Embed Size (px)
Citation preview

8/8/2019 Chemotherapy in Head and Neck Cancers Summary of Recommendations and a Critical Review of Clinical Practice…
http://slidepdf.com/reader/full/chemotherapy-in-head-and-neck-cancers-summary-of-recommendations-and-a-critical 1/7
Chemotherapy in Head and Neck Cancers: Summary of
Recommendations and a Critical Review of Clinical Practice
Guidelines
Weng Ng, Susannah Jacob, Geoff Delaney and Michael Barton
Affiliation: Collaboration for Cancer Outcomes Research and Evaluation (CCORE), Liverpool Hospital and Faculty of Medicine, University of New South Wales,
Sydney, Australia
A B S T R A C T
The management of head and neck cancer is complex and requires a multidisciplinary approach to optimize the balance between the goals
of organ preservation and long-term cure. The role of chemotherapy in head and neck cancers has recently expanded as a result of increasingevidence in the induction and postoperative setting. Several evidence-based clinical practice guidelines have been published by reputablecancer organizations to facilitate the translation of evidence from clinical trials to patient care. There is a high concordance in therecommendations for chemotherapy between the various clinical practice guidelines in head and neck cancers. The quality of evidence for
recommendations for induction, concurrent and postoperative chemotherapy is high, but remains poor in the palliative setting. The mainlimitations of current guideline recommendations are the lack of guidance in addressing the impact of performance status and comorbiditiesin their recommendations for chemotherapy. Population-based studies suggest that the compliance with guideline recommendations for
chemotherapy may be lagging behind newer evidence, and that opportunities for improvement in care exist.
Keywords: Chemotherapy, clinical practice guidelines, review, head and neck cancer, compliance
Correspondence: Weng Ng, Collaboration for Cancer Outcomes Research and Evaluation, Liverpool Hospital, Locked Bag 7103, Liverpool,
NSW, 1871, Australia. Tel: (61)-2-9828-6700; Fax: (61)-2-9828-6670; e-mail: [email protected]
INTRODUCTION
Primary head and neck cancers account for 3.8% of allcancers in Australia [1]. The anatomical subsites in thisheterogeneous population comprise lip (29%), oral cavity (28%), nasopharynx (3%), oropharynx (9%), hypopharynx
(4%), larynx (16%), paranasal sinus and nasal cavity (4%), andsalivary gland (7%) [1]. The management of head and neck cancer is complex and requires a multidisciplinary approachinvolving surgery, radiotherapy, and chemotherapy to opti-mize the balance between the goals of organ preservation andlong-term cure.
Chemotherapy plays an integral role in the cure andpalliation of head and neck cancer patients. Over the past 20 years, the indications for chemotherapy in head and neck cancers have expanded, particularly in the induction andpostoperative setting [2–6]. Patterns of care studies in headand neck cancers have reported that the utilization rates of chemotherapy vary from 12% to 17% [7, 8]. Clinical practiceguidelines have been published to facilitate the translation of evidence from clinical trials to patient care in an effort topromote the highest quality of cancer care. This review willsummarize current recommendations for chemotherapy, the
quality of supportive evidence, and discuss controversies andcompliance with clinical practice guidelines in head and neck
cancers.
EVIDENCE-BASED GUIDELINES
Clinical practice guidelines in head and neck cancers havebeen published by several leading professional cancer organi-zations internationally. In the United States (US), the NationalComprehensive Cancer Network (NCCN) [9] is an alliance of 21 cancer centers whose guidelines are based on a review of evidence in conjunction with expert judgment. This differsfrom the National Cancer Institute (NCI) [10–16], which is part of the National Institutes of Health and the US Department of Health and Human Services, whose recommendations arebased solely on evidence from the strength of the study designand the endpoints measured. The two provincial cancer
agencies in Canada that publish guidelines are the BritishColumbia Cancer Agency (BCCA) [17–24] and Cancer CareOntario (CCO) [25–28]. The guidelines published by theCanadian agencies are based on the best evidence available and
consensus from a multidisciplinary panel. Lastly, the ScottishIntercollegiate Guidelines Network (SIGN) [29] performssystematic review of the scientific literature and publishesguidelines for the National Health Service in Scotland.
SUMMARY OF GUIDELINERECOMMENDATIONS FOR CHEMOTHERAPY
We examined the clinical practice guidelines available on the
September 1, 2009. In general, definitive local treatment with
EUROPEAN JOURNAL OF CLINICAL & MEDICAL ONCOLOGY REVIEW ARTICLE
EJCMO 2010; 2:(1). FEBRUARY 2010 65 www.slm-oncology.com

8/8/2019 Chemotherapy in Head and Neck Cancers Summary of Recommendations and a Critical Review of Clinical Practice…
http://slidepdf.com/reader/full/chemotherapy-in-head-and-neck-cancers-summary-of-recommendations-and-a-critical 2/7
surgery and/or radiotherapy remains the primary management
of early stage (stage 1 and 2) head and neck cancers. There areseveral management options in locally advanced head and neck
cancers (stages 3 and 4) to which the addition of chemotherapy (induction, concurrent, and postoperative) has been shown tobe of benefit (Table 1) [4, 30, 31].
The Meta-Analyses of Chemotherapy in Head and Neck
Cancer (MACH-NC) group demonstrated that concurrent chemoradiation in locally advanced head and neck cancers
(excluding nasopharyngeal carcinoma) improves survival withan absolute benefit of 8% at 5 years over local treatment alone
[32, 33]. The addition of chemotherapy to radiotherapy inlocally advanced nasopharyngeal carcinomas has also beenshown to improve the 5-year survival by 6% over radiotherapy alone by the Meta-Analysis of Chemotherapy in NasopharynxCarcinoma (MAC-NPC) Collaborative Group [34, 35]. In thepostoperative setting, the addition of chemotherapy to radio-therapy also significantly improved locoregional control andoverall survival in locally advanced head and neck cancers at ahigh risk of recurrence when compared with radiotherapy alone
[2–4]. Recently, two large randomized controlled trials havedemonstrated that the addition of docetaxel to cisplatin and 5-
fluorouracil as induction chemotherapy significantly improvedoverall survival in patients with locally advanced head and neck cancers who were unsuitable for surgical management [5, 6].Several ongoing trials are aimed at addressing the optimalapproach to using chemotherapy (sequential vs concurrent).
In the palliative setting, chemotherapy for patients withmetastatic or recurrent head and neck cancers has been shownto induce response rates of 15–44% (Table 2) [9, 36, 37].
Based on the guideline recommendations, chemotherapy
was indicated in the treatment of head and neck cancers inthe following clinical situations:
N Concurrent chemoradiation for locally advanced head andneck cancer
N Postoperative chemoradiation in locally advanced head andneck cancer with high- risk features (extracapsular nodalextension or close/positive margins)
N Induction chemotherapy prior to surgery for locally advanced head and neck cancer
N
Palliative chemotherapy for recurrent or metastatic headand neck cancer.
Table 3 summarizes the specific clinical scenarios andguideline recommendations for chemotherapy for each of theanatomical subsites (lip, oral cavity, nasopharynx, orophar-
ynx, hypopharynx, larynx, paranasal and nasal cavity, salivary gland) of head and neck cancers. The recommendations forchemotherapy were highly consistent between guidelines.
Table 1. Summary of Pivotal Studies for Chemotherapy Indications in Locally Advanced Head and Neck Cancers
Indication Treatment armsLocoregional recurrence
HR (95% CI)DFS or PFS HR
(95% CI)Overall survival HR
(95% CI) Reference
Concurrent chemoradiation
CRT vs RT NR NR 0.81 (0.78–0.86) [33]
P,0.0001 MACH-NC
Postoperativechemoradiationa
Cisplatin+RT vs RT 0.61 (0.41–0.91) 0.78 (0.61–0.99) 0.84 (0.65–1.09) [3]
P50.01 P50.04 P50.19 RTOG 9501
Cisplatin+RT vs RT 18% vs 31% 0.75 (0.56–0.99) 0.70 (0.52–0.95) [2]
P50.007 P50.04 P50.02 EORTC 22931
Inductionchemotherapy
TPF vs PF NR 0.72 (0.57–0.91) 0.73 (0.56–0.94) [6]
P50.007 P50.02 TAX 323
TPF vs PF 0.73 (0.54–0.99) 0.71 (0.56–0.94) 0.70 (0.54–0.90) [5]
P50.04 P50.004 P50.006 TAX 324
aFor high-risk pathological features (extracapsular nodal extension, close/positive surgical margins, N2 or N3 nodal disease, perineural involvement, vasculartumor embolism).HR, hazard ratio; CI, confidence interval; CRT, concurrent chemoradiation; RT, radiotherapy; TPF, cisplatin, docetaxel, 5-fluorouracil; PF, cisplatin, 5-fluorouracil.
Table 2. Response Rates of Palliative Chemotherapy Agents in Advanced/Metastatic Head and Neck Cancers
Agent Response rates
Combination therapy
Cisplatin+5-fluorouracil 27–32%
Cisplatin+paclitaxel 26%
Cisplatin+cetuximab 26%
Single
Docetaxel 27%
Methotrexate 15–26%
Gemcitabinea 44%
aFor advanced nasopharyngeal carcinoma after failure of platinum-basedchemotherapy.
European Journal of Clinical & Medical Oncology
EJCMO 2010; 2:(1). FEBRUARY 2010 66 www.slm-oncology.com

8/8/2019 Chemotherapy in Head and Neck Cancers Summary of Recommendations and a Critical Review of Clinical Practice…
http://slidepdf.com/reader/full/chemotherapy-in-head-and-neck-cancers-summary-of-recommendations-and-a-critical 3/7
Table 3. Head and Neck Cancer: Indications for Chemotherapy—Levels and Sources of Evidence
Clinical scenario Treatment indicated Level of evidencea References
Lip cancer, locoregional disease, distant recurrence following salvagetreatment
Palliative CT IV NCCN [9]
NCI [16]
Lip cancer, locoregional disease, distant recurrence following localtreatment
Palliative CT IV NCCN [9]
NCI [16]
Lip cancer, metastatic disease Palliative CT IV NCCN [9]
NCI [16]
Oral cavity cancer, stage I and II, recurrence, unsalvageable disease Palliative CT IV NCCN [9]
NCI [6]
Oral cavity cancer, stage III and IV, suitable for surgery, extracapsularextension, and/or positive margins
Postoperative RT+CT I NCCN [9]
NCI [6]
CCO [27]
Oral cavity cancer, stage III and IV, suitable for surgery, no extracapsularnodal extension, and/or positive margins, recurrence, unsalvageabledisease
Palliative CT IV NCCN [9]
NCI [6]
Oral cavity cancer, stage III and IV, unsuitable for surgery Radical RT+CT I/IV NCCN [9]
Palliative CT NCI [6]
Nasopharyngeal cancer, stage I, distant recurrence Palliative CT IV NCCN [9]
NCI [14]
Nasopharyngeal cancer, stage I, definitive radiotherapy, recurrencefollowing salvage treatment
Palliative CT IV NCCN [9]
NCI [14]
Nasopharyngeal cancer, stage I, definitive radiotherapy, recurrence,unsalvageable disease
Palliative CT IV NCCN [9]
NCI [14]
Nasopharyngeal cancer, stage II, locoregional recurrence, unsalvageabledisease
Palliative CT III NCCN [9]
NCI [14]
BCCA [21]
Nasopharyngeal cancer, stage II, definitive radiotherapy, recurrencefollowing salvage treatment
Palliative CT III NCCN [9]
NCI [14]
BCCA [21]Nasopharyngeal canc er, stage II, definitive radi otherapy, distant recurrence Pall iati ve CT III NCCN [9]
NCI [14]
BCCA [21]
Nasopharyngeal cancer, stage III and IV Radical RT+CT I NCCN [9]
NCI [14]
CCO [25]
Oropharyngeal cancer, stage I and II, recurrence, unsalvageable disease Palliative CT IV NCCN [9]
NCI [15]
Oropharyngeal cancer, stage III and IV Radical RT+CT/ I NCCN [9]
Chemotherapy in Head and Neck Cancers
www.slm-oncology.com 67 EJCMO 2010; 2:(1). FEBRUARY 2010
8/8/2019 Chemotherapy in Head and Neck Cancers Summary of Recommendations and a Critical Review of Clinical Practice…
http://slidepdf.com/reader/full/chemotherapy-in-head-and-neck-cancers-summary-of-recommendations-and-a-critical 4/7
Figure 1 depicts the number of new indications forchemotherapy and shows the cumulative rise over the past 20 years.
QUALITY OF EVIDENCE AND STRENGTH OFRECOMMENDATIONS
The strength of the recommendations for chemotherapy inthe clinical practice guidelines was based first on a hierarchy of the quality of the supportive evidence used. Therecommendations with a high level of evidence were thosesupported by randomized controlled trials or systematic
reviews, whereas those with lower levels of evidence weresupported by non-randomized controlled trials, case studies,
or expert opinion. In addition, the NCCN guidelines alsoincluded whether there was uniform agreement among theirexpert panel [9]. This differed from the NCI guidelines, whichfurther defined the strength of their recommendations by the
various study endpoints (e.g., overall survival being thestrongest followed by cause-specific mortality and quality of life) from the supportive evidence used [10–16].
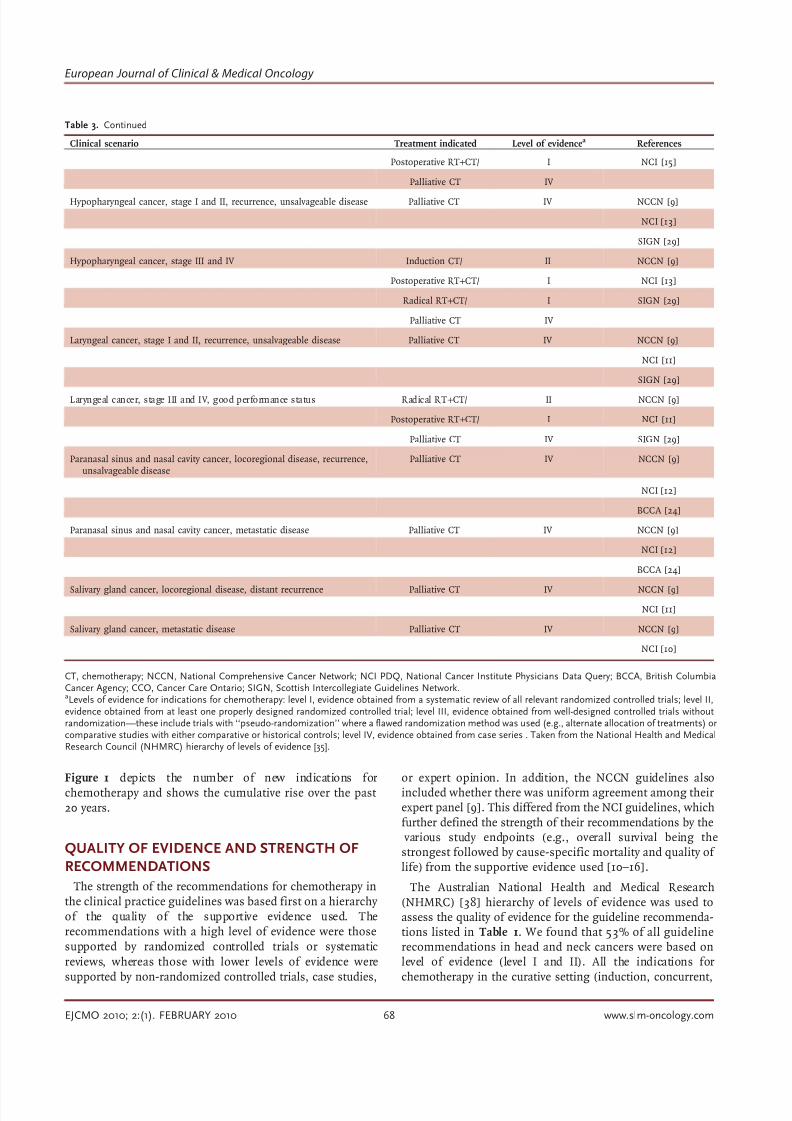
The Australian National Health and Medical Research(NHMRC) [38] hierarchy of levels of evidence was used toassess the quality of evidence for the guideline recommenda-tions listed in Table 1. We found that 53% of all guidelinerecommendations in head and neck cancers were based onlevel of evidence (level I and II). All the indications forchemotherapy in the curative setting (induction, concurrent,
Table 3. Continued
Clinical scenario Treatment indicated Level of evidencea References
Postoperative RT+CT/ I NCI [15]
Palliative CT IV
Hypopharyngeal cancer, stage I and II, recurrence, unsalvageable disease Palliative CT IV NCCN [9]
NCI [13]
SIGN [29]
Hypopharyngeal cancer, stage III and IV Induction CT/ II NCCN [9]
Postoperative RT+CT/ I NCI [13]
Radical RT+CT/ I SIGN [29]
Palliative CT IV
Laryngeal cancer, stage I and II, recurrence, unsalvageable disease Palliative CT IV NCCN [9]
NCI [11]
SIGN [29]
Laryngeal cancer, stage III and IV, good performance status Radical RT+CT/ II NCCN [9]
Postoperative RT+CT/ I NCI [11]
Palliative CT IV SIGN [29]
Paranasal sinus and nasal cavity cancer, locoregional disease, recurrence,unsalvageable disease
Palliative CT IV NCCN [9]
NCI [12]
BCCA [24]
Paranasal sinus and nasal cavity cancer, metastatic disease Palliative CT IV NCCN [9]
NCI [12]
BCCA [24]
Salivary gland cancer, locoregional disease, distant recurrence Palliative CT IV NCCN [9]
NCI [11]
Salivary gland cancer, metastatic disease Palliative CT IV NCCN [9]
NCI [10]
CT, chemotherapy; NCCN, National Comprehensive Cancer Network; NCI PDQ, National Cancer Institute Physicians Data Query; BCCA, British ColumbiaCancer Agency; CCO, Cancer Care Ontario; SIGN, Scottish Intercollegiate Guidelines Network.aLevels of evidence for indications for chemotherapy: level I, evidence obtained from a systematic review of all relevant randomized controlled trials; level II,evidence obtained from at least one properly designed randomized controlled trial; level III, evidence obtained from well-designed controlled trials withoutrandomization—these include trials with ‘‘pseudo-randomization’’ where a flawed randomization method was used (e.g., alternate allocation of treatments) orcomparative studies with either comparative or historical controls; level IV, evidence obtained from case series . Taken from the National Health and MedicalResearch Council (NHMRC) hierarchy of levels of evidence [35].
European Journal of Clinical & Medical Oncology
EJCMO 2010; 2:(1). FEBRUARY 2010 68 www.slm-oncology.com

8/8/2019 Chemotherapy in Head and Neck Cancers Summary of Recommendations and a Critical Review of Clinical Practice…
http://slidepdf.com/reader/full/chemotherapy-in-head-and-neck-cancers-summary-of-recommendations-and-a-critical 5/7
or postoperative) were based on a high level of evidence (levelI and II). Conversely, the indications for palliative chemother-apy were supported by a low level of evidence (level III or IV).
LIMITATIONS AND CONTROVERSIES INGUIDELINE RECOMMENDATIONS
Differences in recommendations and effect of changesin staging over time
The role of chemotherapy in stage 2 nasopharyngeal
carcinoma is controversial. The NCCN guidelines [9]recommend that all patients with T2aN0M0 (stage 2A)tumors should be treated with definitive radiotherapy alone.Conversely, the NCI guidelines [14] recommend that standardtreatment options for stage 2 nasopharyngeal cancer includeeither high-dose radiotherapy to the primary site and cervicalnodes or concurrent chemoradiation. The NCI guidelinerecommendation for concurrent chemotherapy was based onlevel 3 evidence (case series) and not randomized data. TheBC Cancer Agency guidelines state that radiotherapy is theprimary treatment modality and chemoradiotherapy is not standard treatment [21].
A major revision in the American Joint Committee on
Cancer (AJCC) staging for nasopharyngeal carcinoma (5thedition) in 1997 has resulted in an overall downstaging of thepopulation compared with the previous AJCC staging system(4th edition) [39]. Owing to the changes in the staging system, studies that previously enrolled locally advancednasopharyngeal carcinoma (stage 3 and 4 only) will haveincluded some stage 2 patients in the newer classification.The Intergroup study 0099 demonstrated that chemora-diotherapy significantly improved survival when compared
with radiotherapy alone in patients with locally advancednasopharyngeal carcinomas (stage 3 and 4) [40]. This study included patients with T3N0M0 and T1-3N1M0 tumors, whichare now classified as stage 2 according to the newer AJCCstaging system. However, a large phase 3 study from Hong
Kong reported in subgroup analysis that the survival benefit of concurrent chemoradiotherapy over radiotherapy alone wasseen in those with T3 and T4 disease only [41]. No differencein overall survival was found in those with T1 and T2 disease.
Difficulties in assessing performance status and
comorbidities
Performance status and comorbidities are important clinicalfactors that impact on the clinicians’ decision when
prescribing chemotherapy for patients. The prevalence of
comorbidities in the head and neck cancer population issubstantial, with up to 21% of these patients documented ashaving moderate to severe comorbidities [42]. Head and neck cancer patients with severe comorbidities have a pooreroverall survival and greater incidence of treatment complica-tions [43]. Specific guidance on the effect of comorbidities onthe recommendations for chemotherapy is currently lacking in the majority of clinical practice guidelines.
Only the NCCN guideline [9] state that palliative che-motherapy should be considered in patients who haverecurrent incurable head and neck cancers with reasonably good performance status (Eastern Cooperative Oncology
Group (ECOG) 0–2). The other clinical practice guidelines
do not provide any guidance on the effect of performancestatus on their recommendations for chemotherapy.
COMPLIANCE WITH GUIDELINERECOMMENDATIONS
Little is known about the compliance with guidelinerecommendations for chemotherapy in the management of head and neck cancers. Several large population-based studies
have described patterns of chemotherapy utilization in thehead and neck cancer population. The US National Cancer
Database reported that 15% and 17% of patients with headand neck cancers received chemotherapy as part of theirtreatment during the periods 1985–1989 and 1990–1994
Figure 1. Number of indications for chemotherapy and cumulative rise over time in head and neck cancers
Chemotherapy in Head and Neck Cancers
www.slm-oncology.com 69 EJCMO 2010; 2:(1). FEBRUARY 2010

8/8/2019 Chemotherapy in Head and Neck Cancers Summary of Recommendations and a Critical Review of Clinical Practice…
http://slidepdf.com/reader/full/chemotherapy-in-head-and-neck-cancers-summary-of-recommendations-and-a-critical 6/7
respectively [7]. This study included over 100000 patients withhead and neck cancers for each of the study periods. Theactual chemotherapy utilization rates were also analyzed by each head and neck cancer subsite for the combined periodsabove. The actual rates by subsites were lip (1%), oral cavity
(9%), nasopharynx (50%), oropharynx (22%), hypopharynx(24%), larynx (7%), paranasal sinus and nasal cavity (19%),and salivary glands (10%).
In the United Kingdom, the Northern and Yorkshire CancerRegistry and Information Service demonstrated that theoverall chemotherapy utilization rate for head and neck cancers (excluding thyroid cancers) was 12% in 2003 (averageof four cancer networks) [8]. The South Australian hospitalregistry published actual chemotherapy utilization rates forseveral head and neck subsites, which included lip (0%), oralcavity and salivary glands (8%), nasopharynx (21%), orophar-
ynx (27%), and hypopharynx (43%), for patients treatedbetween 1987 to 1998 [44].
We have reported previously that the optimal proportion of all head and neck cancer patients who should receivechemotherapy based on the best available evidence andguideline recommendations has risen significantly from 3%to 36% over the past 20 years [45]. The difference betweenoptimal and actual chemotherapy utilization rates of head andneck cancers was between 5% and 11%, with the greatest discrepancies seen in the subsites of nasopharynx, oropharynx,hypopharynx, and larynx. This suggests that potential improve-ments in the compliance with guideline recommendations forchemotherapy in head and neck cancers may be possible.
CONCLUSIONThe clinical practice guidelines have a high concordance intheir recommendations for chemotherapy in head and neck cancers, suggesting agreement between different guidelinereview committees. A high level of evidence for indications of chemotherapy (induction, concurrent, and postoperative) wasidentified in patients undergoing potential curative treatment.Conversely, the quality of evidence for palliative chemother-apy for patients with recurrent or incurable disease remainspoor and highlights the need for more research and clinicaltrials in this area. The actual compliance with guidelinerecommendations for chemotherapy in head and neck cancersis unknown, but population-based studies suggest that
chemotherapy is underutilized and that opportunities exist to improve care.
Disclosure: The authors declare no conflict of interest.
REFERENCES1. Australian Institute of Health and Welfare (AIHW) and Australasian
Association of Cancer Registries (AACR). Cancer in Australia 2003. Cancer
Series No. 37. Canberra: Australian Institute of Health and Welfare;
2007.
2. Bernier J, Cooper JS. Chemoradiation after surgery for high-risk head and
neck cancer patients: how strong is the evidence? The Oncologist . 2005;10:
215–224.
3. Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concurrent
radiotherapy and chemotherapy for high-risk squamous cell carcinoma of
the head and neck. N Engl J Med. 2004;350:1937–1944.
4. Winquist E, Oliver T, Gilbert R. Postoperative chemoradiotherapy for
advanced squamous cell carcinoma of the head and neck: a systematic
review with meta-analysis. Head & Neck. 2007;29:38–46.
5. Posner MR, Hershock DM, Blajman CR, et al. Cisplatin and fluorouracil
alone or with docetaxel in head and neck cancer. N Engl J Med. 2007;357:
1705–1715.
6. Vermoken JB, Remenar E, van Herpen C, et al. Cisplatin, fluorouracil anddocetaxel in unresectable head and neck cancer. N Engl J Med. 2007;357:
1695–1704.
7. Hoffman HT, Karnell LH, Funk GF, et al. The National Cancer Data Base
Report on Cancer of the Head and Neck. Arch Otolaryngol Head Neck Surg.
1998;124:951–962.
8. Northern and Yorkshire Cancer Registry and Information Service
(NYCRIS). Northern and Yorkshire Cancer Networks. Head and Neck
Factsheet - Incidence, Mortality, Treatment & Survival in Northern &
Yorkshire 2003. http://www.nycris.org.uk. Accessed October 10, 2007.
9. National Comprehensive Cancer Network. Clinical Practice Guidelines in
Oncology, v.1.2009, Head and Neck Cancers. http://www.nccn.org.
Accessed September 1, 2009.
10. National Cancer Institute. PDQ Cancer Information Summaries:
Treatment of Salivary Gland Cancer. http://www.nci.nih.gov. Accessed
September 1, 2009.
11. National Cancer Institute. PDQ Cancer Information Summaries:
Treatment of Laryngeal Cancer. http://www.nci.nih.gov. Accessed
September 1, 2009.
12. National Cancer Institute. PDQ Cancer Information Summaries:
Treatment of Paranasal Sinus and Nasal Cavity Cancer. http://www.nci.
nih.gov. Accessed September 1, 2009.
13. National Cancer Institute. PDQ Cancer Information Summaries:
Treatment of Hypopharyngeal Cancer. http://www.nci.nih.gov. Accessed
September 1, 2009.
14. National Cancer Institute. PDQ Cancer Information Summaries:
Treatment of Nasopharyngeal Cancer. http://www.nci.nih.gov. Accessed
September 1, 2009.
15. National Cancer Institute. PDQ Cancer Information Summaries:
Treatment of Oropharyngeal Cancer. http://www.nci.nih.gov. Accessed
September 1, 2009.
16. National Cancer Institute. PDQ Cancer Information Summaries:Treatment of Lip and Oral Cavity Cancer. http://www.nci.nih.gov.
Accessed September 1, 2009.
17. BC Cancer Agency. Cancer Management Guidelines: Cancer of the Oral
Cavity. http://www.bccancer.bc.ca. Accessed September 1, 2009.
18. BC Cancer Agency. Cancer Management Guidelines: Cancer of the Lip.
http://www.bccancer.bc.ca. Accessed September 1, 2009.
19. BC Cancer Agency. Cancer Management Guidelines: Carcinoma of the
Oropharynx. http://www.bccancer.bc.ca. Accessed September 1, 2009.
20. BC Cancer Agency. Cancer Management Guidelines: Carcinoma of the
Hypopharynx. http://www.bccancer.bc.ca. Accessed September 1, 2009.
21. BC Cancer Agency. Cancer Management Guidelines: Carcinoma of the
Nasopharynx. http://www.bccancer.bc.ca. Accessed September 1, 2009.
22. BC Cancer Agency. Cancer Management Guidelines: Cancer of the
Larynx. http://www.bccancer.bc.ca. Accessed September 1, 2009.
23. BC Cancer Agency. Cancer Management Guidelines: Cancer of the
Salivary Glands. http://www.bccancer.bc.ca. Accessed September 1, 2009.24. BC Cancer Agency. Cancer Management Guidelines: Cancer of the Nasal
Cavity and Paranasal Sinuses. http://www.bccancer.bc.ca. Accessed
September 1, 2009.
25. Cancer Care Ontario Practice Guideline Initiative. Chemotherapy with
radiotherapy for nasopharyngeal cancer: a clinical practice guideline
(evidence-based series #5–7). http://www.cancercare.on.ca. Accessed
September 1, 2009.
26. Cancer Care Ontario Practice Guideline Initiative. Concomitant che-
motherapy and radiotherapy in squamous cell head and neck cancer
(excluding nasopharynx). http://www.cancercare.on.ca. Accessed
September 1, 2009.
27. Cancer Care Ontario Practice Guideline Initiative. The role of post-
operative chemoradiotherapy for advanced squamous cell carcinoma of
the head and neck: a clinical practice guideline. (evidence-based series
#5–10). http://www.cancercare.on.ca. Accessed September 1, 2009.
European Journal of Clinical & Medical Oncology
EJCMO 2010; 2:(1). FEBRUARY 2010 70 www.slm-oncology.com

8/8/2019 Chemotherapy in Head and Neck Cancers Summary of Recommendations and a Critical Review of Clinical Practice…
http://slidepdf.com/reader/full/chemotherapy-in-head-and-neck-cancers-summary-of-recommendations-and-a-critical 7/7
28. Cancer Care Ontario Practice Guideline Initiative. The role of neoadjuvant
chemotherapy in the treatment of locally advanced squamous cell
carcinoma of the head and neck (excluding nasopharynx). http://
www.cancercare.on.ca. Accessed September 1, 2009.
29. Scottish Intercollegiate Guidelines Network. Diagnosis and management
of head and neck cancer. A national clinical guideline. http://
www.sign.ac.uk. Accessed September 1, 2009.30. Gibson MK, Forastiere AA. Reassessment of the role of induction
chemotherapy for head and neck cancer. Lancet Oncol. 2006;7:565–574.
31. Seiwert TY, Cohen EEW. State-of-the-art management of locally advanced
head and neck cancer. Br J Cancer. 2005;92:1341–1348.
32. Pignon JP, Bourhis J, Domenge C, Designe L, MACH-NC Collaborative
Group. Chemotherapy added to locoregional treatment for head and neck
squamous cell carcinoma: three meta-analyses of updated individual
data. Lancet. 2000;355:949–955.
33. Pignon JP, Maire AL, Bourhis J, MACH-NC Collaborative Group. Meta-
analyses of chemotherapy in head and neck cancer (MACH-NC): an
update. Int J Radiat Oncol Biol Phys. 2007;69:S112–S114.
34. Baujat B, Audry H, Bourhis J, et al. Chemotherapy as an adjunct to
radiotherapy in locally advanced nasopharyngeal carcinoma. Cochrane
Database of Systematic Reviews Issue 4.
35. Baujat B, Audry H, Bourhis J, et al. Chemotherapy in locally advanced
nasopharyngeal carcinoma: an individual patient data meta-analysis of eight randomized trials and 1753 patients . Int J Radiat Oncol Biol Phys.
2006;64:47–56.
36. Colevas AD. Chemotherapy options for patients with metastatic or
recurrent squamous cell carcinoma of the head and neck. J Clin Oncol.
2006;24:2644–2652.
37. Zhang L, Zhang Y, Huang PY, et al. Phase II clinical study of gemcitabine
in the treatment of patients with advanced nasopharyngeal carcinoma
after the failure of platinum-based chemotherapy. Cancer Chemother
Pharmacol. 2008;61:33–38.
38. National Health and Medical Research Council. Guide to the Development,
Implementation and Evaluation of Clinical Practice Guidelines, Appendix B.
Canberra: National Health and Medical Research Council; 1998:56.
39. Cooper JS, Cohen R, Stevens RE. A comparison of staging systems for
nasopharyngeal carcinoma. Cancer. 1998;83:213–219.
40. al-Sarraf M, Leblanc M, Giri PG, et al. Chemoradiotherapy versus
radiotherapy in patients with advanced nasopharyngeal cancer: phase IIIRandomized Intergroup Study 0099. J Clin Oncol. 1998;16:1310–1317.
41. Chan ATC, Leung SF, Ngan RKC, et al. Overall survival after concurrent
cisplatin-radiotherapy compared with radiotherapy alone in locoregion-
ally advanced nasopharyngeal carcinoma. J Natl Cancer Inst. 2005;97:536–
539.
42. Piccirillo JF. Importance of comorbidity in head and neck cancer.
Laryngoscope. 2000;110:593–602.
43. Piccirillo JF, Vlahiotis A. Comorbidity in patients with cancer of the head
and neck: prevalence and impact on treatment and prognosis. Curr Oncol
Rep. 2006;8:123–129.
44. SA Cancer Registry. Epidemiology of Cancer in South Australia. September
2000 (Cancer Series No. 22). Adelaide: South Australian Cancer Registry;
2000.
45. Ng W, Jacob S, Delaney G, Barton M. Estimation of an optimal
chemotherapy utilisation rate for head and neck carcinoma: setting an
evidence-based benchmark for the best-quality cancer care. Eur J Cancer.
2009;45:2150–2159.
Chemotherapy in Head and Neck Cancers
www.slm-oncology.com 71 EJCMO 2010; 2:(1). FEBRUARY 2010