skin of type 2 diabetic patients.
dLECs are characterized by increased tissue regeneration efforts, reflected by differentially
regulated genes asscociated with wound healing and tissue remodelling as well as the fact that
we found increased lymphangiogenesis in T2DM skin. This finding also underlined the fact that
we detected an increased number of genes implicated in lymphangiogenesis as well as increased

123
survival. Moreover, it is suggested that LECs are directly and actively involved in lipid and small
molecule transport, highlighted by the differentially regulated genes in the cluster ‘lipid handling
and small molecule biochemistry’.
The data suggest that skin lymphatic vessels react actively on the multiple, metabolic as well as
inflammatory interstitial burden. Inflammatory reaction is a prominent event, as well as
cytoskeletal regulatory pathways that lead to extensive lymphatic vessel expansion and
remodelling in T2DM. Overall, dLECs seem to be actively involved in the skin alterations in the
advanced stage of T2DM skin disease. Moreover, the dLEC transcriptome could include
important marker genes for T2DM, which will lead to alternative therapies as well as future
candidate genes for regulating leukocyte adhesion and migration and potentially be crucial for
clearance of tissue inflammation in type 2 diabetic patients.

124
References Abtahian, F., Guerriero, A., Sebzda, E., Lu, M.‐M., Zhou, R., Mocsai, A., Myers, E. E., Huang, B., Jackson, D. G., Ferrari, V. A., Tybulewicz, V., Lowell, C. A., Lepore, J. J., Koretzky, G. A., and Kahn, M. L. (2003). Regulation of blood and lymphatic vascular separation by signaling proteins slp‐76 and syk. Science, 299(5604):247‐251. Agah, A., Kyriakides, T. R., Letrondo, N., Björkblom, B., and Bornstein, P. (2004). Thrombospondin 2 levels are increased in aged mice: consequences for cutaneous wound healing and angiogenesis. Matrix Biol, 22(7):539‐547. Alberti, K. G. and Zimmet, P. Z. (1998). Definition, diagnosis and classification of diabetes mellitus and its complications. part 1: diagnosis and classification of diabetes mellitus provisional report of a who consultation. Diabet Med, 15(7):539‐553. Alexander JS, Chaitanya GV, Grisham MB, Boktor M. (2010). Emerging roles of lymphatics in inflammatory bowel disease. Ann N Y Acad Sci, 1207 Suppl 1:E75‐85. Algenstaedt, P., Schaefer, C., Biermann, T., Hamann, A., Schwarzloh, B., Greten, H., Rther, W., and Hansen‐Algenstaedt, N. (2003). Microvascular alterations in diabetic mice correlate with level of hyperglycemia. Diabetes, 52(2):542‐549. Alitalo K. (2011). The lymphatic vasculature in disease. Nat Med, 17(11):1371‐1380. Alitalo, K., Tammela, T., and Petrova, T. V. (2005). Lymphangiogenesis in development and human disease. Nature, 438(7070):946‐953. Alizadeh, A. A., Eisen, M. B., Davis, R. E., Ma, C., Lossos, I. S., Rosenwald, A., Boldrick, J. C., Sabet, H., Tran, T., Yu, X., Powell, J. I., Yang, L., Marti, G. E., Moore, T., Hudson, J., Lu, L., Lewis, D. B., Tibshirani, R., Sherlock, G., Chan, W. C., Greiner, T. C., Weisenburger, D. D., Armitage, J. O., Warnke, R., Levy, R., Wilson, W., Grever, M. R., Byrd, J. C., Botstein, D., Brown, P. O., and Staudt, L. M. (2000). Distinct types of diffuse large b‐cell lymphoma identified by gene expression profiling. Nature, 403(6769):503‐511. Allen, T., Zhang, F., Moodie, S. A., Clemens, L. E., Smith, A., Gregoire, F., Bell, A., Muscat, G. E. O., and Gustafson, T. A. (2006). Halofenate is a selective peroxisome proliferator‐activated receptor gamma modulator with antidiabetic activity. Diabetes, 55(9):2523‐2533. Altshuler, D., Hirschhorn, J. N., Klannemark, M., Lindgren, C. M., Vohl, M. C., Nemesh, J., Lane, C. R., Schaffner, S. F., Bolk, S., Brewer, C., Tuomi, T., Gaudet, D., Hudson, T. J., Daly, M., Groop, L., and Lander, E. S. (2000). The common ppargamma pro12ala polymorphism is associated with decreased risk of type 2 diabetes. Nat Genet, 26(1):76‐80. Amatschek, S., Kriehuber, E., Bauer, W., Reininger, B., Meraner, P., Wolpl, A., Schweifer, N., Haslinger, C., Stingl, G., and Maurer, D. (2007). Blood and lymphatic endothelial cell specific differentiation programs are stringently controlled by the tissue environment. Blood, 109(11):4777‐4785. Angeli, V. and Randolph, G. J. (2006). Inflammation, lymphatic function, and dendritic cell migration. Lymphat Res Biol, 4(4):217‐228. Aselli, G. (1627). De lacteibus sive lacteis venis, quarto vasorum mesarai corum genere novo invento mediolani, milano. Asselot‐Chapel, C., Borchiellini, C., Labat‐Robert, J., and Kern, P. (1996). Expression of laminin and type iv collagen by basement membrane‐producing ehs tumors in streptozotocin‐induced diabetic mice: in vivo modulation by low‐molecular‐weight heparin fragments. Biochem Pharmacol, 52(11):1695‐1701. Association, A. D. (2007). Standards of medical care in diabetes. Diabetes Care, 30 Suppl 1:S4‐S41. Association, A. D. (2005). Diagnosis and classification of diabetes mellitus. Diabetes Care, 28 Suppl 1:S37{‐42. Ayers, S. D., Nedrow, K. L., Gillilan, R. E., and Noy, N. (2007). Continuous nucleocytoplasmic shuttling underlies transcriptional activation of ppargamma by fabp4. Biochemistry, 46(23):6744‐6752.

125
Bäckhed, F., Crawford, P. A., O'Donnell, D., and Gordon, J. I. (2007). Postnatal lymphatic partitioning from the blood vasculature in the small intestine requires fasting‐induced adipose factor. Proc Natl Acad Sci U S A, 104(2):606‐611. Baldwin, M. E., Halford, M. M., Roufail, S., Williams, R. A., Hibbs, M. L., Grail, D., Kubo, H., Stacker, S. A., and Achen, M. G. (2005). Vascular endothelial growth factor d is dispensable for development of the lymphatic system. Mol Cell Biol, 25(6):2441‐2449. Balfour, J. A. and Plosker, G. L. (1999). Rosiglitazone. Drugs, 57(6):921‐930; Discussion 931‐932. Baluk, P., Tammela, T., Ator, E., Lyubynska, N., Achen, M. G., Hicklin, D. J., Jeltsch, M., Petrova, T. V., Pytowski, B., Stacker, S. A., Ylä‐Herttuala, S., Jackson, D. G., Alitalo, K., and McDonald, D. M. (2005). Pathogenesis of persistent lymphatic vessel hyperplasia in chronic airway inflammation. J Clin Invest, 115(2):247‐257. Baluk, P., Yao, L.‐C., Feng, J., Romano, T., Jung, S. S., Schreiter, J. L., Yan, L., Shealy, D. J., and McDonald, D. M. (2009). Tnf‐alpha drives remodeling of blood vessels and lymphatics in sustained airway inflammation in mice. J Clin Invest, 119(10):2954‐2964. Banerji, S., Ni, J., Wang, S. X., Clasper, S., Su, J., Tammi, R., Jones, M., and Jackson, D. G. (1999). Lyve‐1, a new homologue of the cd44 glycoprotein, is a lymph‐specific receptor for hyaluronan. J Cell Biol, 144(4):789‐801. Bazigou, E., Xie, S., Chen, C., Weston, A., Miura, N., Sorokin, L., Adams, R., Muro, A. F., Sheppard, D., and Makinen, T. (2009). Integrin‐alpha9 is required for fibronectin matrix assembly during lymphatic valve morphogenesis. Dev Cell, 17(2):175‐186. Belperio JA, Keane MP, Arenberg DA, Addison CL, Ehlert JE, Burdick MD, Strieter RM. (2000). CXC chemokines in angiogenesis. J Leukoc Biol, 68(1):1‐8. Bergman, R. N. and Ader, M. (2000). Free fatty acids and pathogenesis of type 2 diabetes mellitus. Trends Endocrinol Metab, 11(9):351‐356. Bergqvist, L., Strand, S. E., and Persson, B. R. (1983). Particle sizing and biokinetics of interstitial lymphoscintigraphic agents. Semin Nucl Med, 13(1):9‐19. Bertozzi, C. C., Schmaier, A. A., Mericko, P., Hess, P. R., Zou, Z., Chen, M., Chen, C.‐Y., Xu, B., min Lu, M., Zhou, D., Sebzda, E., Santore, M. T., Merianos, D. J., Stadtfeld, M., Flake, A. W., Graf, T., Skoda, R., Maltzman, J. S., Koretzky, G. A., and Kahn, M. L. (2010). Platelets regulate lymphatic vascular development through clec‐2‐slp‐76 signaling. Blood, 116(4):661‐670. Bittner, M., Meltzer, P., Chen, Y., Jiang, Y., Seftor, E., Hendrix, M., Radmacher, M., Simon, R., Yakhini, Z., Ben‐Dor, A., Sampas, N., Dougherty, E., Wang, E., Marincola, F., Gooden, C., Lueders, J., Glatfelter, A., Pollock, P., Carpten, J., Gillanders, E., Leja, D., Dietrich, K., Beaudry, C., Berens, M., Alberts, D., and Sondak, V. (2000). Molecular classification of cutaneous malignant melanoma by gene expression profiling. Nature, 406(6795):536‐540. Bodnar, R. J., Yates, C. C., Rodgers, M. E., Du, X., andWells, A. (2009). Ip‐10 induces dissociation of newly formed blood vessels. J Cell Sci, 122(Pt 12):2064‐2077. Bodnar, R. J., Yates, C. C., and Wells, A. (2006). Ip‐10 blocks vascular endothelial growth factor‐induced endothelial cell motility and tube formation via inhibition of calpain. Circ Res, 98(5):617‐625. Bonifati, C. and Ameglio, F. (1999). Cytokines in psoriasis. Int J Dermatol, 38(4):241‐251. Breiteneder‐Geleff, S., Matsui, K., Soleiman, A., Meraner, P., Poczewski, H., Kalt, R., Schachner, G., and Kerjaschki, D. (1997). Podoplanin, novel 43‐kd membrane protein of glomerular epithelial cells, is down‐regulated in puromycin nephrosis. Am J Pathol, 151(4):1141‐1152. Breiteneder‐Geleff, S., Soleiman, A., Horvat, R., Amann, G., Kowalski, H., and Kerjaschki, D. (1999). Podoplanin –a specific marker for lymphatic endothelium expressed in angiosarcoma. Verh Dtsch Ges Pathol, 83:270‐275. Bridenbaugh, E. A., Gashev, A. A., and Zawieja, D. C. (2003). Lymphatic muscle: a review of contractile function. Lymphat Res Biol, 1(2):147‐158. Brown, P. O. and Botstein, D. (1999). Exploring the new world of the genome with dna microarrays. Nat Genet, 21(1 Suppl):33‐37. Brownlee, M. (2001). Biochemistry and molecular cell biology of diabetic complications. Nature, 414(6865):813‐820.

126
Cabré, A., Lázaro, I., Girona, J., Manzanares, J. M., Marimón, F., Plana, N., Heras, M., and Masana, L. (2007). Fatty acid binding protein 4 is increased in metabolic syndrome and with thiazolidinedione treatment in diabetic patients. Atherosclerosis, 195(1):e150‐e158. Calcutt, N. A., Cooper, M. E., Kern, T. S., and Schmidt, A. M. (2009). Therapies for hyperglycaemia‐induced diabetic complications: from animal models to clinical trials. Nat Rev Drug Discov, 8(5):417‐429. Calles‐Escandon, J. and Cipolla, M. (2001). Diabetes and endothelial dysfunction: a clinical perspective. Endocr Rev, 22(1):36‐52. Cayrol C, Lacroix C, Mathe C, Ecochard V, Ceribelli M, Loreau E, Lazar V, Dessen P, Mantovani R, Aguilar L, Girard JP. (2007). The THAP‐zinc finger protein THAP1 regulates endothelial cell proliferation through modulation of pRB/E2F cell‐cycle target genes. Blood, 109(2):584‐594. Chan, K.‐H. K., Song, Y., Hsu, Y.‐H., You, N.‐C. Y., Tinker, L. F., and Liu, S. (2010). Common genetic variants in fatty acid‐binding protein‐4 (fabp4) and clinical diabetes risk in the women's health initiative observational study. Obesity (Silver Spring). Charles CA, Tomic‐Canic M, Vincek V, Nassiri M, Stojadinovic O, Eaglstein WH, Kirsner RS. (2008). A gene signature of nonhealing venous ulcers: potential diagnostic markers. J Am Acad Dermatol, 59(5):758‐771. Chen, C. C., Mo, F. E., and Lau, L. F. (2001). The angiogenic factor cyr61 activates a genetic program for wound healing in human skin fibroblasts. J Biol Chem, 276(50):47329‐47337. Chia, S., Qadan, M., Newton, R., Ludlam, C. A., Fox, K. A. A., and Newby, D. E. (2003). Intra‐arterial tumor necrosis factor‐alpha impairs endothelium‐dependent vasodilatation and stimulates local tissue plasminogen activator release in humans. Arterioscler Thromb Vasc Biol, 23(4):695‐701. Chiasson, J. L., Gomis, R., Hanefeld, M., Josse, R. G., Karasik, A., and Laakso, M. (1998). The STOP‐NIDDM trial: an international study on the efficacy of an alpha glucosidase inhibitor to prevent type 2 diabetes in a population with impaired glucose tolerance: rationale, design, and preliminary screening data. study to prevent non‐insulin‐dependent diabetes mellitus. Diabetes Care, 21(10):1720‐1725. Christian, S., Ahorn, H., Novatchkova, M., Garin‐Chesa, P., Park, J. E., Weber, G., Eisenhaber, F., Rettig, W. J., and Lenter, M. C. (2001). Molecular cloning and characterization of endoglyx‐1, an emilin‐like multisubunit glycoprotein of vascular endothelium. J Biol Chem, 276(51):48588‐48595. Clasper S, Royston D, Baban D, Cao Y, Ewers S, Butz S, Vestweber D, Jackson DG. (2008). A novel gene expression profile in lymphatics associated with tumor growth and nodal metastasis. Cancer Res, 15;68(18):7293‐7303. Cole, K. A., Krizman, D. B., and Emmert‐Buck, M. R. (1999). The genetics of cancer ‐ a 3d model. Nat Genet, 21(1 Suppl):38‐41. Correia, S., Carvalho, C., Santos, M. S., Sei ca, R., Oliveira, C. R., and Moreira, P. I. (2008). Mechanisms of action of metformin in type 2 diabetes and associated complications: an overview. Mini Rev Med Chem, 8(13):1343‐1354. Cueni, L. N., Chen, L., Zhang, H., Marino, D., Huggenberger, R., Alitalo, A., Bianchi, R., and Detmar, M. (2010a). Podoplanin‐fc reduces lymphatic vessel formation in vitro and in vivo and causes disseminated intravascular coagulation when transgenically expressed in the skin. Blood 18, 116(20):4376‐4384. Cueni, L. N. and Detmar, M. (2008). The lymphatic system in health and disease. Lymphat Res Biol, 6(3‐4):109‐122. Cueni, L. N., Hegyi, I., Shin, J. W., Albinger‐Hegyi, A., Gruber, S., Kunstfeld, R., Moch, H., and Detmar, M. (2010b). Tumor lymphangiogenesis and metastasis to lymph nodes induced by cancer cell expression of podoplanin. Am J Pathol, 177(2):1004‐1016. Danussi, C., Spessotto, P., Petrucco, A., Wassermann, B., Sabatelli, P., Montesi, M., Doliana, R., Bressan, G. M., and Colombatti, A. (2008). Emilin1 deficiency causes structural and functional defects of lymphatic vasculature. Mol Cell Biol, 28(12):4026‐4039. Deeb, S. S., Fajas, L., Nemoto, M., Pihlajamäki, J., Mykkänen, L., Kuusisto, J., Laakso, M., Fujimoto, W., and Auwerx, J. (1998). A pro12ala substitution in ppargamma2 associated with decreased receptor activity, lower body mass index and improved insulin sensitivity. Nat Genet, 20(3):284‐287. de Jongh GJ, Zeeuwen PL, Kucharekova M, Pfundt R, van der Valk PG, Blokx W, Dogan A, Hiemstra PS, van de Kerkhof PC, Schalkwijk J. (2005). High expression levels of keratinocyte antimicrobial proteins in psoriasis compared with atopic dermatitis. J Invest Dermatol, 125(6):1163‐1173.

127
Dixon, J. B., Raghunathan, S., and Swartz, M. A. (2009). A tissue‐engineered model of the intestinal lacteal for evaluating lipid transport by lymphatics. Biotechnol Bioeng, 103(6):1224‐1235. Draghici, S., Khatri, P., Eklund, A. C., and Szallasi, Z. (2006). Reliability and reproducibility issues in dna microarray measurements. Trends Genet, 22(2):101‐109. Du, X. L., Edelstein, D., Rossetti, L., Fantus, I. G., Goldberg, H., Ziyadeh, F., Wu, J., and Brownlee, M. (2000). Hyperglycemia‐induced mitochondrial superoxide overproduction activates the hexosamine pathway and induces plasminogen activator inhibitor‐1 expression by increasing sp1 glycosylation. Proc Natl Acad Sci U S A, 97(22):12222‐12226. Duby, J. J., Campbell, R. K., Setter, S. M., White, J. R., and Rasmussen, K. A. (2004). Diabetic neuropathy: an intensive review. Am J Health Syst Pharm, 61(2):160‐173. Dufour, J. H., Dziejman, M., Liu, M. T., Leung, J. H., Lane, T. E., and Luster, A. D. (2002). Ifn‐gamma‐inducible protein 10 (ip‐10; cxcl10)‐deficient mice reveal a role for ip‐10 in effector T cell generation and trafficking. J Immunol, 168(7):3195‐3204. Dumont, D. J., Jussila, L., Taipale, J., Lymboussaki, A., Mustonen, T., Pajusola, K., Breitman, M., and Alitalo, K. (1998). Cardiovascular failure in mouse embryos deficient in VEGF receptor‐3. Science, 282(5390):946‐949. Dunworth, W. P., Fritz‐Six, K. L., and Caron, K. M. (2008). Adrenomedullin stabilizes the lymphatic endothelial barrier in vitro and in vivo. Peptides, 29(12):2243‐2249. Eberl, G., Marmon, S., Sunshine, M.‐J., Rennert, P. D., Choi, Y., and Littman, D. R. (2004). An essential function for the nuclear receptor rorgamma(t) in the generation of fetal lymphoid tissue inducer cells. Nat Immunol, 5(1):64‐73. Elmasri, H., Karaaslan, C., Teper, Y., Ghelfi, E., Weng, M., Ince, T. A., Kozakewich, H., Bischoff,J., and Cataltepe, S. (2009). Fatty acid binding protein 4 is a target of vegf and a regulator of cell proliferation in endothelial cells. FASEB J, 23(11):3865‐3873. Eming, S. A., Krieg, T., and Davidson, J. M. (2007). Inflammation in wound repair: molecular and cellular mechanisms. J Invest Dermatol, 127(3):514‐525. Enholm B, Paavonen K, Ristimäki A, Kumar V, Gunji Y, Klefstrom J, Kivinen L, Laiho M, Olofsson B, Joukov V, Eriksson U, Alitalo K. (1997). Comparison of VEGF, VEGF‐B, VEGF‐C and Ang‐1 mRNA regulation by serum, growth factors, oncoproteins and hypoxia. Oncogene, 14(20):2475‐2483. Fan, J. B., Chen, X., Halushka, M. K., Berno, A., Huang, X., Ryder, T., Lipshutz, R. J., Lockhart, D. J., and Chakravarti, A. (2000). Parallel genotyping of human snps using generic high‐density oligonucleotide tag arrays. Genome Res, 10(6):853‐860. Fernandez AP, Miteva M, Roberts B, Ricotti C, Rouhani P, Romanelli P. (2011). Histopathologic analysis of dermal lymphatic alterations in chronic venous insufficiency ulcers using D2‐40. J Am Acad Dermatol, 64(6):1123.e1‐12. Ferrell, R. E., Kimak, M. A., Lawrence, E. C., and Finegold, D. N. (2008). Candidate gene analysis in primary lymphedema. Lymphat Res Biol, 6(2):69‐76. Förster, R., Davalos‐Misslitz, A. C., and Rot, A. (2008). Ccr7 and its ligands: balancing immunity and tolerance. Nat Rev Immunol, 8(5):362‐371. Fox, C. S., Coady, S., Sorlie, P. D., Levy, D., Meigs, J. B., D'Agostino, R. B., Wilson, P. W. F., and Savage, P. J. (2004). Trends in cardiovascular complications of diabetes. JAMA, 292(20):2495‐2499. Franois, M., Caprini, A., Hosking, B., Orsenigo, F., Wilhelm, D., Browne, C., Paavonen, K., Karnezis, T., Shayan, R., Downes, M., Davidson, T., Tutt, D., Cheah, K. S. E., Stacker, S. A., Muscat, G. E. O., Achen, M. G., Dejana, E., and Koopman, P. (2008). Sox18 induces development of the lymphatic vasculature in mice. Nature, 456(7222):643‐647. Fritsch, H. and K uhnel, W. (2001). Taschenatlas der Anatomie in 3 Bänden, Teil 2: Innere Organe. Thieme. Fritz‐Six, K. L., Dunworth, W. P., Li, M., and Caron, K. M. (2008). Adrenomedullin signaling is necessary for murine lymphatic vascular development. J Clin Invest, 118(1):40‐50. Fu, J., Gerhardt, H., McDaniel, J. M., Xia, B., Liu, X., Ivanciu, L., Ny, A., Hermans, K., Silasi‐Mansat, R., McGee, S., Nye, E., Ju, T., Ramirez, M. I., Carmeliet, P., Cummings, R. D., Lupu, F., and Xia, L. (2008). Endothelial cell o‐glycan deficiency causes blood/lymphatic misconnections and consequent fatty liver disease in mice. J Clin Invest, 118(11):3725‐3737.

128
Fujita N, Takagi S. (2012). The impact of Aggrus/podoplanin on platelet aggregation and tumor metastasis. J Biochem, [Epub ahead of print] Furuhashi, M. and Hotamisligil, G. S. (2008). Fatty acid‐binding proteins: role in metabolic diseases and potential as drug targets. Nat Rev Drug Discov, 7(6):489‐503. Gal‐Yam, E. N., Egger, G., Iniguez, L., Holster, H., Einarsson, S., Zhang, X., Lin, J. C., Liang, G., Jones, P. A., and Tanay, A. (2008). Frequent switching of polycomb repressive marks and DNA hypermethylation in the pc3 prostate cancer cell line. Proc Natl Acad Sci U S A, 105(35):12979‐12984. Gale, N. W., Prevo, R., Espinosa, J., Ferguson, D. J., Dominguez, M. G., Yancopoulos, G. D., Thurston, G., and Jackson, D. G. (2007). Normal lymphatic development and function in mice deficient for the lymphatic hyaluronan receptor lyve‐1. Mol Cell Biol, 27(2):595‐604. Gale, N. W., Thurston, G., Hackett, S. F., Renard, R., Wang, Q., McClain, J., Martin, C., Witte, C., Witte, M. H., Jackson, D., Suri, C., Campochiaro, P. A., Wiegand, S. J., and Yancopoulos, G. D. (2002). Angiopoietin‐2 is required for postnatal angiogenesis and lymphatic patterning, and only the latter role is rescued by angiopoietin‐1. Dev Cell, 3(3):411‐423. Galiano RD, Tepper OM, Pelo CR, Bhatt KA, Callaghan M, Bastidas N, Bunting S, Steinmetz HG, Gurtner GC. (2004). Topical vascular endothelial growth factor accelerates diabetic wound healing through increased angiogenesis and by mobilizing and recruiting bone marrow‐derived cells. Am J Pathol, 164(6):1935‐1947. Gao, B., Saba, T. M., and Tsan, M.‐F. (2002). Role of alpha(v)beta(3)‐integrin in tnf‐alphainduced endothelial cell migration. Am J Physiol Cell Physiol, 283(4):C1196‐C1205. Gerli, R., Solito, R., Weber, E., and Aglianó, M. (2000). Specific adhesion molecules bind anchoring filaments and endothelial cells in human skin initial lymphatics. Lymphology, 33(4):148‐157. Gillilan, R. E., Ayers, S. D., and Noy, N. (2007). Structural basis for activation of fatty acid‐binding protein 4. J Mol Biol, 372(5):1246‐1260. Gnepp, D. R. and Green, F. H. (1979). Scanning electron microscopy of collecting lymphatic vessels and their comparison to arteries and veins. Scan Electron Microsc, 3(3):756‐762. Goettsch, C., Goettsch, W., Muller, G., Seebach, J., Schnittler, H.‐J., and Morawietz, H. (2009). Nox4 overexpression activates reactive oxygen species and p38 MAPK in human endothelial cells. Biochem Biophys Res Commun, 380(2):355‐360. Goldberg, R. B. (2003). Cardiovascular disease in patients who have diabetes. Cardiol Clin, 21(3):399‐413, vii. Goova MT, Li J, Kislinger T, Qu W, Lu Y, Bucciarelli LG, Nowygrod S, Wolf BM, Caliste X, Yan SF, Stern DM, Schmidt AM. (2001). Blockade of receptor for advanced glycation end‐products restores effective wound healing in diabetic mice. Am J Pathol, 159(2):513‐525. Goren, I., Müller, E., Schiefelbein, D., Christen, U., Pfeilschifter, J., Mühl, H., and Frank, S. (2007). Systemic anti‐tnfalpha treatment restores diabetes‐impaired skin repair in ob/ob mice by inactivation of macrophages. J Invest Dermatol, 127(9):2259‐2267. Götte, M., Joussen, A. M., Klein, C., Andre, P., Wagner, D. D., Hinkes, M. T., Kirchhof, B., Adamis, A. P., and Bernfield, M. (2002). Role of syndecan‐1 in leukocyte‐endothelial interactions in the ocular vasculature. Invest Ophthalmol Vis Sci, 43(4):1135‐1141. Grainger, R. M. (1992). Embryonic lens induction: shedding light on vertebrate tissue determination. Trends Genet, 8(10):349‐355. Grice EA, Snitkin ES, Yockey LJ, Bermudez DM; NISC Comparative Sequencing Program, Liechty KW, Segre JA. (2010). Longitudinal shift in diabetic wound microbiota correlates with prolonged skin defense response. Proc Natl Acad Sci USA, 107(33):14799‐14804. Gröger, M., Niederleithner, H., Kerjaschki, D., and Petzelbauer, P. (2007). A previously unknown dermal blood vessel phenotype in skin inflammation. J Invest Dermatol, 127(12):2893‐2900. Group, U. (1998a). Effect of intensive blood‐glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK prospective diabetes study (UKPDS) group. Lancet, 352(9131):854‐865.

129
Group, U. (1998b). Intensive blood‐glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK prospective diabetes study (UKPDS) group. Lancet, 352(9131):837‐853. Group, U. P. D. S. (1995). United Kingdom prospective diabetes study (UKPDS). 13: Relative efficacy of randomly allocated diet, sulphonylurea, insulin, or metformin in patients with newly diagnosed non‐insulin dependent diabetes followed for three years. BMJ, 310(6972):83‐88. Guttman‐Yassky E, Lowes MA, Fuentes‐Duculan J, Zaba LC, Cardinale I, Nograles KE, Khatcherian A, Novitskaya I, Carucci JA, Bergman R, Krueger JG. (2008). Low expression of the IL‐23/Th17 pathway in atopic dermatitis compared to psoriasis. J Immunol, 181(10):7420‐7427. Haddy, N., Sass, C., Droesch, S., Zaiou, M., Siest, G., Ponthieux, A., Lambert, D., and Visvikis, S. (2003). Il‐6, TNF‐alpha and atherosclerosis risk indicators in a healthy family population: the stanislas cohort. Atherosclerosis, 170(2):277‐283. Hämmerling B, Grund C, Boda‐Heggemann J, Moll R, Franke WW. (2006). The complexus adhaerens of mammalian lymphatic endothelia revisited: a junction even more complex than hitherto thought. Cell Tissue Res, 324(1):55‐67. Hagiwara, A., Takahashi, T., and Oku, N. (1989). Cancer chemotherapy administered by activated carbon particles and liposomes. Crit Rev Oncol Hematol, 9(4):319‐350. Halgren, R. G., Fielden, M. R., Fong, C. J., and Zacharewski, T. R. (2001). Assessment of clone identity and sequence fidelity for 1189 image cdna clones. Nucleic Acids Res, 29(2):582‐588. Halin, C. and Detmar, M. (2008). Chapter 1. inflammation, angiogenesis, and lymphangiogenesis. Methods Enzymol, 445:1‐25. Hansen, L., Gaster, M., Oakeley, E. J., Brusgaard, K., Nielsen, E.‐M. D., Beck‐Nielsen, H., Pedersen, O., and Hemmings, B. A. (2004). Expression profiling of insulin action in human myotubes: induction of inflammatory and pro‐angiogenic pathways in relationship with glycogen synthesis and type 2 diabetes. Biochem Biophys Res Commun, 323(2):685‐695. Hara‐Chikuma, M. and Verkman, A. S. (2008). Aquaporin‐3 facilitates epidermal cell migration and proliferation during wound healing. J Mol Med, 86(2):221‐231. Harvey, N. L. (2008). The link between lymphatic function and adipose biology. Ann N Y Acad Sci, 1131:82‐88. Harvey, N. L., Srinivasan, R. S., Dillard, M. E., Johnson, N. C., Witte, M. H., Boyd, K., Sleeman, M. W., and Oliver, G. (2005). Lymphatic vascular defects promoted by prox1 haploinsufficiency cause adult‐onset obesity. Nat Genet, 37(10):1072‐1081. He, Y., Kozaki, K.‐I., Karpanen, T., Koshikawa, K., Yla‐Herttuala, S., Takahashi, T., and Alitalo, K. (2002). Suppression of tumor lymphangiogenesis and lymph node metastasis by blocking vascular endothelial growth factor receptor 3 signaling. J Natl Cancer Inst, 94(11):819‐825. Heller, E. A., Liu, E., Tager, A. M., Yuan, Q., Lin, A. Y., Ahluwalia, N., Jones, K., Koehn, S. L., Lok, V. M., Aikawa, E., Moore, K. J., Luster, A. D., and Gerszten, R. E. (2006). Chemokine CXCL10 promotes atherogenesis by modulating the local balance of effector and regulatory t cells. Circulation, 113(19):2301‐2312. Hirakawa, S., Hong, Y.‐K., Harvey, N., Schacht, V., Matsuda, K., Libermann, T., and Detmar, M. (2003). Identification of vascular lineage‐specific genes by transcriptional profiling of isolated blood vascular and lymphatic endothelial cells. Am J Pathol, 162(2):575‐586. Hong, Y.‐K., Harvey, N., Noh, Y.‐H., Schacht, V., Hirakawa, S., Detmar, M., and Oliver, G. (2002). Prox1 is a master control gene in the program specifying lymphatic endothelial cell fate. Dev Dyn, 225(3):351‐357. Horra A, Salazar J, Ferré R, Vallvé JC, Guardiola M, Rosales R, Masana L, Ribalta J. (2009) Prox‐1 and FOXC2 gene expression in adipose tissue: A potential contributory role of the lymphatic system to familial combined hyperlipidaemia. Atherosclerosis, 206(2):343‐345. Hotamisligil, G. S. (1999). Mechanisms of tnf‐alpha‐induced insulin resistance. Exp Clin Endocrinol Diabetes, 107(2):119‐125. Hotamisligil, G. S. (2000). Molecular mechanisms of insulin resistance and the role of the adipocyte. Int J Obes Relat Metab Disord, 24 Suppl 4:S23‐S27. Hotamisligil, G. S. (2006). Inflammation and metabolic disorders. Nature, 444(7121):860‐867.

130
Hotamisligil, G. S. (2010). Endoplasmic reticulum stress and the inflammatory basis of metabolic disease. Cell, 140(6):900‐917. Hotamisligil, G. S., Arner, P., Caro, J. F., Atkinson, R. L., and Spiegelman, B. M. (1995). Increased adipose tissue expression of tumor necrosis factor‐alpha in human obesity and insulin resistance. J Clin Invest, 95(5):2409‐2415. Hotamisligil, G. S., Johnson, R. S., Distel, R. J., Ellis, R., Papaioannou, V. E., and Spiegelman, B. M. (1996). Uncoupling of obesity from insulin resistance through a targeted mutation in aP2, the adipocyte fatty acid binding protein. Science, 274(5291):1377‐1379. Hotamisligil, G. S., Murray, D. L., Choy, L. N., and Spiegelman, B. M. (1994). Tumor necrosis factor alpha inhibits signaling from the insulin receptor. Proc Natl Acad Sci U S A, 91(11):4854‐4858. Hotta, K., Funahashi, T., Arita, Y., Takahashi, M., Matsuda, M., Okamoto, Y., Iwahashi, H., Kuriyama, H., Ouchi, N., Maeda, K., Nishida, M., Kihara, S., Sakai, N., Nakajima, T., Hasegawa, K., Muraguchi, M., Ohmoto, Y., Nakamura, T., Yamashita, S., Hanafusa, T., and Matsuzawa, Y. (2000). Plasma concentrations of a novel, adipose‐specific protein, adiponectin, in type 2 diabetic patients. Arterioscler Thromb Vasc Biol, 20(6):1595‐1599. Hu, E., Liang, P., and Spiegelman, B. M. (1996). Adipoq is a novel adipose‐specific gene dysregulated in obesity. J Biol Chem, 271(18):10697‐10703. Huang, D. W., Sherman, B. T., and Lempicki, R. A. (2009). Systematic and integrative analysis of large gene lists using david bioinformatics resources. Nat Protoc, 4(1):44‐57. Huang, X. Z., Wu, J. F., Ferrando, R., Lee, J. H., Wang, Y. L., Farese, R. V., and Sheppard, D. (2000). Fatal bilateral chylothorax in mice lacking the integrin alpha9beta1. Mol Cell Biol, 20(14):5208‐5215. Huggenberger R, Siddiqui SS, Brander D, Ullmann S, Zimmermann K, Antsiferova M, Werner S, Alitalo K, Detmar M. (2011). An important role of lymphatic vessel activation in limiting acute inflammation. Blood, 117(17):4667‐4678. Hughes, J. M., Kuiper, E. J., Klaassen, I., Canning, P., Stitt, A. W., Bezu, J. V., Schalkwijk, C. G., Noorden, C. J. F. V., and Schlingemann, R. O. (2007). Advanced glycation end products cause increased ccn family and extracellular matrix gene expression in the diabetic rodent retina. Diabetologia, 50(5):1089‐1098. Hundal, R. S. and Inzucchi, S. E. (2003). Metformin: new understandings, new uses. Drugs, 63(18):1879‐1894. Huntington, G. and McClure, C. (1910). The anatomy and development of the jugular lymph sac in the domestic cat (felis domestica). Am J Anat, 10:177‐311. Ichise, H., Ichise, T., Ohtani, O., and Yoshida, N. (2009). Phospholipase cgamma2 is necessary for separation of blood and lymphatic vasculature in mice. Development, 136(2):191‐195. Irigoyen M, Ansó E, Martínez E, Garayoa M, Martínez‐Irujo JJ, Rouzaut A. (2007) Hypoxia alters the adhesive properties of lymphatic endothelial cells. A transcriptional and functional study. Biochim Biophys Acta, 1773(6):880‐890. Irjala, H., Johansson, E. L., Grenman, R., Alanen, K., Salmi, M., and Jalkanen, S. (2001). Mannose receptor is a novel ligand for l‐selectin and mediates lymphocyte binding to lymphatic endothelium. J Exp Med, 194(8):1033‐1042. Ishibashi, K., Hara, S., and Kondo, S. (2009). Aquaporin water channels in mammals. Clin Exp Nephrol, 13(2):107‐117. Itani, S. I., Ruderman, N. B., Schmieder, F., and Boden, G. (2002). Lipid‐induced insulin resistance in human muscle is associated with changes in diacylglycerol, protein kinase c, and I kappa b alpha. Diabetes, 51(7):2005‐2011. Jackson, A. J. (1981). Intramuscular absorption and regional lymphatic uptake of liposomeentrapped inulin. Drug Metab Dispos, 9(6):535‐540. Jackson, D. G. (2009). Immunological functions of hyaluronan and its receptors in the lymphatics. Immunol Rev, 230(1):216‐231. Jelinek, J. E. (1994). Cutaneous manifestations of diabetes mellitus. Int J Dermatol, 33(9):605‐617. Jeltsch, M., Kaipainen, A., Joukov, V., Meng, X., Lakso, M., Rauvala, H., Swartz, M., Fukumura, D., Jain, R. K., and Alitalo, K. (1997). Hyperplasia of lymphatic vessels in VEGF‐C transgenic mice. Science, 276(5317):1423‐1425.

131
Jeltsch, M., Tammela, T., Alitalo, K., and Wilting, J. (2003). Genesis and pathogenesis of lymphatic vessels. Cell Tissue Res, 314(1):69‐84. Ji, R.‐C., Kurihara, K., and Kato, S. (2006). Lymphatic vascular endothelial hyaluronan receptor (lyve)‐1‐ and ccl21‐positive lymphatic compartments in the diabetic thymus. Anat Sci Int, 81(4):201‐209. Johnson, L. A., Clasper, S., Holt, A. P., Lalor, P. F., Baban, D., and Jackson, D. G. (2006). An inflammation‐induced mechanism for leukocyte transmigration across lymphatic vessel endothelium. J Exp Med, 203(12):2763‐2777. Johnson, L. A., Prevo, R., Clasper, S., and Jackson, D. G. (2007). Inflammation‐induced uptake and degradation of the lymphatic endothelial hyaluronan receptor LYVE‐1. J Biol Chem, 282(46):33671‐33680. Johnson, N. C., Dillard, M. E., Baluk, P., McDonald, D. M., Harvey, N. L., Frase, S. L., and Oliver, G. (2008). Lymphatic endothelial cell identity is reversible and its maintenance requires PROX1 activity. Genes Dev, 22(23):3282‐3291. Joshi, N., Caputo, G. M., Weitekamp, M. R., and Karchmer, A. W. (1999). Infections in patients with diabetes mellitus. N Engl J Med, 341(25):1906‐1912. Jurisic G, Maby‐El Hajjami H, Karaman S, Ochsenbein AM, Alitalo A, Siddiqui SS, Ochoa Pereira C, Petrova TV, Detmar M. (2012). An unexpected role of semaphorin3a‐neuropilin‐1 signaling in lymphatic vessel maturation and valve formation. Circ Res, 111(4):426‐436. Jurisic, G. and Detmar, M. (2009). Lymphatic endothelium in health and disease. Cell Tissue Res, 335(1):97‐108. Jussila, L. and Alitalo, K. (2002). Vascular growth factors and lymphangiogenesis. Physiol Rev, 82(3):673‐700. Kainulainen, V., Nelimarkka, L., Järveläinen, H., Laato, M., Jalkanen, M., and Elenius, K. (1996). Suppression of syndecan‐1 expression in endothelial cells by tumor necrosis factor‐alpha. J Biol Chem, 271(31):18759‐18766. Kaipainen, A., Korhonen, J., Mustonen, T., van Hinsbergh, V. W., Fang, G. H., Dumont, D., Breitman, M., and Alitalo, K. (1995). Expression of the fms‐like tyrosine kinase 4 gene becomes restricted to lymphatic endothelium during development. Proc Natl Acad Sci U S A, 92(8):3566‐3570. Kang, S., Lee, S.‐P., Kim, K. E., Kim, H.‐Z., Mémet, S., and Koh, G. Y. (2009). Toll‐like receptor 4 in lymphatic endothelial cells contributes to lps‐induced lymphangiogenesis by chemotactic recruitment of macrophages. Blood, 113(11):2605‐2613. Kapoor S. (2012). Podoplanin expression and its emerging role as a prognostic indicator in systemic tumors besides head and neck malignancies. J Surg Oncol, [Epub ahead of print]. Kaprio, J., Tuomilehto, J., Koskenvuo, M., Romanov, K., Reunanen, A., Eriksson, J., Stengård, J., and Kesäniemi, Y. A. (1992). Concordance for type 1 (insulin‐dependent) and type 2 (non insulin‐dependent) diabetes mellitus in a population‐based cohort of twins in Finland. Diabetologia, 35(11):1060‐1067. Karikoski, M., Irjala, H., Maksimow, M., Miiluniemi, M., Granfors, K., Hernesniemi, S., Elima, K., Moldenhauer, G., Schledzewski, K., Kzhyshkowska, J., Goerdt, S., Salmi, M., and Jalkanen, S. (2009). Clever‐1/stabilin‐1 regulates lymphocyte migration within lymphatics and leukocyte entrance to sites of inflammation. Eur J Immunol, 39(12):3477‐3487. Karkkainen, M. J., Haiko, P., Sainio, K., Partanen, J., Taipale, J., Petrova, T. V., Jeltsch, M., Jackson, D. G., Talikka, M., Rauvala, H., Betsholtz, C., and Alitalo, K. (2004). Vascular endothelial growth factor c is required for sprouting of the first lymphatic vessels from embryonic veins. Nat Immunol, 5(1):74‐80. Karkkainen, M. J., Saaristo, A., Jussila, L., Karila, K. A., Lawrence, E. C., Pajusola, K., Bueler, H., Eichmann, A., Kauppinen, R., Kettunen, M. I., Yla‐Herttuala, S., Finegold, D. N., Ferrell, R. E., and Alitalo, K. (2001). A model for gene therapy of human hereditary lymphedema. Proc Natl Acad Sci U S A, 98(22):12677‐12682. Kaufmann, A., Molnár, B., Craciun, C., and Itcus, A. (1980). Diabetic lymphangiopathy. An optical and electron microscopic study. Lymphology, 13(4):202‐206. Kerjaschki, D. (2006). Lymphatic neoangiogenesis in renal transplants: a driving force of chronic rejection? J Nephrol, 19(4):403‐406. Kerjaschki D. (2005). The crucial role of macrophages in lymphangiogenesis. J Clin Invest, 115(9):2316‐2319. Kerjaschki D, Regele HM, Moosberger I, Nagy‐Bojarski K, Watschinger B, Soleiman A, Birner P, Krieger S, Hovorka A, Silberhumer G, Laakkonen P, Petrova T, Langer B, Raab I. (2004). Lymphatic neoangiogenesis in human kidney transplants is associated with immunologically active lymphocytic infiltrates. J Am Soc Nephrol, 15(3):603‐612.

132
Khanna, S., Biswas, S., Shang, Y., Collard, E., Azad, A., Kauh, C., Bhasker, V., Gordillo, G. M., Sen, C. K., and Roy, S. (2010). Macrophage dysfunction impairs resolution of inflammation in the wounds of diabetic mice. PLoS One, 5(3):e9539. Kholová I, Dragneva G, Cermáková P, Laidinen S, Kaskenpää N, Hazes T, Cermáková E, Steiner I, Ylä‐Herttuala S. (2011). Lymphatic vasculature is increased in heart valves, ischaemic and inflamed hearts and in cholesterol‐rich and calcified atherosclerotic lesions. Eur J Clin Invest,41(5):487‐497. Kikkawa, R., Koya, D., and Haneda, M. (2003). Progression of diabetic nephropathy. Am J Kidney Dis, 41(3 Suppl 1):S19‐S21. Kim KE, Koh YJ, Jeon BH, Jang C, Han J, Kataru RP, Schwendener RA, Kim JM, Koh GY. (2009). Role of CD11b+ macrophages in intraperitoneal lipopolysaccharide‐induced aberrant lymphangiogenesis and lymphatic function in the diaphragm. Am J Pathol,175(4):1733‐1745. Kirpichnikov, D., McFarlane, S. I., and Sowers, J. R. (2002). Metformin: an update. Ann Intern Med, 137(1):25‐33. Kivelä, R., Silvennoinen, M., Lehti, M., Kainulainen, H., and Vihko, V. (2007). Effects of acute exercise, exercise training, and diabetes on the expression of lymphangiogenic growth factors and lymphatic vessels in skeletal muscle. Am J Physiol Heart Circ Physiol, 293(4):H2573‐H2579. Koch S, Tugues S, Li X, Gualandi L, Claesson‐Welsh L. (2011). Signal transduction by vascular endothelial growth factor receptors. Biochem J, 437(2):169‐183. Krebs, D. L. and Hilton, D. J. (2003). A new role for SOCS in insulin action. Suppressor of cytokine signaling. Sci STKE, (169):PE6. Kriederman, B. M., Myloyde, T. L., Witte, M. H., Dagenais, S. L., Witte, C. L., Rennels, M., Bernas, M. J., Lynch, M. T., Erickson, R. P., Caulder, M. S., Miura, N., Jackson, D., Brooks, B. P., and Glover, T. W. (2003). Foxc2 haploinsufficient mice are a model for human autosomal dominant lymphedema‐distichiasis syndrome. Hum Mol Genet, 12(10):1179‐1185. Kriehuber, E., Breiteneder‐Geleff, S., Groeger, M., Soleiman, A., Schoppmann, S. F., Stingl, G., Kerjaschki, D., and Maurer, D. (2001). Isolation and characterization of dermal lymphatic and blood endothelial cells reveal stable and functionally specialized cell lineages. J Exp Med, 194(6):797‐808. Kukk, E., Lymboussaki, A., Taira, S., Kaipainen, A., Jeltsch, M., Joukov, V., and Alitalo, K. (1996). Vegf‐c receptor binding and pattern of expression with Vegfr‐3 suggests a role in lymphatic vascular development. Development, 122(12):3829‐3837. Kulesh, D. A., Clive, D. R., Zarlenga, D. S., and Greene, J. J. (1987). Identification of interferon modulated proliferation‐related cDNA sequences. Proc Natl Acad Sci U S A, 84(23):8453‐8457. Kume T. (2010). Specification of arterial, venous, and lymphatic endothelial cells during embryonic development. Histol Histopathol, 25 (5): 637 – 646. Labanaris AP, Polykandriotis E, Horch RE. (2009). The effect of vacuum‐assisted closure on lymph vessels in chronic wounds. J Plast Reconstr Aesthet Surg, 62(8):1068‐1075. Lander, E. S. (1999). Array of hope. Nat Genet, 21(1 Suppl):3‐4. Lapinski PE, Kwon S, Lubeck BA, Wilkinson JE, Srinivasan RS, Sevick‐Muraca E, King PD. RASA1 maintains the lymphatic vasculature in a quiescent functional state in mice. J Clin Invest, 122(2):733‐747. Leak, L. V. (1970). Electron microscopic observations on lymphatic capillaries and the structural components of the connective tissue‐lymph interface. Microvasc Res, 2(4):361‐391. Leak, L. V. and Burke, J. F. (1966). Fine structure of the lymphatic capillary and the adjoining connective tissue area. Am J Anat, 118(3):785‐809. Leak, L. V. and Burke, J. F. (1968). Ultrastructural studies on the lymphatic anchoring filaments. J Cell Biol, 36(1):129‐149. Leu, S.‐J., Lam, S. C.‐T., and Lau, L. F. (2002). Pro‐angiogenic activities of CYR61 (CCN1) mediated through integrins alphaVbeta3 and alpha6beta1 in human umbilical vein endothelial cells. J Biol Chem, 277(48):46248‐46255. Lim, H. Y., Rutkowski, J. M., Helft, J., Reddy, S. T., Swartz, M. A., Randolph, G. J., and Angeli, V. (2009). Hypercholesterolemic mice exhibit lymphatic vessel dysfunction and degeneration. Am J Pathol, 175(3):1328‐1337.

133
Liu FY, Tang XC, Deng M, Chen P, Ji W, Zhang X, Gong L, Woodward Z, Liu J, Zhang L, Sun S, Liu JP, Wu K, Wu MX, Liu XL, Yu MB, Liu Y, Li DW. (2012). The Tumor Suppressor p53 Regulates c‐Maf and Prox‐1 to Control Lens Differentiation. Curr Mol Med, 12(8):917‐928. Luissint, A.‐C., Lutz, P. G., Calderwood, D. A., Couraud, P.‐O., and Bourdoulous, S. (2008). Jam‐l‐mediated leukocyte adhesion to endothelial cells is regulated in cis by alpha4beta1 integrin activation. J Cell Biol, 183(6):1159‐1173. Luong, M. X., Tam, J., Lin, Q., Hagendoorn, J., Moore, K. J., Padera, T. P., Seed, B., Fukumura, D., Kucherlapati, R., and Jain, R. K. (2009). Lack of lymphatic vessel phenotype in lyve‐1/cd44 double knockout mice. J Cell Physiol, 219(2):430‐437. Lyman, G. H., Giuliano, A. E., Somerfield, M. R., Benson, A. B., Bodurka, D. C., Burstein, H. J., Cochran, A. J., Cody, H. S., Edge, S. B., Galper, S., Hayman, J. A., Kim, T. Y., Perkins, C. L., Podoloff, D. A., Sivasubramaniam, V. H., Turner, R. R., Wahl, R., Weaver, D. L., Wolff, A. C., Winer, E. P., and of Clinical Oncology, A. S. (2005). American society of clinical oncology guideline recommendations for sentinel lymph node biopsy in early‐stage breast cancer. J Clin Oncol, 23(30):7703‐7720. Lymboussaki, A., Partanen, T. A., Olofsson, B., Thomas‐Crusells, J., Fletcher, C. D., de Waal, R. M., Kaipainen, A., and Alitalo, K. (1998). Expression of the vascular endothelial growth factor c receptor VEGFR‐3 in lymphatic endothelium of the skin and in vascular tumors. Am J Pathol, 153(2):395‐403. Maby‐El Hajjami H and Petrova TV. (2008). Developmental and pathological lymphangiogenesis: from models to human disease. Histochem Cell Biol, 130(6):1063‐1078. Machnik, A., Neuhofer, W., Jantsch, J., Dahlmann, A., Tammela, T., Machura, K., Park, J.‐K., Beck, F.‐X., M uller, D. N., Derer, W., Goss, J., Ziomber, A., Dietsch, P., Wagner, H., van Rooijen, N., Kurtz, A., Hilgers, K. F., Alitalo, K., Eckardt, K.‐U., Luft, F. C., Kerjaschki, D., and Titze, J. (2009). Macrophages regulate salt‐dependent volume and blood pressure by a vascular endothelial growth factor‐c‐dependent buffering mechanism. Nat Med, 15(5):545‐552. Maerki, C., Meuter, S., Liebi, M., M uhlemann, K., Frederick, M. J., Yawalkar, N., Moser, B., and Wolf, M. (2009). Potent and broad‐spectrum antimicrobial activity of CXCL14 suggests an immediate role in skin infections. J Immunol, 182(1):507‐514. Mäkinen, T., Adams, R. H., Bailey, J., Lu, Q., Ziemiecki, A., Alitalo, K., Klein, R., and Wilkinson, G. A. (2005). Pdz interaction site in ephrinb2 is required for the remodeling of lymphatic vasculature. Genes Dev, 19(3):397‐410. Mahdavian Delavary B, van der Veer WM, van Egmond M, Niessen FB, Beelen RH. (2011). Macrophages in skin injury and repair. Immunobiology,216(7):753‐762. Makowski, L. and Hotamisligil, G. S. (2004). Fatty acid binding proteins‐the evolutionary crossroads of inflammatory and metabolic responses. J Nutr, 134(9):2464S‐2468S. Malhotra D, Fletcher AL, Astarita J, Lukacs‐Kornek V, Tayalia P, Gonzalez SF, Elpek KG, Chang SK, Knoblich K, Hemler ME, Brenner MB, Carroll MC, Mooney DJ, Turley SJ; Immunological Genome Project Consortium. (2012). Transcriptional profiling of stroma from inflamed and resting lymph nodes defines immunological hallmarks. Nat Immunol,13(5):499‐510. Malhotra, A., Igo, R. P., Thameem, F., Kao, W. H. L., Abboud, H. E., Adler, S. G., Arar, N. H., Bowden, D. W., Duggirala, R., Freedman, B. I., Goddard, K. A. B., Ipp, E., Iyengar, S. K., Kimmel, P. L., Knowler, W. C., Kohn, O., Leehey, D., Meoni, L. A., Nelson, R. G., Nicholas, S. B., Parekh, R. S., Rich, S. S., Chen, Y.‐D. I., Saad, M. F., Scavini, M., Schelling, J. R., Sedor, J. R., Shah, V. O., Taylor, K. D., Thornley‐Brown, D., Zager, P. G., Horvath, A., Hanson, R. L., of Nephropathy, F. I., and Group, D. R. (2009). Genome‐wide linkage scans for type 2 diabetes mellitus in four ethnically diverse populations‐significant evidence for linkage on chromosome 4q in african americans: the family investigation of nephropathy and diabetes research group. Diabetes Metab Res Rev, 25(8):740‐747. Maresh, J. G. and Shohet, R. V. (2008). In vivo endothelial gene regulation in diabetes. Cardiovasc Diabetol, 7:8. Martin P, Leibovich SJ. (2005). Inflammatory cells during wound repair: the good, the bad and the ugly. Trends Cell Biol, 15(11):599‐607. Martín‐Villar, E., Scholl, F. G., Gamallo, C., Yurrita, M. M., noz Guerra, M. M., Cruces, J., and Quintanilla, M. (2005). Characterization of human pa2.26 antigen (t1alpha‐2, podoplanin), a small membrane mucin induced in oral squamous cell carcinomas. Int J Cancer, 113(6):899‐910. Marttila‐Ichihara, F., Turja, R., Miiluniemi, M., Karikoski, M., Maksimow, M., Niemelä, J., Martinez‐Pomares, L., Salmi, M., and Jalkanen, S. (2008). Macrophage mannose receptor on lymphatics controls cell trafficking. Blood, 112(1):64‐72.

134
Maruyama, K., Asai, J., Ii, M., Thorne, T., Losordo, D. W., and D'Amore, P. A. (2007). Decreased macrophage number and activation lead to reduced lymphatic vessel formation and contribute to impaired diabetic wound healing. Am J Pathol, 170(4):1178‐1191. Maruyama, K., Ii, M., Cursiefen, C., Jackson, D. G., Keino, H., Tomita, M., Rooijen, N. V., Takenaka, H., D'Amore, P. A., Stein‐Streilein, J., Losordo, D. W., and Streilein, J. W. (2005). Inflammation‐induced lymphangiogenesis in the cornea arises from cd11b‐positive macrophages. J Clin Invest, 115(9):2363‐2372. Matsui, K., Breitender‐Geleff, S., Soleiman, A., Kowalski, H., and Kerjaschki, D. (1999). Podoplanin, a novel 43‐kda membrane protein, controls the shape of podocytes. Nephrol Dial Transplant, 14 Suppl 1:9‐11. Matsui, K., Breiteneder‐Geleff, S., and Kerjaschki, D. (1998). Epitope‐specific antibodies to the 43‐kD glomerular membrane protein podoplanin cause proteinuria and rapid attening of podocytes. J Am Soc Nephrol, 9(11):2013‐2026. Mattacks, C. A., Sadler, D., and Pond, C. M. (2003). The cellular structure and lipid/protein composition of adipose tissue surrounding chronically stimulated lymph nodes in rats. J Anat, 202(6):551‐561. Mebius, R. E. (2003). Organogenesis of lymphoid tissues. Nat Rev Immunol, 3(4):292‐303. Medoff, B. D., Sauty, A., Tager, A. M., Maclean, J. A., Smith, R. N., Mathew, A., Dufour, J. H., and Luster, A. D. (2002). Ifn‐gamma‐inducible protein 10 (cxcl10) contributes to airway hyperreactivity and airway inflammation in a mouse model of asthma. J Immunol, 168(10):5278‐5286. Meigs, J. B., Hu, F. B., Rifai, N., and Manson, J. E. (2004). Biomarkers of endothelial dysfunction and risk of type 2 diabetes mellitus. JAMA, 291(16):1978‐1986. Meriden, T. (2004). Progress with thiazolidinediones in the management of type 2 diabetes mellitus. Clin Ther, 26(2):177‐190. Miklos, G. L. G. and Maleszka, R. (2004). Microarray reality checks in the context of a complex disease. Nat Biotechnol, 22(5):615‐621. Miyasaka, M. and Tanaka, T. (2004). Lymphocyte trafficking across high endothelial venules: dogmas and enigmas. Nat Rev Immunol, 4(5):360‐370. Moczulski, D. K., Fojcik, H., Wielgorecki, A., Trautsolt, W., Gawlik, B., Kosiorz‐Gorczynska, S., Oczko‐Wojciechowska, M., Wiench, M., Strojek, K., Zukowska‐Szczechowska, E., and Grzeszczak, W. (2007). Expression pattern of genes in peripheral blood mononuclear cells in diabetic nephropathy. Diabet Med, 24(3):266‐271. Morigi, M., Angioletti, S., Imberti, B., Donadelli, R., Micheletti, G., Figliuzzi, M., Remuzzi, A., Zoja, C., and Remuzzi, G. (1998). Leukocyte‐endothelial interaction is augmented by high glucose concentrations and hyperglycemia in a nf‐kb‐dependent fashion. J Clin Invest, 101(9):1905‐1915. Moriguchi, P., Sannomiya, P., Lara, P. F., Oliveira‐Filho, R. M., Greco, K. V., and Sudo‐Hayashi, L. S. (2005). Lymphatic system changes in diabetes mellitus: role of insulin and hyperglycemia. Diabetes Metab Res Rev, 21(2):150‐157. Mortimer, P. S., Simmonds, R., Rezvani, M., Robbins, M., Hopewell, J. W., and Ryan, T. J. (1990). The measurement of skin lymph ow by isotope clearance‐reliability, reproducibility, injection dynamics, and the effect of massage. J Invest Dermatol, 95(6):677‐682. Muller, L. M. A. J., Gorter, K. J., Hak, E., Goudzwaard, W. L., Schellevis, F. G., Hoepelman, A. I. M., and Rutten, G. E. H. M. (2005). Increased risk of common infections in patients with type 1 and type 2 diabetes mellitus. Clin Infect Dis, 41(3):281‐288. Nadler, S. T., Stoehr, J. P., Schueler, K. L., Tanimoto, G., Yandell, B. S., and Attie, A. D. (2000). The expression of adipogenic genes is decreased in obesity and diabetes mellitus. Proc Natl Acad Sci U S A, 97(21):11371‐11376. Nathanson, S. D. (2003). Insights into the mechanisms of lymph node metastasis. Cancer, 98(2):413‐423. Navarro, A., Alonso, A., Garrido, P., González, C., Rey, C. G. D., nez, C. O., and Tolivia, J. (2010). Increase in placental apolipoprotein D as an adaptation to human gestational diabetes. Placenta, 31(1):25‐31. Nesto, R. W., Bell, D., Bonow, R. O., Fonseca, V., Grundy, S. M., Horton, E. S., Winter, M. L., Porte, D., Semenkovich, C. F., Smith, S., Young, L. H., and Kahn, R. (2004). Thiazolidinedione use, fluid retention, and congestive heart failure: a consensus statement from the american heart association and american diabetes association. Diabetes Care, 27(1):256‐263.

135
Newman, B., Selby, J. V., King, M. C., Slemenda, C., Fabsitz, R., and Friedman, G. D. (1987). Concordance for type 2 (non‐insulin‐dependent) diabetes mellitus in male twins. Diabetologia, 30(10):763‐768. Nguyen PD, Tutela JP, Thanik VD, Knobel D, Allen RJ Jr, Chang CC, Levine JP, Warren SM, Saadeh PB. (2010). Improved diabetic wound healing through topical silencing of p53 is associated with augmented vasculogenic mediators. Wound Repair Regen, 18(6):553‐559. Nightingale, T. D., Frayne, M. E. F., Clasper, S., Banerji, S., and Jackson, D. G. (2009). A mechanism of sialylation functionally silences the hyaluronan receptor lyve‐1 in lymphatic endothelium. J Biol Chem, 284(6):3935‐3945. Nishikawa, T., Edelstein, D., Du, X. L., Yamagishi, S., Matsumura, T., Kaneda, Y., Yorek, M. A., Beebe, D., Oates, P. J., Hammes, H. P., Giardino, I., and Brownlee, M. (2000). Normalizing mitochondrial superoxide production blocks three pathways of hyperglycaemic damage. Nature, 404(6779):787‐790. Nissen, S. E. and Wolski, K. (2007). Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med, 356(24):2457‐2471. Norrmén, C., Ivanov, K. I., Cheng, J., Zangger, N., Delorenzi, M., Jaquet, M., Miura, N., Puolakkainen, P., Horsley, V., Hu, J., Augustin, H. G., Ylä‐Herttuala, S., Alitalo, K., and Petrova, T. V. (2009). Foxc2 controls formation and maturation of lymphatic collecting vessels through cooperation with NFATc1. J Cell Biol, 185(3):439‐457. Nougues, J., Reyne, Y., and Dulor, J. P. (1988). Differentiation of rabbit adipocyte precursors in primary culture. Int J Obes, 12(4):321‐333. Ny, A., Koch, M., Vandevelde, W., Schneider, M., Fischer, C., Diez‐Juan, A., Neven, E., Geudens, I., Maity, S., Moons, L., Plaisance, S., Lambrechts, D., Carmeliet, P., and Dewerchin, M. (2008). Role of VEGF‐D and VEGFR‐3 in developmental lymphangiogenesis, a chemicogenetic study in xenopus tadpoles. Blood, 112(5):1740‐1749. Ogunbiyi S, Chinien G, Field D, Humphries J, Burand K, Sawyer B, Jeffrey S, Mortimer P, Clasper S, Jackson D, Smith A; London Lymphedema Consortium. (2011) Molecular characterization of dermal lymphatic endothelial cells from primary lymphedema skin. Lymphat Res Biol, 9(1):19‐30. Ohkuma, M. (1979). Histochemical change of the endothelial basal lamina of the diabetic lymphatic vessel. Lymphology, 12(1):37‐39. Ohl, L., Mohaupt, M., Czeloth, N., Hintzen, G., Kiafard, Z., Zwirner, J., Blankenstein, T., Henning, G., and Förster, R. (2004). Ccr7 governs skin dendritic cell migration under inflammatory and steady‐state conditions. Immunity, 21(2):279‐288. Oliver, G. (2004). Lymphatic vasculature development. Nat Rev Immunol, 4(1):35‐45. Oliver, G. and Harvey, N. (2002). A stepwise model of the development of lymphatic vasculature. Ann N Y Acad Sci, 979:159‐65; discussion 188‐96. Oliver, G., Sosa‐Pineda, B., Geisendorf, S., Spana, E. P., Doe, C. Q., and Gruss, P. (1993). Prox 1, a prospero‐related homeobox gene expressed during mouse development. Mech Dev, 44(1):3‐16. Oliver, G. and Srinivasan, R. S. (2010). Endothelial cell plasticity: how to become and remain a lymphatic endothelial cell. Development, 137(3):363‐372. Olsson, A.‐K., Dimberg, A., Kreuger, J., and Claesson‐Welsh, L. (2006). Vegf receptor signaling ‐ in control of vascular function. Nat Rev Mol Cell Biol, 7(5):359‐371. Olszewski, W., Engeset, A., Jaeger, P. M., Sokolowski, J., and Theodorsen, L. (1977). Flow and composition of leg lymph in normal men during venous stasis, muscular activity and local hyperthermia. Acta Physiol Scand, 99(2):149‐155. Ordonez, N. G. (2006). Podoplanin: a novel diagnostic immunohistochemical marker. Adv Anat Pathol, 13(2):83‐88. Ostergård, T., Jessen, N., Schmitz, O., and Mandarino, L. J. (2007). The effect of exercise, training, and inactivity on insulin sensitivity in diabetics and their relatives: what is new? Appl Physiol Nutr Metab, 32(3):541‐548. Parsons, R. J. and McMaster, P. D. (1938). The effect of the pulse upon the formation and flow of lymph. J Exp Med, 68(3):353‐376. Pennisi, D., Gardner, J., Chambers, D., Hosking, B., Peters, J., Muscat, G., Abbott, C., and Koopman, P. (2000). Mutations in SOX18 underlie cardiovascular and hair follicle defects in ragged mice. Nat Genet, 24(4):434‐437.

136
Perou, C. M., Jeffrey, S. S., van de Rijn, M., Rees, C. A., Eisen, M. B., Ross, D. T., Pergamenschikov, A., Williams, C. F., Zhu, S. X., Lee, J. C., Lashkari, D., Shalon, D., Brown, P. O., and Botstein, D. (1999). Distinctive gene expression patterns in human mammary epithelial cells and breast cancers. Proc Natl Acad Sci U S A, 96(16):9212‐9217. Perou, C. M., Sorlie, T., Eisen, M. B., van de Rijn, M., Jeffrey, S. S., Rees, C. A., Pollack, J. R., Ross, D. T., Johnsen, H., Akslen, L. A., Fluge, O., Pergamenschikov, A., Williams, C., Zhu, S. X., Lonning, P. E., Borresen‐Dale, A. L., Brown, P. O., and Botstein, D. (2000). Molecular portraits of human breast tumours. Nature, 406(6797):747‐752. Pessin, J. E. and Saltiel, A. R. (2000). Signaling pathways in insulin action: molecular targets of insulin resistance. J Clin Invest, 106(2):165‐169. Petrova, T. V., Karpanen, T., Norrmén, C., Mellor, R., Tamakoshi, T., Finegold, D., Ferrell, R., Kerjaschki, D., Mortimer, P., Ylä‐Herttuala, S., Miura, N., and Alitalo, K. (2004). Defective valves and abnormal mural cell recruitment underlie lymphatic vascular failure in lymphedema distichiasis. Nat Med, 10(9):974‐981. Petrova, T. V., Mäkinen, T., Mäkelä, T. P., Saarela, J., Virtanen, I., Ferrell, R. E., Finegold, D. N., Kerjaschki, D., Ylä‐Herttuala, S., and Alitalo, K. (2002). Lymphatic endothelial reprogramming of vascular endothelial cells by the prox‐1 homeobox transcription factor. EMBO J, 21(17):4593‐4599. Pfaffl M. W. (2001). A new mathematical model for relative quantification in real‐time RT‐PCR. Nucleic Acids Res, 29(9):e45. Pierce A, Smith DL, Jakobsen LV, Whetton AD, Spooncer E. (2001). The specific enhancement of interferon alpha induced growth inhibition by BCR/ABL only occurs in multipotent cells. Hematol J, 2(4):257‐64. Pierce, M., Keen, H., and Bradley, C. (1995). Risk of diabetes in offspring of parents with noninsulin‐ dependent diabetes. Diabet Med, 12(1):6‐13. Pinhas‐Hamiel, O. and Zeitler, P. (2007). Clinical presentation and treatment of type 2 diabetes in children. Pediatr Diabetes, 8 Suppl 9:16‐27. Pirola L, Balcerczyk A, Tothill RW, Haviv I, Kaspi A, Lunke S, Ziemann M, Karagiannis T, Tonna S, Kowalczyk A, Beresford‐Smith B, Macintyre G, Kelong M, Hongyu Z, Zhu J, El‐Osta A. (2011). Genome‐wide analysis distinguishes hyperglycemia regulated epigenetic signatures of primary vascular cells. Genome Res, 21(10):1601‐1615. Podgrabinska, S., Braun, P., Velasco, P., Kloos, B., Pepper, M. S., and Skobe, M. (2002). Molecular characterization of lymphatic endothelial cells. Proc Natl Acad Sci U S A, 99(25):16069‐16074. Pollock, J. D. (2002). Gene expression profiling: methodological challenges, results, and prospects for addiction research. Chem Phys Lipids, 121(1‐2):241‐256. Pond, C. M. and Mattacks, C. A. (1995). Interactions between adipose tissue around lymph nodes and lymphoid cells in vitro. J Lipid Res, 36(10):2219‐2231. Pond, C. M. and Mattacks, C. A. (1998). In vivo evidence for the involvement of the adipose tissue surrounding lymph nodes in immune responses. Immunol Lett, 63(3):159‐167. Porta, M. and Bandello, F. (2002). Diabetic retinopathya clinical update. Diabetologia, 45(12):1617‐1634. Pradhan, A. D., Rifai, N., Buring, J. E., and Ridker, P. M. (2007). Hemoglobin a1c predicts diabetes but not cardiovascular disease in nondiabetic women. Am J Med, 120(8):720‐727. Pradhan, A. D., Manson, J. E., Rifai, N., Buring, J. E., and Ridker, P. M. (2001). C‐reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA, 286(3):327‐334. Qi, W., Chen, X., Gilbert, R. E., Zhang, Y., Waltham, M., Schache, M., Kelly, D. J., and Pollock, C. A. (2007). High glucose‐induced thioredoxin‐interacting protein in renal proximal tubule cells is independent of transforming growth factor‐beta1. Am J Pathol, 171(3):744‐754. Qu, P., Ji, R. C., and Kato, S. (2003). Histochemical analysis of lymphatic endothelial cells in the pancreas of non‐obese diabetic mice. J Anat, 203(5):523‐530. Qu, P., Ji, R.‐C., Shimoda, H., Miura, M., and Kato, S. (2004). Study on pancreatic lymphatics in nonobese diabetic mouse with prevention of insulitis and diabetes by adjuvant immunotherapy. Anat Rec A Discov Mol Cell Evol Biol, 281(2):1326‐1336. Quaye, I. K., Ababio, G., and Amoah, A. G. (2006). Haptoglobin 2‐2 phenotype is a risk factor for type 2 diabetes in ghana. J Atheroscler Thromb, 13(2):90‐94.

137
Rahman, F. Z., Smith, A. M., Hayee, B., Marks, D. J. B., Bloom, S. L., and Segal, A. W. (2010). Delayed resolution of acute inflammation in ulcerative colitis is associated with elevated cytokine release downstream of TLR4. PLoS One, 5(3):e9891. Rajala, M. W. and Scherer, P. E. (2003). Minireview: The adipocyte‐at the crossroads of energy homeostasis, inflammation, and atherosclerosis. Endocrinology, 144(9):3765‐3773. Ramirez, M. I., Millien, G., Hinds, A., Cao, Y., Seldin, D. C., and Williams, M. C. (2003). T1alpha, a lung type I cell differentiation gene, is required for normal lung cell proliferation and alveolus formation at birth. Dev Biol, 256(1):61‐72. Randolph, G. J., Angeli, V., and Swartz, M. A. (2005). Dendritic‐cell trafficking to lymph nodes through lymphatic vessels. Nat Rev Immunol, 5(8):617‐628. Ratzinger, G., Stoitzner, P., Ebner, S., Lutz, M. B., Layton, G. T., Rainer, C., Senior, R. M., Shipley, J. M., Fritsch, P., Schuler, G., and Romani, N. (2002). Matrix metalloproteinases 9 and 2 are necessary for the migration of Langerhans cells and dermal dendritic cells from human and murine skin. J Immunol, 168(9):4361‐4371. Ravussin, E. and Smith, S. R. (2002). Increased fat intake, impaired fat oxidation, and failure of fat cell proliferation result in ectopic fat storage, insulin resistance, and type 2 diabetes mellitus. Ann N Y Acad Sci, 967:363‐378. Reinehr, T. (2005). Clinical presentation of type 2 diabetes mellitus in children and adolescents. Int J Obes (Lond), 29 Suppl 2:S105‐S110. Rishi, A. K., Joyce‐Brady, M., Fisher, J., Dobbs, L. G., Floros, J., VanderSpek, J., Brody, J. S., and Williams, M. C. (1995). Cloning, characterization, and development expression of a rat lung alveolar type I cell gene in embryonic endodermal and neural derivatives. Dev Biol, 167(1):294‐306. Rockson, S. G. (2001). Lymphedema. Am J Med, 110(4):288‐295. Rockson, S. G. (2008). Diagnosis and management of lymphatic vascular disease. J Am Coll Cardiol, 52(10):799‐806. Roesli, C., Mumprecht, V., Neri, D., and Detmar, M. (2008). Identification of the surface‐accessible, lineage‐specific vascular proteome by two‐dimensional peptide mapping. FASEB J, 22(6):1933‐1944. Rosen, E. D. (2002). The molecular control of adipogenesis, with special reference to lymphatic pathology. Ann N Y Acad Sci, 979:143‐58. Rovenská E, Rovenský J. (2011). Lymphatic vessels: structure and function. Isr Med Assoc J, 13(12):762‐768. Roy S, Khanna S, Rink C, Biswas S, Sen CK. (2008). Characterization of the acute temporal changes in excisional murine cutaneous wound inflammation by screening of the wound‐edge transcriptome. Physiol Genomics,34(2):162‐184. Roy, S., Cagliero, E., and Lorenzi, M. (1996). Fibronectin overexpression in retinal microvessels of patients with diabetes. Invest Ophthalmol Vis Sci, 37(2):258‐266. Roy, S., Maiello, M., and Lorenzi, M. (1994). Increased expression of basement membrane collagen in human diabetic retinopathy. J Clin Invest, 93(1):438‐442. Ruddell A, Kelly‐Spratt KS, Furuya M, Parghi SS, Kemp CJ. (2008). p19/Arf and p53 suppress sentinel lymph node lymphangiogenesis and carcinoma metastasis. Oncogene, 27(22):3145‐3155. Rydén, L., Standl, E., Bartnik, M., den Berghe, G. V., Betteridge, J., de Boer, M.‐J., Cosentino, F., Jönsson, B., Laakso, M., Malmberg, K., Priori, S., Ostergren, J., Tuomilehto, J., Thrainsdottir, I., Vanhorebeek, I., Stramba‐Badiale, M., Lindgren, P., Qiao, Q., Priori, S. G., Blanc, J.‐J., Budaj, A., Camm, J., Dean, V., Deckers, J., Dickstein, K., Lekakis, J., McGregor, K., Metra, M., ao Morais, J., Osterspey, A., Tamargo, J., Zamorano, J. L., Deckers, J. W., Bertrand, M., Charbonnel, B., Erdmann, E., Ferrannini, E., Flyvbjerg, A., Gohlke, H., Juanatey, J. R. G., Graham, I., Monteiro, P. F., Parhofer, K., Pyörälä, K., Raz, I., Schernthaner, G., Volpe, M., Wood, D., on Diabetes, T. F., of the European Society of Cardiology (ESC), C. D., and for the Study of Diabetes (EASD), E. A. (2007). Guidelines on diabetes, pre‐diabetes, and cardiovascular diseases: executive summary. the task force on diabetes and cardiovascular diseases of the european society of cardiology (esc) and of the european association for the study of diabetes (EASD). Eur Heart J, 28(1):88‐136. Saaristo, A., Tammela, T., Farkkilā, A., Kärkkäinen, M., Suominen, E., Ylä‐Herttuala, S., and Alitalo, K. (2006). Vascular endothelial growth factor‐c accelerates diabetic wound healing. Am J Pathol, 169(3):1080‐1087.

138
Saaristo, A., Veikkola, T., Tammela, T., Enholm, B., Karkkainen, M. J., Pajusola, K., Bueler, H., Ylä‐Herttuala, S., and Alitalo, K. (2002). Lymphangiogenic gene therapy with minimal blood vascular side effects. J Exp Med, 196(6):719‐730. Sabin, F. R. (1902). On the origin of the lymphatic system from the veins, and the development of the lymph hearts and thoracic duct in the pig. Am J Anat, 1:367‐389. Salmaggi, A., Gelati, M., Dufour, A., Corsini, E., Pagano, S., Baccalini, R., Ferrero, E., Scabini, S., Silei, V., Ciusani, E., and Rossi, M. D. (2002). Expression and modulation of IFN‐gammainducible chemokines (IP‐10, MIG, and I‐TAC) in human brain endothelium and astrocytes: possible relevance for the immune invasion of the central nervous system and the pathogenesis of multiple sclerosis. J Interferon Cytokine Res, 22(6):631‐640. Salmi, M., Koskinen, K., Henttinen, T., Elima, K., and Jalkanen, S. (2004). Clever‐1 mediates lymphocyte transmigration through vascular and lymphatic endothelium. Blood, 104(13):3849‐3857. Saltiel, A. R. and Kahn, C. R. (2001). Insulin signalling and the regulation of glucose and lipid metabolism. Nature, 414(6865):799‐806. Saxena, R., Voight, B. F., Lyssenko, V., Burtt, N. P., de Bakker, P. I. W., Chen, H., Roix, J. J., Kathiresan, S., Hirschhorn, J. N., Daly, M. J., Hughes, T. E., Groop, L., Altshuler, D., Almgren, P., Florez, J. C., Meyer, J., Ardlie, K., Bostrm, K. B., Isomaa, B., Lettre, G., Lindblad, U., Lyon, H. N., Melander, O., Newton‐Cheh, C., Nilsson, P., Orho‐Melander, M., Råstam, L., Speliotes, E. K., Taskinen, M.‐R., Tuomi, T., Guiducci, C., Berglund, A., Carlson, J., Gianniny, L., Hackett, R., Hall, L., Holmkvist, J., Laurila, E., Sjögren, M., Sterner, M., Surti, A., Svensson, M., Svensson, M., Tewhey, R., Blumenstiel, B., Parkin, M., Defelice, M., Barry, R., Brodeur, W., Camarata, J., Chia, N., Fava, M., Gibbons, J., Handsaker, B., Healy, C., Nguyen, K., Gates, C., Sougnez, C., Gage, D., Nizzari, M., Gabriel, S. B., Chirn, G.‐W., Ma, Q., Parikh, H., Richardson, D., Ricke, D., and Purcell, S. (2007). Genome‐wide association analysis identifies loci for type 2 diabetes and triglyceride levels. Science, 316(5829):1331‐1336. Schacht, V., Dadras, S. S., Johnson, L. A., Jackson, D. G., Hong, Y.‐K., and Detmar, M. (2005). Up‐regulation of the lymphatic marker podoplanin, a mucin‐type transmembrane glycoprotein, in human squamous cell carcinomas and germ cell tumors. Am J Pathol, 166(3):913‐921. Schacht, V., Ramirez, M. I., Hong, Y.‐K., Hirakawa, S., Feng, D., Harvey, N., Williams, M., Dvorak, A. M., Dvorak, H. F., Oliver, G., and Detmar, M. (2003). T1alpha/podoplanin deficiency disrupts normal lymphatic vasculature formation and causes lymphedema. EMBO J, 22(14):3546‐3556. Schachtrup, C., Emmler, T., Bleck, B., Sandqvist, A., and Spener, F. (2004). Functional analysis of peroxisome‐proliferator‐responsive element motifs in genes of fatty acid‐binding proteins. Biochem J, 382(Pt 1):239‐245. Schad, H., Flowaczny, H., Brechtelsbauer, H., and Birkenfeld, G. (1978). The significance of respiration for thoracic duct ow in relation to other driving forces of lymph flow. Pugers Arch, 378(2):121‐125. Schalkwijk, C. G. and Stehouwer, C. D. A. (2005). Vascular complications in diabetes mellitus: the role of endothelial dysfunction. Clin Sci (Lond), 109(2):143‐159. Schena, M. (1996). Genome analysis with gene expression microarrays. Bioessays, 18(5):427‐431. Schena, M., Shalon, D., Davis, R. W., and Brown, P. O. (1995). Quantitative monitoring of gene expression patterns with a complementary dna microarray. Science, 270(5235):467‐470. Schittek, B., Paulmann, M., Senyürek, I., and Steffen, H. (2008). The role of antimicrobial peptides in human skin and in skin infectious diseases. Infect Disord Drug Targets, 8(3):135‐143. Schmid‐Schönbein, G. W. (1990). Microlymphatics and lymph flow. Physiol Rev, 70(4):987‐1028. Schneider, M., Conway, E. M., and Carmeliet, P. (2005). Lymph makes you fat. Nat Genet, 37(10):1023‐1024. Schneider, M., Othman‐Hassan, K., Christ, B., and Wilting, J. (1999). Lymphangioblasts in the avian wing bud. Dev Dyn, 216(4‐5):311‐319. Schulthess, F. T., Paroni, F., Sauter, N. S., Shu, L., Ribaux, P., Haataja, L., Strieter, R. M., Oberholzer, J., King, C. C., and Maedler, K. (2009). CXCL10 impairs beta cell function and viability in diabetes through TLR4 signaling. Cell Metab, 9(2):125‐139. Schwarzenberger, K. and Udey, M. C. (1996). Contact allergens and epidermal proinflammatory cytokines modulate langerhans cell e‐cadherin expression in situ. J Invest Dermatol, 106(3):553‐558.

139
Seaman S, Stevens J, Yang MY, Logsdon D, Graff‐Cherry C, St Croix B. (2007). Genes that distinguish physiological and pathological angiogenesis. Cancer Cell, 11(6):539‐554. Seifarth, C. C., Hinkmann, C., Hahn, E.‐G., Lohmann, T., and Harsch, I. A. (2008). Reduced frequency of peripheral dendritic cells in type 2 diabetes. Exp Clin Endocrinol Diabetes, 116(3):162‐166. Senn, J. J., Klover, P. J., Nowak, I. A., Zimmers, T. A., Koniaris, L. G., Furlanetto, R. W., and Mooney, R. A. (2003). Suppressor of cytokine signaling‐3 (SOCS‐3), a potential mediator of interleukin‐6‐dependent insulin resistance in hepatocytes. J Biol Chem, 278(16):13740‐13746. Seyama K, Kumasaka T, Kurihara M, Mitani K, Sato T. (2010). Lymphangioleiomyomatosis: a disease involving the lymphatic system. Lymphat Res Biol, 8(1):21‐31. Shah, B. R. and Hux, J. E. (2003). Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care, 26(2):510‐513. Shields, J. D., Fleury, M. E., Yong, C., Tomei, A. A., Randolph, G. J., and Swartz, M. A. (2007). Autologous chemotaxis as a mechanism of tumor cell homing to lymphatics via interstitial flow and autocrine CCR7 signaling. Cancer Cell, 11(6):526‐538. Shields, J. D., Kourtis, I. C., Tomei, A. A., Roberts, J. M., and Swartz, M. A. (2010). Induction of lymphoidlike stroma and immune escape by tumors that express the chemokine CCL21. Science, 328(5979):749‐752. Simonson, G. D. and Kendall, D. M. (2005). Diagnosis of insulin resistance and associated syndromes: the spectrum from the metabolic syndrome to type 2 diabetes mellitus. Coron Artery Dis, 16(8):465‐472. Singh, U. P., Venkataraman, C., Singh, R., and Lillard, J. W. (2007). CXCR3 axis: role in inflammatory bowel disease and its therapeutic implication. Endocr Metab Immune Disord Drug Targets, 7(2):111‐123. Sladek, R., Rocheleau, G., Rung, J., Dina, C., Shen, L., Serre, D., Boutin, P., Vincent, D., Belisle, A., Hadjadj, S., Balkau, B., Heude, B., Charpentier, G., Hudson, T. J., Montpetit, A., Pshezhetsky, A. V., Prentki, M., Posner, B. I., Balding, D. J., Meyre, D., Polychronakos, C., and Froguel, P. (2007). A genome‐wide association study identifies novel risk loci for type 2 diabetes. Nature, 445(7130):881‐885. Slyke, P. V., Alami, J., Martin, D., Kuliszewski, M., Leong‐Poi, H., Sefton, M. V., and Dumont, D. (2009). Acceleration of diabetic wound healing by an angiopoietin peptide mimetic. Tissue Eng Part A, 15(6):1269‐1280. Sosa‐Pineda, B., Wigle, J. T., and Oliver, G. (2000). Hepatocyte migration during liver development requires PROX1. Nat Genet, 25(3):254‐255. Soukas, A., Cohen, P., Socci, N. D., and Friedman, J. M. (2000). Leptin‐specific patterns of gene expression in white adipose tissue. Genes Dev, 14(8):963‐980. Stacker, S. A., Achen, M. G., Jussila, L., Baldwin, M. E., and Alitalo, K. (2002). Lymphangiogenesis and cancer metastasis. Nat Rev Cancer, 2(8):573‐583. Stacker, S. A., Caesar, C., Baldwin, M. E., Thornton, G. E., Williams, R. A., Prevo, R., Jackson, D. G., Nishikawa, S., Kubo, H., and Achen, M. G. (2001). VEGF‐D promotes the metastatic spread of tumor cells via the lymphatics. Nat Med, 7(2):186‐191. Staiger, H., Machicao, F., Fritsche, A., and Häring, H.‐U. (2009). Pathomechanisms of type 2 diabetes genes. Endocr Rev, 30(6):557‐585. St Croix B, Rago C, Velculescu V, Traverso G, Romans KE, Montgomery E, Lal A, Riggins GJ, Lengauer C, Vogelstein B, Kinzler KW. (2000) Genes expressed in human tumor endothelium. Science, 18;289(5482):1197‐1202. Stehouwer, C. D., Lambert, J., Donker, A. J., and van Hinsbergh, V. W. (1997). Endothelial dysfunction and pathogenesis of diabetic angiopathy. Cardiovasc Res, 34(1):55‐68. Stehouwer, C. D. and Schaper, N. C. (1996). The pathogenesis of vascular complications of diabetes mellitus: one voice or many? Eur J Clin Invest, 26(7):535‐543. Stokić, D., Wick, N., Biely, C., Gurnhofer, E., and Thurner, S. (2006). Statistically consistent identification of differentially expressed genes in DNA chip data over the whole expression range: relative variance method. Appl Bioinformatics, 5(4):277‐284. Stumvoll, M., Goldstein, B. J., and van Haeften, T. W. (2005). Type 2 diabetes: principles of pathogenesis and therapy. Lancet, 365(9467):1333‐1346.

140
Suzuki‐Inoue, K. (2009). CLEC‐2, the novel platelet activation receptor and its internal ligand, podoplanin. Rinsho Ketsueki, 50(5):389‐398. Suzuki‐Inoue, K., Fuller, G. L. J., García, A., Eble, J. A., Pöhlmann, S., Inoue, O., Gartner, T. K., Hughan, S. C., Pearce, A. C., Laing, G. D., Theakston, R. D. G., Schweighoffer, E., Zitzmann, N., Morita, T., Tybulewicz, V. L. J., Ozaki, Y., and Watson, S. P. (2006). A novel SYK‐dependent mechanism of platelet activation by the c‐type lectin receptor CLEC‐2. Blood, 107(2):542‐549. Suzuki‐Inoue, K., Kato, Y., Inoue, O., Kaneko, M. K., Mishima, K., Yatomi, Y., Yamazaki, Y., Narimatsu, H., and Ozaki, Y. (2007). Involvement of the snake toxin receptor CLEC‐2, in podoplanin‐mediated platelet activation, by cancer cells. J Biol Chem, 282(36):25993‐26001. Swartz MA, Lund AW. (2012). Lymphatic and interstitial flow in the tumour microenvironment: linking mechanobiology with immunity. Nat Rev Cancer. 12(3):210‐219. Swartz, M. A. (2001). The physiology of the lymphatic system. Adv Drug Deliv Rev, 50(1‐2):3‐20. Swartz, M. A. and Skobe, M. (2001). Lymphatic function, lymphangiogenesis, and cancer metastasis. Microsc Res Tech, 55(2):92‐99. Tabibiazar R, Cheung L, Han J, Swanson J, Beilhack A, An A, Dadras SS, Rockson N, Joshi S, Wagner R, Rockson SG. (2006). Inflammatory manifestations of experimental lymphatic insufficiency. PLoS Med,3(7):e254. Tammela, T. and Alitalo, K. (2010). Lymphangiogenesis: Molecular mechanisms and future promise. Cell, 140(4):460‐476. Tammela, T., Enholm, B., Alitalo, K., and Paavonen, K. (2005a). The biology of vascular endothelial growth factors. Cardiovasc Res, 65(3):550‐563. Tammela, T., Petrova, T. V., and Alitalo, K. (2005b). Molecular lymphangiogenesis: new players. Trends Cell Biol, 15(8):434‐441. Tammela, T., Saaristo, A., Lohela, M., Morisada, T., Tornberg, J., Norrmén, C., Oike, Y., Pajusola, K., Thurston, G., Suda, T., Ylä‐Herttuala, S., and Alitalo, K. (2005c). Angiopoietin‐1 promotes lymphatic sprouting and hyperplasia. Blood, 105(12):4642‐4648. Tan, N.‐S., Shaw, N. S., Vinckenbosch, N., Liu, P., Yasmin, R., Desvergne, B., Wahli, W., and Noy, N. (2002). Selective cooperation between fatty acid binding proteins and peroxisome proliferator‐activated receptors in regulating transcription. Mol Cell Biol, 22(14):5114‐5127. Tattersal, R. B. and Fajans, S. S. (1975). Prevalence of diabetes and glucose intolerance in 199 offspring of thirty‐seven conjugal diabetic parents. Diabetes, 24(5):452‐462. Thangarajah H, Vial IN, Chang E, El‐Ftesi S, Januszyk M, Chang EI, Paterno J, Neofytou E, Longaker MT, Gurtner GC. (2009). IFATS collection: Adipose stromal cells adopt a proangiogenic phenotype under the influence of hypoxia. Stem Cells,27(1):266‐274. Tilg, H. and Moschen, A. R. (2008). Inflammatory mechanisms in the regulation of insulin resistance. Mol Med, 14(3‐4):222‐231. Trzewik, J., Mallipattu, S. K., Artmann, G. M., Delano, F. A., and Schmid‐Schönbein, G. W. (2001). Evidence for a second valve system in lymphatics: endothelial microvalves. FASEB J, 15(10):1711‐1717. Tuomilehto, J., Lindström, J., Eriksson, J. G., Valle, T. T., Hämäläinen, H., Ilanne‐Parikka, P., Keinänen‐Kiukaanniemi, S., Laakso, M., Louheranta, A., Rastas, M., Salminen, V., Uusitupa, M., and Group, F. D. P. S. (2001). Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med, 344(18):1343‐1350. Uhrin, P., Zaujec, J., Breuss, J. M., Olcaydu, D., Chrenek, P., Stockinger, H., Fuertbauer, E., Moser, M., Haiko, P., Fässler, R., Alitalo, K., Binder, B. R., and Kerjaschki, D. (2010). Novel function for blood platelets and podoplanin in developmental separation of blood and lymphatic circulation. Blood, 115(19):3997‐4005. Ushio‐Fukai, M. (2007). Vegf signaling through nadph oxidase‐derived ros. Antioxid Redox Signal, 9(6):731‐739. Uysal, K. T., Scheja, L., Wiesbrock, S. M., Bonner‐Weir, S., and Hotamisligil, G. S. (2000). Improved glucose and lipid metabolism in genetically obese mice lacking aP2. Endocrinology, 141(9):3388‐3396.

141
Vainionpää, N., Bützow, R., Hukkanen, M., Jackson, D. G., Pihlajaniemi, T., Sakai, L. Y., and Virtanen, I. (2007). Basement membrane protein distribution in LYVE‐1‐immunoreactive lymphatic vessels of normal tissues and ovarian carcinomas. Cell Tissue Res, 328(2):317‐328. van der Putte, S. C. (1975). The early development of the lymphatic system in mouse embryos. Acta Morphol Neerl Scand, 13(4):245‐286. Van Hattem S, Bootsma AH, Thio HB. (2008). Skin manifestations of diabetes. Cleve Clin J Med, 75(11):772‐787. van Tilburg, J., van Haeften, T. W., Pearson, P., and Wijmenga, C. (2001). Defining the genetic contribution of type 2 diabetes mellitus. J Med Genet, 38(9):569‐578. Vigl B, Aebischer D, Nitschké M, Iolyeva M, Röthlin T, Antsiferova O, Halin C. (2011). Tissue inflammation modulates gene expression of lymphatic endothelial cells and dendritic cell migration in a stimulus‐dependent manner. Blood, 7;118(1):205‐215. Vigl, B., Zgraggen, C., Rehman, N., Banziger‐Tobler, N. E., Detmar, M., and Halin, C. (2009). Coxsackie‐ and adenovirus receptor (car) is expressed in lymphatic vessels in human skin and affects lymphatic endothelial cell function in vitro. Exp Cell Res, 315(2):336‐347. Vijayaraghavan, S., Hitman, G. A., and Kopelman, P. G. (1994). Apolipoprotein‐D polymorphism: a genetic marker for obesity and hyperinsulinemia. J Clin Endocrinol Metab, 79(2):568‐570. von Andrian, U. H. and Mempel, T. R. (2003). Homing and cellular traffic in lymph nodes. Nat Rev Immunol, 3(11):867‐878. von der Weid PY, Rehal S, Ferraz JG. (2011) Role of the lymphatic system in the pathogenesis of Crohn's disease. Curr Opin Gastroenterol, 27(4):335‐341. Wegner, L., Andersen, G., Sparso, T., Grarup, N., Glümer, C., Borch‐Johnsen, K., Jorgensen, T., Hansen, T., and Pedersen, O. (2007). Common variation in LMNA increases susceptibility to type 2 diabetes and associates with elevated fasting glycemia and estimates of body fat and height in the general population: studies of 7,495 danish whites. Diabetes, 56(3):694‐698. Weisberg, S. P., McCann, D., Desai, M., Rosenbaum, M., Leibel, R. L., and Ferrante, A. W. (2003). Obesity is associated with macrophage accumulation in adipose tissue. J Clin Invest, 112(12):1796‐1808. Wetzler C, Kämpfer H, Stallmeyer B, Pfeilschifter J, Frank S. (2000). Large and sustained induction of chemokines during impaired wound healing in the genetically diabetic mouse: prolonged persistence of neutrophils and macrophages during the late phase of repair. J Invest Dermatol, 115(2):245‐253. Wick, N., Bruck, J., Gurnhofer, E., Steiner, C.‐W., Giovanoli, P., Kerjaschki, D., and Thurner, S. (2004). Nonuniform hybridization: a potential source of error in oligonucleotide‐chip experiments with low amounts of starting material. Diagn Mol Pathol, 13(3):151‐159. Wick, N., Haluza, D., Gurnhofer, E., Raab, I., Kasimir, M.‐T., Prinz, M., Steiner, C.‐W., Reinisch, C., Howorka, A., Giovanoli, P., Buchsbaum, S., Krieger, S., Tschachler, E., Petzelbauer, P., and Kerjaschki, D. (2008). Lymphatic precollectors contain a novel, specialized subpopulation of podoplanin low, CCL27‐expressing lymphatic endothelial cells. Am J Pathol, 173(4):1202‐1209. Wick, N., Saharinen, P., Saharinen, J., Gurnhofer, E., Steiner, C. W., Raab, I., Stokic, D., Giovanoli, P., Buchsbaum, S., Burchard, A., Thurner, S., Alitalo, K., and Kerjaschki, D. (2007). Transcriptomal comparison of human dermal lymphatic endothelial cells ex vivo and in vitro. Physiol Genomics, 28(2):179‐192. Wicki, A. and Christofori, G. (2007). The potential role of podoplanin in tumour invasion. Br J Cancer, 96(1):1‐5. Wicki, A., Lehembre, F., Wick, N., Hantusch, B., Kerjaschki, D., and Christofori, G. (2006). Tumor invasion in the absence of epithelial‐mesenchymal transition: podoplanin‐mediated remodeling of the actin cytoskeleton. Cancer Cell, 9(4):261‐272. Wiggins, H. and Rappoport, J. (2010). An agarose spot assay for chemotactic invasion. Biotechniques, 48(2):121‐124. Wigle, J. T., Chowdhury, K., Gruss, P., and Oliver, G. (1999). PROX1 function is crucial for mouse lens‐fibre elongation. Nat Genet, 21(3):318‐322. Wigle, J. T., Harvey, N., Detmar, M., Lagutina, I., Grosveld, G., Gunn, M. D., Jackson, D. G., and Oliver, G. (2002). An essential role for prox1 in the induction of the lymphatic endothelial cell phenotype. EMBO J, 21(7):1505‐1513.

142
Wigle, J. T. and Oliver, G. (1999). PROX1 function is required for the development of the murine lymphatic system. Cell, 98(6):769‐778. Wild, S., Roglic, G., Green, A., Sicree, R., and King, H. (2004). Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care, 27(5):1047‐1053. Wilting, J., Papoutsi, M., Christ, B., Nicolaides, K. H., von Kaisenberg, C. S., Borges, J., Stark, G. B., Alitalo, K., Tomarev, S. I., Niemeyer, C., and Rössler, J. (2002). The transcription factor PROX1 is a marker for lymphatic endothelial cells in normal and diseased human tissues. FASEB J, 16(10):1271‐1273. Wolfrum, C. (2007). Cytoplasmic fatty acid binding protein sensing fatty acids for peroxisome proliferator activated receptor activation. Cell Mol Life Sci, 64(19‐20):2465‐2476. Xu, H., Barnes, G. T., Yang, Q., Tan, G., Yang, D., Chou, C. J., Sole, J., Nichols, A., Ross, J. S., Tartaglia, L. A., and Chen, H. (2003). Chronic inflammation in fat plays a crucial role in the development of obesity‐related insulin resistance. J Clin Invest, 112(12):1821‐1830. Xu, Y., Yuan, L., Mak, J., Pardanaud, L., Caunt, M., Kasman, I., Larrivée, B., Toro, R. D., Suchting, S., Medvinsky, A., Silva, J., Yang, J., Thomas, J.‐L., Koch, A. W., Alitalo, K., Eichmann, A., and Bagri, A. (2010). Neuropilin‐2 mediates VEGF‐C‐induced lymphatic sprouting together with VEGFR3. J Cell Biol, 188(1):115‐130. Yang, C.‐X., Shi, J.‐F., and Gu, G.‐H. (2007). Single nucleotide polymorphism analysis applied to research susceptible genes of type 2 diabetes. Journal of Clinical Rehabilitative Tissue Engineering Research, 11:2559‐2562. Ye, J.‐M., Dzamko, N., Cleasby, M. E., Hegarty, B. D., Furler, S. M., Cooney, G. J., and Kraegen, E. W. (2004). Direct demonstration of lipid sequestration as a mechanism by which rosiglitazone prevents fatty‐acid‐induced insulin resistance in the rat: comparison with metformin. Diabetologia, 47(7):1306‐1313. Yin N, Zhang N, Lal G, Xu J, Yan M, Ding Y, Bromberg JS. (2011) Lymphangiogenesis is required for pancreatic islet inflammation and diabetes. PLoS One, 6(11):e28023. Yki‐Järvinen, H. (2004). Thiazolidinediones. N Engl J Med, 351(11):1106‐1118. Yong C, Bridenbaugh EA, Zawieja DC, Swartz MA. (2007). Microarray analysis of VEGF‐C responsive genes in human lymphatic endothelial cells. Lymphat Res Biol,3(4):183‐207. Yoshizumi, M., Perrella, M. A., Burnett, J. C., and Lee, M. E. (1993). Tumor necrosis factor downregulates an endothelial nitric oxide synthase mRNA by shortening its half‐life. Circ Res, 73(1):205‐209. You, J.‐J., Yang, C.‐H., Chen, M.‐S., and Yang, C.‐M. (2009). Cysteine‐rich 61, a member of the CCN family, as a factor involved in the pathogenesis of proliferative diabetic retinopathy. Invest Ophthalmol Vis Sci, 50(7):3447‐3455. You, L.‐R., Lin, F.‐J., Lee, C. T., DeMayo, F. J., Tsai, M.‐J., and Tsai, S. Y. (2005). Suppression of Notch signalling by the COUP‐TFII transcription factor regulates vein identity. Nature, 435(7038):98‐104. Yuan, L., Moyon, D., Pardanaud, L., Bréant, C., Karkkainen, M. J., Alitalo, K., and Eichmann, A. (2002). Abnormal lymphatic vessel development in neuropilin 2 mutant mice. Development, 129(20):4797‐4806. Zampell JC, Aschen S, Weitman ES, Yan A, Elhadad S, De Brot M, Mehrara BJ. (2012). Regulation of adipogenesis by lymphatic fluid stasis: part I. Adipogenesis, fibrosis, and inflammation. Plast Reconstr Surg, 129(4):825‐834. Zampetaki A, Kiechl S, Drozdov I, Willeit P, Mayr U, Prokopi M, Mayr A, Weger S, Oberhollenzer F, Bonora E, Shah A, Willeit J, Mayr M. (2010). Plasma microRNA profiling reveals loss of endothelial miR‐126 and other microRNAs in type 2 diabetes. Circ Res, 107(6):810‐817. Zeggini, E., Scott, L. J., Saxena, R., Voight, B. F., Marchini, J. L., Hu, T., de Bakker, P. I. W., Abecasis, G. R., Almgren, P., Andersen, G., Ardlie, K., Bostrm, K. B., Bergman, R. N., Bonnycastle, L. L., Borch‐Johnsen, K., Burtt, N. P., Chen, H., Chines, P. S., Daly, M. J., Deodhar, P., Ding, C.‐J., Doney, A. S. F., Duren, W. L., Elliott, K. S., Erdos, M. R., Frayling, T. M., Freathy, R. M., Gianniny, L., Grallert, H., Grarup, N., Groves, C. J., Guiducci, C., Hansen, T., Herder, C., Hitman, G. A., Hughes, T. E., Isomaa, B., Jackson, A. U., Jrgensen, T., Kong, A., Kubalanza, K., Kuruvilla, F. G., Kuusisto, J., Langenberg, C., Lango, H., Lauritzen, T., Li, Y., Lindgren, C. M., Lyssenko, V., Marvelle, A. F., Meisinger, C., Midthjell, K., Mohlke, K. L., Morken, M. A., Morris, A. D., Narisu, N., Nilsson, P., Owen, K. R., Palmer, C. N. A., Payne, F., Perry, J. R. B., Pettersen, E., Platou, C., Prokopenko, I., Qi, L., Qin, L., Rayner, N. W., Rees, M., Roix, J. J., Sandbaek, A., Shields, B., Sjgren, M., Steinthorsdottir, V., Stringham, H. M., Swift, A. J., Thorleifsson, G., Thorsteinsdottir, U., Timpson, N. J., Tuomi, T., Tuomilehto, J., Walker, M., Watanabe, R. M., Weedon, M. N., Willer, C. J., Consortium, W. T. C. C., Illig, T., Hveem, K., Hu, F. B., Laakso, M., Stefansson, K., Pedersen, O., Wareham, N. J., Barroso, I., Hattersley, A. T., Collins, F. S., Groop, L., McCarthy, M. I., Boehnke, M., and

143
Altshuler, D. (2008). Meta‐analysis of genome‐wide association data and large‐scale replication identifies additional susceptibility loci for type 2 diabetes. Nat Genet, 40(5):638‐645. Zen, K., Liu, Y., McCall, I. C., Wu, T., Lee, W., Babbin, B. A., Nusrat, A., and Parkos, C. A. (2005). Neutrophil migration across tight junctions is mediated by adhesive interactions between epithelial coxsackie and adenovirus receptor and a junctional adhesion molecule‐like protein on neutrophils. Mol Biol Cell, 16(6):2694‐2703. Zeyda, M., Farmer, D., Todoric, J., Aszmann, O., Speiser, M., Györi, G., Zlabinger, G. J., and Stulnig, T. M. (2007). Human adipose tissue macrophages are of an anti‐inflammatory phenotype but capable of excessive pro‐inflammatory mediator production. Int J Obes (Lond), 31(9):1420‐1428. Zeyda, M. and Stulnig, T. M. (2007). Adipose tissue macrophages. Immunol Lett, 112(2):61‐67. Zeyda, M. and Stulnig, T. M. (2009). Obesity, inflammation, and insulin resistance‐a mini‐review. Gerontology, 55(4):379‐386. Zhang, Q., Lu, Y., Proulx, S. T., Guo, R., Yao, Z., Schwarz, E. M., Boyce, B. F., and Xing, L. (2007). Increased lymphangiogenesis in joints of mice with inflammatory arthritis. Arthritis Res Ther, 9(6):R118.

144
Curriculum vitae Contact details
Private address: Blumenthalstraße 49 69120 Heidelberg, Deutschland
Working address: University of Heidelberg German Cancer Research Center (DKFZ) Institute of Pathology Helmholtz‐University‐Group "Molecular
RNA Biology & Cancer" Im Neuenheimer Feld 224 Im Neuenheimer Feld 280 69120 Heidelberg 69120 Heidelberg Email: [email protected]; [email protected]‐heidelberg.de Mobil: +49‐1577‐8408901 Personal Information
Date and Place of Birth: 22 June 1983, Lustenau/Vorarlberg, Austria Nationality: Austrian Academic Degree: Medical Doctor (MD) Education
2010present: Resident pathologist at the Institute of Pathology, University Hospital & University of Heidelberg
2010present: Postdoctoral research fellow at the Research Group "Molecular RNA Biology & Cancer" – Dr. Sven Diederichs (www.diederichslab.org) Main focus on: Identification and functional analysis of long noncoding RNAs in hepatocellular carcinoma
2007present: PhD student at the Clinical Institute of Pathology, General
Hospital and Medical University Vienna, Austria: “Molecular and functional characterization of lymphatic vessels and
lymphatic endothelial cells in type 2 diabetes mellitus”

145
July – Dec 2011: Gerok stipend within the SFB TRR77 ‘Liver cancer’: Subproject B3 (Non‐coding RNAs in Hepatocellular Carcinoma), Dr. Sven Diederichs
September 2007: Research internship at the Institute of Physiology, Katowice University,
Poland “Matrix Metalloproteinases in child tumors”
20062007: MD thesis at the Neurological Research Laboratory Innsbruck: ”Matrix Metalloproteinases and their Inhibitors in Multiple Sclerosis: Correlation with Inflammation and Clinical Parameters”
20012007: Studies of Human Medicine at the Medical University of Innsbruck, Austria (Graduation: 08/2007)
Scholarships
2005: Scholarship of the Federal State of Vorarlberg for a study visit at the UniversityHospital Monterrey, Mexico
2006: Merit scholarship of the Medical University of Innsbruck
Language skills German: Mother tongue English: fluent in speaking and writing French: basic Swedish: basic Software skills Statistical software: SPSS, R Office: MS Office (Word, Excel, PowerPoint), Open Office, Adobe Creative Suite
(Acrobat, Illustrator, Photoshop), Latex, Jabref, Endnote Operating systems: Windows, Linux Other activities
Project manager: Molecular mechanisms of diabetic microangiopathy Responsible Organizer:
‐ BRIDGING THE GAP ‐ International workshop on cell communication in health and disease (February 2009 and 2010) at the Medical University of Vienna (www.phd‐cchd.at/cchd‐workshop)
Member of the Young Scientist Association (YSA) of the Medical University (www.ysa‐muv.org) and organisation of the PhD‐Symposium 2010 at the Medical University of Vienna

146
Publications M. Hämmerle, T.M. Keller, B. Hantusch, D. Kerjaschki. Transcriptome analysis reveals inflammatory, growth and lipid metabolic changes of lymphatic vessels in human type 2 diabetes. In revision. T. Gutschner, M. Hämmerle, M. Eißmann, J. Hsu, Y. Kim, G. Hung, A. Revenko, G. Arun, M. Stentrup, M. Groß, M. Zörnig, A. Robert MacLeod, D. L. Spector, S. Diederichs The noncoding RNA MALAT1 is a critical regulator of the metastasis phenotype of lung cancer cells. In revision. M. Polycarpou‐Schwarz, T. Gutschner, M. Hämmerle, S. Grund, A. Roth, C. Hildenbrand, A. Warth, T. Longerich, S. Aulmann, J. Rom, M. Meister, T. Muley, H. Zabeck, S. Schmidt, T. Ivacevic, V. Benes, K. Breuhahn, P. Schnabel, P. Sinn, H. Hoffmann, P. Schirmacher, S. Diederichs Defining the noncoding RNA landscape of lung, liver and breast cancer reveals concerted regulation, novel tumorassociated long ncRNAs and high tissue specificity. Submitted. M. Eißmann*, T. Gutschner*, M. Hämmerle, S. Günther, M. Caudron‐Herger, M. Groß, P. Schirmacher, K. Rippe, T. Braun, M. Zörnig* and S. Diederichs*. Loss of the abundant nuclear noncoding RNA MALAT1 is compatible with life and development. RNA Biology 2012, Aug 1;9(8). M. Zeyda, B. Wernly, S. Demyanets, C. Kaun, M. Hämmerle, B. Hantusch, M. Schranz, A. Neuhofer, B.K. Itariu, M. Keck, G. Prager, J. Wojta, T.M. Stulnig. Severe obesity increases adipose tissue expression of interleukin‐33 and its receptor ST2, both predominantly detectable in endothelial cells of human adipose tissue. Int J Obes (Lond). 2012 Jul 17. [Epub ahead of print] C. Vonach, K. Viola, B. Giessrigl, N. Huttary, I. Raab, R. Kalt, S. Krieger, TP. Vo, S. Madlener, S. Bauer, B. Marian, M. Hämmerle, N. Kretschy, M. Teichmann, B. Hantusch, S. Stary, C. Unger, M. Seelinger, A. Eger, R. Mader, W. Jäger, W. Schmidt, M. Grusch, N. Dolznig, W. Mikulits, G. Krupitza. NFκB mediates the 12(S)HETEinduced endothelial to mesenchymal transition of lymphendothelial cells during the intravasation of breast carcinoma cells. British Journal of Cancer 2011; 105(2):263‐71. D. Kerjaschki, M. Rudas, G. Bartel, Z. Bago‐Horvath, V. Sexl, S. Wolbank, C. Schneckenleithner, H. Dolznig, S. Krieger, B. Hantusch, K. Nagy‐Bojarszky, N. Huttary, I. Raab, R. Kalt, K. Lackner, M. Hämmerle, T. Keller, K. Viola, M. Schreiber, A. Nader, W. Mikulits, M. Gnant, K. Krautgasser, H. Schachner, K. Kaserer, S. Rezar, S. Madlener, C. Vonach, A. Davidovits, H. Nosaka, S. Hirakawa, M. Detmar, K. Alitalo, S. Nijman, F. Offner, T. J. Maier, D. Steinhilber and G. Krupitza. Lipoxygenase driven tumor cell invasion of intrametastatic lymphatic vessels propagates lymph node metastasis of human carcinomas. Journal of Clinical Investigation 2011; 121(5):2000‐12. M. Hämmerle, T.M. Keller, B. Hantusch, D. Stokic, C.W. Steiner, D. Kerjaschki. Transcriptomal comparison of human dermal diabetic versus nondiabetic lymphatic endothelial cells ex vivo. Wiener Klinische Wochenschrift 2008; Vol. 120 (Suppl. 1): 117. B. Kuenz, A. Lutterotti, R. Ehling, C. Gneiss, M. Hämmerle, C. Rainer, F. Deisenhammer, M. Schocke, T. Berger, M. Reindl. Cerebrospinal fluid B cells correlate with early brain inflammation in multiple sclerosis. PLoS ONE. 2008 Jul 2;3(7):e2559.

147
M. Hämmerle, T.M. Keller, B. Hantusch, D. Stokic, N. Wick, E. Gurnhofer, S. Thurner, D. Kerjaschki. Transcriptomal comparison of human dermal diabetic versus nondiabetic lymphatic endothelial cells ex vivo. Der Pathologe 2008, Suppl. 1: 26 (Do‐091). B. Kuenz, A. Lutterotti, R. Ehling, C. Gneiss, M. Hämmerle, M. Schocke, T. Berger, M. Reindl. Cerebrospinal fluid B cells correlate with early brain inflammation in multiple sclerosis. Multiple Sclerosis 2008, 14 (Suppl. 1): S133‐134 (P 356). M. Hämmerle. Matrix metalloproteinases and their inhibitors in multiple sclerosis – Correlation with inflammation and clinical parameters. Medizinische Dissertation, Medizinische Universität Innsbruck. Scientific presentations
Talks: M. Hämmerle Molecular and functional analysis of long noncoding RNAs in hepatocellular carcinoma. German Society of Pathology (DGP), Berlin, Germany, May 2012 M Hämmerle. Noncoding RNA in malignant tumors: A new world of tumor biomarkers and target structures in cancer cells. German Society for Endocrinology (DGE), Mannheim, Germany, March 2012. M. Hämmerle. Molecular and Functional Analysis of long noncoding RNAs in Liver Cancer. SFB TRR77 Annual Meeting, Fulda, Germany, November 2011. M Hämmerle Noncoding RNA profiling in hepatocellular carcinoma. German Society of Pathology (DGP), Leipzig, Germany, June 2011. M. Hämmerle. Morphological and molecular characterization of lymphatic vessels and lymphatic endothelial cells in type 2 diabetes mellitus. Invited talk, German Cancer Research Center, Heidelberg, May 2010. M. Hämmerle. Morphological and molecular characterization of lymphatic vessels and lymphatic endothelial cells in type 2 diabetes mellitus. Invited talk, Institute of Pathology, Heidelberg, April 2010. M. Hämmerle. Characterization of lymphatic endothelial cells in type 2 diabetes mellitus. Hearing of the Austrian Science Fund (FWF), Vienna, May 2009. M. Hämmerle. Characterization of diabetic versus nondiabetic lymphatic endothelial cells ex vivo. '92. Jahrestagung der Deutschen Gesellschaft für Pathologie', Berlin, May 2008.

148
Posters: M. Hämmerle, T. Gutschner, S. Diederichs. Molecular and Functional Analysis of long noncoding RNAs in Liver Cancer. SFB TRR77 Annual Meeting, Fulda, Germany, November 2011. M. Hämmerle, T. Gutschner, H. Uckelmann, M. Baas, K. Breuhahn, P. Schirmacher, S. Diederichs. Molecular and Functional Analysis of long noncoding RNAs in Liver Cancer. 12th Young Scientist Meeting of the German Society of Cell Biology (DGZ): "RNA & Disease", Jena, Germany, September 2011. M. Hämmerle, T.M. Keller, C.W. Steiner, D. Stokic, B. Hantusch D. Kerjaschki. Lymphatic endothelial cells and lymphatic vessels are altered by the diabetic condition. 6th PhD Symposium, Medical University Vienna, June 2010. M. Hämmerle, T.M. Keller, B. Hantusch, C.W. Steiner, D. Haluza, D. Kerjaschki. Characterization of lymphatic endothelial cells in type 2 diabetes. 5th PhD Symposium, Medical University Vienna, June 2009. M. Hämmerle, T.M. Keller, B. Hantusch, C.W. Steiner, D. Haluza, D. Kerjaschki. Characterization of lymphatic endothelial cells in type 2 diabetes. ESH: Interdisciplinary Conference on Angiogenesis, Helsinki, June 2009. M. Hämmerle, T.M. Keller, B. Hantusch, C.W. Steiner, D. Haluza, D. Kerjaschki. Characterization of lymphatic endothelial cells in type 2 diabetes. EMBO Workshop: Lymphatic & blood vasculature ‐ from models to human disease, Biomedicum Helsinki, June 2009. M. Hämmerle, T.M. Keller, B. Hantusch, C.W. Steiner, D. Haluza, D. Kerjaschki. Transcriptomal comparison of diabetic versus nondiabetic lymphatic endothelial cells ex vivo. Joint Annual Meeting of Immunology, Vienna General Hospital, September 2008. M. Hämmerle, T.M. Keller, B. Hantusch, C.W. Steiner, D. Haluza, D. Kerjaschki. Transcriptomal comparison of diabetic versus nondiabetic lymphatic endothelial cells ex vivo. 4th PhD Symposium, Medical University Vienna, May 2008. M. Hämmerle, T.M. Keller, B. Hantusch, C.W. Steiner, D. Haluza, D. Kerjaschki. Transcriptomal comparison of diabetic versus nondiabetic lymphatic endothelial cells ex vivo. Gordon Research Conference, Ventura, March 2008. B. Künz, M. Hämmerle, R. Ehling, A. Lutterotti, C. Gnei, K. Egger, M. Schocke, T. Berger, M. Reindl. Characterization of Cell Populations in Cerebrospinal Fluid of Patients with Multiple Sclerosis. 6. Jahrestagung der Österreichischen Gesellschaft für Neurologie, Innsbruck, February 2008. B. Künz, M. Hämmerle, R. Ehling, C. Gneiss, A. Millonig, F. Deisenhammer, T. Berger, M. Reindl. Characterization of Cell Populations in Cerebrospinal Fluid of Patients with Multiple Sclerosis. 3rd Meeting of Doctoral students from Innsbruck's Medical University, November 2007.