Embed Size (px)
Citation preview

Improving the management of patients withmental ill health in emergency care settingsChecklist
This checklist offers practical support andguidance, as well as diagnostic tools, to helpyou improve the care of patients with mental illhealth who access emergency care services. Itoutlines areas for action and includes examplesof the ways in which some services areaddressing a number of these challenges.
The checklist is intended for anyone involvedin providing care for these patients, including
mental health practitioners and staff workingfor ambulance trusts and in emergencydepartments. We hope it will help you toprovide faster, better treatment for mentalhealth patients in a crisis and improve theirexperience of services.
This is not intended to be a definitive list ofsuggestions. Many of these suggestions havealready been adopted by some trusts, while
others have taken different approaches. We will be updating the list regularly, so further ideas will be welcomed.
Click here to enter the checklistCLOSE
checklistClick toENTER
Professor Sir George Alberti National Clinical Director for Emergency Access
Professor Louis ApplebyNational Clinical Director for Mental Health
USING the
checklist
Last updated September 2004
Welcome
Using this checklistThis checklist has been produced in PDF format. It isdesigned to be used on screen where you can click betweenthe different sections and use the live links to access otherrelevant information and resources on the web.
The checklist is organised into nine main sectionsdisplayed down the side of the page. Just click on a tabto go to the related suggestions and information.
Viewing tip: Go to ‘view’ at the top of your AcrobatReader page and select ‘full screen’ or ‘fit in window’ fromthe drop-down menu to see the checklist more clearly.
Printing tip: PDFs are printer-friendly and can be easilyprinted out for off-line reference.
If you have any feedback about thischecklist email us [email protected]
Click here to enter the checklistCLOSE
checklistClick toENTER
USING the
checklist
Improving the management of patients withmental ill health in emergency care settingsChecklist
ContextIt is estimated that up to five per cent ofthose attending an emergency departmenthave a primary diagnosis of mental ill health,of which substance misuse and deliberateself-harm (DSH) are the largest groups. Afurther 20-30 per cent of attendees have co-existing physical and psychologicalproblems, with much of the latter remainingundetected. It is estimated that 35 per centof emergency departments attendances arerelated to alcohol including violent assaults,road traffic accidents, mental healthemergencies and deliberate self-harm.
In January 2004, a Department of Health audit suggested that up to 10 per cent ofemergency departments’ four hour breachesinvolved patients with mental ill health. Inaddition, a third of patients with mental illhealth wait longer than four hours,
compared to 10 per cent of all patients.Understanding the causes of such delay isessential to being able to achieveimprovements.
These issues can only be addressed throughgenuine local partnerships between allagencies. Most of the actions suggested in this checklist cannot be taken by acutetrusts alone. The first step must be for all therelevant parties to agree how to worktogether. Local emergency care networks arean ideal forum for this. Emergency care leads should ensure that their network has engaged all key parties and hasappropriate representation from local mentalhealth trusts.
The role and functioning of emergencymental health care must be considered in
relation to how the remainder of the localemergency care system and crisis mentalhealth care functions, so as to exploit localstrengths and avoid unnecessary duplicationof resources. This is particularly true forrelationships between those providing crisisservices (e.g. crisis intervention teams,gateway workers, liaison psychiatry teams,approved social worker services). Major re-design will also need to engageother health/social care providers as well as the police.
To qualify for payment of £200,000, mentalhealth trusts have been invited to submitplans to SHAs showing how they willimprove 24/7 crisis services. Their progresswill be assessed over the period March –December 2004.
Click here to enter the checklistCLOSE
checklistClick toENTER
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
General adviceThere are some over-arching principles that will help you bettermanage the care of patients withmental ill health:
Involve and inform patients■ Involve patients in the development
of services. Consider the wholepatient journey from the viewpointof the patient.A change in onecomponent of care often affectsother aspects of the patient journey.
■ Develop clear information onavailable services for patients andfor staff to use in sign-posting andreferring patients.
Work with other service providers■ Develop partnerships between local
mental health services, primary care,ambulance services and emergencydepartments. Mental health trustsshould be actively involved in theiremergency care network.
■ Local implementation teams shouldinclude crisis access to mental healthcare as part of their remit.
■ Develop interagency informationsharing protocols to ensure thatinformation on mental healthpatients at risk of violence to othersor significant harm to themselvescan be shared with all relevantagencies, including emergencydepartments and ambulanceservices.
Back toSTART
CLOSEchecklist Page 1 of 2
Improving the management of patients withmental ill health in emergency care settingsChecklist
Link-upThe Emergency carenetworks checklist providesguidance on establishing orstrengthening existingnetworks. The PatientInformation Toolkit offerspractical support andguidance to help you provideinformation for patients inyour emergency department.Both toolkits are available atwww.dh.gov.uk/PolicyandGuidance/OrganisationPolicy/EmergencyCare/EmergencyCareChecklists
General advice
Benchmarking tool
Useful resources
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
General adviceUnderstand local needsAnalysing data effectively andassessing local needs and issues willhelp you prioritise where local actionshould be targeted. Methodologiessuch as process mapping may behelpful. Consider:
■ What resources are available locally?
■ Who uses your emergency care services and when?
■ How appropriate is this use?
■ What other services are availableto patients with mental ill-health?
■ What delays and blockages arethere? Why do they occur?
Consider new roles and teamswhen planning services■ Develop gateway worker posts -
these are designed to help improveaccess to mental health services for patients and improve theinterface between specialist mentalhealth and other services. It will beimportant that their role and that ofany existing liaison and specialist mental health services are co-ordinated to ensure integration ofeffort and to prevent isolation.
■ Mental health trusts shouldnominate an appropriate memberof staff to act as a liaison personwith emergency departments, suchas a gateway worker or a memberof the local crisis resolution team.Similarly, emergency departmentsshould have a person nominated forliaison with mental health services,such as a member of the liaison
psychiatry service or an appropriateperson from the emergencydepartment itself.
■ There are a variety of ways oforganising appropriate mentalhealth input to emergencydepartments. Models include liaisonpsychiatry services, which alsoprovide valuable support to generalhospital patients, dedicated mentalhealth nurses or dedicated inputfrom specialist mental healthservices.
Back toSTART
CLOSEchecklist Page 2 of 2
Positive practice pages
Improving the management of patients withmental ill health in emergency care settingsChecklist
Training
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
General advice
Ambulance services
General advice
Positive practice – understandingreasons for delayThe 28 day mental health analysis toolfor emergency department data hasbeen developed by the Department ofHealth and the Modernisation Agency.The purpose of this core analysis is toprovide a structure for clinicians andoperational managers to identify theparticular causes of performanceproblems and therefore focusimprovement effort in the placeswhere it will have the most benefit.Use of this analysis is entirely voluntary.
The 28 day mental health analysistool is available.
For further information or to requestthe analysis tool please [email protected]
Back toSTART
CLOSEchecklist
Positive practice 1 2 3Positive practice examples 1 2
Link-upInformation on serviceimprovement programs andmethodologies is availableat the National Institute forMental Health in England orthe Emergency ServicesCollaborative websiteswww.nimhe.org.uk orwww.modern.nhs.uk/scripts/default.asp?site_id=35
Back to general advice
Improving the management of patients withmental ill health in emergency care settingsChecklist
Training
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
General advice
Ambulance services
General advice
Positive practice – sharing patient information betweenservice providersIn the control room at LondonAmbulance Service NHS trust, a pilotscheme to reduce serious incidentsinvolving people with severe mentalillness through timely informationsharing is underway. This service isopen 24 hours a day and is staffed bya team of mental health professionals.The team maintains a database of riskinformation provided by staff incommunity mental health teams,after they have carried out a formalrisk assessment with individual serviceusers, about individuals judged to bea risk either to themselves or toothers. Kirsty Jarvie, project manager,said: "The team have been trained todisclose information within a legal
framework. Therefore, ambulancecrews, mental health staff based inA&E departments and communitymental health professionals, amongstothers, are all able to requestinformation from this service. Theservice also acts as a gateway for mental health staff to accessinformation held by the MetropolitanPolice and London Probation Area."
Back toSTART
CLOSEchecklist
Positive practice 1 2 3Positive practice examples 1 2
Link-upFor further [email protected] seewww.londondevelopmentcentre.org
Back to general advice
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Back toSTART
CLOSEchecklist
Training
Useful resources
Training
It is vital to ensure that emergencycare clinicians have the correct skillsto provide appropriate care forpatients with mental ill health.
■ Every first contact practitioner,including ambulance andemergency department staff,should have training in basicmental health issues and riskassessment. First contactpractitioners should feelconfident in making an initialassessment of people withmental ill health. Further trainingsuch as the management ofbereavement or substance misuse interventions should alsobe considered.
■ Continuing training anddevelopment for emergency carestaff with an interest in mentalhealth or experience in the fieldshould be considered. This couldtake the form of learning setswithin a local area.
■ Common training initiativesinvolving both mental health andemergency care staff not onlyaddress mutual training issues but can also lead to majoroperational benefits.
Positive practice pages
Improving the management of patients withmental ill health in emergency care settingsChecklist
Training
Ambulance services
Back toSTART
CLOSEchecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
TrainingPositive practice examples 1 2
Link-upPositive practice – training foremergency department nursesSt George’s Hospital NHS trust runsa one day training programme foremergency department nurses. Itprovides them with: ■ a broad understanding of mental
ill health and possible causes ofbehaviours and symptoms.
■ an opportunity to exploreattitudes towards people withmental ill health.
■ skills to conduct a triageassessment.
■ skills to manage distressed and/or disturbed patients in an emergency departmentenvironment.
An emergency department nursesaid: "I am more confident aboutworking with patients who havemental health problems and feelbetter equipped to assess thesepatients.”
For further informationcontact [email protected]
Improving the management of patients withmental ill health in emergency care settingsChecklist
Ambulance services
Back toSTART
CLOSEchecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Training
Positive practice – training forwalk-in centre staffA training pilot was carried out ineight walk-in centres (WICs). Its aimwas to develop the capacity andcapabilities of WIC staff to identify,assess and manage patientsattending WICs with mental illhealth. SCAN (Screen, Care, Advice,Next steps) is a focused skills-drivenassessment process used across NHSDirect. Nurses were given three daysof SCAN and risk managementtraining. Elaine Egan-Morriss,project manager, said: "Wedeveloped a CD-ROM called‘Directly about mental health –primary care’ and issued it to allstaff. This incorporated learning onmental health problems andexamples of face to face
consultations that were typical ofthe kind of patients that wouldpresent in primary care. Referralpathways were also developed. Theprogramme improved the servicefor patients with an identifiedmental health need, ensuredreferrals were appropriate andhelped sign-post patients to otherservices.”
Positive practice examples 1 2
Link-upFor further [email protected]
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Back toSTART
CLOSEchecklist
Ambulance services
Useful resources
Ambulance servicesAmbulance staff, including controlroom staff and ambulance crews, areoften the first contact for manypatients with mental ill health in acrisis. There are a number of actionsfor ambulance trusts to help improvethe management of patients withmental ill health.These include:
■ Training to ensure ambulance staffcan understand and recognise basicmental ill health and undertakebasic assessment, including assessment of risk.
■ Working with out of hours GPservices to ensure rapid response to referrals from the ambulanceservice, and to agree appropriateresponse times.
■ Agreeing local response guidelines(comparable to those for emergency departments – seesection on assessment) whenmental health teams are required at a person’s home.
■ Ensuring that ambulance crewshave access to advice aboutmental ill health in general andwhen appropriate, access to adviceabout individual patients.
■ Working with other organisationsto agree appropriate care andtreatment for patients alreadyknown to the service. This couldinclude patients being taken directly by ambulance to mentalhealth units or patients beingreferred direct to primary care, crisis intervention teams or to social services.
Positive practice pages
Improving the management of patients withmental ill health in emergency care settingsChecklist
Ambulance services
Back toSTART
CLOSEchecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Ambulance services
Positive practice – developingalternatives to emergencydepartments for patients withmental ill healthStaffordshire NHS ambulance trusthave taken steps to improve thecare given to patients with mental illhealth by developing alternatives toemergency departments.Paramedics link to the admittingdoctor at the psychiatric unit via the tele-medicine desk at theambulance control room. Wherethe patient is already known to theunit, a decision on next steps can betaken based on:
■ immediate presentation.
■ paramedic assessment of socialcircumstances and risk of violence
■ psychiatric history includingmedication, self-harm attemptsand admissions.
■ standard medical assessment to broadly exclude any organic pathology.
Where the patient requires furtherpsychiatric assessment and/ortreatment, arrangements are thenmade for their admission to thepsychiatric unit. If the patient is notwilling to go to the unit voluntarilyand needs further assessment (witha view to sectioning), the crisisintervention team will be deployedto the scene.
Patients who are intoxicated orhave acutely overdosed are taken tothe emergency department.
Patients who are not known to thepsychiatric services are assessed inconjunction with the crisisintervention team.
Positive practice examples 1
Back to ambulance services
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
AssessmentWaiting for assessment in theemergency department is the singlebiggest cause of delays for patientswith mental ill health. There are anumber of actions that you may wantto consider to improve this stage of the patient journey:
■ Appropriate facilities for theassessment of patients with mental illhealth are vital to ensure thatpatients are treated with privacy anddignity and also to ensure the safetyof both patients and staff. Thisshould include an interview roomwith adequate safety features andappropriate staffing to ensurestaff/patient safety.
■ All available information should beused in making initial assessments. Thismay mean it is necessary to contactthe patient’s GP, community psychiatricnurse or other relevant service provider.
■ Have appropriate psychiatricassessment available 24/7. Staffinglevels should reflect assessed hourlyworkload. There should be seniorpsychiatric staff input as soon aspossible – even before medicalassessment in certain cases.
■ Agree protocols for initial assessmentby emergency department staff andfor referral for mental healthassessment. Assessment checklists,risk matrices or a pro-forma fortelephone referrals from theemergency department to mentalhealth teams can be helpful
Back toSTART
CLOSEchecklist
Positive practice pages
Page 1 of 2
Link-upFurther information aboutassessment facilities isavailable atwww.nhsestates.gov.uk/download/publications_guidance/A&E.pdf or the Royal Collegeof Psychiatrists and BAEM’s‘Psychiatric Services toAccident and Emergency’report is available atwww.rcpsych.ac.uk/publications/cr/cr118.htm
Improving the management of patients withmental ill health in emergency care settingsChecklist
Benchmarking tool
Useful resources
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
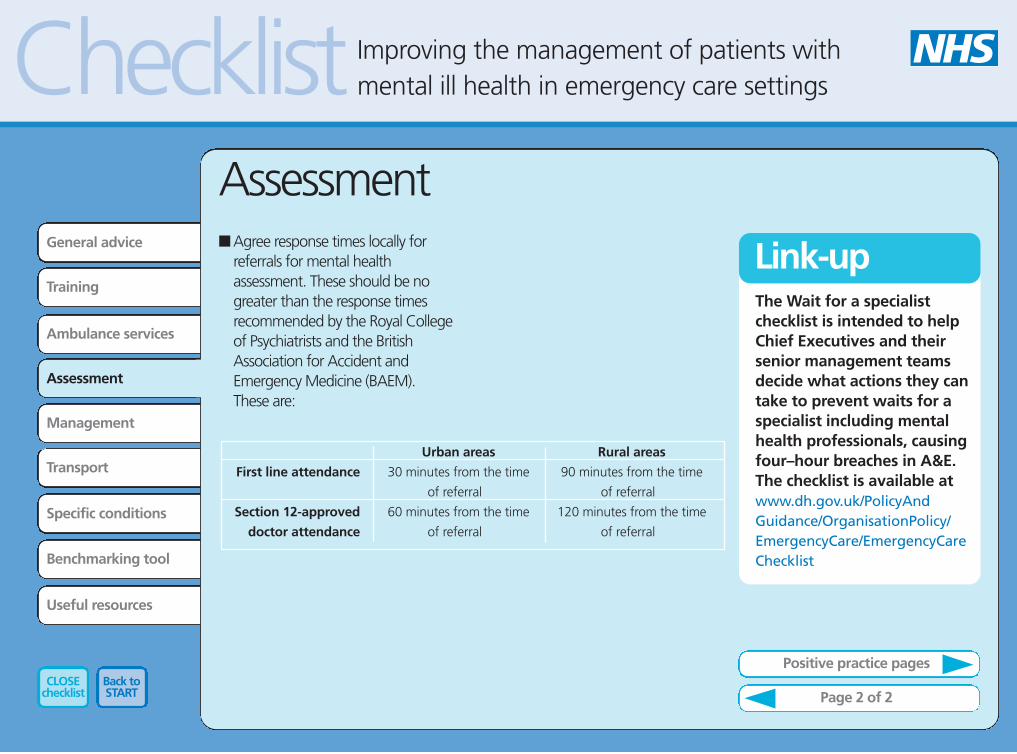
Assessment■ Agree response times locally for
referrals for mental healthassessment. These should be nogreater than the response timesrecommended by the Royal Collegeof Psychiatrists and the BritishAssociation for Accident andEmergency Medicine (BAEM). These are:
Back toSTART
CLOSEchecklist
First line attendance
Section 12-approved
doctor attendance
Urban areas
30 minutes from the time
of referral
60 minutes from the time
of referral
Rural areas
90 minutes from the time
of referral
120 minutes from the time
of referral
Page 2 of 2
Positive practice pages
Link-upThe Wait for a specialistchecklist is intended to helpChief Executives and theirsenior management teamsdecide what actions they cantake to prevent waits for aspecialist including mentalhealth professionals, causingfour–hour breaches in A&E.The checklist is available atwww.dh.gov.uk/PolicyAndGuidance/OrganisationPolicy/EmergencyCare/EmergencyCareChecklist
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Ambulance services
Assessment
Positive practice – rapid access topsychiatric assessmentNewcastle mental health NHS trusthave a crisis resolution and hometreatment service, available 24/7. This means that patients who attendthe emergency department haverapid access to psychiatric assessmentand treatment.
Stephen Niemiec, a nurseconsultant with the crisis assessmentand treatment service, said: "Wehave developed an assessment pro-forma for use in the emergencydepartment. When usedappropriately, it ensures that allpatients experiencing a psychiatriccrisis can be seen quickly. Currently,80 per cent of patients are seenwithin two hours of referral and 98per cent spend no more than four
hours in A&E. Regular liaisonmeetings between ourselves and theA&E team has improvedcommunication and helps resolveclinical pathway issues between thetwo services.”
Back toSTART
CLOSEchecklist
Positive practice 1 2 3 4 5Positive practice examples 1 2 3 4
Link-upFor further [email protected]
Back to assessment
5 6
Improving the management of patients withmental ill health in emergency care settingsChecklist
Ambulance services
Back toSTART
CLOSEchecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Assessment
Positive practice - assessmenttemplates to assist with triageAt St George’s Hospital NHS trust, an assessment template has beendeveloped to assist nurses inundertaking simple, rapidassessments at triage for people with mental ill health problems and/or people who have self-harmed. An initial assessment about thepatient’s level of risk is made,resulting in a risk score ranging from low to very high risk. Referral to senior clinicians within theemergency department or to theliaison psychiatry team, asappropriate, and using agreedprotocols can then be made.
Positive practice examples 1 2 3 4
Link-upFor further informationcontact Nurse consultant,liaison psychiatry team, St George’s [email protected]
Back to assessment
5 6
Improving the management of patients withmental ill health in emergency care settingsChecklist
Ambulance services
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Assessment
Positive practice – improving theappropriateness and timeliness ofreferrals to psychiatryAt the Queen's Medical Centre
NHS trust, an agreed referral pro-forma for use by emergencydepartment staff has beendeveloped as a result of collaborativeworking between the emergencydepartment and the Department for Psychological Medicine,Nottinghamshire Healthcare NHStrust. It helps staff to ask pertinentquestions, gather importantinformation and prioritise. It alsoimproves documentation andinformation gathering.There is also an ongoing
programme of training foremergency department staff onsuicide awareness and risk
assessment. Mo Kontny, East Sector Manager in
the Adult Mental Health Directorateat the Nottinghamshire HealthcareNHS Trust said: "We now haveimproved referral information andprioritisation by the emergencydepartment, which means shorterwaits and an improved experiencefor patients. We feel that theproforma helps to reduce stigma for mental health clients.”
Back toSTART
CLOSEchecklist
Positive practice examples 1 2 3 4
Link-upFor further [email protected]
Back to assessment
5 6
Improving the management of patients withmental ill health in emergency care settingsChecklist
Ambulance services
Transport
General advice
Training
Ambulance services
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Back toSTART
CLOSEchecklist
Assessment
Specific conditions
Link-up
Assessment
Positive practice – nurse referralto the liaison psychiatry teamSouth Tyneside District Hospitalundertook a retrospective audit ofA&E cards of patients presenting withmental ill health problems who didnot require medical treatment. Theresults revealed lengthy waiting timesfor these patients. To address thisissue, triage nurses were giventraining on mental health issues andon how to exclude physical illness orinjury. A mental health triagechecklist was also developed.
Jean Stores, clinical nurse lead inthe A&E mental health liaison teamsaid: "After using the checklist toexclude physical illness, the triagenurse now directly refers the patientto the mental health liaison team. Inagreement with A&E consultants, the
mental health team can now referpatients back to A&E doctors if theyare concerned about the patient'sphysical state. This has resulted infaster treatment for patients. Themean waiting time for patients fromarrival at A&E to being seen by amental health liaison nurse or dutypsychiatrist has fallen from over threehours to around 20 minutes.”
For further informationcontact [email protected]
Positive practice examples 1 2 3 4
Back to assessment
5 6
Improving the management of patients withmental ill health in emergency care settingsChecklist
Back toSTART
CLOSEchecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Assessment
Positive practice – rapid accessto psychiatric assessmentoutside of normal workinghoursDorset Healthcare NHS trust
provides mental health services toabout half a million people living inEast Dorset. Adult communitymental health services are deliveredthrough eleven Community MentalHealth Teams working alongsidespecialist teams for addictions,assertive outreach, earlyintervention, rehabilitation andinpatient services. All CMHNs in adult CMHTs
participate in a service providingcover for patients until 9.00 pm onweekdays and 9.00 am to 5.00 pmover weekends and bank holidays.Three years ago, the service was
extended to provide an assessmentservice to two A&E departments inour area, Royal BournemouthHospital and Poole GeneralHospital. They also added in a nightservice, with a liaison nurse on dutyevery night from 9.00 pm until 9.00am. Their time is ring fenced toundertake assessments in A&E. Prior to referring patients, A&E
staff complete a pro-formadeveloped by the mental healthservice which helps them prioritisepatients and decide who to referon. In 2003, the service undertookabout 1,000 assessments. Mostpatients are discharged from A&Eand referred onto primary care oradult CMHTs for follow-up butabout ten per cent require inpatientadmissions. In these instances the
liaison nurse stays with the patientand provides them with care inA&E. The mental health trust’s ITsystem has been installed in A&E sothat mental health staff can accessICPA information, care plans, riskassessments and other clinicalinformation while they are in thedepartment. There is a training programme for
A&E staff that provides them withan overview of mental illness signsand symptoms, how to conduct abrief screening assessment andinformation about the MentalHealth Act and consent totreatment. This has resulted in
Positive practice examples 1 2 3 4 5 6
Back to assessment
Positive practice continued
Improving the management of patients withmental ill health in emergency care settingsChecklist
Back toSTART
CLOSEchecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Assessment
nurses being more confident whendealing with people with people with mental illness and moreappropriate referrals to the AdultMental Health Service. Most patients presenting to A&E
following an episode of self-harm orwith serious mental illness do solate in the evening or during thenight. The service makes sure thatmental health nurses are availableto undertake assessments at thesetimes, reducing dramatically thenumber of patients who leave A&Ewith out having an appropriateassessment.
Positive practice examples 1 2 3 4 5
Link-upFor further informationcontact the AssertiveOutreach & Crisis ServicesTeam [email protected]
6
Back to assessment
Positive practice continued
Improving the management of patients withmental ill health in emergency care settingsChecklist
Back toSTART
CLOSEchecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Assessment
Positive practice – mental healthassessment tool in A&EAn analysis at Airedale NHS trust
A&E revealed delays in referring tomental health teams and in mentalhealth team members attending toassess patients. To tackle this, a subgroup of the
local emergency care networkengaged lead clinicians andmanagers from both the acute trust and the mental healthprovider. Working in partnership,they identified the bottlenecks andhandoffs. Finally they agreed anaction plan. As a result, triage nurses in A&E
use a mental health assessment toolto help early identification ofpatients’ mental health needs andoperate a system of direct referral
from triage nurse to psychiatricliaison practitioners. This has notonly significantly reduced thenumber of four hour targetbreaches by patients with mentalhealth needs and established asingle point of referral to mentalhealth services through thepsychiatric liaison team. It alsomeans that the mental health needsof patients presenting with physicalconditions can be identified.Another benefit is that A&E staffawareness and knowledge hasincreased. All cases of patients with mental
health needs who spend longerthan four hours in A&E are nowsubject to individual review by bothA&E and mental healthprofessionals. Proposed next steps
include making the mental healthteam active members of the newout of hours primary care team, anda safe area for assessment to be co-located with A&E and the primarycare out of hours centre.
Positive practice examples 1 2 3 4 5 6
Link-up
Back to assessment
For further informationcontact General Manager,Acute Services, AiredaleGeneral Hospital [email protected]
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Transport
Specific conditions
Benchmarking tool
Back toSTART
CLOSEchecklist
Management
Useful resources
ManagementManagement covers manyimportant components. Thischecklist covers two of the mostimportant, admissions and theMental Health Act.
AdmissionsPatients can often be delayedwaiting to be admitted onto a ward.There are a number of actions thathelp address these issues:
■ Area-wide bed managementguidelines and systems to linkacute and mental health resources.
■ Reduction in duplication ofassessment and paperwork by theadmitting team.
■ Make available appropriate short-stay facilities for extendedassessment of patients; forexample patients who are
intoxicated or who havedeliberately harmed themselves.This could be a dedicated unit or a general observation/assessment ward attached to the emergency department.
■ Put in place good links betweenwards and community mentalhealth team to deal proactivelywith potential delays indischarging patients from short-stay units.
Positive practice pages
Admissions
Link-up
Mental Health Act
Faster access – Wait for abed and Wait for a specialistchecklists provide guidanceon deciding actions trustscan take to prevent wait forbeds and wait for specialistscausing 4–hour breaches inA&E. The checklists areavailable at www.dh.gov.uk/PolicyAndGuidance/OrganisationPolicy/EmergencyCare/EmergencyCareChecklists
Improving the management of patients withmental ill health in emergency care settingsChecklist
Ambulance services
Management
Back toSTART
CLOSEchecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Management
Positive practice - Short-termadmission for furtherassessmentManchester Mental Health andSocial Care Trust have a servicecalled "Swift Assessment for theIntensive Resolution ofEmergencies" (SAFIRE). This is anurse-led multidisciplinary servicethat provides further assessment for patients presenting in a crisis at the emergency department and for whom, at the point of initialassessment, there does not appear to be any alternative toinpatient admission.
Within the maximum length of stayof 48 hours, SAFIRE aims to identifyand fully assess the patient’s needsand the most appropriate packageof care. In some instances, this willbe transfer to the in-patient mentalhealth unit. In other cases,alternatives will be appropriate.Damien Longson, consultantpsychiatrist, said: "SAFIRE hassignificantly reduced waits for a bed for psychiatric patientsadmitted from A&E. Furthermore,about 50 per cent of patientstransferred to SAFIRE recoversufficiently within 48 hours to nolonger require in-patient care.”
Positive practice examples 1
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
ManagementMental Health ActThe Mental Health Act must beconcidered when managing patientswith mental ill health in emergencycare settings.
■ The Royal College of Psychiatristsand BAEM recommend thatdoctors able to carry out MentalHealth Act assessments (section12approved) should respond toreferrals within 60 minutes inurban areas, and 120 minutes inrural areas. This is an importantconsideration in deciding whetheran emergency department shouldbe designated as a place of safety.
■ Section 12 doctor rotas should beaccessible to emergency carestaff. These could be availablefrom the hospital switchboard.Access through NHS Direct couldalso be considered.
■ Local inter-agency protocolsshould be agreed for patientsbrought in by the police undersection136. This should coverdesignated places of safety, whostays with the patient, who isresponsible for transport etc.
■ Consider developing alternativeplaces of safety to the emergencydepartment for patients broughtin by the police under section 136of the Mental Health Act, who donot need medical treatment.
Back toSTART
CLOSEchecklist
Admissions Mental Health Act
Positive practice pages
Useful resources
Improving the management of patients withmental ill health in emergency care settingsChecklist
Ambulance services
Management
Back toSTART
CLOSEchecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Management
Positive practice – alternativesto emergency departments forpatients sectioned by the police
In Lambeth, South London,patients who are brought in by thepolice under section136 of theMental Health Act are taken toLambeth Hospital 136 suite. London Ambulance Service will beinvolved in the transfer. If thepatient requires urgent medicalassessment, usually because of self-harm or overdose, they are broughtto the emergency department.
On average, the 136 suite unitundertakes four to five suchassessments per month. Only oneperson in the last six months hasrequired treatment in theemergency department.
The 136 suite provide a securesetting for the assessment to takeplace. It has its own toilet facilitiesand access to refreshments. Onarrival, the person is assessed by a psychiatrist and approved socialworker. After assessment, mostpatients are transferred on a furthersection of the Mental Health Act tothe acute wards based at LambethHospital. A number of patientsagree to informal admission andothers are discharged forcommunity follow-up.
Positive practice examples 1
Link-upFor further informationcontact Eden Ward Manager,Lambeth Hospital [email protected]
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
TransportResponsibilities and response timesfor transport e.g. between theemergency department and themental health unit should beagreed. This is particularly importantwhen patients attend emergencydepartments outside their "home"mental health trust catchment areaand need to be transported back inorder to be admitted to a bed.
Back toSTART
CLOSEchecklist
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Useful resources
Specific conditionsThis section explores two specificcategories of mental health patient;■ Frequent attenders■ Alcohol abusers
We will be developingrecommendations on other specificconditions including deliberate self-harm and care of children andteenagers with mental ill health.
Frequent attendersIt can be helpful for emergencydepartments to keep care plans for patients who regularly attendemergency departments and whoare known to mental healthservices. This could includebackground information about the patients’ condition, details ofappropriate interventions/referralsand the name and contact details ofthe lead mental health clinician forthat patient. If appropriate, care
plans could be shared with otherhealthcare professionals includingambulance staff and those inprimary care.
Back toSTART
CLOSEchecklist
Frequent attenders Alcohol
Useful resources
Positive practice pages
Improving the management of patients withmental ill health in emergency care settingsChecklist
Ambulance services
Specific conditions
Back toSTART
CLOSEchecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Specific conditions
Positive practice – use of careplans to improve the responseto frequent attenders St George’s Hospital NHS trust havecompiled structured care plans thatenable the causes of repeatattendances to be identified andpossible solutions considered. Thesecare plans are kept in theemergency department, and theexistence of a plan is automaticallyprinted on the front of theattendance card when the patientattends the emergency department.
Jim Bolton, a psychiatrist in theliaison psychiatry team said: "Theintroduction of these care plans wasfollowed by a reduction inattendance rates. The availability ofbackground information has led topatients spending less time in A&E.
Staff also felt better equipped tomanage this common clinicalproblem with less frustration and amore satisfactory conclusion.”
Positive practice examples 1
Link-upFor further informationcontact [email protected]
Frequent attenders Alcohol
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Specific conditionsAlcohol abusers■ Introduce simple screening strategy
for harmful and hazardousdrinkers.
■ Assess severity of dependenceusing appropriately trained staff.
■ Provide brief interventions forhazardous drinkers.
■ Develop management protocolsfor specific situations, e.g. alcoholwithdrawal, prevention ofWernicke’s encephalopathy; andappropriate referral for on-goingsupport.
Back toSTART
CLOSEchecklist
Frequent attenders Alcohol
Positive practice pages
Useful resources
Improving the management of patients withmental ill health in emergency care settingsChecklist
Ambulance services
Specific conditions
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Back toSTART
CLOSEchecklist
Positive practice 1
Specific conditions
Positive practice – use ofscreening and briefinterventions with hazardous ordependent drinkers ■ St Mary’s Hospital, London found
that using the PaddingtonAlcohol Test (PAT) in theemergency department to screenfor harmful or hazardous drinkingresulted in a ten-fold increase inreferrals to an alcohol healthworker (AHW) for counselling,generating 27 hours of work perweek. Brief interventions by theAHW resulted in a reduction of43 per cent in alcoholconsumption from 30 to 17 unitsper day. For every two referralsaccepted by the AHW, there wasone less re-attendance within thenext 12 months.
■ St Thomas’ Hospital, Londonestablished a team of psychiatricliaison nurses who made it partof their role to assist in thedetection, assessment andmanagement of alcoholdependent patients. Emphasis isplaced on risk management andon interim care planning in thedepartment. They also advise ondetoxification regimes andappropriate referral. Somepatients are directed to localspecialist alcohol services, whilethose presenting with self-harm,severe withdrawal or confusionalstates are admitted to theemergency departmentobservation ward or a medical bed.
Positive practice examples 1
Link-upFor further informationcontact Consultant in liaisonpsychiatry, St Thomas'[email protected]
Frequent attenders Alcohol
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
This benchmarking tool is based onrecommendations within themental health checklist. It providesguidance covering five keycomponents; Access, Assessment,General management, Wait for abed and Training to enhance themanagement of patients withmental ill health in emergency caresettings.
Objective: to determine if your localexisting services, processes, training& support meet the needs ofpatients with mental health problems, presenting at A&E
Back toSTART
CLOSEchecklist
Select from the list
Access
Assessment
Generalmanagement
Wait for a bed
Training
Next
Benchmarking tool
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
1. Access■ Do you have appropriate A&E
mental health assessment servicesand have they been matched todemand?
■ How do patients and staff accessservices Out-of-Hours?
■ Do ambulance staff and nurses,including those from Walk-inCentres and Minor Injury Unitshave access to assessmentservices directly within the acutetrust & community services oragreed processes to follow?
Back toSTART
CLOSEchecklist
Access
Assessment
Generalmanagement
Wait for a bed
Training
Back NextH
asthe
28d
ayan
a lysisb
eenco
mp
leted?
Benchmarking tool
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
2. Assessment■ Do assessment facilities meet
agreed standards* and ensureprivacy, dignity and safety forpatients and staff?
■ Are there agreed protocols/policies for parallel assessmentsof high volume non complexpatients (e.g. self harm, nontoxic overdose, non complexwounds)?
■ Are there locally agreed responsetimes for mental healthassessment in line with agreedrecommendations*?
■ Have section 12 rotas beenrevised to ensure timeliness ofassessment complies withrecommendations* and are theyaccessible to emergency staff (if
access to specialist reason for delay the DH ‘Waits for Specialist’toolkit may be of use. This can beaccessed at www.dh.gov.uk/PublicationsAndStatistics/Publications/PublicationsPolicyAndGuidance/PublicationsPolicyAndGuidanceArticle/fs/en?CONTENT_ID=4083662&chk=qxJ%2Bn5)?
■ Are there policies / protocols inplace to provide rapid access tomental health services andassessment to help speed up A&Eassessment (e.g. risk assessmentmatrix)?
Back toSTART
CLOSEchecklist
Access
Assessment
Generalmanagement
Wait for a bed
Training
Back NextH
asthe
28d
ayan
a lysisb
eenco
mp
leted?
Benchmarking tool
*Royal College of Phychiatrists & British Association of Emergency Medicine: Psychiatric Services to Emergency, 2003
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
3. General management■ Are there agreed care pathways
for multiple complex attendeesand specific client groups such asthe elderly, confused, deliberateself harm, substance misusepatients?
■ Have the SHA agreed localservices met incentiverequirements and have A&Emental health breaches beeneliminated as a result of thechanges)?
■ Are there identified mental healthemergency care leads and aforum for regular discussion andupdates of local and wholesystem mental health issues?
■ Are there jointly agreed policiesrelating to section 136 and otherdesignated areas of safety?
Back toSTART
CLOSEchecklist
Access
Assessment
Generalmanagement
Wait for a bed
Training
Back NextH
asthe
28d
ayan
a lysisb
eenco
mp
leted?
Benchmarking tool
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
4. Wait for a bed■ Are the area wide mental health
bed occupancy and availabilitylevels shared with mental healthemergency team and acutetrusts?
■ Are there available appropriatefacilities for extendedassessment? These can be usedby patients who are intoxicatedor overdosed for example?
■ Is there proactive managementand involvement from mentalhealth teams to expeditedischarge for short stay patients?
Back toSTART
CLOSEchecklist
Access
Assessment
Generalmanagement
Wait for a bed
Training
Back NextH
asthe
28d
ayan
a lysisb
eenco
mp
leted?
Benchmarking tool
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
5. Training■ Do all first contact practitioners
receive basic training on dealing with patients with mental healthneeds inclusive of bereavementand alcohol training?
■ What, if any specialist training isoffered e.g. substance misuse/risk assessment?
■ Are there joined up traininginitiatives for mental health andemergency care staff or other forums to discuss mutual issues?
Back toSTART
CLOSEchecklist
Access
Assessment
Generalmanagement
Wait for a bed
Training
BackH
asthe
28d
ayan
a lysisb
eenco
mp
leted?
Benchmarking tool
Improving the management of patients withmental ill health in emergency care settingsChecklist
General advice
Training
Ambulance services
Assessment
Management
Transport
Specific conditions
Benchmarking tool
Useful resources
Useful resources■ A series of checklists and toolkits
have been developed. ● 4–hour checklist: reducing
delays for A&E patients● Emergency care networks
checklist● Faster access checklist: wait
for a specialist ● Faster access checklist: wait
for bed ● Faster access toolkit: wait
for bed, further guidance● Patient information toolkit
These are available at:www.dh.gov.uk/PolicyandGuidance/OrganisationPolicy/EmergencyCare/EmergencyCareChecklists/fs/en
■ The Royal College of Psychiatrists /BAEM report “Psychiatric servicesto A&E departments” can bedownloaded at www.rcpsych.ac.uk/publications/cr/cr118.htm
■ Improvements in Emergency Care:Case Studies. ESC Vol 2 August2003 can be found atwww.modern.nhs.uk/scripts/default.asp?site_id=35&id=7902
■ The Emergency ServicesCollaborative has been workingwith every emergency departmentin England to help them makeimprovements to the way theywork for the benefit of patients.Methodology and improvementcase studies can be found atwww.modern.nhs.uk/scripts/default.asp?site_id=35
■ The National Institute for MentalHealth in England works withothers to improve services andsupport for people whoexperience mental distress.Information about current workprogrammes and local deliverystories can be found atwww.nimhe.org.uk
Back toSTART
CLOSEchecklist
Improving the management of patients withmental ill health in emergency care settingsChecklist

![Untitled-1 [] · 2020. 10. 9. · Thi Ill I Il Ill Olli Ill Ill 1 Ill ill Ill Il Ill ill Ill 11 Ill](https://img.pdfslide.net/doc/110x75/60d272307160da1c310a85a5/untitled-1-2020-10-9-thi-ill-i-il-ill-olli-ill-ill-1-ill-ill-ill-il-ill.jpg)



























