-
C
Chemoprevention of squamous cell carcinoma of the headand
neckJohn M. Wrangle and Fadlo R. KhuriPurpose of review
The aim of this article is to summarize progress in
understanding of the biology of squamous cell carcinoma of
the head and neck and of trials to prevent malignant
conversion of oral premalignant lesions and the
development of second primary tumors in those already
treated for squamous cell carcinoma of the head and neck.
Recent findings
The understanding of squamous cell carcinoma of the head
and neck biology is rapidly evolving. Clinical trials for
chemoprevention are involving more diverse regimens,
following disappointing results of retinoid monotherapy.
In-vitro and animal studies form the rationale for the next
generation of studies, employing combination, synergistic
treatments.
Summary
Based on trial data to date, no recommendation for
intervention with a chemopreventive agent can be made. It
is clear, however, that smoking cessation is an effective
intervention for preventing oral premalignant lesions and
second primary tumors. Promising trials are being
conducted and designed currently. The future of this area of
study will involve rational choice of multidrug regimens
based on current understanding of the biology of squamous
cell carcinoma of the head and neck.
Keywords
chemoprevention, head and neck cancer, oral
premalignant lesions, second primary tumors
Curr Opin Oncol 19:180187. 2007 Lippincott Williams &
Wilkins.
Winship Cancer Institute/Emory University, Atlanta, Georgia,
USA
Correspondence to Fadlo R. Khuri, MD, Professor of Hematology,
Oncology,Medicine, Pharmacology and Otolaryngology, Blomeyer Chair
in TranslationalCancer Research, Deputy Director, Clinical and
Translational Research, SectionHead, Hematology and Oncology,
Winship Cancer Institute, Emory UniversitySchool of Medicine, 1365
C Clifton Road, NE, Atlanta, GA 30322, USATel: +1 404 778 4250;
fax: +1 404 778 5520; e-mail: [email protected]
Current Opinion in Oncology 2007, 19:180187opyright Lippincott
Williams & Wilkins. Unautho
180Abbreviations13-cRA 1rized 3-cis retinoic acid
COX cyclooxygenase
EGFR epidermal growth factor receptor
GST glutathione S-transferase
HPV human papilloma virus
OPL oral premalignant lesion
OSCC oral squamous cell carcinoma
RAR retinoic acid receptor
SCCHN squamous cell carcinoma of the head and neck
SPT second primary tumor
TGF transforming growth factor 2007 Lippincott Williams &
Wilkins1040-8746
IntroductionSquamous cell carcinoma of the head and neck
(SCCHN)represents a large, worldwide health burden with
approxi-mately 500 000 cases diagnosed annually [1]. This
oralpremalignant lesion is the subject of study in manyprimary
prevention trials. In the United States, 30 200cases of oral cavity
and pharynx cancer and 7800 deathswere estimated for 2000 [2].
Second primary tumors(SPTs) represent a significant risk to these
patients, withreported rates of development varying from 1.5 to 7%
peryear [3,4]. Because these cancers arise in physicallycompact and
anatomically complex sites, morbidity con-tinues to be high despite
advances in surgery, radiation,and chemotherapy. With expanding
knowledge of theaberrant molecular pathways and stepwise
acquisition ofgenetic mutations in dysplastic and malignant
clones,rational therapeutic options targeting specific mechan-isms
of disease become apparent.
Chemoprevention and field cancerization
Chemoprevention, a concept introduced by Sporn et al.[5], is the
use of natural or synthetic chemicals for thereversal, suppression,
or prevention of conversion of apremalignant lesion to an invasive
form. Chemopreven-tion for head and neck cancer encompasses the
synchro-nous and metachronous development of SPTs within
thecondemned epithelium of the upper aerodigestive tractand lung.
Slaughter et al. [6] introduced the concept offield cancerization
in 1953, suggesting that multipleneoplasias may develop within an
anatomically and histo-logically related site, whether by migration
of a clonallineage to an adjacent site, or by separate clones
obtainingcritical genetic insults as a result of similar
exposuresto tissues throughout a field. Vikram [7] observed
thatSPTs are a major source of morbidity and mortality
inreproduction of this article is prohibited.
mailto:[email protected]
-
C
Chemoprevention of squamous cell cancer Wrangle and Khuri
181adequately treated malignancies of the head and neck.Thus,
successful therapy of SCCHN must include con-sideration of SPT
prevention.
Molecular biology of head and necksquamous cell carcinomaThe
understanding of the molecular pathology ofSCCHN is incomplete,
though rapidly evolving.
P53
A transcription factor important to cell cycle regulation,
theaberrant expression of p53 has been implicated in manycancers.
Its locus on chromosome 17p is deleted in up to60% of SCCHNs [8].
Shin et al. [9] identified a stepwiseincrease in the proportion of
mucosal biopsies with detect-able p53, from normal to hyperplastic
to dysplastic tofrank squamous cell carcinoma. Nees et al. [10]
showedthat p53 is overexpressed in normal epithelia distant fromthe
site of primary tumors. Santos and colleagues [11]found that the
vaccinia-related kinase (VRK1) stabilizesp53 as measured by p53
response proteins.
Cyclooxygenase-2
Cyclooxygenase (COX) 1 is constitutively activated,COX-2 is an
inducible enzyme that is overexpressed inmany premalignant and
malignant tumors including col-orectal adenomas and adenocarcinomas
[12], Barrettsesophagus and esophageal adenocarcinoma
[1315],hepatocellular carcinoma [16], gastric carcinoma [17],as
well as SCCHN [18,19]. Several groups have investi-gated the
mechanistic involvement of COX-2 inSCCHN. Subbaramaiah et al. [20]
showed overexpressionof COX-2 in mouse embryo fibroblasts with p53
mutationswhen compared with wild type p53 cells. Kinugasa et
al.[21] showed decreased invasiveness of human oral squa-mous cell
carcinoma (OSCC) cell lines when treatedwith a selective COX-2
inhibitor, and attributed this effectto downregulation of
metalloproteinase 2 (MMP-2)and CD44. Gallo et al. [22] demonstrated
a correlationbetween COX-2 expression and tumor microvesseldensity,
nodal metastases, and vascular endothelial growthfactor (VEGF) in
SCCHN biopsies. Wang et al. [23]demonstrated decreased tumor
vascularity and sizefollowing celecoxib administration in nude mice
inocu-lated with SCCHN cells.
p16
The tumor suppressor gene p16 encodes an inhibitor
ofcyclin-dependent kinase 4 (CDK4). Loss of p16 functioncontributes
to uncontrolled cell proliferation. The G1regulator retinoblastoma
protein (pRb) is regulated byp16 and cyclin D1, and is lost in many
OSCC lines[24,25]. Holley et al. [26] found an association
betweencyclin D1 polymorphisms and OSCC in tumor biopsies.Zhang et
al. [27] showed that p16 mutations impairp53-imposed G1 arrest.
Estimates of the frequencyopyright Lippincott Williams &
Wilkins. Unauthwith which p16 abnormalities occur vary by study
anddegree of histologic abnormality [2830]. Zhang et al.
[31]poignantly demonstrated a discrepancy between 68SCCHN biopsies
and nine SCCHN cell lines in frequencyof alterations in p16: 10%
and 44% respectively.
Transforming growth factor a and epidermal growth
factor receptor
Epidermal growth factor receptor (EGFR) and one of itsligands,
transforming growth factor (TGF)a, are known toenhance cellular
proliferation in a variety of cancers.Grandis and Tweardy [32,33]
demonstrated increasedlevels of EGFR and TGFa mRNA in SCCHN
tumorbiopsies and the surrounding normal mucosa when com-pared with
normal mucosa. Several groups have reportedeffects of various
interventions on TGFa and EGFRexpression. Beenken et al. [34]
showed that the vitaminA analogue 13-cis retinoic acid (13-cRA)
decreased TGFaexpression in tumor biopsies analyzed before and
afterintervention. Endo et al. [35] transfected an
antisenseTGFageneintosubcutaneousSCCHNxenografts innudemice and
observed decreased TGFa expression andincreased apoptosis within
tumors. He et al. [36] achievedsimilar effects using antisense EGFR
genes. Using theselective retinoic acid receptor (RAR) agonist
LGD1069,Song et al. [37] demonstrated decreased TGFa, EGFR
andproliferation in SCCHN cell lines. Masuda et al. [38] usedthe
green tea constituent, epigallocatechin-3-gallate todecrease VEGF
activity in SCCHN cell lines, attributingthis to inhibition of
nuclear factor-kb and STAT3 activity.
Retinoid biology
In 1925 Wolbach and Howe [39] observed much higherrates of lung
cancer and upper aerodigestive tract malig-nancies in cattle
deprived of dietary vitamin A. Since thattime, much effort has been
invested in understanding thepathophysiological underpinning of
this observation.Administration of isotretinoin upregulates RAR-b
expres-sion [40] and decreases TGFa expression [34]. Whilemany
studies have demonstrated aberrant expression ofRAR-a and b in
SCCHN, the carcinogenic mechanismappears to be distinct from that
of acute promyelocyticleukemia, wherein there is a fusion of
promyelocytic zincfinger (PLZF) and RAR-a in t(15,17) [41].
Human papilloma virus
Several cancers have proven etiologic relationships toviruses,
notably cervical cancer and human papillomavirus (HPV). Based on
the analysis of 36 tumors, Sleboset al. [42] found that 1535% of
SCCHNs contain HPVDNA. Using microarray and PCR they found p16,
p18,CDC7 genes and several transcription factors to be
sig-nificantly overexpressed in HPV-positive compared
withHPV-negative tumors. HPV may be an etiologic agent ina subset
of SCCHN and may have important prognosticimplications [43].orized
reproduction of this article is prohibited.
-
C
182 Head and neckOther genes
Many genes and gene products have been shown to beoverexpressed
in SCCHN including bcl-1 [44], S100A7(psoriasin) [45], eIF4e
[46,47], the p53 homologue AIS[48], opioid growth factor receptor
(OGFr) [49], andglutathione S-transferase (GST)-p [50]. Weed et
al.[51] correlated MUC4 retention with better outcomes.Loss of
E-cadherin and p27 expression is an early step inSCCHN
tumorigenesis [52]. The epigenetic hyper-methylation of SOCS-1 was
associated with SCCHN,presumably via complex mechanisms affecting
STAT3activation [53].
Estimation of risk and surrogate endpointbiomarkersDeveloping
models to accurately predict who willdevelop SCCHN is critical for
the treatment of at riskindividuals and possibly for selection of
candidates forchemoprevention trials. Lee et al. [54] created a
tool formodeling individual risk of SCCHN employing medicalhistory,
histology, and molecular markers. Tobacco useand alcohol are the
most potent risk factors [4], but ahistory of these exposures is
inadequate criteria forselecting high risk individuals. The vast
majority ofindividuals who combine these agents will not
developSCCHN, and genetic variations have been implicated inan
individuals risk [5558].
Many factors predispose tissue toward malignancy, butLippman and
Hong [59] assert that individual molecularmarkers are inadequate to
determine who will progress toSCCHN with sufficient accuracy. One
mechanism bywhich identical exposures to tobacco and alcohol
mayresult in different outcomes is polymorphism in themechanisms of
metabolizing toxic substances. Tobaccoproduct carcinogens undergo
detoxification via cyto-chrome p450 and conjugation, especially by
GST,GSTM1 and GSTT1. Whereas previous studies foundGSTM1 and GSTT1
to be associated with developmentopyright Lippincott Williams &
Wilkins. Unautho
Table 1 Summary of randomized, control chemoprevention trials
in
Study Study agent (dose)
Hong, 1986 [72] 13-cRA (12 mg/kg/day for 3 months)
Stitch, 1988 [76] Vitamin A (200 000 IU/week for 6 months)
Lippman, 1993 [77] 13-cRA (1.5 mg/kg/day for 3 months)
then13-cRA (0.5 mg/kg/day for nine months)or b-carotene (30 mg/day
for nine months)
Sankaranarayanan,1997 [79]
Vitamin A (300 000 IU/week for 12 months)or b-carotene (360
mg/week for 12 months)
Liede, 1998 [80] Vitamin E (50 mg/day indefinitely),
b-carotene(20 mg/day indefinitely), or both
Chiesa, 2005 [83] Fenretinide (200 mg/day for 52 weeks)
13-cRA, 13-cis-retinoic acid.of SCCHN [6062], the CYP system was
not. Individualswho possess the null phenotype of these genes,
thusunderexpressing them, are at significantly higher riskfor
developing SCCHN and SPTs [63,64,65]. Onerecent metaanalysis
confirmed the association of GSTM1and GSTT1, and suggests further
association withGSTP1, and even CYP1A1 [66].
Loss of heterozygosity (LOH) at three locations onchromosome 3p
and at 9p21 was shown to associate withSCCHN by microsatellite
polymorphism deletion map-ping [67,68]. Mao et al. [69] found that
reversal of LOH at3p14, 9p21, and 17p13 may be markers of response
tochemoprevention efforts. Other promising molecularmarkers include
cyclin D1, HIF-a, and MUC4[26,51,70,71].
Clinical trialsClinical trials of chemoprevention in SCCHN can
bedivided into two categories: primary prevention of malig-nant
transformation of oral premalignant lesions (OPLs)(Table 1), and
prevention of SPT in those who haveundergone presumably curative
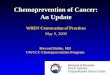
treatment of SCCHN(Table 2). Leukoplakia (Fig. 1) and erythroplakia
areconsidered OPLs. Statistics regarding rates of spon-taneous
regression and malignant conversion are scarce,but in general,
erythroplakia has a much higher likelihoodof progressing to SCCHN
and leukoplakia of spon-taneous regression. Endpoints for OPL
trials are ratesof spontaneous regression and progression to
malignancy.In SPT trials, endpoints include rates of development
ofSPT and overall survival.
Oral premalignant lesion chemopreventiontrialsOPL
chemoprevention trials, while showing earlypromise, have been
hampered by drug toxicity and somedisappointing results.rized
reproduction of this article is prohibited.
oral premalignant lesions
Patients randomized Outcome
44 13-cRA reverses dysplasia and decreasestumor size
54 Vitamin A reverses dysplasia and preventsnew leukoplakias
from forming
70 Low-dose 13-cRA is superior to b-carotenein stabilization or
regression of lesions
Long-term follow up showed no differencein cancer free survival
[78]
160 Either regimen is superior to placebo forinducing regression
of leukoplakia
409 No regimen was superior to placebo atpreventing the
development of leukoplakia
137 Early indication of prevention of malignanttransformations
but discontinued due tolow recruitment
-
C
Chemoprevention of squamous cell cancer Wrangle and Khuri
183
Figure 1 Leukoplakia
This oral premalignant lesion is the subject of study in many
primaryprevention trials. Reproduced with permission from
http://www.dent.ohio-state.edu/oralpath2/nospecivic.htm.Vitamin A,
retinoids, b-carotene, and vitamin E
At similar times, two groups reported positive effects
ofretinoids, or vitamin A and its analogues, on leukoplakia.In a
phase III trial, Hong et al. [72] randomized 44 patientswith
leukoplakia to receive 13-cRA (12 mg/kg for3 months) or placebo. In
the treatment arm, 67% oflesions decreased in size and 54% showed
reversal ofdysplasia versus 10% in both categories among
thosereceiving placebo. Stich et al. [7376] reported
significantrates of leukoplakia remission and suppression
offormation of new lesions among fisherman in Kerala,India, when
administered vitamin A (100 000 IU/day)and b-carotene (180 mg/day)
when compared withplacebo. Because of dose related toxicity
inherent tocertain retinoids, alternate retinoid-receptor,
subtype-specific retinoids and dosing strategies have beenpursued.
Lippman et al. [77] treated patients withleukoplakia with high dose
isotretinoin (1.5 mg/kg/dayopyright Lippincott Williams &
Wilkins. Unauth
Table 2 Summary of randomized, control chemoprevention trials
o
Study Study agent (Dose) P
Hong, 1990 [87] 13-cRA (50100 mg/m2 for12 months)
Bolla, 1994 [89] Etretinate (50 mg/day for one monththen 25
mg/day indefinitely)
Jyothirmayi, 1996 [90] Retinyl palmitate (200 000 IU/day)
EUROSCAN, 2000 [91] Vitamin A (300 000 IU/day for one year,then
150 000 IU/day for one year), orN-acetylcysteine (600 mg/day), or
both
ROG and UTMDACC,2006 [92]
13-cRA (30 mg/day for 3 years)
13-cRA, 13-cis-retinoic acid; ROG, Radiation Oncology Group;
SPT, seconCenter.for 3 months) then randomized them to receive
low-doseisotretinoin (0.5 mg/kg/day for 9 months) or b-carotene(30
mg/day for nine months) and found the low doseisotretinoin arm to
be superior in stabilizing or causingregression of lesions.
Unfortunately, in long-term followup, no significant differences in
cancer-free survival wereseen [78]. Also in Kerala, India,
Sankaranarayanan et al.[79] found both retinyl acetate (300 000
IU/week for12 months) and b-carotene (360 mg/week for 12 months)to
be superior to placebo in inducing spontaneousregression of
leukoplakia. In contrast, Liede et al. [80]saw no statistically
significant differences betweenpatients receiving vitamin E, also
known as a-tocopherol,(50 mg/day), b-carotene, a dimer of retinol
(20 mg/day),both, or placebo. Two groups have concluded
thatfenretinide (200 mg/day), a synthetic retinoid, hasactivity in
leukoplakia and is well tolerated [81,82].While a phase III study
of fentretinide in resectedOPL indicated some activity in
preventing malignantprogression, the study was discontinued due to
lowrecruitment [83].
Other agents in oral premalignant lesions
Armstrong et al. [84] conducted a phase I study ofBowmanBirk
inhibitor, a soybean derived serine pro-tease inhibitor. In a
randomized study of ketorolac, anonselective COX inhibitor, versus
placebo in leuko-plakia, Mulshine et al. [85] found no difference
incomplete or partial response. Rudin et al. [86]
showedtolerability of a mouthwash containing ONYX-015,an attenuated
adenovirus cytotoxic to cells with p53mutations, with reversal of
dysplasia seen in multiplepatients in this small trial.
Second primary tumor chemoprevention trialsEarly OPL trials
suggested a role for chemopreventionof SPT.
First-generation trials
Following promising initial results of retinoids in OPLs,Hong et
al. [87] initiated a trial to see if similar therapyorized
reproduction of this article is prohibited.
f second primary tumors
atients randomized Outcome
103 No effect on the primary tumor, butsignificantly fewer
SPTs
316 No advantage over placebo in preventionof SPTs
93 No advantage over placebo in preventionof SPTs
2592 No differences in overall survival, event-freesurvival, or
rate of SPT formation
1190 Low-dose 13-cRA is ineffective at reducingthe rate of SPT
or death. Smoking cessationis effective for preventing SPTs
[93]
d primary tumor; UTMDACC, University of Texas, MD Anderson
Cancer
http://www.dent.ohio-state.edu/oralpath2/nospecivic.htmhttp://www.dent.ohio-state.edu/oralpath2/nospecivic.htm
-
C
184 Head and neckcould prevent SPT after surgery/radiotherapy
forSCCHN. One hundred and three patients were random-ized to
receive 13-cRA (50100 mg/m2 orally) or placebofor 12 months. During
the course of the trial there wereno differences in the frequency
of local, nodal, ordistant recurrence, but there were significantly
fewerSPTs (4% versus 24% in the placebo arm after 32 monthsof
follow up, P 0.005). Several patients experienceddose-limiting
toxicity. After 54.5 months, the differencebetween the treatment
and placebo group remainedstatistically significant, although
diminished fromprevious levels [88].
Bolla et al. [89] randomly assigned 316 treated cases ofSCCHN
(stage I and II: surgery with or without radio-therapy) to receive
etretinate (50 mg/day for 1 monthfollowed by 25 mg/day orally) or
placebo for 24 months.After 41 months median follow up, no
statisticallysignificant difference was found between the
twogroups.
Jyothirmayi et al. [90] randomized 106 patients whoachieved
complete regression of their SCCHN to retinylpalmitate (200 000
IU/day) or placebo and found nostatistically significance
difference in rates of SPT orlocal recurrence.
Second-generation trials
The European Organization for Research and Treatmentof Cancer
(EUROSCAN) conducted a factorially designedstudy [91] of vitamin A
(300 000 IU/day for 1 yearfollowed by 150 000 IU/day for 1 year),
N-acetylcysteine(600 mg/day), both, or placebo. After median
followup of 49 months for 2592 randomly assigned patients,no
statistically significant difference was observed inoverall
survival, event-free survival, or developmentof SPT.
The Radiotherapy Oncology Group and the Universityof Texas MD
Anderson Cancer Center conducted apivotal study [92] of stage I and
II SCCHN involving1190 patients, randomly assigned to receive
either lowdose 13-cRA (30 mg/day) or placebo for 3 years.
Whilelow-dose isotretinoin was ineffective at reducing the rateof
SPT or death, analysis of the data echoed previousreports: smoking
cessation is the most effective methodof preventing SPT in SCCHN
[93].
Two additional studies with smaller patient populationshave
recently reported no improvement in the rate ofSPT among patients
treated with 13-cRA (0.5 mg/day) orantioxidant vitamins [94].
Bairati et al. [95] reported asignificantly increased rate of SPT
during administrationof vitamin E versus placebo, and a decreased
rate of SPT,though not statistically significant, after
discontinuationof therapy.opyright Lippincott Williams &
Wilkins. UnauthoShin et al. [96] tested the tolerability of a
multidrugregimen in a phase II trial of treated SCCHN
patients.Patients received 13-cRA (50 mg/m2/day orally),
a-toco-pherol (1200 IU/day orally), and IFN-a (3 106
IU/m2subcutaneous injection 3/week). The proportion of5-year
disease free survival in this patient populationwas 79% and the
regimen was well tolerated. Phase IIItesting of this regimen is
currently underway.
DiscussionThe most important consideration in prevention ofSCCHN
has been and will continue to be modificationof risk factors.
Tobacco users must know the dangers theyface, and be assisted in
their efforts to quit. Even for thosealready diagnosed with SCCHN,
smoking cessation willresult in improved outcomes. The future of
SCCHN andSPT chemoprevention lies in the development of
welltolerated, multiagent regimens. Multiple agents havebeen
studied and shown to have activity in SCCHN.Farnesyl transferase
inhibitors decrease the enzymaticactivation of H-ras, which is
mutated in 527% ofSCCHNs, and are currently under phase I/II
investi-gation in SCCHN and lung cancer [9799]. As discussed,COX-2
is overexpressed in SCCHN, and has beenimplicated in several
mechanisms of carcinogenesisincluding apoptosis and angiogenesis.
EGFR inhibitorsare currently under study in SCCHN trials.
Theobservation by Zhang et al. that EGFR and COX-2,inhibited
simultaneously, yield synergistic activityagainst SCCHN xenografts
in nude mice may haveimplications for chemoprevention [100].
ONYX-015,the adenovirus cytotoxic to p53 mutant-containingcells has
completed phase I/II testing, and its role inchemoprevention is
being evaluated [86]. Shin et al. arestudying a three agent
combination of 13-cRA, IFN-a,and a-tocopherol.
ConclusionThe future of SCCHN chemoprevention lies in
combi-nations of agents, the selection of which will be based
uponour evolving understanding of the molecular basis ofSCCHN.
Biomarkers, and risk modeling will be essentialfor assessment of
prognosis and response to treatment.
References and recommended readingPapers of particular interest,
published within the annual period of review, havebeen highlighted
as: of special interest of outstanding interestAdditional
references related to this topic can also be found in the
CurrentWorld Literature section in this issue (p. 267).
1 Kim KB, Khuri FR, Shin DM. Recent advances in the management
ofsquamous cell carcinoma of the head and neck. Expert Rev
Anticancer Ther2001; 1:99110.
2 Greenlee RT, Murray T, Bolden S, Wingo PA. Cancer statistics,
2000. CACancer J Clin 2000; 50:733.
3 Leon X, Ferlito A, Myer CM 3rd, et al. Second primary tumors
in head andneck cancer patients. Acta Otolaryngol 2002;
122:765778.rized reproduction of this article is prohibited.
-
C
Chemoprevention of squamous cell cancer Wrangle and Khuri 1854
Khuri FR, Kim ES, Lee JJ, et al. The impact of smoking status,
diseasestage, and index tumor site on second primary tumor
incidence and tumorrecurrence in the head and neck retinoid
chemoprevention trial. CancerEpidemiol Biomarkers Prev 2001;
10:823829.
5 Sporn MB, Dunlop NM, Newton DL, Smith JM. Prevention of
chemicalcarcinogenesis by vitamin A and its synthetic analogs
(retinoids). FederationProceedings 1976; 35:13321338.
6 Slaughter DP, Southwick HW, Smejkal W. Field cancerization in
oralstratified squamous epithelium; clinical implications of
multicentric origin.Cancer 1953; 6:963968.
7 Vikram B. Changing patterns of failure in advanced head and
neck cancer.Arch Otolaryngol 1984; 110:564565.
8 Maestro R, Gasparotto D, Vukosavljevic T, et al. Three
discrete regions ofdeletion at 3p in head and neck cancers. Cancer
Res 1993; 53:57755779.
9 Shin DM, Kim J, Ro JY, et al. Activation of p53 gene
expression in pre-malignant lesions during head and neck
tumorigenesis. Cancer Res 1994;54:321326.
10 Nees M, Homann N, Discher H, et al. Expression of mutated p53
occurs intumor-distant epithelia of head and neck cancer patients:
a possible mole-cular basis for the development of multiple tumors.
Cancer Res 1993;53:41894196.
11 Santos CR, Rodriguez-Pinilla M, Vega FM, et al. VRK1
signaling pathway inthe context of the proliferation phenotype in
head and neck squamous cellcarcinoma. Mol Cancer Res 2006;
4:177185.
12 Eberhart CE, Coffey RJ, Radhika A, et al. Up-regulation of
cyclooxygenase2 gene expression in human colorectal adenomas and
adenocarcinomas.Gastroenterology 1994; 107:11831188.
13 Yu H-P, Xu S-Q, Liu L, et al. Cyclooxygenase-2 expression in
squamousdysplasia and squamous cell carcinoma of the esophagus.
Cancer Lett2003; 198:193201.
14 Wilson KT, Fu S, Ramanujam KS, Meltzer SJ. Increased
expression ofinducible nitric oxide synthase and cyclooxygenase-2
in Barretts esophagusand associated adenocarcinomas. Cancer Res
1998; 58:29292934.
15 Zimmermann KC, Sarbia M, Weber AA, et al. Cyclooxygenase-2
expressionin human esophageal carcinoma. Cancer Res 1999;
59:198204.
16 Shiota G, Okubo M, Noumi T, et al. Cyclooxygenase-2
expression inhepatocellular carcinoma. Hepatogastroenterology 1999;
46:407412.
17 Ristimaki A, Honkanen N, Jankala H, et al. Expression of
cyclooxygenase-2 inhuman gastric carcinoma. Cancer Res 1997;
57:12761280.
18 Chan G, Boyle JO, Yang EK, et al. Cyclooxygenase-2 expression
is up-regulated in squamous cell carcinoma of the head and neck.
Cancer Res1999; 59:991994.
19 Lin DT, Subbaramaiah K, Shah JP, et al. Cyclooxygenase-2: a
novel moleculartarget for the prevention and treatment of head and
neck cancer. Head Neck2002; 24:792799.
20 Subbaramaiah K, Altorki N, Chung WJ, et al. Inhibition of
cyclooxygenase-2gene expression by p53. J Biol Chem 1999;
274:1091110915.
21 Kinugasa Y, Hatori M, Ito H, et al. Inhibition of
cyclooxygenase-2 suppressesinvasiveness of oral squamous cell
carcinoma cell lines via down-regulationof matrix
metalloproteinase-2 and CD44. Clin Exp Metastasis
2004;21:737745.
22 Gallo O, Franchi A, Magnelli L, et al. Cyclooxygenase-2
pathway correlateswith VEGF expression in head and neck cancer.
Implications for tumorangiogenesis and metastasis. Neoplasia 2001;
3:5361.
23 Wang Z, Fuentes CF, Shapshay SM. Antiangiogenic and
chemopreventiveactivities of celecoxib in oral carcinoma cell.
Laryngoscope 2002; 112:839843.
24 Sartor M, Steingrimsdottir H, Elamin F, et al. Role of
p16/MTS1, cyclin D1and RB in primary oral cancer and oral cancer
cell lines. Br J Cancer 1999;80 (12):7986.
25 Soni S, Kaur J, Kumar A, et al. Alterations of rb pathway
components arefrequent events in patients with oral epithelial
dysplasia and predict clinicaloutcome in patients with squamous
cell carcinoma. Oncology 2005; 68(46):314325.
26 Holley SL, Matthias C, Jahnke V, et al. Association of cyclin
D1 polymorphismwith increased susceptibility to oral squamous cell
carcinoma. Oral Oncology2005; 41:156160.
27 Zhang Y, Xiong Y, Yarbrough WG. ARF promotes MDM2 degradation
andstabilizes p53: ARF-INK4a locus deletion impairs both the Rb and
p53 tumorsuppression pathways. Cell 1998; 92:725734.
28 Cairns P, Mao L, Merlo A, et al. Rates of p16 (MTS1)
mutations in primarytumors with 9p loss. Science 1994;
265:415417.opyright Lippincott Williams & Wilkins. Unauth29
Papadimitrakopoulou VA, Izzo J, Mao L, et al. Cyclin D1 and p16
alterations inadvanced premalignant lesions of the upper
aerodigestive tract: role inresponse to chemoprevention and cancer
development. Clin Cancer Res2001; 7:31273134.
30 van der Riet P, Nawroz H, Hruban RH, et al. Frequent loss of
chromosome9p21-22 early in head and neck cancer progression. Cancer
Res 1994;54:11561158.
31 Zhang SY, Klein-Szanto AJ, Sauter ER, et al. Higher frequency
of alterationsin the p16/CDKN2 gene in squamous cell carcinoma cell
lines than in primarytumors of the head and neck. Cancer Res 1994;
54:50505053.
32 Grandis JR, Tweardy DJ. TGF-alpha and EGFR in head and neck
cancer.J Cell Biochem Suppl 1993; 17F:188191.
33 Grandis JR, Tweardy DJ. Elevated levels of transforming
growth factor alphaand epidermal growth factor receptor messenger
RNA are early markers ofcarcinogenesis in head and neck cancer.
Cancer Res 1993; 53:35793584.
34 Beenken SW, Sellers MT, Huang P, et al. Transforming growth
factor alpha(TGF-alpha) expression in dysplastic oral leukoplakia:
modulation by 13-cisretinoic acid. Head & Neck 1999;
21:566573.
35 Endo S, Zeng Q, Burke NA, et al. TGF-alpha antisense gene
therapy inhibitshead and neck squamous cell carcinoma growth in
vivo. Gene Ther 2000;7:19061914.
36 He Y, Zeng Q, Drenning SD, et al. Inhibition of human
squamous cellcarcinoma growth in vivo by epidermal growth factor
receptor antisenseRNA transcribed from the U6 promoter. J Natl
Cancer Inst 1998; 90:10801087.
37 Song JI, Lango MN, Hwang JD, et al. Abrogation of
transforming growthfactor-alpha/epidermal growth factor receptor
autocrine signaling by anRXR-selective retinoid (LGD1069,
Targretin) in head and neck cancer celllines. Cancer Research 2001;
61:59195925.
38 Masuda M, Suzui M, Lim JTE, et al. Epigallocatechin-3-gallate
decreasesVEGF production in head and neck and breast carcinoma
cells by inhibitingEGFR-related pathways of signal transduction. J
Exp Ther Oncol 2002;2:350359.
39 Wolbach SB, Howe PR. Nutrition Classics. The Journal of
ExperimentalMedicine 42: 753-77, 1925. Tissue changes following
deprivation of fat-soluble A vitamin. S. Burt Wolbach and Percy R.
Howe. Nutr Rev 1978;36:1619.
40 Lotan R, Xu XC, Lippman SM, et al. Suppression of retinoic
acid receptor-beta in premalignant oral lesions and its
up-regulation by isotretinoin. N Engl JMed 1995; 332:14051410.
41 Sun SY, Lotan R. Retinoids and their receptors in cancer
development andchemoprevention. Crit Rev Oncol Hematol 2002;
41:4155.
42 Slebos RJ, Yi Y, Ely K, et al. Gene expression differences
associated withhuman papillomavirus status in head and neck
squamous cell carcinoma. ClinCancer Res 2006; 12 (3 Pt
1):701709.
43 Fakhry C, Gillison ML. Clinical implications of human
papillomavirus in headand neck cancers. J Clin Oncol 2006;
24:26062611.
44 Berenson JR, Yang J, Mickel RA. Frequent amplification of the
bcl-1 locusin head and neck squamous cell carcinomas. Oncogene
1989; 4:11111116.
45 Fukuzawa H, Kiyoshima T, Kobayashi I, et al. Transcription
promoter activity ofthe human S100A7 gene in oral squamous cell
carcinoma cell lines. BiochimBiophys Acta 2006; 1759
(34):171176.
46 Haydon MS, Googe JD, Sorrells DS, et al. Progression of eIF4e
geneamplification and overexpression in benign and malignant tumors
of thehead and neck. Cancer 2000; 88:28032810.
47 Sorrells DL, Ghali GE, Meschonat C, et al. Competitive PCR to
detect eIF4Egene amplification in head and neck cancer. Head Neck
1999; 21:6065.
48 Hibi K, Trink B, Patturajan M, et al. AIS is an oncogene
amplified in squamouscell carcinoma. Proc Natl Acad Sci U S A 2000;
97:54625467.
49 McLaughlin PJ, Zagon IS. Progression of squamous cell
carcinoma of thehead and neck is associated with down-regulation of
the opioid growth factorreceptor. Int J Oncol 2006;
28:15771583.
50 Wang X, Pavelic ZP, Li Y, et al. Overexpression and
amplification ofglutathione S-transferase pi gene in head and neck
squamous cell carcino-mas. Clin Cancer Res 1997; 3:111114.
51 Weed DT, Gomez-Fernandez C, Yasin M, et al. MUC4 and ErbB2
expressionin squamous cell carcinoma of the upper aerodigestive
tract: correlation withclinical outcomes. Laryngoscope 2004; 114 (8
Pt 2 Suppl 101):132.
52 Massarelli E, Brown E, Tran NK, et al. Loss of E-cadherin and
p27 expressionis associated with head and neck squamous
tumorigenesis. Cancer 2005;103:952959.orized reproduction of this
article is prohibited.
-
C
186 Head and neck53
Lee TL, Yeh J, Van Waes C, Chen Z. Epigenetic modification of
SOCS-1differentially regulates STAT3 activation in response to
interleukin-6 receptorand epidermal growth factor receptor
signaling through JAK and/or MEK inhead and neck squamous cell
carcinomas. Mol Cancer Ther 2006;5:819.
Epigenetic modification may become an important therapeutic
target in oncologyin general, and SCCHN in particular.
54 Lee JJ, Hong WK, Hittelman WN, et al. Predicting cancer
development in oralleukoplakia: ten years of translational
research. Clin Cancer Res 2000;6:17021710.
55 Copper MP, Jovanovic A, Nauta JJ, et al. Role of genetic
factors in the etiologyof squamous cell carcinoma of the head and
neck. Arch Otolaryngol HeadNeck Surg 1995; 121:157160.
56 Foulkes WD, Brunet JS, Kowalski LP, et al. Family history of
cancer is arisk factor for squamous cell carcinoma of the head and
neck in Brazil:a casecontrol study. Int J Cancer 1995;
63:769773.
57 Foulkes WD, Brunet JS, Sieh W, et al. Familial risks of
squamous cellcarcinoma of the head and neck: retrospective
case-control study. BMJ1996; 313:716721.
58 Goldgar DE, Easton DF, Cannon-Albright LA, Skolnick MH.
Systematicpopulation-based assessment of cancer risk in
first-degree relatives ofcancer probands. J Natl Cancer Inst 1994;
86:16001608.
59 Lippman SM, Hong WK. Molecular markers of the risk of oral
cancer. N Engl JMed 2001; 344:13231326.
60 Sturgis EM, Castillo EJ, Li L, et al. XPD/ERCC2 EXON 8
Polymorphisms:rarity and lack of significance in risk of squamous
cell carcinoma of the headand neck. Oral Oncol 2002; 38:475477.
61 Sturgis EM, Castillo EJ, Li L, et al. Polymorphisms of DNA
repair geneXRCC1 in squamous cell carcinoma of the head and neck.
Carcinogenesis1999; 20:21252129.
62 Sturgis EM, Zheng R, Li L, et al. XPD/ERCC2 polymorphisms and
risk ofhead and neck cancer: a case-control analysis.
Carcinogenesis 2000;21:22192223.
63
Minard CG, Spitz MR, Wu X, et al. Evaluation of glutathione
S-transferasepolymorphisms and mutagen sensitivity as risk factors
for the development ofsecond primary tumors in patients previously
diagnosed with early-stagehead and neck cancer. Cancer 2006;
106:26362644.
As risk modeling becomes more important to selecting candidates
for chemo-preventive therapy, data such as these become
increasingly relevant.
64 Sturgis EM, Wei Q. Genetic susceptibility: molecular
epidemiology of headand neck cancer. Curr Opin Oncol 2002;
14:310317.
65 Jahnke V, Matthias C, Fryer A, Strange R. Glutathione
S-transferaseand cytochrome-P-450 polymorphism as risk factors for
squamous cellcarcinoma of the larynx. American Journal of Surgery
1996; 172:671673.
66 Hashibe M, Brennan P, Strange RC, et al. Meta- and pooled
analyses ofGSTM1, GSTT1, GSTP1, and CYP1A1 genotypes and risk of
head and neckcancer. Cancer Epidemiol Biomarkers Prev 2003;
12:15091517.
67 Wu CL, Sloan P, Read AP, et al. Deletion mapping on the short
arm ofchromosome 3 in squamous cell carcinoma of the oral cavity.
Cancer Res1994; 54:64846488.
68 Rosin MP, Lam WL, Poh C, et al. 3p14 and 9p21 loss is a
simple tool forpredicting second oral malignancy at previously
treated oral cancer sites.Cancer Res 2002; 62:64476450.
69 Mao L, El-Naggar AK, Papadimitrakopoulou V, et al. Phenotype
and genotypeof advanced premalignant head and neck lesions after
chemopreventivetherapy. J Natl Cancer Inst 1998; 90:15451551.
70 Gross J, Fuchs J, Machulik A, et al. Apoptosis, necrosis and
hypoxia induciblefactor-1 in human head and neck squamous cell
carcinoma cultures. Int JOncol 2005; 27:807814.
71 Miyamoto R, Uzawa N, Nagaoka S, et al. Prognostic
significance of cyclin D1amplification and overexpression in oral
squamous cell carcinomas. OralOncol 2003; 39:610618.
72 Hong WK, Endicott J, Itri LM, et al. 13-cis-retinoic acid in
the treatment of oralleukoplakia. N Engl J Med 1986;
315:15011505.
73 Stich HF, Mathew B, Sankaranarayanan R, Nair MK. Remission of
oralprecancerous lesions of tobacco/areca nut chewers following
administrationof beta-carotene or vitamin A, and maintenance of the
protective effect.Cancer Detect Prev 1991; 15:9398.
74 Stich HF, Mathew B, Sankaranarayanan R, Nair MK. Remission of
precan-cerous lesions in the oral cavity of tobacco chewers and
maintenanceof the protective effect of beta-carotene or vitamin A.
Am J Clin Nutr1991; 53 (1 Suppl):298S304S.opyright Lippincott
Williams & Wilkins. Unautho75 Stich HF, Tsang SS. Promoting
activity of betel quid ingredients and theirinhibition by retinol.
Cancer Lett 1989; 45:7177.
76 Stich HF, Rosin MP, Hornby AP, et al. Remission of oral
leukoplakias andmicronuclei in tobacco/betel quid chewers treated
with beta-caroteneand with beta-carotene plus vitamin A. Int J
Cancer 1988; 42:195199.
77 Lippman SM, Batsakis JG, Toth BB, et al. Comparison of
low-dose iso-tretinoin with beta carotene to prevent oral
carcinogenesis. N Engl J Med1993; 328:1520.
78 Papadimitrakopoulou VA, Hong WK, Lee JS, et al. Low-dose
isotretinoinversus beta-carotene to prevent oral carcinogenesis:
long-term follow-up.J Natl Cancer Inst 1997; 89:257258.
79 Sankaranarayanan R, Mathew B, Varghese C, et al.
Chemoprevention of oralleukoplakia with vitamin A and beta
carotene: an assessment. Oral Oncol1997; 33:231236.
80 Liede K, Hietanen J, Saxen L, et al. Long-term
supplementation with alpha-tocopherol and beta-carotene and
prevalence of oral mucosal lesions insmokers. Oral Dis 1998;
4:7883.
81 Chiesa F, Tradati N, Marazza M, et al. Prevention of local
relapses andnew localisations of oral leukoplakias with the
synthetic retinoid fenretinide(4-HPR). Preliminary results. Eur J
Cancer B Oral Oncol 1992; 28B:97102.
82
Lippman SM, Lee JJ, Martin JW, et al. Fenretinide activity in
retinoid-resistantoral leukoplakia. Clin Cancer Res 2006;
12:31093114.
Fenretinide may have activity in OPL despite retinoid
resistance.
83 Chiesa F, Tradati N, Grigolato R, et al. Randomized trial of
fenretinide(4-HPR) to prevent recurrences, new localizations and
carcinomas inpatients operated on for oral leukoplakia: long-term
results. Int J Cancer2005; 115:625629.
84 Armstrong WB, Wan XS, Kennedy AR, et al. Development of the
Bowman-Birk inhibitor for oral cancer chemoprevention and analysis
of Neu immu-nohistochemical staining intensity with Bowman-Birk
inhibitor concentratetreatment. Laryngoscope 2003;
113:16871702.
85 Mulshine JL, Atkinson JC, Greer RO, et al. Randomized,
double-blind,placebo-controlled phase IIb trial of the
cyclooxygenase inhibitor ketorolacas an oral rinse in oropharyngeal
leukoplakia. Clin Cancer Res 2004;10:15651573.
86 Rudin CM, Cohen EE, Papadimitrakopoulou VA, et al. An
attenuated ade-novirus, ONYX-015, as mouthwash therapy for
premalignant oral dysplasia.J Clin Oncol 2003; 21:45464552.
87 Hong WK, Lippman SM, Itri LM, et al. Prevention of second
primary tumorswith isotretinoin in squamous-cell carcinoma of the
head and neck. N Engl JMed 1990; 323:795801.
88 Benner SE, Pajak TF, Lippman SM, et al. Prevention of second
primarytumors with isotretinoin in patients with squamous cell
carcinoma of the headand neck: long-term follow-up. J Natl Cancer
Inst 1994; 86:140141.
89 Bolla M, Lefur R, Ton Van J, et al. Prevention of second
primary tumours withetretinate in squamous cell carcinoma of the
oral cavity and oropharynx.Results of a multicentric double-blind
randomised study. Eur J Cancer 1994;30A:767772.
90 Jyothirmayi R, Ramadas K, Varghese C, et al. Efficacy of
vitamin A in theprevention of loco-regional recurrence and second
primaries in head andneck cancer. Eur J Cancer B Oral Oncol 1996;
32B:373376.
91 van Zandwijk N, Dalesio O, Pastorino U, et al. EUROSCAN, a
randomizedtrial of vitamin A and N-acetylcysteine in patients with
head and neck canceror lung cancer. For the EUropean Organization
for Research and Treatmentof Cancer Head and Neck and Lung Cancer
Cooperative Groups. J NatlCancer Inst 2000; 92:977986.
92
Khuri FR, Lee JJ, Lippman SM, et al. Randomized phase III trial
of low-doseisotretinoin for prevention of second primary tumors in
stage I and II head andneck cancer patients. J Natl Cancer Inst
2006; 98:441450.
Our phase III study of 1384 patients failed to show that at a
low, tolerable dose ofisotretinoin second primary tumor development
was inhibited. There was atransient protective effect against
recurrence while patients were on the drug,but this was not
significant. The most important finding was that continuedsmoking
was associated with a higher likelihood of death from second
primarytumors, primary tumor recurrence, or other smoking-related
disease.
93 Khuri FR, Kim ES, Lee JJ, et al. The impact of smoking
status, disease stage,and index tumor site on second primary tumor
incidence and tumor recur-rence in the head and neck retinoid
chemoprevention trial. Cancer EpidemiolBiomarkers Prev 2001;
10:823829.
94 Perry CF, Stevens M, Rabie I, et al. Chemoprevention of head
and neckcancer with retinoids: a negative result. Arch Otolaryngol
Head Neck Surg2005; 131:198203.rized reproduction of this article
is prohibited.
-
C
Chemoprevention of squamous cell cancer Wrangle and Khuri 18795
Bairati I, Meyer F, Gelinas M, et al. A randomized trial of
antioxidant vitamins toprevent second primary cancers in head and
neck cancer patients. J NatlCancer Inst 2005; 97:481488.
96 Shin DM, Khuri FR, Murphy B, et al. Combined interferon-alfa,
13-cis-retinoicacid, and alpha-tocopherol in locally advanced head
and neck squamouscell carcinoma: novel bioadjuvant phase II trial.
J Clin Oncol 2001;19:30103017.
97 Anderson JA, Irish JC, McLachlin CM, Ngan BY. H-ras oncogene
mutationand human papillomavirus infection in oral carcinomas. Arch
OtolaryngolHead Neck Surg 1994; 120:755760.opyright Lippincott
Williams & Wilkins. Unauth98 Hahn SM, Bernhard EJ, Regine W, et
al. A phase I trial of the farnesyl-transferase inhibitor L-778,123
and radiotherapy for locally advancedlung and head and neck cancer.
Clin Cancer Res 2002; 8:10651072.
99 Oku N, Shimada K, Itoh H. Ha-ras oncogene product in
humanoral squamous cell carcinoma. Kobe J Med Sci 1989; 35
(56):277286.
100 Zhang X, Chen ZG, Choe MS, et al. Tumor growth inhibition by
simulta-neously blocking epidermal growth factor receptor and
cyclooxygenase-2 ina xenograft model. Clin Cancer Res 2005;
11:62616269.orized reproduction of this article is prohibited.
Chemoprevention of squamous cell carcinoma of the head
andneckIntroductionChemoprevention and field cancerization
Molecular biology of head and neck squamous cell
carcinomaP53Cyclooxygenase-2p16Transforming growth factor and
epidermal growth factor receptorRetinoid biologyHuman papilloma
virusOther genes
Estimation of risk and surrogate endpoint biomarkersClinical
trialsOral premalignant lesion chemoprevention trialsVitamin A,
retinoids, -carotene, and vitamin EOther agents in oral
premalignant lesions
Second primary tumor chemoprevention trialsFirst-generation
trialsSecond-generation trials
DiscussionConclusionReferences and recommended reading